Lecture 19 The Electrocardiogram EKG/ECG Holdorf PhD, MPA, RDMS, RVT.
description
THE ECG IS ONLY ONE PARTOF PATIENT ASSESSMENT
• ONLY measures the ELECTRICITY present in the patients heart
• Tells you NOTHING about cardiac output
• ONLY works if the leads are all properly attached to the patient, the
cable is plugged into the monitor, and the monitor is turned on!!
Patient Assessment• A - Airway– Is the airway OPEN and MAINTAINABLE
• B - Breathing– Respiratory rate and quality
• C - Circulation– Pulse rate and quality– Level of Consciousness– Signs of Perfusion– Cardiac Output - blood pressure
• D - Defibrillation– Is the patient in a rhythm requiring defibrillation
Myocardial Cell Type
• Working Cells
• Electrical System Cells
– Formation of electrical impulse
– Conduction of electrical impulse
Mechanism of Impulse Formation
• Automaticity (normal)
• Reentry (tachydisrhythmias)
Causes of Arrhythmias
• Disturbances in Automaticity
• Disturbances in Conductivity
• Combination of Both
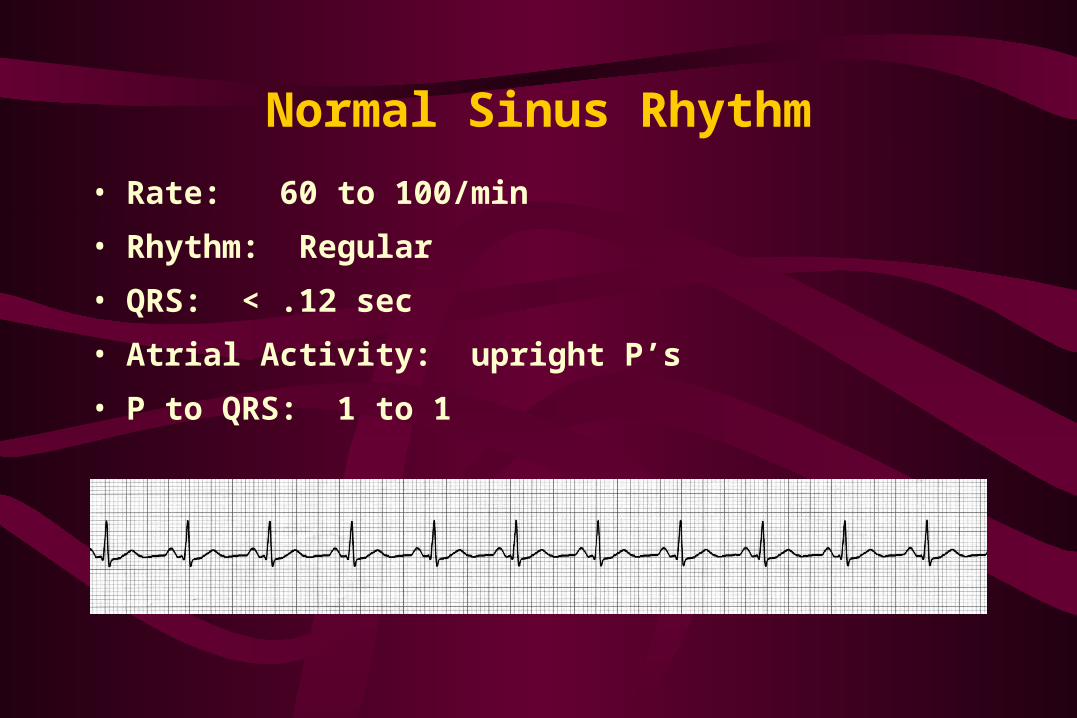
Normal Sinus Rhythm
• Rate: 60 to 100/min
• Rhythm: Regular
• QRS: < .12 sec
• Atrial Activity: upright P’s
• P to QRS: 1 to 1
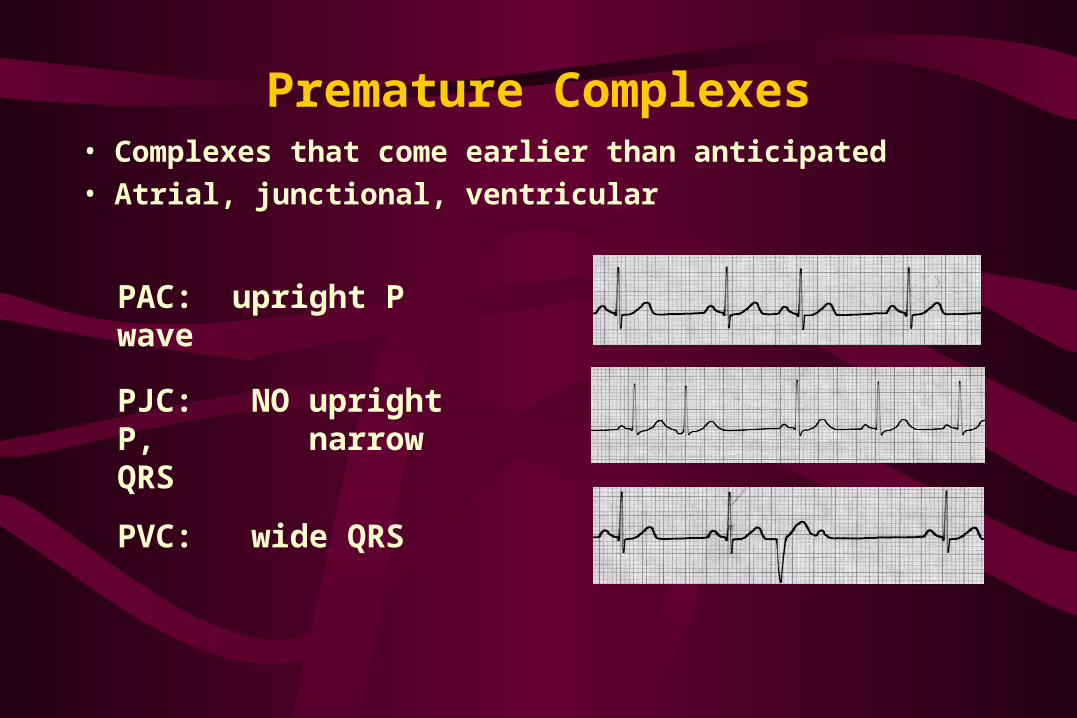
Premature Complexes• Complexes that come earlier than anticipated
• Atrial, junctional, ventricular
PAC: upright P wave
PJC: NO upright P, narrow QRS
PVC: wide QRS
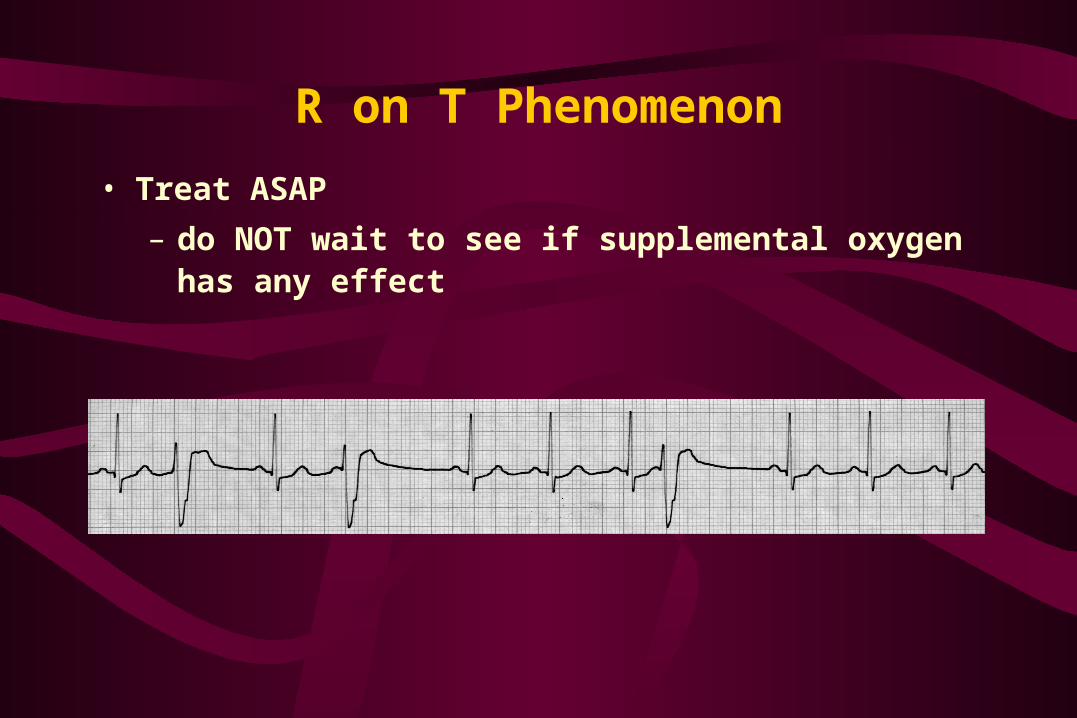
R on T Phenomenon
• Treat ASAP
– do NOT wait to see if supplemental oxygen has any effect
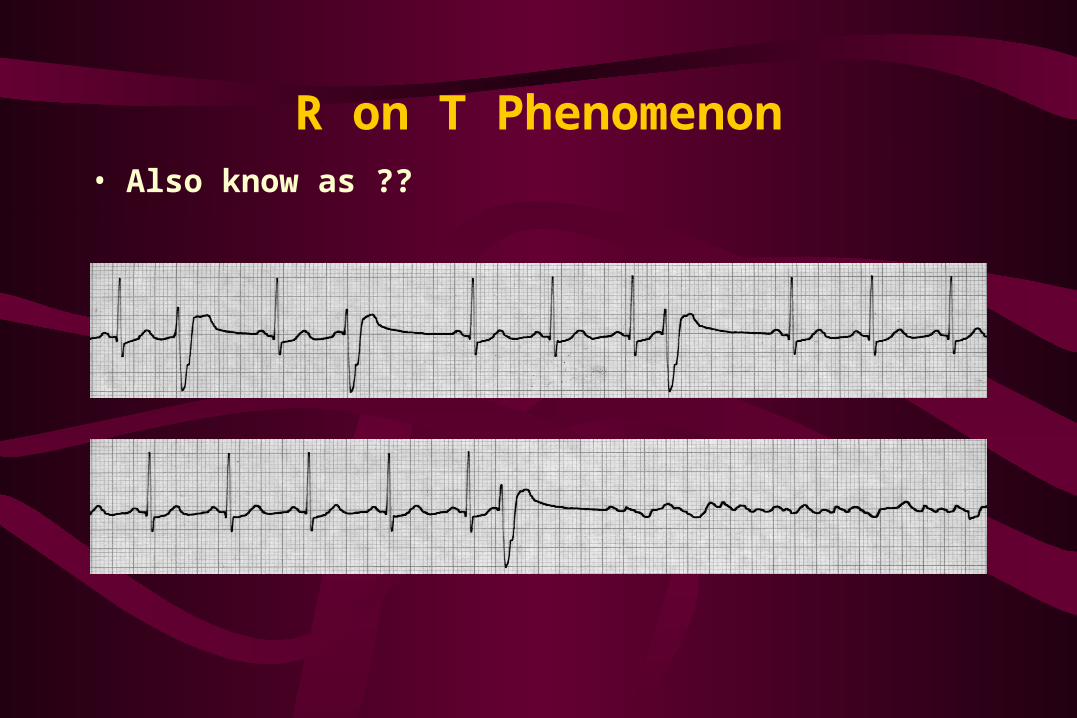
R on T Phenomenon• Also know as ??
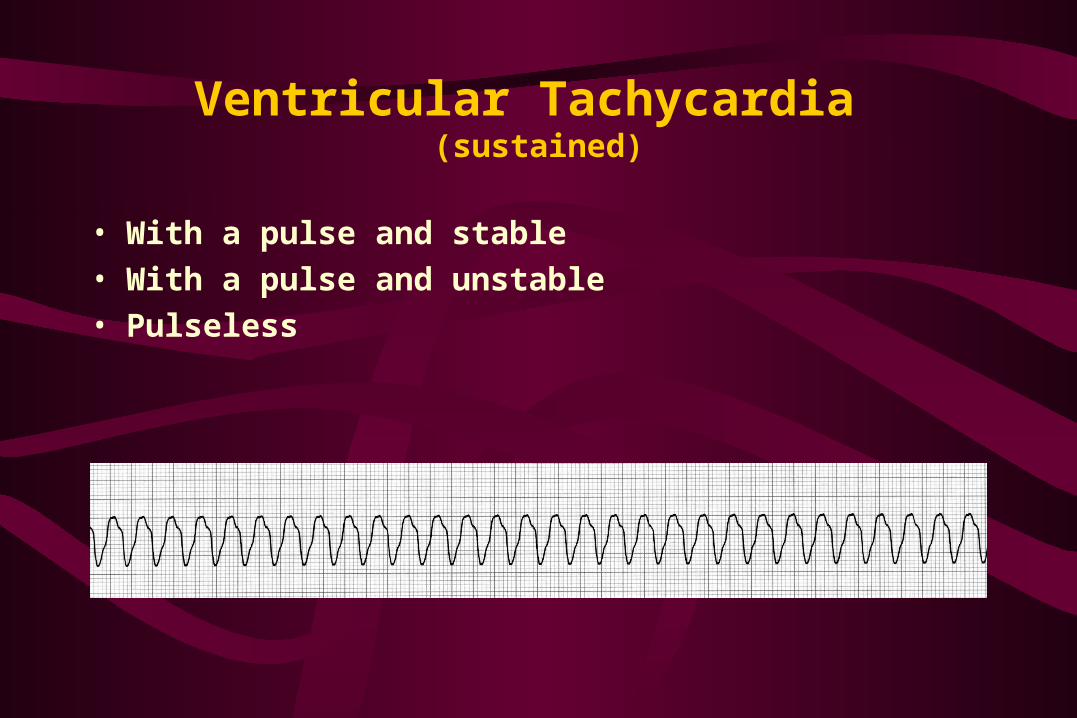
Ventricular Tachycardia (sustained)
• With a pulse and stable• With a pulse and unstable• Pulseless
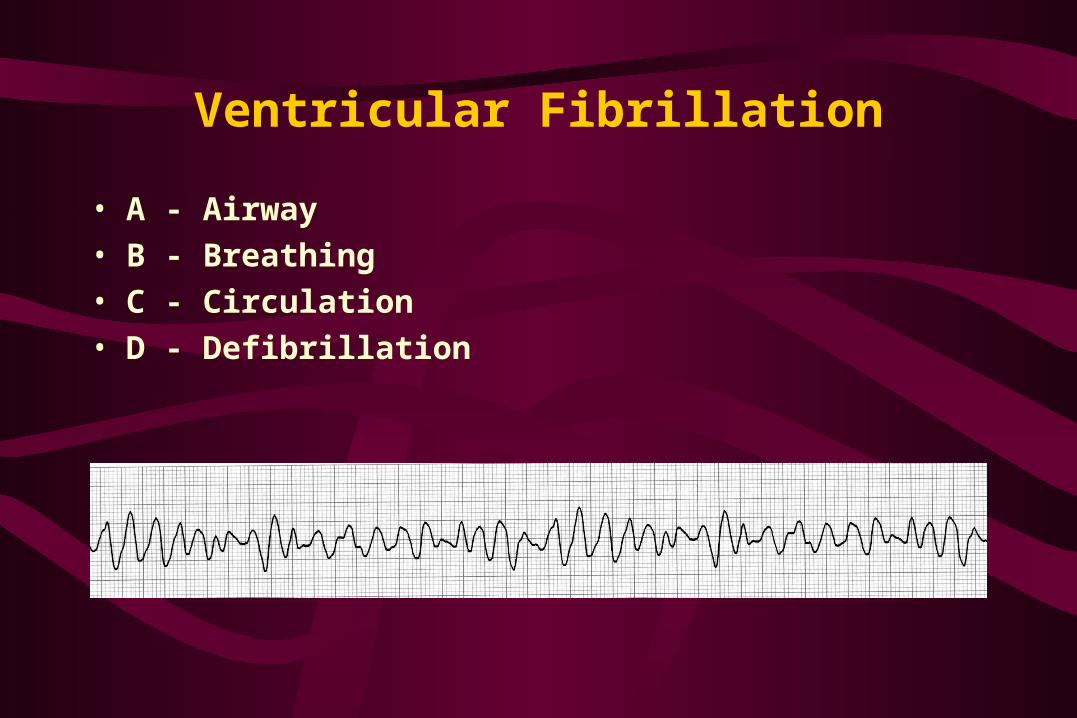
Ventricular Fibrillation
• A - Airway• B - Breathing• C - Circulation• D - Defibrillation
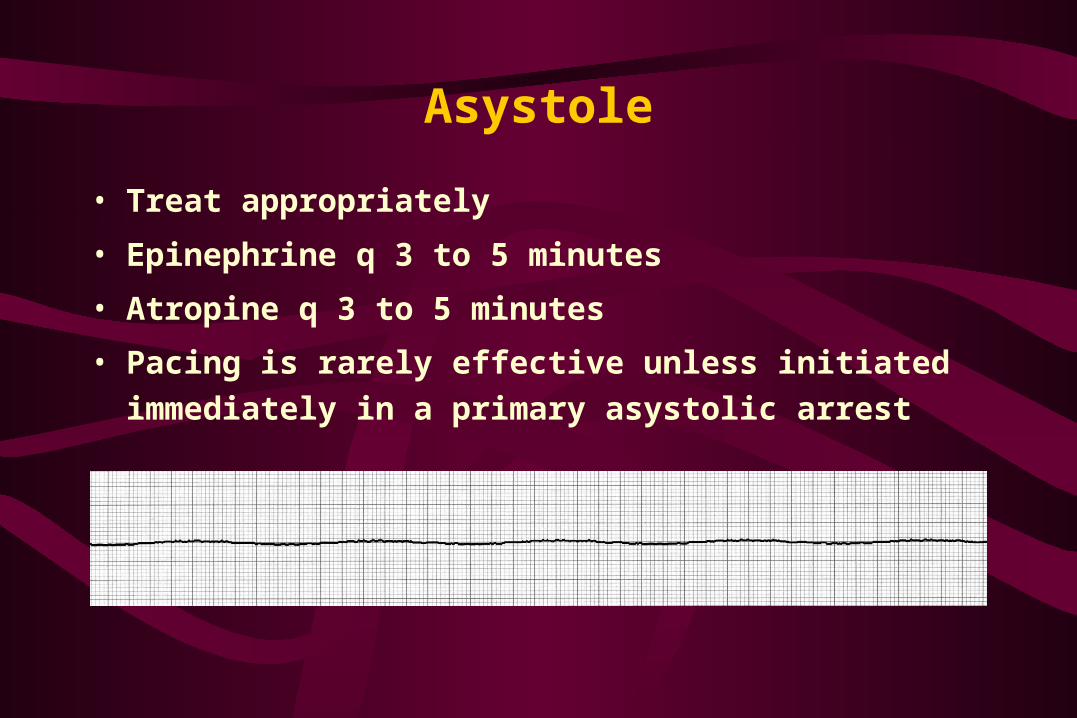
Asystole
• Treat appropriately
• Epinephrine q 3 to 5 minutes
• Atropine q 3 to 5 minutes
• Pacing is rarely effective unless initiated immediately in
a primary asystolic arrest