Abdominal emergencies during pregnancy · PDF fileAbdominal emergencies during pregnancy S107...
11
Journal of Visceral Surgery (2015) 152, S105—S115 Available online at ScienceDirect www.sciencedirect.com REVIEW Abdominal emergencies during pregnancy J. Bouyou a , S. Gaujoux a,b , L. Marcellin b,c,e , M. Leconte a,b , F. Goffinet b,d,e , C. Chapron b,c , B. Dousset a,b,∗ a Service de chirurgie digestive, hépatobiliaire et endocrinienne, Hôpital Cochin, AP-HP, Paris, France b Faculté de médecine, Université Paris Descartes, Sorbonne Paris Cité, Paris, France c Département de gynécologie-obstétrique II et médecine de la reproduction, Hôpital Cochin-Port Royal, AP-HP, Paris, France d Maternité, Hôpital Cochin-Port Royal, Paris, France e DHU Risques et Grossesse, Université Paris Descartes, Paris, France Available online 30 October 2015 KEYWORDS Abdominal emergency; Surgery; Pregnancy; Laparoscopy Summary Abdominal emergencies during pregnancy (excluding obstetrical emergencies) occur in one out of 500—700 pregnancies and may involve gastrointestinal, gynecologic, uro- logic, vascular and traumatic etiologies; surgery is necessary in 0.2—2% of cases. Since these emergencies are relatively rare, patients should be referred to specialized centers where sur- gical, obstetrical and neonatal cares are available, particularly because surgical intervention increases the risk of premature labor. Clinical presentations may be atypical and misleading because of pregnancy-associated anatomical and physiologic alterations, which often result in diagnostic uncertainty and therapeutic delay with increased risks of maternal and infant morbidity. The most common abdominal emergencies are acute appendicitis (best treated by laparoscopic appendectomy), acute calculous cholecystitis (best treated by laparoscopic chole- cystectomy from the first trimester through the early part of the third trimester) and intestinal obstruction (where medical treatment is the first-line approach, just as in the non-pregnant patient). Acute pancreatitis is rare, usually resulting from trans-ampullary passage of gall- stones; it usually resolves with medical treatment but an elevated risk of recurrent episodes justifies laparoscopic cholecystectomy in the 2nd trimester and endoscopic sphincterotomy in the 3rd trimester. The aim of the present work is to review pregnancy-induced anatomical and physiological modifications, to describe the main abdominal emergencies during pregnancy, their specific features and their diagnostic and therapeutic management. © 2015 Published by Elsevier Masson SAS. Abbreviation: ALP, after last period. ∗ Corresponding author at: AP—HP, Groupe Hospitalier Universitaire Ouest, CHU Cochin Broca Hôtel-Dieu, Service de chirurgie digestive, hépatobiliaire et endocrinienne, 27, rue du Faubourg-Saint-Jacques, 75014 Paris, France. E-mail address: [email protected] (B. Dousset). http://dx.doi.org/10.1016/j.jviscsurg.2015.09.017 1878-7886/© 2015 Published by Elsevier Masson SAS. Downloaded from ClinicalKey.com at National Certification Corporation July 25, 2016. For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.
Transcript of Abdominal emergencies during pregnancy · PDF fileAbdominal emergencies during pregnancy S107...

Journal of Visceral Surgery (2015) 152, S105—S115
Available online at
ScienceDirectwww.sciencedirect.com
REVIEW
Abdominal emergencies during pregnancy
J. Bouyoua, S. Gaujouxa,b, L. Marcellinb,c,e,M. Lecontea,b, F. Goffinetb,d,e, C. Chapronb,c,B. Dousseta,b,∗
a Service de chirurgie digestive, hépatobiliaire et endocrinienne, Hôpital Cochin,AP-HP, Paris, Franceb Faculté de médecine, Université Paris Descartes, Sorbonne Paris Cité, Paris, Francec Département de gynécologie-obstétrique II et médecine de la reproduction,Hôpital Cochin-Port Royal, AP-HP, Paris, Franced Maternité, Hôpital Cochin-Port Royal, Paris, Francee DHU Risques et Grossesse, Université Paris Descartes, Paris, France
Available online 30 October 201
KEYWORDSAbdominalemergency;Surgery;Pregnancy;Laparoscopy
Summary Abdominal emergeoccur in one out of 500—700 prlogic, vascular and traumatic etemergencies are relatively rare,gical, obstetrical and neonatal
increases the risk of prematurebecause of pregnancy-associatein diagnostic uncertainty and thmorbidity. The most common ablaparoscopic appendectomy), accystectomy from the first trimesobstruction (where medical treapatient). Acute pancreatitis is
stones; it usually resolves with
justifies laparoscopic cholecystethe 3rd trimester. The aim of thphysiological modifications, to
their specific features and their
© 2015 Published by Elsevier Ma
Abbreviation: ALP, after last period.∗ Corresponding author at: AP—HP, Groupe Hospitalier Universitaire Ou
hépatobiliaire et endocrinienne, 27, rue du Faubourg-Saint-Jacques, 750E-mail address: [email protected] (B. Dousset).
http://dx.doi.org/10.1016/j.jviscsurg.2015.09.0171878-7886/© 2015 Published by Elsevier Masson SAS.
Downloaded from ClinicalKey.com at National Certification CorporatioFor personal use only. No other uses without permission. Copyright ©2016. Elsev
5
ncies during pregnancy (excluding obstetrical emergencies)egnancies and may involve gastrointestinal, gynecologic, uro-iologies; surgery is necessary in 0.2—2% of cases. Since these
patients should be referred to specialized centers where sur-cares are available, particularly because surgical intervention
labor. Clinical presentations may be atypical and misleadingd anatomical and physiologic alterations, which often resulterapeutic delay with increased risks of maternal and infantdominal emergencies are acute appendicitis (best treated byute calculous cholecystitis (best treated by laparoscopic chole-ter through the early part of the third trimester) and intestinaltment is the first-line approach, just as in the non-pregnant
rare, usually resulting from trans-ampullary passage of gall-medical treatment but an elevated risk of recurrent episodesctomy in the 2nd trimester and endoscopic sphincterotomy ine present work is to review pregnancy-induced anatomical anddescribe the main abdominal emergencies during pregnancy,diagnostic and therapeutic management.sson SAS.
est, CHU Cochin Broca Hôtel-Dieu, Service de chirurgie digestive,14 Paris, France.
n July 25, 2016.ier Inc. All rights reserved.

S
I
AfplOpcpmgo(cowmpcbo
cctwaitsia
cpt
Sap
Oao
C
TbwdldwtfitiThte
6 28 24 ± 1.57 33 28 ± 28 37 30 ± 29 41 32 ± 2
ALP: after last period.
32 weeks ALP, the uterine fundal height increases by 0.5 cmper week or 2 cm per month (Table 1).
The position of the gravid uterus
In the 1st trimester of pregnancy, the uterus remains withinthe pelvis, but it becomes intra-abdominal thereafter as theuterus enlarges [10]. At term, the uterine position relativeto surrounding anatomy is:• anterior: adjacent to the anterior abdominal wall
although the greater omentum and small bowel loopsare occasionally interposed anteriorly, particularly whenabdominal adhesions were present prior to pregnancy. Asthe uterus enlarges, the thickness of the abdominal wall
106
ntroduction
bdomino-pelvic pain during pregnancy is a frequent reasonor emergency consultation. Aside from the common-lace minor pains of pregnancy, multiple etiologies mayead to abdominal emergency in the pregnant woman.ne must first consider typical obstetrical causes such aslacental abruption, non-labor-related uterine rupture, sub-apsular hematoma of the liver, hemoperitoneum due tolacenta percreta, each of which has specific manage-ent requirements. Abdominal pain can also arise from
astrointestinal disease (appendicitis, cholecystitis, bowelbstruction, hepatic or splenic rupture), vascular pathologysplenic aneurysm, aortic aneurysmal dissection), gyne-ologic pathology (aseptic necrosis of a uterine fibroid,varian or tubal torsion), urologic pathology (nephrolithiasisith renal colic, pyelonephritis), or trauma. Non-obstetricaledico-surgical emergencies complicate one in 500—700regnancies [1—4]. Many of these pathologies require surgi-al intervention (0.2—2% of cases [5,6]), the most commoneing acute appendicitis [7], adnexal masses (asymptomaticr symptomatic) [8], and acute cholecystitis [9].
The anatomical particularities and physiologic modifi-ations of pregnancy often lead to atypical or misleadinglinical presentations. Since these emergencies are rela-ively rare, most specialists have very limited experienceith them, which may result in diagnostic hesitation or ther-peutic delay. Since two lives are at risk, both mother andnfant, these patients should be managed in specialized cen-ers where surgical management can be supplemented bypecific obstetrical and/or neonatal management depend-ng on the gestational stage. Complications that may arisere often due to delays in diagnosis and management.
The aim of this review is to describe in detail the mostommon medical and surgical emergencies that arise duringregnancy, along with particularities of their diagnostic andherapeutic management.
pecifics of the clinical exam, imaging,
nd laboratory work-up of the pregnantatientptimal management of women presenting with acutebdominal pain during pregnancy requires a close collab-ration between surgeons, obstetricians and radiologists.
linical examination
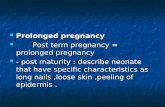
he anatomic and physiologic changes of pregnancy modifyoth the symptoms and the physical examination of patientsith abdominal diseases. The uterus cannot be felt transab-ominally until it rises up out of the pelvis 12 weeks after theast period (ALP). As pregnancy progresses, the uterine fun-us reaches the upper edge of pubis at the end of the 10theek ALP (2nd month) and becomes palpable at the end of
he 12th week ALP when the fundus lies eight cm or threengerbreadths above the symphysis pubis. At 18 weeks ALP,he fundus reaches the level of the umbilicus and at term,t lies 32 cm above the symphysis pubis (Table 1 and Fig. 1).he Fournié formula offers a simple calculation of uterineeight throughout gestation. Between 16 and 32 weeks ALP,he range of measured suprapubic uterine height (in cm) isqual to the number of weeks ALP minus 4 to plus 1. After
FL
Downloaded from ClinicalKey.com at National Certification Corporation JFor personal use only. No other uses without permission. Copyright ©2016. Elsevier
J. Bouyou et al.
Table 1 Normal values of uterine height as a functionof gestational age.
Months ofpregnancy
WeeksALP
Mean uterineheight (cm)
4 20 16 ± 14.5 22 At the
umbilicus ± 15 24 20 ± 1.5
igure 1. Uterine height as a function of gestational age (J.ansac).
uly 25, 2016.Inc. All rights reserved.

Abdominal emergencies during pregnancy
progressively attenuates and the linea alba widens in theumbilical region;
• posteriorly: the median portion of the uterus lies againstthe lumbar spine up to L3 and also borders the inferiorvena cava (IVC) and abdominal aorta;
• laterally: the uterus lies against the ureters as they crossover the psoas muscles. On the right side, the uterus abutsthe appendix, cecum, and ascending colon. If the cecumdoes not have fixed attachments, it is displaced superiorlyalong with the appendix by the enlarging uterus to lieabove the iliac crests. The appendix lies above the iliaccrest by the 32nd week ALP. The right adnexa is displacedposteriorly and masked by the uterus. The left adnexa ismasked posteriorly by the small bowel and the sigmoidcolon. The left round ligament is visible along its entirelength. Toward the end of gestation, the small bowel loopsand the sigmoid colon may be displaced anteriorly;
• superiorly: in the last weeks of gestation, the uterus abutsthe greater omentum and the transverse colon at the levelof L1—L2. It tends to displace the stomach posteriorly. Onthe right, it lies in contact with the inferior border of theliver and the gallbladder.
During the first two trimesters, uterine enlargementmainly involves the fundus, while during the last trimester,the lower uterine segment between the fundus and thecervix enlarges (early in the nullipara and somewhat laterin the multipara). This involves thinning of the isthmic andupper cervical zone of the uterus between the uterine bodyand cervix. This physiologic and anatomic entity disappearsafter delivery. The utero-vesical reflection ascends with theprogressive enlargement of the lower segment so that thebladder covers at least the lower half of the lower uterinesegment during labor.
Physiologic modifications during pregnancy
Physiologic modifications during pregnancy allow for thedevelopment and growth of the fetus, adaptation of themother to pregnancy and her preparation for labor and deliv-ery. A thorough knowledge of the normal physiology of the
pregnant woman is necessary in order to understand anyeventual pathological changes [11,12].General conditionTo a varying degree, pregnant women are subject to weightloss, decreased appetite and nausea during the early stagesof pregnancy. In later pregnancy, anxiety, difficulty in sleep-ing, and diverse abdomino-pelvic pains occur, due either tophysiologic Braxton-Hicks uterine contractions or to articu-lar pain involving the sacroiliac joints, the pubic symphysisand supporting ligaments.
Nausea and vomitingNausea and vomiting occur commonly in the first trimester ofpregnancy with an estimated prevalence of 50—75% [13—15].Despite this, most women maintain a good general condi-tion and symptoms generally resolve spontaneously towardthe end of the third month. Hyperemesis gravidarum isthe pathologic extension of this condition with intractablevomiting, dehydration, weight loss exceeding 5% of bodymass and abnormalities of liver function. Persistent vomi-ting beyond the 20th week ALP is considered pathologic andrequires an etiologic work-up [16].
Downloaded from ClinicalKey.com at National Certification CorporatioFor personal use only. No other uses without permission. Copyright ©2016. Elsev
S107
TemperatureElevated progesterone levels during early pregnancy resultin a temperature exceeding 37 throughout the 1st trimester.This returns to normal during the last two trimesters witha tendency to hypothermia during the last few weeks ofpregnancy [17].
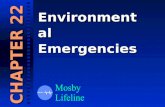
Cardiovascular and hemodynamicmodificationsThe essential characteristic of cardiovascular adaptationsof pregnancy is the early onset of arterial vasodilatation,which may account for increased cardiac output and, in turn,leads to activation of the renin-angiotensin-aldosterone axiswith a resultant increase in ‘‘cardiac work’’ (Fig. 2). At thesame time, sodium and water retention due to the com-bined effect of estrogens and aldosterone secretion resultin hypervolemia. Plasma volume progressively increasesthroughout pregnancy up to the 28th week ALP after whichit stabilizes. This plasma volume augmentation correlateswith the number and size of the fetus(es), and amounts toa 30—40% increase, or > 1000 mL (600—1900 mL) by the thirdtrimester. Cardiac output also increases by 30—50% due to a15% increase in cardiac rate (15% or 15—20 beats/minute inthe third trimester) and to a 30% increase in systolic ejec-tion volume. The glomerular filtration rate (GFR) increasesby 15% in early pregnancy and by 50—70% by late preg-nancy, due to increased renal plasma flow [18]. Arterialpressure is a function of cardiac output and peripheral resis-tance. Despite an increase in cardiac output, blood pressuredecreases by 20—30% due to decreased peripheral resistancefrom the 7th through the 24—28th weeks ALP. Thereafter,arteriovenous shunts created by the feto-placental circu-lation plus the vasomotor effects of placental hormoneslead to a progressive increase in peripheral resistance and areturn of arterial blood pressure to normal pre-pregnancylevels at term. The venous pressure in the upper bodyremains unchanged, but the venous pressure of the lowerextremities increases, especially towards the end of preg-nancy, as dextrorotation of the enlarging uterus compressesthe IVC. Increased IVC pressure impairs venous return from
the lower extremities and favors the development of edemaand venous varicosities of the legs and hemorrhoids.Respiratory modificationThere is an increase of both pulmonary blood flow and oxy-gen uptake. The increased oxygen needs of the fetus andplacenta amount to 20—30% and are manifested clinically bytachypnea in the range of 16 breaths per minute. At least50% of pregnant women have clinical dyspnea at term [19].
Digestive, hepatic and urinary modificationsSlowing of gastric emptying and decreased tone of the loweresophageal sphincter result in gastro-esophageal reflux withsymptoms of heartburn by the end of the first trimester,which progressively worsens throughout pregnancy. Thisaffects 80% of pregnant women and results in frequentepisodes of regurgitation. Acid secretion decreases by 40%;the increase in gastric pH in the first two trimesters mayaccount for decreased gastric tone and motility. This maybe a partial explanation of pregnancy-associated nausea.Small intestinal and colonic transit time is increased withan associated increase in colonic water absorption resultingin a tendency to constipation. High progesterone levels leadto decreased gallbladder tone, poor emptying, and biliary
n July 25, 2016.ier Inc. All rights reserved.

S108 J. Bouyou et al.
F outp
sailalpi
ttdt
UUdobaicw
IIba
dwpm
igure 2. Variation of arterial blood pressure, heart rate, cardiac
tasis. At the same time, higher estrogen levels result inn increased concentration of cholesterol and lithogenic-ty of bile. The combined effects of gallbladder stasis andithogenic bile result in an increased risk of cholecystolithi-
sis during pregnancy. During the third trimester, althoughiver volume is unchanged, the liver is not palpable as it isushed superiorly, posteriorly and to the right by the enlarg-ng uterus.Finally, uterine compression of the ureters at the brim ofhe pelvis causes pyelo-calyceal enlargement beginning athe 6th week ALP; this is more prominent on the right sideue to dextrorotation of the uterus. It results in an increasedendency to urinary stasis and infection [18].
terine contractionsp to a dozen intermittent, non-painful contractions peray should be considered physiologic and normal through-ut the 3rd trimester. After 37 weeks ALP, these contractionsecome more frequent, sustained, and intense; they aressociated with progressive effacement of the lower uter-ne segment in preparation for labor and delivery. Severeontractions before 37 weeks ALP should be considered asarning signs of the onset of premature labor and delivery.
mmune system modificationsn a simplified way of thinking, the fetus can be considered toe a sort of physiologic allograft since it expresses paternalntigens. During pregnancy, the maternal immune system
P
Tae
HR1ii2tfahnttbwmyc
Downloaded from ClinicalKey.com at National Certification Corporation JFor personal use only. No other uses without permission. Copyright ©2016. Elsevier
ut during the course of pregnancy.
evelops transient immune tolerance to fetal antigenshile maintaining its ability to protect against infectiousathogens. Nonetheless, this temporary immunodepressionakes the mother more susceptible to infections [17].
articularities of laboratory findings
he various physiologic adaptations of pregnancy describedbove result in alterations in normal values of laboratoryxaminations (Table 2).
ematologyed blood cell (RBC) mass increases beginning after the2th week ALP. RBC volume increases by 20% under thenfluence of hormonal stimulation of erythropoietin. Withron supplementation, this augmentation may increase from50 mL to 450 mL. However, plasma volume increases morehan RBC volume resulting in relative hemodilution and aall in hemoglobin concentration, the so-called ‘‘physiologicnemia of pregnancy’’. The lower limits of normal foremoglogin concentration and hematocrit during preg-ancy range from 11 g/dL with a hematocrit of 32% inhe 1st and 3rd trimesters, and slightly lower in the 2ndrimester at 10.5 gm/dL. The platelet count remains sta-le, but gestational thrombocytopenia occurs in 4—8% ofomen as pregnancy approaches term; this should not beistaken for a manifestation of the HELLP syndrome (hemol-
sis, elevated liver enzymes, low platelet count), whichomplicates 10—15% of cases of preeclampsia. Physiologic
uly 25, 2016.Inc. All rights reserved.

Abdominal emergencies during pregnancy S109
Table 2 Normal laboratory values at each trimester of pregnancy.
1st trimester 2nd trimester 3rd trimester
Complete blood count
Hemoglobin (g/dL) 11.7—13.7
Hematocrit (%) 36
Leucocytes (per mm3) 3150—15,300Platelet count (per mm3) No change
Liver function testsASAT/ALAT No change
Bilirubin direct (�mol/L) No change
Bilirubin total (�mol/L) No change
Alkaline phosphatase (IU/L) No change
GGT (IU/L) No change
Electrolytes and blood chemistriesNa+ (mmol/L) 140 ± 5
K+ (mmol/L) 3.5—4.5Creatinine (�mol/L) Decreased
Urea (g/L) Decreased
Lipase (IU/L) Decreased
Amylase (IU/L) No change
Total protein (%) No change
Prothrombin time (INR) No change
Other laboratory testsCRP (mg/L) No change
Sedimentation rate (mm/h) Very high
leukocytosis may rise as high as 16,000 WBC/mm3 duringthe 2nd trimester due to an increase in polymorphonuclearleukocytes.
HepatobiliaryPhysiologic and laboratory alterations towards the end ofpregnancy result in increased levels of alkaline phosphatase(2—15 times normal due to placental and osseous produc-tion of iso-enzymes) and fibrinogen and a hemodilutionaldecrease in levels of albumin, bilirubin and �GT. An increaseof liver transaminases to more than twice normal should be
considered pathologic [20].HemostasisMost coagulation factors increase during pregnancy whilecoagulation inhibitors and fibrinolytic capacity decrease.Alterations of the hemostatic mechanism result in a rel-atively hypercoagulable state, which increases throughoutpregnancy [21]. The physiologic increase in fibrinogen levelsduring pregnancy should not be considered to be a markerfor inflammation in this context [22,23].
RenalGFR and creatinine clearance both increase during preg-nancy, along with a hemodilutional decrease in serumcreatinine, urea, iodine, calcium, and uric acid. Interpre-tation of urinary dipstick findings remains unchanged [18].
Particularities of imaging for abdominalemergencies
Ultrasound is the first choice for abdominal imaging in preg-nancy because it is rapid, widely available, and because itavoids radiation exposure. It is an effective diagnostic toolfor gynecologic, gastrointestinal, urinary, and hepatobiliary
Downloaded from ClinicalKey.com at National Certification CorporatioFor personal use only. No other uses without permission. Copyright ©2016. Elsev
9.7—11.5 9.8—12.333 346300—16,100 5000—16,600No change No change
No change No changeNo change No changeNo change No change2—15 × normal 2—15 × normalNo change No change
Stable StableStable StableDecreased DecreasedDecreased DecreasedStable StableNo change No changeNo change No changeNo change No change
No change No changeVery high Very high
pathologies. It is also effective in detecting obstetricalpathologies and assessing fetal condition. Its effectiveness issomewhat limited for evaluation of the intestine, pancreas,ureters and mesenteric vasculature because its visibility islimited by the interposed uterus and by the presence ofintestinal air.
Magnetic resonance imaging (MRI) has been shown to beeffective in evaluating specific etiologies of acute abdomi-nal pain during pregnancy [24]. Because it avoids exposureto ionizing radiation, MRI is the preferred second-line diag-nostic modality when ultrasound is inconclusive. At thepresent time, no scientific evidence has established that
the use of MRI during pregnancy constitutes a risk for thefetus. The American College of Radiology recommends thatMRI be used instead of CT during pregnancy. Gadolinium,administered as a contrast agent, crosses the placentalbarrier into the fetal circulation, is filtered by the fetalkidneys and excreted into the amniotic fluid. It shouldbe used only sparingly since the risks of secondary fetaleffects such as nephrogenic systemic fibrosis have not beenclearly established [25] (CRAT — http://www.lecrat.org/— Reference Center for Teratogenic Agents). The use ofGadolinium enhancement is currently recommended for cer-tain specific obstetrical situations, particularly for casesof invasive placentation (placenta percreta), in order todefine the degree of extension and anatomic relations of theplacenta.While the dosage of X-irradiation from current CT tech-niques is small, X-ray exposure should be avoided duringpregnancy, particularly during the 1st trimester, becauseof possible teratogenic effects. The benefits of CT mustbe weighed against the risks of radiation exposure andclearly explained to the parents. When a patient witha previously unrecognized pregnancy undergoes CT scan,even in early pregnancy, this is not a sufficient indica-tion for termination of pregnancy. However, when CT mustbe performed in a patient with known pregnancy, the
n July 25, 2016.ier Inc. All rights reserved.

S
nia
5nsp8eCtmchd
ir5ce2aaighCsia
Dd
AcdaGtocr
ats•
•
•
•
•
figcap
Ps
Wliitp
aoLpgmar[titop
lire
110
umber of cuts and images should be strictly limited and,f possible, the uterus should be shielded with a leadpron.
Studies have shown that cumulative exposure of up to0 mGy of ionizing radiation (the equivalent of 5 abdomi-al plain X-rays or 1—2 abdominal CT scans) result in noignificant increase in teratogenic risk. CT of the maternalelvis may result in fetal X-ray exposure of between 25 and0 Gy, depending on the parameters of the CT scanner. Sev-ral studies [25,26] have shown that teratogenic effects ofT radiation are very unlikely for doses up to 100 mGy. Theeratogenic effects of ionizing irradiation (microcephaly,icro-ophthalmia, mental retardation, growth retardation,
ataracts, behavioral problems) become evident only afterigher doses of radiation and, in particular, for radiationelivered between the 2nd and 20th week ALP.
Other studies have shown that in utero radiation exposures associated with an increased risk of childhood cancer; thisisk may double (2/1000) when radiation exposure exceeds0 mGy. According to the Oxford Survey of Childhood Can-ers, this increased risk is most marked when radiationxposure occurs during the 1st trimester rather than thend or 3rd trimester, with relative risks of 3.19, 1.29,nd 1.30, respectively [26]. Intravenous iodinated contrastgents have not been shown to increase teratogenic riskn either animals or humans. However, animal studies sug-est that exposed newborns should be tested for neonatalypothyroidism [27]. In sum, the low risks associated withT scan during the 2nd and 3rd trimesters suggest that CTcan with IV contrast can be performed in pregnant women,f necessary, to avoid delay in diagnosis and management ofbdominal emergencies.
iagnostic work-up for abdominal painuring pregnancy
bdominal pain during pregnancy is a common reason foronsultation, albeit with varying degrees of urgency. Theiagnostic hypotheses should be prioritized, taking intoccount the patient’s history and the term of pregnancy.
ynecological and obstetrical conditions that may poten-ially cause abdominal pain must be considered at theutset and rapidly diagnosed to allow prompt appropriateare, especially since two lives, maternal and fetal, are atisk.
Several obstetrical pathologies may present with acutebdominal pain. These often require urgent cesarean sectiono preserve maternal and fetal life; no diagnostic studieshould delay this urgent decision:
retro-placental hematoma preferentially occurs in thesetting of preeclampsia. This typically presents as con-stant intense brutal abdominal pain, with a hypertonic‘‘hard as wood’’ uterus and possibly with metrorrhagia;uterine rupture can occur de novo, or more commonlywith a past history of uterine surgical scar. Abdominal painmay be associated with vaginal bleeding, deformation ofthe abdomen, or hemoperitoneum;subcapsular hematoma of the liver is a specific complica-tion of preeclampsia and the HELLP syndrome;hemoperitoneum may be associated with severe abdom-inal pain in cases of placenta percreta, vascularmalformation, or hemorrhage from an endometriosislesion;utero-adnexal pathologies such as ectopic pregnancy, rup-tured corpus luteum cyst, adnexal torsion or subserosal
dosssibu
ptplnf1ctrpttH3i
Downloaded from ClinicalKey.com at National Certification Corporation JFor personal use only. No other uses without permission. Copyright ©2016. Elsevier
J. Bouyou et al.
fibroid with pedicular torsion are all possible causes ofacute abdomino-pelvic pain in pregnant women that mayrequire urgent surgical management.
Any physician taking care of a pregnant woman mustrst consider these gynecological and obstetrical etiolo-ies of acute abdominal pain. These causes apart, the mainauses of abdominal emergency during pregnancy are acuteppendicitis, acute cholecystitis, bowel obstruction, acuteancreatitis, abdominal trauma and renal colic.
rinciples and particular features ofurgical management
hen a surgical intervention is indicated, the question ofaparoscopic versus laparotomy approach must be discussedn terms of its feasibility during pregnancy. Laparoscopicndications in the treatment of abdominal emergencies inhe pregnant patient are no different from those for a non-regnant a patient [28—30].
Laparotomy has long been the preferred surgicalpproach during pregnancy. However, the developmentf laparoscopy has led to increasingly widespread use.aparoscopy has multiple advantages including: reducedostoperative pain with decreased consumption of anal-esics, particularly morphine; reduced risk of postoperativeaternal hypoventilation; more rapid mobilization and
mbulation with a resultant reduction in thromboembolicisk, parietal complications and duration of hospitalization31]. Specific precautions are necessary to guard againsthe inherent risks of this approach: uterine laceration,ntra-amniotic insufflation, CO2 fetotoxicity due to passiveransplacental diffusion of insufflation gas, and diminutionf utero-placental blood flow due to high intraperitonealressure [32—34].
No studies have shown the superiority of open-aparoscopy versus Verres needle-insufflation. Guidelinesssued by the CNGOF in 2010 recommend against Ver-es needle-insufflation needle beyond 14 weeks ALP; theyncourage open-laparoscopy with incisional placement
etermined by the term of pregnancy, uterine volume andperative indications. Beyond 24 weeks ALP, the incisionhould be placed supra-umbilically. Insufflation pressurehould not exceed 12 mm Hg and changes of patient positionhould be gradual with only moderate Trendelenburg. Allnstrumental contact with the uterus during surgery shoulde avoided since this can cause serosal bleeding or provoketerine contractions [7,35].From an obstetrical viewpoint, spontaneous or inducedre-term delivery should be prevented because of poor fetalolerance, but such complications should be anticipated byre-intervention transfer to surgical unit where a suitableevel of obstetrical and neonatal care is available. Ante-atal steroid administration to accelerate development ofetal pulmonary surfactant (2 intramuscular injections of2 mg of betamethasone at 24 hours interval) should beonsidered on a case-by-case basis when there is risk of pre-erm labor or induced pre-term birth, if the pregnancy haseached a term of fetal viability (≥ 24 weeks ALP) withoutulmonary maturity (34 weeks ALP). There is no indica-ion for routine administration of tocolytic agents unlesshere are symptoms of threatened premature delivery [36].owever, if repeated uterine contractions develop before4 weeks ALP, particularly if there are signs of cervical ripen-ng, tocolysis should be performed using calcium channel
uly 25, 2016.Inc. All rights reserved.

Abdominal emergencies during pregnancy
blockers or atosiban, an oxytocin antagonist. Beta-2 ago-nists should be avoided as first-line tocolytic agents becausethey generate hemodynamic changes that could alter intra-operative anesthetic monitoring. If abdominal emergencyoccurs in late-stage pregnancy, induced labor and deliveryor caesarean delivery can be considered prior to specifictreatment.
Assessment of fetal heart rate by auscultation andmonitoring should be performed before and after the inter-vention, along with an ultrasound assessment of fetalviability (Manning Score). Most anesthetic drugs crossthe blood-placental barrier and it is common to observedecreased fetal activity or decreased responsiveness andvariation in the recorded fetal heart rate.
From an anesthetic point of view, large caliber venousaccess should be established before starting any operation,and all the techniques usually used to control bleeding riskin major surgery are applicable, including maintenance ofnormothermia, monitoring of the depth of anesthesia, andoptimization of hemostasis and proper volume expansion.It is especially important to quickly correct maternal peri-operative hypotension in order to limit fetal repercussionsrelated to decreased utero-placental blood flow.
Pregnancy is associated with a hypercoagulable stateand a 0.1—0.2% incidence of deep venous thrombosis [37].Surgery and pneumoperitoneum may increase this risk.Preventive measures such as compression stockings andearly post-surgical mobilization are recommended. Althoughroutine use of prophylactic anticoagulation is not rec-ommended, this may be suggested for prolonged majorsurgeries, particularly if there are other risk factors (per-sonal history of venous thromboembolic disease, obesity,pelvic surgery, infection or prothrombotic inflammatorystate) [38]. When prophylactic anticoagulation is indicated,there is no contraindication to the use of unfractionatedheparin or low-molecular-weight heparin [39].
Typically, prescribed postoperative medications includ-ing proton pump inhibitors and anti-emetics such asmetoclopramide (Reglan®) are not contraindicated dur-ing pregnancy. All pain medications can be administered,including opioid analgesics. However, non-steroidal anti-
inflammatory drugs (NSAID) are contraindicated beyond24 weeks ALP since they are associated with premature clo-sure of the fetal ductus arteriosus.Incidence, diagnostic particularities andspecific management of major abdominalemergencies during pregnancy
Acute appendicitis
Acute appendicitis is the most common surgical emergencyduring pregnancy with an estimated incidence of 0.5—2 per1000 pregnant women, i.e., 25% of all non-obstetrical surgi-cal emergencies [7] (Table 3). It occurs more frequently inthe 2nd trimester of pregnancy [9,40,41]; pregnancy doesnot modify the overall incidence of appendicitis.
Diagnostic difficulties may arise, particularly during the2nd and 3rd trimesters, due to misleading or atypical sym-ptomatology associated with changes in the appendicealposition as it is displaced progressively upward by the enlarg-ing uterus. Baer et al. [42] described progressive ascent ofthe appendix from the third month onward, reaching thelevel of the iliac crest by the end of the 6th month, and
Downloaded from ClinicalKey.com at National Certification CorporatioFor personal use only. No other uses without permission. Copyright ©2016. Elsev
S111
return to its usual position by the tenth day postpartum[43]. The most suggestive symptom is right lower quad-rant abdominal pain, which is found in 80% of cases [43].But, tenderness can also be localized in the right flank, theright lumbar fossa and sometimes even in the right upperquadrant. Rebound tenderness (55—75% of cases) and mus-cular guarding (50—65%) are classical signs; they can bepartially masked, but should always be sought. A positivepsoas sign is rare. Anorexia, nausea and vomiting are presentin 87% of cases [44], but these nonspecific symptoms arecommonplace early in pregnancy. Fever is present in only50% of cases. Leukocytosis is already physiologically presentin pregnant women and has low sensitivity and specificity,while the CRP level may be normal.
Ultrasound is the key diagnostic tool, especially in the 1sttrimester; technical difficulties decrease its diagnostic valuein the third trimester. The diagnostic accuracy of ultrasoundis highly variable and depends on the experience of the oper-ator; sensitivity and specificity range from 50 to 100% andfrom 33 to 92%, respectively [24]. If ultrasound fails to diag-nose appendicitis because the appendix cannot be clearlyidentified (whether normal or not), MRI is then the second-choice diagnostic modality with a sensitivity of 100% and aspecificity of 94% [45]. If MRI is not available or is impracti-cable, then CT becomes the alternative diagnostic modality.The risk of missing the diagnosis of appendicitis in pregnancyoutweighs the low but finite risks of irradiation. The diag-nostic accuracy of CT during pregnancy is similar to that ofthe general population with a sensitivity and specificity of92% and 99%, respectively.
Diagnostic delay is associated with a higher risk ofcomplications such as perforation, which is associated witha 20—35% rate of fetal loss (versus 1.5% in non-perforatedappendicitis). In a series of 84 patients, Tamir et al. reporteda 43% incidence of appendiceal perforation when surgerywas delayed for more than 24 hours, whereas no cases ofperforation was described when surgical management tookplace within 24 hours following admission [46].
Among other consequences, premature labor is very com-mon (83% rate of premature uterine contractions whenlocalized peritonitis was present) with a pre-term birth rate
exceeding 50% in the 3rd trimester.The treatment of acute appendicitis in pregnant womenis surgical appendectomy; the management strategy must beadapted to several factors such as gestational age, sever-ity of appendicitis, body mass index, history of previousabdominal surgery, ability and preferences of the surgeon.Laparoscopic appendectomy, which has become standardfirst-line treatment during pregnancy is associated with alow complication rate, no matter what the gestational stage[47]. If open laparotomy is chosen, a classical McBurney inci-sion can be used during the 1st trimester. In the 2nd and 3rdtrimester, the incision must be placed higher on the right,while some surgeons feel that an upper midline incisionallows better access to the ceco-appendicular region [48].If generalized peritonitis is present, a longer midline inci-sion extending above and below the umbilicus allows broadaccess for easy exploration and adequate peritoneal lavageand toilet of the entire peritoneal cavity.
Acute cholecystitis
Gallbladder disease, particularly acute cholecystitis, isthe second leading cause of non-obstetrical abdominalemergency after appendicitis. Its incidence is one per1600—10,000 pregnancies. Cholelithiasis is the etiologic
n July 25, 2016.ier Inc. All rights reserved.

S J. Bouyou et al.
inal emergencies during pregnancy.
ity Fetal risk (miscarriage, FDIUa, abortion)
< 1.5% if non-perforated25—30% if perforated
pregnant patients 1—2%< 20%
pregnant patients < 5%rity of trauma Varies with severity of trauma
ctiscrvirnTpumtp
i9titscd
ucdtowiamsbtuwp
B
Bofalsci
increases as pregnancy progresses, particularly during therapid increase in uterine size between 16 and 20 weeks ALPwhen the uterus becomes intra-abdominal, and between32 and 36 weeks when the fetus descends into the pelvis,and also postpartum when the uterus rapidly shrinks in size.Small intestinal volvulus accounts for 9% of bowel obstruc-tions during pregnancy [57]. Other rare causes includingintussusception, strangulated hernia, cancer and divertic-ulitis account for 5% of bowel obstructions during pregnancy[58]. In a relatively old series reported by Perdue et al. in1992 [55], a high maternal mortality of 6% with a 26% rateof fetal mortality were noted, with a 23% rate of intesti-nal resection. Current rates of morbidity and mortalityare much lower due to improved diagnostic and therapeu-tic performance. Symptoms of bowel obstruction are thesame as in non-pregnant patients: abdominal pain with spas-modic cramping, distention, nausea, vomiting, and arrestedintestinal transit of stool and gas. However, the symptomscan be attenuated or atypical; one must be vigilant torule out bowel obstruction when faced with a pregnantpatient with intractable vomiting, especially after the 1sttrimester.
Dilated small bowel loops with dynamic air-fluid levelsare present on plain abdominal X-ray in 82% of patients withan obstructive syndrome [55]. Abdominal X-ray can make the
112
Table 3 Materno-fetal risks associated with major abdom
Pathology Incidence Maternal mortal
Acute appendicitis 1/500—2000 < 1%
Acute cholecystitis 1/1600—10,000 Same as for non-Bowel obstruction 1/1500—16,000 < 5%
Acute pancreatitis 1/1000—3000 Same as for non-Abdominal trauma 6—7% Varies with seve
a FDIU: fetal death in utero.
ause in 90% of cholecystitis. Cholelithiasis is present in 3.5o 10% of pregnant women [49,50]. Symptoms are almostdentical to those in non-pregnant patients and include nau-ea and vomiting, dyspepsia, fatty food intolerance, andolicky right upper quadrant or epigastric pain that mayadiate to the back. However, Murphy’s sign is less rele-ant in advanced-stage pregnancy. The differential diagnosisncludes numerous conditions and one must consider obstet-ic pathology such as gestational acute fatty liver, either deovo or due to HELLP syndrome complicating preeclampsia.he differential diagnosis also includes acute appendicitis,reeclampsia, acute hepatitis, acute pancreatitis, pepticlcer, acute right-sided pyelonephritis, or right basilar pneu-onia. When interpreting laboratory findings, it is important
o remember that an elevated alkaline phosphatase level ishysiological during pregnancy.
Ultrasound is the diagnostic modality of choice becauset is non-invasive, non-irradiating, readily available, and has5—98% sensitivity for detection of gallstones [51]. Conven-ional criteria for ultrasound diagnosis of acute cholecystitisnclude a sonographic Murphy’s sign, presence of cholecys-olithiasis, increased gallbladder size (> 4 cm), gallbladderludge, thickening of the gallbladder wall (> 4 mm), and peri-holecystic fluid. Dilatation of the intra- or extrahepatic bileucts suggests the diagnosis of choledocholithiasis.
Surgery is the first-line of treatment. It reduces these of medications and avoids recurrent bouts of chole-
ystitis that occur in 44—92% of medically treated patientsepending on the pregnancy stage and length of time toerm. Surgery reduces the length of stay and avoids thenset of serious complications such as sepsis or perforationith peritonitis. Furthermore, symptomatic cholelithiasiss associated with a 10% risk of acute gallstone pancre-titis and a 10—20% risk of miscarriage [52]. Non-surgicalanagement is also associated with a higher incidence of
pontaneous abortion, threatened abortion, and prematureirth when compared to patients who underwent cholecys-ectomy [53]. Laparoscopy is the recommended approachp to the beginning of the 3rd trimester. Maternal mortalityith laparoscopic cholecystectomy is not increased by theregnancy [54].
owel obstruction
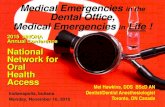
owel obstruction is the third most common cause of non-bstetrical abdominal emergency during pregnancy with arequency of 1 in 1500—16,000 pregnancies. Adhesive bandsccount for 60—70% of obstructions (Fig. 3); this is particu-arly likely when past history includes previous abdominalurgery or peritonitis. Volvulus is found in about 25% ofases [55], while it accounts for < 1% of bowel obstructionsn non-pregnant patients [56]. The risk of cecal volvulus
Figure 3. Small bowel obstruction due to an adhesive band at18 weeks after last period.
Downloaded from ClinicalKey.com at National Certification Corporation July 25, 2016.For personal use only. No other uses without permission. Copyright ©2016. Elsevier Inc. All rights reserved.

Abdominal emergencies during pregnancy
diagnosis of cecal volvulus with a sensitivity of 95%. If bowelobstruction is still suspected despite the absence of typicalfindings on plain X-ray, contrast-enhanced imaging (abdom-inal X-ray after oral gastrografin or CT with IV contrast)may be necessary. The potential risks of fetal irradiationare largely offset by potential risks of maternal and fetalmorbidity and mortality. For cecal volvulus without signsof grave complication, colonoscopy may be useful, but therate of colonoscopic reduction of cecal volvulus is far lowerthan for sigmoid volvulus. It should not be allowed to delaysurgical treatment. The decision tree for therapeutic man-agement is the same as for non-pregnant patients. Medicaltreatment (NPO, nasogastric suction, fluid and electrolyterepletion) should be the initial step unless there are clini-cal, laboratory or imaging signs of clinical gravity. Failure ofmedical treatment or signs of gravity such as fever, tachycar-dia, marked leukocytosis combined with severe abdominalpain are justification for prompt surgical intervention. Amidline laparotomy is recommended with its height adaptedto uterine size [55,56].
Acute pancreatitis
The incidence of acute pancreatitis during pregnancy isapproximately 0.3—1 per 1000 pregnant women. In the gen-eral population, 80% of acute pancreatitis is due either togallstones or to alcoholic pancreatic toxicity (in roughlyequal proportions); during pregnancy, cholelithiasis is by farthe most common etiology, accounting for 67—100% of cases[59]. Hypertriglyceridemia is responsible for 4—6% of acutepancreatitis during pregnancy. Acute pancreatitis occursmore frequently in the 3rd trimester. The diagnosis of acutepancreatitis in pregnancy is also difficult to make becausethe typical symptoms including sudden severe epigastricpain penetrating to the back, with nausea and post-prandialvomiting, ± fever can also evoke a serious obstetric compli-cation such as retro-placental hematoma, or a complicationof preeclampsia or HELLP syndrome that warrants an emer-gency caesarean section. Elevation of lipase level to thricenormal strongly supports the diagnosis. Ultrasound is thefirst-line imaging study and should be complemented by MRI
to assess severity according to the usual criteria; antibioticprophylaxis must be considered for severe forms (beyondBalthazar stage D). Management is the same as for non-pregnant patients (NPO), with IV fluids, electrolyte, andvitamin replacement in an intensive care unit, with moni-toring of the fetal heart rate.Most patients respond to medical treatment within a fewdays and cautious feeding can be allowed by the fourthday. Management decisions following resolution of an acuteepisode are more delicate and depend on the stage of preg-nancy, particularly because the recurrence rate of acutegallstone pancreatitis in pregnant women is 70% (90% dur-ing the initial hospitalization) versus 20—30% for the generalpopulation [60]. Surgery should be avoided during the 1sttrimester, while laparoscopic cholecystectomy should beconsidered in the 2nd trimester. In the 3rd trimester, endo-scopic retrograde cholangiopancreatography (ERCP) withsphincterotomy is a safe and effective alternative thatallows deferral of cholecystectomy until after childbirth[61]. Indeed, the rate of premature birth is almost zerowhen cholecystectomy is performed in the 2nd trimester,but approaches 40% in the 3rd trimester. In the 1970s, thefetal mortality rate was 37%; nowadays thanks to earlierdiagnosis and better neonatal care, perinatal mortality isless than 5% [62,63].
Downloaded from ClinicalKey.com at National Certification CorporatioFor personal use only. No other uses without permission. Copyright ©2016. Elsev
S113
Abdominal trauma
Abdominal trauma occurs during pregnancy with a frequencyof 6—7%, consisting mainly of motor vehicle accidents, phys-ical assault (often domestic violence) and falls. Traumais the most common cause of non-obstetrical maternaldeath, but only 0.3% of injuries require surgical intervention[64,65].
The clinical presentation of abdominal trauma duringpregnancy varies widely. The medical history should clearlyelicit the traumatic mechanism and distinguish direct fromindirect impact. Their consequences must not be underesti-mated, especially in the late stages of pregnancy. Work-upshould include a complete physical examination of themother, specifically searching for visceral, musculo-skeletaland central nervous system trauma. In addition to mater-nal vital signs, the fetal heart rate should be monitoredand an ultrasound assessment of fetal viability performed.A Kleihauer test should be performed to detect the pres-ence of fetal red blood cells in the maternal circulation dueto fetal-maternal hemorrhage. The patient may require a24-hour surveillance hospitalization. In some cases, trivialmaternal damage may result in serious consequences for thefetus. On the other hand, reassurance is warranted if initialassessment shows no significant abnormality in the motheror fetus.
In blunt abdominal trauma, splenic rupture is the mostcommon source of intraperitoneal bleeding. The increasedsize of the abdominal cavity with gradual stretching seems todecrease peritoneal sensation. Signs of peritoneal irritationmay therefore be absent despite the existence of an abdom-inal injury. Uterine rupture is rare before three months ofgestation because the uterus is only slightly enlarged andstill protected within the bony pelvis; it occurs in < 1% oftraffic accidents with violent high kinetic energy transfer[66]. When uterine rupture occurs in this context, fetalprognosis is extremely poor and maternal risk is directlyrelated to the degree of internal bleeding, which can be cat-aclysmic and fatal. Caesarean section for maternal salvageis indicated and carries a high risk of hysterectomy. Placen-tal abruption is very common. It can occur with even minor
injuries, and may sometimes only become apparent after 24to 48 hours. The difference in structure between the rela-tively rigid placenta and the more malleable uterus causesseparation of the interface by a shearing effect. Placentalabruption is found in 2—4% of minor injuries and 20—50% ofmajor trauma. It results in a 20—35% fetal mortality but onlya 1% maternal mortality [66]. In this context, laparoscopy isseldom indicated.Trauma in pregnant women can be classified into fourgroups for whom specific management is adapted:• group 1 consists of patients in early pregnancy, or who
are unaware of pregnancy. It is essential to perform apregnancy test in all women of childbearing age who havesuffered significant trauma in order to adapt the work-up(particularly imaging) and management;
• group 2 consists of patients at < 24 weeks gestation ALP,in whom the fetus is not yet viable, but is still well pro-tected by the pelvis and has suffered little direct damage.Management is focused on the mother and medical ter-mination of pregnancy may be indicated if the maternalprognosis depends on it;
• group 3 consists of patients whose pregnancyis ≥ 24 weeks, in whom a viable fetus is very vulnerable toinjury because of its size and extrapelvic position. Closeand constant monitoring of fetal viability is necessary.
n July 25, 2016.ier Inc. All rights reserved.

S
•
R
Uw[nS(oaac7Rubcc
C
AimuoouimiwTsmca
D
T
R
[
[
[
[
[
[
114
An emergency caesarean section may be indicated iffetal viability is threatened, precipitating the delivery ofa premature newborn with consequences determined bygestational age and birth weight. However, exploratorylaparotomy for suspected maternal hemoperitoneumdoes not always pre-suppose fetal extraction. For afetus that has reached the threshold of viability, survivalafter emergency caesarean section for maternal traumadepends on gestational age and birth weight. More thanhalf (60%) of neonatal deaths are due to a delay in thediagnosis of fetal distress leading to delay in caesareansection [67];group 4 consists of the rare cases of a mother inintractable hemorrhagic shock or cardiac arrest resis-tant to any treatment. Immediate ‘‘post-mortem’’ fetalextraction can be attempted in individual cases butneonatal survival depends on maintaining the fetal-placental circulation (fetal distress is betrayed byabnormalities of fetal heart rate in this context), thedelay interval until extraction, and the availability ofneonatal care at the place of birth. A 70% neonatalsurvival rate is noted when birth occurs within five min-utes after the mother’s death, but this decreases to3% after 20 minutes delay. In all cases, fetal extractionallows improved fetal prognosis after maternal circulatoryarrest, whatever the gestational age [68].
enal colic
rolithiasis is a common disease; the incidence in pregnantomen ranges from 0.026 to 0.5% depending on the study
69]. Diagnosis is based on clinical history, physical exami-ation, laboratory testing, urinalysis and renal ultrasound.tandard analgesic treatment combining Tier 1 analgesicsparacetamol) and antispasmodics provides pain relief in 84%f cases. Non-steroidal anti-inflammatory drugs should bevoided and are contraindicated beyond 24 weeks ALP. Theddition of short-term corticosteroid therapy when renalolic is resistant to standard therapy has been effective in
1% of patients and often permits postponement of surgery.enal drainage by the introduction of a double-J endo-reteral catheter/stent requires ongoing ultrasound andacteriological surveillance throughout pregnancy. Extra-orporeal lithotripsy and percutaneous nephrolithotomy areontraindicated during pregnancy [70,71].onclusion
bdominal pain is a common cause of consultation dur-ng pregnancy. It is often the sign of anxiety-provoking butinor pregnancy-specific pathologies. But, it should not be
nderestimated and requires assessment to rule out gyneco-bstetrical causes. Abdominal pain due to gastrointestinalr urological causes may present with atypical or atten-ated clinical symptoms; morphological assessment andmaging must be performed promptly to rule out causes thatight require surgical intervention. If emergency surgery is
ndicated, it should be performed in a specialized centerithout delay; laparoscopy is usually an effective approach.he risk of spontaneous or induced premature deliveryhould be anticipated as much as possible with the imple-entation of a management strategy to reduce antenatal
omplications. It is crucial to fully inform parents of man-gement choices.
[
[
[
[
[
[
[
[
[
[
Downloaded from ClinicalKey.com at National Certification Corporation JFor personal use only. No other uses without permission. Copyright ©2016. Elsevier
J. Bouyou et al.
isclosure of interest
he authors declare that they have no competing interest.
eferences
[1] Coleman MT, Trianfo VA, Rund DA. Nonobstetric emergenciesin pregnancy: trauma and surgical conditions. Am J ObstetGynecol 1997;177(3):497—502.
[2] Kammerer WS. Nonobstetric surgery in pregnancy. Med ClinNorth Am 1987;71(3):551—60.
[3] Triolo PK. Nonobstetric surgery during pregnancy. J ObstetGynecol Neonatal Nurs 1985;14(3):179—83.
[4] Kammerer WS. Nonobstetric surgery during pregnancy. MedClin North Am 1979;63(6):1157—64.
[5] Brodsky JB. Anesthesia and surgery during early preg-nancy and fetal outcome. Clin Obstet Gynecol 1983;26(2):449—57.
[6] Brodsky JB, Cohen EN, Brown Jr BW, et al. Surgery dur-ing pregnancy and fetal outcome. Am J Obstet Gynecol1980;138(8):1165—7.
[7] Miloudi N, Brahem M, Ben Abid S, et al. Acute appendicitis inpregnancy: specific features of diagnosis and treatment. J ViscSurg 2012;149(4):e275—9.
[8] Goh W, Bohrer J, Zalud I. Management of the adnexal mass inpregnancy. Curr Opin Obstet Gynecol 2014;26(2):49—53.
[9] Gilo NB, Amini D, Landy HJ. Appendicitis and cholecystitis inpregnancy. Clin Obstet Gynecol 2009;52(4):586—96.
10] Kamina P. Anatomie clinique : thorax abdomen pelvis. Vol. 3.2nd ed. Paris: Maloine; 2009.
11] Cabrol D, Pons J, Goffinet F. Traité d’obstétrique. Paris, France:Médecine-Sciences Flammarion; 2003 [ISBN 2-257-12429-4].
12] Fournier A, Laffitte A, Parant O, et al. Modifications del’organisme maternel au cours de la grossesse. In: EMCGynécologie-obstétrique; 1999 [5-008-A-10].
13] Einarson TR, Piwko C, Koren G. Quantifying the global ratesof nausea and vomiting of pregnancy: a meta-analysis. J PopulTher Clin Pharmacol 2013;20(2):e171—83.
14] Maltepe C, Koren G. The management of nausea and vomitingof pregnancy and hyperemesis gravidarum — a 2013 update. JPopul Ther Clin Pharmacol 2013;20(2):e184—92.
15] Jarnfelt-Samsioe A, Samsioe G, Velinder GM. Nausea and vomi-ting in pregnancy — a contribution to its epidemiology. GynecolObstet Invest 1983;16(4):221—9.
16] Joshi D, James A, Quaglia A, et al. Liver disease in pregnancy.Lancet 2010;375(9714):594—605.
17] Fournier A, Laffitte A, Parant O, et al. Modifications del’organisme maternel au cours de la grossesse. In: EncyclopédieMédico-Chirurgicale : gynécologie-obstétrique. Paris: ElsevierMasson SAS; 2005.
18] Cheung KL, Lafayette RA. Renal physiology of pregnancy. AdvChronic Kidney Dis 2013;20(3):209—14.
19] Hegewald MJ, Crapo RO. Respiratory physiology in pregnancy.Clin Chest Med 2011;32(1):1—13 [vii].
20] Bacq Y, Zarka O, Brechot JF, et al. Liver function tests in normalpregnancy: a prospective study of 103 pregnant women and 103matched controls. Hepatology 1996;23(5):1030—4.
21] Bura-Riviere A. Thrombophilia and pregnancy. Rev Prat2012;62(7):937—42.
22] Reger B, Peterfalvi A, Litter I, et al. Challenges in the eval-uation of D-dimer and fibrinogen levels in pregnant women.Thromb Res 2013;131(4):e183—7.
23] Liu J, Yuan E, Lee L. Gestational age-specific reference inter-vals for routine haemostatic assays during normal pregnancy.Clin Chim Acta 2012;413(1—2):258—61.
24] Masselli G, Derchi L, McHugo J, et al. Acute abdominal andpelvic pain in pregnancy: ESUR recommendations. Eur Radiol2013;23(12):3485—500.
25] Tremblay E, Therasse E, Thomassin-Naggara I, et al. Qualityinitiatives: guidelines for use of medical imaging during preg-nancy and lactation. Radiographics 2012;32(3):897—911.
uly 25, 2016.Inc. All rights reserved.

[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Abdominal emergencies during pregnancy
26] Patel SJ, Reede DL, Katz DS, et al. Imaging the pregnant patientfor nonobstetric conditions: algorithms and radiation dose con-siderations. Radiographics 2007;27(6):1705—22.
27] Bourjeily G, Chalhoub M, Phornphutkul C, et al. Neonatal thy-roid function: effect of a single exposure to iodinated contrastmedium in utero. Radiology 2010;256(3):744—50.
28] Oelsner G, Stockheim D, Soriano D, et al. Pregnancy outcomeafter laparoscopy or laparotomy in pregnancy. J Am AssocGynecol Laparosc 2003;10(2):200—4.
29] Reedy MB, Kallen B, Kuehl TJ. Laparoscopy during pregnancy:a study of five fetal outcome parameters with use of theSwedish Health Registry. Am J Obstet Gynecol 1997;177(3):673—9.
30] Reedy MB, Galan HL, Richards WE, et al. Laparoscopy duringpregnancy. A survey of laparoendoscopic surgeons. J ReprodMed 1997;42(1):33—8.
31] Colomb S, Bonnin M, Bolandard F, et al. Pregnant woman anaes-thetic management in gynaecologic laparoscopic surgery at thematernity hospital of Clermont-Ferrand. Ann Fr Anesth Reanim2006;25(1):11—6.
32] Chohan L, Kilpatrick CC. Laparoscopy in pregnancy: a literaturereview. Clin Obstet Gynecol 2009;52(4):557—69.
33] Nezhat FR, Tazuke S, Nezhat CH, et al. Laparoscopy duringpregnancy: a literature review. JSLS 1997;1(1):17—27.
34] Soper NJ. SAGES’ guidelines for diagnosis, treatment, and useof laparoscopy for surgical problems during pregnancy. SurgEndosc 2011;25(11):3477—8.
35] Fatum M, Rojansky N. Laparoscopic surgery during pregnancy.Obstet Gynecol Surv 2001;56(1):50—9.
36] Pearl J, Price R, Richardson W, et al. Guidelines for diagnosis,treatment, and use of laparoscopy for surgical problems duringpregnancy. Surg Endosc 2011;25(11):3479—92.
37] Jorgensen JO, Lalak NJ, North L, et al. Venous stasis dur-ing laparoscopic cholecystectomy. Surg Laparosc Endosc 1994;4(2):128—33.
38] Risk of and prophylaxis for venous thromboembolism in hospi-
tal patients. Thromboembolic Risk Factors (THRIFT) ConsensusGroup. BMJ 1992;305(6853):567—74.39] Casele HL. The use of unfractionated heparin and low-molecular-weight heparins in pregnancy. Clin Obstet Gynecol2006;49(4):895—905.
40] Cunningham FG, McCubbin JH. Appendicitis complicating preg-nancy. Obstet Gynecol 1975;45(4):415—20.
41] Finch DR, Lee E. Acute appendicitis complicating pregnancy inthe Oxford region. Br J Surg 1974;61(2):129—32.
42] Baer J, Reis R, Arens R. Appendicitis in pregnancy with changesin position and axis of the normal appendix in pregnancy. JAMA1932;52:1359—64.
43] Hodjati H, Kazerooni T. Location of the appendix in the gravidpatient: a re-evaluation of the established concept. Int JGynaecol Obstet 2003;81(3):245—7.
44] Basaran A, Basaran M. Diagnosis of acute appendicitis duringpregnancy: a systematic review. Obstet Gynecol Surv 2009;64(7):481—8 [quiz 499].
45] Israel GM, Malguria N, McCarthy S, et al. MRI vs. ultrasound forsuspected appendicitis during pregnancy. J Magn Reson Imaging2008;28(2):428—33.
46] Tamir IL, Bongard FS, Klein SR. Acute appendicitis in thepregnant patient. Am J Surg 1990;160:571—5.
47] Barnes SL, Shane MD, Schoemann MB, et al. Laparoscopicappendectomy after 30 weeks pregnancy: report of twocases and description of technique. Am Surg 2004;70(8):733—6.
[
[
[
[
[
[
[
[
[
[
Downloaded from ClinicalKey.com at National Certification CorporatioFor personal use only. No other uses without permission. Copyright ©2016. Elsev
S115
48] Lebeau R, Diane B, Koffi E, et al. Appendicitis and pregnancy:21 cases. J Gynecol Obstet Biol Reprod (Paris) 2005;34(6):600—5.
49] Tsimoyiannis EC, Antoniou NC, Tsaboulas C, et al. Cholelithiasisduring pregnancy and lactation. Prospective study. Eur J Surg1994;160(11):627—31.
50] Basso L, McCollum PT, Darling MR, et al. A study of cholelithi-asis during pregnancy and its relationship with age, parity,menarche, breast-feeding, dysmenorrhea, oral contraceptionand a maternal history of cholelithiasis. Surg Gynecol Obstet1992;175(1):41—6.
51] Hiatt JR, Hiatt JC, Williams RA, et al. Biliary disease inpregnancy: strategy for surgical management. Am J Surg1986;151(2):263—5.
52] Scott LD. Gallstone disease and pancreatitis in pregnancy. Gas-troenterol Clin North Am 1992;21(4):803—15.
53] Curet MJ. Special problems in laparoscopic surgery. Previousabdominal surgery, obesity, and pregnancy. Surg Clin North Am2000;80(4):1093—110.
54] Cosenza CA, Saffari B, Jabbour N, et al. Surgical manage-ment of biliary gallstone disease during pregnancy. Am J Surg1999;178(6):545—8.
55] Perdue PW, Johnson Jr HW, Stafford PW. Intestinal obstructioncomplicating pregnancy. Am J Surg 1992;164(4):384—8.
56] Pratt AT, Donaldson RC, Evertson LR, et al. Cecal volvulus inpregnancy. Obstet Gynecol 1981;57(6 Suppl.):37S—40S.
57] Yahchouchy E, Zaarour P, Prove S, et al. Recurrent idio-pathic small bowel volvulus during pregnancy. ANZ J Surg2001;71(3):193—4.
58] Connolly MM, Unti JA, Nora PF. Bowel obstruction in pregnancy.Surg Clin North Am 1995;75(1):101—13.
59] Ramin KD, Ramin SM, Richey SD, et al. Acute pancreatitis inpregnancy. Am J Obstet Gynecol 1995;173(1):187—91.
60] Swisher SG, Schmit PJ, Hunt KK, et al. Biliary disease duringpregnancy. Am J Surg 1994;168(6):576—9 [discussion 580—1].
61] Jamidar PA, Beck GJ, Hoffman BJ, et al. Endoscopic retrograde
cholangiopancreatography in pregnancy. Am J Gastroenterol1995;90(8):1263—7.62] Stimac D, Stimac T. Acute pancreatitis during pregnancy. Eur JGastroenterol Hepatol 2011;23(10):839—44.
63] Ducarme G, Maire F, Chatel P, et al. Acute pancreatitis duringpregnancy: a review. J Perinatol 2014;34(2):87—94.
64] El-Kady D, Gilbert WM, Anderson J, et al. Trauma during preg-nancy: an analysis of maternal and fetal outcomes in a largepopulation. Am J Obstet Gynecol 2004;190(6):1661—8.
65] Shah KH, Simons RK, Holbrook T, et al. Trauma in pregnancy:maternal and fetal outcomes. J Trauma 1998;45(1):83—6.
66] Pearlman MD, Tintinalli JE, Lorenz RP. Blunt trauma duringpregnancy. N Engl J Med 1990;323(23):1609—13.
67] Morris Jr JA, Rosenbower TJ, Jurkovich GJ, et al. Infant survivalafter cesarean section for trauma. Ann Surg 1996;223(5):481—8[discussion 488—91].
68] Henderson SO, Mallon WK. Trauma in pregnancy. Emerg MedClin North Am 1998;16(1):209—28.
69] Guichard G, Fromajoux C, Cellarier D, et al. Management ofrenal colic in pregnant women, based on a series of 48 cases.Prog Urol 2008;18(1):29—34.
70] Semins MJ, Matlaga BR. Kidney stones during pregnancy. NatRev Urol 2014;11(3):163—8.
71] Banhidy F, Acs N, Puho EH, et al. Maternal kidney stonesduring pregnancy and adverse birth outcomes, particularly con-genital abnormalities in the offspring. Arch Gynecol Obstet2007;275(6):481—7.
n July 25, 2016.ier Inc. All rights reserved.