Abscess Research Update # 1 - Draft 2 - Abigail McGuire
13
Antibiotic Use in the Treatment of Uncomplicat ed Cutaneous Abscesses Dr . Ab igail McGuire Supervisor: Dr. Mathieu Gatien Methodologist: Dr. Lisa Calder
Transcript of Abscess Research Update # 1 - Draft 2 - Abigail McGuire

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 1/13
Antibiotic Use in the Treatment of
Uncomplicated Cutaneous Abscesses
Dr. Abigail McGuire
Supervisor: Dr. Mathieu GatienMethodologist: Dr. Lisa Calder

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 2/13
Cutaneous Abscesses
• 2% of patient visits to the ED1
• Decision to prescribeantibiotics is variable
– 2012 prospective trial: 79.9%of physicians used both I&Dand antibiotics2
– 2011 retrospective cohortstudy: 88-98% of physiciansprescribed antibiotics3
http://www.daviddarling.info/encyclopedia/A/abscess.html

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 3/13
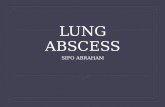
Management of Abscesses:What does the evidence show?
• 90.5 to 95% placebo cure rate – 2007 double-blind RCT of
cephalexin vs. placebo10 – 2010 pediatric double-blind
RCT of TMP-SMX vs. placebo11
• Even in MRSA prevalent areas
TMP-SMX offers no clinicalbenefit above I&D alone13
• Size, induration, erythema notcorrelated to treatment
failure11,12
• Bottom line: No currentevidence for antibiotics inaddition to I&D
h t t p : / / w w w . b
i o m e d c e n t r a
l . c o m / 1 4 7 2 - 6 9 2 0 / 8 / 3 8 / f i g u r e / F 3
h t t p : /
/ n o d b a . i r / d
r . n i l i . k o d a k / 5 0 0 1 6 - 0 - - c e s e c 4 0 . h
t m

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 4/13
Research Project Objectives
• Question: Are our ED physiciansfollowing the best evidence-based practice in the
management of simplecutaneous abscesses?
• Primary Outcome Measure:
Proportion of TOH ED visits for
cutaneous abscesses for whichantibiotics are prescribed
http://www.terryarondberg.com/page/11/

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 5/13
Methods• Design: Retrospective Chart Review
• Setting: TOH EDs – Civic and General
Population: Patients presenting toTOH Emergency Departmentsbetween January 1, 2012 to August31, 2012 who meet the inclusion andexclusion criteria
http://media3.washingtonpost.com/wp-srv/photo/gallery/090417/GAL-09Apr17-1900/media/PHO-09Apr17-158575.jpg

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 6/13
Inclusion Criteria
• All patients dischargedfrom the ED at TOHbetween January 1, 2012
to August 31, 2012 withICD10 diagnosis ofcutaneous abscess – 257 patients
•
Patients ≥ 18 years of age• First presentation
http://www.strategystew.com/2009/04/27/whats-the-point-and-opportunity-of-tweet-chats/

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 7/13
Exclusion Criteria
• HR at Triage ≥ 120 • Temperature at Triage ≥ 38˚C • Systolic BP at Triage ≤ 90 mmHg • Non-cutaneous abscesses (intra-
abdominal, intra-thoracic etc.)
• Post-surgical or post proceduralwound abscesses• Documented human or animal
bite within 30 days prior to visit• Recurrent visit for skin abscess• Breast abscesses and/or mastitis• Genital abscesses• Peri-rectal and peri-anal
abscesses
• Patients already on antibiotics attime of ED visit
• Patients admitted to hospital as aresult of the ED visit for abscess
• Patients with abscessesassociated with arterial or venousinsufficiency ulcers or withunderlying gangrene
• Patients with unusual exposuressuch as underwater injury, heavysoil or farming injuries etc.
• Abscesses around prostheticmaterials
• Abscesses in areas of full-thickness burn wounds

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 8/13
Outcome Measures
• Primary Outcome Measure:
– Proportion of TOH ED visits for the first presentation ofuncomplicated cutaneous abscesses for which antibiotics wereprescribed
• Secondary Outcome Measures:
– Frequency of I &D; frequency of packing – Type, route, duration of antibiotics prescribed – Treatment failure (return to ED within 30 days) – Frequency of obtaining swabs and results of such C&S testing – Frequency of antibiotic prescription in specific patient groups:
• DM, MRSA+, Immunosuppressed, HIV+, IVDU, LTC, homeless, prison inmates
– Qualitative features of abscesses for which antibiotics were given:• Size of abscess (<5cm, ≥5cm), overlying cellulitis, location

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 9/13
Data Collection & Timeline
• Oct 2012: REB approval obtained• 257 patient records retrieved
• Oct 2012: Electronic dataabstraction sheet piloted andadjusted – 50% exclusion rate based on pilot
therefore expected N = 100-128
– Pre-determined values for missing
values on the EMR• Nov 2012: Start data abstraction
• March 2013: End data collection
• April 2013: Clean data & analyze
http://www.revenuexl.com/client-server-based-emr-ehr/

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 10/13
Data Analysis
• Primary outcome:
– Proportion with a 95% CIand p-value of ≤0.05
• Secondary outcomes: – The chi-squared test,
Fisher exact test, or the
student t-testhttp://www.keylogicsolutions.com/onetoonetraining.htm

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 11/13
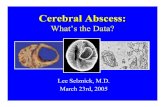
Clinical Importance
• Antibiotics are not benign: – Increasing drug resistance
– Risk of adverse side effects
– Cost for patients
• Need to limit antibioticprescription to cases whereit is absolutely necessary
• Test of whether we are
adhering to evidence-basedpractice at TOH
UptoDate Reproduced with permission from: www.visualdx.com. Copyright Logical Images, Inc
Toxic Epidermal Necrolysis
http://dermatlas.med.jhmi.edu/derm/indexDisplay.cfm?ImageID=1232324374

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 12/13
Questions?
http://deltabiology.com/2011/bacteria-cartoon-comic/cartoon10/

8/12/2019 Abscess Research Update # 1 - Draft 2 - Abigail McGuire
http://slidepdf.com/reader/full/abscess-research-update-1-draft-2-abigail-mcguire 13/13
References1. Rajendran PM, Young DM, Maurer T, Chambers HF, Jacobson MA, Harris HW. Antibiotic Use in The Treatment of Soft Tissue Abscesses: A
Survey of Current Practice. Surgical Infections. 2007;8(2):237-238.
2. May L, Harter K, Yadav K, et al. Practice patterns and management strategies for purulent skin and soft-tissue infections in an urbanacademic ED. The American Journal of Emergency Medicine. 2010;30(2):302-310.
3. Baumann BM, Russo CJ, Pavlik D, et al. Management of Pediatric Skin Abscesses in Pediatric, General Academic and Community EmergencyDepartments. Western Journal of Emergency Medicine. 2011;12(2).
4. Hammond SP, Baden LR. Management of Skin and Soft-Tissue Infection — Polling Results. New England Journal of Medicine. 2008/10/092008;359(15):e20.
5. Merritt C, Mintzer J, Stricker J, Haran JP, Murphy L, Merchant RC. 130 More May Not Be Better: Are Emergency Department CliniciansOverdosing Abscess Patients With Antibiotics? Annals of Emergency Medicine. 2011;58(4, Supplement):S221.
6. Lee MC, Rios A, Aten M, et al. Management and outcome of children with skin and soft tissue abscesses caused by community-acquiredmethicillin-resistant Staphylococcus aureus. Pediatric Infectious Disease Journal.2004;23(2):123-127.
7. Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-Resistant S. aureus Infections among Patients in the Emergency Department. New
England Journal of Medicine. 2006/08/17 2006;355(7):666-674.
8. Paydar KZ, Hansen SL, Charlebois ED, Harris HW, Young DM. Inappropriate antibiotic use in soft tissue infections. Archives of Surgery.
2006;141(9):850-856.
9. Macfie J, Harvey J. The treatment of acute superficial abscesses: A prospective clinical trial. British Journal of Surgery. 1977;64(4):264-266.
10. Rajendran PM, Young D, Maurer T, et al. Randomized, Double-Blind, Placebo-Controlled Trial of Cephalexin for Treatment ofUncomplicated Skin Abscesses in a Population at Risk for Community-Acquired Methicillin-Resistant Staphylococcus aureus Infection.
Antimicrobial Agents and Chemotherapy.2007;51(11):4044-4048.11. Duong M, Markwell S, Peter J, Barenkamp S. Randomized, Controlled Trial of Antibiotics in the Management of Community-Acquired Skin
Abscesses in the Pediatric Patient. Annals of Emergency Medicine. 2010;55(5):401-407.
12. Chen AE, Carroll KC, Diener-West M, et al. Randomized Controlled Trial of Cephalexin Versus Clindamycin for Uncomplicated Pediatric SkinInfections. Pediatrics. 2011;127(3):e573-e580.
13. Schmitz GR, Bruner D, Pitotti R, et al. Randomized Controlled Trial of Trimethoprim-Sulfamethoxazole for Uncomplicated Skin Abscesses inPatients at Risk for Community-Associated Methicillin-Resistant Staphylococcus aureus Infection. Annals of Emergency Medicine.
2010;56(3):283-287.