Hyperthermia and Hypothermia Back to Basics April 2011 Dr. J. Clow, ER.
Upload
griselda-reedCategory
view
217download
0
AccidentalHypothermia

The Basics
Clinical Questions
Treatment

Who gets hypothermia?

Case:
25 M Ice climber…
Temp: 31 degrees

How would you classify this pt’s hypothermia?
31 degrees C

Mild: Core temp. 32 to 35ºC
Moderate: Core temp. 28 to 32ºC
Severe: Core temp. below 28ºC

Mild:34 - amnesia and dysarthria begin33 - ataxia and apathy develop
Moderate:32 - stupor31 - shivering stops30 - dysrhythmias, CO drops, insulin ineffective
Severe:28 - high risk for VF27 - lose reflexes and voluntary movement26 - major A/B disturbance
Profound:19 - flat EEG18 - asystole

Pretend there is no history of exposure…why else could this
patient be hypothermic?

Differential Diagnosis
Increased Heat Loss
Decreased Heat
Production
Impaired Heat Regulation

What mechanisms contribute to heat loss in our patient?
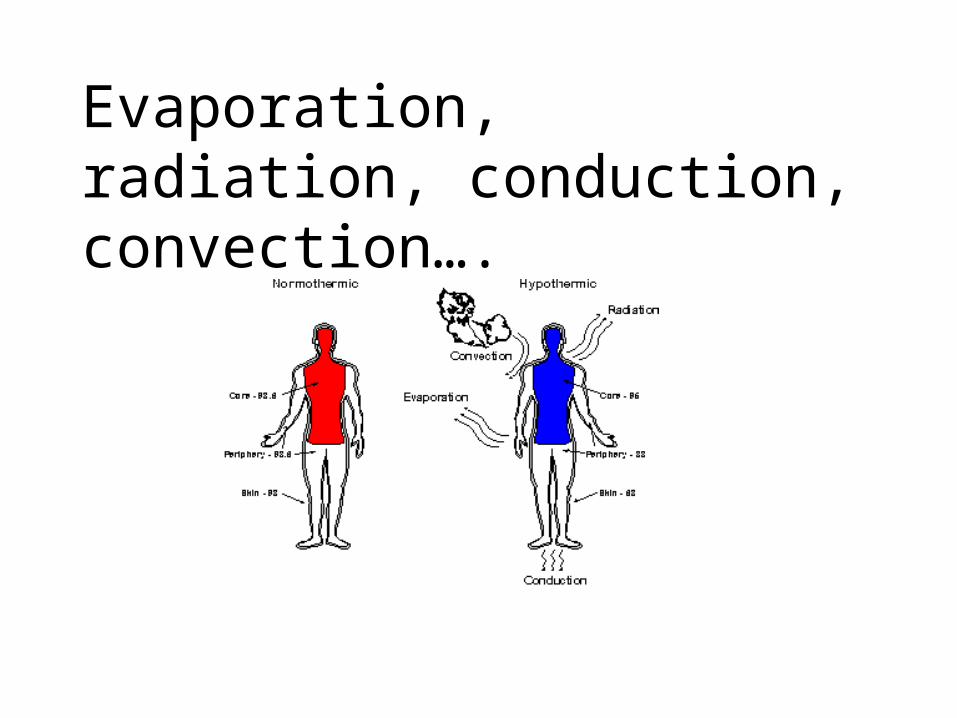
Evaporation, radiation, conduction, convection….

How is the cold affecting this patient?
At the body level?
At the organ system level?

QuickTime™ and a decompressor
are needed to see this picture.

Increase HR
Progressive bradycardia
Ventricular Arrhythmias
Asystole
QuickTime™ and a decompressor
are needed to see this picture.





The J Wave

Cold diuresis
Reduced renal flow

Progressive depression
perfusion maintained until 25 degrees
19 degrees flat EEG

Initial stimulation
Progressive decrease
CO2 retention and Acidosis

Case continued….

What is the most accurate method of measuring his
temperature?
Rectal temperature (insert to 15 cm)- ? Accurately reflect brain/heart temperature- Influenced by adjacent frozen stool- lags behind core temperature changes
Oral- Often do not measure below 34 degrees C.
Tympanic- accurately reflect hypothalamus if true tympanic
Axilla- easily affected by external factors
Esophogeal (insert to 24 cm)-can be affected by warm airway temperature in tubed patient
ChemstripElectrolytesCreatinine, BUNHg, WBC, PltLactateEKGABG
Other: CK, fibrinogen, INR, cortisol, thyroid
Blood Work
Chemstrip:-Insulin ineffective below 30 degrees -persistent elevation despite rewarming signals secondary cause
Hct:-Increases 2% for every drop by 1 degree C-Beware of the hypothermic patient with a normal/low hematocrit
ABG:-Historically controversial-Use uncorrected values
Blood Work

How can you rewarm him?

Passive External Rewarming (PER)
• Providing blankets
• Moving to a warm environment
• Heated IV fluids/oral fluids
**pt must be able to produce their own heat
***slow rise in temperature

Active External Rewarming
• Applying heat to the skin:
– Warm blankets– Bear Hugger– Immersion warming– Brokeback Hug?

Active Internal Rewarming
• Peritoneal dialysis
• Bladder, gastric, or colonic lavage
• Heated intravenous fluids
• Heated humidified oxygen
• Thoracic cavity lavage
• Extracorporeal blood rewarming
• Hemodialysis
Recipe:
Warmed NS
1) Place 1L NS in 650 W microwave
2) Cook on high for 120s, turning and shaking it once at midcycle
3) Agitate before infusion

Inhaled warmed O2
• Use warmed air at 45 degrees celcius
• Up to 2 degrees/hr*

Peritoneal Lavage
• Use Arrow peritoneal lavage kit
• Up to 3 degrees C/hour
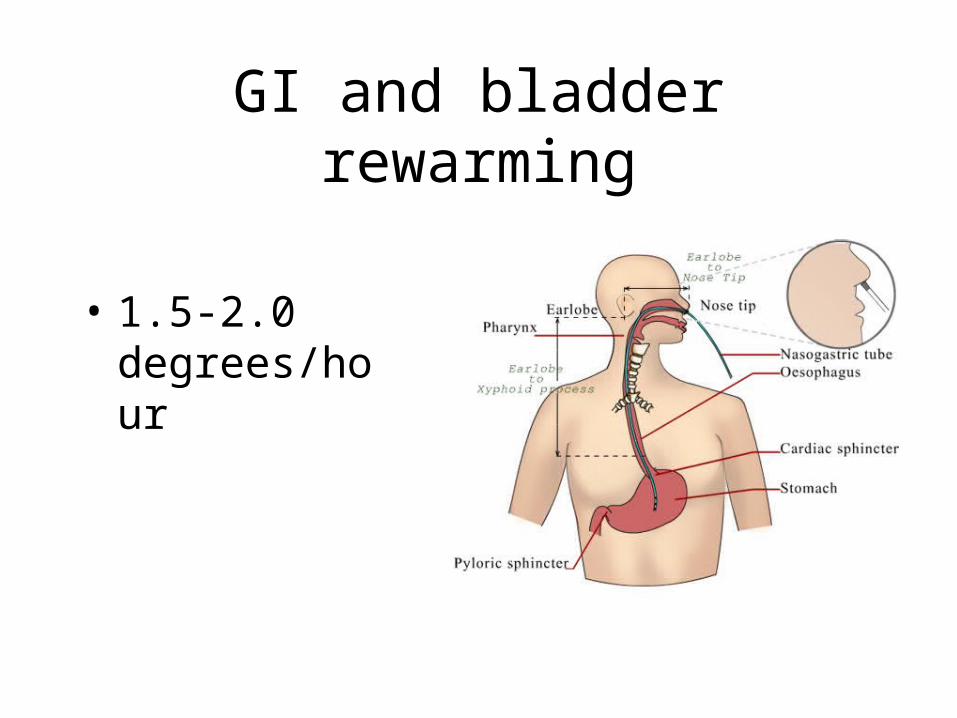
GI and bladder rewarming
• 1.5-2.0 degrees/hour

Thoracic Cavity Lavage
Up to 6 or 7 degrees/hour reported

Cardiac Bypass
• Need to consult CV surgery
• Up to 2 degrees/5 mins

Hemodialysis
• Up to 4.5 degrees/hour

Comparison of Rewarming Rates

Case Continued

• Why has this patient become more hypothermic despite your warming measures?

Approach to rewarming
Mild Hypothermia
Passive External Rewarming
+/- Active External Rewarming

Approach to rewarming
Moderate Hypothermia
Active External Rewarming
Active Internal Rewarming

Approach to Rewarming
Severe Hypothermia
Level 1 callout
If Stable, treat as moderate but be prepared for ecmo
If Unstable, ACLS and prepare for ecmo

ACLS guidelines?BLS:
-prevent heat loss, rewarm-mild AH = passive rewarming-moderate AH = AER-Severe + Stable = AER or AIR-Severe + Unstable = bypass or AIR-Do not withhold ABC’s to rewarm
ACLS:-If in VF or pulseless VT, attempt defibrillation-“Might be reasonable to perform further defibs-“Might be reasonalbe to administer vasopressor”

Cold and Dead?
“Patients with severe accidental hypothermia and cardiac arrest may benefit from resuscitation even in
cases of prolonged downtime and prolonged cpr”

The Obvious:-Decapitation
-Non-compressible chest-Ice in mouth and nose
-DNR order
The Unreliable:-rigor or livor mortis
-fixed pupils-tissue deterioration

Rosens:“Significant predictors of outcome”
asphyxia, prehospital arrest, low or no BP, high BUN, need
for intubation in ER
Literature:
Mt. Hood: only survivors had signs of life on scene, temps were above 20 degrees, K < 7
Mair et al. 1994: K > 10, pH < 6.5,
Others: fibrinogen <50mg/dL, ammonia >250mmol/L


Frostbite

Case:
In minor ER
63 M
Pernio
• Local, inflammatory, bluish-red lesions
• Caused by prolonged vasoconstriction
• Gentle drying and massaging.

Immersion Injury (Trench Foot)

Cold Injury
Non-Freezing
• Pernio• Immersion Injury
• Cold Urticaria
Freezing
• Frostnip• Frostbite

Frostnip
Reversible and superficial
No tissue loss
Pale and discomfort and tingling
Case:
27 F Car broke down on a rural road.Decided to walk out
While walking through wooded area, she gets lost, at one point ending up knee deep in a stream.
She wanders through the forest for 12 hours lost.
Eventually she is spotted by a hunter who calls EMS.

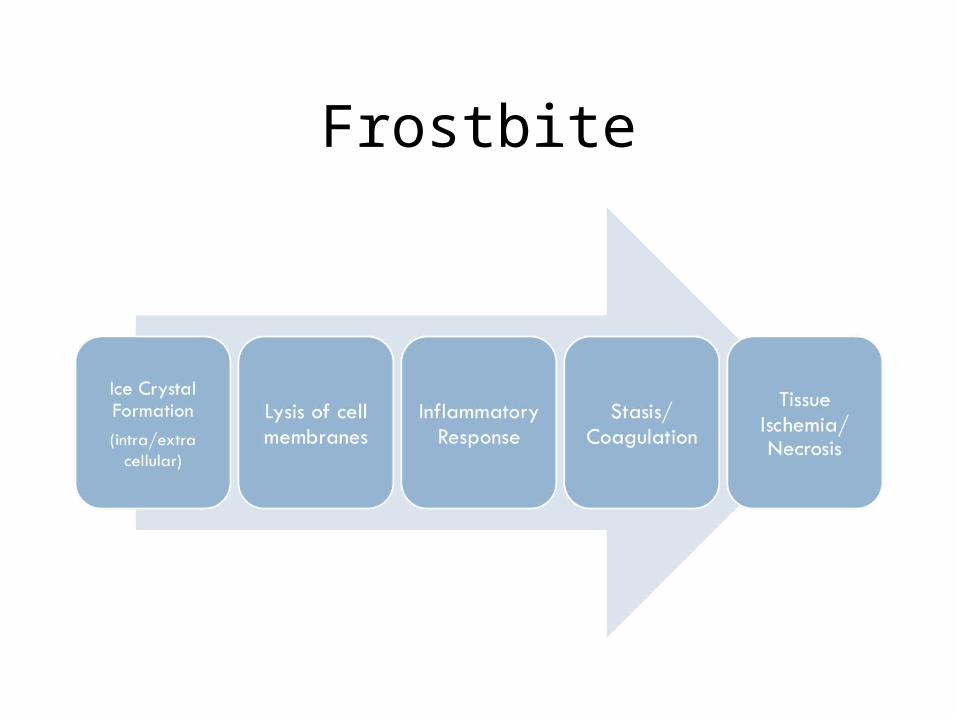
Frostbite

Classification

Treatment
• Remove wet clothing• Rapid rewarming with warm water (40
degrees)• Analgesia!!• NSAID’s?• Td
Treatment
• Thawing:– 40 degrees– Until part feels soft, erythema present– Usually requires 10-30 minutes– Active motion by patient

Treatment
• Post-thaw:– Elevate– Sterile, bulky dressing– Aloe Vera?– Blisters?– TPA?– Heparin?– Abx?– Hyperbaric O2?, Pentoxifylline?

Treatment
• Surgery?
• Admission?

Summary
1) Spectrum of freezing and non-freezing injuries
2) Treat by rapid rewarming
3) Aloe, ibuprofen, and Td (others are controversial)






![Rewarming Techniques Externalottawaemahd.weebly.com/uploads/2/1/7/2/21729574/... · 2018. 9. 9. · production may be activated by accidental hypothermia.[1] Active External Rewarming](https://static.fdocuments.in/doc/165x107/60b0d674e5cf7652cd623a47/rewarming-techniques-2018-9-9-production-may-be-activated-by-accidental-hypothermia1.jpg)