Academic Department of Critical Care Queen Alexandra ...
21
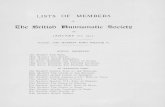
Enteral Feeding Starter Protocol Aim To guide the use of enteral feeding for patients in the first 24-48 hours of admission Scope For all patients starting enteral feeding in DCCQ via nasogastric tube Academic Department of Critical Care Queen Alexandra Hospital Portsmouth Version: 1.5 | Date: 01 Apr 20 | Revision Due: 01 Apr 23 | Authors: S Gavin The use of this guideline is subject to professional judgement and accountability. This guideline has been prepared carefully and in good faith for use within the Department of Critical Care at Queen Alexandra Hospital. No liability can be accepted by Portsmouth Hospitals NHS Trust for any errors, costs or losses arising from the use of this guideline or the information contained herein. Portsmouth Hospitals NHS Trust © 2020 1. Confirm position of feeding tube as per DCCQ Nasogastric Tube Guideline 2. Determine if patient is at high risk of refeeding syndrome as per PHT Refeeding Syndrome Guideline 3. Refer high refeeding risk patients to DCCQ Dietitian and use refeeding target rate below 4. The Dietitian will see all enteral feed patients after 72 hours of admission Bleep 1754 5. For Ivor Lewis patients please feed as per advice in post op note 1. Set target rate of feed based on weight 2 nd Failure Aspirate <250ml 3. Aspirate NGT every 4 hours 2. Start feed Nutrison Protein Plus Multifibre 15ml/hour Replace 150ml Reduce rate of feed by 10ml/hour (Min rate 15ml/hour) Consider prokinetics ABW Target rate Nutrison Protein Plus Multifibre Kcal Protein (g) High Refeeding Risk 15ml/hour x 24 hours 460 23 ≤40kg 33ml/hour x 24 hours 1000 50 40-50kg 40ml/hour x 24 hours 1230 60 ≥60kg 50ml/hour x 24 hours 1536 76 Aspirate >250ml 1 st Failure 3 rd Failure Replace 150ml Maintain current rate of feed (Min rate 15ml/hour) Continue with min rate 15ml/hour If aspirates consistently >250ml consider Post pyloric feeding or TPN Continue to monitor aspirates every 4 hours Return aspirates < 250ml Increase feed by 10ml/hour every 4 hours until target rate achieved
Transcript of Academic Department of Critical Care Queen Alexandra ...

Enteral Feeding Starter Protocol Aim To guide the use of enteral feeding for patients in the first 24-48 hours of admissionScope For all patients starting enteral feeding in DCCQ via nasogastric tube
Academic Department of Critical CareQueen Alexandra Hospital Portsmouth
Version: 1.5 | Date: 01 Apr 20 | Revision Due: 01 Apr 23 | Authors: S GavinThe use of this guideline is subject to professional judgement and accountability. This guideline has been prepared carefully and in good faith for use within the Department of Critical Care at Queen Alexandra Hospital. No liability can be accepted by Portsmouth Hospitals NHS Trust for any errors, costs or losses arising from the use of this guideline or the information contained herein. Portsmouth Hospitals NHS Trust © 2020
1. Confirm position of feeding tube as per DCCQ Nasogastric Tube Guideline 2. Determine if patient is at high risk of refeeding syndrome as per PHT Refeeding Syndrome Guideline3. Refer high refeeding risk patients to DCCQ Dietitian and use refeeding target rate below4. The Dietitian will see all enteral feed patients after 72 hours of admission Bleep 17545. For Ivor Lewis patients please feed as per advice in post op note
1. Set target rate of feed based on weight
2nd Failure
Aspirate <250ml
3. Aspirate NGT every 4 hours
2. Start feed Nutrison Protein Plus Multifibre 15ml/hour
Replace 150ml
Reduce rate of feed by 10ml/hour
(Min rate 15ml/hour)
Consider prokinetics
ABW Target rate Nutrison Protein Plus Multifibre Kcal Protein (g)
High Refeeding Risk 15ml/hour x 24 hours 460 23
≤40kg 33ml/hour x 24 hours 1000 50
40-50kg 40ml/hour x 24 hours 1230 60
≥60kg 50ml/hour x 24 hours 1536 76
Aspirate >250ml
1st Failure 3rd Failure
Replace 150ml
Maintain current rate of feed
(Min rate 15ml/hour)
Continue with min rate 15ml/hour
If aspirates consistently >250ml consider Post pyloric
feeding or TPN
Continue to monitor aspirates every 4 hours
Return aspirates < 250mlIncrease feed by
10ml/hour every 4 hours until target rate achieved

Parenteral (TPN) Feeding Starter Protocol Aim To guide the commencement of TPN in the evenings and weekendsScope For all patients starting TPN feeding in DCCQ in the evenings and weekends
Academic Department of Critical CareQueen Alexandra Hospital Portsmouth
Preparation:
1. Set target rate of feed based on weight
3. Increase rate by 30ml/hour every 24 hours until target rate achieved
2. Start feed Triomel A2 30ml/hour x 24 hours
Bags must not hang >48 hours
Please complete yellow TPN sticker with start time and maximum
hanging time (i.e. 48 hours after start time)
Monitor blood glucose closely
Patient specific TPN must be ordered Mon-Fri
Bespoke TPN must be ordered before 10am Mon-Thurs
Version: 1.5 | Date: 01 Apr 20 | Revision Due: 01 Apr 23 | Authors: S GavinThe use of this guideline is subject to professional judgement and accountability. This guideline has been prepared carefully and in good faith for use within the Department of Critical Care at Queen Alexandra Hospital. No liability can be accepted by Portsmouth Hospitals NHS Trust for any errors, costs or losses arising from the use of this guideline or the information contained herein. Portsmouth Hospitals NHS Trust © 2020
Consider starting parenteral nutrition:Within 24-48hrs (full PN) if:• the enteral route is inaccessible/non-functioning
and the patient is malnourished; or• the enteral route is likely to remain
inaccessible/non-functioning >5 days.
Within 3-7 days (supplementary PN) if:• all methods of enteral feeding have been found
unsuccessfulDecisions are on a case-by-case basis and will depend on likely aetiology and risk of malnutrition.
1. Ensure stock bags of TPN Triomel A2 in DCCQ fridge and dedicated central access lumen available2. Determine if patient is at high risk of refeeding syndrome as per PHT Refeeding Syndrome Guideline3. Refer high refeeding risk patients to DCCQ Dietitian and use refeeding target rate below4. The Dietitian will see all TPN patients Mon-Fri 8:30-16:30 Bleep 1754
Actual Body Weight Target rate Triomel A2 (stock bags) Kcal Protein (g)
High Refeeding Risk 30ml/hour x 24 hours 504 18
≤40kg 63ml/hour x 24 hours 1050 38
40-60kg 74ml/hour x 24 hours 1250 45
≥60kg 90ml/hour x 24 hours 1512 55

Volume Based Feeding ProtocolAim To guide the use of volume based feeding in DCCQScope For all patients that the dietitian deems appropriate to receive volume based feeding
Academic Department of Critical CareQueen Alexandra Hospital Portsmouth
Version: 1.5 | Date: 01 Apr 20 | Revision Due: 01 Apr 23 | Authors: S GavinThe use of this guideline is subject to professional judgement and accountability. This guideline has been prepared carefully and in good faith for use within the Department of Critical Care at Queen Alexandra Hospital. No liability can be accepted by Portsmouth Hospitals NHS Trust for any errors, costs or losses arising from the use of this guideline or the information contained herein. Portsmouth Hospitals NHS Trust © 2020
1. Not for use outside of DCCQ 2. Enteral water is not included in volume based feeding and should be given as per medical team3. The maximum rate of feeding is 150ml/hour
1. Dietitian reviews patient and assesses appropriateness for volume based feeding
To prescribe the feed on CIS as ‘Volume Based Feeding Nutrison…’
2. Dietitian sets the target volume of feed to be received in each 24 hour period (midnight-midnight)
Role of the dietitian
To place a Volume Based Feeding magnet on the patients name board
with the volume target
To create task list reminders to recalculate the rate of the feed twice a
day at 6am and 6pm
Role of the nurse
To calculate the rate of the feed using the ‘Volume Based Feeding Calculator’
found under ‘Links’ on CIS
To record all periods off feed on CIS and recalculate the rate of the feed if it
is off for >1 hour
For patients transferring to the ward the feeding regimen must be converted
to rate based feeding by dividing the target volume by 24

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
TABLE OF CONTENTS
1. Introduction
2. Purpose
3. Scope
4. Definitions
5. Duties and Responsibilities
6. Training Requirements
7. Monitoring Compliance with, and the Effectiveness of Procedural Documents
8. References and Associated Documents
Appendix A. Guideline for Food Service at Ward level
Appendix B. Protected Mealtimes Guideline
Appendix C. Red Tray Guideline
Appendix D. Checklist for the Review and Ratification of Procedural Documents and Consultation
and Proposed Implementation Plan
Appendix E. Equality Impact Assessment

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
1. INTRODUCTION
All body builders know that if you don’t use it you lose it and the same applies to muscle in patients. Enforced bed rest (not using muscles) in volunteer studies shows loss of muscle mass, even in the absence of disease, catabolism and a stress response. Calorie loading during enforced bed rest does not prevent muscle loss and produces fat deposition and fatty liver. Critical illness is associated with worse than just bed rest - a catabolic state, stress and immobility, often fuelled by sepsis, inflammation and endotheliopathy. Starvation may exacerbate the situation and reduces immune function and clearly causes morbidity and mortality in the long term. Feeding is an anabolic process and this is intrinsically difficult in the face of gross catabolism and counter-regulatory hormones. So sickness generates anorexia, gut intolerance of food and reduced nutritional intake. This is a physiological response well preserved though time and species to protect us from excess calorie intake during severe illness. Excessive calories and attempts to manipulate the hormonal milieu (e.g. growth hormone) have been studied and increased morbidity and mortality. This seems to represent a physiological clue that less is more and that we should not force calories upon unwilling physiology. So critical illness produces a perfect storm of catabolism, stress, immobility, potential starvation, with loss of muscle & body protein and immunosuppression. Loss of weight and muscle mass is associated with increased mortality. Hence to maintain, or increase muscle mass, we need …
1. Source Control of Catabolism and Stress Response 2. Promotion of Anabolism
• Feeding • Exercise
The catabolic and stress response to sickness is physiological and necessary. We need to aggressively treat the cause to minimise the need for catabolism and stress and minimise their magnitude (not their presence). Weight gain (of muscle, rather than fat or water) and positive nitrogen balance is only possible once the catabolism is controlled and abolished, the patient is fed and muscle mass promoted by exercise. Hence the rationale of the moto-
Quick Reference Guide: 1. Aim to commence feeding within 24-48 hours of admission 2. Initiate feeding as per Enteral/Parenteral Starter Feeding Protocols 3. A patient is at high risk of refeeding syndrome with: ONE OR MORE OF THE FOLLOWING
§ BMI less than 16 kg/m2 § Unintentional weight loss greater than 15% within the last 3–6 months § Little or no nutritional intake for more than 10 days § Low levels of potassium, phosphate or magnesium prior to feeding
TWO OF MORE OF THE FOLLOWING:
§ Unintentional weight loss greater than 10% within the last 3-6 months § Body Mass Index of less than 18.5kg/m2 § Little or no nutritional intake for 6 - 10 days § A history of alcohol abuse, or drugs including insulin, chemotherapy, antacids or
diuretics

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
med and walking ventilated patients – weaning from long term respiratory failure requires respiratory muscle mass and function. Enteral feeding has been the preferred route of nutrition but the CALORIES study suggested PN was not associated with infection, complications or worse mortality. Enteral feed is simpler, physiological and arguably preserves gut anatomy (villi), IgA secretion and immune function, improved motility, blood flow and possibly preservation of existing bacterial flora (microbiota). Starvation and loss of enteral feeding has profound effects on the gut structure (loss of villi) and function (hormonal changes, immune & gut barrier function, microbe content, absorption capacity). Gut intolerance seems to abate with passing of the critical illness storm. Just as resuscitation and preservation of other organ function takes time (the AKI renal hit takes time to resolve), resuscitation and restoration of the function of the gut takes time. So we cannot expect perfect gut nutrition overnight and should not rush to normalise gut function. Hence we have proposed a slow, gentle pathway towards expected gut function & tolerance of feed.
2. PURPOSE
The purpose of this guideline is to provide an evidence-based framework for nutritional support in critically ill patients.
3. SCOPE
This guideline applies to all critical care patients admitted to DCCQ. This guideline is for use in Critical Care only and is subject to professional judgement and accountability. The ability to comply with this guideline is unlikely to be affected by infection outbreak, flu pandemic or any major incident.
4. DEFINITIONS
MUST: Malnutrition universal screening tool MUAC: Mid upper arm circumference NGT: Nasogastric tube NJT: Nasojejunal tube EN: Enteral Nutrition TPN: Total Parenteral Nutrition (sometimes called simply Parenteral Nutrition, PN)
5. DUTIES AND RESPONSIBILITIES
• Implementation of this guideline is the joint responsibility of critical care medical/ nursing staff.
• This guideline is subject to professional judgment and accountability. • Nutritional support is fundamental to clinical care. There may be times at end of life
when nutritional support may become inappropriate, in an agreed decision involving patient and family and the critical care team.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Nutrition Support Nutrition support should be considered in all critical care patients this includes oral, enteral and parenteral nutrition.
Critical Care Dietitian The critical care dietitian is available Monday-Friday 08:30-16:30, 1.0 whole time equivalent (excluding leave time) and can be contacted on bleep 1754. The critical care dietitian will assess and review all:
• enteral feed patients on day 3 of admission • high risk refeeding patients • parenteral nutrition patients • oral nutrition patients who are at high risk of malnutrition
Nutritional screening All patients in critical care require screening for malnutrition risk e.g. MUST (malnutrition universal screening tool) within 24 hours of admission (1).
• This is recorded on CIS • Patients should be weighed weekly during their admission using a weigh bed, mobile
hoist with weighing scales included, chair scales or stand on scales • MUAC (mid upper arm circumference) is an alternative weight measurement and
should be measured and documented on admission to critical care
Oral nutrition Mealtimes should be conducive to eating and appropriate food provided for individuals. All staff should assist patients in choosing an appropriate diet to meet their needs (nutritional, behavioural and cultural). Special menus are available and the housekeeper should be contacted as needed.
Food service should adhere to the guidelines set out for food service at ward level listed in appendix A. Critical care staff change into clean scrubs daily on site and are required to wear patient specific aprons in each bed space. Therefore do not need to wear a blue apron when collecting meals from the service trolley but must wear the patient specific apron when assisting patients with their food.
The critical care department supports the use of protected mealtimes and the use of red trays in assisting patients to eat their meals. See Appendix B and C.
• Patients at low-medium risk of malnutrition:
o Encourage and assist with meals and snacks o Maintain food record charts o Encourage high calorie, high protein menu choices, coded (H) on the menus o Prescribe and offer Fortisip 2kcal drinks once-twice daily if not finishing meals o Refer to the Critical Care Dietitian if poor oral intakes persist
All patients at high risk of malnutrition should be referred to the dietitian.
Fortisip 2kcal is the standard oral nutritional supplement available on critical care. Other supplements are available but will need to be ordered from the housekeeper.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Enteral Nutrition
In critically ill patients the benefits of nutrition support include: reduced disease severity, improved clinical outcomes, improved wound healing, attenuated metabolic responses to injury, maintain gastrointestinal integrity and function, reduced complications and reduced length of stay (12).
Early nutrition is associated with reduced mortality and infectious morbidity in critical illness. Continuous enteral feeding over 24 hours allows for tighter glycaemic control (2). Raised blood glucose levels are a common response to critical illness and sepsis and can contribute to poor clinical outcomes.There are arguments for a nocturnal feeding break to allow physiological gastric pH but DCCQ patients are on gastric protection regimens, so nocturnal acidity will not occur. During transition from enteral to normal nutrition it may be useful to feed at night and encourage daytime hunger, to allow patients to eat during the day.
• Aims of enteral nutrition in critical care:
o To use the enteral route; gastric or jejunal where possible o To initiate feeding within 24-48 hours of the onset of critical illness o To administer enteral feed continuously over 24 hours o Maintain blood glucose 6-10mml/L
• Before feed is started:
o Ensure appropriate feeding tube is in situ (e.g. Enteral Nutricare 12fr) o Confirm position of feeding tube as per guideline Nasogastric Tubes in Critical
Care o Patient should be positioned at 30-45° before enteral feeding unless clinically
prevented
• Refeeding syndrome Refeeding syndrome describes a potentially fatal medical condition that may affect malnourished and/or ill patients in response to an inappropriately high protein-calorie intake (3).
In starvation, energy is initially derived from glycogen stores and later from the catabolism of adipose tissue (body fat stores) and muscle. The onset of nutrition support can cause a switch to carbohydrate metabolism and associated rapid rise in insulin production.
This insulin release leads to increased cellular uptake of glucose, fluid and electrolytes with associated altered plasma availability of electrolytes. Refeeding syndrome can manifest as either metabolic changes (hypokalaemia, hypophosphataemia, hypomagnesaemia, altered glucose metabolism and fluid balance abnormalities) or physiological changes (i.e. arrhythmias, altered level of consciousness, seizures, cardiac or respiratory depression) and potentially death. It is important to recognise the potential problem and treat hypokalaemia, hypomagnesaemia and hypophosphataemia. Whilst it is a real phenomenon, it is overdiagnosed. It is both avoidable and treatable and provided we maintain potassium, magnesium, phosphate levels that fall, there is little evidence that it is a major problem in critical care.
• A patient is at high risk of refeeding syndrome with:
One or more of the following: o BMI less than 16 kg/m2 o unintentional weight loss greater than 15% within the last 3–6 months o little or no nutritional intake for more than 10 days o low levels of potassium, phosphate or magnesium prior to feeding
or

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Two or more of the following: o BMI less than 18.5 kg/m2 o unintentional weight loss greater than 10% within the last 3–6 months o little or no nutritional intake for more than 5 days o a history of alcohol abuse or drugs including insulin, chemotherapy, antacids or
diuretics
• Treatment o Start feeding at 10kcal/kg for 24 hours o Increase feed every 24 hours to build up to full nutritional requirements over 4-7
days o Prescribe and give refeeding vitamins before starting feed and for 10 days after o Monitor electrolytes daily and correct as needed o Continue to increase feed as per plan. Stopping or reducing feed due to electrolyte
changes increases risk of underfeeding and malnutrition
Give vitamins to patients at risk of refeeding syndrome by the most appropriate route … § Orally
o Thiamine 100mg TDS o Vitamin B co-strong - one tablet TDS o Sanatogen A-Z one tablet OD
§ NGT
o Thiamine 100 mg TDS o Forceval soluble one tablet OD o Vigranon B syrup 5 ml TDS
§ IV o Pabrinex one pair, once per day
Gastric residual volumes
Raised gastric residual volumes may be an indication of gastrointestinal intolerance and are a common cause of feed stoppage which can result in underfeeding. It has been estimated that critical care patients receive only 50% of their target energy requirements due to feed stoppages (4). Consider reasons for failure of enteral feed including ileus, obstruction, electrolyte abnormalities (contribute to or cause ileus), opiates, high pressor needs, multi-organ failure. Opiates slow gut function and may prevent adequate enteral feeding. Consider changing to ketamine as an analgesic DCCQ uses a gastric residual volume cut off of > 250ml and feed should not be stopped or the rate reduced for aspirate volumes less than this. Adherence to aspirate checking as per the Enteral Feed Starter Protocol should aim to minimise the amount of feed a patient misses.
Test feed-gut tolerance
o 4 hourly NGT aspirates to measure gastric residual volumes o Gut tolerance =
§ Gastric residual volumes < 250 ml/4 hours § no vomiting or regurgitation § no distention or abdominal pain
Vomiting/regurgitation may occur associated with pharyngeal suctioning. Do not alter feeding regimen after a single episode of vomiting or regurgitation.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Diarrhoea • may occur in ICU patients for a variety of reasons (see diarrhoea guidelines) • medication side effects e.g. metoclopramide, erythromycin, aminophylline, non
steroidal anti-inflammatory drugs, enteral phosphate/ magnesium preparations • medication additives/preservatives • antibiotic related diarrhoea including • infective causes • lactose intolerance • fat malabsorption • specific feed and fibre
Persistent NGT feed intolerance
• Prokinetics o Metoclopramide and Erythromycin should be considered after 2 failed
nasogastric tube aspirates. o Use individually or together as a trial of prokinetic medication. o Do not continue prokinetics if there is no benefit after a 24 hour trial This should
be discussed with the patient’s consultant o Metoclopramide 10 mg IV. Repeat at 4 hours if unsuccessful. Unlikely to work if
fails initial trial. Side effects include extrapyramidal features. o Erythromycin. There are disadvantages including nausea, QT changes on
ECG with potential arrhythmias (especially in presence of other drugs with similar effects e.g. amiodarone), selection of resistant micro-organisms.
o Diarrhoea is a common side effect of the combination of drugs, which settles on withdrawal of drugs.
• Post pyloric feeding
o Nasojejunal tube (NJT) feeding is an effective and safe way to improve gastrointestinal intolerance and continue to use the enteral feeding route
o Nasojejunal tubes require endoscopic placement and may take time to arrange. Early referral should be considered
o When using a dual lumen NJT, the presence of high gastric aspirate volumes does not mean NJT feeding should be reduced. NJT feeding is usually instituted because of gastric stasis and usually small bowel motility is satisfactory
o Flush fine bore tubes and NJTs with water 8 hourly or after administration of drugs to prevent blockage
• Paracetamol test (5)
o If in doubt about efficacy of absorption of EN, consider a paracetamol absorption test.
§ Ensure there is no recent enteral or parenteral paracetamol § Take a baseline paracetamol level § Give paracetamol dose via NGT and send plasma paracetamol levels at
30 and 60 mins § Failure to detect levels of about 10, indicate failure or delayed absorption § Beware repeat testing, as a negative test means paracetamol is sitting in
the gut and may be absorbed later with the second test bolus

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Hypernatraemia
Hypernatraemia is a common issue in critical care patients this is usually as a result of a negative fluid balance or sodium excess from medications or saline intravenous fluids. Low sodium feeds are expensive and less nutritionally complete for critical care patients. Before changing to a low sodium feed first consider;
• Adding NGT water to correct fluid balance • Review medications to reduce sodium content • Discuss with the dietitian
Oesophagectomy patients
Ivor Lewis patients will usually have a surgical jejunostomy feeding tube placed during surgery. The surgical team will provide guidance on when feeding can be commenced with this tube.
• Feeding is usually commenced at 09:00 day 1 post op with water at 30ml/hour x 12 hours followed by Nutrison 30ml/hour x 12 hours
• Patient should be monitored for signs of feed intolerance or any issues with the feeding jejunostomy site
• Feeding rate is increased by 10ml/hour every 12 hours until target rate reached • Feeding rate must not exceed 50ml/hour in this patient group • Once patients are stable and tolerating target rate of Nutrison, feed can then be
changed to Nutrison Protein Plus (max rate 50ml/hour) to meet full requirements • Please ensure these patients are not started on the DCCQ Enteral Feed Starter
Protocol • The dietitian will aim to see all oesophagectomy patients day 1 post op.
Parenteral Nutrition Parenteral nutrition should be considered; Within 24-48hrs (full PN) if:
• the enteral route is inaccessible/non-functioning and the patient is malnourished; or • the enteral route is likely to remain inaccessible/non-functioning >5 days (13)
Within 3-7 days (supplementary PN) if:
• all methods of enteral feeding have been found unsuccessful Decisions are on a case-by-case basis and will depend on likely aetiology and risk of malnutrition All attempts should be made to facilitate enteral feeding with prokinetics, changing feed type for tolerance and NJT feeding (12).
• Out of hours TPN Critical care has the ability to commence out of hours (evenings and weekends) TPN using Triomel A stock bags available in the fridge on the unit and the Parenteral Nutrition Starter Protocol. This facility is not available to the rest of the hospital. TPN stock bags and the Parenteral Nutrition Starter Protocol must not under any circumstances be provided to another ward.
• TPN evidence
o The CALORIES trial (Harvey NEJM 2014) shows enteral feeding and parenteral feeding produce similar results – there was no increase in infection with PN. Hence old studies are flawed with poorly controlled hyperglycaemia and poor infection control precautions.
o PN and EN can be given together, contrary to earlier suggested guidelines.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
o We treat all lines with aseptic technique, so all our central line ports are clean, we do not have dirty ones! We can start TPN on any central line, whether or not it is previously used for other purposes.
o PN bypasses the gut and so is not subject to gut tolerance considerations. The physiological, stressed, catabolic limitation of nutrients may still limit efficacy of PN. Build up PN slowly in just the same way as enteral feeding.
o By bypassing the gut with PN, nutrition is no longer gut-function-limited but is metabolism-limited. The metabolic response to illness strives to minimise calorie intake during the peak stress of catabolism, suggesting we should increment PN similarly slowly as the catabolism subsides with source control. Hence follow a slow trajectory towards full feeding.
o Do not detach and reattach PN lines for the convenience of transfers. This is significant infection control hazard and abruptly stopping PN can lead to hypoglycaemia.
o Ensure any patient being transferred to another ward, has enough PN bags to tide over to attendance of a dietitian, in office hours.
• Access
o TPN must be given through a centrally place line and must have a dedicated lumen to minimise risk of contamination
• Considerations
o TPN bags must not hang for longer than 48 hours should be covered from daylight with a bag to avoid photodegradation of vitamins and minerals
o Once the bag is disconnected it must be discarded and a new bag commenced o Patient specific ordered bags will arrive from pharmacy at approximately 17:30 each
day o Bags should be left at room temperature for 1 hours before use for patient comfort o A limited number of bespoke TPN bags can be ordered Mon-Thur before 10am
• Monitoring
o Blood glucose levels should be monitored twice daily while on TPN o Liver function and electrolyte should be monitored regularly
• Transferring patients to wards on TPN
o Complete the TPN regimen form in the discharge pack o Send enough TPN bags to ward with patient to continue until the next weekday evening
o Ward team to make referral to ward dietitian for TPN review Volume based feeding This method of enteral feeding allows the rate of the feed to be changed in order to ‘catch up’ on any missed feed in each 24 hour period, midnight-midnight. The feeding volume target resets at midnight every night. The dietitian will review the patient and decide who is appropriate for volume based feeding. Volume based feeding will not be commenced without the involvement of the dietitian. Exclusions include:
• At high risk of refeeding syndrome • Aspirates >250ml, not tolerating enteral feed • Receiving TPN • < 72 hours since admission • Not yet established on full enteral feed • Enteral water that is being given in addition to enteral feed is not included in volume based
feeding and must be given as per the medical team

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
• Volume based feeding is not for use outside DCCQ. For patients transferring to the ward please complete the regimen as if the patient will receive the full volume in 24 hours e.g. volume based feeding target is 1500ml then ward should give feed at 63ml/hour
Feed rate must be recalculated if it has been off for > 1 hour. A task list reminder will be added to appear twice per day at 6am and 6pm. At these time points the feed rate should be checked to ensure the volume target will be achieved by midnight. A volume bases feeding calculator is available on CIS. This can be found under ‘Links’ and near the bottom as ‘Volume Based Feeding Calculator’. An example is also available on this link to explain further. Ensure all periods of feed stoppage are recorded on CIS. The maximum rate of feeding is 150ml/hour. Follow usual aspirate protocol until patient is tolerating feed again and refer to the dietitian to review appropriateness of continuing volume based feeding. 6. TRAINING REQUIREMENTS
• All Critical Care staff will be informed of the content of this guideline and how to access it via the Critical Care Guidelines and SOPs intranet page. Some training requirements will be met educational sessions in MDTs and by the new Critical Care dietitian.
7. MONITORING COMPLIANCE WITH, AND THE EFFECTIVENESS OF, PROCEDURAL DOCUMENTS
• This guideline will be reviewed initially at 6 months and thereafter 4 yearly by the DCCQ Guidelines Group.
• Measurement of compliance will be achieved by unit-based audit. Results reviewed will be fed back to members of the senior medical /nursing team and the Critical Care Governance Group.
8. REFERENCES AND ASSOCIATED DOCUMENTATION
1. Malnutrition in hospital outpatients and inpatients: prevalence, concurrent validity and ease of use of MUST for adults. Stratton, Rebecca J, Hackston, Annemarie, Longmore, David, Dixon, Rod. British Journal of Nutrition, 2004; 92:5
2. Association of glycemic control parameters with clinical outcomes inchronic critical illness. Schulman RC, Moshier EL, Rho L, Casey MF, Godbold JH, Mechanick, JI.Endocr Pract. 2014;20(9):884-893.
3. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. Clinical guideline CG32
4. Enteral tube feeding in the intensive care unit: factors impeding adequate delivery. McClave SA, Sexton LK, Spain DA, et al. Crit Care Med. 1999;27(7):1252-1256.
5. A model of gastric emptying using paracetamol absorption in intensive care patients. Tarling et al. Int Care Med 1997;23:256-60.
6. Trial of Route of Early Nutritional Support in Critically Ill Adults. Harvey SE et al. N Engl J Med 2014;371:1673-84.
7. Permissive Underfeeding of Standard Enteral Feeding in Critically Ill Adults. Arabi YM et al for PermiT Trial Group. N Engl J Med 372;252:2398-2408.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
8. Do we need new prokinetics to reduce enteral feeding intolerance during critical illness? Raymond A, van Zanten H. Critical Care 2016;20:294
9. Metabolic response to the stress of critical illness. Preiser J-C, et al. Br J Anaesth 2014;113(3)945-54.
10. Metabolic and nutritional support of critically ill patients: consensus and controversies. Preiser J-C et al. Critical Care 2015;19:35.
11. Nutrition in the Acute Phase of Critical illness. Casaer MP et al. N Engl Med 2014:370:12 12. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult
Critically Ill Patient: McClave SA et al. Society of Critical Care Medicine (SCCM) and American Society of Parenteral and Enteral Nutrition (ASPEN). JPEN 2016;40:159-211
13. ESPEN guideline on clinical nutrition in the intensive care unit; Singer P et al, Clinical Nutrition 2018
14. Volume Based Feeding in the Critically Ill Patient. McClave, S. A., Saad, M. A., Esterle, M. , Anderson, M. , Jotautas, A. E., Franklin, G. A., Heyland, D. K. and Hurt, R. T. Journal of Parenteral and Enteral Nutrition , 2015, 39: 707-712
15. Implementation and evaluation of a volume-based enteral nutrition protocol in the ICU. Holyk, Amanda; Belden, Valerie; Sirimaturos, Michael; Chiles, Kathryn; Fontenot, Nicole; Lista, Annette; Broadway, Mary; Leon, Raul Sanchez. January 2018 - Volume 46 - Issue 1 - p 201
16. Volume based feeding versus rate based feeding in the critically ill: A UK study. Mina Bharal, Sally Morgan, Tariq Husain, Katerina Hilari, Charlie Morawiec, Kirsty Harrison, Paul Bassett and Alison Culkin. Journal of the Intensive Care Society 2019, Vol. 20(4) 299–308

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Appendix A Guidelines for Food Service at Ward Level
This policy applies to all staff (all disciplines, job roles) caring for inpatients within Portsmouth Hospitals Trust Food hygiene regulations are laid down in the NHS executives ‘Hospital Catering Delivery’ and conform to statutory regulations. All staff working in a ward or clinical area involved in provision of any food, drink or dietary supplement will be classed as food handlers Access to ward kitchens: The regeneration kitchen on each ward is an area supervised by Soft FM services and access for ward staff is at the discretion of Soft FM services. The pantry kitchen in ward areas should allow no access to patients or their visitors. Food handling: All staff taking food to a patient should have washed their hands and have clothing protected by a blue plastic apron. Beverage production: Should be undertaken by ward staff when patients have missed routine beverage times or the late night beverage. Hands should be washed and clothing covered by a plastic apron. Special Dietary Products: Should be checked by a trained member of staff, and if the product needs to be decanted, administered in any way then hands should be washed and clothing covered by a plastic apron. Food brought in by patients, visitors and staff: Should be labelled with the name of the recipient and date the food was brought in. Food should be stored in the refrigerator and discarded after 24 hours. Bringing Food Into Hospital is a leaflet which sets out guidelines for patients and their relatives. Only low risk foods (biscuits, sweets) should be kept in the bedside locker. Refrigerators: Refrigerators in the beverage area should be checked DAILY by the nurse in charge for maintenance, temperature, cleanliness and stock rotation. All food dated over 24 hours should be discarded. All open food should be covered and discarded after 24 hours. Long-life foods should be discarded at the sell by date. Temperatures of the refrigerator should be listed on the log sheet and maintained for all staff to see. High temperatures should be reported to ward manager Volunteers: Those helping with food service and assistance in feeding should have received training in food service/hygiene. Rules of hand-washing and clothing covering still apply. Meal Distribution: Soft FM staff will inform ward staff when food is ready for service. This will be at the same time every day. Each ward has a specific time allocated. Soft FM staff will check the temperature of food prior to service and record this temperature. They will have laid trays with cutlery, napkin etc. Food will be served from the trolley in a discrete area of the ward by a member of the patients services team, under the direction of a qualified member of the clinical team. Each patient’s meal request will be provided from the nursing team and the food plated up accordingly. Where possible the food will be given to the patient immediately and the patient will be ready for their meal. Where patients require assistance in feeding foods will be cut up, food delivery etc will be undertaken. No meals should be ‘put by’ for patients who are off the ward or unable to eat their meal at the food service time. Any food not consumed within one hour of meal service should be discarded. Snack bags are provided for patients who miss their meals. If a snack bag is unacceptable (due to texture etc.) the housekeeper will obtain a meal replacement from the catering department. Disposal of waste food will be undertaken by the Soft FM staff. Out of hours waste food should be discarded in a black plastic bag. Food trolleys, beverage trolleys etc should be cleaned by Soft FM staff.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Appendix B
Protected Mealtimes: Guideline
Protected Mealtimes are a period of time over breakfast, lunch and supper when all non-urgent clinical activity stops. All essential and urgent activity will be met. This guideline is for all staff both ward based and those visiting wards. It should be the aim of all nursing, support staff and housekeeping staff to ensure the ward is ready for mealtimes. Core aims: • To encourage anything that supports and assists patients to eat.
• To plan activities to ensure that nursing and support staff are available to assist at mealtimes.
• To ensure that patients eat their meal is the responsibility of the whole healthcare team.
• To discourage anything that interferes with the meal time.
As such each ward area should: • Establish changes in practices e.g. times of ward rounds, visiting times, etc.
• Obtain agreement with all regular ward visitors e.g. allied health professionals, porters, etc., that interruptions will be minimal at mealtimes
• Agree a start date when the ward will observe a protected mealtime policy
• Provide information for patients, relatives, staff and other departments
Patient Area: • Remind visitors and healthcare staff that patients are easily distracted from their meal and find being watched whilst eating off-putting. Those patients where visitors, carers are available at mealtimes they should support the patient in finishing their meal.
• A quiet and relaxed atmosphere should be created by closing the ward entrance doors and the door to the day room. If patients are using the day room to eat their meal then ensure the room is welcoming, clean and tidy.
• Reduce the noise from any unnecessary equipment e.g. cleaning equipment, radio and television.
• Ensure notices are displayed to inform everyone visiting the ward of the protected mealtime policy and the time of the main meals.
• To ensure that patients needs are met, staff should organise themselves at the beginning of the mealtime to establish who will answer patient call buttons, telephones and assist in food service.
• Make sure that the patient is ready to eat, offer the patient the opportunity to use the toilet before eating and washing hands in preparation for eating and remember to repeat the process after meals.
• Make sure that the environment encourages eating, clearing the bed tray to make space for the patient’s meal, removing items to prevent distraction.
• Providing assistance in cutting food, pouring drinks, removing wrappers etc.
• For those patients who require help in eating this should be undertaken by a qualified member of staff.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
• Patients who are eating poorly, who require help in eating, cutting food etc., should have their meals placed on a red tray.
• All staff should make sure that patients are able to consume their meal.
Provision of food: • Housekeeping staff should inform nursing staff when they are ready to serve meals. • Nursing staff should be available at the meal trolley to accept food for individual patients • Use of the red tray should be dictated by nursing staff § Discourage visiting during mealtimes unless visitors are able to help patients eat their meals.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Appendix C Red trays are a means to highlight patients who either need help with managing their diet, or who are not eating well and their total food intake needs to be monitored.
RED TRAY GUIDELINES
Patient admitted/change in condition
↓ Consider if red tray is appropriate?
Food Record Chart Patient unable to feed themselves/reduced ability to eat
Risk of malnutrition (MUST>2)
↓ Patient and relatives informed if patient falls into a high nutritional risk category
↓ Identify those patients requiring a red tray according to ward’s protocol
(For example red square/T on ward notice board)
↓
Nursing staff checks the whiteboard to see who requires a red tray and ticks box on patient selection form
↓
Suitable meal served on red tray
↓
Those with red trays will a) Require assistance with feeding b) Will require monitoring of intake
↓
Check to see if food record chart completed before removing red tray
↓ Red tray status reviewed daily
MUST score <2 Food Record Chart discontinued Patient able to feed themselves
↓
On discharge if still at risk notify dietitians for follow up at home

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Appendix D
Checklist for the Review and Ratification of Procedural Documents and Consultation and Proposed Implementation Plan
To be completed by the author of the document and attached when the document is submitted for ratification: a blank template can be found on the Trust Intranet. Home page -> Policies -> Templates
CHECKLIST FOR REVIEW AND RATIFICATION
TITLE OF DOCUMENT BEING REVIEWED: YES/NO
N/A COMMENTS
1 Title
Is the title clear and unambiguous? Yes
Will it enable easy searching/access/retrieval?? Yes
Is it clear whether the document is a policy, guideline, procedure, protocol or ICP? Yes
2 Introduction
Are reasons for the development of the document clearly stated? Yes
3 Content
Is there a standard front cover? Yes
Is the document in the correct format? Yes
Is the purpose of the document clear? Yes
Is the scope clearly stated? Yes
Does the scope include the paragraph relating to ability to comply, in the event of a infection outbreak, flu pandemic or any major incident?
Yes
Are the definitions clearly explained? Yes
Are the roles and responsibilities clearly explained? Yes
Does it fulfill the requirements of the relevant Risk Management Standard? (see attached compliance statement) Yes
Is it written in clear, unambiguous language? Yes
4 Evidence Base
Is the type of evidence to support the document explicitly identified? Yes
Are key references cited? Yes
Are the references cited in full? Yes
Are associated documents referenced? Yes
5 Approval Route
Does the document identify which committee/group will approve it? Yes DCCQ Clinical Governance Group
6 Process to Monitor Compliance and Effectiveness
Are there measurable standards or KPIs to support the monitoring of compliance with the effectiveness of the document? Yes
7 Review Date
Is the review date identified? Yes
6 Dissemination and Implementation
Is a completed proposed implementation plan attached? Yes
7 Equality and Diversity
Is a completed Equality Impact Assessment attached? Yes

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Appendix D continued
CONSULTATION AND PROPOSED IMPLEMENTATION PLAN Date to ratification committee 08 Nov 2019
Groups /committees / individuals involved in the development and consultation process
DCCQ Guidelines Group Critical Care Governance Group Multidisciplinary staff working in DCCQ
Is training required to support implementation? Yes
If yes, outline plan to deliver training Multidisciplinary teaching via unit based teaching teams, regular teaching sessions on Fridays and bedside teaching from experienced staff
Outline any additional activities to support implementation
Promotion of introduction of guideline via unit based webpage and verbally through presentation at teaching sessions
Individual Approval
If, as the author, you are happy that the document complies with Trust policy, please sign below and send the document, with this paper, the Equality Impact Assessment and NHSLA checklist (if required) to the chair of the committee/group where it will be ratified. To aid distribution all documentation should be sent electronically wherever possible.
Name Sarah Gavin Date 01/04/20
Signature signed electronically
Committee / Group Approval
If the committee/group is happy to ratify this document, would the chair please sign below and send the policy together with this document, the Equality Impact Assessment, and NHSLA checklist (if required) and the relevant section of the minutes to the Trust Policies Officer. To aid distribution all documentation should be sent electronically wherever possible.
Name Dr Nick Tarmey Date 01/04/20
Signature Signed electronically
If answers to any of the above questions is ‘no’, then please do not send it for ratification.

Nutrition in Critical Care Version 1.5 dated 01 Apr 20
Appendix E
Equality Impact Assessment
To be completed by the author of the document and attached when the document is submitted for ratification: a blank template can be found on the Trust Intranet. Home page -> Policies -> Templates Title of document for assessment DCCQ Nutrition Guideline
Date of assessment 0/04/20
Job title of person responsible for assessment Sarah Gavin
Division/Service DCCQ / CHAT CSC
Yes/No Comments Does the document affect one group less or more favorably than another on the basis of:
• Race No
• Gender (including transgender) No
• Religion or belief No
• Sexual orientation, including lesbian, gay and bisexual people
No
• Age (for HR policies only) No
• Disability – learning disabilities, physical disabilities, sensory impairment and mental health problems
No
Does this document affect an individual’s human rights?
No
If you have identified potential discrimination, are the exceptions valid, legal and/or justified?
If the answers to any of the above questions is ‘yes’ you will need to complete a full Equality Impact Assessment (available from the Equality and Diversity website) or amend the policy such that only an disadvantage than can be justified is included. If you require any general advice please contact staff in the Equality and Diversity Department on 02392 288511