About Sharklet™ – A New Approach in Bacterial...
14
Understanding Sharklet™ Surface Protection Products A novel approach to improving cleanliness of high-touch environmental surfaces Using surface skins featuring the Sharklet™ pattern to decrease microbial burden on environmental surfaces April 2012
Transcript of About Sharklet™ – A New Approach in Bacterial...

Understanding Sharklet™ Surface Protection ProductsA novel approach to improving cleanliness of high-touch environmental surfaces
Using surface skins featuring the Sharklet™ pattern to decrease microbial burden on environmental surfaces
April 2012
© Sharklet Technologies, Inc. All rights reserved

2
Understanding the Sharklet Surface Protection Technology
About Sharklet™ – A New Approach in Bacterial Control.................................................................................3
Technology History...........................................................................................................................................4
The Role of Environmental Surfaces in Hospital-Acquired Infection Rates......................................................4
Sharklet Technology and Test Results..............................................................................................................5
The Sharklet Surface Inhibits Bacterial Attachment, Survival and Touch Transfer.......................................7
MRSA and MSSA – Smooth vs. Sharklet™.................................................................................................7
Pseudomonas aeruginosa – Smooth vs. Sharklet....................................................................................8
Vancomycin-resistant Enterococcus faecalis – Smooth vs. Sharklet.........................................................8
The Next Generation in Surfaces......................................................................................................................8
Contact Sharklet Technologies, Inc...................................................................................................................9
References......................................................................................................................................................10
www.sharklet.com

Scanning electron micrographs of the Sharklet micro-pattern with recessed grooves of varying lengths in silicone elastomer on the left and the alternate version of the Sharklet pattern with raised features on the right. Scale bars in both micrographs are 20 µm.
3
About Sharklet™ – A New Approach in Bacterial Control
Sharklet Technologies, Inc. is a United States company based in Aurora, Colorado. The biotechnology company develops a revolutionary surface product called Sharklet™. Unlike anything in the marketplace today, Sharklet is the only non-toxic, biocide-free and no-kill surface pattern used to inhibit microbial contamination on surfaces. The Sharklet pattern is manufactured into surfaces of products to create bacterial inhibition and to reduce surface-to person transfer of bacteria.
Sharklet is a patented surface technology comprised of millions of raised, microscopic features arranged in distinct diamond shapes to form a continuous micro-pattern (note the Sharklet pattern at right). Each Sharklet diamond measures 22 microns wide (left to right), 16 microns tall (top to bottom of a diamond), and each feature is about 3 microns in height. When manufactured into the surface of products, the pattern cannot be seen with the naked eye or felt to the touch. For reference purposes, each Sharklet diamond is about 1/50th the width of a human hair.
Of note, the Sharklet pattern provides bacterial inhibition through pattern alone – there are no chemicals, biocides, disinfectants or antibiotics eluted from the surface. In tests simulating an ambient hospital environment, the Sharklet patterned surface has shown to significantly reduce survival and touch transference of bacteria.
The Sharklet pattern is manufactured (imprinted) into the surfaces of products to create bacterial inhibition. While multiple products that feature the Sharklet pattern are in development, Sharklet Technologies, Inc. today offers Sharklet™ Surface Protection Products marketed under several brands including Tactivex® and SafeZone Media. The Surface Protection Products are film-based products or “skins” that feature the Sharklet pattern imprinted into the surface. The skins, via a variety of constructions including adhesively-backed films, are directly applied to high-traffic touch points that harbor bacteria and serve as vectors for bacterial transfer.
Until the advent of Sharklet, kill strategies including antibiotics, disinfectants and biocides have been the primary weapons to control bacterial growth. These kill strategies and their overuse has led to increased bacterial resistance, causing harm to people and the environment. The World Health Organization in 2009 named resistant bacteria as a top human health threat.
The applications and opportunities for Sharklet are numerous and the benefits of the benefits are measurable:
No risk for antimicrobial resistance. It is the shape and pattern of the surface alone that disrupts bacteria’s ability to survive, not antimicrobial agents that contribute to the development of “superbugs.”
Defense against multiple strains of bacteria. Sharklet has shown to be effective against many Gram-negative and Gram-positive strains, including clinical isolates, in different media and flow conditions (e.g. Staph a., MRSA, VRE, Pseudomonas aeruginosa and E. coli).
Cleaner surfaces between cleanings. The Sharklet pattern is always at work and serves as a safety net when hand washing and cleaning protocols fail.
www.sharklet.com

4
Ability to reduce costs with improved hygiene. In the healthcare sector, hospital-acquired infections account for $30.5 billion in excess healthcare costs each year. The cost of these infections is estimated between $8,000 and $15,000 per patient.
Sharklet Technologies offers an effective new approach to microorganism control. The deployment of Sharklet-patterned surface products provides an opportunity to address challenges with infection control, enhance cleaning protocols and protect bacteria-prone surfaces between cleanings.
Technology History
While the Sharklet pattern holds great promise to improve the way humans co-exist with microorganisms, the pattern was developed far outside of a laboratory. Sharklet was discovered via a seemingly unrelated problem: how to keep algae from coating the hulls of submarines and ships. In 2002, Dr. Anthony Brennan, a materials science and engineering professor at the University of Florida, was visiting the United States naval base at Pearl Harbor in Oahu as part of Navy-sponsored research. The U.S. Office of Naval Research solicited Dr. Brennan to find new antifouling strategies to reduce use of toxic antifouling paints and trim costs associated with dry dock and drag.
Dr. Brennan was convinced that using an engineered topography could be a key to new antifouling technologies. Clarity struck as he and several colleagues watched an algae-coated nuclear submarine leave port. Dr. Brennan remarked that the submarine looked like a whale lumbering out of the harbor. In turn, he asked which slow moving marine animals don’t foul. The only one? The shark.
Dr. Brennan was inspired to take an actual impression of shark skin, or more specifically, its dermal denticles. Examining the impression with scanning electron microscopy, Dr. Brennan confirmed his theory. Shark skin denticles are arranged in a distinct diamond pattern with tiny riblets. Dr. Brennan measured the ribs’ width-to-height ratios which corresponded to his mathematical model for roughness – one that would discourage microorganisms from settling. The first test of Sharklet yielded impressive results. Sharklet reduced green algae settlement by 85 percent compared to smooth surfaces.
While the U.S. Office of Naval Research continued to fund Dr. Brennan’s work for antifouling strategies, new applications for the pattern emerged. Brennan evaluated Sharklet’s ability to inhibit the growth of other microorganisms. Sharklet proved to be a mighty defense against bacteria.
Similar to algae, bacteria take root singly or in small groups with the intent to establish large colonies, or biofilms. Also similar to other organisms, bacteria seek the path of least energy resistance. Research results suggest that Sharklet keeps biofilms from forming because the pattern requires too much energy for bacteria to colonize. The consequence is that organisms find another place to grow or simply die from inability to signal to other bacteria. In addition to evaluating Sharklet’s ability to inhibit biofilm formation, the technology also proved to inhibit bacteria’s ability to attach and survive on the pattern.
The Role of Environmental Surfaces in Hospital-Acquired Infection Rates
Despite improved knowledge and greater focus prevention, incidences of healthcare-acquired infections (HAIs) have continued to rise in recent decades. HAIs are now among the top six leading causes of death in the United States with 98,987 recorded deaths in 20021. The medical impact of these infections has been matched in magnitude by the economic impact, which includes the costs of the treatment as well as the measures taken by the healthcare community to control and limit the spread of infections. Efforts such as patient monitoring, active surveillance protocols, screening-based isolation protocols, hand hygiene protocols and cleaning and disinfection procedures have become ubiquitous to present-day healthcare epidemiology practice2,3,4.
www.sharklet.com

5
The root of the challenge is in preventing the spread of HAI pathogens that lead to these infections. The most difficult infections to treat are those that include antibiotic-resistant pathogens such as methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE), as well as spore-forming Clostridium difficile 3, 5. The Health Care Infection Control Practices Advisory Committee (HICPAC) defines contact transmission of pathogens as occurring with a contaminated intermediate object or person (“indirect transmission”) or without (“direct transmission”)6. It is well documented that pathogens readily contaminate environmental surfaces near patients and can survive and persist on these inanimate surfaces for weeks to months7,8,9,10. Examples of frequently touched surfaces include bed rails, tray tables, telephones, bedside tables, patient chairs nurse call buttons/handsets9, 11, 12, 13. Indirect transmission in the hospital environment occurs when these contaminated surfaces are touched; pathogens are transferred from environmental surfaces to healthcare workers’ hands and objects, where they can then be transported elsewhere14,15,16. In addition, recent scientific evidence confirms that patients admitted to rooms previously occupied by patients infected or colonized with MRSA, VRE, C. difficile and Acinetobacter baumannii have, on average, a 73 percent increased risk of acquiring the same pathogen from environmental surfaces contaminated by the prior room occupants17,18,19,20,21,22.
In the past decade, numerous guidelines, recommendations, and standards have been introduced that relate to improving environmental hygiene practices in healthcare settings. Healthcare infection control guidelines from the Centers for Disease Control and Prevention (CDC) now emphasize the importance of cleaning and disinfecting ‘high-touch surfaces’ and monitoring these activities to maintain a sanitary environment in the hospital6. These guidelines reflect an evolving mindset that patient area environmental cleanliness in healthcare settings plays a significant role in infection prevention and control.
Despite the increased attention to environmental hygiene, recent studies evaluating the effectiveness of environmental cleaning have show that only 40 percent of near-patient surfaces are cleaned in accordance with existing hospital policies2,12,13,18. Furthermore, certain multi-drug resistant organisms require specific cleaning regimens and products, reflecting a dynamic situation that relies upon ever-changing guidelines and compliance4. In contrast to the abundance of hand sanitizers and cleansers that have been introduced for hospital use to improve hand hygiene, there are surprisingly few technological improvements for reducing environmental surface contamination23.
The need for improved measures to keep environmental surfaces clean and prevent transmission of pathogens may be addressed in the following ways:
1. Technologies / procedures to improve cleaning and disinfection of environmental surfaces2. Surface technologies that reduce microbial presence on the surface.
Ideally, these two approaches would be implemented concurrently, where proper cleaning practices would be complemented by a surface technology that reduces the risk of pathogen transmission between cleanings.
To address this need, Sharklet Technologies has developed and tested Sharklet – a novel, microscopic surface texture to reduce microbial contamination compared to un-textured control surfaces.
Sharklet Technology and Test Results
Sharklet Surface Protection Products address a key unaddressed area of healthcare: surfaces. Today, much attention is given to improving hand washing that reduces transfer of bacteria between people. Surface cleanliness is addressed through the use of standard cleaning techniques including disinfection or through biocidal agents. Yet, reliance on humans to adhere to these protocols begs the question of effectiveness.
Sharklet Surface Protection Products fill a gap in the hygiene continuum. A Sharklet-patterned surface is always at work and provides a cleaner surface between cleanings. Sharklet surfaces also serve as a safety net when hand
www.sharklet.com

The photos above show colonies of S. aureus after one hour of drying on surfaces. The RODAC plates were touched to surfaces that were populated with S. aureus. The Sharklet surface in the two top RODAC plates show significantly less attachment and bacterial growth.
Sharkle
tSmooth
*Testing carried out by Dr. Kenneth Rand, Professor of Pathology and Medicine, University of Florida, College of Medicine
6
washing and cleaning protocols fail. Further, the technology helps break the pathogen transmission loop by protecting surfaces that are most often touched.
Testing data demonstrates Sharklet has two general effects on bacteria to reduce surface contamination. When compared to an un-patterned, smooth surface:
1. Less bacteria attach to the Sharklet pattern2. Less bacteria survive on the Sharklet pattern over time
It is worth noting that competing strategies rely mainly on chemical surface coatings to inhibit bacterial adherence. The antimicrobial coating strategy is hampered by the development of antimicrobial resistant strains of bacteria and by the harmful toxicity that many of these agents rely upon for their biocidal effect. By comparison, the Sharklet pattern adds no chemical coatings or biocidal agents. This purely physical approach to inhibiting microbial attachment does not rely on the incorporation of antimicrobial agents, thus sidestepping the growing problem of multi-drug resistant ‘superbugs.’
The development of antimicrobial coating methods stem from the commonly held belief that cell attachment is primarily influenced by the chemical composition and activity of the surface. While this is an important factor, the influence of surface topography can be a significant factor in affecting cell attachment.
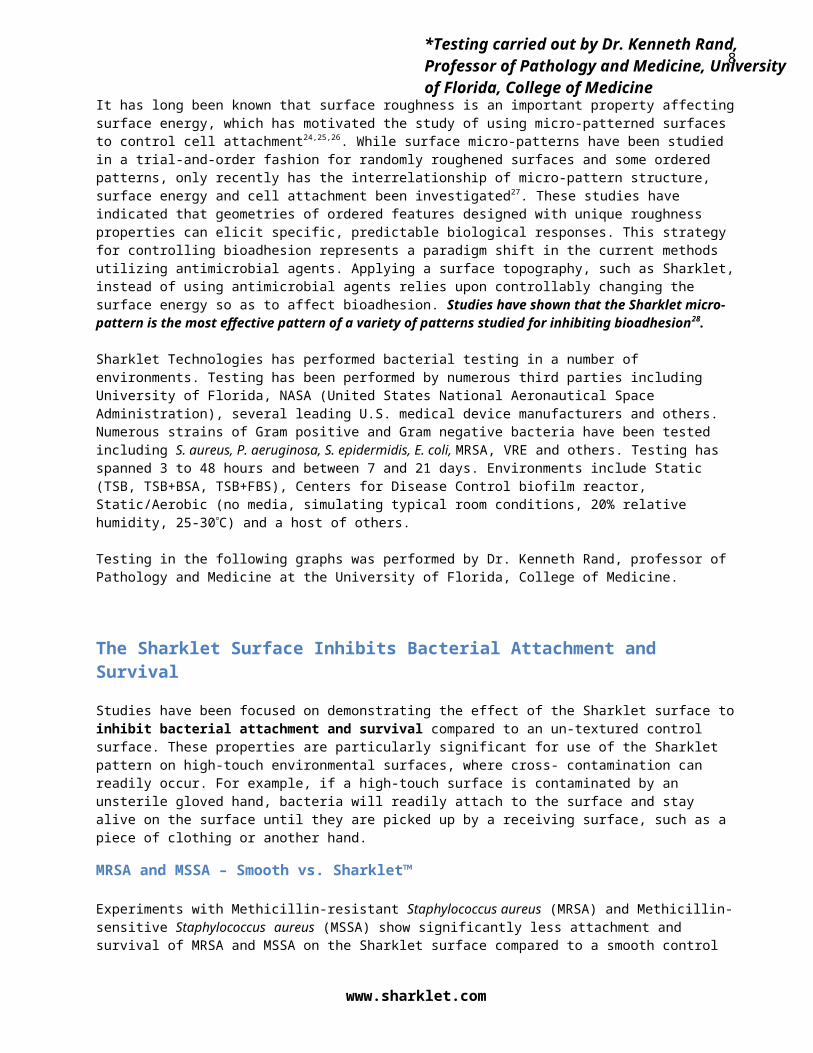
It has long been known that surface roughness is an important property affecting surface energy, which has motivated the study of using micro-patterned surfaces to control cell attachment24,25,26. While surface micro-patterns have been studied in a trial-and-order fashion for randomly roughened surfaces and some ordered patterns, only recently has the interrelationship of micro-pattern structure, surface energy and cell attachment been investigated27. These studies have indicated that geometries of ordered features designed with unique roughness properties can elicit specific, predictable biological responses. This strategy for controlling bioadhesion represents a paradigm shift in the current methods utilizing antimicrobial agents. Applying a surface topography, such as Sharklet, instead of using antimicrobial agents relies upon controllably changing the surface energy so as to affect bioadhesion. Studies have shown that the Sharklet micro-pattern is the most effective pattern of a variety of patterns studied for inhibiting bioadhesion28.
Sharklet Technologies has performed bacterial testing in a number of environments. Testing has been performed by numerous third parties including University of Florida, NASA (United States National Aeronautical Space Administration), several leading U.S. medical device manufacturers and others. Numerous strains of Gram positive and Gram negative bacteria have been tested including S. aureus, P. aeruginosa, S. epidermidis, E. coli, MRSA, VRE and others. Testing has spanned 3 to 48 hours and between 7 and 21 days. Environments include Static (TSB, TSB+BSA, TSB+FBS), Centers for Disease Control biofilm reactor, Static/Aerobic (no media, simulating typical room conditions, 20% relative humidity, 25-30C) and a host of others.
Testing in the following graphs was performed by Dr. Kenneth Rand, professor of Pathology and Medicine at the University of Florida, College of Medicine.
www.sharklet.com

7
The Sharklet Surface Inhibits Bacterial Attachment and Survival
Studies have been focused on demonstrating the effect of the Sharklet surface to inhibit bacterial attachment and survival compared to an un-textured control surface. These properties are particularly significant for use of the Sharklet pattern on high-touch environmental surfaces, where cross- contamination can readily occur. For example, if a high-touch surface is contaminated by an unsterile gloved hand, bacteria will readily attach to the surface and stay alive on the surface until they are picked up by a receiving surface, such as a piece of clothing or another hand.
MRSA and MSSA – Smooth vs. Sharklet™
Experiments with Methicillin-resistant Staphylococcus aureus (MRSA) and Methicillin-sensitive Staphylococcus aureus (MSSA) show significantly less attachment and survival of MRSA and MSSA on the Sharklet surface compared to a smooth control surface after exposure to a highly concentrated suspension of the bacteria. See the table below.
*Indicates p-values of all experiments were less than 0.05.
When survival testing was extended out to 24 hours, the trends for reduced S. aureus attachment and survival continued to hold (see figure below). Sharklet patterned and un-patterned acrylic samples were inoculated and exposed to an aerobic environment for zero, one, three, and 24 hours of drying time. The Sharklet samples maintained 80-99% fewer cells than the un-patterned controls. *Counts from the second 24 hour MRSA experiment were too few to count and were not included in this analysis.
www.sharklet.com
8
Pseudomonas aeruginosa – Smooth vs. SharkletSharklet reduces Pseudomonas aeruginosa by 100 percent versus a smooth surface after one hour of exposure simulating typical room conditions. Laboratory test performed on Sharklet on silicone elastomer.
Vancomycin-resistant Enterococcus faecalis – Smooth vs. SharkletSharklet reduces Vancomycin-resistant Enterococcus faecalis by 99 percent versus a smooth surface of after one hour of exposure simulating typical room conditions. Laboratory test performed on Sharklet on silicone elastomer.
These charts provide a graphical representation of Sharklet Surface Protection Product effectiveness against a variety of bacteria in environments that are reflective of ambient conditions in a healthcare environment.
The Next Generation in Surfaces
While disinfectant solutions and regularly-implemented cleaning protocols are important in high-risk environments such as healthcare facilities, food-preparation facilities, and public high-touch areas, surface protection between cleanings is equally important. The Sharklet surface offers the capability to reduce bacterial burden on surfaces via reduced bacterial attachment and survival, thereby reducing the amount of bacteria able to be transferred from the surface to the next person coming in contact with the surface.
These outcomes provide an overall effect on bacterial cross-contamination: less bacteria attach to a Sharklet surface compared to a smooth un-patterned surface, which results in fewer surviving bacteria over time; which results in lesser amounts of bacteria present that can then be transferred to another contacting surface.
www.sharklet.com

9
This compound, sequential effect offers multiple levels of safeguards for the surface and the people coming into contact with contaminated surfaces. The Sharklet surface thus offers a continuous safeguard for surfaces and people in a manner that does not expose users to toxic chemical agents and does not actively promote antimicrobial resistance.
Contact Sharklet Technologies, Inc.
For more information, contact:
Sharklet Technologies, Inc. 12635 E. Montview Blvd., Suite 160 Aurora, Colorado 80045
720-859-4070
Safe Touch Solutions Inc.996 120th StreetBerwick, Illinois 61417Tel: (309) 426.2600www.safetouchsolutions.net
www.sharklet.com

10
References
www.sharklet.com
1 Klevens RM, “Estimating health care-associated infections and deaths in U.S. hospitals, 2002” Public Health Reports 22: 160 (2007)
2 Carling PC, Parry MF, and Von Beheren SM, “Identifying Opportunities to Enhance Environmental Cleaning in 23 Acute Care Hospitals“ Infect Control Hosp Epidemiol 29: 1-7 (2008)
3 Carling PC and Bartley JM, “Evaluating hygienic cleaning in health care settings: What you do not know can harm your patients“ Am J Infect Control 38: 5 (2010a)
4 Sattar SA, “Promises and pitfalls of recent advances in chemical means of preventing the spread of nosocomial infections by environmental surfaces“ Am J Infect Control 38: S34-40 (2010)
5 Weber DJ, Rutala WA, Miller MB, et al., “Role of hospital surfaces in the transmission of emerging health care-associated pathogens: Norovirus, Clostridium difficile, and Acinetobacter species“ Am J Infect Control 38: S25-33 (2010)
6 Siegel JD, Rhinehart E, Jackson M, et al., “2007 guideline for isolation precautions: preventing transmission of infectious agents in health care settings“ Am J Infect Control 35: S65-164 (2007)
7 Huang R, Mehta S, Weed D, et al., “Methicillin-resistant Staphylococcus aureus survival on hospital fomites“ Infect Control Hosp Epidemiol 27: 1267-1269 (2006)
8 Kramer A, Schwebke I, and Kampf G, “How long do nosocomial pathogens persist on inanimate surfaces? A systematic review“ BMC Infect Dis 6: 130 (2006)
9 Boyce JM, “Environmental contamination makes an important contribution to hospital infection“ J Hosp Infect 65(S2): 50–54 (2007)
10 Dancer SJ, “The role of environmental cleaning in the control of hospital-acquired infection” J Hosp Infect 72: 378-385 (2009)
11 Carling PC, Briggs J, Hylander D, et al., “An evaluation of patient area cleaning in 3 hospitals using a novel targeting methodology” Am J Infect Control 34: 513-519 (2006)
12 White LF, Dancer SJ, Robertson C, et al., “Are hygiene standards useful in assessing infection risk?“ Am J Infect Control 36: 381-4 (2008)
13 Carling PC, Parry MF, Bruno-Murtha LA, et al., “Improving environmental hygiene in 27 intensive care units to decrease multidrug-resistant bacterial transmission“ Crit Care Med 38: 4 (2010b)
14 Bhalla A, Pultz NJ, Gries DM, et al., “Acquisition of nosocomial pathogens on hands after contact with environmental surfaces near hospitalized patients” Infect Control Hosp Epidemiol 29: 149-154 (2008)
15 Hayden MK, Blom DW, Lyle EA, et al., “Risk of hand or glove contamination after contact with patients colonized with vancomycin-resistant Enterococcus or the colonized patients’ environment” Infect Control Hosp Epidemiol 29: 149-154 (2008)
16 Morgan DJ, Liang SY, Smith CL, et al., “Frequent multi-drug resistant Acinetobacter baumannii contamination of gloves, gowns, and hands of healthcare workers” Infect Control Hosp Epidemiol 31(7): 716-721 (2010)
17 Denton M, Wilcox MH, Parnell P, et al., “Role of environmental cleaning in controlling an outbreak of Acinetobacter baumannii on a neurosurgical intensive care unit” J Hosp Infect 56: 106-110 (2004)
18 Hayden MK, Bonten MJM, Blom DW, et al., “Reduction in Acquisition of Vancomycin-Resistant Enterococcus after Enforcement of Routine Environmental Cleaning Measures“ Clin Infect Dis 42: 1552–60 (2006)
19 Huang SS, Datta R, and Platt R, “Risk of Acquiring Antibiotic-Resistant Bacteria From Prior Room Occupants“ Arch Intern Med 166: 1945-1951 (2006)
20 Hardy KJ, Oppenheim BA, Gossain S, et al., “A study of the relationship between environmental contamination with methicillin-resistant Staphylococcus aureus (MRSA) and patients’ acquisition of MRSA” Infect Control Hosp Epidemiol 27: 127-132 (2006)

21 Shaugnessy M, Micielli R, Depestel D, et al., “Evaluation of hospital room assignment and acquisition of Clostridium difficile associated diarrhea” Abstract K-4194. Presented at 48th Annual ICAAC/IDSA 46th Annual Meeting. Washington, DC. October 2008.
22 Drees M, Snydman DR, Schmid CH, et al., “Antibiotic exposure and room contamination among patients colonized with vancomycin-resistant Enterococci” Infect Control Hosp Epidemiol 29: 709-715 (2008)
23 Page K, Wilson M, and Parkin IP, “Antimicrobial surfaces and their potential in reducing the role of the inanimate environment in the incidence of hospital-acquired infections“ J Mater Chem 19: 3819–3831 (2009)
24 Schmidt JA, von Recum AF, “Texturing of polymer surfaces at the cellular level” Biomaterials 12(4): 385 (1991)
25 den Braber 1998, de Ruijter JE, Ginsel LA, von Recum AF, Jansen JA, “Orientation of ECM protein deposition, fibroblast cytoskeleton, and attachment complex components on silicone microgrooved surfaces” J Biomed Mater Res 40(2): 291 (1998)
26 van Kooten TG, von Recum AF, “Cell adhesion to textured silicone surfaces: the influence of time of adhesion and texture on focal contact and fibronectin fibril formation” Tissue Eng 5: 223 (1999)
27 Carman ML, Estes TG, Feinberg AW, Schumacher JF, Wilkerson W, Wilson LH, Callow ME, Callow JA, Brennan AB, “Engineered antifouling microtopographies – correlating wettability with cell attachment” Biofouling 22(1): 11 (2006)
28 Schumacher JF, Long CJ, Callow ME, Finlay JA, Callow JA, Brennan AB, “Engineered nanoforce gradients for inhibition of settlement (attachment) of swimming algal spores” Langmuir 24(9): 4931 (2008)