
Accreditation manual - Guvernul Romaniei · “Dr.onstantin Papilian” luj Emergency Military...
258
ACCREDITATION MANUAL 2017
Transcript of Accreditation manual - Guvernul Romaniei · “Dr.onstantin Papilian” luj Emergency Military...

1
ACCREDITATION
MANUAL
2017

2

3
Warning
We warn the hospitals that the use by another organization of the hospital
accreditation standards, developed and adopted by ANMCS, is not recognized
by the Romanian health system.
Co-ordinating Group for
Standards elaboration: Experts group
Coordinator - Vasile Cepoi, MD Vasile Astărăstoae
Sorin Ungureanu, MD Carmen Angheluță
Marius Filip, MD Mariana Brudașcă
Andrei David Daniel Burghelea
Nicoleta Manu, MD Ana-Maria Dădulescu
Andrei Ștefan, MD Adina Geană
Nirvana Georgescu
Daniela Marghidan
Doina Miron
Daniela Moșoiu
Antonia Nițescu
Georgel Rusu
Relu Chițac

4
Manual Authors The Validation Panel Group
Co-ordinator – Dr. Vasile CEPOI Dr. Sorin UNGUREANU Dr.Marius FILIP Ec. Andrei DAVID Dr. Nicoleta MANU Dr. Andrei ȘTEFAN Psih. Alexandru DICU
Diana Loreta PĂUN, representative of Administraţia Prezidenţială; Dragoş CONDREA, representative of Secretariatul General al
Guvernului; Marin POPESCU, representative of Secretariatul General al
Guvernului; Mihai COCULESCU, representative of Academia Română; Mircea IFRIM, representative of Academia de Ştiinţe Medicale; Dan DUMITRAŞCU, representative of Asociaţia Naţională a
Universităţilor de Medicină şi Farmacie din România; Alin COSTACHE, representative of Casa Naţională de Asigurări de
Sănătate; Gheorghe BORCEAN, representative of Colegiul Medicilor din
România; Radu CÂMPIAN, representative of Colegiul Medicilor Dentişti din
România; Viorica TOTOREAN, representative of Ordinul Asistenţilor Medicali
Generalişti, Moaşelor şi Asistenţilor Medicali din România;
Constanţa POPA, representative of Ordinul Biochimiştilor, Biologilor şi Chimiştilor în Sistemul Sanitar din România;
Dănuţ CĂPĂŢÎNĂ, representative of Asociaţia Spitalelor din România;
Speranţa PRADA PETRIA, representative of Asociaţia Naţională a Farmaciştilor de Spital din România;
Silvia Gabriela SCÎNTEE, representative of Şcoala Naţională de Sănătate Publică, Management şi Perfecţionare în Domeniul Sanitar Bucureşti;
Adrian GROM, representative of Societatea Naţională de Medicină a Familiei;
Marius SEPI, representative of Federaţia SANITAS din România; Viorel ROTILĂ, representative of Federaţia „Solidaritatea Sanitară”
din România; Florin CHIRCULESCU, representative of Sindicatul „Dr. Ioan
CANTACUZINO”; Cristina Ileana BERTEANU, representative of Asociaţia
Transplantaţilor din România; Radu GĂNESCU, representative of Coaliţia Organizaţiilor
Pacienţilor cu Afecţiuni Cronice din România (COPAC); Raluca TÎRZIU, representative of Asociaţia Naţională pentru
Protecţia Pacienţilor.

5
We thank the hospitals that have supported ANMCS's effort to
develop Hospitality Accreditation Standards, 2nd Edition, by
participating in the Pilot 1 and Pilot 2 testing process:
Pilot 1:
Hospital City
Colentina Clinic Hospital Bucharest
SANADOR Hospital Bucharest
Institut of Oncology Bucharest Institut of Oncology “Prof. Dr. Ion Chiricuta” Cluj Cluj Napoca Emergency Clinical Hospital for Children Cluj “Prof.dr.Octavian Fodor” Gastroentorology and Hepatology
Regional Institute Cluj
Regional Institut for Oncology Iasi
“Sf. Spiridon” Cliniq Hospital Iasi
Pilot 2:
Hospital City
Clinical Hospital CF no. 2 Bucharest
“Grigore Alexandrescu” Emergency Clinical Hospital for Children Bucharest
“Filantropia” Clinical Hospital for Obstretics and Ginaecology Bucharest “Bagdasar Arseni” Emergency Clinical Hospital Bucharest Cluj Napoca County Emergency Clinical Hospital Cluj “Prof.dr.Ion Chiricuță” Oncologic Institute Cluj Cluj Napoca Emergency Clinical Hospital for Children Cluj
“Prof.dr.Octavian Fodor” Gastroentorology and Hepatology Regional Institute
Cluj
Cluj Kidney Transplant and Urology Institute Cluj “Dr.Constantin Papilian” Cluj Emergency Military Hospital Cluj “Prof.dr.George I.M. Georgescu” Institute of Cardio-Vascular
Diseases Iasi
“Dr. C.I.Parhon” Clinical Hospital Iasi Socola Psychiatric Clinical Hospital Iasi CFR Iasi Clinical Hospital Iasi Piatra-Neamt Emergency County Hospital Piatra Neamț “Sf. Dimitrie” City Hospital of Tg. Neamt Tg.Neamț

6

7
Contents
INTRODUCTION ....................................................................................................................................... 9
Accreditation Manual ...................................................................................................................... 9
Evolution of Hospital Accreditation Standards .............................................................................. 10
Overall Objectives in this Accreditation Cycle ............................................................................... 10
Healthcare Services Quality in the Hospital .................................................................................. 11
2. WHAT IS ACCREDITATION ................................................................................................................ 13
Evaluation .............................................................................................................................................. 15
Registration/eligibility conditions .................................................................................................. 16
Statement of terms and the use of the standardisation system in evaluation. ............................ 19
Selection and organisation of standards to be used during the accreditation process. ............... 22
Expected outcomes from the accreditation process. .................................................................... 22
The conduct. .................................................................................................................................. 24
Beneficiaries of the accreditation process Stakeholders involved in the accreditation process. . 24
3. REGISTRATION/ELIGIBILITY TERMS .................................................................................................. 26
4. IMPLEMENTATION OF QUALITY MANAGEMENT............................................................................. 27
5. WHAT DO THE STANDARDS BRING IN TERM OF NOVELTY ............................................................. 30
What is new in the second edition of the Hospital Standards? .................................................... 30
6. MAPPING .......................................................................................................................................... 36
7. DESCRIPTION OF ACREDITATION STANDARDS ................................................................................ 98
01. Strategic and organisational management ............................................................................. 98
02. Clinical management ............................................................................................................. 134
03. Medical ethics and the patient rights .................................................................................... 182

8
8. DESCRIPTION OF THE EVALUATION AND ACCREDITATION PROCESS ........................................... 190
Enumeration of the steps taken by users in the accreditation process. ..................................... 190
Description of the hospital evaluation process ........................................................................... 192
Document Analysis ...................................................................................................................... 194
Interview ...................................................................................................................................... 195
Open-closed questions ................................................................................................................ 196
Direct observation ....................................................................................................................... 197
Instruments used by the evaluator ............................................................................................. 199
Hospital evaluation - timetable of activities of the evaluation committee ................................. 200
1. Pre-visit ............................................................................................................................ 200
2. Actual visit ........................................................................................................................ 201
3. Post-visit ........................................................................................................................... 206
4. Evaluation File .................................................................................................................. 207
The evaluators and the evaluation board ................................................................................... 209
The activity of the evaluators in the evaluation committee ....................................................... 209
Development of the draft evaluation report and of the evaluation report ................................ 229
Training and profile of evaluators ............................................................................................... 231
Evaluation visit requirements ...................................................................................................... 233
What A.N.M.C.S. does in relation to the hospital. ...................................................................... 233
9. ACCREDITATION CATEGORIES, EVALUATION SCALES (FOR INDICATORS) .................................... 240
10. MONITORING ................................................................................................................................ 245
Methodology for monitoring accredited hospitals ..................................................................... 245
11. GLOSSARY ..................................................................................................................................... 250

9
INTRODUCTION
Accreditation Manual
The discussion on quality is as old as medicine. Healthcare professionals have always
been concerned with the effectiveness of their interventions. Costs were a secondary
concern and with the society medicalisation, there came a period when costs were not at all
a matter for the medical professionals. The development of medical technologies induced,
together with the increasing complexity of the medical interventions, higher healthcare
services costs and, implicitly, an interest in more efficient spending in healthcare. This
complexity calls for a new approach on healthcare services management, by involving all
personnel in feeling accountable both for patient safety and effective healthcare services
and for more efficient spending, aiming at reducing healthcare services costs to increase
accessibility. The concept of quality management in healthcare management proposes the
adoption of a set of requirements which meet these objectives, by stakeholder consensus.
As a principle, the development of an organisation’s quality system is voluntary. This
voluntary pursuit should be understood in the sense of Eduard Deming’s words “It is not
necessary to deliver quality; survival is not mandatory”.
The “mandatory voluntary” accreditation is a topic for debate in the medical world and
it induces the perception of a legal regulation, imposing formal and bureaucratic compliance.
It is not owned by professionals as an external evaluation mechanism of good practice in
healthcare which should lead to better results, more effective healthcare services and
proper spending of public money, namely more efficient use of resources. We see here a
controversy between the ethical attitude of the physician “I do what’s best for the patient”
and the economic approach of the management “not everything medicine can do makes
economic sense”. Actually, what is needed is a way to create ownership on both sides.
The dispute between the positions of power in a hospital (management and
operational) has relied so far on the transfer of responsibility from one to the other. The
result of this dispute should be accountability on both sides, by proper, real time
communication with regard to the balance between resources and services. The
implementation of quality management pursues this harmonisation by joint acceptance of
the responsibilities of the two main structural components of a hospital.
The introduction in Law 95/2006 on healthcare reform of mandatory hospital
accreditation, the establishment of the National Commission for Accreditation of Hospitals in
2008, by GD no. 1148 of 18 September 2008, and the first cycle of hospital accreditation
were the first steps in the development of a quality assurance and improvement system in
the Romanian healthcare system.

10
Evolution of Hospital Accreditation Standards
The first edition of the accreditation standards approved by Order of the Minister of
Health 972/2010, underpinning the accreditation of 434 hospitals in the first accreditation
cycle, was replaced by a second edition adopted by consensus by the Management Board of
ANMCS, after intense public debate within 8 regional conferences and one national
conference. After being piloted in 30 hospitals, various unclarities in the requirement
phrasing and structural shortcomings were identified, therefore the committee of experts
revised it and delivered a revised second edition which was analysed and voted by the
Management Board and adopted by consensus.
This new edition, which will be used for the second cycle of hospital accreditation,
planned for July 2017-July 2018, is subject to evaluation for accreditation by ISQua. The table
below presents the changes made, compared to the first edition. The number of references
was reduced, from 11 to 3, to ensure correlation with the functional structure of hospitals,
for better understanding of their goal, objectives and implementation.
Overall Objectives in this Accreditation Cycle
The experience of the first accreditation cycle showed that, for healthcare
professionals to adhere to the shift from an oral organisational culture to a written culture,
where healthcare organisation and provision is formalised by procedures and protocols, it is
necessary that the accreditation standards underpinning the implementation of a quality
management system should reflect the relevant aspects of the medical activity, in relation to
an organisational management which supports the activity of the medical professionals and
is jointly accountable for quality assurance and improvement of healthcare services and
patient safety.
With this edition, ANMCS intended to initiate a quality pursuit at hospital level, based
on professional dynamics. The objectives were:
To develop a hospital development strategy which meets the healthcare needs
of the population it serves, to ensure better access to healthcare services and
prevent overprovision of services which generates, among others, undue costs;
To correlate the package of services provided with the hospital mission and
available resources, to prevent provision of care which exceeds competency,
exposing the patient to uncontrollable risks;
To ensure continuity of healthcare, a prerequisite for improving healthcare
effectiveness and efficiency;
To develop a healthcare risk management system, especially for clinical risks,
to increase patient safety;
To create the necessary conditions for patient-centred healthcare, in
compliance with the principles of ethics and with patient rights;

11
The accreditation methodology aims at objective quality appraisal, to prevent risks
associated to the implementation of a quality management system, first of all related to
limiting bureaucracy and formalism, better correlation with other quality efforts
(management control, various certifications, authorisations etc.), valorisation and
recognition of each hospital.
Accreditation is the only approach which provides external evaluation, objective and
equidistant, and an overall analysis of the hospital healthcare provision, identifying both
hospital disfunctionalities and those generated by healthcare system regulations, based on
which ANMCS recommends actions to improve healthcare services quality and patient
safety.
The equidistance and objectivity of healthcare services quality appraisal are ensured
by the collective management of ANMCS, represented by the Management Board, consisting
in representatives of all stakeholders, namely patient associations, professional associations
and trade unions, governmental structures in the field of healthcare and the presidential
administration.
The accreditation process includes several stages, as provided by MH Order 446/2017.
Healthcare Services Quality in the Hospital
The development of actions for quality assurance and improvement of healthcare
services and patient safety in a hospital requires a first stage consisting in the
implementation of a set of principles and values leading to the change of organisational
culture and the control of key cross-cutting processes for quality assurance in healthcare,
such as: adopting actions to achieve international patient safety objectives, patient chart
quality, prevention and control of healthcare-related infections, procedures related to
vigilance in risk prevention (pharmacovigilance, materiovigilance) etc.
Accreditation confirms that hospital employees, following manager’s decision, are
engaged in the process of changing the manner of working, so as to contribute to the
implementation of the best clinical and management practices that would provide for
continuing quality assurance and improvement of services provided by the hospital and safe
medical practices, to obtain the best results in terms of healthcare effectiveness and
efficiency and to prevent occurrence of undesirable events.
Accreditation measures the quality of healthcare services at the level of the entire
hospital, it is not the accreditation of each sector of activity. Therefore, it measures the
overall compliance with the accreditation standards, against the indicators reached by each
structure, not the compliance of each structure. If a unit or a department are not
operational due to lack of staff, it should be declared officially closed by the public health
directorate.

12
It is a peer review performed by specialists in healthcare, economy, law, focused on
general aspects of healthcare organisation, which may be risk factors for the quality of
healthcare services and patient safety, but it does not represent an in-depth analysis of the
medical performance, by specialty.
Therefore, evaluators look for answers to the following questions:
To answer these questions, there must be procedures, protocols, methodologies and
instructions that enable the implementation of best practices both in clinical activities and in
management.
In order to confirm the effectiveness and efficiency of healthcare provision, the
hospital must present its own analysis, performed during the self-assessment process at the
level of unit/department and clinical audit at hospital level. Patient safety efforts are
demonstrated by the implementation of clinical risk management. This accreditation cycle
will have a special focus on the risk register at unit/department level, prevention measures,
risk mitigation and identification and reporting without pointing fingers in case of
healthcare-related adverse events, hindsight analysis procedures to learn from mistakes.

13
2. WHAT IS ACCREDITATION?
Accreditation of healthcare facilities – is the process of validation of healthcare
services compliance with the accreditation standards adopted by ANMCS and approved
according to law, whereby healthcare facilities are classified by accreditation categories to
provide confidence in their technical, professional and organisational competence.1
It is a process of external and, in principle, independent evaluation performed
by professionals trained for this – evaluators.
It focuses on three dimensions: quality management system implementation,
process organisation to provide healthcare services and improvement of
professional practices.
This, accreditation regards the hospital as a set of processes undertaken by an
organisation having as a result patient-centred healthcare services.
ACCREDITATION GOAL:
Healthcare services should ensure patient, staff, data and environmental
safety;
Healthcare services provided should meet the needs of the communities they
serve;
Healthcare facilities should accept patients within the limits of their
competence and resources.
1 Law no. 185/2017 on quality assurance in the health system.

14
Accreditation benefits and advantages
for the patient
• Increased patient safety and satisfaction;
• Lower infection risk for patients,
caregivers, employees, volunteers and
students/residents;
• Lower infection risk of the healthcare
environment (bed sheets, food,
accommodation, environment);
Accreditation benefits and advantages
for the hospital
• Increased credibility of the healthcare
facility and trust in the healthcare
services they provide;
• Increased quality and safety of medical
activity;
• Increased trust among the staff of
healthcare facilities, contributing to
their motivation and to building the
organisational culture;
• Increased predictability of healthcare
facility activities;
• Study of adverse events as a learning
from error process;
• Increased effectiveness and efficiency
of healthcare services
• Increased employee satisfaction;
• Lower risks generated by the external
environment.

15
Evaluation
Evaluation is the activity of analysing the level of healthcare facility compliance with
the accreditation standards, undertaken by external evaluators of healthcare services,
independent from all stakeholders, upon request of the healthcare facility to commence the
accreditation procedure2.
The evaluation process is structured in 3 stages, namely:
The evaluation process is finalised when the evaluators submit all materials
representing the hospital evaluation file to the specialist structures of A.N.M.C.S.
2 Law no. 185/2017 on quality assurance in the health system.

16
Registration/eligibility conditions
The evaluation preparation stage, coordinated by the specialist structures of the
National Authority of Quality Management in Health, hereinafter called A.N.M.C.S., includes
the following main activities:
a) Hospital registration for the accreditation procedure with A.N.M.C.S., by filling in
and submitting the template form developed by the specialist structures of A.N.M.C.S. The
accredited hospitals shall submit the registration application within one year, but no less
than 9 months before the validity of the accreditation certificate expires, and those
submitting for the first time the registration application for the accreditation procedure
within one year from the publication of the order to which this annex is an integral part shall
be evaluated according to the provisions of this order;
b) Identification by A.N.M.C.S. of the necessary human resources for the evaluation
visit and planning of the evaluation visit;
c) Communication by A.N.M.C.S. of the response to the application, of the estimated
period for the performance of the evaluation visit and of the amount of the accreditation
fee, estimated based on the statements in the hospital identification form. The evaluation
visit duration, which underpins the estimation of the amount of the accreditation fee, shall
be calculated according to the visit duration calculation form, hereinafter called FCD, whose
template is approved by order of the A.N.M.C.S. president;
d) In case of structure changes occurred after the submission of the accreditation
application, FCD shall be updated and shall determine a recalculation of the fee according to
the new structure;
e) The accreditation fee calculation method and formula shall be established according
to the provisions of the Order of the Minister of Health and of the President of the Authority
of Quality Management in Health no. 1.350/668/2016 approving the accreditation fee
calculation method, valid for the accreditation cycle related to the period 2017-2021;
f) Communication by A.N.M.C.S., at least 9 months prior to the period planned or the
performance of the evaluation visit, of the initiation of the evaluation preparation stage, and
of the deadline within which the hospital should make available for A.N.M.C.S. the
mandatory documents requested, hereinafter called DOS, and the additional documents
necessary for the evaluation and accreditation process, hereinafter called DS;
g) DOS means documents certifying the legality of the hospital operations, internal
regulations on activities with major impact on patient and staff safety, hospital structure and
the proof of payment of the accreditation fee. The means of accreditation fee payment are
set by order of the A.N.M.C.S. president;

17
h) Analysis of DOS and DS by the specialist structures of A.N.M.C.S.;
i) If the analysis performed according to the provisions of letter h) finds that the
mandatory requirements have been fulfilled, the evaluation visit shall be performed in the
period initially announced, and A.N.M.C.S. shall set up and approve the evaluation
committee for accreditation purposes, depending on the hospital specificity. The evaluation
committee shall be set up according to the provisions of the Order of the President of the
Authority of Quality Management in Health no. 136/20153 approving the Operational
Procedure for random distribution in the memberships of the hospital evaluation
committees of evaluators included in the A.N.M.C.S.’s Register of Healthcare Services
Evaluators specialised in hospital evaluation, and for the appointment of committee
presidents. The information on the membership of the evaluation committee and on the
visit period shall be published by A.N.M.C.S. on the institution website;
j) After the committee membership has been set, A.N.M.C.S. shall conclude contracts
with the members of the evaluation team, and they shall be trained by A.N.M.C.S. staff;
k) If the analysis performed according to the provisions of letter h) indicates that the
hospital does not meet the minimum mandatory requirements to start the evaluation visit,
A.N.M.C.S. shall submit the hospital a request to complete the documentation, within 30
calendar days after the request receipt;
l) In case the documentation is complete upon expiry of the 30-day deadline, the
provisions of letters h) and i) shall apply;
m) In case the documentation is not complete upon expiry of the 30-day deadline, the
evaluation visit shall be postponed by A.N.M.C.S., and the hospital shall be responsible for
the consequences of non-accreditation. The visit shall be re-planned according to A.N.M.C.S.
resources.
3 The Order of the President of the Authority of Quality Management in Health no. 136/2015 was not published
in the Official Journal of Romania, Part I.

18
Stages for QMS implementation in a medical facility:
Decision-making
Analysis (consultation)
Organise the quality structure
Train the coordination committee
Launch the project
Train all personnel
Draft documentation
First application of documentation and first internal audits
Evaluation conclusions and documentation review
Second application of documentation
Validation audit
Finalise documentation
Certification audit
Corrective actions

19
Statement of terms and the use of the standardisation system in
evaluation.
Accreditation is a process that entails external and, in principle, independent
evaluation, carried out by purposely trained persons – evaluators, followed by an analysis
that determines the level of accreditation, and results in the accreditation as such, followed
by a period when the maintenance of compliance with the accreditation requirements is
monitored.
The accreditation of a hospital organisation is focused on three dimensions, namely
the quality management system, organisation of healthcare services and efforts to improve
practices (processes).
Thus, the accreditation looks at the hospital as a system of structures, activities and
outcomes, as an organisation.
The STANDARDS establish the expectations on a hospital’s performance, structure and
processes that should ensure (as outcomes) quality, safe and compliant care, treatment and
service s for each patient. At the end of the day, a standard is the value of the expected or
targeted quality.
Thus, the decision to accredit a hospital means measuring the conformity with various
standards.
The accreditation process covers all public and private healthcare facilities with beds:
including one day, acute conditions, chronic conditions, long term and recovery care.
Standards are designed to define the targeted, desired or
expected higher quality, in terms of an organisation’s processes
and outcomes and in direct relation with the patient’s
satisfaction and health status benefits.
Standards are reunited in chapters named references (3 such references are used in
this cycle of accreditation), and are described by criteria. While the standards are envisaged
targets, the criteria are measurable and define objectives to be achieved by complying with
the standards.
Criteria are supplementary information, details or
circumstances related to a standard within a reference. Criteria
are used in the accreditation audit as a method for defining the
evaluation framework and for qualifying a referred element, for
the purpose of making a judgement or an appreciation on the
conformity of a practice or activity.

20
Each criterion is defined by the concurrent existence of:
The requirements are what is requested for proving the criteria,
so they are activities performed by the users (hospitals)
through which the objectives (criteria) are achieved. The
criteria and requirements of standards are part of the
standards.
Beyond them, in the process of measuring the compliance with the requirements, the
indicators are defined as concrete instruments proposed by ANMCS to measure the
compliance of users with the requirements of standards. They can be regarded as stages
fulfilled to carry out the activities which the requirements imply. The indicators are not
mandatory, are only the vision of ANMCS regarding the measurement of compliance with
the standard requirements.
The hospital may have its own way in which it should be compliant with the standard
requirements! Thus, it shall show the evaluators how and bring the evidence used to check
them (both the fulfilment of requirements and the way in which they are fulfilled).
The evaluation of performance is definitely an evaluation of success, and the accuracy
of such measurement is given by the use of specifically selected quality indicators. The
indicators are part of the set and measurement instruments while the standards are
described and detailed through criteria and characterised and concretely anchored by
requirements.

21
The objectivity of this type of finding is given by the use of indicators specific to each
criterion, and the scalable consideration allows a nuance to the issuing of evaluation
judgment.
The indicators have features which qualify them as measurements units intended to
measure an evolution in quantitative terms; they are quantifiable and reveal whether an
activity was or not efficiently and effectively managed and carried out.
The quality of an indicator is given by the fact that it constantly measures the same
element of a situation, regardless of the context.
Several categories or types of indicators applicable for the criteria and evaluation
requirements are recognised:
They are expressed in absolute values or as numeric report, there being simple
indicators and composite indicators. The indicators shall be applicable to different
dimensions of quality, being also indicators measuring the effectiveness (relation between
the results and initially proposed objectives), the efficiency (relation between the results and
used means to achieve them) and the availability or accessibility (service provided at the
right time, in the right place, the right time and corresponding intensity measure).

22
Selection and organisation of standards to be used during the
accreditation process.
The standards, criteria and requirements and measurement indicators are grouped
into checklists (according to annex 1 to this guideline), grouping for a list exactly those
standards, criteria and requirements which are relevant for the subject/domain for which
they are applicable.
The indicators proving the fulfilment of those requirements are mentioned in the
checklists.
The checklists are instruments for data collection, containing indicator packages
generally referring to a single activity, thus taking part in the development of the entire
image of quality and safety of services in the hospital.
The indicators were built on the principle of logical succession of the stages of an
activity: first of all an interrogation is made on the existence of an activity, then the degree
of its development, then the good or bad experience accumulated by the activity, and then
the existence of a type of evaluation of that activity and the existence of data and
information on the evaluation and, finally, any measures taken to correct the deficiencies.
Another used principle is to collect the same data, by the same indicators, from several
sources, so that there should be an indirect and remote verification of the verisimilitude of
answers received by the evaluators from their interlocutors in hospitals. The principle is met
in social sciences under the name of “quiz”. For this reason, the identical indicators were
spread in several checklists and even in several reference chapters.
Expected outcomes from the accreditation process.
General results from the perspective of the healthcare system:
Accreditation of hospitals enlisted in the process and obtaining and keeping a level
of accreditation positioning them with the accredited status.
Maintaining a minimum reasonable level of satisfaction of users to standards and
accreditation methodology.
Permanently obtaining a correct feedback regarding the level of standard updating
in relation to the situation in the healthcare system.
Specific results from the hospital. During the 9-month period from the registration in
the accreditation process, the main results which are expected from the hospitals are:
- understanding and deepening the concept of quality management in healthcare,
- understanding the accreditation standards, criteria and their requirements,

23
- verification of the initial level of compliance with the standards, criteria,
requirements,
- use of own department or person responsible for the quality management to
improve the compliance with the standards, where necessary,
- preparation of documents/records proving the compliance with the standard
requirements and fulfilment,
- establishing the responsible persons by the hospital to communicate with the
evaluation team, responsible persons with the required competences regarding
the requirements for which they received a delegation.
During the evaluation period, starting from the pre-visit (2 months), continuing during
the evaluation visit and then being finalised during the post-visit (3 weeks), the results
expected by the hospitals are:

24
After the establishment of the accreditation level, for the accredited hospitals and
those without a compliance plan, the maintenance of the level of compliance with the
accreditation standards, the results expected from the hospital being:
The conduct.
In relation to ANMCS and the external evaluators which are part of the
evaluation team, the hospital representatives must promptly answer all applications by
submitting documents, providing the access or the requested additional information.
In their entire activity, the hospitals must show interest and a permanent active
concern for increasing the quality of services and their positive reception by the patients, to
increase the efficiency of the medical procedure and the administrative procedure but also
for the traceability and predictability of its processes.
Beneficiaries of the accreditation process Stakeholders involved in the
accreditation process.
The beneficiaries of the accreditation process are first and foremost the hospitals
registered within the accreditation process. For them, due to the efforts of increasing the
quality and the compliance with ANMCS quality standards, the preparation of structure,
organisation of healthcare services, establishment and procedural processes and flows of

25
activities, forecasting the impact or result., all these are benefits already from the stage of
preparation for the accreditation. At the same time, increasing the customers’ confidence in
the provided services is the competitive benefit in the community and in the fundraising and
new patient market.
The most important beneficiaries of the accreditation process are yet the beneficiaries,
for which the increase in the level of service quality and the ensured degree of safety are
arguments to support the quality management system in healthcare.
For the hospital staff, the benefit is the increase in traceability and predictability of
activities, which contributes to the increase of occupational safety and determines the
possibility of professional development and increase in competences at the workplace.
For the healthcare system and financiers/insurers, the accreditation is the guarantee
of knowledge, monitoring and mitigating the functional and institutional risks.
In the accreditation process, four parties are involved:

26
3. REGISTRATION/ELIGIBILITY TERMS
The conditions wich has to be realised by users (hospitals) are:

27
4. IMPLEMENTATION OF QUALITY MANAGEMENT
In essence, the modern healthcare quality movement started 1917, when the
American College of Surgeons compiled the first set of minimal standards
based on which hospitals can identify and put right wanting services. Later on, the strategy
formed the basis for an accreditation process that, since 1951, has been managed by the
Joint Commission on the Accreditation of Healthcare Organizations. In Canada, the Canadian
Council on Health Services Accreditation – CCHSA has been fulfilling the same role since
1959.
In the `80s, inspection process failures, continuing failure to constantly
provide satisfactory quality services, and the rise in costs, alongside the
emergence of industrial management models, caused developed countries to reassess the
accreditation and standards based quality concept. Healthcare organisations in USA began to
test industrial Continuous Quality Improvement (CQI) and Total Quality Management (TQM)
philosophies, initiated in 1949 by Japanese engineers.
As a result, the accreditation process moved on from passive inspections to ascertain
quality to driving and implementing the quality improvement concept.
In 1991, the UK National Healthcare Service adopted a formal quality policy
and the quality improvement concept and translated it into healthcare
practice.
In 1966, Avedis Donabedian, in his article that became of reference,
introduces the concepts of Structure, Process and Outcome that are currently
the main paradigm in healthcare quality assurance. Through his approach to quality
assessment, Donabedian completely changed the traditional view on healthcare systems;
healthcare issues will no longer be seen as a chain of unrelated events, but rather as the
outcome of a complex, process, guided by general principles.
In 1985, a group of healthcare professionals met in Udine, in Northern Italy,
to discuss the issue of quality assurance in medicine. This put the basis of
the International Society for Quality in Healthcare - ISQua). In time, by organising
conferences, printing a journal and other initiatives, ISQua became the main global promoter

28
of healthcare quality. In 1995, after an international meeting where various proposals were
presented, the decision was taken to locate the ISQua’s Secretariat General in Australia, and
its European Region branch, in Ireland. ISQua is a not-for-profit organisation and is managed
by an Executive Board that is elected every 2 years by the general Assembly of Members. The
members of the Executive Board are representatives of countries from Europe, North and
South America, Asia and the Pacific region.
Based on quality philosophies, the quality management principles were stated.
Adapted to the hospital organisation, they are:

29
In some countries, the theoretical quality model is based on the minimum acceptable
quality. In others, it is based on the highest expected level of quality, making up a number of
desiderates.
The common principle of most accreditation processes is visiting the evaluated facility,
applying evaluation tools such as direct observation, questionnaires, checking existence of
paperwork and looking for factual evidence of concern for quality and safety.
The standards, criteria and, above all the requirements (and then the measurable
markers, called indicators), are dynamic elements of the accreditation system of values. In
other words, that which today validates quality, tomorrow may become unsuitable or even
contrary. For this reason, these elements require constant assessment and adaptation to the
developments in healthcare system.
Currently, accreditation no longer represents a sum of numeric data on all the
standards. The requirements also have binary values, meaning that one or another of the
elements that combine to define the overall snapshot of a hospital and is services may be in
place or may be missing. On the other hand, the evaluation visit itself is no longer a full
inspection, limited to measuring normative quantitative values.
Today, it is considered that the level of accreditation defines the level achieved by the
organisation in terms of quality management, on the one hand, and, on the other hand, the
place that the hospital has as provider on the healthcare market and its potential for
development and continued existence on this market.
The total quality management doctrine is based on the involvement of institutional
management in increasing customer satisfaction, staff participation in decision making and
identification various stages of processes that are may be improved. Through this approach,
quality becomes the focal point of the organisation’s development and evolution, including
hospitals that, thus, gain access to funding, in a market that is regulated by local and national
healthcare and resource allocation polices.

30
5. WHAT DO THE STANDARDS BRING IN TERM OF NOVELTY
What is new in the second edition of the Hospital Standards?
Why were these amendments necessary?
Large number of indicators
- Difficult for evaluators to appraise the quality of activity
- Difficult for those evaluated to demonstrate compliance
Many indicators were not relevant for the quality of services
Certain indicators were not clearly or adequately defined or were not timely
Interpretable indicators. Evaluators could reach different interpretations, and
this influenced evaluation objectivity.
The first edition induced a formalistic approach, and led to excessive hospital
bureaucracy.
It was necessary to take into account the international hospital accreditation
standards - ISQua principles.
International recognition of the Romanian standards was necessary, by their accreditation by ISQua and in the context of Directive 2011/24/EU on the free movement of patients across the European Union.
It was necessary to update the standards according to:
- The evolution of the legislation in the field
- The developments regarding the situation in hospitals in terms of certain aspects of the healthcare services provided (poor or inadequate services which impact not only healthcare provision quality but, primarily, patient safety).

31
What was changed?
The references were reorganised, from 11 into only 3 references.
The number of standards was reduced, from 90 to 27, and of indicators, from 2226 to
1794.
The notion of “Criterion” was introduced to define the objectives of the standard.

32
The structure of the standards focused on:
The standards were formulated succinctly, trying to avoid formalism, and interpretable
or unclear wording.
The development of the second edition aimed at:
33
New elements were introduces, concepts of the “market economy”, clear definitions
of activities with risks for the patient, elements to monitor in the post-accreditation period,
such as:
The strategy for developing the package of standards relied on the following aspects:
Analysis of elements regulated by legislation whose compliance is strictly
monitored/controlled;
Analysis of negative trends in the hospital activity (especially related to
personnel and management attitudes), where, despite the fact that there were
specific regulations in place, compliance, if any, is in most cases questionable;
Identification of aspects not covered by legislation in hospital activity, including
activity authorisation (the standards have motivating requirements which exceed
legal regulations, but do not breach them);

34
Consideration of specific elements of hospital activity within the European
Union.
Alignment to natural international developments in the field of hospital
healthcare.
Reformulation of standards from the first edition according to suggestions from
ANMCS “beneficiaries” - hospitals, and from evaluators, patient
representatives, professional or employee associations.
The goal was to establish a “journey” for the structural and conceptual evolution of the
hospital:

35

36
6. MAPPING
Second edition of standards
First edition of standards
Code Enunciation Type Transposition Code Enunciation Type
01 ORGANIZATIONAL AND STRATEGIC MANAGEMENT
Ref rephrased 01
ORGANIZATIONAL AND STRATEGIC MANAGEMENT
Ref
01.01
The strategy and the strategic management of the organization are according to health care demand and to the dynamics of the healthcare services.
S rephrased 01.01
The strategy and the strategic management of the organization are according to health care demand and to the dynamics of the healthcare services.
S
01.01.01
The strategic plan is based on an analysis of the population healthcare and service market needs.
Cr New criteria
01.01.01.01
The organization has performed / used an analysis of the related population healthcare needs and of the market of healthcare services in the assigned territory.
R New requierment
01.01.01.02
The results of the analysis of the population healthcare needs and of the market of healthcare services are used in establishing the strategic objectives of the hospital.
R New requirement
01.01.02
The strategic plan designed by the hospital is supported at all decision levels.
Cr New criteria
01.01.02.01
The strategic plan is based on the identified available and potential resources.
R criterion taken as a requirement
01.01.01
The strategic plan of the institution is based on coherent planning and periodic evaluation of the actions
Cr

37
01.01.02.02
The strategic plan aims to improve the quality of services and patients’ safety.
R criterion taken as a requirement
01.01.02
The institution's strategic plan is to provide full care to its patients
Cr
01.01.02.03
The objectives of the strategic plan are acknowledged by all the structures involved in their achievement.
R New requierment
01.01.03
The strategic plan is implemented with the participation of all the activity sectors
Cr rephrased 01.09.01 Objectives are regularly evaluated and adjusted accordingly
Cr
01.01.03.01
At the hospital level there is an active team responsible for periodical evaluations of the level of implementation of the strategic objectives.
R
01.01.03.02
The heads of all the activity sectors periodically analyze the level of achievement of the strategic objectives.
R criterion taken as a requirement
01.01.03
The director Committee and the Institutions' Councils participate in the development, implementation and evaluation of the Strategic Plan
Cr
01.01.03.03
The annual planning of the activities takes into account the established strategic objectives.
R New requirement
01.01.04
The strategy of the clinical institutions and of the clinical hospitals includes the development of the scientific research sector.
Cr New criterion
01.01.04.01
Scientific research takes into account the development objectives of the hospital.
R New requirement
01.01.04.02
Innovation through research improves the quality and performance of the medical activity.
R New requirement
01.01.04.03
The medical institute coordinates the innovation/research activity of hospitals that
R New requirement
38
operate in the field.
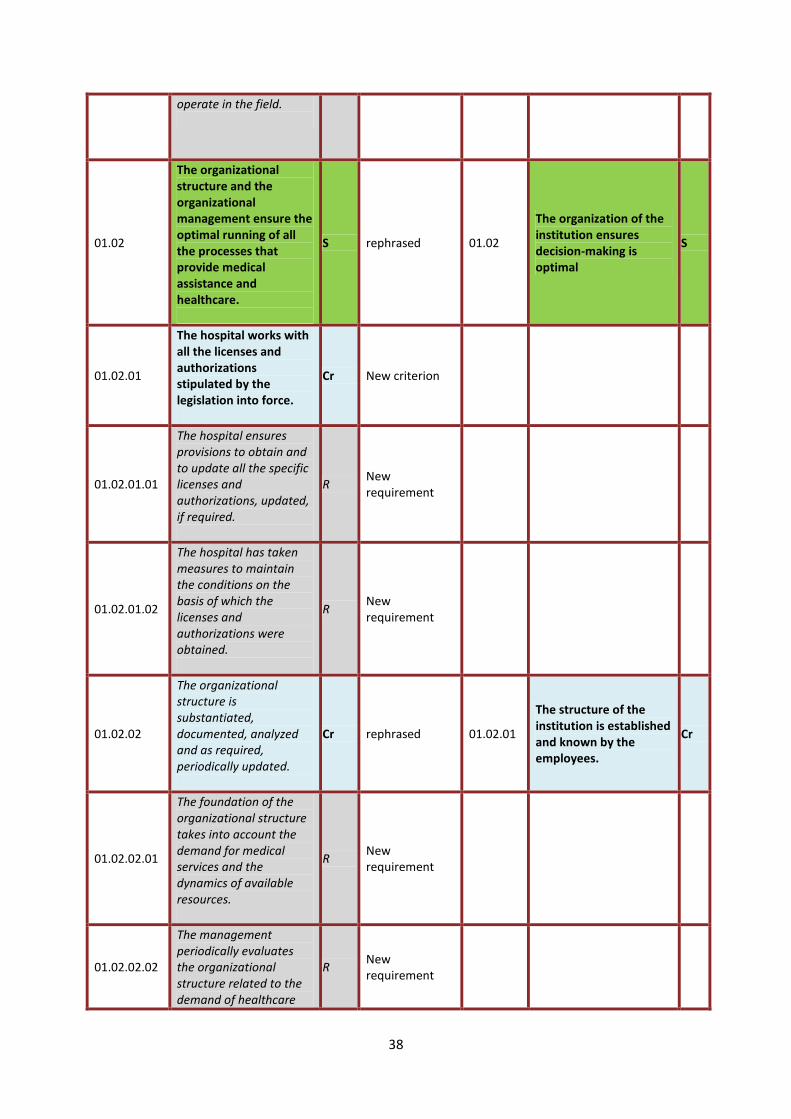
01.02
The organizational structure and the organizational management ensure the optimal running of all the processes that provide medical assistance and healthcare.
S rephrased 01.02
The organization of the institution ensures decision-making is optimal
S
01.02.01
The hospital works with all the licenses and authorizations stipulated by the legislation into force.
Cr New criterion
01.02.01.01
The hospital ensures provisions to obtain and to update all the specific licenses and authorizations, updated, if required.
R New requirement
01.02.01.02
The hospital has taken measures to maintain the conditions on the basis of which the licenses and authorizations were obtained.
R New requirement
01.02.02
The organizational structure is substantiated, documented, analyzed and as required, periodically updated.
Cr rephrased 01.02.01
The structure of the institution is established and known by the employees.
Cr
01.02.02.01
The foundation of the organizational structure takes into account the demand for medical services and the dynamics of available resources.
R New requirement
01.02.02.02
The management periodically evaluates the organizational structure related to the demand of healthcare
R New requirement

39
services.
01.02.02.03
The management periodically analyses the organizational development process at and updates the organizational structure accordingly
R New requirement
01.02.03
The functional structures of the hospital (commissions, committees, councils) are operational, ensuring process integration and the consolidation of the management quality control.
Cr merged and rephrased criteria
01.02.02 The Board of Directors (C.A.) exercises its duties constantly
Cr
01.02.03
The Steering Committee (C.D.) and the Ethics Council are required according to their competencies.
Cr
01.02.03.01
The functional structures of the hospital (commissions, committees, councils) have been established and are active.
R New requirement
01.02.03.02
The activity of the functional structures (commissions, committees and councils) of the hospital substantiates the decision-making process.
R New requirement
01.03
The human resources management ensures staff recruitment according to the mission stated by the hospital.
S reference taken as a standard
03 HUMAN RESOURCES MANAGEMENT
Ref
01.03.01
The human resource policy is documented and adapted to the needs of the unit organization and functioning.
Cr standard taken as a criterion
03.03 The employment policy is tailored to the needs of the institution
S
01.03.01.01
The hospital management establishes the need of staff according to the volume
R merged and rephrased criteria
03.01.01
The human resources development strategy is in line with the institution's needs
Cr

40
of activity in order to optimize the services provision process, while taking into account the staffing norms.
03.02.01
The institution provides a human resources structure in line with its objectives
Cr
03.09.01 The institution shall continuously assess the working conditions
Cr
03.09.02 The institution has a plan to improve working conditions
Cr
01.03.01.02
The hospital management annually analyzes the position structure and makes adequate provisions for its adaptation to the identified needs.
R reformulatted 03.02.02
The organization of human resources is based on the planning and assessment of the institution's needs
Cr
01.03.01.03
The hospital management ensures that a Yearly Plan of selection, recruitment and professional development of the staff is elaborated and implemented.
R criterii comasate si reformulate
01.08.02
The sector manager is concerned with increasing the professional level of the subordinate staff
Cr
03.01.01
The human resources development strategy is in line with the institution's needs
Cr
03.03.01
Organizing hiring competitions in accordance with the institution's development plan
Cr
03.05.01
The work of staff representation structures is carried out properly
Cr
01.03.01.04
The continuous vocational training is based on a plan that is adequate to the specific and needs of the unit, while including the financing sources.
R merged and rephrased criteria
03.01.03 The human resources department has clearly defined tasks
Cr
03.06.02
The institution assesses the needs of staff in relation to their own professional development
Cr
03.07.01
The institution is concerned with the professional training of all staff employed
Cr
03.07.02 The training program is tailored to the needs of the organization
Cr

41
01.03.02
The need of staff is established according to the technical capacity, hotel accommodation, addressability, treated morbidity, staff norms and to the working time audit, if required.
Cr rephrased 03.01.02
The human resources policy takes into account the institution's professional qualification level
Cr
01.03.02.01
The need for medical and auxiliary staff in the bed sections / compartments is established according to the degree of dependence of the categories of treated patients.
R criterion taken as a requirement
01.07.01
The organizational structure of the sectors of activity is constantly adapted to the needs of the patient's care
Cr
01.03.02.02
The need of staff is estimated in order to ensure the use of the existing technical resources at optimal capacity.
R New requierment
01.03.02.03
The staff working in the unit is qualified and authorized, according to the law.
R merged and rephrased criteria
03.04.01
Fundamental information about the institution is presented to the new employee
Cr
03.04.02
The institution ensures for each new employee the necessary training for the protection of the work and the quality of the provided services
Cr
03.06.01 The institution has periodic staff evaluation procedures
Cr
03.10.02
Heads of medical services have responsibilities for human resources management within the department
Cr
01.03.03
Personnel policy motivates employees and determines quality improvement.
Cr rephrased 01.09.02
The results and performance of the hospital are subject to constant communication within the organization
Cr

42
01.03.03.01
The employees are involved in the decision-making process and impact how attributions are performed while submitting to the social dialogue mechanisms.
R New requirement
01.03.03.02
The employees’ level of satisfaction is evaluated periodically.
R New requirement
01.03.03.03
The hospital ensures compliance with the quality of professional life requirements.
R New requirement
01.04
The financial and administrative management responds to the strategical and operational objectives of the hospital.
S rephrased 01.04 The activity of the institution is based on budget forecasts
S
01.04.01
The hospital has a financial strategy regarding development.
Cr Merged and rephrased requierments
01.04.01 The institution has a financial strategy
Cr
04.01.01
The institution has a strategy for procurement in the technical adminis- trative field
Cr
01.04.01.01
The investments are established according to the strategic objectives regarding the hospital development, taking into account the satisfaction of the served community needs or the attraction of new consumers.
R New requierment
01.04.01.02
The hospital establishes an annual plan of investments that complies to the approved budget.
R New requierment
01.04.02
The income and expenditure budget of the hospital supports the achievement of the annual plan of services.
Cr New criterion

43
01.04.02.01
The income and expenditure budget of the hospital is developed by justifying expenditures.
R criterion taken as a requirement
01.04.01 The institution has a financial strategy
Cr
01.04.02.02
The hospital periodically analyses incomes in relation to the incurred expenditures.
R criterion taken as a requirement
01.04.02
Professionals are involved in the development of budgetary policy
Cr
01.04.03
The budget is periodically updated from the perspective of streamlining the service delivery process.
Cr rephrased 04.01.02
The institution's specialized technical staff is involved in the procurement strategy
Cr
01.04.03.01
The hospital has implemented a methodology of monitoring the cost of medical services.
R criterion taken as a requirement
01.04.02
Professionals are involved in the development of budgetary policy
Cr
01.04.03.02
The hospital periodically analyses the process of service delivery with the participation of all management levels.
R merged and rephrased criteria
01.04.03
Investments are set in accordance with the objectives of the institution and with a view to satisfying the needs of the community served or attracting new consumers
Cr
01.08.01
The situation of the allocation of funds for each sector of activity is known by its manager
Cr
01.04.04
The supply of the activity sectors ensures continuity in service delivery.
Cr standard taken as a criterion
01.05 The institution has mechanisms to oversee its management
S
01.04.04.01
The hospital ensures the inventory and monitoring of the critical products and services.
R merged and rephrased criteria
01.04.03
Investments are set in accordance with the objectives of the institution and with a view to satisfying the needs of the community served or attracting new consumers
Cr
04.01.04
The institution has adapted procedures for the various emergency situations
Cr

44
04.02.02
The institution ensures the functionality of the equipment, installations and buildings
Cr
04.02.04
The institution provides repairs to equipment, installations and buildings
Cr
01.04.04.02
The hospital performs a periodical analysis of the stocks.
R merged and rephrased criteria
01.05.01 Methods of controlling the management are met
Cr
04.01.01
The institution has a strategy for procurement in the technical administrative field
Cr
01.04.04.03 Supply of business sectors is related to consumption.
R merged and rephrased criteria
01.05.01 Methods of controlling the management are met
Cr
04.01.01
The institution has a strategy for procurement in the technical administrative field
Cr
09.02.02
The institution monitors and controls the risks generated by medical equipment
Cr
01.04.04.04
The hospital ensures the product supply and services for exceptional cases.
R criterion taken as a requirement
04.01.04
The institution has adapted procedures for the various emergency situations
Cr
01.05
The information system responds to information needs and determines their effective use in the hospital.
S reference taken as a standard
02 OPERATIONAL INFORMATION MANAGEMENT
Ref
01.05.01
The information system provides the necessary data for the documentation of hospital activities.
Cr standard taken as a criterion
02.01
The information system corresponds to the institution's needs
S
01.05.01.01
The information system integrates information needs and external requests (formal or informal) from all activity sectors.
R
criterion taken as a requirement
02.01.01
The development of the information system and the computerization of the institution are correlated with the institution's data and information needs
Cr

45
01.05.01.02
The information system administration ensures its adaptation to the requirements of the hospital activity.
R
criterion taken as a requirement
02.01.02
The institution's information system allows assessment of the achievement of the objectives of the strategic plan
Cr
01.05.02
Circuits and information flows support the conduct of activities and the decision-making process.
Cr rephrased 02.03.02
The management establishes the objectives of the service of processing information and documents
Cr
01.05.02.01
Circuits and information flows ensure that data is transmitted in the required and timely format.
R
criterion taken as a requirement
07.05.01
Medical data is available at all times to staff involved in patient care
Cr
01.05.02.02
Circuits and information flows contain alert systems that prevent the occurrence of decisional errors.
R new requirement
01.05.03
Information processes underpin effective decisions within the hospital.
Cr rephrased 02.03.04
The Information and Document Processing Service is responsible for the quality of medical data and the information system
Cr
01.05.03.01
The data carrier for each activity in the hospital (paper-based, magnetic, electronic) and the flow of information are clearly defined and respected.
R new requirement
01.05.03.02
The operability of the implemented informational procedures ensures that hospital activity is more efficient.
R new requirement
01.05.04
The information system and the data storage environment ensure the confidentiality, integrity and security of the data.
Cr standard taken as a criterion
02.02
Information management respects privacy and data security
S

46
01.05.04.01
The hospital respects the law in force regarding data security.
R
merged and rephrased criteria
02.02.01
The confidentiality of patient and employee data is ensured at all times
Cr
03.08.01
The institution has a secured personal data management system
Cr
03.08.03
The institution guarantees the confidentiality of the staff data
Cr
06.07.01
Institution guarantees the patient's anonymity and confidentiality
Cr
01.05.04.02
Access to information, their processing and protection is regulated for each professional category.
R
merged and rephrased criteria
02.02.02
Access to patient data and security of this data is ensured
Cr
03.08.01
institution has a secured personal data management system
Cr
03.08.03
The institution guarantees the confidentiality of the staff data
Cr
07.01.04
The patient has guaranteed access to their own file, either directly or through a designated person
Cr
01.05.04.03
The hospital provides back-up information systems
R merged and rephrased criteria
02.04.02
The institution ensures the functionality of the information system
Cr
03.08.01
The institution has a secured personal data management system
Cr
01.05.04.04
The hospital monitors and controls the use of information systems.
R new requirement
01.05.04.05
Preservation and archiving of documents, information and records ensures the confidentiality, integrity
R merged and rephrased criteria
02.02.03
The institution protects the information resulting from the processing of patient
Cr

47
and security of the data.
data
03.08.01
Institution has a secured personal data management system
Cr
03.08.03
The institution guarantees the confidentiality of the staff data
Cr
06.07.01
Institution guarantees the patient's anonymity and confidentiality
Cr
07.03.01
The institution clearly defines the duties of the staff related to the patient file
Cr
07.03.03 Conditions for archiving patient files are ensured
Cr
07.05.02
Patient data are kept under the specified security and duration
Cr
01.05.04.06
Destruction of documents / records is performed while taking into confidentiality and data security.
R
criterion taken as a requirement
07.03.03 Conditions for archiving patient files are ensured
Cr
01.05.05
The information system provides documentation and supports the educational process of hospital employees.
Cr new requierment
01.05.05.01
The information system provides documentation and information to hospital employees.
R new requierment
01.05.05.02
The information system supports the process of training and professional development of hospital employees.
R new requierment

48
01.06
The existing communication system of the hospital meets needs of the organization and of the beneficiaries.
S rephrased 01.03
Internal and external communication strategy of the institution is viable
S
01.06.01
External communication meets the needs of the beneficiaries and of the hospital.
Cr new requierment
01.06.01.01
The hospital has diversified the communication channels for the public.
R
merged and rephrased criteria
01.03.01 Institution has an internal communication policy
Cr
06.01.03
Institution is concerned that information of interest will become public
Cr
08.02.08
Institution is involved in the program to prevent and combat the effects of tobacco products
Cr
01.06.01.02
The hospital's website ensures effective communication.
R
merged and rephrased criteria
06.01.03
Institution is concerned that information of interest will become public
Cr
06.03.02
Access to the practical information on the stay is ensured for the patient and the homeowner
Cr
06.03.03
Financial administrative information is made available to the patient
Cr
01.06.01.03
The hospital provides the necessary conditions for easy orientation.
R
merged and rephrased criteria
06.01.02
Primary orientation information is appropriately signaled outside and inside the institution
Cr
06.06.03
Institution provides unlimited access of the patient to the hospital, except for the risk sectors
Cr

49
01.06.01.04
The hospital provides the necessary conditions for staff identification.
R Criterion taken as requierment
06.03.04
The institution provides an information system on the professional status and identity of medical staff
Cr
01.06.01.05
Communication with the media provides information to the public and the promotion of the hospital.
R
merged and rephrased criteria
01.03.02 Institution has a public relations strategy
Cr
06.01.03
Institution is concerned that information of interest will become public
Cr
06.07.03 Media access to the hospital is regulated
Cr
01.06.01.06
The hospital provides information on the medical work that is being performed.
R
merged and rephrased criteria
01.03.02 Institution has a public relations strategy
Cr
06.01.03
Institution is concerned that information of interest will become public
Cr
06.03.02
Access to the practical information on the stay is ensured for the patient and the homeowner
Cr
06.03.06
The relatives receive information about pacient care participation
Cr
01.06.01.07
External communication is achieved with the continuity of the healthcare process.
R
merged and rephrased criteria
06.01.03
Institution is concerned that information of interest will become public
Cr
06.03.05
The patient is informed of the social and medical services they can benefit from after discharge
Cr
01.06.01.08
The hospital ensures communication with other healthcare units and administrative structures.
R Criterion taken as requierment
06.03.05
The patient is informed of the social and medical services they can benefit from after discharge
Cr
01.06.02
Internal communication responds to the needs of the patients and of the hospital.
Cr rephrased 01.03.01 The institution has an internal communication policy
Cr
01.06.02.01
The hospital has implemented models of professional communication between medical team members.
R Criterion taken as requierment
03.05.02
Formal and informal communication is promoted within the organization
Cr

50
01.06.02.02
The hospital has established and uses specific communication protocols between professionals.
R
merged and rephrased criteria
03.05.02
Formal and informal communication is promoted within the organization
Cr
07.02.02 Updating files is kept confidential
Cr
01.06.02.03
The internal rules are communicated to the staff and to the patients.
R Criterion taken as requierment
06.01.01
The institution has brought to the attention of staff and patients the legal provisions on patient rights
Cr
01.06.03 Communication aims to involve the patient in the healthcare process.
Cr rephrased 01.03.01 The institution has an internal communication policy
Cr
01.06.03.01
Communication between employees and the patients / guardians aims to educate them to be involved in taking and observing therapeutic decisions.
R
merged and rephrased criteria
06.04.01
Information is provided directly to the patient or his / her appointed representative
Cr
06.05.02
The patient is involved in making decisions about their care and treatment
Cr
06.06.06
The institution respects the patient's refusal to admit or continue treatment
Cr
06.10.01
The institution is concerned with informing and educating its patients
Cr
08.04.04
The patient benefits from education related to maintaining his / her health
Cr
01.06.03.02
The hospital annually reviews the efficiency and effectiveness of communication.
R Criterion taken as requierment
05.04.03
The institution ensures continuous monitoring and evaluation of internal and external communication systems
Cr
01.07
The service quality management system is operational and ensures that all the processes related to monitoring and quality improvement are performed.
S
reference taken as a standard
05 SERVICES QUALITY MANAGEMENT
Ref
rephrased 01.07
The business sectors are involved in achieving the quality objectives of the institution
S

51
01.07.01
The quality management system aims to continuously optimize processes within the organization.
Cr new criterion
01.07.01.02
The hospital management ensures the organization of the service quality management system.
R merged and rephrased criteria
01.07.02
The competencies and areas of responsibility of Heads of industry are defined
Cr
05.01.01
Institution leadership and business sectors define their policy of quality
Cr
05.01.04 The institution defines responsibilities for quality management
Cr
01.07.01.03
The Quality of Service Management structure coordinates the process of ensuring and improving the quality of patient health and safety services in collaboration with the heads of all sectors of activity.
R merged and rephrased criteria
01.07.03
Managers of the business sectors ensure continuous quality evaluation and improvement
Cr
05.01.02
The quality management program has precise quantifiable targets.
Cr
05.01.03
The institution has an information policy on the objectives and results of the quality of service management
Cr
05.03.03 Hospital ambulatory is involved in increasing the quality of care
Cr
01.07.01.04
The hospital is concerned with the quality certification of its activities.
R criterion taken as a requirement
05.01.01
Institution leadership and business sectors define their policy of quality
Cr
01.07.02
The quality management structure (QMS) and the hospital management promote a culture of quality in the hospital.
Cr new criterion
01.07.02.01
The hospital has established and observes of the principles and values of quality, in agreement with the stated mission.
R criterion taken as a requirement
05.01.01
Institution leadership and business sectors define their policy of quality
Cr
01.07.02.02 The hospital is concerned with the implementation
R merged and rephrased
05.01.04 The institution defines responsibilities for
Cr

52
and development of a quality culture in the hospital.
criteria quality management
05.01.05 Quality of Care Management Policy is about staff training
Cr
01.07.03
The hospital develops and implements an action plan to ensure and improve the quality and safety of patient services across the entire hospital.
Cr rephrased 05.03.02
There are multidisciplinary teams involved in quality improvement actions
Cr
01.07.03.01
The annual planning of the QMS activities ensures compliance with the requirements of accreditation standards.
R
criterion taken as a requirement
08.15.01
The institution is constantly assessing the professional performance
Cr
01.07.03.02
The action plan for the implementation of quality management services
R
criterion taken as a requirement
08.15.01
The institution is constantly assessing the professional performance
Cr
01.07.03.03
QMS monitors the implementation of the action plan to ensure and improve service quality and patients safety.
R
merged and rephrased criteria
01.06.01
The services provided by each department and department are monitored and evaluated
Cr
05.04.01
Institution ensures continuous monitoring and evaluation of the quality of care
Cr
05.04.04
Institution benefits from the results of monitoring and evaluating the quality of the services provided
Cr
08.15.02
Institution and each department monitors performance indicators and assesses the performance and outcomes of care work
Cr
08.15.03 Sentinel events are recorded and analyzed
Cr
01.07.03.04
Based on QMS recommendations, the hospital takes steps to improve the quality of
R
merged and rephrased criteria
01.06.01
Services provided by each department and department are monitored and evaluated
Cr

53
health care and patient safety.
05.04.04
Institution benefits from the results of monitoring and evaluating the quality of the services provided
Cr
08.15.02
Institution and each department monitors performance indicators and assesses the performance and outcomes of care work
Cr
01.07.04
The hospital aims to increase the level of the patients’ satisfaction.
Cr standard taken as a criterion
07.02 Quality policy is based on patient needs
S
01.07.04.01
The hospital designs and periodically updates patient satisfaction questionnaires.
R
criterion taken as a requirement
05.02.01
institution identifies the needs of patients and patients and assesses their degree of satisfaction
Cr
01.07.04.02
QMS systematically analyses information resulted from the processing of questionnaires and issues recommendations.
R
merged and rephrased criteria
05.02.02
Improving service quality is based on the implementation of improvement measures
Cr
05.02.03
The institution communicates to its specialists the information derived from the processing of patient satisfaction data
Cr
01.07.04.03
The hospital uses periodic analysis of complaints received to improve the provided medical services.
R
merged and rephrased criteria
05.02.04
The institution improves quality by developing a system for collecting and analyzing complaints and / or complaints
Cr
06.01.04
The institution provides patients and visitors with a register of complaints and suggestions
Cr
06.09.01
The institution facilitates the expression of patient suggestions, complaints and/or complaints
Cr
06.09.03
All complaints and/or complaints from patients are analyzed and received a response
Cr
01.07.05
The Quality Improvement Program comprises the effectiveness of the hospital activity.
Cr merged and rephrased criteria
01.07.03
Managers of the business sectors ensure continuous quality evaluation and improvement
Cr

54
05.03.01
Service efficiency policy is made in the order of priorities
Cr
01.07.05.01
An evaluation means of the efficiency quality improvement processes in the hospital is established.
R new requierment
01.07.05.02
The results of QMS evaluations are used in order to streamline activities.
R new requierment
01.08
Non-clinical risk management prevents damage and underpins decision-making process.
S rephrased 09.01
There is a policy of preventing and managing risks and unwanted events
S
01.08.01
All management levels have implemented risk management provisions that are specific to their own activity.
Cr new criterion
01.08.01.01
All department managers have organized the identification, analysis and treatment of risks.
R merged and rephrased criteria
09.01.01
The management of the institution together with the specialists defines the risk prevention policy
Cr
09.01.03 The institution defines and monitors the different risk categories
Cr
01.08.01.02
The hospital has a risk register and monitors the effectiveness of the prevention measures.
R merged and rephrased criteria
09.01.02 The risk prevention program has precise, measurable objectives
Cr
09.01.04 Staff training policy also addresses risk prevention
Cr
01.08.01.03
The hospital management performs risk analyses based on type, occurrence probability and impact and implements customized measures.
R merged and rephrased criteria
09.01.01
The management of the institution together with the specialists defines the risk prevention policy
Cr
09.01.03 The institution defines and monitors the different risk categories
Cr
01.08.02
Non-clinical risk management ensures that patients, employees and visitors are protected against potential damage.
Cr standard taken as a criterion
04.02
The institution ensures the safety and maintenance of equipment, installations and buildings
S

55
01.08.02.01
The places and conditions with potential of physical risk for the persons’ safety (risk of falling down, of slipping, of hitting, etc.) have been identified and preventive measures have been implemented.
R merged and rephrased criteria
08.09.01
The institution provides and evaluates the facilities needed for surgical and birth procedures
Cr
09.03.01
The institution guarantees that its processes are not harmful to the physical environment
Cr
09.04.01
Information on infrastructure and undesirable events is collected
Cr
09.04.02
There is concern about the reduction of infrastructure risks in the event of unwanted events
Cr
10.08.01
There are measures to reduce the risk of contamination of the hospital environment
Cr
01.08.02.02
Waste management respects the prevention of toxic and infectious contamination rules.
R merged and rephrased criteria
04.07
Waste management complies with the principles of hygiene and protection of people and the environment
S
09.03.01
The institution guarantees that its processes are not harmful to the physical environment
Cr
09.03.03 The institution monitors and controls the risks to the environment
Cr
01.08.02.03 The operation of the vital services of the hospital is ensured.
R
criterion taken as a requirement
10.08.02
The staff is trained to observe the procedures for the protection of the in-hospital environment
Cr
01.08.02.04
The capacity and number of elevators comply with the volume, types and flows of hospital transport.
R new requierment
01.08.02.05
Protection and security measures for goods and people have been adopted by the hospital.
R
Standard/ criterion taken as a requirement
04.08
The institution ensures measures for the safety of patients and their assets as well as their own staff
S

56
06.06.02
The institution has procedures regarding the patient's access to his / her assets
Cr
09.05 There is a policy on patrimony security
S
01.08.02.06 The hospital implements measures to manage earthquake risk.
R merged and rephrased criteria
04.02.01
The institution shall periodically assess the technical condition of the equipment, installations and buildings
Cr
09.04.01
Information on infrastructure and undesirable events is collected
Cr
01.08.02.07
The hospital implements measures to manage fire risk.
R
Standard/ criterion taken as a requirement
04.09
The institution takes measures to ensure people's security through a fire prevention and evacuation plan
S
05.10.06 The institution shall assess the fire-fighting capacity
Cr
09.04.01
Information on infrastructure and undesirable events is collected
Cr
09.06.01
Assess the effectiveness of the fire prevention and fire-fighting program
Cr
01.08.02.08
The hospital implements measures to manage explosion risk.
R criterion taken as requierment
09.04.01
Information on infrastructure and undesirable events is collected
Cr
01.08.02.09
The hospital implements measures to manage the risk of chemical and biological contamination
R merged and rephrased criteria
09.03.02
Our own staff are prepared to avoid environmental accidents by toxic substances and emissions (chemical and radioactive)
Cr
09.03.03 The institution monitors and controls the risks to the environment
Cr
09.04.01
Information on infrastructure and undesirable events is collected
Cr

57
10.06.01
The institution shall define and implement measures to prevent contamination with pathogens in biological products
Cr
01.08.02.10
The hospital implements measures to manage radiation risk.
R criterion taken as requierment
09.03.02
The personal staff is prepared to avoid environmental accidents by toxic substances and emissions (chemical and radioactive)
Cr
01.08.02.11
The hospital implements measures for the employees’ physical safety.
R merged and rephrased criteria
10.06.03
The institution provides immunization of specialists with regard to infectious risk
Cr
10.06.04
The institution takes measures to prevent contamination of its specialists
Cr
01.08.02.12
Those responsible for technological risk prevention are nominated by decision and trained in this respect.
R merged and rephrased criteria
02.04.02
The institution shall ensure the functionality of the information system
Cr
09.02.03
The institution shall ensure the maintenance and proper use of the equipment
Cr
10.07.02
The personnel is trained in the use and maintenance of multi-purpose tools and equipment
Cr
01.08.02.13
The personnel who are exposed to risk are regularly trained on compliance with risk-prevention measures that specific to each activity.
R merged and rephrased criteria
04.02.03
The institution provides staff trained for the current maintenance of equipment, installations and buildings
Cr
09.02.01
The institution is concerned with the training of specialists designated for the use of medical devices, instruments and devices
Cr
10.06.01
The institution shall define and implement measures to prevent contamination with pathogens in biological products
Cr
10.07.02
The personnel is trained in the use and maintenance of multi-purpose tools and
Cr

58
equipment
01.08.02.14
The hospital management undergoes periodic evaluations on physical and technological risk prevention measures.
R criterion taken as requierment
09.04.03
Undesirable events are analyzed and improvement measures are taken
Cr
01.08.03
The means of action, responsibilities and resources available for exceptional situations are organized and regulated to ensure the hospital's functionality. Cr
Standard/ criterion taken as a requirement
09.01.05
The institution monitors the risk prevention policy and informs the staff about them.
Cr
09.06
There are evaluation and intervention programs for emergencies, disasters, natural disasters
S
01.08.03.01
Hospital intervention teams for disasters or catastrophes have been updated.
R merged and rephrased criteria
04.02.05
Warning systems allow rapid intervention in case of damage to equipment and installations
Cr
09.06.03
The institution monitors the intervention program for situations of high gravity
Cr
09.06.02
The institution is aware of its responsibilities in situations of disasters or natural disasters
Cr
01.08.03.02
Within the hospital, there is a reserve of resources available in the event of natural disaster and catastrophe.
R new requierment
01.08.03.03
The hospital holds an inventory of resources designed for specific tasks in the event of mobilization and war.
R new requierment

59
01.09
The environment of care provides the necessary conditions for healthcare.
S new standard
01.09.01
The environment of care is organized to comply with the hospital's capacity and competencies.
Cr new criterion
01.09.01.01
Patient accommodation conditions meet the particularities of each patient.
R merged and rephrased criteria
04.10.01
The institution continually assesses and improves hotel conditions
Cr
08.02.02 Serviciile administrative sunt implicate în primirea pacienţilor
Cr
08.02.07
The institution provides solutions for the accommodation of the relatives
Cr
08.05.04
There is a concordance between the patient's state of health and the hotel conditions
Cr
08.09.01
The institution provides and evaluates the facilities needed for surgical and birth procedures
Cr
08.09.02
The institution provides and evaluates the facilities needed to care for patients in the ATI service
Cr
08.09.03 The institution provides safety systems for intraoperative patients
Cr
01.09.01.02
Care is provided with respect for the right to privacy.
R criterion taken as a requirement
06.06.01
The right to privacy of the patient is respected throughout the period of hospitalization
Cr
01.09.01.03
Patients circulate in a safe and comfortable way on well-established routes.
R
standard / criterion taken as requirement
04.06 Specific transport circuits are organized and coordinated
S
04.10.05
The institution continually assesses and improves the services for the transport of patients, visitors and staff
Cr

60
08.06.04 Patient transport within the hospital contributes to the continuity of care
Cr
01.09.01.04
Cleaning and disinfection of spaces and equipment is regulated and monitored.
R
standard/ criterion taken as requirement
04.05
The institution ensures the safety and hygiene of the premises and equipment
S
10.08.02
The staff is trained to observe the procedures for the protection of the in-hospital environment
Cr
01.09.01.05 The institution ensures and assumes the quality of sterilization.
R criterion taken as requirement
10.07.01 The institution ensures the quality of sterilization
Cr
01.09.01.06
The patients’ meals are established in accordance with the hygienic-dietary recommendations corresponding to pathology.
R
merged and rephrased criteria
04.03.01
The institution provides qualitative and quantitative nutrition to patients, carers and medical staff
Cr
04.03.04
The institution takes into consideration the expectations of medical and personal staff in setting up various menus
Cr
06.06.05
The institution respects confessional membership and facilitates the practice of religion
Cr
01.09.01.07
The institution provides qualitative and quantitative nutrition for patients, caregivers and medical staff in safe food conditions.
R
merged and rephrased criteria
04.03.01
The institution provides qualitative and quantitative nutrition to patients, relatives and medical staff
Cr
10.09.01
The kitchen of the institution respects the rules of hygiene and quality
Cr
01.09.01.08
The institution ensures the circulation of food in compliance with hygiene rules. .
R
merged and rephrased criteria
04.03.02
The institution provides food circuits to consumers in compliance with hygiene rules
Cr
10.09.01
The kitchen of the institution respects the rules of hygiene and quality
Cr
01.09.01.09
The institution provides qualitative and quantitative linen, laundry and effects for patients, caregivers and
R criterion taken as requirement
04.04.01
The institution provides qualitative and quantitative linen, laundry and effects for patients, caregivers and
Cr

61
medical staff. medical staff.
01.09.01.10 The institution ensures that the circulation of linen, laundry and effects complies with hygiene rules.
R
merged and rephrased criteria
04.04.02
Instituţia asigură sortarea lenjeriei şi a efectelor în fiecare etapă respectând regulile de igienă
Cr
04.04.05
The institution provides sorting of linen and effects at each stage in accordance with hygiene rules
Cr
01.09.02
The environment of care is evaluated and permanently adapted to the needs of healthcare.
Cr standard / criterion taken as requirement
04.10 The quality of the patient's care environment is assessed
S
05.04.02
The institution ensures the continuous monitoring and evaluation of the administrative services (the hospital component of the hospital)
Cr
01.09.02.01
The institution continually evaluates and improves patient accommodation conditions.
R criterion taken as requirement
04.10.01
The institution continually assesses and improves hotel conditions
Cr
01.09.02.02
The institution continually evaluates and improves food services.
R
merged and rephrased criteria
04.03.03
Patients' expectations and nutrition requirements are taken into account and evaluated periodically to ensure quality food
Cr
04.10.04
The institution continuously assesses and improves food supply and storage services and food preparation services
Cr
01.09.02.03
The institution continually evaluates and improves the laundry service.
R
merged and rephrased criteria
04.04.04
The evaluation of the quality of lingerie and effects is constantly achieved
Cr
04.10.03
The institution continually assesses and improves the laundry service
Cr
01.09.02.04 The institution con-stantly evaluates and im-proves the environment.
R criterion taken as requierment
04.10.02 The institution constant-ly assesses and human-izes the environment
Cr

62
02 CLINICAL MANAGEMENT
Ref rephrased 08
HEALTH CARE
MANAGEMENT Ref
02.01
Patients are cared for according to their needs, to the mission and available resources of the hospital.
S new standard
02.01.01
The hospital has established the technical and professional competency level.
Cr new criterion
02.01.01.01
The hospital evaluates the population groups of patients with clinical-biological particularities, in order to identify and satisfy their needs and specific pathologies.
C Criterion taken as a requierment
01.02.04
The needs of the medical services of the population underlie the proposals made by the medical council regarding the development of the hospital activity
Cr
02.01.01.02 The hospital has identified pathologies for which it has resources.
C new requierment
02.01.02
Access to healthcare services is facilitated according to patient caregiving needs.
Cr standard taken as a criterion
08.01 The institution has a policy for receiving and highlighting patients
S
02.01.02.01
The hospital has regulated appointments and consultations for patients.
R
merged and rephrased criteria
08.01.02
The institution organizes the accommodation and the establishment of the first care measures
Cr
08.02.01 The Patient Reception Service is permanently insured
Cr
08.02.06 The institution plans admissions of patients with chronic conditions
Cr
02.01.02.02
The patient scheduling system is organized so as not to infer with emergency healthcare interventions.
R new requierment
02.01.03
The hospital has organized the emergency medical service.
Cr rephrased 08.01.01
The institution has the necessary facilities for receiving, registering and admitting patients
Cr

63
02.01.03.01
The hospital permanently ensures the emergency medical services, within the limits of its competencies.
R Criterion taken as a requierment
08.06.03
Vital emergency management in the institution is being carried out
Cr
02.01.03.02
The medical staff employed in the Emergency Receiving Unit / Primary Emergency compartment (ER/EC) is qualified according to law and is periodically trained, especially as regards the attitude in the lower incidents.
R new requierment
02.01.03.03
The emergency service (the emergency ward / UPU / CPU) is organized efficiently and effectively.
R
merged and rephrased criteria
06.02.01 The institution provides appropriate care in all emergencies
Cr
0802.03
The institution has organized the emergency service for the triage, investigation and stabilization of patients in serious condition
Cr
08.02.05
The institution aims at reducing the waiting time until the care is taken
Cr
02.01.04
The hospital provides services adapted to people with disabilities, special needs or aggressive manifestations.
Cr rephrased 06.02.02 The rights of people with special needs are respected
Cr
02.01.04.01
The patient with disabilities or special needs has adequate reception conditions.
R
merged and rephrased criteria
06.03.01
The institution fulfills the conditions for communicating with patients
Cr
06.06.05
The institution respects confessional membership and facilitates the practice of religion
Cr
08.04.01
Situations requiring special care are identified for the patient
Cr

64
02.01.04.02
The hospital is prepared for the management of the patient with aggressive behaviour.
R new requierment
02.01.05
Psychiatric hospitals or hospitals with psychiatric wards provide services adapted to psychiatric patients.
Cr new criterion
02.01.05.01
The psychiatric hospital or with psychiatric wards regulates the involuntary hospitalization of the psychiatric patient.
R new requierment
02.01.05.02
The psychiatric hospital or with psychiatric wards regulates patient internment for psychiatric forensic expertise.
R new requierment
02.01.05.03
The psychiatric hospital / with psychiatric wards regulates caregiving for arrested or convicted psychiatric patients.
R new requierment
02.01.05.04
Psychiatric hospital or with psychiatric wards has special measures to prevent and limit the consequences of behavioural manifestations of the psychiatric patient that may endanger the patient, the people around, or material goods.
R new requierment
02.01.05.05
The discharge of the psychiatric patient from psychiatric hospitals or psychiatric wards is regulated and adapted to the way of admission.
R new requierment

65
02.02
The initial evaluation aims to identify patients' needs in the context of known exposure to risk factors (environmental, social, economic, behavioural and biological) and establishes the need for care and medical care for them.
S new standard
02.02.01
The hospital clearly defines the process of patient needs assessment in order to establish the appropriate health care plan.
Cr New criterion
02.02.01.01
Depending on the patient’s initial identification, a decision regarding the patient’s admission and the means of treatment as ambulatory care / day-hospitalization / continuous hospitalization is made.
R Criterion taken as a requierment
08.03.04
The patient is initially and consistently assessed from the point of view of his health
Cr
02.02.01.02
The hospital has designed a procedure to refer patients whose pathologies fall outside of its area of competency and facilitates access to the services they need.
R Criterion taken as a requierment
08.02.04
The institution has ensured communication with partner institutions for taking patients with pathology different from their own profile
Cr
02.02.01.03
The hospital regulates the recognition of patient investigations performed by other hospital units as well as their repetition.
R new requierment
02.02.02
Initial patient evaluation includes psycho-social and socio-economic factors to ensure the continuity of caregiving.
Cr new criterion
02.02.02.01
The hospital provides treatment for patients with psycho-emotional and socio-economic peculiarities that can
R new requierment

66
affect the care process.
02.02.02.02
The patient's route through the system is determined in relation to his/her psycho-social and socio-economic profile.
R New requierment
02.02.02.03
Management of acute or chronic pain starts from the initial evaluation stage.
R Criterion taken as a requierment
08.04.02
Acute or chronic pain and mental suffering are investigated, prevented, and treated
Cr
02.03
Medical practice addresses the patient in an integrated and specific way, ensuring continuity of care and health care.
S New standard
02.03.01
The case management is based on the use of diagnostic and treatment protocols
Cr Standard taken as acriterion
08.14
The departments and departments of the institution use diagnostic and therapeutic protocols
S
02.03.01.01
Health care provisions are established according to a schedule by the treating physician.
R New requierment
2.03.01.02
The diagnostic and treatment protocols are established according to the principles medicine based on evidence, clinical experience and the technical and technical-material resources of the hospital.
R merged and rephrased criteria
05.03.04 Each section adopts specific patient care protocols
Cr
08.14.01
The institution is concerned with the development and implementation of good practice protocols
Cr
02.03.01.03
Diagnostic and treatment protocols are used individually, according to the particularities of the case.
R merged and rephrased criteria
05.03.04 Each section adopts specific patient care protocols
Cr
08.14.01
The institution is concerned with the development and implementation of good practice protocols
Cr
02.03.01.04 Evaluation of the efficiency and effectiveness of the
R merged and rephrased criteria
05.03.05 Each department monitors the use of adopted protocols
Cr

67
protocols is carried out periodically.
08.14.02
The efficiency of clinical protocols is evaluated and adjustments measures are proposed
Cr
02.03.01.05
Protocol update is performed when periodic assessment of their efficiency and effectiveness requires so, or when new good practice in the field is available.
R merged and rephrased criteria
05.03.06
The institution shall take into account national and international recommendations on care procedures
Cr
08.14.02
The efficiency of clinical protocols is evaluated and adjustments measures are proposed
Cr
02.03.02
An integrated approach to patient care is routinely performed in medical practice.
Cr new criterion
02.03.02.01
The hospital provides a multidisciplinary, complete and personalized approach of medical practice.
R standard/criterion taken as a requirement
01.06.02
The institution provides multidisciplinary consultations for solving complex problems
Cr
01.06.04
The relationships between the institutions' activity sectors allow multidisciplinary care of the patient
Cr
08.05.02 The institution provides a multidisciplinary approach to patient care
Cr
08.07
The management of the patient with surgical potential is based on communication between specialized multidisciplinary teams
S
02.03.02.02
Interdisciplinary consultations are documented and written in the clinical record sheet (CRS).
R merged and rephrased criteria
01.06.02
The institution provides multidisciplinary consultations for solving complex problems
Cr
01.06.04
The relationships between the institutions' activity sectors allow multidisciplinary care of the patient
Cr
02.03.02.03
The second medical opinion is analysed and used by the hospital to improve medical practice.
R new requirement

68
02.03.02.04
The hospital is concerned with the detection of patients with chronic kidney disease (CKD).
R new requirement
02.03.02.05
The Multidisciplinary Oncological Commission decides on the treatment of the oncological patient.
R new requirement
02.03.03 The hospital ensures the continuity of care after the initial evaluation.
Cr new criterion
02.03.03.01
The hospital ensures the necessary conditions for the continuity of care.
R merged and rephrased criteria
08.03.02
Complementary investigations and care are based on the objective clinical examination
Cr
08.05.01
Medical staff ensures complete and personalized care of the patient
Cr
08.05.03
Patient care is provided through consultation with internal and external specialists, including at the patient's request
Cr
08.06.02 Patient care is ensured permanently
Cr
02.03.03.02
The hospital provides conditions for patient access to the necessary recovery / rehabilitation services, depending on pathology.
R new requirement
02.03.04
The care plan of the patient is an integral part of the case management.
Cr new criterion
02.03.04.01
Medical staff ensures complete and personalized care of the patient.
R criterion taken as a requirement
08.03.03 The patient is involved in establishing the care plan
Cr
02.03.04.02
The individualized care plan is completed by the medical assistant, based on medical recommendations.
R new requirement
02.03.04.03 The care plan is designed according to the patient's evolution.
R criterion taken as a requirement
08.06.05
The patient's state of health is subject to regular assessments and readjustments
Cr

69
02.03.04.04
At discharge, a care plan is developed which is transmitted both to the patient / family member and the family doctor / physician who sent the patient to hospital.
R criterion taken as a requirement
08.12.02
Upon discharge, the patient receives the information and documentation necessary to continue outpatient care
Cr
02.03.04.05
The need for medical care staff is established according to the need of patient care.
R new requirement
02.03.05
Medical records are filled out correctly, completely and on time real time, avoiding redundancy, while access to them is regulated.
Cr standard taken as a criterion
07.04
The way of recording the medical data in the patient file ensures a good quality of information for the specialists
S
02.03.05.01
The hospital establishes the necessary data to be collected, recorded and monitored throughout the hospitalization period.
R criterion taken as a requirement
07.01.01 Patient care is constantly adapted to clinical development
Cr
02.03.05.02
The medical staff records information on the care that has been provided, the results of the investigations and the therapeutic recommendations according to specialty.
R standard/criterion taken as a requirement
07.01.02
The institution is concerned about progressive and constant accumulation of patient data
Cr
07.03.02 Medical records are duly completed
Cr
07.04.01 FOCG is duly completed Cr
07.04.02
The patient's health status, treatment, and progression are recorded on a daily basis in the observation sheet
Cr
07.06
Patient data management is continuously evaluated and improved
S
08.03.01 Patient route data is accessible to staff and keepers
Cr
02.04 The hospital promotes the "baby-friendly" concept (BFH).
S new standard

70
02.04.01
The hospital has adopted a policy to promote breastfeeding in neonatology departments.
Cr new criterion
02.04.01.01
The hospital supports a breastfeeding program as a healthy diet for newborn and infant feeding.
R new requirement
02.04.01.02
Mothers who are hospitalized are informed about the benefits of breastfeeding.
R new requirement
02.04.01.03
Medical staff in obstetrics-gynaecology and neonatology is continuously trained to acquire the skills needed to implement the Breastfeeding Promote Program.
R new requirement
02.04.01.04 The hospital provides facilities to promote and support breastfeeding.
R new requirement
02.04.02
The hospital is concerned with the identification and prevention of newborn illnesses.
Cr new criterion
02.04.02.01 The hospital prevents newborn infectious diseases.
R new requirement
02.04.02.02 The hospital identifies newborn malformations / deficiencies.
R new requirement
02.04.03
The hospital is concerned with ensuring a friendly climate for children.
Cr new criterion
02.04.03.01 The hospital provides conditions adapted to child care.
R criterion taken as a requirement
10.09.02
The institution is concerned with the hygiene of feeding newborns
Cr
02.04.03.02 The hospital provides support services for childcare.
R new requirement

71
02.05
The paraclinical services correspond to the investigation needs.
S rephrased 08.10
Clinical and paraclinical medical analysis laboratories as well as pathological anatomy ensure the continuity of care
S
02.05.01
The whole activity of the paraclinical services is carried out in collaboration with clinical doctors.
Cr new criterion
02.05.01.01
The sections define and estimate the need for paraclinical services depending on the hospital competency level.
R merged and rephrased criteria
08.10.01
The conditions for prescribing, taking, conducting and communicating exam results are established
Cr
08.11.03
The results of investigations as well as nuclear and rehabilitation therapies are communicated in a timely manner
Cr
02.05.01.02
The paraclinical services specialists are part of the multidisciplinary team to treat complex cases.
R criterion taken as a requirement
08.10.02
Depending on medical circumstances, the exam requirements specify the required clinical information and the objectives of the application
Cr
02.05.02
Paraclinical services respond to the needs of investigating patients in terms of accessibility, quality and time to achieve results.
Cr new criterion
02.05.02.01
Monitoring and analysis of nonconformities are used to improve paraclinical activity.
R new requirement
02.05.02.02
The reference intervals of the investigation results, the alerting values and the established critical values, are communicated at the same time with the results’ transmission.
R criterion taken as a requirement
08.10.03
The results of the examinations meet the needs of the clinical activity sectors in terms of quality and transmission period
Cr

72
02.05.02.03
The practices of radio-diagnostic, interventional radiology and functional explorations are focused on the real needs of the patient, while being monitored and evaluated periodically.
R criterion taken as a requirement
08.10.04 Mechanisms are in place to analyze the use of laboratory tests
Cr
02.05.03
The laboratory aims to meet investigation needs in optimal conditions.
Cr new criterion
02.05.03.01
The laboratory establishes solutions to meet investigation needs efficiently and effectively.
R criterion taken as a requirement
08.10.05 The institution also applies other ways to meet this standard
Cr
02.05.03.02
The hospital has regulated the necessary conditions for conducting the laboratory pre-examination and post-test procedures.
R new requirement
02.06
The Nephrology Hospital / Nephrology Department Hospital ensures the continuity of medical assistance for patients with chronic kidney disease (CKD).
S new standard
02.06.01
The Nephrology Hospital or the hospital with nephrology departments provides access to patients with CKD to individualized and optimized renal
Cr new criterion
02.06.01.01
The patients registered in the nephrology unit / division are treated and monitored to reduce the CKD progression rate.
R new requirement

73
02.06.01.02
The hospital with nephrology units / divisions prepares CKD patients for renal replacement therapy.
R new requirement
02.06.02
RRT efficiency and effectiveness are constant concerns for the dialysis unit.
Cr rephrased 11.01.03
The staff of the institution is involved in the security policy of dialysis patients
Cr
02.06.02.01
The unit that initiates dialysis decides on how RRT is conducted (haemodialysis, peritoneal dialysis, kidney transplantation), in agreement with the patients and their families.
R new requirement
02.06.02.02
The unit that initiates dialysis collaborates with the nephrology units / divisions that recommend the initiation of treatment and with the ambulatory dialysis centres that perform the dialysis treatment.
R new requirement
02.06.03
The day-care hospital dialysis unit monitors the evolution (medical performance of dialysis treatment) of dialysis patients.
Cr new criterion
02.06.03.01
The day-care hospital dialysis unit records and communicates on-line and in real time all parameters for monitoring the medical performance of dialysis treatment in the format and frequency requested by the Romanian Renal Register.
R new requirement
02.06.03.02
The day-care hospital dialysis unit controls the anaemia of dialysis patients.
R new requirement

74
02.06.03.03
The day-care hospital dialysis unit controls mineral metabolism.
R new requirement
02.06.03.04 The day-care hospital dialysis unit controls acidosis.
R new requirement
02.06.03.05
The day-care hospital dialysis unit monitors the infectious disease specific to the patient receiving dialysis.
R new requirement
02.06.03.06
The day-care hospital dialysis unit monitors the nutrition status of dialysis patients.
R new requirement
02.06.03.07
The day-care hospital dialysis unit monitors dialysis efficiency (HD / DP).
R new requirement
02.06.03.08
The day-care hospital dialysis unit is concerned about the life quality of the patients.
R new requirement
02.06.03.09 The dialysis unit has a policy of increasing patient autonomy.
R new requirement
02.07
Radiotherapy and/or nuclear medicine ensure(s) the specific treatment needs.
S rephrased 08.11
The institution organized the radiodiagnostic, radiotherapy, nuclear medicine, functional explorations, medical recovery and physiotherapy
S
02.07.01
The practice of radiotherapy / nuclear medicine is adapted to the specific needs of the patient.
Cr new criterion
02.07.01.01
Radiotherapy / nuclear medicine service equipment meets patient-specific treatment needs.
R criterion taken as a requirement
08.11.01
The institution has established rules on the operation of medical radiology and imaging services, radiotherapy and nuclear therapy, functional exploration and recovery
Cr

75
02.07.01.02
Radiotherapy/Nuclear Medicine comply with the rules of good practice.
R criterion taken as a requirement
08.11.02
The objective examination of the patient justifies requests for radiological investigations, ionizing and nuclear radiation therapies and for functional exploration and recovery
Cr
02.07.02
The practice of radiotherapy / nuclear medicine is monitored and evaluated periodically.
Cr rephrased 08.11.04
The institution monitors the consumption of imaging, nuclear exploration and recovery
Cr
02.07.02.01
Radiotherapy / Nuclear medicine used in the treatment of the oncological patient is monitored.
R new requirement
02.07.02.02
The practice of radiotherapy / nuclear medicine is constantly evaluated and improved.
R new requirement
02.08
Palliative and terminal care addresses patients with progressive chronical diseases and their families, seeking to improve their quality of life by relieving suffering.
S new standard
02.08.01
The management of the patients with progressive chronical diseases and with needs of palliative care is individual and non-discriminatory.
Cr new criterion
02.08.01.01
The needs of palliative care for the patients with progressive chronical disease are promptly identified and adequate measures are taken.
R new requirement
02.08.01.02
The hospitalization of patients with chronic progressive illness and palliative care needs is based on the decision of a multidisciplinary commission.
R new requirement

76
02.08.01.03
The staff involved in the care of the patients with progressive chronical diseases has undergone certified training in palliative care.
R new requirement
02.08.01.04
Pain and the other symptoms that are specific to progressive chronical diseases are controlled through adequate measures.
R new requirement
02.08.01.05
“Complex case” patients with progressive chronical diseases receive palliative specialized care.
R new requirement
02.08.02
Palliative care is provided in a home-like environment, adapted to the patients with a high degree of dependency.
Cr new criterion
02.08.02.01
The infrastructure is adapted to the special needs of the patient on palliative care, with a high degree of dependency, by respecting his/her intimacy.
R merged and rephrased criteria
06.06.01
The right to privacy of the patient is respected throughout the period of hospitalization
Cr
08.02.07
The institution provides solutions for the accommodation of the prisoners
Cr
02.08.02.02
The infrastructure allows for palliative care related services to be carried out.
R new requirement
02.08.03
Palliative care services allow for improvement in the life quality of the patient and of his / her family / guardians.
Cr new criterion
02.08.03.01
On patient admission in the hospital palliative care ward, a comprehensive evaluation of the patient / family / guardians is performed.
R new requirement

77
02.08.03.02
The aims of palliative care, the understanding of the diagnosis and prognosis are assessed and documented along with the patient / family / family member.
R new requirement
02.08.03.03
The signs and symptoms of the terminal condition are evaluated using standard scales and are documented.
R new requirement
02.08.03.04
The management plan of the patient in need of palliative care is developed by a multidisciplinary team, based on specific and updated protocols, according to the evolution of the pathology or changing needs of the patient / family / guardians.
R new requirement
02.08.03.05
Communication between the medical team and the patient / family / guardians is permanent and plays an important role in palliative care.
R new requirement
02.08.03.06
On discharge, the patient’s options regarding care continuity are taken into account.
R new requirement
02.08.04
Medical palliative care is provided by a multidisciplinary team.
Cr new criterion
02.08.04.01
The minimal structure of the multidisciplinary team comprises: a palliative doctor, pharmacist clinician, nurses, social worker, psychologist, spiritual mentor.
R new requirement

78
02.08.04.02
Taking into account the patient needs, the multidisciplinary team includes other specialists, such as: kinesiotherapy therapists, occupational therapists, play therapists, dieticians, volunteers, etc.
R new requirement
02.08.04.03
The members of the multidisciplinary palliative care team of the palliative care services undergo continuous training programs.
R new requirement
02.08.04.04
The institution has a coherent program of monitoring and support for the health of the staff involved in palliative care.
R new requirement
02.08.05
The management of the terminal condition respects the dignity and comfort of the patient, ensuring family support
Cr rephrased 08.04.03
The specific needs of the end-of-life patient (terminal phases) are identified
Cr
02.08.05.01
The terminal condition is identified and the family/guardians are informed.
R new requirement
02.08.05.02
The medical staff observes the protocol of terminal condition.
R new requirement
02.09
Pharmaceutical and medication management ensures the continuity of treatment and patient safety.
S rephrased 08.08
The sections of the institution and the pharmacy ensure the continuity of care
S
02.09.01
The hospital follows regulations and guidelines on prescribing medical substances and monitors prescriptions.
Cr new criterion

79
02.09.01.01
The hospital has established conditions for medication prescription that are acknowledged by the unit/pharmacy.
R merged and rephrased criteria
08.08.01
The prescribing conditions of medicines are established and known
Cr
08.08.03
The prescription of medicines and the use of devices are within the competence of each specialty
Cr
02.09.01.02
Pharmacologists / Clinical pharmacists are actively involved in prescribing and monitoring medication.
R new requirement
02.09.01.03
The pharmacy provides the medication that is necessary to support the continuity of the medical treatment.
R criterion taken as a requirement
08.08.02
The supply conditions of medical sections with medical supplies and medical devices are established and known
Cr
02.09.02
The infrastructure and organization of the pharmaceutical activity support the traceability of common medication.
Cr new criterion
02.09.02.01
The activities and responsibilities specific to the pharmaceutical specialty are recorded according to the legislation in force.
R new requirement
02.09.02.02
The activities and responsibilities specific to the pharmaceutical specialty are recorded according to the legislation in force.
R criterion taken as a requirement
08.04
The institution monitors the use of medicines and the use of medical devices
Cr
02.09.02.03
The organization and equipment of the pharmacy comply with the legislation in force, in accordance with the traceability of the medicinal product.
R criterion taken as a requirement
08.04
The institution monitors the use of medicines and the use of medical devices
Cr
02.09.02.04
The informational route of pharmaceutical products is respected.
R new requirement

80
02.09.02.05
Medication from clinical trials is maintained and managed under optimal conditions by the hospital pharmacy / chief pharmacist, and its use is monitored by the pharmacist / clinical pharmacist.
R new requirement
02.10
The hospital has implemented good practices on antibiotic therapy.
S new standard
02.10.01
The hospital has organized prescription and monitoring of antibiotic therapy.
Cr new criterion
02.10.01.01
The hospital has established the functional structures with attributions in the implementation and monitoring of good practices on antibiotic usage.
R criterion taken as a requirement
10.05.01 The institution monitors the use of antibiotics
Cr
02.10.01.02
The structures involved in the implementation and monitoring of good practices on antibiotic usage have established handling procedures.
R criterion taken as a requirement
10.05.02
The institution shall adopt and apply protocols on the use of antibiotics
Cr
02.10.02
Prescription of antibiotics is medically justified and ensures the traceability of their use.
Cr new criterion
02.10.02.01
Prescription of antibiotics is performed according to recognized antibiotic guidelines and antibiotic results, as appropriate.
R new requirement
02.10.02.02
Prescription duration is established according to evolution and is documented.
R new requirement
02.10.02.03 Records of antibiotic prescription allow for the traceability of its use.
R new requirement

81
02.10.03
The hospital pharmacy is directly involved in observing good practices on the antibiotic therapy.
Cr rephrased 10.05.03
There is a regular analysis of antibiotic consumption correlated with antibiotic resistance
Cr
02.10.03.01
The pharmacy provides the necessary antibiotics, taking into account the evolution of antibiotic resistance, and monitors the consumption of antibiotics and the complete route of the dispended products, including those that have not been administered.
R new requirement
02.10.03.02
The pharmacy checks whether good practices on prescription and usage of antibiotics are followed.
R new requirement
02.10.03.03
The pharmacy periodically informs the prescribers, the hospital management and the medical staff on the available antibiotics, as well as on the antibiotic usage across various units / bed wards.
R new requirement
02.10.04
The activity of the microbiology laboratory supports the observance of good practices in the use of antibiotics.
Cr new criterion
02.10.04.01
The microbiology department of the medical laboratory has internal quality control procedures for antibiotic-resistance investigations.
R new requirement

82
02.10.04.02
The microbiology department of the medical laboratory collaborates with the Department of prevention and mitigation of healthcare-related infections (DPMHI), with the pharmacy, physicians and with the hospital management on the issue of monitoring data on antibiotics resistance.
C new requirement
02.10.05
Clinical services have regulated the use of antibiotics, according to good practices.
Cr new criterion
02.10.05.01
Clinical services have implemented antibiotic and antibiotic prophylaxis regulations related to the specialty and section for the main clinical situations.
R new requirement
02.10.05.02
Antibiotic consumption, as well as prescription traceability and antibiotic usage are ensured.
R new requirement
02.11
Management of healthcare-associated infections follows good practices in the field.
S reference taken as a standard
10 MANAGEMENT OF NOSOCOMIAL INFECTIONS
REF
02.11.01
The hospital management has organized the supervision, prevention and mitigation of healthcare-related infections.
Cr new criterion
02.11.01.01
The hospital management has adopted measures to set up structures involved in the prevention of healthcare-associated infections.
R merged and rephrased criteria
10.01.01 Control of infectious risk is based on an annual or multiannual plan
Cr
10.02.01
The management and specialists of the institution develop the methodology for
Cr

83
controlling infectious risk
10.02.02 The responsibilities of each sector of activity are defined
Cr
10.03.01
The institution organized the nursing home surveillance and control service
Cr
10.03.02 The IN Prevention Officer is aware of the infectious risk situation
Cr
10.03.03
Communication between the sectors of activity for the prevention and reduction of nosocomial infections is ensured
Cr
10.03.05
The management of the hospital ensures the coordination of the activities for prevention and control of nosocomial infections
Cr
02.11.01.02
The hospital management ensures the implementing conditions for the provisions in the annual activity plan for the supervision, prevention and mitigation of healthcare-related infections.
R merged and rephrased criteria
10.01.01 Control of infectious risk is based on an annual or multiannual plan
Cr
10.02.01
The management and specialists of the institution develop the methodology for controlling infectious risk
Cr
10.02.02 The responsibilities of each sector of activity are defined
Cr
02.11.01.03
Supervision, prevention and mitigation of healthcare-related infections and contagious diseases are organized and coordinated across every hospital structure.
R merged and rephrased criteria
10.01.02
The plan for the control of nosocomial infections contains epidemiological monitoring
Cr
10.02.04 The staff is formed to prevent nosocomial infections
Cr
10.03.04
Any administrative-structural change project of the institution envisages the reduction of infectious risk
Cr
10.10.02 There is an internal communication system for nosocomial
Cr
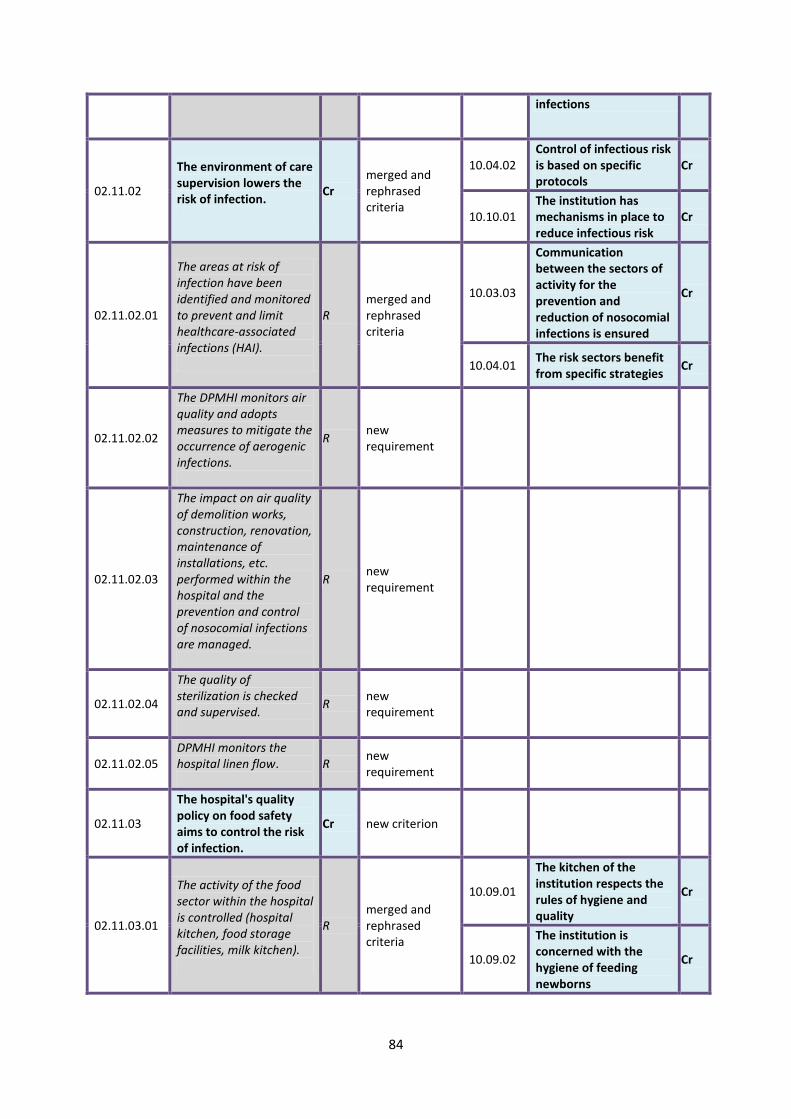
84
infections
02.11.02
The environment of care supervision lowers the risk of infection.
Cr merged and rephrased criteria
10.04.02 Control of infectious risk is based on specific protocols
Cr
10.10.01 The institution has mechanisms in place to reduce infectious risk
Cr
02.11.02.01
The areas at risk of infection have been identified and monitored to prevent and limit healthcare-associated infections (HAI).
R merged and rephrased criteria
10.03.03
Communication between the sectors of activity for the prevention and reduction of nosocomial infections is ensured
Cr
10.04.01 The risk sectors benefit from specific strategies
Cr
02.11.02.02
The DPMHI monitors air quality and adopts measures to mitigate the occurrence of aerogenic infections.
R new requirement
02.11.02.03
The impact on air quality of demolition works, construction, renovation, maintenance of installations, etc. performed within the hospital and the prevention and control of nosocomial infections are managed.
R new requirement
02.11.02.04
The quality of sterilization is checked and supervised.
R new requirement
02.11.02.05 DPMHI monitors the hospital linen flow.
R new requirement
02.11.03
The hospital's quality policy on food safety aims to control the risk of infection.
Cr new criterion
02.11.03.01
The activity of the food sector within the hospital is controlled (hospital kitchen, food storage facilities, milk kitchen).
R merged and rephrased criteria
10.09.01
The kitchen of the institution respects the rules of hygiene and quality
Cr
10.09.02
The institution is concerned with the hygiene of feeding newborns
Cr

85
02.11.03.02
Compliance with food safety rules for infection prevention is assessed.
R new requirement
02.11.04
The clinical management of the medical structures prevents and mitigates the risk of infection.
Cr new criterion
02.11.04.01
The medical structures (sections / compartments, laboratories, pharmacy, etc.) identify, assess and address the risk of infection posed by healthcare-related activities.
R criterion taken as a requirement
10.04.01 The risk sectors benefit from specific strategies
Cr
02.11.04.02
Curative doctors identify patients at risk of infection and take measures to mitigate it.
R criterion taken as a requirement
10.04.03 Patients and visitors are informed of the risk of contamination
Cr
02.11.04.03
Traceability of processes regarding the appropriate use of medical devices, sanitary materials and multi-purpose equipment is ensured and monitored to prevent and mitigate healthcare-related infections.
R new requirement
02.11.04.04
DPMHI supervises compliance with the rules of hand hygiene.
R new requirement
02.11.04.05
The hospital complies with the national supervision procedures for hospital-acquired infections.
R criterion taken as a requirement
10.04.02 Control of infectious risk is based on specific protocols
Cr
02.11.04.06
The hospital manages the risk of infection the staff might be subjected to.
R criterion taken as a requirement
10.06.02
The institution monitors and uses information on staff contamination episodes
Cr
02.11.04.07
The specialized hospital or the department of obstetrics adopts measures to prevent
R new requirement

86
prenatal risk of infection.
02.12
The hospital issues and implements policies to ensure and improve patient safety.
S new standard
02.12.01
The hospital has a proactive policy to prevent clinical risks.
Cr new criterion
02.12.01.01
For each medical sector, clinical risks are periodically documented, identified and assessed as an integral part of the risk register.
R new requirement
02.12.01.02
The hospital develops and implements a sentinel event management system.
R criterion taken as a requirement
10.02.03
The institution communicates to its specialists and external forces, episodes of nosocomial infections in order to prevent their spread
Cr
02.12.01.03
The hospital has developed and implemented a procedure for managing adverse events and those with the potential to affect the patient ("near miss").
R new requirement
02.12.01.04
The hospital has a functional patient identification system based on at least two identifying elements.
R criterion taken as a requirement
08.06.01 Patient identification is done at each stage of care
Cr
02.12.02
The hospital aims to identify and prevent risks and medication errors.
Cr new criterion
02.12.02.01
The patient medication recording and communication system prevents incompatible or unrecommendable associations.
R new requirement

87
02.12.02.02
The storage and handling of high-risk medicine or medication with similar names / packaging are regulated in the hospital.
R new requirement
02.12.02.03
Specific regulations on the storage and dispensing of psychotropic and narcotic drugs are followed.
R new requirement
02.12.02.04
Specific regulations on the storage and release of cytostatic medication are followed.
R new requirement
02.12.02.05
Specific regulations on the storage and release of electrolyte concentrate solutions are followed.
R new requirement
02.12.03
The transfer of patient information and responsibilities ensure continuity of care and safety.
Cr new criterion
02.12.03.01
The handover of the case is performed by following patient information and responsibility transfer procedures, as established by the hospital.
R new requirement
02.12.03.02
Patient information and responsibility transfer procedures in case handover are monitored and assessed.
R new requirement
02.12.04
The hospital aims to increase the safety of surgery and anaesthesia.
Cr standard taken as a criterion
08.07
The management of the patient with surgical potential is based on communication between specialized multidisciplinary teams
S
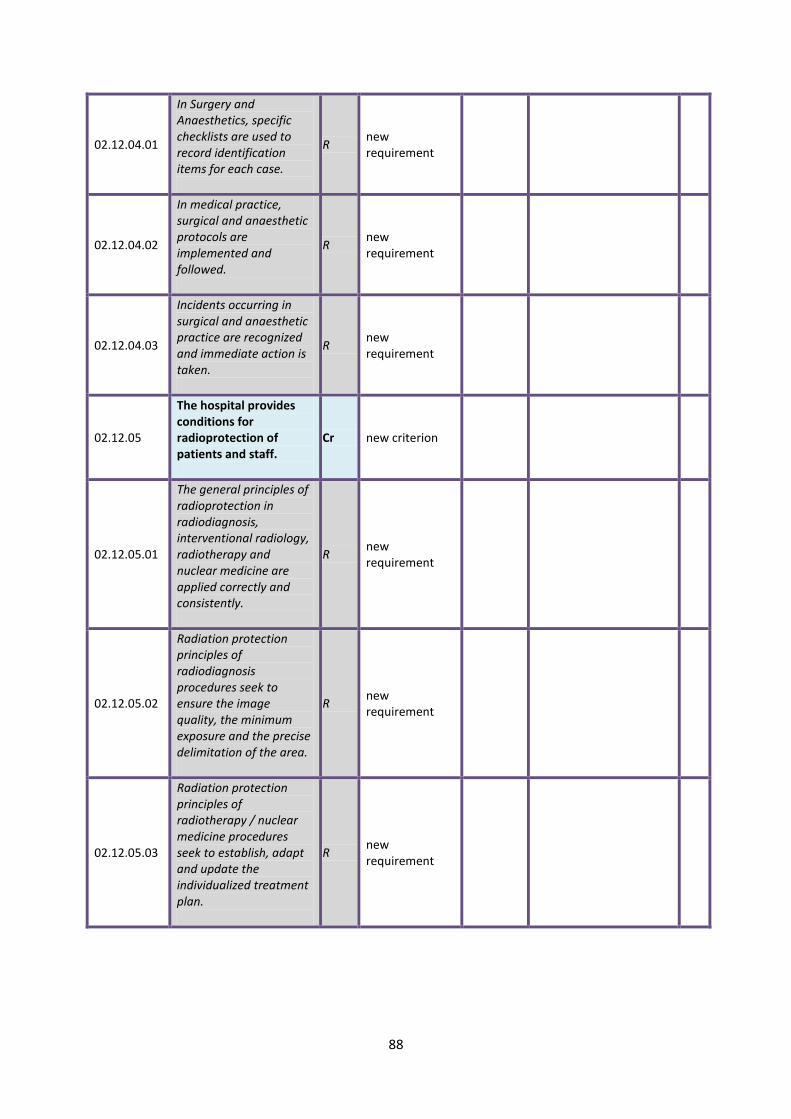
88
02.12.04.01
In Surgery and Anaesthetics, specific checklists are used to record identification items for each case.
R new requirement
02.12.04.02
In medical practice, surgical and anaesthetic protocols are implemented and followed.
R new requirement
02.12.04.03
Incidents occurring in surgical and anaesthetic practice are recognized and immediate action is taken.
R new requirement
02.12.05
The hospital provides conditions for radioprotection of patients and staff.
Cr new criterion
02.12.05.01
The general principles of radioprotection in radiodiagnosis, interventional radiology, radiotherapy and nuclear medicine are applied correctly and consistently.
R new requirement
02.12.05.02
Radiation protection principles of radiodiagnosis procedures seek to ensure the image quality, the minimum exposure and the precise delimitation of the area.
R new requirement
02.12.05.03
Radiation protection principles of radiotherapy / nuclear medicine procedures seek to establish, adapt and update the individualized treatment plan.
R new requirement

89
02.12.05.04
The principles of radioprotection of interventional radiology seek to follow specific protocols to optimize the time of intervention.
R new requirement
02.12.05.05
Individuals who voluntarily help a patient are informed of the risks associated with voluntary exposure and are provided with the necessary protection.
R new requirement
02.12.06
The hospital seeks to identify and mitigate the risks associated with the investigative process.
Cr new criterion
02.12.06.01
The clinical laboratory identifies and evaluates microbiological risks.
R new requirement
02.12.06.02
The microbiological risks of the clinical laboratory are analysed and good practice rules are established.
R new requirement
02.12.07
The hospital seeks to identify and mitigate the causes of injuries by falling / hitting.
Cr new criterion
02.12.07.01
The hospital seeks to identify and mitigate the causes of injuries by falling / hitting.
R new requirement
02.12.07.02
Informing and educating the patient / guardians and staff help reduce the risk of falling.
R new requirement
02.12.07.03
The hospital provides the necessary resources for carrying out the sampling and/or transplantation activity, ensuring efficiency and patient safety.
Cr new criterion

90
02.12.07.04
The hospital provides the necessary conditions for organ / tissue / cell procurement.
R standard/criterion taken as a requirement
06.05.05
The institution respects the consent of legal representatives of adults who can not manifest their will
Cr
06.05.06
The institution respects the patient's right to tissue and organ transplantation and transplantation.
Cr
11.01.02
The leadership of the institution defines the transplant security policy
Cr
11.05
The institution has procedures for organ procurement within the national network
S
02.12.07.05
The hospital provides the necessary conditions for organ / tissue / cell transplantation.
R standard/criterion taken as a requirement
06.05.06
The institution respects the patient's right to tissue and organ transplantation and transplantation.
Cr
11.06 The transplantation methodology is evaluated and improved
S
02.12.07.06
The hospital organizes procurement / transplantation in accordance with the regulations of the National Transplant Agency.
R standard preluat ca cerinta
11.06 The transplantation methodology is evaluated and improved
S
02.13
The hospital has implemented good transfusion and haemovigilance practices.
S new standard
02.13.01
The hospital has organized the prescribing and monitoring of transfusion and haemovigilance therapy.
Cr new criterion
02.13.01.02
The hospital fulfils the conditions for safe transfusion therapy.
R merged and rephrased criteria
11.01.01
The management of the institution defines the transfusion security policy
Cr

91
11.02.02 The institution respects the stages of the transfusion process
Cr
02.13.01.03
The functional structures of the hospital with responsibilities in implementing and monitoring the correct use of transfusion therapy comply with the specific working arrangements.
R merged and rephrased criteria
11.03.02
Information on transfusion risks is accessible to healthcare professionals
Cr
11.03.03 Transfusion security is subject to continuous evaluation
Cr
02.13.02
Prescription of blood and derivatives is medically based and ensures the traceability of their use.
Cr new criterion
02.13.02.01
Prescribing blood and derivatives is performed according to the National Guidelines for the Use of Blood and Human Blood Components.
R new requirement
02.13.02.02
Blood transfusion records allow traceability of the process.
R criterion taken as a requirement
11.02.03 The transfused patient is informed, medically trained and dispensary
Cr
02.13.02.03
The hospital provides total blood and blood components, taking into account the dynamics of hospitalized morbidity, and monitors the consumption and the complete route of released products, including those that have not been administered.
R criterion taken as a requirement
11.02.01 The institution has a policy of supplying and using blood products
Cr
02.14
Clinical audit assesses the efficacy and effectiveness of healthcare.
S new standard
02.14.01 Clinical audit activity is organized.
Cr new criterion
02.14.01.01
Internal clinical audit missions are planned annually.
R new requirement
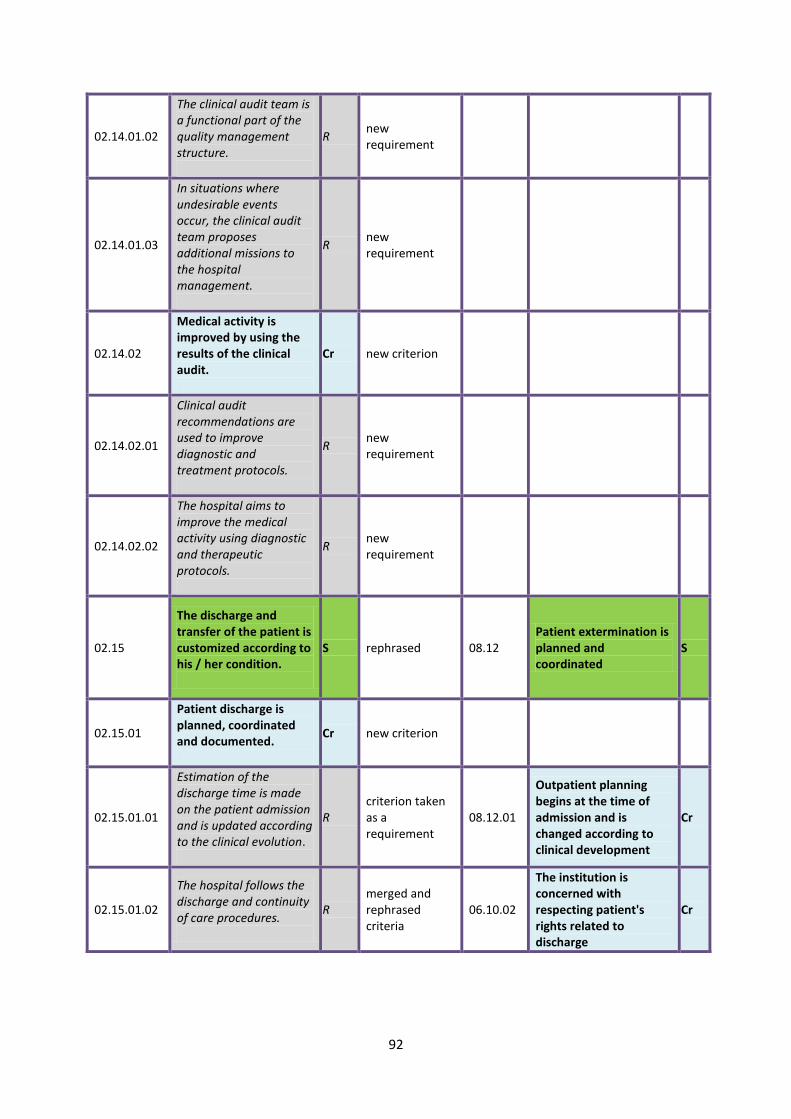
92
02.14.01.02
The clinical audit team is a functional part of the quality management structure.
R new requirement
02.14.01.03
In situations where undesirable events occur, the clinical audit team proposes additional missions to the hospital management.
R new requirement
02.14.02
Medical activity is improved by using the results of the clinical audit.
Cr new criterion
02.14.02.01
Clinical audit recommendations are used to improve diagnostic and treatment protocols.
R new requirement
02.14.02.02
The hospital aims to improve the medical activity using diagnostic and therapeutic protocols.
R new requirement
02.15
The discharge and transfer of the patient is customized according to his / her condition.
S rephrased 08.12 Patient extermination is planned and coordinated
S
02.15.01
Patient discharge is planned, coordinated and documented.
Cr new criterion
02.15.01.01
Estimation of the discharge time is made on the patient admission and is updated according to the clinical evolution.
R criterion taken as a requirement
08.12.01
Outpatient planning begins at the time of admission and is changed according to clinical development
Cr
02.15.01.02
The hospital follows the discharge and continuity of care procedures.
R merged and rephrased criteria
06.10.02
The institution is concerned with respecting patient's rights related to discharge
Cr

93
08.12.02
Upon discharge, the patient receives the information and documentation necessary to continue outpatient care
Cr
08.12.03
The patient and caregivers are involved in setting the discharge date
Cr
02.15.02
The hospital has procedures related to patients in critical condition or death.
Cr standard taken as a criterion
08.13
The institution has procedures related to critical situations or death
S
02.15.02.01
The patient guardians are alerted in case of degradation of the patient's condition, including imminence of death/ death.
R criterion taken as a requirement
08.13.01
Apostillers are alerted in case of degradation of the patient's condition, including the occurrence of death
Cr
02.15.02.02
The dignity of the patient in critical condition / terminal phase and his / her spiritual / cultural beliefs, previous decisions related to this event are taken into account.
R merged and rephrased criteria
08.13.02
The beliefs of the deceased patient and the needs of his or her associates are taken into account
Cr
08.13.03
The dignity of the patient in critical condition or terminal phase is ensured by establishing palliative treatment, including pain
Cr
02.15.02.03
The hospital has regulated the procedure to be followed in the event of a patient’s death .
R criterion taken as a requirement
08.13.04
The laboratory of pathological anatomy and procreation is organized
Cr

94
03 MEDICAL ETHICS AND THE PATIENT RIGHTS
REF new refference
03.01
The hospital promotes respect for patient autonomy.
S new standard
03.01.01
The medical practice is regulated to be consis-tent with the ethical and legal provisions that apply to informed consent (IC).
Cr standard taken as a criterion
06.05
The treatment and investigation plan is based on the informed consent of the patient
S
03.01.01.01
The hospital has devel-oped procedures and policies on how the IC is acquired.
R merged and rephrased criteria
06.04.02
The patient and / or the patient is informed about the proposed treatment and its risks
Cr
06.05.01
The institution respects the process of obtaining informed consent,which is required for all medi-cal procedures
Cr
06.05.02
The patient is involved in making decisions about their care and treatment
Cr
03.01.01.02
The medical staff is preoccupied with identi-fying vulnerabilities in the process of acquiring the informed consent.
R new requirement
03.01.01.03
Measures have been implemented to diminish the effects of the identi-fied vulnerabilities in the process of acquiring the informed consent.
R new requirement
03.01.02
Measures regarding the consistency of medical practice with the ethical and legal norms on pa-tient medical data confi-dentiality are in place.
Cr new criterion
03.01.02.01
The hospital uses a uniqe procedure to ensure con-fidentiality and verifies compliance by medical staff.
R merged and rephrased criteria
06.07.02
The institution guaran-tees the professional secrecy related to the medical act
Cr
07.02.01
The institution shall ensure that its staff retain the confidentiality of patient data
Cr

95
03.01.02.03
Measures have been applied to diminish of the effects of the identified vulnerabilities related to the confidentiality of the medical data.
R new requirement
03.02
The hospital respects the principles of equity, social justice and patients' rights.
S new standard
03.02.01
The hospital has policies to prevent discrimination in providing medical services.
Cr standard taken as a criterion
06.02 The right to health care is ensured on a non-discriminatory basis
S
03.02.01.01
The hospital regulates the prevention of discrimination.
R new requirement
03.02.01.02
A functional and regulated ethical council has been established within the hospital.
R criterion taken as a requirement
06.09.02 Conciliation procedures are organized by the institution
Cr
03.02.02
The hospital ensures access to personal medical information.
Cr new criterion
03.02.02.01
The hospital regulates the procedure of releasing medical documents to patients / family members / relatives / empowered authorities.
R criterion taken as a requirement
07.04.04
FOCG information on diagnosis, health and lifestyle and therapeutic recommendations available to the patient
Cr
03.02.02.02
The hospital regulates how the patient's personal medical data is made available to authorized authorities / other institutions.
R new requirement
03.02.03
The hospital ensures the right of the patient to a second medical opinion.
Cr new criterion

96
03.02.03.01
The hospital regulates the circumstances in which the patients can receive a second medical opinion, including from doctors who are not hospital employees.
R new requirement
03.02.03.02
The hospital regulates the conditions in which patients can benefit from a second medical opinion from doctors who are employed by the hospital.
R new requirement
03.02.04
The hospital is concerned with patient protection in relation with the external environment.
Cr new criterion
03.02.04.01
The hospital regulates access of the media in the institution and to the patients.
R new requirement
03.02.04.02 The hospital protects the patient against the external intrusions.
R new requirement
03.02.05
The hospital allows the patients’ audio / photo / video recording for medical / didactical / research purpose and to avoid accusations of malpractice.
Cr new criterion
03.02.05.01
The hospital ensures the conditions and procedures for patients’ audio / photo / video recording for medical / didactical / research purpose and trains the medical staff in this respect.
R new requirement
03.02.05.02
The hospital ensures the patient's audio / photo / video recording and recording conditions for medical, teaching and research purposes.
R merged and rephrased criteria
06.05.03
The institution allows the inclusion of its patients in a scientific research only after obtaining its written consent
Cr

97
06.06.04
The institution obtains the patient's consent for his / her participation in clinical education
Cr
07.01.03
The institution ensures the protection of the confidentiality of patient files and information
Cr
03.03
The hospital promotes the principles of philanthropy and safety.
S new standard
03.03.01
The hospital only operates within the limits of its competency.
Cr new criterion
03.03.01.01
For each section, the hospital ensures medical personnel with appropriate competencies.
R new requirement
03.03.01.02
The hospital provides medical staff training to prevent deskilling.
R new requirement
03.03.02
Exceeding competency is allowed for the patient benefit.
Cr new criterion
03.03.02.01
The hospital regulates the conditions of performing one’s duties outside medical competency in the patient's interest.
R new requirement
03.03.02.02
The hospital ensures medical staff instruction on respecting the patient's rights in situations that require performing outside medical competency.
R new requirement

98
7. DESCRIPTION OF ACREDITATION STANDARDS
01. Strategic and organisational management
The goal of the reference is to determine the hospital to design and substantiate
hospital activities based on the strategies and policies developed by the management
structures, leading to increased effectiveness of the interface with the healthcare system,
while maintaining and increasing its market share, setting long-term goals and objectives for
the organisation, taking the necessary actions and allocating the necessary resources to
achieve these objectives, according to the organisation mission.
The overall objectives of the reference are:
To identify the position held by the hospital in the healthcare system and the
position it intends to hold on medium-term
Integrated approach on the hospital and its environment
-
To correlate organisation activities with resource capabilities
To set a pre-determined course of planned action to achieve the intended
objectives
To establish a consistent structure of actions in terms of behaviour, taking
into account and favouring an intense organisational learning process with
the implementation of quality management and organisational culture
development.
Organisation strategy and strategic management
are consistent with the healthcare needs and the
dynamics of the healthcare services market.
The goal of this standard is to determine the hospital to set a planned development
direction, supported by hospital governance, consistent with healthcare services supply and
demand, and health policy objectives and supported by the actual and potential human
resources in place.
99
The standard requires that the hospital should develop and implement a solid
medium- and long-term strategic plan (structure, resources, services), to ensure integration,
continuity and coherence of clinical and organisational processes.
The overall objectives of the standard are:
To develop a sustainable and documented strategic plan, adapted to the
hospital
To put in place the necessary conditions for the implementation of the
strategy and of national health policies
To develop healthcare services according to the real needs identified and
to the current context of healthcare services.
The specific objectives to achieve this standard are:
- To establish the healthcare needs of the population and the market
Fulfilment of this criterion is reflected by the use of an initial market and
needs analysis (which will underpin the plan), by the action plan and by
performance of regular measurements of results obtained.
The analysis should include information in: demographics (population
number, density, distribution by gender, age groups, urban-rural, birth rate,
mortality), morbidity (incidence and prevalence) for at least the 10 main
categories of conditions (most frequent at hospital level), number of services
(admissions, day hospitalisation, outpatient consultations, laboratory and
imaging investigations-tests, health programmes implemented etc.), funding
level and sources (value of CAS contracts, value of contracts for healthcare
programmes, own revenues, value of non-reimbursable funding, number and
value of grants, revenues from the local budget, revenues from transfers from
the state budget through the Ministry of Health), specialist staff – physicians
and nurses (number of positions in the organisation chart, number of
positions filled, number of civil law contracts – on call duties or others,
number of residents) by category and specialty.
- The strategic plan is assumed at all decision-making levels
Fulfilment of this criterion is reflected by the development of a strategic
plan which should set the vision and the mission of the hospital, should
include specific SMART objectives and should define the necessary policy and
action lines for its implementation.
- All sectors of activity participate in the implementation of the strategic plan
This criterion requires that the hospital should operationalise its strategic
plan, by creating links with all levels of activity and correlating the strategic

100
plan with the annual plans (service development plan, procurement plan, list
of investments and running and extensive repairs, training, quality
improvement plan etc.).
Fulfilment of this criterion is reflected by the manner and level of
interactions of clinical and administrative activities with hospital policy on the
quality of services provided and the concern for patient safety.
- The strategy of clinical institutes and hospital includes the development of the
scientific research sector
The goal of this criterion is to foster research and innovation of healthcare
services necessary to solve the health problems of hospital patients, by
correlation with new and modern technologies for complex pathologies,
including by creating multidisciplinary medical teams to enhance professional
expertise and increase the facility competency.
Fulfilment of this criterion is reflected by the level and frequency of
updating/adapting new technologies, management and clinical processes at
hospital level.
In order to achieve the specific objectives, the hospital undertakes the following activities:
The strategic plan is based on an analysis of the population
healthcare and service market needs.
01.01.01.01. The organization has performed / used an analysis of the related
population healthcare needs and of the market of healthcare services
in the assigned territory.
01.01.01.02. The results of the analysis of the population healthcare needs and of
the market of healthcare services are used in establishing the
strategic objectives of the hospital.
The strategic plan designed by the hospital is supported at all
decision levels.
01.01.02.01. The strategic plan is based on the identified available and potential
resources.
01.01.02.02. The strategic plan aims to improve the quality of services and
patients' safety.
01.01.02.03. The objectives of the strategic plan are acknowledged by all the
structures involved in their achievement.

101
The strategic plan is implemented with the participation of all the
activity sectors.
01.01.03.01. At the hospital level there is an active team responsible for periodical
evaluations of the level of implementation of the strategic objectives.
01.01.03.02. The heads of all the activity sectors periodically analyze the level of
achievement of the strategic objectives.
01.01.03.03. The annual planning of the activities takes into account the
established strategic objectives.
The strategy of the clinical institutions and of the clinical hospitals
includes the development of the scientific research sector.
01.01.04.01. Scientific research takes into account the development objectives of
the hospital.
01.01.04.02. Innovation through research improves the quality and performance
of the medical activity.
01.01.04.03. The medical institute coordinates the innovation / research activity of
hospitals that operate in the field.
The organizational structure and the
organizational management ensure the optimal
running of all the processes that provide medical
assistance and healthcare.
The goal of this standard is to determine the hospital to set process planning and
adopt procedures based on the clear definition of the problems identified, on the choice of
solutions, after the evaluation of possible alternatives, according to the specific conditions of
the internal and external environment, risk assessment and individual and collective
assumption, after defining prevention alternatives.
The standard requires that the hospital should adapt and develop its structure, should
define roles and plan activities on medium- and long terms, based on market requirements
and adapted to the organisation and operation model of a modern hospital.
102
The overall objectives of the standard are:
To develop a solid organisational framework adapted to the specificity of
activities, based on modern management principles
To promote an organisational culture based on healthcare services planning
and results performance
To streamline the organisation integration process at local and regional
levels
To promote a system of ongoing monitoring and evaluation of the efficiency
and sustainability of the organisational structure
To record and document activities and decisions at organisation level
To ensure cooperation within the organisation
The specific objectives to achieve this standard are:
- Hospital operation with all authorisations and permits provided by the
legislation in force
This criterion requires that the hospital should be permanently concerned
with maintaining and updating the necessary conditions for the smooth
operation of all services, ensuring compliance with legal requirements at all
times.
Fulfilment of this criterion requires that all permits and authorisations
provided by law are obtained and valid and complaint, and all activities
covered by them are monitored.
- The organisational structure is substantiated, documented, reviewed and
regularly updated, as appropriate
By fulfilling this criterion, the hospital develops and supports its
organisational and operational framework according to the mission and
objectives proposed.
- The functional structures at hospital level (commissions, committees, boards)
are operational, and ensure integration of processes and strengthening of
management control.
Fulfilment of this criterion is reflected by the quality and frequency of
cooperation between the various sectors of activity and by the coherence of

103
the management control system. The goal of this criterion is to set up and
operationalised all multidisciplinary commissions and committees (clinical and
administrative), to ensure technical and managerial coordination of all issues,
in all fields of activity.
In order to achieve the specific objectives, the hospital undertakes the following activities:
The hospital works with all the licenses and authorizations
stipulated by the legislation into force.
01.02.01.01. The hospital ensures provisions to obtain and to update all the
specific licenses and authorizations, updated, if required.
01.02.01.02. The hospital has taken measures to maintain the conditions on the
basis of which the licenses and authorizations were obtained.
The organizational structure is substantiated, documented,
analyzed and as required, periodically updated.
01.02.02.01. The foundation of the organizational structure takes into account the
demand for medical services and the dynamics of available resources.
01.02.02.02. The management periodically evaluates the organizational structure
related to the demand of healthcare services.
01.02.02.03. The management periodically analyses the organizational
development process at and updates the organizational structure
accordingly.
The functional structures of the hospital (commissions,
committees, councils) are operational, ensuring process
integration and the consolidation of the management quality
control.
01.02.03.01. The functional structures of the hospital (commissions, committees,
councils) have been established and are active.
01.02.02.02. The activity of the functional structures (commissions, committees
and councils) of the hospital substantiates the decision-making
process.

104
The human resources management ensures staff
recruitment according to the mission stated by the
hospital.
The goal of this standard is to determine the hospital to ensure the human resources
development process, in terms of needs related to the categories, number, competences
and distribution of personnel. The standard fosters personnel planning, recruitment,
training, retention and motivation, so as to ensure continuing performance improvement,
according to best practices in the field.
The overall objectives of the standard are:
Human resources planning, at least on medium-term, according to the real needs of the hospital
Human resources development, by proper dimensioning, qualification and
regular improvement of skills
The specific objectives to achieve this standard are:
- Human resources policy is documented and adapted to the hospital
organisation and operation needs.
The goal of this criterion is to determine the hospital to develop and
implement a human resources policy based on modern personnel planning,
selection, recruitment and motivation principles and practices. In order to
fulfil this criterion, the hospital must perform regular identification and
evaluation of future needs (at least on medium-term) in the field of human
resources and operate an adequate records system.
- Human resources needs are identified according to the technical and
accommodation capacity, addressability, morbidity treated, personnel
regulations and work time audit, as appropriate.
The goal of this criterion is to determine the hospital to perform
permanent (dynamic) analysis of personnel needs and to adopt realistic
measures to reduce personnel deficit and foster employee retention
(motivation). The hospital has the obligation to organise flexible working
hours (rounds and on call activities), within the limits provided by law, so as to
cater as best possible for the specific needs of the patients (number, level of
dependence etc).
- The human resources policy motivates employees and fosters quality
improvement.

105
The criterion makes the hospital permanently consider and evaluate
employee motivation, and adapt actions based on (existing) issues, so as to
reduce the risk of professional plateau, demotivation, resignation etc.
In order to achieve the specific objectives, the hospital undertakes the following activities:
The human resource policy is documented and adapted to the
needs of the unit organization and functioning.
01.03.01.01. The hospital management establishes the need of staff according to
the volume of activity in order to optimize the services provision
process, while taking into account the staffing norms.
01.03.01.02. The hospital management annually analyzes the position structure
and makes adequate provisions for its adaptation to the identified
needs.
01.03.01.03. The hospital management ensures that a Yearly Plan of selection,
recruitment and professional development of the staff is elaborated
and implemented.
01.03.01.04. The continuous vocational training is based on a plan that is
adequate to the specific and needs of the unit, while including the
financing sources.
The need of staff is established according to the technical
capacity, hotel accommodation, addressability, treated morbidity,
staff norms and to the working time audit, if required.
01.03.02.01. The need for medical and auxiliary staff in the bed sections /
compartments is established according to the degree of dependence
of the categories of treated patients.
01.03.02.02. The need of staff is estimated in order to ensure the use of the
existing technical resources at optimal capacity.
01.03.02.03. The staff working in the unit is qualified and authorized, according to
the law.

106
01.03.03. Personnel policy motivates employees and determines
quality improvement.
01.03.03.01. The employees are involved in the decision-making process and
impact how attributions are performed while submitting to the social
dialogue mechanisms.
01.03.03.02. The employees' level of satisfaction is evaluated periodically.
01.03.03.03. The hospital ensures compliance with the quality of professional life
requirements.
The financial and administrative management
responds to the strategical and operational
objectives of the hospital.
The goal of this standard is to prompt the hospital to adopt a rational approach to
ensuring efficient financial and physical resources, based on the strategic and operational
objectives of the hospital, and to avoid a formal approach on the matter, and to determine
the hospital to ensure the necessary financial and physical resources so as to provide patient
healthcare services according to the hospital competency level and to the number of
services expected to provide according to the annual healthcare services plan.
The overall objectives of the standard are:
- To ensure financial support for continued activity. A possible interruption of activity would influence achievement of objectives.
The financial and administrative management, a component of the hospital management, supports the achievement of hospital objectives, informs decisions in a realistic manner and is necessary for the organisation and implementation of hospital activities, and for ensuring healthcare services by efficient resource attraction, allocation, adaptation and use, while maintaining the specific financial records and ensuring compliance with the legal provisions and generally accepted accounting principles, thus ensuring the “financial health” of the hospital and optimum performance.
- To make available financial information generated by the overall use of resources, broke down by activity or by service, financial information on the activity (contracted fees, revenues, receipts), economic performance (revenues against expenditure), expected revenues, trends, used for decision-making purposes by the governance structures.
107
A sound financial policy for the hospital relies on two principles:
- Capacity to continue activity; - Profitability: positive financial results, financial balance development capacity. These are reflected by the annual financial plan, by the use of
funding, hospital development, procurement of goods, services and equipment, recruitment of personnel according to each objective, budget planning and execution, service contracts, pricing.
Financial management operates at different levels: 1. Prospective, by forecasting revenues, expenditure and financial results,
substantiated as follows: - Financial planning – plans expenditure based on expected revenues, to
achieve organisation objectives, - Monthly, quarterly, annual revenues and expenditure budget forecast,
by objectives, activities or programmes. 2. Operational – monitors and records current revenues from the basic activity
and running expenses for personnel (wages, taxes, travel), expenses for goods and services (drugs, sanitary materials, reactives, food, other materials, transport, utilities, rent, repairs, equipment maintenance, etc.).
3. Retrospective – evaluation in money of inputs – resources used – and outputs – services provided.
The specific objectives to achieve this standard are:
- The hospital has a financial strategy for development.
The hospital must provide the necessary financial resources to implement
the development plan by identifying financial resources – fund raising, efficient
allocation and use of resources, to provide healthcare services to the patients.
- The hospital revenues and expenditure budget supports the implementation of
the annual healthcare plan.
The requirements of this criterion aim at determining both the management team and the healthcare professionals to demonstrate responsible behaviour in substantiating expenditure so that the necessary expenses for healthcare services provision should be covered from the revenues gained according to the financial strategy of the hospital.
- The budget is regularly updated for a cost-effective service provision process.
The main goal of the evaluation of the economic performance of the hospital is the efficient use of financial resources available, namely economic operation ensuring the best healthcare benefits with the available resources. The requirements of this criterion aim at determining both the management team and the healthcare professionals to demonstrate responsible behaviour in terms of adequate use of resources which should determine a decrease of costs per patient, resource allocation based on normative needs and

108
results, with the aim of getting maximum benefits and increasing the quality of healthcare provision. Evaluation will be performed for each department, by physicians or medical teams, and will compare and identify causes and will propose solutions to increase efficiency.
- The supply of activity fields ensures service provision continuity. Hospital management identifies the main threats to the continuity of processes and activities, and takes all necessary steps so that activity may continue anytime, in all circumstances and at all levels, regardless the nature of a major disturbance. The requirements of this criterion aim at determining both the management team and the healthcare professionals to demonstrate responsible behaviour in terms of ensuring supplies for all sectors of activity, according to the requirements communicated by the heads of units and departments to provide healthcare services which meet patients’ needs.
In order to achieve the specific objectives, the hospital undertakes the following activities:
The hospital has a financial strategy regarding development.
01.04.01.01. The investments are established according to the strategic objectives
regarding the hospital development, taking into account the
satisfaction of the served community needs or the attraction of new
consumers.
01.04.01.02. The hospital establishes an annual plan of investments that complies
to the approved budget.
The income and expenditure budget of the hospital supports the
achievement of the annual plan of services.
01.04.02.01. The income and expenditure budget of the hospital is developed by
justifying expenditures.
01.04.02.02. The hospital periodically analyses incomes in relation to the incurred
expenditures.

109
The budget is periodically updated from the perspective of
streamlining the service delivery process.
01.04.03.01. The hospital has implemented a methodology of monitoring the cost
of medical services.
01.04.03.02. The hospital periodically analyses the process of service delivery with
the participation of all management levels.
The supply of the activity sectors ensures continuity in service
delivery.
01.04.04.01. The hospital ensures the inventory and monitoring of the critical
products and services.
01.04.04.02. The hospital performs a periodical analysis of the stocks.
01.04.04.03. The supply of the activity sectors is correlated with consumption.
01.04.04.04. The hospital ensures the product supply and services for exceptional
cases.
The information system responds to information
needs and determines their effective use in the
hospital.
The goal of this standard is to determine the hospital to organise the information system
both in terms of infrastructure, by building a complete, validated, operational, and flexible
database adapted too needs, and in terms of functionality (planning, specifications, analysis,
design, implementation, structure, behaviour, inputs and outputs), with converging
information flows, which should ensure effective communication between various
structures, using the best information registration, submission and storage support, and
data safety and security.
The hospital is a complex economic and social system, a construct of
interdependent elements which enable the delivery of its activity, namely healthcare
services provision. The analysis of the organisational and operational structure of such a
system highlights the following components:

110
decision-making system;
operational system; information system.
As long as the information system is the link between the decision-making system and
the operational system, it is crucial that this component is operational and well organised.
The functionality of the medical information system relies on the fact that patient data are
the most important information used by the healthcare information system. Even though
one can make a distinction between administrative and medical data, such data coexist in a
piece of information, therefore the system managing such data must contain the overall
information, regardless the type of data used and the data sources. Also, the administrative
information must be corroborated with the medical information, so as to enable efficient
and effective functionality of the hospital.
On the other hand, the patient file, although individual, is not used by the patient, but
by the professionals of the system, of the hospital and of the community the patient belongs
to. The data are used for the benefit of the patient, but this is a largely indirect benefit,
because the main result of the implementation of the patient file concept is the
effectiveness of healthcare provision. As long as the Romanian health system remains mainly
a public system, the patient is less interested in the cost of the treatment and mainly

111
interested in its efficiency. Consequently, patient data are of interest rather for the
institutional framework and less for the individual, therefore patient data should be
integrated in the overall information management policy of the hospital, as a component of
the organisational and strategic management.
Human activity, regardless its type, generates information. The more complex and
dynamic the activity, the richer and more varied the information. In any organisation, one
may distinguish two types of interrelated data which may change their nature based on their
association with or removal from a certain context:
- Personal data / information, and
- General data / information (of public interest, in case of public hospitals).
Formally, the two types of information are regulated by:
- Law 677 / 2001 on personal data protection and free movement of such data, which defines the categories of personal data, provides for general and special rules on personal data processing, with specific paragraphs on personal data which may identify the person and personal data on health condition. - Law 544 / 2001 on free access to data of public interest (in case of public institutions), or the obligations of public institutions related to the transparency of decision-making processes.
Regardless the nature of information, may it be medical, administrative, scientific,
educational, and the source of information, it should be treated according to its classification
as confidential or public / general. Thus, if we speak of confidential data, they should comply
with the same principles, regardless whether they are provided by patients, hospital
employees or third parties. Equally, the legislation on information protection should be
enforced for all fields of activity, together with the legislation applicable to that field. From a
practical perspective, it does not make sense to multiply qualitative criteria applicable to
information by differentiating information by type of data medical – non-medical, as the
national practice does not use different principles applicable according to this classification.
Similarly, the international literature in the field treats hospital information as a whole,
taking into account the nature of such information, and includes a section for medical
information as a sub-category of personal data, particular for the healthcare system.
The information system developed gradually, based on general principles that enable
answers to questions like:
How can I easily obtain information from all hospital departments?
How can I exchange information or liaise with other similar institutions?
How can I manage a situation efficiently using the information system?
The information system ensures the management of all information within an
organisation, using all available methods and procedures. The information is identified and

112
registered within an economic and social system at the level of organisational and functional
links called workstations. A logical sequence of workstations represents an information
circuit.
A workstation is individualised by the following elements:
- Inputs
- Storage time
- Processing operations
- Outputs
All information and decisions (characterised by content, frequency, quality, volume,
shape, support) necessary for carrying out an activity or operation, communicated between
two workstations, make an information flow.
There is close interdependence between the information circuit and the
information flow, as the information circuit reflects the route and the means
which ensure the information journey from generation to archiving, and
the information flow reflects all information exchanged, necessary for a certain
activity.
The information system includes, in a comprehensive approach, both information
circuits and flows, and the information processing methods and techniques.
The IT system is a component of the information system, namely that part which
takes over and solves the data collection, processing, communication, storage and
presentation tasks, with the support of computers. In order to fulfil its role within the
information system, the IT system includes all resources and techniques which enable
automatic data processing. These resources fall under the following categories:
· Equipment (Hardware) – the technical foundation of the IT system;
· Programmes (Software) including the base software (mainly the operating system)
and applicatons software;
· Information base;
· All human resources and organisational framework – specialist personnel
(programmer analysists, system engineers, operators).
Automatic data processing within an information system is the very process by which
data are subject to the collection, communication, processing and storage operations.
Data collection consists in data identification where data are generated and data
conversion on adequate supports to enable automatic processing. In this stage we speak of
primary data.
113
Data processing means the process of turning primary data into final data, after a
sequence of operations imposed by the requirements of the users and by the specificity of
the computers and processing technology.
Data communication ensures communication of both primary data from their
generating sources to to automatic processing systems, and of data processing results to the
beneficiaries.
Data storage consists in data saving and storage on specific memory supports, for
further consultation and processing.
The modern coordinates of IT systems indicate mainly the use of computer networks
as hardware support and of database management systems as software support, the
database being the information core of any IT system.
The wide openness provided by the Internet makes the use of databases distributed
on computer networks the most viable solution for the efficient use in management
processes of the remarkable performance of current PCs, but this also involves the
development of strong encryption solutions which ensure information confidentiality in case
of personal data.
The widespread use of electronic data collection in healthcare leads to an exponential
increase of heterogeneous clinical data from patients. Collection, management, integration
and analysis of such data are essential to identify illnesses and related treatments.
Some major issues related to the analysis of clinical data are caused by the fact that
they are either incomplete, or using different measurements, and push for the integration of
incompatible collection procedures. The main challenges for clinical data management are
to discover the patient interactions with the information system and to integrate various
sources of data.
The hospital information system includes structured and unstructured data which are
data for which we can provide a model or not. For example, in clinical, it is important to
highlight those processes (variables) which are frequent in a certain diagnosis.
Therefore, the analysis of clinical data requires new, efficient and effective methods to
extract compact and relevant information: the interdisciplinary field “data mining”, which
guides the process of automatic discovery of knowledge, is a natural way of tackling the
complex task of clinical data analysis. The IT systems largely take over this task.

114
Before discussing what IT system we want, we should know what we want the system
to be able to do. A common problem is purchasing an IT system which does not have the
necessary characteristics or produces results which are not relevant.
As there were no unitary regulations on the IT standards, and no supplier accreditation
or certification system, the IT systems were developed and organised in a hectic manner.
Consequently, instead of supporting the medical activity, IT rather generated confusion,
bureaucracy and uncertainty. There were parallel primary data collection efforts,
overlapping reporting flows, incompatibilities cause by different definitions of indicators and
proprietary codifications etc. From the perspective of implementing specific investments, IT
solutions were repeatedly developed for sectors that already had acceptable solutions, to
the detriment of other areas, and this generated inefficient use of public funds. Such “traps”
can be avoided by setting clear objectives for the IT system and prior testing of the
technologies envisaged.
Sound management relies on succinct, updated, complete and clear information so as to
meet the information requirements of each stage of the PDCA (Plan/Do/Check/(re)Act)
cycle. In order to obtain the information, we need primary data collected from various
sources which we process; nowadays data are usually processed automatically, using
dedicated electronic equipment.
For an organisation to operate efficiently, it must identify and manage several related
activities. Medical activity, as a whole, is resource-consuming and it should be managed so
that inputs are turned into outputs, creating a process where patient data are the main
information used. Coordinated integration and IT services management, information
management and, implicitly, patient data management guarantee permanent control,
improved efficiency and continuing improvement opportunities.
The overall objectives of the standard are:
- To implement in Romanian hospitals high-performance IT systems able to
support practitioners’ needs in providing efficient, effective and quality
medical activities;
- To create the prerequisites for shifting patient file from individual to
community level

115
The specific objectives to achieve this standard are:
- The information system provides the necessary data to document hospital
activity
What do I want to (can) do?
Define the structures involved (organisational structure, organisation chart)
=> define the services I want to deliver (hospitalisation, outpatient care,
paraclinical investigations, recovery services, palliative care, etc.)
From an organisational perspective, the hospital has a structure which helps
detailed definition of structures up to unit level which serve the medical and
administrative activity of the hospital, setting subordination relationships and
personnel needs.
After structures are defined, the hospital issues the Hospital Organisation
and Functioning Regulation, which stipulates the duties, competences,
authority levels, responsibilities and relationships for each entity.
What information is of interest for me? What information may I and must I
provide?
Inputs, input processing procedures and outputs are defined for each
activity. This stage is important not only in the process of identifying
information needs, but also for employee rview and workload definition for
each position. Both inputs and outputs always have an information
component, namely data/information and documents used. The healthcare
system tends to be heavily dominated by documents with templates provided
by law or with a minimum level of consistency. Nevertheless, the use of
documents within a department must be specified either as nomenclature or
in the working methodology, either as an annex to operational procedures
presenting the customised template and possible instructions for filling it in or
interpreting it, with mention of confidentiality level. All documents must be
inventoried and implemented in a unitary manner. The structures responsible
with the inventory of the types of documents and data communicated are the
Public Relations Department / Public Information Coordinator on the one
hand, and the Structure for information resources and communications
security.
On the one hand, Law 544 / 2001 provides for the obligation to
communicate by default the list of documents of public interest and the list of
categories of documents produces and/or managed, according to law, which
means that the website of each (public) institution should publish such a list.
On the other hand, Law 677 / 2001 stipulates the obligation of any entity
which purchases, processes and stores personal data to be registered as a
personal data operator.
- Information processes efficiently substantiate hospital decisions
- Information processes efficiently substantiate hospital decisions

116
- The IT system and all data storage means (information management means)
ensure data confidentiality, integrity and security
The registration as personal data operator is mandatory and involves formal stages
related to data confidentiality, integrity and security, and the development of an information
resources security policy, according to the provisions of Order 52 / 2002 approving minimal
security requirements for personal data processing.
Data confidentiality should be considered the general rule, not a procedural activity. If
the confidentiality obligation is provided only by the job description and is regulated by a
procedure, the effects of such provisions cease with the termination of the employment
contract.
Consequently, the information included in the confidentiality clause must be
mentioned in the internal regulation, by reference to the generic name of activity which is
object to such clauses or by their detailed description and by introducing the confidentiality
clause in the individual employment contracts.
Data integrity (accurate, complete) may be ensured only by ongoing verifications.
Hence, the Security Policy must provide for verification filters. Example: the IT system
includes restrictions for wrong data registration. The database coordinator checks that
printed/written records match electronic records. The head nurse checks the ward situation
with the patient journey and with the information supply sheet in the IT system.
- The information system documents and supports employee educational
process in the hospital.
In order to achieve the specific objectives, the hospital undertakes the following activities:
The information system provides the necessary data for the
documentation of hospital activities.
01.05.01.01. The information system integrates information needs and external
requests (formal or informal) from all activity sectors.
01.05.01.02. The information system administration ensures its adaptation to the
requirements of the hospital activity.

117
Circuits and information flows support the conduct of activities
and the decision-making process.
01.05.02.01. Circuits and information flows ensure that data is transmitted in the
required and timely format.
01.05.02.02. Circuits and information flows contain alert systems that prevent the
occurrence of decisional errors.
Information processes underpin effective decisions within the
hospital.
01.05.03.01. The data carrier for each activity in the hospital (paper-based,
magnetic, electronic) and the flow of information are clearly defined
and respected.
01.05.03.02. The operability of the implemented informational procedures
ensures that hospital activity is more efficient.
The information system and the data storage environment ensure
the confidentiality, integrity and security of the data.
01.05.04.01. The hospital respects the law in force regarding data security.
01.05.04.02. Access to information, their processing and protection is regulated
for each professional category.
01.05.04.03. The hospital provides back-up information systems.
01.05.04.04. The hospital monitors and controls the use of information systems.
01.05.04.05. Preservation and archiving of documents, information and records
ensures the confidentiality, integrity and security of the data.
01.05.04.06. Destruction of documents / records is performed while taking into
confidentiality and data security.
The information system provides documentation and supports
the educational process of hospital employees.
01.05.05.01. The information system provides documentation and information to
hospital employees.
01.05.05.02. The information system supports the process of training and
professional development of hospital employees.
118
The existing communication system of the hospital
meets needs of the organization and of the
beneficiaries.
The goal of this standard is to determine the hospital to establish communication of
information from personnel and organisation to patient/caregivers, between hospital
professionals or with external professionals, and create the prerequisite of patient-centred
healthcare provision.
The overall objectives of the standard are:
To improve institutional and professional communication with the patient
To encourage patient-oriented educational processes and to introduce the
concept of therapeutic education with active involvement of patients in the
healthcare provision process – turning the patient into a partner of the
healthcare professional
To optimise diagnosis and therapy by multidisciplinary approach of the
patient by teams of professionals employed by the hospital or teams created
with professionals from other healthcare facilities, to solve the case
The specific objectives to achieve this standard are:
- External communication meets the beneficiary and hospital needs
The hospital informs the patient on the services provided, using various
communication channels and guiding the patient for easy access to services.
- Internal communication meets patient and hospital needs
Communication between the medical team members covers all necessary
aspects to ensure information quality and accuracy.
Medical communication is the main factor for harmonising the efforts
made by various healthcare professionals for the patient under their care.
Consequently, the hospital must ensure that:
- Medical personnel communicate in a professional manner all aspects
related to healthcare provision in the team responsible with
healthcare provision and that the personnel makes all efforts to
ensure the quality and accuracy of information communicated;
- Medical personnel communicate in a professional manner with the
patient and his/her family, involving them and encouraging them to
become partners in the healthcare provision process. Thus, the
hospital regulates, supervises and improves patient interaction

119
processes: informed consent, evaluation of communication needs,
adaptation to the cultural and spiritual needs of the patient, the
manner in which essential information is communicated and the
framework of this process.
- The hospital implements a system to evaluate the patient/caregivers
training needs, there is a structure which delivers such education,
there is a specialist training system for the personnel delivering such
education, there are quality objectives proposed and regular review
of such objectives and continuing improvement actions for this
process
The criterion should answer the following questions: do the medical
personnel have the same semantic perception of the terminology used in the
healthcare provision process? Is the information exchanged by the members
of the medical teams participating in the healthcare process sufficient to
ensure quality and continuity? Is interdisciplinary cooperation a current and
functional practice? Are there clear records of the interactions with the
patient?
In order to fulfil these requirements, the hospital uses standard disease
codification systems, standard procedure codes, symbols and definition. At
the same time, the hospital is concerned with the identification of situations
which are not complaint with the codification systems used and keeps records
of such situations as well.
The quality of information exchanged between the medical team members
and between them and external medical teams is carefully monitored.
Medical personnel use systems to check both the quantity of information –
minimal set of information, and the quality of medical information submitted
– alert values, parameters for certain functions, etc. The medical personnel
are trained to use checklist upon patient admission /discharge/ transfer and
there is concern for the continuing improvement of this system.
The institution regulates and monitors specifically medical communication
in critical areas – before surgical interventions, intensive care departments,
anaesthetic therapies. Monitoring and regulation target communication both
between the medical team members and between them and the patient.
- Communication with the patient targets the patient’s involvement in the
healthcare process.
To turn the communication process between the medical personnel and
the patient/patient’s family from a formal one-way process into a constructive
and participative dialogue, to empower both parties for the success of the
healthcare provision.
To educate the patient and his/her family to enable them to make
informed decisions on the healthcare process.

120
In order to achieve the specific objectives, the hospital undertakes the following activities:
External communication meets the needs of the beneficiaries and
of the hospital.
01.06.01.01. The hospital has diversified the communication channels for the
public.
01.06.01.02. The hospital's website ensures effective communication.
01.06.01.03. The hospital provides the necessary conditions for easy orientation.
01.06.01.04. The hospital provides the necessary conditions for staff identification.
01.06.01.05. Communication with the media provides information to the public
and the promotion of the hospital.
01.06.01.06. The hospital provides information on the medical work that is being
performed.
01.06.01.07. External communication is achieved with the continuity of the
healthcare process.
01.06.01.08. The hospital ensures communication with other healthcare units and
administrative structures.
Internal communication responds to the needs of the patients
and of the hospital.
01.06.02.01. The hospital has implemented models of professional communication
between medical team members.
01.06.02.02. The hospital has established and uses specific communication
protocols between professionals.
01.06.02.03. The internal rules are communicated to the staff and to the patients.
Communication aims to involve the patient in the healthcare
process.
01.06.03.01. Communication between employees and the patients / guardians
aims to educate them to be involved in taking and observing
therapeutic decisions.
01.06.03.02. The hospital annually reviews the efficiency and effectiveness of
communication.

121
The service quality management system is
operational and ensures that all the processes
related to monitoring and quality improvement
are performed.
The goal of this standard is to determine the hospital to engage in a continuing quality
assurance and improvement process and in increasing patient safety, by setting up and
operationalisation of a structure specialised in quality management and developing an
organisational process to create a quality culture at the level of each medical and managerial
team in the hospital.
The standard targets the organisational aspects of quality management, which should
determine the implementation of procedures and protocols that are specific to each
operational structure in the hospital, regular self-assessment of each structure, performance
evaluation at hospital level and regular external evaluation.
The overall objectives of the standard are:
- To ensure the organisational framework for the development of service
quality
Continuing improvement of service quality and patient safety
requires a quality improvement plan in place and a well implemented
programme. The governance structure (Management Board/Board of
Directors – according to the hospital organisation type) approves this
programme, and the manager assumes responsibility together with
the medical director and the heads of units/departments for resource
allocation. The programme is managed by a person with experience
in quality management implementation (quality management
coordinator). (JCI Accreditation Standard for Hospitals, 5th Edition).
The quality improvement plan is developed is developed in
cooperation by the heads of departments and the hospital manager
and the quality management structure of the hospital. The
improvements proposed target the activity of the hospital as a whole,
but also the activity of each department, so that the final version of
the programme will have a list of general improvements for the
entire hospital and at least one specific improvement for each
department (e.g.: the quality improvement programme provides that
the IN rate for the entire hospital will be x% lower that the previous
year, and in BO the IN rate will be 0%). The role of the plan is to
centralise all improvement initiatives at hospital level, to harmonise
them and to coordinate the improvement efforts at central level.
The plan relies on the analysis of institution performance data

122
Retroactive analysis of
- internal or external adverse events from the previous year and
of the quarterly/biannual/annual quality reports from the previous
year, highlighting improvement areas
- patient satisfaction questionnaires, at least from the last year
Proactive analysis of
- risks generated by activities with high risk potential (e.g.: ICU
and ED), or high workload activities
- improvement proposals formulated by all members of
personnel
- good practice models from other institutions. (IHI- Improving
Health and Healthcare Worldwide)
- Analyse improvement proposals submitted by the heads of
units and departments
- Promote the quality improvement process in service provision
- Define relevant performance indicators
- Monitor, measure and improve hospital performance
The quality improvement programme relies on actual current scientific information, and includes activity improvement actions in the following areas (JCI 5th edition):
- Patient care (including the use of clinical guides)
- Accommodation conditions
- Organisation management and effectiveness of care and
services (including patient satisfaction monitoring, nosocomial
infections control and the use of human resources)
- Implementation of patient safety standards
- More efficient hospital activity
The plan must include actions for the development of an
organisational culture of safety and for the implementation of
patient safety standards (JCI 5th edition).
The plan includes indicators to monitor the efficiency of actions.
The indicators are SMART, have a target and the frequency of
measurement defined.
The plan is disseminated in the hospital and the personnel are
trained on this. For the programme to be efficient, the hospital
personnel must be informed on it, must be familiar with the
improvements proposed and must be trained on the actions to be
undertaken to achieve those improvements.
- To create an adequate framework for adverse events management
(definition, reporting, analysis and prevention)

123
The specific objectives to achieve this standard are:
- The quality management system target ongoing optimisation of organisation
processes
The role of the quality management structure is to help the manager and
heads of departments select which indicators will be measured. Indicators are
used to support management decisions and patient care decisions. The
analysis of these indicators may identify a hospital evolution pattern, may be
used to benchmark hospital performance, therefore data selection,
measurement and aggregation are crucial.
Indicators to be measured
- Relevant indicators for the improvements proposed
- Structure/process/result indicators
- EBM indicators
The following will be defined for each indicator: how it is calculated,
measurement period, data source, indicator relevance, data analysis method,
relevant size of the sample used for data collection, groups targeted by
results dissemination.
The quality improvement programme provides at least one annual analysis
on the cost/efficiency impact of the implanted improvements (JCI 5th edition).
Performance indicators are used.
Indicators are analysed at least one year prior implementation.
Indicators are measured at least one year after improvement
implementation.
- The quality management structure (QMS) together with the hospital
management ensure the development of a quality culture in the hospital
- The hospital develops and implements an action plan of quality assurance and
improvement of healthcare services and patient safety for the entire hospital
The quality improvement programme must include at least one session to
analyse the impact of the improvements obtained on hospital performance.
The analysis is performed with the involvement of (by) the hospital
manager (of Management Board), based on the results made available by the
quality management structure.
Analysis method: evaluate the necessary resources for the existing process,
then the necessary resources for the improved process. Resources may be
human resources (e.g., time allocated for various activities), or physical
resources (equipment, technologies, etc.). This analysis may prove useful to
evaluate the efficiency of the improvements proposed.
Examples of more efficient hospital activities are the implementation of
good practice guides and healthcare protocols and organisation of hospital
outpatient facilities to provide complementary services to those provided by

124
the hospital. The implementation of good practice guides and healthcare
protocols leads to reducing variations in patient care, limiting the excessive or
the insufficient use of certain services and ensuring consistent results of
healthcare, for the benefit of patients. The organisation of outpatient care
facilities may reduce the burden on the hospital and the number of
unnecessary hospitalisation days, ensuring both patient examination prior to
admission and patient monitoring after discharge.
- The hospital focuses on increasing patient satisfaction
Patients have the right to express their opinions on he healthcare received,
to lodge complaints and, when possible, to receive answers to such
complaints. Patient satisfaction measurement and identification of activities
generating the least level of satisfaction, as well as complaint analysis and
corrective actions – are efficient instruments to improve patient experience
during hospitalisation, and to increase the quality of healthcare services
provided by the hospital. It is important that the results of this activity should
be communicated to the hospital personnel, together with the improvement
actions adopted by the management.
In order to achieve the specific objectives, the hospital undertakes the following activities:
The quality management system aims to continuously optimize
processes within the organization.
01.07.01.01. The hospital management ensures the organization of the service
quality management system.
01.07.01.02. The Quality of Service Management structure coordinates the
process of ensuring and improving the quality of patient health and
safety services in collaboration with the heads of all sectors of
activity.
01.07.01.03. The hospital is concerned with the quality certification of its
activities.
The quality management structure (QMS) and the hospital
management promote a culture of quality in the hospital.
01.07.02.01. The hospital has established and observes of the principles and
values of quality, in agreement with the stated mission.
01.07.02.02. The hospital is concerned with the implementation and development
of a quality culture in the hospital.

125
The hospital develops and implements an action plan to ensure
and improve the quality and safety of patient services across the
entire hospital.
01.07.03.01. The annual planning of the QMS activities ensures compliance with
the requirements of accreditation standards.
01.07.03.02. The action plan for the implementation of quality management
services and patients safety is assumed by the management of the
unit.
01.07.03.03. QMS monitors the implementation of the action plan to ensure and
improve service quality and patients safety.
01.07.03.04. Based on QMS recommendations, the hospital takes steps to improve
the quality of health care and patient safety.
The hospital aims to increase the level of the patients'
satisfaction.
01.07.04.01. The hospital designs and periodically updates patient satisfaction
questionnaires.
01.07.04.02. QMS systematically analyses information resulted from the
processing of questionnaires and issues recommendations.
01.07.04.03. The hospital uses periodic analysis of complaints received to improve
the provided medical services.
The Quality Improvement Program comprises the effectiveness of
the hospital activity.
01.07.05.01. An evaluation means of the efficiency quality improvement processes
in the hospital is established.
01.07.05.02. The results of QMS evaluations are used in order to streamline
activities.

126
Non-clinical risk management prevents damage
and underpins decision-making process.
The goal of this standard is to determine the hospital establish the objective
instrument for evaluating the stage of implementation of the hospital management
concerns to the safety of people and environment in the area of responsibility.
The major objectives of the standard are:
- the presence of the hospital unit safety/security culture and the organisation in
specific areas in the management team concerns;
- providing the relationship framework in the areas covered by the security
concept (in the unit, in the locality, with the financing institution, with the higher
hierarchic institution/structure, with the neighbours, with the bearers of
expertise);
The specific objectives for meeting the standard are:
- All management levels have implemented the management of risks specific to
own activities
The risk management may be summarised as follows:
- Identification of hazard - Elimination of hazard if reasonably possible - Analysis of hazard if it cannot be eliminated and risk evaluation - Taking measures to limit the consequences - Risk monitoring
The risk evaluation must cover each activity and workplace in the hospital, considering each component of the labour system, respectively worker, task, protective equipment for the employees but also for the patients or caretakers and the environment. The risk evaluation serves to continuously improve the conditions and, to that end, requires adequate and sustained documentation. To understand the approach of risk evaluation, it is important to define the basic terms: Hazard: anything which can cause harm Risk: combination between the seriousness of injury and the probability of a hazard to cause the injury Risk evaluation: hazard evaluation process at the workplace Prevention: implementation of measures to eliminate or reduce the risk before an event occurs A risk evaluation must be:
- Systematic - following a defined procedure, namely a methodology - Comprehensive - to designate priorities to the recommended measures - Proper - as regards the seriousness and probability of hazards - Documented - to prove that the recommended measures are based on evidence

127
The general scheme of risk evaluation methodology goes through the following stages:
ACTIVITY INSTRUMENT RESULT
Site plan Hazard matrix
Matrix
M
Form the team
Define the workplaces and
evaluation areas
Site plan Hazard matrix
Evaluation team
General examination General examination checklist
PPP Model
Identified non-conformities
PPP
Identify the specific
hazards
Specific hazard checklists
PPP Model
Identified specific hazards
PPP
Analyse the hazards Define the workplaces and
evaluation areas
Evidence for
subsequent evaluation
Risk category assigned to
each hazard Risk category grid Evaluate the hazards
Plan the actions PPP Model
Monitor the actions PPP Model
Technical, organizational,
hygienic and sanitary
measures, responsibilities,
deadlines
PPP
Stage of registered
measures PPP

128
To evaluate the hazards, the risk evaluation methodology proposed below is semi-
quantitative, in accordance with those proposed by several European standards in this area.
The first step is to evaluate each hazard from the point of view of the following injury
severity classes, which take into account the condition and physical strength, gender, age
and specific risk groups:
- Deadly: the hazard consequence is an accident or a deadly disease
- Very serious: the hazard consequence is a serious accident resulting in the
invalidity or temporary incapacity for work of more than 90 days (more than 90
days of sick leave)
- Serious: the hazard consequence is an accident resulting in the temporary
incapacity for work of 3 to 90 days (3 to 90 days of sick leave)
- Moderate: the hazard consequence is a work accident resulting in the temporary
incapacity for work of 1-2 days (less than 3 days of sick leave)
The second step is to evaluate the likelihood of a hazard to cause injuries.
In this regard, four factors must be considered:
- Intrinsic characteristics of the hazard (e.g. lift condition)
- Possibility to recognise a hazard to avoid subsequent consequences
- Possibility of a dangerous situation
- Frequency and duration of exposure to a dangerous situation
The risk evaluation team must eventually reach a consensus based on evidence to
assign to a hazard a probability of occurrence class, according to the following scheme:
- Very likely: hazard occurs at most every 10 days
- Likely: hazard occurs every six months
- Rarely: hazard occurs once a year
- Very rarely: hazard occurs every five years
- Unlikely: hazard occurs at most every 5 years
The combination of the injury seriousness and the probability of a hazard to cause an injury leads to the following risk categories:
Risk category 5: immediate actions and ending work are required until the seriousness
and/or probability of risk is/are reduced by technical measures
Risk category 4: actions are required but work may continue if at least
organisational measures/regulations/protocol have been taken
Risk category 3: actions are required and at least medium-term measures must be
implemented
Risk category 2: no actions are required, but the hazard must be supervised
Risk category 1: the risk is negligible

129
Risk category grid
SERIOUSNESS
PROBABILITY
DEADLY VERY SERIOUS SERIOUS MODERATE
VERY LIKELY 5 5 4 4
LIKELY 5 4 4 3
RARELY 4 4 3 3
VERY RARELY 4 3 3 2
UNLIKELY 3 3 2 1
The actions which may be undertaken to mitigate the risk depend on the approaches
to be used alone or in combination:
- Fight against the risk by technical measures - Risk control by organisational measures, regulations, protocols - Training workers - Use of personal protective equipment as ultimate solution
The choice of actions to be undertaken is followed by the estimation of the residual
risk after the implementation of risk mitigation measures.
At least 6 months after the implementation of measures, a new risk evaluation is
recommended to be carried out with the aim of measuring the incurred residual risk. If it is
comparable to the estimated residual risk, the decided risk mitigation measures have been
proper. If there are unacceptable differences, in that the residual risk is higher than
estimated, the decided measures neither have been implemented nor are sufficient or
appropriate.

130
- The non-clinical risk management provides the protection of patients, employees
and visitors against any damages
- The way of action, responsibilities and reserve of resources usable in exceptional
cases are organised and regulated to ensure the hospital's functionality
To meet the specific objectives, the hospital carries out the following activities:
All management levels have implemented risk management
provisions that are specific to their own activity.
01.08.01.01. All department managers have organized the identification, analysis
and treatment of risks.
01.08.01.02. The hospital has a risk register and monitors the effectiveness of the
prevention measures.
01.08.01.03. The hospital management performs risk analyses based on type,
occurrence probability and impact and implements customized
measures.
Non-clinical risk management ensures that patients, employees
and visitors are protected against potential damage.
01.08.02.01. The places and conditions with potential of physical risk for the
persons' safety (risk of falling down, of slipping, of hitting, etc.) have
been identified and preventive measures have been implemented.
01.08.02.02. Waste management respects the prevention of toxic and infectious
contamination rules.
01.08.02.03. The operation of the vital services of the hospital is ensured.
01.08.02.04. The capacity and number of elevators comply with the volume, types
and flows of hospital transport.
01.08.02.05. Protection and security measures for goods and people have been
adopted by the hospital.
01.08.02.06. The hospital implements measures to manage earthquake risk.
01.08.02.07. The hospital implements measures to manage fire risk.

131
01.08.02.08. The hospital implements measures to manage explosion risk.
01.08.02.09. The hospital implements measures to manage the risk of chemical
and biological contamination.
01.08.02.10. The hospital implements measures to manage radiation risk.
01.08.02.11. The hospital implements measures for the employees' physical
safety.
01.08.02.12. Those responsible for technological risk prevention are nominated by
decision and trained in this respect.
01.08.02.13. The personnel who are exposed to risk are regularly trained on
compliance with risk-prevention measures that specific to each
activity.
01.08.02.14. The hospital management undergoes periodic evaluations on physical
and technological risk prevention measures.
The means of action, responsibilities and resources available for
exceptional situations are organized and regulated to ensure the
hospital's functionality.
01.08.03.01. Hospital intervention teams for disasters or catastrophes have been
updated.
01.08.03.02. Within the hospital, there is a reserve of resources available in the
event of natural disaster and catastrophe.
01.08.03.03. The hospital holds an inventory of resources designed for specific
tasks in the event of mobilization and war.

132
The environment of care provides the necessary
conditions for healthcare.
The goal of this standard is to determine the hospital establish the conditions of the in-hospital
care environment supporting the defence and regeneration of the patient’s body which is removed
from its environment and the mitigation of negative effects of hospitalization-related stress, concern
for the disease, interruption of permanent connections with work, family and friends and
psychological affections which may occur during the admission (anxiety, fear, loneliness,
abandonment, estrangement, helplessness).
The major objectives of the standard are:
- To ensure accommodation and environmental conditions tailored to the hospital
services and patient healthcare service particularities
The accommodation and environmental conditions ensure a supporting
climate with influences on a patient's recovery capacity. Green spaces with
relaxation areas, maintaining a well-adapted sound threshold, brightness of
rooms and common spaces, used colour range, adaptation and marking of the
journeys of patients with physical particularities, provision of a companion while
travelling through the hospital contribute to the formation of a climate
favourable to health or balance. The access to the hospital, wards, saloons,
bathrooms and furniture or bathrooms tailored to the patients’ particularities or
recreation facilities contribute to the comfort perceived by the patient or
caregivers.
- Cleaning, disinfection and antisepsis of premises and equipment should ensure a
safe care environment.
The observance of cleaning, disinfection and asepsis conditions protects
the patient against the infections associated to the medical procedures and
contributes to the maintenance of his safety.
- Ensuring the patient-adapted diet safety conditions
The diet adapted to the pathology for which he has been admitted,
associated pathology, special physiological states or preferences resulted as a
consequence of religious beliefs, etc., which is safely provided, is part of the
individualised healthcare services provided to the patient.
The specific objectives for meeting the standard are:
- The care environment organisation complies with the conditions on the capacity
and competences undertaken by the hospital
- The care environment is evaluated and permanently tailored to the healthcare
needs

133
To meet the specific objectives, the hospital carries out the following activities:
The environment of care is organized to comply with the
hospital's capacity and competencies.
01.09.01.01. Patient accommodation conditions meet the particularities of each
patient.
01.09.01.02. Care is provided with respect for the right to privacy.
01.09.01.03. Patients circulate in a safe and comfortable way on well-established
routes.
01.09.01.04. Cleaning and disinfection of spaces and equipment is regulated and
monitored.
01.09.01.05. The institution ensures and assumes the quality of sterilization.
01.09.01.06. The patients' meals are established in accordance with the hygienic-
dietary recommendations corresponding to pathology.
01.09.01.07. The institution provides qualitative and quantitative nutrition for
patients, caregivers and medical staff in safe food conditions.
01.09.01.08. The institution ensures the circulation of food in compliance with
hygiene rules.
01.09.01.09. The institution provides qualitative and quantitative linen, laundry
and effects for patients, caregivers and medical staff.
01.09.01.10. The institution ensures that the circulation of linen, laundry and
effects complies with hygiene rules.
The environment of care is evaluated and permanently adapted
to the needs of healthcare.
01.09.02.01. The institution continually evaluates and improves patient
accommodation conditions.
01.09.02.02. The institution continually evaluates and improves food services.
01.09.02.03. The institution continually evaluates and improves the laundry
service.
01.09.02.04. The institution constantly evaluates and improves the environment.

134
02. Clinical management
The reference goal is to focus the healthcare services on knowledge and satisfaction
of the patient’s needs generated by illness in safe clinical conditions.
The hospital must implement the best practices (efficient, effective and safe for the
patient), in accordance with his health needs, providing the access to healthcare services
and their continuation in a way that allows the traceability of processes through proper,
non-bureaucratic and real-time documentation.
The major objectives of the reference are:
Definition of the hospital mission depending on the level of available
resources, establishing the level of competence, expressed according to
the types and complexity of available services determined by the
technical, material and professional capacity;
Establishment of the consistency between the patients’ healthcare needs,
hospital mission and resources;
Limitation of medical services provided within the hospital competences;
Ensuring the quality of medical services and the patient’ safety, by
continuously monitoring the results of healthcare, their effectiveness and
efficiency.
The clinical governance follows the stages of the patient’s journey from the taking over
to the solving of the case, its objectives being reflected in the presented standards.

135
The provision of healthcare to patients is done
according to their needs, hospital's mission and
available resources.
The goal of this standard is to determine the hospital professionals' and management
team's responsible behaviour in making decisions to provide healthcare to a patient so as to
avoid the provision of healthcare, under continuous, day or outpatient hospitalization of
patients whose health problems exceed the level of competence of the hospital, either by
the lack of qualification or experience of the medical team or the insufficiency of technical
and material resources.
The major objectives of the standard are:
- The hospital should define the level of competence according to the level of
performance of available human, technical, material and financial resources
- The hospital should identify the categories of patients who cannot be taken over
and the types of interventions which cannot be carried out and for which,
- either the patients are directed to other healthcare units from the
beginning, as a result of the triage
- or, after providing medical services corresponding to the level of
competence, the patients are directed to other healthcare units, for the
medical services which the hospital cannot provide but for which there
are protocols/collaboration agreements with other healthcare units.
The specific objectives for meeting the standard are:
- The hospital has established its technical and professional degree of competence
To meet this objective, the hospital professionals establish the level of high
performance of the human resources for each specialisation, confirmed by the
material resources of the hospital. Based on these, they define the healthcare
services that the hospital can offer. The target population groups benefiting from
the identified services and clinical and biological particularities thereof shall be
established. The categories of patients for whom the hospital has resources to
provide the identified healthcare services shall be established. The triage criteria
and the case solving method shall be established.
- The provision of healthcare to patients is organised to facilitate the access to
healthcare services according to their needs.
The hospital organises the patient scheduling system, complying with the
concept of system focused on the patient, avoiding bureaucracy, blockages or
postponements of required healthcare services. An efficient scheduling system

136
allows the patient who has accessed a healthcare service to follow a journey
defined and programmed by the professionals.
- The hospital has organised an emergency medical service.
The hospital is ready to ensure the access and solve the medical and
surgical emergencies addressed to the hospital. The implementation of the
triage criteria determines the decision to solve by providing healthcare to the
patient or stabilising the vital functions and directing him to another healthcare
unit. The hospital professionals are ready to receive the patient with disabilities,
special needs, aggressive or psychiatric manifestations. The hospital preparation
for the psychiatric patient is different for the hospital with special
wards/departments compared to the hospital that does not provide specialised
services. If the patient’s disease for which he has addressed the hospital is
classified into the level of competence undertaken by the hospital, and the
psychiatric disease is associated, the collaboration of the hospital with the
«proximity psychiatrist» allows the case to be resolved.
To meet the specific objectives, the hospital carries out the following activities:
The hospital has established the technical and professional
competency level.
02.01.01.01. The hospital evaluates the population groups of patients with clinical-
biological particularities, in order to identify and satisfy their needs
and specific pathologies.
02.01.01.02. The hospital has identified pathologies for which it has resources.
Access to healthcare services is facilitated according to patient
caregiving needs.
02.01.02.01. The hospital has regulated appointments and consultations for
patients.
02.01.02.02. The patient scheduling system is organized so as not to infer with
emergency healthcare interventions.

137
The hospital has organized the emergency medical service.
02.01.03.01. The hospital permanently ensures the emergency medical services,
within the limits of its competencies.
02.01.03.02. The medical staff employed in the Emergency Receipt / Primary
Emergency Unit (UPU / CPU) is qualified according to law and is
periodically trained, especially as regards the attitude in the lower
incidents.
02.01.03.03. The emergency service (the emergency ward / UPU / CPU) is
organized efficiently and effectively.
The hospital provides services adapted to people with disabilities,
special needs or aggressive manifestations.
02.01.04.01. The patient with disabilities or special needs has adequate reception
conditions.
02.01.04.02. The hospital is prepared for the management of the patient with
aggressive behaviour.
Psychiatric hospitals or hospitals with psychiatric wards provide
services adapted to psychiatric patients.
02.01.05.01. The psychiatric hospital or with psychiatric wards regulates the
involuntary hospitalization of the psychiatric patient.
02.01.05.02. The psychiatric hospital or with psychiatric wards regulates patient
internment for psychiatric forensic expertise.
02.01.05.03. The psychiatric hospital / with psychiatric wards regulates caregiving
for arrested or convicted psychiatric patients.
02.01.05.04. Psychiatric hospital or with psychiatric wards has special measures to
prevent and limit the consequences of behavioural manifestations of
the psychiatric patient that may endanger the patient, the people
around, or material goods.
02.01.05.05. The discharge of the psychiatric patient from psychiatric hospitals or
psychiatric wards is regulated and adapted to the way of admission.

138
The initial evaluation aims to identify patient's
needs in the context of known exposure to risk
factors (environmental, social, economic,
behavioural and biological) and establishes the
need for care and medical care for them.
The goal of this standard is to determine the hospital professionals evaluate the
patient in order to identify the patient's needs in the context of the exposure to risk factors
(biological, environmental, behavioural, social and economic) and planning healthcare
services in accordance with the identified needs.
The major objectives of the standard are:
- Patient’s evaluation
The patient addressing the healthcare unit, scheduled or as emergency, is
examined and the case solving method is established based on the criteria set out
by the hospital - outpatient, admission as day hospitalisation, continuous
hospitalisation or direction to other healthcare unit. The decision to admit the
patient from the outpatient department, Emergency Assessment Unit, Emergency
Department or emergency room, is followed by the patient's evaluation which is
a complex process, including the following elements:
1. Evaluation of pain using a score established by the hospital professionals
2. Evaluation of the degree of infection using Carmeli score
3. Evaluation of the risk of falling, using a score established by the hospital
professionals, followed by the patient marking, using a code perceivable
and known by the hospital professionals
4. Evaluation of the level of dependency using a score established by the
hospital professionals
5. Evaluation of disabilities and special needs
6. Evaluation of special conditions of the care environment (isolation for
infectious or immunocompromised potential, bed with protection,
foldable, with a certain height, anti-bedsore mattress, blanket allowing
heating/cooling adjustment, etc.)
7. Psycho-emotional (aggression, fear, etc.), psycho-behavioural (religious,
ethnic, etc. particularities) and socio-economic (region, age, gender
particularities, etc.) evaluation
- establishes the patient’s journey as long as it requires healthcare services
The patient's journey is established from admission, is recorded in the
medical documents, considering the evaluation from the admission and is
adapted and recorded according to the patient's evolution.

139
The specific objectives for meeting the standard are:
- The patient's needs evaluation process is well-defined in the hospital to establish
the case solving method.
- The patient's initial evaluation includes the psychobehavioural and socio-
economic factors to ensure the healthcare service continuity
To meet the specific objectives, the hospital carries out the following activities:
The hospital clearly defines the process of patient needs
assessment in order to establish the appropriate health care plan.
02.02.01.01. Depending on the patient's initial identification, a decision regarding
the patient's admission and the means of treatment as ambulatory
care / day-hospitalization / continuous hospitalization is made.
02.02.01.02. The hospital has designed a procedure to refer patients whose
pathologies fall outside of its area of competency and facilitates
access to the services they need.
02.02.01.03. The hospital regulates the recognition of patient investigations
performed by other hospital units, as well as their repetition.
Initial patient evaluation includes psycho-social and socio-
economic factors to ensure the continuity of caregiving.
02.02.02.01. The hospital provides treatment for patients with psycho-emotional
and socio-economic peculiarities that can affect the care process.
02.02.02.02. The patient's route through the system is determined in relation to
his / her psycho-social and socio-economic profile.
02.02.02.03. Management of acute or chronic pain starts from the initial
evaluation stage.

140
Medical practice addresses the patient in an
integrated and specific way, ensuring continuity of
care and health care.
The goal of this standard is to improve the collaboration between healthcare
professionals and the transformation of the medical procedure into the patient's healthcare
until the case is solved (“to cure” into “to care”).
The major objectives of the standard are:
- Unitary, multidisciplinary, integrated and adapted approach of the patient
The unitary approach of the patient is the guarantee for the patient who
addresses the hospital that if he has a condition that can be diagnosed and
treated by several professionals in the same department or in different
departments of the hospital the care is the same, being materialised for the
patient in risk mitigation.
The healthcare is a process in which a complex team made of the treating
physician, physicians of the same specialty or other clinical and paraclinical
specialties, related services (psychologist, physio-kinetotherapists, physicists,
etc.), nurses, orderlies etc., takes part. The therapeutic and care decision-making
process is coordinated and integrated by the treating physician, but it involves all
authors of the multidisciplinary team, complying with the diagnosis and
treatment protocols in the hospital, tailored to the patient’s particularities.
- Ensuring the continuity of healthcare based on evidence
The healthcare and healthcare service continuity is ensured by the
physicians and healthcare staff, which is based on the fact that the use of
hospital’s material resources continues.
The evaluations, recommendations, activities and obtained results are
recorded in the medical documents. Ensuring the continuity of healthcare also
involves the accuracy of the transfer of information to the on-call shift, change of
shift, transfer of information in the investigative process, transfer of information
from the treating physician to the healthcare staff and from the healthcare staff
to the treating physician, the transfer of information in the care process (hygiene,
food) etc.

141
The specific objectives for meeting the standard are:
- The case management is based on the use of diagnosis and treatment protocols
The diagnosis and treatment protocols belong to the hospital, are drawn up by
the hospital's professionals, adapting the Diagnosis and Therapeutic Guidelines
from the national level to the technical and material possibilities of the hospital
and the diagnostic and treatment novelties in the field. For the cases in which
there are no Diagnosis and Treatment Guidelines at national level, the reference
is represented by the specialised treaties in the field, tailored to the possibilities
of the hospital and its professional experience. Their elaboration is preceded by
the identification of the clinical diagnosis and treatment risk, evaluated and
recorded risk in the Sole Risk Register and the estimation of the residual risk after
the protocol implementation.
The format of the diagnosis and treatment protocol is unitary at the level of
hospital, mutually agreed by its professionals.
We recommend the compliance of at least the following structures in the
elaboration of the diagnosis and treatment protocol:
Abbreviations used in the document A. INTRODUCTION
A.1. Diagnosis: A.2. Code of disease (CIM 10): A.3. Users: A.4. Goals of protocol A.8. Definitions used in the document A.9. Epidemiological information
B. GENERALITIES
B.1. Level of primary healthcare institutions B.2. Level of specialised consultancy B.3. Level of in-patient unit
C.1. CONDUCT ALGORITHMS C.2. DESCRIPTION OF METHODS, TECHNIQUES AND PROCEDURES
C.2.1. Classification. C.2.2. Etiology. C.2.3. Prophylaxis C.2.4. Patient’s conduct C.2.4.1. History C.2.4.2. Physical examination

142
C.2.4.3. Paraclinical examinations C.2.4.4. Differential diagnosis C.2.4.5. Hospitalisation criteria C.2.4.6. Treatment C.2.4.7. Evolution C.2.4.8. Supervision of patients C.2.5. Complications
D. HUMAN RESOURCES AND MATERIALS NECESSARY TO COMPLY WITH THE PROTOCOL PROVISIONS
D.1. Primary healthcare institutions D.2. Departments and consultative-diagnosis institutions D.3. General departments of regional, county, and municipal hospitals D.4. Specialised centre or clinics
E. INDICATORS FOR MONITORING THE PROTOCOL IMPLEMENTATION References
Those cases which are found very rarely in the hospital casuistry and
which, for this reason, are a risk of forgetting the skills necessary for the recognition, diagnosis and treatment thereof are also considered as risk activities.
The diagnosis and treatment protocols are formalised (approved, accepted
by the legal department - as applicable, registered in the Unique Register at the QMS level), disseminated, trained by the people who apply and implement them.
The principle underlying their elaboration is ”write about what you are doing and do what you are writing”.
The structures implementing the diagnosis and treatment protocols
periodically (6 months) analyse the results of the protocol implementation. If the targeted results correspond to those obtained, they are recorded. If there are differences between the obtained results and those targeted or if changes have occurred in the diagnosis or treatment approach, the protocol has to be reviewed or re-edited, as applicable (more than 60% of the content changes determine the re-editing). The same structures periodically (1 year) evaluate the effectiveness and efficiency of the protocol implementation and if the estimated residual risk corresponds to the obtained residual risk. If there is no acceptable correspondence it is necessary to improve the protocol or to take additional measures to mitigate the clinical risk.
QMS makes the evaluation according to the planning approved by the
hospital management, the level of protocol implementation and elaborates, if applicable, the proposal for measures to improve it. The findings are submitted for approval to the evaluated sector and the hospital management.
143
- The integrated approach of the patient is useful medical practice
Achieving the goal has resulted in the implementation of the case
management through the multidisciplinary approach, establishing the patient's
journey and ensuring the continuity of healthcare services.
Multidisciplinarity in the patient's integrated approach aims at training the
teams at the hospital level, as well as at consulting the specialists in other
healthcare units, on the initiative of the hospital specialists. An organized form of
this multidisciplinary consultation is represented by the in-hospital teams,
where, following the diagnosis, the patient's situation is presented to the team,
who decides the optimal therapeutic behaviour and plans the patient for the
stages of treatment made in the hospital or other healthcare units, ensuring the
continuity of treatment and observance of the optimal time interval between its
different stages, as well as the stage evaluations with possible adaptations of the
treatment to the patient's evolution.
- The hospital ensures the continuity of the medical procedure subsequent to the
initial evaluation
The hospital’s concern to solve the case is not limited to the treatment of
the patient according to the assumed level of competence. If medical services
completing the healthcare provided by the hospital are required to fully solve the
case, its professionals order and get involved in the patient’s planning in medical
services required to fully solve the disease episode (e.g. recovery).
- The patient care plan is an integral part of the case management
The requirements of this criterion aim at determining by the management
team and professionals a responsible behaviour as regards the provision of
healthcare to a patient according to the professional competences of the
healthcare staff and the establishment of the needed healthcare staff, tailored to
the needs of the treated patients.
The healthcare plan is an assembly of organised and systematic activities
and operations allowing the provision of individualised healthcare services. This
process is focused on the specific reactions of each individual to a real/potential
health change.
Data collection - allows an inventory of all issues regarding the patient in
his entirety to be done. They inform about what the patient is, his suffering, his
life habits, and the state of satisfying the fundamental needs.

144
There are fourteen fundamental needs (according to Virginia Henderson), namely:

145
Independence and satisfaction of needs.
Independence is the state in which the individual manages to satisfy his needs through
actions that he accomplishes himself without the help of another person.
Dependence is the person's inability to undertake alone, without the help of another
person, actions that allow him to reach an acceptable level in satisfying his needs so as to be
independent.
Sources of difficulty are defined as the cause of dependency, representing any major
obstacle preventing the satisfaction of one or more fundamental needs.
The factors causing difficulty sources are: - physical and chemical factors - psychological factors - emotions, feelings, etc. - social factors - spiritual factors - lack of knowledge required for the avoidance of illnesses
The data analysis and interpretation (healthcare diagnosis) - allows the dependency
issues and difficulty sources generating them to be emphasised, namely the elaboration of
the “nursing diagnosis” which includes the communication of the patient’s results.
The healthcare planning (objectives) - shall be done by considering all sources of
information and the participation of all collaborators within the healthcare team.

146
The healthcare service planning has two components:
- the healthcare service objective aims at the attitude, behaviour, patient or
family’s action, collectivity. It has five features:
- specificity - the uniqueness of the patient
- performance - what the patient can do
- involvement - how the patient acts
- realism - how the patient acts
- observability
- intervention - allows the nurse to determine how to act to correct the patient's
dependency problems.
The execution or implementation of healthcare services (interventions) is aimed at
specifying the interventions and helping the patient to maintain or regain independence or
some degree of independence.
The evaluation is to analyse the obtained result: if the interventions have been proper,
if the desired result has been obtained, if new data have appeared in the patient’s evolution
(data which must be noted) and if the readjustment of interventions, objectives is required.
It is an absolute condition of the quality of healthcare services. The evaluation must be done
on a regular basis at different time intervals. Two issues are analysed: obtained result and
patient’s satisfaction.
- The medical data are recorded correctly, completely, in real time and avoiding
the redundancy, the access thereto being regulated
There are many substantiated reasons to keep the medical service records
and two of them are above all others:
1. The medical documents are forensic documents and include complete
records of all medical activities carried out for the patient;
2. To allow the healthcare services to continue for the patient both
inside the department and to provide the related services (e.g.
preoperative and postoperative medical treatment, emergency
medical interventions, tests, operations, etc.) the records made in the
healthcare system must be clear, accurate, correct and made in real
time (which means that they must be recorded as closely as possible
from the actual time of the occurrence of the described/archived
events).
The result for meeting this objective is to reduce unjustified bureaucracy,
to ensure the collection and recording of valid data, ensuring the process
traceability, communication between professionals and the patient.

147
To meet the specific objectives, the hospital carries out the following activities:
The case management is based on the use of diagnostic and
treatment protocols.
02.03.01.01. Health care provisions are established according to a schedule by the
treating physician.
02.03.01.02. The diagnostic and treatment protocols are established according to
the principles medicine based on evidence, clinical experience and
the technical and technical-material resources of the hospital.
02.03.01.03. Diagnostic and treatment protocols are used individually, according
to the particularities of the case.
02.03.01.04. Evaluation of the efficiency and effectiveness of the protocols is
carried out periodically.
02.03.01.05. Protocol update is performed when periodic assessment of their
efficiency and effectiveness requires so, or when new good practice
in the field is available.
An integrated approach to patient care is routinely performed in
medical practice.
02.03.02.01. The hospital provides a multidisciplinary, complete and personalized
approach of medical practice.
02.03.02.02. Interdisciplinary consultations are documented and written in the
clinical record sheet (CRS).
02.03.02.03. The second medical opinion is analysed and used by the hospital to
improve medical practice.
02.03.02.04. The hospital is concerned with the detection of patients with chronic
kidney disease (CKD).
02.03.02.05. The Multidisciplinary Oncological Commission decides on the
treatment of the oncological patient.
148
The hospital ensures the continuity of care after the initial
evaluation.
02.03.03.01. The hospital ensures the necessary conditions for the continuity of
care.
02.03.03.02. The hospital provides conditions for patient access to the necessary
recovery / rehabilitation services, depending on pathology.
The care plan of the patient is an integral part of the case
management.
02.03.04.01. Medical staff ensures complete and personalized care of the patient.
02.03.04.02. The individualized care plan is completed by the medical assistant,
based on medical recommendations.
02.03.04.03. The care plan is designed according to the patient's evolution.
02.03.04.04. At discharge, a care plan is developed which is transmitted both to
the patient / family member and the family doctor / physician who
sent the patient to hospital.
02.03.04.05. The need for medical care staff is established according to the need
of patient care.
Medical records are filled out correctly, completely and on time
real time, avoiding redundancy, while access to them is regulated.
02.03.05.01. The hospital establishes the necessary data to be collected, recorded
and monitored throughout the hospitalization period.
02.03.05.02. The medical staff records information on the care that has been
provided, the results of the investigations and the therapeutic
recommendations according to specialty.

149
The hospital promotes the "baby-friendly" concept
(BFH).
The goal of this standard is to make the hospital adapt the provided healthcare
services which it provides to the specific nature of the healthcare services required for the
child, tailored to the particularities of his age stages.
The major objectives of the standard are:
- Adaptation of healthcare services for hospitals with neonatology/premature
babies wards/departments
The particularity of healthcare services in hospitals with
neonatology/premature babies wards/departments is represented by the
amplitude of the prevention in carrying out hospital activities. It includes the
education of caregivers, the immunisation of patients and the early identification
of the newborn malformations.
- Adaptation of healthcare services for hospitals with paediatrics
wards/departments
The child needs a care environment tailored to the specific development
stages and the conditions offered by the hospitals providing paediatric medical
services must be an answer to the identified particularities.
The specific objectives for meeting the standard are:
- The hospital has adopted a policy to promote the breastfeeding in the
neonatology departments
The breastfeeding is a WHO recommendation and is the best immediate
natural immunisation program of the newborn and the active involvement of the
specialists in informing the parents of the breastfeeding benefits during
pregnancy ensures the best conditions to accept it and ensures the premise of a
child's eutrophic development.
- The hospital is concerned with the identification and prevention of illness in
newborns.
The information of parents to understand the benefits of vaccination in
children, the first immunisation and early discovery of malformations of the
newborn, initiating or guiding for treatment in specialised services, are the
priorities followed in hospitals with neonatology/premature babies
wards/departments
- The hospital is concerned with ensuring a friendly climate, adapted to the child.

150
Besides the furniture and bathroom adapted to the child's needs, he needs
the presence of a parent during hospitalisation. Play areas or schooling conditions
for school-aged children with long-term hospitalization are some of the
adaptations of hospital conditions that aim to reduce the risk of healthcare
services provided to a child.
To meet the specific objectives, the hospital carries out the following activities:
The hospital has adopted a policy to promote breastfeeding in
neonatology departments.
02.04.01.01. The hospital supports a breastfeeding program as a healthy diet for
newborn and infant feeding.
02.04.01.02. Mothers who are hospitalized are informed about the benefits of
breastfeeding.
02.04.01.03. Medical staff in obstetrics-gynaecology and neonatology is
continuously trained to acquire the skills needed to implement the
Breastfeeding Promote Program.
02.04.01.04. The hospital provides facilities to promote and support
breastfeeding.
The hospital is concerned with the identification and prevention
of newborn illnesses.
02.04.02.01. The hospital prevents newborn infectious diseases.
02.04.02.02. The hospital identifies newborn malformations / deficiencies.
The hospital is concerned with ensuring a friendly climate for
children.
02.04.03.01. The hospital provides conditions adapted to child care.
02.04.03.02. The hospital provides support services for childcare.

151
The paraclinical services correspond to the
investigation needs.
The goal of this standard is to establish the conditions for the provision of paraclinical
services to ensure the continuity of clinical services provided by the hospital.
The major objectives of the standard are:
- The satisfaction of the need for paraclinical services in accordance with the level
of competence undertaken by the hospital.
In order to establish the diagnosis of the patients, the specialised clinicians
use usual paraclinical investigations specific to the speciality and complexity of
the undertaken pathology. The features of provided paraclinical services are:
1. satisfy the need for investigations;
2. the acuity of results,
3. the time from making the recommendation to issuing the results, with
the possibility of prioritizing the emergencies,
4. the information of the used reference intervals,
5. the use of a signalling system for the results outside the reference
range,
6. the use of an alert system for critical results.
- Management of the paraclinical investigation process, including the pre-
examination, examination and release of the results
The result of the paraclinical investigations is dependent on the entire
examination process, which begins with the patient's preparation for the
investigation and/or the method of sampling (if applicable), the way of recording
the established data, the transport of the samples (as appropriate), the
conditions of the investigation, the validation of the investigation with the
interpretation of the results and sending them to the prescribing physician. The
errors may intervene in any stage and may influence the accuracy of the result.
The laboratory monitors all stages to ensure the fidelity of the issued
results.
The specific objectives for meeting the standard are:
- The entire activity of the paraclinical services is done in collaboration with the
clinicians
The needed paraclinical services are established together with the
clinicians, depending on the specialties which they serve, the complexity of the
treated cases, the time required to receive the results, human resources and
existing materials of the laboratory, average of estimated applications.

152
- The paraclinical services answer the patients’ needs for investigation as regards
the accessibility, quality and time interval until the results are obtained
The evaluation of the entire investigative process is a permanent concern,
which results in errors being identified and corrective measures being taken and
repetition being prevented.
- The laboratory is concerned with the satisfaction of the investigation needs in
optimal conditions
For the investigations whose efficiency requirements are not met or for
which the hospital has no resources, it can be opted for the service outsourcing,
until they reach their profitability threshold or obtain the necessary resources.
For the outsourced services, the hospital ensures that the accuracy of
investigation is complied with by the contractual terms.
The training of own and external staff of the laboratory involved in the
patient’s preparation for investigation and/or the sampling method (as
applicable) is done by the laboratory staff, prepared in this regard.
To meet the specific objectives, the hospital carries out the following activities:
The whole activity of the paraclinical services is carried out in
collaboration with clinical doctors.
02.05.01.01. The sections define and estimate the need for paraclinical services
depending on the hospital competency level.
02.05.01.02. The paraclinical services specialists are part of the multidisciplinary
team to treat complex cases.
Paraclinical services respond to the needs of investigating
patients in terms of accessibility, quality and time to achieve
results.
02.05.02.01. Monitoring and analysis of nonconformities are used to improve
paraclinical activity.
02.05.02.02. The reference intervals of the investigation results, the alerting
values and the established critical values, are communicated at the
same time with the results' transmission.
02.05.02.03. The practices of radio-diagnostic, interventional radiology and
functional explorations are focused on the real needs of the patient,
while being monitored and evaluated periodically.

153
The laboratory aims to meet investigation needs in optimal
conditions.
02.05.03.01. The laboratory establishes solutions to meet investigation needs
efficiently and effectively.
02.05.03.02. The hospital has regulated the necessary conditions for conducting
the laboratory pre-examination and post-test procedures.
The Nephrology Hospital / Nephrology
Department Hospital ensures the continuity of
medical assistance for patients with chronic kidney
disease.
The goal of this standard is to increase the life quality of patients with a chronic kidney
disease.
This goal is achieved by the patient's integrated approach, in multidisciplinary teams,
with the involvement of all professionals with whom the patient interacts in order to identify
those areas of chronic renal failure where therapeutic effort, research and social support are
very important.
The major objectives of the standard are:
- decrease in patients with kidney function substitution treatment
Early identification of kidney disease as a basic disease or as a consequence
of a cardiac disease, screening of the parameters identifying its onset, with the
monitoring of treatments, patient approach in multidisciplinary in-hospital teams
and their collaboration in integrated medical network, initiation of kidney
function substitution treatment at the right time, generates control of the
number of patients with kidney function substitution treatment.
- decrease of mortality in patients with kidney function substitution treatment
Integrated approach of patients with kidney function substitution
treatment, with active involvement, including of the family physician, in the
supervision, monitoring and health education of patients of this type, continued
medical supervision have a great influence on the prevention of complications
with impact on the mortality of the patient with kidney function substitution
treatment.
154
- increase in the quality of life of the patient with chronic kidney disease
The preparation of a plan of measures that ensures and acts on preserving
the dimensions of the quantitative indicators, but especially of the qualitative
indicators of life quality, is the first step to stop the complications and, implicitly,
to preserve the quality of life of the patients with chronic kidney disease. The
study of the quality of life of patients suffering from this disease is a precursor to
the development of rehabilitation programs, which ultimately aim both at
lowering the cost of healthcare services for these patients and increasing the
quality of life.
The specific objectives for meeting the standard are:
- The Nephrology Hospital or the hospital with nephrology departments provides
the patients with CKD with the access to individualised kidney function
substitution treatment (KFST) and in due time
- The effectiveness and efficacy of KFST (kidney function substitution treatment)
are constant concerns of the dialysis unit
- The daily hospitalization dialysis unit monitors the evolution (medical
performance of dialysis treatment) of dialysis patients
To meet the specific objectives, the hospital carries out the following activities:
Spitalul de nefrologie sau cu secții de nefrologie asigură accesul
pacienților cu BCR la tratamentul de supleere a funcției renale
(TSFR) individualizat și la momentul optim.
02.06.01.01. The patients registered in the nephrology unit / division are treated
and monitored to reduce the CKD progression rate.
02.06.01.02. The hospital with nephrology units / divisions prepares CKD patients
for renal replacement therapy.
RRT efficiency and effectiveness are constant concerns for the
dialysis unit.
02.06.02.01. The unit that initiates dialysis decides on how RRT is conducted
(haemodialysis, peritoneal dialysis, kidney transplantation), in
agreement with the patients and their families.
02.06.02.02. The unit that initiates dialysis collaborates with the nephrology units
/ divisions that recommend the initiation of treatment and with the
ambulatory dialysis centres that perform the dialysis treatment.

155
The day-care hospital dialysis unit monitors the evolution
(medical performance of dialysis treatment) of dialysis patients.
02.06.03.01. The day-care hospital dialysis unit records and communicates on-line
and in real time all parameters for monitoring the medical
performance of dialysis treatment in the format and frequency
requested by the Romanian Renal Register.
02.06.03.02. The day-care hospital dialysis unit controls the anaemia of dialysis
patients.
02.06.03.03. The day-care hospital dialysis unit controls mineral metabolism.
02.06.03.04. The day-care hospital dialysis unit controls acidosis.
02.06.03.05. The day-care hospital dialysis unit monitors the infectious disease
specific to the patient receiving dialysis.
02.06.03.06. The day-care hospital dialysis unit monitors the nutrition status of
dialysis patients.
02.06.03.07. The day-care hospital dialysis unit monitors dialysis efficiency (HD /
DP).
02.06.03.08. The day-care hospital dialysis unit is concerned about the life quality
of the patients.
02.06.03.09. The dialysis unit has a policy of increasing patient autonomy.
Radiotherapy and/or nuclear medicine ensure(s)
the specific treatment needs.
The goal of this standard is to ensure the access of all neoplastic patients, who have
been recommended radiotherapy, to this treatment, in the optimal period recommended by
the oncological team.
The major objectives of the standard are:
- Increased survival and quality of life for neoplastic patients, for all locations with
radiotherapy/nuclear therapy

156
- Improvement of the specific radiotherapy activity indices (shortening waiting lists, taking the optimal number of patients, specifying the purpose of radiotherapy - curative, symptomatic, palliative, adjuvant)
- The use of modern advanced radiotherapy techniques (modulated radiotherapy, image-guided radiotherapy, total body irradiation, stereotaxia), which make it possible to achieve extremely precise, high-intensity irradiation, which has, at the same time, minimal side effects and complications, thereby providing patients with better quality of life
- Diversification of radioactive isotopes used in nuclear medicine with the extension of its scope and in the palliative sector, improving the living conditions of patients.
The specific objectives for meeting the standard are:
- The radiotherapy/nuclear medicine practice is adapted to the specific needs of
the patient
- The radiotherapy/nuclear medicine practice is monitored and evaluated
periodically
To meet the specific objectives, the hospital carries out the following activities:
The practice of radiotherapy / nuclear medicine is adapted to the
specific needs of the patient.
02.07.01.01. Radiotherapy / nuclear medicine service equipment meets patient-
specific treatment needs.
02.07.01.02. Radiotherapy / Nuclear Medicine comply with the rules of good
practice.
The practice of radiotherapy / nuclear medicine is monitored and
evaluated periodically.
02.07.02.01. Radiotherapy / Nuclear medicine used in the treatment of the
oncological patient is monitored.
02.07.02.02. The practice of radiotherapy / nuclear medicine is constantly
evaluated and improved.

157
Palliative and terminal care addresses patients
with progressive chronical diseases and their
families, seeking to improve their quality of life by
relieving suffering.
The goal of this standard is to encourage the hospital in the holistic approach of
palliative healthcare services, by developing and ensuring the continuity of palliative
healthcare services, promoting the quality, consistency and safety of these services, and the
collaboration between palliative healthcare service providers and other healthcare units
involved in caring for these patients.
The major objectives of the standard are:
- holistic approach, interdisciplinary case management
- use of standardised instruments in evaluation and documentation
- evaluations in dynamics
- precision in pain diagnosis and other symptoms
- implementing the palliative guidelines
- ensuring the accommodation conditions for persons with high level of
dependency, with adapted equipment, specialized and continuously trained staff
- prevention of the emotional exhaustion risk
- professional assistance in the terminal phase and mourning period.
Palliative healthcare service refers to that healthcare focused on the patient and family optimizing the life quality by anticipating, preventing and treating the suffering. The palliative healthcare service is provided throughout the chronic progressive disease with concomitant treatments that aim at extending the survival and address the patient's physical, intellectual, emotional, social and spiritual needs by facilitating his autonomy through access to information and decision-making. The palliative healthcare service is also addressed to the patient's family, supporting them in coping with the complex consequences of the illness, disease-related dependency and provides support during the mourning period. Terminal healthcare service is a component of palliative healthcare service and refers to the patient's last days of life when the focus is on providing the patient comfort and support for the family, a support that continues during mourning.

158
The specific objectives for meeting the standard are:
- The management of patients with progressive chronic diseases and palliative
healthcare needs is individualised and non-discriminatory
- The palliative healthcare services are provided in a proper environment, as close
as the familiar environment, adapted to the patients with high level of
dependency.
- The palliative healthcare services ensure the improvement of the quality of life of
the patient and the family/caregivers
- The palliative healthcare service is provided by a pluridisciplinary team
- The terminal phase management respects the dignity and comfort of the patient,
providing family support
To meet the specific objectives, the hospital carries out the following activities:
The management of the patients with progressive chronical
diseases and with needs of palliative care is individual and non-
discriminatory.
02.08.01.01. The needs of palliative care for the patients with progressive
chronical disease are promptly identified and adequate measures are
taken.
02.08.01.02. The hospitalization of patients with chronic progressive illness and
palliative care needs is based on the decision of a multidisciplinary
commission.
02.08.01.03. The staff involved in the care of the patients with progressive
chronical diseases has undergone certified training in palliative care.
02.08.01.04. Pain and the other symptoms that are specific to progressive
chronical diseases are controlled through adequate measures.
02.08.01.05. Complex case patients with progressive chronical diseases receive
palliative specialized care.

159
Palliative care is provided in a home-like environment, adapted to
the patients with a high degree of dependency.
02.08.02.01. The infrastructure is adapted to the special needs of the patient on
palliative care, with a high degree of dependency, by respecting his /
her intimacy.
02.08.02.02. The infrastructure allows for palliative care related services to be
carried out.
Palliative care services allow for improvement in the life quality of
the patient and of his / her family / guardians.
02.08.03.01. On patient admission in the hospital palliative care ward, a
comprehensive evaluation of the patient / family / guardians is
performed.
02.08.03.02. The aims of palliative care, the understanding of the diagnosis and
prognosis are assessed and documented along with the patient /
family / family member.
02.08.03.03. The signs and symptoms of the terminal condition are evaluated
using standard scales and are documented.
02.08.03.04. The management plan of the patient in need of palliative care is
developed by a multidisciplinary team, based on specific and updated
protocols, according to the evolution of the pathology or changing
needs of the patient / family / guardians.
02.08.03.05. Communication between the medical team and the patient / family /
guardians is permanent and plays an important role in palliative care.
02.08.03.06. On discharge, the patient's options regarding care continuity are
taken into account.
Medical palliative care is provided by a multidisciplinary team.
02.08.04.01. The minimal structure of the multidisciplinary team comprises: a
palliative doctor, pharmacist clinician, nurses, social worker,
psychologist, spiritual mentor.

160
02.08.04.02. Taking into account the patient needs, the multidisciplinary team
includes other specialists, such as: kinesiotherapy therapists,
occupational therapists, play therapists, dieticians, volunteers, etc.
02.08.04.03. The members of the multidisciplinary palliative care team of the
palliative care services undergo continuous training programs.
02.08.04.04. The institution has a coherent program of monitoring and support for
the health of the staff involved in palliative care.
The management of the terminal condition respects the dignity
and comfort of the patient, ensuring family support.
02.08.05.01. The terminal condition is identified and the family / guardians are
informed.
02.08.05.02. The medical staff observes the protocol of terminal condition.
Pharmaceutical and medication management
ensures the continuity of treatment and patient
safety.
The goal of this standard is to establish the conditions for the provision of
pharmaceutical services to ensure the continuity of clinical services provided by the hospital
so as to allow the establishment of the traceability of the medication.
The major objectives of the standard are:
- the treatment schedules tailored to the patient's individual needs are supported by existing medication, ensuring the continuity of healthcare services
- the records of the pharmaceutical service are clear, exact, accurate, complete,
current, allowing the monitoring of drug traceability and intervention where it
requires evaluation, control or correction of a process, pharmacoepidemiological,
pharmacovigilance and economical-financial evaluations of treatments prescribed
for the judicious use of medication.

161
The specific objectives for meeting the standard are:
- In the hospital, the rules of medical prescription and prescription monitoring are
used.
- Infrastructure and organisation of pharmaceutical activity support the traceability
of common medication
To meet the specific objectives, the hospital carries out the following activities:
The hospital follows regulations and guidelines on prescribing
medical substances and monitors prescriptions.
02.09.01.01. The hospital has established conditions for medication prescription
that are acknowledged by the unit / pharmacy.
02.09.01.02. Pharmacologists / Clinical pharmacists are actively involved in
prescribing and monitoring medication.
02.09.01.03. The pharmacy provides the medication that is necessary to support
the continuity of the medical treatment.
The infrastructure and organization of the pharmaceutical activity
support the traceability of common medication.
02.09.02.01. The activities and responsibilities specific to the pharmaceutical
specialty are recorded according to the legislation in force.
02.09.02.02. The organization of pharmaceutical activity is based on specific
procedures and instructions.
02.09.02.03. The organization and equipment of the pharmacy comply with the
legislation in force, in accordance with the traceability of the
medicinal product.
02.09.02.04. The informational route of pharmaceutical products is respected.
02.09.02.05. Medication from clinical trials is maintained and managed under
optimal conditions by the hospital pharmacy / chief pharmacist, and
its use is monitored by the pharmacist / clinical pharmacist.

162
The hospital has implemented good practices on
antibiotic therapy.
The goal of this standard is to make the professionals and hospital management make
a collective effort to adopt the measures to correctly use the antibiotics allowing the
provision of the best possible treatment for the patient and the limitation of the rick of
bacterial resistance.
Proper use of antibiotics, in addition to complying with all rules of drug therapy, should
also take into account their particularity regarding their interaction with microbial flora,
leading to the selection of resistant pathogens that can be transmitted in the context of
medical procedure-related contamination.
High antibiotic consumption, prevalence of resistance, additional infection-related costs, patient's safety risks require that the healthcare units undergo a process of improving their own practices, with the regular evaluation of the effectiveness of medical practices with regard to this risk.
The major objectives of the standard are:
- Improving the quality of healthcare and patient's safety.
- Preventing emergence of resistant microbial flora. - Respect for good practice in antibiotic therapy with a multidisciplinary approach
in a team consisting of a clinician, microbiologist, infectious disease physician,
epidemiologist and clinician pharmacist and compliance with the "gold
standards" in the choice of antibiotic and in the combination of antibiotics
The specific objectives for meeting the standard are:
- The hospital has organised the prescribing and monitoring of antibiotic therapy The judicious use of antibiotics in the hospital involves two categories of activities: the organisation of the general antibiotics prescription, release, distribution and administration methods at the unit level, e.g. the regulation based on prescription protocols, aimed at preventing the emergence of resistant microbial flora.
- The prescription of antibiotics is medically grounded and ensures the traceability
of their use
The antibiotics prescription should consider its recording in medical documents and the correct transmission of information to all parties involved in releasing, delivering, distributing and administering medications, such as the patient identification data, dosages, routes and pace of administration, the name of the prescriber, ensuring the traceability of the process, analysis of consumption and fairness of prescription.

163
In order to improve the initial choice of antibiotics, it is advisable to: develop protocols according to the type of infection and the ecological specific nature of the hospital, which are easily accessible for the medical team; the existence of the reserve list of antibiotics with specific indications of their use; the access to information, preferably through a computer system, to help prescribe antibiotics correctly (recommendations, information on bacterial resistance, alerts taking into account the service protocols and patient particularities); the revaluation after 24-72 hours, depending on the clinical course, obtaining microbiological data, to determine the nature of the bacterial infection; the extension of the treatment over three to four days should be subject to an interdisciplinary analysis and endorsed by the chief physician of the department; the approach of antibiotic therapy from the point of view of infectious risk management, identifying the prescribing and administration errors; the establishment of the preventive measures is an obligation of the responsible structures within the hospital management. For most infections, monotherapy is sufficient. The antibiotic association can aim at rapidly destroying the microbial inoculum, avoiding the development of resistant bacteria, but can result in increased selection pressure on commensal flora. For this reason, it is only necessary for the association to be made in well-defined and substantiated cases. The association aims at expanding the antimicrobial spectrum in case of severe infections which are difficult or impossible to be microbiologically documented, Pseudomonas aeruginosa infections, etc. No two antibiotics of the same class or with side effects for the same organ
are associated, and, as a rule, the antibiotic association is not maintained for
more than three days (according to Azoicăi and Manciuc, 2008).
- Hospital pharmacy is directly involved in meeting the good antibiotic therapy
practices
The pharmacy follows the dynamics of antibiotic use, continuously
providing the antibiotics necessary for the treatment and prophylactic antibiotic
treatment, established together with the hospital professionals, by constantly
informing them (including the laboratory) of the existing antibiotics and the
consumption for each physician.
- The activity of the microbiology laboratory supports the observance of good
practices in the use of antibiotics
The collection of microbiological samples is done prior to the initiation of any antibiotic therapy, even in situations of severe infections, such as septic shock requiring the administration of antibiotics from the first hour; the antibiotics are administered only when there are clinically-biological arguments evident for the presence of bacterial infection or an emergency for the prognosis of the patient; the antibiotic is chosen according to the known sensitivity of the microbial flora in question but with the least effect on the commensal flora; the

164
effect of antibiotic therapy is re-evaluated after 24-72 hours and recorded in the observation chart; the management of antibiotic therapy is done only after the antibiogram; the posology and the rate of administration are individualised taking into account the particularities of the case (age, associated pathologies - renal, hepatic impairment, medullary aplasia, etc.); the decision to extend the antibiotic therapy over seven to ten days should be clinically and biologically substantiated (in prolonged therapy, the benefit/risk ratio is unfavourable); the oral route of administration is preferred, if possible. The antibiotics used for the antibiogram must respect the sensitivity of germ classes (restricted spectrum antibiotics are recommended), should be adapted to existing antibiotics in the hospital pharmacy, subject to the conditions of effectiveness and efficiency of use. The laboratory monitors the evolution of microbial resistance to the used
antibiotics and informs the clinicians about its acquirement.
- The clinical services have regulated the use of antibiotics, according to good
practice
The prescribing physicians monitor the changes in microbial susceptibility
to antibiotics and to overcoming the accepted resistance threshold and may
decide to stop antibiotics in the hospital for a while. The decision to change the
used antibiotics is in line with good practice.
The used prophylactic antibiotic treatment takes into account germs found
in the hospital, their susceptibility to antibiotics, the target of their use, and their
effectiveness. The antibiotics used in illness prevention adapt annually to
dynamic conditions in the hospital.
To meet the specific objectives, the hospital carries out the following activities:
The hospital has organized prescription and monitoring of
antibiotic therapy.
02.10.01.01. The hospital has established the functional structures with
attributions in the implementation and monitoring of good practices
on antibiotic usage.
02.10.01.02. The structures involved in the implementation and monitoring of
good practices on antibiotic usage have established handling
procedures.

165
Prescription of antibiotics is medically justified and ensures the
traceability of their use.
02.10.02.01. Prescription of antibiotics is performed according to recognized
antibiotic guidelines and antibiotic results, as appropriate.
02.10.02.02. Prescription duration is established according to evolution and is
documented.
02.10.02.03. Records of antibiotic prescription allow for the traceability of its use.
The hospital pharmacy is directly involved in observing good
practices on the antibiotic therapy.
02.10.03.01. The pharmacy provides the necessary antibiotics, taking into account
the evolution of antibiotic resistance, and monitors the consumption
of antibiotics and the complete route of the dispended products,
including those that have not been administered.
02.10.03.02. The pharmacy checks whether good practices on prescription and
usage of antibiotics are followed.
02.10.03.03. The pharmacy periodically informs the prescribers, the hospital
management and the medical staff on the available antibiotics, as
well as on the antibiotic usage across various units / bed wards.
The activity of the microbiology laboratory supports the
observance of good practices in the use of antibiotics.
02.10.04.01. The microbiology department of the medical laboratory has internal
quality control procedures for antibiotic-resistance investigations.
02.10.04.02. The microbiology department of the medical laboratory collaborates
with the Department of prevention and mitigation of healthcare-
related infections (DPMHI), with the pharmacy, physicians and with
the hospital management on the issue of monitoring data on
antibiotics resistance.

166
Clinical services have regulated the use of antibiotics, according to
good practices.
02.10.05.01. Clinical services have implemented antibiotic and antibiotic
prophylaxis regulations related to the specialty and section for the
main clinical situations.
02.10.05.02. Antibiotic consumption, as well as prescription traceability and
antibiotic usage are ensured.
Management of healthcare-associated infections
follows good practices in the field.
The goal of this standard is to make the hospital management and its professionals
show understanding and good knowledge of the risk and injuries which may be incurred as a
result of the healthcare associated infections, having a constructive concern for the
identification of multifactorial solutions aiming at the evaluation and control of the
infectious risk.
The HAI associated risks and injuries may result from:
1. The failure to know/insufficient knowledge or poor implementation of
requirements defined as Standard Precautions and Additional Precautions.
2. Antibiotic prophylaxis/antibiotic therapy schemes erroneously prescribed,
improperly and excessively implemented, which increasingly determine the
selection of bacterial strains resistant to antibiotics and/or resistance factors,
with major implications in the epidemiology of transmissible diseases, including
the healthcare associated infections and healthcare services, including the
probable onset of resistant bacteria carrier status.
3. Lack of a set of documented protocols regarding the rational use of antibiotics,
epidemiological alert, prevention and control actions, healthcare services,
hospital supervision.
4. Lack of corroboration between the control of antibiotics use and HAI supervision
and control measures.
The healthcare associated infections and healthcare services are a problem
of the healthcare systems all over the world. In the contemporary institutional
medicine, it is known that HAI may induce serious suffering to patients, such as:
- Increase of morbidity by the occurrence of complications to the underlying
disease, sequelae, dysfunctions

167
- Increase of the hospitalization period
- Increase of the rate of readmission into hospital
- Increase of costs by additional healthcare services required to be
ensured/provided to the affected patients
- Affecting the quality of the patient's life
- Patient's death.
The major objectives of the standard are:
- Development of an infectious risk management program, in which it should be
explained, understood, realized and voluntarily implemented by the entire
healthcare and technical and administrative staff and, subsequently, a continuous
and coherent supervision plan should be adopted.
- Establishing a durable culture regarding the safety and security of the patient and
the increase of the healthcare quality.
- Adherence of the staff to cleaning procedures and protocols,
disinfection, sterilisation, hand hygiene, use of biocidal products and medical
devices, observance of aseptic and antiseptic techniques, use of disposable
healthcare and reusable materials, etc.
- Implementation of an audit for the antibiotic therapies, by monitoring
the use of antibiotics and the circulation of multi-resistant bacterial strains (the
tendency of the number of isolates of resistant microorganisms), the
implementation of rational antibiotic use measures (elimination/restriction of
classes of antibiotics, correct prescription, cyclical change of antibiotic in long-
term therapies, etc.).
The specific objectives to meet the standard are:
- The hospital management has organised the supervision, prevention and
limitation of healthcare associated infections.
- The supervision of the care environment reduces the degree of infectious risk
- The hospital's quality policy regarding the food safety considers the control of the
infectious risk.
- The clinical management of the medical structures prevents and limits the
infectious risk

168
To meet the specific objectives, the hospital carries out the following activities:
The hospital management has organized the supervision,
prevention and mitigation of healthcare-related infections.
02.11.01.01. The hospital management has adopted measures to set up structures
involved in the prevention of healthcare-associated infections.
02.11.01.02. The hospital management ensures the implementing conditions for
the provisions in the annual activity plan for the supervision,
prevention and mitigation of healthcare-related infections.
02.11.01.03. Supervision, prevention and mitigation of healthcare-related
infections and contagious diseases are organized and coordinated
across every hospital structure.
The environment of care supervision lowers the risk of infection.
02.11.02.01. The areas at risk of infection have been identified and monitored to
prevent and limit healthcare-associated infections (HAI).
02.11.02.02. The DPMHI monitors air quality and adopts measures to mitigate the
occurrence of aerogenic infections.
02.11.02.03. The impact on air quality of demolition works, construction,
renovation, maintenance of installations, etc. performed within the
hospital and the prevention and control of nosocomial infections are
managed.
02.11.02.04. The quality of sterilization is checked and supervised.
02.11.02.05. DPMHI monitors the hospital linen flow.
The hospital's quality policy on food safety aims to control the
risk of infection.
02.11.03.01. The activity of the food sector within the hospital is controlled
(hospital kitchen, food storage facilities, milk kitchen).
02.11.03.02. Compliance with food safety rules for infection prevention is
assessed.

169
The clinical management of the medical structures prevents and
mitigates the risk of infection.
02.11.04.01. The medical structures (sections / compartments, laboratories,
pharmacy, etc.) identify, assess and address the risk of infection
posed by healthcare-related activities.
02.11.04.02. Curative doctors identify patients at risk of infection and take
measures to mitigate it.
02.11.04.03. Traceability of processes regarding the appropriate use of medical
devices, sanitary materials and multi-purpose equipment is ensured
and monitored to prevent and mitigate healthcare-related infections.
02.11.04.04. DPMHI supervises compliance with the rules of hand hygiene.
02.11.04.05. The hospital complies with the national supervision procedures for
hospital-acquired infections.
02.11.04.06. The hospital manages the risk of infection the staff might be
subjected to.
02.11.04.07. The specialized hospital or the department of obstetrics adopts
measures to prevent prenatal risk of infection.
02.12. The hospital issues and implements policies
to ensure and improve patient safety.
The goal of this standard is to determine the hospital professionals identify the cases
in which the patient might suffer injuries by the intervention or non-intervention of the
medical team and the adoption of measures allowing the risk to be undertaken so as to
guarantee the patients’ safety in the healthcare system.
The patients’ safety in hospitals is the most important dimension of the healthcare
service quality. To ensure it, the professionals identify the existing risks in relation to the
healthcare activity. They can be:
- Voluntary clinical risk - when the physician assumes an intervention, with known
risk, so as to increase the performance of treatment (example - the decision to
use a more aggressive chemotherapy protocol, to increase the recovery chances,
but with most known side effects)

170
- Involuntary risk - is the exposure to risks occurring as a result of errors or
unknown risks, about which there is no information (example - erroneous dosage
of medication, erroneous transmission of medical information, etc. or side effects
to medication, which were not notified until that date).
The acceptable risks are residual risks or risks remaining after all preventive
measures have been taken. Their acceptability equally aims at the medical team
and the patient:
- Acceptability of professionals - of the technical risk by the physician and his team:
the risks of interventions which can be avoided or mitigated by
professionalism/competence of the medical team/existence of resources,
undertaking an attitude with lower injuries vs. an attitude with higher injuries
(side effects of medication, harm of a mutilation surgery - amputation of the
diabetic leg)
- The risk acceptability by the patient is done by his informed consent
- The social acceptability is marked by the emotional nature of the risk
acceptability - road accidents vs. aviation accidents, provided that the society
becomes more and more demanding (example - in the past, old age was deemed
a cause of death, and the expectations from the healthcare system were limited,
but these expectations currently increased.
The risk acceptability in healthcare involves the consideration of these three issues of
the acceptability level: by the society, by professionals, by the patients.
Taking risks is inseparable from human activity. In healthcare, the non-taking of risks
paradoxically leads to the increase in risks for the patient. The risk management aims at
balancing the rate between the benefits and injuries to make the risk acceptable.
The major objectives of the standard are:
- Identification of clinical risks
- Elimination of unacceptable clinical risks
- Prevention of acceptable risks which are required to be undertaken for
the patient’s protection.
The identification of risks aims at obtaining the maximum safety for the patient, is
done as a result of the evaluation of the degree of risk according to the likelihood of
occurrence and the impact of the consequences.
The risk management is done through the adoption of protocols and procedures that
are part of the measures designed to prevent or limit their occurrence.

171
The undertaking is done at the level of:
- Hospital, by establishing its mission according to the competence
- Department, by establishing the undertaken risks
- At the level of the professional team and at the level of the physician
according to the formal competences and clinical experience
The specific objectives for meeting the standard are:
- The hospital has a proactive policy for the prevention of clinical risks
The goal of the criterion is that the hospitals should provide the
corresponding specialized healthcare services according to the best practices, to
the patients deemed to have a high risk and the services deemed to have a risk
which are provided for certain categories of patients, through proper training of
the initial evaluation of patients and the provision of healthcare services.
The hospitals must provide services for a wide variety of patients. Some
groups of patients are deemed to have a high risk due to the age, general
condition, healthcare needs. This category may include children, teenagers,
vicious elders, persons who cannot talk for themselves, terminal illness patients,
patients with intense pain, pregnant women in labour, term pregnant women,
patients with psychological and emotional disorders, drug/alcohol addicts,
comatose patients, patients receiving chemotherapy, immobilized patients,
patients with transmissible diseases, abused or neglected patients, etc. They are
deemed high risk patients due to the special needs, effects of complex
treatments which they undergo, the toxic effects of the treatment, etc. These
conditions require the change of the initial patient evaluation method by
increased warning against any problems of evolution and reaction to
investigations and treatment, to identify and prevent the risks. The family’s
involvement is often required.
The services deemed to have a high risk are those involving emergency
interventions, support of the vital signs, treatment with high degree of toxicity,
etc., for groups of patients such as: patients in the emergency department,
comatose patients, patients requiring intensive care, patients with infectious
diseases, immunosuppressed patients, dialysis, healthcare services for
immobilized patients, chemotherapy, and healthcare services for patients within
the risk groups. To meet this objective, it is necessary to identify the patients and
risk services, to develop clinical protocols and procedures for evaluation and
healthcare, training of the staff to implement the protocols and procedures.
- The hospital aims at identifying and preventing the risks and errors related to the
medication.

172
The incorrect use (such as dosage, frequency, concentration, association in
the administration, etc.) of medication may determine the occurrence of adverse
events which are extremely dangerous for the patients, which is why WHO, JCI,
other organisations established a list of high risk medication. The management of
this medication requires a careful approach, differentiated at the level of hospital
departments, for the limitation of the access, correct storage, prescription,
manipulation, administration, supervision, etc. The goal is to support the
hospitals so as to structure and implement a high risk medication management
procedure to prevent the accidents associated with the administration of
medication for the patient.
- The transfer of information and responsibilities on the patient provide the
continuity of care and his safety.
The occurrence of adverse events is due to the deficit of communication
and clarity of the transfer of responsibility and essential information between the
specialists who take care of the patient: at the change of on-call shift, the change
of shift, the movement or transfer of the patient between the departments or the
transfer to other healthcare unit. The goal is to support the hospitals so as to
structure and implement regulations facilitating the patient’s safety under
transfer between shifts, departments or inside the hospital.
- The hospital aims at increasing the safety of the surgical and anaesthetic
procedures.
The surgical and anaesthetic procedures are among the most risky for
patients and are generating frequent accidents and incidents. Many organisations
implemented protocols for the surgery safety, providing the prevention of events,
such as the operation of other organ, other patient, use of other procedure,
anaesthetic and surgical incidents, etc.
This criterion follows that the hospitals adapt to their own conditions and
apply a self-control method "checklist" to avoid surgical accidents for surgical
patients and for those with invasive procedures. The multidisciplinary
involvement, improvement of communication between the professionals and
with the patients, standardisation of the process to avoid mistakes such as wrong
patient, wrong organ, wrong procedure, anaesthetic and surgical incidents, are
aimed at.
The operation of the 24/7 AICU service ensures the emergency clinical
interventions for critical patients, with the support of vital signs. The cardio-
respiratory support makes the difference between life and death or can avoid
serious brain damage. The fast performance of all processes in this sector
involves a thorough professional training with constant training that maintains at
a high level of response the AICU staff. Knowing the clinical risks and

173
implementing measures to eliminate or mitigate them is essential in AICU for the
patient survival.
- The conditions for the patients’ and staff’s radioprotection are provided in the
hospital.
The use of ionizing radiation to establish a diagnosis is not without risk for
both the patients and the healthcare staff in laboratories. Thus, the specific
regulations in the use of ionizing radiation are strict, are relatively unitary, are
applicable in all member countries of the European Community, USA, Canada.
These regulations refer both to the minimum mandatory level, the
constructive endowments of laboratories, the acceptability criteria of the used
radiological installations and the reference levels of the radiation dosages
administered to the patients in the radiological investigation process. The
national regulatory bodies (in Romania, the National Commission for Nuclear
Activities Control) authorises the use of radiological installations only if, within
the laboratories, there is an implemented quality management system which is
monitored by the holder of the authorisation (hospital), establishing a practice
self-control process, the role of the regulatory body being limited to the periodic
verification of the compliance with the conditions and limits mentioned in the
authorisations for nuclear activities. Therefore, an activity authorised by NCNAC
does not guarantee, although it requires a self-control by the hospital, the
processes specific to the medical practice using ionizing radiations.
- The hospital aims at identifying and mitigating the risks associated with the
investigative process.
The incorrect identification of the patient, the patient’s non-correlation as
individual with the indications/performance of tests, tests with their results or
prescribed and conducted treatments are frequent causes for the occurrence of
adverse events. The goal of this criterion is to help the hospitals structure and
implement a procedure for the correct identification of the patient in all
aforementioned cases.
- The hospital aims at identifying and reducing the causes generating bodily injuries
by falling/hitting.
The falling of patients in hospitals are among the most common adverse
events with important consequences on the patients, determining complications,
disabilities, extension of the hospitalisation or even death of the patients. The
goal of the criterion is to direct the hospital to proactively determine the
conditions in the hospital with the risk of falling/hitting and the patients found at
this risk, the measures to avoid such risks, the instruments to monitor such
patients.

174
- The hospital ensures the resources required to carry out the harvesting and/or
transplant in effective and safe conditions for the patient.
The organ transplant is seldom a salvation procedure, most of the time
representing the only option left for the patients with advanced diseases. The
transplant is not exempted from risks. The transmission of infections from the
donor or the contamination of the organ/tissue/cells during the transport,
keeping or even the transplant require very rigorous preventive measures and
the error-free operation of the medical team involved both in the harvesting of
the organ/tissue/cells, the monitoring of its transport, keeping and transplant
thereof.
To meet the specific objectives, the hospital carries out the following activities:
The hospital has a proactive policy to prevent clinical risks.
02.12.01.01. For each medical sector, clinical risks are periodically documented,
identified and assessed as an integral part of the risk register.
02.12.01.02. The hospital develops and implements a sentinel event management
system.
02.12.01.03. The hospital has developed and implemented a procedure for
managing adverse events and those with the potential to affect the
patient ("near miss").
02.12.01.04. The hospital has a functional patient identification system based on
at least two identifying elements.
The hospital aims to identify and prevent risks and medication
errors.
02.12.02.01. The patient medication recording and communication system
prevents incompatible or unrecommendable associations.
02.12.02.02. The storage and handling of high-risk medicine or medication with
similar names / packaging are regulated in the hospital.
02.12.02.03. Specific regulations on the storage and dispensing of psychotropic
and narcotic drugs are followed.

175
02.12.02.04. Specific regulations on the storage and release of cytostatic
medication are followed.
02.12.02.05. Specific regulations on the storage and release of electrolyte
concentrate solutions are followed.
The transfer of patient information and responsibilities ensure
continuity of care and safety.
02.12.03.01. The handover of the case is performed by following patient
information and responsibility transfer procedures, as established by
the hospital.
02.12.03.02. Patient information and responsibility transfer procedures in case
handover are monitored and assessed.
The hospital aims to increase the safety of surgery and
anaesthesia.
02.12.04.01. In Surgery and Anaesthetics, specific checklists are used to record
identification items for each case.
02.12.04.02. In medical practice, surgical and anaesthetic protocols are
implemented and followed.
02.12.04.03. Incidents occurring in surgical and anaesthetic practice are
recognized and immediate action is taken.
The hospital provides conditions for radioprotection of patients
and staff.
02.12.05.01. The general principles of radioprotection in radiodiagnosis,
interventional radiology, radiotherapy and nuclear medicine are
applied correctly and consistently.
02.12.05.02. Radiation protection principles of radiodiagnosis procedures seek to
ensure the image quality, the minimum exposure and the precise
delimitation of the area.

176
02.12.05.03. Radiation protection principles of radiotherapy / nuclear medicine
procedures seek to establish, adapt and update the individualized
treatment plan.
02.12.05.04. The principles of radioprotection of interventional radiology seek to
follow specific protocols to optimize the time of intervention.
02.12.05.05. Individuals who voluntarily help a patient are informed of the risks
associated with voluntary exposure and are provided with the
necessary protection.
02.12.06. The hospital seeks to identify and mitigate the risks
associated with the investigative process.
02.12.06.01. The clinical laboratory identifies and evaluates microbiological risks.
02.12.06.02. The microbiological risks of the clinical laboratory are analysed and
good practice rules are established.
The hospital seeks to identify and mitigate the causes of injuries
by falling / hitting.
02.12.07.01. The hospital identifies patients at risk of falling and takes measures to
prevent and mitigate the consequences.
02.12.07.02. Informing and educating the patient / guardians and staff help
reduce the risk of falling.
02.12.07.03. The hospital provides the necessary resources for carrying out the
sampling and/or transplantation activity, ensuring efficiency and
patient safety.
02.12.07.04. The hospital provides the necessary conditions for organ / tissue /
cell procurement.
02.12.07.05. The hospital provides the necessary conditions for organ / tissue /
cell transplantation.
02.12.07.06. The hospital organizes procurement / transplantation in accordance
with the regulations of the National Transplant Agency.

177
The hospital has implemented good transfusion
and haemovigilance practices.
The goal of this standard is to make the hospital establish and ensure the quality
control of the recommendation, transport and administration of blood and blood products
to safely perform the transfusion for the patient.
The major objective of the standard is:
- Implementation of hemovigilance rules
The hospital, as a third party supplier of healthcare services, is ready for
the case in which a patient may require blood or blood product transfusion. All
hospitals with continuous hospitalisation, whose structure include surgical
wards/departments, except ophthalmology, organised and authorised a Blood
Transfusion Unit. The hospitals with wards/departments for acute disease
patients in the internal medicine, paediatrics, cardiovascular, gastroenterology,
pneumophthisiology, clinical haematology, medical oncology, radiotherapy
specialties organised and authorised a Blood Transfusion Unit.
The hospital organises and monitors the blood and blood product transport
so that they are transported at a temperature adapted to each transported
product, from the Transfusion Centre to the hospital and, if necessary, from the
Blood Transfusion Unit to the building/hospital where its administration is
performed. The staff involved in the transfusion process is periodically and
specifically trained, safely ensures the administration of blood and blood
products.
The specific objectives for meeting the standard are:
- The hospital has organised the prescribing and monitoring of transfusion therapy
and hemovigilance.
- The prescription of blood and derivates is medically grounded and ensures the
traceability of their usage.

178
To meet the specific objectives, the hospital carries out the following activities:
The hospital has organized the prescribing and monitoring of
transfusion and haemovigilance therapy.
02.13.01.02. The hospital fulfils the conditions for safe transfusion therapy.
02.13.01.03. The functional structures of the hospital with responsibilities in
implementing and monitoring the correct use of transfusion therapy
comply with the specific working arrangements.
Prescription of blood and derivatives is medically based and
ensures the traceability of their use.
02.13.02.01. Prescribing blood and derivatives is performed according to the
National Guidelines for the Use of Blood and Human Blood
Components.
02.13.02.02. Blood transfusion records allow traceability of the process.
02.13.02.03. The hospital provides total blood and blood components, taking into
account the dynamics of hospitalized morbidity, and monitors the
consumption and the complete route of released products, including
those that have not been administered.
Clinical audit assesses the efficacy and
effectiveness of healthcare.
The goal of this standard is to make the hospital improve the medical activity, by
organising the clinical audit of the diagnosis and treatment protocols.
The clinical audit is a regular review of the effectiveness and efficiency of clinical
protocols. It is recommended that the analysis includes the professional team's findings
regarding the application of the protocols, overall efficacy and considerations regarding the
individualisation of the protocols and the suitability to the patients' health needs.
The analysis is done by a specialised medical structure:
- in the department - is the self-evaluation by the medical team

179
- in the hospital (for example medical council) - is the official evaluation of the
professional practice quality by the hospital management
One of the most important «indicators» for keeping under control the quality is the
variability of the professional practice expressed through costs related to the results. In the
planning process, the estimation of these costs is the starting point for the establishment of
regular monitoring and evaluation of the clinical activity.
Four stages are distinguished:
- Preparation and choice of subject - protocol to evaluate
- Evaluation
- Prospective
- Retrospective
- Revaluation
- Maintaining the actions
- Improvement actions
- The results of the clinical audit underlie the improvement of medical practice
The major objective of the standard is:
- The result of the clinical audit should determine the improvement of diagnosis and
treatment protocols
The specific objectives for meeting the standard are:
- The clinical audit activity is organised.
- The improvement of the medical activity shall be done by using the results of the
clinical audit.
To meet the specific objectives, the hospital carries out the following activities:
Clinical audit activity is organized.
02.14.01.01. Internal clinical audit missions are planned annually.
02.14.01.02. The clinical audit team is a functional part of the quality management
structure.
02.14.01.03. In situations where undesirable events occur, the clinical audit team
proposes additional missions to the hospital management.

180
Medical activity is improved by using the results of the clinical
audit.
02.14.02.01. Clinical audit recommendations are used to improve diagnostic and
treatment protocols.
02.14.02.02. The hospital aims to improve the medical activity using diagnostic
and therapeutic protocols.
The discharge and transfer of the patient is
customized according to his / her condition.
The goal of this standard is to determine the hospital professional establish the
patient’s discharge criteria according to his health and the continuity of care after discharge.
The discharge is forecasted since the patient’s admission, but the moment when this
should be done depends on the discharge criteria established by the hospital, the patient's
condition, the fulfilment of the care plan objectives and it is decided upon together with the
patient and his family, as applicable.
After discharge, the patient may need:
1. outpatient healthcare
2. home care
3. recovery healthcare
4. healthcare in a chronic disease hospital
5. healthcare exceeding the level of competence of the hospital
6. family care
The major objective of the standard is:
- Planning the continuity of healthcare after discharge
The hospital establishes the set of data accompanying the patient at
discharge, which also includes the therapeutic and care plan. It is communicated
to the family physician and/or attending consultant in the outpatient
department. The changeable factors of illness progression are identified and the
intervention method is mentioned, specifying the clinical and paraclinical
elements for monitoring the evolution of disease and the cases in which it is
necessary that the patient comes back to the hospital. The planning of healthcare

181
continuity after the discharge is done until the case is solved or the family is
assisted in case of the patient’s death.
The specific objectives for meeting the standard are:
- The discharge is planned, coordinated and documented.
- The hospital has procedures related to critical conditions or death.
To meet the specific objectives, the hospital carries out the following activities:
Patient discharge is planned, coordinated and documented.
02.15.01.01. Estimation of the discharge time is made on the patient admission
and is updated according to the clinical evolution.
02.15.01.02. The hospital follows the discharge and continuity of care procedures.
The hospital has procedures related to patients in critical
condition or death.
02.15.02.01. The patient guardians are alerted in case of degradation of the
patient's condition, including imminence of death / death.
02.15.02.02. The dignity of the patient in critical condition / terminal phase and his
/ her spiritual / cultural beliefs, previous decisions related to this
event are taken into account.
02.15.02.03. The hospital has regulated the procedure to be followed in the event
of a patient's death.

182
03. Medical ethics and the patient rights
The goal of this reference is to make the hospital establish the conditions for carrying out the activity so that it allows the achievement of qualitative goals required for the medical procedure, complying with the patients’ rights, protecting them against professional errors but also protecting the medical staff and the healthcare unit against the risk of civil liability. The recently conducted research4 in Romania have shown that the legal regulations applicable to medical practice are not known and fully complied with by the medical staff, being identified seven major fields of vulnerability in fields such as: informed consent, compliance with the medical data confidentiality, access of patients to personal medical information, access of patients to treatment - discrimination, access of mass-media, patient’s right to a second medical opinion and imitation of own specialty. The direct consequences are represented by: the risk of injuries to patients, the exit from the protection framework of malpractice insurance, and the direct harm to the quality of medical services provided to patients and their safety by failing to observe some of the rights conferred by law. The failure to know the legal regulations does not remove the physician’s/medical institution's liability.
Role of medical laws in the context of quality management If we refer to the technical/scientific component of healthcare service quality5 it is required to comply with the legal requirements applicable to medical practice, at individual (medical staff) and institutional level. The failure to comply with them draws the civil liability, with any important financial losses, together with those related to image and reputation. The civil liability of the medical staff recognises causes both in the scientific/technical component of medical practice, as well as in ethics. The law states very clearly this situation: the medical staff are civilly liable for injuries caused by "error, including negligence, recklessness or insufficient medical knowledge in the exercise of the profession, through individual acts in the prevention, diagnosis or treatment procedures”6, but also for non-observance of ethical principles applicable to medical activity ("the medical staff shall also be liable civilly for damages arising out of the non-compliance with the regulations of this title on confidentiality, informed consent and obligation to provide healthcare"7). From the point of view of the interpersonal quality component, compliance with the legal regulations on patients' rights is all the more important as they can be perceived directly by them. Patients do not necessarily have the necessary knowledge to evaluate the
4 A. Nanu, D.. Georgescu, V. Voicu, B. Ioan, Locul și relevanța prevederilor legale în contextul practicii medicale din România [Source and relevance of legal provisions in the context of medical practice in Romania], Revista Română de Bioetică [Romanian Bio-ethics Review], Vol. 9, No. 4, October - December 2011 5 I. L. Gheorghe et. al, Managementul spitalului / Şcoala Naţională de Sănătate Publică şi Management Sanitar [Hospital Management / National School for Public Health and Health Management] - Bucharest : Public H Press, 2006 ISBN (10) 973-87776-2-3 6 Art. 653, par. 2, LAW no. 95 of the 14th of April, 2006 updated, on health reform 7 Art. 653, par. 3, LAW no. 95 of the 14th of April, 2006 updated, on health reform

183
technical/scientific competence of the medical procedure, but they know how they feel, how they have been treated and whether their rights, their own moral values have been respected. The major objectives of the reference are:
adaptation of qualitative requirements of the medical service to the
current context of knowledge and compliance with the medical laws
management of civil exposure risk of professionals and hospital in the
interaction with the patients affected as a result of a medical error
In such approach, we also have to consider the health and disease as values. The values are important in the health and disease concepts.
The standards consider 13 principles:
Human dignity and human rights
Benefit and injury
Autonomy and individual responsibility
Consent
Persons without the capacity to consent
Respect for human vulnerability and personal integrity
Intimacy and confidentiality
Equality, justice and equity
Non-discrimination and non-stigmatisation
Respect for cultural diversity and pluralism
Solidarity and cooperation
Social responsibility and health
Sharing benefits

184
Few mentions are necessary to understand the philosophy of building standards:
A limitation of the rights and values of patients is the equality of opportunity in the
access to the healthcare system and distribution of resources. The financial implications of
the healthcare services and their access by the patients have opened another set of mortal
problems, all being related to justice, the right to have healthcare services and a correct
distribution of few resources.
The medical service supplier and professionals must comply with the patients’ values
although, in some cases, the patients’ values cannot be accepted by the physicians because
they are in conflict with other bioethical principles. Then the duty of the medical staff is
expressed by the "do no harm" principle. The balance between benefits and risks is essential
to determine when various processes are beneficial and when they are not.
The moral duty is not just not to hurt others but to help them and bring them benefits.
This is especially important for healthcare professionals, since their purpose is to do
everything they can for people with healthcare needs. This has always been the most
important principle of medical ethics, but today not only health professionals, but primarily
patients can determine what is beneficial and not for patients.
All ethical standards and requirements relate to the two international programming
documents:
Article 1 of the Universal Declaration of Human Rights (1848), "All human beings are
born free and equal in dignity and rights." The declaration establishes the human rights
(such as freedom of repression, freedom of expression and association) and the inherent
dignity of every human being.
The European Convention on Human Rights and Biomedicine, in Article 1, declares
protection of the dignity and identity of all people and guarantees to everyone, without
discrimination, respect for their integrity and other fundamental rights and freedoms,
related to the application of biology and medicine as a primary goal.
The ethical standards ensure respect for the patient dignity and autonomy by forcing
the provider to build mechanisms for the protection and implementation of bioethics
principles.

185
The hospital promotes the respect for the patient’s
autonomy
The goal of this standard is to involve the hospital management in the development of the
ethical dimension in the organisational culture, creating an organisational framework
ensuring the training of the staff in this field and the structure evaluating, in ethical terms,
the decisions and attitudes of management and practitioners.
The major objectives of the standard are:
- to be able to identify ethical issues in medicine
- to be able to provide rational justifications for ethical decisions
- to be able to implement the ethical principles of the Universal Declaration on
Bioethics and Human Rights
- to be able to differentiate an ethical problem from other issues
- to be able to reason with ethical issues
The specific objectives for meeting the standard are:
- The hospital ensures the conformity of medical practice with the ethical and legal
requirements which are applicable to the informed consent (IC)
- The hospital provides measures for the confidentiality of medical practice with
the ethical and legal requirements applicable to the confidentiality of the
patient’s medical data.
To meet the specific objectives, the hospital carries out the following activities:
The medical practice is regulated to be consistent with the ethical
and legal provisions that apply to informed consent (IC).
03.01.01.01. The hospital has developed procedures and policies on how the IC is
acquired.
03.01.01.02. The medical staff is preoccupied with identifying vulnerabilities in the
process of acquiring the informed consent.
03.01.01.03. Measures have been implemented to diminish the effects of the
identified vulnerabilities in the process of acquiring the informed
consent.

186
Measures regarding the consistency of medical practice with the
ethical and legal norms on patient medical data confidentiality
are in place.
03.01.02.01. The hospital uses a unique procedure to ensure confidentiality and
verifies compliance by medical staff.
03.01.02.02. Measures have been applied to diminish of the effects of the
identified vulnerabilities related to the confidentiality of the medical
data.
The hospital respects the principles of equity,
social justice and patients' rights.
The goal of this standard is to comply with the patient’s right to healthcare services, in
direct relation to his medical needs identified by the professionals but also those perceived
by the patient, to the medical documents included thereof, his therapeutic education
according to his training level, to the attitude towards illness and religious perceptions, and
to be protected from third parties' interference with him or his information. The ethical
dimension of this relationship with the patient requires in many cases an evaluation made by
professionals with special training in the field.
The major objectives of the standard are:
- Allocation of medical resources without discrimination by respecting the rights of
all people to healthcare - people with similar problems should be treated in a
similar way (horizontal equity), and people with differentiated problems should
be treated differently (vertical equity)
- The act of carrying out the professional procedure should be done by respecting
the human dignity
- The interaction of professionals and hospital with the patient shall be done by
making sure that the interest and welfare of the human being prevails the
society’s interest or science

187
The specific objectives for meeting the standard are:
- The hospital has policies to prevent discrimination in providing medical services
- The hospital ensures the access to personal medical information
- The hospital ensures the conditions required to exercise the patient's right to a
second medical opinion
- The hospital is concerned with the patients’ protection in relation to the external
environment
- The hospital regulates the audio/photo/video recording of patients for
medical/teaching/research purposes and for avoiding the malpractice accusations
To meet the specific objectives, the hospital carries out the following activities:
The hospital has policies to prevent discrimination in providing
medical services.
03.02.01.01. The hospital regulates the prevention of discrimination.
03.02.01.02. A functional and regulated ethical council has been established
within the hospital.
The hospital ensures access to personal medical information.
03.02.02.01. The hospital regulates the procedure of releasing medical documents
to patients / family members / relatives / empowered authorities.
03.02.02.02. The hospital regulates how the patient's personal medical data is
made available to authorized authorities / other institutions.
The hospital ensures the right of the patient to a second medical
opinion.
03.02.03.01. The hospital regulates the circumstances in which the patients can
receive a second medical opinion, including from doctors who are not
hospital employees.
03.02.03.02. The hospital regulates the conditions in which patients can benefit
from a second medical opinion from doctors who are employed by
the hospital.

188
The hospital is concerned with patient protection in relation with
the external environment.
03.02.04.01. The hospital regulates access of the media in the institution and to
the patients.
03.02.04.02. The hospital protects the patient against the external intrusions.
The hospital allows the patients' audio / photo / video recording
for medical / didactical / research purpose and to avoid
accusations of malpractice.
03.02.05.01. The hospital ensures the conditions and procedures for patients'
audio / photo / video recording for medical / didactical / research
purpose and trains the medical staff in this respect.
03.02.05.02. The hospital ensures the patient's audio / photo / video recording
and recording conditions for medical, teaching and research
purposes.
The hospital promotes the principles of
philanthropy and safety.
The goal of this standard is to determine the professionals and hospital management
ensure that the medical activity which they carry out improves the health and living
conditions of the patient, physicians and their patients, assuming the involvement of various
accepted degrees of injury so as to obtain the estimated result.
The major objectives of the standard are:
- Implementation of the ethical principle « primum non nocere »
- Implementation of the ethical principle of « benefit »
The specific objectives for meeting the standard are:
- The hospital requires the limitation of practice to the competence held within the
specialty
- The limits of competence are allowed to be exceeded in the patient's interest.

189
To meet the specific objectives, the hospital carries out the following activities:
The hospital only operates within the limits of its competency.
03.03.01.01. For each section, the hospital ensures medical personnel with
appropriate competencies.
03.03.01.02. The hospital provides medical staff training to prevent deskilling.
Exceeding competency is allowed for the patient benefit.
03.03.02.01. The hospital regulates the conditions of performing one's duties
outside medical competency in the patient's interest.
03.03.02.02. The hospital ensures medical staff instruction on respecting the
patient's rights in situations that require performing outside medical
competency.

190
8. DESCRIPTION OF THE EVALUATION AND ACCREDITATION
PROCESS
Enumeration of the steps taken by users in the accreditation process.
The hospital activities within the accreditation process are:
1. submits to ANMCS the request for the registration in the
accreditation process, 9 months prior to the expiration of the
previous accreditation or to the date of the evaluation visit.
2. uploads, in the CAPESARO application, the mandatory documents
for the hospital (DOS), before the start of the evaluation stage (which
includes the pre-visit, the actual visit and the post-visit)
3. pays the accreditation fee, before the start of the evaluation stage
1. in the pre-visit, answers to the requests for documents (DS) by
uploading them in the CAPESARO application, within 2 days from the
receipt of such request
2. within maximum 2 days from the receipt of the of the visit timetable in
draft version, analyses it, proposes the agreed version and appoints, by
means of the hospital manager’s decision, the hospitals representatives
who will answer to the requests of the evaluation board.
3. ensures all the necessary conditions throughout the evaluation visit
4. during the evaluation visits, presents to the evaluation board the
documents requested by the evaluation team members
5. makes available to the evaluation board all requested documents and
answers to the questions asked by the evaluation team members in order

191
to verify the compliance with the requirements of the hospital
accreditation standards
6. fills in, during the evaluation visit, all the forms and questionnaires
received from the evaluation board, including the questionnaire for
monitoring the accreditation standards (which included the users’
feedback).
7. uploads in the CAPESARO application, during the post-visit stage, all
clarification documents requested by the team of external evaluators
during the visit or included in the evaluation report.
8. agrees, with or without objections, on the draft evaluation report,
within maximum 5 days from its receipt
9. receives the evaluation report and registers it in the internal register,
on the day of its receipt from the evaluation board
10. sends feedback on the activity of the members of the evaluation
board who made the evaluation of the hospital, by filling in the
questionnaire in the CAPESARO application, after the receipt of the
evaluation report
1. receives the accreditation report and, as the case may be, the
compliance plan
2. within 6 months from the receipt of the compliance plan, puts into
practice all the requested measures
3. receives evaluation, compliance or monitoring visits, as the case may
be, on the dates set by ANMCS, ensuring all the necessary conditions for
the boards set up for these purposes
4. carries out the specific activities during the monitoring period in order
to maintain the accreditation level received: notifies the undesirable
events within the terms indicated in the methodology, receives the visits
of ANMCS for the hospital re-evaluation, as part of the monitoring
triggered by special events.

192
Description of the hospital evaluation process
Planning the visits
Evaluation visits are some of the most important processes of accreditation, which is
why they are the object of a thorough planning, including steps to be taken before as well as
during the actual visits. The first planning is made by means of the multi-annual plan, which
sets the calendar of the evaluation visits of the hospitals and which is approved by the
A.N.M.C.S. Management Board. This plan is updated permanently, as only hospitals who
meet the requirements for the initiation of the evaluation visits are planned for the
assignment to an evaluation board.
Self-assessment
The self-assessment form for hospitals is enclosed to the present Guide and also
available in the CAPESARO application. It is a standard form which allows hospitals to assess
their compliance to the accreditation standards. It also includes instructions for filling the
form. At the same time, the CAPESARO application makes available a mechanism for
calculating the estimated level of compliance to the accreditation standards. This way,
hospitals have the possibility of self-assessing their level of quality in relation to A.N.M.C.S.
standards.
Assigning the evaluation board
According to A.N.M.C.S. procedures for random selection of the members within the
evaluation boards, for those hospitals which meet the requirements for the initiation of the
evaluation visits, meaning:
they have submitted the request for accreditation,
they have submitted the documents on the structure and number of services which
are to be accredited,
they have submitted the mandatory documents and
have also delivered a self-assessment of the level of compliance by filling in the self-
assessment sheet
have paid the accreditation fee according to the minimal amount set down by
A.N.M.C.S.,
the number of the evaluation board members is established depending on the
hospital structure (number of locations, departments, beds, specialties etc.) and its
classification.

193
Evaluation visit duration
The duration of an evaluation visit varies between 2 and 5 days and is calculated so
that the time needed by the members of the evaluation board to apply the checklists does
not exceed the normal work schedule of a working day, for each of the evaluators. If
needed, in order not to exceed the 5 days maximum duration of an evaluation visit, the
number of evaluators assigned in the board can be supplemented.
Scheduling the evaluation visit
Once set the period of the evaluation visit, the evaluation board proposes to the
hospital the evaluation visit timetable, which sets the order, the location and the time of
applying the checklists, as well as the interlocutors with whom the lists are applied. This
timetable is approved with or without amendments by the hospital manager, and becomes
effective once the kick-off meeting ends.
Evaluation report
After the evaluation visit, during the post-visit period, the evaluation board prepares
the draft evaluation report, based on the applied checklists. It is then submitted to the
hospital for approval, with or without objections. Objections must be sent in writing,
through an official document signed by the hospital manager and bearing a registration
number. Within the term mentioned in the procedure, for each objection the evaluators
shall formulate an opinion and prepare support documents, which are then sent to
A.N.M.C.S. together with the hospital objections. Within the term also mentioned in the
A.N.M.C.S. regulations, the Committee for analysing objections meets, in order to accept or
reasonably reject the objections raised by the hospital. The decision of the Committee for
analysing objections is then communicated to the members of the evaluation board in order
to write the Evaluation report, which is submitted to the hospital which registers and
confirms its receipt.
The evaluation report, together with the file with the evaluation documents, are the
documents on the basis of which the accreditation level is set. Also, these are the documents
used by A.N.M.C.S. to draw up the accreditation report and eventually the compliance plan.

194
General assessment considerations and tools used:
Document Analysis
The documents to be analysed are the documents submitted by the hospital using the
application CaPeSaRo, and the documents made available by ANMCS and/or requested by
evaluators from hospital representatives during the evaluation visit.
Document analysis is performed throughout the 3 stages of the evaluation process
(pre-visit, visit and post-visit) and it is underpinned by the following principles:
At the end of each stage of the evaluation process (pre-visit, visit, post-visit) the
documents analysed shall be inventoried, with mentions of the date/period (days) of their
verification, the person (evaluator) who performed the analysis, and the checklists used to
request/analyse the documents.
N.B. The inventory of documents analysed is unique for each evaluation team and it
includes 3 sections, each related to one of the 3 stages of the evaluation process (pre-
visit, visit, post-visit). Each document analysed shall be mentioned only once in the
Register, in a separate column, and the next columns shall indicate the date/period
when the document was analysed, the name of each evaluator who analysed the
document and the list/lists considered .

195
Interview
General considerations:
The manner of conducting the interview and of formulating the questions is crucial for
collecting information and developing productive relationships.
The evaluator shall pay attention to verbal, non-verbal and para-verbal communication
(tone, attitude, voice pitch etc.) both when communicating a message and when receiving
the answer of the interviewee, as all these elements contribute to the accurate
interpretation of the information received.
When you go to interview someone, it is recommended that you should not have
other documents with you (lists, other interviews already completed etc.) besides those
strictly necessary for the interview (so as not to give your interlocutor the feeling you are in
a rush, inattentive etc.).
Avoid interference in the relationship between your interlocutor and the hospital
under evaluation (e.g.: do not say things like: “you are / you are not right...”, “I’ll speak with
them, see what I can do...” etc.).
Only 7% of the capacity to communicate with others depends on the words we use.

196
Start the interview by explaining:
All these are mentioned in the introduction of our questionnaires.
Open-closed questions
Closed questions – meaning
predefined response options – are
useful to get a direct answer to a
specific question. They may be
helpful when you have to get to the
point, when the interviewee avoids
giving specific details, lost focus or
avoids a certain subject. Closed
questions are less useful to
encourage dialogue, obtain details
or explore a certain direction.
Example of closed questions: “Do
you have an action plan for ...?”
Open or semi-open questions – meaning lack of response options, respectively for
predefined response options there are also la “other.... please indicate your opinion on etc.”
– they provide more information than the closed questions, encourage dialogue and give the
interviewee scope for answer. Examples of open questions:
“Can you describe (tell me)....?” “What is your opinion about...?”

197
The interview must end with you thanking the interviewee for his/her time and
cooperation.
At the end, it is recommended that you show the interviewee the document on which
you recorded the interview.
The self-administered questionnaire – the respondent is
given a time interval to fill in alone his/her answers (in our case,
about one day).
In this case, it is recommended that, before distributing
the questionnaires, you should brief the group of persons
targeted (employees, patients, caregivers) on the purpose of
the questionnaire and how it should be filled in. Make sure the
target group understood what the self-administered
questionnaire aims at and consent to fill it in.
Make sure that the means to collect the self-administered questionnaires observes the
right to privacy, anonymity and data confidentiality.
Direct observation
Direct observation allows the evaluator:

198
The main 3 categories of elements considered in direct observation are:
It is recommended that direct observation should be a permanent process, also
performed during the time allocated to validate other lists (interviews, focus-group etc.) or
even while walking between wards/departments, so that it conveys the evaluator as much
information as possible.
During the direct observation process, it is preferable that you are not influenced or
distracted by others (employees, patients, caregivers).
It is important to respect patient privacy when observing patient care practices.

199
Instruments used by the evaluator
The main instruments used for hospital accreditation are:
01
02
03
04
Hospital identification form – a template document developed by thespecialist structures of A.N.M.C.S., requesting the hospital to provideinformation on the identification data and on its organisational andoperational structure
List of mandatory documents requested - a template document developed by the specialist structures of A.N.M.C.S., requesting the hospital to submit those documents whose existence and compliance are prerequisites to initiate the evaluation stage
List of additional documents necessary for the evaluation and accreditation process - a template document developed by the specialist structures of A.N.M.C.S., requesting the hospital to submit those documents whose existence is necessary to initiate the evaluation visit
Self-assessment form – a template document developed by the specialist structures of A.N.M.C.S., requesting the hospital to submit information on meeting the requirements of the accreditation standards in successive stages of the evaluation and accreditation process
05Compliance Plan for evaluation purposes – a document submitted by A.N.M.C.S. to the hospital under accreditation procedure, communicating the hospital any non-compliance which prevents the initiation of the evaluation visit
06 The evaluation visit timetable – a document including the hours and theobjectives to be evaluated
07
08
09
Meetings minutes - a documents including the important aspects discussed by evaluators and representatives of the hospital under evaluation
Checklist - a template document developed by the specialist structures of A.N.M.C.S., used for data collection purposes
List of documents requested during the actual evaluation – a template document developed by the specialist structures of A.N.M.C.S., including the additional documents requested by evaluators form the hospital representatives during the evaluation process
10Questionnaire - an instrument developed by the specialist structures of A.N.M.C.S., applied at individual level only after having obtained the consent and after having guaranteed confidentiality and anonymity

200
Hospital evaluation - timetable of activities of the evaluation committee
The evaluation stage, coordinated by the evaluation committee, shall include the pre-
visit, actual visit and post-visit.
1. Pre-visit
It shall include the following main activities:
11
12
13
14
Identification and non-compliance form – a template document developedby the specialist structures of A.N.M.C.S. and filled in by evaluators, whonote, during the evaluation visit, facts disturbing the visit
Special situations form – an unilateral document drafted by the evaluation committee to indicate facts which hinder the evaluation visit or endanger patient or hospital personnel safety, submitted to the A.N.M.C.S. president, which may lead to the suspension of the evaluation visit
Draft evaluation report – a written communication submitted by the evaluation committee to the hospital, on the results of the evaluation visit for accreditation purposes, submitted to the hospital to formulate possible objections
Evaluation Report – a written communication submitted by the evaluation committee to the hospital, on the results of the evaluation visit for accreditation purposes, submitted to the hospital after having analysed and solved any possible objections
15Register of analysed documents – template form (table) developed by the specialist structures of A.N.M.C.S., which enables systematic analysis of documents

201
Briefing
Participants All ANMCS evaluators selected.
Location ANMCS – room made available for evaluators
Duration 60- 120 minutes
Activities Introduction of evaluation team members.
Presentation of hospital and self-assessment form. The team of
evaluators analyse the self-assessment form submitted by the
hospital, and become familiar with the hospital structure,
organization and particularities.
The team of evaluators receive access to CaPeSaRo, to visualise the
hospital DOS.
Appointment of the evaluation committee secretary.
Distribution of documentation (checklists, questionnaires/interview,
list of centralising documents, in-out register etc). Detailed
presentation of working instruments.
The coordinating evaluator or the physician in the team sets the
timetable; in case there is no coordinating evaluator, the physician
assumes team coordination.
Submission of timetable to the hospital by fax/e-mail.
Discussion of organisation matters.
2. Actual visit
It includes the following main activities:

202
Filling in the special situations form, in case of identifying deficiencies which endanger
patient or hospital personnel safety, by which the evaluation committee notifies such
findings to A.N.M.C.S. The A.N.M.C.S. president may decide to suspend the evaluation visit.
In this case, the accreditation process may be re-commenced, with the approval of the
A.N.M.C.S. Management Board.
The main aspects monitored, hospital disfunctionalities which may lead to the use of Special
Situations Form are:

203
Kick-off meeting
Participants All ANMCS evaluators, hospital manager and accreditation coordinator, any
other hospital employee. The coordinating evaluator shall preside the meeting –
on behalf of ANMCS.
Location To be determined by the hospital.
Duration 30 minutes - 1 hour
Activities Discussions on the visit timetable. Presentation of non-compliances in the checklists filled in during the
pre-visit stage. Drafting the kick-off meeting minute which records all discussions
during the meeting. The kick-off meeting minute is a template filled in by the evaluation committee secretary and signed by the hospital representatives who participated in the meeting and by the evaluation committee.
Description of evaluation structure and content.
Presentation of sanitation tests application.
Evaluators answer all questions related to the evaluation agenda. Evaluators
explain the use of the patient journey method.
If the time allows, it is recommended that after the kick-off meeting the evaluators
should become familiar with the room made available for their activities, with the
equipment and to make a short hospital visit:
Evaluators Induction
Participants All ANMCS evaluators
Location Room made available for evaluators
Duration 10 minutes
Activities - Evaluators become familiar with the room, check the technical equipment
(computer; fax, copier).
Hospital presentation
Participants All ANMCS evaluators; accreditation coordinator, on behalf of the hospital.
Location If the visit agenda allows, the evaluation route for each member of the
evaluation team may be presented.
Duration 30 minutes
Activities Identification of objectives allocate to each evaluator. Evaluators become
familiar with the hospital, with hospital, patient and personnel circuits.

204
Daily information meeting
Participants All ANMCS evaluators, hospital manager and accreditation
coordinator, any other hospital employee. The coordinating
evaluator shall preside the meeting.
Location To be determined by the hospital.
Duration 30 minutes - 1 hour
Objective and Activities The purpose of the meeting is to assist the organization management
understand the evaluation process.
Presentation of the evaluators team report on any changes
related to indicators the previous day, and, as applicable,
new details and information presented by the organisation
related to mentions from the information report of the
evaluators.
Validation/invalidation of numerical indicators collection and
calculation method.
Presentation of ongoing hospital processes/activities (patient
registration, discharge etc.)
Failure to fulfil sentinel indicators.
Notification of functional exploration / diagnostic or
therapeutic endoscopy laboratories; may propose a
timetable change, with the hospital approval.
These meetings shall focus on the presentation of trends which
(may) determine significant concerns and risk of non-compliance
with a standard.
The briefing is also a useful opportunity to request and receive
additional information which the hospital management can
provide.
During these meetings, the evaluators shall highlight any positive
elements or good performance identified.
At the end, the evaluation visit agenda for the forthcoming period
shall be revised and adjusted, according to the evaluation needs of
the organisation, as appropriate.
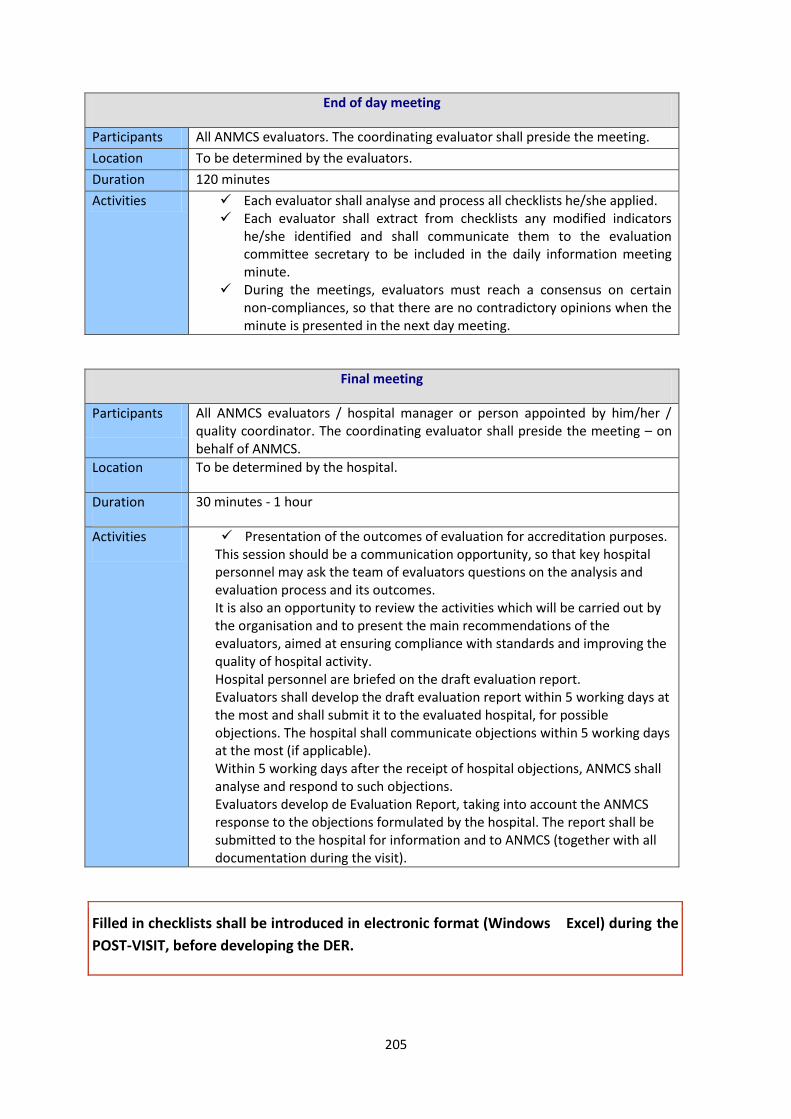
205
End of day meeting
Participants All ANMCS evaluators. The coordinating evaluator shall preside the meeting.
Location To be determined by the evaluators.
Duration 120 minutes
Activities Each evaluator shall analyse and process all checklists he/she applied. Each evaluator shall extract from checklists any modified indicators
he/she identified and shall communicate them to the evaluation committee secretary to be included in the daily information meeting minute.
During the meetings, evaluators must reach a consensus on certain non-compliances, so that there are no contradictory opinions when the minute is presented in the next day meeting.
Final meeting
Participants All ANMCS evaluators / hospital manager or person appointed by him/her / quality coordinator. The coordinating evaluator shall preside the meeting – on behalf of ANMCS.
Location To be determined by the hospital.
Duration 30 minutes - 1 hour
Activities Presentation of the outcomes of evaluation for accreditation purposes. This session should be a communication opportunity, so that key hospital personnel may ask the team of evaluators questions on the analysis and evaluation process and its outcomes. It is also an opportunity to review the activities which will be carried out by the organisation and to present the main recommendations of the evaluators, aimed at ensuring compliance with standards and improving the quality of hospital activity. Hospital personnel are briefed on the draft evaluation report. Evaluators shall develop the draft evaluation report within 5 working days at the most and shall submit it to the evaluated hospital, for possible objections. The hospital shall communicate objections within 5 working days at the most (if applicable). Within 5 working days after the receipt of hospital objections, ANMCS shall analyse and respond to such objections. Evaluators develop de Evaluation Report, taking into account the ANMCS response to the objections formulated by the hospital. The report shall be submitted to the hospital for information and to ANMCS (together with all documentation during the visit).
Filled in checklists shall be introduced in electronic format (Windows Excel) during the
POST-VISIT, before developing the DER.

206
3. Post-visit
It shall include the following main activities:
Hospital evaluation ends with submission to ANMCS of the evaluation file, by the
evaluation committee.

207
4. Evaluation File

208
Documents in electronic format shall be delivered by each member as follows:
There must be 100% match between the printed versions of the Checklists, the
information included in the minutes, and the electronic version of the Checklists.
Otherwise, the president of the evaluation committee shall submit again the entire
evaluation file to the evaluation committee, to be reviewed.

209
The evaluators and the evaluation board
The healthcare service evaluator is an individual specialised in healthcare services
quality management who holds, pursuant to law, the graduation certificate for healthcare
services evaluators or for hospital evaluators training and/or improvement courses, as
appropriate.
Evaluators are specially trained persons who, on the basis of an agreement signed with
A.N.M.C.S., carry out the external and independent evaluation process, on behalf and for
A.N.M.C.S.
The evaluation board is the team assigned by A.N.M.C.S., under the coordination of a
president, an employee of A.N.M.C.S., who has the responsibility to carry out all activities
related to the evaluation process (pre-visit, actual visit and post-visit) for a certain hospital,
and also to draw up all documents provided by the evaluation procedure of A.N.M.C.S., the
document by which the evaluation process is ended being the evaluation report.
The evaluation report is a collective document, drawn up and assumed by all members
of the evaluation board.
The activity of the evaluators in the evaluation committee
Drafting the visit timetable and selection of interlocutors with whom to apply the lists –
general rules
The visit timetable shall be established considering the following:
The evaluator consults SC Annexes and the hospital documents to establish
the sectors of activity to be evaluated;
It is recommended that, when consulting the SC to establish the
sectors of activ ity to be evaluated, patient journey in the hospital
should be considered, so that the processes underpinning the
provision of healthcare services in each type of healthcare provider
should allow for an integrated approach (including the integrated
outpatient clinic, day hospitalisation, laboratories serving the hospital
etc.)8;
8 There are cases when a hospital has multiple locations, thus it also has several SC. In such cases, evaluators shall consider
all sectors of activity involved in the healthcare service provision at the level of that hospital (e.g: hospitals which only
1. General rules

210
The necessary time to evaluate each sector is determined (based on the
maximum time recommended to fill in data collection instruments);
The information obtained by applying the steps described above (points
1.1. – 1.2.) is validated by comparing it with the Evaluation Visit Duration
Form (EVDF) developed by HEAU;
The daily timetable is set for each evaluator and agreed with all team members, taking into account: a. The maximum amount of time necessary to fill in each data collection
instrument;
b. The necessary time for evaluators to travel to external locations (if
applicable);
c. Profession and/skills of each evaluator;
d. Necessary time for the secretary to fulfil his/her specific tasks;
e. Additional time necessary for the coordinating evaluator to analyse
special situations which might occur during the evaluation visit for
accreditation purposes, to check the validation by signature of all
instruments applied by evaluators, and to advise the EC members on the
significance or role of certain indicators, in order to evaluate certain
situations or appraise special circumstances;
f. The specificity of each sector evaluated; it is recommended that:
- A.T.I. and the department of surgery/operating room/delivery
room should be evaluated ding the second part of the day, to
avoid interference with hospital activities,
- The food area should only be evaluated during the hours when
the hospital staff is not preparing patient meals,
- Radiology and Nuclear Medicine should be evaluated during
the first part of the day, considering their short working hours,
- the integrated outpatient clinic should be evaluated during the
first part of the day, when they are providing services to
patients, so that the information collected should be relevant,
- The interviews and questionnaires should be applied to
patients during the second part of the day,
- Direct observation of wards/departments should be performed
prior to the dialogue with the head nurse of that ward, so that
the evaluator may already have identified positive/negative
aspects;
provide day hospitalisation services, for which thy ensure the necessary investigations through their own laboratory, which is part of the same Romanian legal entity).

211
- ED/CPU/emergency room (both for the dialogue with an
interlocutor and for direct observation) should be evaluated in
the second part of the day, preferably;
- It is preferable that those sectors of activity whose evaluation
against the checklist requires longer time should be evaluated
in the second part of the day, so that fewer interlocutors have
to stay extra hours (administrative, HRSOW, financial-
accounting, archives, statistics/DRG, SPLIAM
- Dialogues with heads of departments should take place during
the first part of the day, starting with the heads of the medical
departments, then the heads of surgical departments);
Day hospitalisation is assimilated to a continuing hospitalisation ward for the
purposes of the Checklists.
Direct observation checklists and interview checklists by department and type
of activity shall be applied by the same evaluator. Direct observation
checklists shall be used prior to interview checklists.
Data collection instruments shall be allocated to the evaluators so as they all have
equal workloads.
The timetable shall mention all meetings necessary to fill in the checklists, including
the direct observation activities, the patient satisfaction questionnaire developed by
ANMCS, the interview with patients to map their journey.
The timetable shall consider (if needed) a 5-15 minute break, necessary to arrive from
one location to another.
The timetable includes:
- at the beginning of the first day of the visit (60 min);
The kick-off meeting
- at the beginning of each day of the visit, except for the kick-off meeting takes place (30 min)
Daily information meetings
Final information meeting
- evening meetings of the committee members
Evening meetings
Timetable
- at the end of the evaluation visit (60 min)

212
The checklists shall be filled in as follows:
Once, the following lists:
Checklist no. 1. Authorisations and quality certifications; it is recommended
that it should be filled in by the evaluator from “other specialties” category;
Checklist no. 2. Hospital strategic plan and management plan; filled in by the
evaluator from “other specialties” category;
Checklist no. 3. Organisation and Functioning Regulation / Internal Regulation
(OFR/IR); filled in by the physician evaluator;
Checklist no. 4. Hospital internet page; it is recommended that it should be
filled in by the evaluator from “nurse” category.
The following checklists:
Checklists no. 5-8, 11, 14-18, 21-24, 68 shall be filed in by the evaluator from “other
specialties” category;
Checklists no. 9, 12-13, 25-29, 32, 35-46 shall be filed in by the evaluator from
“physician” category;
Checklists no. 10, 19-20, 30-31, 33-34, 49 shall be filed in by the evaluator from
“nurse” category;
Checklists no. 27-28, 47-48, 50-63 should shall be filed in by the evaluator from
“physician” or “nurse” category;
Checklist no. 5. Strategic Management (manager) shall be filled in only once
per hospital, with the hospital manager as an interlocutor, and shall be
applied by the same evaluator who applies checklist no. 2;
Checklist no. 6. External Organisational Communication shall be filled in only
once per hospital, with the communication department coordinator as an
interlocutor or, in case there is no such coordinator, with the manager
2. Specific rules
Pre-visit
Visit

213
Checklist no. 7. Management of Ed ucation and Re search activities shall be
filled in only once for clinical hospitals or clinical institutes, with the research-
development manager as an interlocutor;
Checklist no. 8. Organisational Management (management board duties) shall
be filled in only once, with the entire management board as interlocutor;
Checklist no. 9. Medical Management at ho spital level (medical manager
duties) shall be filled in only once, with the medical manager as interlocutor;
Checklist no. 10. Healthcare management at hospital level (healthcare
manager /hospital head nurse duties) shall be filled in only once, with the
healthcare manager /hospital head nurse as interlocutor, and if the hospital
does not have a healthcare manager /hospital head nurse, the checklist shall
apply with the medical manager.
N.B. If the kitchen and/or laundry services are outsourced, the questions on the
kitchen/laundry services shall apply to the provisions of the contact between the
hospital and service provider, with the same interlocutor as mentioned above.
Checklist no. 11. Quality Management (QMS duties) shall be filled in only
once, with the QMC as interlocutor;
Checklist no. 12. Medical Decision-Making Support (medical board duties)
shall be filled in only once, with the medical manager as main interlocutor,
and the members of the medical board as guests;
Checklist no. 13. Management of Healthcare-associated Infections
(SPLIAAM/CPLIAAM duties) shall be filled in only once, with the
SPLIAAM/CPLIAAM coordinator;
Checklist no. 14. Financial-Accounting Management shall be filled in only
once, with the financial-accounting manager;
2.15. Checklist no. 15. Procurement Management shall be filled in only once,
with the head of the procurement unit;
Checklist no. 16. Administrative Management (hospital administration) shall
be filled in only once, with the head of the administrative unit;

214
Checklist no. 17. Direct Observation – yard/access ways shall be applied only
once per location, prior to checklist 16, by he same evaluator who applies
checklist 16;
Checklist no. 18. Direct Observation – within the hospital /common areas shall
be applied in each facility (building);
Checklist no. 19. Direct Observation – kitchen, shall be applied only to those
locations where there is a kitchen and by the same evaluator who applies
checklist no.10;
Checklist no. 20. Direct Observation – laundry, shall be applied only to those
locations where there is a laundry and by the same evaluator who applies
checklist no.10;
Checklist no. 21. Human Resources Management shall be filled in only once,
with the human resources manager; if this service is outsources it shall be
applied with the manager or contract coordinator (person who performs
service acceptance);
Checklist no. 22. Legal support, shall be filled in only once, with the head of
the legal department; if this service is outsources it shall be applied with the
manager or contract coordinator (person who performs service acceptance);
Checklist no. 23. Information Management (statistics and IT support) shall be
filled in only once, with the IT coordinator and with the head of the statistics
unit;
Checklist no. 24. Archive Management shall be filled in only once, in those
locations where the archive is stored; if this service is outsources it shall be
applied only once with the head of the administrative department or contract
coordinator (person who performs service acceptance);
Checklist no. 25. Medical-Surgical Emergency Management in ED/CPU shall be
applied in every location with ED/CPU with the head physician / ED/CPU
coordinator;
Checklist no. 26. Direct Observation – ED/CPU shall be applied in every
location with ED/CPU by the same evaluator who fills in Checklist no. 25, prior
to Checklist no. 25;

215
Che cklist no. 27. Medical-Surgical Emergency Management in the Emergency
Room shall be applied with the medical manager or with any person
delegated by him/her, in all locations which have Emergency Rooms and for
all existing Emergency Rooms included in the SC;
Checklist no. 28. Direct Observation – Emergency Room shall be applied in all
locations and for all Emergency Rooms, by the same evaluator who applies
Checklist no. 27, prior to Checklist no. 27;
Checklist no. 29. Medical Management at department level has as an
interlocutor the head of department /coordinator and as guests the members
of the physicians team at department/unit level. It applies as a common part
for any type of stand-alone department/unit with continuing hospitalisation
beds (including AIC) or day hospitalisation;
Checklist no. 30. Direct Observation – care environment at department level,
applied prior to Checklist no. 31, by the same evaluator who applies Checklist
no. 31;
Checklist no. 31. Healthcare Management at department level has as
interlocutor the head nurse /coordinating nurse and as guests the members
of the healthcare team at department/unit level for the healthcare activity
undertaken in any department/unit, day hospitalisation or AIC;
Checklist no. 32. AIC Management shall apply with the head of AIC
department/AIC coordinator; it is an additional list to Checklist no. 29 in the
evaluation of the stand-alone department/unit, and they are applied by the
same evaluator. In case of AIC units from other departments, Checklist no. 32
shall apply without Checklist no. 29 to the AIC department coordinator, by
the same evaluator who evaluated the department/unit the AIC department is
a part of;
Checklist no. 33. Direct Observation – AIC healthcare environment at AIC
department/unit level, applied prior to Checklist no. 31 at AIC level, by the
same evaluator who applies Checklist no. 31 in the AIC department/unit. For
the IT/ITC units which are part of the neurology, neonatology, cardiology etc.
departments, Checklist no. 33 shall be applied for that unit by the evaluator
who fills in Checklist no. 31 in the department the IT/ITC unit is part of;

216
Checklist no. 34. Blood and Blo od Products Management has as interlocutors
the UTS coordinator and the president of the hemovigilance committee. It
shall be applied to all hospitals which have UTS in thir structure and to
hospitals without UTS, but which have surgical specialties under continuing
hospitalisation (except those with only one profile, ophthalmology), and to
hospitals with clinical hematology units, internal medicine acute patients,
pediatrics, cardiovascular, gastroenterology, pneumology, medical oncology,
radiotherapy units;
Checklist no. 35. Healthcare Management for pregnant women and new
mothers is an additional checklist for obstetrics or obstetrics-gynecology
units/departments; it accompanies Checklist no. 29, and is applied by the
same evaluator who applies Checklist no. 29 in that department. For
obstetrics or obstetrics-gynecology departments which are part of other
units/departments, it shall be applied without Checklist no. 29 to the unit
coordinator, by the same evaluator who evaluated the department/unit the
obstetrics or obstetrics-gynecology unit is a part of;
Checklist no. 36. Healthcare Management for new-borns/premature babies is
an additional checklist applied for stand-alone neonatology/premature babies
units; it accompanies Checklist no. 29, and is applied by the same evaluator
who applies Checklist no. 29 in that department. For neonatology/premature
babies units which are part of other units/departments, it shall be applied
without Checklist no. 29 to the unit coordinator, by the same evaluator who
evaluated the department/unit the neonatology/premature babies unit is a
part of;
Checklist no. 37. Pediatric Healthcare Management is an additional checklist
applied for stand-alone pediatric units; it accompanies Checklist no. 29, and is
applied by the same evaluator who applies Checklist no. 29 in that
department. For pediatric units which are part of other units/departments, it
shall be applied without Checklist no. 29 to the unit coordinator, by the same
evaluator who evaluated the department/unit the pediatric unit is a part of;
Checklist no. 38. Healthcare Management for adult psychiatric patients is an
additional checklist applied for stand-alone psychiatry units; it accompanies
Checklist no. 29, and is applied by the same evaluator who applies Checklist
no. 29 in that department. For pediatric units which are part of other
units/departments, it shall be applied without Checklist no. 29 to the unit
coordinator, by the same evaluator who evaluated the department/unit the
pediatric unit is a part of;

217
Checklist no. 39. Healthcare Management for chronic kidney disease patients
is an additional checklist applied for stand-alone nephrology units; it
accompanies Checklist no. 29, and is ap plied by the same evaluator who
applies Checklist no. 29 in that department. For nephrology units which are
part of other units/departments, it shall be applied without Checklist no. 29
to the unit coordinator, by the same evaluator who evaluated the
department/unit the nephrology unit is a part of;
Checklist no. 40. Healthcare Management for dialysed patients is applied to
dialysis services within each dialysis unit;
Checklist no. 41. Healthcare Management for oncologic patients is an
additional checklist applied for stand-alone oncology, radiotherapy, surgical
oncology units; it accompanies Checklist no. 29, and is applied by the same
evaluator who applies Checklist no. 29 in that department. For oncology,
radiotherapy, surgical oncology units which are part of other
units/departments, it shall be applied without Checklist no. 29 to the unit
coordinator, by the same evaluator who evaluated the department/unit the
oncology, radiotherapy, surgical oncology unit is a part of;
Checklist no. 42. Healthcare Management for oncologic patients undergoing
radiotherapy is an additional checklist applied for stand-alone radiotherapy
units; it accompanies Checklist no. 29, and is applied by the same evaluator
who applies Checklist no. 29 in that department. For radiotherapy units which
are part of other units/departments, it shall be applied without Checklist no.
29 to the unit coordinator, by the same evaluator who evaluated the
department/unit the radiotherapy unit is a part of.
Checklist no. 43. Healthcare Management for nuclear medicine is an
additional checklist applied for stand-alone nuclear medicine units; it
accompanies Checklist no. 29, and is applied by the same evaluator who
applies Checklist no. 29 in that department. For nuclear medicine units which
are part of other units/departments, it shall be applied without Checklist no.
29 to the unit coordinator, by the same evaluator who evaluated the
department/unit the nuclear medicine unit is a part of.
Checklist no. 44. Palliative Care Management is an additional checklist applied
for stand-alone units; it accompanies Checklist no. 29, and is applied by the
same evaluator who applies Checklist no. 29 in that department. For palliative
care units which are part of other units/departments, it shall be applied

218
without Checklist no. 29 to the unit coordinator, by the same evaluator who
evaluated the department/unit the palliative care unit is a part of;
Checklist no. 45. Cell/Tissue/Organ Harvesting Management shall be applied
to units/departments where cell/tissue/organ harvesting is performed, in
hospitals authorised to perform cell/tissue/organ harvesting, with the
coordinator of harvesting activities in that hospital and with the key donation
person (usually an AIC physician);
Checklist no. 46. Cell/Tissue/Organ Transplantation Management is an
additional checklist applied for stand-alone cell/tissue/organ transplantation
units; it accompanies Checklist no. 29, and is applied by the same evaluator
who applies Checklist no. 29 in that department. For cell/tissue/organ
transplantation units which are part of other units/departments, it shall be
applied without Checklist no. 29 to the unit coordinator, by the same
evaluator who evaluated the department/unit the cell/tissue/organ
transplantation unit is a part of;
Checklist no. 47. Department of Surgery (DS) Management / Labour and
Delivery Department (LDD) Management/ Independent Surgical Unit (ISU)
Management/ Operating Room (OR) Management / Delivery Room (DR)
Management shall be applied to the Departments of Surgery (DS)/ Labour and
Delivery Departments (LDD)/ Independent Surgical Units (ISU)/ Operating
Rooms (OR)/ Delivery Rooms (DR), with the DS/LDD/ISU/OR/DR coordinator
as interlocutor;
Checklist no. 48. Direct Observation – DS/ Delivery Room shall be applied to
all Departments of Surgery (DS)/ Labour and Delivery Departments (LDD)/
Independent Surgical Units (ISU)/ Operating Rooms (OR)/ Delivery Rooms
(DR), by the same evaluator who applied Checklist no. 47;
Checklist no. 49. Sterilisation Management shall apply to all sterilisation units
declared by the hospital, with the sterilisation unit coordinator as
interlocutor;
Checklist no. 50. Radiotherapy Facility Management shall apply to all
radiotherapy facilities declared by the hospital, with the radiotherapy facility
coordinator as interlocutor;
Checklist no. 51. Direct Observation – Radiotherapy Facility shall apply to all
radiotherapy facilities, by the same evaluator who applied Checklist no. 50;

219
Checklist no. 52. Balneo-physio-kinetotherapy and recovery facilities
management shall apply to all balneo-physio-kinetotherapy and recovery
facilities, with the treatment facility coordinator as interlocutor;
Checklist no. 53. Direct Observation – BPT Treatment Facility shall apply to all
balneo-physio-kinetotherapy and recovery facilities or BPT units by the same
evaluator who applied Checklist no. 52;
Checklist no. 54. Paraclinical Healthcare Management shall apply as a
common part or any type of stand-alone laboratory or to any paraclinical
services contract of the hospital, with the head of laboratory as interlocutor,
and for outsourced activities, the medical manager or the contract
coordinator (person who performs service acceptance);
Checklist no. 55. Clinical Laboratory Management is an additional checklist
applied for the clinical laboratory or any independent unit within the clinical
laboratory together with Checklist no. 54, by the same evaluator who applies
Checklist no. 54. Only Checklist no. 55. Clinical laboratory management shall
apply for laboratories;
Checklist no. 56. Anatomical Pathology Laboratory Management is an
additional checklist applied for the anatomical pathology laboratory or any
independent anatomical pathology unit together with Checklist no. 54, by the
same evaluator who applies Checklist no. 54. Only Checklist no. 56.
Anatomical pathology laboratory management shall apply for laboratories;
Checklist no. 57. Radiology, Imaging, Interventional Radiology and Nuclear
Medicine Laboratory Management is an additional checklist applied for the
radiology, imaging, interventional radiology and nuclear medicine laboratory
any independent unit within the radiology, imaging, interventional radiology
and nuclear medicine laboratory together with Checklist no. 54, by the same
evaluator who applies Checklist no. 54. Only Checklist no. 57 shall apply for
laboratories;
Checklist no. 58. Diagnostic and Interventional Endoscopy Laboratory
Management is an additional checklist applied for the diagnostic and
interventional endoscopy laboratory. Only Checklist no. 58 shall apply for
laboratory units, in diagnostic and interventional endoscopy laboratory units;
Checklist no. 59. Pharmacy Management shall apply to all authorised hospital
pharmacies;

220
Checklist no. 60. Drugs and Sanitary Materials Management shall apply in
pharmacies or hospitals with outsourced services, with the medical manager
as interlocutor for the latter;
Checklist no. 61. Oncologic Drugs Management is an additional checklist
applied in those locations where there is an oncology/radiotherapy/clinical
hematology unit/department, with the head pharmacist as interlocutor, if the
hospital states that cytostatics are prepared in the pharmacy; the checklist
accompanies Checklist no. 59 and is applied by the same evaluator. If the
hospital states that cytostatics are prepared in the departments, this checklist
accompanies Checklist no. 29, with the head of department as interlocutor,
and the checklist shall be applied for each department where cytostatics are
prepared, by the evaluator who performs the interview in that department;
Checklist no. 62. Outpatient Clinic Management Management shall be applied
once to the hospital for the integrated outpatient clinic, with the medical
manager as interlocutor, or for the stand-alone outpatient clinic, with the
outpatient coordinator as interlocutor; in case the hospital has both an
integrated outpatient facility and a specialist outpatient clinic, the Checklist
shall be applied to each structure, with the above mentioned interlocutors;
Checklist no. 63. Direct Observation – Outpatient Clinic shall apply in all
locations where there are outpatient facilities and shall be applied by the
same evaluator who applied Checklist no. 62;
Checklist no. 68. Interview with employees/union representative shall be filled
in only once during the visit;
The following checklists shall apply:
Checklists no. 66-67 shall be filled in by the evaluator from “other specialties”
category;
Checklists no. 65, 70 shall be filled in by the evaluator from “physician” category;
Checklists no. 64, 69 shall be filled in by the evaluator from “nurse” category;
Checklist no. 69. Evaluation of Protocols and Procedures shall be filled in only
once, by centralising the data collected during the pre-visit stage and
validated during the visit;
Post-visit

221
Checklist no. 64. – Patient Journey shall be filled in only once, by centralising
the data collected during visit. The checklist pplicatoin has two components,
the first is the patient interview, with 10-minute duration, followed by the
enactment of the journey declared by the patient, 20-minute duration. A copy
of the PC shall be requested and the evaluator shall follow up along the
patient journey whether the elements obtained during the interview are
consistent with the PC and other medical documents records;
Checklist no. 65. Emergency Drills in the hospital – shall be filled in only once,
by centralising the data collected during the drills performed in each location
of the hospital;
Checklist no. 66. Patient Interview (ANMCS form by applying the
questionnaire) shall be filled in only once, by centralising the data collected
during visit;
Checklist no. 67. Employee Interview (ANMCS form by applying the
questionnaire) shall be filled in only once, by centralising the data collected
during visit;
Checklist no. 70. PC/medical documents (printed and/or digital format) - shall
be filled in only once, by centralising the data collected during visit.
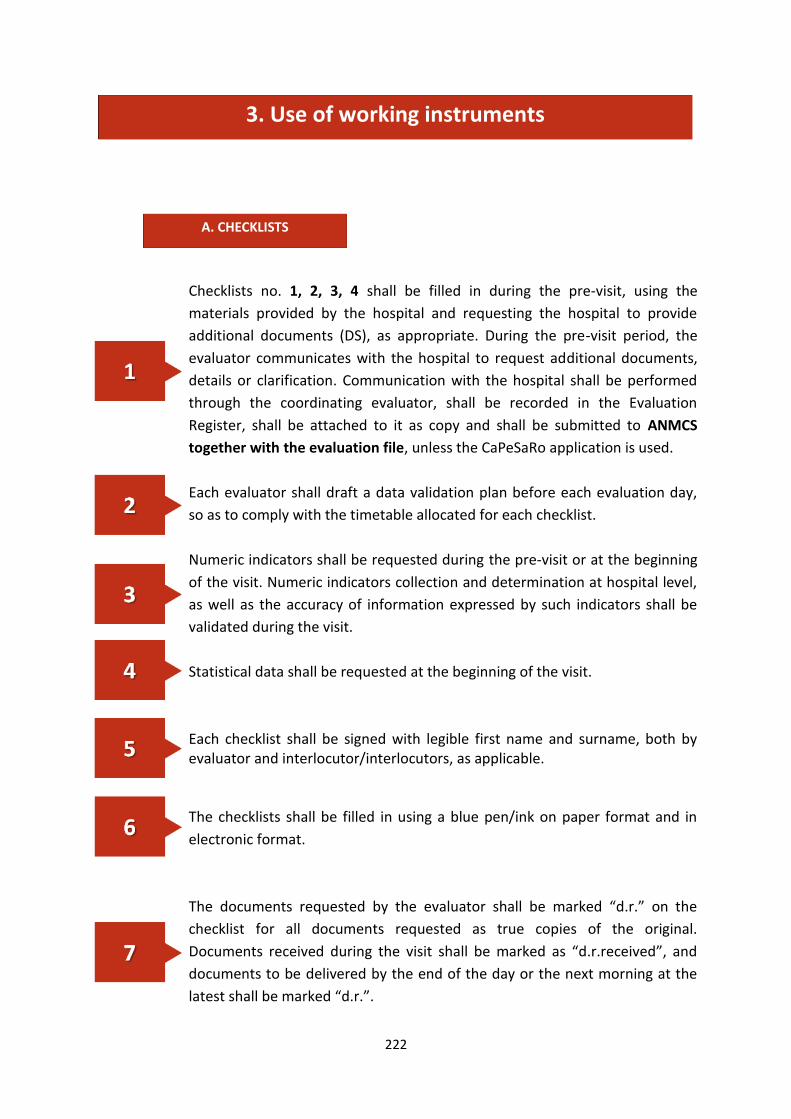
222
Checklists no. 1, 2, 3, 4 shall be filled in during the pre-visit, using the
materials provided by the hospital and requesting the hospital to provide
additional documents (DS), as appropriate. During the pre-visit period, the
evaluator communicates with the hospital to request additional documents,
details or clarification. Communication with the hospital shall be performed
through the coordinating evaluator, shall be recorded in the Evaluation
Register, shall be attached to it as copy and shall be submitted to ANMCS
together with the evaluation file, unless the CaPeSaRo application is used.
Each evaluator shall draft a data validation plan before each evaluation day,
so as to comply with the timetable allocated for each checklist.
Numeric indicators shall be requested during the pre-visit or at the beginning
of the visit. Numeric indicators collection and determination at hospital level,
as well as the accuracy of information expressed by such indicators shall be
validated during the visit.
Statistical data shall be requested at the beginning of the visit.
Each checklist shall be signed with legible first name and surname, both by evaluator and interlocutor/interlocutors, as applicable. The checklists shall be filled in using a blue pen/ink on paper format and in
electronic format.
The documents requested by the evaluator shall be marked “d.r.” on the
checklist for all documents requested as true copies of the original.
Documents received during the visit shall be marked as “d.r.received”, and
documents to be delivered by the end of the day or the next morning at the
latest shall be marked “d.r.”.
3. Use of working instruments
A. CHECKLISTS

223
Documents requested and marked “d.r.” which were not received/delivered
by the end of the visit shall be marked “n” (not received/delivered) after
“d.r.”.
After having applied the checklist, it shall be signed on each page by the
evaluator and his/her interlocutor, and a copy of the filled in checklist shall be
handed to the interlocutor. After the copy was handed in to the interlocutor,
the printed checklist CANNOT be modified.
Documents requested shall be delivered by the hospital together with a
document list, signed by the hospital representatives and registered with the
hospital registration office and with the evaluation committee register.
All copies of documents delivered by the hospital shall be marked as “true
copy of the original” and shall be hand-signed by the hospital representative
on each page.
The centralising list of documents requested shall be filled in by the evaluation
committee secretary and shall include all documents requested by evaluators.
Evaluators who apply Checklists no. 29 and 31 shall discuss with all heads of
departments/stand-alone units or day hospitalisation units, and with all
department/stand-alone unit/day hospitalisation unit head nurses.
In case the heads of department/ unit or department/unit head nurse
is/becomes unavailable for objective reasons (annual leave, sick leave etc.),
discussions may be carried out with their substitutes, only after having
checked the replacement decision issued by the manager and signed by the
substitute.
If the day hospitalisation unit includes beds undertaking healthcare activities
covered by Checklists no. 35, 37-42, 44, these checklists shall be added to
Checklist no. 29.
The Observations field of the checklists shall be filled in using handwritten
capital letters. The checklists include the requirement of the indicator. If the
hospital used a different manner to fulfil the requirement, this shall be noted
near the requirement, in the Observations field, mentioning the alternative
indicators used by the hospital, only if such indicators are “SMART”.

224
For indicators which apply to contract provisions (for example – outsourced
activities), the question shall be asked using the requirement corresponding
to the indicator.
If during the evaluation visit evaluators identify in the hospital certain
structures (departments, units, clinics, laboratories) which are not mentioned
by the SC, and the hospital requests their evaluation for accreditation
purposes, evaluators shall notify ANMCS through the coordinating evaluator,
and shall draft an Identification and Non-Compliance Form (INCF).
The checklists mention the maximum amount of time necessary to fill them
in.
It is recommended that the evaluator should not repeat the evaluation of a
department/unit (“point of no return” principle).
“Batch of 4” for verification: for every 4 indicators which may be checked by
documents, a supporting document shall be requested. In case the supporting
document cannot be presented, move to “batch of 3”, etc.
“NOT APPLICABLE” indicators are those indicators related to activities which
are not part of the specificity of the hospital under evaluation.
If you tick the NOT APPLICABLE column, present solid justification in the
OBSERVATIONS column. Otherwise, the indicator shall be considered NON-
COMPLIANT!
Indicators related to aggressive patients or palliative care patients do NOT
have the NOT APPLICABLE option in Checklist no. 29 (for palliative care
patients, there is an exception for the neonatology unit).
Checklist no. 69. Protocols and Procedures Evaluation.
During the pre-visit, each evaluator shall select 2-3 protocols/procedures
related to each sector under evaluation from the List of procedures and
protocols presented by the hospital in DOS, then they shall study them and
request DS for them. During the pre-visit they evaluate the level of
formalisation, dissemination, training of personnel and monitoring of
protocol/procedure implementation by QMS, according to the annual plan
and to the implementation improvement plan, if applicable.

225
The following aspects are evaluated during the visit:
a) Implementation of protocol/procedure at sector level;
b) Existence of the risk identified and mentioned in the risk register,
which imposed the development of the protocol/procedure;
c) Existence of evaluation of residual risk obtained compared to the one
initially estimated;
d) Definition, use and regular evaluation of indicators which measure
the results generated by the implementation of that
protocol/procedure;
e) Regular evaluation of effectiveness and efficiency of
protocol/procedure use with possible revisions or updates.
In case of non-compliance with the elements indicated, the evaluator may
extend the verification to several protocols/procedures. In case non-
compliance is identified in other protocols/procedures as well, all indicators
related to the evaluation of protocols/procedures become non-compliant.
PC shall be requested and received in compliance with patient data
confidentiality rules. In order to fill in Checklist no.70, the evaluator shall
request 3 PC for each department, with day hospitalisation assimilated to a
department, of which 2 PC from the hospital archive and 1 PC from the recent
archive of the department, and 3 aditional PC of deceased patients.
Checklists no. 64, 65, 66, 67, 70 which are filled in during the post-visit stage
shall not be included in the draft evaluation report, but shall be part of the
evaluation report.
Checklist 69 Protocols and Procedures Evaluation shall be filled in during the
visit and finalised during the post-visit stage, shall not be included in the draft
evaluation report, but shall be an integral part of the evaluation report.
All direct observation checklists shall not be included in the draft evaluation
report, but shall be an integral part of the evaluation report.
The checklists shall be centralised as follows:
The checklists which were applied several times by evaluators during the
evaluation visit for accreditation purposes shall be centralised in one “Sheet”,
which shall be renamed “centralised”. Thus, all checklists applied by the
evaluator during the evaluation visit shall be in the centralised list + L
centralised);

226
- Qualitative indicators from the repeated checklists shall be centralised as
follows:
YES + NO (only once or several times) = NO;
YES (only once or several times) + Not Applicable = YES;
NO (only once or several times) + Not Applicable = NO;
Not Applicable + Not Applicable = Not Applicable.
- Qualitative indicators from the repeated checklists shall be centralised by
mentioning in the centralising checklist, in the “observations” field related to
the indicator, all values identified in each checklist included in the centralising
checklist;
- The observations related to an indicator shall be centralised by
mentioning in the centralising checklist, in the “observations” field related to
the indicator, all observations identified in each checklist included in the
centralising checklist.
When the data collection period is not specified, the last finalised calendar year shall
be considered.
In case the question is not applicable to the specificity of the hospital, mention NA (not
applicable).
1. It is recommended that the ANMCS questionnaire for patients and the
interview for the “patient journey” should be performed in the second part of
the day, towards the end of the visit.
2. Selection of respondents from the patients shall consider their
hospitalisation duration, as follows: patients hospitalised for minimum 3 days
– maximum 7 days, for continuing hospitalisation patients shall be selected.
Day hospitalisation questionnaires shall be an exception from this rule.
Questionnaires NO shall be applied to AIC/TI/TIC and ED/CPU patients. In the
neonatology departments, the questionnaire shall be applied to the mothers
of hospitalised children. In the pediatrics department the questionnaire shall
be applied to caregivers of hospitalised children, for children younger than 14
years old or directly to the children if aged between 14 and 18 years old.
B. QUESTIONNAIRES / INTERVIEW

227
In case of psychiatric hospitals, competent patients shall be selected. The hospital
shall be requested to provide a list of competent patients, and the evaluator shall
select the patients for the interview from this list.
No questionnaires/interviews shall be applied in prison hospitals and/or high security
hospitals.
It is imperative that evaluators should not endanger patient health or safety with their
interventions, and should not interfere in any way with healthcare services provision or
hospitalisation conditions.
Equally, the evaluators have the obligation to clearly specify to patients that they do
not have role or purpose to change anything in their healthcare provision process or to
interfere in any way in their relationship with the hospital personnel or management, at any
level; similarly, for the hospital employees, the evaluator shall clearly specify that he/she
does not have and cannot have any role in regulating a situation or changing the position of
that employee; also, the evaluator shall not make any intervention in case of pre-existing
conflict situations or conflict situations occurred during the visit, is such situation is not
related to his/her presence or activity; the evaluator may not be called for conciliation or
amicable solutions regardless the context and the parties – between patients, between
patients and hospital employees, or between hospital employees.
Patient Questionnaire
Minimum 6 - maximum 30 patients, but no more than 2 per department shall be
selected to apply the patient questionnaire, at hospital level.
One evaluator shall distribute and collect all questionnaires and fill in Checklist no.
66 after the visit.
Patient Interview
One patient for each location (facility) shall be selected for the patient interview.
The patient journey analysis starts with the place/department or unit where the
patient is located, with an interview with the patient (pre-structured interview); then, the
analysis shall continue with each department/unit with which the patient had contact, from
his/her arrival to the hospital (emergency unit/inpatient registration) until the interview.

228
In all “patient journey” stages, the evaluator shall discuss (direct interviews or
interactive sessions) with the persons that patient was in contact, or, if such persons are not
available, with another person who delivers the same type of services. Besides this
approach, the evaluator shall perform brief direct observations on the spot in these
departments. This type of analysis enables an objective image on the patient’s perception of
the quality of care and services provided, by comparison to the results of the direct
observation performed by the evaluator.
One evaluator shall collect all interviews and fill in Checklist no. 64, after the visit.
Employee Questionnaire
The Employee Questionnaire, an A.N.M.C.S. form, shall be applied using the interview
technique with the employee. The questionnaire shall be administered to minim 10
employees, maximum 5% of the total number of employees, and shall cover all
departments, and all categories of employees (e.g.: a physician may be selected from one
department, and a nurse from another department etc).
Only one questionnaire shall be applied as interview with the employees’
representative, by the same evaluator who fills in Checklist no. 68.
All other questionnaires are self-administered by employees.
One evaluator shall collect all questionnaires and fill in Checklist no. 67, either
during the visit, or in the period immediately after the visit.
The Identification and Non-Compliance Form (INCF) shall be filled in by
evaluators for those situations which might occur during the visit and lead to
the identification of certain aspects which disturb / may disturb the
evaluation process. Such situations may be related to the hospital (e.g.:
structures which were not included in the SC, were not reported prior to the
visit and the hospital requests they should be included in the evaluation) or to
the evaluators (e.g.: repeated failure to fulfil the daily tasks allocated to
them). Non-compliance shall be considered those aspects belonging to
(generated by) the internal environment of the hospital or of the team of
evaluators which influence the fairness/impartiality/sustainability of the
evaluation process.
C. SPECIAL FORMS

229
The Special Situations Form (SSF) shall be filled in by evaluators for those
situations when special aspects might occur whose immediate solution is not
under the remit of the hospital or of the evaluators team (e.g.: extreme
temperatures imposing the cease of operations, extended damage to water,
electricity, heating supply systems, serious illness of one or several evaluators,
work-related accidents, quarantine etc.). Special situations are those aspects
belonging to (generated by) the external environment of the hospital or of the
team of evaluators which impose the suspension of the evaluation process. In
certain situations, serious disfunctionalities of the internal environment of the
hospital, which are incompatible with the implementation of quality
management in the hospital, may turn into special situations which suspend
the visit.
Development of the draft evaluation report and of the evaluation report
Report preparation starts during the evaluation visit, through regular
meetings of evaluators, focused on exchange of information, planning and
coordination of actions so as to reach the visit objectives within the time
allocated for the visit. Each evaluator shall analyse and organise the data
collected so that they may be further integrated in the final report and reflect
the level of compliance with various standards within the organisation.
Draft report/report format: size A4, Word, font Times New Roman 12, align
text “justify”, line spacing at 1.15, print on both sides
All members of the evaluation team shall participate in the development of
the Draft Evaluation Report and shall be responsible for the accuracy and
reliability of information collected and processed by analysis.
The draft evaluation report shall be delivered in two copies, one for ANMCS
and one for the hospital. The letter to the hospital notifying the submission of
the draft report shall specifically mention the deadline for submitting
objections.
Objections formulated by the hospital shall be submitted by the president of
the evaluation committee to the objection analysis committee, together with
the viewpoint of the evaluation committee.

230
The conclusions of the analysis committee shall be signed by all its members
and shall be submitted to the evaluation committee in paper and electronic
format, signed and registered, to develop the evaluation report. The
conclusions of the analysis committee are binding for the evaluation
committee and shall be included in the evaluation report.
The evaluation report is a collective document, developed and assumed by all
members of the evaluation committee.
The evaluation report shall be delivered in two copies, one for ANMCS and
one for the hospital and shall be signed on each page by all members of the
evaluation committee.
All correspondence between evaluators and hospital shall be registered with the
evaluation register and attached to the evaluation file.
All correspondence between evaluators and hospital, and ANMCS, respectively, shall
be sent through the coordinating evaluator/ president of the evaluation committee.
The coordinating evaluator/ president of the evaluation committee shall coordinate
the activity of the evaluation committee, and shall set the daily timetable of the visit
for each member of the evaluation committee, so that the members of the evaluation
committee share an equal workload.
The hourly timetable set initially, during the pre-visit stage, shall be submitted to the
hospital with an accompanying letter.
The draft evaluation report and the Evaluation Report do not establish the
accreditation level; the specialist unit of ANMCS shall process and interpret the indicators
and information collected by the evaluation committee for accreditation purposes.

231
Training and profile of evaluators
Evaluators follow an intense training programme. The first level refers to the initial
training, through the Training programme for evaluators, carried out by A.N.M.C.S., in
partnership with the National School of Public Health, Management and Professional
Development in Bucharest (SNSPMPDSB), the sole body which can provide initial and
continuous training, as part of a protocol signed with A.N.M.C.S. which agreed both on the
training curriculum as well as the trainers.
The training curriculum and the training programme handbook for the healthcare
services or hospital evaluators were developed together with A.N.M.C.S. and with its
approval.
Following this initial programme, in order to add additional information, a
Specialization programme for evaluators is organized, also in partnership with SNSPMPDSB,
a programme intended to cover the continuous training level for evaluators.
Beside these 2 special training programmes, which include both theory and practice, at
A.N.M.C.S. level, evaluators are included in specialized trainings where they analyse up-to-
date information from the evaluation practice. These trainings also take the form of plenary
sessions, with the support of directors of different departments, support divisions and of the
A.N.M.C.S. president. Another level of training takes place within the evaluation board,
being carried out by the president of the board, which details, explains and presents the
work instruments, the forms used as well as the particularities of the hospital which is to be
evaluated.
The essential abilities of an evaluator are: the ability to conduct an interview, apply a
questionnaire, analytical and critical observation thinking, ability to synthesize.

232
Evaluator qualities:

233
Evaluation visit requirements
What A.N.M.C.S. does in relation to the hospital.
before the start date of the accreditation procedure for the hospital, makes
available the Accreditation standards for hospitals
after the hospital registration in the accreditation procedure, that is 9 months
prior to the date when the scheduling procedure of the evaluation visit starts,
gives access to the CAPESARO application
after the submission of the hospital request to enter the accreditation
procedure, 9 months prior to the date when the scheduling procedure of the

234
evaluation visit starts, makes available the accreditation manual and the self-
assessment guide, which included the self-assessment form
once the hospital fills in and uploads in the CAPESARO application the self-
assessment form and the document presenting the identification data and the
functional description of the unit, within the 9 calendar month period from
the request of the hospital of entering the accreditation procedure, calculates
and informs the hospital management on the amount of the accreditation fee
after the payment, by the hospital, of the accreditation fee, A.N.N.C.S. sets
the date of the evaluation visit. 2 month prior to this date, the preliminary
activities for the preparation of the evaluation visit start. In the pre-visit stage,
specific instruments are applied by the external evaluators of A.N.M.C.S.
during the maximum 1 week period of the evaluation visit, but also in the 3
weeks following the visit (post-visit), monitors and supervises the activity of
the evaluation board
sends the Accreditation report to the hospital, with the following
accreditation levels: accredited; accredited with recommendations;
conditional accreditation; accredited with a compliance plan; not accredited.
For the compliance plan, gives the hospital the possibility to prove the
implementation of at least the requested measures, in a 6 month period from
the receipt of the plan. At the end of the 6 month period, it starts the
compliance visit
receives and answers possible appeals
ensures the monitoring of hospitals on a 4 year period from the end of the
evaluation process (pre-visit, actual visit and post-visit)
in special situations, starts the monitoring visit following which it can decide
to maintain the accreditation or set a compliance plan

235
A.N.M.C.S. sends to hospitals:
The legal description of the evaluation and accreditation process is made by the Order
of the President of ANMCS no. 446/2017, as follows:
ART. 5
(1) The evaluation stage, coordinated by the evaluation committee, shall include the
pre-visit, the actual visit and the post-visit.
(2) The pre-visit shall include the following main activities:
(a) Communication with the hospital and development of a report on DOS and
DS compliance which shall be submitted to A.N.M.C.S.;
(b) Based on the report mentioned at letter a), A.N.M.C.S. may decide to
cancel the evaluation visit;
c) Development of the evaluation visit plan and it communication to the
hospital;
(3) The actual visit to the hospital includes the following main activities:
a) The kick-off meeting, with the participation of hospital representatives, in
order to establish in detail how the hospital visit will take place;
b) The information meeting at the beginning of each day, with the
participation of hospital representatives;
c) Reaching the specific objectives allocated to each evaluator within the
evaluation committee, by using the data collection techniques and
instruments and by appraising the processes within the hospital;
d) Final information meeting, with the participation of hospital
representatives, in order to present the preliminary conclusions of the
evaluation visit;
236
e) The draft evaluation report shall be commenced during the evaluation visit,
and each evaluation has the obligation to include in the draft report their
own interim conclusions and to archive the documents developed or
received during the evaluation stage, which shall be submitted to
A.N.M.C.S. together with the evaluation report;
f) Filling in the special situations form, for those situations which hinder the
evaluation process, whereby the evaluation committee requests
A.N.M.C.S. to suspend the evaluation visit. The A.N.M.C.S. president may
decide to suspend the evaluation visit. In this case, the entire activity of
the hospital shall be considered non-compliant. The accreditation process
may be re-commenced, upon request of the hospital, with the approval of
the A.N.M.C.S. Management Board, according to the provisions of Art. 4
of this procedure;
g) Filling in the special situations form, in case of identifying deficiencies which
endanger patient or hospital personnel safety, by which the evaluation
committee notifies such findings to A.N.M.C.S. The A.N.M.C.S. president
may decide to suspend the evaluation visit. In this case, the accreditation
process may be re-commenced, with the approval of the A.N.M.C.S.
Management Board, according to the provisions of Art. 4 of this
procedure.
(4) The post-visit shall include the following main activities:
a) Development of the draft evaluation report by the members of the
evaluation committee and its submission to the evaluated hospital, within
maximum 5 working days after the actual visit to the hospital has been
finalised;
b) Within maximum 5 working days after having received the draft evaluation
report, the hospital shall formulate in writing objections on certain
aspects included in the report, as applicable;
c) Analysis by A.N.M.C.S. staff, within maximum 5 working days after receipt,
of the objections formulated by the hospital and submission of conclusions
to the evaluation committee members;
d) Development of the evaluation report by the evaluation committee
members, within maximum 5 working days after having received the
conclusions, and its communication to the hospital. The hospital may
formulate no other objections against the evaluation report.

237
ART. 6
The accreditation stage shall include the following main activities:
a) Development of the accreditation report by the Hospital Evaluation and
Accreditation Unit, based on the documents used during the evaluation
process;
b) Issuance of the Order of A.N.M.C.S. President on the accreditation or non-
accreditation of the hospital, as applicable, and its communication to the
hospital.
ART. 7
The accreditation certificate shall be issued to those hospitals which obtained
accreditation, within maximum 90 working days after the Order of A.N.M.C.S.
President on the accreditation has been communicated to the hospital.
ART. 8
(1) The internal evaluation (self-assessment) by the hospital consists in the
analysis of services provided, of the performance and monitoring
indicators and in the communication of its conclusions to A.N.M.C.S., as
well as submission of other specific information requested by A.N.M.C.S.
throughout the evaluation process.
(2) The external evaluation consists in the stages provided by Art. 3 of this
procedure.
ART. 9
(1) The data collection techniques used in the evaluation and accreditation process
are:
a) Analysis of documents provided by the hospital;
b) Direct observation – on the spot observation to note compliance with
predefined requirements or how activities are carried out, without
interference by evaluators;
c) Focus groups – a quality research technique, by which the members of a
group made of hospital representatives and the evaluation committee
members express their viewpoints on the topics under discussion, within a
limited period of time;

238
d) Interview – aims at data collection by direct discussion, during the actual
visit;
e) Simulation of processes to identify clinical risks.
(2) Validation of data collected consists in their verification by the evaluation
committee, by examination, recalculation, comparison and agreement to
confirm the reality of the data collected.
ART. 10
The main instruments used for hospital accreditation are:
a) Hospital identification form – a template document developed by the
specialist structures of A.N.M.C.S., requesting the hospital to provide
information on the identification data and on its organisational and
operational structure;
b) List of mandatory documents requested - a template document developed
by the specialist structures of A.N.M.C.S., requesting the hospital to
submit the documents whose existence and compliance are a prerequisite
for the initiation of the evaluation stage;
c) List of additional documents necessary for the evaluation and accreditation
process - a template document developed by the specialist structures of
A.N.M.C.S., requesting the hospital to submit the documents whose
existence is necessary for the initiation of the evaluation stage;
d) Self-assessment form – a template document developed by the specialist
structures of A.N.M.C.S., requesting the hospital to submit information on
meeting the requirements of the accreditation standards in successive
stages of the evaluation and accreditation process;
e) Compliance Plan for evaluation purposes – a document submitted by
A.N.M.C.S. to the hospital under accreditation procedure, communicating
the hospital any non-compliance which prevents the initiation of the
evaluation procedure.
f) The evaluation visit timetable – a document including the hours and the
objectives to be evaluated;
g) Meetings minutes – a documents including the important aspects discussed
by evaluators and representatives of the hospital under evaluation;
h) Checklist – a template document developed by the specialist structures of
A.N.M.C.S., used for data collection purposes;
i) List of documents requested during the actual evaluation – a template
document developed by the specialist structures of A.N.M.C.S., including
the additional documents requested by evaluators form the hospital
representatives during the evaluation process;

239
j) Questionnaire – an instrument developed by the specialist structures of
A.N.M.C.S., applied at individual level only after having obtained the
consent and after having guaranteed confidentiality and anonymity;
k) Identification and non-compliance form – a template document developed
by the specialist structures of A.N.M.C.S. and filled in by evaluators, who
note, during the evaluation visit, facts disturbing the visit;
l) Special situations form – an unilateral document drafted by the evaluation
committee to indicate facts which hinder the evaluation visit or endanger
patient or hospital personnel safety, submitted to the A.N.M.C.S.
president, which may lead to the suspension of the evaluation visit;
m) Draft evaluation report – a written communication submitted by the
evaluation committee to the hospital, on the results of the evaluation visit
for accreditation purposes, submitted to the hospital to formulate possible
objections;
n) Evaluation Report – a written communication submitted by the evaluation
committee to the hospital, on the results of the evaluation visit for
accreditation purposes, submitted to the hospital after having analysed
and solved any possible objections;
o) Accreditation Report – a document developed by the specialist structures of
A.N.M.C.S. underpinning the issuance of the accreditation or non-
accreditation order of the A.N.M.C.S. president, as applicable.
ART. 11
(1) A.N.M.C.S. shall publish on its webpage the references, standards, criteria,
requirements and verification instruments.
(2) All documents used in the evaluation and accreditation process, deadlines and
document submission methods, as well as conditions for postponing, cancelling
or suspending the evaluation visit shall be established by order of the A.N.M.C.S.
president.

240
9. ACCREDITATION CATEGORIES, EVALUATION SCALES
(FOR INDICATORS)
Following the analysis performed, based on the requirements of the second revised
edition of hospital accreditation standards, on the experience of the first accreditation cycle,
in order to highlight the overall fulfilment of accreditation standards, we propose the
following classification by accreditation categories:
I. Category I – Accredited
II. Category II – Accredited with recommendations
III. Category III – Accredited with caution
IV. Category IV – Accredited with limited confidence
V. Category V – Decision to extend the accreditation process
VI. Category VI – Not accredited
In order to fall under any accreditation category, hospital must meet the following
mandatory minimum general conditions:
a. More than 51% compliance with each standard;
b. 100% compliance with the following critical indicators on patient safety:
b1. The hospital holds all mandatory authorisations or permits provided
by law
b2. No deficiencies related to infrastructure and circuits which expose
patients and employees or visitors to major risks (e.g.. failure to
observe rules on explosives or hazardous waste handling and storage,
on prevention of falling, electrocution etc.);
b3. Access control in areas with risk of contamination (surgery
department, delivery department, Intensive Care units/departments,
neonatology, etc.).
Position in an accreditation category is determined by the cumulative fulfilment of the
following 3 criteria, with category level given by the lowest value/level:
1. Total score obtained – indication of the number of points scored, as percentage of
the total number of points that hospital could have obtained.
The total score on the level of compliance with accreditation standards is calculated
against the following criteria:
- Indicators representing legal requirements/obligations, which must be
complied with according to law and therefore do not reflect a special concern
of the hospital for quality and safety – compliance is scored with 0 points,
non-compliance (-10) points

241
- Indicators on regular determinations/reporting necessary to maintain
authorisations, care measured as follows:
- Regular determinations/reporting performed within the deadlines
imposed, with results within accepted limits: 0 points
- Regular determinations/reporting performed within the deadlines
imposed, with results beyond accepted limits, for which corrective
actions were taken: (-) 5 points
- Failure to perform regular determinations/reporting necessary to
maintain authorisations within their deadlines: (-) 10 points
- Quality appraisal indicators which, according to WHO requirements and with
ISQua principles reflect hospital’s concern with patient, employee and data
safety and security, activity planning, environmental protection, which are
measured on a scale from 0 to +10, based on:
Relevance for service quality and patient safety, reflecting the risk level
associated with non-compliance with that indicator
Difficulty to comply with – complexity of necessary resources and
activities
Level of compliance
2. Number of indicators scored (-10) obtained, as percentage of the total number of
indicators scored (-10) applicable to that hospital. Indicators scored (-10) are those
indicators which represent legal obligations or indicators whose non-compliance reflects
severe deficiencies at hospital level which endanger/may endanger patient, employee, data
and environmental safety.
3. Existence or non-existence of a compliance plan with the sanitary certificate (SC)
assumed by the hospital management and approved by the supervisory body or by
shareholders, in case of private hospitals, and period of time assumed for its
implementation.

242
Category I – Accredited
Criteria:
- Total score exceeds 90%
- No indicators scored (-10)
- SC without compliance plan
Hospitals falling under this category are accredited without recommendations and
encouraged, by promotion by ANMCS, to maintain and improve their efforts. They may be
rewarded by the public health insurance system in the service contract. They may be
appointed by the Minister of Health to provide quality management methodological
guidance for other hospitals in their administrative-territorial area.
Category II – Accredited with recommendations:
Criteria:
- Total score between70 – 89.99%;
- Less than 10% of the indicators which might be scored (-10) applicable to
that hospital receive this score;
- SC compliance plan is assumed by the hospital and approved by the
supervisory body or by shareholders to be implemented within 12 months from
the receipt of the accreditation report.
In case of failure to implement the plan within the period assumed, the hospital main
remain in this category for the rest of the 5-year term or may request ANMCS a re-
evaluation to reach category I. In case of failure to observe the assumed interval, the
hospital may apply for a 12-months extension; in this case, the hospital is placed in the next
category.

243
Category III – Accredited with caution:
This category includes hospitals from category II which applied for an extension of the
compliance plan implementation period or hospitals which, according to the evaluation,
meet the following classification criteria:
- Score between 51-69.99%;
- Between 10% and 30% of the indicators which might be scored (-10) applicable
to that hospital receive this score;
- SC compliance plan is assumed by the hospital and approved by the supervisory
body or by shareholders to be implemented within 24 months from the receipt
of the accreditation report.
In case of failure to implement the plan within the period assumed, the hospital main
remain in the category given by the other criteria for the rest of the 5-year term or may
request ANMCS a re-evaluation to reach superior categories I. In case of failure to observe
the assumed interval, the hospital placed in category IV.
Category IV – Accredited with limited confidence:
This category includes hospitals which fulfil any of the first two criteria of categories I,
II or III, but which did not assume the implementation of the compliance plan or assumed its
implementation within a time interval exceeding 24 months from the receipt of the
accreditation report or which exceeded the 24-month period initially assumed.
When reporting full resolution of non-compliances include in the SC compliance plan,
these hospital may request ANMCS to be placed in the accreditation category indicated by
the other criteria.

244
Category V – Decision to extend the accreditation process:
This category includes, for a period of maximum 6 months after the receipt of the
accreditation report, the hospitals which fulfil the following criteria:
- Total score exceeds 51%;
- 2 standards at the most scored less than 51% and/or between 30% and 50% of
the indicators which might be scored (-10), applicable to that hospital, received
this score.
- Failure to assume or comply with a deadline for the implementation of the SC
compliance plan.
During this period, the hospital is considered under accreditation procedure and must
meet the criteria to be placed under on of the categories I, II, III, or IV, otherwise, after those
6 months, the hospital is declared not accredited.
Category VI – Not accredited
This category includes:
- Hospitals which obtained a total score below 51% after the evaluation process
or
- Hospitals which had more than two standards fulfilled below 50%
or
- Hospitals which had more than 50% of the indicators which might be scored (-
10), applicable to those hospitals, with this score,
or
- Hospitals under category V which did not meet the criteria to be placed under
one of the accreditation categories within 6 months after the receipt of the
accreditation report.
The hospitals in this category may register for a new accreditation procedure in the
following accreditation cycle, pursuant to the legal provisions in force when applying for
registration or within the same accreditation cycle, on decision issued by the minister of
health.

245
10. MONITORING
Methodology for monitoring accredited hospitals
ART. 1 Definitions
1. Monitoring – verification of the accredited hospital compliance with the
requirements of the accreditation standards and with the other legal provisions
applicable throughout the accreditation validity period. Monitoring is performed
in successive stages, planned and communicated to the hospital, so that the
process does not hinder its activity and the hospital has sufficient time to adopt
and implement the necessary actions to improve healthcare services quality and
patient safety, as well as any legal amendments approved.
2. Monitoring indicator - instrument used to verify compliance with the
requirements of the standards against which the hospital was evaluated and
then accredited. For this purpose, in the monitoring activity, the National
Authority for Quality Management in Health (hereinafter called A.N.M.C.S.) may
use both indicators from the evaluation process, and new indicators, developed
based on the experience acquired and on the legal amendments occurred.
3. Adverse event – event considered preventable, which represents an
unintentional and undesired harm, injury, illness, temporary or permanent
disability or even death of the patient, associated to healthcare provision.
4. Sentinel/catastrophic event - adverse event involving serious harm to patient’s
health with long-term consequences, permanent disability or patient death
which reflects serious deficiencies in the healthcare provider’s policies and
procedures, lack of interest for safety and an organisation at risk in service
provision. Such an event signals the need for immediate investigation and
adoption of adequate corrective actions.
5. Near miss event - Incident or potential incident, which was avoided and did not
cause harm, although it could have caused harm.
6. Monitoring visit – hospital visit, carried out by a monitoring team consisting in
A.N.M.C.S personnel.
ART. 2 Organisation of monitoring activities
1. For monitoring purposes, the Unit for Healthcare Services Standards within
A.N.M.C.S. develops the specific documentation and working instruments
consisting in the set of indicators for annual monitoring accompanied by the
validation grid, and the set of indicators for biannual monitoring.

246
2. A zonal monitoring coordinator (hereinafter called ZMC) will be appointed in the
monitoring process, and will be responsible with the communication with the
hospital. Each ZMC is allocated a number of hospitals within his/her area of
responsibility. They will maintain permanent communication with the quality
management coordinator (hereinafter called QMC) within the hospital allocated.
3. Communication between A.N.M.C.S. and the QMC of the hospital under the
monitoring process will be carried out, among other means, by using the e-mail
address: [email protected] and the CaPeSaRo application. For this
purpose, all hospitals have the obligation to create an account and access this
application. The hospital QMC is directly responsible for the accuracy and
truthfulness of the information submitted, and is liable to penalties as provided
by law for the offence of misrepresentation.
ART. 3 Monitoring implementation
Monitoring shall be carried out as follows:
a) Annual monitoring;
b) Biannual monitoring;
c) Ongoing monitoring of adverse events occurred;
d) Ongoing monitoring of the approved structure of the hospital.
ART. 4 Annual monitoring
1. Annual monitoring is performed by analysing the set of indicators provided for
annual monitoring, reported by the hospital using the methods and within the
deadlines communicated by A.N.M.C.S. This analysis is performed by ZMC.
2. Following the analysis, ZMC develops the Interim Monitoring Report.
3. The Interim Monitoring Report is the document issued by ZMC based on the
analysis, according to the validation grid related to each set of monitoring
indicators, and to the indicators and documents made available by the hospital.
The Interim Monitoring Report, endorsed according to internal procedures, shall
be approved by the A.N.M.C.S. president nd submitted to the hospital.
4. In case the findings identify complete failure to fulfil the indicators requested,
the Interim Monitoring Report becomes the Final Monitoring Report.
5. In case of finding non-compliances in the indicators reported, a Monitoring
Requirements Compliance Plan shall be drafted.

247
6. The Monitoring Requirements Compliance Plan is part of the Interim Monitoring
Report, and presents the hospital the non-compliances found and the deadline
of maximum 3 months from communication within which the hospital must
remedy any such non-compliances and communicate ZMC the actions taken.
Failure to comply with the deadline or implementation of the plan below 75%
shall lead to the initiation of a monitoring visit.
ART. 5 Monitoring visit
1. An announced visit is carried out in the following situations:
a) The hospital repeatedly refused either to submit the documentation
required or to comply with the deadlines established by this methodology,
or does not use the requested template for the necessary documents in
this process, either by altering their predefined content or by sending
incomplete documents;
b) The hospital does not comply with the deadlines established by the
Monitoring Requirements Compliance Plan;
c) The hospital implements the Monitoring Requirements Compliance Plan
below 75%;
d) The hospital does not report the adverse events associated to healthcare
provision within the deadlines and using the methods provided by this
methodology.
2. An unannounced visit may be carried out at any time during the accreditation
validity period, upon decision of the A.N.M.C.S president.
3. The monitoring team is appointed by order of the A.N.M.C.S president, and
consists in at least 2 A.N.M.C.S. employees who have the following main tasks:
a) On-the-spot check of compliance with all indicators established for that
monitoring stage;
b) Development of a monitoring visit report, within 5 working days after the
completion of the visit. The monitoring visit report is the document
developed by the monitoring team which indicates both any non-
compliance identified and the motivations of the team, the observations of
the hospital and any other finding. In case of unannounced visits, the
monitoring visit report will replace or confirm, as appropriate, the Interim
Monitoring Report. If the unannounced visit identifies non-compliances
with monitoring indicators or irregularities with compliance with
accreditation standards, the monitoring visit report shall be submitted,

248
according to internal procedures, to inform the Monitoring Requirements
Compliance Plan;
c) Submission of the monitoring visit report, according to internal procedures,
either to inform or confirm the Final Monitoring Report, in case of
announced visits, or of unannounced visit where no non-compliances with
monitoring indicators or irregularities with compliance with accreditation
standards are found, or to inform, confirm or amend the Monitoring
Requirements Compliance Plan.
ART. 6 Final Monitoring Report
(1) The Final Monitoring Report is the document developed by A.N.M.C.S. based on
an analysis of al information and documents resulted or obtained pursuant to
Art. 4 and 5, which indicates all unremedied non-compliances and is submitted
to the hospital and hospital governance (supervisory body according to Law no.
95/2006 on healthcare reform, as republished and further amended and
supplemented).
(2) In case of implementation below 75% of the monitoring validation grid provided
by Art. 2 (1), besides unremedied non-compliances, the Final Monitoring Report
shall also include a proposal to initiate the re-evaluation of that hospital.
ART. 7 Biannual monitoring
1. Biannual monitoring consists in reporting, according tothe deadlines
communicated by A.N.M.C.S., on the set of biannual monitoring indicators,
whose dynamic analysis may determine the evolution of the hospital in the
process of improving the quality of healthcare services provided and patient
safety. Based on the indicators reported, A.N.M.C.S. shall establish, by categories
of hospitals, the national average of the value of each indicator.
2. Failure to submit such information within the deadlines and using the methods
provided by this methodology may trigger the initiation of a monitoring visit.
3. Customised results of this analysis, including at least the indicator, the value of
the indicator, the national average and the deviation from the average shall be
published on the A.N.M.C.S. website and be used as a benchmark to hospital
performance evaluation.

249
ART. 8 Monitoring of adverse/sentinel/near-miss
events
1. Monitoring of adverse/sentinel/near-miss events involves reporting by the
hospital and collection by A.N.M.C.S. of adverse events related to healthcare
provision, without pointing fingers, in order to learn from.
2. Hospitals must report such events within maximum 24 hours from their
occurrence and them within maximum 30 from such reporting, must submit a
report analysing the causes leading to the occurrence of that event and the
actions identified to prevent recurrence.
3. Failure to submit such information within the deadlines and using the methods
provided by this methodology may trigger the initiation of a monitoring visit.
4. Data submitted by all hospitals are anonymised and centralised by A.N.M.C.S. at
the end of each month and published during the first decade of the following
month on the A.N.M.C.S. website under the section "For Professionals", for
consultation purposes. Access of professionals to this section may be made only
by using individual access codes.
ART. 9 Monitoring structural changes by setting
up or removal of standalone departments/units
1. Any such changes shall be reported within maximum 30 days from the operating
authorisation of the new structure.
2. A set of indicators and monitoring documents specific to the new structure
resulted shall be developed and communicated to the hospital within maximum
30 days. The hospital has the obligation to report within maximum 6 months on
the compliance with indicators, then a monitoring visit is initiated. The results of
this monitoring visit shall be communicated to the interested authorities.
ART. 10 Measures adopted following monitoring
The measures adopted following monitoring may be:
a) Confirmation of hospital compliance until the next monitoring, if the Final
Monitoring Report indicates the implementation of at least 75% of the
monitoring validation grid;
b) Initiation of hospital re-evaluation process, only in the case of the first two
monitoring stages, if the Final Monitoring Report indicates the implementation
below 75% of the monitoring validation grid.

250
11. GLOSSARY
Accreditation
The action of recognition or acknowledgement by an external evaluation body of the level of compliance with accreditation standards, resulted after an external and independent technical evaluation, establishing the performance level of an organisation (healthcare organisation) against those standards. See also ISQua accreditation.
ISQua accreditation
Public recognition by ISQua of the manner in which a body with the role of external evaluator which develops standards in a healthcare system meets the ISQua international standards or principles, after this body underwent an independent external evaluation of its organisational performance, of the standards they developed and/or of the training/education programmes on standards.
Threat External factor which may exploit the vulnerability of an organisation by actions or facts which cause imbalance or instability and generate life threatening situations, endanger the bodily integrity or freedom of persons or values;
Risk analysis for physical security
Activity undertaken to identify threats and vulnerabilities which may endanger people’s life, bodily integrity or freedom or may prejudice the values owned by the organisation, in order to determine the impact and to evaluate security risks, underpinning the necessary actions to limit or eliminate them;
Healthcare All medical acts undertaken for diagnosis, therapeutic or rehabilitation and recovery purposes
Audit Systematic and independent examination and review of activities to determine whether they match the objectives set and the accepted rules to reach them.
Good practices Approach which may deliver the best outcomes, selected by a systematic analysis process which proved it to be a good example or a success. It is further adapted to cater for a given organisation.
Risk management framework
A set of components which provide the basis and the organisation rules for the design, implementation, monitoring, review and continuing improvement of risk management within the organisation. The framework should be integrated in the overall strategic and operational policies and practices of the organisation.
Qualified Holding the required certificates, trained and legally and professionally licensed to perform specific activities.
Quality Level of excellence, extent to which an organisation meets the needs and the expectations of its customers (patients)
Research
Production of new knowledge, recognised as such, as a result of systematic, sometimes random search, using field-specific methods an techniques, in order to advance knowledge, with or without intention to achieve long-term economic or social benefits, with or without intention to transfer them to enforcement sectors (fundamental, applied, experimental)
Certification Formal recognition of compliance against approved standards, validated by external evaluation.
Information circuit
Path taken by information or a category of information between issuer and recipient
Customers Natural or legal persons to whom the organisation provides services, goods or works.
Code of conduct Documented set of principles and recommendations, agreed to shape and maintain certain behaviours, which provide all parties involved information on the responsibilities and expectations generated by that code.
Hospital competence
Capacity to provide assistance and healthcare evaluated by: formal professional competence (certification of training in the field) and practical competence (medical team experience) and technical and physical resources necessary to provide assistance and healthcare in place
Competence Individual knowledge and skills, adequate to provide certain services and guarantee that those knowledge and skills are assessed regularly.
Complexity Number of medical specialties in a hospital

251
Community Individuals, families, groups and organisations which interact, cooperate to undertake joint activities and participate in solving common concerns which, in general, occur within a common geographic area or environment.
Confidentiality Guarantee of limitations of the right to use or distribute information received from individuals or organisations.
Consent Assent or approval given by a customer (patient), his/her caregivers, guardians or guardianship supervisory authority.
Dose constraint
Dose constraint is a restriction imposed to the doses a person may receive from a given source and a useful tool for optimisation of radiation protection. Dose constraint relies on a prospective evaluation of doses, using well managed practices or the rationale of a professional, and is not a dose limit. A threshold dose level or dose output, maintained at the lowest reasonable level, to allow delivery of diagnostic information required, considering social and economic factors, it is a protection improvement tool.
Interdisciplinary consultation
It relies on transfer of concepts and methodologies from two or more fields (domains, specialties), to the treating physician, in order to solve certain problems which cannot be properly researched by one field/speciality. Interdisciplinarity involves clarification of new working practices and assumptions for each specialty involved, and integrated interaction for the unitary diagnosis and treatment of a certain condition.
Continuity of care
Extent to which patient healthcare is coordinated between practitioners and organisations in time
Contract Formal agreement stipulating the terms and conditions for services received or provided from or to another organisation. The contract and contracted services are monitored and coordinated.
Criterion A specific step which must be taken or an activity which must be carried out to meet a requirement or a standard.
Culture A shared system of values, beliefs and behaviours.
Data Unorganised facts or aspects which may generate information.
DDD
Defined Daily Dose = (according to WHO) the assumed average maintenance dose per day for a drug used for its main indication in adults. DDD is a statistical measure of active substance consumption defined by the World Health Organisation (WHO). It is used to standardise comparison of active substance consumption between various drugs or various healthcare environments.
Dependency
Individual’s incapacity to adopt certain behaviours or to undertake alone, without the help of another person, actions which allow him/her to achieve an acceptable level of satisfaction of basic needs. (Nursing Guide with evaluation and care techniques for basic needs - coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Executive Director
A person holding a management position in an organisation, appointed by the management body of the organisation. Other titles, such as manager, director or general manager may be used.
Scope Field of activity (medical, social, economic, scientific, cultural etc.) in which various types of services provided by the organisation are delivered under certain conditions and limitations.
Human Resources record
All information about an employee of the institution (staff member). It includes human resources management data such as: holidays, recommendations, performance reviews, qualifications, employment registration and conditions.
Rights Something that can be claimed by a person, as a rightfully, fair, legal or moral entitlement. A formal description of the services customers may expect and claim from an organisation.
Multidisciplinary team
A multidisciplinary team includes professionals from various medical specialties, who bring together their own working methodologies to build a diagnosis or treatment procedure which adds up the activity of all team members to reach a common outcome. Under multidisciplinary relations, cooperation between scientific fields may be “mutual and cumulative, but not interactive”. Multidisciplinarity is a non-integrative combination of scientific specialties where each specialty maintains its working methodologies and assumptions without adopting changes
252
or developments from other specialties, within multidisciplinary relations.
Pluridisciplinary team
A team of professionals from various professions (physician, psychologist, social worker, spiritual guide) who cooperate by systemic transgressive interference focused on the patient and on the quality of the patient’s overall condition. Pluridisciplinarity relies on the use of independent methods and theories from various disciplines and their application to shape, structure and understand various phenomena and processes which transcend healthcare, but start from it. Pluridisciplinarity occurs when a general assumption applies creatively to other scientific fields and generates a new set of systems, laws, relations and structures.
Education Systematic learning and training of necessary activities to develop, acquire or change knowledge, attitudes, values and skills.
Effectiveness Extent to which services, interventions or actions are provided according to existing good practices to reach objectives and accomplish best results. A dimension of quality.
Ethics/ Ethical Set of recognised principles guiding professional and moral conduct.
Evaluation Appraisal of success in reaching expected objectives and outcomes regarding the organisation, services, programmes or customers.
External evaluation of the organisation
Highly objective appraisal performed by a recognised body of professionals who are not employed by the organisation and who evaluate as objectively as possible the performance of a user against the quality standards applicable.
Quality assessment
Planned and systematic collection and analysis of data related to a service, usually focused on the specifications related to its content and operation and to customer-oriented outcomes.
Evaluator External professional with expertise in the field who may appraise the organisation performance against agreed standards.
Adverse event
Any medical incident which may occur during healthcare activities, or outside such activities (unfavourable and unintended response)/event considered, which represents an unintentional and undesired harm, injury, illness, temporary or permanent disability or even death of the patient, associated to healthcare provision
Undesirable event
Any event endangering patient’s life or safety
Sentinel event
Adverse event involving serious harm to patient’s health with long-term consequences, permanent disability or patient death which reflects serious deficiencies in the healthcare provider’s policies and procedures, lack of interest for safety and an organisation at risk in service provision. Such an event signals the need for immediate investigation and adoption of adequate corrective actions
"Near miss" event
Incident or potential incident, which was avoided and did not cause harm, although it could have caused harm.
Function examination
Medical investigation of the health condition by evaluation, using specialised devices, of the functioning parameters of various organs/organ systems in the human body: – respiratory function (spirometry), cardiovascular system (EKG- electrocardiogram), kidney function (probes?), gastric secretion, liver function, bile ducts, pancreas (intubation or fibroscopy-endoscopy: oesophagus, gastroscopy, colonoscopy), visual analyser (visual acuity), acoustic-vestibular analyser (audiometry), nervous system (EEG - electroencephalogram). It requires the use of specialist equipment, and it is performed upon request of a specialist physician.
Data mining A process used to analyse large sets of data and extract relevant information using mathematical and statistical methods.
Reliability Extent to which results are validated by repeated measurements made by different persons or at different times by the same person, when what is being measured did not change in the interval between measurements.
Information flow Quantity of information passed between issuer and beneficiary along the information circuit, characterised by certain properties - length, speed, reliability, cost, etc
Provider of healthcare services
Legal organisation, entity or group of entities, with or without legal personality, which provide healthcare services, primary assistance, community assistance, services for acute patients, specialist healthcare services etc.

253
Risk management
A systematic process of identification, evaluation and actions to prevent or manage within the organisation health or safety risks at clinical, administrative, property or occupational levels.
Guideline Thematic document including guiding principles and actions on a certain topic.
Practice Guide
A document on a certain theme which presents tools describing processes based on clinical trials or endorsed by experts as most efficient in the evaluation and/or treatment of a patient with a certain symptom, condition or diagnosis, or which describes a specific procedure.
Level of dependency
Level of dependency or severity of dependency of a care beneficiary - the level of autonomy compared to a person who, without the help of another person, may undertake alone the necessary actions to satisfy his/her basic needs. This may be determined after the evaluation of the independence / dependency function of each basic need. (Nursing Guide with evaluation and care techniques for basic needs - coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Population groups with clinical-biologic particularities: children, elderly, pregnant women, people with disabilities etc.
Groups of people who live in the same geographic area and have various properties / common/similar specificities in terms of their health condition and of clinical or biological criteria.
Governance Function which determines the direction, the objectives and the development policy of an organisation in order to accomplish its mission and which allows monitoring of achievements and policy implementation.
Diagnostic nuclear imaging
(performed in Nuclear Medicine laboratories, uses the physical properties of certain radioactive isotopes): myocardial, brain, lung scintigraphy, bone scintigraphy, kidney scintigraphy, Spect-CT, positron emission tomography (PET), hybrid PET- CT versions (PET scanner – computed tomography) or PET-RM (PET scanner – magnetic resonance)
Security incident Event occurring with an uncontrolled evolution, which generates unwanted consequences on persons and/or assets and/or activities within an organisation and which requires immediate action to reinstate the previous situation;
Incidents Unusual, unexpected events which may involve an element of risk or may have a negative impact on customers, groups, staff or organisation.
Independence
Reaching an acceptable level in basic needs satisfaction (including physiological and psychological needs) by actions undertaken by the individual himself/herself, without the help of another person. (Nursing Guide with evaluation and care techniques for basic needs - coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Indicator
Performance measurement tool used to monitor, evaluate and improve the quality of services. Indicators are related to structure, process and outcomes. They are calculated according to a compliance ratio, for example they have a numerator and a denominator so that they and be compared and used as benchmarks.
Data integrity The meaning of data is not different from the meaning registered in the source document; data are not accidentally or intentionally.
Interoperability Capacity of different entities / systems / software applications to exchange data through a common set of procedures so that they answer specifically to certain problems or fields of activity.
Preventive maintenance
A planned, scheduled, cyclic process of functional evaluation of equipment, performed before using new equipment and regularly throughout the equipment life cycle. The purpose is to maintain equipment performance according to manufacturer specifications. It includes a verification of safety of equipment use.
Healthcare All specific care activities to cater for the basic needs of each patient, complementary to nursing
254
Records Documents certifying results obtained or providing evidence of activities performed, which are the result of key processes, for example human resources records, customer records, customer reports.
Procedure justification
Analysis of specific benefits of patient care, against risks (e.g.: exposure to ionising radiation); it is performed individually, considering economic, social factors, costs etc. and existence of other specific procedures (e.g.: no exposure to radiation); if the procedure cannot be justified, it shall not be performed.
Clinical laboratory
A medical specialty department within a hospital, which, based on biological samples collected from the human (generally blood samples) performs biochemical investigations to place the results within specific parameters of diagnostic relevance. E.g. haematology, biochemistry, bacteriology, immunology, cytology; pathology laboratory
Radiology and Medical Imaging Laboratory
Medical specialty department performing investigations: - X-ray investigations: radiography, fluoroscopy, tomodensitometry or computed tomography with or without contrast, mammography, DEXA bone densitometry; - ultrasound: abdominal-pelvic ultrasound, fetal morphology, cardiovascular ultrasound, thyroid ultrasound, musculoskeletal ultrasound, mammary glands and genitals, eye ultrasound, transesophageal ultrasound, transfontanellar ultrasound; - Nuclear Magnetic Resonance (NMR)
Networking Connections, contacts, collaborators/partners and collaboration/work relationships with others.
Management
Science and technique of organisation and management, all organisation, leadership and management activities of any type of organised activity or economic unit for manufacturing, services or trade (including medical services). Stages: setting targets or goals, by planning and budgeting, definition of processes to reach these objectives and allocation of resources to implement these plans. Take actions to implement the plans by organising, employment of personnel, control and problem-solving.
Information management
Information management and control system including data which are organised, interpreted and usable. The information may be written, audio, video or pictures.
Security action Basic component of a security solution, corresponding to one or several threats and vulnerabilities identified by the risk analysis, whose purpose is to reduce related risks;
Feedback mechanism
How an organisation checks the effect caused by its actions or services by direct liaison with their beneficiaries
Security mechanisms
Solutions which include several security actions, operating according to predefined scenarios, to secure one or several facilities, when they are located within the same perimeter;
High-risk drugs
Drugs which are dangerous for the human body (may lead to death, miscarriage, permanent or temporary, local or general health damage etc., due to failure to non-compliance with the dose prescribed or due to substances which may cause allergies or toxic reactions when associated with other substances present in food)
Mentoring Guidance and continuing training programme for evaluators and external users where training is provided by unmediated assistance (face-to-face and distance learning) of a mentor
Mission General written statement of an organisation’s position and goals. The mission differentiates organisations.
Dangerous substances
Also called harmful agents – any chemical, physical or biological factor present in the work environment (occupational environment) which may endanger employee health.
Nursing International term used by the World Health Organisation for the specific function of licensed nurse, which helps sick or healthy individuals perform those activities which contribute to maintaining or recovering their health.
Objective A goal which should be achieved if the organisation is to reach its purposes. It is the translation of goals at a specific, concrete level, where results may be measured.
Objectives of care
Description of behaviour expected as a response of patient’s health to a treatment, a result we want to achieve following interventions. (Nursing Guide with evaluation and care techniques for basic needs - coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)

255
Procedure optimisation
Amendment of procedural parameters so that they respond best to the purpose of the procedure, with least side effects and/or related risks. In radiodiagnosis, obtaining a good quality image with minimal exposure to ionising radiation; in radiotherapy, accurate release of desired dose in the target volume, with minimal exposure of peritumoral healthy tissues and/or radiosensitive organs.
Management body
Natural persons, groups or agencies with authority and responsibility for setting the strategic guidelines and the organisation operation. Also known as Board, Committee, Commissioners Committee.
External evaluation body
Acknowledged body in the field which provides an independent evaluation of an organisation’s performance, against specific quality standards for the functions of that organisation.
Accredited Dosimetry Body
A body responsible with benchmarking and verification of individual dosimetry surveillance instruments and reading or interpreting their indications, or for radioactivity measurements in the human body or in biological samples, or for dose evaluation and determination, accredited by the National Commission for Nuclear Activities Control.
Organisation It comprises all structures/locations under the management of the organisation management body/owner, to who it reports.
Induction A process by which employees become familiar with all work-related aspects and their responsibilities.
High Performance
Exceeding own results, obtaining top results by using state-of-the-art technologies and mastering best practices in the field, development of practices with results exceeding those obtained to date by top professionals
Personnel Employees of an organisation
PLAN A detailed document which identifies the needs, the list of strategies to cover those needs and sets targets and objectives. The document may include descriptions, policies and procedures, practice guides, protocols or a combination thereof (JCI 5th edition)
Operational Plan
Organisation’s management document explaining how to transpose into practice the organisation’s strategy. It is a result f strategic planning and it includes the necessary processes, actions and resources to achieve the objectives set by the strategy.
Strategic Plan A formal plan formal setting the overall goals and aiming at positioning and adjusting the organisation according to its environment.
Patient Care Plan
A written document summing up the stages of the nursing process which informs each member of the healthcare team on the patient and the interventions performed. Regardless the nursing theory used for the patient care plan, it should include: the nursing diagnosis, the objectives of care, nurse interventions and evaluation of interventions. The nursing process is turned into action by using the patient care plan.
Complaint Oral or written description of a problem, aspect or dissatisfaction with the services received.
Policies Documented statements formalising the task and concept approach according to the objectives of the organisation.
Radiodiagnosis practice
Getting a medical diagnosis based on a radiologic examination. Radiologic examination uses radiology and medical imaging methods as well as diagnostic nuclear imaging.
Radiologic procedure
Medical diagnostic or treatment procedure using ionising X, gamma, electron, neutron radiation etc.
Procedures Sets of written instructions which communicated approved and recommended steps for a specific action or set of actions so that results are predictable and responsibilities are clear and assumed.
IT procedures All elements establishing the means of collection, registration, submission, processing and archiving of a category of information, mentioning operations to be performed, their sequence, support, formulas, models and treatment of information used.
Process Series of interdependent activities and communications leading to delivery of services.
Care process
An organised and planned process, a rational method to plan and promote individualised interventions in order to obtain a good health condition for the individual, family and community. It is a scientific method of solving the individual’s current and potential problems, based on the physiologic, psychological, socio-cultural and spiritual needs of the

256
individual. It focuses on the particular responses of each individual (or group of individuals), to a real or potential health change. (Nursing Guide with evaluation and care techniques for basic needs - coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Programme Official organised system or plan, which guides actions toward a specific goal. (JCI 5th edition)
Physical protection
All measures aimed at preventing, identifying and responding to theft, sabotage, unauthorised access, unauthorised activities related to nuclear and radiologic equipment, nuclear materials and other sources of ionising radiation; (similar information/Law 182/art. 15, i): all classified information security and protection activities, by physical check measures and devices and technical means)
CARE PROTOCOL
A plan which identifies all patient’s care needs, lists the strategies used o cover these needs, identifies treatment targets and objectives. The care plan specifies the criteria against which certain interventions should be finalised and documents how the patient reaches the targets during his/her care programme. The care plan relies on data collected during patient evaluation. The care plan template may differ from one organisation to another. The plan is guided by specific practice guides, by protocols and combined guides and protocol, and by specific policies and procedures.
Interventional Radiology
Performance of medical procedures (invasive and minimum invasive, intraoperative) using imaging technologies for guidance. Practitioners may be radiologists or clinicians of various specialties (cardiology, urology, orthopedics, vascular surgery, general surgery, neurosurgery, thoracic surgery, pediatric surgery). Equipment used in interventional radiology: angiography equipment, C-arm fluoroscopy equipment, extracorporeal lithotriptor, dedicated imaging equipment for intraoperative ultrasound explorations. Hybrid imaging systems (PET-CT or PET - MR) may only be used by physicians with both specialties, Radiology/ Medical Imaging licensed for CT or MRI and Nuclear Medicine
Duty Duty and obligation to undertake tasks or activities. This duty cannot be delegated and it should be transparent for all parties involved.
Responsiveness Being able to offer respect to others, customer-orientation, encourage the customer to participate and obtain customer agreement. A dimension of quality.
Recruitment and Selection
Processes used to attract, select and appoint personnel and evaluators.
Public recognition
Independent external public recognition/acknowledgement.
Results Consequences of an action, operation, service or intervention.
Risk Likelihood or possibility that danger, loss or prejudice should occur. This may be related to staff and public health and welfare, to property, reputation, organisation’s operation environment, financial stability, market share and other valuables.
Risk related to medical care in the hospital
Likelihood of prejudice generated while the patient is within hospital premises with other causes than those related to nursing or healthcare
Clinical risk Likelihood of prejudice generated by a medical diagnostic or therapeutic intervention or due to inaccurate appraisal of patient condition and needs
Infectious risk
Likelihood of prejudice as a consequence of major epidemiologic factors (microorganism, microorganism, environmental factors) and of secondary factors (climate, social factors) leading to possible biologic contamination. Treating physicians identify infectious risk patients and take action to limit the risk.
Scalability Scalability of a data processing system consists in its capacity of similar behaviour, without faults, when the volume of data processed increases and/or when it is capable to provide better results with additional resources (usually, hardware)
Goals General statements describing the results an organisation wants and providing the necessary guidelines for daily activities and decisions. Goals support the organisation’s mission.
Dependency score
Score obtained after an evaluation of basic deficit needs to determine the patient’s dependency level.
Nuclear security All technical and organisational measures to ensure smooth operation of nuclear

257
equipment, to prevent and limit its damage and ensure protection of personnel subject to professional exposure, of population, environment and assets against exposure to ionising radiation or radioactive contamination exceeding the limits allowed by the legislation in force;
Services
Action serving or benefiting someone; work delivered for or to somebody’s interest. The American Marketing Association defines services as: activity offered for sale, which provides advantages and satisfaction without entailing a physical exchange in the form of goods.
Safety Trust that potential risks are avoided and unintentional results are avoided or minimised.
Nuclear safety
All physical protection and nuclear guarantee control measures. A set of technical and organisational measures to: - Ensure safe operation of nuclear equipment; - Prevent and limit their damage; - Ensure personnel, public and environmental protection against radiation of radioactive contamination
Nurse call Central system whereby any patient may ask medical personnel assistance when he/she needs help
Medical staff alert in case of major emergencies
Alert system used by medical staff to alert emergency intervention team (UPU sau ATI)
Document control system
A planned system to check how important documents, especially policies and procedures, are issued, amended and used within the organisation. The system needs each document to have a unique identification, to include the date of issuance, updates and authorisation. Issuance of documents within the organisation is controlled and all copies of each document are accessible and can be tracked. Use of outdated documents is prevented.
Security system Integrated set of organisational, technical and procedural actions aiming at securing physical security for an organisation or facility;
Information systems
Electronic and manual data and information planning, organisation, analysis and control systems.
IT system It may defined as the set of data, information, information flows and circuits, information processing procedures and means designed to contribute to setting and achieving the objectives of the organisation.
Stakeholder Individuals, organisations or groups which have an interest or participate in a service. Shareholders or members of the management board of an organisation.
Standard Desired and achievable level of performance used to measure current performance.
Strategy Long-term management document designed to set objectives and plan the course of action to be implemented.
GOVERNANCE STRUCTURE
It may vary from one hospital to another. Usually this category includes: hospital owners (in case of private hospitals), a group of persons supervising how the hospital is managed, responsible for high quality healthcare service provision (JCI)
Nursing research surveys
For the purposes of this document, nursing research surveys are research undertaken in the hospital where in which nurses were involved in cooperation with University research departments; for development of Bachelor, Master’s or PhD thesis; for development of specialist books, articles or papers presented in scientific events.
Sustainability
Quality of anthropic activity to unfold without exhausting available resources, therefore without compromising possibilities to satisfy future needs. At macroeconomic level, it entails a balance between growth and available resources (including identification of alternative resources). From the standards perspective, it is the extent to which a healthcare system provides infrastructure, workforce, facilities and equipment, innovation and responsiveness to emerging needs, e.g. research, monitoring. It is a dimension of quality.
Dashboard An instrument including overall information on the activities to be undertaken
Medical technology
(WHO definition) “devices, medicines, medical and surgical procedures – and related knowledge – used in the prevention, diagnosis, treatment of infections, rehabilitation and organisational support systems providing healthcare”

258
Validity Relation between data obtained and the purpose for which they were requested or extent to which they reflect what they intend to measure.
Values Principles, beliefs or philosophies guiding behaviour which may involve social/ ethical issues.
Performance review
Continuous process whereby a manager and another staff member review staff performance, set performance objectives and evaluate progress made to achieve them.
Vision Describes what the organisation wants to be.
Vulnerability Characteristic acquired, with or without intention, by a person, facility, values etc., which may be used or may deliberately or unconsciously lead to prejudice against that entity.



![i rffi lUl3] U I lUJ to) 0 D:»[u] a n](https://static.fdocuments.in/doc/165x107/61fde34375588463287310dd/i-rffi-lul3-u-i-luj-to-0-du-a-n.jpg)




![Polling District: Queniborough - Charnwood...par-tea leense leenee bgcp oxi0U COAGL$ Eaa agLapÅ roqaG ' g LUJ (con) ablLJL]GÀ 2b!UusÀ 69 E LUJ eau] e.Yÿ 00 6!qaGnngh BLO pense](https://static.fdocuments.in/doc/165x107/5e77aa5cdad058766400e94d/polling-district-queniborough-charnwood-par-tea-leense-leenee-bgcp-oxi0u.jpg)








