Hypothermia, Prevention, Recognition, Treatment_ Hypothermia Special Situations
date post
19-Dec-2015Category
view
216download
1
Accidental Hypothermia
François Dufresne
McGill Emergency Medicine
May 2nd 2001
The Case of Tommy
• 23h10• Call from MD working in James Bay• Male, 27 y.o. Unresponsive.• Found in snow, cross-country skiing• Normal Airway. Breathing. O2 sat.• Femoral pulse + (35) BP.• GCS=3 TR = 28C.• IV. Monitor. Mask with 100% O2

The Case of Tommy…
• Friend told MD: PMH. Rx. drugs. EtOH
• Major foot deformity
• Looks like fell in ski and could not return home by himself…
• MD has some questions for you…
The Case of Tommy…
• Should he intubate? Are there risks to precipitate dysrythmias?
• Cold myocardium prone to arythmias?
• How should he rewarm the patient?• Danger of afterdrop?
• He wants an ABG but should he ask for the blood to be warmed to normal T for analysis…or it doesn’t matter?
Answer: You’ll call him back…
The Case of Tommy…
• MD calls you back 30 minutes later
• Pt in cardiac arrest : V.fib. Now 27C• 3 shocks
• Epinephrine + re-shock
• Having Amiodarone prepared…
• How long should he do CPR and rescussitation?
Anything wrong ?Answer ?

Introduction
• Maritime / War litterature
• Hannibal experience in 218 B.C
Hannibal against Rome

Introduction
• EtOH • Mental illness • Homelessness • Province of Quebec Cold

Plan
• Definitions
• Physiology
• Pathophysiology
• Labs findings : ABG, ECG
• Rewarming methods
• Afterdrop
• ACLS 2000 guidelines
Definitions
• Primary VS Secondary
• Primary– Normal thermoregulation– Overwhelming cold exposure
• Secondary– Abnormal thermogenesis– Multiple causes
Definitions
• Hypothermia : < 35C
• Mild : 32-35C• Moderate : 28-32C• Severe : < 28C
Physiology: Heat production
• Basal metabolism (Metabolic rate)– Heart / Liver
• Anterior hypothalamus
• Thyroid / Sympathetic
• Preshivering muscle tone (2x)
• Shivering (2-5x)
• Posterior hypothalamus
Physiology: Heat dissipation
• Radiation (55-65%)• Gradient between environement and
exposed body area.
• Conduction (2-3%)• Direct contact with cold substance
• Convection (10-15%)• Wind…
• Evaporation (20-35%)
Physiology…
• Above 32C:– Vasoconstriction– Shivering– Basal metabolic rate
• Below 32C:– No shivering
• Below 24C:– No basal metabolic rate
Pathophysiology
Cardiovascular– Initial tachycardia– Gradual bradycardia : HR 50% at 28C.– Not consistent ?
• Hypoglycemia, intoxication, hypovolemia,…?
– Refractory to atropine BP CI– A.fib (T < 32C)– V.fib (T < 28C)
Pathophysiology…
CNS– Cerebral metabolism 6% / 1C– Normal autoregulation until 25C– EEG flat at 19C
Renal– Cold diuresis
• Peripheral vasoconstriction
• Failure to reabsorb Na+ and water.
Pathophysiology…
Respiratory– CO2 production 50% at 30C– Decreased RR– ARDS possible
Hematology– Hemostasis and coagulation impaired– Problems with CPB
Mild (> 32C)
• Increase metabolic rate
• Maximum shivering thermogenesis
• Amnesia / dysarthria / ataxia
• Loss of coordination
• Tachycardic, tachypneic
• Normal BP
Moderate (28– 32C)
• Stupor
• No shivering
• Bradycardic / A.fib BP RR
• Pupils dilated (< 30C)
Severe (<28C )
• Coma• No corneal or oculocephalic reflexes BP• V.fib (Maximum risk: 22C)• Apnea• Asystole• Areflexia / fixed pupils• Flat EEG (19C)

Lab findings : ECG
• Woman, 75 y.o
• Found unconscious in her apartment


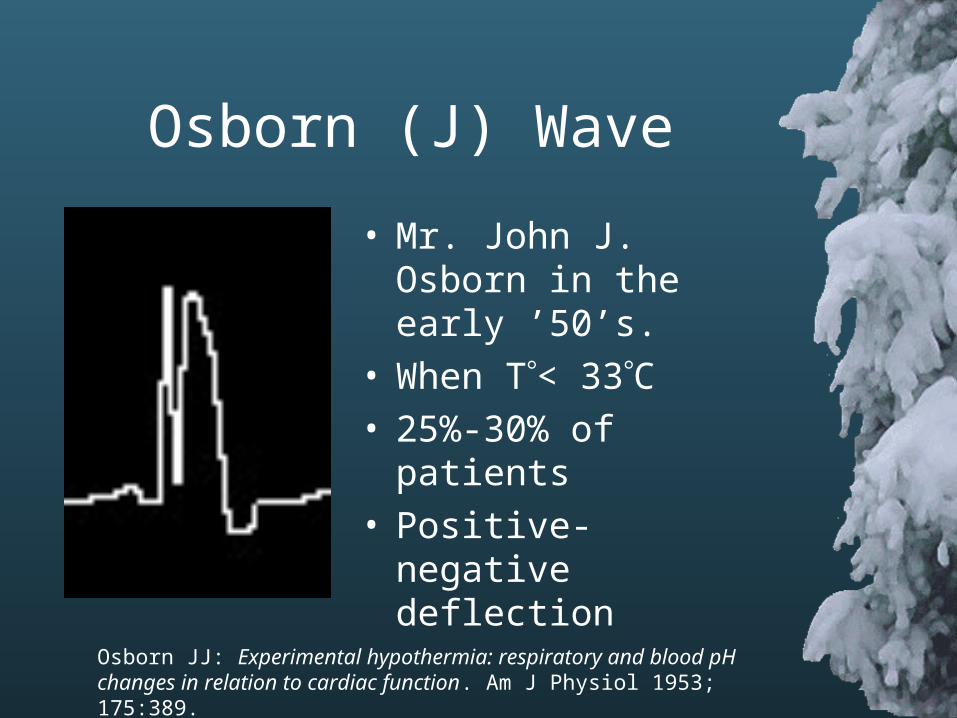
Osborn (J) Wave
• Mr. John J. Osborn in the early ’50’s.
• When T< 33C• 25%-30% of patients• Positive-negative
deflection
Osborn JJ: Experimental hypothermia: respiratory and blood pH changes in relation to cardiac function. Am J Physiol 1953; 175:389.
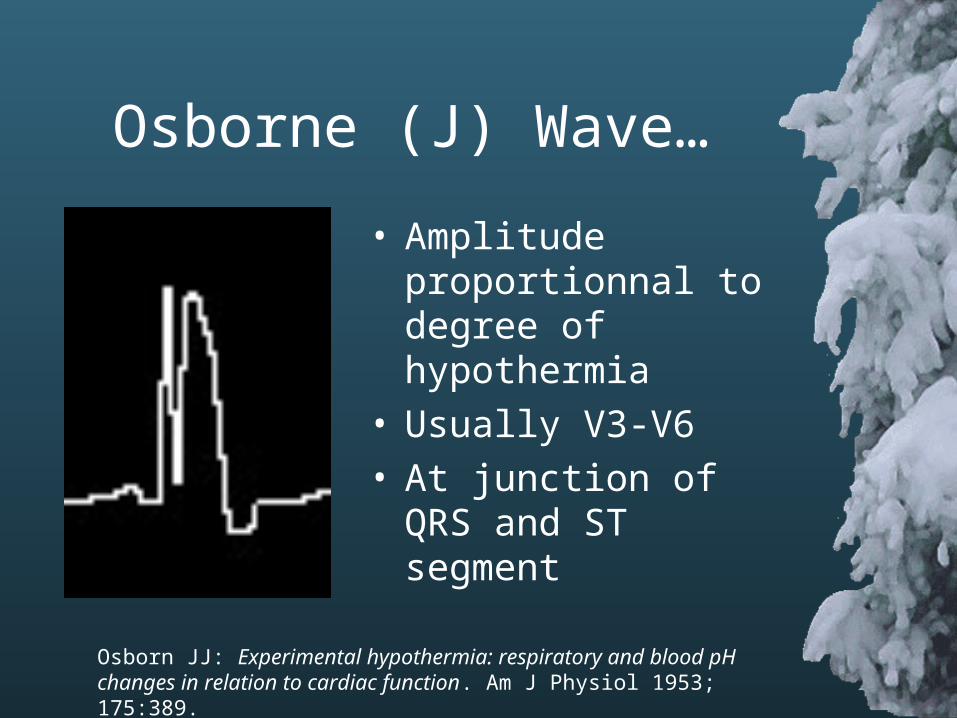
Osborne (J) Wave…
• Amplitude proportionnal to degree of hypothermia
• Usually V3-V6• At junction of QRS and
ST segment
Osborn JJ: Experimental hypothermia: respiratory and blood pH changes in relation to cardiac function. Am J Physiol 1953; 175:389.
ECG in Hypothermia
• Muscle tremors artifacts
• Early changes– Bradycardia– T wave inversion– Prolonged PR, QRS and QT intervals
• A.fib when T < 32C• V.fib when T < 28C
Lab findings : ABG
• Man, 45 y.o,. • Rectal T= 30C. LOC Intubated.• Acid-base status?• Technician asks you if he should warm
the blood before analysis…A) Don’t warm it : 30CB) Warm it to 37CC) heu…(30+37)/2….33.5CD) Both and I’ll pick the best one.
ABG in Hypothermia
• 1st ABG (30C):• pH = 7.5• pCO2 = 27
• 2nd ABG (37C):• pH = 7.4• pCO2 = 40
• Which one do you pick?• Will you try to RR or VT to pCO2 ?• Everything’s perfect, I don’t touch the
ventilator ?• The answer ? ….
The Good One !!!
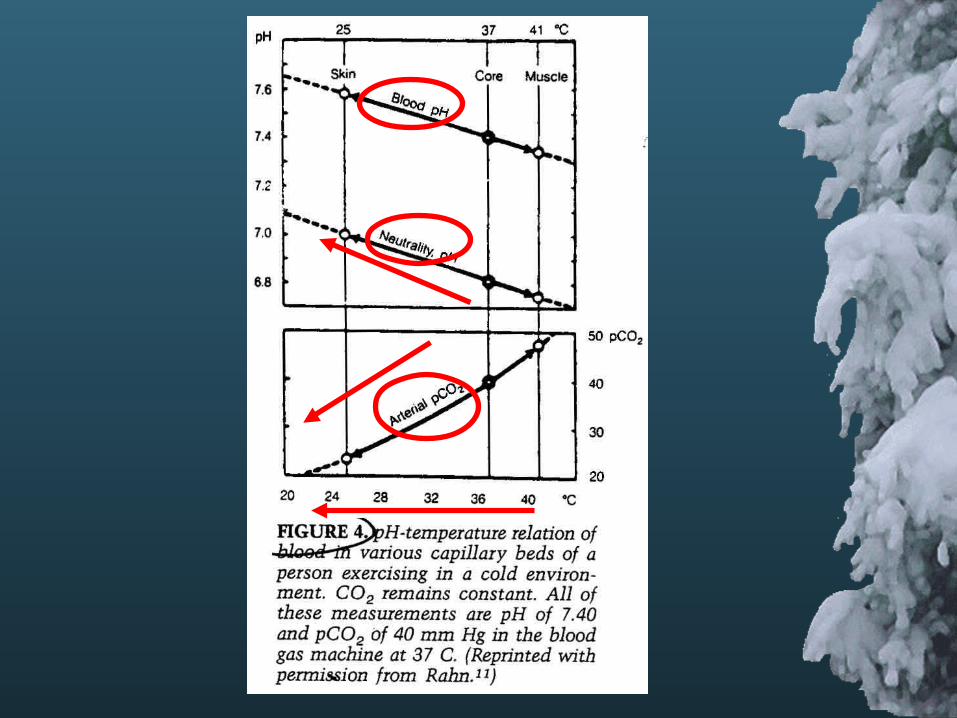
ABG in Hypothermia……the rationale
• pH of water at any given T defines neutrality
• H2O H+ + OH-
• As T , less free H+ and OH- are generated and pH of neutrality .
• As T , CO2 content is the same but pCO2 .
Delaney KA and al. Assessment of Acid-Base Disturbances in Hypothermia and their physiologic consequences. Ann Emerg Med, Jan 1989; 18:72-82.
So…
• 1st ABG (30C):• pH = 7.5
• pCO2 = 27
• 2nd ABG (37C):• pH = 7.4
• pCO2 = 40
ABG in Hypothermia……the rationale
• ABG machines usually warms blood to 37C.
• So use the UNCORRECTED ABG for normal T .
Delaney KA and al. Assessment of Acid-Base Disturbances in Hypothermia and their physiologic consequences. Ann Emerg Med, Jan 1989; 18:72-82.
Rewarming methods :Passive rewarming
• Endogenous heat production– Shivering, metabolic rate, TSH, sympathetic,…
• Involves decreasing heat loss– Remove from cold environnement– Remove wet clothes– Provide blanket
Passive rewarming…
• O2 consumption can > 90%
• CO2 production can by 65%
• Possible anaerobic metabolism Rewarming rate : 0.5C - 2.0C /h
• Method of choice for mild hypothermia
• Adjunt for moderate hypothermia
Rewarming methods :Active external rewarming
• Heat to body surfaces– Heating blankets (fluid filled)– Air blankets– Radiant warmers– Immersion in hot bath– Water bottles / Heating pads
• Less effective than internal rewarming if vasoconstricted +++
Active external rewarming…
• Concern about afterdrop.
• Rewarming rates : 1C – 2.5C / h
• Circulatory problem may be by applying devices to trunk only.
• Very few prospective controlled study comparing methods.
Forced Air Blankets
• ED patients• Moderate to severe hypothermia (< 32C)• Exclusion criteria
– Cardiac arrest
– Hypothalamic lesions
• 16 patients• Randomized to passive insulation with cotton
blanket or forced air blanket @ 43C .
Mark T. Steele and al. Forced Air Speeds Rewarming in Accidental Hypothermia, Ann Emerg Med, April 1996; 27:479-484.
Forced Air Blanket…
• All patients: warm iv fluids @ 38C• Warm O2 (40C)
• End point: T = 35C• Looked at:
– Rates of rewarming– Skin damage by blankets
Mark T. Steele and al. Forced Air Speeds Rewarming in Accidental Hypothermia, Ann Emerg Med, April 1996; 27:479-484.
Forced Air Blanket…
Results
• No afterdrop in both groups
• No skin erythema/damage
• Rewarming rates (p=0.01)– Forced-Air: 2.4C / h– Regular blanket: 1.4C / h
Mark T. Steele and al. Forced Air Speeds Rewarming in Accidental Hypothermia, Ann Emerg Med, April 1996; 27:479-484.
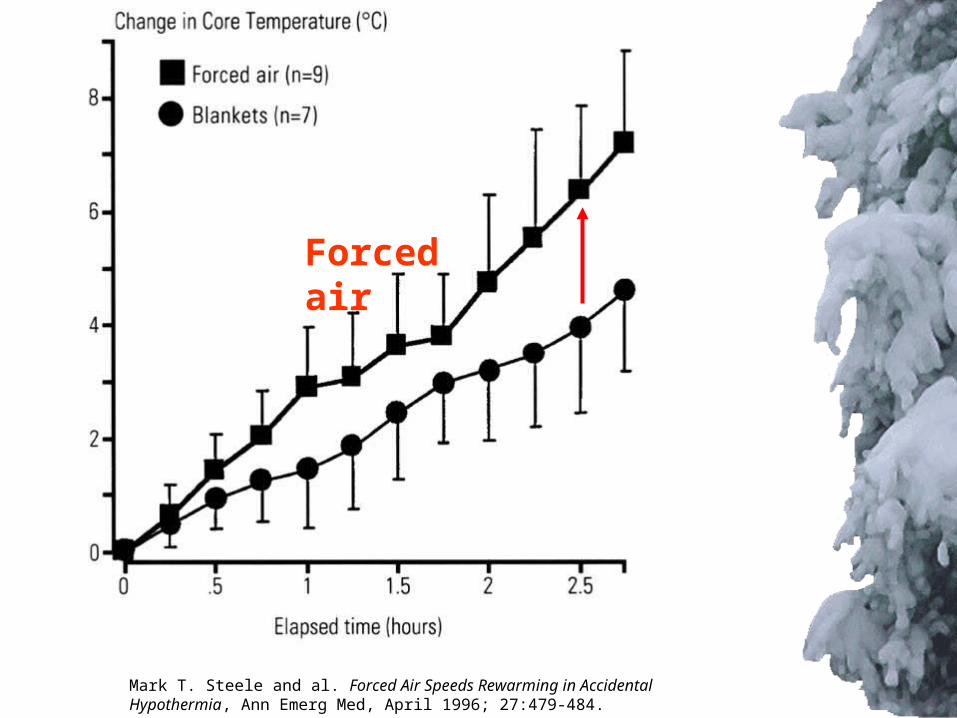
Mark T. Steele and al. Forced Air Speeds Rewarming in Accidental Hypothermia, Ann Emerg Med, April 1996; 27:479-484.
Forced air
Electrical heating blanket
• Carbon fiber-resistive blanket VS Passive rewarming
• 8 patients• Induced-hypothermia (33C)• Skin thermal flux transducer• CO2 concentration production through mask• Compared:
– rates of rewarming– core heat content
Greif R and al, Resistive heating is more effective than metallic-foil insulation in an experimental model of accidental hypothermia: a randomized controlled trial. Ann Emerg Med. April 2000; 35: 337-345.

Electrical heating
Results
• Core heat content >> electrical heating
• Rates 1.5C/h > with electical heating
• No afterdrop both groups
Greif R and al, Resistive heating is more effective than metallic-foil insulation in an experimental model of accidental hypothermia: a randomized controlled trial. Ann Emerg Med. April 2000; 35: 337-345.
Rewarming methods :Active internal (core) rewarming
• Warm iv fluids• Warm, humid oxygen• Peritoneal lavage• Gastric / Esophageal lavage• Bladder / Rectal lavage• Pleural / Mediastinal lavage• Microwaves (Diathermy)• Extracorporeal circulatory rewarming
Warm iv fluids
• Up to 45C shown to be safe
• 65C fluid studied in dogs– Journal of Trauma 1993 (8 dogs)– American Journal of Surgery 1996 (10 dogs)– Through IVC – Safe. No Complications– 2.9C/h compared to 1.25C/h (J Trauma)– 3.7C/h compared to 1.75C/h (Am J Surg)
Warm iv fluids…
• Saline…Not RL• Long tubulure = lost of heat
• Can use microwave for saline (No D5W)– Annals of EM, 1984 and 1985
– 1L of NS to 39C : 2 minutes at high power.
• No microwave rewarming for PRBC– Hemolysis
– Hemoglobinuria
– Transfusion reaction
Warm, humidified O2
• 42C-46C• Prevent heat loss
• Negligible heat gain
• Very important in management of hypothermic patient:– Up to 30% of heat production lost
through airway.
Gastric/Oesophageal/ Bladder/Rectal lavage
• Not shown to be better than external rewarming.
• Limited surface area
• Limited heat exchange
• Limited utility (!)
• Recommend as last resort when other modalities not available.
Peritoneal lavage
• Fluid at 40-45C• Up to 12 L/h• KCl free• Hepatic rewarming• Renal support when dialysate is used• 2C-4C / h• C.I.
– Abdominal trauma– Acute abdomen– Free intra-abdominal air
Peritoneal lavage…
• Almost all studies before 1980• Almost all animal studies• Critical Care Medicine 1988
– 11 dogs– Comparing peritoneal/pleural lavage and
heated aerosol inhalation– Peritoneal and pleural lavage equivalent 6C/h/m2
– Heated inhalation alone : little heat gain

Pleural lavageClosed-thoracic lavage
Continuous thoracic cavity lavage• Two large (38F) ipsilateral chest tubes
• 1: 2nd or 3rd anterior intercostal space, midclavicular.
• 2: 5th or 6th intercostal space, posterior axillary line.
• NS or tap water @ 42C• Rewarms heart + greater vessels
Hall KN and al. Closed thoracic cavity lavage in the treatment of severe hypothermia in human beings. Ann Emerg Med, Feb 1990;19:204-206.

Mediastinal lavage
• Requires certain expertise
• Limited clinical experience
• Case reports
• Internal cardiac massage
• 8C / h
Douglas D. Brunette, Hypothermic cardiac arrest: An 11 year review of ED management and outcome. Am J Emerg Med 2000; 18:418-422.
Extracorporeal blood rewarming techniques
• Hemodialysis
• Arteriovenous rewarming
• Venovenous rewarming
• Cardiopulmonary bypass
Extracorporeal blood rewarming…
- Hemodialysis : renal dysfunction
- AV depends on the pt’s BP
- CPB is the « Gold Standard ».
- CPB improves long term survival and neurologic outcome.- 15 of 32 long term survivors and none
had neurologic deficits (7 years later).
B.H. Walpoth and al. Outcome of survivors of accidental deep hypothermia and circulatory arrest treated with extracorporeal blood warming, N Engl J Med, 1997;337:1500-5

Diathermy
• Ultrasonic waves
• Microwaves
• Short waves
• Few studies
• Radio wave regional hyperthermia: Experience with Tx of tumors.
• Not widespread because of dosages in human poorly defined.
Diathermy…
• Prospective• Radio Wave vs.
Peritoneal lavage• 6 dogs• Rate of rewarming
3x > for Radio wave.
J.D. White and al. Controlled comparison of Radio Wave regional hyperthermia and peritoneal lavage rewarming after immersion hypthermia, J Trauma, 1985; (25)10: 989-993.

The Afterdrop Phenomenon• Continued fall in deep core T during
the initial period of rewarming.• First described by James Currie in 1798• Theory of Burton and Edholm (1955):
– Attributed to peripheral vasodilatation– Return of cold blood to central circulation– Cooling of myocardium
• Accepted theory until mid ’80’s
Burton, A.C., and O.G. Edholm. Man in Cold Environment. London: Arnold, 1955, p.216.
Paul Webb,An alternative explanation.
J. Appl. Physiol. 1986
• Fall of T during active rewarming:– Up to 2C– 10 – 30 min
• Used calorimeter, rectal, esophageal and tympanic probes.
• Heat loss calculation
Webb, Paul. Afterdrop of body temperature during rewarming: an alternative explanation. J.Appl.Physiol. 60(2): 385-390, 1986.
2 mecanisms for afterdrop
• Convection mecanism– Return of cold blood from periphery– Minimal is any contribution
• Conduction mecanism– Thermal gradient principal– Heat flow principal
Webb, Paul. Afterdrop of body temperature during rewarming: an alternative explanation. J.Appl.Physiol. 60(2): 385-390, 1986.
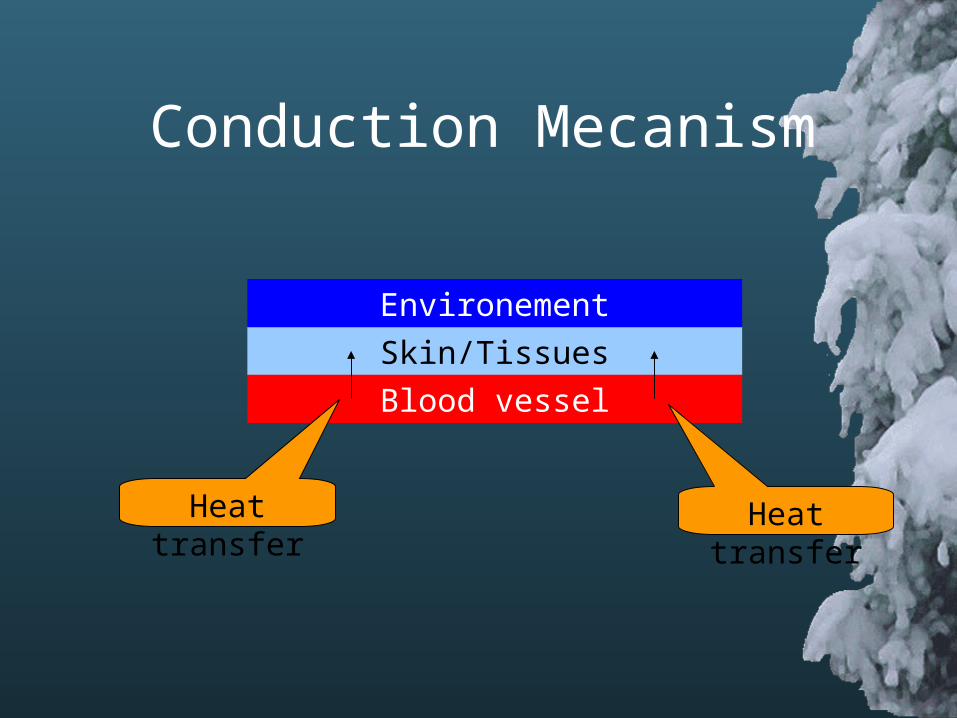
Skin/Tissues
Blood vessel
Environement
Heat transfer
Conduction Mecanism
Heat transfer

Afterdrop: an alternative explanation
• Active external rewarming increase threat of further cooling of the heart…as much as thought before.
• Correlated by many other papers
•Savard, G.K., K.E. Cooper, W.L. Veale, and T.J. Malkinson. Peripheral blood flow during rewarming from mild hypothermia in humans. J. Appl. Physiol. 58(1): 4-13, 1985.
•Romet, Tiit T. Mechanism of afterdrop after cold water immersion. J.Appl.Physiol. 65(4): 1535-1538, 1988.
The Alcatraz/San Francisco Swim Study
• San Francisco Bay…contest…
• Swims from Alcatraz Island to shore
• No wetsuits or protective clothing
• Water T = 12C (53F)
• Outside : T = 10C• 3 Km
• 11 subjects for study
• 23 y.o to 70 y.o (!)
• Measured T after contest.Thomas J. Nuckton and al. Hypothermia and afterdrop following open water swimming: The Alcatrax/San Francisco Swim Study. Am J Emerg Med 2000; 18:703-707.
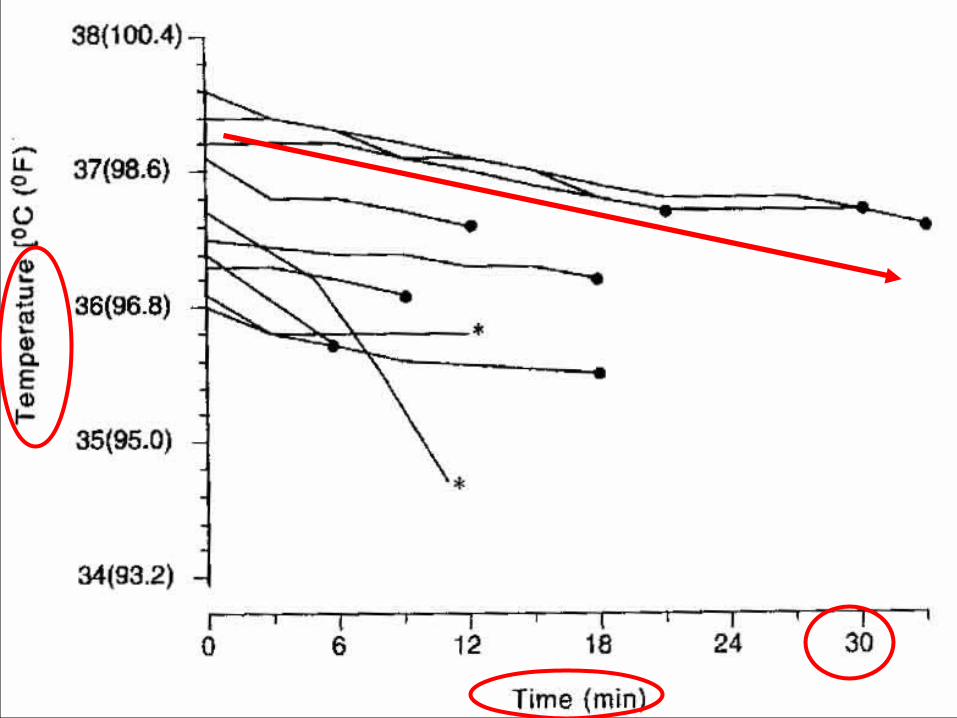
Afterdrop conclusion
• Rectal T lags behing esophageal T and is often > than esophageal and pulmonary T.
• Think about it but you can probably not prevent it.
• Issue with active external rewarming• Other concerns about external rewarming:
– Acidosis
– Hypotension
Management: ED issues
Intubation• General belief it can induce arythmias• Danzl, Multicenter Hypothermia
Survey, Annals Emerg Med, Sept.87.– Data from 13 ED– 428 cases– 117 intubation– NO arythmias
Management: ED issues
Bretylium• Recommended for V.fib in hypothermia• Removed from new ACLS 2000:
availability and limited supply occurrence of side effects
• Still recommend in textbooks (Rosen)• Recommended by US Wilderness
Emergency Medical Services Institute• Based on Dogs studies• Good for prophylaxis only
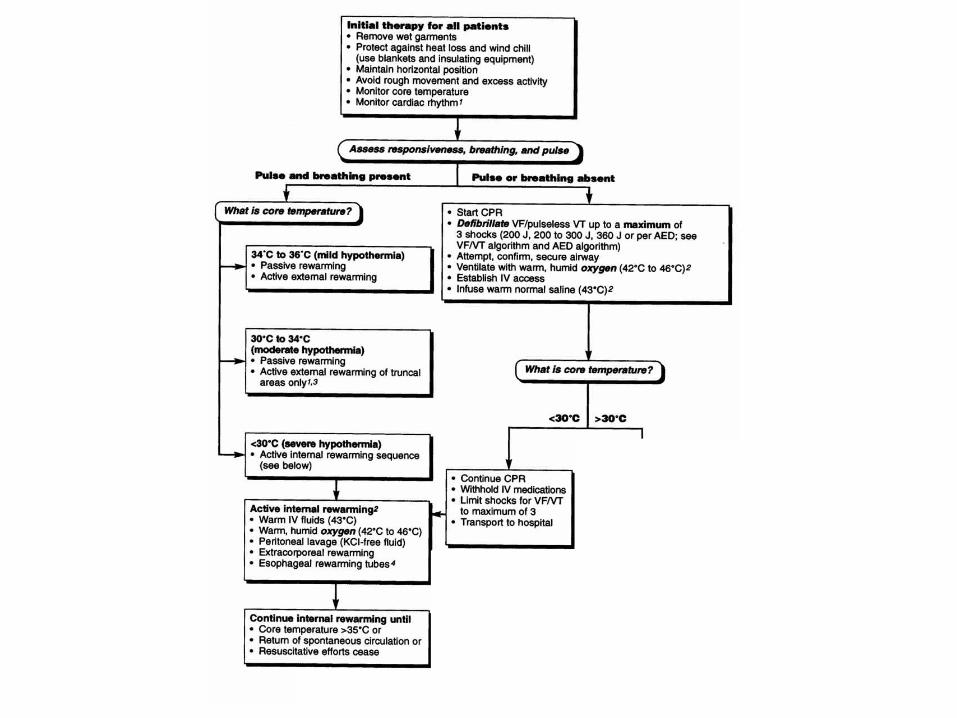
Management: ED issues
Drugs / Shocks
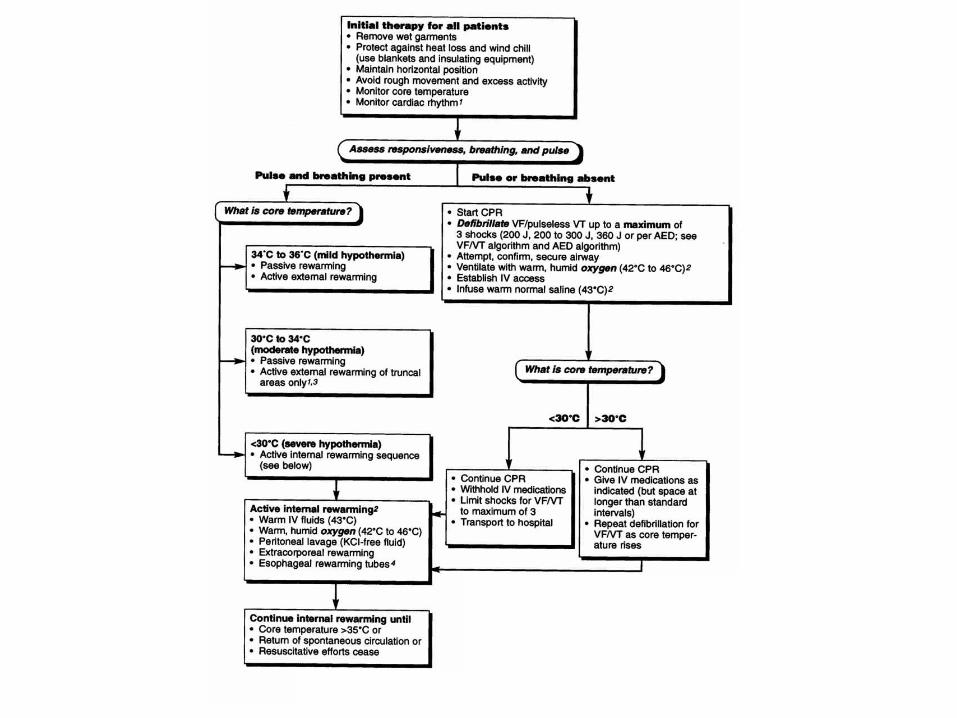
• NO drugs if T < 30C– Not efficacious– Not metabolised
• If > 30C, intervals between doses
• If < 30C and failure of 3 shocks
Management: ED issues
Drugs / Shocks
• NO drugs if T < 30C– Not efficacious– Not metabolised
• If > 30C, intervals between doses
• If < 30C and failure of 3 shocks
Defer subsequent shock + Rx until T > 30C
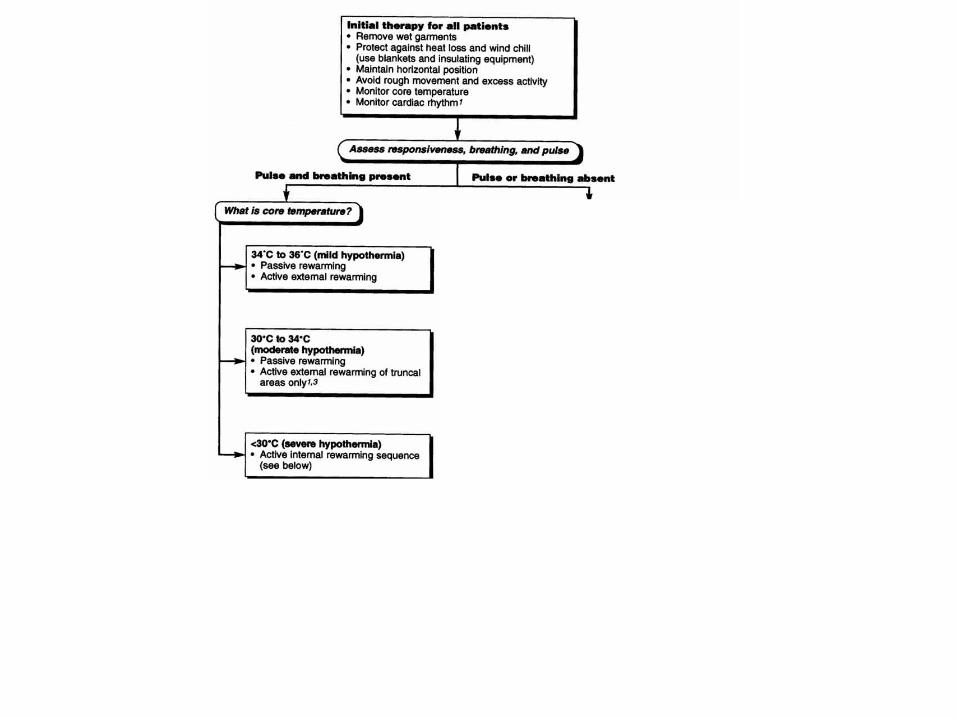
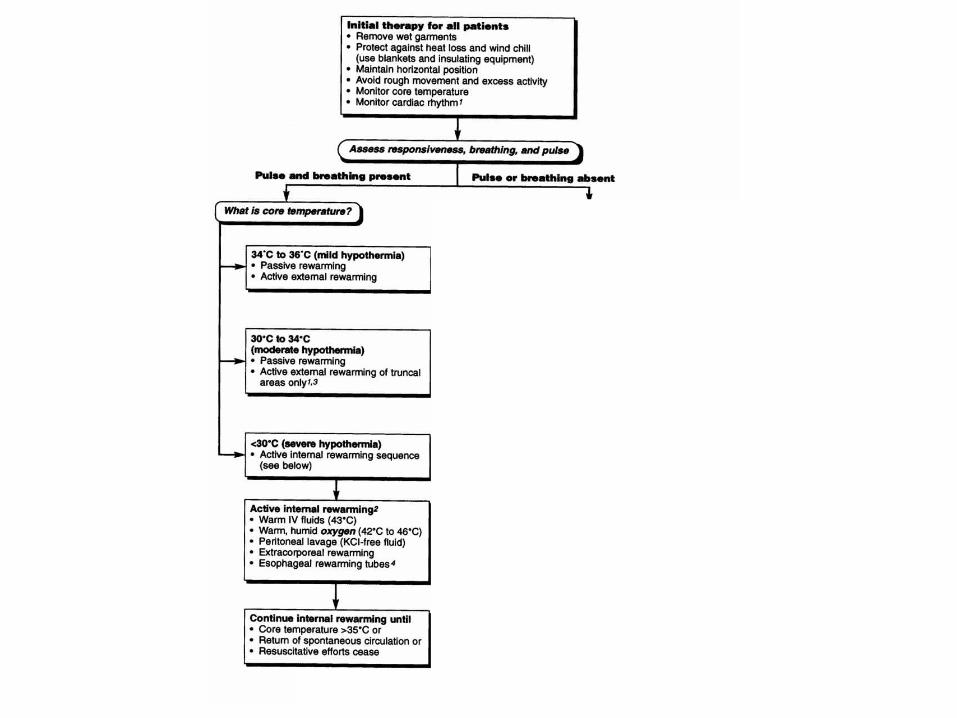
ACLS 2000
The algorithm…



Conclusion
• Hypothermia is rare but treatable
• Good outcome after prolonged arrests
• Include Hypothermia in your Dx
• Include T as a 5th vital sign…
• Call early to organize CPB if available if patient in cardiac arrest
• Prevention is still the best…and…
Play carefully…
From Journal Le Soleil, february 2001
The End