Acupuncture for Refractory Cases of Sudden Hearing Loss
7
Acupuncture for Refractory Cases of Sudden Sensorineural Hearing Loss Chang Shik Yin, KMD, PhD, 1 Hi-Joon Park, KMD, PhD, 1 and Hae Jeong Nam, KMD, PhD 2 Abstract Objectives: The aim of this study was to investigate the effect of acupuncture on the treatment of refractory sensorineural hearing loss (SSHL), treatment of which remains a major clinical challenge. Design: The study design was descriptive research to document the effect of acupuncture in a series of SSHL cases. Setting: The study was conducted in the outpatient clinic of Kyung Hee University Hospital. Subjects: The subjects analyzed were 17 patients with refractory SSHL of more than 3 weeks after a failed trial of conventional treatment including corticosteroids. Interventions: Acupuncture sessions were performed twice a week using a modified Saam acupuncture formula and such acupoints as GV14, GV15, and others, in addition to usual patient care educations. Main outcome measures: Improvement was defined as increased hearing threshold from initial measurement by more than 20 dB in at least two contiguous frequencies of audiometric testing. An audiogram pattern was also analyzed. Results: The average refractory period before acupuncture treatment was 213.9 days (range 22–1460). First follow-up measurement after 9.5 times of acupuncture treatment for 29.9 days showed improvement in 4 of 16 cases examined (25.0%) and second follow-up measurement after 18.7 times of acupuncture treatment for 70.4 days in another 4 of 12 cases examined (33.3%). A total improvement rate after day 70.4 post initial visit was 47.1% (8 of 17 cases). As to the audiogram pattern, an ascending or midhumping pattern was related to a good prognosis, while a descending pattern was not. Conclusions: These findings suggest that acupuncture might be effective in refractory sensorineural hearing loss with failure of conventional therapy. Introduction S udden sensorineural hearing loss (SSHL), most cases of which are idiopathic, 1 is defined as a 30 dB or more level of hearing loss in three or more consecutive frequencies that occurs within a 3-day period. 2 Idiopathic sensorineural hearing loss, a form of sensorineural hearing loss that may be effectively managed by a primary care physician, 3 is a rare but possibly frightening experience, with overall reported inci- dence ranging from 5 to 20 per 100,000 people per year. 4 In addition to the uncertainty of the cause, controversy over the treatment is ongoing. SSHL lacks a strong evidence-based guideline. 2 Evidence is questionable even for systemic steroid therapy, one of the most frequently used treatments. 5 The spontaneous recovery rate, whether partial or complete, is known to be as high as 68%–89% 6 or 50%–70% and there is no study that provides convincing evidence of recovery rate over spontaneous recovery rate. 7 Treatment of SSHL remains a major clinical challenge in the field of sensorineural disorders and otology, considering the stressful impact of SSHL on quality of life. 6 As most spontaneous recoveries occur 1 to 2 weeks after the onset, 8,9 treatment of refractory cases of idi- opathic SSHL that conventional therapy failed to improve would be still more difficult. Acupuncture, an ancient art of healing, has been widely used in East Asia and its frequent indication includes neu- rological conditions. 10 Although several studies reported the positive effects of acupuncture, 11,12 there have been negative reports over the effect of acupuncture on SSHL, 13,14 and previous studies often lacked definite diagnostic standards. 15 This retrospective case review study analyzed medical records to investigate the effect of acupuncture on the treatment of refractory idiopathic SSHL, and definite diag- nostic criteria of audiometric testing were adopted. Clinical 1 Acupuncture and Meridian Science Research Center, Kyung Hee University, Seoul, Republic of Korea. 2 Department of Ophthalmology and Otorhinolaryngology, College of Korean Medicine, Kyung Hee University, Seoul, Republic of Korea. THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE Volume 16, Number 9, 2010, pp. 973–978 ª Mary Ann Liebert, Inc. DOI: 10.1089/acm.2009.0542 973
-
Upload
bayu-agustinus -
Category
Documents
-
view
29 -
download
1
description
fff
Transcript of Acupuncture for Refractory Cases of Sudden Hearing Loss

Acupuncture for Refractory Cases of SuddenSensorineural Hearing Loss
Chang Shik Yin, KMD, PhD,1 Hi-Joon Park, KMD, PhD,1 and Hae Jeong Nam, KMD, PhD2
Abstract
Objectives: The aim of this study was to investigate the effect of acupuncture on the treatment of refractorysensorineural hearing loss (SSHL), treatment of which remains a major clinical challenge.Design: The study design was descriptive research to document the effect of acupuncture in a series of SSHLcases.Setting: The study was conducted in the outpatient clinic of Kyung Hee University Hospital.Subjects: The subjects analyzed were 17 patients with refractory SSHL of more than 3 weeks after a failed trial ofconventional treatment including corticosteroids.Interventions: Acupuncture sessions were performed twice a week using a modified Saam acupuncture formulaand such acupoints as GV14, GV15, and others, in addition to usual patient care educations.Main outcome measures: Improvement was defined as increased hearing threshold from initial measurement bymore than 20 dB in at least two contiguous frequencies of audiometric testing. An audiogram pattern was alsoanalyzed.Results: The average refractory period before acupuncture treatment was 213.9 days (range 22–1460). Firstfollow-up measurement after 9.5 times of acupuncture treatment for 29.9 days showed improvement in 4 of 16cases examined (25.0%) and second follow-up measurement after 18.7 times of acupuncture treatment for 70.4days in another 4 of 12 cases examined (33.3%). A total improvement rate after day 70.4 post initial visit was47.1% (8 of 17 cases). As to the audiogram pattern, an ascending or midhumping pattern was related to a goodprognosis, while a descending pattern was not.Conclusions: These findings suggest that acupuncture might be effective in refractory sensorineural hearing losswith failure of conventional therapy.
Introduction
Sudden sensorineural hearing loss (SSHL), most casesof which are idiopathic,1 is defined as a 30 dB or more
level of hearing loss in three or more consecutive frequenciesthat occurs within a 3-day period.2 Idiopathic sensorineuralhearing loss, a form of sensorineural hearing loss that may beeffectively managed by a primary care physician,3 is a rare butpossibly frightening experience, with overall reported inci-dence ranging from 5 to 20 per 100,000 people per year.4 Inaddition to the uncertainty of the cause, controversy over thetreatment is ongoing. SSHL lacks a strong evidence-basedguideline.2 Evidence is questionable even for systemic steroidtherapy, one of the most frequently used treatments.5 Thespontaneous recovery rate, whether partial or complete, isknown to be as high as 68%–89%6 or 50%–70% and there is nostudy that provides convincing evidence of recovery rate over
spontaneous recovery rate.7 Treatment of SSHL remains amajor clinical challenge in the field of sensorineural disordersand otology, considering the stressful impact of SSHL onquality of life.6 As most spontaneous recoveries occur 1 to 2weeks after the onset,8,9 treatment of refractory cases of idi-opathic SSHL that conventional therapy failed to improvewould be still more difficult.
Acupuncture, an ancient art of healing, has been widelyused in East Asia and its frequent indication includes neu-rological conditions.10 Although several studies reported thepositive effects of acupuncture,11,12 there have been negativereports over the effect of acupuncture on SSHL,13,14 andprevious studies often lacked definite diagnostic standards.15
This retrospective case review study analyzed medicalrecords to investigate the effect of acupuncture on thetreatment of refractory idiopathic SSHL, and definite diag-nostic criteria of audiometric testing were adopted. Clinical
1Acupuncture and Meridian Science Research Center, Kyung Hee University, Seoul, Republic of Korea.2Department of Ophthalmology and Otorhinolaryngology, College of Korean Medicine, Kyung Hee University, Seoul, Republic of Korea.
THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINEVolume 16, Number 9, 2010, pp. 973–978ª Mary Ann Liebert, Inc.DOI: 10.1089/acm.2009.0542
973

data were analyzed in relation to pattern of pure tone au-diogram and improvement rate.
Materials and Methods
Patients
We reviewed medical records of SSHL patients whovisited Kyung Hee Oriental Medical Hospital, Seoul fromJanuary 2008 to January 2009. Patients involved in the studymet the following inclusion criteria: (1) a diagnosis of SSHL,defined as greater than 30 dB of hearing loss at three ormore consecutive frequencies, developing within 72 hours;(2) no improvement in hearing following previous therapyincluding systemic corticosteroid treatment; (3) refractoryperiod until the start of acupuncture treatment being morethan 21 days; and (4) symptomatic state and hearing lossaudiogram of more than 30 dB hearing level in 3 or moreconsecutive frequencies2 on the day of initial visit; (5) noprevious symptom of hearing loss in the affected ear, and(6) one or more follow-up audiometric tests. Exclusioncriteria were recurrent or secondary SSHL, and fewer thanfive acupuncture treatments. History and previously per-formed magnetic resonance image or computed tomogra-phy were noted to exclude patients with SSHL causedby pathologies in the internal auditory canal or cerebello-pontine angle area, trauma, noise, tumors, otitis media, andMeniere’s disease. Patients with hearing loss in both earswere also excluded.
All patients had persistent hearing loss after conventionaltherapy such as an initial course of oral steroids, anticoagu-lants, or intravenous steroid injection. All patients underwentfull otolaryngologic history taking, physical examination, androutine audiologic evaluation. This study was approved bythe Institutional Review Board of Kyung Hee UniversityHospital.
Audiogram
The pure tone audiograms were performed on the day ofinitial visit and the day of follow-up measurements: 1st fol-low-up measurement after about 10 times of acupuncturetreatment and 2nd follow-up measurement after about 20times of acupuncture treatment (GSI 61; Grason-Stadler, Inc.,WI). Hearing threshold level was measured in the frequen-cies of 0.125, 0.25, 0.5, 1, 2, 4, and 8 kHz.16 Hearing im-provement in this study was defined as increased thresholdlevels of hearing from initial measurement by more than20 dB in two or more of contiguous frequencies.9 Pure toneaudiogram patterns at initial measurement were classifiedinto five patterns: (1) ascending pattern of low-tone loss; (2)descending pattern of high-tone loss; (3) midhumping pat-tern of high- and low-tone loss; (4) mid-dipping pattern ofmidtone loss; and (5) flat pattern of high-, mid-, and low-toneloss, as modified from the classifications of previous re-ports.9,16
Acupuncture treatment
The acupuncture practitioner completed a 6-year full-timedidactic and practicum course of traditional medicine whereacupuncture is one of the major modalities, with clinical andresearch experience in the field of acupuncture and neuro-logic conditions for more than 10 years. Acupuncture treat-
ments were usually scheduled about 2 times a week andallowed to be increased to 3 times a week or decreased toonce a week in frequency when clinically suggested as nec-essary. Style of acupuncture was minimally individualizedformulae that included Saam acupuncture17 points plussyndrome pattern-based points selected locally, adjacently,or remotely. Bilateral points were stimulated using 36� 2needles in a session. Needles (0.25-mm diameter and 40-mmlength, Dong Bang, Gyeonggi-do, Korea) were manuallyinserted subcutaneously or intramuscularly. De qi responsewas searched for when stimulating points located in extrem-ities. Needle retention time was 10 minutes. Patients werealso instructed on usual management strategies includinglifestyle advice to abstain from overexertion. Since thisretrospective study did not include control patients, priorreports on the refractory condition of SSHL served as ahistorical control.
Stimulated acupuncture points included (1) GV14 (Dae-chu), GV15 (Amun), GV16 (Pungbu), GB20 (Pungji), GB21(Gyeonjeong), BL10 (Cheonju), SI4 (Wangol), SI15 (Gyeonjung-su), and additional local points, if necessary, in prone posi-tion, followed by (2) TE21 (Imun), TE22 (Hwaryo), SI19(Cheonggung), GB2 (Cheonghoe), ST7 (Hagwan), BL2 (Chanjuk),LI20 (Yeonghyang), GV20 (Baekhoe), EX-HN3 (Indang), andliver tonification formula of Saam acupuncture theory17 onleft side (KI10, Eumgok; LR8, Gokcheon; LU8, Gyeonggeo; andLR4, Jungbong) with contralateral LI4 (Hapgok), LR3 (Tae-chung), and ST36 (Joksamni) in supine position. Local or ad-jacent points in the head and neck region may provide anonspecific relieving effect and the variation of Liver tonifi-cation formula may provide a tonifying effect on the Livermeridian, thus sedating the Gallbladder meridian and hear-ing loss condition.17
Data collection and statistical analysis
Collected data included demographics, related symp-toms such as tinnitus and vertigo, and pattern and pro-gression of pure tone audiograms. Audiogram patternand improvement rate was compared between improvedand nonimproved groups. Statistical comparisons wereperformed with Mann–Whitney U test using SPSS statisti-cal software (version 17 for Windows). Values werepresented as mean� standard deviation with significancelevel of 0.05.
Results
Patients
A total of 17 patients were included in this study.Refractory period until acupuncture treatment was an aver-age of 213.9 days (range 22–1460). Related symptoms weretinnitus, vertigo, and subjective feeling of obstruction in theear (Table 1).
Improvement rate
On the day of first follow-up measurement, 4 patientsshowed improvement and 12 patients did not (improvementrate 25%). One (1) patient failed to continue until first follow-up measurement day. On the day of second follow-upmeasurement, another 4 patients showed improvement and8 patients did not (improvement rate 33%). First follow-up
974 YIN ET AL.

measurement was performed after 29.9� 17.2 days of treat-ment (acupuncture treatment number 9.5� 1.3). Secondfollow-up measurement was performed after 70.4� 26.1days of treatment (acupuncture treatment number
18.7� 2.4). A total improvement rate was 47% (8 of 17) after70.4 days of treatment.
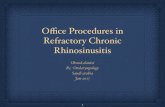
In Table 2, hearing improvement at two follow-up mea-surements was compared between improved and non-improved groups. In improved groups, hearing thresholdlevel was significantly increased at 0.25 and 8 kHz ( p< 0.05)of first follow-up measurement, and at 0.125, 0.25, 0.5( p< 0.05), and 1 kHz ( p< 0.01) of second follow-up mea-surement. Hearing threshold levels of lower frequenciesshowed improvement but higher frequencies did not (Fig. 1).
Audiogram pattern
As to the audiogram pattern of the 17 patients, mid-humping, ascending, and descending pattern was frequentand flat pattern was observed in only 1 patient. Mid-dippingpattern was not observed. On the day of first follow-upmeasurement, 4 patients with ascending or midhumpingpattern showed improvement, but patients with descendingor flat pattern did not. On the day of second follow-upmeasurement, 4 patients with ascending, midhumping, orflat pattern showed improvement, but patients with des-cending pattern did not. There was no improved case withdescending audiogram pattern (Table 3).
Discussion
In this study, medical records of 17 patients with refrac-tory idiopathic SSHL were reviewed and analyzed in relationto improvement rate and pure tone audiogram pattern.Acupuncture formula in this study was modified from Ko-rean acupuncture, which is practical, simple, and approacheseach patient in a holistic perspective.17
SSHL is a controversial subject with unclear causes.18
Possible causes that have been discussed are viral infections,microcirculatory injuries,3 ruptures of the inner ear membrane,autoimmune diseases,18 and abnormal cellular stress responseswithin the cochlea.19 SSHL, a medical emergency with a lowincidence rate, still remains a disorder without a rationaltreatment approach. Although new treatment methods such asintratympanic dexamethasone,20 ozone,21 and magnesium22
have been tried, oral corticosteroid therapy is frequently
Table 1. Demographic Data of the Patients
n (Improved group/nonimproved)a
Initial Follow-up 1 Follow-up 2
Gender, n (%)Female 6 (35) 2/4 1/3Male 11 (65) 2/8 3/5
Age (years), n (%)20–29 1 (6) 0/1 1/030–39 5 (29) 3/1 0/240–49 6 (35) 1/5 2/250–59 2 (12) 0/2 0/260–69 2 (12) 0/2 0/270–79 1 (6) 0/1 1/0
Site, n (%)Right 12 (71) 3/9 3/5Left 5 (29) 1/3 1/3
Relatedsymptoms, n (%)
Tinnitus, present 16 (94) 4/11 4/7Tinnitus, not present 1 (6) 0/1 0/1Vertigo, present 10 (59) 2/7 1/6Vertigo, not present 7 (41) 2/5 3/2Subjective feeling
of obstructionin the ear, present
11 (65) 3/8 3/4
Subjective feelingof obstruction inthe ear, not present
6 (35) 1/4 1/4
aPure tone audiometric testing was performed after 9.5� 1.3 timesof acupuncture treatment for 29.9� 17.2 days (follow-up measure-ment 1) and after 18.7� 2.4 times of acupuncture treatment for70.4� 26.1 days (follow-up measurement 2). Hearing improvementmeans increased threshold from initial measurements by more than20 dB in at least two contiguous frequencies.
n, number.
Table 2. Hearing Improvement from Initial Thresholds in Nonimproved and Improved Group
Hearing threshold level changeon follow-up measurement 1 (dB)
Hearing threshold level changeon follow-up measurement 2 (dB)
Hearing thresholdfrequency (kHz)
Nonimprovedgroup (n¼ 12)
Improvedgroup (n¼ 4)
Nonimprovedgroup (n¼ 8)
Improvedgroup (n¼ 4)
0.125 5.0� 7.4 21.3� 20.2 �1.3� 8.3 20.0� 7.1**0.25 5.0� 8.5 23.8� 14.9* 0.0� 8.9 23.8� 7.5**0.5 5.8� 9.0 12.5� 6.5 �5.0� 16.0 27.5� 11.9**1 2.9� 10.3 8.8� 11.1 �3.1� 16.2 17.5� 12.6*2 3.8� 11.5 17.5� 17.6 �0.6� 17.2 10.0� 7.14 1.3� 12.8 15.0� 24.8 �3.1� 17.9 11.3� 21.48 �1.7� 17.5 17.5� 10.4* 1.3� 13.6 �1.3� 27.8
Refractory sudden sensorineural hearing loss patients received acupuncture treatment after an average 213.9 days of refractory period.Pure tone audiometric testing was performed after 9.5� 1.3 times of acupuncture treatment for 29.9� 17.2 days (follow-up measurement 1)and after 18.7� 2.4 times of acupuncture treatment for 70.4� 26.1 days (follow-up measurement 2). Hearing improvement means increasedthreshold from initial measurements by more than 20 dB in at least two contiguous frequencies. Values are presented as mean� standarddeviation. *p< 0.05, **p< 0.01 compared to the nonimproved group by Mann–Whitney U test.
n, number.
ACUPUNCTURE FOR HEARING LOSS 975

discussed as a ‘‘gold standard’’ treatment3,5,6 despite the lack ofevidence of its efficacy.5,7
A total improvement rate until day 70.4� 17.2 post initialvisit was 47% (8 of 17 cases) in the cases reviewed in thisstudy. There are only a few study reports on long-term fol-low-up or delayed improvement of patients with idiopathicSSHL.9,23 In the previous reports, a patient group (n¼ 3) thatstarted treatment during the period from day 21 to day 60after onset was reported to show improvement in 33%,9 anda patient group (n¼ 156) that was followed up for more than3 months after 10 days of inpatient treatment was reported toshow improvement in 25%.23
The improvement rate of the cases managed with acu-puncture in this study is somewhat higher than those pre-viously reported, considering the long refractory period of213.9 days (range 22–1440).
Of the five audiogram patterns, midhumping and as-cending patterns were the most frequent ones. Mid-dipping
FIG. 1. Hearing threshold levels of initial and follow-up measurements. Hearing threshold patterns of the nonimprovedgroup (A, n¼ 12) and the improved group (B, n¼ 4) on the day of the first follow-up measurement. Hearing thresholdpatterns of the nonimproved group (C, n¼ 8) and the improved group (D, n¼ 4) on the day of the second follow-upmeasurement. Follow-up measurement was performed after 9.5� 1.3 times of acupuncture treatment for 29.9� 17.2 days andafter 18.7� 2.4 times of acupuncture treatment for 70.4� 26.1 days. Hearing improvement means increased threshold frominitial measurements by more than 20 dB in at least two contiguous frequencies. Values are presented as mean� standarderror of the mean. *p< 0.05, **p< 0.01 compared to the nonimproved group by Mann–Whitney U test.
Table 3. Audiogram Pattern and Hearing
Improvement
N (improved/nonimproved)
Audiogrampatterna n (%)
Follow-upmeasurement 1
Follow-upmeasurement 2
Ascending 5 (29) 2/3 2/1Descending 5 (29) 0/4 0/4Midhumping 6 (35) 2/4 1/3Mid-dipping 0 (0) 0/0 0/0Flat 1 (6) 0/1 1/0
aPure tone audiogram patterns of initial measurement wereclassified into five patterns: (1) ascending pattern of low-tone loss,(2) descending pattern of high-tone loss, (3) midhumping pattern ofhigh- and low-tone loss, (4) mid-dipping pattern of midtone loss,and (5) flat pattern of high-, mid, and low-tone loss.
n, number.
976 YIN ET AL.

pattern was not observed. Ascending pattern was previouslyreported to be one of the most frequent ones.9,16 Flat pattern,the most frequent pattern in a previous report,16 was notfrequent in this study. This may be due to a difference inspecifics when classification criteria were applied to an in-dividual audiogram. In relation to hearing improvement,patients with midhumping and ascending pattern showed afair improvement rate, but patients with descending patternshowed no improvement. Although no correlation was re-ported between audiogram patterns and hearing improve-ment,16 our results compare favorably with those in previousreports: ascending pattern is known to be related with agood prognosis.4,6,8,9
Related symptoms observed include tinnitus, vertigo, andsubjective feeling of obstruction in the ear. Several studiesreported that vertigo is related to a poor prognosis,4,8,23,24
although no correlation was reported between relatedsymptoms and hearing improvement.16,25 We tried to ana-lyze related symptoms in relation to hearing improvementusing w2 analysis, but none showed significant relation withhearing improvement, possibly due to the small sample size(data not shown). Younger patients (20–49 years) tended toshow a good prognosis when compared with older patients(50–79), and vertigo symptoms tended to be related withpoor prognosis. Notably, a 72-year- old woman with hearingloss over 150 days experienced improvement after 20 acu-puncture treatments (Table 1). The extended treatment pe-riod possibly provided a positive clinical outcome, whichshould be further explored and researched. The small samplesize and retrospective analysis design without a controlgroup may prevent any definite conclusion from this study.The small number of patients with widely varied symptomsmeans that this can only indicate a trend. Notwithstandingthe limitations, this study should encourage further work inthis field.
Conclusions
In conclusion, we found a possibility that acupuncture maybe developed as an effective complementary modality whenintegrated into a management program for refractory SSHL.
Acknowledgments
This work was supported by the Korea Science and En-gineering Foundation (KOSEF) grant funded by the Koreagovernment (MEST) (R11-2005-014).
Disclosure Statement
No competing financial interests exist.
References
1. Fetterman BL, Saunders JE, Luxford WM. Prognosis andtreatment of sudden sensorineural hearing loss. Am J Otol1996;17:529–536.
2. Shemirani NL, Schmidt M, Friedland DR. Sudden sensori-neural hearing loss: An evaluation of treatment and man-agement approaches by referring physicians. OtolaryngolHead Neck Surg 2009;140:86–91.
3. Yueh B, Shapiro N, MacLean CH, et al. Screening andmanagement of adult hearing loss in primary care: Scientificreview. JAMA 2003;289:1976–1985.
4. Byl FM Jr. Sudden hearing loss: Eight years’ experienceand suggested prognostic table. Laryngoscope 1984;94:647–661.
5. Conlin AE, Parnes LS. Treatment of sudden sensorineuralhearing loss: I. A systematic review. Arch Otolaryngol HeadNeck Surg 2007;133:582–586.
6. Alexiou C, Arnold W, Fauser C, et al. Sudden sensorineuralhearing loss: Does application of glucocorticoids makesense? Arch Otolaryngol Head Neck Surg 2001;127:253–258.
7. Ghosh A, Jackson R. Best evidence topic report: Steroids insudden sensorineural hearing loss. Emerg Med J 2005;22:732–733.
8. Mattucci KF, Bachoura L. Sudden hearing loss: Ten years’experience. Bull N Y Acad Med 1982;58:464–470.
9. Tiong TS. Prognostic indicators of management of suddensensorineural hearing loss in an Asian hospital. SingaporeMed J 2007;48:45–49.
10. Lee H, Park HJ, Park J, et al. Acupuncture application forneurological disorders. Neurol Res 2007;29(suppl 1):S49–S54.
11. Li SL, Zhang H, Li H, et al. Effects of acupuncture andcontinuous multiple points pulse stimulation on linguisticfrequency hearing loss in the patient of sensorineural hear-ing loss. Zhongguo Zhen Jiu 2005;25:407–410.
12. Yoon HS, Lee SE, Han EJ, et al. Six cases of sudden senso-rineural hearing loss. J Orien Med Ophthal OtolaryngolDermatol 2003;16:221–243.
13. Vincent CA, Richardson PH. Acupuncture for some com-mon disorders: A review of evaluative research. J R Coll GenPract 1987;37:77–81.
14. Borton TE. Acupuncture and sensorineural hearing loss: Areview. South Med J 1976;69:600–601.
15. Liu B, Du YH. Evaluation of the literatures of clinical studieson acupuncture and moxibustion for treatment of sensori-neural hearing loss. Zhongguo Zhen Jiu 2005;25:893–896.
16. Penido Nde O, Ramos HV, Barros FA, et al. Clinical, etio-logical and progression factors of hearing in sudden deaf-ness. Braz J Otorhinolaryngol 2005;71:633–638.
17. Yin CS, Park HJ, Chae Y, et al. Korean acupuncture: Theindividualized and practical acupuncture. Neurol Res 2007;29(suppl 1):S10–S15.
18. Lazarini PR, Camargo AC. Idiopathic sudden sensorineuralhearing loss: Etiopathogenic aspects. Braz J Otorhinolar-yngol 2006;72:554–561.
19. Merchant SN, Durand ML, Adams JC. Sudden deafness: Is itviral? ORL J Otorhinolaryngol Relat Spec 2008;70:52–60.
20. Plontke SK, Lowenheim H, Mertens J, et al. Randomized,double blind, placebo controlled trial on the safety andefficacy of continuous intratympanic dexamethasone de-livered via a round window catheter for severe to pro-found sudden idiopathic sensorineural hearing loss afterfailure of systemic therapy. Laryngoscope 2009;119:359–369.
21. Ragab A, Shreef E, Behiry E, et al. Randomised, double-blinded, placebo-controlled, clinical trial of ozone therapy astreatment of sudden sensorineural hearing loss. J LaryngolOtol 2009;123:54–60.
22. Conlin AE, Parnes LS. Treatment of sudden sensorineuralhearing loss: II. A meta-analysis. Arch Otolaryngol HeadNeck Surg 2007;133:582–586.
23. Gordin A, Goldenberg D, Golz A, et al. Magnesium: A newtherapy for idiopathic sudden sensorineural hearing loss.Otol Neurotol 2002;23:447–451.
ACUPUNCTURE FOR HEARING LOSS 977

24. Lee DH, Jun BC, Laa JH, et al. Clinical analysis of delayedimprovement in sudden sensorineural hearing loss. Korean JOtolaryngol 2006;49:695–698.
25. Pino Rivero V, Trinidad Ruız G, Marcos Garcıa M, et al.Statistical study and clinical results by comparison of twodifferent protocols in the treatment of sudden hearing loss.Acta Otorrinolaringol Esp 2005;56:63–67.
26. Weng SF, Chen YS, Liu TC, et al. Prognostic factors ofsudden sensorineural hearing loss in diabetic patients. Dia-betes Care 2004;27:2560–2561.
Address correspondence to:Hae Jeong Nam, KMD, PhD
Department of Ophthalmology and OtorhinolaryngologyCollege of Korean Medicine
Kyung Hee University1 Hoegi-dong, Dongdaemun-gu
Seoul 130-701Republic of Korea
E-mail: [email protected]
978 YIN ET AL.

Copyright of Journal of Alternative & Complementary Medicine is the property of Mary Ann Liebert, Inc. and
its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.