
Relationship between deep subcutaneous abdominal adipose ...

ABDOMINAL WALLS AND INGUINAL REGION Dr. Milton M. Sholley
SUGGESTED READING
Essential Clinical Anatomy 3 rd ed. (ECA): pp. 118132 Head to Toe Questions in Gross Anatomy: Begin questions #607756.
OBJECTIVE
This lecture is designed to provide the student with a thorough understanding of the gross structure of the anterolateral abdominal wall and an introduction to the inguinal region.
LECTURE OUTLINE
I. Definition of region: In general the abdomen is that region of the body bounded above by the diaphragm and below by the plane of the pelvic inlet (the plane bounded by the sacral promontory, arcuate lines, pectineal lines, and pubic symphysis).
II. Landmarks on the anterior abdominal wall
A. Umbilicus lies in the anterior midline at vertebral level L3L4 (lower in obese people)
B. Three vertical lines are related to the rectus abdominis muscles:
1. The linea alba is a median line formed by the fusion of several layers of aponeuroses between the two rectus abdominis muscles. Surgical incisions through the linea alba provide extensive access to the abdominal cavity, are relatively bloodless, but may result in weakening of the abdominal wall.
2. The two linea semilunaris are located lateral to the two rectus muscles.
C. For clinical description, the abdominal surface may be subdivided in two ways:
Midline
Transumbilical line
Right upper quadrant
Left upper quadrant
Right lower quadrant
Left lower quadrant
Costal arch
Intertubercular line
Transpyloric line
Midclavicular lines
Epigastric region
Umbilical
region
Hypogastric region Inguinal
ligament
1. Quadrants formed by a median vertical line (midline) and a transverse line through the umbilicus

2. Nine regions formed by the two midclavicular lines, which run vertically and intersect the midpoints of the inguinal ligaments, a transversely oriented transpyloric line, and a transversely oriented intertubercular line (connecting the anterior tubercles of the iliac crests) and named according to the scheme in the following table:
Nine regions
right hypochondriac epigastric left hypochondriac right lumbar umbilical left lumbar right inguinal hypogastric left inguinal
III. Superficial structures
A. Langer's Lines are lines of tension within the skin. In the abdominal region these lines of tension run in a basically horizontal direction. Thus, horizontal surgical incisions through the abdominal skin lie parallel to the tension lines and tend to provide a better cosmetic result when healed than vertical incisions.
B. Two strata of subcutaneous connective tissue (superficial fascia) are present on the lower abdominal wall. These layers have specific connections, boundaries, and specializations to be described in the lecture.
1. A superficial fatty layer (Camper's fascia)
2. A deeper membranous layer (Scarpa's fascia)
3. The deeper membranous layer continues into the perineal region (Colles' fascia)
C. Cutaneous nerves. (Their main trunks lie between the internal oblique and transversus abdominis muscles, but their superficial branches supply dermatomes on the abdominal wall.)
1. Intercostal nerves T7T11 (T10 supplies the dermatome that crosses the umbilicus.)
2. Subcostal nerve (T12)
3. Iliohypogastric nerve (T12 & L1)
4. Ilioinguinal nerve (L1) (Supplies the pubic region, anterior scrotum or labia majora, and a patch of skin on the anterior thigh.)

D. Cutaneous blood vessels
1. 10th and 11th intercostal arteries
2. Subcostal artery
3. Musculophrenic and superior epigastric arteries
4. Inferior epigastric artery
5. Three branches from the femoral artery, namely the:
a. Superficial epigastric artery
b. Superficial circumflex iliac artery
c. Superficial external pudendal artery
E. Cutaneous lymphatics
1. Above the umbilicus the lymph vessels drain into sternal, pectoral and axillary nodes of their respective sides.
2. Below the umbilicus the lymph vessels drain into superficial inguinal nodes of their respective sides.
IV. Abdominal wall muscles and their specializations
A. External abdominal oblique (see muscle chart)
The aponeurosis of the external abdominal oblique muscle contains an opening (superficial inguinal ring) traversed by the spermatic cord (male) or the round ligament of the uterus (female). Additionally, the aponeurosis has the following specializations:
1. The inguinal ligament, which is the inferior, rolledunder border of the aponeurosis and spans the gap between the anterior superior iliac spine (ASIS) and the pubic tubercle.
2. The lacunar ligament, which represents the more medial rolled under fibers of the inguinal ligament and attaches to the medial end of the pectineal line.
3. The pectineal ligament, which is a more lateral continuation of fibers from the lacunar ligament and runs parallel to the pectineal line.

Pubic tubercle
Inguinal ligament
ASIS Superficial inguinal ring
Lacunar ligament
Pectineal ligament
Femoral ring
See Grant's Atlas: 12 th Ed. Fig. 5.17B, page 372
4. The reflected inguinal ligament, which is a minor extension of the inguinal ligament from the pubic tubercle upward to the linea alba.
5. The medial and lateral crura and intercrural fibers:
a. The medial crus forms the superomedial margin of the superficial inguinal ring.
b. The lateral crus forms the inferior margin of the superficial inguinal ring.
c. The intercrural fibers form the superolateral margin of the superficial inguinal ring.
6. The external spermatic fascia, which is a thin fascial continuation of the external abdominal oblique aponeurosis from the edges of the superficial inguinal ring onto and investing the spermatic cord.
B. Internal abdominal oblique (see muscle chart)
1. It ends in an aponeurosis at the linea semilunaris.
2. In the upper 3/4 of the abdomen the aponeurosis splits and passes around both sides of the rectus abdominis muscle.
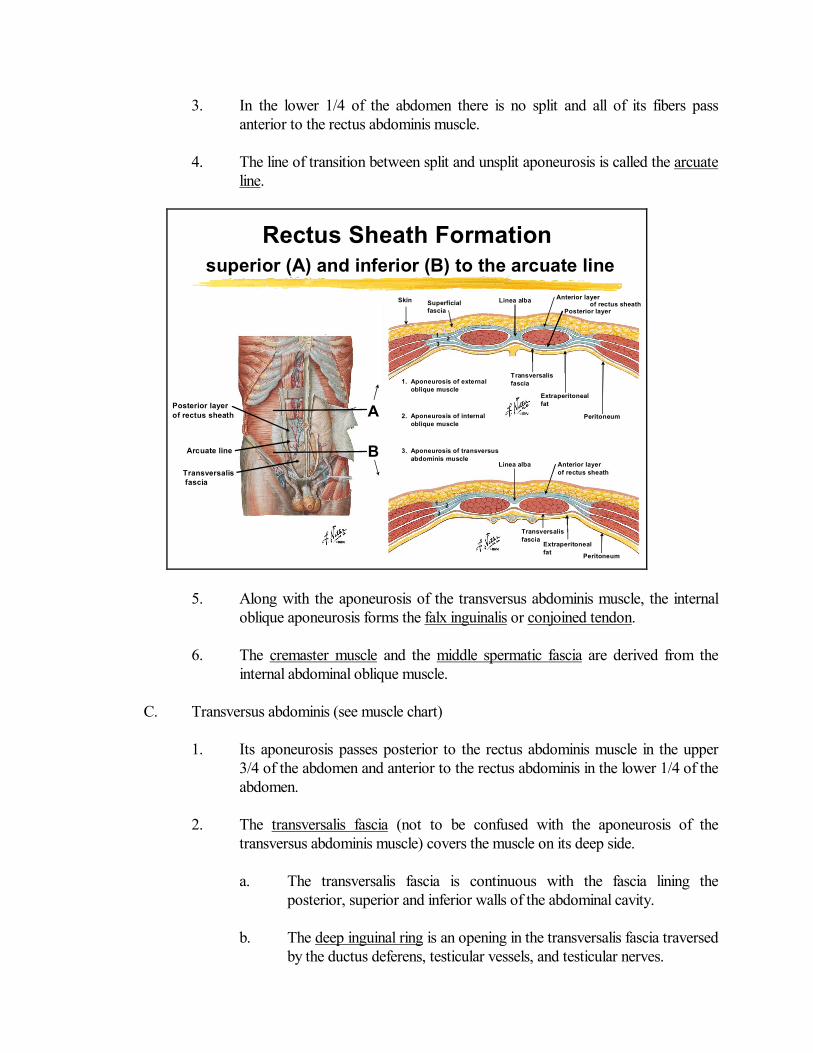
3. In the lower 1/4 of the abdomen there is no split and all of its fibers pass anterior to the rectus abdominis muscle.
4. The line of transition between split and unsplit aponeurosis is called the arcuate line.
Posterior layer of rectus sheath
Arcuate line
Transversalis fascia
A
B
Rectus Sheath Formation superior (A) and inferior (B) to the arcuate line
Linea alba
Anterior layer of rectus sheath
Linea alba
Posterior layer
Anterior layer of rectus sheath
Transversalis fascia
Peritoneum
Extraperitoneal fat
Transversalis fascia
Peritoneum
Extraperitoneal fat
1. Aponeurosis of external oblique muscle
2. Aponeurosis of internal oblique muscle
3. Aponeurosis of transversus abdominis muscle
1 2 3
1 2 3
Skin Superficial fascia
5. Along with the aponeurosis of the transversus abdominis muscle, the internal oblique aponeurosis forms the falx inguinalis or conjoined tendon.
6. The cremaster muscle and the middle spermatic fascia are derived from the internal abdominal oblique muscle.
C. Transversus abdominis (see muscle chart)
1. Its aponeurosis passes posterior to the rectus abdominis muscle in the upper 3/4 of the abdomen and anterior to the rectus abdominis in the lower 1/4 of the abdomen.
2. The transversalis fascia (not to be confused with the aponeurosis of the transversus abdominis muscle) covers the muscle on its deep side.
a. The transversalis fascia is continuous with the fascia lining the posterior, superior and inferior walls of the abdominal cavity.
b. The deep inguinal ring is an opening in the transversalis fascia traversed by the ductus deferens, testicular vessels, and testicular nerves.

c. The internal spermatic fascia is derived from the transversalis fascia at the margins of the deep inguinal ring.
D. Rectus abdominis (see muscle chart)
1. Two long vertical muscles, lying on either side of the linea alba
2. Each muscle is surrounded by a rectus sheath (see the previous figure), formed by various layers of the aponeuroses of the three flat muscles.
E. Pyramidalis muscle (see muscle chart)
1. It is frequently absent.
2. When present, it lies anterior to the inferior end of the rectus abdominis muscle, inside the rectus sheath.
V. Inguinal canal
The inguinal canal is a passageway through the inferior part of the anterior abdominal wall for the spermatic cord in the male and the round ligament of the uterus in the female.
A. Boundaries of the inguinal canal (refer to the diagrams on the next page):
1. Anterior wall
a. External oblique aponeurosis over the entire length of the canal
b. Internal oblique muscle on the lateral onethird
2. Posterior wall
a. Transversalis fascia over the entire length
b. Falx inguinalis (conjoined tendon) on the medial onethird
c. Reflected inguinal ligament on the medial onethird

3. Roof
a. Arched fibers of transversus abdominis muscle over the lateral one third
b. Arched fibers of internal oblique and transversus abdominis over the middle and medial onethirds
4. Floor
a. Inguinal ligament along the entire length
b. Lacunar ligament also along the medial onethird
Boundaries of the Inguinal Canal
B. The inguinal canal in the male is a passageway for the spermatic cord, which contains the following structures wrapped within the internal spermatic fascia:
1. Ductus (vas) deferens
2. Deferential artery and vein
3. Testicular artery
4. Pampiniform plexus of veins
5. Lymphatics
6. Autonomic nerves of the testis
These diagrams are from A Textbook of Human Anatomy (1 st ed.) by Roger C. Crafts. They represent cross sections of the inguinal canal itself, but would be parasagittal sections with regard to the whole body.

C. Also traversing all or part of the inguinal canal are the:
1. Ilioinguinal nerve
2. Genital branch of the genitofemoral nerve
IV. Posterior abdominal wall
A. Diaphragm
B. Quadratus lumborum muscle (see muscle chart)
C. Psoas major muscle (see muscle chart)


















