ACUTE CHOLECYSTITS - admin.indepreview.comadmin.indepreview.com/article/VOL. 15 No. 04/004 295...
7
Key Contents Pathology of Acute Cholecystitis Carries of Acute Cholecystitis Investigation for Acute Cholecystitis Treatment for Acute Cholecystitis Learning Objectives To describe of Acute Cholecystitis To understand diagnostic features of Acute Cholecystitis To explain management of Acute Cholecystitis Article Citation: Tahir S.M, Acute Cholecystits. Indep Rev Oct-Dec 2013;15(10-12): 417-423 ACUTE CHOLECYSTITS Indep Rev Oct-Dec 2013;15(10-12) IR-295 Muhammad Shuja Tahir Key words: Acute Pneumonia, Nosocomial Pneumonia, Grey Repatriation of Pneumonia. Correspondence Address: DR. MUHAMMAD SHUJA TAHIR Professor of Surgery Independent Medical College / Independent University Hospital [email protected] 417 www.indepreview.com Indep Rev Oct-Dec 2013;15(10-12) 417-423
Transcript of ACUTE CHOLECYSTITS - admin.indepreview.comadmin.indepreview.com/article/VOL. 15 No. 04/004 295...

Key Contents
Pathology of Acute CholecystitisCarries of Acute Cholecystitis
Investigation for Acute Cholecystitis Treatment for Acute Cholecystitis
Learning Objectives
To describe of Acute CholecystitisTo understand diagnostic features of Acute Cholecystitis
To explain management of Acute Cholecystitis
Article Citation: Tahir S.M, Acute Cholecystits. Indep Rev Oct-Dec 2013;15(10-12): 417-423
ACUTE CHOLECYSTITS
Indep Rev Oct-Dec 2013;15(10-12) IR-295
Muhammad Shuja Tahir
Key words: Acute Pneumonia, Nosocomial Pneumonia, Grey Repatriation of Pneumonia.
Correspondence Address:
DR. MUHAMMAD SHUJA TAHIR Professor of Surgery Independent Medical College / Independent University [email protected]
417www.indepreview.comIndep Rev Oct-Dec 2013;15(10-12) 417-423

2
Acute cholecystitis is the acute inflammation of the gall bladder and it presents as an emergency with upper abdominal pain, fever and vomiting. The onset of the symptoms may be sudden or gradual.
CLINICAL FEATURESPAINIt is severe, agonizing and of sudden onset lasting for more than 12hrs. It is located in the right hypochondrium and radiates to the back in between the shoulder blades. The pain may be felt in the epigastrium. It may be continuous and progressive with the progress in the disease process. The pain may be colicky in nature and it may be worse in post-prandial period in obstructive cholecystitis.
Acute cholecystitis is obstructive in nature in 95% of cases due to impaction of stone in the
1Hartmann's pouch or cystic duct . The pain may
2occur during night always at about same time .
NAUSEA AND VOMITINGThese symptoms are present earlier during the attack and continue throughout the illness. The vomiting makes the pain even worse. It is usually because of pylorospasm.
PYREXIAO
It is almost always present. Sometimes 38 C degrees centigrade or even higher degrees are
associated with rigors. This happens specially in fulminating cases.
JAUNDICEIt may be present due to inflammation of the biliary passages. Cholangitis is associated in 20-25% of the patients. Obstructive jaundice may also be associated with acute cholecystitis. Bile duct stones are present in 23% of the patients with acute cholecystitis.
ABDOMINAL DISTENSIONMild abdominal distension is seen in severe cases of acute cholecystitis.
TENDERNESS AND RIGIDITYIt is present in the right hypochondrium.
MURPHY'S SIGN It is inspiratory arrest during palpation of the right subcostal region due to pain. It is positive in
3acute cholecystitis .
BOAS' SIGNIt is the presence of area of hyperaesthesia below the tip of right scapula and opposite T , T and 11 12
3L1 vertebrae in the posterior axillary line .
418www.indepreview.comIndep Rev Oct-Dec 2013;15(10-12) 417-423
Inflamed gall bladder seen with naked eye
Murphy’s Sign
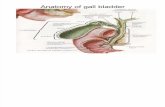
Acute Cholecystitis

MASS UPPER ABDOMENA tender palpable mass of variable size is present in the right hypochondrium and subcostal area. It is present in 25% of the patients. It indicates following complications of acute cholecystitis ; Mass formation due to omental
adhesions along inflammed gall bladder. Empyema of gall bladder. Per forat ion and local abscess
formation. Carcinoma gall bladder associated with
acute inflammation.
BLOOD EXAMINATION Haemoglobin estimation Total leucocyte count (leucocytosis) Differential leucocyte count(polymorphs
are Increased) Sedimentation rate (raised) Liver function tests done to rule out
associated Hepatic pathology and in case of Jaundice to define the type of jaundice
Screening for Hepatitis B & C Clotting profile is advisable in cases of
jaundice Urea and electrolytes: may be disturbed
due to vomiting and dehydration.
ULTRASOUND SCAN The diagnosis is usually confirmed by ultrasonography. The diagnostic characteristics are ; Thick walled (>3mm) gall bladder Distended gall bladder with/without
stones in cases of acalculous cholecystitis
Pericholecystic fluid Murphy’s sign elicited by ultrasound
probe.
RADIOLOGICAL EXAMINATIONX-ray of the chest and abdomen (plain). These help in the diagnosis of radio opaque gall stones and chest lesions (pneumonia and pleural
3
419www.indepreview.comIndep Rev Oct-Dec 2013;15(10-12) 417-423
Boas Sign (red area represents area of hyperaesthesia)
Acute cholecystitis with gallstone
Inflammed gallbladder with pericholecystic fluid (white arrow)
Acute Cholecystitis

Discharge Percutaneous Cholecystostomy
Determine Surgical risk
High risk (ASA III-V)
Clinical Improvement
Clinical deterioration
Low risk (ASA I,II)
Clinical Improvement
Clinical deterioration
Delayed Cholecystecomy
after 6 weeks
Early Cholecystectomywith in 24 hours
Emergency Cholecystectomy
Delayed Cholecystectomy
Hospital admission Supportive care
Antibiotics
Acute Cholecystitis
4
420www.indepreview.comIndep Rev Oct-Dec 2013;15(10-12) 417-423
Acute Cholecystitis

5
421www.indepreview.com
effusion). Oral cholecystogram is not performed during acute attack of cholecystitis. In fact this investigation is no more performed for any indication.
ULTRASOUND SCAN It is the best investigation during acute cholecystitis as it helps to confirm the diagnosis immediately and it is not invasive at all.
CT SCANCT scan is extremely helpful in the diagnosis of acute cholecystitis. It is available at most of the places.
DIFFERENTIAL DIAGNOSISThis condition is to be differentiated from all causes of acute abdomen and certain chest lesions such as ; Acute appendicitis. (specially high and retrocaecal) Perforated duodenal ulcer Acute pancreatitis. Acute pyelonephritis on right side. Acute coronary thrombosis (Inferior wall ischemia) Right basal pneumonia.
TREATMENTAcute cholecystitis is a surgical emergency and requires treatment which is initially conservative and followed by definitive surgical treatment.
CONSERVATIVEMost patients respond to conservative treatment. More than 90 % of patients get satisfactory relief from acute attack of cholecystitis with the following conservative regimen : Nil by mouth and NG aspiration Fluid and Electrolyte replacement
Indep Rev Oct-Dec 2013;15(10-12) 417-423
Ultrasound scan showing inflamed gall bladder
Ultrasound scan showing inflamed gall bladder
CT Scan showing inflamed gall bladder
Acute Cholecystitis

Parenteral Analgesia Parenteral Antibiotic
NIL BY MOUTH AND NG ASPIRATION Rest to the gall bladder and biliary passages is provided by stopping oral intake. It is further offered to upper gastrointestinal track by nasogastric aspiration.
FLUIDS AND ELECTROLYTESFluids and electrolytes are given intravenously or in less severe cases, oral fluids may be permitted.
PARENTERAL ANALGESICS:Parenteral analgesia is given to make the patients pain free. NSAIDS in mild and moderate cases. Narcotic analgesia is recommended in severe pain.
ANTIBIOTICSQuinolones, penicillins and appropriate antibiotics (cephalosporins) to cover gram negative gut organism, are used parenterally or orally. Diabetics are prone to gangrenous cholecystitis. Anaerobic cover should be provided to them (e.g. metronidazole).
SURGICAL Conservative management is followed by definitive surgical removal of gall bladder. It can be either laparoscopic or open depending upon the choice of surgeon and facilities available. The timing of surgery is of crucial importance.
EARLY CHOLECYSTECTOMY This is removal of gall bladder within 24 to 48 hours of acute episode. It is the preferred timing for surgery in patients who have responded to conservative measures.
DELAYED CHOLECYSTECTOMY Six to twelve week after the relief of acute episode, delayed cholecystectomy is performed.
URGENT CHOLECYSTECTOMY This is an emergency procedure indicated in following conditions; Failed response to conservative
measures Generalized peritonitis Diabetic patientsCholecystectomy can be performed through open surgery or laparoscopic surgery depending upon expertise available. If signs of peritonitis develop or the patient fails to get relief after conservative management.
6
422www.indepreview.comIndep Rev Oct-Dec 2013;15(10-12) 417-423
Inflammed gall bladder seen at laparotomy
Inflammed gall bladder with stone
Acute Cholecystitis

7
423www.indepreview.com
Acute Cholecystitis
Indep Rev Oct-Dec 2013;15(10-12) 417-423
Cholecystectomy is considered as early as possible.
COMPLICATIONS Empyema of the gall bladder. Gangrene of the gall bladder.
Gas gangrene. Local abscess formation. Perforation and peritonitis. Internal fistula formation.
Chronic cholecystitis.
REFERENCES1. A Cuschieri. GR Giles. AR Moossa. Essential
surgical practice third edition. Butterworth Heineman. 1995. p:1175-1237.
2. Tranerso LW. Clinical manifestation and impact of gall stone disease. American journal of surgery. [JC:3z4]1993 Apr. 165(4): 405-9.
3. Shuja Tahir. Mahnaaz Roohi. Zahid Yasin
Hashmi. Surgery clinical examination system third edition. URO-OBS (Pvt) LTD. 1992 Dec. p: 131-133.
4. Runbens DJ. Hepatobiliary imaging and its pitfalls. Radiol clin north am 2004; 42:257-278.
5. Cameron IC, Chadwicke management of acute chole cystitis in U.k hospitals: time for a change. postgrad med J2004;80:292-294.