
Abscess Drainage of Perforated Appendicitis
8
422 AJR:194, February 2010 cases. For reasons that remain unclear, how- ever, a substantial minority (| 10–25%) of patients with perforated acute appendicitis may not respond to initial nonsurgical treat- ment with percutaneous drainage, leading to prolonged hospitalization, repeated percu- taneous procedures, multiple follow-up CT examinations, and in some cases, urgent ap- pendectomy [9, 10]. The results of the few studies [6, 9, 10] conducted in attempts to identify factors predictive of the outcome of percutaneous drainage in patients with per- forated acute appendicitis have been conflict- ing. This lack of agreement generates uncer- tainty in the clinical care of these patients, leading to wide variations in clinical practice among surgeons at different institutions and even among surgeons at the same institution. The purposes of this study were to retrospec- tively investigate the effectiveness and safety Percutaneous Abscess Drainage in Patients With Perforated Acute Appendicitis: Effectiveness, Safety, and Prediction of Outcome Daniele Marin 1 Lisa M. Ho 1 Huiman Barnhart 2 Amy M. Neville 1 Rebekah R. White 3 Erik K. Paulson 1 Marin D, Ho LM, Barnhart H, Neville AM, White RR, Paulson EK 1 Department of Radiology, Duke University Medical Center, Box 3808, Durham, NC 27710. Address correspondence to Erik K. Paulson ([email protected]). 2 Department of Biostatistics and Bioinformatics, Duke University Medical Center, Durham, NC. 3 Department of Surgery, Duke University Medical Center, Durham, NC. AJR 2010; 194:422–429 0361–803X/10/1942–422 © American Roentgen Ray Society A cute appendicitis is a common clinical problem with an incidence of approximately 1 case per 1,000 persons per year [1]. Although immediate appendectomy is the treatment of choice of patients with uncomplicated acute appendicitis, there is no consensus on the opti- mal treatment of the approximately 2–6% of patients whose condition becomes manifest at a later stage with appendiceal perforation with or without appendiceal abscess [2–4]. Imaging-guided percutaneous drainage in combination with broad-spectrum IV an- tibiotics is an effective, minimally invasive treatment of patients with acute appendici- tis complicated by perforation and abscess [5–8]. This approach manages the initial in- flammatory process and is followed by either elective interval appendectomy or conserva- tive nonoperative management in selected Keywords: abdominal abscess, effectiveness, percutaneous drainage, perforated acute appendicitis DOI:10.2214/AJR.09.3098 Received May 26, 2009; accepted after revision July 30, 2009. OBJECTIVE. The purposes of this study were to retrospectively investigate the effective- ness and safety of CT-guided percutaneous drainage in the treatment of patients with acute appendicitis complicated by perforation and to identify CT findings and procedure-related factors predictive of clinical and procedure outcome. From March 2005 through December 2008, 41 con- secutively registered patients (24 men, 17 women; age range, 18–75 years) underwent CT- guided percutaneous drainage for the management of acute appendicitis complicated by per- foration and abscess. Three board-certified radiologists independently reviewed preprocedure CT images. Patients were assigned to one of three risk categories on the basis of the CT find- ings. Success and failure of percutaneous drainage were defined on a per-patient (i.e., clinical outcome) and per-procedure (i.e., technical outcome) basis. Immediate, periprocedure, and delayed complications were recorded. The association between candidate predictive vari- ables, including demographic characteristics, preprocedure CT findings, and procedure-relat- ed factors and clinical or technical outcome was assessed with logistic regression models. Fifty-two CT-guided procedures were performed on 41 patients. Percutane- ous drainage had clinical and technical success rates of 90% (37 of 41 patients, 47 of 52 pro- cedures) with no procedure-related complications. In seven patients (19%) clinical success required repeated drainage procedures. A large, poorly defined periappendiceal abscess and an extraluminal appendicolith on preprocedure CT images were independent predictors of clinical failure of percutaneous drainage. CT-guided percutaneous drainage is both effective and safe in the treatment of patients with acute appendicitis complicated by perforation and abscess. The clinical and technical success rates are high. Marin et al. Abscess Drainage for Acute Appendicitis Gastrointestinal Imaging Original Research
-
Upload
devi-palanivelu -
Category
Documents
-
view
377 -
download
6
Transcript of Abscess Drainage of Perforated Appendicitis
422 AJR:194, February 2010
cases. For reasons that remain unclear, how-ever, a substantial minority ( 10–25%) of patients with perforated acute appendicitis may not respond to initial nonsurgical treat-ment with percutaneous drainage, leading to prolonged hospitalization, repeated percu-taneous procedures, multiple follow-up CT examinations, and in some cases, urgent ap-pendectomy [9, 10]. The results of the few studies [6, 9, 10] conducted in attempts to identify factors predictive of the outcome of percutaneous drainage in patients with per-forated acute appendicitis have been conflict-ing. This lack of agreement generates uncer-tainty in the clinical care of these patients, leading to wide variations in clinical practice among surgeons at different institutions and even among surgeons at the same institution. The purposes of this study were to retrospec-tively investigate the effectiveness and safety
Percutaneous Abscess Drainage in Patients With Perforated Acute Appendicitis: Effectiveness, Safety, and Prediction of Outcome
Daniele Marin1 Lisa M. Ho1 Huiman Barnhart2 Amy M. Neville1 Rebekah R. White3 Erik K. Paulson1
Marin D, Ho LM, Barnhart H, Neville AM, White RR, Paulson EK
1Department of Radiology, Duke University Medical Center, Box 3808, Durham, NC 27710. Address correspondence to Erik K. Paulson ([email protected]).
2Department of Biostatistics and Bioinformatics, Duke University Medical Center, Durham, NC.
3Department of Surgery, Duke University Medical Center, Durham, NC.
AJR 2010; 194:422–429
0361–803X/10/1942–422
© American Roentgen Ray Society
Acute appendicitis is a common clinical problem with an incidence of approximately 1 case per 1,000 persons per year [1]. Although
immediate appendectomy is the treatment of choice of patients with uncomplicated acute appendicitis, there is no consensus on the opti-mal treatment of the approximately 2–6% of patients whose condition becomes manifest at a later stage with appendiceal perforation with or without appendiceal abscess [2–4].
Imaging-guided percutaneous drainage in combination with broad-spectrum IV an-tibiotics is an effective, minimally invasive treatment of patients with acute appendici-tis complicated by perforation and abscess [5–8]. This approach manages the initial in-flammatory process and is followed by either elective interval appendectomy or conserva-tive nonoperative management in selected
Keywords: abdominal abscess, effectiveness, percutaneous drainage, perforated acute appendicitis
DOI:10.2214/AJR.09.3098
Received May 26, 2009; accepted after revision July 30, 2009.
OBJECTIVE. The purposes of this study were to retrospectively investigate the effective-ness and safety of CT-guided percutaneous drainage in the treatment of patients with acute appendicitis complicated by perforation and to identify CT findings and procedure-related factors predictive of clinical and procedure outcome.
From March 2005 through December 2008, 41 con-secutively registered patients (24 men, 17 women; age range, 18–75 years) underwent CT-guided percutaneous drainage for the management of acute appendicitis complicated by per-foration and abscess. Three board-certified radiologists independently reviewed preprocedure CT images. Patients were assigned to one of three risk categories on the basis of the CT find-ings. Success and failure of percutaneous drainage were defined on a per-patient (i.e., clinical outcome) and per-procedure (i.e., technical outcome) basis. Immediate, periprocedure, and delayed complications were recorded. The association between candidate predictive vari-ables, including demographic characteristics, preprocedure CT findings, and procedure-relat-ed factors and clinical or technical outcome was assessed with logistic regression models.
Fifty-two CT-guided procedures were performed on 41 patients. Percutane-ous drainage had clinical and technical success rates of 90% (37 of 41 patients, 47 of 52 pro-cedures) with no procedure-related complications. In seven patients (19%) clinical success required repeated drainage procedures. A large, poorly defined periappendiceal abscess and an extraluminal appendicolith on preprocedure CT images were independent predictors of clinical failure of percutaneous drainage.
CT-guided percutaneous drainage is both effective and safe in the treatment of patients with acute appendicitis complicated by perforation and abscess. The clinical and technical success rates are high.
Marin et al.Abscess Drainage for Acute Appendicitis
Gastrointestinal ImagingOriginal Research
AJR:194, February 2010 423
Abscess Drainage for Acute Appendicitis
of CT-guided percutaneous drainage in the care of patients with acute appendicitis com-plicated by perforation and to identify CT findings and procedure-related factors pre-dictive of clinical and procedure outcome.
Materials and MethodsThis retrospective single-center HIPAA-com-
pliant study was approved by our institutional re-view board. The requirement for informed con-sent was waived.
Patient SelectionWe reviewed the interventional procedure log
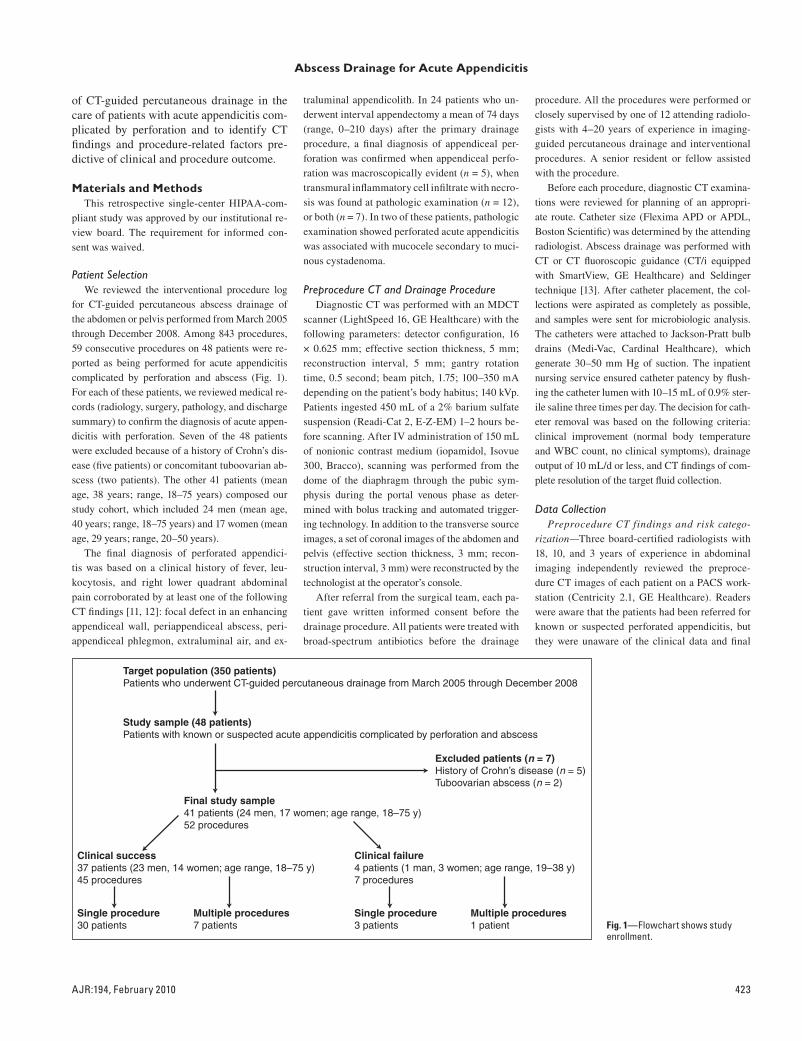
for CT-guided percutaneous abscess drainage of the abdomen or pelvis performed from March 2005 through December 2008. Among 843 procedures, 59 consecutive procedures on 48 patients were re-ported as being performed for acute appendicitis complicated by perforation and abscess (Fig. 1). For each of these patients, we reviewed medical re-cords (radiology, surgery, pathology, and discharge summary) to confirm the diagnosis of acute appen-dicitis with perforation. Seven of the 48 patients were excluded because of a history of Crohn’s dis-ease (five patients) or concomitant tuboovarian ab-scess (two patients). The other 41 patients (mean age, 38 years; range, 18–75 years) composed our study cohort, which included 24 men (mean age, 40 years; range, 18–75 years) and 17 women (mean age, 29 years; range, 20–50 years).
The final diagnosis of perforated appendici-tis was based on a clinical history of fever, leu-kocytosis, and right lower quadrant abdominal pain corroborated by at least one of the following CT findings [11, 12]: focal defect in an enhancing appendiceal wall, periappendiceal abscess, peri-appendiceal phlegmon, extraluminal air, and ex-
traluminal appendicolith. In 24 patients who un-derwent interval appendectomy a mean of 74 days (range, 0–210 days) after the primary drainage procedure, a final diagnosis of appendiceal per-foration was confirmed when appendiceal perfo-ration was macroscopically evident (n = 5), when transmural inflammatory cell infiltrate with necro-sis was found at pathologic examination (n = 12), or both (n = 7). In two of these patients, pathologic examination showed perforated acute appendicitis was associated with mucocele secondary to muci-nous cystadenoma.
Preprocedure CT and Drainage ProcedureDiagnostic CT was performed with an MDCT
scanner (LightSpeed 16, GE Healthcare) with the following parameters: detector configuration, 16 ! 0.625 mm; effective section thickness, 5 mm; reconstruction interval, 5 mm; gantry rotation time, 0.5 second; beam pitch, 1.75; 100–350 mA depending on the patient’s body habitus; 140 kVp. Patients ingested 450 mL of a 2% barium sulfate suspension (Readi-Cat 2, E-Z-EM) 1–2 hours be-fore scanning. After IV administration of 150 mL of nonionic contrast medium (iopamidol, Isovue 300, Bracco), scanning was performed from the dome of the diaphragm through the pubic sym-physis during the portal venous phase as deter-mined with bolus tracking and automated trigger-ing technology. In addition to the transverse source images, a set of coronal images of the abdomen and pelvis (effective section thickness, 3 mm; recon-struction interval, 3 mm) were reconstructed by the technologist at the operator’s console.
After referral from the surgical team, each pa-tient gave written informed consent before the drainage procedure. All patients were treated with broad-spectrum antibiotics before the drainage
procedure. All the procedures were performed or closely supervised by one of 12 attending radiolo-gists with 4–20 years of experience in imaging-guided percutaneous drainage and interventional procedures. A senior resident or fellow assisted with the procedure.
Before each procedure, diagnostic CT examina-tions were reviewed for planning of an appropri-ate route. Catheter size (Flexima APD or APDL, Boston Scientific) was determined by the attending radiologist. Abscess drainage was performed with CT or CT fluoroscopic guidance (CT/i equipped with SmartView, GE Healthcare) and Seldinger technique [13]. After catheter placement, the col-lections were aspirated as completely as possible, and samples were sent for microbiologic analysis. The catheters were attached to Jackson-Pratt bulb drains (Medi-Vac, Cardinal Healthcare), which generate 30–50 mm Hg of suction. The inpatient nursing service ensured catheter patency by flush-ing the catheter lumen with 10–15 mL of 0.9% ster-ile saline three times per day. The decision for cath-eter removal was based on the following criteria: clinical improvement (normal body temperature and WBC count, no clinical symptoms), drainage output of 10 mL/d or less, and CT findings of com-plete resolution of the target fluid collection.
Data CollectionPreprocedure CT findings and risk catego-
rization—Three board-certified radiologists with 18, 10, and 3 years of experience in abdominal imaging independently reviewed the preproce-dure CT images of each patient on a PACS work-station (Centricity 2.1, GE Healthcare). Readers were aware that the patients had been referred for known or suspected perforated appendicitis, but they were unaware of the clinical data and final
Fig. 1—Flowchart shows study enrollment.
424 AJR:194, February 2010
Marin et al.
outcome (see later, Effectiveness). Because we were not attempting to determine the diagnostic accuracy of CT, disagreement was resolved by consensus. Readers assessed contrast-enhanced CT images of each patient for visualization of the appendix and the presence of a periappendiceal abscess (defined as a fluid collection adjacent to the appendix with attenuation of 0–20 HU), peri-appendiceal phlegmon (defined as areas of 20-HU or greater attenuation in the fat tissue surround-ing the appendix), extraluminal gas or appendi-colith, and small-bowel obstruction. If an abscess was identified, readers also documented the size (defined as the single largest transverse diameter) and margins (either well-circumscribed or poorly defined) of the fluid collection.
In an attempt at stratification according to se-verity of inflammatory disease and size and com-plexity of abscess, patients were assigned to one of three risk categories on the basis of the CT find-ings. Based on a classification system described by Jeffrey et al. [6], the categories were 1, periap-
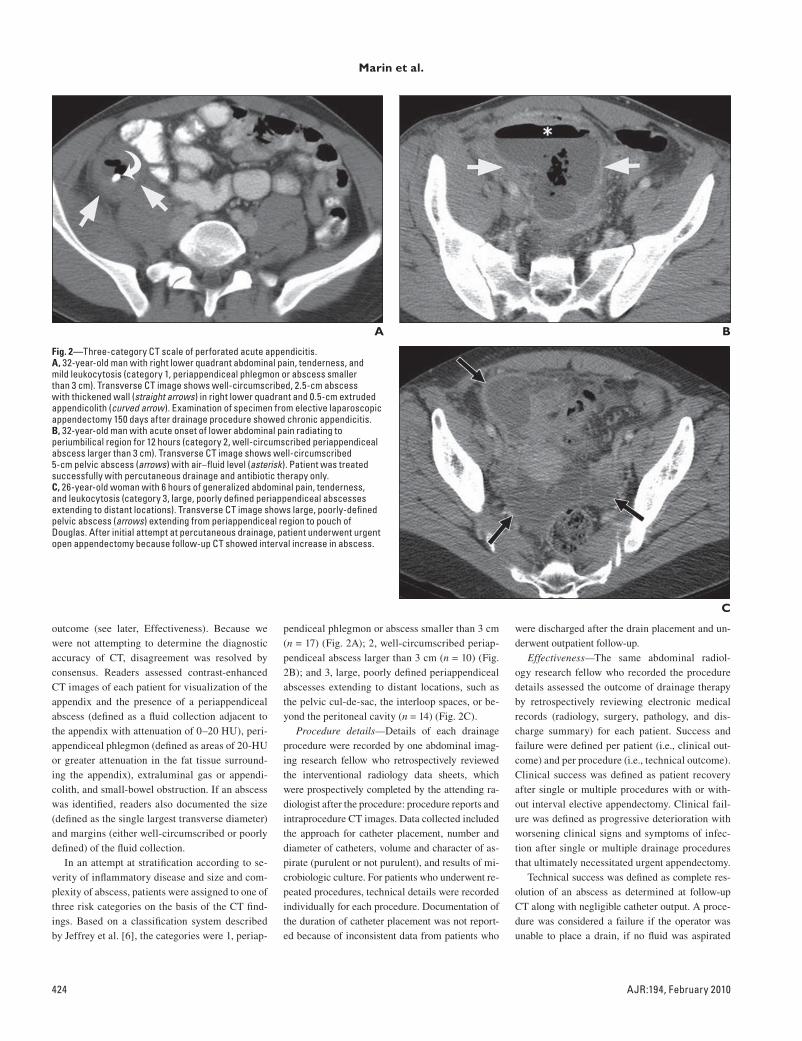
pendiceal phlegmon or abscess smaller than 3 cm (n = 17) (Fig. 2A); 2, well-circumscribed periap-pendiceal abscess larger than 3 cm (n = 10) (Fig. 2B); and 3, large, poorly defined periappendiceal abscesses extending to distant locations, such as the pelvic cul-de-sac, the interloop spaces, or be-yond the peritoneal cavity (n = 14) (Fig. 2C).
Procedure details—Details of each drainage procedure were recorded by one abdominal imag-ing research fellow who retrospectively reviewed the interventional radiology data sheets, which were prospectively completed by the attending ra-diologist after the procedure: procedure reports and intraprocedure CT images. Data collected included the approach for catheter placement, number and diameter of catheters, volume and character of as-pirate (purulent or not purulent), and results of mi-crobiologic culture. For patients who underwent re-peated procedures, technical details were recorded individually for each procedure. Documentation of the duration of catheter placement was not report-ed because of inconsistent data from patients who
were discharged after the drain placement and un-derwent outpatient follow-up.
Effectiveness—The same abdominal radiol-ogy research fellow who recorded the procedure details assessed the outcome of drainage therapy by retrospectively reviewing electronic medical records (radiology, surgery, pathology, and dis-charge summary) for each patient. Success and failure were defined per patient (i.e., clinical out-come) and per procedure (i.e., technical outcome). Clinical success was defined as patient recovery after single or multiple procedures with or with-out interval elective appendectomy. Clinical fail-ure was defined as progressive deterioration with worsening clinical signs and symptoms of infec-tion after single or multiple drainage procedures that ultimately necessitated urgent appendectomy.
Technical success was defined as complete res-olution of an abscess as determined at follow-up CT along with negligible catheter output. A proce-dure was considered a failure if the operator was unable to place a drain, if no fluid was aspirated
A
C
Fig. 2—Three-category CT scale of perforated acute appendicitis.A, 32-year-old man with right lower quadrant abdominal pain, tenderness, and mild leukocytosis (category 1, periappendiceal phlegmon or abscess smaller than 3 cm). Transverse CT image shows well-circumscribed, 2.5-cm abscess with thickened wall (straight arrows) in right lower quadrant and 0.5-cm extruded appendicolith (curved arrow). Examination of specimen from elective laparoscopic appendectomy 150 days after drainage procedure showed chronic appendicitis.B, 32-year-old man with acute onset of lower abdominal pain radiating to periumbilical region for 12 hours (category 2, well-circumscribed periappendiceal abscess larger than 3 cm). Transverse CT image shows well-circumscribed 5-cm pelvic abscess (arrows) with air–fluid level (asterisk). Patient was treated successfully with percutaneous drainage and antibiotic therapy only.C, 26-year-old woman with 6 hours of generalized abdominal pain, tenderness, and leukocytosis (category 3, large, poorly defined periappendiceal abscesses extending to distant locations). Transverse CT image shows large, poorly-defined pelvic abscess (arrows) extending from periappendiceal region to pouch of Douglas. After initial attempt at percutaneous drainage, patient underwent urgent open appendectomy because follow-up CT showed interval increase in abscess.
B
AJR:194, February 2010 425
Abscess Drainage for Acute Appendicitis
after successful catheter placement, or if follow-up imaging more than 1 day after the procedure showed enlargement of the abscess that necessi-tated either secondary drainage or urgent appen-dectomy. Repeated drainage procedures because of development of a new abscess in a different lo-cation were not deemed technical failure and were evaluated separately. Abscesses that became evi-dent after surgical appendectomy were excluded from our analysis. Immediate, periprocedure, and delayed complications were recorded per treatment and were classified in accordance with suggested reporting criteria [14].
Predictive variables—Candidate predictive variables selected included demographic charac-teristics (age and sex), preprocedure CT findings (risk category and presence of extraluminal gas or appendicolith and small-bowel obstruction), and factors related to the first procedure (approach for catheter placement, number and diameter of cath-eters, volume and character of aspirate, and results of microbiologic culture). The association between these variables and clinical or technical outcome was assessed with logistic regression models. Be-
cause of the small number of patients who under-went multiple procedures, only the first procedure was considered in the association analysis. Vari-ables in the univariate analysis with p < 0.20 were entered into multivariate logistic regression analy-sis in a search for independent factors predictive of outcome. Backward-forward and stepwise proce-dures were used for model selection with entry and stay level of 0.10. Because of the exploratory nature of the analyses with a small sample size, p 0.1 was considered to indicate statistical significance. All statistical analyses were performed with statis-tical software (SAS version 9.1.3, SAS Institute).
Preprocedure CT Findings, Risk Category, and Procedure Details
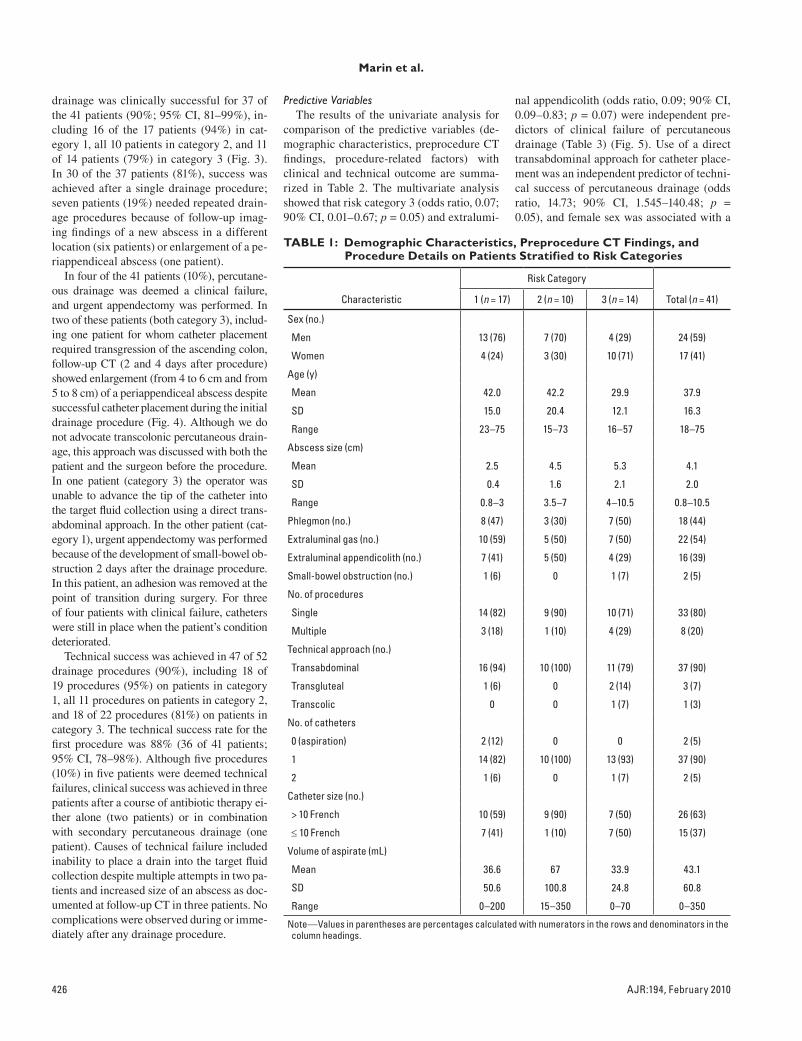
Table 1 summarizes the demographic characteristics, preprocedure CT findings, and procedure details for patients in differ-ent risk categories. In 39 of the 41 patients (95%), perforated acute appendicitis became manifest as a periappendiceal abscess (mean size, 4.1 cm; range, 0.8–10.5 cm) at the initial
CT examination. The abscess was associated with an extraluminal appendicolith in 16 of the patients (39%). In no patient were mul-tiple abscesses present throughout the abdo-men or pelvis. Unequivocal identification of the appendix was possible in 24 of the 41 pa-tients (59%). In 37 of the 41 patients (90%), percutaneous drainage was preferentially performed through a direct transabdominal approach with a single catheter greater than 10-French. Except for two patients in whom percutaneous drainage was performed de-spite the absence of fluid collections at pre-procedure CT, 5–350 mL of fluid was aspirat-ed during the drainage procedure. Aspiration revealed purulent fluid in most of the patients (34 of 41, 83%).
EffectivenessFifty-two CT-guided procedures were per-
formed on 41 patients, including a single pro-cedure on 33 patients, two procedures on six patients, three procedures on one patient, and four procedures on one patient. Percutaneous
A
C
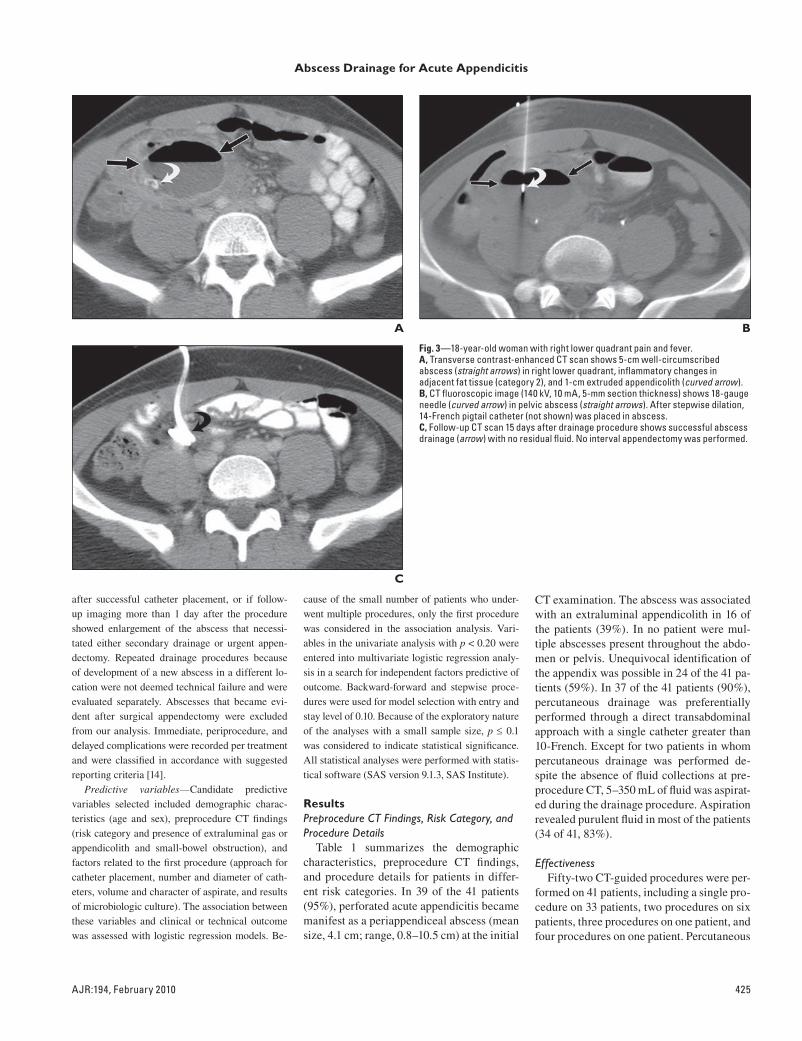
Fig. 3—18-year-old woman with right lower quadrant pain and fever.A, Transverse contrast-enhanced CT scan shows 5-cm well-circumscribed abscess (straight arrows) in right lower quadrant, inflammatory changes in adjacent fat tissue (category 2), and 1-cm extruded appendicolith (curved arrow).B, CT fluoroscopic image (140 kV, 10 mA, 5-mm section thickness) shows 18-gauge needle (curved arrow) in pelvic abscess (straight arrows). After stepwise dilation, 14-French pigtail catheter (not shown) was placed in abscess.C, Follow-up CT scan 15 days after drainage procedure shows successful abscess drainage (arrow) with no residual fluid. No interval appendectomy was performed.
B
426 AJR:194, February 2010
Marin et al.
drainage was clinically successful for 37 of the 41 patients (90%; 95% CI, 81–99%), in-cluding 16 of the 17 patients (94%) in cat-egory 1, all 10 patients in category 2, and 11 of 14 patients (79%) in category 3 (Fig. 3). In 30 of the 37 patients (81%), success was achieved after a single drainage procedure; seven patients (19%) needed repeated drain-age procedures because of follow-up imag-ing findings of a new abscess in a different location (six patients) or enlargement of a pe-riappendiceal abscess (one patient).
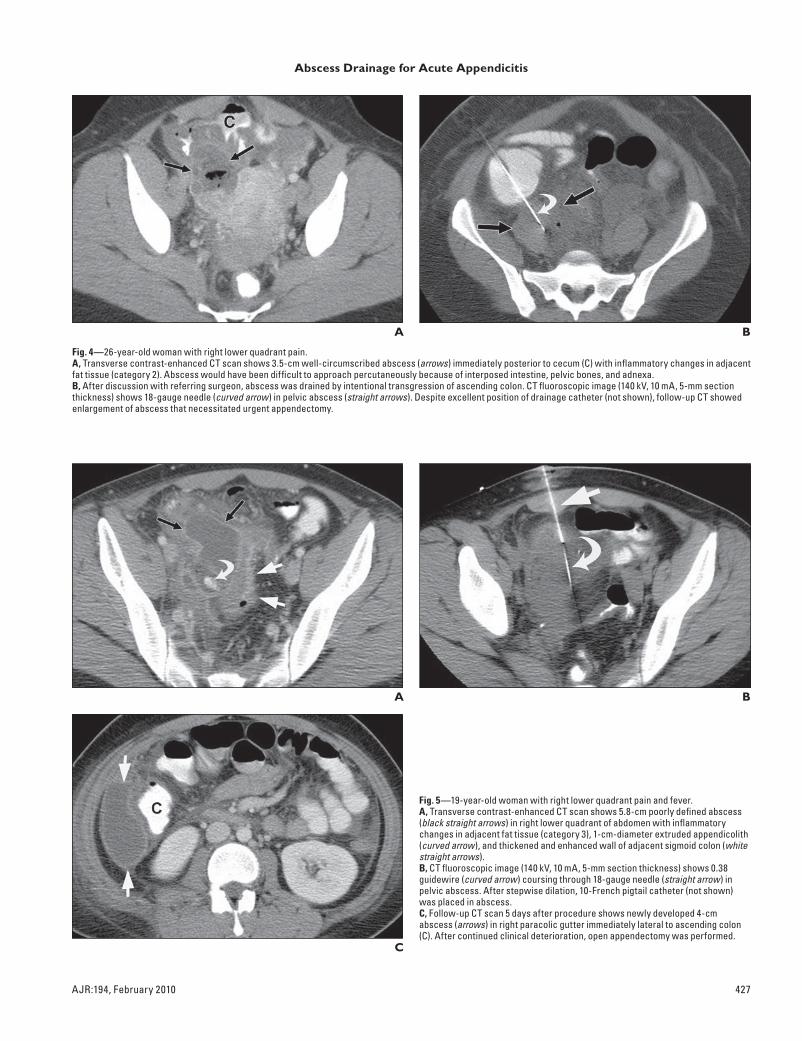
In four of the 41 patients (10%), percutane-ous drainage was deemed a clinical failure, and urgent appendectomy was performed. In two of these patients (both category 3), includ-ing one patient for whom catheter placement required transgression of the ascending colon, follow-up CT (2 and 4 days after procedure) showed enlargement (from 4 to 6 cm and from 5 to 8 cm) of a periappendiceal abscess despite successful catheter placement during the initial drainage procedure (Fig. 4). Although we do not advocate transcolonic percutaneous drain-age, this approach was discussed with both the patient and the surgeon before the procedure. In one patient (category 3) the operator was unable to advance the tip of the catheter into the target fluid collection using a direct trans-abdominal approach. In the other patient (cat-egory 1), urgent appendectomy was performed because of the development of small-bowel ob-struction 2 days after the drainage procedure. In this patient, an adhesion was removed at the point of transition during surgery. For three of four patients with clinical failure, catheters were still in place when the patient’s condition deteriorated.
Technical success was achieved in 47 of 52 drainage procedures (90%), including 18 of 19 procedures (95%) on patients in category 1, all 11 procedures on patients in category 2, and 18 of 22 procedures (81%) on patients in category 3. The technical success rate for the first procedure was 88% (36 of 41 patients; 95% CI, 78–98%). Although five procedures (10%) in five patients were deemed technical failures, clinical success was achieved in three patients after a course of antibiotic therapy ei-ther alone (two patients) or in combination with secondary percutaneous drainage (one patient). Causes of technical failure included inability to place a drain into the target fluid collection despite multiple attempts in two pa-tients and increased size of an abscess as doc-umented at follow-up CT in three patients. No complications were observed during or imme-diately after any drainage procedure.
Predictive VariablesThe results of the univariate analysis for
comparison of the predictive variables (de-mographic characteristics, preprocedure CT findings, procedure-related factors) with clinical and technical outcome are summa-rized in Table 2. The multivariate analysis showed that risk category 3 (odds ratio, 0.07; 90% CI, 0.01–0.67; p = 0.05) and extralumi-
nal appendicolith (odds ratio, 0.09; 90% CI, 0.09–0.83; p = 0.07) were independent pre-dictors of clinical failure of percutaneous drainage (Table 3) (Fig. 5). Use of a direct transabdominal approach for catheter place-ment was an independent predictor of techni-cal success of percutaneous drainage (odds ratio, 14.73; 90% CI, 1.545–140.48; p = 0.05), and female sex was associated with a
Characteristic
Risk Category
Total (n = 41)1 (n = 17) 2 (n = 10) 3 (n = 14)
Sex (no.)
Men 13 (76) 7 (70) 4 (29) 24 (59)
Women 4 (24) 3 (30) 10 (71) 17 (41)
Age (y)
Mean 42.0 42.2 29.9 37.9
SD 15.0 20.4 12.1 16.3
Range 23–75 15–73 16–57 18–75
Abscess size (cm)
Mean 2.5 4.5 5.3 4.1
SD 0.4 1.6 2.1 2.0
Range 0.8–3 3.5–7 4–10.5 0.8–10.5
Phlegmon (no.) 8 (47) 3 (30) 7 (50) 18 (44)
Extraluminal gas (no.) 10 (59) 5 (50) 7 (50) 22 (54)
Extraluminal appendicolith (no.) 7 (41) 5 (50) 4 (29) 16 (39)
Small-bowel obstruction (no.) 1 (6) 0 1 (7) 2 (5)
No. of procedures
Single 14 (82) 9 (90) 10 (71) 33 (80)
Multiple 3 (18) 1 (10) 4 (29) 8 (20)
Technical approach (no.)
Transabdominal 16 (94) 10 (100) 11 (79) 37 (90)
Transgluteal 1 (6) 0 2 (14) 3 (7)
Transcolic 0 0 1 (7) 1 (3)
No. of catheters
0 (aspiration) 2 (12) 0 0 2 (5)
1 14 (82) 10 (100) 13 (93) 37 (90)
2 1 (6) 0 1 (7) 2 (5)
Catheter size (no.)
> 10 French 10 (59) 9 (90) 7 (50) 26 (63)
10 French 7 (41) 1 (10) 7 (50) 15 (37)
Volume of aspirate (mL)
Mean 36.6 67 33.9 43.1
SD 50.6 100.8 24.8 60.8
Range 0–200 15–350 0–70 0–350
Note—Values in parentheses are percentages calculated with numerators in the rows and denominators in the column headings.
AJR:194, February 2010 427
Abscess Drainage for Acute Appendicitis
A
Fig. 4—26-year-old woman with right lower quadrant pain.A, Transverse contrast-enhanced CT scan shows 3.5-cm well-circumscribed abscess (arrows) immediately posterior to cecum (C) with inflammatory changes in adjacent fat tissue (category 2). Abscess would have been difficult to approach percutaneously because of interposed intestine, pelvic bones, and adnexa.B, After discussion with referring surgeon, abscess was drained by intentional transgression of ascending colon. CT fluoroscopic image (140 kV, 10 mA, 5-mm section thickness) shows 18-gauge needle (curved arrow) in pelvic abscess (straight arrows). Despite excellent position of drainage catheter (not shown), follow-up CT showed enlargement of abscess that necessitated urgent appendectomy.
B
A
C
Fig. 5—19-year-old woman with right lower quadrant pain and fever.A, Transverse contrast-enhanced CT scan shows 5.8-cm poorly defined abscess (black straight arrows) in right lower quadrant of abdomen with inflammatory changes in adjacent fat tissue (category 3), 1-cm-diameter extruded appendicolith (curved arrow), and thickened and enhanced wall of adjacent sigmoid colon (white straight arrows).B, CT fluoroscopic image (140 kV, 10 mA, 5-mm section thickness) shows 0.38 guidewire (curved arrow) coursing through 18-gauge needle (straight arrow) in pelvic abscess. After stepwise dilation, 10-French pigtail catheter (not shown) was placed in abscess.C, Follow-up CT scan 5 days after procedure shows newly developed 4-cm abscess (arrows) in right paracolic gutter immediately lateral to ascending colon (C). After continued clinical deterioration, open appendectomy was performed.
B
428 AJR:194, February 2010
Marin et al.
lower rate of technical success (odds ratio, 0.12; 90% CI, 0.01–0.99; p = 0.1) (Table 3).
DiscussionOur results show that percutaneous drain-
age is effective and safe in the treatment of
patients with acute appendicitis complicat-ed by perforation and abscess. Both clinical and technical success rates were 90% (37 of 41 patients and 47 of 52 procedures), and no procedure-related complications occurred. In patients with a well-circumscribed peri-
Technical Outcome
Variables
Clinical Outcome Outcome of First Procedure
Success (n = 37)
Failure (n = 4) p
Success (n = 36)
Failure (n = 5) p
Sex (no.) 0.18 0.09
Men 23 (62) 1 (25) 23 (64) 1 (20)
Women 14 (38) 3 (75) 13 (36) 4 (80)
Age (y) 0.24 0.24
Mean 38.9 28.3 39.1 29.6
SD 16.7 7.9 17.1 3.6
Risk category (no.) 0.11 0.05
1–2 26 (70) 1 (25) 26 (72) 1 (20)
3 11 (30) 3 (75) 10 (28) 4 (80)
Extraluminal gas (no.) 21 (57) 1 (25) 0.25 20 (56) 2 (40) 0.52
Extraluminal appendicolith (no.) 13 (35) 3 (75) 0.16 13 (36) 3 (60) 0.32
Small bowel obstruction (no.) 2 (6) 0 (0) NA 2 (6) 0 (0) NA
No. of procedures 0.77
Single 30 (81) 3 (75)
Multiple 7 (19) 1 (25)
Technical approach (no.) 0.02 0.04
Standard 35 (95) 2 (50) 34 (94) 3 (60)
Nonstandard 2 (5) 2 (50) 2 (6) 2 (40)
No. of catheters (no.) NA NA
1 33 (90) 4 (100) 34 (94) 5 (100)
2 2 (5) 0 (0) 2 (6) 0 (0)
Catheter size (no.) 0.56 0.26
> 10 French 24 (65) 2 (50) 24 (67) 2 (60)
10 French 13 (35) 2 (50) 12 (33) 3 (40)
Volume of aspirate (no.) 0.77 NA
> 50 mL 7 (19) 1 (25) 8 (22) 0 (0)
50 mL 30 (81) 3 (75) 28 (78) 5 (100)
Character of aspirate (no.)a 0.31 NA
Purulent 32 (86) 2 (50) 30 (83) 2 (50)
Nonpurulent 4 (11) 1 (25) 5 (14) 1 (25)
Microbiologic culture (no.)a NA NA
Polymicrobial 34 (92) 3 (75) 34 (90) 3 (75)
Monomicrobial 2 (6) 0 (0) 2 (6) 0 (0)
Note—Values in parentheses are percentages calculated with numerators in the rows and denominators in the column headings. NA = not applicable for data with zero frequency.
aNo fluid was in two patients.
appendiceal abscess (categories 1 and 2), the clinical and technical success rates of percu-taneous drainage increased to 92% and 96%. Our data compare favorably with the results of previously published studies [5–8] and confirm the effectiveness of percutaneous drainage in combination with broad-spec-trum antibiotics in the treatment of patients with acute appendicitis complicated by per-foration and abscess. There is compelling ev-idence that among these patients, immediate appendectomy is associated with substan-tially higher risk of complications, including hemorrhage, fistula formation, wound infec-tion, prolonged ileus, and adhesions [4].
Another clinically important finding of our study is that besides the high clinical suc-cess rate (81%, 30 of 37 patients), which was achieved after a single drainage procedure, percutaneous drainage was clinically success-ful in seven of eight patients (88%) who un-derwent repeated procedures, most commonly because of the development of a new abscess at a location distant from the primary site of infection. These results, which are consistent with the 92% clinical success reported by McCann and colleagues [15] in a study with patients with acute appendicitis complicated by multiple abdominal abscesses, emphasize the importance of secondary drainage in the treatment of patients with perforated acute appendicitis in whom new intraabdominal ab-scesses develop after the first drainage proce-dure. At the same time, our data highlight the need for close clinical and CT follow-up af-ter percutaneous drainage for early detection and prompt management of persistent or new-ly developed abscesses.
In our study, initial nonsurgical manage-ment with percutaneous drainage failed to control the acute inflammatory process in four of 41 patients, resulting in a 10% clinical fail-ure rate. In accordance with results of previous analyses [6, 9], we found that a large, poorly defined periappendiceal abscess (category 3) and extraluminal appendicolith were the two most specific predictors of unfavorable clinical outcome of percutaneous drainage. This find-ing, which remained significant after adjust-ments for other potential prognostic factors, has two important clinical implications. First, it reinforces the current clinical practice of per-forming urgent appendectomy on patients with perforated acute appendicitis that becomes ev-ident at a later stage with more generalized, potentially life-threatening signs and symp-toms of peritoneal infection. Second, it cor-roborates the hypothesis that patients with an

AJR:194, February 2010 429
Abscess Drainage for Acute Appendicitis
extraluminal appendicolith after appendiceal perforation have a poorer prognosis, including increased risk of recurrent abscess and other complications [16]. The presence of an appen-dicolith can act as a nidus for continuous in-fection and abscess formation. This notion jus-tifies the need for elective interval removal of a dropped appendicolith with either surgery or CT-guided percutaneous extraction and stone basket catheters [16, 17].
In our study, percutaneous abscess drainage through a direct transabdominal approach was associated with a significantly higher prob-ability of procedure success. In a minority of patients, however, an alternative approach, in-cluding a transgluteal route in three patients and intentional transgression of the ascending colon in one patient, was necessary because of the presence of deep-seated, less accessible ab-scesses. These approaches were not associated with major periprocedure complications, such as hemorrhage or injury to the sciatic nerve but resulted in both clinical and procedure fail-ure in two of four cases (50%). Although this finding did not reach statistical significance, it needs to be emphasized that many authorities have discouraged transgression of the small or large bowel for drainage of deep-seated ab-scesses [18]. In our patient who needed colonic transgression, the risks of this approach were discussed with both the patient and the refer-ring surgeon before the procedure.
Besides its retrospective nature, potential limitations of our study merit consideration. First, the relatively small sample size probably limited the statistical power to detect associa-tions between CT findings and technique-relat-ed factors and the outcome variables. Second, we restricted our analysis to patients with con-clusive diagnostic criteria for perforated acute appendicitis at CT [11, 12]. This approach might have introduced selection bias because it is possible that some patients with atypical clinical or CT manifestations of perforated acute appendicitis might have been excluded
from the study. In addition, because we includ-ed only patients with perforated acute appen-dicitis who were referred to our interventional radiology service for a percutaneous drainage procedure, we cannot compare the effective-ness of percutaneous drainage with that of oth-er treatments, such as immediate appendecto-my and antibiotic therapy alone. Our results also reflect the experience of a single tertiary referral center with a high volume of percuta-neous drainage procedures. It remains to be determined whether our results can be gener-alized to smaller community hospitals. Final-ly, our work was focused on adults; we believe similar results can be achieved in the treatment of children with perforated appendicitis.
CT-guided percutaneous drainage is both effective and safe in the care of patients with acute appendicitis complicated by perforation and abscess, having clinical and technical success rates of 90%. In patients with prepro-cedure CT findings of large, poorly defined periappendiceal abscesses or extraluminal ap-pendicoliths, percutaneous drainage is associ-ated with a less favorable clinical outcome.
1. National Center for Health Statistics. Ambulatory and inpatient procedures in the United States, 1996. National Center for Health Statistics Series 13, no. 139. Atlanta, GA: National Center for Health Statistics
2. Brown CV, Abrishami M, Muller M, Velmahos GC. Appendiceal abscess: immediate operation or percutaneous drainage? Am Surg 2003; 69:829–832
3. Goh BK, Chui CH, Yap TL, et al. Is early laparo-scopic appendectomy feasible in children with acute appendicitis presenting with an appendiceal mass? A prospective study. J Pediatr Surg 2005; 40:1134–1137
4. Gibeily GJ, Ross MN, Manning DB, Wherry DC, Kao TC. Late-presenting appendicitis: a laparo-scopic approach to a complicated problem. Surg
Endosc 2003; 17:725–729
and Clinical and Technical Outcomes
Variable
Clinical Outcome Outcome of First Procedure
Odds Ratio 90% CI p Odds Ratio 90% CI p
Sex NI 0.12 0.01–0.99 0.10
Risk category (3 vs 1 or 2) 0.07 0.01–0.67 0.05 NI
Extraluminal appendicolith 0.09 0.09–0.83 0.07 NI
Technical approach NI 14.7 1.55–140.48 0.05
Note—NI = not included and not significant at 0.10 level.
5. Jamieson DH, Chait PG, Filler R. Interventional drainage of appendiceal abscesses in children. AJR 1997; 169:1619–1622
6. Jeffrey RB Jr, Federle MP, Tolentino CS. Periap-pendiceal inflammatory masses: CT-directed management and clinical outcome in 70 patients. Radiology 1988; 167:13–16
7. Roach JP, Partrick DA, Bruny JL, Allshouse MJ, Karrer FM, Ziegler MM. Complicated appendici-tis in children: a clear role for drainage and de-layed appendectomy. Am J Surg 2007; 194:769–772
8. Lasson A, Lundagårds J, Lorén I, Nilsson PE. Ap-pendiceal abscesses: primary percutaneous drain-age and selective interval appendicectomy. Eur J
Surg 2002; 168:264–269 9. Aprahamian CJ, Barnhart DC, Bledsoe SE, Vaid
Y, Harmon CM. Failure in the nonoperative man-agement of pediatric ruptured appendicitis: pre-dictors and consequences. J Pediatr Surg 2007; 42:934–938
10. Nadler EP, Reblock KK, Vaughan KG, Meza MP, Ford HR, Gaines BA. Predictors of outcome for children with perforated appendicitis initially treated with non-operative management. Surg
Infect (Larchmt) 2004; 5:349–356 11. Horrow MM, White DS, Horrow JC. Differentia-
tion of perforated from nonperforated appendici-tis at CT. Radiology 2003; 227:46–51
12. Tsuboi M, Takase K, Kaneda I, et al. Perforated and nonperforated appendicitis: defect in enhanc-ing appendiceal wall—depiction with multi-de-tector row CT. Radiology 2008; 246:142–147
13. Paulson EK, Sheafor DH, Enterline DS, et al. CT fluoroscopy-guided interventional procedures: techniques and radiation dose to radiologists. Ra-
diology 2001; 220:161–167 14. Cancer Therapy Evaluation Program. Common
terminology criteria for adverse events, version 3.0. National Cancer Institute Website. ctep.can-cer.gov/reporting/ctc.html. Published December 12, 2003. Accessed May 1, 2009
15. McCann JW, Maroo S, Wales P, et al. Image-guided drainage of multiple intraabdominal ab-scesses in children with perforated appendicitis: an alternative to laparotomy. Pediatr Radiol 2008; 38:661–668
16. Singh AK, Hahn PF, Gervais D, Vijayraghavan G, Mueller PR. Dropped appendicolith: CT findings and implications for management. AJR 2008; 190:707–711
17. Buckley O, Geoghegan T, Ridgeway P, Colhoun E, Snow A, Torreggiani WC. The usefulness of CT guided drainage of abscesses caused by retained appendicoliths. Eur J Radiol 2006; 60:80–83
18. Maher MM, Gervais DA, Kalra MK, et al. The inaccessible or undrainable abscess: how to drain it. RadioGraphics 2004; 24:717–735

















![Psoas Abscess Due to Appendicitis; Case Report And Review ...drain abscess and resecting the diseased bowel may be an op-tion [11]. An occasional patient may require multiple operations](https://static.fdocuments.in/doc/165x107/5e2d154e1c5e933ab1601d8e/psoas-abscess-due-to-appendicitis-case-report-and-review-drain-abscess-and.jpg)
