Activity after retirement
5
Physiotherapy Research International Physiother. Res. Int. 11(1) 51–55 (2006) Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/pri.38 51 Physiother. Res. Int. 11: 51–55 (2006) Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri Case report: Activity after retirement ELIZABETH BRYANT and MARION TREW Clinical Research Centre for Health Profes- sions, University of Brighton, UK ALISON BRUCE School of Engineering, University of Brighton, UK INTRODUCTION Retirement is considered a critical stage of life with profound changes in an individual’s lifestyle. Sudden changes in physical activ- ity levels could be reflected in changes in several key physiological parameters related to falling, lower limb strength, joint range of motion and balance performance. This Case Report provides details of one female (aged 56) who had fallen twice during the 12 months prior to retirement. Assessments of lower limb strength, joint range of motion, balance performance and physical activity levels were undertaken at baseline (one week pre-retirement) and repeated six and 12 months later. Contrary to expectations, this previously sedentary female reported sig- nificant lifestyle changes after retirement by taking up new physical activities, which resulted in substantial improvements in her lower limb strength, joint range of motion and balance performance. The normal ageing process results in a gradual decline in physical performance starting as early as 30 years of age. Reduc- tions in muscle mass and strength with ageing have been reported (Lindle et al., 1997; Akima et al., 2001; Trappe et al., 2001), as well as deteriorations in balance performance (Woollacott, 1993; Era et al., 2002) and reductions in joint range of motion (Vandervoort et al., 1992; Mecagni et al., 2000). Furthermore, ageing is generally associated with a reduction in habitual levels of physical activity (Hardman and Stensel, 2003). It is understood that a change in phys- ical activity levels at almost any chronologi- cal age can have either a positive or negative effect on numerous physiological parameters (Astrand and Rodahl, 1986), including those related to falling in later life (Lord et al., 1995; Ferretti et al., 2001). Retirement from full-time employment is an important transitional process, which can result in substantial changes in an individu- al’s lifestyle (Sterns and Hurd-Gray, 1999). With increased life expectancy, an individual could spend a third of their lifetime in retire- ment. It is in this period that falls start to become commonplace and they have been linked to lower limb muscle weakness (Whipple et al., 1987; Skelton et al., 2002), reduced joint range of motion (Studentski et al., 1991; O’Brien et al., 1997) and balance instability (Maki et al., 1994; Stel et al., 2003). It appears that, for some individuals, retire- ment may be viewed as a period of well- earned rest and senescence after a lifetime of productive employment, and thus it is the potential watershed for a decrease in physical activity levels. For others, retirement may offer the freedom and opportunity to partici- pate in new physical activities or spend more
-
Upload
elizabeth-bryant -
Category
Documents
-
view
213 -
download
0
Transcript of Activity after retirement
Physiotherapy Research InternationalPhysiother. Res. Int. 11(1) 51–55 (2006)Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pri.38
51
Physiother. Res. Int. 11: 51–55 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
Case report: Activity after retirement
ELIZABETH BRYANT and MARION TREW Clinical Research Centre for Health Profes-sions, University of Brighton, UK
ALISON BRUCE School of Engineering, University of Brighton, UK
INTRODUCTION
Retirement is considered a critical stage of life with profound changes in an individual’s lifestyle. Sudden changes in physical activ-ity levels could be reflected in changes in several key physiological parameters related to falling, lower limb strength, joint range of motion and balance performance. This Case Report provides details of one female (aged 56) who had fallen twice during the 12 months prior to retirement. Assessments of lower limb strength, joint range of motion, balance performance and physical activity levels were undertaken at baseline (one week pre-retirement) and repeated six and 12 months later. Contrary to expectations, this previously sedentary female reported sig-nificant lifestyle changes after retirement by taking up new physical activities, which resulted in substantial improvements in her lower limb strength, joint range of motion and balance performance.
The normal ageing process results in a gradual decline in physical performance starting as early as 30 years of age. Reduc-tions in muscle mass and strength with ageing have been reported (Lindle et al., 1997; Akima et al., 2001; Trappe et al., 2001), as well as deteriorations in balance performance (Woollacott, 1993; Era et al., 2002) and reductions in joint range of motion
(Vandervoort et al., 1992; Mecagni et al., 2000). Furthermore, ageing is generally associated with a reduction in habitual levels of physical activity (Hardman and Stensel, 2003). It is understood that a change in phys-ical activity levels at almost any chronologi-cal age can have either a positive or negative effect on numerous physiological parameters (Astrand and Rodahl, 1986), including those related to falling in later life (Lord et al., 1995; Ferretti et al., 2001).
Retirement from full-time employment is an important transitional process, which can result in substantial changes in an individu-al’s lifestyle (Sterns and Hurd-Gray, 1999). With increased life expectancy, an individual could spend a third of their lifetime in retire-ment. It is in this period that falls start to become commonplace and they have been linked to lower limb muscle weakness (Whipple et al., 1987; Skelton et al., 2002), reduced joint range of motion (Studentski et al., 1991; O’Brien et al., 1997) and balance instability (Maki et al., 1994; Stel et al., 2003). It appears that, for some individuals, retire-ment may be viewed as a period of well-earned rest and senescence after a lifetime of productive employment, and thus it is the potential watershed for a decrease in physical activity levels. For others, retirement may offer the freedom and opportunity to partici-pate in new physical activities or spend more

Bryant et al.52
Physiother. Res. Int. 11: 51–55 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
time participating in current physically active leisure pursuits (Long, 1987; Jonsson et al., 2000; Evenson et al., 2002).
CASE DESCRIPTION
Mrs A, aged 56, had been employed as a health professional for over 30 years. At her initial assessment (one week pre-retirement) Mrs A reported having fallen twice during the previous 12 months. She was not taking any medication and reported no visual impairments. Mrs A commented that she undertook the minimal level of physical activity outside the workplace. Her husband undertook all the household chores, for example shopping, cooking, housework. Before volunteering for the study, Mrs A had decided that she needed to take action to improve her physical fitness and overall well-being once ceasing full-time employ-ment. She advised the researcher that she planned to join a local gymnasium when she retired from full-time employment.
Measurements
Measurements of lower limb strength, joint range of motion, balance performance and activity levels were undertaken at baseline, one week pre-retirement, and were repeated six and 12 months after retirement. Peak torque of the knee extensor/flexor muscle groups was measured bilaterally using an isokinetic dynamometer (Biodex 2, Shirley, NY). Isokinetic concentric contractions were performed at an angular velocity of 60°/s. Lower limb joint range of motion was measured using flexible electrogoniometers (Biometrics Ltd, Blackwood, Gwent). Mea-surements of hip extension, knee flexion and ankle range of motion were undertaken. Balance performance was assessed during quiet standing on a force platform (Kistler
Instruments Ltd, Winterthur, Switzerland). Balance tasks included standing barefoot with the feet together (eyes open and eyes closed) and single limb stance trials for a period of 30 seconds. Activity levels were determined using a questionnaire (Voorrips et al., 1991). Ethical approval for this study was granted by the University Research Ethics Committee, and informed consent was obtained from Mrs A prior to participation.
Baseline data pre-retirement
Mrs A reported having several unexplained falls prior to commencing the study. Outside work she led a very sedentary lifestyle, which was reflected in her low activity score. Mrs A showed signs of lower limb muscle weak-ness, displaying peak torque values substan-tially lower than previously reported (Sunnerhagen et al., 2000; Hughes et al., 2001) using the same measurement protocol with volunteers of similar age groups and body size. The peak torque values recorded for Mrs A were similar to the peak torque values reported from a group of elderly nursing home residents with a mean age 82 years (Whipple et al., 1987). In addition, Mrs A displayed signs of balance instability with significantly larger centre of pressure dis-placement values than previously reported for this age group (Maki et al., 1990; Blaszczyk et al., 2000), in particular in the medial-lateral plane, whilst standing with the feet together (eyes open and eyes closed). The values exhibited by Mrs A were similar to those found in earlier studies where greater centre of pressure displacement values were reported in the medial-lateral plane in fallers than non-fallers (Maki et al., 1994; Stel et al., 2003) performing a similar balance task. Mrs A also exhibited a limited range of movement at the ankle joint. Her total range
Activity after retirement 53
Physiother. Res. Int. 11: 51–55 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
of movement from full plantar flexion to full dorsiflexion was only 39°.
Follow-up data after retirement
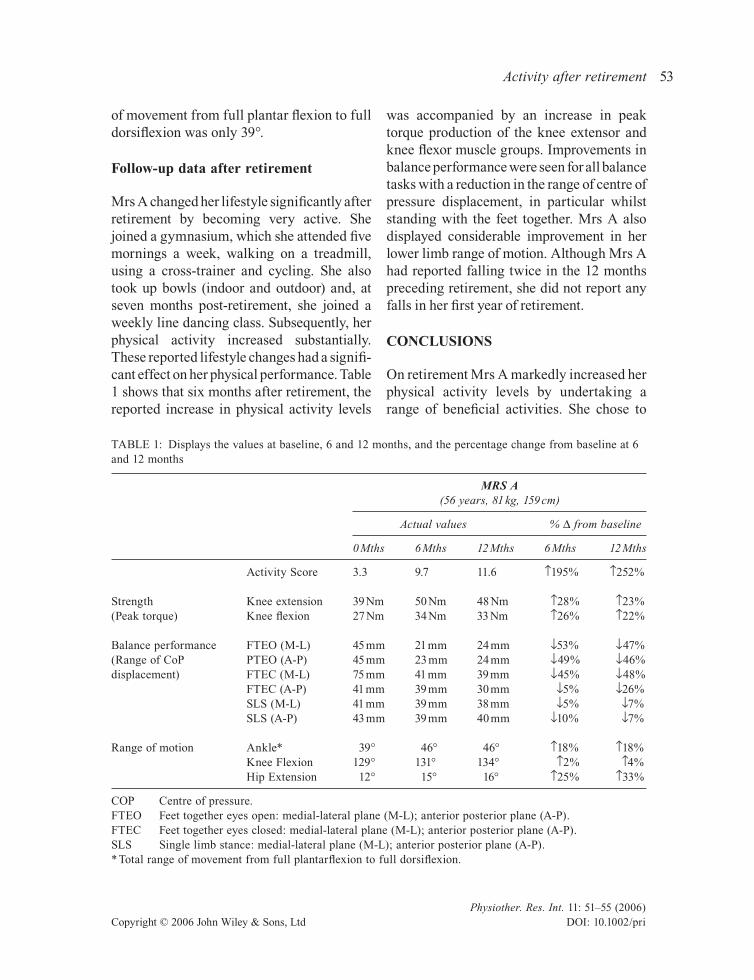
Mrs A changed her lifestyle significantly after retirement by becoming very active. She joined a gymnasium, which she attended five mornings a week, walking on a treadmill, using a cross-trainer and cycling. She also took up bowls (indoor and outdoor) and, at seven months post-retirement, she joined a weekly line dancing class. Subsequently, her physical activity increased substantially. These reported lifestyle changes had a signifi-cant effect on her physical performance. Table 1 shows that six months after retirement, the reported increase in physical activity levels
was accompanied by an increase in peak torque production of the knee extensor and knee flexor muscle groups. Improvements in balance performance were seen for all balance tasks with a reduction in the range of centre of pressure displacement, in particular whilst standing with the feet together. Mrs A also displayed considerable improvement in her lower limb range of motion. Although Mrs A had reported falling twice in the 12 months preceding retirement, she did not report any falls in her first year of retirement.
CONClUSIONS
On retirement Mrs A markedly increased her physical activity levels by undertaking a range of beneficial activities. She chose to
TABLE 1: Displays the values at baseline, 6 and 12 months, and the percentage change from baseline at 6 and 12 months
MRS A (56 years, 81 kg, 159 cm)
Actual values % D from baseline
0 Mths 6 Mths 12 Mths 6 Mths 12 Mths
Activity Score 3.3 9.7 11.6 ↑195% ↑252%
Strength Knee extension 39 Nm 50 Nm 48 Nm ↑28% ↑23%(Peak torque) Knee flexion 27 Nm 34 Nm 33 Nm ↑26% ↑22%
Balance performance FTEO (M-L) 45 mm 21 mm 24 mm ↓53% ↓47%(Range of CoP PTEO (A-P) 45 mm 23 mm 24 mm ↓49% ↓46%displacement) FTEC (M-L) 75 mm 41 mm 39 mm ↓45% ↓48% FTEC (A-P) 41 mm 39 mm 30 mm ↓5% ↓26% SLS (M-L) 41 mm 39 mm 38 mm ↓5% ↓7% SLS (A-P) 43 mm 39 mm 40 mm ↓10% ↓7%
Range of motion Ankle* 39° 46° 46° ↑18% ↑18% Knee Flexion 129° 131° 134° ↑2% ↑4% Hip Extension 12° 15° 16° ↑25% ↑33%
COP Centre of pressure.FTEO Feet together eyes open: medial-lateral plane (M-L); anterior posterior plane (A-P).FTEC Feet together eyes closed: medial-lateral plane (M-L); anterior posterior plane (A-P).SLS Single limb stance: medial-lateral plane (M-L); anterior posterior plane (A-P).* Total range of movement from full plantarflexion to full dorsiflexion.

Bryant et al.54
Physiother. Res. Int. 11: 51–55 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
take up bowling, an activity that challenges both balance and joint range of movement, line dancing to benefit balance and aerobic function, and the gymnasium activities for improvements in both aerobic and anaerobic ability. Her results illustrate the effect of positive lifestyle changes after retirement. Following substantial increases in physical activity levels, improvements were seen in her balance performance (a reduced range of CoP displacement whilst standing quietly), together with an increase in lower limb strength and improvements in her lower limb joint range of motion. Most importantly, she had not had any falls since retiring.
This finding illustrates that even without guidance from an exercise specialist Mrs A was able to achieve substantial increases in physical activity levels, which produced physiological benefits within a relatively short period of time. Mrs A had fallen twice during the 12 months prior to entering this study and in the initial stages showed signs of muscle weakness, balance instability and limited joint range of motion. The substantial lifestyle changes she undertook at retirement certainly reduced her risk of falling, and will help her to maintain her functional indepen-dence during the early stages of retirement.
REFERENCES
Akima H, Kano Y, Enomoto Y, Ishizu M, Okada M, Oishi Y et al. Muscle function in 164 men and women aged 20–84 yrs. Medicine and Science in Sports and Exercise 2001; 33: 220–226.
Astrand P-O, Rodahl K. Textbook of Work Physiol-ogy: Physiological Bases of Exercise (third edition). New York, NY: McGraw-Hill, 1986.
Blaszczyk JW, Prince F, Raiche M, Hebert R. Effect of ageing and vision on limb load asymmetry during quiet stance. Journal of Biomechanics 2000; 33: 1243–1248.
Era P, Heikkinen E, Gause-Nilsson I, Schroll M. Pos-tural balance in elderly people: changes over a five year follow up and its predictive value for
survival. Aging — Clinical & Experimental Research 2002; 14: 37–46.
Evenson KR, Rosamond WD, Cai J, Diez-Roux AV, Brancati FL. Atherosclerosis risk in communities Study I. Influence of retirement on leisure-time physical activity: the atherosclerosis risk in com-munities study. American Journal of Epidemiol-ogy 2002; 155: 692–699.
Ferretti G, Berg HE, Minetti AE, Moia C, Rampichini S, Narici MV. Maximal instantaneous muscular power after prolonged bed rest in humans. Journal of Applied Physiology 2001; 90: 431–435.
Hardman AE, Stensel DJ. Physical Activity and Health: The Evidence Explained. London: Rout-ledge, 2003.
Hughes VA, Frontera WR, Wood M, Evans WJ, Dallal GE, Roubenoff R et al. Longitudinal muscle strength changes in older adults: influence of muscle mass, physical activity, and health. Journal of Gerontology 2001; 56: B209–B217.
Jonsson H, Borell L, Sadlo G. Retirement: an occu-pational transition with consequences for tempo-rality, balance and meaning of occupations. Journal of Occupational Science 2000; 7: 5–13.
Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J et al. Age and gender comparisons of muscle strength in 654 women and men aged 20–93 yr. Journal of Applied Physiology 1997; 83: 1581–1587.
Long J. Continuity as a basis for change: leisure and male retirement. Leisure Studies 1987; 6: 55–70.
Lord SR, Ward JA, Williams P, Strudwick M. The effect of a 12-month exercise trial on balance, strength and falls in older women: a randomized controlled trial. Journal of the American Geriat-rics Society 1995; 43: 1198–1206.
Maki BE, Holliday PJ, Fernie GR. Aging and postural control. A comparison of spontaneous and induced sway balance tests. Journal of the American Geri-atrics Society 1990; 38: 1–9.
Maki BE, Holliday PJ, Topper AK. A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. Journal of Gerontology 1994; 49: M72–84.
Mecagni C, Pulliam-Smith J, Roberts KE, O’Sullivan SB. Balance and ankle range of motion in com-munity dwelling women aged 64 to 87 years: a correlational study. Physical Therapy 2000; 80: 1004–1011.
O’Brien K, Culham E, Pickles B. Balance and skele-tal alignment in a group of elderly female fallers

Activity after retirement 55
Physiother. Res. Int. 11: 51–55 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
and nonfallers. Journal of Gerontology 1997; 52A: B221–B226.
Skelton D, Kennedy J, Rutherford OM. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age and Ageing 2002; 31: 119–125.
Stel VS, Smit JH, Pluijm SMF, Lips P. Balance and mobility performance as treatable risk factors for recurrent falling in older persons. Journal of Clinical Epidemiology 2003; 56: 659–668.
Sterns HL, Hurd-Gray J. Work, leisure and retire-ment. In: Cavanaugh J, Krauss-Whitbourne S (eds), Gerontology: An Interdisciplinary Perspec-tive. Oxford: Oxford University Press, 1999; 355–390.
Studentski S, Duncan PW, Chandler J. Postural responses and effector factors in persons with unexplained falls: results and methodologic issues. Journal of the American Geriatrics Society 1991; 39: 229–234.
Sunnerhagen KS, Herdberg M, Henning G, Cider A, Svantesson U. Muscle performance in an urban population sample of 40 to 79 year old men and women. Scandinavian Journal of Rehabilitation Medicine 2000; 32: 159–167.
Trappe TA, Lindquist DM, Carrithers JA. Muscle-specific atrophy of the quadriceps femoris with
aging. Journal of Applied Physiology 2001; 90: 2070–2074.
Vandervoort AA, Chesworth BM, Cunningham DA, Paterson DH, Rechnitzer PA, Koval JJ. Age and sex effects of mobility on the human ankle. Journal of Gerontology 1992; 47: M17–M21.
Voorrips LE, Ravelli ACJ, Dongelmans PCA, Deurenberg P, Staveren WAV. A physical activity questionnaire for the elderly. Medicine and Science in Sports and Exercise 1991; 23: 974–979.
Whipple RH, Wolfson LI, Amerman PM. The relation-ship of knee and ankle weakness to falls in nursing home residents: an isokinetic study. Journal of the American Geriatrics Society 1987; 35: 13–20.
Woollacott MH. Age-related changes in posture and movement. Journal of Gerontology 1993; 48: 56–60.
Address correspondence to: Dr Elizabeth C Bryant, University of Brighton, Clinical Research Centre for Health Professions, Aldro Building, 49 Darley Road, Eastbourne, East Sussex BN20 7UR, UK (E-mail: [email protected]).
(Submitted September 2005; accepted November 2005)