actualizaciones en toxicologia.pdf

of 7
-
Upload
freddy-cuervo-camargo -
Category
Documents
-
view
213 -
download
0
Transcript of actualizaciones en toxicologia.pdf
-
8/22/2019 actualizaciones en toxicologia.pdf
1/7
Update in Nonpulmonary Critical Care
Am J Respir Crit Care Med Vol 166. pp 915, 2002DOI: 10.1164/rccm.2108138Internet address: www.atsjournals.org
(Received in original form August 31, 2001; accepted in final form March 27, 2002 )
Correspondence and requests for reprints should be addressed to Nicholas S. Hill,M.D., Pulmonary, Critical Care, and Sleep Division, TuftsNew England MedicalCenter, 750 Washington Street, #257, Boston, MA 02111. E-mail: [email protected]
Update in Clinical Toxicology
Jason Chu, Richard Y. Wang, and Nicholas S. Hill
Division of Pulmonary, Critical Care, and Sleep Medicine, TuftsNew England Medical Center, Boston, Massachusetts; New York City Poison
Control Center, Department of Health, New York; Division of Emergency Medicine, New York University School of Medicine, New York, New York;and Grady Health System, Department of Emergency Medicine, Atlanta, Georgia
Each year, new agents are added to the pharmacopoeia, ex-panding the list of possible toxicologic reactions. In response,new antidotes are introduced, uses of more established anti-dotes evolve, and new therapeutic approaches to well-estab-lished toxicologic syndromes are developed. This brief updateon critical care toxicology focuses on a few of the most impor-tant new developments. The recognition and management ofthe serotonin syndrome are discussed as an example of a toxi-cologic syndrome that is occurring more frequently as a conse-quence of the introduction of new pharmacotherapies. New de-velopments in the therapy of well-known toxicologic reactions
are next considered in relation to acetaminophen overinges-tion. Examples of evolving uses of older antidotes include oct-reotide to treat sulfonylurea overdose and glucose and insulinto treat calcium channel blocker overdose. Finally, we examinenew antidotes including fomepizole to inhibit alcohol dehydro-genase, and snake antivenom antibodies to treat envenoma-tions. Critical care specialists must keep abreast of these trendsto most effectively care for patients with toxicologic exposures.
GENERAL APPROACH TO TOXICOLOGIC SYNDROMES
The approach to therapy of acute toxicologic syndromes hasgradually evolved. The need to obtain a complete history andto seek clues on physical examination remains essential (Table1). The prehospital care record is important because this rep-resents the patients status before institution of therapy. Onarrival at the hospital, pharmacologic intervention can con-found the clinical findings and make it difficult to recognize aspecific toxicologic syndrome. The use of emetics is now dis-couraged, but gastric lavage is still performed routinely inmany centers for the prompt removal of pills and fragments.However, even this practice is becoming more selective be-cause of controlled trials indicating that outcomes are not im-proved by performing gastric evacuation in all patients (1, 2).Gavage should still be performed in patients arriving withinan hour of a potentially significant ingestion or after ingestionof toxins that do not adsorb to charcoal, such as heavy metalsor lithium (3, 4). Prompt administration of activated charcoalinto the gastrointestinal tract remains a mainstay of therapy
for most other overingestions, with the exception of small or-ganic compounds that are readily absorbed by the gut (e.g.,methanol, ethylene glycol) but adsorb poorly to charcoal (3).A prompt consultation with either the regional poison centeror a medical toxicologist as soon as a toxic reaction or over-
dose is suspected helps to assure that clinicians are providingoptimal therapy in a timely fashion.
SEROTONIN SYNDROME
The medical therapy of psychiatric disorders such as depres-sion and bipolar affective disorders includes agents that in-crease central nervous system (CNS) serotonin transmissionand activity. The serotonin syndrome is a complication of theuse or misuse of such medications and is characterized by confu-sion, autonomic instability, and neuromuscular abnormalities
(Table 2). This constellation of symptoms was first seen in the1950s in patients receiving iproniazid and pethidine (meperi-
dine) and in the 1960s in patients receiving L
-tryptophan (58).The pathophysiology of the serotonin syndrome is not entirelyclear, but animal studies have confirmed the role of serotoninand the identity of the responsible receptors. In rats, serotoninsyndrome is blocked by the nonspecific 5-hydroxytryptamineantagonists methysergide and metergoline, but not by specific
5-hydroxytryptamine
2
receptor antagonists such as ketanserinand pipamperone (9). This implicates 5-hydroxytryptamine
1A
receptor activation in the brainstem and spinal cord as playingan important role in the genesis of the syndrome.
The serotonin syndrome is most often seen in patients who
are taking two or more medications at therapeutic doses that in-
crease CNS serotonergic activity by different mechanisms (Ta-ble 3). The most commonly reported combinations are monoam-ine oxidase inhibitors with meperidine, tryptophan, selectiveserotonin reuptake inhibitors, or tricyclic antidepressants (5,8). Single agents can also precipitate the syndrome, sometimesat therapeutic doses, but mainly in association with overinges-tion. A prospective study observed the development of signsand symptoms of serotonin syndrome in 16 of 38 patients tak-ing clomipramine, a tricyclic antidepressant that increases CNSserotonergic activity (10). 3,4-Methylenedioxymethamphet-amine (Ecstasy) has also been reported to cause the syndromeas a single agent (11). An inadequate washout period betweenthe cessation of one serotonergic agent and the start of an-other can also precipitate the syndrome.
The most important step in managing the serotonin syn-
drome is to recognize the symptoms in a patient taking sero-tonergic medications. After reviewing 12 reports in the litera-ture that included 38 cases of serotonin syndrome, Sternbachdeveloped a set of criteria for diagnosing the serotonin syn-
drome (8) (
see
Table 2). Symptoms typically start minutes tohours after drug ingestion and usually resolve within 12 to 24hours. Mild cases present with limited symptoms, whereasmore severe cases have an altered sensorium and muscular hy-peractivity as evidenced by myoclonus, shivering, rigidity, andhyperthermia. Untreated patients are at risk of developingrhabdomyolysis, renal failure, hepatic dysfunction, dissemi-nated intravascular coagulation, and in massive overingestion,cardiovascular collapse and death. Treatment is directed at
-
8/22/2019 actualizaciones en toxicologia.pdf
2/7
10
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 166 2002
avoiding all serotonergic medications, such as meperidine ordextromethorphan, and decreasing the muscular hyperactivitywith benzodiazepines and associated hyperthermia with rapidexternal cooling. Cyproheptadine or neuromuscular blockademay be necessary if benzodiazepines fail (12). With good sup-portive care applied promptly, most patients recover quickly(5, 8).
N
-ACETYLCYSTEINE FOR FULMINANT HEPATIC FAILUREFROM ACETAMINOPHEN TOXICITY
Acetaminophen is one of the most commonly used pharma-ceutical agents, and it is found in multiple over-the-counterand prescription medications. Not surprisingly, it is also the mostcommon cause of drug overdose reported to the American Asso-ciation of Poison Control Centers. Management of acetamin-ophen overdose consists of appropriate gastric decontamina-tion, supportive care, and administration ofN
-acetylcysteinetherapy, based on an adaptation of the RumackMatthew no-mogram (13). At therapeutic doses, acetaminophen is metab-olized primarily by glucuronidation and sulfation in the liver,with a minor proportion of drug undergoing P-450 metabolismto the toxic metabolite N
-acetylbenzoquinoneimine, which isdetoxified by hepatic glutathione. When excessive quantitiesof acetaminophen are ingested (i.e., acute ingestions of greaterthan 7.5 g in an adult or 150 mg/kg in a child) (14), endoge-nous glutathione stores are depleted, allowing N
-acetylbenzo-quinoneimine to accumulate and react with cellular proteins,causing hepatic and renal dysfunction.
N
-acetylcysteine serves as an antidote by repleting glu-tathione reserves and acting as a glutathione substitute intra-cellularly. If given within 8 hours of acetaminophen ingestion,
N
-acetylcysteine prevents hepatotoxicity (15). Patients who be-gin N
-acetylcysteine therapy later than 8 hours postingestionor have ingested large doses of acetaminophen chronically areat risk of hepatotoxicity despite therapy. A small subset of hepa-totoxic patients will develop fulminant hepatic failure. Previ-ously, patients developing fulminant hepatic failure had highmorbidity and mortality rates. However, advances in ortho-
topic liver transplantation and the increasingly liberal use ofprolonged intravenous as opposed to limited courses of oral
N
-acetylcysteine have decreased the mortality of these patientsand have led to the development of a set of prognostic criteriato identify those at risk of mortality (16). Patients with the sin-gle criterion of a systemic pH less than 7.30 after fluid and he-modynamic resuscitation have a 95% mortality.
In addition, a combination of a prothrombin time greaterthan 100 seconds, serum creatinine greater than 3.3 mg/dl, andgrade III or IV hepatic encephalopathy predicts a mortality of77% (16).
Although it was long thought that initiation ofN
-acetylcys-teine beyond the first 16 hours after ingestion was probablyfutile, evidence supporting the idea that late administrationmight be effective was provided in 1990, when a retrospectiveanalysis showed a significant reduction in mortality of patientswith fulminant acetaminophen-induced hepatic failure treatedwith late intravenous N
-acetylcysteine (37% in the treatmentgroup compared with 58% in the untreated group) (17). Amongsurvivors, the mean time from ingestion to the beginning oftherapy was 15.5 hours, with a delay of up to 36 hours in one
patient (17). Subsequently, a prospective trial randomized 50patients with fulminant acetaminophen-induced hepatic fail-ure to receive late intravenous N
-acetylcysteine versus vehiclecontrol (18). Experimental therapy was continued until eachpatient either recovered, died, or underwent liver transplanta-tion. The treatment group had a median time from overdose to
N
-acetylcysteine therapy of 53 hours (range, 36 to 80 hours).Compared with the untreated group, those treated with N
-acet-ylcysteine had reduced mortality (52 versus 80%), a lower in-cidence of cerebral edema (40 versus 68%), and required less in-
otropic medication for blood pressure support (all p
0.05).The beneficial effect ofN
-acetylcysteine in these patients maybe from improved oxygen transport and consumption at thetissue level, as suggested by the increase in the oxygen-extrac-tion ratio among treated patients observed in another trial (19).
Patients who develop fulminant hepatic failure after acet-aminophen ingestion, regardless of how much time has passedsince the ingestion, should be treated with N
-acetylcysteine,preferably via the intravenous route. However, practical con-straints or product unavailability may necessitate initiation oftherapy by the oral or enteral route. We recommend a loadingdose of 140 mg/kg, followed by a maintenance dose of 70 mg/kg every 4 hours. This is continued until the biochemical indi-cators of hepatotoxicity have improved substantially. If theenteral route is not functioning and intravenous medication isunavailable, it is possible to create an intravenous solutionfrom the oral preparation (20). However, it is important tohave an experienced pharmacist prepare the solution because
TABLE 1. CLINICAL FINDINGS OF TOXICOLOGIC SYNDROMESCOMMONLY ENCOUNTERED IN THE CRITICAL CARE SETTING
Toxicologic Syndrome Clinical Findings
Anticholinergic CNS effects:
Hallucinations, confusion, sedation, seizures
Peripheral effects:
Decreased GI motility, dry mucosa and
skin, hyperthermia, mydriasis,
tachycardia, urinary retention
Cholinergic CNS effects:
Confusion, lethargy, seizuresPeripheral effects:
SLUDGE, BBB
Opioid Bradycardia, CNS depression, decreased
GI motility, hypotension, miosis,
respiratory depression
Sedativehypnotic Bradycardia, CNS depression, hypotension,
respiratory depression
Benzodiazepine CNS depression, normal vital signs,
no respiratory depression in oral overdose
without concomitant CNS depressants
Sympathomimetic Agitation, d iaphoresis, h ypertension,
hyperthermia, tachycardia,
severe cases: cardiac dysrhythmias,
seizures
Definition of abbreviations
: BBB
bradycardia, bronchorrhea, bronchospasm; CNS
central nervous system; GI
gastrointestinal; SLUDGE
salivation, lacrimation, urina-tion, diarrhea, GI motility, emesis.
TABLE 2. SUGGESTED DIAGNOSTIC CRITERIA FORSEROTONIN SYNDROME*
Coincident with the addition of or increase in a known serotonergic agent to an
established medical regimen, at least three of the followoing clinical features
should be present:
Mental status changes (confusion, hypomania) Shivering
Agitation Tremor
Myoclonus Diarrhea
Hyperreflexia Incoordination
Diaphoresis Fever
Other etiologies (e.g., infectious, metabolic, substance abuse, or withdrawal)
must be excluded
A neuroleptic must not have been started or increased in dosage before the onset
of the signs and symptoms listed above
* Adapted from Sternbach (8).
-
8/22/2019 actualizaciones en toxicologia.pdf
3/7
Update in Nonpulmonary Critical Care 11
adverse reactions occur frequently, including cutaneous reac-tions in 10% and bronchospasm in 5%, with a 2.8-fold in-
creased risk in patients with asthma (21). Preparation of a di-lute solution with a 0.2-
m pore size filter, slowed infusion ofthe bolus (over 3060 minutes), and pretreatment of asthmapatients with antihistamines are recommended.
OCTREOTIDE FOR SULFONYLUREA OVERDOSE
The number of different medications to treat diabetes mellitushas increased dramatically, but sulfonylureas remain a main-stay of therapy and overdoses are common. Sulfonylureas in-hibit potassium ion efflux in vitro
and increase pancreatic
cell sensitivity to glucose in vivo
(22), potentiating the secre-tion of insulin. Thus, sulfonylurea overdose leads to a hyperin-sulinemic state that causes hypoglycemia, the severity and du-
ration of which is related to the potency and half-life of thespecific drug ingested. In past studies, the overall mortality ofpatients experiencing severe hypoglycemia from sulfonylureaswas approximately 10% (23). Treatment of sulfonylurea-inducedhypoglycemia starts with glucose therapy, oral or intravenousor both, and gastrointestinal decontamination. Other commonlyused therapies include glucagon, diazoxide, corticosteroids, andurinary alkalinization to enhance urinary elimination for chlo-propamide overdose. In the past, hypokalemia, hypophos-phatemia, and rebound hypoglycemia have been problematic,particularly after overdoses of sulfonylureas with prolongedhalf-lives.
Octreotide is a synthetic analog of somatostatin that hasgreater potency and a longer duration of action. Besides theirinhibitory action on insulin release, somatostatin and oct-reotide both inhibit CNS release of growth hormone and thy-rotropin and secretion of gastrointestinal tract hormones suchas gastrin, secretin, and motilin (24). In addition to its emerg-ing role as a therapy for sulfonylurea overdose, octreotide iscurrently used in the treatment of growth hormone- and thy-rotropin-secreting pituitary adenomas, metastatic pancreaticislet cell and carcinoid tumors, bleeding esophageal varices,and secretory diarrhea (25).
Studies examining the effects of somatostatin and oct-reotide on sulfonylurea-induced hypoglycemia have includedanimal and volunteer human studies. These have demonstratedthe short-term inhibitory effect of somatostatin on insulin re-lease during glucose infusions or tolbutamide administration
(26, 27). Compared with somatostatin, octreotide has an equalinhibitory effect on insulin release but a longer duration of ac-tion, averaging 6 to 8 hours. In a randomized cross-over studyof eight healthy subjects given glipizide orally on three sepa-rate days, octreotide infusion lowered insulin levels and glu-cose infusion requirements significantly more than treatmentwith glucose alone or diazoxide plus glucose. When therapy wasstopped 13 hours after glipizide ingestion, only two of eightsubjects developed hypoglycemia after therapy with octreotide,whereas all subjects had rebound hypoglycemia within 90 min-utes of stopping therapy with glucose alone or diazoxide plusglucose (28).
Octreotide has now been used successfully in many cases ofhypoglycemia secondary to sulfonylurea overdose (29, 30). Inthese reports, the adult doses ranged from 40 to 100
g, ad-ministered subcutaneously, and frequency of administrationranged from every 6 to every 12 hours. The duration of ther-apy depends on the duration of action of the sulfonylurea agent,but it can last from 48 to 72 hours. Octreotide is well toleratedand, as long as blood sugars are closely monitored and therapyis continued until hypoglycemia resolves, complications arefew and mortality nil. Most of the complications of octreotideoccur in patients with acromegaly or insulinomas receivinghigh-dose long-term therapy, in whom it may worsen glycemic
control (31, 32). These problems are rarely encountered in pa-tients undergoing short-term therapy for sulfonylurea over-dose. Adverse effects that may be seen during acute adminis-tration include injection site pain, nausea, vomiting, diarrhea,and possibly hyperglycemia. Because some patients experi-ence delayed hypoglycemia after cessation of octreotide ther-apy, they should be observed for rebound hypoglycemia for atleast 12 to 24 hours after the last dose (28).
Although octreotide offers mainly convenience advantagesand would not be expected to lower the mortality rate com-pared with a carefully monitored glucose infusion, it is alsoeconomical, costing less than $150.00 for a 3-day course oftherapy, and potentially reducing the need for frequent glu-cose measurements. For these reasons, it should now be con-
sidered first-line therapy for any patient who ingests a sulfonyl-urea agent and develops symptomatic hypoglycemia or a serumglucose concentration less than 60 mg/dl that is refractory todextrose supplementation.
INSULIN AND GLUCOSE IN CALCIUM CHANNELBLOCKER TOXICITY
Calcium channel blockers inhibit calcium influx by blockingL-type voltage-sensitive calcium channels on the outer cellmembrane. This blockade decreases vascular smooth muscletone, leading to arterial dilation, and has a negative inotropiceffect on the myocardium. It also inhibits sinoatrial and atrio-ventricular nodal functions, causing decreased chronotropy(mainly by the phenylalkylamine and benzothiazepine classagents). In the setting of calcium channel blocker overdose,these effects translate into hypotension and myocardial con-duction defects.
The therapy of calcium channel blocker overdose focuseson restoring cardiac function and systemic blood pressure andinvolves multiple additive therapies. Calcium salts (e.g., chlo-ride, gluconate), glucagon, atropine, catecholamines, phospho-diesterase inhibitors, cardiac pacing, and intra-aortic ballooncounterpulsation have all been tried, but no one modality hasdemonstrated superiority over the others. More recently, insu-lin and glucose have been added to the list of therapies.
Insulin and glucose have been used in futile attempts tominimize myocardial damage after infarction. This approach
TABLE 3. PHARMACOLOGIC AGENTS THAT ENHANCE CNSSEROTONIN ACTIVITY: LISTED BY MECHANISMSOF ENHANCEMENT
Serotonin agonists Inhibit serotonin reuptake
Buspirone Amphetamines
Ergot alkaloids Cocaine
Lithium Meperidine
LSD Nefazadone, trazadone
mCPP Selective serotonin reuptake inhibitors
Metaclopramide Tramadol
Triptans Tricyclic antidepresants
Increase serotonin release Inhibit serotonin breakdown
Amphetamines Monoamine oxidase inhibitors
Cocaine Enhance serotonin synthesis
Codeine and derivatives
L
-Tryptophan
Dexfenfluramine
Dextromethorphan
Fenfluramine
MDMA
Definition of abbreviations
: CNS
central nervous system; LSD
lysergic acid dieth-ylamide; mCPP
meta-chlorophenylpiperazine; MDMA
methylenedioxymetham-phetamine.
-
8/22/2019 actualizaciones en toxicologia.pdf
4/7
12
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 166 2002
was based on the observations that although myocytes nor-mally utilize free fatty acids as substrates for energy metabo-lism, stressed myocardium shifts to glucose as the preferredsubstrate (33). More recently, however, experimental studieshave shown improved myocardial inotropy and survival in ex-perimental animals with verapamil poisoning treated with in-sulin infusions as compared with controls (34, 35). In one study,all dogs treated with insulin for their verapamil-induced myo-cardial toxicity survived, whereas mortality was 100 and 67%among those treated with glucagon and epinephrine, respec-tively (p
0.05) (34). These favorable effects may be attribut-able to counteraction by exogenous insulin of the diabeto-genic effect of acute verapamil poisoning, including blockadeof pancreatic insulin release and increased systemic insulin re-sistance (36). In these experimental models, insulin also im-proved lactate oxidation and reversed the diminished fatty aciduptake of verapamil-toxic myocardium (37).
Although clinical data on the use of insulin and glucose forcalcium channel blocker toxicity are scanty, a study of calciumchannel blocker toxicity in patients who failed traditionaltreatments suggests that the beneficial actions that were ob-served in animals also occur in humans (38). In this case series,the mean insulin infusion rate was 0.5 IU/kg per hour (range,0.110 IU/kg per hour), with systemic blood pressure improv-
ing within 60 to 90 minutes. The duration of the insulin infu-sion depended on the patients clinical condition and responseto therapy, but ranged from 9 to 49 hours with a mean of 27hours. The major adverse effects were hypoglycemia and hy-pokalemia (as low as 2.2 mEq/L). Although glucose was in-fused throughout the insulin infusion, serum glucose concen-tration fell to less than 60 mg/dl in four of five patients, withthe lowest being 29 mg/dl, underscoring the need for close glu-cose monitoring. The glucose infusion was adjusted accord-ingly, with peak glucose infusion rates ranging from 10 to 75g/hour (38).
Based on the current evidence, patients experiencing brady-cardia or hypotension after ingesting calcium channel blockersshould be initially resuscitated with traditional therapies such
as intravenous crystalloid fluids, calcium salts, and glucagon.Those who have persistent hypotension, bradyarrhythmias, orconduction disturbances should be infused with insulin andglucose. Severely bradycardic and hypotensive patients mayrequire vasopressor agents, cardiac pacing, or temporary intra-aortic balloon counterpulsation until they can metabolize thecalcium channel blocker.
4-METHYLPYRAZOLE (FOMEPIZOLE) FOR METHANOLOR ETHYLENE GLYCOL INGESTIONS
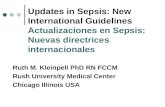
The traditional management of toxic alcohol ingestions usesethanol infusions and hemodialysis if serum levels exceed cer-tain thresholds. The two most commonly ingested toxic alco-hols, methanol and ethylene glycol (found mostly in wind-shield washer fluid and automobile antifreeze, respectively),are not themselves highly toxic; however, they produce toxicmetabolites when metabolized by alcohol dehydrogenase (
see
Figure 1). Therefore, initial therapy is directed at decreasingthe production of the toxic metabolites. Ethanol is an effectiveinhibitor of toxic metabolite production from the toxic alco-hols because it has a higher affinity as a substrate for alcoholdehydrogenase. However, to achieve effective inhibition oftoxic alcohol metabolism by alcohol dehydrogenase, ethanollevels must be high (at least 100 mg/dl or 25% of the serumtoxic alcohol concentration, whichever is higher).
Adverse effects of ethanol infusions include phlebitis andfluid overload, whereas the oral route causes gastrointestinal
distress. Central nervous system intoxication and fatty infiltra-tion of the liver occur with both routes. Although ethanol isinexpensive, administration is complicated by the need for fre-quent monitoring of serum ethanol levels and repeated dosageadjustments because ethanol enhances its own metabolism(39). Because of these problems associated with chronic etha-nol administration, alternative inhibitors of alcohol dehydrog-enase have been sought. Early studies showed that pyrazole isan effective inhibitor of alcohol dehydrogenase in animals poi-soned with ethylene glycol (40), but it caused bone marrow,liver, and renal toxicity. 4-Methylpyrazole (or fomepizole) wasdeveloped as a less toxic alternative. In multiple animal mod-els, it has proven to be an effective inhibitor of alcohol dehy-drogenase, without the toxicities associated with pyrazole (41).Also, multiple clinical reports have documented its utility inboth methanol and ethylene glycol poisoning.
Two prospective, observational multicenter trials have evalu-ated the effectiveness of fomepizole in toxic alcohol poisoning.In the first (42), 19 patients with ethylene glycol poisoning hadsubstantial improvements of their metabolic acidoses withinhours of initiation of fomepizole therapy. In addition, the meanserum glycolate level fell from 89.7 mg/dl (range, 0264.4 mg/dl)to 0 mg/dl over 24 hours. Seventeen patients underwent con-comitant hemodialysis, and nine, who presented later after in-
gestion and had higher plasma glycolate concentrations (
97mg/dl), had impaired kidney function. Eighteen of the 19patients survived, one succumbing to complications of an acute
Figure 1. Schematic of pathways for methanol and ethylene glycolmetabolism. Ethanol saturates and fomepizole inhibits alcohol dehy-drogenase (ADH), and both thereby block the formation of toxic inter-mediates such as formic and glycolic acids. If unmetabolized, metha-nol and ethylene are slowly excreted intact in the urine, but hemodialysisis often used to speed clearance. Several metabolic intermediates havebeen omitted for clarity of presentation.
-
8/22/2019 actualizaciones en toxicologia.pdf
5/7
Update in Nonpulmonary Critical Care 13
myocardial infarction that occurred before the initiation oftherapy. Fomepizole therapy was administered intravenously,using a loading dose of 15 mg/kg, followed by maintenance bo-lus doses of 10 mg/kg every 12 hours for 48 hours. The bolusdoses were then increased to 15 mg/kg every 12 hours becauseof autoinduction of fomepizole hepatic metabolism. Therapywas continued until the serum ethylene glycol concentrationwas less than 20 mg/dl, requiring a mean of 3.5 doses of fome-pizole per patient (range, 17 doses) (42).
The second study was another prospective observationaltrial of 11 patients poisoned with methanol (43). Fomepizoletreatment was associated with a decrease in serum formic acidconcentration, normalization of blood pH from the initial acid-emia, and return of visual acuity abnormalities to baseline sta-tus by the time of hospital discharge. Seven patients underwenthemodialysis and nine patients survived, with two succumbingto anoxic brain injury that was present at the time of enroll-ment. The fomepizole dosing regimen was the same as for eth-ylene glycol described here previously, with patients in themethanol study receiving a median of four doses per patient(range, 110 doses). Fomepizole was well tolerated in bothstudies. Adverse side effects included headache, rash, tachy-cardia, anxiety, and seizures, but these were deemed more likelyto be related to the alcohol ingestion than to the fomepizole.
These studies support the clinical safety and efficacy offomepizole as an alcohol dehydrogenase inhibitor. It effec-tively inhibits the formation of toxic metabolites, rapidly im-proves metabolic imbalances, and prevents end-organ damage(e.g., renal failure or blindness). As shown in Table 4, fomepi-zole markedly prolongs the elimination half-lives of ethyleneglycol and methanol, even more on average than ethanol (4446), thus effectively preventing the generation of toxic metab-olites. Concomitant hemodialysis is still usually required in pa-tients with high alcohol levels or high anion gap acidoses, how-ever, to accelerate the removal of the alcohols and toxicmetabolites (44, 46). Although the studies have been uncon-trolled and provide no direct comparison to traditional ther-apy with ethanol, they demonstrate that fomepizole has several
advantages over ethanol therapy, including easier administra-tion and monitoring and the avoidance of mental statuschanges, hypoglycemia, and hepatotoxicity. For these reasons,fomepizole is preferred to ethanol infusion for the therapy oftoxic alcohol ingestions. The recommended dosing regimen isthe same as that used in the study protocols (42, 43). Patientsreceiving hemodialysis require an additional bolus dose of 15mg/kg at the end of each dialysis session, and therapy is con-tinued until the serum ethylene glycol or methanol concentra-tion is less than 20 mg/dl.
However, fomepizole is unlikely to reduce mortality belowthat of a carefully monitored ethanol infusion, and consideringthat the cost to treat an adult with fomepizole for 48 hours isapproximately $5,000 for the drug alone, therapy should be re-
served for serious intoxications. The U.S. Food and Drug Ad-ministration has approved fomepizole for individuals
12years old with ethylene glycol or methanol poisoning. On thebasis of the above-described studies, the authors recommendreserving the use of fomepizole for intoxications with toxic al-cohol levels greater than 20 mg/dl, metabolic acidosis (bicar-bonate level less than 20 mEq/L), or a urine-to-serum osmolargap greater than 10 mOsm/L. Fomepizole therapy is also ad-visable when there is a lack of experience with ethanol ther-apy or the inability to provide frequent laboratory monitoringin confirmed poisonings.
SNAKE Fab ANTIVENOM
Most of the roughly 10,000 venomous snake bites reported an-nually in the United States are caused by members of the sub-family Crotalinae (pit vipers). Pit vipers are divided into threegenera: Crotalus
(rattlesnakes), Sistrurus
(pygmy rattlesnakesand massasauga), and Agkistrodon
(copperheads and watermoccasins). Crotaline venom is complex and composed of pro-teolytic enzymes, neurotoxins, cardiotoxins, direct lytic factors,hemolysins, and coagulation and anticoagulation factors (47,48). Standard treatment for envenomations includes general-ized wound care and antivenom therapy. For years, the only
antivenom available in the United States has been an equine-derived serum IgG (Antivenin Crotalidae Polyvalent [ACP];Wyeth, Paoli, PA). Although this antivenin has been effective,its use is associated with a high occurrence (23%) of acute hy-persensitivity reactions, including urticaria, anaphylactoid re-actions, and anaphylaxis (49). In addition, the incidence of se-rum sickness can be as high as 80% when more than five vialsof ACP are administered (50, 51). Consequently, physicianshave hesitated to use antivenom unless patients show moder-ate to severe signs of envenomation or progression of enveno-mation (
see
Table 5).More recently, ovine-derived serum monovalent Fab anti-
venom (Crofab) (Savage Laboratories, Melville, NY) was de-veloped for crotaline poisoning and has been used in two hu-
man trials. Venoms used in the production of the ACP andFab antivenoms are listed in Table 6. By eliminating the Fcfragment, the Fab preparation greatly reduces the risk of aller-gic reactions. The first trial was a prospective series of 11 pa-tients who were each initially treated with 4 vials of Fab anti-venom and an additional 4 vials if clinical signs or laboratoryvalues worsened. All patients were observed in the hospitalfor at least 48 hours and followed up at 7 and 14 days (52).Three patients had worsening of symptoms after initiation oftherapy, and six received the full eight vials of antivenom. Af-ter 7 days, one patient still had a prolonged prothrombin timeand three had hypofibrinogenemia.
The second trial prospectively monitored 38 patients withmoderate pit viper envenomations, initially treated with 4 to12 vials of the Fab antivenom (53). Local symptoms were sta-bilized within 24 hours in all treated patients. Twenty patients(53%) had late, persistent, or recurrent thrombocytopeniaand hypofibrinogenemia, persisting up to 2 weeks in a few pa-tients. During follow-up, 28 patients received additional Fabantivenom for an average total dose of 10.9 vials per patient.Six patients (16%) had mild to moderate hypersensitivity re-actions, another six (16%) developed serum sickness, and nonedeveloped anaphylaxis. No patient in either trial had clinicallysignificant bleeding. The occurrence of immunologic reactionsreported for the Fab antivenom is much lower than for theACP antivenom. The incidence of recurrent coagulopathy inpatients treated with the ACP antivenom is approximately45%, which is slightly less than the Fab antivenom (54).
TABLE 4. MEAN HALF-LIVES OF ELIMINATION* OF ETHYLENEGLYCOL AND METHANOL
Drug
Alone
With
Ethanol
With
Fomepizole
With Ethanol
and
Hemodialysis
Ethylene
glycol 2.54.5 (44)
17 (46) 19.7 (42) 2.6 (45)
Methanol 3.01 (46)
43 (46) 54 (43) 3.5 (46)
* In hours.
Numbers in parentheses indicate reference source. These were not direct compari-sons from controlled trials, and values should serve as approximations only.
Derived from low-level infusions in normal subjects. Half-life is longer at toxic levels.
-
8/22/2019 actualizaciones en toxicologia.pdf
6/7
14
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 166 2002
The treatment regimen for the Fab antivenom is an initialintravenous dose of four to six vials, which can be repeatedwithin 1 hour if the manifestations (e.g., local swelling, coagul-opathy) are not controlled after the first dose. An additionaltwo vials are administered every 6 hours for 18 hours to pre-vent the recurrence of manifestations. Retreatment with twomore vials of Fab antivenom is recommended if any of the
following occur: fibrinogen less than 50
g/ml, platelet countless than 25,000/mm
3
, international normalized ratio (INR)greater than 3.0, activated partial thromboplastin time (aPTT)greater than 50 seconds, or if the coagulopathy worsens (54).All patients treated with Fab antivenom require hospitaliza-tion for close monitoring of symptoms and the need for fur-ther therapy, and monitoring up to 2 weeks after envenoma-tion may be necessary.
The more favorable side effect profile of the Fab anti-venom has established it as the antivenin of first choice forCrotalinae envenomations and, from a riskbenefit perspec-tive, favors earlier initiation of therapy and treatment of milderenvenomations. In addition, the manufacturer has stoppedproduction of ACP, so the Fab antivenom has become the
only antivenin available for Crotalinae envenomations. How-ever, the Fab antivenom has some disadvantages, including ahigh rate of coagulopathy and considerable expense. Eachtwo-vial kit costs approximately $1,700 (U.S.), and thereforethe drug cost for a complete course of Fab antivenin therapycan be as much as $14,000. Therefore, from a costeffective-ness perspective, therapy should still be reserved for patientswith moderate to severe envenomations.
CONCLUSION
As is the case with most fields in medicine, clinical toxicologyhas rapidly evolved as the number of toxicologic syndromes
and antidotes has increased in response to the ever-expandingpharmacopoeia. In the current update, we have focused onseveral areas in which significant changes have occurred. Inthe case of serotonin syndrome, the rapidly increasing use ofserotonin reuptake inhibitors in the therapy of depression ne-cessitates that clinicians recognize the manifestations of thesyndrome and be aware of potential drug interactions that are
likely to produce it. The use of late N
-acetylcysteine for fulmi-nant liver injury from acetaminophen overdose is a change inthe approach, reflecting new evidence that some ameliorationof injury and improved survival may occur, even when used incases that previously would have been considered irreversible.Octreotide for sulfonylurea overdoses and insulin and glucosefor calcium channel blocker overingestions represent newer,inexpensive applications of older therapies. Fomepizole fortoxic alcohol ingestions is a new antidote that is becoming astandard of care because of its efficacy and safety in compari-son with ethanol infusions, despite its greater expense. Finally,with regard to pit viper envenomations, the older polyvalentantivenom has been replaced with a newer Fab antivenomthat is associated with a much lower risk of allergic reactions.
The topics covered in this update were selected to highlightdevelopments in the field of clinical toxicology that impact oncritical care medicine, but the list is far from exhaustive. Ap-proaches to the management of toxicologic syndromes will un-doubtedly continue to expand and evolve, and critical care cli-nicians are encouraged to keep abreast of new developments.
Acknowledgment
:
The authors thank Jan Hayden for assistance in prepara-tion of the manuscript.
References
1. Merigian KS, Woodard M, Hedges JR, Stuebing R, Rushkin MC. Pro-spective evaluation of gastric emptying in the self-poisoned patient.
Am J Emerg Med
1990;8:479483.
2. Pond SM, Lewis-Driver DJ, Williams GM, Green AC, Stevenson NW.Gastric emptying in acute overdose: a prospective randomized con-trolled trial. Med J Aust
1995;163:345349.3. Kulig K, Bar-Or D, Cantrill SV, Rosen P, Rumack BH. Management of
acutely poisoned patients without gastric emptying.Ann Emerg Med
1985;14:562567.4. Decker WJ, Combs HF, Corby DG. Adsorption of drugs and poisons by
activated charcoal. Toxicol Appl Pharmacol
1968;13:454460.5. Sporer KA. The serotonin syndrome: implicated drugs, pathophysiology
and management. Drug Saf
1995;13:94104.6. Oates JA, Sjoerdsma A. Neurologic effects of tryptophan in patients re-
ceiving a monoamine oxidase inhibitor. Neurology
1960;10:10761078.7. Smith B, Prockop DJ. Central nervous effects of ingestion ofL
-tryp-tophan by normal subjects. N Engl J Med
1962;267:13381341.8. Sternbach H. The serotonin syndrome.Am J Psychiatry
1991;148:705713.9. Lucki I, Nobler MS, Frazer A. Differential actions of serotonin antago-
TABLE 5. GRADING SCALE FOR THE SEVERITY OF CROTALINAE ENVENOMATIONS
Envenomation
Local Signs and
Symptoms
Systemic Signs and
Symptoms
Coagulation
Parameters Bleeding
Mild Limited swelling, None Normal None
pain, and ecchymosis
Moderate Swelling, pain, and Minor: nausea, vomiting, Minor None
ecchymosis beyond anxiety, oral parasthesias, abnormalities
bite; moderate to unusual taste;
severe pain mild hypotension,
tachycardia, and tachypnea
Severe Marked swelling, Severe: altered mental Markedly Severepain, and ecchymosis status, hypotension, abnormal, bleeding,
beyond bite; tachycardia, respiratory hemolysis epistaxis,
early blisters compromise, weakness, hematuria
renal failure,
cardiopulmonary arrest
TABLE 6. VENOMS USED TO PRODUCE SNAKE ANTIVENOM
Venoms Used in Production of:
ACP CroFab
Crotalus adamanteus
,
Crotalus adamanteus
,
eastern diamondback eastern diamondback
Crotalus atrox
,
Crotalus atrox
,
western diamondback western diamondback
Crotalus durissus terrificus
,
Crotalus scutulatus
,
tropical rattlesnake Mojave rattlesnake
Bothrops atrox
,
Agkistrodon piscivorus
,
fer-de-lance cottonmouth
Definition of abbreviations
: ACP
antivenin crotalidae polyvalent; CroFab
crotal-idae polyvalent immune Fab.
-
8/22/2019 actualizaciones en toxicologia.pdf
7/7
Update in Nonpulmonary Critical Care 15
nists on two behavioral models of serotonin receptor activation in therat.J Pharmacol Exp Ther
1984;1:133139.10. Lejoyeux M, Rouillon F, Ades J. Prospective evaluation of the serotonin
syndrome in depressed patients treated with clomipramine.Acta Psy-chiatr Scand
1993;88:369371.11. Dowling GP, McDonough ET, Bost RO. Eve and ecstasy: a report
of five deaths associated with the use of MDEA and MDMA. JAMA
1987;257:16151617.12. Graudins A, Stearman A, Chan B. Treatment of the serotonin syndrome
with cyproheptadine.J Emerg Med
1998;16:615619.13. Rumack BH, Peterson RC, Koch GG, Amara IA. Acetaminophen over-
dose.Arch Intern Med
1981;141:380385.14. Anker AL, Smilkstein MJ. Acetaminophen concepts and controversies.
Emerg Med Clin North Am
1994;12:335349.15. Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH. Efficacy of oral
N
-acetylcysteine in the treatment of acetaminophen overdose: analy-sis of the national multicenter study (19761985). N Engl J Med
1988;319:15571562.
16. OGrady JG, Alexander GJM, Hayllar KM, Williams R. Early indicators ofprognosis in fulminant hepatic failure. Gastroenterology
1989;97:439445.17. Harrison PM, Keays R, Bray GP, Alexander GJ, Williams R. Improved
outcome of paracetamol-induced fulminant hepatic failure by late ad-ministration of acetylcysteine. Lancet
1990;335:15721573.18. Keays R, Harrison PM, Wendon JA, Forbes A, Gove C, Alexander GJ.
Intravenous acetylcysteine in paracetamol induced fulminant hepaticfailure: a prospective controlled trial. BMJ
1991;330:10261030.19. Harrison PM, Wendon JA, Gimson AES, Alexander GJ, Williams R.
Improvement by acetylcysteine of hemodynamics and oxygen trans-
port in fulminant hepatic failure. N Engl J Med
1991;324:18521857.20. Yip L, Dart RC, Hurlbut KM. Intravenous administration of oral N
-ace-tylcysteine. Crit Care Med
1998;26:4043.21. Schmidt LE, Dalhoff K. Risk factors in the development of adverse reac-
tions to N
-acetylcysteine in patients with paracetamol poisoning. Br JClin Pharmacol
2001;51:8791.22.
Gerich JE. Oral hypoglycemic agents. N Engl J Med
1989;321:12311245.23. Seltzer HS. Drug-induced hypoglycemia: a review of 1418 cases. Endo-
crinol Metab Clin North Am
1989;18:163183.24. Katz M, Erstad BL. Octreotide, a new somatostatin analogue. Clin
Pharm
1989;8:255273.25. Lamberts SWJ, Van der Lely AJ, de Herder WW, Hofland LJ. Oct-
reotide.
N Engl J Med
1996;334:246254.26. Alberti KGMM, Christensen NJ, Christensen SE, Hansen AP, Iversen J,
Lanbaek K, Seyer-Hansen K, Orskou H. Inhibition of insulin secre-tion by somatostatin. Lancet
1973;2:12991301.27. Gerich JE, Lorenzi M, Schneider V, Forsham PH. Effect of somatostatin
on plasma glucose and insulin responses to glucagons and tolbutamidein man.J Clin Endocrinol Metab
1974;39:10571060.28. Boyle PJ, Justice K, Krentz AJ, Nagy RJ, Schade DS. Octreotide re-
verses hyperinsulinemia and prevents hypoglycemia induced by sul-fonylurea overdoses.J Clin Endocrinol Metab
1993;76:752756.29. Krentz AJ, Boyle PJ, Justice KM, Wright AD, Schade DS. Successful
treatment of severe refractory sulfonylurea-induced hypoglycemiawith octreotide. Diabetes Care
1993;16:184186.30. McLaughlin SA, Crandall CS, McKinney PE. Octreotide: an antidote for
sulfonylurea-induced hypoglycemia.Ann Emerg Med
2000;36:133138.31. Stehouwer CD, Lems WF, Fischer HR, Hackeng WH, Naafs MA. Ag-
gravation of hypoglycemia in insulinoma patients by the long-actingsomatostatin analogue octreotide (Sandostatin).Acta Endocrinol
1989;121:3440.
32. Gama R, Marks V, Wright J, Teale JD. Octreotide exacerbated fastinghyperglycaemia in a patient with a proinsulinoma: the glucostatic im-
portance of pancreatic glucagon. Clin Endocrinol
1995;43:117120.
33. Opie LH. Metabolism of free fatty acids, glucose and catecholamines inacute myocardial infarction: relation to myocardial ischemia and in-farct size.Am J Cardiol
1975;36:938953.34. Kline JA, Tomaszewski CA, Schroeder JD, Raymond RM. Insulin is a
superior antidote for cardiovascular toxicity induced by verapamil inthe anesthetized canine.J Pharmacol Exp Ther1993;267:744750.
35. Kline JA, Raymond RM, Leonova ED, Williams TC, Watts JA. Insulinimproves heart function and metabolism during non-ischemic cardio-genic shock in awake canines. Cardiovasc Res 1997;34:289298.
36. Kline JA, Raymond RM, Shroeder D, Watts JA. The diabetogenic ef-fects of acute verapamil poisoning. Toxicol Appl Pharmacol 1997;
145:357362.37. Yuan TH, Herns WP, Tomaszewski CA, Ford MD, Kline JA. Insulin im-
proves heart function and metabolism during non-ischemic cardio-genic shock in awake canines. Cardiovasc Res 1997;34:289298.
38. Yuan TH, Herns WP, Tomaszewski CA, Ford MD, Kline JA. Insulinglucose as adjunctive therapy for severe calcium channel antagonistpoisoning.J Toxicol Clin Toxicol1999;37:463474.
39. Jacobsen D, McMartin KE. Antidotes for methanol and ethylene glycolpoisoning.J Toxicol Clin Toxicol1997;35:127143.
40. Van Stee E, Harris A, Horton M, Black KC. The treatment of ethyleneglycol toxicosis with pyrazole.J Pharmacol Exp Ther1975;192:251259.
41. McMartin K, Hedstrom K, Tolk B, Ostling-Wentzell H, Blomstrand R.Studies on the metabolic interactions between 4-methylpyrazole andmethanol using monkeys as an animal model.Arch Biochem Biophys1980;199:606614.
42. Brent J, McMartin K, Phillips S, Burkhart KK, Donovan JW, Wells M,Kulig K. Fomepizole for the treatment of ethylene glycol poisoning. N
Engl J Med 1999;340:832838.43. Brent J, McMartin K, Phillips S, Aaron C, Kulig K. Fomepizole for the
treatment of methanol poisoning. N Engl J Med 2001;344:424429.44. Peterson CD, Collins AJ, Himes JM, Bullock ML, Keane WF. Ethylene
glycol poisoning: pharmacokinetics during therapy with ethanol andhemodialysis. N Engl J Med 1981;304:2123.
45. Jacobsen D, Hewlett TP, Webb R, Brown ST, Ordinario AT, McMartinKE. Ethylene glycol intoxication: implications for management. AnnEmerg Med 2000;36:114125.
46. Palatnick W, Redman LW, Sitar DS, Tenenbein M. Methanol half-lifeduring ethanol administration: implications for management of meth-anol poisoning.Ann Emerg Med 1995;26:202207.
47. Iyaniwura TT. Snake venom constituents: biochemistry and toxicology.Part 1. Vet Hum Toxicol1991;33:468474.
48. Jurkovich GI, Luterman A, McCullar K, Ramenofsky ML, Curreri PW.Complications of Crotalidae antivenin therapy. J Trauma 1988;28:10321037.
49. Kunkel DB, Curry SC, Vance MV, Ryan PJ. Reptile envenomations.JToxicol Clin Toxicol1984;21:503526.
50. Dart RC, Seifert SA, Carroll L. Mixed nonspecific crotalid antivenomovine Fab for the treatment of crotalid venom poisoning.Ann EmergMed 1997;30:3339.
51. Dart RC, McNally J. Efficacy, safety and use of snake antivenoms in theUnited States.Ann Emerg Med 2001;37:181188.
52. Dart RC, Seifert SA, Carroll L, Clark RF, Hall E, Boyer-Hassen LV,Curry SC, Kitchens CS, Garcia RA. Affinity-purified, mixed mono-specific crotalid antivenom ovine Fab for the treatment of crotalidvenom poisoning.Ann Emerg Med 1997;30:3339.
53. Boyer LV, Seifert SA, Clark RF, McNally JT, Williams SR, Nordt SP,Walter FG, Dart RC. Recurrent and persistent coagulopathy follow-ing pit viper envenomation.Arch Intern Med 1999;159:706710.
54. Boyer LV, Seifert SA, Cain JS. Recurrence phenomena after immunoglob-ulin therapy for snake envenomations: 2. Guidelines for clinical manage-
ment with crotalline Fab antivenom.Ann Emerg Med2001;37:196201.