Acs
3
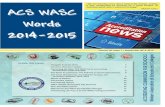
ADULT INTERNAL MEDICINE ACUTE CORONARY SYNDROME AIMS Beware: - Any arm/chest pain - New onset "indigestion" - Diaphoresis/Nausea - Determine Risk Group: - Ask re cardiac risk factors - Atypical Sx: (diabetics, indigenous, elderly, women) - Serum marker (troponin) - High Risk chest pain - at rest - prolonged (>10 mins) - recurrent - assoc with syncope, LVF Bleeding risk - major bleeding or transfusion are strong predictors of mortality - assess bleeding risk all High Risk NSTEACS patients - Elevated Troponin -Search for alternative cause in Acute illness (esp. aortic dissection, pulmonary embolism, sepsis, tachy or brady arrhythmias; - acute neurological disease incl stroke or SAH Dx : Establish Risk Stratification High risk pts Intermediate risk pts Low risk pts HIGH RISK PATIENTS: (6/12 risk death or MI >10%) - Repetitive ,Prolonged(>10min) or Ongoing pain - ST depression (> 0.5mm) or new T-wave inversions(2mm) in >2 leads - Transient ST elevation (0.5mm) in >2 contiguous leads - Elevated serum Troponin - Prior PCI (within 6/12) or prior CABG - Heart failure, shock or syncope - (EF<40% ; SBP<90mmHg) - new mitral regurgitation - Diabetes (+ typical Sx ACS) - CRF (eGFR <60ml/min + typical Sx ACS) INTERMEDIATE RISK PTS: (6/12 risk death or MI 2-10%) - History of prolonged, repetitive chest pain or pain at rest (last 48 hrs; currently resolved) - Two or more Risk factors - known HTN - family Hx - active smoking - hyperlipidaemia - Known CHD - prior AMI with LVEF40% - Coronary disease >50% stenosed coronary arteries - Age over 65 yrs - Diabetes + atypical Sx of ACS - eGFR <60 ml/min + atypical Sx of ACS LOW RISK PTS: (i) Chest pain resolved & not recurred (ii) Normal ECG (iii) No detectable troponin (iv) No high/intermediate risk features ie. Includes: - onset angina past month - worsening severity, freq of angina Tx: Low risk pts Intermediate risk pts High risk pts 1. LOW RISK PTS: Principal = discharge on upgraded medical Rx PLUS urgent cardiac follow-up - Check meds – make sure patient has: - Aspirin daily - GTN PRN - Repeat Troponin 3 hrs after onset of pain if initial test negative then at 6 hrs - Should be referred for a cardiac assessment within 4 wk's (EST or Sistemibi scan)
-
Upload
samer-farhan -
Category
Documents
-
view
213 -
download
1
description
acute coronary syndrome, chest pain, adult medicine
Transcript of Acs

ADULT INTERNAL MEDICINEACUTE CORONARY SYNDROMEAIMSBeware: - Any arm/chest pain - New onset "indigestion" - Diaphoresis/Nausea - Determine Risk Group:
- Ask re cardiac risk factors - Atypical Sx: (diabetics, indigenous,
elderly, women) - Serum marker (troponin) - High Risk chest pain
- at rest - prolonged (>10 mins) - recurrent - assoc with syncope, LVF
Bleeding risk- major bleeding or transfusion are strong
predictors of mortality- assess bleeding risk all High Risk
NSTEACS patients- Elevated Troponin
-Search for alternative cause in Acute illness (esp. aortic dissection, pulmonary embolism, sepsis, tachy or brady arrhythmias;
- acute neurological disease incl stroke or SAH
Dx : Establish Risk StratificationHigh risk ptsIntermediate risk ptsLow risk pts
HIGH RISK PATIENTS: (6/12 risk death or MI >10%) - Repetitive ,Prolonged(>10min) or Ongoing
pain - ST depression (> 0.5mm) or new T-wave
inversions(2mm) in >2 leads - Transient ST elevation (0.5mm) in >2
contiguous leads - Elevated serum Troponin - Prior PCI (within 6/12) or prior CABG - Heart failure, shock or syncope - (EF<40% ; SBP<90mmHg) - new mitral regurgitation- Diabetes (+ typical Sx ACS) - CRF (eGFR <60ml/min + typical Sx ACS)
INTERMEDIATE RISK PTS: (6/12 risk death or MI 2-10%) - History of prolonged, repetitive chest pain
or pain at rest (last 48 hrs; currently
resolved)
- Two or more Risk factors- known HTN- family Hx - active smoking - hyperlipidaemia
- Known CHD - prior AMI with LVEF40% - Coronary disease >50% stenosed coronary
arteries - Age over 65 yrs - Diabetes + atypical Sx of ACS - eGFR <60 ml/min + atypical Sx of ACS
LOW RISK PTS: (i) Chest pain resolved & not recurred (ii) Normal ECG (iii) No detectable troponin (iv) No high/intermediate risk features ie. Includes: - onset angina past month - worsening severity, freq of angina
Tx: Low risk ptsIntermediate risk ptsHigh risk pts
1. LOW RISK PTS: Principal = discharge on upgraded medical Rx PLUS urgent cardiac follow-up - Check meds – make sure patient has:
- Aspirin daily - GTN PRN
- Repeat Troponin 3 hrs after onset of pain if initial test negative then at 6 hrs - Should be referred for a cardiac assessment within 4 wk's (EST or Sistemibi scan)
2. INTERMEDIATE RISK PTS: Principal = risk stratify + reclassify into HIGH or LOW riskObs: Telemtery - Intensive observation (telemetry) &
investigation for at least 8 hrs - Cardiac monitoring - Frequent ECG's Q3H or ST segment monitoring - Repeat Troponin 6 hrs after onset of pain (if +ve) and 3 hours post Sx if –ve
Initial Mx (MONA)- O2 – if SaO2 <93%- GTN- Aspirin – 300mg + 150mg daily/ consider
clopidogrel 300mg stat + 75mg daily
Invx - ECG

- CXR- Bloods: Tp, FBC, Coags, CK Aim to reclassify within 24 hrs(high / low risk) - If pt. remains pain free with all tests
negative then exercise stress test before discharge
ANY POSITIVE RESULTS CALL FOR A RECLASSIFICATION AS HIGH RISK cardiology consult!!! Re- lysis or PCI
3. HIGH RISK PTS: Principal = - Aggressive medical Rx + coronary
angiography / revascularisation - Balance of Ischaemic Risk & Bleeding Risk
for individual patient essential - seek early Cardiology advice
Tx Obs: Telemtery - Intensive observation (telemetry) &
investigation for at least 8 hrs - Cardiac monitoring - Frequent ECG's Q3H or ST segment monitoring - Repeat Troponin 6 hrs after onset of pain (if +ve) and 3 hours post Sx if –ve
Initial Mx (MONA)- O2 – if SaO2 <93%- GTN- Aspirin – 300mg + 150mg daily/ consider- + Clopidogrel 300mg stat + 75mg daily
Invx - ECG- CXR- Bloods: Tp, FBC, Coags, CK
Definitive Management (by cardiology team)- LMWH –
- 72 hrs 1mg/kg b.d. - reduce dose in elderly or renal impairment(0.8mg/kg b.d. or 1mg/kg once daily)
- IF increased bleeding risk consider IV. Heparin – - bolus 4000 u/s infusion 800 - 1000 u/s
per hour APTT monitoring- Clopidogrel
- 300mg stat plus 75 mg daily (unless surgery likely within 5 days)
- IF undergoing PCI consider high dose regime (600mg bolus plus 150mg/d ) - seek advice
- Tirofiban (GII/PIII) anti-platelet - Continue supportive treatment with
morphine (2.5mg IV. bolus prn.) & nitratesNitrates
- Early use of below unless C-Ind in all patients with ACS- Beta blockers - Ace inhibitors - Statin High Dose (eg atorvastatin 80mg)
Cardiology team to arrange for: - Angiography within 48 hrs recommended - Percutaneous coronary intervention - Bypass surgery
LONG TERM Mx (i) Cardiac Rehabilitation Program - Education - Risk factor modification - Regular exercise- GTT if not Dx diabetic(ii) Written action plan for Chest Pain (iii) Depression - common - poorer outcomes
NOTESBleeding risk increasedTroponinTimi score
1. BLEEDING RISK INCREASED- age >75- female- Hx bleeding (esp. recent)- Hx stroke, TIA- creatinine clearance <60mL/min- diabetes- heart failure- PVD- anaemia- concomitant use of GP IIb/IIIa inhibitor- enoxaparin 48 hrs prior to intervention- body weight < 60kg
2. TROPONIN- High sensitivity assays recommended (TnT
or TnI )- Positive test IF - level > 99%ile
OR - change of >50% above an initial baseline
level- Negative test IF
- not positive (above)- one assay taken >6 hrs from Sx onset
- Action on Positive test- cardiac consultation if ACS suspectted (usually changing levels)
Search for alternative cause - Acute illness (usually changing levels)
esp. aortic dissection, pulmonary embolism, sepsis, tachy or brady arrhythmias, acute neurological disease incl. stroke or SAH

- Subacute / Chronic conditions (usually stable levels over 24 hr period)i.e. Cardiac contusion or surgery; CCF acute or chronic; aortic valve disease; HOCM; severe pulm HPT; renal failure; inflammatory cardiac disease (eg. pericarditis SBE); burns > 30%; infiltrative disease; extreme exertion
3. TIMI Score: 1-7 (risk of death)Score 1 for each category: - age >65 - 2 cardiac RF's including diabetes - >1 episode chest pain at rest <24hrs - prior angiographic stenosis >50% - ST depression >=0.5mm - elevated cardiac markers - use of aspirin previous 7 days Result /7 - 4/7 or greater high risk of death or MI in
next 2 weeks - Seek specialist advice - early transfer
appropriate