Acute appendicitis during pregnancy
4
Click here to load reader
-
Upload
alberto-gomez -
Category
Documents
-
view
217 -
download
3
Transcript of Acute appendicitis during pregnancy

Acute Appendicitis during Pregnancy
Albert0 Gomez, MD, Phoenix, Arizona
MacDonald Wood, MD, FACS, Phoenix, Arizona
Acute appendicitis is the most common surgical emergency occurring during pregnancy [I], but it is infrequently encountered by an individual surgeon. Diagnosis of acute appendicitis is often difficult in the pregnant patient as the symptoms may be at- tributed to the pregnancy. Physical findings may be obscured or altered by the cephalad displacement of the appendix as pregnancy progresses. Difficulty in diagnosis and delay in treatment may result in complications or death for the fetus or the mother or both.
The present report is a retrospective review and analysis of an eight year experience (1970-1977) from three metropolitan hospitals in Phoenix (Maricopa County General, Good Samaritan, and St. Joseph’s) of patients having acute appendicitis during preg- nancy. The diagnosis of acute appendicitis was made by operative and histologic examinations in thirty- five patients. There was zero maternal mortality and no fetal loss.
The diagnostic problems, management, and complications are presented and a review of medical publications discussed.
Clinical Experience
Patients with acute appendicitis occurring during pregnancy, which was diagnosed and treated at three large hospitals in the Phoenix metropolitan area over an eight year period (1970-1977), were analyzed. Excluded from this review were cases in which the histologic study of the appendix showed periappendicitis, chronic appendicitis, or normal appendix.
From Department of Surgery, Maricopa County General Hospital, Phoenix, Arizona.
Reprint requests should be addressed to Albert0 Gomez, MD, Maricopa County General Hospital, 2601 East Roosevelt Street, Phoenix, Arizona 85008.
Presented at the Thirtieth Annual Meeting of the Southwestern Surgical Congress, Palm Springs, California, April 17-20, 1978.
For each patient the length of gestation was divided into trimesters. There were no case reports of appendicitis during labor or in the puerperium.
Incidence. During this period there were 76,608 deliv- eries. The number of deliveries and reports of acute ap- pendicitis were about equally divided between the three hospitals. The incidence of acute appendicitis (35 cases) was 1 per 2,188 deliveries.
Age and Purity. Acute appendicitis was most common in the twenty to twenty-five year age group, but the age range extended from fifteen to thirty-four years (average, 22 years). It was most frequently seen in women having two or more pregnancies (24 patients, 66 per cent).
Duration of Pregnancy. Acute appendicitis was less common in the last trimester (26 per cent). Almost half the patients were in the second trimester. (Table I.)
Symptoms and Findings. Eighty-eight per cent of the patients had symptoms for less than 24 hours. (Table I.) The duration of symptoms ranged from 6 hours to six days. Four pregnant women had complaints for more than 24 hours. One patient, with a thirty week pregnancy, had been ill for six days before hospital admission, and her operation was not performed for an additional four days (see Oper- ative Findings).
Fifty-one per cent (18 patients) were anorexic. Nausea and vomiting were common complaints (71 and 54 per cent). Dysuria was infrequent (8.5 per cent).
Each patient complained of abdominal pain and had tenderness in the abdomen. Muscle guarding and rebound tenderness were usually detected (68 and 77 per cent, re- spectively). An elevated temperature (greater than 98.6’F) was observed in twenty-one patients (60 per cent).
Pain and tenderness in the right lower quadrant of the abdomen were most frequently observed during the first six months of pregnancy and were the most common findings in our series. (Table II.) The two patients who had diffuse abdominal pain and tenderness were in their third trimester of pregnancy.
White blood cell counts of more than 15,000/mm3 were found in only one third of patients, and three (8.5 per cent) had leukocytosis of more than 20,00O/mms. A normal uri-
180 The Amertcan Journal of Surgery

Appendicitis during Pregnancy
TABLE I Time Lapse from Onset to Admission and Admission to Operation per Trimester
Patients in Each Trimester 1st 2nd 3rd
(n=9) (n=17) (n = 9)
From Onset to Admission <12 hr 1 1 12-24 hr 8 14 7 >24 hr 2 2
From Admission to Operation <12 hr 7 16 6 12-24 hr 1 1 2 >24 hr 1 1
TABLE II Location of Pain and Tenderness in Patients in Different Trimesters
Total (n = 35) Location
Patients in Each Trimester
1st 2nd 3rd Total
2 29
4
Right lower quadrant 16 9 3 27 Right upper quadrant 1 3 4 Flank 1 1 2 Diffuse 2 2
29 4 2
nalysis result was a common finding (29 patients, 82.8 per cent).
One patient in her first trimester was ill for 29 hours, and a definite diagnosis could not be established. At laparos- copy pus was seen, and immediate laparotomy was done. A perforated appendix with generalized peritonitis was found.
Operative Management. Twenty-nine patients were operated on within 12 hours after admission, and four during the next 24 hours. The range of time to operation was as short as 1 hour to a delay in one patient of 29 hours and in another of as long as four days after admission. (Table I.)
Each patient received a general anesthetic, and the op- eration was performed by a general surgeon.
The location of the incision varied; a McBurney mus- cle-splitting incision was used in twenty-two patients, a lower midline incision in three, a right paramedian incision in seven, and an upper midline incision in three.
Operative Findings. (Table ZZZ.) Uncomplicated acute appendicitis was found in twenty-seven patients (77.1 per cent).
Appendicitis with gangrene but no perforation was found in four patients (11.4 per cent). Symptoms were present from 12 to 24 hours, and each was operated on within 6 hours of admission (see Complications).
Four patients had acute appendicitis with perforation, and two of these had generalized peritonitis. One had symptoms for 8 hours before admission but waited 29 hours before appendectomy was performed; no complication developed. The other patient had had complaints for 24 hours; premature delivery after a thirty-three week ges- tation occurred on the first postoperative day.
Two patients who had acute appendicitis with perfora- tion had abscess formation. One had symptoms for only 24 hours and was operated on within the next 16 hours. The other waited for six days before hospital admission, and appendectomy was not performed for an additional four days. Neither patient had complications.
Complications. Complications were minimal. The rec- ords of five patients had no information available after hospital discharge as to maternal or fetal outcome. In the remaining group there were no maternal deaths and there was no fetal loss. Three patients, thirty, thirty-three, and
thirty-four weeks pregnant, went into premature labor after appendectomy, with survival of the infants; one pa- tient had acute appendicitis, one had appendicitis with gangrene, and one had perforation and generalized peri- tonitis.
The only wound complication was a superficial infection in a woman with a ten week gestation who had been ill for 12 hours and was operated on 2 hours after hospital ad- mission. She had appendicitis with gangrene without perforation. One patient had atelectasis with fever and another had a urinary tract infection.
Duration of Hospitalization. The average hospital stay was 5.4 days, with a range extending from four to fifteen days.
Comments
Incidence. The incidence of appendicitis occurring during pregnancy varies with different authors. Ba- baknia, Parse, and Woodruff [2] in a recent review of 503,496 deliveries reported an incidence of ap- pendicitis of 1 in 1,500 deliveries. The incidence in our report is 1 per 2,188 deliveries.
Acute appendicitis is considered to be the most frequent extrauterine complication of pregnancy requiring surgery [3]. Basically it is the same disease process as in the nonpregnant woman, but the diag- nosis may be more difficult in the pregnant patient with the site of the appendix shifting as the preg- nancy progresses. Appendicitis is not more common during pregnancy.
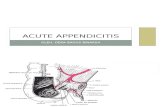
Position of Append&. Baer, Reis, and Arens [4] in 1932 demonstrated the variations in the position of the appendix caused by the enlarged uterus. The appendix lies at the iliac crest level at the fifth month of pregnancy and rises above this level during the last
TABLE III Operative Findings According to Trimester
Patients in Each Trimester
1st 2nd 3rd Total
Acute inflammation 6 14 7 27 Gangrene 2 2 4 Perforation 1 1 2 4
Total 9 17 9 35
Volume 137, February 1979 181

Gomez and Wood
Figure 1. Changes in position and direction of appendix during pregnancy. Postpartum (PP) position of the ap- pendix. (Rap&ted with permission of the publisher [ 4 1. Copyr/ght lg33, American Medfcaf Association. )
trimester [4]. This displacement accounts for the localization of pain and tenderness in the right upper quadrant and flank whenever inflammation spreads to the parietal peritoneum. (Figure 1.)
In the latter months of pregnancy it is imperative to diagnose acute appendicitis early. The infectious process may disseminate more rapidly than usual because the bulk of the uterus displaces the omentum upward, preventing its confinement of the infection. The appendix is also elevated from its normal posi- tion in the false pelvis into the general abdominal cavity [5].
Symptoms and Findings. The most constant clinical signs encountered in acute appendicitis during pregnancy are vague pain in the right side of the abdomen and intraabdominal inflammation [6]. In our series each patient complained of abdominal .pain at the time of admission to the hospital.
Abdominal tenderness is noted in the majority of patients, and as pregnancy advances, the pain and tenderness are situated higher and more laterally in
182
the abdomen. Anorexia is usually considered to be present in almost all patients with appendicitis, but in our series only 51 per cent of the patients had this symptom.
Rebound tenderness and muscle guarding are valuable findings in the diagnosis of appendicitis in pregnancy, but because of the laxity of the abdominal muscles, these signs are found less frequently in the gravid patient [7]. In our series muscle guarding was noted in 68 per cent of the patients and rebound tenderness in 77 per cent.
The laboratory findings during pregnancy should be interpreted carefully, since leukocytosis is normal during pregnancy and may be as much as 15,OOW mm3 [I]. In our series the white blood cell counts ranged from 5,500 to 22,000/mm3, and 77 per cent of our patients had counts of more than lO,OOO/mms. All patients with appendicitis with gangrene and with perforation had white blood cell counts of more than 12,000/mm3.
Incision. The type and location of incision vary according to the stage of gestation. A muscle-splitting incision centered over the point of maximum ten- derness provides excellent exposure, and tilting the patient 30 degrees toward the left side may be of help
[71. Laparoscopy. Laparoscopy was diagnostic in one
of our patients in whom the disease could not be es- tablished clinically. In cases of abdominal pain of unknown cause, laparoscopy may resolve the ques- tion of acute appendicitis. This diagnostic tool can greatly improve patient management and often makes laparotomy unnecessary [a].
Hormone Therapy. Hormone therapy in the pre- vention of premature labor is of doubtful value [3]. Progesterone was given to three of our patients; no complications occurred.
Antibiotics. The use of routine antibiotics in acute appendicitis is debatable. In our series twelve pa- tients were given antibiotics prior to surgery. Anti- biotic administration was continued postoperatively in eight patients in whom gangrene or perforation was found.
The routine use of antibiotics in simple acute in- flammation seems unjustified. Several studies have demonstrated antibiotics to be of no benefit in non- perforative appendicitis [9] and should be reserved only for patients with clinical evidence of gangrene or perforation [IO].
Maternal and Fetal Mortality. Since the report of Babler [II] in 1908 of a maternal mortality of 24 per cent, there has been a dramatic decline in the death rate from acute appendicitis during pregnancy. Of two large current reported series (19761, one by
The American Journal of Surgery

Appendicitis during Pregnancy
Townsend and Greias [12] gives a maternal mortality of 0.4 per cent and one by Babaknia, Parsa, and Woodruff [2] gives a mortality of 0.01 per cent. (Table IV.) Maternal mortality now occurs infre- quently and is almost always associated with acute appendicitis with perforation and generalized peri- tonitis. In our series there were no maternal deaths.
The decline in maternal mortality has been at- tributed by some [3,14] to the use of antibiotics. Realistically, the low mortality is probably due to multiple factors: better fluid and nutritional support; prompt diagnosis and treatment; better anesthesia; and overall improved surgical care as well as antibi- otics.
Fetal loss has likewise decreased from 40 per cent in 1908 to 8.5 per cent in 1976. (Table IV.) Never- theless, general peritonitis adversely affects the outcome of pregnancy. Although the rate of preg- nancy interruption associated with generalized per- itonitis has decreased by half over the past seventy years, there still was a fetal loss of 35.7 per cent in 1976. (Table V.) There was no fetal loss in our series; the three premature deliveries all resulted in healthy babies.
Delay in operative intervention is the main cause of maternal death and of fetal loss.
Conclusions
(1) The diagnosis of acute appendicitis occurring during the first six months of pregnancy can usually be made with little difficulty. The clinical and labo- ratory findings are essentially the same as those in the nonpregnant patient.
(2) Difficulty in diagnosis exists in the third tri- mester when the appendix is displaced from its usual normal location.
(3) Delay in operative intervention is the main cause of fetal loss and of maternal complications.
(4) If appendicitis is suspected in a pregnant woman, immediate operation is indicated.
Summary
Case reports (1970-1977) of thirty-five pregnant women with acute appendicitis were reviewed. Eighty-eight per cent had symptoms less than 24 hours and were operated on within 12 hours. No maternal or fetal loss occurred. Morbidity and mor-
TABLE IV Acute Appendicitis during Pregnancy
No. of Maternal Fetal Author Cases Mortality Mortality
Babler[ll] (1908) 207 24.0% 40.0% McDonald[lS] (1929) 274 13.5% 37.0% Black[S] (1960) 273 4.6% 17.0% Brant[74] (1967) 256 2.0% 17.3% Townsend[72] (1976) 451 0.4% 8.5% Babaknia/2] (1976) 333 0.01% 8.7%
TABLE V Fetal Mortality with Per’onitls
Mortalitv
Babler[lI] (1908) 78.8% Meiling[ 151 (1947) 72.0% Hoffm~~[l~] (1953) Babaknia[2] (1976)
35.2% 35.7%
tality should be minimal if, when appendicitis is suspected in a pregnant woman, immediate operation is performed.
References
1. O’Neill JP: Surgical conditions compiiiting pregnancy. I. Acute appendicitis-real and simulated. A& NZJ Obstet Gyneco/ 9: 94, 1969.
2. Babaknia A, Parsa H, Woodruff JD: Appendicitis during preg- nancy. O&et -co/ 50: 40. 1977.
3. Sarason EL, Bauman S: Acute appendicitis in pregnancy: dlf- ficulties in diagnosis. obstet Gyneco/ 22: 382, 1963.
4. Baer JL, Reis RA, Arens RA: Appendicitis in pregnancy. JAMA 98: 1359, 1932.
5. Black WP: Acute appendicitis in pregnancy. Br Med J 1: 1938, 1960.
6. Roseman GWE: Acute appendicitis in pregnancy. S Afr Med J 49: 1459,1975.
7. Cunningham FG, McCubbin JH: Appendicitis complicating pregnancy. Obstet Gynecol45: 415, 1975.
8. Robinson HB, Smith GW: Applications for laparoscopy in general surgery. Surg Gynecol Obstet 143: 829, 1976.
9. Law D, Law R, Eiseman B: The continuing challenge of acute and perforated appendicitis. Am J Surg 131: 533, 1976.
IO. Stone HH, Sanders SL, Martin JD, Jr: Perforated appendicitis in children. Surgery 69: 673, 1971.
11. Babler EA: Perforative appendicitis complicating pregnancy. JAMA 51: 1310, 1908.
12. Townsend JM, Greiss FC: Appendicitis in pregnancy. South Med J69: 1161, 1976.
13. McDonaM AL: Appendicitis in pregnancy. Am J Obsret Gyneco/ 18: 110, 1929.
14. &ant HA: Acute appendicitis in pregnancy. Obstet Gyneco/ 29: 130, 1967.
15. Meiling RL: Appendicitis complicating pregnancy, labor and the puerperium. Surg @neco/ obstet 85: 5 12, 1947.
16. Hoffman ES, Suzuki M: Acute appendicitis in pregnancy, A ten year survey. Am J Obstet Gynecol67: 1338, 1954.
Volume 137, February 1979 183












![Acute Appendicitis[1]](https://static.fdocuments.in/doc/165x107/577cd3341a28ab9e7896e8e0/acute-appendicitis1.jpg)