abm final presentation
25
Vertebral Implants Submitted by : Goutham Chinni (K474R658) Gopi Krishna Mandadi(K353X443) Shravani Kasaragadda (W268D427)
-
Upload
gopi-krishna-mandadi -
Category
Documents
-
view
125 -
download
4
Transcript of abm final presentation

Vertebral Implants
Submitted by :Goutham Chinni (K474R658)Gopi Krishna Mandadi(K353X443)Shravani Kasaragadda (W268D427)

• Back pain is that the second most typical reason for medical practitioner visits within the US, and affects up to 84 % of patients at some purpose in their lives. For several patients, neck and back pain is usually thanks to injury or spinal instability through trauma, unwellness or degeneration. This will cause impingement of neural structures leading to pain, numbness, or weakness
3 Joint Complex

Spinal Stability Spinal stability refers to the power of the spine phase to limit
excessive displacement that may presumably lead to disabling deformity or medicine symptoms because of impingement on the neural structure and nerve roots. Factors that {may} contribute to instability may have an effect on the bones, disc, joints, or ligaments. These embrace trauma, tumors, infections, inflammatory diseases, animal tissue disorders, inherent disorders and chronic disorders

Vertebral instrumentation Vertebral instrumentation is intended to stabilize the spine and
forestall excessive motion at the affected phase because the bones fuse along. It provides immediate stability of the affected phase of the spine and obviates the necessity for external fixation devices like rigid collars, braces, and halo traction. This enables for a larger quality of life for patients in real time following surgery. These internal fixation devices like screws, plates, associate degreed rods area unit mounted to the bone bodies and mix to make an instrumentation construct

• Modern spinal fixation devices are manufactured from biocompatible metallic alloys like chrome steel and metal. Whereas these became standard because of their strength and fatigue resistance, they possess radiographic challenges and biomechanical limitations. First and foremost, metallic materials area unit radio logically problematic. Artifacts created by metals in computerized tomography (CT) and magnetic resonance (MR) imaging, also as obfuscation of bone by metals in tabular x-rays, inhibit visual image of latest bone growth so, creating it tough for physicians to assess progression of arthrodesis. Second, implants that area unit stiffer than natural bone area unit subject to alleged stress shielding. When 2 bones area unit coalesced along, the state of compressive forces between them determines the extent of modeling or transforming

• According to Wolff’s law, bone apposition among a fusion graft is ruled partially by the state of compressive stresses among it. Because of this it's been projected that stiff metallic implants could protect the graft from the strain needed for fusion, delaying or preventing the method. This may induce induced effects like device-related osteopenia, intervertebral device protrusion into a neighboring vertebral body, and fracture or instability. Implants developed out of less stiff materials could stop this stress shielding and foster higher clinical outcomes compared to ancient devices
Planar X-ray of Patient Immediately after Surgery with PEEK Cage and Titanium Rod Construct Implanted in the Lumbar Spine

Intra-Vertebral Implants• The purpose of this implant is to
support and stabilize the spinal column in cases of total or partial vertebroctomy. The adaptive geometry of the implant will be adjusted to varied anatomies. The length of the implant will be modified once the implant was set in situ by a special tool permitting its two parts to maneuver vertically with relation to one another. The area between the highest and also the bottom plates will be full of segments of bone which will grow and fuse the highest and also the bottom bone. One of the most expected advantages from customizing end plate geometry of bone implants is that the reduced risk and potential for subsidence into the bone end plate
Intra Vertebral Implants

• Coating of Metallic Implants with SCPC Bioactive Ceramic:• Coating orthopedic implants with bioactive ceramics has the potential to
boost material-tissue integration and supply higher fixation of the device. SCPC has been coated on Ti-6Al-4V yet as Co-Cr alloys exploitation action deposition (EPD) technique. SEM image of SCPC coating on Ti-6Al-4V foam bone implant. (Left) SCPC Nano-particles uniformly coated the outer surface as well because the entire thickness of the porous implant. (Right)Cross-section analysis showed that SCPC coating forms an identical coating thickness 3-5 millimeter (arrow) over the inner surfaces of the Ti alloy foam disc
SEM image of SCPC coating

• First-ever 3D-printed vertebra implanted in 12-year-old cancer patient’s spine (A Recent
Invention at Peking University). https://www.youtube.com/watch?v=83ytVGxcWl8
• - Review:
• BEIJING – A 12-year-old cancer patient in China underwent a first-of-its-kind operation to implant a 3D-printed vertebra into his spine, Reuters reported
• During the 5-hour procedure, surgeons at Peking University Hospital in Beijing removed a tumor from Qin Minglin’s spine before implanting the 3D-printed vertebra. The novel device was made from titanium powder and included a series of tiny pores which will allow the bone to grow and bond to the structure as it heals.

Currently, the standard procedure for this kind of operation involves removing the bone and inserting a titanium tube held in place by screws and surgical cement. However, the tube can become detached over time. For this surgical procedure, doctors used a combination of scans and specialized engineering software to create a perfect replica of the piece of the patient’s spine that needed to be replaced.We can use iconographic tests on patients such as a computed [tomography], or CT scans, and convert the CT data into 3D-printing data in order to produce an internal fixation with exactly the same structure as the patient's bone structure
3D Vertebra

Material Considerations
• Generally, biomaterials used in vertebral Implant can be classified in three groups: Metals, ceramics and polymers. Ideally, material properties of the implants should have a low elastic modulus close to cortical bone, high wear resistance, high corrosion resistance, high fracture toughness and high ductility.
• In the last century, Vertebral Implants were mainly manufactured of metal alloys such as stainless steel, pure Titanium and Titanium-aluminum-vanadium. In recent years, developments in the field of non-metallic biomaterials lead to the application of new materials such as PEEK and composite materials. Before Implanting, the physical characteristics of the material must be observed.
Resorbable Plate and Screw System beside Nonresorbable titanium system

Physical Characteristics of the Implants
Strength:
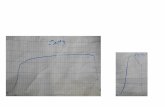
• The ability of the Material to withstand an applied stress is called strength. Yield strength
refers to the point in the stress strain curve after which plastic deformation occurs. Strength
of a material may vary with the stress (compressive, tensile or shear) applied. For most
vertebral Implants fatigue strength is the most relevant criteria, as it refers material ability to
withstand alternating stresses under cyclic loading. This is especially important during the
daily routine of the patient. Strength of a metallic material is depending on its microstructure
and can be altered in the fabrication process (Casting, Forging, Annealing etc.)
Flexibility: Elastic Modulus
• The Elastic modulus describes the magnitude at which a material deforms when subjected to
stress. It is determined from the linear slope of a stress-versus-strain curve. In order to
minimize stress shielding, the elastic modulus of implants should be in the range of cortical
bone.

• Corrosion Resistance: Degradation of materials into its constituent atoms caused by electrochemical reactions
with its surroundings is called Corrosion. The human body fluids present a very hostile environment to metals making corrosion resistance an important aspect in the biocompatibility of a material. The occurrence of small holes in the surface due to break-up of the corrosion resistant oxide film is called Pitting Corrosion. Crevice corrosion can occur in rod/screw or plate/screw connections of vertebral instrumentation through development of corrosion, while galvanic corrosion results from two different metals with different electrode potentials and body fluid forming a voltage cell.
• Wear Resistance: Relative motion between surfaces in contact causes erosion of the material called wear. In
contrast to Corrosion, wear is produced by a mechanical action in form of contact and motion causing the removal of small particles from a surface. Wear debris can induce inflammatory reaction causing local bone loss and threatening implant fixation. Generally, the amount of wear increases with the applied load and decreases with the hardness of the worn surface.
• Biocompatibility: Generally, biocompatibility is defined as the ability of a material to perform with an
appropriate host response in a specific application. For Implants, this can be interpreted as the property of being biologically compatible by not producing a toxic, injurious or immunological response in the human body.

Materials used in Vertebral Implants:
• The bulk of Orthopedic implants used for skeletal reconstructions (E.g., plates, screws, rods and joint
replacements) are manufactured of metallic biomaterials. This is due to their ability to withstand high
and also dynamic loads. In order to improve implant fixation and/or cell ingrowth, the anchoring
surfaces can be roughened, precoated or refined with porous coatings.
• An excerpt of material properties of commonly used Implant materials and its comparision to cortical
bone is listed in the below table.

Metals and their usage as Implants
1. Metals:• The majority of Implants used in vertebral Instrumentation (screws,
rods, hooks, vertebral body replacements,etc.) are manufactured of metallic materials. They provide high tensile, compressive, shear and fatigue strength, biocompatibility, corrosion and wear resistance required in the application of load bearing implants in orthopedic surgery. Flexibility and strength of a metallic alloy also depends on the fabrication processes (casting, cold and hot forging). After fabrication, the material properties can be enhanced by heat treatment (annealing). Wear resistance can be further improved by processes such as nitriding and Ion Implantation.

Contd..
1.1 Stainless steel:• The most commonly used Stainless steel is 316L (ASTM
F138, F139). It is composed of iron, carbon, chromium, nickel and molybdenum .while the carbon content is kept low, the alloying additions improve the corrosion resistance. While stainless steel has been and is used in fracture plates, pedicle instrumentation and screws, a trend towards Titanium (Ti)-based implants due to the superior biocompatibility was seen in recent years. However, stainless steel implants still gain a worldwide popularity due its cost-effectiveness compared to Ti-based alloys.

1.2 Cobalt Chromium Alloys:• The most commonly used cobalt-chromium alloys are cobalt-nickel-chromium-molybdenum • (CoNiCrMo, ASTM F562) and cobalt-chromium-molybdenum (CoCrMo, ASTM F75). While Chromium improves
the corrosion resistance, molybdenum increases the strength and make it strong, hard, biocompatible and corrosion resistant. Due to these characteristics, it is used in joint replacements and fracture stabilisations requiring a long service life. However, the high percentage of nickel in CoNiCrMo raises concerns of possible toxicity by wear particles.
1.3 Titanium Alloys:• The increased biocompatibility and corrosion resistance of titanium-alloys compared to stainless steel and CoCr alloys
is attributed to a stable oxide film protecting it from corrosion. The elastic modulus of titanium alloys is closer to bone and approximately half of stainless steel and CoCr alloys, while their strength generally exceeds that of stainless steel. Due to the lower resistance to wear compared to CoCr alloys, Ti-alloys are hardly applied as bearing material.
• An advantage of Ti-based alloys is their feature to produce fewer artefacts in computer tomography (CT) and magnetic resonance imaging (MRI) scans.
2. Ceramics:• Ceramics are characterized by a high wear resistance, low friction and good compatibility, but also reduced fracture
toughness. Therefore, they are mainly used for bearing surfaces in joint replacements. The most commonly used ceramics are hydroxyapatite and glass ceramics, zirconia (ZrO2) and Alumina (Al2O3) in the form of implant coatings.
3. Polymers:• Generally, considering all types of medical applications, polymers from the largest group of biomaterials. For
polymers used in orthopaedic implants, the most important characteristics for choosing a specific polymer are yield stress, wear rate and creep resistance.
3.1 Polyethylene (PE):• Low friction coefficient, low wear rate and resistance to creep of PE in the form ultra-high molecular weight
polyethylene (UHMWPE) are the reasons for PE being the most common bearing material in total joint anthroplasty (TJA).

Results & Discussions

Results
• Individuals suffering from spinal fractures—caused by osteoporosis or weakened bones—now have another option to reduce pain, restore function and improve quality of life, according to a study of 300 patients treated with a new type of vertebral augmentation.
• Made of medical polymer, the implant is designed to treat painful and debilitating vertebral compression fractures, which cause the bones in the spine to collapse and, left untreated, can lead to pain and a condition called kyphosis (or a curvature of the spine). Recently cleared by the U.S. Food and Drug Administration (FDA), the implant provides a new treatment alternative to vertebroplasty and kyphoplasty, the current standards of care.
• Kiva System as a Vertebral Augmentation Treatment—A Safety and Effectiveness Trial (KAST) was a study conducted with FDA approval in which 153 patients with one or two painful osteoporotic vertebral compression fractures received the new implant and 147 had balloon kyphoplasty.

Contd… • Patients were treated at one of 21 centers in the United States,
Canada, Belgium, France and Germany and were followed for one year. Results of the study confirmed that the implant provided essentially the same amount of pain relief and improvement in daily function based on accepted measures for pain and function (visual analogue score, VAS; Oswestry Disability Index, ODI) and safety.
• Researchers also found patients who had the implant were more likely to benefit from a reduction in the angle of the kyphosis and less likely to have the bone cement leak.
• Moreover, the study showed a clinically important trend in that the implant patients were less likely to suffer a fracture in adjacent vertebra.

Advantages to Vertebral Stimulation Treatment
• There are many advantages to spinal cord or peripheral nerve field stimulation for the treatment of chronic back pain
• A trial can test patient response before the patient commits to a permanent implant.• It has few side effects and is easily reversible; if it doesn’t work or is no longer
needed it can be removed.• Implantation of the system is minimally invasive, requiring a relatively minor surgical
procedure on an outpatient basis.• Leads are inserted just under the skin, and patients can travel anywhere, and
participate in any recreational activities, including swimming.• Achieving pain relief with spinal cord stimulation or peripheral nerve field stimulation
can allow patients to reduce or eliminate their use of narcotic drugs.• Ongoing advances in neurostimulator technology give patients more control to adjust
the stimulation if their pain changes in location or severity.• Continual improvements in the design of electrodes and longer lasting, rechargeable
batteries mean that implantable systems can be placed in locations to give optimal and more efficient pain control than other modalities.

Disadvantages of Spinal Cord Stimulation• As with any chronic pain treatment, there are also a number of potential
disadvantages with spinal cord stimulation, including:• Spinal cord stimulation does not work for everyone. Most studies show that
50% to 60% of people find meaningful pain relief with spinal cord stimulation.
• It does not eliminate the pain. A successful outcome of spinal cord stimulation is considered to be pain relief of 50% or more.
• Spinal cord stimulation does not address the source of the pain. The system is designed to interrupt pain signals being sent to the brain, but it does not correct any underlying anatomical problem. For many people with chronic pain, this is the right approach to treatment. However, for those with a correctable anatomic lesion, treatments to address the source of the pain should be tried first.
• The treatment involves an implant and surgery. As with any surgical procedure and implant, there are certain risks and potential complications associated with spinal cord stimulation and peripheral nerve field stimulation, discussed below.

Future Work (A study from Journal) • This biocompatible composite
material, with endless fiber content over 60% of volume, distinguishes itself with its excellence mechanical strength and its fatigue resistance.
• The well-known spinal expert, Professor Friedrich Magrel, developed both implants through extensive research at icotec.
• He used the first composite implants to execute his ideas and obtain the assumed product standards that are developing as orthopedic and neurosurgeons discover the main advantages of composites. Standard Titanium plants that are tend to fatigue problems are still being replaced in some areas by biocompatible thermoplastic composites..

References• Kulkarni, R. K., E. G. Moore, et al. (1971). "Biodegradable poly(lactic acid) polymers." J Biomed Mater Res
5(3): 169-81.• Kulkarni, R. K., K. C. Pani, et al. (1966). "Polylactic acid for surgical implants." Arch Surg 93(5): 839-43.• Kurtz, S. M. and J. N. Devine (2007). "PEEK biomaterials in trauma, orthopedic, and spinal implants."
Biomaterials 28(32): 4845-69.• Lippman, C. R., M. Hajjar, et al. (2004). "Cervical spine fusion with bioabsorbable cages."Neurosurg Focus
16(3): E4.• Lyons, A. S., B. P. Sherman, et al. (2011). "Failure of resorbable plates and screws in an ovine model of
anterior cervical discectomy and fusion." Spine J 11(9): 876-83.Majola, A., S. Vainionpaa, et al. (1992). "Intramedullary fixation of cortical bone osteotomies with self-reinforced polylactic rods in rabbits." IntOrthop 16(1): 101-8.
• Mayberry, J. C., J. T. Terhes, et al. (2003). "Absorbable plates for rib fracture repair: preliminary experience." J Trauma 55(5): 835-9.
• Panagiotacopulos, N. D., M. H. Pope, et al. (1987). "Water content in human intervertebral discs. Part II. Viscoelastic behavior." Spine (Phila Pa 1976) 12(9): 918-24.
• Smit, T. H., T. A. Engels, et al. (2010). "Time-dependent failure in load-bearing polymers: a potential hazard in structural applications of polylactides." J Mater Sci Mater Med 21(3): 871-8.
• Smit, T. H., T. A. Engels, et al. (2008). "Time-dependent mechanical strength of 70/30 Poly(L, DL-lactide): shedding light on the premature failure of degradable spinal cages." Spine (Phila Pa 1976) 33(1): 14-8.
• Smith, A. J., M. Arginteanu, et al. (2010). "Increased incidence of cage migration and nonunion in instrumented transforaminal lumbar interbody fusion with bioabsorbable cages." J Neurosurg Spine 13(3): 388-93.

• Springer, M. A., E. A. van Binsbergen, et al. (1998)."[Resorbable rods and screws for fixation of ankle fractures.A randomized clinical prospective study]."Unfallchirurg 101(5):377-81.
• Thomas, K. A., J. M. Toth, et al. (2008). "Bioresorbablepolylactideinterbody implants in an ovine anterior cervical discectomy and fusion model: three-year results." Spine (Phila Pa 1976) 33(7): 734-42.
• Tomasino, A., H. Gebhard, et al. (2009). "Bioabsorbable instrumentation for single-levelcervical degenerative disc disease: a radiological and clinical outcome study." J Neurosurg
• Toth, J. M., B. T. Estes, et al. (2002). "Evaluation of 70/30 poly (L-lactide-co-D,L-lactide) for use as a resorbableinterbody fusion cage." J Neurosurg 97(4 Suppl): 423-32.
• Vaccaro, A. R., J. A. Carrino, et al. (2002). "Use of a bioabsorbable anterior cervical plate in the treatment of cervical degenerative and traumatic disc disruption." J Neurosurg 97(4 Suppl): 473-80.
• vanManen, C. J., M. L. Dekker, et al. (2008). "Bio-resorbable versus metal implants in wrist fractures: a randomised trial." Arch Orthop Trauma Surg 128(12): 1413-7.
• Wang, M. Y., A. D. Levi, et al. (2002). "Polylactic acid mesh reconstruction of the anterior iliac crest after bone harvesting reduces early postoperative pain after anterior cervical fusion surgery." Neurosurgery 51(2): 413-6; discussion 416.
• Welch, W. C., K. A. Thomas, et al. (2002). "Use of polylactideresorbable film as an adhesion barrier." J Neurosurg 97(4 Suppl): 413-22.
• White, A. and M. Panjabi (1990).Clinical Biomechanics of the Spine. Philadelphia, Lippincott.• Yong-Hing, K. and W. H. Kirkaldy-Willis (1983)."The pathophysiology of degenerative disease of the
lumbar spine."OrthopClin North Am 14(3): 491-504.• Yong-Hing, K., J. Reilly, et al. (1980). "Prevention of nerve root adhesions after laminectomy." Spine (Phila
Pa 1976) 5(1): 59-64.
• WEBSITES• http://www.foxnews.com/health/2014/08/28/first-ever-3d-printed-vertebra-implanted-in-12-year-old-cancer-
patients-spine/• http://www.jeccomposites.com/news/composites-news/new-generation-spinal-implants-launched• http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2200680/