Acne
91
ACNE
-
Upload
ibrahim-mohammed -
Category
Health & Medicine
-
view
489 -
download
0
description
Asked questions concerning acne. How does acne develops ? Factors for development of acne What are the predisposing factors Is it familiar? Is it controllable. Is it associated with diet or dust? Does cosmetics cause acne. Does drugs cause acne. Does stress has any role in causation of the acne
Transcript of Acne

ACNE


Acne Vulgaris Asked questions concerning acne. How does acne develops ? Factors for development of acne What are the predisposing factors Is it familiar? Is it controllable. Is it associated with diet or dust? Does cosmetics cause acne. Does drugs cause acne. Does stress has any role in
causation of the acne ?


I. The distal portion, or acroinfundibulum, is very similar to the adjacent epidermis. It displays keratinization with a granular layer, and corneocytes (squames) are shed into the lumen.
II. The lower part, or infrainfundibulum, is quite different. It shows a distinct pattern of trichilemmal keratinization and no granular layer.
PILOSEBACEOUS UNITThe infundibulum is divided into two parts

Different types of sebaceous follicles

Sebaceous follicles have a rich normal flora of bacteria (e.g. S. epidermidis and Propionibacterium spp. such as P. acnes) and fungi (e.g. Malassezia spp.). They also harbor Demodex mites, which in number in older adults & are rarely seen in prepubertal children.

SEBACEOUS GLANDSDevelopment
Sebaceous glands are derived from the epidermis as buds from developing hair follicle root sheaths and grow downward into the dermis.

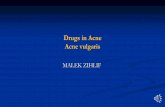
DHT0
500100015002000
Birth Puberty
pg/mL
Sebaceous glands are present at birth, and sebum production is relatively high at this time. It soon declines and remains low until puberty, at which time it again increases.
Androgens, in particular 5α-dihydrotestosterone (DHT), appear to be the major factor that controls the development of the glands & the production of sebum.
SEBACEOUS GLANDSDevelopment

The level of sebum production at the end of puberty remains constant through mid-adulthood. Sebum production declines in women after menopause, and in men during the sixth to seventh decade of life.
SEBACEOUS GLANDSDevelopment

Sebum is a light yellow viscous fluid. Secretion of sebum is holocrine, that is, the
sebocytes disintegrate and thereby release their sebum as they migrate towards the central gland and sebaceous duct.
Sebocyte turnover time is approximately 14 days.
The flow of sebum is relatively continuous.
SEBACEOUS GLANDSFunction

The amount of sebum produced varies among individuals and races average rate in adults is approximately 1 mg/10 cm2 every 3 hours
Sebum production that is less than 0.5 mg/10 cm2 every 3 hours is associated with sebostasis or dry skin.
1.5–4.0 mg/10 cm2 every 3 hours is considered excessive and results in the clinical condition known as seborrhea.
SEBACEOUS GLANDSFunction

Sebaceous glands also play important roles in;1. Cutaneous endocrine function (including the
hypothalamus–pituitary–adrenal-like axis of the skin as well as androgen metabolism).
2. Producing androgens. 3. Innate immunity. 4. Producing cytokines.5. Producing antimicrobial peptides that also
contribute to acne pathogenesis.6. Producing neuropeptides.
SEBACEOUS GLANDSFunction

ACNE VULGARIS

Acne Vulgaris
Definition
Is a multifactorial chronic inflammatory
disease of the PSU, characterized
by comedones , papules, pustules,
nodules, cysts and often scar.

Acne Vulgaris
INTRODUCTION
Primarily a disorder of adolescence. No cure, but the disease can be controlled
through medications. Significant economic & psychologic impact;
likelihood of self-consciousness, Low self esteem Social isolation, Depression Suicidal ideation.

Acne Vulgaris
EPIDEMIOLOGY
Affects approximately 85% of young people between 12 and 24 years of age.
During adolescence, acne is more common in males than females
During adulthood, acne is more common in females than males
35% of women and 20% of men reported having acne in their 30s,
26% of women and 12% of men were still affected in their 40s.

Acne Vulgaris
EPIDEMIOLOGY
risk for the development of acne include those with an XYY karyotype or endocrine disorders such as;1. Polycystic ovarian syndrome (PCOS),2. Hyperandrogenism,3. Hypercortisolism 4. Precocious puberty.

PATHOGENESIS OF ACNE VULGARIS


PATHOGENESIS OF ACNE VULGARIS
Puberty Androgens
Hyperkeratosis
Open Comedone(blackhead)
Closed Comedone(whitehead)
Sebum
P. Acnes
Pustules/Cysts
Scarring
Hair Follicle Sebaceous Gland
Rupture
Distress
Pilosebaceous unit
Comedone


Acne Vulgaris
PATHOGENESIS Four important factors;
I. Hyperactivity of the sebaceous gland
II. Follicular plugging & comedo formation
III.InflammationIV.Proliferation of
propionobacterium acnes

Acne Vulgaris
PATHOGENESIS
I. SEBUM PRODUCTION The sebaceous gland is controlled primarily
by hormonal stimulation After the first 6 m of life (when sebum production is relatively high), the rate decreases & remains stable throughout childhood. At adrenarche, sebum production dramatically increases.
Although the overall composition of sebum is the same in persons with or without acne but those with acne have larger sebaceous glands & excess sebum production.

Acne Vulgaris
PATHOGENESIS
I. SEBUM PRODUCTION Human sebum contains:
1. Triglycerides & FFA2. Wax esters3. Squalene4. Cholesterol esters5. Cholesterol

I. SEBUM PRODUCTION Androgens are produced both outside the sebaceous
unit, primarily from the gonads and adrenal glands, and locally within the gland via the action of androgen-metabolizing enzymes e.g. 5α-reductase.
Androgen receptors, found in the cells of the basal layer of the sebaceous gland and the outer root sheath of the hair follicle, are responsive to testosterone and 5α-dihydrotestosterone (DHT), the most potent androgens. DHT has a 5–10-fold greater affinity than testosterone for the androgen receptor and is thought to be the principal androgen mediating sebum production.
Acne Vulgaris
PATHOGENESIS

I. SEBUM PRODUCTION The role of androgens in sebaceous gland activity begins
during the neonatal period. From birth until approximately 6–12 months of age, infant
boys have elevated levels of luteinizing hormone (LH), which stimulates testicular production of testosterone.
In addition, both male and female infants exhibit increased levels of dehydroepiandrosterone (DHEA) and DHEA sulfate (DHEAS) secondary to a large, androgen-producing “fetal zone” in the adrenal gland that involutes over the first year of life.
Both testicular and adrenal androgen production decrease substantially by 1 year of age and remain at a stable nadir until adrenarche.
Acne Vulgaris
PATHOGENESIS


DHT is mainly derived from testosterone

I. SEBUM PRODUCTION With the onset of adrenarche (typically at 7–8
years of age, usually heralding menarche by several years) adrenal production circulating levels of DHEAS. This hormone can serve as a precursor for the synthesis of more potent androgens within the sebaceous gland. The rise in serum levels of DHEAS in prepubescent children is associated with an increase in sebum production and the initial development of comedonal acne.
Eunuchs, who lack testicular function, do not get acne.
Acne Vulgaris
PATHOGENESIS

I. SEBUM PRODUCTION Acne may respond to treatment with lower-dose oral
contraceptives containing 0.035–0.050 mg of ethinyl estradiol or its esters, higher doses of estrogen are often required to demonstrate a reduction in sebum secretion. Estrogens may act by several mechanisms, including:
1. Directly opposing the effects of androgens locally within the sebaceous gland.
2. Inhibiting the production of androgens by gonadal tissue via a negative feedback loop whereby pituitary gonadotropin release is inhibited.
3. Regulating genes that negatively influence sebaceous gland growth or sebum production.
Acne Vulgaris
PATHOGENESIS

Acne Vulgaris
PATHOGENESIS
I. SEBUM PRODUCTION Sebum in sebaceous glands and within the ducts is
sterile and contains no free fatty acids Sebum TG are broken down in the infundibulum
into FFA by P. acnes. FFA promote further bacterial clumping and
colonization (inflammation and comedon) Free fatty acids are also chemotactic and attract
neutrophils.

II. FOLLICULAR PLUGGING & COMEDO FORMATION;
This begins in the keratinized lining of the infundibulum. Comedo formation occurs when the corneocytes, which are normally shed into the lumen of the follicle and extruded through the follicular ostium, are retained and accumulate & intercellular cohesiveness of the corneocytes retention hyperkeratosis .
Acne Vulgaris
PATHOGENESIS


II. FOLLICULAR PLUGGING & COMEDO FORMATION;
Corneocytes production is accelerated as well. This combination of increased cellular cohesion and proliferation occurs in the proximal portion of the infundibulum, the infra-infundibulum, and it creates a bottleneck phenomenon and subsequent microcomedo formation (1 mm or less in diameter). In the underlying follicular epithelium, keratohyaline granules are increased in size and number, whereas lamellar granules and tonofilaments are decreased.
Acne Vulgaris
PATHOGENESIS

II. FOLLICULAR PLUGGING & COMEDO FORMATION;
As the comedo expands, the sebaceous lobule undergoes regression.
Because of the very narrow opening to the skin surface, there is initially an accumulation of loosely packed shed keratinocytes, sebum and bacteria. With expansion of the comedo, the contents become closely packed, creating whorled lamellar concretions. As the pressure increase, rupture of the comedo wall with extrusion of the immunogenic keratin and sebum occurs, with resultant inflammation
Acne Vulgaris
PATHOGENESIS

III. INFLAMMATORY RESPONSES; Inflammation is not only the result of comedo rupture, as it is
also seen early in acne lesion formation. For example, in acne-prone sites, the number of CD4+ T cells and levels of IL-1 have been shown to be perifollicularly prior to hyperkeratinization.
Acne Vulgaris
PATHOGENESIS
physical manipulation, or harsh scrubbing releases FFAs, bacteria, and keratin into tissues,


III. INFLAMMATORY RESPONSES; The type of inflammatory response determines the clinical
lesion seen: If neutrophils predominate (typical of early lesions), a
suppurative PUSTULE is formed. Neutrophils also promote the inflammatory response by releasing lysosomal enzymes and generating reactive oxygen species, and levels of the latter in the skin and plasma may correspond with acne severity.
Influx of lymphocytes (predominately T-helper [Th] cells) and foreign body-type giant cells, in addition to neutrophils, results in INFLAMED PAPULES, NODULES AND CYSTS.
Acne Vulgaris
PATHOGENESIS

IV. PROPIONIBACTERIUM ACNES Gram-positive, non-motile rods are found
deep within the sebaceous follicle They are anaerobic/microaerophilic and
naturally produce porphyrins (primarily coproporphyrin III) that fluoresce with Wood’s lamp illumination of any sebaceous-dense area, including normal skin → yellow fluorescence.
Acne Vulgaris
PATHOGENESIS

IV. PROPIONIBACTERIUM ACNES release of enzymes that contribute to
comedo rupture, lipases and chemotactic factors, as well as stimulation of a host response (by inflammatory cells and keratinocytes) that involves production of proinflammatory mediators and reactive oxygen species.
Acne Vulgaris
PATHOGENESIS

proinflammatory cytokines

IV. PROPIONIBACTERIUM ACNES Interactions between the skin’s innate
immune system and P. acnes play an important role in acne pathogenesis. One mechanism is via TLRs.
Acne Vulgaris
PATHOGENESIS

IV. PROPIONIBACTERIUM ACNES TLR2 is found on the surface of macrophages
surrounding acne follicles, and P. acnes has been found to expression of TLR2 and TLR4 on keratinocytes. P. acnes has been shown to stimulate the release of proinflammatory mediators (e.g. IL-1, IL-8, IL-12, TNF-α, matrix metalloproteinases) through the TLR2 pathway; IL-8 results in neutrophil recruitment, the
release of lysosomal enzymes and subsequent disruption of the follicular epithelium,
IL-12 promotes Th1 responses.
Acne Vulgaris
PATHOGENESIS

IV. PROPIONIBACTERIUM ACNES Antimicrobial peptides such as Beta-defensin-2,
cathelicidins & psoriasin work synergistically to protect the pilosebaceous unit from P. acnes.
P. acnes can induce monocytes to differentiate into two distinct innate immune cell subsets: (1) CD209+ macrophages (development of which
is promoted by tretinoin) that more effectively phagocytose and kill P. acnes.
(2) CD1b+ dendritic cells that activate T cells and release proinflammatory cytokines.
Acne Vulgaris
PATHOGENESIS

Acne Vulgaris
PATHOGENESIS
Other factors;
Genetic factors Dietary factors

Acne Vulgaris
PATHOGENESIS
GENETIC FACTORS; The number, size and activity of sebaceous
glands is inherited. The concordance rate for the prevalence and
severity of acne among identical twins is extremely high.
It is a widely held belief that acne (including nodulocystic acne) runs in families, and an association between moderate to severe acne and a family history of acne has been observed in several studies.

DIETARY FACTORS; The relationship between diet
and acne remains a subject of controversy.
Over the past decade, observational studies have found that milk intake (especially skim milk) is positively associated with acne prevalence & severity, and prospective studies have documented a link between a high glycemic-load diet and acne risk.
Acne Vulgaris
PATHOGENESIS

Role of diet in acne


Aggravating factors1. Change in sebaceous activity and
hormonal level (e.g. before or during premenstrual cycle).
2. High humidity & sweating conditions.3. Local irritation or friction.4. Rough or occlusive clothing.5. Cosmetics (having greasy base).6. Diet; chocolate, nuts, fats colas, or
carbohydrates.7. Oils greases, or dyes in hair product.8. Certain drugs like steroids, testosterone,
and estrogen
Acne Vulgaris
PATHOGENESIS

CLINICAL PICTURE OF ACNE VULGARIS


Acne is typically found in sites with well-developed sebaceous glands, most often the face and upper trunk
Face occurs; cheeks> nose>forehead>chin

Non-inflammatory/

CLINICAL PRESENTATION ACCORDING TO TYPE OF LESION:
I. Non-Inflammatory: ComedonalII. Inflammatory:
Papulo-pustularNodulo-cystic
Acne Vulgaris
C/P

NON-INFLAMMATORY ACNE:
“BLACKHEAD” – (open comedo) dome-shaped papules with a conspicuous dilated follicular opening that is filled with an inspissated core of shed keratin. Melanin deposition and lipid oxidation within the debris may be responsible for the black coloration upon exposure to air . “Ice-pick”-type scarring sometimes results from comedones alone.
“WHITEHEAD”– (closed comedo) small (~1 mm), skin-colored papules with no apparent follicular opening or associated erythema. These lesions may be subtle and better appreciated upon palpation, stretching or side-lighting of the skin
Acne Vulgaris
C/P




INFLAMMATORY ACNE: also originates with (micro)comedo
formation, followed by the development of papules, pustules, nodules and cysts of varying severity.
Acne Vulgaris
C/P

Erythematous papules typically range from 1 to 5 mm in diameter, dt. FFA [P. acnes lipase] irritatation of the follicular wall.
Pustules tend to be approximately equal in size & are filled with white pus & normal flora.
As the severity of lesions progresses, nodules form and become markedly inflamed, indurated and tender.
The cysts of acne are deeper & filled with a combination of pus & serosanguineous fluid.
In patients with severe nodulocystic acne, these lesions frequently coalesce to form large, complex inflamed plaques that can include sinus tracts.
Acne Vulgaris
C/P




Early treatment of acne is essential for the prevention of lasting cosmetic disfigurement due to scarring.
Erythema and postinflammatory hyperpigmentation often persist after resolution of inflammatory acne lesions. Although the pigmentary changes usually fade over many months if the acne is brought under control.
Acne Vulgaris
C/P





Mild Acne

Moderate Acne

Moderately Severe

Severe Acne

Severe AcneAcne conglobata





ICE PICK SCARS

BOXCAR

ROLLING

HYPERTROPHIC

DIAGNOSIS OF ACNE VULGARIS

DIAGNOSIS OF ACNE VULGARIS
Histopathologic examination
Demonstrates the stages of acnegenesis that parallel the clinical findings.
MICROCOMEDONES; A mildly distended follicle with a narrowed follicular opening is impacted by shed keratinocytes. The granular layer at this stage is prominent.

DIAGNOSIS OF ACNE VULGARIS
Histopathologic examination
IN CLOSED COMEDONES; the degree of follicular distension is increased and a compact cystic structure forms. Within the cystic space, eosinophilic keratinaceous debris, hair, and numerous bacteria are present.
OPEN COMEDONES have broad, expanded follicular ostia and greater overall follicular distension. The sebaceous glands are typically atrophic or absent. A mild perivascular mononuclear cell infiltrate circles the expanding follicle.

DIAGNOSIS OF ACNE VULGARIS
Histopathologic examination
As the follicular epithelium distends, the cystic contents inevitably begin to rupture into the dermis. The highly immunogenic cystic contents (keratin, hair and bacteria) induce a marked inflammatory response. Neutrophils first appear, creating a PUSTULE.
As the lesion matures, foreign body granulomatous inflammation engulfs the Follicle/plasma cells, foreign body giant cells, and proliferation of fibroblasts and end-stage SCARRING can result.
In acne fulminans, there is massive inflammation with varying degrees of overlying NECROSIS. Comedones are rarely observed. Severe scarring may be seen in resolving lesions.


DIAGNOSIS OF ACNE VULGARIS
Histopathologic examination


References
Jessica San Juan Microbiology Prof. Dr. Wafaa Afify Bolognia 3rd ed.