ABNORMALITIES OF FECAL ELIMINATION
23
BY TIMOTHY OLADOSU ABNORMALITIES OF FECAL ELIMINATION
Transcript of ABNORMALITIES OF FECAL ELIMINATION

B Y
T I M O T H Y O L A D O S U
ABNORMALITIES OF FECAL ELIMINATION

OUTLINE
• Introduction
• Constipation • Causes
• Clinical manifestations
• Diagnostic findings
• Management
• Drugs used in constipation
• Complications
• Diarrhea • Causes
• Clinical manifestations
• Diagnostic findings
• Management
• Complications
• Fecal incontinence • Causes
• Clinical manifestations
• Diagnostic findings
• Management

INTRODUCTION
• Changes in patterns of fecal elimination are
symptoms of functional disorders or disease states in
the GIT
• The most common changes seen are;
• Constipation
• Diarrhea, and
• Fecal incontinence

CONSTIPATION
• It is a term used to describe;
• An abnormal infrequency or irregularity of defecation
• Abnormal hardening of stools that makes their passage
difficult and sometimes painful
• A decrease in stool volume
• Retention of stool in the rectum for a prolonged period of
time
• Any variation from normal habits may be seen as a
problem

CAUSES
• Constipation can be caused by; • Certain medications (e.g. tranquilizers, anticholinergics,
antidepressants, antihypertensives, opioids, antacids with aluminium, iron)
• Rectal or anal disorders (e.g. hemorrhoids, fissures) • Obstruction (e.g. cancer of the bowel)
• Endocrine disorders (e.g. hypothyroidism, pheochromocytoma)
• Lead poisoning
• Connective tissue disorders (e.g. scleroderma, lupus erythematosus)
• Metabolic, neurologic, and neuromuscular conditions (e.g. diabetes mellitus, Hirschsprung’s disease, Parkinson’s disease, multiple sclerosis)
• Opoids analgesics • Diseases of the colon (e.g. irritable bowel syndrome, diverticular
disease)
• Acute abdomen (e.g. appendicitis)

• Other causes include;
• Weakness
• Immobility
• Debility
• Fatigue
• Inability to increase intra-abdominal pressure(as seen in
emphysema)
• Ignoring the urge to defeacate
• Dietary habits (low consumption of fiber and inadequate
fluid intake)
• Lack of regular exercise
• A stress-filled life

CLINICAL MANIFESTATIONS
• Abdominal distention
• Borborygmus (intestinal rumbling)
• Pain
• Pressure
• Decreased appetite
• Headache
• Fatigue
• Indigestion
• Sensation of incomplete emptying
• Straining at stool
• Elimination of small-volume, hard, dry stool

DIAGNOSTIC FINDINGS
• Patient history
• Physical examination
• Barium enema
• Stool testing for occult blood
• Sigmoidoscopy
• Anorectal manometry
• Defecography and bowel transit studies

MANAGEMENT
• Treatment is aimed at the underlying cause
• Inclusion of fiber in the diet with an increase in fluid
intake
• Routine exercise to strengthen abdominal muscles
• Discontinuity of laxative abuse

DRUGS USED FOR CONSTIPATION DRUG CATEGORY AND EXAMPLES MECHANISM OF ACTION NURSING CONSIDERATIONS
CHEMICAL STIMULANTS
bisacodyl (Dulcolax)
cascara (generic)
castor oil (Neoloid)
senna (Senokot
Directly stimulate the nerve
plexus in the intestinal wall,
causing increased movement
and stimulation of local
reflexes. Lead to intestinal
evacuation
Prior to administration assess client’s abdomen for
tenderness, rigidity, and bowel sounds.
Ask when client had last bowel movement.
Repeated use in the older adult may cause
orthostatic hypotension and weakness from
electrolyte loss.
Encourage client to maintain adequate fluid intake.
After administration assess client for:
-Bowel activity and stool consistency
- Bowel sounds
- Serum electrolytes for clients with repeated use
BULK FORMING AGENTS
magnesiumsulfate (Epsom salts)
magnesiumcitrate (Citrate of
Magnesium)
magnesiumhydroxide (Milk of
Magnesia)
polycarbophil (FiberCon)
psyllium (Metamucil
Increase intestinal motility by
increasing fluids in intestinal
contents. This in turn enlarges
bulk, stimulates local stretch
receptors, and activates bowel
reflex activity
Prior to administration assess client’s abdomen for
tenderness, rigidity, and bowel sounds.
Ask when client had last bowel movement.
Magnesium products may cause ECG changes with
prolonged use.
After administration assess the client for:
-Amount, color, and consistency of stool
-Daily pattern of bowel activity
- Bowel sounds
- BUN, serum creatinine, and magnesium levels for
clients with repeated or chronic use
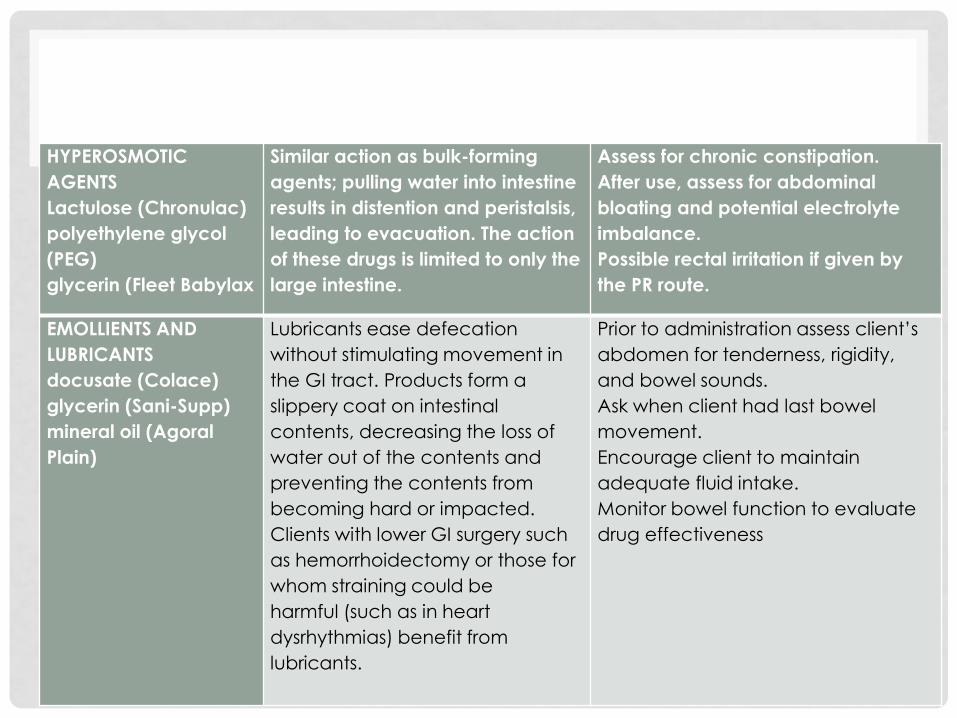
HYPEROSMOTIC
AGENTS
Lactulose (Chronulac)
polyethylene glycol
(PEG)
glycerin (Fleet Babylax
Similar action as bulk-forming
agents; pulling water into intestine
results in distention and peristalsis,
leading to evacuation. The action
of these drugs is limited to only the
large intestine.
Assess for chronic constipation.
After use, assess for abdominal
bloating and potential electrolyte
imbalance.
Possible rectal irritation if given by
the PR route.
EMOLLIENTS AND
LUBRICANTS
docusate (Colace)
glycerin (Sani-Supp)
mineral oil (Agoral
Plain)
Lubricants ease defecation
without stimulating movement in
the GI tract. Products form a
slippery coat on intestinal
contents, decreasing the loss of
water out of the contents and
preventing the contents from
becoming hard or impacted.
Clients with lower GI surgery such
as hemorrhoidectomy or those for
whom straining could be
harmful (such as in heart
dysrhythmias) benefit from
lubricants.
Prior to administration assess client’s
abdomen for tenderness, rigidity,
and bowel sounds.
Ask when client had last bowel
movement.
Encourage client to maintain
adequate fluid intake.
Monitor bowel function to evaluate
drug effectiveness

COMPLICATIONS
• Hypertension
• Fecal impaction
• Hemorrhoids
• Fissures
• megacolon

DIARRHEA
• Diarrhea can be defined as; • Increased frequency of bowel movements (more than 3
times per day)
• Increased amount of stool (more than 200g/day)
• Altered consistency (looseness) of stool
• It is usually associated with urgency, perianal discomfort, incontinence, or a combination of these
• Diarrhea can be acute or chronic;
• Acute diarrhea is most often associated with infection and is usually self-limiting
• Chronic diarrhea persists for a longer period of time and may return sporadically

CAUSES
• The most common cause is infection by bacterial, parasitic or viral agents
• Lactose intolerance
• Food allergies or intolerance
• Uremia
• Intestinal diseases e.g. diverticulitis, ulcerative colitis, malabsorption, intestinal obstruction
• Rapid addition of fiber to diet
• Consumption of highly spiced or seasoned food
• Overuse of laxatives
• Adverse effect of drugs esp antibiotics
• Concentrated tube-feeding formulas
• Irritable bowel syndrome
• Immunoglobulin A deficiency
• Overeating
• Metabolic disorders & diseases e.g. cystic fibrosis, pancreatic insufficiency, inflammatory bowel diseases

CLINICAL MANIFESTATIONS
• Increased frequency and fluid content of stool
• Abdominal cramps
• Distention
• Intestinal rumbling (borborygmus)
• Anorexia
• Thirst
• Ineffectual straining (tenesmus)
• Fluid and electrolyte imbalances
• dehydration

DIAGNOSTIC FINDINGS
• Detailed history
• Complete blood count
• Urinalysis
• Stool examination for infectious or parasitic
organisms, bacterial, toxins, blood, fat & electrolytes
• Endoscopy
• Barium enema

MANAGEMENT
• Primary management is directed at; • Controlling symptoms • Preventing complications • Eliminating or treating the underlying disease
• Medications such as antibiotics, anti-inflammatory agents may reduce the severity
• Administration of an antidiarrheal agent, such as diphenoxylate hydrochloride with atropine sulfate (Lomotil), loperamide hydrochloride (Imodium), or a combination product such as kaolin and pectin (Kaopectate)
• Fluid and electrolyte replacement by either the oral or intravenous (IV) route
• Dietary adjustments, which may involve eliminating foods that cause diarrhea
• Total parenteral nutrition (TPN) if diarrhea is severe and prolonged and if the introduction of oral fluid and food results in another episode of diarrhea

COMPLICATIONS
• Muscle weakness
• Paresthesia
• Hypotension
• Anorexia
• Cardiac dysrhythmias (due to loss of potassium)
• Urinary output of less than 30mL/hour

FECAL INCONTINENCE
• Is the involuntary passage of stool from the rectum
• The following factors influence it;
• Ability of the rectum to sense & accommodate stool
• Amount & consistency of stool
• Integrity of the anal sphincters & musculature
• Rectal motility
CAUSES
• Trauma (post rectal surgeries)
• Neurologic disorder (e.g. stroke, multiple sclerosis, diabetic neuropathy, dementia)
• Inflammation
• Infection
• Radiation treatment
• Fecal impaction
• Pelvic floor relaxation
• Laxative abuse
• Medications
• Advancing age (i.e. weakness or loss of anal or rectal muscle tone)

CLINICAL MANIFESTATIONS
• Minor soiling
• Occasional urgency and loss of control
• Complete incontinence
• Poor control of flatus
• Diarrhea

DIAGNOSTIC FINDINGS
• Detailed history
• Rectal examination
• Flexible sigmoidoscopy to rule out tumors,
inflammation or fissures
• X-ray studies
• Barium enema
• CT scans
• Anorectal manometry
MANAGEMENT
• Fecal incontinence is frequently a symptom of fecal
impaction, once the impaction is removed & the
rectum is cleansed, normal function resume
• If fecal incontinence is related to diarrhea, the
incontinence may disappear when that process is
successfully treated
• Surgical procedures include;
• Surgical reconstruction
• Sphincter repair
• Fecal diversion