ielts fever Listening TEST · Listening TEST listeningTest 29 Ielts fever ielts fever 1

ABNORMAL FEVER IN THE
PEDIATRIC PATIENTLisa Allen PA-C ∙ Maine Coast Pediatrics ∙ Northern Light Maine Coast Hospital

LISA ALLEN PA-C
• Gordon College – Wenham, Massachusetts 1998-2002
• Mount Desert Island Hospital – Bar Harbor, ME 1999-2006
• University of New England – Portland Maine 2006-2008
• Maine Coast Pediatrics – Ellsworth Maine 2008-present
AFFILIATIONS
I have no affiliations to reveal

OUTLINE
• What is a fever?
• Fever with seizure activity
• Fever with no other symptoms
• Prolonged fever

HOW DOES ONE MEASURE A TEMPERATURE?
• “He felt warm when I kissed his forehead.” – The Mommy Test
• “She looked red and sweaty.”
• “I could feel he was burning up.”
• “I took her temp with one of those ear thingies.”
• “The school nurse sent her home because she had a fever of 99°F.”
• “I took his temp under his armpit and then added a degree.”
• “My daughter always runs low so a ‘normal’ temperature is a fever for her.”
• “I would never violate my child my putting that thing in his butt!”
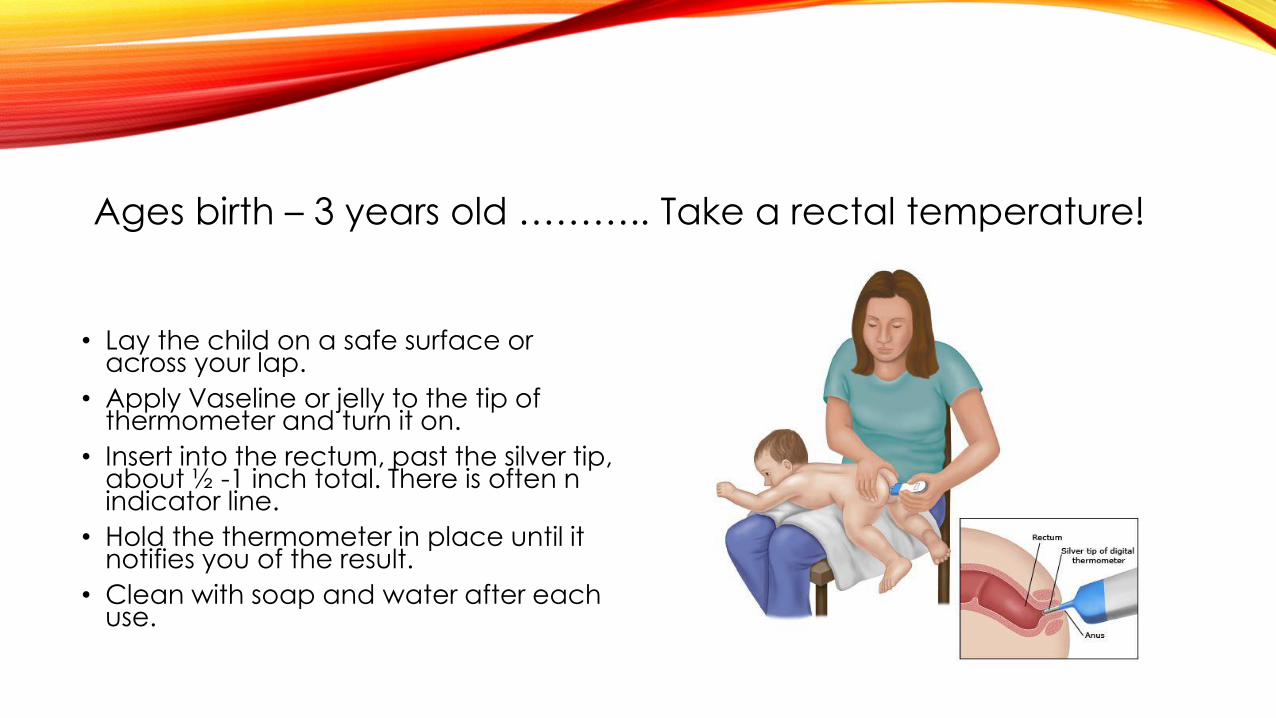
Ages birth – 3 years old ……….. Take a rectal temperature!
• Lay the child on a safe surface or across your lap.
• Apply Vaseline or jelly to the tip of thermometer and turn it on.
• Insert into the rectum, past the silver tip, about ½ -1 inch total. There is often n indicator line.
• Hold the thermometer in place until it notifies you of the result.
• Clean with soap and water after each use.

If the parents refuse a rectal temperature, you make take an axillary temperature.
• Lay the child on a safe surface.
• Turn on the thermometer.
• Place the thermometer in a dry armpit.
• Close the armpit by holding the elbow against the chest.
• Hold the thermometer in place until it notifies you of a result.
• Clean with soap and water after each use.

Ages 3 years and older – take an oral temperature.
• Have the child lay or sit on a safe surface.
• Turn on the thermometer.
• Place the thermometer under the tongue.
• Close the mouth with the thermometer remaining in place under the tongue.
• Hold the thermometer in place until it notifies you of a result.
• Clean with soap and water after each use.

If the parents refuse an oral temperature, or the patient is unable to comply, you make take an axillary temperature.
• Lay the child on a safe surface.
• Turn on the thermometer.
• Place the thermometer in a dry armpit.
• Close the armpit by holding the elbow against the chest.
• Hold the thermometer in place until it notifies you of a result.
• Clean with soap and water after each use.

WHAT IS A FEVER?
• In an infant ages birth – 2 months, a fever constitutes any temperature over:
100.4• In any child over age 2 months, a fever constitutes any temperature over:
100.7
SHOULD I TREAT THE FEVER??
• Leave it alone… the fever serves a purpose!
• Oh My God… her blood is going to boil!!
• Treat the fever if it is causing distress in the child.
• Body aches, headaches, belly pain
• Not eating or drinking well
• Fussy and uncomfortable
• Ibuprofen 10mg/kg every 6 hours
• Acetominophen 15mg/kg every 4 hours

FEVER IN THE NEONATE
Any child with a fever who is under 2 months old, needs a full septic workup. Please consult a pediatrician or send the patient to the emergency department.
• Labs (CBC, CRP, CMP, blood culture)
• Urinalysis
• Lumbar puncture
• CXR, EKG or other tests

LAST YEAR…
•Fever with upper respiratory symptoms
•Fever with gastrointestinal symptoms
•Fever with dermatological symptoms
•Fever with musculoskeletal symptoms

FEVER WITH SEIZURE
ACTIVITY
Occur in children ages 6 months – 5 years
Usually due to a combination of the developing neurological system in addition to a genetic susceptibility

FEBRILE SEIZURES
Multiple risk factors…
• Fever
• Due to the height of the fever, reaching a fever threshold?
• Due to the rate of rise of the fever?
• Viral infections
• Recent immunizations
• DTwP – no longer given
• MMR
• Family history of febrile seizures

FEBRILE SEIZURES
80% 20%
1/3 of patients will experience a recurrence of simple febrile seizures with another illness/fever

FEVER WITH NO OTHER
SYMPTOMS
FEVER WITH NO OTHER SYMPTOMS
• First 24 hours:• Perform a good exam• Check a urinalysis to rule out urinary tract infection
• After 48 hours:• Perform another good exam• Check labs including CBC, ESR, and CRP
• After 5 days:• Perform another good exam• Check labs including CBC, ESR and CRP• Order CXR• Order blood cultures
• Prolonged fever without symptoms: • Consult with infectious disease

FIRST 24 HOURS
• Perform a good exam
• Check the ears
• Check the throat
• Listen to the heart and lungs
• Examine the skin
• Examine the joints
• Check a urinalysis to rule out urinary tract infection

URINARY TRACT INFECTION
• This is a common hidden cause of fever in children, especially females
• Most often caused by e.coli (80%)
• Common in children who
• Are potty training
• Learning to wipe on their own
• Starting to bathe on their own

UTI
Treatment Recommendations
• Hospitalization and parental treatment if:• Ill or toxic appearing (concern for urosepsis)
• Less than 2 months old
• CVA tenderness, vomiting
• Immunodeficiency or known urinary abnormality
• Otherwise, oral antibiotics are necessary: • Amoxicillin 25-50mg/kg… but approximately 50% resistance rates!
• Second or Third generation cephalosporin… but expensive $$
• Sulfa… but monitor culture results due to increasing resistance
UTI
SCHOOL/DAYCARE
Urinary tract infections are not contagious. Therefore, there is no need to keep the child home unless they continue to have a fever or need additional supportive care.

AFTER 48 HOURS
• Perform another good exam
• Perform labs including:
• CBC with diff
• CRP and ESR

LABORATORY RESULTS
Bacteremia:
WBC ≥ 15
ANC ≥ 10
CRP ≥ 8
Viremia:
WBC < 15
ANC ≤ 10
CRP ≤ 2
↑ lymphs

ROSEOLA
• Caused by herpes virus 6 and 7
• AKA: Roseola infantum, Sixth disease, exanthem subitum
• Characterized by high fever, often with rapid spikes (and sometimes associated with febrile seizures), which last 1-4 days. Once fever resolves, it is then followed by the morbilliform rash.
• The rash blanches and will last around 48 hours.
ROSEOLA
Treatment Recommendations
• Ibuprofen and acetaminophen as needed for the fever.
• Once the rash appears, no treatment is needed.
• The rash rarely itches or causes any problems.
• It will resolve on its own within a couple of days.

ROSEOLA
SCHOOL/DAYCARE
Once the rash appears, the patient is no longer contagious! Therefore, they may return to school or daycare even with the rash.

INFLUENZA
• Most commonly seen in the winter months
• Characterized by cough, fever, tachypnea, retractions, hypoxemia
• Much higher morbidity in patients who are infants, have chronic disease (asthma, heart disease, diabetes), or are immuno-compromised (congenital, on chemo, JIA)
• Vaccines are available!!

INFLUENZA
Treatment Recommendations
• Consider oseltamivir (Tamiflu) 3mg/kg twice daily for 5 days in children who:• Are under 2 years of age
• Immunocompromised
• Have chronic disease
• Are hospitalized
• Start within 48 hours of symptoms developing
• Supportive treatment• Push fluids
• Ibuprofen and acetaminophen as needed for fever and discomfort

INFLUENZA
Prevention
• Influenza vaccine
• 2 doses, 1 month apart, when children receive the vaccine for the first time under age 8.
• After that, 1 dose per year (similar to adults)
• We recommend the injection over the intranasal preparation
INFLUENZA
SCHOOL/DAYCARE
Influenza is highly contagious. However, most children will have been exposed before the onset of symptoms. Therefore, exclusion is limited to those who continue to have fever or require additional care.

INFLUENZA

PEDIATRIC CANCER
ACUTE LMPYHOCYTIC LEUKEMIA
• The most common cause of childhood malignancy or cancer
• Accounts for 25% of all pediatric cancers; 5x more common than other cancers
• 2015: 41 cases per 1 million children

AFTER 5 DAYS
• Perform another good exam
• Repeat labs including CBC and CRP
• Order a chest xray
• Order blood cultures

LABORATORY RESULTS
Bacteremia:
WBC ≥ 15
ANC ≥ 10
CRP ≥ 8
Viremia:
WBC < 15
ANC ≤ 10
CRP ≤ 2
↑ lymphs

PROLONGED FEVER

GREATER THAN 7 DAYS
• Perform another good exam
• Repeat labs
• CONSULT WITH INFECTIOUS DISEASE SPECIALIST

PFAPA
• PFAPA = Periodic fever aphthous stomatitis, pharyngitis, and adenitis
• More than 3 documented episodes of fever, lasting no more than 7 days, occurring at regular intervals (usually 3-6 weeks)
• Pharyngitis but tender cervical lymphadenopathy or aphthous ulcers
• Normal laboratory studies in between episodes
• Otherwise normal growth and health
• Symptoms respond immediately to a single dose of prednisone 2mg/kg (max = 60mg)

KAWASAKI DISEASE• Characterized by high fever lasting greater than 5 days in addition to at least 4 of the
following:• Bilateral bulbar conjunctivitis• Oral mucosal changes (cracked lips, strawberry tongue)• Changes in the extremities (erythema, induration, periungual peeling) – often painful initially,
followed by desquamation• Exanthem – erythematous, diffuse, nonspecific maculopapular rash• Cervical lymphadenopathy

KAWASAKI DISEASE
• Treatment:
• High dose IV Ig
• High doses of aspirin… monitor for Reyes syndrome
• Management:
• Echocardiogram (at onset, 2 weeks, 6-8 weeks)
• Defer all live virus vaccines for 1 year
• Peak incidence in children age 9-11 months; rare under age 3 months
• Caused by ? (unknown)
• Monitor closely for
• Cardiac disease
• Arthritis and arthralgias
• Hepatic dysfunction
• Transient hearing loss
• Aseptic meningitis
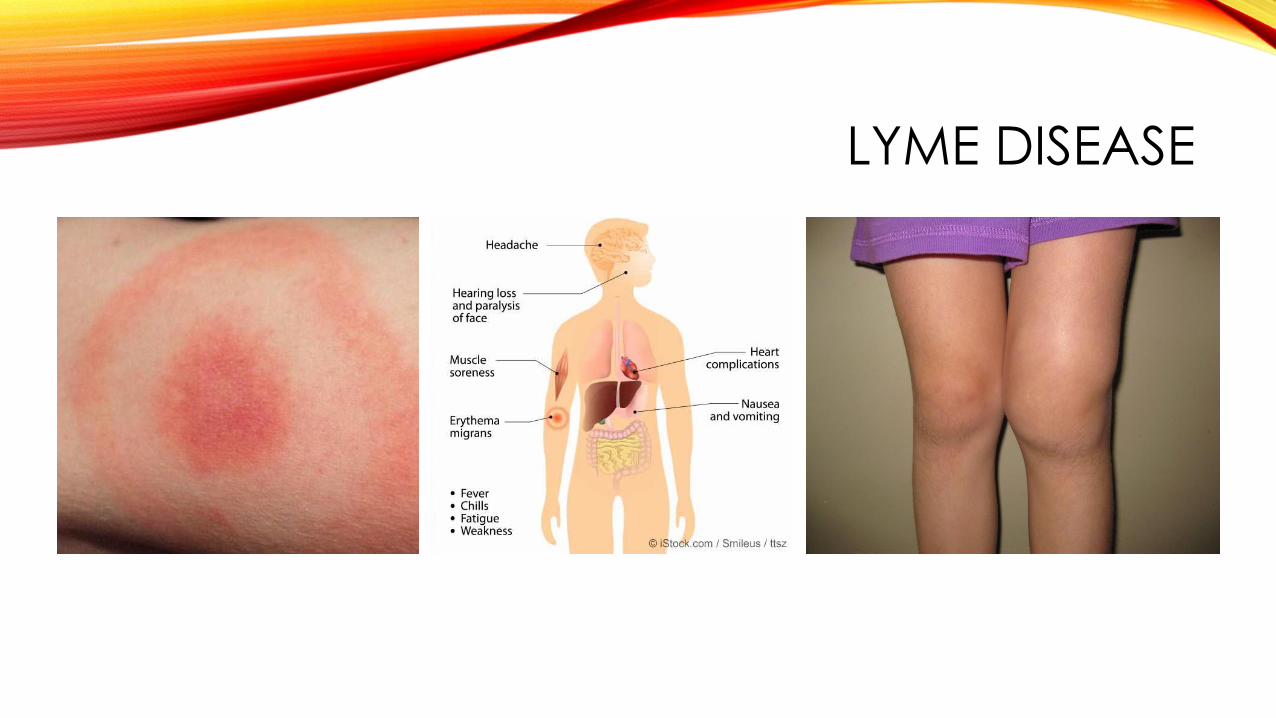
LYME DISEASE
• Caused by Borrelia bacteria which is spread through the bite of a deer tick
• Characterized by low grade fever with joint pain and swelling or erythema migrans rash
• Too much debate…
LYME DISEASE

LYME DISEASE
Treatment Recommendations
• Doxycycline 2mg/kg/dose (max = 100mg/dose) twice daily for 10-21 days
• Only recommended for children over age 8
• Amoxicillin 50mg/kg (max = 500mg/dose) divided BID for 10-21 days
• Is testing necessary?
• Is ongoing antibiotic use necessary?
LYME DISEASE
SCHOOL/DAYCARE
There is no concern that lyme disease is contagious from person to person. Therefore, the child may immediately return to daycare or school.

CASE PRESENTATION

THANK YOU!!