
Accountable Innovation - Healthcare Leadership Council · Accountable Innovation ... (CMMI), a...
21
Accountable Innovation Reforms to Strengthen and Sustain the Center for Medicare and Medicaid Innovation Funding for this research was provided by the Healthcare Leadership Council.
Transcript of Accountable Innovation - Healthcare Leadership Council · Accountable Innovation ... (CMMI), a...
Accountable InnovationReforms to Strengthen and Sustain the Center for Medicare and Medicaid Innovation
Funding for this research was provided
by the Healthcare Leadership Council.

2
Executive Summary
Accountable Innovation: Reforms to Strengthen and Sustain the Center for Medicare and Medicaid Innovation
Actors across the public and private sectors are looking to value-based payment and delivery models to improve quality and cost-efficiency in healthcare. The Center for Medicare and Medicaid Innovation (CMMI), a federal entity created by Section 3021 of the Patient Protection and Affordable Care Act (ACA), is at the center of these efforts.
CMMI was established to test new models that have the potential to improve quality without increasing costs, or reduce costs without harming quality of care for patients. If model tests are successful, and meet certain criteria, the Secretary of Health and Human Services may expand them. The Center, which provides a promising platform for healthcare innovation, was given considerable latitude to accomplish these tasks. However, recent experience suggests that reforms may be needed to improve predictability, promote collaboration with the private sector, and protect patients.
CMMI currently operates 44 model tests that include grants to states for payment and delivery reform activities, initiatives to speed adoption of best practices, and payment demonstrations that directly modify Medicare reimbursement. As the ACA did not precisely define procedures and standards CMMI is expected to meet, gaps between stakeholder understanding of the agency’s mission and actual practices have emerged. This paper highlights several key issues that should be addressed in order to strengthen and sustain CMMI:
Key Issue 1: Proposals for Large-Scale, Mandatory Models
Recent CMMI proposals, including the Comprehensive Care for Joint Replacement Model (CJR), Part B Drug Payment Model, and Cardiac Bundled Payment Model have prompted concerns from the patient and provider communities because they exceed the common understanding of what constitutes a “model test.” Unlike earlier CMMI model tests, which have been small and voluntary, more recent proposals mandate the participation of providers in large cross sections of the country.
These large scale, mandatory program designs pose unique challenges, including enhanced risks to beneficiaries, overlap with other CMMI demonstrations, and compliance challenges for providers—as noted by MedPAC and others.
The scope of recent CMMI models exceeds the common understanding of a “model test.”
CJR Cardiac Bundles Part B Drug Proposal
17%MSAs
83%MSAs
33%MSAs
75%PCSAs
25%PCSAs
67%MSAs
Mandatory participation in model Non-participation
Model denominator information is as follows: CJR (OMB-provided number of total MSA areas, including Puerto Rico - 389); CR (denominator of 294 total possible MSAs, after exclusion criteria noted in regulation)MSA: metropolitan statistical area; PCSA: primary care service area

3
Key Issue 2: Tension Between Testing, Expansion, and Permanent Changes in Healthcare Policy
CMMI utilizes a two-phase process for demonstrations. In Phase I (testing), CMMI can test new models to see if they improve quality or decrease costs. In Phase II (expansion), CMMI can expand Phase I models that meet certain criteria with respect to their impact on quality, cost, and access.
Section 3021 does not clearly define the parameters of a Phase I model test with respect to scope and duration, and this lack of clarity is reflected in practice. Phase I model tests that have been re-launched, like the Comprehensive Primary Care Initiative, or transitioned from voluntary to mandatory, like CMMI’s bundled payment programs, raise questions about the meaningfulness of the distinction between Phase I and Phase II and the criteria that must be satisfied for model expansion.
Similarly, CMMI’s Phase II expansion authority and competing interpretations of that authority underscore a tension between CMMI’s role as hub for testing new policies and Congress’ role in setting the laws and policies that govern Medicare, Medicaid and CHIP. CBO’s scoring assumptions with respect to CMMI, which attribute potential savings of $34 billion over 10 years to CMMI’s broad reach and flexible process, reinforce this tension.
Key Issue 3: Inconsistent Stakeholder Engagement and Limited Insight Into Model Results
Section 3021 requires CMMI to collect input from interested parties through open door forums or other mechanisms. CMMI has engaged stakeholders at various points through meetings, Requests for Information, and technical expert panels, but the level of interaction between CMMI and stakeholders has been inconsistent across models. Some models, like the Oncology Care Model, were developed over a period of years with multiple opportunities for public comment. Others, like the CJR model, were rapidly deployed with limited opportunities for input.
Stakeholders also have limited insight into the progress of CMMI model tests over time. Private sector stakeholders have expressed frustration that information on the early experience with CMMI models is not more readily available to facilitate and improve upon parallel efforts in the private sector.
Key Issue 4: Gaps in Monitoring and Evaluation
Section 3021 requires CMMI to conduct an evaluation of each model test, to include an analysis of the quality of care furnished under the model and the impact of the model on program spending. However, establishing appropriate methods to monitor for quality and access issues has proved challenging for some models, and robust, evidenced-based quality measures may not exist for some clinical areas in which CMMI is interested in testing models. This poses challenges for assessing model results, but also places patients at risk. Without a robust monitoring strategy, unintended effects that negatively impact quality of care in CMMI models could go undetected.
There is consensus throughout the healthcare system that it is valuable to effectively and appropriately test new healthcare delivery and payment systems that can improve the cost and quality of care. However, patients, providers, and Members of Congress of both parties are now raising concerns that large-scale demonstration projects, developed without stakeholder input and lacking protections for patients, could inadvertently impact patient access to care. And, given the extremely wide latitude Section 3021 confers to CMMI, there is also concern among stakeholders that models could significantly restructure portions of the Medicare or Medicaid programs without input and appropriate oversight from Congress, endangering patient access. This uncertainly is already leading to political opposition, which threatens progress toward innovative and sustainable value-based payment models.
It is in the best interests of patients, members of the healthcare sector, and CMMI itself for safeguards to be put in place that ensure demonstration projects are focused and reasonably limited in scope so that they do not become untested changes to large portions of our healthcare system. There must be collaboration with providers, the patient community, and the private sector in their selection, construction and implementation. Applying these safeguards will ensure that CMMI’s work best serves current patients and the future of Medicare, Medicaid, and CHIP.

4
IntroductionThe United States (US) healthcare system faces continued growth in healthcare costs. In response, actors across the system are looking towards value-based payment models as one potential solution. These models seek to reform payment and delivery systems to reward quality and cost efficiency. Commercial insurers, physicians, and hospitals are exploring new payment arrangements, such as pay-for-performance contracts and accountable care organizations (ACOs). Primary care and specialty physicians are becoming patient-centered medical homes. Similarly, pharmaceutical companies are entering into outcomes-based contracting arrangements that tie payment for medicines directly to achieving results for patients (see sidebar).
In January 2015, the U.S. Secretary of Health and Human Services announced that the agency would build upon and seek to further catalyze these efforts by committing to move 50 percent of Medicare payments to “alternative payment models” (APMs) that hold providers accountable for the cost and quality of care by 2018. This initiative was undertaken in an effort to address what some consider to be misaligned incentives in the Medicare Fee For Service system that lead to inefficiency and poor quality. The Center for Medicare and Medicaid Innovation (CMMI), a new government agency created by Section 3021 of the Patient Protection and Affordable Care Act (ACA), is at the center of these efforts.
CMMI was established to test new payment and delivery models with the potential to improve quality without increasing costs, or reduce costs without harming quality of care for patients in an effort to address delivery system reform, which had received little previous attention. There is no consensus roadmap for how to transform the healthcare system. Therefore, a certain amount of testing, experimentation, and hypothesizing is necessary to determine which healthcare models offer the best solutions for managing costs while ensuring patients get the care they need. The architects of CMMI recognized such experimentation would be needed and designed the Center to have significant flexibility to test new models in Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). This flexibility has yielded several promising initiatives; since its inception, CMMI has launched over 40 demonstration programs aimed at achieving
Private-Sector Value Initiatives
• Blue Cross Blue Shield of Massachusetts developed its Alternative Quality Contract in 2008, giving provider groups an annual budget for meeting all the healthcare needs of their patients while hitting quality targets. A recent study showed this approach improved the quality of care while cutting costs as much as 10% below their historical FFS’ levels.*
• Oncologist John Sprandio, MD pioneered the Oncology Patient-Centered Medical Home (OPCMH), a model of care that enhances value for patients, oncology providers and payers by reengineering the proccesses of care delivery to empower the care team and optimize physician-patient interactions. The OPCMH model is associated with a significant decline in emergency room visits and hospitalizations for cancer patients.†
• Cigna entered into value-based contracts with Amgen and Sanofi/Regeneron for their PCSK9 inhibitors in 2016. The contracts modify the cost of the cholesterol-lowering drugs REPATHA® (evolocumab) and PRALUENT® (alirocumab) based on how well patients respond to the medications, aligning incentives by linking financial terms to improved customer health.‡
• Southwest General and Anthem Blue Cross and Blue Shield in Ohio announced in 2016 they agreed on a bundled-payment structure for Anthem members in Northeast Ohio. Anthem will reimburse a hospital a set amount to cover the entire spectrum of a patient's care for total hip and total knee replacement procedures, from diagnosis to recovery.**
* “Study: Payment Model Lowers Medical Spending, Improves Care,” Harvard Medical School. July 11, 2012. https://hms.harvard.edu/news/study-payment-model-lowers-medical-spending-improves-care-7-11-12. Accessed October 26, 2016.† http://www.communityoncology.org/UserFiles/pdfs/co-js-medical-home.pdf .‡ “Cigna’s Two New Value-Based Contracts With Pharma for PCSK9 Inhibitor Cholesterol Drugs Tie Financial Terms to Improved Customer Health.” Cigna. May 11, 2015. http://www.cigna.com/newsroom/news-releases/2016/cignas-two-new-value-based-contracts-with-pharma-for-pcsk9-inhibitor-cholesterol-drugs-tie-financial-terms-to-improved-customer-health. Accessed November 9, 2016. ** “Southwest General, Anthem Blue Cross Blue Shield offering bundled payment model.” Crain’s Cleveland Business. September 15, 2016. http://www.crainscleveland.com/article/20160914/NEWS/160919920/southwest-general-anthem-blue-cross-blue-shield-offering-bundled. Accessed November 9, 2016.
The Center for Medicare and Medicaid Innovation (CMMI), a new government agency created by Section 3021 of the Patient Protection and Affordable Care Act
(ACA), is at the center of these efforts.

5
the goals of improving quality and lowering costs. Many Medicare, Medicaid, and CHIP beneficiaries are already benefiting from CMMI’s work.
CMMI can play a constructive role as a catalyst for health system change at a critical time in which stakeholders industry-wide are working to improve healthcare value. This relatively new Center, however, stands at a crossroads. While CMMI’s broad flexibility allows for innovation, it also poses risks. Some of these challenges have come to the forefront in recent months as the agency has pursued a wider range of experiments, and pursued testing of broader and more aggressive models.
Section 3021 introduces a certain amount of uncertainty to Medicare, Medicaid, and CHIP policy because new model tests can be rapidly developed and deployed with limited safeguards or opportunities for input and can sharply change existing policy. Whether these models are successes or failures, the testing itself has an impact on the patients, physicians, and other stakeholders affected by them. Learnings from these efforts can inform future public and private initiatives, but only with well-designed tests, strong evaluations, and regular communication from the agency. In addition, some recent proposals have prompted concerns that the breadth and speed of reforms may be leaving patients and providers behind—to the detriment of providers’ ability to offer high-quality care to patients and beneficiaries’ continued ability to access the services they need. Stakeholders across the healthcare industry are also concerned that CMMI approaches and priorities could shift dramatically with changes in leadership.
There is broad consensus across the healthcare industry that CMMI’s work is important and could have great potential value. However, for CMMI to maximize and sustain its successes, it must collaborate effectively with the private sector. That means committing to true tests of new concepts, implementing necessary standards and safeguards, and committing to a more consistent, predictable process to develop, test, and expand new payment models.
In this paper, we explore CMMI’s progress and evolution over its first six years of operation, and the opportunities and challenges that have arisen since its inception. We also examine the importance of, and necessary conditions to support, effective collaboration between CMMI and the private sector.
Early Results From CMMI Initiatives
• Pioneer ACO. The latest preliminary evaluation report (2015) described savings of $384m to Medicare over first 2 years, with improved quality.*
• Partnership for Patients. Only one P4P evaluation has been released, which estimated possible cumulative savings (not including program costs) of $3.1-$4 billion (and 15,000 avoided deaths) over 2011-13 due to reduction in patient harm. No final evaluation has been released for the original model.†
• Comprehensive Primary Care. The latest preliminary evaluation report suggests positive impacts on quality. The latest shared savings results (program year 2015) were positive, with 4 of 7 regions achieving shared savings (in aggregate, $57.7 million, nearly equivalent to the $58 million paid in care management fees to the practices).‡
• Federally Qualified Health Center Advanced Primary Care Practice Demonstration. Both preliminary evaluations suggested that the model actually increased total Medicare costs and did not have an impact on quality. It was terminated at the end of its scheduled 3-year run time.**
* https://innovation.cms.gov/Files/reports/PioneerACOEvalRpt2.pdf† https://innovation.cms.gov/Files/reports/PFPEvalProgRpt.pdf ‡ https://innovation.cms.gov/Files/reports/cpci-evalrpt2.pdf ** https://innovation.cms.gov/Files/reports/FQHCEvalRpt.pdf and https://innovation.cms.gov/Files/reports/fqhc-scndevalrpt.pdf
This relatively new Center, however, stands at a crossroads. While CMMI’s broad flexibility allows
for innovation, it also poses risks.
6
Signed into law in 2010, the ACA included highly visible changes such as expanding Medicaid and introducing the Health Insurance Marketplace (exchanges) to cover more uninsured Americans, closing the Medicare Part D coverage gap (“donut hole”) and removing pre-existing condition exclusions from health plans.
Section 3021 of the ACA, which established CMMI, may have as large an effect on healthcare as these provisions, but is likely not familiar to many Americans. As mentioned, the ACA gave CMMI wide authority to test healthcare payment and delivery models that have the potential to improve quality and/or reduce costs. Unlike previous Center for Medicare & Medicare Services (CMS) demonstration authorities, which were more prescriptive, the ACA granted CMMI considerable latitude to design, test, and expand new models in an effort to speed adoption of successful programs.
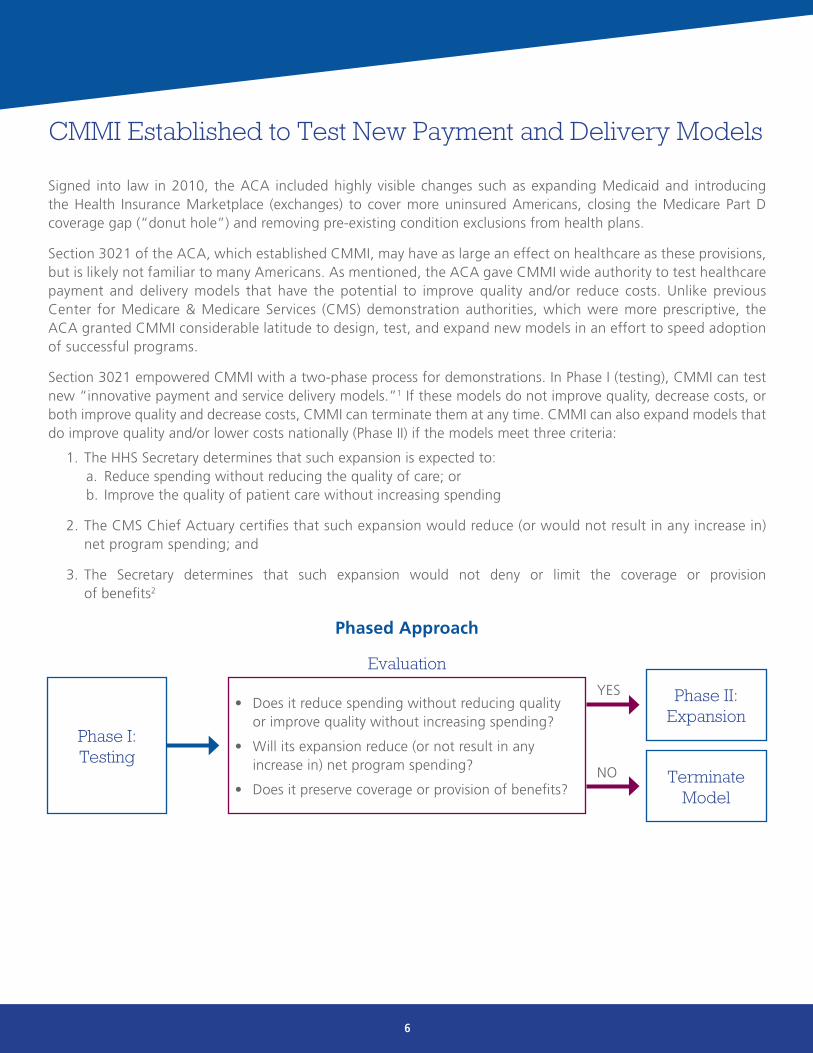
Section 3021 empowered CMMI with a two-phase process for demonstrations. In Phase I (testing), CMMI can test new “innovative payment and service delivery models.”1 If these models do not improve quality, decrease costs, or both improve quality and decrease costs, CMMI can terminate them at any time. CMMI can also expand models that do improve quality and/or lower costs nationally (Phase II) if the models meet three criteria:
1. The HHS Secretary determines that such expansion is expected to:a. Reduce spending without reducing the quality of care; or b. Improve the quality of patient care without increasing spending
2. The CMS Chief Actuary certifies that such expansion would reduce (or would not result in any increase in) net program spending; and
3. The Secretary determines that such expansion would not deny or limit the coverage or provision of benefits2
CMMI Established to Test New Payment and Delivery Models
Phase I: Testing
Evaluation
• Does it reduce spending without reducing quality or improve quality without increasing spending?
• Will its expansion reduce (or not result in any increase in) net program spending?
• Does it preserve coverage or provision of benefits?
Phased Approach
Phase II: Expansion
YES
Terminate Model
NO

7
The ACA appropriated $10 billion for CMMI every 10 years to design, implement, and evaluate Phase I models.3
As of 2016, CMMI has spent nearly $6.1 billion on such efforts.4 As of October 2016, CMMI has launched 44 model tests under its Section 3021 authority. The models comprise a range of forms, including grants to states and initiatives to speed adoption of best practices and transform the delivery system. Approximately half of the initiatives are payment demonstrations that directly modify reimbursement methodologies, for example, by holding providers of healthcare services accountable for spending. Payment demonstrations may include models focused on primary care (e.g., the Comprehensive Primary Care Initiative), bundled payments (e.g., the Bundled Payments for Care Improvement Initiative) and ACOs (e.g., the Next Generation ACO program).5
A majority of CMMI’s models have been voluntary for participants, and have attracted robust participation. CMMI models have wide geographic distribution across the continental United States, as well as in Alaska, Hawaii, and Puerto Rico.6
CMMI Portfolio and Progress
Most CMMI models are scheduled to last five years and remain in the early stages of testing. As a result, it is still too early to make firm conclusions about the impact of CMMI model tests. Few test models are complete. Of the 44 Section 3021 models, most only have had a preliminary evaluation. As a result, final data and results are not available. To date, only two (4.5%)—the Pioneer Accountable Care Organization Model and the Diabetes Prevention Program—have been certified by the CMS Office of the Actuary (a requirement for a test model to expand).7,8 Of those two models, only one—the Pioneer ACO program—was certified to reduce costs.9
Wide Geographic Distribution for CMMI Models
Key: Red squares indicate models run at the state level; blue circles indicate healthcare facilities where Innovation Models are being testedSource: https://innovation.cms.gov/
8
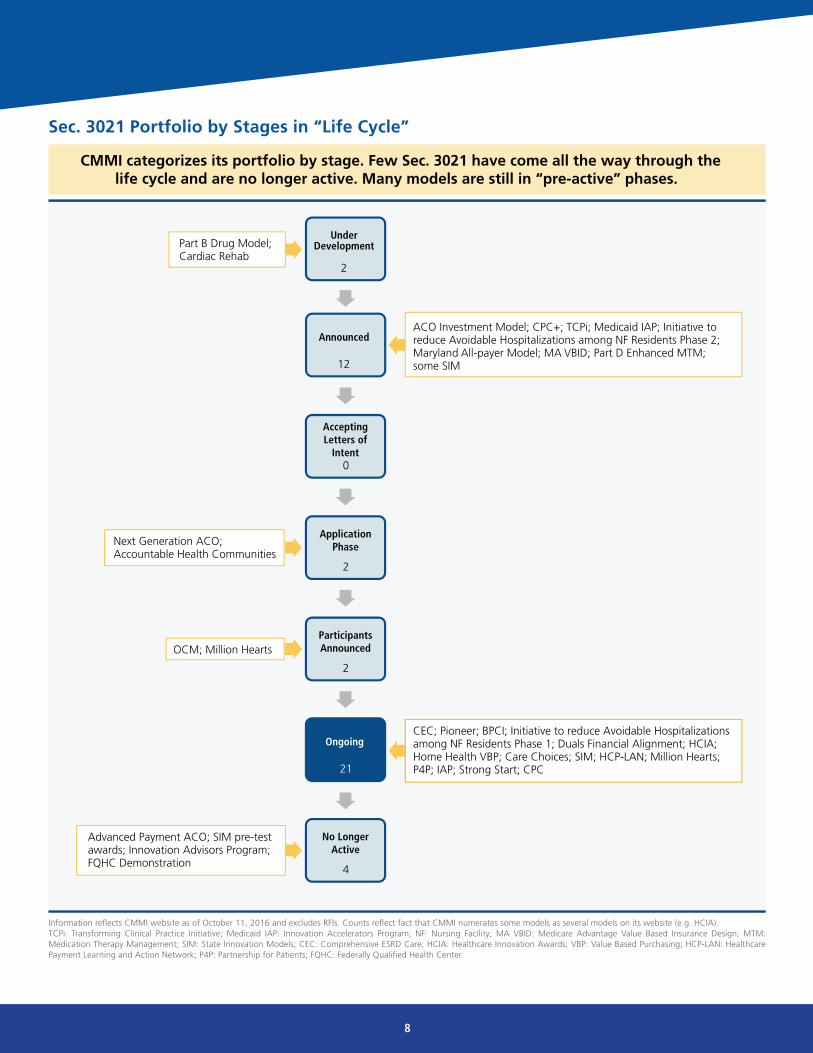
Sec. 3021 Portfolio by Stages in “Life Cycle”
CMMI categorizes its portfolio by stage. Few Sec. 3021 have come all the way through thelife cycle and are no longer active. Many models are still in “pre-active” phases.
ParticipantsAnnounced
2
OCM; Million Hearts
Ongoing
21
CEC; Pioneer; BPCI; Initiative to reduce Avoidable Hospitalizations among NF Residents Phase 1; Duals Financial Alignment; HCIA; Home Health VBP; Care Choices; SIM; HCP-LAN; Million Hearts; P4P; IAP; Strong Start; CPC
No LongerActive
4
Advanced Payment ACO; SIM pre-test awards; Innovation Advisors Program;FQHC Demonstration
AcceptingLetters of
Intent0
ACO Investment Model; CPC+; TCPi; Medicaid IAP; Initiative to reduce Avoidable Hospitalizations among NF Residents Phase 2; Maryland All-payer Model; MA VBID; Part D Enhanced MTM; some SIM
Under Development
2
Part B Drug Model; Cardiac Rehab
Announced
12
ApplicationPhase
2
Next Generation ACO; Accountable Health Communities
Information reflects CMMI website as of October 11, 2016 and excludes RFIs. Counts reflect fact that CMMI numerates some models as several models on its website (e.g. HCIA).TCPi: Transforming Clinical Practice Initiative; Medicaid IAP: Innovation Accelerators Program; NF: Nursing Facility; MA VBID: Medicare Advantage Value Based Insurance Design; MTM: Medication Therapy Management; SIM: State Innovation Models; CEC: Comprehensive ESRD Care; HCIA: Healthcare Innovation Awards; VBP: Value Based Purchasing; HCP-LAN: Healthcare Payment Learning and Action Network; P4P: Partnership for Patients; FQHC: Federally Qualified Health Center.
9
CMMI was intended to allow CMS to move quickly in identifying, testing, supporting, evaluating, and implementing successful demonstrations on a larger scale. It also allows CMS to quickly abandon ineffective concepts.
However, Congress did set some basic parameters to govern CMMI’s work. CMMI must:
• Give preference to models that also improve the coordination, quality, and efficiency of the affected population.1
• Consult representatives of relevant federal agencies, and clinical and analytical experts with expertise in medicine and healthcare management10 and use open door forums or other mechanisms to seek input from interested parties.
• Test payment and service delivery models that:
1. Address a defined population for which there are deficits in care leading to poor clinical outcomes or potentially avoidable expenditures;
2. Reduce costs while preserving or enhancing quality of care; and
3. Focus on models expected to reduce program costs under the applicable title while preserving or enhancing the quality of care received by individuals receiving benefits under such title.11
• Terminate or modify model design or implementation unless the HHS Secretary and CMS Chief Actuary determine, after testing has begun, the model will improve quality without increasing costs, reduce costs without reducing quality, or a combination of the two, both improve quality and reduce costs.12 A model must be cancelled or changed unless HHS or CMS determines it is fulfilling goals of reducing costs and/or increasing quality.
• Evaluate each model’s provision of quality of care and change in spending, and make the evaluation available to the public in a timely fashion.13
• Select quality measures reflecting national priorities for quality improvement and patient-centered care.14
• Submit to Congress a report on delivery models tested, any models chosen for expansion, and the results from evaluations.15
Within these basic parameters, Section 3021 provides wide latitude for the agency in the design, implementation, modification and expansion of model tests. Few specifics precisely define the procedures or standards the agency is expected to meet.
In light of CMMI’s authority to change how Medicare beneficiaries obtain healthcare and the lack of clear, specific standards governing the Center’s initiatives, it is important to establish criteria for assessing CMMI’s operations, and the implications they have for patients, providers, and other stakeholders. CMMI’s operations can be evaluated against a relatively short list of basic elements as described on the next page.
Opportunities and Challenges
A model must be cancelled or changed unless HHS or CMS determines
it is fulfilling goals of reducing costs and/or increasing quality.
10
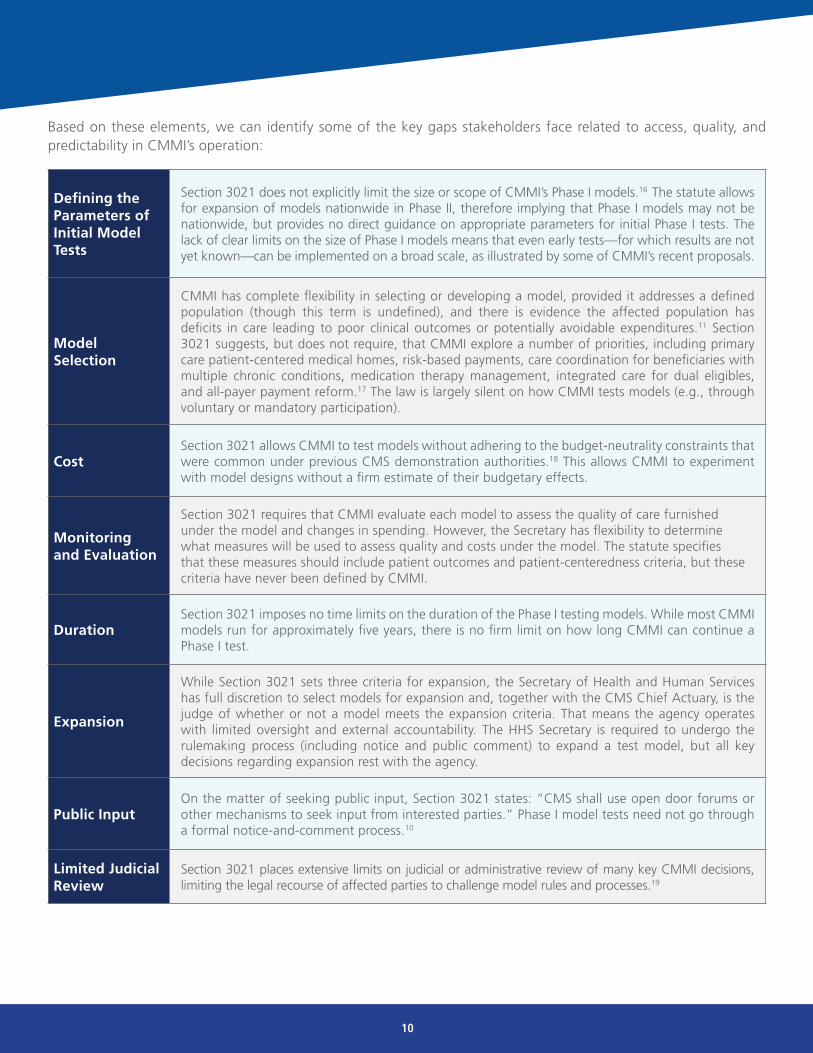
Defining the Parameters of Initial Model Tests
Section 3021 does not explicitly limit the size or scope of CMMI’s Phase I models.16 The statute allows for expansion of models nationwide in Phase II, therefore implying that Phase I models may not be nationwide, but provides no direct guidance on appropriate parameters for initial Phase I tests. The lack of clear limits on the size of Phase I models means that even early tests—for which results are not yet known—can be implemented on a broad scale, as illustrated by some of CMMI’s recent proposals.
Model Selection
CMMI has complete flexibility in selecting or developing a model, provided it addresses a defined population (though this term is undefined), and there is evidence the affected population has deficits in care leading to poor clinical outcomes or potentially avoidable expenditures.11 Section 3021 suggests, but does not require, that CMMI explore a number of priorities, including primary care patient-centered medical homes, risk-based payments, care coordination for beneficiaries with multiple chronic conditions, medication therapy management, integrated care for dual eligibles, and all-payer payment reform.17 The law is largely silent on how CMMI tests models (e.g., through voluntary or mandatory participation).
CostSection 3021 allows CMMI to test models without adhering to the budget-neutrality constraints that were common under previous CMS demonstration authorities.18 This allows CMMI to experiment with model designs without a firm estimate of their budgetary effects.
Monitoring and Evaluation
Section 3021 requires that CMMI evaluate each model to assess the quality of care furnished under the model and changes in spending. However, the Secretary has flexibility to determine what measures will be used to assess quality and costs under the model. The statute specifies that these measures should include patient outcomes and patient-centeredness criteria, but these criteria have never been defined by CMMI.
DurationSection 3021 imposes no time limits on the duration of the Phase I testing models. While most CMMI models run for approximately five years, there is no firm limit on how long CMMI can continue a Phase I test.
Expansion
While Section 3021 sets three criteria for expansion, the Secretary of Health and Human Services has full discretion to select models for expansion and, together with the CMS Chief Actuary, is the judge of whether or not a model meets the expansion criteria. That means the agency operates with limited oversight and external accountability. The HHS Secretary is required to undergo the rulemaking process (including notice and public comment) to expand a test model, but all key decisions regarding expansion rest with the agency.
Public InputOn the matter of seeking public input, Section 3021 states: “CMS shall use open door forums or other mechanisms to seek input from interested parties.” Phase I model tests need not go through a formal notice-and-comment process.10
Limited Judicial Review
Section 3021 places extensive limits on judicial or administrative review of many key CMMI decisions, limiting the legal recourse of affected parties to challenge model rules and processes.19
Based on these elements, we can identify some of the key gaps stakeholders face related to access, quality, and predictability in CMMI’s operation:

11
With most of its activities to date, CMMI has balanced the risks and rewards of testing new payment and delivery models with reasonable use of its authority. For example, CMMI’s work on ACOs has evolved over time, incorporating ongoing feedback from providers and payers. Even so, the latitude granted to CMMI by Section 3021 means it operates with limited input from affected patients and providers, minimal oversight, and limited accountability to stakeholders, Congress, and the general public.
Recently, CMMI has departed from its established approach of testing small scale, voluntary models by proposing several large scale payment initiatives. Patients, providers, and Members of Congress have raised concerns that these initiatives pose enhanced risks to patients and the healthcare system and push the boundaries of CMMI’s intended mission. These stakeholders are concerned that by rapidly advancing these more aggressive proposals, CMMI risks undercutting its goal of improving healthcare value and could unintentionally adversely affect patient access to needed medical care.
Rate of Model Participation Varies Across Models
The scope of recent CMMI models exceeds the common understanding of a “model test.”
CJR Cardiac Bundles Part B Drug Proposal
17%MSAs
83%MSAs
33%MSAs
75%PCSAs
25%PCSAs
67%MSAs
Mandatory participation in model Non-participation
Model denominator information is as follows: CJR (OMB-provided number of total MSA areas, including Puerto Rico - 389); CR (denominator of 294 total possible MSAs, after exclusion criteria noted in regulation)MSA: metropolitan statistical area; PCSA: primary care service area
Ongoing CMMI operations have brought to light several key issues: 1. The shift in design of Phase I tests from smaller, voluntary designs to larger, mandatory models; 2. Challenges in achieving balance between recommending rapid expansion of successful tests and Congress’ role in effecting permanent policy change; 3. Lack of a consistent, open process to engage a wide variety of stakeholders; and 4. Gaps in the monitoring and evaluation strategy for model tests. In addition, policymakers and thought leaders have recently highlighted the unique challenges that CMMI’s construct creates regarding estimation of savings related to CMMI, and the extent to which Congressional Budget Office (CBO) scoring assumptions have reinforced barriers to meaningful Congressional engagement.
These issues are discussed in greater detail on the following pages.
Recent CMMI proposals, which include the Comprehensive Care for Joint Replacement Model (CJR), Part B Drug Payment Model, and Cardiac Bundled Payment Model, have prompted concerns from the patient and provider communities because they exceed the common understanding of what constitutes a “model test.” While, traditionally, “test models” have limited enrollment and voluntary participation to allow CMS to better understand costs and benefits, all three of these proposals, described in greater detail below, mandate the participation of providers in large cross sections of the country.
• Comprehensive Care for Joint Replacement Model (CJR). The CJR model tests bundled payment for an episode of care associated with hip and knee replacements to encourage hospitals, physicians, and post acute care providers to coordinate to improve the quality and coordination of care from initial hospitalization through recovery. Started in April 2016, the model mandates participation by over 800 hospitals in 67 metropolitan statistical areas (MSAs), or almost one-fifth (17.5%) of the country.20
• Proposed Part B Drug Payment Model. The Part B Drug Payment Model is designed to determine if the average sales price payment methodology for Part B drugs drives prescribing patterns. The model, proposed in March 2016, would cut provider reimbursement for many Part B-covered drugs, which could put additional financial strain on practices and result in more patients receiving treatment in higher-cost sites of care such as hospital outpatient departments. The mandatory model, if adopted, will enroll physicians in 75% of the country.21
• Cardiac Bundled Payment Model. The Cardiac Bundled Payment Model would make affected hospitals financially accountable for the cost and quality of all care associated with bypass surgery and heart attacks. Starting in 2017, the model will require participation by hospitals in over one-quarter of the country (98 MSAs, or 25.6%) to test bundled payments for heart failure and coronary artery bypass grafting (CABG), and almost 12% of the country (45 MSAs, or 11.7%) to test bundled payments for cardiac rehabilitation.22
These large-scale, mandatory program designs pose unique challenges. First, these models could pose enhanced risks to beneficiaries. With respect to the CJR model, some have raised concerns that this model may exacerbate existing racial and socio-economic disparities in joint replacement utilization.23 The Medicare Payment Advisory Commission (MedPAC) has expressed concerns about the Cardiac Bundled Payment Model cardiology bundled payment demonstrations, which follow a similar design as the CJR. Specifically, MedPAC noted the lack of evidence to support the model and its potential impact on beneficiary care.24 Finally, the Part B Drug Payment Model was met with widespread opposition from patients, providers, and Members of Congress for its potential to harm patient access and quality of care, and notable lack of safeguards to protect beneficiaries.
Key Issue 1: Proposals for Large-Scale, Mandatory Models
12

13
Because these models are intended to be tests, their specific implications are not yet known. As a result, rolling these model tests out on a large scale, particularly given the gaps in real-time monitoring and quality measurement discussed below, may not be prudent. Untested models that mandate participation by large swaths of the provider community could prompt changes in care processes that may prove difficult to reverse or alter if the model increases costs or compromises quality. If models are first tested on a small scale, these potential unintended consequences can be quickly identified and mitigated before causing broad harm. However, if initial test models operate on a large scale or even near-nationwide basis, unintended consequences may prove irreversible.
In addition, large-scale mandatory models risk subjecting providers to multiple, competing payment structures. A complicating factor of large-scale models is they increase the likelihood the model will overlap with other CMS models and demonstrations. Overlapping models make it difficult to tease apart which policy change influenced cost or quality, thus undermining the sole purpose for testing the model. While CMMI pledges to carefully monitor outcomes, quality-of-care measures included in the mandatory models may not suffice as checks and balances.
Mandatory models also place a significant burden on providers, many of whom are already devoting significant resources to respond to the changing payment and delivery landscape. These models will require many physicians and hospitals to expend valuable time to understand the logic and algorithms of the overlapping models so items and services are properly assigned. Were the test models voluntary, providers could account for this additional layer of planning in their decision to participate; however, the mandatory nature of these models necessitates that analysis, regardless of previous commitments for those resources.
And these resources may already be devoted to existing voluntary programs. For example, the proposed Part B Payment Model overlaps with the Oncology Care Model (OCM); both change how Part B drugs are paid for and, while the Part B Model is not yet finalized, it is possible providers who voluntarily enrolled in the OCM could find themselves subject to the mandatory payment cuts in the Part B Drug Payment Model. Large-scale, mandatory models also may undercut meaningful progress providers have made with commercial payers. Pushing providers to change—but letting them select their method of change—could be more beneficial and further advance best practices, as not all reforms fit with all patients, medical specialties, or geographic regions. Providers are currently subject to comprehensive quality-improvement programs that evaluate measures such as cost control, so the motivation to reform is already present without further mandates from CMMI.
For example, the Medicare Access and CHIP Reauthorization Act (MACRA) links Medicare physician payments to metrics of cost, quality, and clinical practice improvement through its Merit-Based Incentive Payment System. MACRA also provides a 5-percent annual bonus payment to clinicians who participate in select APMs, creating a significant incentive for clinicians to participate in CMMI models on a voluntary basis.
If initial test models operate on a large scale or even near-nationwide basis, unintended consequences may
prove irreversible.

14
While the majority of CMMI’s work to date has focused on Phase I (model testing), CMMI is authorized to expand successful models. The distinction between testing and expansion may appear straightforward, but in practice has proved to be much more complex.
As discussed above, Section 3021 does not clearly define the parameters of a model test beyond the requirement that tests address a defined population that has deficits in care. The breadth of these undefined parameters, and the leeway they offer the Center, is reflected in CMMI’s testing activities, which do not always clearly define individual demonstration programs. Of the models in CMMI’s current portfolio, several have been “re-launched” as new tests.
For example, the Comprehensive Primary Care initiative (CPC) ran from January 2013 and will end in December 2016. Beginning in 2017, CMMI will re-launch this model as the CPC-Plus Initiative, a similarly structured model test with select changes. Several other models have been re-launched upon their conclusion. The Advanced Payment ACO Model was re-launched as the ACO Investment Initiative, and the Partnership for Patients was re-launched as the Hospital Engagement Networks. For other Phase I model tests, CMMI has used its initial voluntary model as the basis to propose mandatory tests. The voluntary Bundled Payments for Care Improvement model served as the basis for both the mandatory CJR and Cardiac Bundled Payment Models.
Though CMMI considers relaunched models and the above mandatory versions of its bundled payment programs to be Phase I tests, they are in effect “expansions” in duration or scope of existing models. If CMMI can continuously relaunch or otherwise extend Phase I tests, it raises questions about the meaningfulness of the distinction between Phase I and Phase II, and criteria that must be satisfied for a model to transition to Phase II.
Key Issue 2: Tension Between Testing, Expansion, and Permanent Changes in Healthcare Policy

15
Congressional Budget Office (CBO) Scoring Assumptions May Hinder Congress’ Oversight
A recent hearing held by the House Budget Committee spotlighted an unexpected barrier to Congress’ ability to oversee CMMI activities. The CBO estimates that CMMI will generate $34 billion in federal savings over the next 10 years. Because CBO attributes this high potential for savings largely to CMMI’s broad reach and flexible process, rather than to any specific policy it expects to lower costs while maintaining or improving quality, legislative proposals that overlap with or intervene in CMMI activities are scored by CBO with a cost to the federal government.* This means that to enact CMMI related legislation, Congress must find offsets under PAYGO procedures.
This dynamic challenges Congress’ ability to oversee CMMI. For example, if Congress wishes to prevent implementation of a CMMI program in order to protect Medicare beneficiaries, it must make other mandatory spending cuts to offset the cost of the legislation. It also challenges Congress ability to legislate in the Medicare space; if Congress wishes to pass legislation that overlaps with a current or proposed CMMI program, CBO may score the legislation at a cost, thus requiring offsets under PAYGO rules. The effective consequence of Congress having to follow PAYGO procedures to offset any estimated savings from Section 3021 models it wants to stop or change would be for the executive branch to specify government funding requirements to the legislative branch, which impedes Congress’ oversight and budgetary roles and may contravene Article I of the Constitution.
* Mark Hadley, Deputy Director Congressional Budget Office. “Testimony: CBO’s Estimates of the Budgetary Effects of the Center for Medicare & Medicaid Innovation.” http://budget.house.gov/uploadedfiles/09-07-2016-cmmi_testimony.pdf. September 7, 2016.
CMMI’s expansion authority also raises questions about how CMMI intersects with Congress’ role legislating permanent changes to the Medicare, Medicaid, and CHIP programs. In Phase I testing, CMMI has the ability to waive provisions of the law in order to facilitate a model test. For example, many CMMI programs waive aspects of the Anti-Kickback Statute to facilitate close collaboration between providers that might not otherwise be permitted under the law. A plain reading of the CMMI statute suggests that this ability to waive provisions of the law only applies when CMMI is testing models. However, CMS described in the 2017 Medicare Physician Fee Schedule Final Rule its interpretation that the waiver authority extends to model expansions as well:
“In our view, the Secretary is authorized to waive requirements of Title XI, Title XVIII, and sections 1902(a)(1), 1902(a)(13), 1902(m)(2)(A)(iii), and 1934 of the Act (other than subsections (b)(1)(A) and (c)(5) of such section) in connection with expanded model tests.”29
Regardless of how one interprets Section 3021, the discussion of CMMI’s waiver authority with respect to expansion underscores an area of tension between CMMI’s role testing policy options and Congress’s role in setting the laws and policies governing Medicare, Medicaid, and CHIP. While it is important for CMMI to have flexibility to innovate and build on successes, Congress must also continue to set the direction for permanent changes in policy and fulfill its constitutional responsibility to approve permanent changes to federal law. In addition, Congress has a duty to oversee implementation of CMMI to ensure the agency complies with the statute and to protect beneficiaries from harmful policy changes if needed.
[There is] a tension between CMMI’s role testing policy options as an innovation hub and Congress’
role in setting the laws and policies governing Medicare, Medicaid, and CHIP.

16
Key Issue 3: Inconsistent Stakeholder Engagement and Limited Insight into Model Results
The US healthcare system is characterized by a broad, interconnected variety of payment systems, providers, and facilities. This breadth presents an opportunity to gather feedback from a wide range of vantage points and hear from those directly and indirectly affected by proposed models.
As noted above, Section 3021 requires CMMI to collect input from interested parties through open door forums or other mechanisms. CMMI has engaged stakeholders through various avenues such as meetings and more formal Requests for Information, but the level of interaction between CMMI and stakeholders has been inconsistent. For example, CMS incorporated a high level of stakeholder input into its design of the OCM, a voluntary Section 3021 model that tests care management and episode-based payments for cancer patients. CMMI developed the OCM through a multi-year process that began with the convening of a multi-stakeholder technical expert panel25 and included opportunities for public comment on the preliminary model design. CMMI also retained the RAND Corporation to conduct a simulation of model effects to identify and mitigate potential unintended consequences.26 As a result of these efforts, the OCM has fairly broad support within the oncology community; 200 oncology practices nationwide voluntarily enrolled in the program.
By contrast, many stakeholders agree that CMMI did not seek adequate advanced input into the model design for the Comprehensive Care for Joint Replacement Model, which would require hospitals in 67 metropolitan statistical areas to participate in a mandatory bundled payment test. Unlike the process used for the OCM, CMS issued this model as a Notice of Proposed Rulemaking without an advanced notice-and-comment opportunity. Proposal of this model was met with concern by hospitals and Members of Congress, who requested that CMS delay implementation of the rule.27
CMMI has engaged stakeholders through various avenues such as
meetings and more formal Requests for Information, but the level of interaction between CMMI and
stakeholders has been inconsistent.

17
CMMI also offers limited insight into its work plan. As a result, stakeholders are largely uninformed regarding the development of models that may impact them, and often cannot offer their insight during the critical early-development process in order to identify potential pitfalls and improve the model. This creates a highly unpredictable environment for future payment policy. Though CMS has placed the large-scale, mandatory models in the formal notice-and-comment rule-making process, the likelihood of CMS instituting major restructuring of the models shrinks by the time the models have reached the proposed rule stage. At best, stakeholders can influence the models at the periphery.
Stakeholders also have limited insight into the progress of various test models over time. Private sector stakeholders have expressed frustration that information on the early experience with CMMI models is not more readily available to facilitate and improve upon parallel efforts in the private sector. Evaluation results are routinely published on the CMMI website, but these evaluation reports often do not include anecdotal experience from model participants. This makes it challenging for private sector actors to transfer and expand best practices. Enhanced communication and collaboration with the private sector would speed adoption of best practices and increase the pool of data to analyze, allowing multiple parties to vet the models and/or to even improve them.
In addition, more consistent release of the quality and spending data that underpins CMMI’s evaluations would allow independent parties to verify the model test results and validate CMMI’s findings with respect to costs and quality, which could strengthen support.

18
Section 3021 requires CMMI to conduct an evaluation of each model test. The evaluation must include an analysis of the quality of care furnished under the model, including the measurement of patient-level outcomes and patient-centeredness criteria and the impact of the model on program spending. The statute states that model results will be made available to the public “in a timely fashion” and states and other participating entities may have “to collect and report information…necessary to monitor and evaluate” the models.28 CMMI typically hires private research and consulting firms (e.g., Mathematica and RTI) to act as the evaluators with support from the Research and Evaluation Group within CMMI. Currently, at least one preliminary evaluation report is available for each model that has been running for at least three years, but no final evaluation reports have been published for any Section 3021 models.
Establishing appropriate methods to monitor for quality and access issues has proved challenging for some models. When CMMI released its Part B Drug Payment Model proposal in March 2016, patient advocates raised concerns that the model did not include sufficient information on how CMMI intended to monitor for unintended consequences beyond a limited appeals process. Subsequently, advocates who support and oppose the model alike have come forward with recommendations to improve the monitoring strategy. Without a robust monitoring strategy, unintended effects that negatively impact quality of care in CMMI models could go undetected.
Effective monitoring and evaluation can also be challenged by the rapidly evolving quality measurement landscape. Robust, evidenced-based quality measures may not exist for some clinical areas in which CMMI is interested in testing models. Organizations like the National Quality Forum Measures Application Partnership are working to identify and fill these measure gaps. Even when appropriate measures are available, evaluators may not have the ability to compare quality performance against a match control group if measure reporting requirements are exclusive to the test model.
Key Issue 4: Gaps in Monitoring and Evaluation
19
Conclusion
As our healthcare system evolves toward value-based care, it is essential to test new ideas that have the potential to
make healthcare more quality driven, cost efficient, and patient-focused. The CMMI provides such a platform with
which to experiment and evaluate new payment and delivery approaches. Because of the potential impact, however,
on patients, healthcare providers, and other health system stakeholders, it is essential that such experimentation
comply with the original intent of CMMI as a test bed for new healthcare payment and delivery policies that can be
broadly implemented by both the public and private sectors to improve quality and reduce costs.
CMMI needs appropriate authority to operate well designed initiatives that are true tests. To innovate, the agency must
have a certain degree of flexibility. However, given the extremely wide latitude Section 3021 confers to CMMI and its
ability to set aside the laws and policies adopted by Congress, there is concern among stakeholders on what might come
next from CMMI. There is nothing preventing CMMI from testing a model with the following parameters:
• Includes all Medicare and/or Medicaid beneficiaries in the US
• Increases costs
• Operating in perpetuity
• No opportunity for public input
• Completely new Medicare and/or Medicaid payment methodology for items and services
• Limited ability to undergo judicial or administrative review
• Compromises quality and patient access to care
In effect, CMMI could “test” a model that completely restructures the Medicare or Medicaid program. This
uncertainty has the potential to stifle progress toward innovative and sustainable value-based payment models
among stakeholders because they will not want to start to down a path only to have changes superimposed on their
carefully vetted, voluntary efforts.
The concept of effectively and appropriately testing new healthcare delivery and payment models that can improve
care and affordability is sound. CMMI’s first six years of experience show its promise, but also underscores challenges
for the private sector. As discussed above, several recent CMMI proposed demonstration projects could have an
adverse effect on patients and their access to essential care since they affect significant portions of the healthcare
system — to the point of essentially becoming changes to federal payment policy. Congress should have the ability
to intervene in these matters, but its ability to do so is hampered by Congressional Budget Office scoring rules that
assume theoretical savings from CMMI initiatives. Safeguards must be put in place to ensure that what should be
limited, focused demonstration projects do not become sweeping, untested changes to our healthcare system,
affecting the lives of millions. Additionally, changes to improve predictability and collaboration with the private
sector will ensure that CMMI’s work best serves patients, providers, and actors through the healthcare sector.
20
References
1. SSA §1115A(a)(1).
2. SSA §1115A(c).
3. SSA §1115A(f)(1).
4. Department of Health and Human Services. Fiscal Year 2017 “Budget in Brief.” http://www.hhs.gov/sites/default/files/fy2017-budget-in-brief.pdf. Accessed November 10, 2016.
5. Center for Medicare and Medicaid Innovation. “Innovation Models.” https://innovation.cms.gov/initiatives/#views=models. Accessed October 28, 2016.
6. Center for Medicare and Medicaid Innovation. “Where Innovation is happening” https://innovation.cms.gov/initiatives/map/index.html. Accessed October 28, 2016.
7. CMS Office of the Actuary. Certification of Pioneer Model Savings. https://www.cms.gov/Research-Statistics-Data-and-Systems/Research/ActuarialStudies/Downloads/Pioneer-Certification-2015-04-10.pdf. Published April 10, 2015. Accessed October 26, 2016.
8. CMS Office of the Actuary. Certification of Medicare Diabetes Prevention Program. https://www.cms.gov/Research-Statistics-Data-and-Systems/Research/ActuarialStudies/Downloads/Diabetes-Prevention-Certification-2016-03-14.pdf. Published March 14, 2016. Accessed October 26, 2016.
9. CMS. Medicare Diabetes Prevention Program Expansion. https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-07-07.html. Published July 7, 2016. Accessed October 21, 2016.
10. SSA §1115A(a)(3).
11. SSA §1115A(b)(2)(A).
12. SSA §1115A(b)(3)(B).
13. SSA §1115A(b)(4).
14. SSA §1115A(b)(4)(C).
15. SSA §1115A(g).
16. SSA §1115A(a)(5).
17. SSA §1115A(b)(2)(B).
18. SSA §1115A(b)(3)(A).
19. SSA §1115A(d)(2).
20. Center for Medicare and Medicaid Services. Medicare Program; Comprehensive Care for Joint Replacement Payment Model for Acute Care Hospitals Furnishing Lower Extremity Joint Replacement Services Final Rule. 80 Federal Register 73273.
21. Center for Medicare and Medicaid Services. Medicare Program; Part B Drug Payment Model Proposed Rule. 81 Federal Register 13229.Center for Medicare and Medicaid Services. Medicare Program; Advancing Care Coordination Through Episode Payment Models (EPMs); Cardiac Rehabilitation Incentive Payment Model; and Changes to the Comprehensive Care for Joint Replacement Model (CJR) Proposed Rule. 81 FR 50793.
22. The CMS Comprehensive Care Model and Racial Disparity in Joint Replacement. Said A. Ibrahim, MD, MPH, MBA; Hyunjee Kim, PhD; K. John McConnell, PhD. JAMA. Published online September 19, 2016. doi:10.1001/jama.2016.12330
23. The CMS Comprehensive Care Model and Racial Disparity in Joint Replacement. Said A. Ibrahim, MD, MPH, MBA; Hyunjee Kim, PhD; K. John McConnell, PhD JAMA. Published online September 19, 2016. doi:10.1001/jama.2016.12330
24. Medicare Payment Advisory Commission. http://www.medpac.gov/docs/default-source/comment-letters/09302016_epmbundling_medpac_comment_sec.pdf?sfvrsn=0
25. Brookings and MITRE. Specialty Payment Model Opportunities Assessment and Design: Summary of the Technical Expert Panel for Oncology. http://www2.mitre.org/public/payment_models/Brookings_Oncology_TEP_Summary.pdf. December 17, 2013.
26. RAND and MITRE. Specialty Payment Model Opportunities and Assessment: Oncology Simulation Report. http://www2.mitre.org/public/payment_models/Oncology_Simulation_Report_14-3380.pdf. 2014.
27. Member of Congress Letter to Acting Administrator Andy Slavitt and Deputy Administrator Patrick Conway. September 21, 2015.
28. SSA §1115A(b)(4)(B).
29. 2017 Medicare Physician Fee Schedule Final Rule. https://s3.amazonaws.com/public-inspection.federalregister.gov/2016-26668.pdf.

21
Where knowledge, reach and partnership shape healthcare delivery. © November 2016
Funding for this research was provided
by the Healthcare Leadership Council.


















