
Acute kidney injury slideshare
30
Acute Kidney Injury in Children Azilah Sulaiman
-
Upload
azilah-sulaiman -
Category
Education
-
view
132 -
download
9
Transcript of Acute kidney injury slideshare

Acute Kidney Injury in Children
Azilah Sulaiman

• Case scenario…..
2

Discussion…

Introduction
Abrupt decrease in kidney function that include, but is not limited to acute renal failure
Reversible increase in blood concentration of creatinine and nitrogenous waste products & inability of kidney to regulate fluid and electrolyte homeostasis appropriately
Broad clinical syndrome: encompasses various etiologies
Specific kidney diseases
Non-specific conditions e.g. ischemia, toxic injury
Extra-renal pathology
More than one etiologies may coexist at the same time
Epidemiological evidence supporting the notion that “even mild, reversible AKI has important clinical consequences including risk of death”
1. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–1382. Acute kidney injury in children, S. Phillips Andreoli, Pediatr Nephrol (2009) 24:253–263
4

Acute kidney injury in children,S. Phillips Andreoli, Pediatr Nephrol (2009) 24:253–263 5

• Concerns: suboptimal care contributes to development of acute kidney injury
• 2009 – NCEPOD reports the results of an enquiry into deaths of a large group of adult
patients with acute kidney injury that described systemic deficiencies in the care of patient
who died of AKI
“ ONLY 50% of these patient received GOOD care. Other deficiencies in the care of patient
who died of AKI included failure in AKI prevention, recognition, therapy and timely access to
specialist services”
• NICE develops its first guideline in AKI in adults, children and young people in 2013
• AIMS:
• Early intervention
• Importance of risk assessment and prevention
• Early recognition and treatment
Prevention, detection and management of acute kidney injury up to the point of renal replacement therapy; NICE clinical guideline 20136

Risk Assessment…
• Kidney – usually able to withstand several insults without causing significant structural or functional change
• If present: indicate severe systemic derangement and predicts poor prognosis
• Risk of AKI: by exposure to factors that cause AKI, by presence of factors that increased susceptibility to AKI
• Risk assessment:
• Hospital acquired AKI
• Community- acquired AKI
7Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–138

8Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–138

How to….
Prevent AKI:
• Consider pediatric early warning score (PEWS) to identify children and young
people who are at risk of developing AKI
• Best: PEWS with multiparameter or aggregate weighted scoring systems that measure
HR/RR/SBP/ GCS/ O2 saturation/ temperature/ capillary refill time
• Measure urine output
• To record weight twice daily to determine fluid balance
• Measure renal profile ± lactate, blood glucose and blood gas
9Prevention, detection and management of acute kidney injury up to the point of renal replacement therapy; NICE clinical guideline 2013

Detecting AKI:
• Serum creatinine (sCr) still remains the cornerstone of clinical diagnosis of AKI
• Criteria that may be used:
• RIFLE
• pRIFLE
• the slow rate of rise in sCr might prohibit accurate classification of AKI. Consequently, the criteria emphasizes estimated creatinine clearance (using the Schwartz formula) over fold increase in sCr
• Application of pRIFLE definitions has, however, been inconsistent between studies and consequently associated with differing risk between studies
• AKIN
• KDIGO
• Adult and pediatric AKI definitions have been harmonized to emphasize fold change in sCr in adults and children
Acute kidney injury: an intensivist’s perspective, John R. Prowle, Pediatr Nephrol (2014) 29:13–21 10
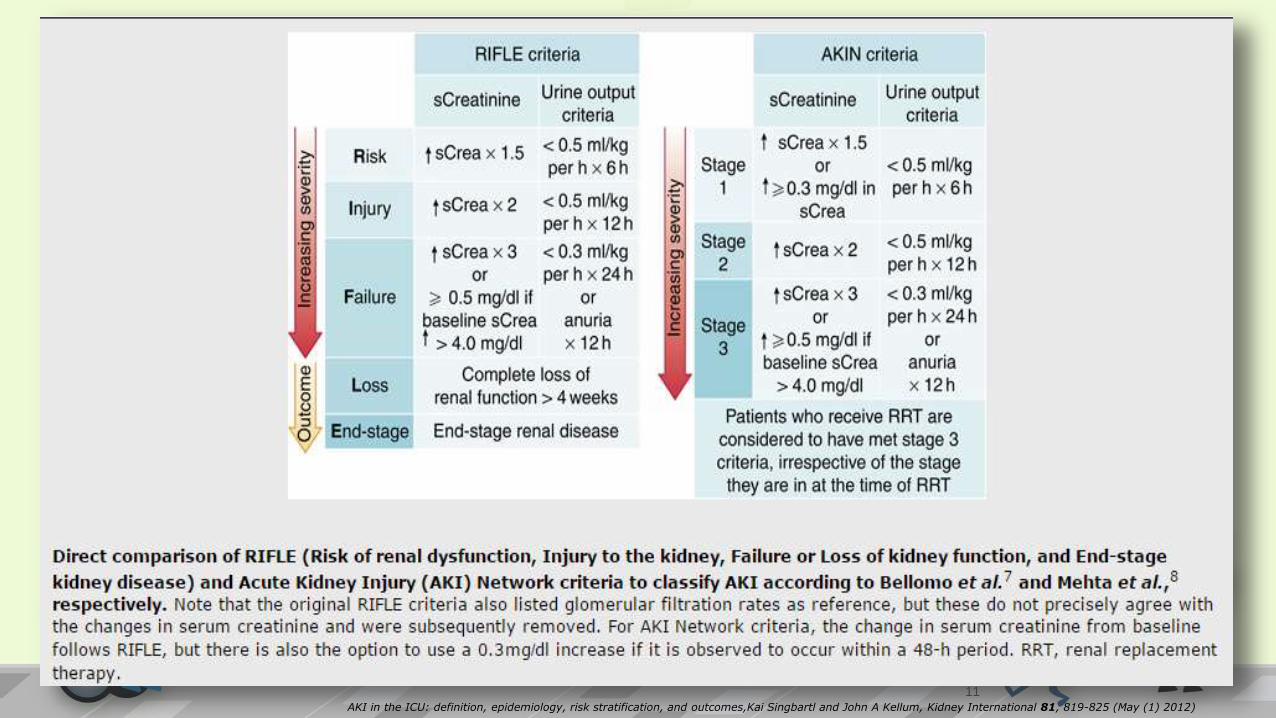
AKI in the ICU: definition, epidemiology, risk stratification, and outcomes,Kai Singbartl and John A Kellum, Kidney International 81, 819-825 (May (1) 2012)
11

12

KDIGO staging system for severity of AKI
Defines AKI as any of the following:
• serum creatinine by 0.3mg.dL (≥26µmol.L) within 48Hrs
OR
• serum creatinine to ≥1.5 times baseline, which is known or presumed to have occurred within prior 7 days
OR
• Urine volume <0.5ml/kg/H for 6 Hrs
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13813

14

Management of AKI
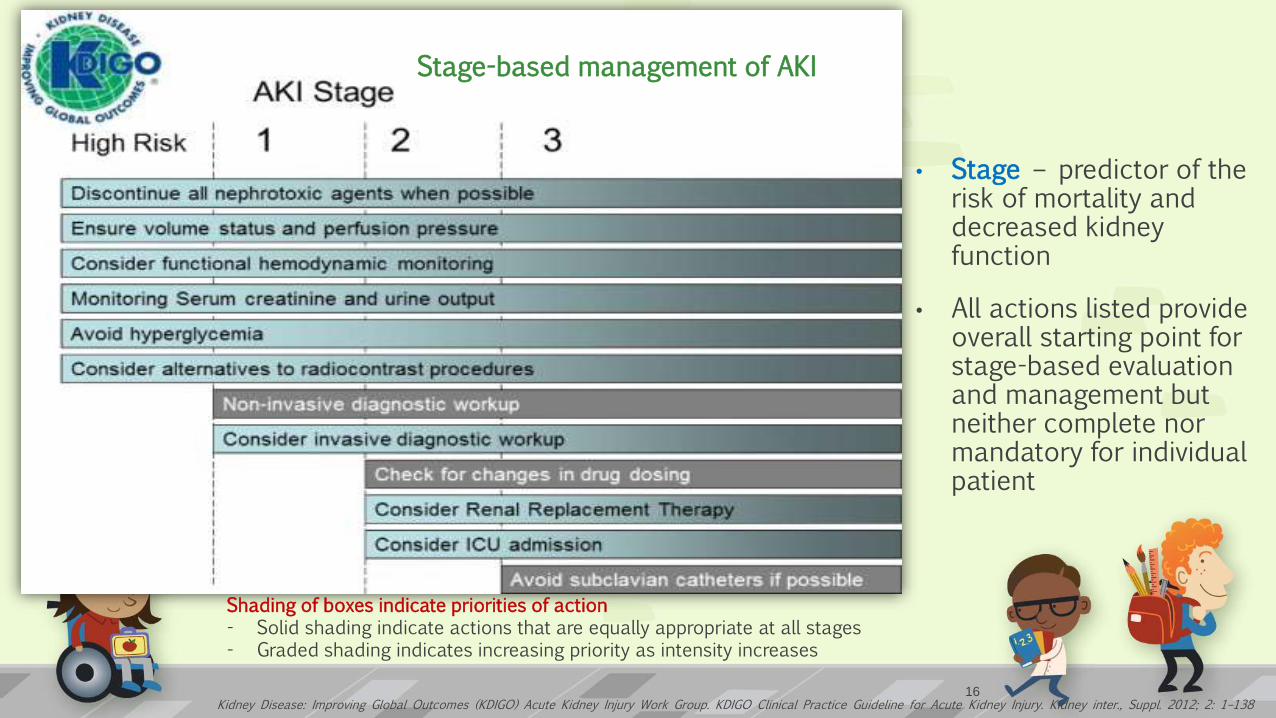
Stage-based management of AKI
Shading of boxes indicate priorities of action- Solid shading indicate actions that are equally appropriate at all stages- Graded shading indicates increasing priority as intensity increases
• Stage – predictor of the risk of mortality and decreased kidney function
• All actions listed provide overall starting point for stage-based evaluation and management but neither complete nor mandatory for individual patient
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13816

Fluid Management
Fluid overload
• Associated with increased morbidity and mortality in adult and children developing AKI
• Degree of fluid overload has been suggested as an Index of AKI severity in pediatric population
• Associated with impaired recovery of renal function in patient surviving critical illness
“Children have smaller window of appropriate treatment as they are more at risk of harm from inadequate cardiac preload & more sensitive to adverse effects of fluid overload”
17

Acute kidney injury: an intensivist’s perspective, John R. Prowle, Pediatr Nephrol (2014) 29:13–21 18

Protocolized hemodynamic management
• Suggested for use to prevent development or worsening of AKI in high risk patient in perioperative settings or in patient with sepsis induced tissue hypoperfusion
(defined as hypotension persisting after initial fluid challenge or blood lactate >4mmolL)
• Should be started as soon as hypoperfusion is recognized – “Early goal directed therapy”
• During 1st 6 hours of resuscitation to achieve specific physiologic end-points: GOALS of initial resuscitation
1. CVP 8-12mmHg or 12-15mmHg in ventilated patients
2. MAP ≥ 65mmHg
3. Urine output ≥ 0.5ml/kg/hr
4. Superior vena cava oxygenation or mixed venous oxygen saturation 70% or 65% respectively
• Suggest targeting resuscitation to normalize lactate in patients with elevated lactate level
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–138Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 19
Diuretics and dopamine receptor agonist
• Diuretics and “ renal dose” dopamine commonly used to prevent or limit AKI
Diuretics:
• Observational studies: 59-70% of patient with AKI were given diuretics at the time of nephrology consultation or before the start of RRT
• Stimulation of urine output eases management of AKI but conversion of oliguric to non-oliguric AKI – not proven to alter the course of renal failure
• Retrospective study does actually demonstrated the use of diuretics in AKI was associated with adverse outcome
• High dose of frusemide can cause ototoxicity, continued use in individual patients with AKI need to take into consideration the risk and potential benefits or lack of benefits
• Using diuretics is not recommended to prevent AKI or treat AKI except in the management of fluid overload
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13821

‘Renal dose’ dopamine
• 0.5µg/kg/min to 3-5µg/kg/min
• To improve renal perfusion following ischemic insult – common in intensive units
• Action: increased renal blood flow by promoting vasodilatation
• May improve urine output by promoting natriuresis
• No definitive studies to demonstrate low dose dopamine are effective in decreasing need for dialysis or improve survival times in patient with AKI
• Some study showed that renal dose dopamine is not effective in therapy of AKI and one study demonstrated that low doses worsened renal perfusion and renal function
Lauschke A, Teichgraber UKM, Frei U, Eckardt KU (2006) “Low-dose” dopamine worsens renal perfusion in patients with acute renal failure. Kidney Int69:1669–1674
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13822

General supportive management
Glycemic control
• Tight glycemic control frequently used in patient at risk of AKI or developed AKI
• Help reduce severity of AKI
• Intensive Insulin Therapy (IIT – glucose 4.44-6.11mmol/L) vs. Conventional Insulin therapy (CIT-glucose 9.99-11.1mmol/L) in critically ill patient
• Risk of hypoglycemia is higher in IIT (NICE-SUGAR trial in adult)
• Work group suggestion: using insulin to prevent hyperglycemia
• Aim glucose control between 6.11mmol/L to 8.33mmol/L
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13823

Nutritional aspect:
• Protein-calorie malnutrition is an important independent predictor of in-hospital mortality in patients with AKI
• Must consider metabolic derangement and proinflammatory state associated with renal failure and derangement of nutritional balance due to RRT
• Suggest achieving total energy intake of 20-30kcal/kg/day in patients with any stage of AKI
• Avoid restriction of protein intake with the aim of preventing or delaying initiation of RRT
• Protein administration:
• 0.8-1.0g/kg/day in noncatabolic AKI
• 1.0-1.5g/kg/day in patient with AKI on dialysis
• Up to maximum 1.7g/kg/day in patient on continuous renal replacement therapy (CRRT) and in hypercatabolic patient
• Suggest enteral feeding – help maintain gut integrity, reduce gut atrophy & bacterial or endotoxin translocation
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13824
Referring to Nephrologist:
• Discuss the management of acute kidney injury with nephrologist as soon as possible and within 24hours of detection when ≥ 1 of the following present:
1. When patients meet the criteria for renal replacement therapy
2. Possible diagnosis that may need specialist treatment (e.g. vasculitis, glomerulonephritis, tubulointerstitial nephritis or myeloma)
3. Acute kidney injury with no clear cause
4. Inadequate response to treatment
5. Complications associated with AKI
6. Stage 3 AKI according to pRIFLE, AKIN or KDIGO criteria
7. Renal transplant patient
8. Chronic kidney disease stage 4 or 5
Prevention, detection and management of acute kidney injury up to the point of renal replacement therapy; NICE clinical guideline 201325

Timing for Renal Replacement Therapy
26

Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–13827
• Discontinue RRT when it is no longer required, either because intrinsic kidney function has recovered to the point that it is adequate to meet patient needs, or because RRT is no longer consistent with the goals of care
28
Prognosis of AKI• Highly dependent on etiology of AKI
• Those developing AKI as a part of multiorgan failure has higher mortality rate than children with intrinsic cause of AKI e.g. HUS, or RPGN.
• Recovery: depends on etiology
• Nephrotoxic AKI and hypoxic/ischemic AKI – usually recover normal renal function
• Some still can have CKD
• Children that suffer substantial loss of nephrons as in HUS/ RPGN – at risk of renal failure long after initial insult
• Follow up:1. Adult- 2-3years
2. Children and young people: longer follow up beyond puberty
3. Important complications for children – hypertension, proteinuria, reduced renal function
1. Acute kidney injury in children, S. Phillips Andreoli, Pediatr Nephrol (2009) 24:253–2632. Prevention, detection and management of acute kidney injury up to the point of renal replacement therapy; NICE clinical guideline 201329

TAKE HOME MESSAGES:
30
REFERENCES:
1. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter., Suppl. 2012; 2: 1–138.
2. Acute kidney injury: an intensivist’s perspective, John R. Prowle, Pediatr Nephrol (2014) 29:13–21
3. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes, Kai Singbartl and John A Kellum, Kidney International 81, 819-825 (May (1) 2012
4. Prevention, detection and management of acute kidney injury up to the point of renal replacement therapy; NICE clinical guideline 2013
5. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012
6. Acute kidney injury in children, S. Phillips Andreoli, Pediatr Nephrol (2009) 24:253–263














