
Acute otitis media - DiVA Portal
57
1 Umeå University Medical Dissertations New series No 868*ISSN 0346-6612*ISBN 91-7305-569-7 From the Department of Clinical Sciences, Otorhinolaryngology, Umeå University, Umeå; Department of Otorhinolaryngology, The Jubileum Institute, Lund University, Lund; Department of Otorhinolaryngology, Sundsvall, Sweden Experimental Acute Otitis Media Aspects on treatment, protection and structural changes Eva Westman Umeå University 2003
Transcript of Acute otitis media - DiVA Portal
1
Umeå University Medical Dissertations
New series No 868*ISSN 0346-6612*ISBN 91-7305-569-7
From the Department of Clinical Sciences, Otorhinolaryngology, Umeå University, Umeå;Department of Otorhinolaryngology, The Jubileum Institute, Lund University, Lund;
Department of Otorhinolaryngology, Sundsvall, Sweden
Experimental Acute Otitis Media
Aspects on treatment, protection and structuralchanges
Eva Westman
Umeå University 2003

2
Copyright © 2003 by Eva Westman
Department of Clinical Sciences, Otorhinolaryngology,Umeå University
SE-901 85 Umeå, Sweden
ISSN 0346-6612
ISBN 91-7305-569-7
Printed by Kaltes Grafiska AB, Sundsvall 2003

3
To Björn, Jonas and Alfred
When someone believes in you, and there are family and friends by your side,what seems impossible can be achieved
4
5
CONTENTSABSTRACT 6ABBREVIATIONS 7ORIGINAL PAPERS 8INTRODUCTION 9
1. Acute otitis media in humans 91.1 Definitions and diagnosis 91.2 Epidemiology 101.3 Microbiology in AOM 111.3.1 The role of viruses 111.3.2 Bacteria 111.4 Treatment of AOM 131.4.1 Background 131.4.2 Antibiotics and antibiotic resistance 141.5 Prevention 171.6 Pathogenesis 171.7 Host responses to AOM 182. Animal models for studies of middle ear pathology 192.1 Different models 192.2 Anatomy and histopathology of rat middle ear 20
AIMS 21MATERIAL AND METHODS 22
1. Animals and surgical procedures 222. Otomicroscopy 223. Experimental design 224. Bacterial strains and preparations 245. Pharmacokinetics and pharmacodynamics of amoxicillin 266. Morphological examination and tissue preparation 267. Immunoassays 278. RT-PCR 279. Statistical analysis 28
RESULTS 291. Amoxicillin treatment in recurrent AOM caused by NTHi (Paper I) 292. Amoxicillin treatment of NTHi with non-beta-lactamase-mediated
resistance (PaperII) 303. The ability of beta-lactamase-producing NTHi to shelter a penicillin-
susceptible S. pneumoniae in mixed AOM during amoxicillin treatment (Paper III) 32
4. AOM caused by M. catarrhalis (Paper IV) 34DISCUSSION 36
Question 1: Is an untreated middle ear infection better than a treated one inpromoting protective host responses? 36Question 2: Are bacteria with acquired resistance less virulent? 37Question 3: Can beta-lactamases always neutralize penicillins? 37Question 4: Are all AOM pathogens equally important? 38
CONCLUSIONS 40SUMMARY IN SWEDISH 41ACKNOWLEDGEMENTS 43REFERENCES 44PAPER I-IV

6
ABSTRACT
Acute otitis media (AOM) is a common disease in childhood and is one of the mostcommon causes for outpatient antibiotic treatment. The major aetiological agents ofAOM have varied over the decades. Now the three most common pathogens areStreptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis. Theresistance patterns of these organisms have also varied from the beginning of theantibiotic era to the situation we have today with an increasing incidence of penicillin-resistant S. pneumoniae and a moderate to high frequency of beta-lactamase productionin H. influenzae and M. catarrhalis. In Sweden we have continued to use theScandinavian treatment policy of penicillins as the first-line antibiotic treatment ofAOM, which has been implemented with good results in the past. The question is if thispolicy will continue to have acceptable treatment results.In order to investigate aspects of treatment, protection and structural changes in AOM,an animal model was used.
Amoxicillin treatment of AOM caused by H. influenzae was studied. Amoxicillintreatment was shown to shorten the duration of the infection and to reduce themorphological changes normally observed after an untreated AOM. The influence ofantibiotic treatment on recurrent AOM was evaluated. Amoxicillin treatment did notlead to less protection against reinfection. Abstaining from antibiotics did not improvethe levels of serum IgG antibodies. The IgG levels were significantly higher in treatedanimals after rechallenge. AOM caused by H. influenzae with a non-beta-lactamase-mediated resistance to beta-lactams was investigated and it was observed that duringamoxicillin treatment the chromosomal changes mediating resistance were possiblyadvantageous for the bacterium. In cultures from children with AOM, there issometimes growth of several bacteria. The possibility of a sheltering effect of beta-lactamase-producing H. influenzae on a penicillin-sensitive S. pneumoniae in a mixedinfection was investigated, and amoxicillin was shown to eradicate the pneumococcifrom the middle ear despite the presence of beta-lactamase. An increasingly culturedbacterium in nasopharynx and in AOM is M. catarrhalis. It is now beta-lactamase-producing in almost 100% of cases and is thus not eradicated by penicillins. An animalmodel of AOM caused by beta-lactamase-producing M. catarrhalis was established tostudy the course of this infection with the possibility of evaluating aspects of virulencebetween AOM pathogens. The AOM observed was a self-limiting disease.
The results obtained in this study in a rat model support the continuing use of penicillinsas first-line drugs in the treatment of AOM. Penicillins are not sufficient to treat allcausative agents, but the majority of pathogens including the most virulent bacteria areeradicated from the middle ear.
Key words: acute otitis media, penicillins, rat, treatment, protection, beta-lactamase,Moraxella catarrhalis, Haemophilus influenzae.
7
ABBREVIATIONS
AOM acute otitis mediacfu colony-forming unitsELISA enzyme-linked immunosorbent assayET Eustachian tubeIg immunoglobulinIL interleukinLOS lipooligosaccharideLPS lipopolysaccharideMBC minimum bactericidal concentrationMEE middle ear effusionMIC minimum inhibitory concentrationNTHi non-typeable Haemophilus influenzaeOME otitis media with effusionOMP outer membrane proteinPBP penicillin-binding proteinPCR polymerase chain reactionRT-PCR reverse transcribed polymerase chain reactionpcV penicillinVPMN polymorphonuclear leukocytePNSP penicillin non-susceptible Streptococcus pneumoniaeTEM transmission electron microscopyTGF transforming growth factorTM tympanic membraneTNF tumor necrosis factor

8
ORIGINAL PAPERS
This thesis is based upon the following publications and manuscripts, which will bereferred to in the text by their respective Roman numerals:
I. Westman E, Melhus Å. 2002. The treatment of Haemophilus influenzaeacute otitis media with amoxicillin protects against reinfection but notagainst structural changes. Journal of Antimicrobial Chemotherapy 49:141–147.
II. Melhus Å, Jansson H, Westman E, Hermansson A, Forsgren A, PrellnerK. 1997. Amoxicillin treatment of experimental acute otitis media causedby Haemophilus influenzae with non-beta-lactamase-mediated resistanceto beta-lactams: aspects of virulence and treatment. Antimicrobial Agentsand Chemotherapy 41: 1979–1984.
III. Westman E, Lundin S, Hermansson A, Melhus Å. 2003. Lack ofprotection of Streptococcus pneumoniae by beta-lactamase producingnontypeable Haemophilus influenzae during experimental acute otitismedia. Submitted.
IV. Westman E, Melhus Å, Hellström S, Hermansson A. 1999. Moraxellacatarrhalis-induced purulent otitis media in the rat middle ear. Structure,protection and serum antibodies. APMIS 107: 737–46.
Reprints of papers were made with the kind permission of the publishers.

9
INTRODUCTION
1. Acute otitis media in humans
Introduction
Acute otitis media (AOM) is the most common cause of antibiotic prescription forchildren in the developed world and a disease with a considerable burden ineconomic costs for society. It causes suffering in young children but hasconsequences for the whole family. The introduction of antibiotics in the treatmentof AOM had a dramatic impact and reduced the number of complications and theoverall morbidity.
But now, approximately 50 years later, we are asking ourselves whetherwe should continue with our treatment policies or not. This is a consequence of theincreasing resistance in AOM pathogens that has occurred worldwide and has led tothe increasing use of broad-spectrum antibiotics which seem to further promote thedevelopment of bacterial resistance. More recent studies of treatment of AOM,which often focus on the relief of symptoms and not the eradication of bacteria fromthe middle ear, have only shown a limited benefit of antibiotic treatment. Afterantibiotic treatment the bacteria can be eradicated from the middle ear, but theinflammation and the concurrent viral infections may still continue to givesymptoms. A confounding factor in this research area is the poor definitions ofAOM that exist and the varying diagnostic accuracy observed.
Differences occur between countries concerning incidence, prevalence ofAOM pathogens, prescription patterns and use of antibiotics. Resistant bacteriaoccur with a remarkable variation between countries which implies that treatmentpolicies play a role.
1.1 Definitions and diagnosis
Definitions
A definition of AOM that is accepted and used all over the world does not exist.One definition of AOM that has been widely used is the presence of middle eareffusion (indicated by abnormal mobility and/or position of the tympanicmembrane[TM]) and acute symptoms and signs of an infection (earache, irritability,fever, poor appetite, vomiting and/or diarrhoea). Acute discharge throughperforation of the TM or through a tympanostomy tube is also defined as AOM(Karma et al 1987, Rosenfeld & Bluestone 2003).
Otitis media with effusion (OME) is an inflammation of the middle earwith middle ear effusion (MEE) but without the acute symptoms and signsaccompanying AOM and there is no perforation of the TM (Rosenfeld & Bluestone2003).
Diagnosis
Making a correct diagnosis of AOM is often difficult, particularly in young children,and over-diagnosis of AOM is common (Garbutt et al 2003). Paediatricians fromseveral countries were evaluated for diagnostic accuracy of AOM and OME and itwas evident that they often misdiagnosed OME as AOM (Pichichero 2003). Use of

10
a pneumatic otoscope and tympanometry may reduce the number of diagnosedAOM by >30 % (Blomgren & Pitkaranta 2003). In a recent review it was found thata cloudy, bulging, or clearly immobile TM is highly suggestive of AOM and adistinctly red TM also increases the likelihood (Rothman et al 2003). The reviewalso suggests that ear pain may be an important symptom but that other symptomsare not reliable. For proper diagnosis of AOM or OME, visual examination of theTM is essential.
2.2 Epidemiology
The incidence of AOM varies and is dependent on the age of the child and theseason of the year. The highest peaks occur during the fall, winter and spring(Ruuskanen et al 1989, Pukander et al 1982). At least one episode of AOM isexperienced by approximately 50% of all children before their first birthday(Ruuskanen & Heikkinen 1994, Alho et al 1991, Sipilä et al 1987), and the peakincidence of AOM occurs between the ages of 6 to 18 months (Pukander et al 1982,Lundgren et al 1983, Sipilä et al 1987, Teele et al 1989, Alho et al 1991, Paradise etal 1997). Recurrent episodes of AOM are common, and two or more episodes werereported in 20% of infants by 6 months of age (Daly et al 1999).
In a study in Finland the occurrence of AOM increased by 68% from the1970s to the 1990s. The clinical picture of AOM has in this period become milder,with fewer febrile patients and a decreased rate of spontaneous otorrhea, butchildren are more often treated with broader spectrum antibiotics (Joki-Erkkilä et al2000).
Risk factors
Several risk factors for AOM have been identified and these vary in different studiesdepending on the environment. Host-related factors are young age (Jero & Karma1997), male sex (Teele et al 1989) and genetic predisposition (Casselbrant et al1999, Kvaerner et al 1997). Other factors are attendance at day care (Alho et al1990), parental smoking (Stenström et al 1993), not being breast-fed (Duncan et al1993, Duffy et al 1997), siblings (Varon et al 2000) and the use of pacifiers(Niemelä et al 1995, Uhari et al 1996).
Complications
The acute complications of AOM may be intratemporal or intracranial.Intratemporal complications include mastoiditis, facial paralysis, petrositis andlabyrinthitis, while intracranial complications include meningitis, extraduralabscesses, subdural empyema, focal otitic encephalitis, brain abscess, dural sinusthrombosis and otic hydrocephalus (Rosenfeld & Bluestone 2003). The frequency ofcomplications due to AOM was higher in the early antibiotic era than is reportedtoday.
In the 1950s, 17 % of children who were not treated with antibiotics developedmastoiditis (Rudberg 1954). In a Danish study the clinical picture of mastoiditisfrom 1977 to 1996 had changed. During the last 10-year period there was fewercases of AOM in the childrens background, shorter duration of hospitalisation, andthe more frequent presence of Streptococcus pyogenes (Petersen et al 1998). Themost common organisms recovered from cultures in mastoiditis are S. pneumoniae

11
and S. pyogenes (Spratley et al 2000, Luntz et al 2001). It is interesting to note thata multinational survey showed that the incidence rate of acute mastoiditis in theNetherlands, where a restrictive antibiotic policy is advocated for AOM, is slightlyhigher than in many countries with higher antibiotic prescription rates (Van Zuijlenet al 2001).
1.3 Microbiology in AOM
1.3.1 The role of viruses
A viral respiratory infection often precedes AOM episodes. In particular, respiratorysyncytial-virus, influenza A and B, and adenovirus infections confer an increasedrisk of AOM in the following 2 weeks (Heikkinen et al 1995). Viruses have beenisolated from the MEE in 40% of cases (Canafax et al 1998) but as a sole pathogenonly in 6% (Heikkinen 2000). The detection of viruses has conventionally rangedbetween 30% and 50%, but a recent study using antigen detection and PCR forseveral viruses could document viral infection in the nasopharyngeal specimens of90% of the children with AOM (Heikkinen & Chonmaitree 2003).
Although AOM in many children is diagnosed concurrently with upperrespiratory tract infection, the development of AOM only occurs after a certain timeinterval after the onset of the viral infection. After onset of upper respiratoryinfection in children attending day care the highest incidence of AOM was observedon day 3 and 75% were diagnosed during the first week after the onset of respiratorysymptoms (Ruuskanen & Heikkinen 1994). During respiratory infection the balanceof normal bacterial flora in the nasopharynx is altered with an increase in AOMpathogens and a decrease in the non-pathogen bacterial flora (Faden et al 1990).
1.3.2 Bacteria
The most common method for obtaining bacterial cultures is nasopharyngeal swabs.The ideal is to be able to culture from the MEE directly, and that may be possible inthe draining ear but is more difficult with an intact TM. Today tympanocenthesis isnot done routinely and nasopharyngeal swabs are thus the method available inroutine practice. Bacteria cultured in the nasopharynx are correlated to thepathogens found in AOM in MEE, but the nasopharynx is not a sterile location. Thehuman nasopharynx is a natural reservoir for AOM pathogens (Stenfors & Raisanen1990) and these could be acquired from 31% of healthy infants at 2 months, from49% at 6 months and from 62% at 10 months of age (Aniansson et al 1992).Colonisation is a dynamic process with a change in bacterial strains over time(Faden et al 1995). Bacterial species such as Streptococcus viridans and anaerobicstreptococci, which may have inhibitory activity against potential pathogens, alsocolonise the nasopharynx (Brook & Gober 1998, Tano et al 2000).
In the first half of the twentieth century the most frequently isolatedbacterium in AOM was S. pyogenes but since the 1950s it has become less common(Haugsten & Lorentzen 1980). Now the major pathogens in AOM are S.pneumoniae, Haemophilus influenzae and Moraxella catarrhalis (Jacobs et al1998). Of these S. pneumoniae and H. influenzae have been isolated as majorcausative agents all over the world, while the occurrence of M. catarrhalis showsconsiderable differences between geographic regions (Kamme et al 1971, DelCastillo et al 1996, Bluestone et al 1992, Del Beccaro et al 1992, Kilpi et al 2001).
12
In varying degrees two or more bacterial species are isolated from middle ears inAOM and this can occur in a small percentage to 29% in a recent study (Ruohola etal 2003). The duration of MEE was longer in children with two or more bacterialtypes, compared to those with only one pathogen or in whom no pathogen wasdetected. One-quarter to one-third of bacterial cultures in AOM yield no growth ordisplay only non-pathogens such as Staphylococcus epidermidis or diphteroides, butthe detection of pathogens depends on culture methods (Del Beccaro et al 1992).
Streptococcus pneumoniae
S. pneumoniae was identified as an AOM pathogen in the late 1800s. It was roughlyas common as S. pyogenes up to the 1950s, after which it has been the most frequentbacteria associated with AOM (Nielsen 1945, Del Beccaro et al 1992). In the 1990spneumococci have been isolated from middle ear fluid samples obtained duringAOM in 30-50% of cases (Jacobs et al 1998).
S. pneumoniae is an encapsulated gram-positive diplo-coccus, and thecapsule is the most important virulence factor. The serotypes, 3, 6, 9, 14, 18, 19 and23 have been the most common in AOM over decades (Nielsen 1945, Orange &Gray 1993). Today S. pneumoniae is the microorganism most often associated withsevere and fatal complications in AOM (Barry et al 1999, Goldstein et al 1998,Klein 1994). Spontaneous clearance from the middle ear is approximately 20%(Klein 1993, Rosenfeld et al 1994, Howie & Ploussard 1972), the lowest of the threecommon pathogens.
Non-typeable Haemophilus influenzae
H. influenzae was first classified as a pathogen causing AOM (Wirth 1928) in 1928but more regularly after 1945 (Nielsen 1945) at least partly because of failure todetect the bacterium with special growth requirements. Now it is found in variableproportions of AOM from 10-40% (Jacobs et al 1998). In the 1950s it was alsoshown that in the majority of cases, H. influenzae is non-encapsulated (Bjuggren &Thunevall 1950).
Non-typeable H. influenzae (NTHi) strains are small gram-negativecoccobacilli, which neither produce nor have the genetic material to code for apolysaccharide capsule. Lacking a capsule, H. influenzae is thus less virulent than S.pneumoniae. Lipooligosaccharide (LOS) is a major component of the outermembrane. This endotoxin is responsible for cytokine activation in an infection andcontributes to the interaction with the host. Eight biotypes of H. influenzae havebeen identified (Kilian 1991) and the most frequently occurring in AOM arebiotypes II and III.
In a recent study of children up to 2 years of age (Kilpi et al 2001), thebacterium was associated with recurrent AOM and with older age in the child. Thecarriage rate of NTHi is high and may be up to 70% in children (Kuklinska & Kilian1984), and the bacteria occur as obligate parasites on the mucous membranes ofhumans.
Children with AOM caused by NTHi developed serum bactericidalactivity following infection. However, when a new episode of AOM caused byNTHi followed, bactericidal activity against the first isolate was not effective invitro against the second isolate (Bernstein et al 1992). The spontaneous clearance

13
rate of NTHi from the middle ear is approximately 50 % (Klein 1993, Rosenfeld etal 1994, Howie & Ploussard 1972).
Moraxella catarrhalis
M. catarrhalis (earlier Branhamella and Neisseria) was for many years regarded asa non-pathogenic organism. The organism was first described in 1896 (Frosch &Kolle 1896, Verduin et al 2002). It has been recognised as a specific pathogen inAOM since 1927 (Hart 1927) but not until the 1980s (Kovatch et al 1983) was itfully recognised as an AOM pathogen. Since then the proportion of AOM associatedwith M. catarrhalis has increased up to as much as 23% of AOM cases (Kilpi et al2001).
M. catarrhalis is a gram-negative diplococcus that expresses the endotoxinLOS but lacks a capsule and is thus less virulent than S. pneumoniae. Severecomplications after AOM are rare, and the organism seldom causes serious systemicdisease (Marchant 1990, Murphy 1996). Studies indicate that the severity ofsymptoms and number of bacteria during an AOM episode appear to be lower forM. catarrhalis than for S. pneumoniae or H. influenzae (Faden et al 1992, Van Hareet al 1987).
Studies to date are in agreement that M. catarrhalis is a geneticallyheterogeneous species from which successful clones occasionally proliferate(Enright & McKenzie 1997, Verduin et al 2002). The carriage rate of M. catarrhalisis high in children, up to 75% (Verduin et al 2002, Faden et al 1994), and is higherin winter and autumn than in spring and summer (Van Hare et al 1987). Arelationship between colonisation of M. catarrhalis and the development of AOMhas also been shown (Faden et al 1994). The spontaneous clearance rate from themiddle ear is high, approximately 80% (Klein 1993, Rosenfeld et al 1994).
1.4 Treatment of AOM
1.4.1 Background
The management of AOM has recently been much debated. In part this has been aconsequence of the continued escalation in incidence of antibiotic-resistant upperairway pathogens. Antibiotics have been routinely used for the treatment of AOM inmost countries since the early 1950s. Recently this practice has been under scrutinyand several studies are conducted to measure the benefit of antibiotic treatment. Thepractice of antibiotic treatment for AOM has been questioned because of a highspontaneous resolution and wide diagnostic criteria for AOM (van Buchem et al1981, Mygind et al 1981, Del Mar et al 1997). When evaluating the natural historyof untreated AOM, about 60% of children with AOM initially managed withoutantibiotics are symptom free in 24 hours. By 2-3 days 80% are without residualsymptoms, excluding MEE. Residual MEE after AOM is common, with 65%occurrence at 2 weeks, 40% at 1 month and 25% at 3 months (Rosenfeld &Bluestone 2003). Three months after AOM no difference between the penicillin andthe placebo groups with regard to the results of otoscopy and tympanometry wereobserved (Mygind et al 1981)
Several recently published meta-analyses (Rosenfeld et al 1994, Takata etal 2001, Glasziou et al 2000) support the conclusion that antibiotics exert only amodest benefit compared with placebo for children with AOM and that there has

14
been no demonstrable superiority of any antibiotic over amoxicillin in the treatmentof this condition. The meta-analysis made in Evidence-based Otitis Media(Rosenfeld & Bluestone 2003) found that initial antibiotic therapy did not relieveAOM symptoms by 24 hours, but provided 4% greater relief by 2-3 days.Antibiotic-treated children had 9% greater symptom relief by 4-7 days. However, inchildren with pneumococcal AOM, the penicillin-treatment was shown to reducepain (Mygind et al 1981), but not in children with AOM caused by H. influenzae.The benefit of antibiotic treatment can possibly be related to bacterial species.
Several of the studies included in the meta-analyses excluded childrenunder 2 years of age, including all studies that reported outcomes at 24 hours, andthe diagnosis of AOM varied. Nearly all trials excluded children with immunedeficiencies, cleft palate, craniofacial anomalies, pre-existing OME, complicatedAOM, and concurrent bacterial infections (sinusitis, bronchitis), and some trialsexcluded children under 2 years of age, those with recurrent AOM, or those withsevere symptoms. All children with irregular clinical courses received antibiotics.Damoiseaux et al found a greater antibiotic benefit at 4-7 days for children under 2years of age compared with studies limited to older children (van Buchem et al1981, Burke et al 1991, Damoiseaux et al 2000, Rosenfeld & Bluestone 2003).When scrutinising randomly controlled trials, the children are not a random sampleof children with AOM but seem to represent a select group with less severesymptoms. Consequently, results can maybe not be broadly extrapolated to allchildren with AOM, especially not to children with severe symptoms and youngage.
1.4.2 Antibiotics and antibiotic resistance
Antibiotic resistance promotion
The major cause of antibiotic resistance seems to be the use of antibiotics. A studyin Iceland showed that mainly co-trimoxazole and erythromycin selected penicillinnon-susceptible S. pneumoniae (PNSP) in children who had received three or morecourses of treatment (Arason et al 1996). In another study co-trimoxazole wasreported to be the only antibiotic associated with a significantly increased risk ofcarriage of PNSP (Melander et al 1998). Other data obtained in Europe show thatwhen comparing antibiotic sales and PNSP, the antimicrobial resistance of S.pneumoniae to penicillins is correlated with use of beta-lactam antibiotics andmacrolides (Bronzwaer et al 2002).
The role of antibiotic treatment of AOM is to facilitate healing of infectionand avoid complications and sequelae. Antibiotics vary in their type of interactionwith the pathogens. Eradicating bacteria from the middle ear increases clinicalimprovement by about 30% compared with failure to eliminate pathogens (Carlin etal 1991, Dagan et al 1998, Marchant et al 1992).
Bacteria have a remarkable array of tools at their disposal to overcomeantibiotics. A single genetic mutation may lead to resistance with only slightalterations of the pathogenicity or viability of the bacterial strain. The extent towhich bacteria develop resistance to antimicrobial drugs vary, but so far resistancehas developed to all antimicrobial drugs.
15
Penicillins
The story begins in 1928 when Alexander Fleming described a substance he calledpenicillin that had the ability to eradicate bacteria (Fleming 1929). Several yearspassed until the research began in earnest during the Second World War. In 1953 abiosynthetic penicillin fenoximetylpenicillin, or penicillinV (pcV) was constructedwhich was an important step forward for oral treatment opportunities. The core ofthe penicillin molecule was synthesised in 1959 and a number of semi syntheticpenicillins were thereafter manufactured, among them ampicillin and amoxicillin.
Penicillins belong to the beta-lactam class. These drugs act by a time-dependent killing mechanism; that is, they must reach concentrations in the MEEthat are above the MIC of the pathogen and remain above this concentration for atleast 40-50% of the dosing interval (Craig & Andes 1996).
Since the beginning of the antibiotic era, pcV has been a first-line drug intreatment of AOM in Scandinavia and continues to be. Motives to keep pcV havebeen low cost, bactericidal effect, few adverse effects and a low tendency forinducing bacterial resistance. The narrow antibacterial spectrum seems to be ofimportance in not promoting PNSP, even though several studies have shown acorrelation with beta-lactams and development of bacterial resistance (Bronzwaer etal 2002, Nasrin et al 2002). The disadvantages with the use of pcV are the lowabsorption from the gastro-intestinal tract (ca 50%), the high degree of proteinbinding (80%) resulting in a low free microbiologically active part, the limitedantibacterial spectrum against gram-negative bacteria and the bad taste of the oralmixtures.
In the 1970s, ampicillin and amoxicillin were found to be effective againstS. pneumoniae and H. influenzae. Amoxicillin displaced ampicillin due to the lowerincidence of diarrhoea. Amoxicillin has been the recommended drug for initialroutine empiric therapy of uncomplicated AOM for 25 years in the United Statesbecause of its clinical efficacy and long record of safety. It is highly effectiveagainst S. pneumoniae and displays the best pharmacodynamic profile against PNSPof any of the commonly available oral antimicrobial agents (Craig & Andes 1996).Pharmacodynamic studies indicate that with higher doses of amoxicillin (70-90mg/kg/day vs. 40-45 mg/kg/day), higher middle ear concentrations are achieved andthese are sufficient to eliminate PNSP (Lister et al 1997, Canafax et al 1998). Whencomparing pcV and amoxicillin, amoxicillin is better absorbed from the gastro-intestinal-tract and reaches higher middle ear concentrations. The half-life ofamoxicillin is longer and the protein binding is lower (Block 1995, Craig 1996). Iferadication of bacteria from the middle ear is to be achieved in AOM caused by H.influenzae, amoxicillin is a better choice than pcV (Howie 1985). Amoxicillin,however, has more adverse effects and a broader anti-bacterial spectrum.
Adding the beta-lactamase inhibitor clavulanate to amoxicillin is a methodto neutralise the beta-lactamases produced by H. influenzae and M. catarrhalis. Datasupport the efficacy of amoxicillin-clavulanate to eradicate beta-lactamaseproducing H. influenzae from the middle ears. For M catarrhalis the data arelimited, and it is not possible to conclude that amoxicillin-clavulanate is superior toamoxicillin (Dagan et al 2001), in part due to the high spontaneous clearance rates.
16
The Scandinavian treatment policy
A roundtable conference in Helsingborg in 1966 was the starting point in theprocess leading to the Swedish or Scandinavian policy of treatment with pcV. Theconference led to an article (Juhlin et al 1967) on the question of the adequate doseof penicillin with the recommendation from the conference that the dose should beat least double the earlier recommended dose. Research followed and the dosage ofpcV was tested in clinical studies (Lundgren et al 1967, Kamme et al 1969). Theresults were in concordance with the conference recommendation. The doubleddose, 52 mg/kg/day, meant a treatment outcome of 88%, independent ofbacteriological aetiology. Further studies showed later that it was possible to reducethe treatment period from 10 days to 5 days and from administration 3-4 times perday to 2 times daily with the same treatment outcome (Rundcrantz & Sundför 1974,Ingvarsson et al 1980, Ingvarsson & Lundgren 1982). With the higher dose regimethe MICs for S. pneumoniae, S. pyogenes and M. catarrhalis were cleared by thepenicillin concentration in the middle ear with a broad margin and the MICs clearedfor H. influenzae in 90% of cases. The treatment policy recommends pcV as thefirst-line therapeutic choice, in a high dose regime (50mg/kg/day) twice or threetimes daily to children and adults, with a treatment period of 5 days in AOM. Thispolicy is still being used despite the increasing bacterial resistance.
Pneumococcal resistance
The mechanism of pneumococcal resistance to penicillin G and other beta-lactamantibiotics involves alterations in one or more of the penicillin-binding proteins(PBPs) causing their lowered affinity to beta-lactam antibiotics. All beta-lactamsexert their effect by binding to enzymes in the bacterial cell wall so that the buildingof the cell wall is stopped.
The prevalence of resistant strains of the common AOM pathogens isincreasing. One of the most alarming changes has been observed among strains of S.pneumoniae. In the 1940s, all S. pneumoniae strains were susceptible to penicillin. Itwas not until the 1960s that reports of strains of pneumococci with intermediatelevels of penicillin resistance began to appear (Appelbaum 1992). Now theprevalence of S. pneumoniae with reduced susceptibility for penicillin varies withhigh prevalence (30-40%) in some regions, notably southern Europe, and lowprevalence in other regions (Gehanno et al 2001, Hoban et al 2001). In Sweden theprevalence of PNSP is <10% according to STRAMA (Swedish StrategicProgramme for the Rational use of Antimicrobial agents and Surveillance ofResistance, www.strama.org, www.srga.org).
Resistance among gram-negative bacteria
Beta-lactamases are enzymes capable of hydrolysing the beta-lactam ring ofpenicillins, and related antimicrobial drugs, rendering them inactive. There aredozens of beta-lactamases which vary in substrate specificity, host range anddifficulty to treat.
In M. catarrhalis two types of beta-lactamases can be found (Verduin et al2002), and recent studies have suggested that one of these beta-lactamases may havea gram-positive origin which makes M. catarrhalis the first gram-negative bacterialspecies possessing such a beta-lactamase (Bootsma et al 1999). The beta-lactamases

17
from M. catarrhalis have also been shown to be able to shelter concomitant bacteriaby inactivating penicillin therapy (Hol et al 1994). In the beginning of the antibioticera this pathogen was penicillin susceptible but has since then aquired beta-lactamase producing capability. Today 90% or more of all isolates are beta-lactamase producing (Manninen et al 1997).
H. influenzae has two different mechanisms of antibiotic resistance. Themost common mechanism of resistance is the production of beta-lactamase (Bruntonet al 1986, Medeiros et al 1986). Another mechanism for resistance to ampicillin isa structural alteration of the PBPs (Clairoux et al 1992) that is chromosomallymediated. Beta-lactamase production is increasing in the world but varies betweencountries. In Finland beta-lactamase production increased from 8% to 24% over 5years (Manninen et al 1997) and in the United States a prevalence of 47% (Jacobs etal 1998) has been observed. Overall in 15 countries 17% of isolates have beenidentified as beta-lactamase positive (Bandak et al 2001).
1.5 Prevention
There exists no method with complete success in prevention of AOM. Severalmethods are used including antimicrobial prophylaxis (Williams et al 1993,Rosenfeld & Bluestone2003) and tympanostomy tube insertion with or withoutadenoidectomy (Gonzalez et al 1986, Casselbrant et al 1992, Rosenfeld &Bluestone 2003). Tympanostomy tube insertions may reduce the incidence of newAOM by 50% – 60% (Rosenfeld & Bluestone 2003). Modification of risk factorsmay also decrease AOM (Niemelä et al 2000).
Opportunities exist for immunoprophylaxis by targeting viral respiratorypathogens and bacterial otopathogens. Passive immunisation with differentimmunoglobulins has not had any proven effect on recurrent AOM (Kalm et al1986, Jörgensen et al 1990, Shurin et al 1993). Vaccines for preventing diseasecaused by S. pneumoniae have focused on the capsule even though each of thedescribed 90 serotypes has a unique polysaccharide composition with limited cross-reaction among serotypes. The earlier available vaccines against S. pneumoniaehave not shown any clinically efficient prevention of AOM (Mäkelä et al 1980).Now new conjugated pneumococcal vaccines are available and have been tested inclinical studies. The reduction was 6 % on overall AOM, 34% of the episodes thatwere caused by pneumococci, and 57% reduction on AOM caused by thepneumococcal serotypes included in the vaccine (Eskola et al 2001). Findings inthese studies support the principle that high serum antibody concentrations result inbetter protection for AOM.However, intervention strategies that target only a selected population of bacterialotopathogens are likely to have a limited effect as replacement of bacterial strains isobserved that will potentially reduce the benefit of immunization (Veenhoven et al2003).
1.6 Pathogenesis
The correlation between the pathogens found in the nasopharynx and in the MEE(Loos et al 1989) indicates that the bacteria in AOM originate in the nasopharynx.The middle ear cavity is normally a sterile compartment which is maintained by themucociliary system together with the enzymes and antibodies secreted by theepithelial cells of the Eustachian tube (ET) and the middle ear (Lim et al 2000).
18
Abnormal anatomy and dysfunction of the tube are involved in the development ofAOM (Bylander-Groth & Stenström 1998). An infection in the nasopharynx and ETlead to increased mucous secretion that can obstruct the ET resulting in a negativemiddle ear pressure (Bluestone 1996), and the bacteria can then enter the middle ear.
The bacteria then stimulate the host cellular responses leading to cytokinesynthesis and a modulation on inflammatory cells (Henderson et al 1996).Cytokines are bioactive proteins that regulate proliferation, chemotaxis, and theactivation of inflammatory cells (Nicod 1993). The pro-inflammatory cytokines areTNF-α, IL-1 and IL-6, while others are anti-inflammatory like IL-10 or TGF-β. IL-1β is the earliest cytokine detected in MEE (Sato et al 1999) and the concentrationof IL-1 decreases during antibiotic treatment on days 4-5 (Barzilai et al 1999).
The inflammatory process has now started which is critical for thedestruction of bacteria but it may also lead to mucosal damage in the host withscarring and polyp formation (Patel et al 1993). Vasodilatation occur (Robbins &Cotran 1979) and within 30 minutes the neutrophils transmigrate from the vessels.The cytokines also causes structural changes of the endothelial cell layer and laterthe tissues are infiltrated by monocytes and T-cells (Pober & Cotran 1990) and B-cells are recruited to the middle ear.
TGF-β is a potent multifunctional cytokine which regulates the proliferation of cells,embryonic development, wound healing, and angiogenesis (Dhainaut et al 2003,Fjellbirkeland et al 2003). TGF-β has well known anti-inflammatory and immune-suppressive properties. It is also capable of promoting inflammation whosesustained production underlies the development of tissue fibrosis (Dhainaut et al2003). TGF-β can influence the process of T-cell migration and activation in localinflammation (Ludviksson & Gunnlaugsdottir 2003). In a murine model TGF-β wasshown to regulate airway responses via its effects on T-cells (Schramm et al 2003).TGF-β has an important role in bone modelling and the development of bone quality(Geiser et al 1998).
1.7 Host responses to AOM
There are systemic and local immune reactions involved in the human immuneresponse. In the middle ear mucosa, which is a part of the respiratory system, thehealthy mucosa only has a few lymphocytes and no lymphoid tissue. The circulatingantibodies that are secreted into the middle ear therefore play an important role inthe defence (Ryan et al 1990).
Mucosal responses
The first line of defence is the mucosa of the upper respiratory tract which acts as aphysical barrier. Multiple defence systems cooperate in controlling bacterialattachment. On the surface of these membranes there is a mucous layer that can trappathogens, cilial activity resulting in transport and epithelial cells that sheds outerepithelial layers (Wood & Davis 1980). Nasopharyngeal colonization with bacterialpathogens stimulates the production of mucosal as well as serum antibodies to thepathogens (Faden 2001). Decoys are presented, i.e glycoproteins, which mayprevent bacterial adhesion (Zopf & Roth 1996). Secreted immunoglobulins andcomplement ligands may also trap or coat the bacteria and prevent bacterialadherence. S-IgA, IgM and IgG take part in this process (Brandtzaeg 1992). Specific

19
IgA mucosal antibodies limit the duration and the frequency of colonization. Whenthe specific immune response is not mature, between 6 to 18 months, the mannose-binding lectin is also an important component responsible for this function (Turner1996).
Systemic responses
The specific immune system is divided into the B-cell system, in whichimmunoglobulins are secreted from plasma cells (mature B cells), and the T cellsystem, in which mature cytotoxic T lymphocytes kill infected cells. These systemsare not fully matured before the age of about 18 months. Secretory IgA antibodyprevents bacteria from attaching the epithelium and does not activate complement.IgG antibodies can opsonize the bacteria for phagocytosis and can activate acomplement cascade (Stenfors 1999). It has been observed that humoral antibodiescan prevent AOM caused by S. pneumoniae or NTHi (Barenkamp 1986, Rapola etal 2001). After unilateral middle ear infection and recovery; both ears are protectedat rechallenge with the homologous isolate because of a humoral immune response(Melhus et al 1995). In a rat model protection against ipsilateral and contralateralrechallenge following middle ear infection with S. pneumoniae has also beenreported (Svinhufvud et al 1991). Local immune responses following initial middleear infection could protect the contralateral ear, but the role of local vs. humoralimmunity could not be distinguished. Serum IgG antibodies can protect childrenagainst the development of AOM, but does not affect colonization (Faden 2001).
2. Animal models for studies of middle ear pathology
2.1 Different models
The common pathogens of AOM in humans have been extensively studied in animalmodels. The use of animal models has had a large impact on the knowledge we nowhave given the advantage of control over the animal and the microenvironment inthe disease process which enables sequential and repeated observations ofhistological, immunologic, cytological and biochemical variables.
Several different species have been used including chinchilla (Bakaletz etal 1999), rat (Hermansson et al 1988), mouse (Sabirov et al 2001), gerbil (Parra etal 2002) and guinea pig (Sato 1997). AOM models of both S. pneumoniae and H.influenzae have been established in several species, but it has been difficult todevelop an animal model for M. catarrhalis (Doyle 1989). The animals maydevelop AOM, but the bacteria are rapidly eliminated from the middle ear (Chung etal 1994, Doyle 1989, Fulghum & Marrow 1996).
It has been difficult to find an ideal animal model for studies of AOM butthe various models have made it possible to study several aspects of AOM. One ofthe most frequently used models has been the chinchilla (Giebink 1999). The middleear cavity and Eustachian tube structures of chinchillas and gerbils are similar butdiffer from those of the rat. The middle ear of the chinchilla also differs from that ofhumans mainly in that it has a multilobular tympanic cavity and patulous or semi-patulous ET (Doyle 1985). The rat has been increasingly used since the introductionof an AOM model in the 1980s (Hermansson et al 1988) due to the advantage ofinbred strains, commercially available antibodies, and near-complete genetic data.One animal that now is being increasingly studied in otitis media research is the
20
mouse, mainly because of the vast possibilities with knock-out strains for the studiesof pathogenesis (Melhus & Ryan 2003).
2.2 Anatomy and histopathology of rat middle ear
The rat middle ear has small bullae and almost horizontal ETs that are usuallyclosed. The ET mucosa contain large concentrations of goblet cells but relativelyfew mucous glands (Daniels et al 1982). The opening pressure of the rat ETcorresponds to that in humans (Hellström & Stenfors 1983). The ET is connected tothe epitympanon via two distinct tracts of ciliated and secretory cells. Rat andhuman mucosa show similarities in the distribution of the mucociliary transportsystem (Albiin et al 1986).The rat middle ear is located in the temporal bone andwell protected but its TM is easily accessible for inspection with an ordinaryotomicroscope. The three-dimensional structure of the rat tympanic cavity hassimilarities to that of man but lacks mastoid air cells and has tympanic bullae thatprotrude from the floor of the cavity (Hebel & Stromberg 1978, Hellström et al1982). The TM, with the pars tensa and the relatively large pars flaccida, forms themajor portion of the lateral wall. In the medial wall the promontory, the round andoval windows with stapes, and the tympanal opening of the ET are located. Exceptthe two tracts of ciliated and secretory cells the tympanic cavity is lined with asimple, squamous-cuboidal, non-ciliated epithelium. During pathological conditionsthis simple epithelium will change and the ciliates and secretory cells appear in largenumbers outside the tracts. The laboratory rat can develop AOM spontaneously buthas rarely done so in our hands.

21
AIMS
The aims of the present study were to explore various aspects of the Scandinaviantreatment policy in a rat model.
The specific aims were:
• To evaluate the response of AOM to amoxicillin treatment with specialreference to the otomicroscopic appearance of the TM, morphologicalchanges in the middle ear and serum-antibody response.
• To study the influence of amoxicillin treatment on recurrent AOM caused byNTHi.
• To study the effects of amoxicillin treatment on AOM induced by penicillin-resistant non-typeable H. influenzae, with both beta-lactamase-mediated andnon-beta-lactamase-mediated resistance.
• To evaluate if it is possible to eradicate a penicillin-susceptible strain of S.pneumoniae with amoxicillin when the bacteria co exist with a beta-lactamase-producing H. influenzae in the middle ear.
• To establish an animal model of AOM caused by M. catarrhalis and tocompare differences in clinical courses between AOM pathogens.
22
MATERIAL AND METHODS
1. Animals and surgical procedures
Healthy male Sprague-Dawley rats were used in all studies. When starting theexperiments the animals weighed 200-450g. The animals were kept under standardlaboratory conditions and given food and water ad libitum. For otomicroscopicexaminations or during operations, the animals were anesthetised intravenously withmethohexital or intraperitoneally with chloral hydrate. All experiments wereapproved by the Animal Ethics Committee in Lund/Malmö.
To induce AOM, bacterial inoculations were made directly into the middleear bulla. The bulla was exposed through a ventral midline incision and bluntdissection of the soft tissue. With a fine needle approximately 0.05 ml of thebacterial suspension was instilled through the bony wall. The animals were thensutured. The procedure was performed in exactly the same manner duringrechallenge.
2. Otomicroscopy
In all studies animals were inspected under an otomicroscope at various intervals.The inspections were carried out by a team member unaware of the identity of eachanimal. The status of the TM and the quality and quantity of the effusion behind theTM were evaluated. Direct visualisation of opaque fluid behind the TM wasrequired for diagnosis of AOM.
3. Experimental design
Paper I
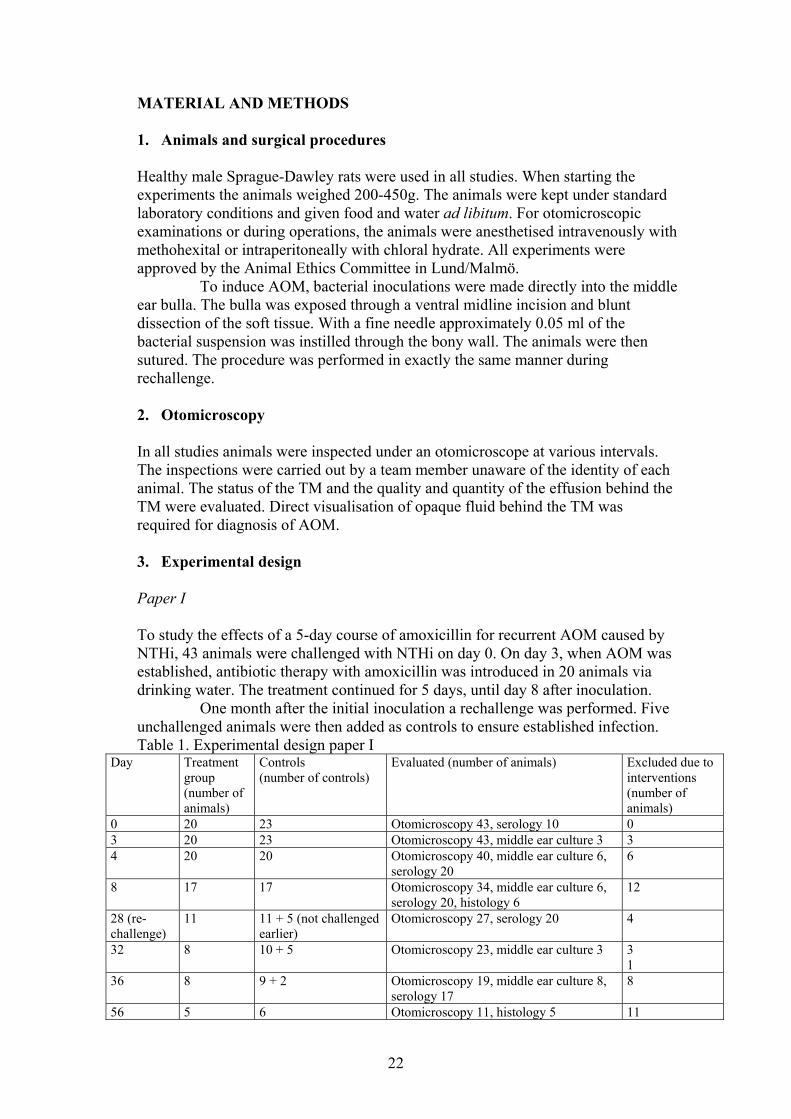
To study the effects of a 5-day course of amoxicillin for recurrent AOM caused byNTHi, 43 animals were challenged with NTHi on day 0. On day 3, when AOM wasestablished, antibiotic therapy with amoxicillin was introduced in 20 animals viadrinking water. The treatment continued for 5 days, until day 8 after inoculation.
One month after the initial inoculation a rechallenge was performed. Fiveunchallenged animals were then added as controls to ensure established infection. Table 1. Experimental design paper I
Day Treatmentgroup(number ofanimals)
Controls(number of controls)
Evaluated (number of animals) Excluded due tointerventions(number ofanimals)
0 20 23 Otomicroscopy 43, serology 10 03 20 23 Otomicroscopy 43, middle ear culture 3 34 20 20 Otomicroscopy 40, middle ear culture 6,
serology 206
8 17 17 Otomicroscopy 34, middle ear culture 6,serology 20, histology 6
12
28 (re-challenge)
11 11 + 5 (not challengedearlier)
Otomicroscopy 27, serology 20 4
32 8 10 + 5 Otomicroscopy 23, middle ear culture 3 3 1
36 8 9 + 2 Otomicroscopy 19, middle ear culture 8,serology 17
8
56 5 6 Otomicroscopy 11, histology 5 11

23
Paper II
To study the effects of amoxicillin treatment on the outcome of AOM afterchallenge with non-typeable H. influenzae strains with and without chromosomalchanges mediating reduced susceptibility to beta-lactams, 70 rats were used.
On day 0 the animals were challenged with wild-type strain 3655 (n = 35)or transformant strain 3655/4700 (n = 35). Antibiotic therapy with amoxicillin wasintroduced on day 3 in 25 animals in each challenge group. Middle ear fluid samplesfor culture were obtained from all animals on day 8 except those that were randomlyselected from the treatment groups for morphological examination.
Table 2. Experimental design paper IIDay Treatment groups (strains
3655+3655/4700) (numberof animals)
Controls (strains3655+3655/4700)(number of animals)
Evaluated (number of animals) Excluded due tointerventions(number ofanimals)
0 25 + 25 10 + 103 25 + 25 10 + 10 Otomicroscopy 35 + 354 25 + 25 10 + 10 Otomicroscopy 35 + 35,
histology 5 + 510
5 20 + 20 10 + 10 Otomicroscopy 30 + 306 20 + 20 10 + 10 Otomicroscopy 30 + 307 20 + 20 10 + 10 Otomicroscopy 30 + 308 20 + 20 10 + 10 Otomicroscopy 30 + 30,
middle ear culture 15 + 15, histology 5 + 5
50
56 5 + 5 0 Histology 5 + 5 10
Paper III
To investigate if amoxicillin treatment could eradicate pneumococci even if a beta-lactamase-producing NTHi co existed in the middle ear, a total of 78 animals werechallenged with S. pneumoniae (groups A and D), NTHi (group E) or a combinationof both bacteria (groups B and C). Forty-four animals were treated with amoxicillinwhile the remaining 34 animals served as controls.
A rechallenge was performed 1 month after the initial inoculation in whicha total of 20 animals from groups A-C were challenged in the left contralateralmiddle ear with the pneumococcal strain. At this rechallenge four unchallengedanimals were added as controls.
From day 0 to day 56 after challenge, the animals were repeatedlyinspected under an otomicroscope. Bacterial samples from the middle ears werecollected either from the ear canal of animals with spontaneously perforated TM orbilateral infections (day 3, n = 25) or by inserting a swab directly into the middle earcavity after opening up the bulla (day 8, n = 40). For histological studies animalswere sacrificed on days 3 (groups A-B, n = 3 + 3), 8 (groups A-C, n = 3 + 3 + 3) and56 (groups A-C, n = 6 + 4 + 5). Animals were also sacrificed on day 56 (groups Band C, n = 8 + 8) to study the gene expression of TGF-β.
24
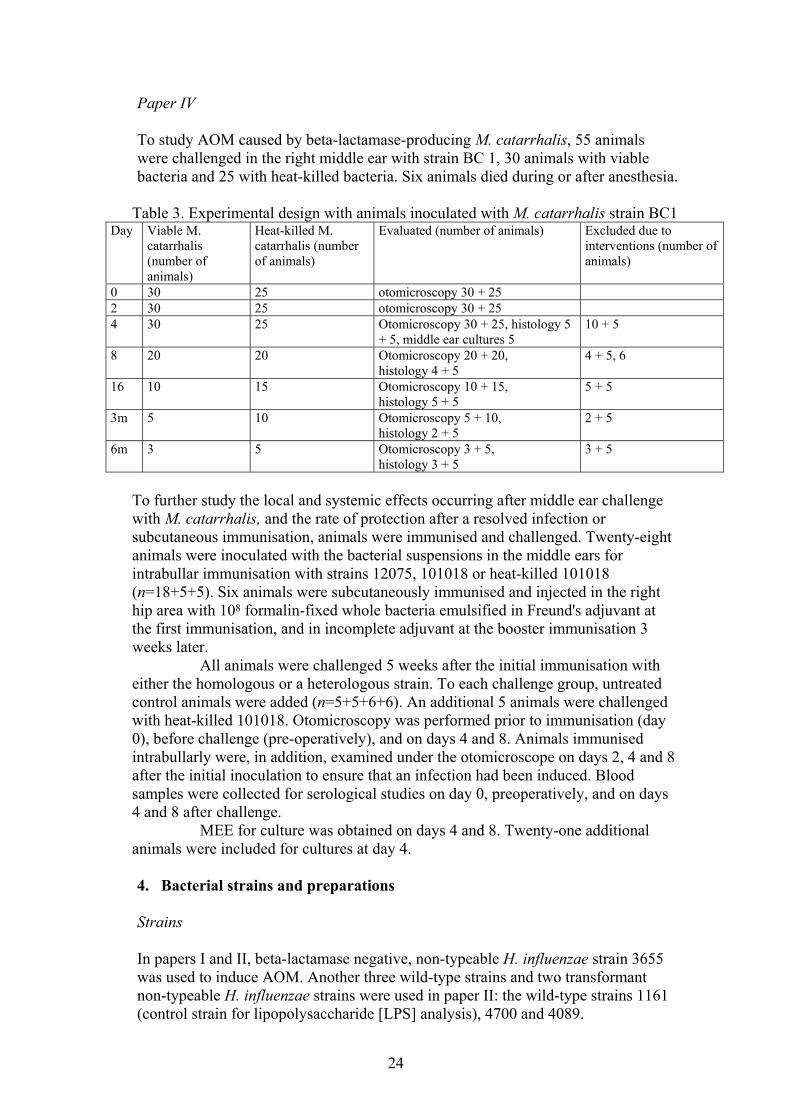
Paper IV
To study AOM caused by beta-lactamase-producing M. catarrhalis, 55 animalswere challenged in the right middle ear with strain BC 1, 30 animals with viablebacteria and 25 with heat-killed bacteria. Six animals died during or after anesthesia.
Table 3. Experimental design with animals inoculated with M. catarrhalis strain BC1Day Viable M.
catarrhalis(number ofanimals)
Heat-killed M.catarrhalis (numberof animals)
Evaluated (number of animals) Excluded due tointerventions (number ofanimals)
0 30 25 otomicroscopy 30 + 252 30 25 otomicroscopy 30 + 254 30 25 Otomicroscopy 30 + 25, histology 5
+ 5, middle ear cultures 510 + 5
8 20 20 Otomicroscopy 20 + 20,histology 4 + 5
4 + 5, 6
16 10 15 Otomicroscopy 10 + 15,histology 5 + 5
5 + 5
3m 5 10 Otomicroscopy 5 + 10,histology 2 + 5
2 + 5
6m 3 5 Otomicroscopy 3 + 5,histology 3 + 5
3 + 5
To further study the local and systemic effects occurring after middle ear challengewith M. catarrhalis, and the rate of protection after a resolved infection orsubcutaneous immunisation, animals were immunised and challenged. Twenty-eightanimals were inoculated with the bacterial suspensions in the middle ears forintrabullar immunisation with strains 12075, 101018 or heat-killed 101018(n=18+5+5). Six animals were subcutaneously immunised and injected in the righthip area with 108 formalin-fixed whole bacteria emulsified in Freund's adjuvant atthe first immunisation, and in incomplete adjuvant at the booster immunisation 3weeks later.
All animals were challenged 5 weeks after the initial immunisation witheither the homologous or a heterologous strain. To each challenge group, untreatedcontrol animals were added (n=5+5+6+6). An additional 5 animals were challengedwith heat-killed 101018. Otomicroscopy was performed prior to immunisation (day0), before challenge (pre-operatively), and on days 4 and 8. Animals immunisedintrabullarly were, in addition, examined under the otomicroscope on days 2, 4 and 8after the initial inoculation to ensure that an infection had been induced. Bloodsamples were collected for serological studies on day 0, preoperatively, and on days4 and 8 after challenge.
MEE for culture was obtained on days 4 and 8. Twenty-one additionalanimals were included for cultures at day 4.
4. Bacterial strains and preparations
Strains
In papers I and II, beta-lactamase negative, non-typeable H. influenzae strain 3655was used to induce AOM. Another three wild-type strains and two transformantnon-typeable H. influenzae strains were used in paper II: the wild-type strains 1161(control strain for lipopolysaccharide [LPS] analysis), 4700 and 4089.
25
A beta-lactamase-producing non-typeable H. influenzae strain 3144 was used inpaper III together with a penicillin-susceptible strain of S. pneumoniae type 3.
In paper IV four different strains of M. catarrhalis were used: strains BC1, 101018, 12075 and 101224.
All bacteria that were not donated from other laboratories were identifiedwith conventional methods.
Inoculum preparations for challenge
The bacteria were stored at -70°C, and all cultures were initially inoculated fromthese frozen stocks. The media used were chocolate agar, chocolate agarsupplemented with 1% enrichment (an in-house mixture corresponding toIsoVitaleX [BBL]), and 1% hemin or BHI broth or agar supplemented with NADand hemin, each at 10µg/ml, and if indicated, ampicillin at 50µg/ml.
The inocula for challenge or rechallenge of the middle ear were preparedby growing the bacteria at 37°C in an atmosphere with 5% CO2. The bacteria wereharvested by centrifugation and resuspended in fresh culture medium to an opticaldensity of 1 at 620 nm. The bacterial suspensions were thereafter diluted withsupplemented fresh medium to the varying inoculum concentrations between 103 -108 cfu/ml.
For paper IV whole cell formalin-fixed M. catarrhalis strain 12075 forsubcutaneous immunisation was prepared according to a modified version of themethod described by Green et al (1993). Three 1-ml portions of strains BC1 and101018 were heat-killed by boiling in water for 2 minutes.
Genetic transformation
Genetic transformation of H. influenzae was performed in paper II. DNA from non-typeable strains H. influenzae 4700 and 4089 was prepared by a modification(Poulsen et al 1988) of the method described by Moxon et al (1984). Non-typeableH. influenzae 3655 cells were made competent by a modified (Barnhart et al 1963)aerobic-anaerobic incubation procedure (Goodgal & Herriot 1961) and weretransformed with approximately 1µg of sheared chromosomal DNA. Thetransformation mixtures were plated, and colonies that grew on the selective agarwere purified.
Growth rate
In paper II the growth rate was assessed by measuring the turbidity of bacterialcultures in a spectrophotometer.
Determination of MIC and MBC
The determinations of MICs in paper II of penicillin V, amoxicillin, cefaclor,cefuroxime and cefotaxime were made by an agar dilution method. Antibiotics wereadded to the agar at twofold dilutions in freshly prepared solutions. Inocula wereapplied to the surface of the agar and the plates were incubated overnight.Staphylococcus aureus ATCC 29213, Escherichia coli ATCC 25922, Enterococcusfaecalis 29212 and H. influenzae NCTC 8468 were included as quality control

26
strains. The lowest antibiotic concentration which completely inhibited bacterialgrowth was recorded as the MIC.
The MICs of bensylpenicillin, ampicillin, cefuroxime and cefotaxime weredetermined by Etest (Biodisk AB, Solna, Sweden) as an extra control. The MICsand MBCs in paper III were determined by Etest.
Purification of LPS
LPS for paper II were purified by a small scale modification (Fomsgaard et al 1993)of the hot phenol-water extraction method (Westphal et al 1965) from wild typestrain 1161, 3655, 4700 and 4089 and transformed strains 3655/4700 and 3655/4089grown overnight on chocolate agar. Electrophoretic separation was then done(Schägger & von Jagow 1987), and the LPS were visualised with the Instaviewsilver staining kit (BDH Laboratory Supplies, Poole, England).
5. Pharmacokinetics and pharmacodynamics of amoxicillin
The antibiotic treatment in papers I, II and III was administered via drinking water.Amoxicillin (Imacillin; AstraZeneca, Södertälje, Sweden) was used, which is a first-line therapeutic drug in the treatment of AOM in many countries (Dowell &Schwartz 1997, Froom et al 1997). A dose of 250mg/500ml was administered, therecommended dose for rats by veterinary standards. Water consumption wasmeasured in all studies with amoxicillin treatment on a daily basis during thetreatment period.
The water consumption was followed more closely in these studies in severalanimals in whom the serum concentrations of amoxicillin were measured during twoperiods of 12 hours in each animal.
6. Morphological examination and tissue preparation
In papers I-IV middle ear tissues were examined for structural changes. In paper I the whole bullae were removed and fixation was performed in 4%paraformaldehyde for 24 hours. The middle ears were then decalcified and afterdehydration embedded in paraffin, sectioned and stained. Serial sections, in whichboth the pars tensa and the cochlea were present, were examined under lightmicroscopy. The epithelial lining of the middle ear cavity was studied. The degreeof inflammation was registered with emphasis on the presence of inflammatory cellsand vascular changes. Metaplastic changes, representing a transformation ofnormally flat epithelium into a cuboidal or cylindrical epithelium with or withoutcilia, were registered. The changes were graded as minor, moderate or extensive.After sacrifice the tympanic bullae was opened (papers II, III, IV) and the middleear cavity filled with a fixative solution containing 3% glutaraldehyde. The pieces oftissue were collected from well-defined areas of the middle ear (Hermansson et al1990) as seen in the schematic drawings of the medial upper and lateral lower wallsof the rat middle ear. (fig 1)

27
Fig 1. Schematic drawing of rat middle ear. Theareas represent (a) tympanal orifice ofEustachian tube, (b) posterior portion of sulcuspromontorialis occipitalis, (c) fossa nasalis, (d)attic space, (e) pars flaccida and (f) pars tensa.
In papers II and IV, pieces of tissue werecollected from all of these areas. Pieces werecollected from areas c and e in paper III andfrom areas b, c and e in paper I.
The tissue samples were collected under anotomicroscope and processed for microscopy.The changes were graded semi-quantitatively orthe degree of inflammation was registered withemphasis on inflammatory cells, vascularreaction, metaplasia and epithelial proliferation.
Specimens from the sulcus promontorialis occipitalis in paper IV werealso evaluated by a point-counting technique (Weibel 1989), and the relativevolumes occupied by goblet cells were determined. In addition these specimenswere sectioned for transmission electron microscopy (TEM) and the goblet cellsfurther scrutinised.
7. Immunoassays
The IgG response (paper I, III) was analysed with an enzyme-linked immunosorbentassay (ELISA). Blood samples were collected and stored at -20°C until analysed. Inpaper I the serum antibodies were measured with a previously described ELISA(Melhus et al, 1995) with modifications. Microtiter plates were coated overnightwith whole strain 3655 cells with antigen concentrations predetermined to yieldoptimal readings. The plates were blocked and after each step washed. Diluted testsera were allowed to react. Anti-rat IgG was added and the plates incubated. Theprocess was then halted and the optical densities were measured in aspectrophotometer.
Experiments were performed in triplicate and two internal controls wereincluded on each plate. The titres were averages of the three optical densityreadings. The blood samples from paper IV were also analysed with the above-described ELISA technique except that the plates were coated with whole strain101018 bacteria
8. RT-PCR
To detect the gene expression of TGF-β in paper IV, mRNA was extracted fromfrozen middle ear samples using Dynabeads Oligo (dT)25 (Dynal A.S., Oslo,Norway). After eluting the mRNA from the beads, it was reverse transcribed andamplified as described previously (Melhus & Ryan 2000) and all samples werefurther analysed in a competitive PCR assay (Melhus & Ryan 2000).

28
9. Statistical analysis
Fisher’s exact test was used for statistical analyses of the otomicroscopy results.Mann-Whitney’s test was used for statistical analysis of the quantitated pathologicaland serological findings in paper I. Student’s t-test was used for the serologicalfindings in paper III and in paper IV for comparison of mRNA-levels. A differencewas considered statistically significant if P was ≤0.05.
29
RESULTS
1. Amoxicillin treatment in recurrent AOM caused by NTHi (paper I)
Clinical observations and otomicroscopy
Apart from the middle ear infections the animals appeared clinically healthythroughout the study. The amoxicillin was well tolerated. All animals developedAOM after the first challenge and once the amoxicillin had been introduced therewas no progress of the AOM otomicroscopically.
Table 4. Otomicroscopic appearance after challenge. At day 28 rechallenge wasperformed. No: no effusion. Clear, turbid or opaque describes the appearance of theMEE behind the TM.
Treatment Day 0 Day 3 Day 8 Day 28 Day32 Day 36Amoxicillin Challenge 10 opaque 8 no
1 turbid 1 opaque
Rechallenge 6 no1 clear1 turbid
No
No treatment Challenge 10 opaque 3 clear1 turbid6 opaque
Rechallenge 7 no1 turbid2 opaque
No
After 8 days, 8 out of 10 animals in the treatment group had recoveredfully while none had in the untreated control group (P = 0.03)After rechallenge the presence of white plaques in the TMs was observed in 4animals in the treatment group.
Bacterial cultures
Table 5. Growth of NTHi in bacterial culturesDay 4 Day 8GrowthNo treatment Treatment No treatment Treatment
Abundant 3Sparse 2 1No growth 1 2 3
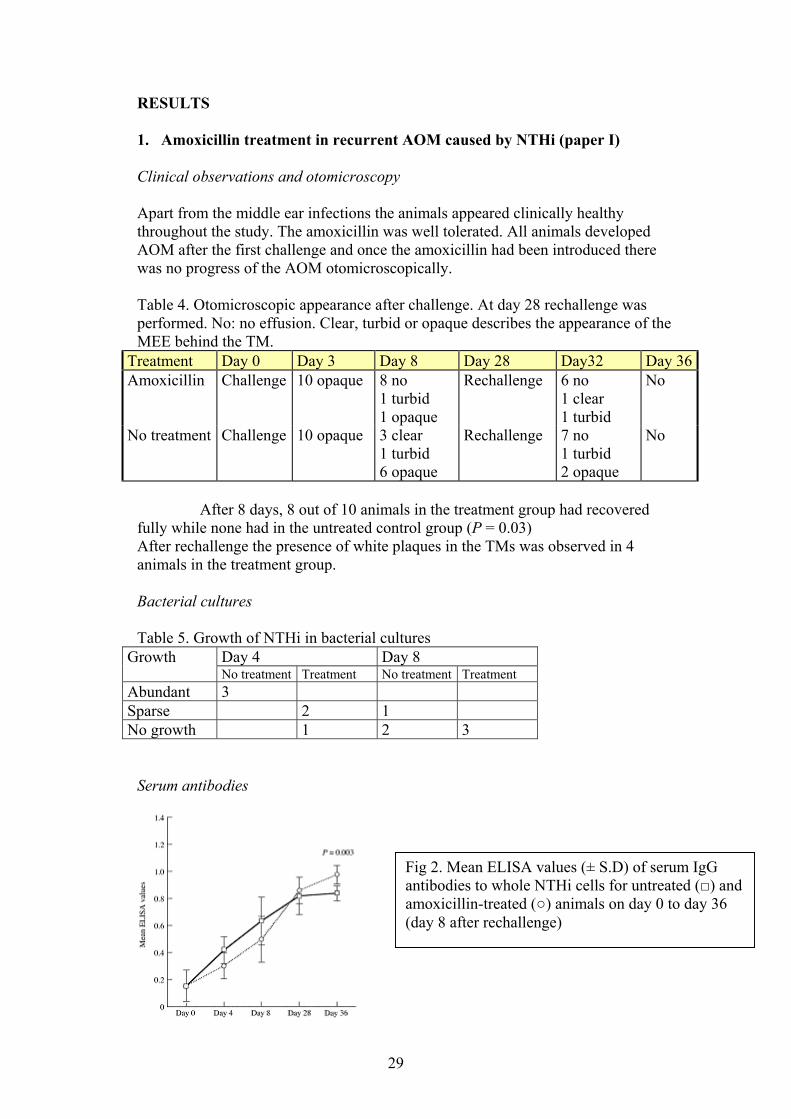
Serum antibodies
Fig 2. Mean ELISA values (± S.D) of serum IgGantibodies to whole NTHi cells for untreated (□) andamoxicillin-treated (○) animals on day 0 to day 36(day 8 after rechallenge)
30
Low levels of IgG antibodies to NTHi cells were detected in the pre-challenge sera. During the treatment period there was no significant differencebetween the ELISA values in either the treatment or no treatment groups. Allanimals developed IgG antibodies after the challenge and after 28 days the meanELISA values were similar for the two groups. After rechallenge, on day 36, theELISA values were higher in the treatment group (P = 0.003) which had receivedamoxicillin during the first middle ear infection.
Protection
After rechallenge only 2 animals developed AOM otomicroscopically, both from thepreviously untreated group (2/10). The difference in protection between the groupswas not significant and none were culture-positive.
Structural changes
The tissue samples were divided into three categories: (1) no changes, into which anunchallenged animal and 1 treated animal from day 28 were assigned; (2) minorchanges, into which treated animals from day 28 and 1 from day 56 were assigned;and (3) major changes, into which untreated animals from day 28 and treatedanimals on day 56 were assigned. The category with major changes wascharacterised by the presence of inflammatory cells, dilated vessels, metaplasia ofthe epithelium and increased numbers of goblet cells and ciliated cells.
Summary: The protection of recurrent AOM was not improved by abstaining fromantibiotic therapy.
2. Amoxicillin treatment of NTHi with non-beta-lactamase-mediatedresistance (paper II)
Characterisation of strains and growth rates
The activities of five antibiotics were tested against the various nontypeable H.influenzae strains. The degree of resistance to beta-lactams was similar amongst thedonor and the transformant strains, except in the cephalosporins.
To induce AOM the donor strains required a dose of at least 100-foldgreater than required for the recipient and the transformant strains. Despite the highconcentrations used the course of the AOM was shorter than that caused by anyother strain. Recipient strain 3655 demonstrated the highest growth rate followed bytransformant strain 3655/4700. Lowest growth rate was observed with donor strain4700.
The LPSs of the transformant strains were characterised bothphysiochemically and antigenically. The amounts of LPS expressed, theelectrophoretic mobilities and the immunoreactive patterns of the LPSs for thetransformant strains were identical to those for the recipient strain. The transformantstrain had the same biotype as strain 3655.

31
Clinical observations and otomicroscopy
Apart from the middle ear infections the animals appeared clinically healthythroughout the study. The amoxicillin was well tolerated. With antibiotics the duration of a middle ear infection caused by the fullysusceptible strain was shortened by at least 2 days compared with the course in thecontrol animals. For the animals challenged with the strain with reducedsusceptibility, recovery was not quite as rapid, especially not during the first days oftreatment. The gain in recovery time for animals treated compared with the controlanimals was at least 1 day.
Table 6. Number of animals with no effusion/normal appearance during thetreatment period as seen otomicroscopically.
Bacterialstrain
Treatment Day 3 Day 4 Day 5 Day 6 Day 7 Day 8
Amoxicillin (n=10) 1 6 10 10Wild type strain 3655 No treatment (n=10) 5
Amoxicillin(n=10) 3 5 10Transformant strain3655/4700
No treatment (n=10) 1 3 6
Bacterial cultures
All cultures of specimens from middle ears challenged with donor strains werenegative on day 8. Cultures from animals challenged with the fully susceptible strainwere negative in 9/10 after amoxicillin treatment compared with 5/10 in thecontrols. The corresponding figures for animals challenged with the strain withreduced susceptibility were 8/10 after amoxicillin treatment and 5/10 in the notreatment group.
Structural changes
The structural changes observed in animals challenged with 3655/4700 werecomparable to those seen after strain 3655 with only minor and no definitedifferences in either the quantity or the quality of the changes observed at anyobservation time. The histological changes observed in the middle ear of animalsinfected with the susceptible strain that were amoxicillin-treated were less severecompared with the changes observed after no treatment or treatment of rats infectedwith bacteria with reduced susceptibilities to beta-lactams. The most substantialdifference was that the pars flaccida of the TM exhibited a normal appearance inmost animals after 2 months (4/5 vs. 0/5 animals; P = 0.02)
Summary: Chromosomal changes mediating a relatively low level of resistance tobeta-lactams seem to be advantageous for H. influenzae during amoxicillintreatment of AOM in the rat.
32
3. The ability of beta-lactamase-producing NTHi to shelter a penicillin-susceptible S. pneumoniae in mixed AOM during amoxicillin treatment(paper III)
Clinical observations and otomicroscopy
All animals developed AOM after first challenge. In 8 (10%) animals the infectionprogressed into a bilateral middle ear infection on day 4. Of these animals, 4belonged to the mixed group with no treatment, 2 belonged to the mixed group withamoxicillin treatment, and 2 belonged to the group challenged with S. pneumoniaewith no treatment. Seven (9%) animals developed a severe systemic infection andsuccumbed. Four (57%) of these animals had a bilateral infection. Of the 7 animalsthat succumbed, 2 were from the pneumococcal group and the deaths occurred early(days 3 and 4), 2 were from the group with mixed infection that were treated (theysuccumbed on days 4 and 5), and 3 were from the group with mixed infection andsuccumbed on days 4 (n=1) and 6 (n=2). The treatment significantly accelerated the resolution of the pneumococcal AOM incontrast to mixed infection. On day 8, 94% of the animals had clearedotomicroscopically, with no or clear effusion, whereas 60% of the amoxicillin-treated animals with mixed infections had cleared otomicroscopically and 45% ofthe non-treated animals. Opaque effusion could only be observed in the two groupswith mixed infection after day 7. On day 56 the presence of white plaques in the TMwas substantial in the right ear of all animals with a resolved mixed infection,independent of antibiotic therapy.
Bacterial cultures
Table 7. Bacterial cultures from day 3, when amoxicillin-treatment started, and fromday 8, at the end of the treatment periodInocula Treatment Growth on day 3 Growth on day 8Pnc Amoxicillin - 0/10Pnc/NTHi Amoxicillin - Pnc 0/11
NTHi 5/11Pnc/NTHi No NTHi 16/16
Pnc 7/16Pnc 4/10NTHi 1/10
Pnc No 3/3 3/3NTHi No 5/6 2/6
TGF-β
The expression of TGF-β differed between animal groups with mixed infections. Inthe amoxicillin-treated group the transcript levels were lower (mean 25.9 ± 11.1 fg)compared with the untreated group (mean 35.4 ± 27.5 fg), but the difference was notstatistically significant (P = 0.34)
33
Protection
Table 8. Protective rate after rechallenge in the left ear. The results are similar in thedifferent groups with no significant differences
Structural changes
The specimens were categorised and assigned to 3 groups depending on theinflammatory reaction observed. The different groups were: no or minor changes,moderate changes and major changes.
On day 3 there were 2 groups, moderate and major changes. The groupwith major changes showed a massive inflammatory response with abundantinflammatory cells.
On day 8 the degree of inflammation had decreased in 3 animals withamoxicillin treatment. The specimens with mixed infections were all but oneassigned to the category with major changes with numerous inflammatory cells stillpresent. Ciliated cells and goblet cells were increased in number and also present inthe inner epithelium of the pars flaccida.
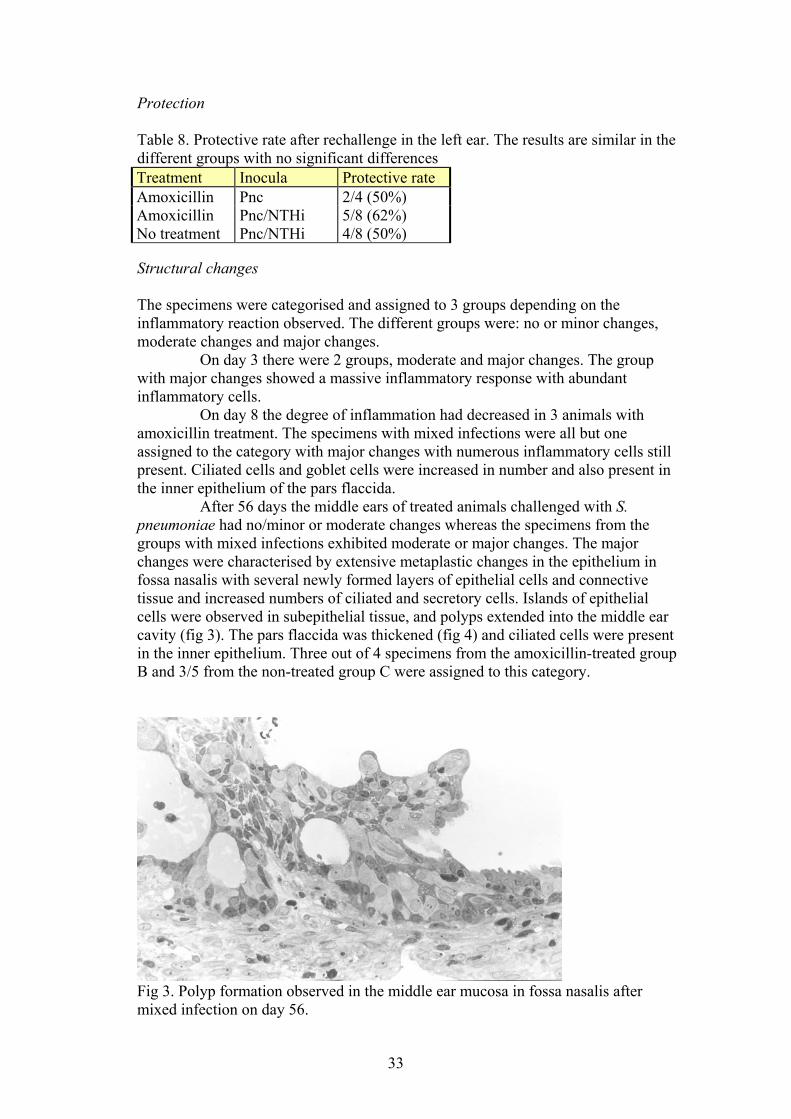
After 56 days the middle ears of treated animals challenged with S.pneumoniae had no/minor or moderate changes whereas the specimens from thegroups with mixed infections exhibited moderate or major changes. The majorchanges were characterised by extensive metaplastic changes in the epithelium infossa nasalis with several newly formed layers of epithelial cells and connectivetissue and increased numbers of ciliated and secretory cells. Islands of epithelialcells were observed in subepithelial tissue, and polyps extended into the middle earcavity (fig 3). The pars flaccida was thickened (fig 4) and ciliated cells were presentin the inner epithelium. Three out of 4 specimens from the amoxicillin-treated groupB and 3/5 from the non-treated group C were assigned to this category.
Fig 3. Polyp formation observed in the middle ear mucosa in fossa nasalis aftermixed infection on day 56.
Treatment Inocula Protective rateAmoxicillin Pnc 2/4 (50%)Amoxicillin Pnc/NTHi 5/8 (62%)No treatment Pnc/NTHi 4/8 (50%)

34
Fig 4. Pars flaccida with substantial changes after mixed infection on day 56.
Summary: The beta-lactamase producing H. influenzae did not demonstrate abilityto protect S. pneumoniae during amoxicillin treatment, but the mixed infectionappeared to increase the mucosal changes.
4. AOM caused by M. catarrhalis (paper IV)
Clinical observations and otomicroscopy
Apart from the middle ear infections the animals appeared clinically healthythroughout the study. All strains of M. catarrhalis used induced AOM at aconcentration of 108 cfu/ml. The course of a M. catarrhalis-induced middle earinfection was generally as follows: on day 2 a clear and slightly yellow effusioncould be observed otomicroscopically. Small amounts of pus-like effusion appearedin 50%. Two days later the animals presented an opaque effusion fillingapproximately 2/3 of the middle ear cavity. On day 8 a normalised status wasobserved or there were small amounts of clear or turbid fluid behind the parsflaccida. After 5 weeks no changes were noted except in animals inoculated withstrain BC 1. In these animals a transparent effusion was present on day 16, and after3 months. After 6 months all TMs appeared normal and no effusion was noted. Heat-killed bacteria generated no opaque effusion but a transparent effusion wasobserved in a majority of animals that lasted no longer than 16 days.
Bacterial cultures
Middle ear cultures, from non-immunised animals challenged with viable bacteria,on days 4 and 8 after inoculation were positive in 58% (15/26) and 12% (1/8),respectively.
Serum antibodies
Intrabullar challenge with viable strain 101018 induced the highest levels of IgGresponse. In contrast the antibody response elicited by heat-killed bacteria wasweaker. The protection against AOM did not correlate with the induced antibodyresponse.
35
Protection
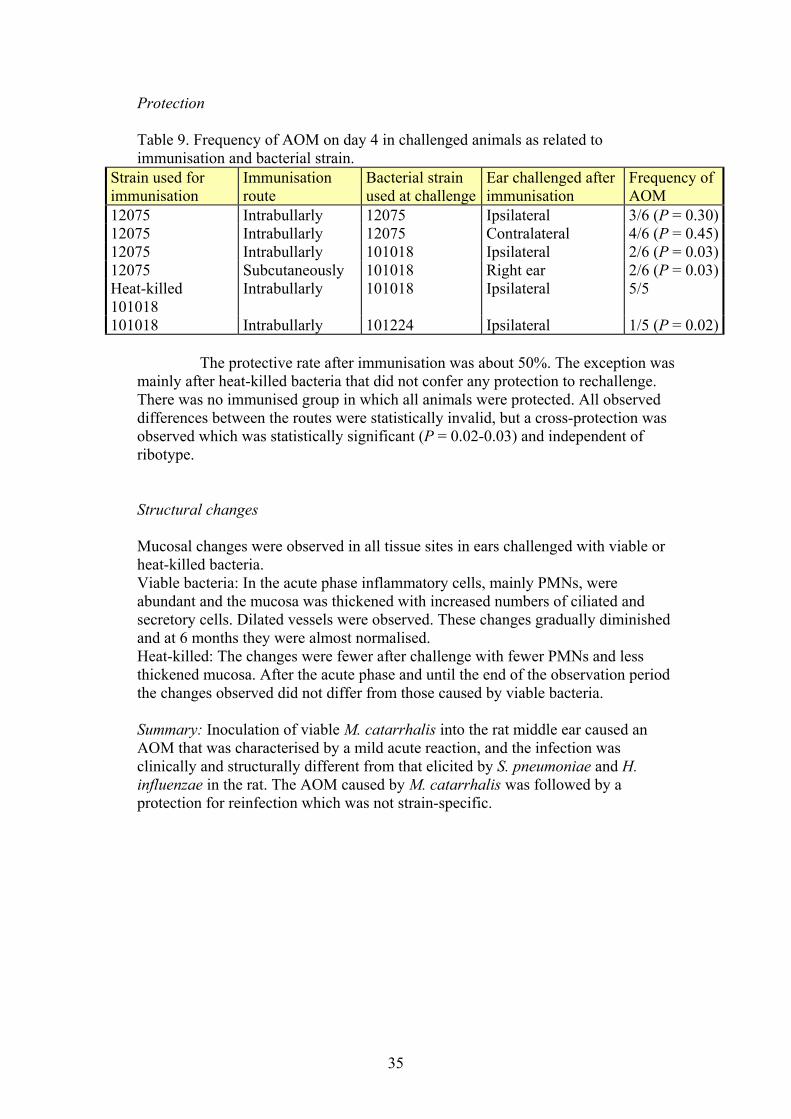
Table 9. Frequency of AOM on day 4 in challenged animals as related toimmunisation and bacterial strain.
Strain used forimmunisation
Immunisationroute
Bacterial strainused at challenge
Ear challenged afterimmunisation
Frequency ofAOM
12075 Intrabullarly 12075 Ipsilateral 3/6 (P = 0.30)12075 Intrabullarly 12075 Contralateral 4/6 (P = 0.45)12075 Intrabullarly 101018 Ipsilateral 2/6 (P = 0.03)12075 Subcutaneously 101018 Right ear 2/6 (P = 0.03)Heat-killed101018
Intrabullarly 101018 Ipsilateral 5/5
101018 Intrabullarly 101224 Ipsilateral 1/5 (P = 0.02)
The protective rate after immunisation was about 50%. The exception wasmainly after heat-killed bacteria that did not confer any protection to rechallenge.There was no immunised group in which all animals were protected. All observeddifferences between the routes were statistically invalid, but a cross-protection wasobserved which was statistically significant (P = 0.02-0.03) and independent ofribotype.
Structural changes
Mucosal changes were observed in all tissue sites in ears challenged with viable orheat-killed bacteria. Viable bacteria: In the acute phase inflammatory cells, mainly PMNs, wereabundant and the mucosa was thickened with increased numbers of ciliated andsecretory cells. Dilated vessels were observed. These changes gradually diminishedand at 6 months they were almost normalised.Heat-killed: The changes were fewer after challenge with fewer PMNs and lessthickened mucosa. After the acute phase and until the end of the observation periodthe changes observed did not differ from those caused by viable bacteria.
Summary: Inoculation of viable M. catarrhalis into the rat middle ear caused anAOM that was characterised by a mild acute reaction, and the infection wasclinically and structurally different from that elicited by S. pneumoniae and H.influenzae in the rat. The AOM caused by M. catarrhalis was followed by aprotection for reinfection which was not strain-specific.

36
DISCUSSION
In this study several questions related to the Scandinavian treatment policy wereaddressed.
Question 1: Is an untreated middle ear infection better than a treated one inpromoting protective host responses?
It is often assumed that antibiotic treatment affects the host responses negatively. Inpaper I the production of IgG antibodies was slightly affected by the amoxicillintreatment during the initial AOM induced by NTHi. However, after rechallengethere was a significantly higher serum antibody production in the earlieramoxicillin-treated animals compared with the untreated animals (fig 2.). Thebackground to this significantly increased IgG-production after rechallenge is notclear. Immune-responses are modulated by two different types of immunity. Type 1immunity is characterized by intense phagocytic activity and type 2 immunity ischaracterized by high antibody titres. Severe systemic stress or overwhelmingmicrobial load can cause an imbalance in the immune responses. Administration ofantibiotics can restore the systemic balance, which allows successful host responsesto clear the infection (Spellberg & Edwards 2001). Thus, the amoxicillin treatmentmay have initiated an earlier shift to type 2 immunity by reducing the bioburden.
High serum IgG levels do not necessarily entail a good protection. Onlyby challenging immunised animals, the protective function of mounted serumantibodies can be tested. The antibody-production after AOM and subcutaneousvaccination by M. catarrhalis was cross-protective, i.e. the protection observed wasnot only against the homologous strain, but also against heterologous strains ofvarious ribotypes. In contrast, the protection after an NTHi infection has beenshown to be strain-specific (Karasic et al 1985). NTHi is associated with recurrentAOM and older children, whereas M. catarrhalis mainly causes AOM in youngerchildren (Kilpi et al 2001). It is possible that the host only needs to be exposed to afew M. catarrhalis strains to develop adequate immune responses to all strains.
The antibiotic treatment reduced the inflammatory reaction and preventedstructural changes in the middle ear mucosa. A resolution without major structuralchanges appeared to be advantageous at renewed contact with bacteria, since theprotection in treated animals was excellent, 100%. However, after rechallengestructural changes were seen in all animals independent of earlier treatment.Therefore there seemed to be no long-term beneficial effect of antibiotic treatmenton the development of structural changes during subsequent AOM episodes.
An important participant in inflammatory processes is TGF-β, an anti-inflammatory cytokine that facilitates the anabolic effects of growth factors ontissue repair. In experimental AOM induced by NTHi, it has been demonstrated thatthe occurrence of polyps and adhesions in the middle ear coincide with higher levelsof TGF-β transcripts. Furthermore, during antibiotic treatment the expression of theTGF-β gene is decreased (Melhus 2001). In paper III, the TGF-β expression levelswere also reduced after antibiotic treatment. The reduction was not significant. Apossible explanation to this could be the resistant NTHi cells, which maintained theinflammatory process and the demand for a continued expression of TGF-β.
37
Question 2: Are bacteria with acquired resistance less virulent?
Acquisition of resistance usually costs some loss in virulence for bacteria. However,in the presence of antibiotics carriage of genes encoding resistance can give abacterial strain an advantage. Resistance in bacteria is not normally considered to bea virulence factor, but during selective antibiotic pressure these genes are importantfor the survival of a bacterium, especially when entering into competition with otherbacteria.
In papers II and III, the NTHi strains with acquired resistance toamoxicillin exhibited a reduced growth rate and a relatively low ability to persist atthe infectious site when not under a selective pressure. During amoxicillintreatment, the NTHi cells with non-beta-lactamase-mediated resistance toamoxicillin influenced the course of the AOM by delaying the resolution of thepurulent effusion. Furthermore, the late histological changes in the middle earcorresponded to those found in untreated animals challenged with the susceptiblestrain. The acquisition of chromosomal resistance mediating increased MICs ofseveral beta-lactams probably cost the micro-organisms more than the acquisition ofbeta-lactamase genes. The chromosomal resistance involves a structural alteration ofthe PBPs in the cell wall. This alteration may mediate possible defects in themetabolism or the replication of the bacterium.
Antibiotic use promotes bacterial resistance. If antibiotics are not presentthe resistant bacteria may be exchanged in the competition with other moresusceptible bacteria (Seppälä et al 1997). Widely diverse patterns of antibioticresistance can be found in adjacent countries in Europe, which suggests that nationalpatterns in the practice of medicine and prescribing may be important factors indetermining the frequency of resistance. Micro-organisms do not respect nationalboundaries. In Sweden, the resistance pattern among AOM pathogens and theirisolation frequency are probably the result of the antibiotics prescribed. PcV isefficient in eradicating S. pneumoniae but it is less efficient in eradicating gram-negative bacteria, such as NTHi and M. catarrhalis. The native NTHi population isprobably more resistant to pcV than M. catarrhalis but the beta-lactamase producedby M. catarrhalis is notably very efficient in neutralising penicillins. The highfrequency of beta-lactamase production in M. catarrhalis is probably promoted bythe ecological selection exerted by pcV. In Sweden, and also in Finland, theprevalence of M. catarrhalis in AOM is higher than in other countries where pcV isnot prescribed (Kilpi et al 2001, Gehanno et al 2001).
Question 3: Can beta-lactamases always neutralize penicillins?
The widespread use of beta-lactams has led to prevalent beta-lactamase productionamong the gram-negative pathogens. Experimental evidence exists for a shelteringeffect of beta-lactamase producing bacteria in several types of mixed infections(Brook & Gilmore 1993, Hol et al 1994).
In paper III, the beta-lactamase-producing H. influenzae did notdemonstrate an ability to protect S. pneumoniae during amoxicillin treatment. Thus,the presence of beta-lactamase-producing bacteria in a polymicrobial middle earinfection does not automatically render penicillins ineffective against otherwisesusceptible bacteria. Several studies have reported that there are differences in theability of the beta-lactamases to protect concomitant bacteria (Renneberg & Walder1989, Hol et al 1994). M. catarrhalis has been shown to produce a beta-lactamase
38
with a better degrading effect than that NTHi may harbour. It is therefore possiblethat the results obtained in paper III would have been different with a M. catarrhalisstrain instead of an NTHi strain.
With this as a background, should the spectrum of the prescribedantimicrobial drugs for AOM always cover beta-lactamase-producing bacteria? Aconsequence would be an increased use of broad-spectrum antibiotics and thereby agreater ecological impact on the gastrointestinal and nasopharyngeal flora (Brook&Gober 1998). The competition between the upper respiratory tract pathogens andcommensals in the nasopharynx may be of greater importance for the developmentof AOM and recurrent disease than earlier assumed (Roos et al 2001, Joki-Erkkilä etal 2002). It is even possible that not all beta-lactamase-producing bacteria should beeradicated, as the presence of beta-lactamase-producing M. catarrhalis appears toprevent the development of penicillin resistance among pneumococcal isolates in thenasopharynx (Joki-Erkkilä et al 2002).
Question 4: Are all AOM pathogens equally important?
To answer this question it was necessary to establish an AOM model for M.catarrhalis. In paper IV inoculation of viable M. catarrhalis into the rat middle earcaused an AOM that was characterised by a mild acute reaction. The infection wasclinically and structurally different from that elicited by S. pneumoniae and H.influenzae in the rat (Hermansson et al 1988, Melhus et al 1994, Magnusson et al1997).
Various properties of M. catarrhalis have made it difficult to develop ananimal model (Chung et al 1994, Doyle 1998, Fulghum & Marrow 1996, Melhus2003). When developing the rat model it was obvious that this bacterium must behandled delicately. It had to be used shortly after its isolation from the infectioussite, and it required high inoculation doses (Paper IV). Furthermore, the strain usedshould probably be isolated from the middle ear of an AOM patient and not from thenasopharynx of a healthy individual, since it is difficult to induce AOM in the rat inthe latter case (unpublished data).
Paper IV demonstrated that the AOM caused by M. catarrhalis is a self-limiting disease with few changes in the middle ear after resolution compared withthe other major AOM pathogens. This suggests a low virulence and it is thereforenot surprising that M. catarrhalis was not considered a pathogen until the mid 1980s(Kovatch et al 1983, Shurin & Van Hare 1986).
S. pneumoniae has the lowest spontaneous clearance rate and is the micro-organism most often associated with severe and fatal complications in AOM. Thusthe antimicrobial drug routinely used for AOM treatment must have a spectrumwhich covers this bacterium in order to be efficacious. The spontaneous clearancerates for the two other major AOM pathogens are higher and for M. catarrhalis it isapproximately 80%. Differences between the courses of AOM in the rat caused byS. pneumoniae, H. influenzae and M. catarrhalis include inoculation dose, durationof MEE, frequency of positive middle ear cultures, structural changes in the middleears, frequency of severe systemic infections, frequency of myringosclerosis, andprotection rate. These findings are similar to those found in humans.
The most pronounced structural changes observed in the rat modeloccurred after the mixed infection in paper III. It occurred both in untreated andantibiotic treated animals with polyp formation, metaplasia in the epithelium withseveral layers of cells, and presence of inflammatory cells, dilated vessels and

39
epithelial proliferation. Otherwise the most prominent inflammation on day 3, in theacute phase, was observed in middle ears challenged with S. pneumonie (paper III),with massive inflammation and deranged middle ear epithelium with dilated vessels.After the acute inflammatory reaction had abated, the long-term inflammatorychanges were most pronounced after the NTHi-induced AOM. Vascular changesand metaplasia occurred after 2 months in pars flaccida and in fossa nasalis inuntreated animals challenged with the susceptible strain and in treated animalsinoculated with the resistant strain (paper II). The morphological changes after a M.catarrhalis infection were the mildest, but the bacterium still induced a long-terminflammation.
Changes in the goblet cells after a M. catarrhalis AOM differed fromthose observed after a pneumococcal AOM, with an increased total volume ofgoblet cells and various alterations in the appearance of the goblet cell granules(paper IV). NTHi have been demonstrated to induce even more pronounced changesin the goblet cells (Magnusson et al 1997). Cayé-Thomassen and co-workers havealso shown that capsulated and non-typeable H. influenzae induce the most severeand protracted histopathologic changes, as evaluated by the increase of goblet-celldensity and the formation of polyps and fibrous adhesions. According to theirstudies, S. pneumoniae induces almost the same changes, but has a tendency topromote new bone formation. M. catarrhalis, finally, induces the slightest changes(Cayé-Thomassen & Tos 2001).
The effect on the middle ear mucosa can be an aspect of how the bacterialcell wall is constructed, and what type of toxin the bacterium therefore mainly relyon to injure the host. S. pneumoniae, which is a gram-positive bacterium, causes adirect and intense acute reaction probably through the production of exotoxins.NTHi and M. catarrhalis are gram-negative bacteria, whose endotoxin in the cellmembrane induces inflammatory host responses. Secondary to these host responses,the tissues are destroyed. Due to their endotoxin, gram-negative bacteria are capableof inducing inflammation even if they no longer multiply or are viable in the middleear (DeMaria 1999). Thus, the inflammatory process is prolonged by the residualendotoxins. When gram-positive bacteria are mixed with gram-negative bacteria,exotoxins are combined with endotoxins, and the most pronounced structuralchanges are therefore observed.
The use of the penicillins pcV and amoxicillin as first-line drugs in AOMseems to be a wise choice due to their high ability to eradicate S. pneumoniae, themost virulent bacterium. In contrast to pcV, amoxicillin is effective in eradicatingthe majority of NTHi strains and even PNSP in higher doses (Lister et al 1997,Canafax et al 1998). Beta-lactamase producing bacteria, and M. catarrhalis inparticular, are not eradicated with this treatment, but these microbes appear to beless virulent and are not a target for the initial therapy. If penicillins are used, amajority of the AOM pathogens are eradicated without the negative ecological risksof more broad-spectrum antibiotics.

40
CONCLUSIONS
Amoxicillin treatment:
• eradicated S. pneumoniae and NTHi from the middle ear.
• eradicated S. pneumoniae in the presence of beta-lactamase.
• shortened the duration of AOM caused by NTHi or S. pneumoniae.
• reduced the morphological changes normally observed after an untreatedAOM but did not prevent further tissue damage in the long run.
• did not reduce the protection against reinfection with S. pneumoniae andNTHi and induced significantly higher IgG levels after rechallenge.
• seemed to be advantageous for NTHi with beta-lactamase production andchromosomal alterations mediating a relatively low level of resistance to beta-lactams.
Moraxella catarrhalis:
• induced an AOM in the rat model that was a self-limiting disease.
• induced a protection that was not strain-specific.
In conclusion: There is still a lot that supports the Scandinavian treatment policy.Penicillins are not sufficient to treat all causative agents, but the majority of pathogensincluding the most virulent bacteria are eradicated from the middle ear.
41
SUMMARY IN SWEDISH
Bakgrund: Öroninflammation är en av barnaårens vanligaste sjukdomar. Den ärockså den enskilt vanligaste orsaken till antibiotikabehandling av små barn. Denleder till lidande hos barnet och orsakar stora kostnader för samhället.
Öroninflammationen kommer vanligen efter en övre luftvägsinfektionorsakad av virus. I de europeiska länderna och Nordamerika är de tre vanligastebakterierna som orsakar öroninflammationer Streptococcus pneumoniae,Haemophilus influenzae och Moraxella catarrhalis. Förekomsten avantibiotikaresistens hos dessa har förändrats från antibiotikaerans början till densituation vi har idag. Det finns en ökande förekomst av resistenta S. pneumoniae ochen måttlig till hög förekomst av beta-laktamasproduktion hos H. influenzae och M.catarrhalis. Beta-laktamas är ett ämne som bakterien använder i sitt försvar motbeta-laktamantibiotika som t.ex. penicillinV eller amoxicillin. Dessa bryts ner avbeta-laktamaset och kan inte utöva sin bakteriedödande effekt. I Sverige har vifortsatt att använda den skandinaviska behandlingsmodellen, med penicilliner somförstahandspreparat mot öroninflammationer. I många andra länder har man gåttöver till bred-spektrumantibiotika. Bakterieresistens varierar betydligt mellan olikaländer, vilket antyder att behandlingsprinciperna i de olika länderna spelar roll förresistensutvecklingen. Frågan är om vår behandlingsstrategi kommer att ha fortsattlika goda resultat.
Syfte: De frågor vi försöker besvara är: Är en obehandladöroninflammation bättre än en antibiotikabehandlad öroninflammation förutvecklingen av infektionsförsvaret? Har bakterier med förvärvadantibiotikaresistens mindre sjukdomsframkallande förmåga? Kan beta-laktamasalltid neutralisera penicilliner? Är alla bakterier som orsakar öroninflammationerlika viktiga att behandla?
Metod: En djurmodell användes för att undersöka olika aspekter avbehandling, skydd och histologiska förändringar vid bakteriell öroninflammation.
Resultat: I artikel I gavs en femdagars kur med amoxicillin till råttor medöroninflammation orsakad av H. influenzae. Behandlingen förkortade infektionenslängd och minskade de histologiska förändringar som normalt kan ses efterobehandlad öroninflammation. Effekten av antibiotikabehandling på återkommandeöroninflammation studerades också. Vid en andra öroninflammation sågs ett likagott skydd hos de som tidigare fått antibiotikabehandling som de som inte fåttbehandling, dvs. amoxicillinbehandling påverkade inte immunsvaret negativt.Antikroppsproduktionen var vid den andra öroninflammationen till och med högre iden grupp som fått behandling, jämfört med i den grupp som inte fått behandling vidden första infektionen.
I artikel II, där öroninflammationen orsakades av H. influenzae med enkromosomal resistens mot beta-laktam antibiotika, observerades att den genetiskaförändringen som leder till resistens hos bakterien kan ske utan alltför storminskning i den sjukdomsframkallande förmågan hos bakterien.Resistensutvecklingen mot antibiotika kan också vara till fördel för bakterien då denunder antibiotikabehandlingen överlevde längre.
I artikel III undersöktes om en bakterie som producerar beta-laktamasmöjligen skulle kunna skydda en penicillinkänslig bakterie motantibiotikabehandling när de förekommer samtidigt i en infektion. Vi visade attamoxicillin kunde avdöda de S. pneumoniae som fanns i örat, trots närvaro av beta-laktamasproducerande H. influenzae.

42
I artikel IVundersöktes en annan bakterie som så gott som alltid är beta-laktamasproducerande, M. catarrhalis.. När denna bakterie förekommer iodlingssvar kan det leda till att bredspektrumantibiotika ordineras som behandling.Vi kunde etablera en djurmodell av öroninflammation orsakad av M. catarrhalis.Den öroninflammation som observerades var en lindrig sjukdom med kort förlopp.
Konklusion: Penicillinerna kan inte behandla alla bakterier som orsakaröroninflammation, men de kan sannolikt ta bort de bakterier som ger allvarligainfektioner med risk för komplikationer. Trots att den skandinaviskabehandlingsmodellen funnits i många år och att känsligheten för penicilliner harminskat hos en del av de bakterier som orsakar öroninflammationer, finns detmycket som talar för att den fortfarande fungerar bra.

43
ACKNOWLEDGMENTS
The journey has been long, and I have met so many skilful and stimulating peopleduring the years that has supported and helped me, which I would like to thank. Thiswould not have been possible without your help. To ALL of you, my sinceregratitude!
In particular I wish to thank:
Ann Hermansson, my tutor and guide in the research area, for your enthusiasm andyour support and for making me feel welcome from the very first moment. Thanksfor your friendship and for sharing your expertise.
Sten Hellström, my tutor who gave me the opportunity to begin research. Thanks foryour encouragement as a tutor, your generosity in sharing techniques and for yourvaluable comments.
Åsa Melhus, for all the knowledge you shared, the work you so skilfully achievedand for always being available for me. Thanks to you and Bellman for sharing yourhome and your friendship.
All my coworkers and cowriters for a fruitful cooperation.
All my colleagues, Thomas, Carl-Olof, Hans-Erik, Per, Katrin, Christian, Erika,Ulrik, Jian, Anders, Lars, Ulf and all other co-workers in the ENT-clinic inSundsvall, Härnösand and Sollefteå. Thanks for saving me in the end and for takingcare of my patients with great patience, I´ll be back!
Mid Sweden Research and Development Center in Sundsvall, for the generosity andhelp you all so willingly shared.
The ENT–clinic in Umeå with old and new colleagues: Andrea, P-O, Annika, Karin,Cecilia and Katarina. The ENT-clinic in Lund which I visited during the years: Karin Prellner, whoalways had supporting comments, and Ulla Wide.
The people in the laboratory in Umeå, Ann-Louise, Cathrine and Kristina, yourwork was invaluable.
Till mina föräldrar, Börje och Elsie, för att ni alltid har stöttat och uppmuntrat ochhjälpt till.Mina syskon, Helena och Robert, för att ni alltid finns där och ställer upp i med- ochmotgångar.
Till Björn, Jonas och Alfred för er kärlek och ert tålamod.
Financial support was provided by grants from the Swedish Medical ResearchCouncil (17X-06578, 17X-06857, 16X-03163), Mid Sweden Research andDevelopment Center, Swedish Society of Medicine, Forssman’s foundation, MalmöHealth Services District Foundations
44
REFERENCES
Albiin N, Hellström S, Stenfors L-E, Cerne A. (1986). Middle ear mucosa in rats andhumans. Ann Otol Rhinol Laryngol 126 (Suppl):2-15
Alho OP, Koivu M et al. (1990). Risk factors for recurrent acute otitis media andrespiratory infection in infancy. Int J Pediatr Otorhinolaryngol 19(2):151-61.
Alho OP, Koivu M et al. (1991). The occurrence of acute otitis media in infants. A life-table analysis. Int J Pediatr Otorhinolaryngol 21(1):7-14.
Aniansson G., Alm B, et al. (1992). Nasopharyngeal colonization during the first yearof life. J Infect Dis 165 Suppl 1: S38-42.
Appelbaum PC. (1992). Antimicrobial resistance in Streptococcus pneumoniae: anoverwiev. Clin Infect Dis 15(1):77-83.
Arason VA, Kristinsson KG, et al. (1996). Do antimicrobials increase the carriage rateof penicillin resistant pneumococci in children? Cross sectional prevalence study. BMJ313:387-391.
Bakaletz LO, Kennedy BJ, Novotny LA, Duquesne G, Cohen J, Lobet Y. (1999).Protection against development of otitis media induced by nontypeable Haemophilusinfluenzae by both active and passive immunization in a chinchilla model of virus-bacterium superinfection. Infect Immun 67(6):2746-62. Erratum in: Infect Immun67(10):5545
Bandak SI, Turnak MR, et al. (2001). Antibiotic susceptibilities among recent clinicalisolates of Haemophilus influenzae and Moraxella catarrhalis from fifteen countries.Eur J Clin Microb Inf Dis 20(1):55-60.
Barenkamp SJ. (1986). Protection by serum antibodies in experimental nontypeableHaemophilus influenzae otitis media. Infect Immun 52:331-335.
Barnhart BJ, Herriot RM. (1963). Penetration of deoxyribonucleic acid into Hemophilusinfluenzae. Biochem Biophys Acta 76:25-39.
Barry, B., Delattre J, Vié F, Bedos J.-P, Géhanno P. (1999). Otogenicintracranial infections in adults. Laryngoscope 109:483-487.
Barzilai A, Leibovitz E, et al. (1999). Dynamics of interleukin-1 production in middleear fluid during acute otitis media treated with antibiotics. Infection 27(3):173-6.
Bernstein JM, Faden HS et al. (1992). Recurrent otitis media with non-typableHaemophilus influenzae: the role of serum bactericidal antibody.Int J PediatrOtorhinolaryngol. 23(1):1-13.
Bjuggren G, Thunevall G. (1950). The Pfeiffer bacillus in otitis in children. A sero-bacteriological and clinical study. Acta Otolaryngol 38:130-46.
45
Block SL, Harrison CJ, et al. (1995). Penicillin-resistant Streptococcus pneumoniae inacute otitis media: risk factors, susceptibility patterns and antimicrobial management.Pediatr Infect Dis J 14(9):751-9.
Blomgren, K, Pitkaranta A. (2003). Is it possible to diagnose acute otitis mediaaccurately in primary health care? Fam Pract 20(5): 524-7.
Bluestone CD, Stephenson JS, et al.(1992).Ten-year review of otitis media pathogens.Pediatr Infect Dis J 11(8 Suppl): S7-11.
Bluestone CD. (1996). Pathogenesis of otitis media: role of eustachian tube.Pediatr Infect Dis J. 15(4):281-91.
Bootsma HJ, Aerts PC, Posthuma G, Harmsen T, Verhoef J, van Dijk H, Mooi FR.(1999). Moraxella (Branhamella) catarrhalis BRO beta-lactamase: a lipoprotein ofgram-positive origin? J Bacteriol. 181(16):5090-3.
Brandtzaeg P. (1992). Humoral immune response patterns of human mucosae: inductionand relation to bacterial respiratory tract infections. J Infect Dis 165 (Suppl 1):S167-S176.
Bronzwaer S, Cars O, et al. (2002). A European study on the relationship betweenantimicrobial use and antimicrobial resistance. Emerg Inf Dis 8: 278-282.
Brook I., Gilmore JD. (1993). Evaluation of bacterial interference and β-lactamase production in management of experimental infection with group Abeta-hemolytic streptococci. Antimicrob. Agents Chemother 37:1452-1455.
Brook I, Gober AE. (1998). Bacterial interference in the nasopharynx followingantimicrobial therapy of acute otitis media. J Antimicrob Chemother 41(4): 489-92.
Brunton J, Clare D, Meier MA. (1986). Molecular epidemiology of antibiotic resistanceplasmids of Haemophilus species and Neisseria gonorrhoeae. Rev Infect Dis 8:713-24.
Burke P, Bain J et al. (1991). Acute red ear in children: controlled trial of non-antibiotictreatment in general practice. BMJ 303:558-62.
Bylander-Groth A, Stenström C. (1998). Eustachian tube function and otitis media inchildren. Ear Nose Throat J 77(9): 762-4, 766, 768-9.
Canafax DM, Yuan Z, et al. (1998). Amoxicillin middle ear fluid penetration andpharmacokinetics in children with acute otitis media. Pediatr Infect Dis J 17(2): 149-56
Carlin SA, Marchant CD, et al. (1991). Host factors and early therapeutic response inacute otitis media. J Pediatr 118:178-83.
Casselbrant ML, Kaleida PH, Rockette HE, Paradise JL, Bluestone CD, Kurs-Lasky M,Nozza RJ, Wald ER. (1992). Efficacy of antimicrobial prophylaxis and oftympanostomy tube insertion for prevention of recurrent acute otitis media: results of arandomized clinical trial. Pediatr Infect Dis J. 11(4):278-86

46
Casselbrant ML., Mandel EM, et al. (1999). The heritability of otitis media: a twin andtriplet study. Jama 282(22): 2125-30.
Cayé-Thomasen P, Tos M. (2001). Histopathologic differences due to bacterial speciesin acute otitis media. Int J Ped Otorhinolaryngol 63:99-110
Chung MH, Enrique R, Lim DJ, De Maria TF. (1994). Moraxella (Branhamella)catarrhalis-induced experimental otitis media in the chinchilla. Acta Otolaryngol(Stockh) 114:415-22.
Clairoux N, Picard M, Brochu A, Rousseau N, Gourde P, Beauchamp D, Parr TR, Jr,Bergeron MG, Malouin F. (1992). Molecular basis of the non-β-lactamase-mediatedresistance to β-lactam antibiotics in strains of Haemophilus influenzae isolated inCanada. Antimicrob Agents Chemother 36:1504-1513.
Craig WA, Andes D. (1996) Pharmacokinetics and pharmacodynamics of antibiotics inotitis media. Pediatr Infect Dis J 15(3):255-9.
Craig WA. (1996). Antimicrobial resistance issues of the future. Diagn Microbiol InfectDis 25(4):213-7.
Dagan R, Leibovitz E, et al. (1998). Early eradication of pathogens from middle earfluid during antibiotic treatment of acute otitis media is associated with improvedclinical outcome. Pediatr Infect Dis J 17(9):776-82.
Dagan R, Klugman KP, Craig WA, Baquero F. (2001). Evidence to support therationale that bacterial eradication in respiratory tract infection is an important aim ofantimicrobial therapy. J Antimicrob Chemother 47(2):129-40.
Daly KA, BrownJE, et al. (1999). Epidemiology of otitis media onset by six months ofage. Pediatrics 103(6 Pt 1): 1158-66.
Damoiseaux R, van Balen F, et al. (2000). Primary care based randomised double blindtrial of amoxicillin versus placebo for acute otitis media in children aged under 2 years.BMJ 320:350-354.
Daniels HJ, III, Fulgham RS, Brinn JE, Barrett KA. (1982). Comparative anatomy ofEustachian tube and middle ear cavity in animal models for otitis media. Ann OtolRhinol Laryngol 91:82-89.
Del Beccaro MA, Mendelman PM, et al. (1992). Bacteriology of acute otitis media: anew perspective. J Pediatr 120(1): 81-4.
Del Castillo F, Baquero-Artigao F, Garcia-Perea A. (1998). Influence of recentantibiotic theraphy on antimicrobial resistance of Streptococcus pneumoniae in childrenwith acute otitis media in Spain. Pediatr Infect Dis J 17:94-97.
Del Mar CB, Glasziou, PP, Hayem M. (1997). Are antibiotics indicated as initialtreatment for children with acute otitis media? A meta-analysis. BMJ 314:1526-9.

47
DeMaria TF. (1999). Localization of nontypeable Haemophilus influenzae endotoxin inthe middle and inner ear during experimental otitis media. Acta Otolaryngol 119(5):583-7.
Dhainaut JF, Charpentier J, Chiche JD. (2003). Transforming growth factor-β: Amediator of cell regulation in acute respiratory distress. Crit Care Med 31 (Suppl):S258-64.
Dowell SF, Schwartz B. (1997). Resistant pneumococci: protecting patients throughjudicious use of antibiotics. Am Fam Physician 55:1647-1654.
Doyle WJ. (1985). Eustachian tube function in the chinchilla. Arch Otolaryngol111:305-308.
Doyle WJ. (1989). Animal models of otitis media: other pathogens. Pediatr Infect Dis J8:S45-7.
Duffy LC, Faden H, et al. (1997). Exclusive breastfeeding protects against bacterialcolonization and day care exposure to otitis media. Pediatrics 100(4): E7.
Duncan B, Ey J, et al. (1993). Exclusive breast-feeding for at least 4 months protectsagainst otitis media. Pediatrics 91(5): 867-72.
Enright MC, McKenzie H. (1997). Moraxella (Branhamella) catarrhalis-clinical andmolecular aspects of a rediscovered pathogen. J Med Micrbiol 46:360-370.
Eskola J, Kilpi T, et al. (2001). Efficacy of a pneumococcal conjugate vaccine againstacute otitis media. N Engl J Med 344(6):403-9.
Faden H., Stanievich J, et al. (1990). Changes in nasopharyngeal flora during otitismedia of childhood. Pediatr Infect Dis J 9(9): 623-6.
Faden H, Hong J, Murphy T. (1992). Immune response to outer membrane antigens ofMoraxella catarrhalis in children with otitis media. Infect Immun 60:3824-9.
Faden H, Karabuchi Y, Hong JJ. (1994). Epidemiology of Moraxella catarrhalis inchildren during the first 2 years of life: relationship to otitis media. J Infect Dis.169(6):1312-7.
Faden H, Duffy L, et al. (1995). Epidemiology of nasopharyngeal colonization withnontypeable Haemophilus influenzae in the first 2 years of life. J Infect Dis 172(1): 132-5.
Faden H. (2001). The microbiologic and immunologic basis for recurrent otitis media inchildren. Eur J Pediatr 160:407-413.
Fleming A. (1929). On the antibacterial action of cultures of Penicillum with specialreference to their use in the isolation of B. Influenzae. Br J Exp Pathol 10:226-36.

48
Fjellbirkeland L, Cambier S, Broaddus VC, Hill A, Brunetta P, Dolganov G, Jablons D,Nishimura SL. ( 2003). Integrin alphavbeta8-mediated activation of transforminggrowth factor-beta inhibits human airway epithelial proliferation in intact bronchialtissue. Am J Pathol. 163(2):533-42.
Frosch P, KolleW. (1896). Die Mikrokokken, p. 154-155. In: C. Flugge (ed.), DieMikroorganism, 3rd ed, vol 2.Verlag von Vogel, Leipzig, Germany.
Fomsgaard A, Shand GH, Freudenberg MA, Galanos C, Conrad RS, Kronborg G,Høiby N. (1993). Antibodies from chronically infected cystic fibrosis patients react withlipopolysaccharides extracted by new micromethods from all serotypes of Pseudomonasaeruginosa. APMIS 101:101-112
Froom J., Culpepper L, Jacobs M, DeMelker RA, Green LA, Van Buchem L, Grob P,Heeren T. (1997). Antimicrobials for acute otitis media? A review from theinternational primary care network. BMJ 315:98-102.
Fulghum RS, Marrow HG. (1996). Experimental otitis media with Moraxella(Branhamella) catarrhalis. Ann Otol Rhinol Laryngol 105:234-41.
Garbutt J., Jeffe DB, et al. (2003). Diagnosis and treatment of acute otitis media: anassessment. Pediatrics 112(1 Pt 1): 143-9.
Gehanno P, Panajotopoulos A, Barry B, Nguyen L, Levy D, Bingen E, Berche P.(2001). Microbiology of otitis media in the Paris, France, area from 1987 to 1997.Pediatr Infect Dis J 20(6):570-3.
Giebink GS. (1999). Otitis media: the chinchilla model. Microb Drug Resist 5(1):57-72
Geiser AG, Zeng QQ, Sato M, Helvering LM, Hirano T, Turner CH. (1998). Decreasedbone mass and bone elasticity in mice lacking the transforming growth factor–beta 1gene. Bone 23(2):87-93.
Glasziou PP, Del Mar CB, et al. (2000). Antibiotics for acute otitis media in children.Cochrane Database Syst Rev. (4):CD000219. Review.
Goldstein NA, Casselbrant ML, Bluestone CD, Kurs-Lasky M. (1998). Intratemporalcomplications of acute otitis media in infants and children. Otolaryngol Head NeckSurg. 119:444-454.
Gonzalez C, Arnold JE, et al. (1986). Prevention of recurrent acute otitis media:chemoprophylaxis versus tympanostomy tubes. Laryngoscope 96:1330-4.
Goodgal SH, Herriot RM. (1961). Studies of transformation of Haemophilus influenzae.1. Competence. J Gen Physiol. 44:1201-1227.
Green BA, Vasques ME, Zlotnick GW, Quigley-Reape G, Swartz JD, Green I, et al.(1993). Evaluation of mixtures of purified Haemophilus influenzae outer membraneproteins in protection against challenge with nontypeable H. influenzae in the chinchillaotitis media model. Infect Immun 61:1950-7.

49
Hart V. (1927). The bacteriology of acute ears. Laryngoscope 37:56-61.
Haugsten P, Lorentzen P (1980). The bacterial etiology of acute suppurative otitismedia. J Laryngol Otol 94(2): 169-76.
Hebel R, Stromberg MW. (1976). Anatomy of the laboratory rat. Williams & WilkinsCo., Baltimore.
Heikkinen T., Waris M, et al. (1995). Incidence of acute otitis media associated withgroup A and B respiratory syncytial virus infections. Acta Paediatr 84(4): 419-23.
Heikkinen T. (2000). The role of respiratory viruses in otitis media. Vaccine 19 Suppl 1:S51-5.
Heikkinen T, Chonmaitree T. (2003). Importance of respiratory viruses in acute otitismedia. Clin Microbiol Rev 16(2): 230-41.
Hellström S, Salén B, Stenfors L-E. (1982). Anatomy of the rat middle ear. A studyunder the dissection microscope. Acta Anat 112:346-352.
Hellström S, Stenfors LE. (1983). The pressure equilibrating function of pars flaccida inmiddle ear mechanics. Acta Physiol Scand. 118(4):337-41.
Henderson B, Poole S, Wilson M. (1996). Bacterial modulins: a novel class of virulencefactors which cause host tissue pathology by inducing cytokine synthesis. Micrbiol Rev60:316-341.
Hermansson A, Emgård P, Prellner K, Hellström S. (1988). A rat model forpneumococcal otitis media. Am J Otolaryngol 9:97-101.
Hermansson A, Prellner K, Hellström S. (1990). Persistent structural changes in themiddle ear mucosa of the rat, after an experimentally induced episode of pneumococcalotitis media. Acta Otolaryngol (Stockh) 109:421-430.
Hoban DJ, Doern GV, Fluit AC, Roussel-Delvallez M, Jones RN. (2001). Worldwideprevalence of antimicrobial resistance in Streptococcus pneumoniae, Haemophilusinfluenzae, and Moraxella catarrhalis in the SENTRY Antimicrobial SurveillanceProgram, 1997-1999. Clin Infect Dis. 32 Suppl 2:S81-93.
Hol C, Van Dijke EEM, Verduin CM, Verhoef J,Van Dijk H. 1994. Experimentalevidence for Moraxella-induced penicillin neutralization in pneumococcal pneumonia.J. Infect. Dis. 170:1613-1616.
Howie VM, Ploussard JH. (1972). Efficacy of fixed combination antibiotics versusseparate components in otitis media. Effectiveness of erythromycin estrolate, triplesulphonamide, ampicillin, erythromycin estolate- triple sulphonamide, and placebo in280 patients with acute otitis media under two and one-half years of age. Clin Pediatr(Phila) 11(4): 205-14.
50
Howie VM, Dillard R, Lawrence B. (1985). In vivo sensitivity test in otitis media:efficacy of antibiotics. Pediatrics 75:8-13.
Ingvarsson L, Kamme C, Lundgren K. (1980). Concentration of penicillin V in serumand middle ear exudates during treatment of acute otitis media. Ann Otol RhinolLaryngol (Suppl) 68:275-77.
Ingvarsson L, Lundgren K. (1982). Penicillin treatment of acute otitis media in children:a study of the duration of treatment. Acta Otolaryngol 94:283-7.
Jacobs MR, Dagan R, et al. (1998). Prevalence of antimicrobial-resistant pathogens inmiddle ear fluid: multinational study of 917 children with acute otitis media.Antimicrob Agents Chemother 42(3): 589-95.
Jero J, Karma P (1997). Prognosis of acute otitis media. Factors associated with thedevelopment of recurrent acute otitis media. Acta Otolaryngol Suppl 529: 30-3.
Joki-Erkkilä VP, Pukander J, et al. (2000). Alteration of clinical picture and treatment ofpediatric acute otitis media over the past two decades. Int J Pediatr Otorhinolaryngol55(3): 197-201.
Joki-Erkkilä VP, Aittoniemi J, et al. (2002). Beta-Lactamase-producing Moraxellacatarrhalis may prevent the emergence of penicillin-resistant Streptococcus pneumoniaein children with recurrent acute otitis media. Int J Pediatr Otorhinolaryngol 63(3): 219-22.
Juhlin J, Möller O, Thulin KE. (1967) Är vår nuvarande perorala dosering av V-penicillin adekvat? Läkartidningen 64:3609-11.
Jörgensen F, Andersson B, Hanson LA, Nylen O, Eden CS. (1990). Gamma-globulintreatment of recurrent acute otitis media in children. Pediatr Infect Dis J.9(6):389-94.
Kalm O, Prellner K, Christensen P. (1986). The effect of intravenous immunoglobulintreatment in recurrent acute otitis media. Int J Pediatr Otorhinolaryngol. 11(3):237-46
Kamme C, Lundgren K, Rundcrantz H. (1969). The concentration of penicillin V inserum and middle ear exudates in acute otitis media in children. Scand J Infect Dis1:77-83.
Kamme C, Lundgren K, et al. (1971). The aetiology of acute otitis media in children.Occurrence of bacteria, L forms of bacteria and mycoplasma in the middle ear exudate.Relationship between bacterial findings in the middle ear exudate, nasopharynx andthroat. Scand J Infect Dis 3(3): 217-23
Karasic RB, Trumpp CE, Gnehm HE, Rice PA, Pelton SI. (1985). Modification of otitismedia in chinchillas rechallenged with nontypeable Haemophilus influenzae andserological response to outer membrane agents. J Infect Dis 151:273-279.

51
Karma P, Palva T, et al. (1987). Finnish approach to the treatment of acute otitis media.Report of the Finnish Consensus Conference. Ann Otol Rhinol Laryngol Suppl 129: 1-19.
Kilian M. (1991). Haemophilus. In: Balows A (chief ed.): Manual of clinicalmicrobiology, fifth edition. American Society for Microbiology, Washington DC, pp.463-470.
Kilpi T, Herva E, et al. (2001). Bacteriology of acute otitis media in a cohort of Finnishchildren followed for the first two years of life. Pediatr Infect Dis J 20(7): 654-62.
Klein JO. (1993). Microbiologic efficacy of antibacterial drugs for acute otitis media.Pediatr Infect Dis J 12:973-975.
Klein JO. (1994). Otitis media. Clin Infect Dis 19:823-833.
Kovatch AL, Wald ER, et al. (1983). Β-lactamase-producing Branhamella catarrhaliscausing otitis media in children. J Pediatr 102(2):261-264.
Kuklinska D, Kilian M. (1984). Relative proportions of Haemophilus species in thethroat of healthy children and adults. Eur J Clin Microbiol 3:249-252.
Kvaerner KJ, Tambs K, et al. (1997). Distribution and heritability of recurrent earinfections. Ann Otol Rhinol Laryngol 106(8): 624-32.
Lister PD, Pong A, et al. (1997). Rationale behind high-dose amoxicillin therapy foracute otitis media due to penicillin-non-susceptible pneumococci: support from in vitropharmacodynamic studies. Antimicrob Agents Chemother 41(9):1926-32.
Lim DJ, Chun YM, Lee HY, Moon SK, Chang KH, Li JD, Andalibi A. (2000). Cellbiology of tubotympanum in relation to pathogenesis of otitis media - a review.Vaccine. 19 Suppl 1:S17-25.
Loos BG, Bernstein JM, Dryja DM, Murphy TF, Dickinson DP. (1989). Determinationof the epidemiology and transmission of nontypeable Haemophilus influenzae inchildren with otitis media by comparison of total genomic DNA restriction fingerprints.Infect Immun 57:2751-2757.
Ludviksson BR, Gunnlaugsdottir B. (2003). Transforming growth factor-β as aregulator of site-specific T-cell inflammatory response. Scand J Immunol 58:129-138.
Lundgren K, Ingvarsson L. (1983). Epidemiology of acute otitis media in children.Scand J Infect Dis Suppl 39: 19-25.
Lundgren K, Rundcrantz H. (1967). Otitis media acuta hos barn. Läkartidningen 64:63-70
Luntz M, Brodsky A, et al. (2001). Acute mastoiditis--the antibiotic era: a multicenterstudy. Int J Pediatr Otorhinolaryngol 57(1): 1-9.
52
Magnusson K, Hermansson A, Melhus Å, Hellström S. (1997). The tympanicmembrane and the middle ear mucosa during non-typeable Haemophilus influenzae andHaemophilus influenzae type b acute otitis media: a study in the rat. Acta Otolaryngol(Stockh) 117:396-405.
Manninen R, Huovinen P, Nissinen A. (1997). Increasing antimicrobial resistance inStreptococcus pneuominae, Haemophilus influenzae and Moraxella catarrhalis inFinland. J Antimicrob Cemother 40:387-92.
Marchant CD. (1990). Spectrum of disease due to Branhamella catarrhalis in childrenwith particular reference to acute otitis media. Am J Med 14:158-98.
Marchant CD, Carlin SA, Johnson CE, Shurin PA. (1992).Measuring the comparativeefficacy of antibacterial agents for acute otitis media: the "Pollyanna phenomenon".J Pediatr. 120(1):72-7.
Medeiros AA, Levesque R, Jacoby GA. (1986). An animal source for the ROB-1 beta-lactamase of Haemophilus influenzae type b.Antimicrob Agents Chemother.29(2):212-5. Erratum in: Antimicrob Agents Chemother 1986 Apr;29(4):720.
Melander E, Mölstad S, et al. (1998). Previous antibiotic consumption and other riskfactors for carriage of penicillin-resistant Streptococcus pneumoniae in children. Eur JClin Microb 17(12):834-838.
Melhus Å, Hermansson A, Prellner K. (1994). Nontypeable and encapsulatedHaemophilus influenzae yield different clinical courses of experimental otitis media.Acta Otolaryngol (Stockh) 114:289-94.
Melhus Å, Hermansson A, Akkoyunlu M, Forsgren A, Prellner K. (1995). Experimentalrecurrent otitis media induced by Haemophilus influenzae: protection and serumantibodies. Am J Otolaryngol 16:383-90.
Melhus Å, Ryan AF. (2000). Expression of cytokine genes during pneumococcal andnontypeable Haemophilus influenzae acute otitis media in the rat. Infect Immun68:4024-31.
Melhus Å. (2001). Effects of amoxicillin on the expression of cytokines duringexperimental acute otitis media caused by non-typeable Haemophilus influenzae. JAntimicrobial Chemother 48(3):397-402.
Melhus Å, Ryan F (2003) A mouse model for acute otitis media. APMIS. 111(10):989-994
Moxon ER, Deich RA, Connelly C. (1984). Cloning of chromosomal DNA fromHaemophilus influenzae. J Clin Invest 73:298-306.
Murphy TF. (1996). Branhamella catarrhalis: epidemiology, surface antigenic structure,and immune response. Microbiol Rev 60:267-79.
53
Mygind N, Meistrup-Larsen KI, Thomsen J, Thomsen VF, Josefsson K, Sorensen H.(1981). Penicillin in acute otitis media: a double-blind placebo-controlled trial. ClinOtolaryngol 6(1): 5-13.
Mäkelä PH, Sibakov M, Herva E, Henrichsen J, Luotonen J, Timonen M, Leinonen M,Koskela M, Pukander J, Pontynen S, Grönroos P, Karma P (1980). Pneumococcalvaccine and otitis media. Lancet. 2(8194):547-51.
Nasrin D, Collignon PJ, et al. (2002). Effect of beta lactam antibiotic use in children onpneumococcal resistance to penicillin: prospective cohort study. BMJ.324(7328):28-30
Nicod LP. (1993) Cytokines. 1. Overview.Thorax. 48(6):660-7.
Nielsen J. (1945). Studies of the aetiology of acute otitis media. Copenhagen: EjnarMunksgaard.
Niemelä M, Uhari M, et al. (1995). A pacifier increases the risk of recurrent acute otitismedia in children in day care centers. Pediatrics 96(5 Pt 1): 884-8
Orange M, Gray BM. (1993). Pneumococcal serotypes causing disease in children inAlabama. Pediatr Infect Dis J 12(3): 244-6.
Paradise JL, Rockette HE, et al. (1997). Otitis media in 2253 Pittsburgh-area infants:prevalence and risk factors during the first two years of life. Pediatrics 99(3): 318-33.
Parra A, Ponte C, et al. (2002). Optimal dose of amoxicillin in treatment of otitis mediacaused by a penicillin-resistant pneumococcus strain in the gerbil model. AntimicrobAgents Chemother 46(3):859-862.
Patel JA, Chonmaitree T, Schmalstieg F. (1993). Effect of modulation ofpolymorphonuclear leukocyte migration with anti-CD18 antibody on pathogenesis ofexperimental otitis media in guinea pigs. Infect Immun 61:1132-1135.
Petersen CG, Ovesen T, et al. (1998). Acute mastoidectomy in a Danish county from1977 to 1996 with focus on the bacteriology. Int J Pediatr Otorhinolaryngol 45(1): 21-9.
Pober JS, Cotran RS. (1990). The role of endothelial cells in inflammation.Transplantation 50:537-544.
Pichichero ME. (2003). Diagnostic accuracy of otitis media and tympanocentesis skillsassessment among pediatricians. Eur J Clin Microbiol Infect Dis 22(9): 519-24.
Poulsen K, Hjorth JP, Kilian M. (1988). Limited diversity of the immunoglobulin A1protease gene (iga) among Haemophilus influenzae serotype b strains. Infect Immun56:987-992.
Pukander J, Karma P, Sipilä M. (1982). Occurrence and recurrence of acute otitis mediaamong children. Acta Otolaryngol (Stockh) 94:479-486.
54
Rapola S, Kilpi T, et al (2001). Do antibodies to pneumococcal surface adhesin aprevent pneumococcal involvement in acute otitis media. J Infect Dis 184(5):577-81.
Renneberg J, Walder M. (1989). The role of beta-lactamase in mixed infections in micein relation to treatment with ampicillin. J. Infect. Dis. 160:337-341.
Robbins SL, Cotran RS. (1979). Pathologic basis of disease, second edition. Saunders,Philadelphia, pp 55-106.
Rosenfeld RM, Vertrees JE, et al. (1994). Clinical efficacy of antimicrobial drugs foracute otitis media: metaanalysis of 5400 children from thirty-three randomized trials. JPediatr 124(3): 355-67.
Rosenfeld RM, Bluestone CD. (2003). Evidence-based otitis media. Second edition. BCDecker Inc.
Rothman R, Owens T, et al. (2003). Does this child have acute otitis media? Jama290(12): 1633-40.
Roos K, Grahn-Håkansson E, Holm S. 2001. Effect of recolonisation with “interfering”α streptococci on recurrences of acute and secretory otitis media in children:randomised placebo controlled trial. BJM 322:1-4.
Rudberg RD. (1954). Acute otitis media: comparative therapeutic results ofsulphonamide and penicillin administered in various forms. Acta Otolaryngol (Stockh)113 (Suppl):9-79.
Rundcrantz H, Sundför A. (1974). Förenklad dosering av penicillin. Läkartidningen71:71-2
Ruohola A, Heikkinen T, Meurman O, Puhakka T, Lindblad N, Ruuskanen O. (2003).Antibiotic treatment of acute otorrhea through tympanostomy tube: randomized double-blind placebo-controlled study with daily follow up. Pediatrics 111:1061-7.
Ruuskanen O, Arola M, et al. (1989). Acute otitis media and respiratory virusinfections. Pediatr Infect Dis J 8(2): 94-9.
Ruuskanen O, Heikkinen T. (1994). Viral-bacterial interaction in acute otitis media.Pediatr Infect Dis J 13(11): 1047-9.
Ryan AF, Sharp PA, Harris JP. (1990). Lymphocyte circulation to the middle ear. ActaOtolaryngol (Stockh) 109:278-287.
Sabirov A, Kodama S, et al. (2001). Intanasal immunization enhances clearance ofnontypeable Haemophilus influenzae and reduces stimulation of tumor necrosis factoralpha in the murine model of otitis media. Infect Immun 69(5):2964-2971.
Sato K. (1997). Experimental otitis media induced by nonviable Moraxella catarrhalis inthe guinea pig model. Auris Nasus Larynx 24:233-38.
55
Sato K, Liebeler CL, et al (1999). Middle ear fluid cytokine and inflammatory cellkinetics in the chinchilla otitis media model. Infect Immun 67(4):1943-1946.
Schramm C, Herz U, et al. (2003). TGF-β regulates airway responses via T-cells. JImmunol 170:1313-1319.
Schägger H, von Jagow G. (1987). Tricine-sodium dodecyl sulfate-polyacrylamide gelelectrophoresis fort he separation of proteins in the range from 1 to 100 kDa. AnalBiochem 166:368-379.
Seppälä H, Klaukka T, et al. (1997). The effect of changes in the consumption ofmacrolide antibiotics on erythromycin resistance in group A streptococci in Finland.Finnish study group for antimicrobial resistance. N Eng J Med 337(7):491-2.
Shurin PA, Van Hare GF. (1986). Therapy of acute otitis media caused by Branhamellacatarrhalis. Preliminary report. Drugs 31 (Suppl 3):122-24.
Shurin PA, Rehmus JM, Johnson CE, Marchant CD, Carlin SA, Super DM, Van HareGF, Jones PK, Ambrosino DM, Siber GR. (1993) Bacterial polysaccharide immuneglobulin for prophylaxis of acute otitis media in high-risk children.J Pediatr.123(5):801-10.
Spellberg B, Edwards JE, Jr. (2001). Type1/type 2 immunity in infectious diseases. ClinInfect Dis 32:76-102.
Sipilä M, Pukander J, et al. (1987). Incidence of acute otitis media up to the age of 1 1/2years in urban infants. Acta Otolaryngol 104(1-2): 138-45.
Spratley J, Silveira H, et al. (2000). Acute mastoiditis in children: review of the currentstatus. Int J Pediatr Otorhinolaryngol 56(1): 33-40.
Stenfors LE, Raisanen S. (1990). Occurrence of middle ear pathogens in thenasopharynx of young individuals. A quantitative and qualitative study in four agegroups. Acta Otolaryngol 109: 142-8.
Stenfors LE. (1999) Non-specific and specific immunity to bacterial invasion of themiddle ear cavity. Int J Pediatr Otorhinolaryngol. 49 Suppl 1:S223-6
Stenström R, Bernard PA, et al. (1993). Exposure to environmental tobacco smoke as arisk factor for recurrent acute otitis media in children under the age of five years. Int JPediatr Otorhinolaryngol 27(2): 127-36.
Svinhufvud M, Prellner K, Hermansson A, Schalen C.(1991) Experimental recurrentpneumococcal otitis media. Protection and serum antibodies. Acta Otolaryngol.111(6):1083-9.
Takata GS, Chan LS, et al. (2001). Evidence assessment of management of acute otitismedia: I. The role of antibiotics in treatment of uncomplicated acute otitis media.Pediatrics 108(2):239-247.
56
Tano K, Grahn-Håkansson E, et al. (2000). Inhibition of OM pathogens by alpha-hemolytic streptococci from healthy children, children with SOM and children withrAOM. Int J Pediatr Otorhinolaryngol 56(3): 185-90.
Teele DW, Klein JO, et al. (1989). Epidemiology of otitis media during the first sevenyears of life in children in greater Boston: a prospective, cohort study. J Infect Dis160(1): 83-94.
Turner MW. (1996) Mannose-binding lectin: the pluripotent molecule of the innateimmune system. Immunol Today 17(11):532-40
Uhari M, Mantysaari K, et al. (1996). A meta-analytic review of the risk factors foracute otitis media. Clin Infect Dis 22(6): 1079-83.
Van Buchem FL, Dunk JHM, et al (1981). Therapy of acute otitis media: myringotomy,antibiotics, or neither: a double-blind study in children. Lancet 2:883-7.
Van Hare GF, Shurin PA, Marchant CD, Cartelli NA, Johnson CE, Fulton D, et al.(1987) Acute otitis media caused by Branhamella catarrhalis: biology and therapy. RevInfect Dis 9:16-27.
Van Zuijlen DA, Schilder AG, et al. (2001). National differences in incidence of acutemastoiditis: relationship to prescribing patterns of antibiotics for acute otitis media?Pediatr Infect Dis J 20(2): 140-4.
Varon E, Levy C, et al. (2000). Impact of antimicrobial therapy on nasopharyngealcarriage of Streptococcus pneumoniae, Haemophilus influenzae, and Branhamellacatarrhalis in children with respiratory tract infections. Clin Infect Dis 31(2): 477-81
Veenhoven R, Bogaert D, et al. (2003). Effect of conjugate pneumococcal vaccinefollowed by polysaccharide pneumococcal vaccine on recurrent acute otitis media: arandomised study. Lancet 361(9376):2170-1.
Weibel ER. (1989). Stereological Methods. Vol 1. Practical methods for BiologicalMorphometry. Academic Press, third printing pp 28-30
Verduin CM, Hol C et al. (2002). Moraxella catarrhalis: From emerging to establishedpathogen. Clin Microb Rev 15(1):125-144.
Westphal O, Jann K. (1965). Bacterial lipopolysaccharides: extraction with phenol-water and further application of the procedure. Methods Carbohydr Chem 5:83-91.
Williams RL, Chalmers TC, Stange KC, Chalmers FT, Bowlin SJ. (1993) Use ofantibiotics in preventing recurrent acute otitis media and in treating otitis media witheffusion. A meta-analytic attempt to resolve the brouhaha. JAMA. 270(11):1344-51.Erratum in: JAMA 1994 Feb 9;271(6):430
Wirth E. (1928). Studien zur klinischen Bakteriologie der akutenMittelohrenentzündung. Passow-Schaefer Beitr 26:190-232.

57
Wood WB,Jr, Davis BD. (1980) Host parasite relations in bacterial infections. In: DavisBD, Dulbecco R, Eisen HN, Ginsberg HS (eds): Microbiology: including immunologyand molecular genetics, third edition. Harper & Row Publishers, Inc pp 551-593.
Zopf D, Roth S. (1996). Oligosaccharide anti-infective agents. Lancet 347:1017-1021.


















