
Decompressive Abdominal Laparotomy for Abdominal Compartment ...
S
Abdominal Compartment Syndrome A case base approach to Intra-Abdominal Hypertension & Abdominal Compartment Syndrome
Brandon Braddock, MPAS, PA-C
Pulmonary/Critical Care
Objectives
S Identify etiologies of Intra-abdominal hypertension and Abdominal compartment syndrome
S Identify clinical signs and symptoms of Intra-abdominal hypertension and Abdominal compartment syndrome
S Recognize and implement the use of bladder pressures for the diagnosis of Intra-abdominal hypertension and Abdominal compartment syndrome
S Recognize and understand treatment modalities for Intra-abdominal hypertension and Abdominal compartment syndrome
Patient History
S Patient S: 35 year old obese Caucasian female
S PMHx
S Chronic anemia
S Poly-substance abuse w/ IVDA
S Alcohol abuse
S Alcohol induced Cirrhosis
S R hip abscess
S Chronic pancreatitis
Surgical Hx
S Bilateral total hip arthroplasty – 2009
S Recurrent R hip infections and chronic dislocations
ED Presentation
S Chief Complaint:
S Altered mental status
S Last seen in her usual state of health by patient’s significant other one night prior when she went to bed.
S HPI:
S Reportedly, upon waking, the patient was confused and was repeatedly saying “I’m scared.” Patient’s significant other denied patient’s active IVDA however did report patient takes morphine & dilaudid which she obtained “on the streets”
ED Presentation cont.
S Vital Signs
S Temperature: 95.9° F
S Heart rate: 120bpm
S Respiration rate: 26 breaths/min
S SpO2: 95%
S Blood pressure: 79/48mmHg
S Relevant physical Exam:
S Pale, jaundiced appearing – moderate distress
S Lungs clear
S Normal BS, soft, non-tender, non-distended abdomen
S + Edema/erythema of R hip w/ blanching & purulent drainage
S Awake, alert – not following commands
ED Presentation cont.
S Relevant Lab Results
S WBC 3.1
S Hgb 5.8
S Platelets: 127
S aPTT 68.4
S PT 34.1/INR 3.44
S Glucose 149
S BUN 10/Cr 2.9
S Sodium 126
S Potassium 2.7
S Arterial lactate 4.55
S Relevant Imaging Studies
S CT brain – neg
S CT abdomen/pelvis - pancolitis, chronic pancreatitis, bibasilar consolidation
S CT R. lower extremity – Chronic hip dislocation, surrounding edema
Assessment
S Severe sepsis with septic shock and multi-organ failure secondary to:
S Pancolitis
S PNA
S UTI
S Cx (+) MSSA Bacteremia
S Acute hypoxemic respiratory failure defined as hypoxemia w/ PaO2 < 60 on ABG
S Required intubation & full MVS
S Septic shock induced hypotension defined as: a systolic BP less than 90mmHg for a period greater than 15 minutes despite adequate fluid resuscitation or Lactate > 4 (previous guidelines)
S Refractory to IVF (30ml/kg) & required vasopressor support
Assessment cont.
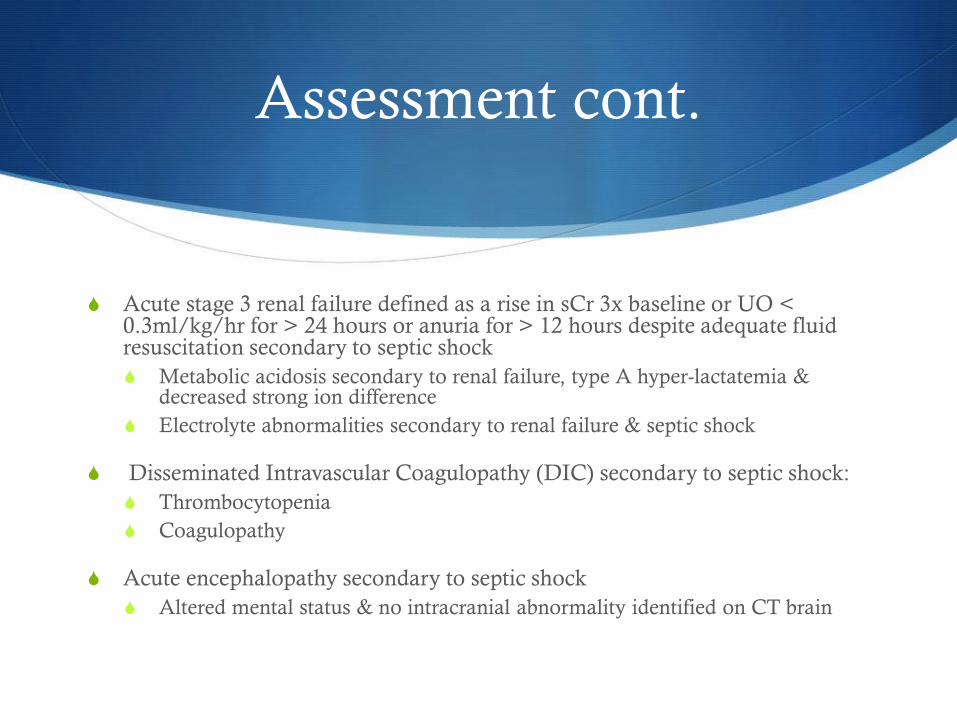
S Acute stage 3 renal failure defined as a rise in sCr 3x baseline or UO < 0.3ml/kg/hr for > 24 hours or anuria for > 12 hours despite adequate fluid resuscitation secondary to septic shock
S Metabolic acidosis secondary to renal failure, type A hyper-lactatemia & decreased strong ion difference
S Electrolyte abnormalities secondary to renal failure & septic shock
S Disseminated Intravascular Coagulopathy (DIC) secondary to septic shock:
S Thrombocytopenia
S Coagulopathy
S Acute encephalopathy secondary to septic shock
S Altered mental status & no intracranial abnormality identified on CT brain
Clinical Course
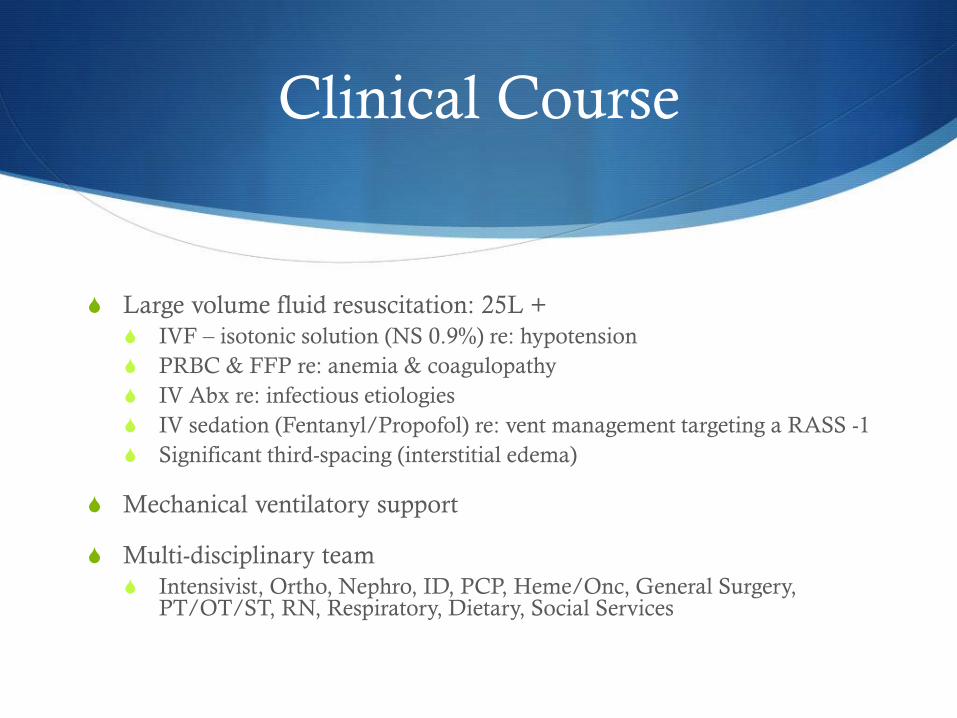
S Large volume fluid resuscitation: 25L +
S IVF – isotonic solution (NS 0.9%) re: hypotension
S PRBC & FFP re: anemia & coagulopathy
S IV Abx re: infectious etiologies
S IV sedation (Fentanyl/Propofol) re: vent management targeting a RASS -1
S Significant third-spacing (interstitial edema)
S Mechanical ventilatory support
S Multi-disciplinary team
S Intensivist, Ortho, Nephro, ID, PCP, Heme/Onc, General Surgery, PT/OT/ST, RN, Respiratory, Dietary, Social Services
Repeat Physical Exam
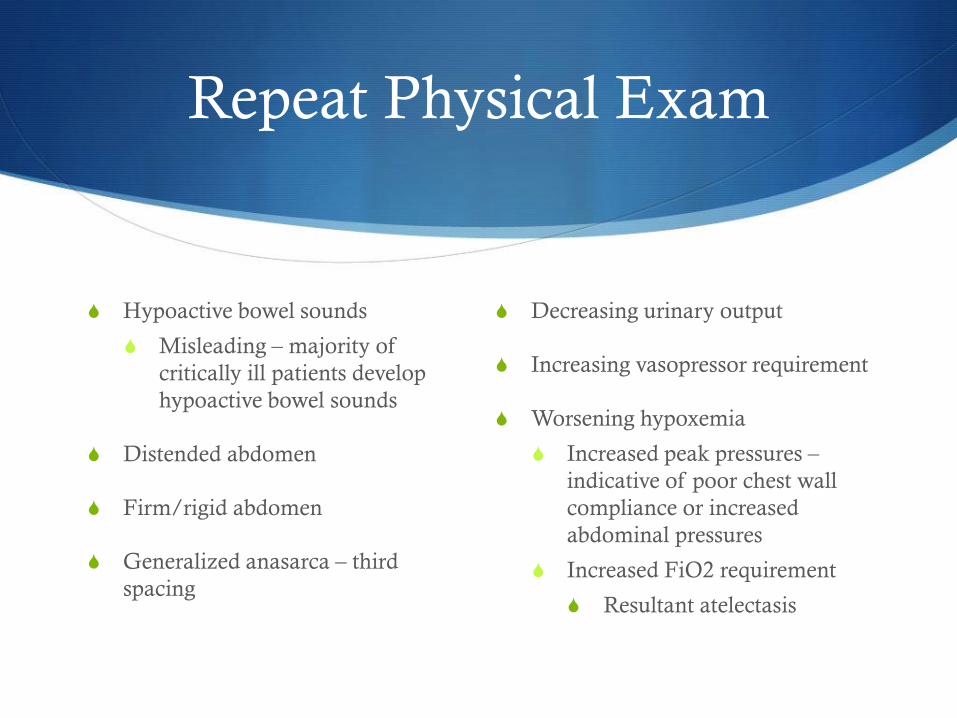
S Hypoactive bowel sounds
S Misleading – majority of
critically ill patients develop
hypoactive bowel sounds
S Distended abdomen
S Firm/rigid abdomen
S Generalized anasarca – third
spacing
S Decreasing urinary output
S Increasing vasopressor requirement
S Worsening hypoxemia
S Increased peak pressures –
indicative of poor chest wall
compliance or increased
abdominal pressures
S Increased FiO2 requirement
S Resultant atelectasis
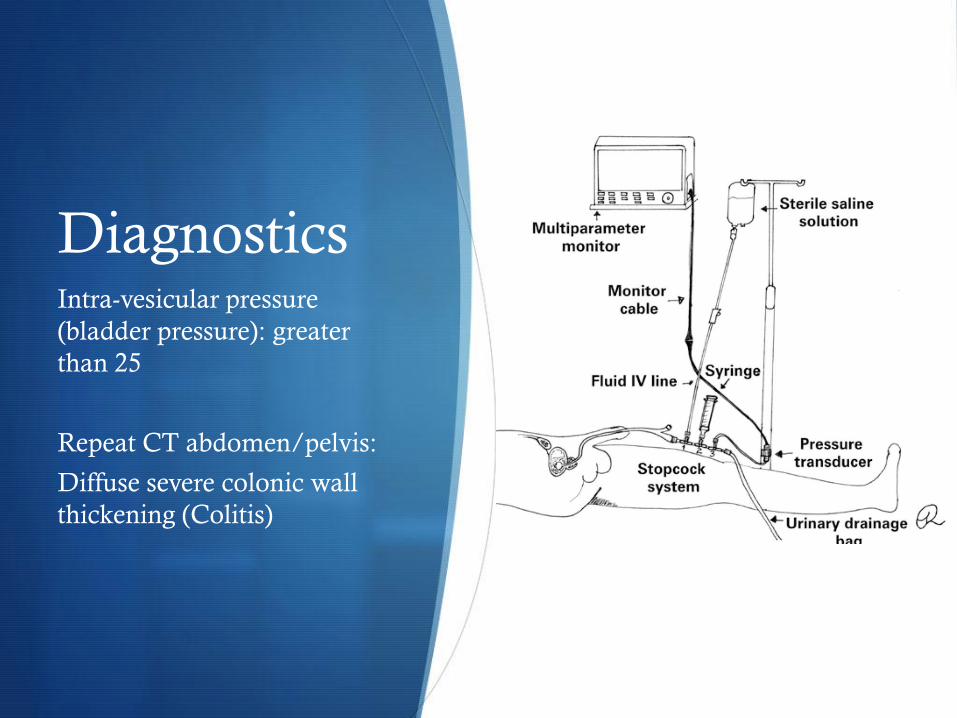
Diagnostics Intra-vesicular pressure
(bladder pressure): greater
than 25
Repeat CT abdomen/pelvis:
Diffuse severe colonic wall
thickening (Colitis)
Assessment 2.0
S Severe sepsis with septic shock and multi-
organ failure – refractory to aggressive
treatment
S Required multiple vasopressors
S Acute hypoxemic respiratory failure –
declining status with increased V/Q
mismatch + hypervolemia induced
pulmonary edema requiring - increased
PEEP & FiO2
S Acute stage 3 renal failure – progressive to
anuria despite optimal fluid resuscitation
& improved sCr
S DIC – refractory w/ worsening
coagulopathy – INR rising
Assessment 2.0 cont.
S Acute cholestasis secondary to septic
shock as evident by rising
aminotransferases & bilirubin
S Critical-illness related adrenal insufficiency
– required stress dose steroids
S Worsening metabolic acidosis w/ pH 7.0
by ABG & worsening hyper-lactatemia
despite initial improvement
S DDx now includes
S Intra-abdominal hypertension &
abdominal compartment syndrome as
a result of
S Diffuse colitis & generalized ileus
S Cholestasis
S Septic shock
S Profound interstitial edema
secondary to large volume
resuscitation and septic shock
induced capillary leak
Defining IAH & ACS
S Intra-Abdominal Hypertension (IAH)
S A steady state pressure of greater than 12mmHg concealed within the abdominal cavity
S Abdominal Perfusion Pressure (APP)
S Defined as Mean Arterial Pressure (MAP) – Intra-Abdominal Pressure (IAP)
S Abdominal Compartment Syndrome (ACS)
S A sustained IAP > 20mmHg (with or without an APP < 60) that is associated with new organ dysfunction/failure – research purposes

Defining IAH & ACS
S Primary Intra-Abdominal Hypertension or ACS
S Condition associated with injury or disease originating from
the abdomino-pelvic cavity
S Secondary Intra-Abdominal Hypertension or ACS
S Condition associated with injury or disease not originating
from the abdomino-pelvic cavity
Intra-abdominal Hypertension
S Grade I- defined as intra-abdominal pressure 12-15 mmHg
S Grade II- defined as intra-abdominal pressure 16-20 mmHg
S Grade III- defined as intra-abdominal pressure 21-25 mmHg
S Grade IV- defined as intra-abdominal pressure > 25 mmHg
IAH Acuity
S Acute
S Elevated IAP developing over the course of several hours i.e trauma, intra-abdominal hemorrhage – concerning for progression to ACS
S Subacute
S Elevated IAP developing over days i.e. critically ill patients
S Critically ill patients generally have an IAP 5-7mmHg
S Chronic
S Elevated IAP developing over months/years i.e pregnancy, obesity – generally not progressive to ACS
Risk Factors
Primary
S Abdominal trauma
S Abdominal surgery
S Cirrhosis w/ascites
S Gastroparesis/ileus
S Ogilvie’s syndrome
S Volvulus
S Pancreatitis
S Abdominal abscess
S Retroperitoneal bleed
Secondary
S Large IVF resuscitation
S Mechanical ventilation
S Sepsis and/or septic shock
S Burns
S Metabolic acidosis
S Third spacing/interstitial
edema
Physiologic Consequence Cardiovascular
S Impaired cardiac function
S Increased IAP leads to reduced ventricular compliance & contractility
S Can occur at IAP as low as 10mmHg
S Exacerbated in underlying heart failure
S Reduced venous return
S Increased IAP leads to compressed IVC and decreased preload & decreased cardiac output – exacerbated by hypovolemia
S Increased systemic vascular resistance & venous hydrostatic pressure
S Increased third spacing & DVT risk
Physiologic Consequence Pulmonary
S Increased risk of alveolar barotrauma
S Increased peak & plateau pressures
S Reduced lung & chest wall compliance
S Increased V/Q mismatch – arterial hypoxemia & hypercapnia
S Accentuated in patient’s requiring large IVF, bronchospasm (COPD exacerbation) & pt’s requiring increased PEEP
S Increased risk of pulmonary infection/ventilator acquired pneumonia
S Increased duration of vent support – poor ventilation
S Increased atelectasis, edema, pleural effusions
S May require NIPPV and/or MVS if not already
Physiologic Consequence Renal
S Renal vein compression
S Increases venous resistance and impaired venous drainage; studies
suggest the primary cause of renal impairment
S Renal artery vasoconstriction & sympathetic response
S Induced by sympathetic nervous system & RAAS system due to decreased cardiac output
S Oliguria typically noted when IAP > 15mmHg
S Anuria occurring when IAP > 30mmHg
Physiologic Consequence Gastrointestinal
S Mesenteric ischemia
S Decreased mesenteric vein flow due to increased intestinal edema
leading to worsening IAP and possibly ACS as well as bowel necrosis
and lactic acidosis – vicious cycle
S Studies suggested mesenteric blood flow is reduced with an IAP as
low as 10mmHg
S Intestinal mucosal perfusion decreased with IAP > 20mmHg
Physiologic Consequence Gastrointestinal
S Bowel hypo-perfusion
S Targeting abdominal profusion pressure – 60mmhg (MAP – IAP)
S Increased bacterial translocation
S Can occur at IAP of only 10mmHg – more prominent in cases of hemorrhage
S Hepatic dysfunction
S Impaired toxin clearance i.e Lactate
S Impaired production of coagulation factors
S Impaired protein production i.e Albumin
S Leads to decreased hydrostatic pressure & development of ascites & increased IAP
S Exacerbated in patients with underlying liver disease; our patient has a hx of EtOH
cirrhosis

Physiologic Consequence Central Nervous System
Cerebral Ischemia
S Increased intracranial pressure
leading to decreased cerebral
perfusion & ultimately cerebral
ischemia
S Secondary to decreased
venous return/decreased
cardiac output

Symptoms
S Generalized complaints
S Malaise/fatigue
S Weakness
S Dyspnea
S Abdominal bloating
S Abdominal pain
S Limitations in patient
assessment/symptoms
S Patient’s unable to
communicate
S Encephalopathic
S Mechanical ventilatory
support
Physical Signs
S Distended/firm abdomen
S Decreased bowel sounds - misleading
S Significant third spacing
S + Fluid wave (ascites)
S Increased JVD
S Worsening obtundation
S Cool/diaphoretic skin
S Progressive organ dysfunction despite
treatment
S Progressive oliguria/anuria
S Increased vent support
S Increased FiO2
S Increased PEEP
S Decreased tidal volumes
S Refractory hypotension
Physical Signs
S Limitation in physical exam
S Poor predictor of ACS; prospective cohort study (N=42) of
blunt abdominal trauma demonstrated:
S Sensitivity 56%
S Specificity 87%
S PPV 35%
S NPV 94%
Diagnostics
S Imaging: not helpful in the diagnosis of ACS
S Chest radiograph may show:
S Low lung volumes, raised hemi-diaphragm, atelectasis
S CT abdomen/pelvis may show:
S Extrinsic compression of IVC
S Abdominal distention
S Renal compression
S Bowel thickening
S Inguinal herniation
Diagnostics
S Definite dx requires intra-abdominal pressure monitoring
S Can be measured via multiple modalities including:
S Intragastric
S Intracolonic
S Intravesicular (bladder)
S IVC catheters
S Gold standard as defined by the WSACS for IAH/ACS screening:
S Intravesicular (bladder) pressure
Bladder Pressure Technique
S Patient must be in supine position
S Clamp Foley catheter drainage tube
S Instill a maximum of 25ml sterile saline into the bladder via the aspiration port of the Foley
S 18g needle attached to a pressure transducer is inserted into the aspiration port (needle-less systems available)
S Pressure is measured at end-expiration once the transducer is zeroed at the level of the mid-axillary line
Therapeutic Interventions
Noninvasive Bowel Decompression
S Nasogastric or orogastric tube placement
S Placement of bowel management systems. i.e Rectal tube placement
S Maintain supine position or head of bed no greater than 30 degrees of elevation if possible (risk assessment for VAP, aspiration, ICP)
Invasive Decompression
S Procedure dependent upon cause
S Ascites paracentesis
S Abdominal
abscess/hematoma/hemoperi
toneum percutaneous
needle aspiration
S Burns escharotomy
Therapeutic Interventions
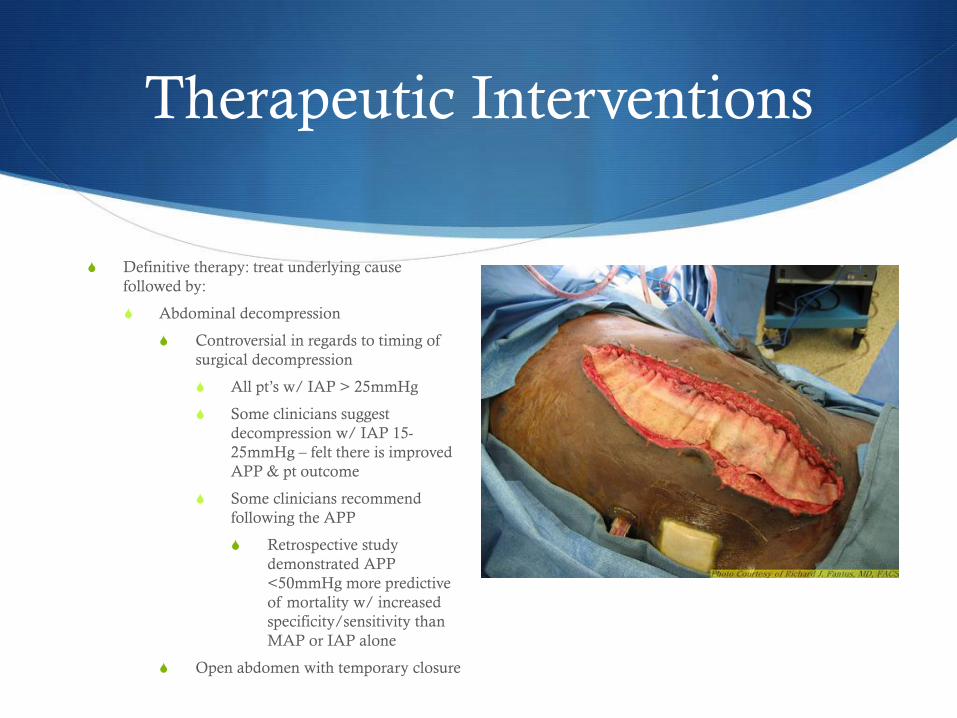
S Definitive therapy: treat underlying cause
followed by:
S Abdominal decompression
S Controversial in regards to timing of
surgical decompression
S All pt’s w/ IAP > 25mmHg
S Some clinicians suggest
decompression w/ IAP 15-
25mmHg – felt there is improved
APP & pt outcome
S Some clinicians recommend
following the APP
S Retrospective study
demonstrated APP
<50mmHg more predictive
of mortality w/ increased
specificity/sensitivity than
MAP or IAP alone
S Open abdomen with temporary closure
Therapeutic Intervention
Patient S
S Due to patient’s refractory and progressive multi-organ failure in conjunction with elevated intra-vesicular pressures she underwent abdominal decompression and was noted intra-operatively to have IAP in excess of 20mmHg
S She was transferred back to SICU post-operatively in critical condition however tolerated the procedure adequately
S Vasopressor requirement had improved
S 24hrs post-op she underwent closure of
her open abdomen after resolution of
the acute phase of her abdominal
compartment syndrome
Outcome
S Unfortunately, due to patient S’s severe and refractory multi-
organ failure triggered by severe sepsis and septic shock
further treatment was deemed futile.
S At the discretion of her significant other, as well as input
from a multifaceted team, a terminal wean was requested.
S Ultimately, the patient succumbed to her illness following
withdrawal of life support.

Summary
S Intra-abdominal Hypertension & Abdominal Compartment Syndrome can be caused by numerous etiologies both primary and secondary
S Early recognition of developing signs/symptoms prompts urgent treatment
S Although IAH alone is not a predictor of MOF, mortality for patients who progress to ACS ranges from 40-100 percent
S Bladder pressures remain the gold standard for IAP monitoring
S Definitive treatment is by surgical abdominal decompression
References
S Gestring, M. M. (2015, February 5). Abdominal Compartment Syndrome. (H. Sanfey, & E. Bulger, Editors) Retrieved April 2016, from Up to Date: http://www.uptodate.com/contents/abdominal-compartment-syndrome
S World Society of Abdominal Compartment Syndrome. (2013). World Society of Abdominal Compartment Syndrome. Retrieved from WSACS.org: www.WSACS.org
S Malbrain ML, Cheatham ML, Kirkpatrick A, et al. Results from the International Conference of Experts on Intra-abdominal Hypertension and Abdominal Compartment Syndrome. I. Definitions. Intensive Care Med 2006; 32: 1722.
S Cheatham ML, White MW, Sagraves SG, et al. Abdominal perfusion pressure: a superior parameter in the assessment of intra-abdominal hypertension. J Trauma 2000; 49:621
S Bloomfield GL, Dalton JM, Sugerman HG, et al. Treatment of increasing intracranial pressure secondary to the acute abdominal compartment syndrome in a patient with combined abdominal and head trauma. J Trauma 1995; 39:1168.
S Citerio G, Vascotto E, Villa F, et al. Induced abdominal compartment syndrome increases intracranial pressure in neurotrauma patients: a prospective study. Crit Care Med 2001; 29:1466
S Joseph DK, Dutton RP, Aarabi B, Scalea TM. Decompressive laparotomy to treat intractable intracranial hypertension after traumatic brain injury. J Trauma 2004; 57:687
S Kirkpatrick AW, Brenneman FD, McLean RF, et al. Is clinical examination an accurate indicator of raised intra-abdominal pressure in critically injury patients? Can J Surg 2000; 43:207.
S Sugrue M, Bauman A, Jones F, et al. Clinical examination is an inaccurate predictor of intraabdominal pressure. World J Surg 2002; 26:1428
S Balogh ZJ, martin A, Van Wessem KP, et al. Mission ot eliminate postinjury abdominal compartment syndrome. Arch Surg 2011; 146:938
S De Waele JJ, Kimball E, Malbrain M, et al Decompressive laparotomy for abdominal compartment syndrome. Br J Surg 2016.
S An G, West MA. Abdominal compartment syndrome: a concise clinical review. Crit Care Med 2008; 36: 1304
S Kron IL, Harman PK, Nolan SP. The measurement of intra-abdominal pressure as a criterion for abdominal re-exploration. Ann Surg 1984; 199: 28




![Abdominal compartment syndrome[1]](https://static.fdocuments.in/doc/165x107/556ca315d8b42a44468b4d32/abdominal-compartment-syndrome1.jpg)
![Original Article Open components separation and underlay ... · ma, pancreatitis, peritonitis, abdominal vascu-lar emergencies, and abdominal compartment syndrome (ACS) [4]. Patients](https://static.fdocuments.in/doc/165x107/5f0b59517e708231d430136f/original-article-open-components-separation-and-underlay-ma-pancreatitis-peritonitis.jpg)












