[Abstract TPS4666]Trybeca-1: A randomized, phase 3 study ... › wp-content › uploads ›...
1
Asparagine Asparagine actively transported into RBC Asparagine hydrolyzed inside RBC Asparagine degradation products Shielded Asparaginase remains in RBC Prolonged Activity Reduced Toxicity Study Design Acknowledgements: The authors wish to thank the patients and their families, all investigators and site personnel. Additional support was provided by Sabine Kacel. Editorial assistance was provided by Cadence Communications and Research, funded by Erytech Pharma. Corresponding Author: Pascal Hammel, MD, PhD: [email protected] [Abstract TPS4666] Trybeca-1: A randomized, phase 3 study of eryaspase in combination with chemotherapy versus chemotherapy alone as second-line treatment in patients with pancreatic adenocarcinoma (NCT03665441). P.Hammel, MD 1 ; R. Berardi, MD 2 ; GY. Creemers, MD, PhD 3 ; E. Van Cutsem, MD, PhD 4 ; A. Cubillo, MD 5 ; R. Greil, MD 6 ; H. Wasan, MD 7 ; JP. Metges, MD 8 ; M. Noel, MD 9 ; P. Nygren, MD 10 ; P. Österlund, MD 11 ; T. Seufferlein, MD 12 ; T. Macarulla, MD 13 ; A. Gupta, BA 14 ; L. Grummer 14 ; N. Biswas-Baldwin 14 ; R. Kay 15 ; H. Youssoufian, MD 15 ; I. El-Hariry, MD 14 ; M. Hidalgo, MD, PhD 16 1 Hôpital Beaujon, Clichy, France; 2 Azienda Ospedaliero Universitaria Ospedali Riuniti di Ancona-Umberto, Italy; 3 Catharina Hospital Eindhoven, Netherlands; 4 University Hospitals Gasthuisberg / Leuven & KULeuven, Belgium; 5 HM Hospitales, Madrid, Spain; 6 Paracelsus Medical University Salzburg, Salzburg Cancer research Institute-CCCIT, and Cancer Cluster Salzburg, Austria; 7 Hammersmith Hospital, London, UK; 8 Institut de Cancérologie et D'hématologie Du CHRU Brest, France; 9 MedStar Georgetown University Hospital, Washington, DC, USA; 10 Akademiska Sjukhuset I Uppsala, Sweden; 11 Tampereen yliopistollinen sairaala, Finland; 12 Universitätsklinikum Ulm, Germany; 13 Vall D’Hebron University hospital, Vall d´Hebrón Institute of Oncology, Barcelona, Spain; 14 Erytech Pharma, Lyon, France; 15 Consultant to Erytech Pharma, Boston, USA; 16 Weill Cornell Medicine, New York, USA. Study Participants (N = ~500): • Stage III or IV Pancreatic Cancer • One prior therapy in advanced setting • Performance Status of 0/1 • In a recent randomized phase 2 study in patients with advanced PAC whose disease progressed following first-line treatment (NCT02195180), the addition of eryaspase to chemotherapy demonstrated clinically meaningful improvement in median OS (6.0 vs. 4.4 months, respectively), with a 40% risk reduction in death rate. 9 • The safety profile of eryaspase combined with chemotherapy was comparable with the known safety profile for each chemotherapy used, respectively. 9 • These results provided a rationale for initiating this ongoing confirmatory phase 3 pivotal trial (Trybeca-1, NCT03665441). Study Rationale Trybeca-1 Participating Countries • The observed mortality rate of pancreatic cancer in the United States has continued to increase over the past three decades and is predicted to become the third most common cause of cancer-related deaths by 2035 if new screening and treatment options are not implemented. 1 • Pancreatic adenocarcinoma (PAC) is characterized by extensive reprogramming of cellular metabolism, such as constitutive activation of KRAS signaling and utilization of asparagine and glutamine to circumvent the nutrient-poor, hypoxic microenvironment. Perturbation of these pathways through deprivation of glutamine and asparagine results in loss of cell viability. 2 • In vitro studies have demonstrated promising anti-cancer effects for L-asparaginase (ASNase) against human pancreatic tumor cell lines. 3-5 • The role of ASNase as a therapeutic option in solid tumors has been faced with challenges related to its narrow therapeutic index. In a small pilot Phase 2 study, ASNase was given to 10 patients with advanced pancreatic cancer. No efficacy could be demonstrated, but toxicity was significant. 6 • In addition, in Phase 1 study, pegylated ASNase (Oncaspar ® ) was evaluated in combination with gemcitabine in 17 patients with various solid tumors. The study was terminated early due to toxicity and a selected dose for Phase 2 would have needed to be below the expected biologically effective range. Though inconclusive, this study left the possibility that a safer form of ASNase could be therapeutic. 7 • To address this issue, we encapsulated ASNase within red blood cells (RBCs), thereby prolonging the activity and reducing the toxicity of the free enzyme. This form of encapsulated ASNase is the investigational drug product eryaspase. 8 • Eryaspase has been previously shown to be a well-tolerated and an effective chemotherapy partner in patients with acute lymphoblastic leukemia (ALL) and PAC. 8,9 1L Gemcitabine-based Chemotherapy 1L Fluoropyrimidine- based Chemotherapy 2L FOLFIRI/NALIRI +/- eryaspase 2L Gemcitabine/ Abraxane +/- eryaspase 1:1 1:1 • Treat until Disease Progression or Unacceptable Toxicity • Continue to follow up for survival Key Eligibility Criteria • Eighteen (18) years of age or older • Histologically confirmed pancreatic adenocarcinoma (PAC) • Stage III or IV disease • Received only one prior line of systemic chemotherapy with or without targeted agents, immunotherapy, or radiotherapy for treatment of advanced PAC • Radiological evidence of disease progression following most recent prior treatment • ECOG PS of 0 or ECOG PS of 1 and score of ≥80 on Karnofsky Performance Status Scale • Available tumor tissue samples • Adequate organ function • Brain metastasis is allowed, if stable • Life expectancy of >12 weeks Statistical Plan • Patients are stratified based on performance status, choice of chemotherapy, and time since diagnosis of advanced disease • The study assumes a recruitment period of approximately 22 months and a mOS in the control group of 6 months, and the study size will be based on the recruitment of approximately 500 patients • There will be a superiority interim analysis built in the study design, when approximately two thirds of the events have been accrued. The design has a power to detect differences based on the hazard ratio of 0.725 of approximately 90% • An IDMC is established to review safety at regular intervals and to review efficacy data at the planned interim and final analyses. IDMC last reviewed the trial safety data in April 2020 and suggested the trial continue as planned. Treatment Administration • Eryaspase (100 U/kg) will be given every two weeks (on Day 1 and 15 of each 4-week cycle), intravenously (IV) via a standard infusion line over approximately 30 minutes, followed by chemotherapy • Chemotherapy will be one of the following two treatment regimens, according to the previous therapy received: • Gemcitabine (1000 mg/m 2 )/Abraxane ® (125 mg/m 2 ): Days 1, 8, and 15 of each 4-week cycle • Onivyde ® (Onivyde 70 mg/m 2 )/5-FU (2400 mg/m 2 over 46 hours)/leucovorin (400 mg/m 2 ): Days 1 and 15 of each 4-week cycle OR FOLFIRI [irinotecan (180 mg/m 2 ), 5-FU (5-FU 400 mg/m 2 bolus followed by 2400 mg/m 2 infusion over 46 hours), and leucovorin (400 mg/m 2 )]: Days 1 and 15 of each 4-week cycle Primary Objective • Improvement in OS compared to chemotherapy alone Secondary Objectives • To compare progression-free survival (PFS), objective response rate (ORR), duration of response (DoR), and the disease control rate (DCR) between treatment arms • To evaluate the safety and tolerability of eryaspase in combination with chemotherapy versus chemotherapy alone • To assess the effect of eryaspase on quality of life (QoL) • To determine the pharmacokinetics and pharmacodynamics of eryaspase • To assess the immunogenicity of eryaspase in terms of induction of anti-asparaginase antibodies and neutralizing antibodies • To evaluate the relationship of clinical outcome with relevant biomarkers and genetic changes present in tumor tissues and blood and/or serum samples Study Progress • This is a global trial that is enrolling patients in several European countries and the United States • Currently over 75% of the planned 500 patients have already been enrolled into the trial • CTA approvals in: US, UK, Spain, Finland, Netherlands, Belgium, France, Italy, Czech Republic, Sweden, Austria, and Germany • If you currently treat patients with advanced pancreatic cancer, you may refer for second-line treatment to the Trybeca-1 investigational center at: [email protected] References 1. Ma J, Jemal A, Fedewa SA, et al. The American Cancer Society 2035 challenge goal on cancer mortality reduction. CA Cancer J Clin. 2019;69(5):351-362. 2. Kawada K, Toda K, Sakai Y. Targeting metabolic reprogramming in KRAS-driven cancers. Int J Clin Oncol. 2017;22(4):651-659. 3. Wu MC, Arimura GK, Yunis AA. Mechanism of sensitivity of cultured pancreatic carcinoma to asparaginase. Int J Cancer. 1978;22(6):728-733. 4. Yunis AA, Arimura GK, Russin DJ. Human pancreatic carcinoma (MIA PaCa-2) in continuous culture: sensitivity to asparaginase. Int J Cancer. 1977;19(1):128-135. 5. Dufour E, Gay F, Aguera K, et al. Pancreatic tumor sensitivity to plasma L-asparagine starvation. Pancreas. 2012;41(6):940-948. 6. Lessner HE, Valenstein S, Kaplan R, DeSimone P, Yunis A. Phase II study of L-asparaginase in the treatment of pancreatic carcinoma. Cancer Treat Rep. 1980;64(12):1359-1361. 7. Borad MJ, Babiker HM, Anthony S, et al. A multicenter, open-label, Phase 1 study evaluating the safety and tolerability of pegaspargase in combination with gemcitabine in advanced metastatic solid tumors and lymphoma. Cancer Invest. 2015;33(5):172-179. 8. El-Hariry I, Aguera K, Hoke F, et al. Pharmacodynamic characterization of eryaspase (L-asparaginase encapsulated in red blood cells) in combination with chemotherapy in a phase 2/3 trial in patients with relapsed acute lymphoblastic leukemia (NCT01518517). Journal of Clinical Oncology. 2018;36(15_suppl):7049-7049. 9. Hammel P, Fabienne P, Mineur L, et al. Erythrocyte-encapsulated asparaginase (eryaspase) combined with chemotherapy in second-line treatment of advanced pancreatic cancer: An open-label, randomized Phase IIb trial. Eur J Cancer. 2019;124:91-101. 0 10 20 30 40 50 60 70 80 90 100 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 Survival probability (%) Time (months) Asparaginase Eryaspase Arm Control Arm Median Overall Survival 6 months 4.4 months Hazard Ratio 0.60, p=0.008 Eryaspase Arm Control Arm Number at Risk Eryaspase Arm 95 83 67 45 29 24 15 11 8 8 4 4 4 1 1 1 1 0 Control Arm 46 35 22 15 8 6 3 0 Eryaspase Mechanism of Action Previous Phase 2 Study Experience in Pancreatic Cancer
Transcript of [Abstract TPS4666]Trybeca-1: A randomized, phase 3 study ... › wp-content › uploads ›...
![Page 1: [Abstract TPS4666]Trybeca-1: A randomized, phase 3 study ... › wp-content › uploads › ASCO_2020... · interim and final analyses. IDMC last reviewed the trial safety data in](https://reader036.fdocuments.in/reader036/viewer/2022070821/5f20a0a9176a8f35ee4ed6bc/html5/thumbnails/1.jpg)
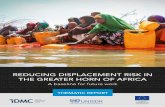
Asparagine
Asparagine actively transported into RBC
Asparagine hydrolyzed inside RBC
Asparagine degradation products
Shielded Asparaginase remains in RBC
Prolonged Activity
Reduced Toxicity
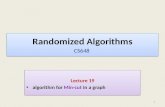
Study Design
Acknowledgements: The authors wish to thank the patients and their families, all investigators and site personnel. Additional support was provided by Sabine Kacel. Editorial assistance was provided by Cadence Communications and Research, funded by Erytech Pharma.
Corresponding Author: Pascal Hammel, MD, PhD: [email protected]
[AbstractTPS4666] Trybeca-1:Arandomized,phase3studyoferyaspaseincombinationwithchemotherapyversuschemotherapyaloneassecond-linetreatmentinpatientswithpancreaticadenocarcinoma (NCT03665441).
P. Hammel, MD1; R. Berardi, MD2; GY. Creemers, MD, PhD3; E. Van Cutsem, MD, PhD4; A. Cubillo, MD5; R. Greil, MD6; H. Wasan, MD7; JP. Metges, MD8; M. Noel, MD9; P. Nygren, MD10;P. Österlund, MD11; T. Seufferlein, MD12; T. Macarulla, MD13; A. Gupta, BA14; L. Grummer14; N. Biswas-Baldwin14; R. Kay15; H. Youssoufian, MD15; I. El-Hariry, MD14; M. Hidalgo, MD, PhD16
1Hôpital Beaujon, Clichy, France; 2Azienda Ospedaliero Universitaria Ospedali Riuniti di Ancona-Umberto, Italy; 3Catharina Hospital Eindhoven, Netherlands; 4University Hospitals Gasthuisberg / Leuven & KULeuven, Belgium; 5HM Hospitales, Madrid, Spain; 6Paracelsus Medical University Salzburg, Salzburg Cancer research Institute-CCCIT, and Cancer Cluster Salzburg, Austria; 7Hammersmith Hospital, London, UK; 8Institut de Cancérologie et D'hématologie Du CHRU Brest, France; 9MedStar Georgetown University Hospital, Washington, DC, USA; 10Akademiska Sjukhuset I Uppsala, Sweden; 11Tampereen yliopistollinen sairaala, Finland; 12Universitätsklinikum Ulm, Germany;
13Vall D’Hebron University hospital, Vall d´Hebrón Institute of Oncology, Barcelona, Spain; 14Erytech Pharma, Lyon, France; 15Consultant to Erytech Pharma, Boston, USA; 16Weill Cornell Medicine, New York, USA.
Study Participants (N = ~500):• Stage III or IV Pancreatic Cancer• One prior therapy in advanced setting• Performance Status of 0/1
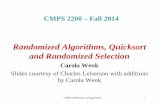
• In a recent randomized phase 2 study in patients with advanced PAC whose disease progressed following first-line treatment (NCT02195180), the addition of eryaspase to chemotherapy demonstrated clinically meaningful improvement in median OS (6.0 vs. 4.4 months, respectively), with a 40% risk reduction in death rate.9
• The safety profile of eryaspase combined with chemotherapy was comparable with the known safety profile for each chemotherapy used, respectively.9
• These results provided a rationale for initiating this ongoing confirmatory phase 3 pivotal trial (Trybeca-1, NCT03665441).
StudyRationale
Trybeca-1 Participating Countries
• The observed mortality rate of pancreatic cancer in the United States has continued to increase over the past three decades and is predicted to become the third most common cause of cancer-related deaths by 2035 if new screening and treatment options are not implemented.1
• Pancreatic adenocarcinoma (PAC) is characterized by extensive reprogramming of cellular metabolism, such as constitutive activation of KRAS signaling and utilization of asparagine and glutamine to circumvent the nutrient-poor, hypoxic microenvironment. Perturbation of these pathways through deprivation of glutamine and asparagine results in loss of cell viability.2
• In vitro studies have demonstrated promising anti-cancer effects for L-asparaginase (ASNase) against human pancreatic tumor cell lines.3-5
• The role of ASNase as a therapeutic option in solid tumors has been faced with challenges related to its narrow therapeutic index. In a small pilot Phase 2 study, ASNase was given to 10 patients with advanced pancreatic cancer. No efficacy could be demonstrated, but toxicity was significant.6
• In addition, in Phase 1 study, pegylated ASNase (Oncaspar®) was evaluated in combination with gemcitabine in 17 patients with various solid tumors. The study was terminated early due to toxicity and a selected dose for Phase 2 would have needed to be below the expected biologically effective range. Though inconclusive, this study left the possibility that a safer form of ASNase could be therapeutic.7
• To address this issue, we encapsulated ASNase within red blood cells (RBCs), thereby prolonging the activity and reducing the toxicity of the free enzyme. This form of encapsulated ASNase is the investigational drug product eryaspase.8
• Eryaspase has been previously shown to be a well-tolerated and an effective chemotherapy partner in patients with acute lymphoblastic leukemia (ALL) and PAC.8,9
1LGemcitabine-basedChemotherapy
1LFluoropyrimidine-basedChemotherapy
2LFOLFIRI/NALIRI+/- eryaspase
2LGemcitabine/Abraxane
+/- eryaspase
1:1
1:1
• TreatuntilDiseaseProgressionorUnacceptableToxicity
• Continuetofollowupforsurvival
Key Eligibility Criteria• Eighteen (18) years of age or older• Histologically confirmed pancreatic adenocarcinoma (PAC)• Stage III or IV disease• Received only one prior line of systemic chemotherapy with or without targeted agents,
immunotherapy, or radiotherapy for treatment of advanced PAC• Radiological evidence of disease progression following most recent prior treatment• ECOG PS of 0 or ECOG PS of 1 and score of ≥80 on Karnofsky Performance Status Scale• Available tumor tissue samples• Adequate organ function
• Brain metastasis is allowed, if stable • Life expectancy of >12 weeks
Statistical Plan• Patients are stratified based on performance status, choice of chemotherapy, and time since diagnosis
of advanced disease• The study assumes a recruitment period of approximately 22 months and a mOS in the control group
of 6 months, and the study size will be based on the recruitment of approximately 500 patients
• There will be a superiority interim analysis built in the study design, when approximately two thirds of the events have been accrued. The design has a power to detect differences based on the hazard ratio of 0.725 of approximately 90%
• An IDMC is established to review safety at regular intervals and to review efficacy data at the planned interim and final analyses. IDMC last reviewed the trial safety data in April 2020 and suggested the trial continue as planned.
Treatment Administration• Eryaspase (100 U/kg) will be given every two weeks (on Day 1 and 15 of each 4-week cycle),
intravenously (IV) via a standard infusion line over approximately 30 minutes, followed by chemotherapy
• Chemotherapy will be one of the following two treatment regimens, according to the previous therapy received:
• Gemcitabine (1000 mg/m2)/Abraxane® (125 mg/m2): Days 1, 8, and 15 of each 4-week cycle
• Onivyde® (Onivyde 70 mg/m2)/5-FU (2400 mg/m2 over 46 hours)/leucovorin (400 mg/m2): Days 1 and 15 of each 4-week cycle OR
FOLFIRI [irinotecan (180 mg/m2), 5-FU (5-FU 400 mg/m2 bolus followed by 2400 mg/m2
infusion over 46 hours), and leucovorin (400 mg/m2)]: Days 1 and 15 of each 4-week cycle
Primary Objective• Improvement in OS compared to chemotherapy alone
Secondary Objectives• To compare progression-free survival (PFS), objective response rate (ORR), duration of response
(DoR), and the disease control rate (DCR) between treatment arms• To evaluate the safety and tolerability of eryaspase in combination with chemotherapy versus
chemotherapy alone• To assess the effect of eryaspase on quality of life (QoL) • To determine the pharmacokinetics and pharmacodynamics of eryaspase
• To assess the immunogenicity of eryaspase in terms of induction of anti-asparaginase antibodies and neutralizing antibodies
• To evaluate the relationship of clinical outcome with relevant biomarkers and genetic changes present in tumor tissues and blood and/or serum samples
Study Progress• This is a global trial that is enrolling patients in several European countries and the United States• Currently over 75% of the planned 500 patients have already been enrolled into the trial• CTA approvals in: US, UK, Spain, Finland, Netherlands, Belgium, France, Italy, Czech Republic,
Sweden, Austria, and Germany
• If you currently treat patients with advanced pancreatic cancer, you may refer for second-line treatment to the Trybeca-1 investigational center at: [email protected]
References1. Ma J, Jemal A, Fedewa SA, et al. The American Cancer Society 2035 challenge goal on cancer mortality
reduction. CA Cancer J Clin. 2019;69(5):351-362.2. Kawada K, Toda K, Sakai Y. Targeting metabolic reprogramming in KRAS-driven cancers. Int J Clin Oncol.
2017;22(4):651-659.3. Wu MC, Arimura GK, Yunis AA. Mechanism of sensitivity of cultured pancreatic carcinoma to asparaginase. Int J
Cancer. 1978;22(6):728-733.4. Yunis AA, Arimura GK, Russin DJ. Human pancreatic carcinoma (MIA PaCa-2) in continuous culture: sensitivity to
asparaginase. Int J Cancer. 1977;19(1):128-135.5. Dufour E, Gay F, Aguera K, et al. Pancreatic tumor sensitivity to plasma L-asparagine starvation. Pancreas.
2012;41(6):940-948.6. Lessner HE, Valenstein S, Kaplan R, DeSimone P, Yunis A. Phase II study of L-asparaginase in the treatment of
pancreatic carcinoma. Cancer Treat Rep. 1980;64(12):1359-1361.7. Borad MJ, Babiker HM, Anthony S, et al. A multicenter, open-label, Phase 1 study evaluating the safety and
tolerability of pegaspargase in combination with gemcitabine in advanced metastatic solid tumors and lymphoma. Cancer Invest. 2015;33(5):172-179.
8. El-Hariry I, Aguera K, Hoke F, et al. Pharmacodynamic characterization of eryaspase (L-asparaginase encapsulated in red blood cells) in combination with chemotherapy in a phase 2/3 trial in patients with relapsed acute lymphoblastic leukemia (NCT01518517). Journal of Clinical Oncology. 2018;36(15_suppl):7049-7049.
9. Hammel P, Fabienne P, Mineur L, et al. Erythrocyte-encapsulated asparaginase (eryaspase) combined with chemotherapy in second-line treatment of advanced pancreatic cancer: An open-label, randomized Phase IIb trial. Eur J Cancer. 2019;124:91-101.
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Surv
ival
pro
babi
lity
(%)
Time (months)
AsparaginaseEryaspaseArm ControlArm
Median Overall Survival 6 months 4.4 months
Hazard Ratio 0.60, p=0.008
Eryaspase Arm
Control Arm
Number at Risk
Eryaspase Arm 95 83 67 45 29 24 15 11 8 8 4 4 4 1 1 1 1 0
Control Arm 46 35 22 15 8 6 3 0
Eryaspase Mechanism of Action
Previous Phase 2 Study Experience in Pancreatic Cancer