ACP REVIEW: Rheumatology Volume 1
108
ACP REVIEW: Rheumatology Volume 1 GREGORY GARDNER, MD, MACP GILLILAND-HENDERSON PROFESSOR OF MEDICINE DIVISION OF RHEUMATOLOGY UNIVERSITY OF WASHINGTON
Transcript of ACP REVIEW: Rheumatology Volume 1
ACP REVIEW:Rheumatology Volume 1
GREGORY GARDNER, MD, MACP
GILLILAND-HENDERSON PROFESSOR OF MEDICINE
DIVIS ION OF RHEUMATOLOGY
UNIVERSITY OF WASHINGTON

Outline
•Sorting out synovitis
•Common musculoskeletal conditions on the boards
•Arthritis and more arthritis
•Rash and arthritis
•Goutology

BASIC CONCEPTS TO SORT OUT SYNOVITIS

Inflammatory
◦ AM stiffness > 30 min (often several hrs)
◦ Improvement with activity
◦ Swelling common
◦ Rheumatoid arthritis, polymyalgia rheumatica
Mechanical
◦ 10-15 minutes of AM stiffness
◦ Pain worse with use
◦ Osteoarthritis, tendonitis
Fibromyalgia
◦ Non-restorative sleep
◦ Fatigue
◦ Memory difficulty
◦ Pain in up to 19 different areas
◦ Exercise intolerance i.e. feeling “wiped out”
Pearl #1: Three Patterns of Joint Pain
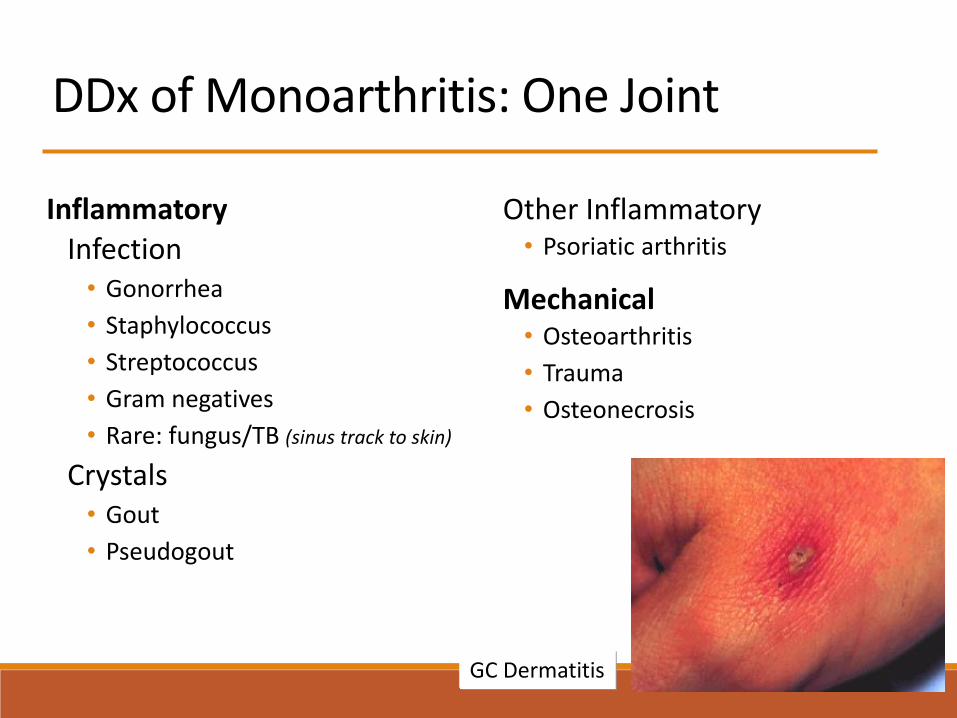
DDx of Monoarthritis: One Joint
InflammatoryInfection• Gonorrhea
• Staphylococcus
• Streptococcus
• Gram negatives
• Rare: fungus/TB (sinus track to skin)
Crystals• Gout
• Pseudogout
Other Inflammatory• Psoriatic arthritis
Mechanical• Osteoarthritis
• Trauma
• Osteonecrosis
GC Dermatitis

DDx of Pauciarthritis: 2-5 Joints
InflammatoryInfection
• Lyme arthritis
• Recurrent large knee effusions
• Bacteria
Other
• Polymyalgia rheumatica
• Spondyloarthropathy
• Psoriatic arthritis
• Reactive arthritis
•Sarcoidosis• Lofgren syndrome: lower
extremity periarthritis, E nodosum, hilar adenopathy
• Chronic arthritis
Crystals• Gout (rarely polyarticular)
Mechanical• Osteoarthritis
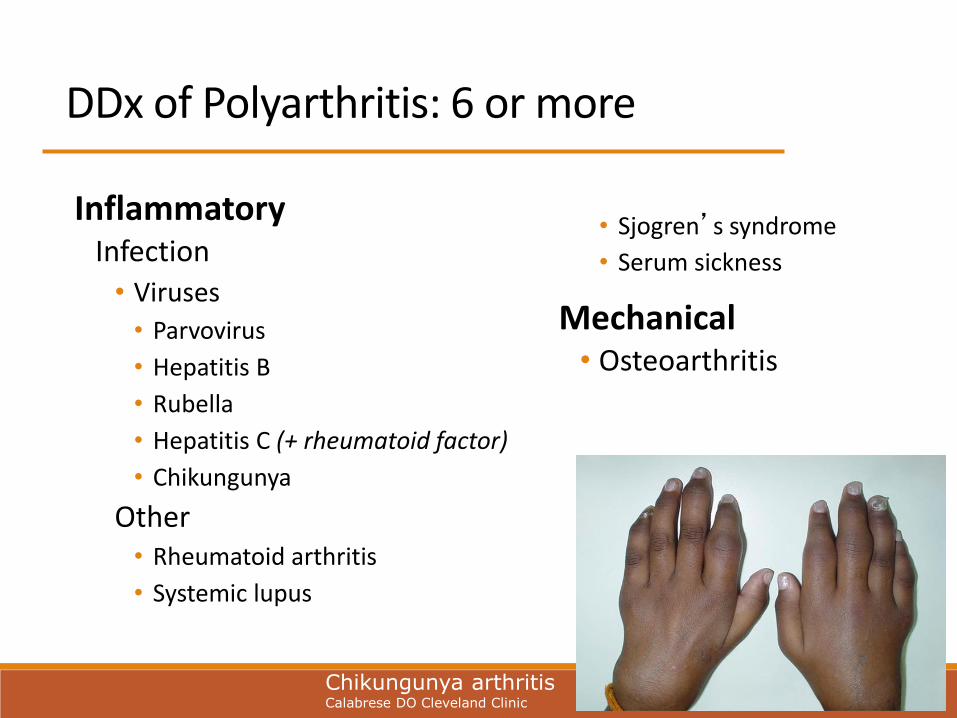
DDx of Polyarthritis: 6 or more
InflammatoryInfection
• Viruses
• Parvovirus
• Hepatitis B
• Rubella
• Hepatitis C (+ rheumatoid factor)
• Chikungunya
Other• Rheumatoid arthritis
• Systemic lupus
• Sjogren’s syndrome
• Serum sickness
Mechanical• Osteoarthritis
Chikungunya arthritisCalabrese DO Cleveland Clinic

DDx of a Very Painful Joint
Bugs• NG Bacterial arthritis
• Gonococcal arthritis
Blood• ACL tear
• Intra-articular fracture
• Meniscal tear
• Anticoagulant use
• Hemophilia
BBC Joint
Fat floating on blood = ?
Crystals• Gout
• Pseudogout
“Don’t touch my joint, don’t move my joint”

Common Musculoskeletal Issue that Show up on the Boards

Patient Presentation 1 Hx: A 55-year-old right-handed male complains of right shoulder pain for 1 month. Pain with reaching for his wallet & overhead activities. Has pain when sleeping on right side. Began after painting his house. No paresthesia nor radiation of pain.
Exam: Pain on active abduction between 60 and 120o. Pain on resisted right arm abduction with no obvious weakness on abduction, external or internal rotation. No atrophy of shoulder girdle musculature
The most likely cause of this
patient’s symptoms is:
A. Bicipital tendonitis
B. Acromioclavicular arthritis
C. Rotator cuff disease
D. Glenohumeral arthritis
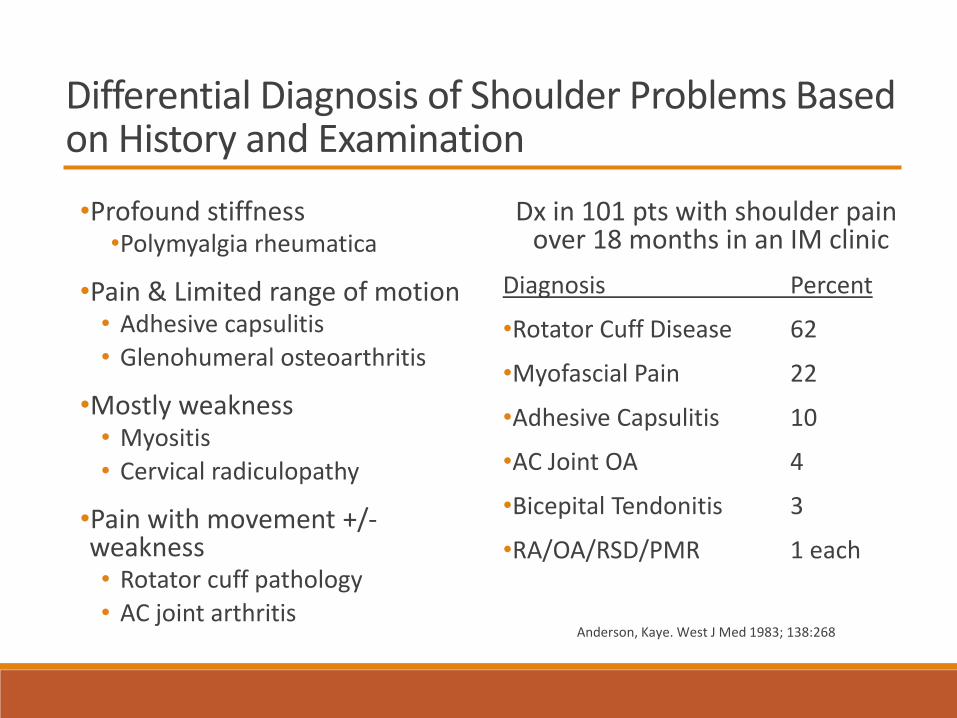
Differential Diagnosis of Shoulder Problems Based on History and Examination
•Profound stiffness •Polymyalgia rheumatica
•Pain & Limited range of motion• Adhesive capsulitis
• Glenohumeral osteoarthritis
•Mostly weakness• Myositis
• Cervical radiculopathy
•Pain with movement +/-weakness• Rotator cuff pathology
• AC joint arthritis
Dx in 101 pts with shoulder pain over 18 months in an IM clinic
Diagnosis Percent
•Rotator Cuff Disease 62
•Myofascial Pain 22
•Adhesive Capsulitis 10
•AC Joint OA 4
•Bicepital Tendonitis 3
•RA/OA/RSD/PMR 1 each
Anderson, Kaye. West J Med 1983; 138:268

Rotator Cuff DiseaseFunction of rotator cuff
• Stabilize GH joint
• Internal and external rotation, abduction
• Depress humeral head in glenoid to prevent impingement
Muscles
• Supraspinatus, Infraspinatus, Teres Minor, Infraspinatus
Risk factors for developing RTC disease• Age over 50 yrs (30% > 60yrs)
• Diabetes
• Work with frequent use of arms above 90o
Impingement zone
Leong HT, et al. J Rehabil Med. 2019 Oct 4;51(9):627-637.

Rotator Cuff Disease
Symptoms of rotator cuff disease• Painful arc of abduction 60-120o *
• Pain with lying on shoulder
• Pain with overhead activity
• RTC tear: weakness may be present with specific resisted motions• Supraspinatus given its position is most oft torn tendon
• “Drop test positive” for complete RTC tear
Continuum of disease• Tendonitis partial thickness tear full thickness cuff tear
arthropathy
Treatment• Physical therapy has most important long-term impact
• Subacromial injection is adjunctive to PT
• Surgical decompression open vs arthroscopic
Dang A, Davies M. Sports Med Arthrosc Rev. 2018 Sep;26(3):129-133.

Images: Rotator Cuff disease
High riding HH; Cuff Tear Arthropathy
High riding HH in RA
Ultrasound showing supraspinatus tear
Large shoulder effusion cuff tear arthropathy

Patient Presentation 2
72 y/o woman was working in yard, heard pop, arm looks like this. Has “Popeye” muscle
Most common underlying cause of this finding is:
A. Rotator cuff disease
B. Recent use of quinolone antibiotics
C. Underlying inflammatory arthritis
D. Corticosteroid use

Patient Presentation 3
Hx: 59-year-old male with 6 months of progressive pain with use of the right shoulder comes to clinic. He has difficulty washing his hair, reaching for his wallet, and these motions are painful.
Exam: there is decreased ROM of the shoulder with pain throughout the limited range. Mild muscle atrophy present about the shoulder. Feeling of creaking with ROM
Next step would be:
A. Shoulder CT scan
B. Shoulder MRI scan
C. Shoulder ultrasound
D. Shoulder x-ray 3 views

OA of Shoulder
Shoulder OsteoarthritisMajor risk factors
• Age > 50 yrs for primary OA
• Activity/trauma
• Inflammatory arthritis i.e. RA, PsA
• Metabolic arthritis ie hemochromatosis
• Advanced RTC tear ie cuff tear arthropathy
Symptoms and signs
• Diffuse shoulder pain
• Painful limited ROM is most plains
• Xrays (external/internal/axillary views) show osteophytes on inferior humeral head and inferior glenoid and joint space narrowing
Treatment• Pain management (acetaminophen, NSAIDs)
• PT/OT
• Total shoulder arthroplasty
Macías-Hernández SI, et al. Disabil Rehabil. 2017 Aug;39(16):1674-1682.
Gardner’s rule 35: anybody over age 50 with a stiff shoulder deserves an X-ray

Patient Presentation 4: Pain in wrist after fall on outstretched hand with snuff box tenderness
Greatest sequela for this injury is:
A. Scaphoid osteonecrosis C. Radial nerve injury
B. Arthritis of CMC joint D. Ulnar artery injury
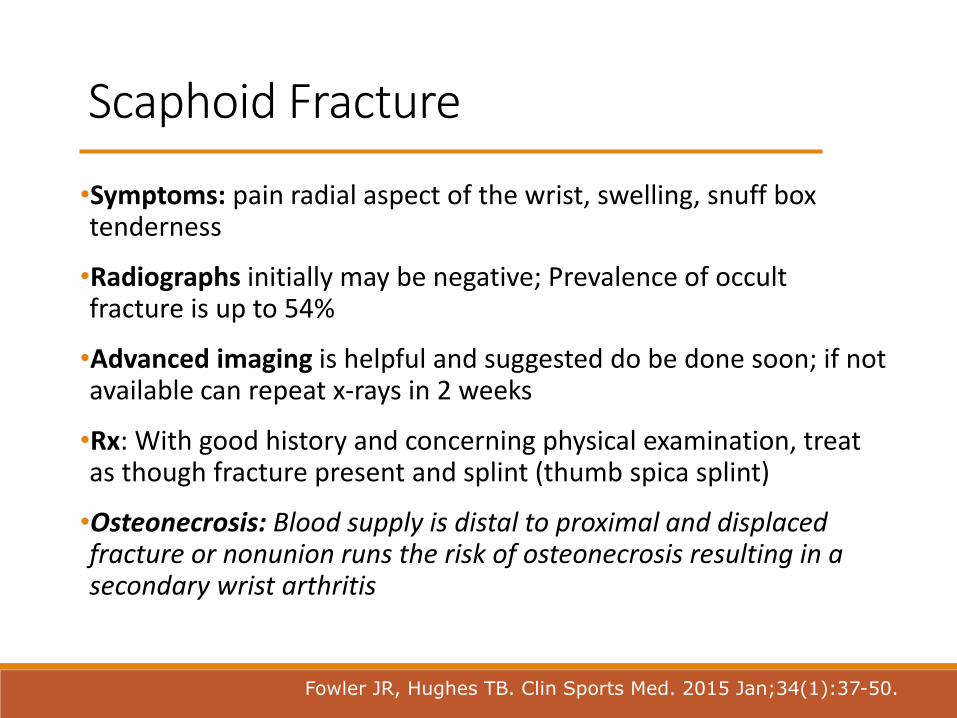
Scaphoid Fracture
•Symptoms: pain radial aspect of the wrist, swelling, snuff box tenderness
•Radiographs initially may be negative; Prevalence of occult fracture is up to 54%
•Advanced imaging is helpful and suggested do be done soon; if not available can repeat x-rays in 2 weeks
•Rx: With good history and concerning physical examination, treat as though fracture present and splint (thumb spica splint)
•Osteonecrosis: Blood supply is distal to proximal and displaced fracture or nonunion runs the risk of osteonecrosis resulting in a secondary wrist arthritis
Fowler JR, Hughes TB. Clin Sports Med. 2015 Jan;34(1):37-50.

Patient Presentation 5
A 55 y/o old woman complains of 1 week of pain in the base of her thumb. She has been trimming her roses prior to the onset of the discomfort. She has noted that there is some swelling along the distal radius and pain with ulnar deviation of the wrist
The most useful diagnostic test would be:A. EMG/NCS
B. X-ray of hand/wrist
C. Musculoskeletal ultrasound
D. Finkelstein test
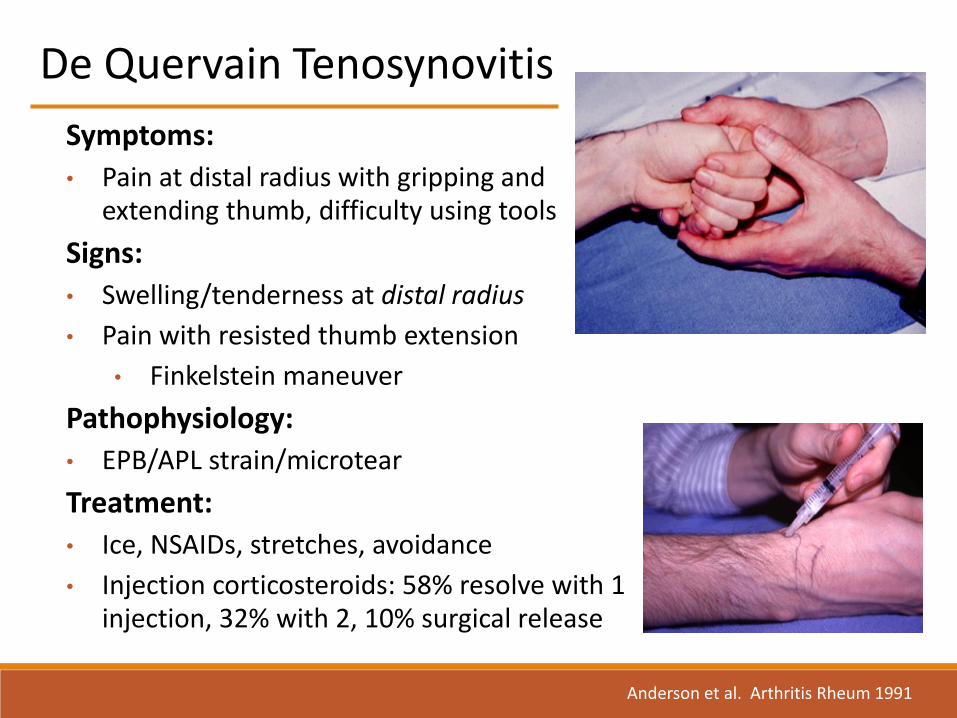
De Quervain Tenosynovitis
Symptoms:
• Pain at distal radius with gripping and extending thumb, difficulty using tools
Signs:
• Swelling/tenderness at distal radius
• Pain with resisted thumb extension
• Finkelstein maneuver
Pathophysiology:
• EPB/APL strain/microtear
Treatment:
• Ice, NSAIDs, stretches, avoidance
• Injection corticosteroids: 58% resolve with 1 injection, 32% with 2, 10% surgical release
Anderson et al. Arthritis Rheum 1991

Patient Presentation 6
Hx: 29 y/o woman recently post partum has tried to go back to exercise but finds her knees ache. Has trouble getting off the couch because of knee pain and going downstairs is also painful. Walking level ground is not a problem.
Exam: is unremarkable except for some patellofemoral crepitus with active ROM
Next step is:
A. Prednisone 10 mg/day
B. X-ray of knees including sunrise view
C. MRI scan of knees
D. Physical therapy
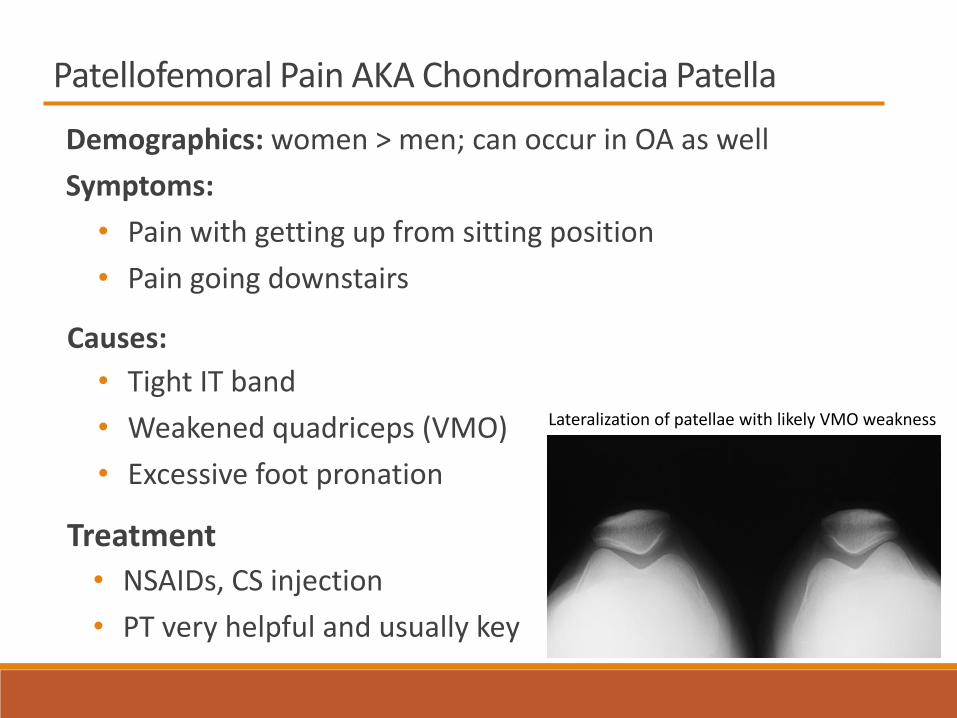
Patellofemoral Pain AKA Chondromalacia Patella
Demographics: women > men; can occur in OA as well
Symptoms:
• Pain with getting up from sitting position
• Pain going downstairs
Causes:
• Tight IT band
• Weakened quadriceps (VMO)
• Excessive foot pronation
Treatment
• NSAIDs, CS injection
• PT very helpful and usually key
Lateralization of patellae with likely VMO weakness

Patient Presentation 7: RA patient with calf swelling
Most likely cause of swelling is:A. Gastoc muscle rupture C. Venous thrombosisB. Baker cyst D. Calf hematoma

Baker’s Cyst
•Location: Bursa b/w gastrocnemius &
semimembranosus tendons
•Causes: Fluid from within knee pushed into
bursa behind the knee with walking
•Dx: Exam, Ultrasound, MRI
•Treatment: Address knee fluid!
Intra-articular injection, US guided aspiration
and injection, occasionally surgery
•Complication: posterior knee pain, venous
obstruction, rupture with calf pain and
fluid/blood tracking down leg
(pseudothrombophlebitis)
Herman AM, Marzo JM. Popliteal cysts: a current review. Orthopedics. 2014 Aug;37(8):e678-84.

Patient Presentation 8
HX: A 53 y/o woman complains of pain
and numbness b/w her right 3rd and
4th toes. Present especially with
wearing shoes. Feels best in bare feet.
Exam: shows no tenderness of MTP
joints, no callous formation but a click
is felt when palpating the 3rd and 4th
MTP interspace while transverse
loading the MTPs of the right foot
The next step is to:
A. MRI scan of foot
B. Wear wide toed shoes
C. Refer to podiatry
D. AP/oblique X-ray of
foot

Morton’s Neuroma
Location: Most common in 3rd/4th MTP interspace (aka interdigital neuroma)
Pathology: Perineural fibrosis of branches of plantar nerve
Symptoms & Signs:
• Burning pain and numbness into toes while wearing shoes especially narrow toed shoes
• Tenderness/nodule at interspace
• Mulder’s sign (click with transverse loading)
Dx: exam, US, MRI if needed
Rx: metatarsal bar/pad, wide toe box shoes, steroid injection from dorsal surface NOT plantar as may cause fat pad atrophy, surgery if needed
UpToDate
Researchgate
Valisena et al. Foot Ankle Surg 2018;4:271-281
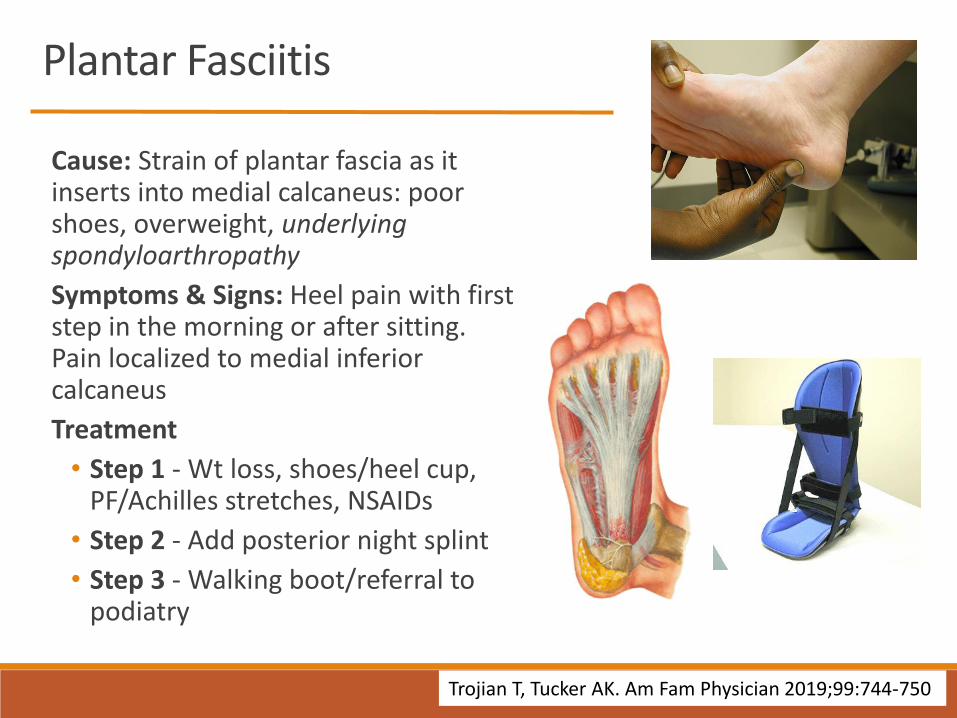
Plantar Fasciitis
Cause: Strain of plantar fascia as it inserts into medial calcaneus: poor shoes, overweight, underlying spondyloarthropathy
Symptoms & Signs: Heel pain with first step in the morning or after sitting. Pain localized to medial inferior calcaneus
Treatment
• Step 1 - Wt loss, shoes/heel cup, PF/Achilles stretches, NSAIDs
• Step 2 - Add posterior night splint
• Step 3 - Walking boot/referral to podiatry
Trojian T, Tucker AK. Am Fam Physician 2019;99:744-750
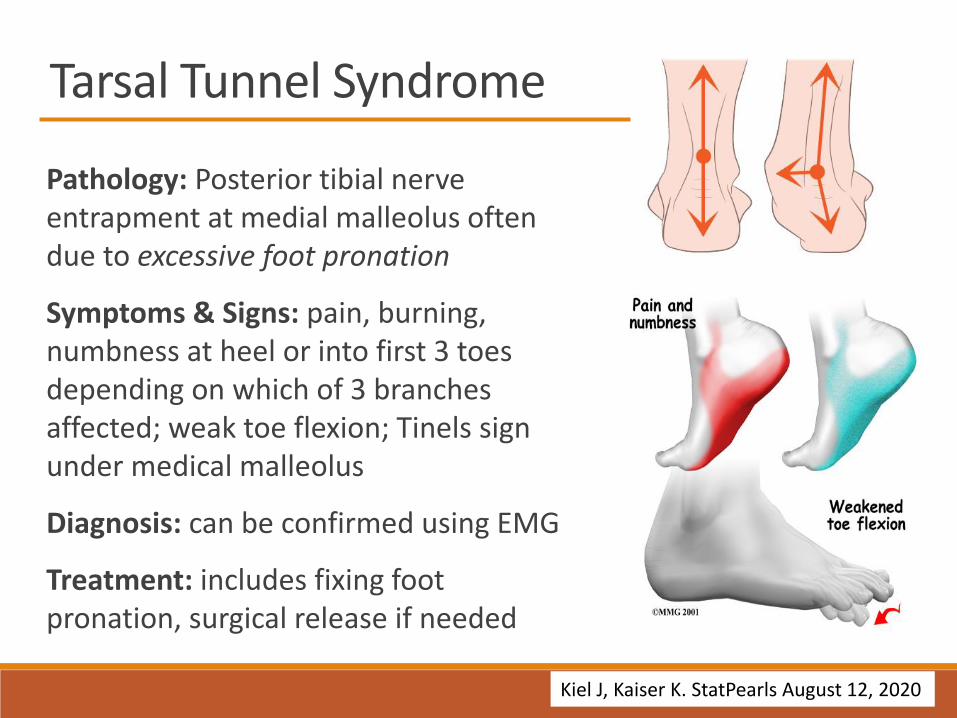
Tarsal Tunnel Syndrome
Pathology: Posterior tibial nerve entrapment at medial malleolus often due to excessive foot pronation
Symptoms & Signs: pain, burning, numbness at heel or into first 3 toes depending on which of 3 branches affected; weak toe flexion; Tinels sign under medical malleolus
Diagnosis: can be confirmed using EMG
Treatment: includes fixing foot pronation, surgical release if needed
Kiel J, Kaiser K. StatPearls August 12, 2020

Patient Presentation 9
A 65-year-old male noted pain in the left Achilles tendon 2 weeks after taking ciprofloxacin for sinusitis. A week after the pain began, he felt a sudden jolt of pain and has had a difficult time walking. He has a history of PMR and has been on prednisone at 5 mg day and tapering slowly.
The most useful next step to look for Achilles’ tendon rupture is:
A. Thompson’s Test
B. Ultrasound examination of the tendon
C. MRI examination of the tendon
D. Gardner’s maneuver

Achilles Tendonitis
DDx:
• Insertional pain think spondyloarthropathy, mid tendon pain think trauma/overuse
• Quinolone Abx tendonopathy most often affects Achilles, rupture in 30% of cases
• Gout and hyperlipidemias can also affect tendon (picture is tendon xanthoma)
Dx: exam, US, MRI; complete tear of tendon may be Dxed by preforming Thompson’s test; squeeze calf and foot should plantar flex if tendon is intact
Rx: Rest, NSAIDs, immobilization, PT, surgery
Maffulli N, et a. Foot Ankle Surg 2020
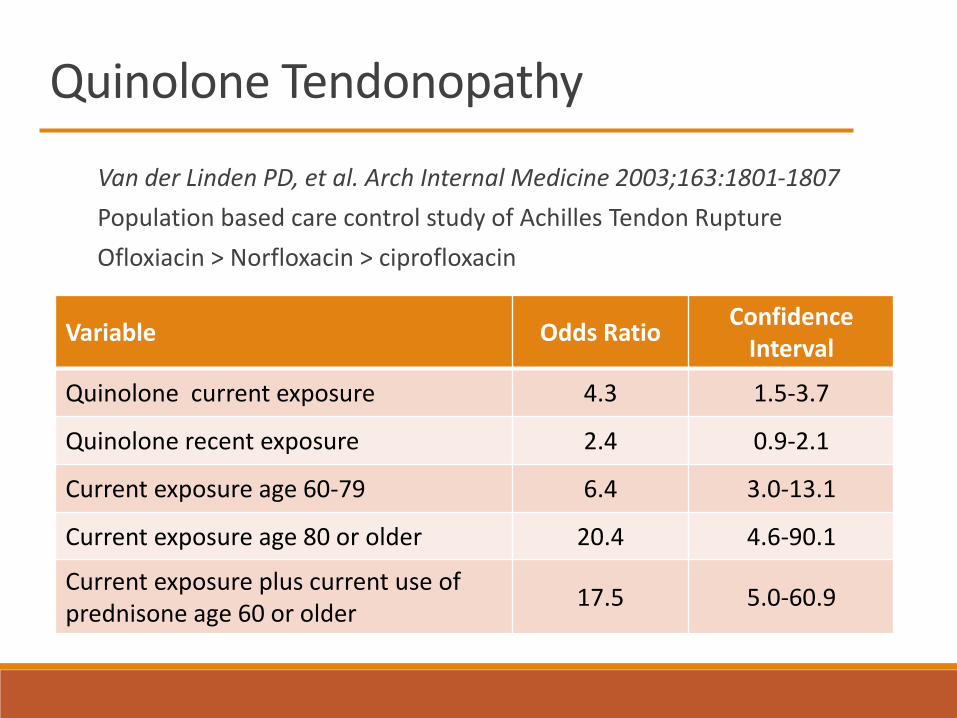
Quinolone Tendonopathy
Van der Linden PD, et al. Arch Internal Medicine 2003;163:1801-1807
Population based care control study of Achilles Tendon Rupture
Ofloxiacin > Norfloxacin > ciprofloxacin
Variable Odds RatioConfidence
Interval
Quinolone current exposure 4.3 1.5-3.7
Quinolone recent exposure 2.4 0.9-2.1
Current exposure age 60-79 6.4 3.0-13.1
Current exposure age 80 or older 20.4 4.6-90.1
Current exposure plus current use of prednisone age 60 or older
17.5 5.0-60.9

Arthritis and More Arthritis

Rheumatoid Arthritis
Inflammatory polyarthritis
Women > men
AM stiffness > 30 minutes
Laboratory tests◦ ESR/CRP◦ Rheumatoid factor◦ CCP
Radiographic changes◦ Marginal erosions◦ Subluxation◦ Deviation◦ Osteopenia
Joint distribution…..

Earliest RA

Advancing RA
Note MCP prominence

Advanced RA
Note ulnar deviation
and MCP subluxation
As well as cock up
deformities of toes

1896 1901
The Natural History of RA as Modeled by Pierre Auguste Renoir
The arthritis progresses
1903 1911
Autoantibodies in Rheumatoid Arthritis:Rheumatoid Factor and Cyclic Citrullinated Peptide
Pathophysiology• RF is an antibody directed against the patients own IgG
• CCP is directed against citrullinate peptides that form as a result of inflammation
Sensitivity/specificity
• RF sensitivity 75% and specificity of 50%; RF seen in other diseases
• Hepatitis B&C, TB, fungal infections, Sjogren’s syndrome, mixed connective tissue disease, Waldenstrom’s macroglobulinemia, etc
• CCP sensitivity 75% but specificity of 96%
Other
• RF higher level = worse prognosis
• CCP may be present for up to 14 year before arthritis appears; higher the level = worse the prognosis
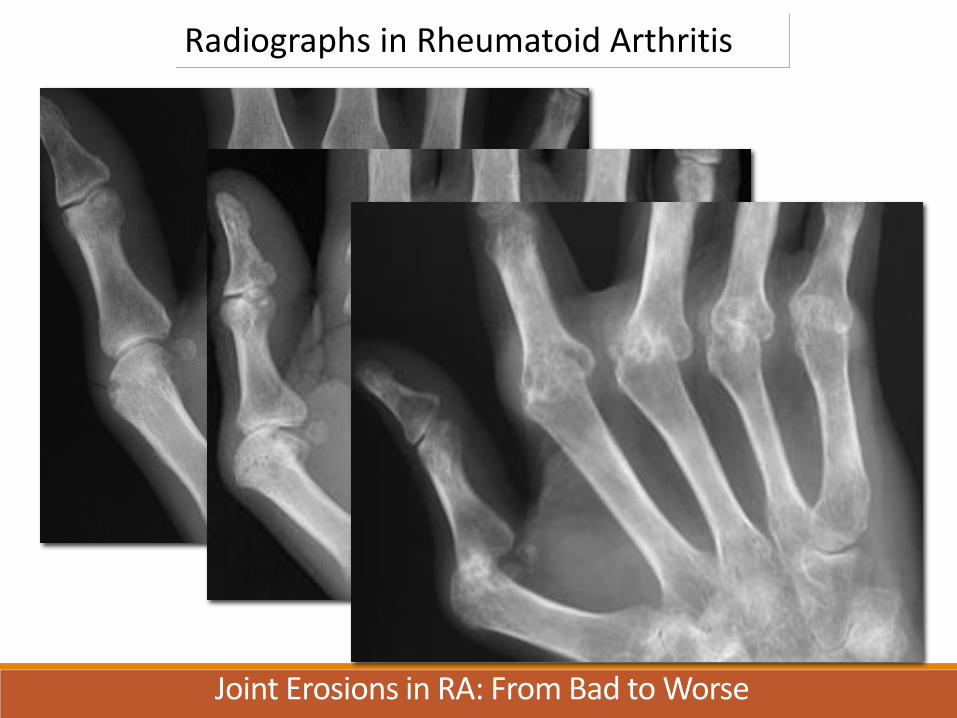
Radiographs in Rheumatoid Arthritis
Joint Erosions in RA: From Bad to Worse
“What we need in RA is a drug for which one does not need a statistician to see
the beneficial effects”
Irving Kushner, M.D.
J Rheumatol 1989;16:1-4
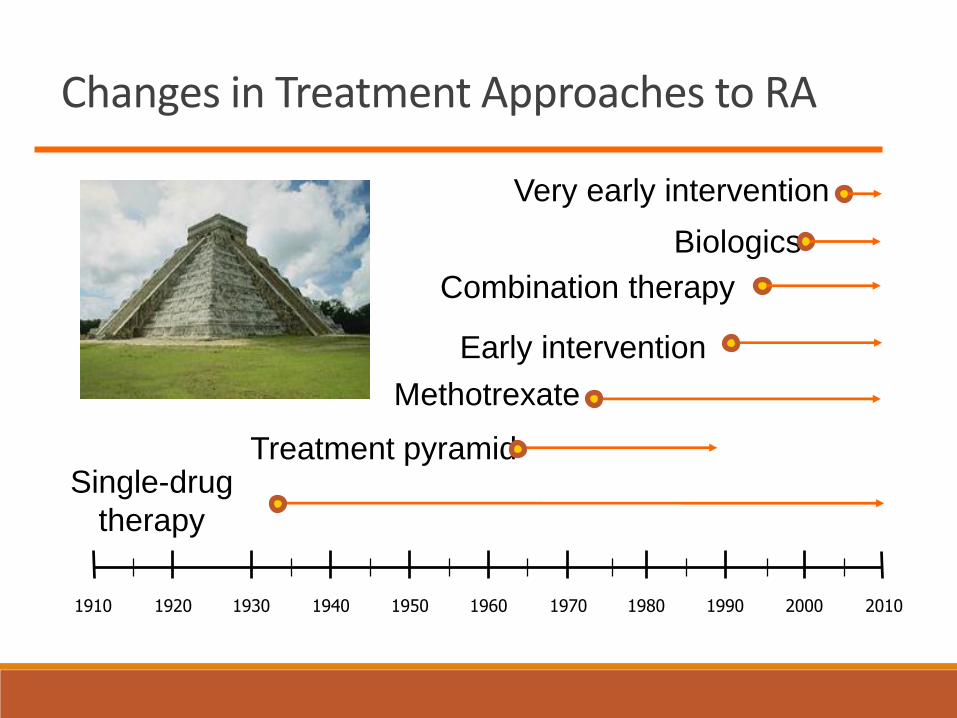
Changes in Treatment Approaches to RA
1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
Early intervention
Combination therapy
Single-drug
therapy
Treatment pyramid
Biologics
Methotrexate
Very early intervention
Treatment Principles of RA 2021
•Early recognition, early therapy, treat to target
•Aggressive Rx for patients with concerning features• Erosions at presentation
• Extra-articular features ie nodules
• Large number of joints involved
•Methotrexate is anchor medication
•Routine measure of disease activity with modification of therapy to achieve low disease activity or remission
Therapies For RA 2021
Conventional DMARDs
• Methotrexate
• Hydroxychloroquine
• Leflunomide
• Sulfasalazine
Anti-TNF agents
• Etanercept
• Adalimumab
• Infliximab
• Certozilumab
• Golimumab
Anti-B cell agents
• Rituximab
Anti-T cell agents• Abatacept
Anti-IL6 receptor antagonists• Tocilizumab
• Sarilimumab
JAK inhibitors• Tofacitinib
• Barcitinib
• Upacitinib
IL-1 receptor antagonists• Anakinra
Patient Presentation 10
Hx: 34-year-old-woman with 6-year history of RA comes to urgent care due to painful oral ulcers, nausea, and vomiting. Began with nausea and vomiting x 7 days and has had a hard time keeping hydrated. 2 day ago, had onset of painful oral ulcers. Several family members with GI illness. Continued taking medications for RA that consists of methotrexate 20 mg sc weekly.
Exam: BP 90/60, HR 110, temp 37.9 c. Looks ill. Has multiple oral ulcers on buccal mucosa and tongue. No joint swelling or deformities noted
Labs WBC 1.9k, HCT 35% platelet 229k, creatinine 1.7. BUN 65
Next step after hydration is:
A. Start dialysis
B. Give IV folinic acid
C. Administer activated charcoal
D. Start filgrastim
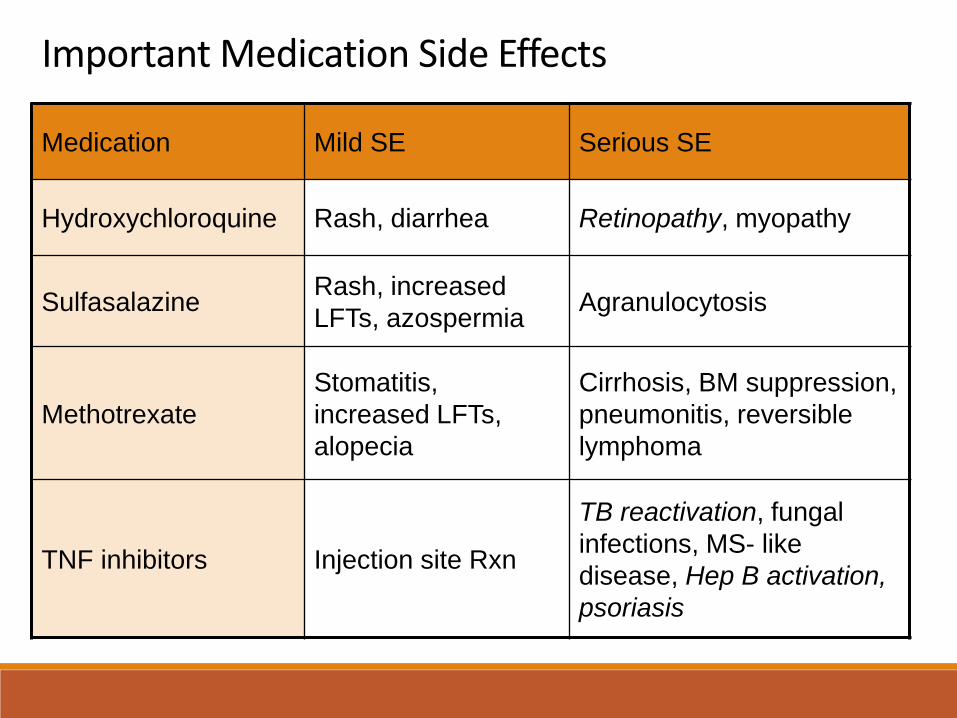
Important Medication Side Effects
Medication Mild SE Serious SE
Hydroxychloroquine Rash, diarrhea Retinopathy, myopathy
SulfasalazineRash, increased
LFTs, azospermiaAgranulocytosis
Methotrexate
Stomatitis,
increased LFTs,
alopecia
Cirrhosis, BM suppression,
pneumonitis, reversible
lymphoma
TNF inhibitors Injection site Rxn
TB reactivation, fungal
infections, MS- like
disease, Hep B activation,
psoriasis

Patient Presentation 11
A 55 y/o male with 15 years of RA comes to clinic for DOE. Noted DOE with stairs about 6 months ago. Now having DOE with walking more than 1/4 mile. No PND, orthopnea, LE edema, wheezing. Does have a persistent non-productive cough though.
Most useful next test would be
A. High resolution CT scan of chest
B. Echocardiogram
C. Right heart catherization
D. Ventilation/perfusion scan of lungs

Rheumatoid Arthritis:Extra-Articular Disease
Scleritis/Scleromalacia
Nodules
Rheumatoid ILD

Rheumatoid ILD
Epidemiology • 5-10% of RA patients
• Male > female
• Age 50-60
• 4.9 yrs of disease
• High titer RF/CCP
HRCT patterns• Usual interstitial pneumonitis
• Non-specific interstitial pneumonitis
• Organizing pneumonia
• Lymphocytic interstitial pneumonitis
Treatment• Steroids
• Mycophenolate/Azathioprine
• Rituximab
• Antifibrotics
Outcome• Second only to cardiac as cause
of mortality in RA
• ILD associated pulmonary HTN may also contribute to mortality
• UIP pattern has highest mortality

Important complication of RA
Felty’s syndrome• Leukopenia, splenomegaly, RA, Infections, leg
ulcers
C1-C2 subluxation• Neck pain, myelopathy, C spine flexion/extension
views, MRI
Septic arthritis• Large joints, fewer systemic symptoms, Staph >
Strep > gram negatives
Tendon ruptures• Especially ring/little finger extensor tendons
Rheumatoid Vasculitis (PAN like)• Male, foot drop, wrist drop, skin ulcers, GI

Patient Presentation 12
A 55 y/o male with arthritis has
this x-ray. The term used to
describe this finding is :
A. Opera glass deformity
B. Pencil point deformity
C. Pencil in a cup deformity
D. Shark tooth deformity

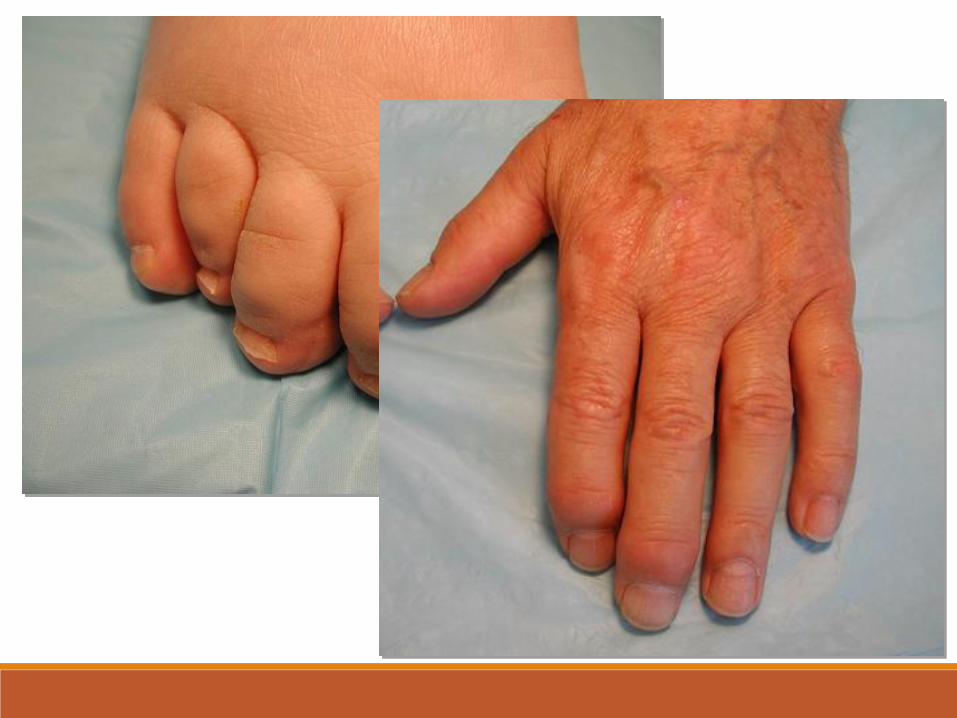
Psoriatic Arthritis
•Men = women
•7-20% of psoriasis pts develop PsA
•Types of disease• Pauciarthritis
• Polyarthritis
• DIP invovement
• Arthritis mutilans
• Spondylitis
•Enthesopathy
•Joint distribution…
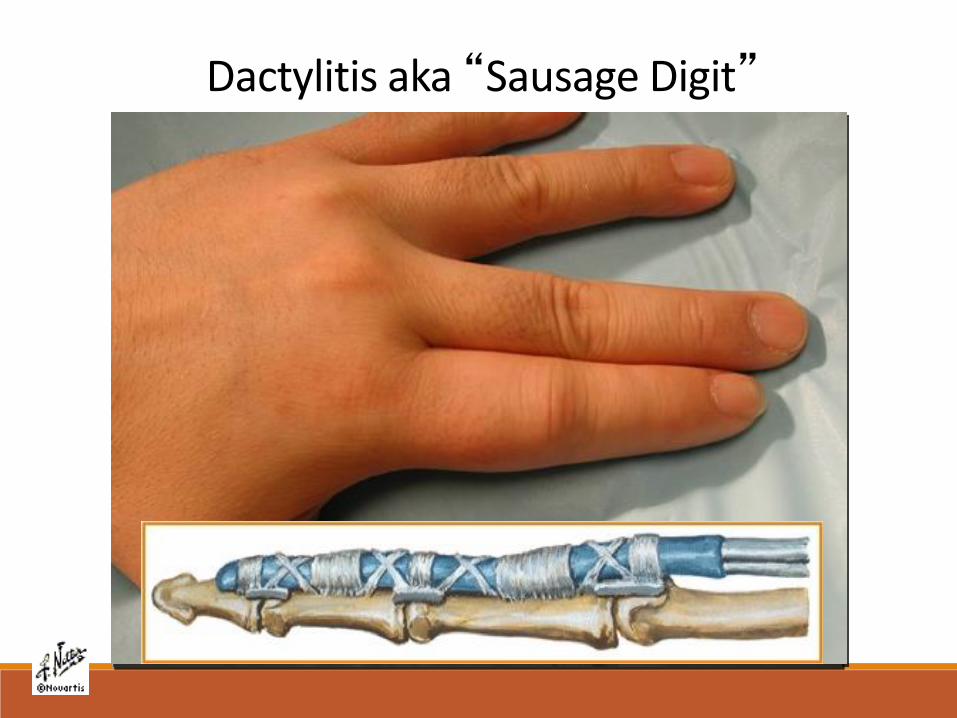
Diagnosis By Pattern RecognitionDactylitis aka “Sausage Digit”


Psoriatic Arthritis:Radiographic features
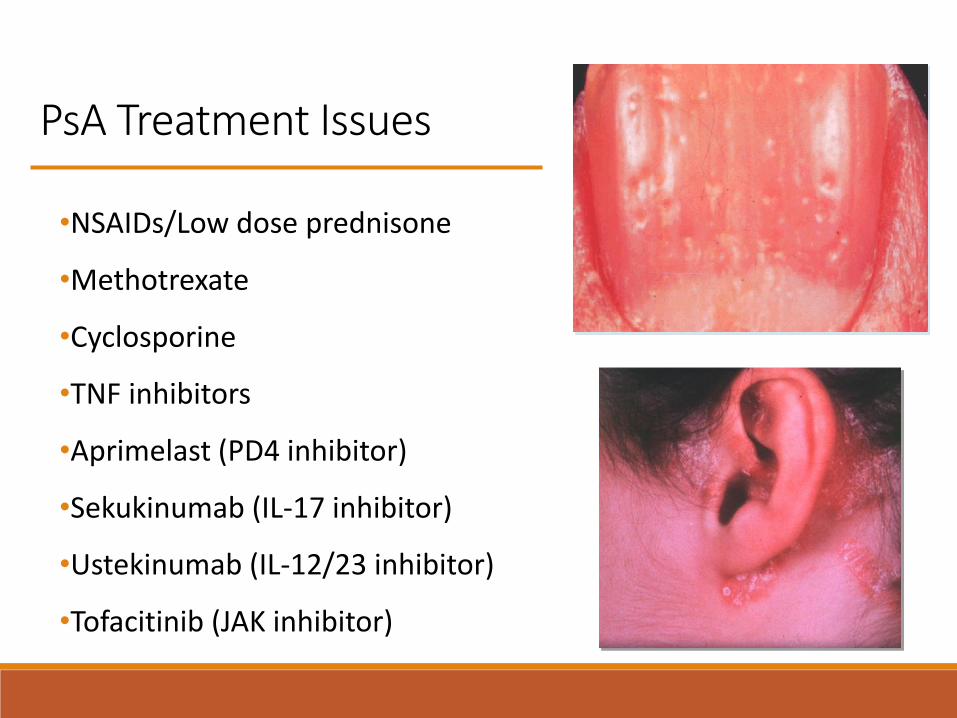
PsA Treatment Issues
•NSAIDs/Low dose prednisone
•Methotrexate
•Cyclosporine
•TNF inhibitors
•Aprimelast (PD4 inhibitor)
•Sekukinumab (IL-17 inhibitor)
•Ustekinumab (IL-12/23 inhibitor)
•Tofacitinib (JAK inhibitor)

Patient Presentation 13
A 25 years old male
with recent GI illness
after a trip to Mexico
comes to clinic with
eye pain and
redness, joint pain,
and a rash on his
hands and feet.
Rash as noted.
Name of this rash is:
A. Palmar plantar pustulosis
B. Punctate psoriasis
C. Keretodermablennorrhagicum
D. Glomus of the fromus

Reactive Arthritis AKA Reiter’s Syndrome
•Pauci to polyarthritis
•Men > women
•AM stiffness > 30 minutes
•Mucocutaneous involvement
•Enthesitis prominent
•Follows infectious illness
usually GU or GI
•Joint distribution…..
Infectious Agent Associated with ReA in HLA-B27 + Individuals
•Chlamydia trachomatis
•Shigella flexneri
•Salmonella species
•Yersinia species
•Clostridium difficle
•Campylobacter fetus jejuni
•Chlamydia pneumoniae
•Intravesical injection of BCG to treat bladder CA
Salmonella 1.4 millioncases/year 2% complicated
by chronic arthritisCDC website
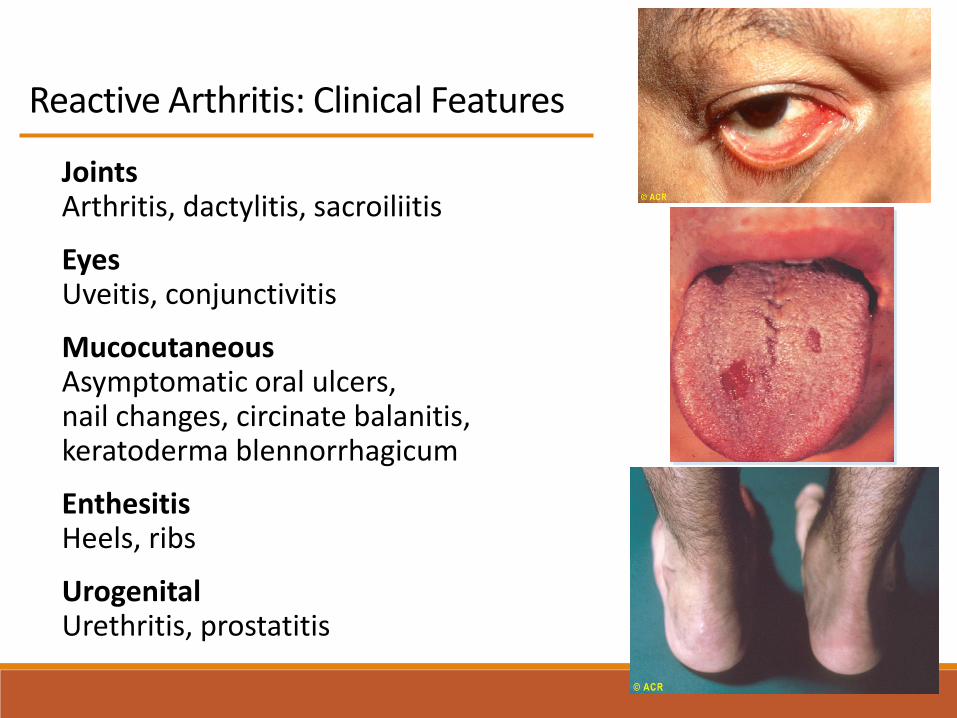
Reactive Arthritis: Clinical Features
JointsArthritis, dactylitis, sacroiliitis
EyesUveitis, conjunctivitis
Mucocutaneous Asymptomatic oral ulcers, nail changes, circinate balanitis, keratoderma blennorrhagicum
EnthesitisHeels, ribs
UrogenitalUrethritis, prostatitis

Tenosynovitis
Reactive arthritis
Synovitis

Keretoderma blennorrhagicum
Keratoderma and balanitis
Reactive arthritis

Reactive Arthritis - Outcome
•75% have waxing and waning course. Attacks last 6 weeks to 6 months
•25% have persistent disease
•Has been linked to HIV infection
•Morbidity includes:• Aortitis
• Cardiac conduction abnormalities
• Erosive arthritis (often the feet)
• Vision damaging uveitis
•Treatment similar to PsANail changes

Patient Presentation 14
Hx: A 22 y/o male complains of 3 weeks of low back pain
especially at night and early AM. Feels better during the day
especially when he is active.
Exam: VVS Afebrile. General exam is normal. Positive
Patrick maneuver on both sides. Schoeber test is normal.
Hyperextension of the lumbar spine causes pain
Labs: HCT 34%, ESR 45 mm/hr
Xrays: AP pelvis shows erosion at the SI joints
Patient Presentation 14
The next step should be:
A. Start NSAID therapy
B. Check HLA B27 test
C. CT scan of SI joints
D. Order MRI scan of SI joints

DDx of Inflammatory Low Back Pain
Spondylitis• Ankylosing spondylitis
• Psoriatic spondylitis
• Reactive arthritis
• Inflammatory bowel disease
Infection• Bacterial
• TB
Tumor
P prostate
B breast
K kidney
T thyroid
L liver
M multiple myeloma
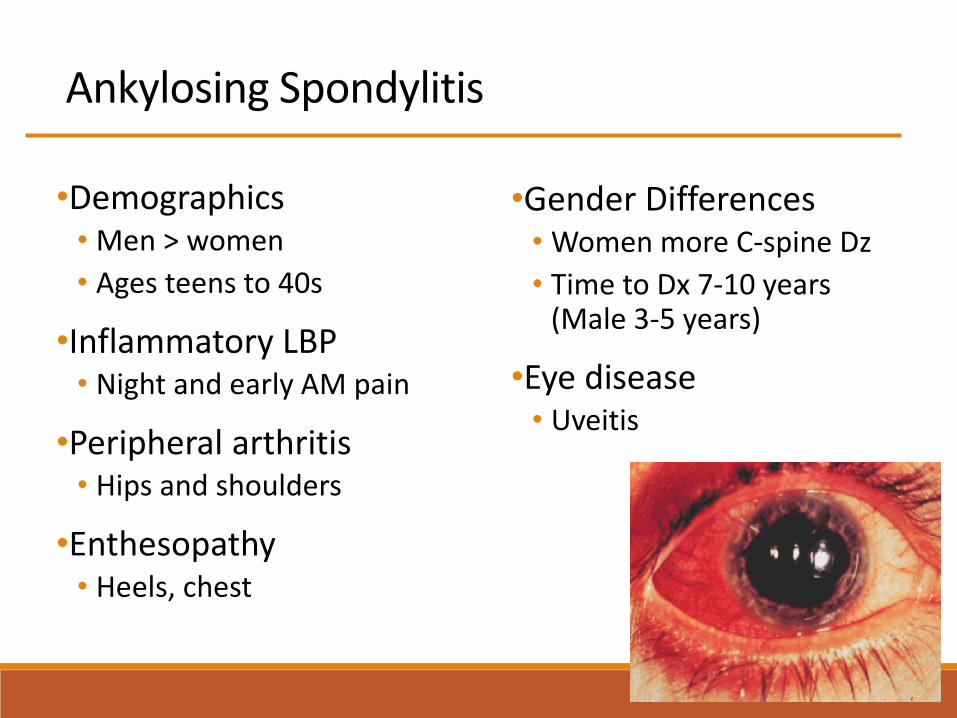
Ankylosing Spondylitis
•Demographics• Men > women
• Ages teens to 40s
•Inflammatory LBP• Night and early AM pain
•Peripheral arthritis• Hips and shoulders
•Enthesopathy• Heels, chest
•Gender Differences• Women more C-spine Dz
• Time to Dx 7-10 years(Male 3-5 years)
•Eye disease• Uveitis
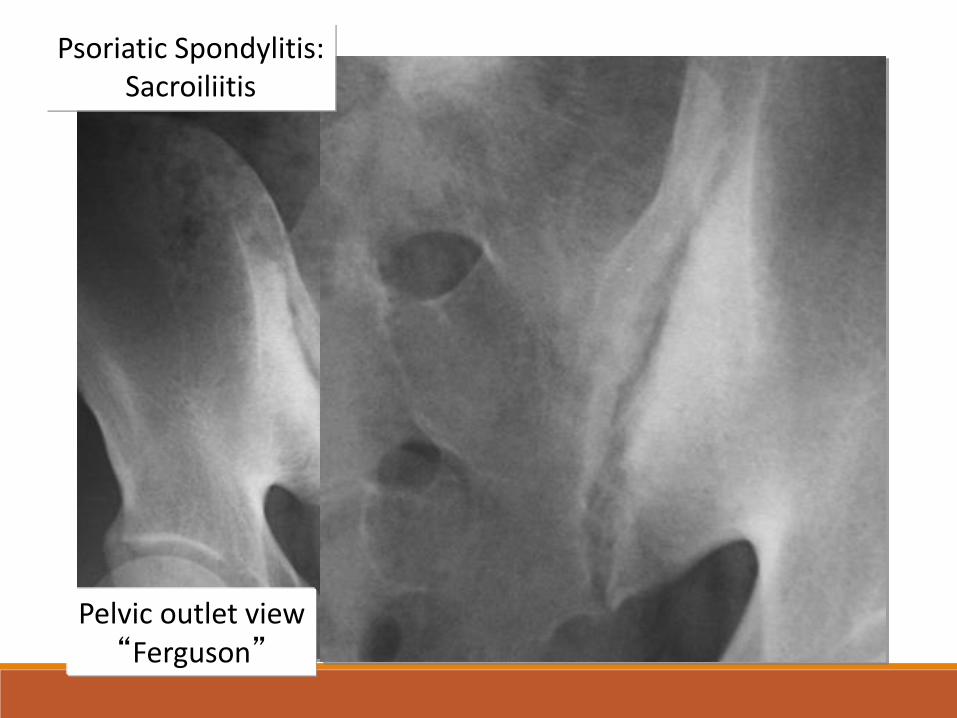
Psoriatic Spondylitis:Sacroiliitis
Pelvic outlet view“Ferguson”
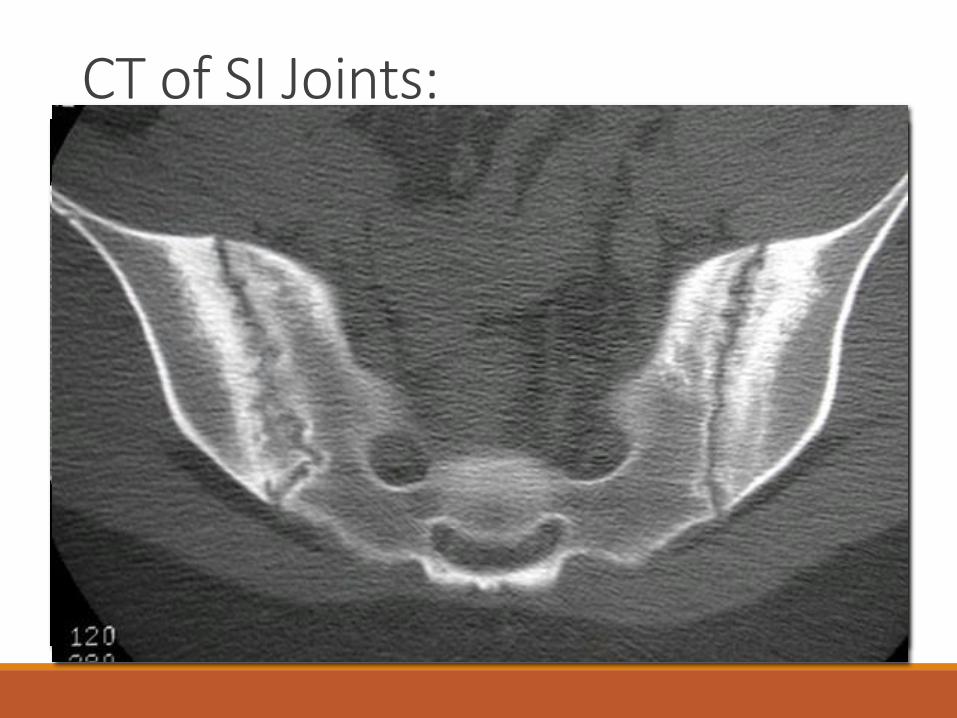
CT of SI Joints:
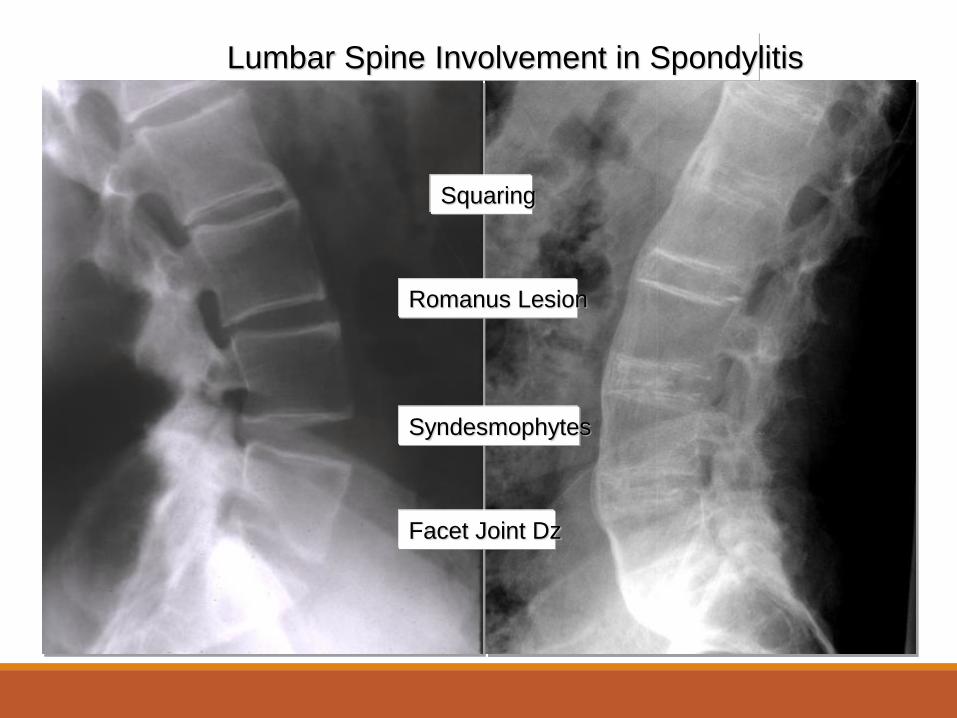
Romanus Lesion
Squaring
Syndesmophytes
Facet Joint Dz
Lumbar Spine Involvement in Spondylitis


AS: Important Complications/Outcome
•Vertebral disc space Fx follows mild trauma at C5-C7
•Bilateral upper lobe pulmonary fibrosis
•Restrictive pulmonary Dz due to rib cage immobility
•Vision threatening uveitis
•Cauda equina syndrome• Saddle anesthesia
• LE weakness
• Bowel/bladder incontinence
•Amyloidosis
•Aortic valve incompetence
•Mortality increase after 20 yrs of disease

Patient Presentation 15
Hx: 48 y/o male, Mike Testaronie, former WWF wrestler,
complains of bilateral hand pain. Minimal morning
stiffness but has pain with activity especially driving his
muscle boat on Lake Washington. The MCPs in
particular are painful. Has been on methotrexate for Dx
of RA without benefit
Exam: Tenderness & swelling of 2nd, 3rd, and 4th MCP
joints both hands. X-ray of right hand as shown

Patient Presentation 15
The next step would be:
A. Start NSAIDs and reassure
B. Check CCP antibody
C. Start low dose prednisone
D. Check ferritin level

Osteoarthritis
•Senior age group
•Mechanical pain/deformity
•Primary v secondary OA
Spine
Hands
Hips
Knees
1st MTP
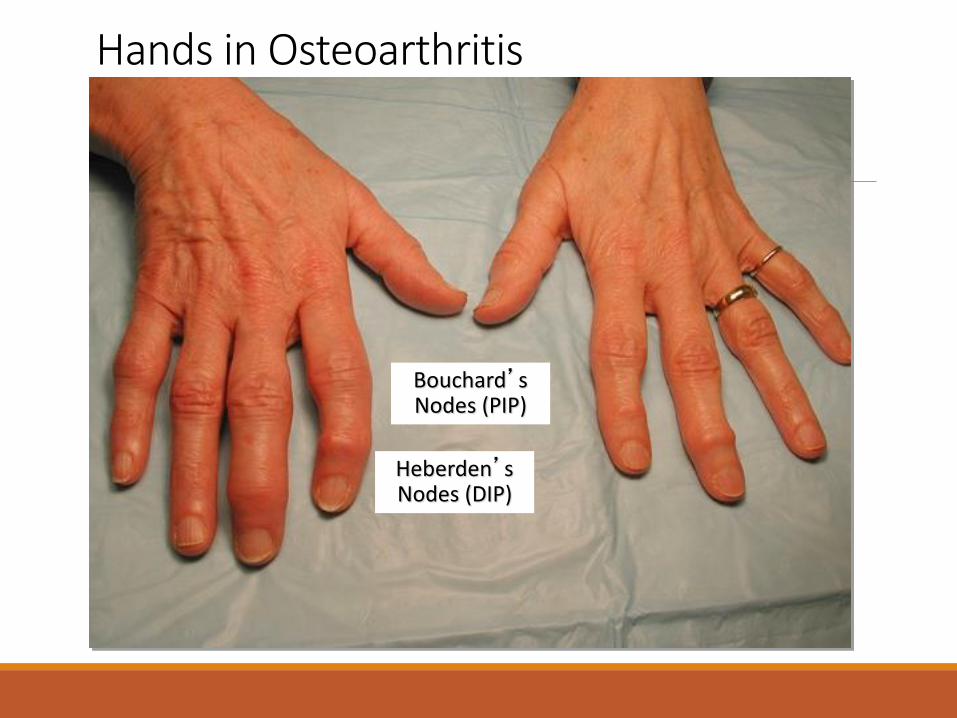
Heberden’sNodes (DIP)
Bouchard’sNodes (PIP)
Hands in Osteoarthritis

Hand in Osteoarthritis

X-Ray Changes in OA

Summary of Suggested Rx in OA of the Hand, Knee, and Hip2019 American College of Rheumatology/Arthritis Foundation Guidelines
Non-pharmacologic therapy• Hand: CMC brace
• Hip and knee:
• Weight loss
• Exercise
• Tai chi/yoga
• Cane
• Tibiofemoral brace
• Not recommended: TENS
Pharmacologic therapy• Hand
• Oral NSAID
• Topical NSAID conditionally recommended
• Knee
• Topical NSAID
• Oral NSAID
• Glucocorticoid injection
• Hip
• Oral NSAID
• US guided corticosteroid injection
• Not recommended: glucosamine, chondroitin, bisphosphonates, stem cell injections

Osteoarthritis
PsoriaticArthritis
Gout
DDx of DIP
arthritis
Pearl: Major Causes of DIP Arthritis
Rash and Arthritis
Patient Presentation 16
Hx: 30 y/o woman complains of 3 weeks of fever to 1010, sore throat, lumps in her neck, joint pain in hands, wrists, and knees, and an intermittent rash on chest and extremities. Works as an elementary school teacher.
Exam: Temp 100.80, pulse 100, mild MP rash on chest, arms and legs, enlarged cervical lymph nodes bilaterally, swelling of wrists, and knees.
Initial labs: WBC 25,000, HCT 34%, ALT and AST 1.5 times normal and CRP 200 mg/l (0-10 normal)
The most useful next test
would be:
A. Serum ferritin
B. ANA panel
C. Hepatitis B studies
D. Parvovirus IgM/IgG
Rash and Arthritis: the Viruses
• Parvovirus - net-like rash, polyarthralgia/itis, self-limited
• Rubella - rash, polyarthralgias, post-wild type and
immunization
• Hepatitis B - prodrome rash and polyarthralgias/it;
precedes hepatitis and resolves when hepatitis develops
• Hepatitis C - chronic polyarthralgias/itis, palpable
purpura of cryoglobulinemia, 50-70% of Hepatitis C
infected patients are rheumatoid factor positive
• Chikungunya - arthritis, fever, rash intense myalgias
Rash and Arthritis: Other Stuff
•Lyme disease - Erythema migrans, Bell’s palsy, heart block, polyarthritis; late knee oligoarthritis
•Gonococcal - Pauciarthritis to monoarthritis, fever, pustular dermatitis
•Stills Disease – Yamaguchi criteria: Major: Fever > 39, rash, arthralgias/arthritis, leukocytosis. Minor: lymphadenopathy, hepatosplenomegaly, sore throat, LFTs. Hyperferritinemia
•Serum sickness - fever, rash, and arthritis with exposure to drug (Abx, antithymocyte globulin, chimeric antibodies)
•Systemic Lupus - TBD

ACR, Mayo Clinic, UpToDate
Erythema Migrans
Parvo in Child
Parvo on trunk
Dermatitis in GC
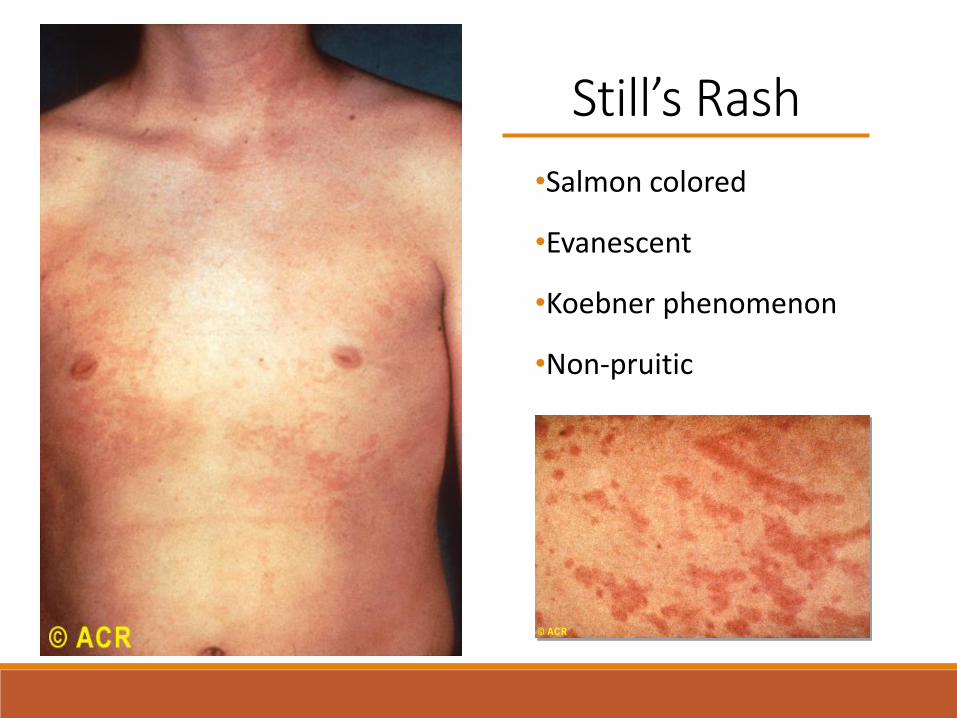
Still’s Rash
•Salmon colored
•Evanescent
•Koebner phenomenon
•Non-pruitic

Crystalline Arthritis

Patient Presentation 17
Hx: A 60 y/o male has 1 days of severe pain in right knee. 3 days post-op for CABG. Unable to bend knee
Exam: mildly obese male in mild distress. Right knee is held in 350
of flexion and resists attempts to flex and extend the knee. Moderate effusion present. Knee is warm to palpation.
Xray: of knee as noted

Patient Presentation 17
The next step is to:
A. Start naproxen 500 mg BID
B. Inject knee with 40 mg of triamcinolone
C. Aspirate knee and send for culture/crystal analysis
D. Order MRI scan of the knee

CPPD images
DIEPPE P , SWAN A. Ann Rheum Dis 1999;58:261-263

CPPD Disease
•Calcium Pyrophosphate Arthritis
• AKA pseudogout
• Rare in young adults
• Predilection for wrist and knee
• Crystals positively birefringent, squares,
rhomboids, rectangles
•Treatment is similar to gout acutely
• NSAID, steroids, colchicine
• Evaluate for underlying metabolic disease, use NSAID or
colchicine for prophylaxis
Causes of
chondrocalcinosis
A acromegaly
H hemochromatosis
O orchronosis
T thyroid disease
T trauma
I idiopathic
P parathyroid disease
Rosenthal AK, Ryan LM. N Engl J Med. 2016 Jun 30;374(26):2575-84

Patient Presentation 18
HPI - Patient is a 55 y/o male with a Hx of mild HTN who comes to your clinic with 2 days of severe pain in his left 1st toe and medial ankle. He is unable to walk on it without severe pain and even the sheet on it is uncomfortable. Had a similar yet milder attack 1 year ago.
Meds - HCTZ 25 mg/day
Habits - 6-12 beers/week
Exam - Wt 200 lbs, Ht 5’6,” B/P 140/90, severe redness and tenderness to the medial left ankle and left 1st MTP.
Labs - Normal CBC/chem panel, uric acid 6.9 mg/dlaspiration of 1st MTP reveals (see next slide)

Patient Presentation
Needle shaped MSU crystals
Direction of first order red compensator

Patient Presentation 18
The next best step is to:
A. Provide alcohol counselling
B. Start oral prednisone 35 mg a day for 7 days
C. Stop HCTZ and start losartan
D. Begin allopurinol 100 mg po qd
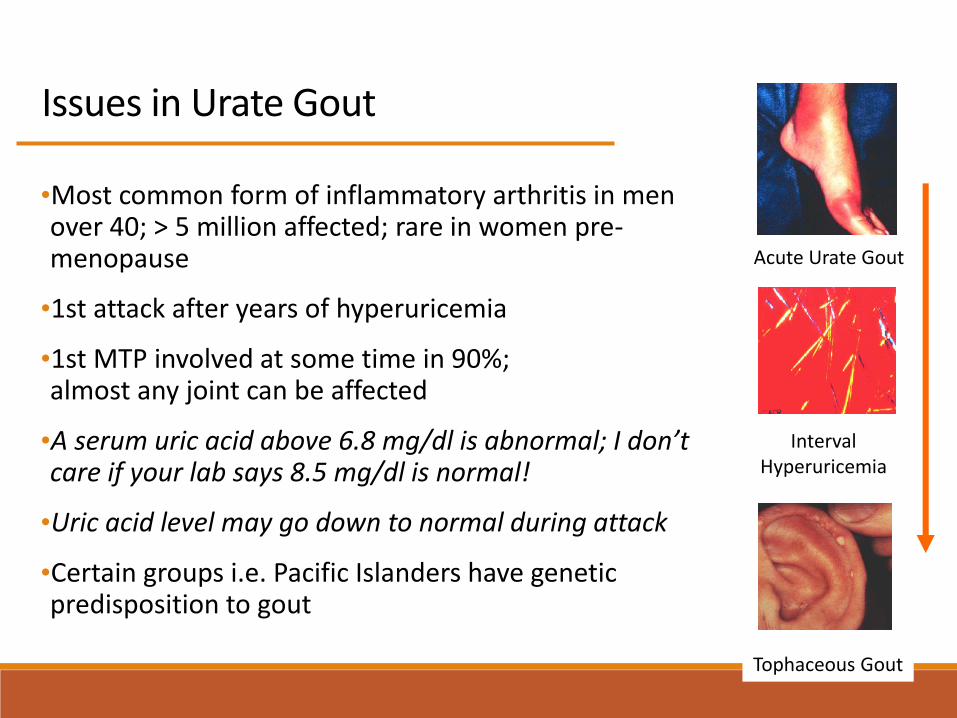
Issues in Urate Gout
•Most common form of inflammatory arthritis in men over 40; > 5 million affected; rare in women pre-menopause
•1st attack after years of hyperuricemia
•1st MTP involved at some time in 90%;almost any joint can be affected
•A serum uric acid above 6.8 mg/dl is abnormal; I don’t care if your lab says 8.5 mg/dl is normal!
•Uric acid level may go down to normal during attack
•Certain groups i.e. Pacific Islanders have genetic predisposition to gout
Acute Urate Gout
IntervalHyperuricemia
Tophaceous Gout
Step 1: Options for Treatment of Acute Gout
•NSAIDS: Maximum dose for 5-7 days; Naproxen 500 mg BID x 5 days
•Oral Prednisone/Prednisolone: 35 mg/day for 5-7 days or 40 mg with 7-10 day taper
•Intramuscular Corticosteroids: Depomedrol 120 mg or triamcinalone 60 mg IM are options
•Intra-articular steroids
•Colchicine: 1.2 mg followed in one hour by 0.6 mg. Start within first 24 hours
•Anakinra IL-1 inhibitor: not FDA approved. 100 mg SC daily time 1-3 days

Step 2: Modify Risk Factors
•Avoid medications that raise uric acid level
• Minimize ETOH especially beer/ale
• Encourage slow wt loss
• Rapid weight loss may precipitate gouty attack
• Obesity affects uric acid production and clearnace
• Discuss a low purine diet and one low on fructose
Medications that raise SUA• Diuretics
• Niacin
• Calcineurin inhibitors
• Laxatives in excess
• Low dose ASA
Medications that lower SUA• Losartan

Step 3: Decisions Regarding Hypouricemic Therapy
•Reasons to consider hypouricemic therapy• > 2 attacks/year, tophi, kidney stones, chronic persistent gout
•Hypouricemic agents• Allopurinol - 100-800 mg/d; rash, hypersensitivity syndrome;
reduce dose of azathioprine to 1/4
• Febuxistat - 40-80 mg/d; liver toxicity, azathioprine issue
• Probenecid - 250-1000 mg BID; use with meals and hydration; decrease elimination of meds ie PCN
•Lowering uric acid INCREASES risk of gouty attack• Use colchicine prophylaxis where possible 0.6-1.2 mg/day
• If unable to use, consider NSAID or prednisone,
2020 ACR Guidelines for the Treatment of Gout:Strong Recommendations
•Use ULT in pts with tophi or > 2 attacks per year
•Xanthine oxidase inhibitor (XOI) allopurinol is first line therapy
starting low dose (100 mg/day)and titrating to SUA < 6 mg/dl
•Start prophylaxis with ULT (Colchicine, NSAID, prednisone)
•Pt who have failed XOI ULT and have tophi or have frequent gout
attacks recommend using pegloticase IV
•Conditional recommendation to screen for HLA B5801 allele in
Koreans, Thais, Han Chinese, and African Americans before
starting allopurinol due to increased risk of allopurinol
hypersensitivity syndrome
Fitzgerald JD, et al Arthritis Care and Research June 2020 P 1-17

Patient Presentation 19
Hx: A 44-year-old male with gout and mild CKD reports progressive weakness in his arms and legs as well as paresthesia. He has been on colchicine 0.6 mg BID and allopurinol 500 mg per day with good control of his gout. Also takes thyroid replacement
Exam: show 4+ strength in the arm abductors and 3+ hip flexors. Distal strength is 5/5
Labs: CK is 2,200 GFR is 30 ml/minute
The next best step is to:
A. Stop allopurinol
B. Stop colchicine
C. Increase thyroid replacement
D. Start steroids

Tophi Recognition

Allopurinol plus patience


From Bad to Worse