
Abnormalities of the Placenta, Umbilical Cord, and Membranes Prepared by: Mr’s Raheegeh Awni.
33
Abnormalities of the Placenta, Umbilical Cord, and Membranes Prepared by: Mr’s Raheegeh Awni
-
Upload
anissa-cobb -
Category
Documents
-
view
246 -
download
4
Transcript of Abnormalities of the Placenta, Umbilical Cord, and Membranes Prepared by: Mr’s Raheegeh Awni.

Abnormalities of the Placenta, Umbilical Cord, and Membranes
Prepared by: Mr’s Raheegeh Awni

Placental Abnormalities
• Placental and fetal size and weight roughly correlate in a linear fashion.
• There is also evidence that fetal growth depends on placental weight, which is less with small-for-gestational age infants.
According to Mathews and associates, this is not dependent on nutrients.
Multiple Placentas with a Single Fetus
• The placenta occasionally is separated into lobes.
• When the division is incomplete and the vessels of fetal origin extend from one lobe to the other before uniting to form the umbilical cord, the condition is termed placenta bipartita or bilobata.
• Fox (1978) cited its incidence to be at about 1 in every 350 deliveries

placenta bipartita
Succenturiate Lobes
• One or more small accessory lobes that develop in the membranes at a distance from the periphery of the main placenta, to which they usually have vascular connections of fetal origin.
• It is a smaller version of the bilobed placenta, • Incidence is about 5 percent• The accessory lobe may sometimes be retained in the uterus
after delivery and may cause serious hemorrhage. • In some cases, an accompanying vasa previa may cause
dangerous fetal hemorrhage at delivery

Succenturiate Lobes

Membranaceous Placenta
• Very rarely, all of the fetal membranes are covered by functioning villi, and the placenta develops as a thin membranous structure occupying the entire periphery of the chorion.
• This finding is called placenta membranacea and also is referred to as placenta diffusa. Diagnosis often can be made using sonography.
• It may occasionally give rise to serious hemorrhage because of associated placenta previa or accreta.

Ring-Shaped Placenta
• In fewer than 1 in 6000 deliveries, the placenta is annular in shape, and sometimes a complete ring of placental tissue is present.
• This development may be a variant of membranaceous placenta.
• Because of tissue atrophy in a portion of the ring, a horseshoe shape is more common. These abnormalities appear to be associated with a greater likelihood of antepartum and postpartum bleeding and fetal growth restriction


Placenta Accreta, Increta, and Percreta
• These abnormalities are serious variations in which trophoblastic tissues invade the myometrium to varying depths.
• They are much more likely with placenta previa or with implantation over a prior uterine incision or perforation.
• Hemorrhage is a frequent complication

Degenerative Placental Lesions
• Degenerative lesions may result from trophoblast aging, or impairment of uteroplacental circulation with infarction.
• Deposition of calcium salts is heaviest on the maternal surface in the basal plate.
• It is more extensive in smokers whose placentas also have reduced fetal capillary diameters (Larsen and co-workers, 2002).
• Extensive calcification is found in 10 to 15 percent of all placentas at term
• (This can be seen with sonography, and Spirt and colleagues (1982) reported that by 33 weeks more than half of placentas have some degree of calcification.
• It is difficult to correlate the degree of calcium deposition with pregnancy outcome.

Abnormalities of the Membranes
• Meconium Staining• The presence of meconium in amnionic fluid is
relatively common and was identified in 12 percent.
• Preterm fetuses seldom pass meconium. It is uncommon prior to 38 weeks, after which it increases to 25 to 30 percent after 42 weeks.

• Staining of the amnion can be obvious within 1 to 3 hours after meconium passage.
• Although more prolonged exposure results in staining of the chorion, umbilical cord, and decidua, meconium passage cannot be timed or dated accurately

• Neonatal morbidity and mortality associated with meconium is characterized by the meconium aspiration syndrome.
• Severe disease requires ventilatory assistance and has a mortality rate of about 10 percent.
• Although it is commonly held that meconium aspiration syndrome is primarily the result of aspiration of thick, tenacious meconium, Ghidini and Spong (2001) concluded from their review that thin meconium also was associated with respiratory insufficiency.

Chorioamnionitis
• Inflammation of the fetal membranes usually is a manifestation of intrauterine infection.
• It frequently is associated with prolonged membrane rupture and long labor.
• infection is characterized by clouding of the membranes .
• There also may be a foul odor, depending on bacterial species and concentration.

• When mono- and polymorphonuclear leukocytes infiltrate the chorion, the resulting microscopical finding is designated chorioamnionitis.
• These cells are maternal in origin. Conversely, if leukocytes are found in amnionic fluid (amnionitis), or the umbilical cord (funisitis), the cells are fetal in origin.
• Before 20 weeks, almost all polymorphonuclear leukocytes are maternal in origin, but later the inflammatory response is both maternal and fetal.
• (Microscopic evidence for inflammation of these structures is much more common in preterm deliveries.

Umbilical Cord Abnormalities
• The cord develops in close association with the amnion.
• The cord serves a vital function, but it unfortunately is susceptible to entanglement, compression, and occlusion.
• Collins and Collins (2000) reported a 1-percent incidence of potentially harmful cord complications.

Length
• Cord length at term has appreciable variation, and extremes range from no cord (achordia) to lengths up to 300 cm.
• Short umbilical cords may be associated with adverse perinatal outcomes such as fetal growth restriction, congenital malformations, intrapartum distress, and a twofold risk of death.
• Excessively long cords are more likely to cause complications such as prolapse.

• Excessively long cords are described to be more than two standard deviations, which was 70 cm or longer.
• Pregnancies involving a fetus with a long cord were associated with maternal systemic disease and delivery complications.
• There were more cases of cord entanglement, fetal distress, fetal anomalies, and respiratory distress.
• Perinatal mortality was increased nearly threefold, albeit with borderline statistical significance.

• Heredity is a determinant factor of cord length factor, and 9 percent of women with an excessively long cord.
• Miller and associates (1981) identified the cord to be shortened appreciably when there had been either chronic fetal constraint from oligohydramnios or decreased fetal movement, such as with Down syndrome or limb dysfunction.

Cord Coiling
• In most cases, the umbilical vessels course through the cord in a spiraled manner.
• Several authors have observed a significant increase in various adverse outcomes in fetuses with hypocoiled cords.
• meconium staining• preterm birth, • and fetal distress

hypercoiled cords
• Rana and associates (1995) found a higher incidence of:
• preterm delivery• cocaine abuse in women with.

Single Umbilical Artery
• Identification of a two-vessel cord is an important observation.
• About one fourth of all infants with only one umbilical artery have associated congenital anomalies.
• In a review of nearly 350,000 deliveries, Heifetz (1984) found an incidence of a single artery to be 0.63 percent in liveborns, 1.92 percent in neonates with perinatal death, and 3 percent in twins.
Risk factors• diabetes, • epilepsy,• preeclampsia, • antepartum hemorrhage, • oligohydramnios, • and hydramnios.• Over half of these of two-vessel cords had serious
malformations as tracheoesophageal fistula.• most are associated with chromosomal
abnormalities.

Velamentous Insertion
• This insertion is of considerable importance. • The umbilical vessels separate in the membranes at a
distance from the placental margin.• Velamentous insertion occurs much more frequently
with twins, and Feldman and associates (2002) identified it in 28 percent of triplets.

Velamentous Insertion
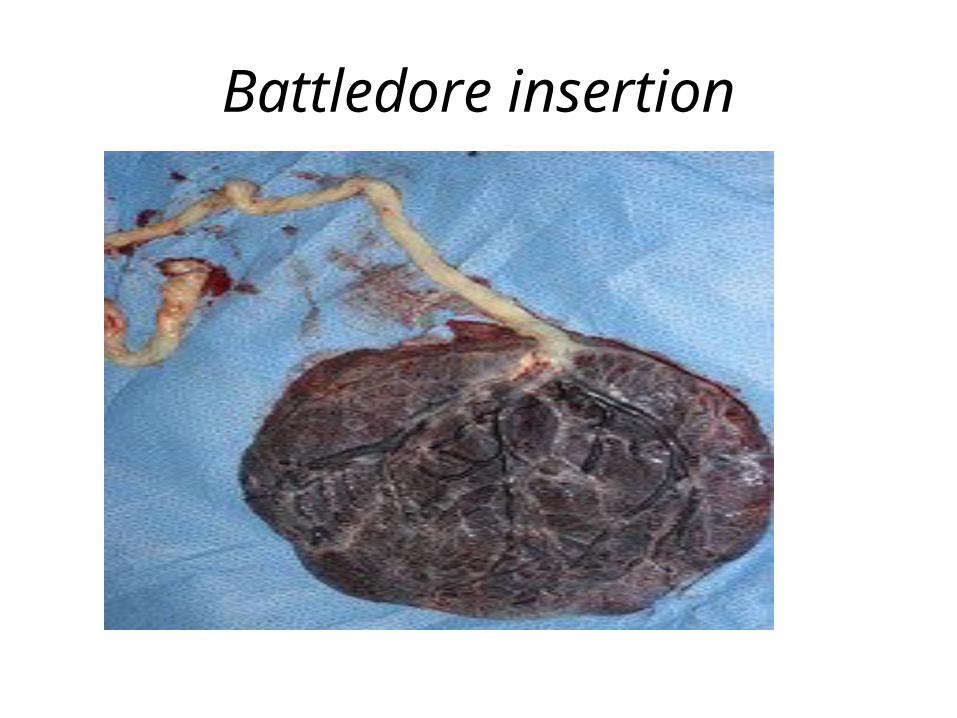
Battledore insertion.
• Cord insertion at the placental margin is sometimes referred to as a Battledore placenta.
• It is found in about 7 percent of term placentas (
• With the exception of the cord being pulled off during delivery of the placenta, it is of little clinical significance.
Battledore insertion

Vasa Previa
• Is associated with velamentous insertion when some of the fetal vessels in the membranes cross the region of the cervical os below the presenting fetal part.
• Vasa previa was identified in 18, for an incidence of 1 in about 5200 pregnancies.
• About half were associated with velamentous insertion and the rest divided between marginal cord insertions and bilobed or succenturiate-lobed placentas.

COMPLICATIONS
• membrane rupture may be accompanied by tearing of a fetal vessel..
• fetal mortality compared when discovered at delivery.

Knots
• False knots, which result from kinking of the vessels to accommodate to the length of the cord, should be distinguished from true knots, which result from active fetal movements.
• The incidence is especially high in monoamnionic twins.
• Venous stasis may lead to mural thrombosis and fetal hypoxia, causing death or neurological morbidity.
• Collins and Collins (2000) estimate a 6 percent incidence of stillbirths when true knots are found



















