
ABC_of_Psychological_Medicine.pdf
69
Edited by Richard Mayou, Michael Sharpe and Alan Carson ABC OF PSYCHOLOGICAL MEDICINE
-
Upload
maxim-popescu -
Category
Documents
-
view
214 -
download
0
Transcript of ABC_of_Psychological_Medicine.pdf
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 1/69
Edited by Richard Mayou, Michael Sharpe and Alan Carson
ABCOF
PSYCHOLOGICAL
MEDICINE

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 2/69
ABC OF
PSYCHOLOGICAL MEDICINE

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 3/69

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 4/69
ABC OFPSYCHOLOGICAL MEDICINE
Edited by
RICHARD MAYOU
Professor of Psychiatry, University of Oxford, Warneford Hospital, Oxford
MICHAEL SHARPEReader in Psychological Medicine, University of Edinburgh
and
ALAN CARSONConsultant Neuropsychiatrist, NHS Lothian and Honorary Senior Lecturer,
University of Edinburgh

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 5/69
© BMJ Publishing Group 2003
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system,or transmitted, in any form or by any means, electronic, mechanical, photocopying,recording and/or otherwise, without the prior written permission of the publishers.
First published in 2003
by BMJ Books, BMA House, Tavistock Square,London WC1H 9JR
www.bmjbooks.com
British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Librar y
ISBN 0 7279 1556 8
Typeset by Newgen Imaging Systems and BMJ Electronic ProductionPrinted and bound in Spain by GraphyCems, Navarra
Cover image depicts computer artwork of a face patterned with vertical lines with a magneticresonance imaging (MRI) scan in the background. The MRI scan allows the internal features of
the head to be seen. At the centre is the nasal cavity (red), and above that is the front part of the brain (blue and red). This region of the brain is part of the cerebrum, and is concerned
with conscious thought, personality and memor y. With permission from
Alfred Pasieka/Science Photo Library.
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 6/69
v
Contents
Contributors vi
Preface vii
Introduction viii
1 The consultation 1
Linda Gask, Tim Usherwood
2 Beginning treatment 4
Jonathan Price, Laurence Leaver
3 Organising care for chronic illness 7
Michael Von Korff, Russell E Glasgow, Michael Sharpe
4 Depression in medical patients 10
Robert Peveler, Alan Carson, Gary Rodin
5 Anxiety in medical patients 14
Allan House, Dan Stark
6 Functional somatic symptoms and syndromes 17
Richard Mayou, Andrew Farmer
7 Chronic multiple functional somatic symptoms 21
Christopher Bass, Stephanie May
8 Cancer 25
Craig A White, Una Macleod
9 Trauma 29
Richard Mayou, Andrew Farmer
10 Fatigue 33
Michael Sharpe, David Wilks
11 Musculoskeletal pain 37
Chris J Main, Amanda C de C Williams
12 Abdominal pain and functional gastrointestinal disorders 41
Elspeth Guthrie, David Thompson
13 Chest pain 44
Christopher Bass, Richard Mayou
14 Delirium 48
Tom Brown, Michael Boyle
Index 53

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 7/69
vi
Christopher Bass
Consultant, Department of Psychological Medicine,
John Radcliffe Hospital, Oxford
Michael Boyle
General Practitioner, Linlithgow Health Centre, Linlithgow,
West Lothian
Tom Brown
Consultant Psychiatrist, St John’s Hospital at Howden,
Livingston, West Lothian
Alan CarsonConsultant Neuropsychiatrist, NHS Lothian and Honorary
Senior Lecturer, University of Edinburgh
Andrew Farmer
Senior Research Fellow, Department of Public Health and
Primary Care, University of Oxford
Linda Gask
Reader in Psychiatry, University of Manchester
Russell E Glasgow
Senior Scientist, AMC Cancer Research Center, Denver,
Colorado, USA
Elspeth Guthrie
Professor of Psychological Medicine and Medical Psychotherapy,
School of Psychiatry and Behavioural Sciences, University of
Manchester
Allan House
Professor of Liaison Psychiatry, Academic Unit of Psychiatry and
Behavioural Sciences, School of Medicine, University of Leeds
Michael Von Korff
Senior Investigator, Center for Health Studies, Group Health
Cooperative of Puget Sound, Seattle, WA, USA
Laurence LeaverGeneral Practitioner, Jericho Health Centre, Oxford
Una Macleod
Lecturer in General Practice, Department of General Practice,
University of Glasgow
Chris J Main
Head of the Department of Behavioural Medicine, Hope
Hospital, Salford
Stephanie May
General Practitioner, Stockwell Group Practice,
Stockwell Road, London
Richard Mayou
Professor of Psychiatry, University of Oxford,
Warneford Hospital, Oxford
Robert Peveler
Professor of Liaison Psychiatry, University of Southampton
Jonathan Price
Clinical Tutor in Psychiatry, Department of Psychiatry,
University of Oxford
Gary Rodin
Professor of Psychiatry, University of Toronto, Canada
Michael Sharpe
Reader in Psychological Medicine,
University of Edinburgh
Dan Stark
Specialist Regsitrar in Medical Oncology,
Academic Unit of Oncology, St James’s University Hospital,
Leeds
David Thompson
Professor of Medicine, Section of Gastrointestinal Science,
Hope Hospital, Salford
Tim Usherwood
Professor in General Practice, University of Sydney,
NSW, Australia
Craig A White
Macmillan Consultant in Psychosocial Oncology,
Ayrshire and Arran Primary Care NHS Trust
David Wilks
Consultant in Infectious Diseases, Western General Hospital,
Edinburgh
Amanda C de C Williams
Senior Lecturer in Clinical Health Psychology,
Guy’s, King’s, and St Thomas’s School of Medicine,
University of London
Contributors

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 8/69
vii
Preface
Psychological medicine has a long history. Until the development of pharmacological and other specific treatments, it was a mainstay
of a physician’s practice. Since then the successes of biomedical theory during the 20th century have led to a loss of interest in
the psychological aspects of medicine and core clinical skills have sometimes been neglected. Although many modern doctors
are comfortable with the latest advances in molecular medicine, they lack confidence in applying similar intellectual rigour to the
psychological problems of their patients. These deficiencies are particularly apparent in the management of patients with chronic
disease and of patients whose symptoms seem out of proportion to disease pathology.
Accumulating research evidence now clearly shows that psychological variables make a substantial contribution to the outcome
of most common medical conditions. The identification of problems, appropriate formulation and the implementation of
appropriate treatment results in not only better outcomes for patients but also in greater satisfaction for the doctors treating them.
A rediscovery of the psychological aspects of medicine is underway.
This ABC of psychological medicine is a practical and evidence based overview of the psychological aspects of medical practice. It
aims to guide practitioners and to provide them with not only relevant information but also an intellectual structure for assessing
and managing their patients. The emphasis is on day to day practice and problems rather than psychological theory. The bookassumes knowledge of medical assessment, investigation, and treatment.
The opening three chapters describe general principles within which individual assessment and treatment can be formulated.
They include the clinical examination and the initiation of treatment but also a critique of the structure within which care is
delivered, which can often be as critical as the individual’s consultation. The following three chapters describe the core skills of
psychological medicine: the assessment and management of anxiety, depression, and functional somatic symptoms. The remaining
chapters then describe how these skills are transferred and adapted in specific situations including the care of patients with cancer,
trauma, musculoskeletal pain, fatigue, chest pain, abdominal pain, and delirium. This list is not comprehensive but provides a range
of examples that should help the reader to adapt the principles to their own practice.
Psychological medicine is an extension of existing clinical knowledge and skills. Indeed many practitioners will recognise it as
a formalisation of the medicine they have been practising for many years. We hope that this book will both engage the curiosity
and interest of those to whom the subject matter is novel, and encourage and inform those who already understand and apply
its principles.
Richard Mayou, Michael Sharpe, Alan J Carson, 2002

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 9/69
viii
Introduction
It is becoming increasingly clear that we can improve medical care by paying more attention to psychological aspects of medicalassessment and treatment. The study and practice of such factors is often called psychological medicine. Although the development of specialist consultation-liaison psychiatry (liaison psychiatry in the United Kingdom) and health psychology contribute topsychological medicine, the task is much wider and has major implications for the organisation and practice of care. This book aimsto explain some of those implications.
Disorders that are traditionally, and perhaps misleadingly, termed “psychiatric” are highly prevalent in medical populations. At least 25-30% of general medical patients have coexisting depressive, anxiety, somatoform, or alcohol misuse disorders.1 Several factorsaccount for the co-occurrence of medical and psychiatric disorders. First, a medical disorder can occasionally be a cause of thepsychiatric disorder (for example, hypothyroidism as a biological cause of depression). Second, cardiovascular diseases, neurologicaldisorders, cancer, diabetes, and many other medical diseases increase the risk of depression and other psychiatric disorders. Such socalled comorbidity is common, but its causal linkage with psychological conditions remains poorly understood. A third factor iscoincidence—common conditions such as hypertension and depression may coexist in the same patient because both are prevalent.
Another reason for psychological medicine is the prevalence of symptoms that are unexplained by disease. Although physicalsymptoms account for more than half of all visits to doctors, at least a third of these symptoms remain medically unexplained.2,3 Thisphenomenon is referred to as somatisation—the seeking of health care for somatic symptoms that suggest a medical disorder but represent instead an underlying depressive, anxiety, or somatoform disorder. Most patients with these mental disorders preferentially report somatic rather than emotional symptoms. Further, there are the common but poorly understood symptom syndromes suchas fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome, for which the relative contributions of mind and body arenot yet elucidated.4
Psychological medicine is important in the management of all these problems; both psychotropic medications and cognitivebehavioural treatments have proved effective in the treatment of common physical symptoms and syndromes in numerous studiesin general practice.5,6 Although such treatments have traditionally been considered “psychiatric”, they are also beneficial in patients
without overt psychiatric disorders. Countries on both sides of the Atlantic have a long way to go in developing psychologicalmedicine, the chasm in America between medical and psychiatric care is particularly deep. The “carve out” or organisationalseparations of mental health services in the managed care systems in the United States is one example of how ingrained the dualism
of mind and body still is and of the reconciliation that must occur.Psychological medicine does not mean relabelling all such patients as “psychiatric”. Many patients prefer to have these problemsregarded as “medical” and conceptualised in terms of a neurotransmitter imbalance or a functional bodily disturbance.7 Concomitant psychological distress is best framed in terms of being a consequence rather than a cause of persistent physical symptoms. Prematureefforts to reattribute somatic complaints to psychological mechanisms may be perceived by the patient as rejection. A moreaetiologically neutral but psychologically sophisticated approach that initially focuses on symptomatic treatment, reassurance,activation, and restoration of function has proved more effective.8
There are better alternatives than simply to relegate such problems to the province of specialist psychiatry. One is to train generalpractitioners to diagnose and treat common “psychiatric” disorders.9 Although treatment with psychotropic medication is their most feasible option, general practitioners can also be trained to deliver other psychological treatments. A second option is to use nursesor social workers with specialised training who can work with general practitioners or psychiatrists to manage medication as well asdeliver psychotherapies and behavioural interventions. A third model is collaborative care, where the general practitioner’smanagement is augmented but not replaced by visits to a psychiatrist, often on site in the general practitioner’s surgery. Stepped careprovides an overall principle of management whereby patients only move on to more complex and expensive forms of care where
simpler management by the healthcare team is either ineffective or inappropriate. Most studies have been conducted in generalmedical practices, but patients seen by medical specialists also warrant attention.3
Psychological medicine may also be delivered in innovative ways. Promising data exist for behavioural interventions conductedoutside the doctor’s office, including case management by telephone, cognitive behavioural therapy given through a computer,bibliotherapy—self study by patients—and home visits (for example, for chronic fatigue syndrome).
Medical treatment that integrates a psychological approach has been shown to improve patient outcomes. The benefits of treatingcommon physical symptoms and psychological distress effectively in medical patients include not only improved quality of life andsocial and work functioning, but also greater satisfaction on the part of patient and doctor and reduced use of healthcare services.2
What do we need to do? Better detection of these problems need not be time consuming. For example, screening for depressionmay require as few as one or two questions. Optimal management of patients with persistent physical symptoms and common mentaldisorders may require longer or more frequent visits to a doctor, help in educating and following up patients by a nurse casemanager, other system changes, and specialist mental health consultations for more complex cases.10 The competing demands of general practice must be explicitly addressed if we are to enable the general practitioner to practise psychological medicine
effectively.11
Yet this approach is no different to what is also required for many chronic medical disorders such as diabetes, asthma, and heart disease, for which it has been proved that care in concordance with guidelines requires appreciable reorganisation of medicalservices.12

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 10/69
ix
Neither chronic “medical” nor “psychiatric” disorders can be managed adequately in the current environment of generalpractice, where the typical patient must be seen in 10–15 minutes or less. The quick visit may work for the patient with a commoncold or a single condition, such as well controlled hypertension, but will not suffice for the prevalent and disabling symptoms anddisorders comprising psychological medicine. Evidence based treatments exist. Using them in a way that is integrated with generalmedical care will improve both patients’ physical health and their psychological wellbeing.
Kurt Kroenke*Professor of Medicine, Department of Medicine,
Regenstrief Institute for Health Care,Indianapolis, IN, USA
* KK has received fees for speaking and research from Pfizer and Eli Lilly.
References
1. Ormel J, Von Korff M, Ustun TB, Pini S, Korten A, Oldehinkel T. Common mental disorders and disability across cultures: resultsfrom the WHO collaborative study on psychological problems in general health care. JAMA 1994;272:1741-48.
2. Kroenke K. Studying symptoms: sampling and measurement issues. Ann Intern Med 2001;134:844-55.3. Reid S, Wessely S, Crayford T, Hotopf M. Medically unexplained symptoms in frequent attenders of secondary health care:
retrospective cohort study. BMJ 2001;322:1-4.
4. Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many? Lancet 1999;354:936-9.5. O’Malley PG, Jackson JL, Santoro J, Tomkins G, Balden E, Kroenke K. Antidepressant therapy for unexplained symptoms andsymptom syndromes. J Fam Pract 1999;48:980-90.
6. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlledclinical trials. Psychother Psychosom 2000;69:205-15.
7. Sharpe M, Carson A. “Unexplained”somatic symptoms, functional syndromes, and somatization: do we need a paradigm shift?Ann Intern Med 2001;134:926-30.
8. Von Korff M, Moore JC. Stepped care for back pain: activating approaches for primary care. Ann Intern Med 2001;134:911-17.9. Kroenke K, Taylor-Vaisey A, Dietrich AJ, Oxman TE. Interventions to improve provider diagnosis and treatment of mental
disorders in primary care: a critical review of the literature. Psychosomatics 2000;41:39-52.10. Rubenstein LV, Jackson-Triche M, Unutzer J, Miranda J, Minnium K, Pearson ML, et al. Evidence-based care for depression in
managed primary care practices. Health Aff 1999;18:89-105.11. Klinkman MS. Competing demands in psychosocial care: a model for the identification and treatment of depressive disorders in
primary care. Gen Hosp Psychiatry 1997;19:98-111.
12. Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q 1996;74:511-44.
Introduction

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 11/69

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 12/69
1 The consultationLinda Gask, Tim Usherwood
The success of any consultation depends on how well thepatient and doctor communicate with each other. There is now
firm evidence linking the quality of this communication toclinical outcomes.
The dual focus —Patients are not exclusively physically ill or exclusively emotionally distressed. Often they are both. At thestart of a consultation it is usually not possible to distinguish
between these states. It is the doctor’s task to listen actively tothe patient’s story, seeking and noticing evidence for bothphysical illness and emotional distress.
Involving patients —Changes in society and health care in thepast decade have resulted in real changes in what people expect from their doctors and in how doctors view patients. Inaddition, greater emphasis has been placed on the reduction of risk factors, with attempts to persuade people to take preventive
action and avoid risks to health. Many patients want moreinformation than they are given. They also want to take somepart in deciding about their treatment in the light of its chancesof success and any side effects. Some patients, of course, do not
wish to participate in decision making; they would prefer their doctor to decide on a single course of action and to advise themaccordingly. The skill lies in achieving the correct balance for each patient.
A comprehensive model — The “three function” model for themedical encounter provides a template for the parallelfunctions of the clinical interview. This is now widely used inmedical schools.
Starting the interviewResearch has shown the importance of listening to patients’opening statements without interruption. Doctors often ask about the first issue mentioned by their patients, yet this maynot be what is concerning them most. Once a doctor hasinterrupted, patients rarely introduce new issues. If uninterrupted, most patients stop talking within 60 seconds,often well before. The doctor can then ask if a patient has anyfurther concerns, summarise what the patient has just said, or propose an agenda —“I wonder if I could start by asking yousome more questions about your headaches, then we need todiscuss the worries that your son has been causing you.”
Detecting and responding to emotional issuesEven when their problems are psychological or social, patientsusually present with physical symptoms. They are also likely togive verbal or non-verbal cues. Verbal cues are words or phrasesthat hint at psychological or social problems. Non-verbal cuesinclude changes in posture, eye contact, and tone of voice that reflect emotional distress.
It is important to notice and respond to cues at the timethey are offered by patients. Failure to do so may inhibit patients from further disclosures and limit the consultation todiscussion of physical symptoms. Conversely, physicalsymptoms must be taken seriously and adequately evaluated.
Several of the skills of active listening are valuable in discussing physical, psychological, and social issues with patients. Theseskills have been clearly shown to be linked to recognition of emotional problems when used by general practitioners.
Three functions of the medical consultation
1 Build the relationshipx Greet the patient warmly and by namex Detect and respond to emotional issues
x Active listening
2 Collect datax Do not interrupt patient x Elicit patient’s explanatory model
x Consider other factorsx Develop shared understanding
3 Agree a management plan
x Provide informationx Appropriate use of reassurancex Negotiate a management plan
x Make linksx Negotiate behaviour change
Responding to patients’ “cues”
Verbal cuesx State your observation—“You say that recently you have been
feeling fed-up and irritable”x Repeat the patient’s own words—“Not well since your mother died”x Seek clarification—“What do you mean when you say you always
feel tired?”
Non-verbal cuesx Comment on your observation—“I can hear tears in your voice”x
Ask a question—
“I wonder if that upsets you more than you like toadmit?”
Aspects of interview style that aid assessment of patients’ emotional problems
Early in the interviewx Make good eye contact x Clarify presenting complaint x Use directive questions for physical complaintsx Begin with open ended questions, moving to closed questions later
Interview stylex Make empathic commentsx Pick up verbal cues
x Pick up non-verbal cuesx Do not read notes while taking patient’s historyx Deal with over-talkativenessx Ask more questions about the history of the emotional problem
Visiting the sick woman , by Quiringh Gerritsz van Brekelenkam (c 1620-68)
1

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 13/69
Eliciting a patient’s explanatory model When people consult a doctor, they do so with explanatoryideas about their problems and with anxieties and concerns that reflect these ideas. They are also likely to have hopes andexpectations concerning the care that they will receive. It isimportant not to make assumptions about patients’ health
beliefs, concerns, and expectations but to elicit these as a basisfor providing information and negotiating a management plan.
People’s health beliefs and behaviours develop and are
sustained within families, and families are deeply affected by theillness of a family member. “Thinking family” can help to avoiddifficult and frustrating interactions with family members.
Providing informationDoctors should consider three key questions when providing information to a patient:v What does the patient already know?v What does the patient want to know?v What does the patient need to know?
The first question emphasises the importance of building onthe patient’s existing explanatory model, adding to what he or
she already knows, and correcting inaccuracies. The second andthird reflect the need to address two agendas, the patient’s andthe doctor’s. In addition, it is important for the doctor to showongoing concern and emotional support, making empathiccomments, legitimising the patient’s concerns, and offering support.
Negotiating a management plan The ideal management plan is one that reflects current best evidence on treatment, is tailored to the situation andpreferences of the patient, and addresses emotional and socialissues. Both patient and doctor should be involved indeveloping the plan, although one or the other may have thegreater input depending on the nature of the problem and theinclinations of the patient.
Appropriate use of reassuranceReassurance is effective only when doctors understand exactly
what it is that their patients fear and when they address thesefears truthfully and accurately. Often it is not possible toreassure patients about the diagnosis or outcome of disease, but it is always possible to provide support and to show personalconcern for them.
Dealing with difficult emotions: denial, anger, and fear Denial — When patients deny the seriousness of their illness
you should never be tempted to force them into facing it. The
decision on how to address denial must be based on howadaptive the denial is, what kind of support is available to thepatient, and how well prepared the patient is to deal with thefears that underlie the denial.
Think family
When interviewing an individualx Ask how family members view the problemx Ask about impact of the problem on family functionx Discuss implications of management plan for the family
When a family member comes in with patient x Acknowledge relative’s presencex Check that patient is comfortable with relative’s presencex
Clarify reasons for relative coming x Ask for relative’s observations and opinions of the problemx Solicit relative’s help in treatment if appropriatex If patient is an adolescent accompanied by an adult always spend
part of consultation without the adult present x Never take sides
Negotiating a management plan
Ascertain expectationsx What does patient know?x What does patient want?—Investigation? Management? Outcomes?
Advise on options
x Elicit patient’s preferencesDevelop a planx Involve patient x Tailor preferred option to patient’s needs and situationx “Think family”
Check understanding x Ensure that patient is clear about planx Consider a written summary
Advise on contingency management x What should patient do if things do not go according to plan?
Agree arrangements for follow up and review
Reassurance is an essentialskill of bedside medicine.(Hippocrates (469-399 bc ),the “father of bedsidemedicine”)
Active listening skillsOpen ended questions —Questions that cannot be answered in one
word require patient to expandOpen-to-closed cones— Move towards closed questions at the end of a
section of the consultationChecking— Repeat back to patient to ensure that you have understood Facilitation— Encourage patient both verbally (“Go on”) and
non-verbally (nodding)
Legitimising patient’s feelings— “This is clearly worrying you a great deal,” followed by, “You have an awful lot to cope with,” or,“I think most people would feel the same way”
Surveying the field —Repeated signals that further details are wanted:“Is there anything else?”
Empathic comments —“This is clearly worrying you a great deal”Offering support —“I am worried about you, and I want to know how I
can help you best with this problem” Negotiating priorities —If there are several problems draw up a list and
negotiate which to deal with first
Summarising —
Check what was reported and use as a link to next part of interview. This helps to develop a shared understanding of the problemsand to control flow of interview if there is too much information
ABC of Psychological Medicine
2

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 14/69
Anger —If patients or relatives become angry, try to avoid being defensive. Acknowledge the feelings that are expressedand ask about the reasons for these. Take concerns seriouslyand indicate that you will take appropriate action.
Fear —Many patients are frightened that they may have someserious disease. It is crucial to ensure that you have addressed what a patient is really worried about as well as checking that the patient has correctly understood what you are concerned
about.
MotivationEfforts to help people reduce alcohol consumption, stopsmoking, and manage chronic illness have highlighted theimportance of good interviewing skills in motivating patients tochange their behaviour. This is not to say that patients nolonger have the responsibility for such change, but doctorsshould recognise that they bear some responsibility for ensuring that patients get the best possible help in arriving at the decision to change.
Making the link between emotions and physical symptoms
Particular strategies may be needed to help people who present with physical symptoms of psychological distress but who havenot made the link between these and their emotional and lifeproblems. However, it is essential that you do not go faster thanthe patient and try to force the patient to accept your explanation.
Feeling understood —Ensuring that the patient feelsunderstood is essential. It is crucial to get the patient on your side and show that you are taking his or her problems seriously.Start from the patient’s viewpoint and find out what the patient thinks may be causing the symptoms, while at the same timepicking up any verbal and non-verbal cues of emotional distress.
Broadening the agenda can begin when all the informationhas been gathered. The aim is to broaden the agenda from one
where the problem is seen essentially as physical to one where both physical and psychological problems can beacknowledged. Acknowledging the reality of the patient’s painor other symptoms is essential and must be done sensitively.Summarise by reminding the patient of all the symptoms, bothphysical and emotional, that you have elicited and link them tolife events if this is possible.
Negotiating explanations can involve various techniques. Onlyone or two will be appropriate for each patient, and different techniques may be useful at different times. Simple explanationis the commonest, but it is insufficient to say “Anxiety causesheadaches.” A three stage explanation is required in whichanxiety is linked to muscle tension, which then causes pain. A
similar approach can be used to explain how depression causeslowering of the pain threshold, which results in pain being felt more severely than it otherwise would be.
Once the patient and doctor have agreed that psychologicaldistress is an important factor in the patient’s illness, they canstart to examine management options to address this. Even if the patient has significant physical disease, it is important todetect and manage psychological comorbidity.
Helping patients to change their behaviour
Explore motivation for changex Build rapport and be neutralx Help draw up list of problems and prioritiesx Is problem behaviour on patient’s agenda?x If not, raise it sensitivelyx Does patient consider the behaviour to be a problem?x Do others?
Clarify patient’s view of the problemx Help draw up a balance sheet of pros and consx Empathise with difficulty of changing x Reinforce statements that express a desire to changex Resist saying why you think patient ought to changex Summarise frequentlyx Discuss statements that are contradictory
Promote resolution
If no change is wanted negotiate if, when, and how to review x Enable informed decision making x Give basic information about safety or risks of behaviour x Provide results of any examination or test x Highlight potential medical, legal, or social consequencesx Explain likely outcome of potential choices or interventionsx Get feedback from patient x Give patient responsibility for decision
Key stages in linking somatic symptoms of emotionaldistress
x Helping patient to feel understoodx Broadening agenda to cover physical, psychological, and social
issuesx Negotiating explanations for how physical symptoms, psychological
distress, and social problems may be linked via physiologicalmechanisms
Evidence based summary
x The style with which a doctor listens to a patient will influence what the patient says
x Effective communication between doctor and patient leads toimproved outcome for many common diseases
x Patients’ compliance will be improved if the management plan has been negotiated jointly
Lang F, Floyd MR, Beine KL. Clues to patients’ explanations and concerns about their illnesses—a call for active listening. Arch Fam Med 2000;9:222-7
Stewart MA. Effective physician-patient communication and health outcomes: a review. Can Med Assoc J 1995;152:1423-33
Roter D, Hall JA, Merisca R, Nordstron B, Cretin D, Svarstad B. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care 1998;36:1138-61
Further reading
x Cole SA, Bird J. The medical interview: the three function approach .St Louis, MO: Harcourt Health Sciences, 2000
x Gask L, Morriss R, Goldberg D. Reattribution: managing somatic presentation of emotional distress . 2nd ed. Manchester: Universityof Manchester, 2000. (Teaching videotape available [email protected])
x Usherwood T. Understanding the consultation. Milton Keynes: OpenUniversity Press, 1999Visiting the sick woman is held at the Hermitage and is reproduced with
permission of Bridgeman Art Library.
The consultation
3

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 15/69
2 Beginning treatment Jonathan Price, Laurence Leaver
Traditionally, the management of newly presenting patients hastwo stages—assessment and then treatment. However, this two
stage approach has limitations. When underlying diseasepathology is diagnosed there may be delays in starting effectivetreatment. If no disease is found reassurance is often ineffective.In both cases many patients are left feeling uncertain anddissatisfied. Lack of immediate information and agreed plansmay mean that patients and their families become anxious anddraw inappropriate conclusions, and an opportunity to engagethem fully in their management is missed.
If simple diagnosis is supplemented with fuller explanation,patient satisfaction and outcomes are improved. This can beachieved by integrating assessment and treatment. The aim of an integrated consultation is that the patient leaves with a clear understanding of the likely diagnosis, feeling that concerns have
been addressed, and knowledge of the treatment and prognosis(that is, the assessment becomes part of the treatment). Thisapproach can be adopted in primary and secondary care andcan be applied to patients with or without an obvious diseaseexplanation for their symptoms. The integrated approach mayrequire more time, but this is offset by a likely reduction inpatients’ subsequent attendance and use of resources.
This article describes principles and practical procedures for effective communication and simple interventions. They can beapplied to various clinical situations—such as straightforwardsingle consultation, augmenting brief medical care, andpromoting an effective start to continuing treatment and care.
General principlesIntegrating physical and psychological careSomatic symptoms are subjective and have two components, a somatic element (a bodily sensation due to physiology or pathology) and a psychological element (related to thoughtsand beliefs about the symptoms). Traditional management focuses only on the somatic component, with the aim of detecting and treating underlying pathology. Addressing thepsychological component in the consultation as well, withsimple psychological interventions, is likely to reduce distressand disability and reduce the need for subsequent specialist treatment.
Providing continuitySeeing the same doctor on each visit increases patient satisfaction. Continuity may also improve medical outcomes,including distress, compliance, preventive care, and resourceuse. Problems resulting from lack of continuity can beminimised by effective communication between doctors.
Involving the patient The psychological factors of beliefs and attitudes about illnessand treatment are major determinants of outcome. Hence,strategies that increase understanding, sense of control, andparticipation in treatment can have large benefits. One exampleis written management plans agreed between doctor and
patient. This approach is the basis of the Department of Health’s “Expert Patient Programme,” which aims to helppatients to “act as experts in managing their own condition,
with appropriate support from health and social care services.”
Mismatch of expectations and experiences
What patients want What some patients get
To know the cause No diagnosis
Explanation and information Poor explanation that does not address their needs and concerns
Advice and treatment Inadequate advice
Reassurance Lack of reassurance
To be taken seriously by a sympathetic and competent doctor
Feeling that doctor is uninterestedor believes symptoms areunimportant
Disease centred versus patient centred consultations Disease centred— Doctor concentrates on standard medical agenda of
diagnosis through systematic inquiries about patient’s symptomsand medical history
Patient centred— Doctor works to patient’s agenda, including listening and allowing patient to explain all the reasons for attending,feelings, and expectations. Decision making may be shared, andplans are explicit and agreed. Patient centred consultations needtake no longer than traditional disease centred consultations
Communication between doctors
x Reduce need for communication between doctors by providing continuity of care whenever possible
x Brief, structured letters are more likely to be read than lengthy,unstructured letters
x Letters from primary to secondary care should provide relevant background information and a clear reason for referral
x Letters from secondary to primary care should provide onlyessential information, address the needs of referrer, and outline a proposed management plan and what has been discussed withpatient
x Avoid using letters for medical records purposes rather thancommunication
x The telephone can be a prompt and effective means of communication and is particularly useful in complex cases
Taking time to listen to and address patients’ ideas, concerns, andexpectations can improve outcomes (Charcot at the Saltpêtrière byLuis Jimenez y Aranda, 1889, in the Provincial Museum of Art, Seville)
4

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 16/69
Thinking “family”Relatives’ illness beliefs and attitudes are also crucial to outcomeand are therefore worth addressing. Key people may be invitedto join a consultation (with the patient’s permission) and their concerns identified, acknowledged, and addressed. Activelyinvolving relatives, who will spend more time with the patient than will the doctor, allows them to function as co-therapists.
Effective communication
Gaining and demonstrating understanding Simple techniques can be used to improve communication. Thefirst two stages of the three function approach (see previousarticle) are appropriate. The first stage is building a relationshipin which a patient gives his or her history and feels understood.
The second stage is for the doctor to share his or her understanding of the illness with the patient. In cases that aremore complicated it may be most effective to add an additional
brief session with a practice or clinic nurse.
Providing information for patientsPatients require information about the likely cause of their illness, details of any test results and their meaning, and a discussion of possible treatments. Even when this informationhas been given in a consultation, however, many patients do not understand or remember what they are told. Hence, theprovision of simple written information can be a time efficient
way of improving patient outcomes.One way of providing written information is to copy
correspondence such as referral and assessment letters to thepatient concerned. For those not used to doing this, it may seema challenge, but any changes needed to make the lettersunderstandable (and acceptable) to patients are arguablydesirable in any case. Letters should be clearly structured,medical jargon minimised, pejorative terms omitted, and
common words that may be misinterpreted (such as “chronic”)explained.
Well written patient information materials (leaflets and books) are available, as are guidelines for their development. The National Electronic Library of Health (www.nelh.nhs.uk) isa new internet resource that aims to provide high qualityinformation for healthcare consumers and is linked to NHSDirect Online (www.nhsdirect.nhs.uk/main.jhtml). There arealso many books to recommend—such as Chronic Fatigue Syndrome (CFS/ME): The Facts (see Further reading list).Information is most helpful if it addresses not only the natureof the problem, its prognosis, and treatment options, but alsoself care and ways of coping.
The assessment as treatment
Reassurance Worry about health (health anxiety) is a common cause of distress and disability in those with and without serious disease.Reassurance is therefore a key component of starting treatment.
The first step is to elicit and acknowledge patients’expectations, concerns, and illness beliefs. This is followed byhistory taking, examination, and if necessary investigation.Premature reassurance (such as “I’m sure its nothing much”)may be construed as the doctor not taking the problemseriously. Finally, the explanation should address all of a patient’s concerns and is best based on the patient’s
understanding of how his or her body functions, which maydiffer from the doctor’s.
A modest increase in consultation time, provision of writteninformation, and perhaps the use of trained nursing staff to
Gaining understanding of patients’ concerns
x Read referral letter or notes, or both, before seeing patient x Encourage patients to discuss their presenting concerns without
interruption or premature closurex Explore patients’ presenting complaints, concerns, and
understanding (beliefs)x Inquire about disabilityx Inquire about self care activitiesx Show support and empathyx Use silence appropriatelyx Use non-verbal communication such as eye contact, nods, and
leaning forward
Showing your understanding of patients’ concerns
x Relay key messages—such as, “The symptoms are real,” “We willlook after you,” and “You’re not alone”
x Take patients seriously and make sure they know it x Don’t dismiss presenting complaints, whether or not relevant
pathology is foundx
Explain your understanding of the problem—
what it is, what it isn’t,treatment, and the future. A diagram may helpx Consider offering a positive explanation in the absence of relevant
physical pathologyx Reassurex Avoid mixed messagesx Encourage and answer questionsx Share decisionsx Communicate the management plan effectively, both verbally and
in writing x Provide self care information, including advice on lifestyle changex Explain how to get routine or emergency follow up, and what to
look out for that would change the management plan
Providing information
x Invite and answer questionsx Use lay terms, and build on patient’s understanding of illness
wherever possiblex Avoid medical jargon and terms with multiple meanings, such as
“chronic”x Involve relativesx Provide written material when availablex Provide a written management plan when appropriate
The complexity of reassurance
General reassurancex To know it will be OK x To know I will be looked after x To know there are others like me
Reassurance about causex To know what it isx To know what it is not x To know it’s not serious
“There are several possible causes, not just cancer”“It’s not cancer”“It will get better”
Reassurance about cure
x To know it can be treatedx To know it will be treatedx To know how it will be treatedx To know the complaint will go away
Beginning treatment
5
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 17/69
facilitate information giving, can all enhance doctor-patient communication and, therefore, reassurance. Although extra time and effort may be needed, it may well reduce subsequent demand on resources.
Being positiveDoctors themselves are potentially powerful therapeutic agents. There is evidence that being deliberately positive in a
consultation may increase this effect. In one randomised trial,general practice patients received either a positive consultation(firm diagnosis and good prognosis) or a non-positiveconsultation (no firm diagnosis and uncertain prognosis). Two weeks later, the positive consultation, which was simple and brief, had improved symptoms, with a number needed to treat of four (95% confidence interval 3 to 9).
Using tests as treatment Tests should ideally be informative and reassuring for bothdoctors and patients. However, there is increasing evidence that tests may not reassure some patients and may even increasetheir anxiety. This is most likely with patients who are already
anxious about their health. When weighing the pros and consof ordering a test, doctors should take account of the potentialpsychological impact on their patient (both positive andnegative).
Providing explanations after negative investigationEven when tests are reported as normal, some patients are not reassured. Such patients may benefit from an explanation of what is wrong with them, not just what is not wrong. A cognitive behavioural model can be used to explain how interactions between physiology, thoughts, and emotion can causesymptoms without pathology. Simple headache provides ananalogy: the pain is real, and often distressing and disabling, but
is usually associated with “stress.” Diagnoses such as “tensionheadache” and “irritable bowel syndrome” can be helpful inreducing patients’ anxiety about sinister causes for their symptoms.
Planning for the future
Maintaining and increasing activitiesSometimes patients unnecessarily avoid or reduce their activities for fear it will make their illness worse. This coping strategy magnifies disability. Planning a graded return towardsnormal activities is one of the most effective ways of helping such patients. A plan should specify clearly what activity, for
how long, when, with whom, and how often. It is best if the planis written down and reviewed regularly. A collaborativeapproach increases the chances of success.
Follow upPositively following up patients who have presented for the first time can be an effective use of time. It allows review andmodification of the management plan and may be particularlyeffective if the same doctor is seen.
Characteristics of brief psychological intervention
x Brief, single session interventionx Suitable for more complex problems, such as in secondary carex Delivered with or soon after clinic attendancex Integrated with usual carex Uses cognitive understanding of health anxietyx Minimises negative aspects of patient experiencex Reinforces positive aspects of patient experiencex Provides explicit explanation and reassurance
Evidence based summary
x The quality of communication, both in history taking and in
discussing a management plan, influences patient outcomex Patients should be encouraged to take an active role in maintaining
or improving their own health, and doctors should ensure they aregiven the necessary information and opportunities for self management
x Reassurance involves eliciting and acknowledging patients’expectations, concerns, and illness beliefs
Coulter A, Entwistle V, Gilbert D. Sharing decisions with patients: is theinformation good enough? BMJ 1999;318:318-22
Di Blasi Z, Harkness E, Ernst E, Georgiou A, Kleijnen J. Influence of context effects on health outcomes: a systematic review. Lancet 2001;357:575-762
Stewart M. Effective physician-patient communication and health outcomes: a review. Can Med Assoc J 1995;152:1423-33
Thomas KB. General practice consultations: is there any point in being positive? BMJ 1997;294:1200-2
Further reading
x Balint M. The doctor, his patient,and the illness . Tunbridge Wells:Pitman Medical, 1957
x Department of Health. The NHS plan—A plan for investment. A plan for reform . London: DoH, 2000
x Campling F, Sharpe M. Chronic fatigue syndrome (CFS/ME): the facts .Oxford: Oxford University Press, 2000
x Department of Health. The expert patient:a new approach to chronic disease management for the 21st century . 2001 (www.ohn.gov.uk/ohn/people/ep_report.pdf
Distress Minor physicaldisease
Bodilysensations
Cognitions
Physiologicalvariations
Socialbehaviour
Symptoms EmotionsAttentionBehaviour
Responseof others Psychophysiologicalchanges
A simple cognitive model of physical symptoms. A cognitive model is one in which the patient’s thoughts and beliefs are seen as central to the aetiology,perception, and presentation of the problem
The painting of Charcot is reproduced with per mission of the Wellcome Library.
ABC of Psychological Medicine
6

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 18/69
3 Organising care for chronic illnessMichael Von Korff, Russell E Glasgow, Michael Sharpe
A major and increasing task for health services is themanagement of chronic illness. Although the details of chronic
illness management will depend on the illness in question,many of the principles are common to all chronic conditions.
Principles of effective management Whatever health services may offer, most of the day to dayresponsibilities for the care of chronic illness fall on patientsand their families. Planners and organisers of medical care must therefore recognise that health care will be most effective if it isdelivered in collaboration with patients and their families. Toenable patients to play an active role in their care, healthservices must not only provide good medical treatment but alsoimprove patients’ knowledge and self management skills. This
can be done by supplementing medical care with educationaland cognitive behavioural interventions. Chronic diseasetreatment programmes have tended to underestimate the needfor this aspect of care, and, consequently, many treatment programmes have been psychologically naive and, as a result,less effective than they could have been.
Services also need to be not merely reactive to patients’requests but proactive with planned follow up. Finally, to bemost efficient, interventions are best organised in a steppedfashion—that is, the more complex and expensive interventionsare given only when simpler and cheaper ones have beenshown to be inadequate or inappropriate.
Collaboration with patients and families To win the collaboration of patients and their families, thoseproviding care need to elicit, negotiate and agree on a definitionof the problem they are working on with each patient. Theymust then agree on the targets and goals for management anddevelop an individualised collaborative self management plan. This plan should be based on established cognitive behaviouralprinciples and on the evidence relating to the management of the chronic condition.
In order to implement collaborative care, patients and their families require access to the necessary information andservices to enable them to play a full and informed role. Theneed for collaborative care in which patients play an active rolehas been highlighted in Britain with the development of the
concept of the “expert patient.”
Encouraging self care Active self care is critical to the optimal management of chronicillness. Interventions to optimise self care are based on cognitive behavioural principles.
They start with an assessment of patients’ attitudes and beliefs about their illness and their chosen coping behaviours. This assessment then guides the provision of information, theresolution of misunderstandings and misinterpretations, andcollaborative goal setting. These are agreed between patient andmembers of the healthcare team.
The outcome of this initial assessment takes the form of a
personal action plan, a written agreement between thosedelivering care and the patient. The patient keeps a copy of theplan, and the healthcare team keeps another. The plan can be written on brief, standardised forms. The plan is not static but is
Common elements of effective chronic illness management
x Collaboration between service providers and patientsx A personalised written care planx Tailored education in self management x Planned follow upx Monitoring of outcome and adherence to treatment x Targeted use of specialist consultation of referralx Protocols for stepped care
Principles of collaboration
x Understanding of patients’ beliefs, wishes, and circumstancesx Understanding of family beliefs and needsx Identification of a single person to be main link with each patient x Collaborative definition of problems and goalsx Negotiated agreed plans regularly reviewedx Active follow up with patientsx Regular team review
The UK “expert patient” programme*
x Encouragement of self care protocols, nationally and locallyx Development of electronic and written self care materialx Training programmes, national and localx Integrating self care into local health planning x Nurse led telephone service (NHS Direct)
* From; Department of Health. The expert patient: a new approach to chronic disease management for the 21st century (www.ohn.gov.uk/ohn/people/expert)
Treating chronic conditions must involve the family
7
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 19/69
developed over time: the initial goals and the care plandesigned to achieve them are refined in view of the patient’sprogress and the identification of factors that are either helpfulor unhelpful in achieving the desired outcome.
Active follow up The personal action plan guides the patient’s follow up contacts. Active planned follow up ensures that the plan is carried out
and that modifications to it are made as needed. These steps arerepeated in an iterative, ongoing, and flexible way rather than allat once in a single visit. Because the care of chronic illness is a long term process, the work of supporting self care does not need to be done all at once but can be spread over manycontacts.
Individualised stepped careStepped care provides a framework for using limited resourcesto greatest effect. Professional care is stepped in intensity—that is, it starts with limited professional input and systematicmonitoring and is then augmented for patients who do not achieve an acceptable outcome. Initial and subsequent treatments are selected according to evidence based guidelinesin light of a patient’s progress.
The principle of increasing intensity of professional input for those who do not respond to initial management is familiar in primary care. However, organised stepped care requires thesystematic monitoring of progress and higher levels of coordination between specialist care, care management, andprimary care than generally exist. The primary care team, a specialist consultant (when needed), and a care manager (whenneeded) work together to provide the level of professionalsupport needed to achieve a favourable outcome. Stepped careis individualised according to each patient’s preferences andprogress.
Skills required by those delivering care
The team providing care must not only be familiar with a patient’s condition but must also possess the psychological skillsto help the patient achieve self care. They also need access tospecialists in psychological and psychiatric management toprovide supervision and consultation in selected cases. Thenecessary psychological skills includev Anxiety management v Recognition and treatment of depressionv Cognitive behavioural analysisv Cognitive behavioural principles of step by step changev Ability to monitor patient’s progress.
Changes in the organisation of care Achieving collaboration between healthcare providers andchronically ill patients requires organisational changes in sixrelated areas.
Organisation of care —Clinical leadership should encourageefforts to improve quality, including development of incentivesfor improved care and reorganisation of acute care toencourage self care.
Clinical information systems — A disease (or disorder) registryshould be set up that identifies the population to be served and
includes information on the performance of guideline basedcare, including self care tasks. The registry should permit identification of patients with specific needs, reminder systems,and tailored treatment planning.
Plan for collaborative self care
1 Assessment x Assess patient’s self management beliefs, attitudes, and knowledgex Identify personal barriers and supportsx Collaborate in setting goalsx Develop individually tailored strategies and problem solving
2 Goal setting and personal action planx List goals in behavioural termsx Identify barriers to implementationx Make plans that address barriers to progressx Provide a follow up planx Share the plan with all members of the healthcare team
3 Active follow up to monitor progress and support patient
Levels of stepped care
1 Systematic routine assessment and preventivemaintenance
2 Self care with low intensity support 3 Care management in primary care
4 Intensive care management with specialist advice5 Specialist care
Assumptions of stepped care
x Different individuals require different levels of carex The optimal level of care is determined by monitoring outcomesx Moving from lower to higher levels of care based on patient
outcomes can increases effectiveness and lower costs
Example of changes in organisation of care for patientswith diabetes
Organisation of carex Primary care clinic initiates year long effort to reorganise diabetes
carex Team is set up and meets regularly to make changes, monitor
progress, and address obstacles
Clinical information systemsx Team develops a register of all patients with diabetes in the clinic,
with records of HbA1C values, eye and foot examinations, and goalsand key elements of patients’ personal action plans
Delivery system designx
Clinic nurses assigned responsibility for diabetes case management x Doctors agree to provide planned visits for all diabetic patients at
least once a year, including preventive services (such as eye and foot examinations, ordering HbA1C tests, screening for depression)
x Clinic support staff maintain the register and print out a statusreport before each visit
Decision support x Team agrees on standard evidence based guidelines and adapts
them to clinic and liaison with the specialist diabetic clinicx Team agrees a standard form for planned visits
Community resourcesx Nurse case managers plan training in diabetes self management.
The nurses are trained to co-lead the course at regular intervals
Self care support x Nurse case managers decide that every diabetic patient will have a
personal action plan developed within a year x Each nurse sees one patient a week until this goal is accomplishedx Nurses telephone patients who have not been seen for six months
and those who need extra support to achieve their goals
ABC of Psychological Medicine
8

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 20/69
Delivery system design —Practice team roles should be changedin the organisation of visits and in follow up care. Usefulinnovations include group visits, planned visits, and telephonedelivered care.
Decision support —Evidence based practice guidelines andprotocols should be made effective by integrating informationand reminders into visits. There should be collaborative support from relevant medical specialties.
Community resources —
Links should be established withcommunity resources, especially for vulnerable populationssuch as elderly, low income, and deprived populations.
Self care support — Tailored educational resources, skillstraining, and psychosocial support are effective. Successful self care programmes rely on collaboration; patient centredinterventions for managing illness are especially beneficial.
Is this approach feasible for the large numbers of patientsseen in busy primary and secondary care settings? There isgrowing experience with integrating support for self care to thedelivery of routine medical care. Specific techniques such ascognitive behavioural interventions and the use of nurses andother staff as care managers have been found to be both
feasible and effective. However, the full implementation of thisapproach in primary care requires substantial organisationalchanges. These enable medical and other expertise to be usedmore effectively and efficiently. They also enable doctors toobtain greater satisfaction in being responsible for higher quality care.
Evidence that it works
Collaborative self care has been used to guide efforts toimprove the quality of chronic illness care in many different healthcare settings and for many different chronic conditionsincluding diabetes, heart failure, geriatric care, depression, andasthma. This approach gives patients the confidence and skillsfor self care and for getting what they need from the healthcaresystem (that is, becoming active, informed patients). Sucheffective support of patients is more likely to occur when theproviders of care themselves have the information, training,resources, and time to deliver effective interventions (that is, area well prepared, proactive practice team).
There is now considerable evidence and practicalexperience that supports fundamental changes in the way weorganise and deliver health care to better support patients whoare living with a chronic condition. Consequently, we need toinclude psychological and behavioural expertise as essentialsupplements to basic medical treatment.
Patient centred care is more than a respectful attitude or a
style of clinical interviewing. It means that healthcare systemsare organised to maximise the effectiveness of patients tomanage their chronic illness themselves.
Psychological medicine will make its full contribution only when an awareness of the importance of psychological and behavioural factors is fully integrated into general medical care.
Making evidence based care time and cost effective
Problemsx Time for patient carex Time for assessing evidencex Unrealistic patient expectations and demandsx Lack of patient understanding of behavioural basis of self carex Lack of involvement of patients in clinical decisionsx Lack of professional skills
x Access to disparate community and medical servicesSolutionsx Treatment protocolsx Involvement of healthcare teamx Use of self help proceduresx Formalising links with local health, social, and voluntary agenciesx Liaison with specialist medical, psychiatric, and psychological
servicesx Continuing professional development
Evidence based summary
x Collaborative and adaptive approaches to self care that arestructured and integrated into medical services improve outcomesfor many chronic diseases
x Systematic setting of therapeutic goals and monitoring of clinicaltreatment and outcomes are integral to this approach
x Such an approach to health care will often require changes to the way in which teams and primary and secondar y care servicesinteract
Department of Health. The expert patient: a new approach to chronic disease management for the 21st century (www.ohn.gov.uk/ohn/people/ep_report.pdf)
Gibson PG, Coughlan J, Wilson AJ, Abramson M, Bauman A, Hensley MJ, et al.Self-management education and regular practitioner review for adults withasthma. Cochrane Database Syst Rev 2000;(2): CD001117
Further reading
x Department of Health. The expert patient:a new approach to chronic disease management for the 21st century. (www.ohn.gov.uk/ohn/people/ep_report.pdf)
x Lorig KR, Sobel DS, Stewart AL, Brown BW Jr, Bandura A, Ritter P,et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalisation.
Med Care 1999;37:5-14x Von Korff M, Gruman J, Schaefer J, Curry S, Wagner EH.
Collaborative management of chronic illness. Ann Intern Med 1997;127:1097-102
x Wagner EH, Glasgow RE, Davis C, Bonomi AE, Provost L,McCulloch D, et al. Quality improvement in chronic illness care: a collaborative approach. Jt Comm J Qual Improv 2001;27:63-80
x Wolpert HA, Anderson BJ. Management of diabetes: are doctorsframing the benefits from the wrong perspective? BMJ 2001;323:994-6
Work on this article was supported by grants from the Robert Wood JohnsonFoundation National Program for Improving Chronic Illness Care, NIMHgrants MH51338 and MH41739, and NIH grant P01 DE08773.
The picture is reproduced with permission of CC Studio/SPL.
Organising care for chronic illness
9

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 21/69
4 Depression in medical patientsRobert Peveler, Alan Carson, Gary Rodin
Depressive illness is usually treatable. It is common and resultsin marked disability, diminished survival, and increased
healthcare costs. As a result, it is essential that all doctors have a basic understanding of its diagnosis and management. Inpatients with physical illness depression mayx Be a coincidental associationx Be a complication of physical illnessx Cause or exacerbate somatic symptoms (such as fatigue,malaise, or pain).
Clinical features and classification The term depression describes a spectrum of mood disturbanceranging from mild to severe and from transient to persistent.
Depressive symptoms are continuously distributed in anypopulation but are judged to be of clinical significance whenthey interfere with normal activities and persist for at least two
weeks, in which case a diagnosis of a depressive illness or disorder may be made. The diagnosis depends on the presenceof two cardinal symptoms of persistent and pervasive low moodand loss of interest or pleasure in usual activities.
Adjustment disorders are milder or more short lived episodesof depression and are thought to result from stressfulexperiences.
Major depressive disorder refers to a syndrome that requiresthe presence of five or more symptoms of depression in thesame two week period.
Dysthymia covers persistent symptoms of depression that may not be severe enough to meet the criteria for major depression, in which depressed mood is present for two or more years. Such chronic forms of depression are associated
with an increased risk of subsequent major depression,considerable social disability, and unhealthy lifestyle choicessuch as poor diet or cigarette smoking.
Manic depressive (bipolar) disorder relates to the occurrence of episodes of both major depression and mania.
Epidemiology
The World Health Organization estimates that depression will become the second most important cause of disability worldwide (after ischaemic heart disease) by 2020. Major depressive disorder affects 1 in 20 people during their lifetime.Both major depression and dysthymia seem to be morecommon in women.
Depressive illness is strongly associated with physicaldisease. Up to a third of physically ill patients attending hospitalhave depressive symptoms. Depression is even more commonin patients withx Life threatening or chronic physical illnessx Unpleasant and demanding treatment x Low social support and other adverse social circumstancesx Personal or family history of depression or other
psychological vulnerabilityx Alcoholism and substance misusex Drug treatments that cause depression as a side effect, such asantihypertensives, corticosteroids, and chemotherapy agents.
Criteria for major depression*
Five or more of the following symptoms during the same two week period representing a change from normalx Depressed mood†x Substantial weight loss or weight
gainx Insomnia or hypersomnia x Feelings of worthlessness or
inappropriate guilt x Recurrent thoughts of death or
suicide or suicide attempt
x Decreased interest or pleasure†
x Psychomotor retardation or agitation
x Fatigue or loss of energyx Diminished ability to think or
concentrate
*From Diagnostic and Statistical Manual of Mental Disorders , fourth edition†One of these symptoms must be present
Aretaeus of Cappadocia(circa 81-138 ad )is credited withthe first clinical
description of depression
Percentage of population
40 30 20 10 0
MenWomen
10 20 30 40
Fatigue
WorryIrritability
Sleep problems
Depression
Obsessions
AnxietyDepressive ideas
Lost concentration
Phobias
Compulsions
Somatic symptoms
Physical health worries
Panic
“Neurotic”symptoms,including depression, arecontinuouslydistributed in theUK population
Months after infarction
M o r t a l i t y ( % )
00
10
15
20
25
30
5
1 2 3 4 5 6
Depressed patients
Non-depressed patients
The association
betweendepression andmortality aftermyocardialinfarction
10

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 22/69
Risk factors Anxiety, sadness, and somatic discomfort are part of the normalpsychological response to life stress, including medical illness.Clinical depression is a final common pathway resulting fromthe interaction of biological, psychological, and social factors.
The likelihood of this outcome depends on such factors asgenetic and family predisposition, the clinical course of a
concurrent medical illness, the nature of the treatment,functional disability, the effectiveness of individual coping strategies, and the availability of social and other support.
In the attempts to understand the relation between physicalillness and depression there has been much debate about thedirection of causality. In particular, there has been speculationthat certain illnesses—such as stroke, Parkinson’s disease,multiple sclerosis, and pancreatic cancer —may cause depression
via direct biological mechanisms. Stroke has perhaps receivedthe most attention, but studies have failed to convincingly showdirect aetiological mechanisms.
Recognition and diagnosisIn spite of its enormous clinical and public health importance,depressive illness is often underdiagnosed and undertreated,particularly when it coexists with physical illness. This oftencauses great distress for patients who have mistakenly assumedthat symptoms such as weakness or fatigue are due to anunderlying medical condition.
All medical practitioners must be able to diagnose andmanage depressive illness effectively. This depends onx Alertness to clues in interviewsx Patients’ manner x The use of screening questions in those at risk —in particular,two questions about low mood and lack of pleasure in life can
detect up to 95% of patients with major depression.Self report screening instruments, such as the Beck depression inventory (BDI) and the hospital anxiety anddepression scale (HADS) cannot replace systematic clinicalassessment, but they are useful in drawing attention to depressionand other emotional disturbances in clinical settings where moodis not routinely assessed. Doctors must be aware that persistent low mood and lack of interest and pleasure in life cannot beaccounted for by severe physical illness alone. The usual responseto illness and treatment is impressive resilience.
If there is doubt about the diagnosis, a doctor may resort toan empirical trial of treatment to establish whether there is
benefit. The wider availability of safer drugs and psychologicaltreatments makes this option more attractive than in the past.
Management The main aims of treatment are to improve mood and qualityof life, reduce the risk of medical complications, improvecompliance with and outcome of physical treatment, andfacilitate the “appropriate” use of healthcare resources. Thedevelopment of a treatment plan depends on systematicassessment that should, whenever possible, not only involve thepatients but also their partners or other key family members.
Milder or briefer adjustment disorders can be managed byprimary care staff without recourse to specialist referral.Education, advice, and reassurance are of value. It is important
that primary care staff are familiar with the properties and useof the commoner antidepressant drugs, and the value of brief psychological treatments such as cognitive behaviour therapy,interpersonal therapy, and problem solving.
Reasons why depression is missed
x Difficulty distinguishing psychological symptoms of depression,such as sadness and loss of interest, from a “realistic” response tostressful physical illness
x Confusion over whether physical symptoms of depression are dueto an underlying medical condition
x Negative attitudes to diagnosis of depressionx Unsuitability of clinical setting for discussion of personal and
emotional mattersx Patients’ unwillingness to report symptoms of depression
Screening questions for depression
x How have you been feeling recently?x Have you been low in spirits?x Have you been able to enjoy the things you
usually enjoy?x Have you had your usual level of energy, or have
you been feeling tired?x How has your sleep been?x Have you been able to concentrate on newspaper
articles or your favourite television or radioprogrammes?
Multiple stressors of illness
Sadness(Normative response)
Somatic distressAnxiety
Personal meaning
PersonalitySocial support
Life stagePrior experiences
of mastery
Social supportMedical complications
Genetic loadingCoping strategies
Persistent subthresholdsymptoms Depressive disorders
Pathways to depression
Insomnia
"Memory loss"
Fatigue andtiredness
Painful jointsand back
Weight loss
Disruptedmenses
Malaise
Headache
Chest pain
Nausea,vomiting, and
constipation
Physical symptoms that may be due to depression
Depression in medical patients
11

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 23/69
Patients with more enduring or severe symptoms willusually require specific forms of treatment, usually drug treatment. Staff should also be able to assess suicidal thinking and risk. For patients with suicidal ideation or those whosedepression has not responded to initial management, specialist referral is the next step in management.
Drug treatment
Antidepressants have been shown to be effective in treating major depressive disorder irrespective of whether the mooddisturbance is “understandable.” There have been far fewer trials of antidepressants in patients who are also physicallyunwell, but the available evidence is in keeping with thetreatment of depression generally.
One of the commonest questions is which antidepressant should be used. For non-specialists, the range of available drugs,and the claims made about them can be bewildering. There arefour main classes of antidepressant x Tricyclicsx Selective serotonin reuptake inhibitorsx Monoamine oxidase inhibitorsx
Others (noradrenaline reuptake inhibitors).
Choice of agent Data from the Cochrane Collaboration and other systematicreviews show that the differences in overall tolerability betweendifferent preparations is minimal. In general, patients areslightly less likely to drop out of trials because of unacceptableside effects when taking a selective serotonin reuptake inhibitor
but are slightly less likely to drop out because of treatment inefficacy when taking a tricyclic. Rather than continuouslyexperimenting with a range of different drugs, clinicians shouldstick to prescribing one drug from each class in order to
become familiar with their dosing regimens, actions,interactions, and side effects. Clinicians should also be aware
that in certain situations one class of drug may be moreadvisable than others.
Adequacy of treatment The debate about different preparations has obscured a potentially more important issue—that of drug dose andcompliance. Most prescriptions for antidepressants are for inadequate doses and for inadequate time periods. Thisproblem is compounded by only a minority of patientscomplying with the prescribed treatment. A recent householdsurvey by the Royal College of Psychiatrists showed that manypeople believed that antidepressants were addictive and couldpermanently damage the brain.
Explanation To treat patients successfully with antidepressants, doctors must be able to show their patient that they have understood thepatient’s problems, considered the issues, and are advising the
best available treatment (see previous chapters). Before starting treatment, patients should be given an explanation of sideeffects and be reassured that side effects tend to be worseduring the first two weeks of treatment and then diminish. Theyneed to be warned that they are unlikely to feel benefits fromtreatment in the first four weeks. They should be given followup appointments during this period in order to encouragecompliance.
Duration of treatment After initial treatment has led to remission of symptoms,subsequent treatment can be divided into two phases. Firstly,four to six months of continuous treatment at full dose are
Clinical assessment of suicidal intent
Low level risk
Clinical picture x Suicidal ideation but no suicide
attemptsx Supportive environment x Physically healthyx No history of psychiatric illness
Action Consider referral to mentalhealth professional for routine appointment (not always necessary)
Moderate level risk
Clinical picture x Low lethality suicide attempt (patient’s
perception of lethality)x Frequent thoughts of suicidex Previous suicide attemptsx Persistent depressive symptomsx Serious medical illnessx Inadequate social support x History of psychiatric illness
Action Refer to mental healthprofessional, to be seen assoon as possible
High level risk
Clinical picture x Definite plan for suicide (When?
Where? How?)x Major depressive disorder, severex High lethality suicide attempt or
multiple attemptsx Advanced medical diseasex Social isolationx History of psychiatric illness
Action Refer to mental healthprofessional for immediateassessment
Comparison: Antidepressants v Placebo
Outcome: Lack of improvement at end of study
Condition Control
Odds ratio
(95% CI)
Weighting
(%)
Odds ratio
(95% CI)Drug
Cancer
Cancer
Diabetes
Head injuryHeart disease
HIV or AIDS
HIV
HIV
Lung disease
Multiple sclerosis
Physical illness, elderly
Physical illness
Stroke
Total
19/37
17/27
12/17
3/46/8
21/25
36/47
11/22
16/18
8/14
35/43
21/30
24/33
229/325
0.1 1 10
0.29 (0.11 to 0.75)
0.30 (0.10 to 0.85)
0.54 (0.14 to 2.07)
0.39 (0.03 to 4.54)0.04 (0.01 to 0.26)
0.52 (0.17 to 1.60)
0.26 (0.12 to 0.59)
0.57 (0.18 to 1.80)
0.14 (0.04 to 0.56)
0.49 (0.12 to 1.95)
0.42 (0.16 to 1.11)
1.34 (0.43 to 4.18)
0.41 (0.15 to 1.10)
0.37 (0.27 to 0.51)
11.2
9.0
5.4
1.73.0
8.0
15.2
7.6
5.3
5.2
10.5
7.7
10.2
100.0
8/36
9/28
10/18
3/61/16
36/50
22/50
9/25
8/18
7/18
25/39
22/29
17/33
177/366
No of patients
Meta-analysis of randomised controlled trials of drug treatment of depression in the physically ill
H e a l t h
Time
"Normalcy"P r o g
r e s s i o n t o
d i s o r d e r
Symptoms
Syndrome
Acute treatment
(6-12 weeks)
Response
Remission
Continuation
treatment(4-9 months)
Maintenance
treatment(>1 year)
Recovery
RecurrenceRelapse
Relapse
Chart of clinical course indicating remission, recovery, and relapse
ABC of Psychological Medicine
12

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 24/69
necessary to consolidate remission and prevent early relapse.Secondly, consideration must be given to preventivemaintenance treatment, to reduce the risks of recurrence of depression. This is usually indicated if the patient has had twoor more episodes of depression within the past five years.Psychological treatment may also help to prevent recurrenceand can be used in combination with drug treatment.
Psychological treatment Psychological treatment can range from discussion and simpleproblem solving to more specialised cognitive or dynamic behavioural psychotherapies. In many cases, brief treatment bynon-specialists in primary and secondary care can be effective.Such interventions may include education and reassuranceabout the common reactions to the threats and lossesassociated with illness and empathic listening to patients’ views,uncertainties, and beliefs about the illness. Education and adviceabout the medical condition and associated depression mayprevent needless worry, reduce feelings of helplessness, anddiminish irrational fears. Therapeutic approaches that support or promote active coping strategies are an important aspect of
treatment in physically ill patients.Cognitive behavioural principles may be used bynon-specialists to correct distorted thinking and to encourage behaviours that contribute to patients’ sense of mastery and wellbeing. Training in briefer forms of treatment using cognitive behavioural principles for primar y care staff may be a worthwhile investment.
Cognitive behaviour therapy, interpersonal therapy, andproblem solving have all been shown to be effective for treating depression, although there has been only limited evaluation of their effectiveness in physically ill populations. Although timeconsuming by comparison with drug treatment, psychologicaltreatment may reduce relapse rates and may be cost effective inthe long run. Some patients may require preliminary treatment
with drugs to enable them to make best use of psychologicaltreatment.
Service organisationDepression is so common in physically ill patients that it is not feasible for all cases to be managed by mental health specialists. There are advantages to collaborative management withprimary care staff working closely with mental health specialists.Community based mental health services may be less accessibleto general hospitals and often lack specialist knowledge about assessment and treatment when an important physical illness isalso present. Liaison psychiatry services are often well placed toprovide support, training, and psychiatric expertise to general
hospital patients in a timely fashion.
Problem solving in psychological treatment
x Define and list the problemsx Choose a problem for actionx List alternative courses of actionx Evaluate courses of action and choose the best x Try the actionx Evaluate the resultsx Repeat until major problems have been solved
Evidence based summary
x Depressive illness is an important cause of morbidity and disabilityin physically ill patients
x All patients with depression should be examined for suicidalideation
x Depression is treatable in physically ill patients
Wells KB, Stewart A, Hays RD, Burnam MA, Rogers W, Daniels M, et al. Thefunctioning and well-being of depressed patients. Results from the medicaloutcomes study. JAMA 1989;262:914-9
Carson AJ, Best S, Warlow C, Sharpe M. How common is suicidal ideationamong neurology outpatients? BMJ 2000;320:1311-2
Gill D, Hatcher S. Antidepressants for depression in medical illness. Cochrane Database Syst Rev 2000;(4):CD001312
Further reading
x Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M,Eshleman S, et al. Lifetime and 12-month prevalence of DSM-IIIRpsychiatric disorders in the United States: results of the nationalcomorbidity survey. Arch Gen Psychiatr 1994;51,8-19
x Rodin G, Craven J, Littlefield C. Depression in the medically ill: an
integrated approach . New York NY: Brunner/Mazel, 1991x Royal College of Physicians, Royal College of Psychiatrists. The
psychological care of medical patients: recognition of need and service provision . London: RCP, RCPsych, 1995
The diagram of the distribution of neurotic symptoms in the UK population is adapted from Jenkins et al Psychol Med 1997;27:765-74. Thegraph of association between depression and mortality after myocardialinfarction. is adapted from Frasure Smith et al JAMA 1993;270: 1819-25. The diagram showing pathways to depression is adapted from Rodin et al Depression in the medically ill 1991. The meta-analysis of trials comparing antidepressants is adapted from Gill and Hatcher Cochrane Database Syst
Rev 2000;(4):CD001312.
Depression in medical patients
13
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 25/69
5 Anxiety in medical patients Allan House, Dan Stark
Doctors often consider anxiety to be a normal response tophysical illness. Yet, anxiety afflicts only a minority of patients
and tends not to be prolonged. Any severe or persistent anxiousresponse to physical illness merits further assessment.
What is anxiety? Anxiety is a universal and generally adaptive response to a threat, but in certain circumstances it can become maladaptive.Characteristics that distinguish abnormal from adaptive anxietyincludex Anxiety out of proportion to the level of threat x Persistence or deterioration without intervention ( > 3 weeks)x Symptoms that are unacceptable regardless of the level of threat, including
Recurrent panic attacksSevere physical symptoms
Abnormal beliefs such as thoughts of sudden deathx Disruption of usual or desirable functioning.
One way to judge whether anxiety is abnormal is to assess whether it is having a negative effect on the patient’sfunctioning.
Abnormal anxiety can present with various typicalsymptoms and signs, which includex Autonomic overactivityx Behaviours such as restlessness and reassurance seeking x Changes in thinking, including intrusive catastrophicthoughts, worry, and poor concentrationx Physical symptoms such as muscle tension or fatigue.
Classification of abnormal anxiety Abnormal anxiety can be classified according to its clinicalfeatures. In standardised diagnostic systems there are four mainpatterns of abnormal anxiety.
Anxious adjustment disorder — Anxiety is closely linked in timeto the onset of a stressor.
Generalised anxiety disorder — Anxiety is more pervasive andpersistent, occurring in many different settings.
Panic disorder — Anxiety comes in waves or attacks and isoften associated with panicky thoughts (catastrophic thoughts)of impending disaster and can lead to repeated emergencymedical presentations.
Phobic anxiety—
Anxiety is provoked by exposure to a specificfeared object or situation. Medically related phobic stimuliinclude blood, hospitals, needles, doctors and (especially)dentists, and painful or unpleasant procedures.
Additionally, anxiety often presents in association withdepression. Mixed anxiety and depressive disorders are muchmore common than anxiety disorders alone. Treatment for thedepression may resolve the anxiety. Anxiety can also be thepresenting feature of other psychiatric illnesses common inphysically ill people, such as delirium or drug and alcoholmisuse.
Somatic and psychological symptoms of anxiety disorders
In all anxiety disordersx Palpitations, pounding heart,
accelerated heart ratex Trembling or shaking x Difficulty in breathing x Chest pain or discomfort x Feeling dizzy, unsteady, faint,
light headedx Fear of losing control, going
crazy, passing out
x Sweating x Dry mouthx Feeling of choking x Nausea or abdominal discomfort x Feeling that objects are unreal or
that self is distant x Fear of dying x Numbness or tingling sensationsx Hot flushes or cold chills
In more severe or generalised anxiety disordersx Muscle tension or aches and
painsx Feeling keyed up, on edge, or
mentally tensex Exaggerated response to
minor surprises or being startled
x Persistent irritability
x Restlessness, inability to relaxx Sensation of difficulty
swallowing, lump in the throat x Difficulty concentrating or
“mind going blank” fromanxiety or worry
x Difficulty in getting to sleep because of worry
Distinguishing features of anxiety disorders
Anxious adjustment disorder Prevalence in general population— Not knownCardinal features x
Onset of symptoms within 1 month of an identifiable stressor x No specific situation or response
Generalised anxiety disorder Prevalence in general population— 31 cases/1000 adultsCardinal features x Period of 6 months with prominent tension, worry, and feelings of
apprehension about everyday problemsx Present in most situations and no specific response
Panic disorder Prevalence in general population— 8 cases/1000 adultsCardinal features x Discrete episode of intense fear or discomfort with crescendo
pattern; starts abruptly and reaches a maximum in a few minutesx Occurs in many situations, with a hurried exit the typical response
Phobia
Prevalence in general population— 11 cases/1000 adultsCardinal features x No specific symptom patternx Occurs in specific situations, with an avoidance response
William Cullen(1710-90) coined theterm neurosis (thoughthe term as he used it
bears little resemblanceto modern concepts of anxiety disorders)
14
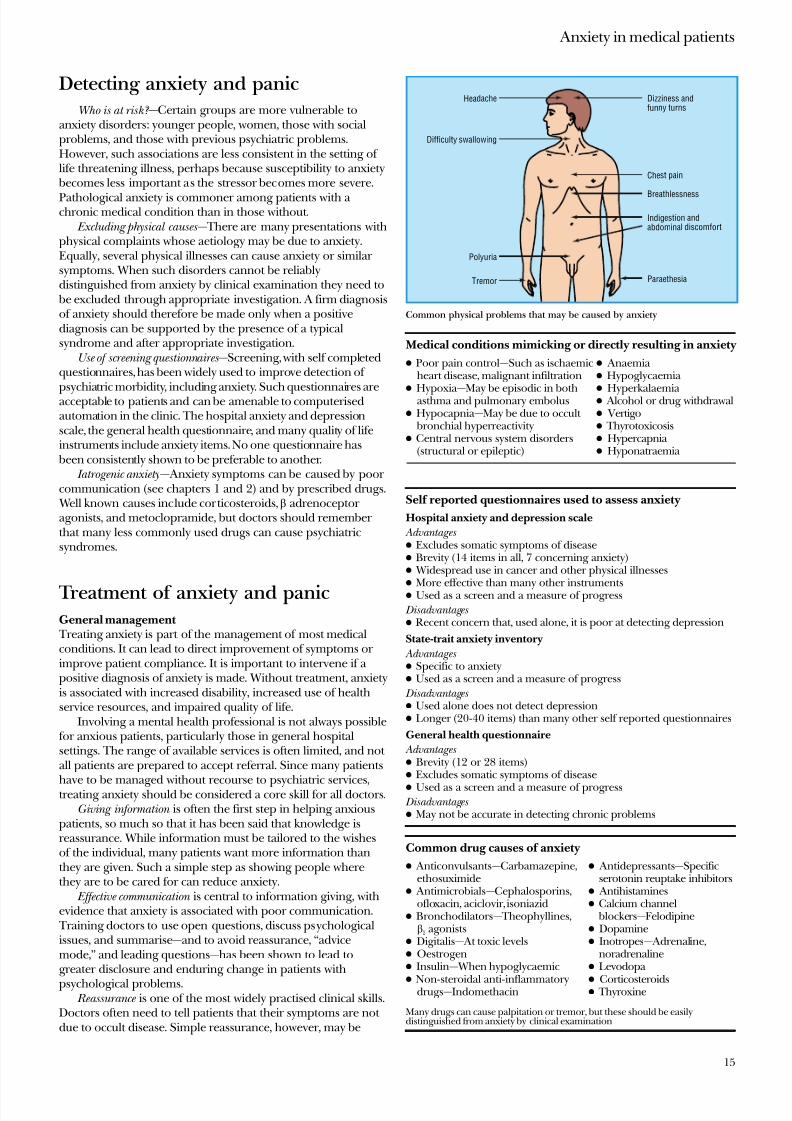
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 26/69
Detecting anxiety and panicWho is at risk? —Certain groups are more vulnerable to
anxiety disorders: younger people, women, those with socialproblems, and those with previous psychiatric problems.However, such associations are less consistent in the setting of life threatening illness, perhaps because susceptibility to anxiety becomes less important as the stressor becomes more severe.
Pathological anxiety is commoner among patients with a chronic medical condition than in those without.
Excluding physical causes — There are many presentations withphysical complaints whose aetiology may be due to anxiety.Equally, several physical illnesses can cause anxiety or similar symptoms. When such disorders cannot be reliablydistinguished from anxiety by clinical examination they need to be excluded through appropriate investigation. A firm diagnosisof anxiety should therefore be made only when a positivediagnosis can be supported by the presence of a typicalsyndrome and after appropriate investigation.
Use of screening questionnaires —Screening, with self completedquestionnaires, has been widely used to improve detection of
psychiatric morbidity, including anxiety. Such questionnaires areacceptable to patients and can be amenable to computerisedautomation in the clinic. The hospital anxiety and depressionscale, the general health questionnaire, and many quality of lifeinstruments include anxiety items. No one questionnaire has been consistently shown to be preferable to another.
Iatrogenic anxiety— Anxiety symptoms can be caused by poor communication (see chapters 1 and 2) and by prescribed drugs. Well known causes include corticosteroids, adrenoceptor agonists, and metoclopramide, but doctors should remember that many less commonly used drugs can cause psychiatricsyndromes.
Treatment of anxiety and panicGeneral management Treating anxiety is part of the management of most medicalconditions. It can lead to direct improvement of symptoms or improve patient compliance. It is important to intervene if a positive diagnosis of anxiety is made. Without treatment, anxietyis associated with increased disability, increased use of healthservice resources, and impaired quality of life.
Involving a mental health professional is not always possiblefor anxious patients, particularly those in general hospitalsettings. The range of available services is often limited, and not all patients are prepared to accept referral. Since many patients
have to be managed without recourse to psychiatric services,treating anxiety should be considered a core skill for all doctors.Giving information is often the first step in helping anxious
patients, so much so that it has been said that knowledge isreassurance. While information must be tailored to the wishesof the individual, many patients want more information thanthey are given. Such a simple step as showing people wherethey are to be cared for can reduce anxiety.
Effective communication is central to information giving, withevidence that anxiety is associated with poor communication. Training doctors to use open questions, discuss psychologicalissues, and summarise—and to avoid reassurance, “advicemode,” and leading questions—has been shown to lead togreater disclosure and enduring change in patients with
psychological problems. Reassurance is one of the most widely practised clinical skills.
Doctors often need to tell patients that their symptoms are not due to occult disease. Simple reassurance, however, may be
Medical conditions mimicking or directly resulting in anxiety
x Poor pain control—Such as ischaemicheart disease, malignant infiltration
x
Hypoxia —
May be episodic in bothasthma and pulmonary embolusx Hypocapnia —May be due to occult
bronchial hyperreactivityx Central nervous system disorders
(structural or epileptic)
x Anaemia x Hypoglycaemia x
Hyperkalaemia x Alcohol or drug withdrawalx Vertigox Thyrotoxicosisx Hypercapnia x Hyponatraemia
Self reported questionnaires used to assess anxiety
Hospital anxiety and depression scale
Advantages x Excludes somatic symptoms of diseasex Brevity (14 items in all, 7 concerning anxiety)x Widespread use in cancer and other physical illnessesx More effective than many other instrumentsx Used as a screen and a measure of progress
Disadvantages x Recent concern that, used alone, it is poor at detecting depression
State-trait anxiety inventory
Advantages x Specific to anxietyx Used as a screen and a measure of progress
Disadvantages x Used alone does not detect depressionx Longer (20-40 items) than many other self reported questionnaires
General health questionnaire
Advantages x Brevity (12 or 28 items)x Excludes somatic symptoms of diseasex Used as a screen and a measure of progress
Disadvantages x May not be accurate in detecting chronic problems
Common drug causes of anxiety
x Anticonvulsants—Carbamazepine,ethosuximide
x Antimicrobials—Cephalosporins,ofloxacin, aciclovir, isoniazid
x Bronchodilators— Theophyllines,2 agonists
x Digitalis— At toxic levelsx Oestrogenx Insulin— When hypoglycaemicx
Non-steroidal anti-inflammatorydrugs—Indomethacin
x Antidepressants—Specificserotonin reuptake inhibitors
x Antihistaminesx Calcium channel
blockers—Felodipinex Dopaminex Inotropes— Adrenaline,
noradrenalinex Levodopa x
Corticosteroidsx Thyroxine
Many drugs can cause palpitation or tremor, but these should be easilydistinguished from anxiety by clinical examination
Headache
Difficulty swallowing
Polyuria
Indigestion andabdominal discomfort
Chest pain
Paraethesia
Breathlessness
Dizziness andfunny turns
Tremor
Common physical problems that may be caused by anxiety
Anxiety in medical patients
15

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 27/69
ineffective for anxious patients; their anxiety may be reducedinitially by the consultation, but it rapidly returns. Severaltheoretical models of this problem have been suggested, basedon the patterns of thinking (“cognitions”) of people who aredifficult to reassure.
Preparation for unpleasant procedures can remove theadditional burden of facing the unknown. It may also allowplanning of short term tactics for dealing with anxiety
provoking circumstances. Anxious patients are highly vigilant and overaware of threatening stimuli. They often use “quick fix”techniques based on avoidance of threat to reduce anxiety; suchstrategies are generally maladaptive and result in increasing disability. In some medical situations, however, such avoidancemay not be a bad thing if the threat is temporary. A similar effect is seen with use of benzodiazepine to provide temporaryrelief from anxiety symptoms that will not recur because thestressor is not persistent.
Behavioural treatments are among the most effectivetreatments for anxiety disorders. Many patients restrict their activities in response to anxiety, which often has the effect of increasing both the level of anxiety and the degree of disability
in the longer term. The principle of treatment is that controlledexposure to the anxiety producing stimulus will eventually leadto diminution in symptoms. Although specific behaviouraltreatments will normally be conducted by specialists, other clinicians should be aware of the basic principles. It is important to encourage and help patients to maintain their normalactivities as much as possible, even if this causes temporaryincreases in anxiety.
Drug treatments —Several drugs can be used to treat anxiety,each with its own advantages and disadvantages. Long term benzodiazepine dependence and misuse are considered by manyto be a problem in medical practice. Although the evidence for this is conflicting, the use of benzodiazepines may be reserved for the short term treatment of anxiety and for emergencies.
Drug withdrawal —
Dependence on other substances,particularly analgesics and alcohol, occurs fairly frequently inthe context of anxiety. This often results from self medicationfor anxiety. In this situation withdrawal from the existing “treatment” will be an important part of the anxietymanagement programme.
Role of specialist psychological treatment Clinical studies indicate that psychological interventions for anxiety can be effective both in general psychiatric settings andfor physically ill patients. The most popular, and those with the best evidence to support them, are based on the principles of behaviour, cognitive behaviour, or interpersonal therapy.
In behaviour and cognitive behaviour therapies the mainaim is to help patients identify and challenge unhelpful ways of thinking about and coping with physical symptoms and their meaning, about themselves, and about how they should livetheir lives. In interpersonal therapies the main focus is onrelationships with family members and friends—how suchrelationships are affected by illness and how they influencepatients’ current emotional state. Patients need to know that such therapies may be both brief and practical. Fewer than sixsessions may be enough, concentrating on symptoms or theimmediate problems associated with them and learning new ways of dealing with problems. In only a minority of cases ismore extended therapy needed, usually when anxiety is longer standing and only partially due to associated physical disease.
Drug interventions in anxious medical patients
Blockersx Benefits unproved in randomised controlled trialsx Help to control palpitation and tremor, but not anxiety itself x Often used for performance anxiety, such as in interviews or
examinationsTricyclic antidepressants (such as imipramine)x Likely to be beneficial (number needed to treat = 3)x Anxiolytic effect is slow in onset (weeks)x Not dependency inducing x Useful in panic disorder or in anxiety with depressionx Anticholinergic effects can be ameliorated by a low starting dose
Selective serotonin reuptake inhibitors (such as sertraline)x Benefit unproved but suggestedx Less anticholinergic effects than tricyclic antidepressantsx Start at low dose in anxious patients
Short acting benzodiazepines (such as alprazolam)x Effectiveness and relative lack of toxicity well establishedx All benzodiazepines can induce dependencyx Rapid onset of effect, but problems may recur on withdrawal
x Less likely to accumulate in liver Antipsychotics (such as haloperidol)x Benefits unproved in randomised controlled trialsx Useful adjunct to benzodiazepinesx Less respiratory depression that benzodiazepinesx Not dependency inducing x Risk of acute dystonia, akathisia, and parkinsonismx Avoid long term use because of risk of tardive dyskinesia
Buspironex Limited evidence for effectiveness from randomised controlled
trials, few clinicians are convincedx Causes some nausea and dizziness
Further reading x Noyes R, Hoehn-Saric R. Anxiety in the medically ill: disorders due
to medical conditions and substances. In: Noyes R, Hoehn-Saric R,eds. The anxiety disorders . Cambridge: Cambridge University Press,1998:285-334
x Colon EA, Popkin MK. Anxiety and panic. In: Rundell JR, Wise MG,eds. Textbook of consultation-liaison psychiatry. Washington DC: American Psychiatric Press, 1996:403-25
x Westra HA, Stewart SH. Cognitive behavioural therapy andpharmacotherapy: complementary or contradictory approaches tothe treatment of anxiety? Clin Psychol Rev 1998;18:307-40
x Cochrane Depression Anxiety and Neurosis Group. See list of reviews at www.update-software.com/abstracts/g240index.htm
Beliefs
Tending to interpret everyday bodilysymptoms as indicative of serious disease
(Anxiety influences patient's ability toassess degree of airway obstruction)
Concerns
Health worry and preoccupation, fear
of serious illness and of death. Canbe intrusive and difficult to control
(Concerns rise that asthma is worsening,leading to increased anxiety)
Behaviours
Reassurance seeking, including
seeking medical consultations(Patient takes increasing doses
of medication without anyalleviation of symptoms)
Characteristic features of health anxiety (using the example of asthma)
ABC of Psychological Medicine
16

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 28/69
6 Functional somatic symptoms and syndromesRichard Mayou, Andrew Farmer
Concern about symptoms is a major reason for patients to seek medical help. Many of the somatic symptoms that they present
with—
such as pain, weakness, and fatigue—
remain unexplained by identifiable disease even after extensive medical assessment.Several general terms have been used to describe thisproblem—somatisation, somatoform, abnormal illness behaviour,medically unexplained symptoms, and functional symptoms. We will use the term functional symptoms, which does not assumepsychogenesis but only a disturbance in bodily functioning.
Classification of functional syndromesMost functional symptoms are transient, but a sizeable minority become persistent. Persistent symptoms are often multiple and
disabling and may be described as functional syndromes. Although different medical and psychiatric classifications of functional syndromes exist, these are simply alternative ways of describing the same conditions.
Medical syndromes (such as fibromyalgia and chronic fatigue,chronic pain, and irritable bowel syndromes) highlight patternsof somatic symptoms, often in relation to particular bodilysystems. Although they are useful in everyday medical practice,recent studies show there is substantial overlap between them.
Psychiatric syndromes (such as anxiety, depression, andsomatoform disorders) highlight psychological processes andthe number of somatic symptoms irrespective of the bodilysystem to which they refer. Depression and anxiety often
present with somatic symptoms that may resolve with effectivetreatment of these disorders. In other cases the appropriatepsychiatric diagnostic category is a somatoform disorder.
The existence of parallel classificatory systems is confusing.Both have merits, and both are imperfect. For many functionalsymptoms, a simple description of the symptom qualified withthe descriptors single or multiple and acute or chronic maysuffice. When diagnosis of a functional syndrome seemsappropriate a combination of medical and psychiatricdescriptors conveys the most information, such as “irritable bowel syndrome with anxiety disorder.”
A major obstacle to effective management is patients feeling disbelieved by their doctor. Patients who present with symptomsthat are not associated with disease may be thought by some to
be “putting it on.” The deliberate manufacture of symptoms or signs, however, is probably rare in ordinary practice.
EpidemiologyCommunity based studies report annual prevalences of 6-36%for individual troublesome symptoms. In primary care only a small proportion of patients presenting with such symptomsever receive a specific disease diagnosis. The World HealthOrganization found functional symptoms to be common anddisabling in primary care patients in all countries and culturesstudied. Up to half of these patients remain disabled by their
symptoms a year after presentation, the outcome being worsefor those referred to secondary and tertiary care. The clinicaland public health importance of functional symptoms has beengreatly underestimated.
Some common functional symptoms and
syndromesx Muscle and joint pain (fibromyalgia)x Low back painx Tension headachex Atypical facial painx Chronic fatiguex Non-cardiac chest painx Palpitationx Non-ulcer dyspepsia x Irritable bowelx Dizzinessx Insomnia
René Descartes, who formulated the philosophicalprinciple of separation of brain and mind. This hasled to continuing dualism—separation of body andmind—in Western medicine and difficulty inaccepting the interaction of physical andpsychological factors in aetiology
3 y e a r i n c i d e n c e ( % )
C h e
s t p a i n
F a t i g
u e
D i z z i n
e s s
H e a d a c h e
O e d e m a
B a c k
p a i n
D
y s p n
o e a
I n s o m n i a
A b d o m
i n a l p
a i n
N u m
b n e s s
0
2
4
6
8
10
Organic cause
Three year incidence of 10 common presenting symptoms and proportionof symptoms with a suspected organic cause in US primary care
17
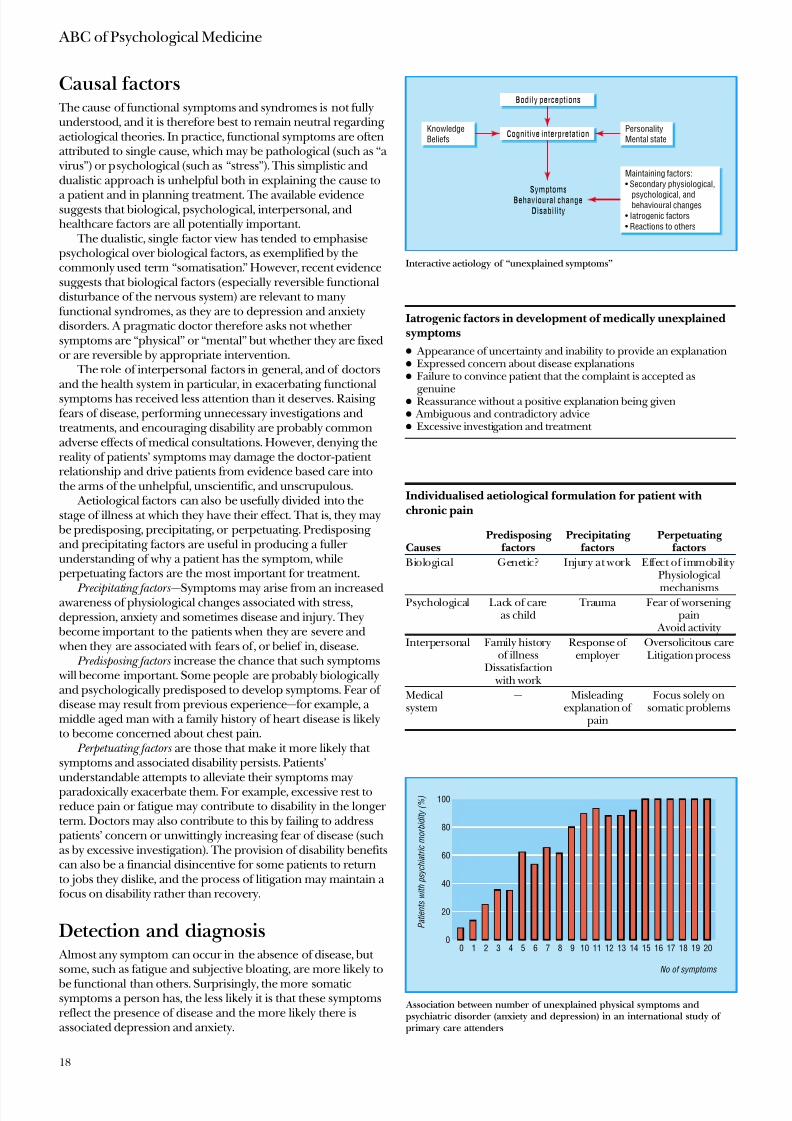
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 29/69
Causal factors The cause of functional symptoms and syndromes is not fullyunderstood, and it is therefore best to remain neutral regarding aetiological theories. In practice, functional symptoms are oftenattributed to single cause, which may be pathological (such as “a
virus”) or psychological (such as “stress”). This simplistic anddualistic approach is unhelpful both in explaining the cause to
a patient and in planning treatment. The available evidencesuggests that biological, psychological, interpersonal, andhealthcare factors are all potentially important.
The dualistic, single factor view has tended to emphasisepsychological over biological factors, as exemplified by thecommonly used term “somatisation.” However, recent evidencesuggests that biological factors (especially reversible functionaldisturbance of the nervous system) are relevant to manyfunctional syndromes, as they are to depression and anxietydisorders. A pragmatic doctor therefore asks not whether symptoms are “physical” or “mental” but whether they are fixedor are reversible by appropriate intervention.
The role of interpersonal factors in general, and of doctorsand the health system in particular, in exacerbating functionalsymptoms has received less attention than it deserves. Raising fears of disease, performing unnecessary investigations andtreatments, and encouraging disability are probably commonadverse effects of medical consultations. However, denying thereality of patients’ symptoms may damage the doctor-patient relationship and drive patients from evidence based care intothe arms of the unhelpful, unscientific, and unscrupulous.
Aetiological factors can also be usefully divided into thestage of illness at which they have their effect. That is, they may
be predisposing, precipitating, or perpetuating. Predisposing and precipitating factors are useful in producing a fuller understanding of why a patient has the symptom, whileperpetuating factors are the most important for treatment.
Precipitating factors —
Symptoms may arise from an increasedawareness of physiological changes associated with stress,depression, anxiety and sometimes disease and injury. They
become important to the patients when they are severe and when they are associated with fears of , or belief in, disease.
Predisposing factors increase the chance that such symptoms will become important. Some people are probably biologicallyand psychologically predisposed to develop symptoms. Fear of disease may result from previous experience—for example, a middle aged man with a family history of heart disease is likelyto become concerned about chest pain.
Perpetuating factors are those that make it more likely that symptoms and associated disability persists. Patients’understandable attempts to alleviate their symptoms mayparadoxically exacerbate them. For example, excessive rest toreduce pain or fatigue may contribute to disability in the longer term. Doctors may also contribute to this by failing to addresspatients’ concern or unwittingly increasing fear of disease (suchas by excessive investigation). The provision of disability benefitscan also be a financial disincentive for some patients to returnto jobs they dislike, and the process of litigation may maintain a focus on disability rather than recovery.
Detection and diagnosis Almost any symptom can occur in the absence of disease, but some, such as fatigue and subjective bloating, are more likely to
be functional than others. Surprisingly, the more somaticsymptoms a person has, the less likely it is that these symptomsreflect the presence of disease and the more likely there isassociated depression and anxiety.
Iatrogenic factors in development of medically unexplainedsymptoms
x Appearance of uncertainty and inability to provide an explanationx Expressed concern about disease explanationsx Failure to convince patient that the complaint is accepted as
genuinex Reassurance without a positive explanation being givenx Ambiguous and contradictory advicex Excessive investigation and treatment
Individualised aetiological formulation for patient withchronic pain
CausesPredisposing
factorsPrecipitating
factorsPerpetuating
factors
Biological Genetic? Injury at work Effect of immobilityPhysiological
mechanismsPsychological Lack of care
as child Trauma Fear of worsening
pain Avoid activity
Interpersonal Family historyof illness
Dissatisfaction with work
Response of employer
Oversolicitous careLitigation process
Medicalsystem
— Misleading explanation of
pain
Focus solely onsomatic problems
Bodily perceptions
Personality
Mental state
Knowledge
Beliefs
SymptomsBehavioural change
Disability
Maintaining factors:
• Secondary physiological,
psychological, and behavioural changes
• Iatrogenic factors
• Reactions to others
Cognitive interpretation
Interactive aetiology of “unexplained symptoms”
P a t i e n t s w i t h p s y c h i a t r i c m o r b i d i t y ( % )
No of symptoms
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Association between number of unexplained physical symptoms andpsychiatric disorder (anxiety and depression) in an international study of primary care attenders
ABC of Psychological Medicine
18

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 30/69
Patients with functional symptoms can be detected bymaintaining an awareness of the problem when seeing newpatients and by the use of somatic symptom questionnaires(large numbers of symptoms are more likely to be functional).
Management Although it is essential to consider disease as the cause of thepatient’s symptoms an approach exclusively devoted to this canlead to difficulties if none is found. Making explicit from thestart the possibility that the symptoms may turn out to befunctional keeps the option of a wider discussion open. Even if more specialist treatment is needed, then the problem has, fromthe outset, been framed in a way that enables psychologicaltreatment to be presented as part of continuing medical carerather than as an unacceptable and dismissive alternative. Inthis way it is possible to avoid an anxious disabled patient being treated by a bewildered frustrated doctor.
Investigation An appropriate physical examination and necessary medicallyindicated investigation are clearly essential. Thereafter, beforefurther investigation is done, the potential adversepsychological effect on the patient should be balanced against the likelihood and value of new information that may beobtained.
Reassurance and explanationMost patients are reassured by being told that the symptomsthey have are common and rarely associated with disease andthat their doctor is familiar with them. This is especially so if accompanied by the promise of further review should thesymptoms persist.
Reassurance needs to be used carefully, however. It isessential to elicit patients’ specific concerns about their symptoms and to target reassurance appropriately. The simplerepetition of bland reassurance that fails to address patients’fears is ineffective. If patients have severe anxiety about disease(hypochondriasis) repeated reassurance is not only ineffective
but may even perpetuate the problem. A positive explanation for symptoms is usually more helpful
that a simple statement that there is no disease. Most patients will accept explanations that include psychological and socialfactors as well as physiological ones as long as the reality of symptom is accepted. The explanation can usefully show thelink between these factors—for example, how anxiety can leadto physiological changes in the autonomic nervous system that
cause somatic symptoms, which, if regarded as further evidenceof disease, lead to more anxiety.
Further non-specialist treatment A minority of patients need more than simple reassurance andexplanation. Treatment should address patients’ illness fearsand beliefs, reduce anxiety and depression, and encourage a gradual return to normal activities.
There is good evidence that antidepressants often help, even when there are no clear symptoms of depression. Practicaladvice is needed, especially on coping effectively with symptomsand gradually returning to normal activity and work. Other useful interventions include help in dealing with major
personal, family, or social difficulties and involving a closerelative in management. Other members of the primary care or hospital team may be able to offer help with treatment, followup, and practical help.
Principles of assessment
x Identify patients’ concerns and beliefsx Review history of functional symptomsx Explicitly consider both disease and functional diagnosesx Appropriate medical assessment with explanation of findingsx Ask questions about patients’ reaction to and coping with
symptomsx Use screening questions for psychiatric and social problemsx Consider interviewing relatives
Principles of treatment
x Explain that the symptoms are real and familiar to doctor x Provide a positive explanation, including how behavioural,
psychological, and emotional factors may exacerbatephysiologically based somatic symptoms
x Offer opportunity for discussion of patient’s and family’s worriesx Give practical advice on coping with symptoms and encourage
return to normal activity and work x Identify and treat depression and anxiety disordersx Discuss and agree a treatment planx Follow up and review
Non-specialist specific treatments
x Provide information and advicex Agree a simple behavioural plan with patient and familyx Give advice about anxiety management x Encourage use of diariesx Advise about graded increase in activitiesx Prescribe antidepressant drug x Explain use of appropriate self help programmes
Specialist treatments
x Full and comprehensive assessment and explanation based onspecialist assessment
x Cognitive behaviour therapyx Supervised programme of graded increase in activity
x Antidepressants when these were previously not accepted or ineffective
x Illness specific interventions (such as rehabilitation programme for chronic pain)
Functional somatic symptoms were common after combat in the first world war, such as this soldier’s “hysterical pseudohypertrophic muscularspasms.” The course and outcome of such symptoms can now be seen tohave been substantially determined by varied medical and militaryapproaches to prevention and treatment
Functional somatic symptoms and syndromes
19
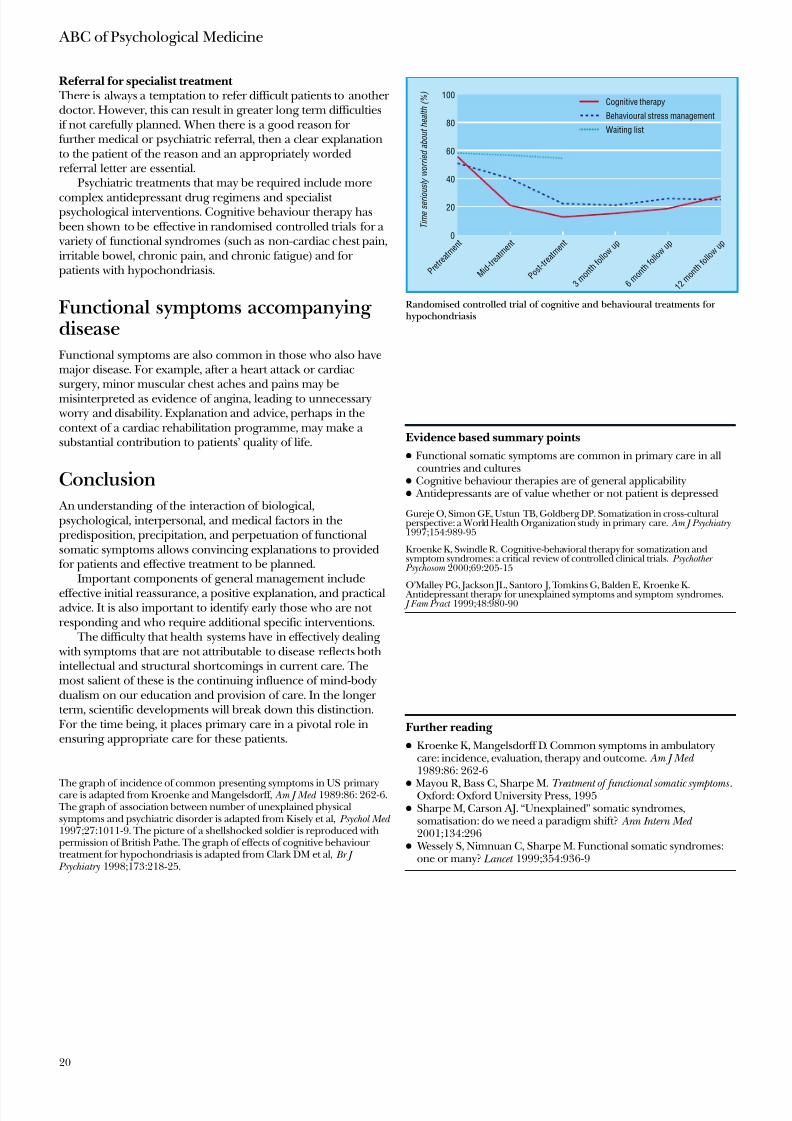
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 31/69
Referral for specialist treatment There is always a temptation to refer difficult patients to another doctor. However, this can result in greater long term difficultiesif not carefully planned. When there is a good reason for further medical or psychiatric referral, then a clear explanationto the patient of the reason and an appropriately wordedreferral letter are essential.
Psychiatric treatments that may be required include more
complex antidepressant drug regimens and specialist psychological interventions. Cognitive behaviour therapy has been shown to be effective in randomised controlled trials for a variety of functional syndromes (such as non-cardiac chest pain,irritable bowel, chronic pain, and chronic fatigue) and for patients with hypochondriasis.
Functional symptoms accompanying diseaseFunctional symptoms are also common in those who also havemajor disease. For example, after a heart attack or cardiacsurgery, minor muscular chest aches and pains may bemisinterpreted as evidence of angina, leading to unnecessary worry and disability. Explanation and advice, perhaps in thecontext of a cardiac rehabilitation programme, may make a substantial contribution to patients’ quality of life.
Conclusion An understanding of the interaction of biological,psychological, interpersonal, and medical factors in thepredisposition, precipitation, and perpetuation of functionalsomatic symptoms allows convincing explanations to providedfor patients and effective treatment to be planned.
Important components of general management include
effective initial reassurance, a positive explanation, and practicaladvice. It is also important to identify early those who are not responding and who require additional specific interventions.
The difficulty that health systems have in effectively dealing with symptoms that are not attributable to disease reflects bothintellectual and structural shortcomings in current care. Themost salient of these is the continuing influence of mind-bodydualism on our education and provision of care. In the longer term, scientific developments will break down this distinction.For the time being, it places primary care in a pivotal role inensuring appropriate care for these patients.
Evidence based summary points
x Functional somatic symptoms are common in primary care in allcountries and cultures
x Cognitive behaviour therapies are of general applicabilityx Antidepressants are of value whether or not patient is depressed
Gureje O, Simon GE, Ustun TB, Goldberg DP. Somatization in cross-culturalperspective: a World Health Organization study in primary care. Am J Psychiatry1997;154:989-95
Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization andsymptom syndromes: a critical review of controlled clinical trials. Psychother
Psychosom 2000;69:205-15
O’Malley PG, Jackson JL, Santoro J, Tomkins G, Balden E, Kroenke K. Antidepressant therapy for unexplained symptoms and symptom syndromes. J Fam Pract 1999;48:980-90
Further reading
x Kroenke K, Mangelsdorff D. Common symptoms in ambulatorycare: incidence, evaluation, therapy and outcome. Am J Med 1989:86: 262-6
x Mayou R, Bass C, Sharpe M. Treatment of functional somatic symptoms .Oxford: Oxford University Press, 1995x Sharpe M, Carson AJ. “Unexplained” somatic syndromes,
somatisation: do we need a paradigm shift? Ann Intern Med 2001;134:296
x Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes:one or many? Lancet 1999;354:936-9
The graph of incidence of common presenting symptoms in US primarycare is adapted from Kroenke and Mangelsdorff, Am J Med 1989:86: 262-6. The graph of association between number of unexplained physicalsymptoms and psychiatric disorder is adapted from Kisely et al, Psychol Med 1997;27:1011-9. The picture of a shellshocked soldier is reproduced withpermission of British Pathe. The graph of effects of cognitive behaviour treatment for hypochondriasis is adapted from Clark DM et al, Br J
Psychiatry 1998;173:218-25.
T i m e s e r i o
u s l y w o r r i e d a b o u t h e a l t h ( % )
0
P r e t r
e a t m
e n t
M i d - t r e
a t m e n t
P o s t - t r e
a t m e n t
3 m o n t h
f o l l o w
u p
6 m o n t h
f o l l o w
u p
1 2 m o n t h
f o l l o w
u p
20
40
60
80
100Cognitive therapy
Behavioural stress management
Waiting list
Randomised controlled trial of cognitive and behavioural treatments forhypochondriasis
ABC of Psychological Medicine
20
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 32/69
7 Chronic multiple functional somatic symptomsChristopher Bass, Stephanie May
The previous ar ticle in this series described the assessment andmanagement of patients with functional somatic symptoms.
Most such patients make no more than normal demands ondoctors and can be helped with the approach outlined.However, a minority have more complex needs and requireadditional management strategies. These patients typically havea longstanding pattern of presenting with various functionalsymptoms, have had multiple referrals for investigation of these,and are regarded by their doctors as difficult to help.
TerminologyBecause such patients may evoke despair, anger, and frustrationin doctors, they may be referred to as “heartsink patients,”“difficult patients,” “fat folder patients,” and “chroniccomplainers.” The use of these terms is inadvisable. If patientsread such descriptions in their medical notes they are likely to
be offended and lose faith in their doctor and may make a complaint. In psychiatric diagnostic classifications these patientsare often referred to as having somatisation disorder. We prefer the term “chronic multiple functional symptoms” (CMFS).
Epidemiology and detection The prevalence of CMFS depends upon the number of different symptoms required for diagnosis and on the setting. Whilst eachprimary care doctor will have an average of 10-15 of suchpatients, they are more common in specialist medical settings
where they may account for as many as 10% of referrals.
Most patients with CMFS are women. They often haverecurrent depressive disorder and a longstanding difficulty withpersonal relationships and may misuse substances. There is anassociation with an emotionally deprived childhood andchildhood physical and sexual abuse. Some patients will clearlyhave general disturbances of personality.
The risk of iatrogenic har m from over-investigation andover-prescribing for somatic complaints makes it important that patients with CMFS are positively identified and their management planned, usually in primary care. Potential CMFSpatients may be identified simply by the thickness of their paper notes, from records of attendance and hospital referral, and byobservation of medical, nursing, or clerical staff.
Management in primary careAssessment
It is helpful if one doctor is identified as a patient’s principalcarer. Once a patient is identified as possibly having CMFS a systematic assessment is desirable. The case notes should bereviewed and the patient seen for one or more extendedconsultations.
Case notes —Patients with CMFS often have extensive casenotes. Unless these are reviewed, much potentially usefulinformation may remain hidden. It is also helpful to compile a summary of these records and to evaluate critically the accuracyof any previously listed complaints and diagnoses. The summary
should include key investigations performed to date and anyinformation about patients’ personal and family circumstances.
Long appointment —During one or more long appointment a patient’s current problems and history should be fully explored.
Charles Darwin (1809-82) suffered from chronic anxiety and varied physicalsymptoms that began shortly after his voyage in the Beagle to South America(1831-6). Despite many suggested medical explanations, these symptoms,
which disabled him for the rest of his life and largely confined him to hishome, remain medically unexplained
“Fat files” are a simple indicator of a high level of contact with medicalservices, which may indicate multiple chronic functional somatic complaints
21

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 33/69
Patients should be encouraged to talk not only about their symptoms but also about their concerns, emotional state, andsocial situation and the association of these with their symptoms. At the end of the assessment, patient and doctor should agree a current problem list, which can then berecorded in the notes.
Management The initial long interviews serve not only to derive a problemlist but also to foster a positive relationship between doctor andpatient. Thereafter, the doctor should arrange to see the patient at regular, though not necessarily frequent, fixed intervals.
These consultations should not be contingent on the patient developing new symptoms. Consultation outside these timesshould be discouraged.
Planned review All symptoms reported by patients during these consultationsmust be acknowledged as valid. A detailed review of symptomsenhances the doctor-patient relationship and minimises the
likelihood of missing new disease.Reassurance that “nothing is wrong” may be unhelpful,possibly because a patient’s aim may be to develop anunderstanding relationship with the doctor rather than relief of symptoms. Focused physical examination can be helpful, but there is a risk of patients receiving multiple diagnostic tests andreferrals to specialists, and these should be minimised. Patientsalso often accumulate unnecessary prescribed drugs, and if sothese should be reduced gradually over time.
If a satisfactory rapport can be established with a patient,new information about his or her emotional state, relationshipdifficulties, or childhood abuse may be revealed. In such casesthe doctor may need to offer the patient a further long appointment to reassess the need for specialist psychological
care.
Support for doctors General practitioners managing patients with CMFS shouldarrange ongoing support for themselves, perhaps from a partner or another member of the primary care team with
whom they can discuss their patients. A doctor and, for example, a practice nurse can jointly manage some of thesepatients if there is an agreed management plan and clear communication.
Referral to psychiatric servicesNot all doctors will consider that they have the necessary skillsor time to manage these patients effectively. Review by anappropriate specialist can then be helpful. Unfortunately, thedecline in the number of “general physicians” and specialist mental health services’ increasing focus on psychotic illnessmean there are few appropriate specialists to refer to.
If referral is sought two questions must be considered: “Arethere any local and appropriate psychiatric services?” and “Howcan I prepare the patient for this referral?” If available, liaisonpsychiatry services are often the most appropriate andexperienced in this area of practice. To prepare the patient, a discussion emphasising the distressing nature of chronic illnessand the expertise of the services in this area, together with a
promise of continuing support from the primary care team, canhelp to make the referral seem less rejecting. If possible, thepsychiatrist should visit the practice or medical department andconduct a joint consultation.
Assessment of chronic multiple functional somaticsymptoms
x Elicit a history of the current complaints, paying special attention torecent life events
x Find out what the patient has been told by other doctors (as well asfriends, relatives, and alternative practitioners). Does this accord
with the medical findings?x Elicit an illness history that addresses previous experience of
physical symptoms and contact with medical services (such asillness as a child, illness of parents and its impact on childhooddevelopment, operations, time off school and sickness absence)
x Explore psychological and interpersonal factors in patient’sdevelopment (such as quality of parental care, early abusiveexperiences, psychiatric history)
x Interview a partner or reliable informant (this may take place,consent permitting, in the patient’s presence)
x After the interview attempt a provisional formulation
Useful interviewing skills for doctors managing patients withmultiple physical complaints
x Adopt a flexible interviewing style—“I wonder if you’ve thought of it
like this?”x Try to remind the patient that physical and emotional symptoms
often coexist —“I’m struck by the fact that, in addition to the fatigue,you’ve also been feeling very low and cannot sleep”
x Try “reframing” the physical complaints to indicate important temporal relationship between emergence of patient’s somatic andemotional symptoms and relevant life events
x Respond appropriately to “emotional” cues such as anger x Explore patient’s illness beliefs and worst fears—“What is your worst
fear about this pain?”
Management strategy for patients with chronic multiplefunctional somatic symptoms
x Try to be proactive rather than reactive—
Arrange to see patients at regular, fixed intervals, rather than allowing them to dictate timing and frequency of visits
x During appointments, aim to broaden the agenda with patients— This involves establishing a problem list and allowing patients todiscuss relevant psychosocial problems
x Stop or reduce unnecessary drugsx Try to minimise patients’ contacts with other specialists or
practitioners— This will reduce iatrogenic harm and makecontainment easier if only one or two practitioners are involved
x Try to co-opt a relative as a therapeutic ally to implement your management goals
x Reduce your expectation of cure and instead aim for containment and damage limitation
x Encourage patients (and yourself) to think in terms of coping and
not curing
Explanations to the patient
Present patient’s problems as a summary with an invitation tocomment:“So let me see if I’ve understood you properly: you have had a lot of pain in your abdomen, with bloating and distension for the past four years. You have been attending the (GP) surgery most weeks becauseyou’ve been very worried about cancer (and about your husbandleaving you). You also told me that these pains often occur when youare anxious and panicky, and at these times other physical complaintssuch as trembling and nausea occur.“I’m struck by the fact that all these complaints began soon after you
had a very frightening experience in hospital, when your appendix was removed and you felt that ‘No one was listening to my complaintsor pain.’“Have I got that right, or is there anything I’ve left out?”
ABC of Psychological Medicine
22
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 34/69
Specialist assessment Before interviewing a patient, it is useful to request both thegeneral practice and hospital notes and summarise the medicalhistory. A typed summary of the “illness history” can be kept asa permanent record in the notes. This summary can guidefuture management and is especially useful when a patient isadmitted subsequently as an emergency or when the receiving doctor has no prior knowledge of the patient.
Several important interviewing skills should be used during the assessment. These skills can be learnt using structured roleplaying and video feedback. They form the basis of a techniquecalled reattribution, which has been developed to help themanagement of patients with functional somatic symptoms.
Specialist management
If a patient can understand and agree an initial sharedformulation of the problems, an important first stage is reached.From this a plan of management can be negotiated. It is best toadopt a collaborative approach rather than a didactic or paternalistic manner. If it is difficult to arrive at anunderstanding of why the patient developed these symptoms at this particular time, then an alternative approach may have to be adopted. In essence this involves the doctor attempting toaddress those factors that are maintaining the symptoms.
Assessment and management go hand in hand. One of themain aims of management is to modify patients’ oftenunrealistic expectations of the medical profession and toremind them of the limits to medicine. In many cases hopesmay have been falsely raised, and patients expect either a cure
or at least a considerable improvement in symptoms. Althoughthis is desirable, it may not be attainable. Instead, the doctor should attempt to broaden the agenda, with an emphasis onhelping patients to address personal concerns and life problemsas well as somatic complaints. It is also necessary to encouragethem to concentrate on coping rather than seeking a cure.
This process requires patience, and a capacity to toleratefrustration and setbacks. It may require several discussions in which the same issues are reviewed. In the long term, however,it can be rewarding for both patient and doctor.
Common problems in management
Management may be complicated by various factors. Firstly,preoccupation and anxious concern about symptoms may leadpatients to make unhelpful demands of their doctor, whichprove difficult to resist.
What is the cause of functional somatic symptoms?
x A variety of biological, psychological, and social factors have beenshown to be associated with functional symptoms; the contributionof these factors will vary between patientsRecent developments in neuroscience show altered functioning of the nervous system associated with functional symptoms, making the labelling of these as “entirely psychological” increasing inappropriate
x With our current knowledge, it is best to maintain “aetiologicalneutrality” about the cause of functional symptoms
x The main task of treatment is to identify those factors that may bemaintaining a patient’s symptoms and disability
Maintaining factors that should be focus of treatment inpatients with multiple somatic symptoms
x Depression, anxiety, or panic disorder x Chronic marital or family discordx Physical inactivityx Occupational stressx Abnormal illness beliefsx Iatrogenic factorsx Pending medicolegal and insurance claims
Biomedical approach
Symptoms
Investigations
Drugs
Operations
Disability
Curing
Biopsychosocial approach
Engaging with distress
Broaden agenda
Problem solving
Involve relatives
Rehabilitation
Coping
The aim of treatment for patients with chronic multiple functionalsymptoms is to add a biopsychosocial perspective to the existing biomedicalapproach
Summary of a 15 year “segment” of the life of a patient with chronic multiple functional somatic symptoms
Date (age) Symptoms (life events) Referral Investigations Outcome
1970 (18) Abdominal pain GP to surgical outpatients Appendicectomy Nor mal appendix
1973 (21) Pregnant (boyfriend in prison) GP to obstetrics andgynaecology outpatients
Termination of pregnancy —
1975-7(23-25)
Bloating, abdominal pain, blackouts (stressful divorce)
GP to gastroenterology andneurology outpatients
All tests normal Diagnosis of irr itable bowelsyndrome and unexplained
syncope. Treated with fibre1979 (27) Pelvic pain (wants to be
sterilised)GP to obstetrics andgynaecology outpatients
Sterilised, ovaries preserved Pelvic pain persists for 2 years after surgery
1981 (29) Fatigue (problems at work) GP to infectious diseaseclinic
Nothing abnormal detected Diagnosis of myalgicencephalomyelitis made by patient. Joins self help group
1983 (31) Aching, painful muscles GP to rheumatology clinic Mild cervical spondylosis.No treatment
Treated with amitriptyline 50 mg on referral to pain clinic. Someimprovement
1985 (34) Chest pain and breathlessness(son truanting from school)
Accident and emergency tochest clinic
Nothing abnormal detected,probable hyperventilation
Refer to psychiatric services
Chronic multiple functional somatic symptoms
23

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 35/69
Secondly, there may be evidence of longstanding interpersonal difficulties, as indicated by remarks such as“Nobody cares” or “It’s disgusting what doctors can do to you.”Such comments may suggest that the patient’s relationship withthe doctor may reflect poor quality parental care or emotionaldeprivation in childhood. They are important for two reasons:firstly, the doctor may take these remarks personally, becomedemoralised or angry, and retaliate, which will destroy the
doctor-patient relationship; and, secondly, the attitudes revealedmay require more detailed psychological exploration.
Finally, iatrogenic factors may intervene that are beyond thetreating doctor’s control. Because these patients have often visited several specialists, conventional and alternative, they mayhave been given inappropriate information and advice,inappropriate treatment, or, in some cases, frank misdiagnosis.
Factitious disorders and malingering Factitious disordersFactitious disorders are characterised by feigned physical or psychological symptoms and signs presented with the aim of
receiving medical care. They are therefore different fromfunctional symptoms. The judgment that a symptom isproduced intentionally requires direct evidence and exclusionof other causes. Most patients with factitious disorders are women with stable social networks, and more than half of these work in medically related occupations. Once factitious disorder is diagnosed, it is important to confront the patient but remainsupportive. When factitious disorder is established in a person working in health care it is advisable to organise a multidisciplinary meeting involving the patient’s generalpractitioner, a physician and surgeon, a psychiatrist, and a medicolegal representative.
If, and only if, the deliberate feigning of symptoms and signscan be established (such as by observation of self mutilation)
should patients be confronted. It is helpful if both a psychiatrist and the referring doctor (who should have met to discuss theaims, content, and possible outcomes of the meeting beforehand) can carry out the confrontation jointly. This“supportive confrontation” is done by gently but firmly telling the patient that you are aware of the role of their behaviour inthe illness whilst at the same time offering psychological care tohelp with this. After confrontation, patients usually stop the behaviour or leave the clinic. Only sometimes do they engage inthe psychiatric care offered.
Malingering A distinction should be made between factitious disorders andmalingering. Malingerers deliberately feign symptoms toachieve a goal (such as to avoid imprisonment or gain money).Malingering is behaviour and not a diagnosis. The extent to which a doctor feels it necessary to confront this issue willdepend on the individual circumstances.
ConclusionPatients with multiple longstanding functional symptoms arerelatively uncommon, but their interaction with the healthsystem is memorable in that it often leaves both them and their doctors frustrated. Their effective management requires that special attention be paid to their interpersonal difficulties(including those arising in their relationship with the doctor),
the limiting of unhelpful demands, and the avoidance of iatrogenic harm. As with any chronic illness, confident management and getting to know a patient as a person canchange what is often a frustrating task into a rewarding one.
Münchausen’s syndrome
x Münchausen’s syndrome is an uncommonsubtype of factitious illness in which the patient, who is often a man with sociopathic traits and anitinerant lifestyle, has a long career of attending multiple hospitals with factitious symptoms andsigns
x Management is as for factitious disorder, but engagement with psychiatric treatment is rare
Evidence based summary
x Prevalence of chronic multiple functional somatic symptomsdepends on how many functional symptoms are required—thefewer symptoms the higher the prevalence
x Patients with chronic multiple functional somatic symptoms(somatisation disorder) can be effectively managed in primary care, with resulting cost savings
Kroenke K, Spitzer RL, deGruy FV, Hahn SR, Linzer M, Williams JB, et al.Multisomatoform disorder. An alternative to undifferentiated somatoformdisorder for the somatizing patient in primary care. Arch Gen Psychiatr y1997;54:352-8
Smith GR, Monson RA, Ray DC. Psychiatric consultation in somatizationdisorder —a randomized controlled study. N Engl J Med 1986;314:1407-13
Suggested reading
x Bass C. Management of somatisation disorder. Prescribers J 1996;36:198-205
x Dixon DM, Sweeney KG, Pereira Gray DJ. The physician healer ancient magic or modern science? Br J Gen Pract 1999;49:309-12
x Fink P, Rosendal M, Toft T. Assessment and treatment of functionaldisorders in general practice: the extended reattribution andmanagement model—an advanced educational program for nonpsychiatric doctors. Psychosom 2002;43:93-131
x Smith GR. Management of patients with multiple symptoms. In:
Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms . Oxford: Oxford University Press, 1995:175-87
x Tate P. The doctor’s communication handbook. Oxford: RadcliffeMedical Press, 1994
Failing to recognise and institute appropriate management forpatients with multiple functional somatic symptoms may lead toiatrogenic harm from excessive and inappropriate medical andsurgical intervention
ABC of Psychological Medicine
24
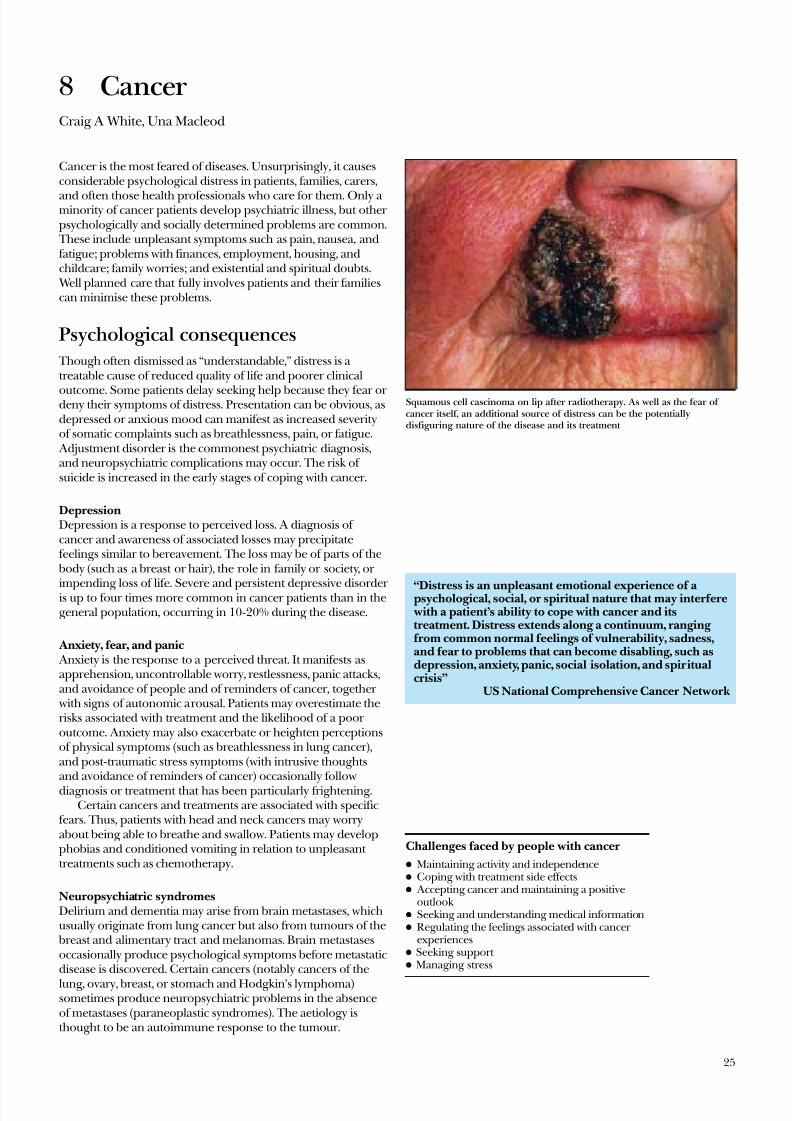
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 36/69
8 CancerCraig A White, Una Macleod
Cancer is the most feared of diseases. Unsurprisingly, it causesconsiderable psychological distress in patients, families, carers,
and often those health professionals who care for them. Only a minority of cancer patients develop psychiatric illness, but other psychologically and socially determined problems are common.
These include unpleasant symptoms such as pain, nausea, andfatigue; problems with finances, employment, housing, andchildcare; family worries; and existential and spiritual doubts.
Well planned care that fully involves patients and their familiescan minimise these problems.
Psychological consequences Though often dismissed as “understandable,” distress is a treatable cause of reduced quality of life and poorer clinical
outcome. Some patients delay seeking help because they fear or deny their symptoms of distress. Presentation can be obvious, asdepressed or anxious mood can manifest as increased severityof somatic complaints such as breathlessness, pain, or fatigue.
Adjustment disorder is the commonest psychiatric diagnosis,and neuropsychiatric complications may occur. The risk of suicide is increased in the early stages of coping with cancer.
DepressionDepression is a response to perceived loss. A diagnosis of cancer and awareness of associated losses may precipitatefeelings similar to bereavement. The loss may be of parts of the
body (such as a breast or hair), the role in family or society, or
impending loss of life. Severe and persistent depressive disorder is up to four times more common in cancer patients than in thegeneral population, occurring in 10-20% during the disease.
Anxiety, fear, and panic Anxiety is the response to a perceived threat. It manifests asapprehension, uncontrollable worry, restlessness, panic attacks,and avoidance of people and of reminders of cancer, together
with signs of autonomic arousal. Patients may overestimate therisks associated with treatment and the likelihood of a poor outcome. Anxiety may also exacerbate or heighten perceptionsof physical symptoms (such as breathlessness in lung cancer),and post-traumatic stress symptoms (with intrusive thoughtsand avoidance of reminders of cancer) occasionally followdiagnosis or treatment that has been particularly frightening.
Certain cancers and treatments are associated with specificfears. Thus, patients with head and neck cancers may worryabout being able to breathe and swallow. Patients may developphobias and conditioned vomiting in relation to unpleasant treatments such as chemotherapy.
Neuropsychiatric syndromesDelirium and dementia may arise from brain metastases, whichusually originate from lung cancer but also from tumours of the
breast and alimentary tract and melanomas. Brain metastasesoccasionally produce psychological symptoms before metastaticdisease is discovered. Certain cancers (notably cancers of the
lung, ovary, breast, or stomach and Hodgkin’s lymphoma)sometimes produce neuropsychiatric problems in the absenceof metastases (paraneoplastic syndromes). The aetiology isthought to be an autoimmune response to the tumour.
“Distress is an unpleasant emotional experience of apsychological, social, or spiritual nature that may interferewith a patient’s ability to cope with cancer and itstreatment. Distress extends along a continuum, ranging from common normal feelings of vulnerability, sadness,and fear to problems that can become disabling, such asdepression, anxiety, panic, social isolation, and spiritualcrisis”
US National Comprehensive Cancer Network
Challenges faced by people with cancer
x Maintaining activity and independencex Coping with treatment side effectsx Accepting cancer and maintaining a positive
outlook x Seeking and understanding medical informationx Regulating the feelings associated with cancer
experiencesx Seeking support x Managing stress
Squamous cell cascinoma on lip after radiotherapy. As well as the fear of cancer itself, an additional source of distress can be the potentiallydisfiguring nature of the disease and its treatment
25

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 37/69
Who becomes distressed? The severity of emotional distress is more closely related to a patient’s pre-existing vulnerability than to the characteristics of the cancer. Distress is also more likely to occur at specific pointsin a patient’s experience of cancer:
Diagnosis —Investigation and diagnosis are particularlystressful and can cause shock, anger, and disbelief as well as
emotional distress. These resolve without intervention in most patients, but especially high levels of distress at this time arepredictive of later emotional problems. It can help if doctorsexplain that patients’ feelings are expected and normal (“I
would expect you to have times when you feel tearful andcannot get it out of your head”).
During treatment — Treatment itself can be a potent cause of distress. It may involve hospital attendance but also unpleasant surgery, radiotherapy, or chemotherapy. Side effects include hair loss and disfigurement. Patients worry about whether treatment is working and are likely to become distressed at times of apparent treatment failure.
End of treatment — At the end of apparently successful
treatment some patients can experience “rebound” distressassociated with the fear that the cancer might recur or spread. The ending of a prolonged relationship with the cancer servicestaff can lead to a sense of loss and vulnerability. It is only at thistime that some patients become fully aware of the impact of their cancer experience.
After treatment —Like those with other life threatening illnesses, patients who survive cancer may reorder their lifepriorities and experience psychological benefits including a greater appreciation of some aspects of their life. Others needhelp to overcome continuing worries, including preoccupation
with loss and illness, a tendency to avoid reminders of cancer,and difficulties coping with intimacy, return to work, and fearsof recurrence. Fear of recurrence can manifest as a form of
health anxiety with misinterpretation of physiologicalsensations (such as believing that pain associated with a musclestrain represents a recurrence of cancer) and the anxiousseeking of reassurance.
Recurrence —Patients who believe they have been cured (that is, those most likely to be surprised by recurrence) are at greater risk of severe distress if recurrence occurs. Most patients report recurrence of cancer as more distressing than receiving theinitial diagnosis.
Terminal disease — About 40% of people who develop cancer will die as a result. The terminal phase commonly brings fear of uncontrolled pain, of the process of dying, of what happensafter death, and of the fate of loved ones. Depression is
common in the terminal phase, especially in those with poorlycontrolled physical symptoms.
Management People with cancer benefit from care in which psychologicaland medical care are coordinated. Apart from the obvious
Risk factors for psychiatric disorder
Patient x History of psychiatric disorder x Social isolationx Dissatisfaction with medical carex Poor coping (such as not seeking information or
talking to friends)
Cancerx Limitation of activitiesx Disfiguring x Poor prognosis
Treatment x Disfiguring x Isolating (such as bone marrow transplant)x Side effects
Issues to be considered in planning care
x Patient’s and family’s understanding of the illness and its treatment x Patient’s and family’s understanding of help availablex Explanation of how symptomatic relief will be providedx How the patient can be fully involved in carex Who will be managing the treatment planx Routine and emergency contact arrangementsx Practical help in everyday activitiesx Support at home—role of hospital and residential carex Involving and supporting family and friends
Psychological care for cancer patients
In primary carex Need for agreed local protocolsx Multidisciplinary skills and resourcesx Individually agreed collaborative care for each
patient x Regular liaison with specialist units and local
agenciesx Local training for all involved
In specialist unitsx Training in psychological aspects of care for all staff x Regular review of all individual treatment plansx Protocols for routine management of “at risk” patients (such as relapse after chemotherapy)
x Involvement of specialist nurses and other staff with psychological expertisex Access to psychiatrists and clinical psychologists with special interest in managing cancer
problems for consultation and supervisionx Use of self help methods and voluntary agencies
Depression is common in the terminal phase of cancer,especially in patients with poorly controlled physicalsymptoms (Resignation by Carl Wilhelm Wilhelmson(1866-1928))
ABC of Psychological Medicine
26
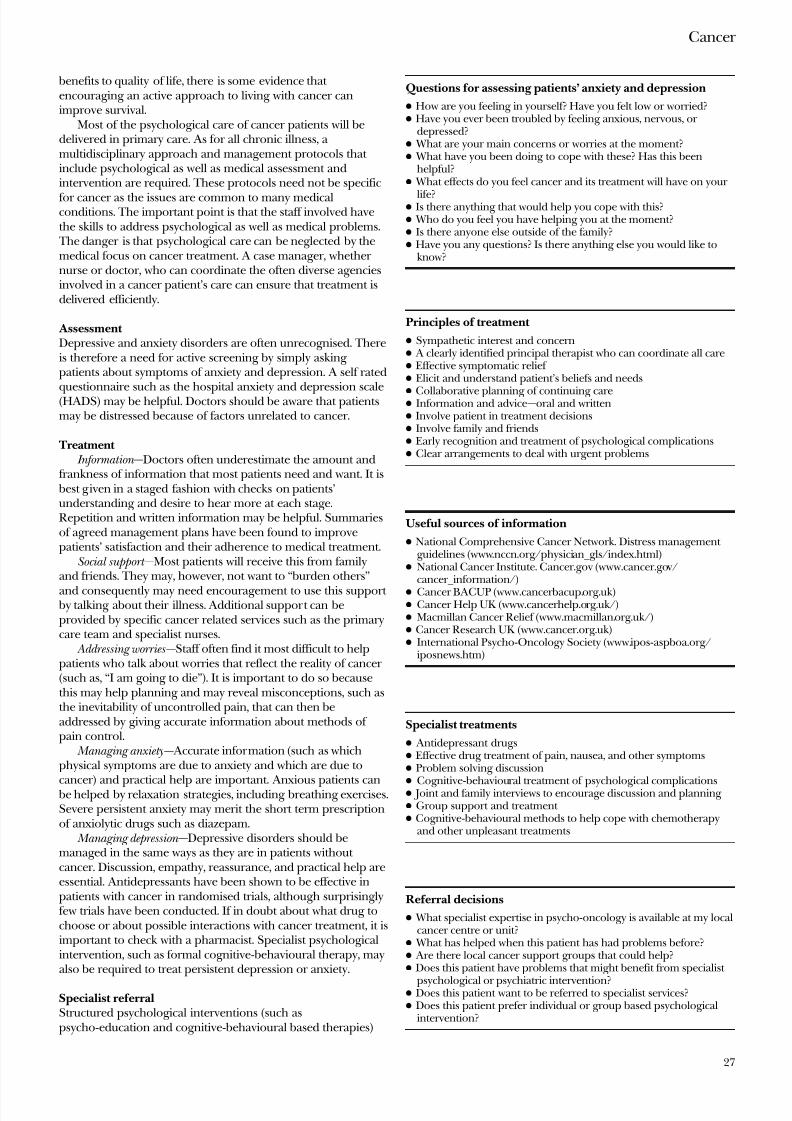
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 38/69
benefits to quality of life, there is some evidence that encouraging an active approach to living with cancer canimprove survival.
Most of the psychological care of cancer patients will bedelivered in primary care. As for all chronic illness, a multidisciplinary approach and management protocols that include psychological as well as medical assessment andintervention are required. These protocols need not be specific
for cancer as the issues are common to many medicalconditions. The important point is that the staff involved havethe skills to address psychological as well as medical problems. The danger is that psychological care can be neglected by themedical focus on cancer treatment. A case manager, whether nurse or doctor, who can coordinate the often diverse agenciesinvolved in a cancer patient’s care can ensure that treatment isdelivered efficiently.
Assessment Depressive and anxiety disorders are often unrecognised. Thereis therefore a need for active screening by simply asking patients about symptoms of anxiety and depression. A self rated
questionnaire such as the hospital anxiety and depression scale(HADS) may be helpful. Doctors should be aware that patientsmay be distressed because of factors unrelated to cancer.
Treatment Information —Doctors often underestimate the amount and
frankness of information that most patients need and want. It is best given in a staged fashion with checks on patients’understanding and desire to hear more at each stage.Repetition and written information may be helpful. Summariesof agreed management plans have been found to improvepatients’ satisfaction and their adherence to medical treatment.
Social support —Most patients will receive this from familyand friends. They may, however, not want to “burden others”
and consequently may need encouragement to use this support by talking about their illness. Additional support can beprovided by specific cancer related services such as the primarycare team and specialist nurses.
Addressing worries —Staff often find it most difficult to helppatients who talk about worries that reflect the reality of cancer (such as, “I am going to die”). It is important to do so becausethis may help planning and may reveal misconceptions, such asthe inevitability of uncontrolled pain, that can then beaddressed by giving accurate information about methods of pain control.
Managing anxiety— Accurate information (such as whichphysical symptoms are due to anxiety and which are due to
cancer) and practical help are important. Anxious patients can be helped by relaxation strategies, including breathing exercises.Severe persistent anxiety may merit the short term prescriptionof anxiolytic drugs such as diazepam.
Managing depression —Depressive disorders should bemanaged in the same ways as they are in patients without cancer. Discussion, empathy, reassurance, and practical help areessential. Antidepressants have been shown to be effective inpatients with cancer in randomised trials, although surprisinglyfew trials have been conducted. If in doubt about what drug tochoose or about possible interactions with cancer treatment, it isimportant to check with a pharmacist. Specialist psychologicalintervention, such as formal cognitive-behavioural therapy, mayalso be required to treat persistent depression or anxiety.
Specialist referralStructured psychological interventions (such aspsycho-education and cognitive-behavioural based therapies)
Questions for assessing patients’ anxiety and depression
x How are you feeling in yourself? Have you felt low or worried?x Have you ever been troubled by feeling anxious, nervous, or
depressed?x What are your main concerns or worries at the moment?x What have you been doing to cope with these? Has this been
helpful?x What effects do you feel cancer and its treatment will have on your
life?x Is there anything that would help you cope with this?x Who do you feel you have helping you at the moment?x Is there anyone else outside of the family?x Have you any questions? Is there anything else you would like to
know?
Principles of treatment
x Sympathetic interest and concernx A clearly identified principal therapist who can coordinate all carex Effective symptomatic relief x Elicit and understand patient’s beliefs and needs
x Collaborative planning of continuing carex Information and advice—oral and writtenx Involve patient in treatment decisionsx Involve family and friendsx Early recognition and treatment of psychological complicationsx Clear arrangements to deal with urgent problems
Useful sources of information
x National Comprehensive Cancer Network. Distress management guidelines (www.nccn.org/physician_gls/index.html)
x National Cancer Institute. Cancer.gov (www.cancer.gov/cancer_information/)
x Cancer BACUP (www.cancerbacup.org.uk)x Cancer Help UK (www.cancerhelp.org.uk/)x Macmillan Cancer Relief (www.macmillan.org.uk/)x Cancer Research UK (www.cancer.org.uk)x International Psycho-Oncology Society (www.ipos-aspboa.org/
iposnews.htm)
Specialist treatments
x Antidepressant drugsx Effective drug treatment of pain, nausea, and other symptomsx Problem solving discussionx
Cognitive-behavioural treatment of psychological complicationsx Joint and family interviews to encourage discussion and planning x Group support and treatment x Cognitive-behavioural methods to help cope with chemotherapy
and other unpleasant treatments
Referral decisions
x What specialist expertise in psycho-oncology is available at my localcancer centre or unit?
x What has helped when this patient has had problems before?x Are there local cancer support groups that could help?x Does this patient have problems that might benefit from specialist
psychological or psychiatric intervention?x Does this patient want to be referred to specialist services?x Does this patient prefer individual or group based psychological
intervention?
Cancer
27

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 39/69
have been shown to reduce anxiety and depression in cancer patients and to improve adherence to medical treatment.
Patients with severe or persistent distress may need referralto an experienced clinical psychologist or psychiatrist. Anincreasing number of mental health professionals are attachedto cancer centres and units, and other staff such asappropriately trained specialist nurses play an increasinglyimportant role.
Increasing numbers of non-NHS agencies also offer psychological care for patients with cancer. When referring patients to such services it is important to check their qualityand to ensure that their contribution is coordinated within anoverall care plan.
The picture of skin cancer is reproduced with permission of Dr P Marazziand Science Photo Library. Resignation is held at the Nationalmuseum,Stockholm, and is reproduced with permission of Bridgeman Art Library.
Evidence based summary
x Antidepressants are effective in treating depressed mood in cancer patients
x Cognitive-behavioural treatments are effective in relieving distress,especially anxiety, and in reducing disability
x Psychological interventions can be effective in relieving specificcancer related symptoms such as breathlessness
McDaniel JS, Musselman DL, Porter MR, Reed DA, Nemeroff CB. Depression inpatients with cancer. Diagnosis, biology, and treatment. Arch Gen Psychiatr y1995;52:89-99Sheard T, Maguire P. The effect of psychological inter ventions on anxiety anddepression in cancer patients: results of two meta-analyses. Br J Cancer 1999;80:1770-80Bredin M, Corner J, Krishnasamy M, Plant H, Bailey C, A’Hern R. Multicentrerandomised controlled trial of nursing intervention for breathlessness inpatients with lung cancer. BMJ 1999;318:901-4
Further reading
x Barraclough J. Cancer and emotion : a practical guide to psycho-oncology.3rd ed. Chichester: John Wiley, 1998
x Burton M, Watson M. Counselling patients with cancer . Chichester: John Wiley, 1998
x Faulkener A, Maguire P. Talking to cancer patients and their relatives.
Oxford: Oxford Medical Publications, 1994x Holland JC. Psycho-oncology. Oxford: Oxford University Press, 1998x Lewis S, Holland JC. The human side of cancer: living with hope,coping
with uncertainty. London: Harper Collins, 2000x Scott JT, Entwistle V, Sowden AJ, Watt I. Recordings or summaries
of consultations for people with cancer. Cochrane Database of Systematic Reviews. 2001
ABC of Psychological Medicine
28

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 40/69
9 TraumaRichard Mayou, Andrew Farmer
Minor physical trauma is a part of everyday life, and for most people these injuries are of only transient importance, but some
have psychiatric and social complications. Most peopleexperience major trauma at some time in their lives.
Psychological, behavioural, and social factors are all relevant to the subjective intensity of physical symptoms and their consequences for work, leisure, and family life. As a result,disability may become greater than might be expected from theseverity of the physical injuries.
Psychological and interpersonal factors also contribute tothe cause of trauma, and clinicians should be alert to these andtheir implications for treatment. Tactful questioning, carefulexamination, and detailed record keeping are essential,especially for non-accidental injury by a patient or others:x Ask for a detailed description of the cause of the incident x
Ask about previous trauma x Ask about substance misuse—alcohol and drugsx Look for patterns of injuries that may be non-accidental,deliberate self harm, or inflicted by othersx Check recordsx If suspicious speak to other informantsx Discuss findings and suspicions with a colleague.
Dealing with the acute event At a major incident it is important that members of theemergency services, especially ambulance staff and police,should seem calm and in control. This helps to relieve distressand prevent victims from suffering further injury. Explanationand encouragement can reduce fear at the prospect of being taken to hospital by ambulance. The needs of uninjuredrelatives and others involved should also be considered. Clearlyrecorded details of the incident, injury, and the extent of anyloss of consciousness may be useful in later assessment as wellas in the preparation of subsequent medicolegal reports.
Many people attend hospital emergency departments for minor cuts, bruises, or pain, or for “a check up” after being involved in an incident, whereas others attend their generalpractitioner. Immediate distress is common. Clear explanation,advice, and discussion at the outset can prevent later problemsin returning to normal activities and enable early recognition of
psychological and social consequences. A sympathetic approachis needed that includes suitable analgesia, reassurance about thelikely resolution of symptoms, and encouragement to return tonormal activity. Some patients may already be considering compensation, and records should be kept with this in mind.
Advice about return to work and other activitiesPatients with painful injuries that should improve within days or weeks are often uncertain how to behave and how soon toreturn to work. The assessment is an opportunity to give adviceabout this. Patients need information on the cause of their symptoms, their likely impact on daily life, and a positive planfor return to normal activity; this includes discussing the type of
work normally done, the employer’s attitude to time away from work, and opportunities for a graded increase in activity. Good,rapid communication between hospital and primary care isessential.
Lifetime prevalence of specific traumatic events (n=2181)
Type of trauma Prevalence
Assault 38%
Serious car or motor vehicle crash 28%
Other serious accident or injury 14%
Fire, flood, earthquake, or other natural disaster 17%
Other shocking experience 43%
Diagnosed with a life threatening illness 5%
Learning about traumas to others 62%Sudden, unexpected death of close friend or relative 60%
Any trauma 90%
Immediate management
x Physical treatment, including adequate analgesia x Sympathetic discussion of acute distressx Explanation and appropriate reassurance about treatment and
prognosisx Appropriate encouragement for graded return to work and other
activitiesx Indicate what help will be available for continuing psychological
symptoms and social problemsx Information and support to relatives
Detail of VerySlippy Weather by James Gillray(1757-1815)
Immediate effects of frightening trauma
x Causes a varied picture of anxiety, numbness, dissociation (feeling distanced from events, having fragmentary memories), andsometimes apparently inappropriate calmness
x Those who believe they are the innocent victims of others’misbehaviour are often angry, and this may be exacerbated bysubsequent frustrations
x The term “acute stress disorder” is now used for a combination of distress, intrusive memories (flashbacks, nightmares), avoidance, andnumbing in the months after the trauma. It occurs in 20-50% of those who have suffered major trauma
x The severity of emotional symptoms is much more closely relatedto how frightening the trauma was than to the severity of the injury;even uninjured victims may suffer considerable distress
x Severe distress is usually temporary but indicates a risk of long termpost-traumatic symptoms
29
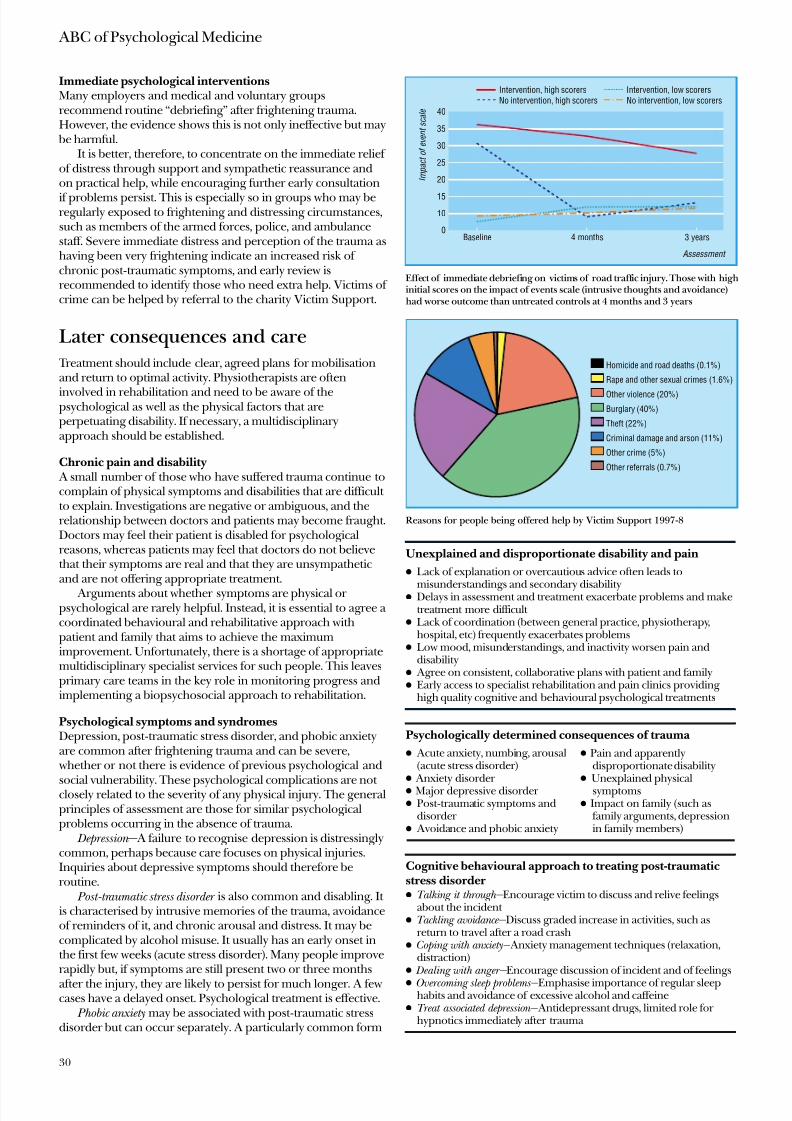
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 41/69
Immediate psychological interventionsMany employers and medical and voluntary groupsrecommend routine “debriefing” after frightening trauma.However, the evidence shows this is not only ineffective but may
be harmful.It is better, therefore, to concentrate on the immediate relief
of distress through support and sympathetic reassurance andon practical help, while encouraging further early consultation
if problems persist. This is especially so in groups who may beregularly exposed to frightening and distressing circumstances,such as members of the armed forces, police, and ambulancestaff. Severe immediate distress and perception of the trauma ashaving been very frightening indicate an increased risk of chronic post-traumatic symptoms, and early review isrecommended to identify those who need extra help. Victims of crime can be helped by referral to the charity Victim Support.
Later consequences and care Treatment should include clear, agreed plans for mobilisationand return to optimal activity. Physiotherapists are often
involved in rehabilitation and need to be aware of thepsychological as well as the physical factors that areperpetuating disability. If necessary, a multidisciplinaryapproach should be established.
Chronic pain and disability A small number of those who have suffered trauma continue tocomplain of physical symptoms and disabilities that are difficult to explain. Investigations are negative or ambiguous, and therelationship between doctors and patients may become fraught.Doctors may feel their patient is disabled for psychologicalreasons, whereas patients may feel that doctors do not believethat their symptoms are real and that they are unsympatheticand are not offering appropriate treatment.
Arguments about whether symptoms are physical or psychological are rarely helpful. Instead, it is essential to agree a coordinated behavioural and rehabilitative approach withpatient and family that aims to achieve the maximumimprovement. Unfortunately, there is a shortage of appropriatemultidisciplinary specialist services for such people. This leavesprimary care teams in the key role in monitoring progress andimplementing a biopsychosocial approach to rehabilitation.
Psychological symptoms and syndromesDepression, post-traumatic stress disorder, and phobic anxietyare common after frightening trauma and can be severe,
whether or not there is evidence of previous psychological and
social vulnerability. These psychological complications are not closely related to the severity of any physical injury. The generalprinciples of assessment are those for similar psychologicalproblems occurring in the absence of trauma.
Depression — A failure to recognise depression is distressinglycommon, perhaps because care focuses on physical injuries.Inquiries about depressive symptoms should therefore beroutine.
Post-traumatic stress disorder is also common and disabling. It is characterised by intrusive memories of the trauma, avoidanceof reminders of it, and chronic arousal and distress. It may becomplicated by alcohol misuse. It usually has an early onset inthe first few weeks (acute stress disorder). Many people improverapidly but, if symptoms are still present two or three months
after the injury, they are likely to persist for much longer. A fewcases have a delayed onset. Psychological treatment is effective.
Phobic anxiety may be associated with post-traumatic stressdisorder but can occur separately. A particularly common form
Unexplained and disproportionate disability and pain
x Lack of explanation or overcautious advice often leads to
misunderstandings and secondary disabilityx Delays in assessment and treatment exacerbate problems and make
treatment more difficult x Lack of coordination (between general practice, physiotherapy,
hospital, etc) frequently exacerbates problemsx Low mood, misunderstandings, and inactivity worsen pain and
disabilityx Agree on consistent, collaborative plans with patient and familyx Early access to specialist rehabilitation and pain clinics providing
high quality cognitive and behavioural psychological treatments
Psychologically determined consequences of trauma
x Acute anxiety, numbing, arousal(acute stress disorder)
x Anxiety disorder x Major depressive disorder x Post-traumatic symptoms and
disorder x Avoidance and phobic anxiety
x Pain and apparentlydisproportionate disability
x Unexplained physicalsymptoms
x Impact on family (such asfamily arguments, depressionin family members)
Cognitive behavioural approach to treating post-traumaticstress disorderx Talking it through— Encourage victim to discuss and relive feelings
about the incident x Tackling avoidance— Discuss graded increase in activities, such as
return to travel after a road crashx Coping with anxiety— Anxiety management techniques (relaxation,
distraction)x Dealing with anger— Encourage discussion of incident and of feelings
x Overcoming sleep problems— Emphasise importance of regular sleephabits and avoidance of excessive alcohol and caffeine
x Treat associated depression— Antidepressant drugs, limited role for hypnotics immediately after trauma
I m p a c t o f e v e n t s c a l e
Baseline 4 months
Assessment
3 years
Intervention, low scorersNo intervention, low scorers
0
15
20
25
30
35
40
10
Intervention, high scorersNo intervention, high scorers
Effect of immediate debriefing on victims of road traffic injury. Those with highinitial scores on the impact of events scale (intrusive thoughts and avoidance)had worse outcome than untreated controls at 4 months and 3 years
Homicide and road deaths (0.1%)
Rape and other sexual crimes (1.6%)
Other violence (20%)
Burglary (40%)
Theft (22%)
Criminal damage and arson (11%)
Other crime (5%)
Other referrals (0.7%)
Reasons for people being offered help by Victim Support 1997-8
ABC of Psychological Medicine
30
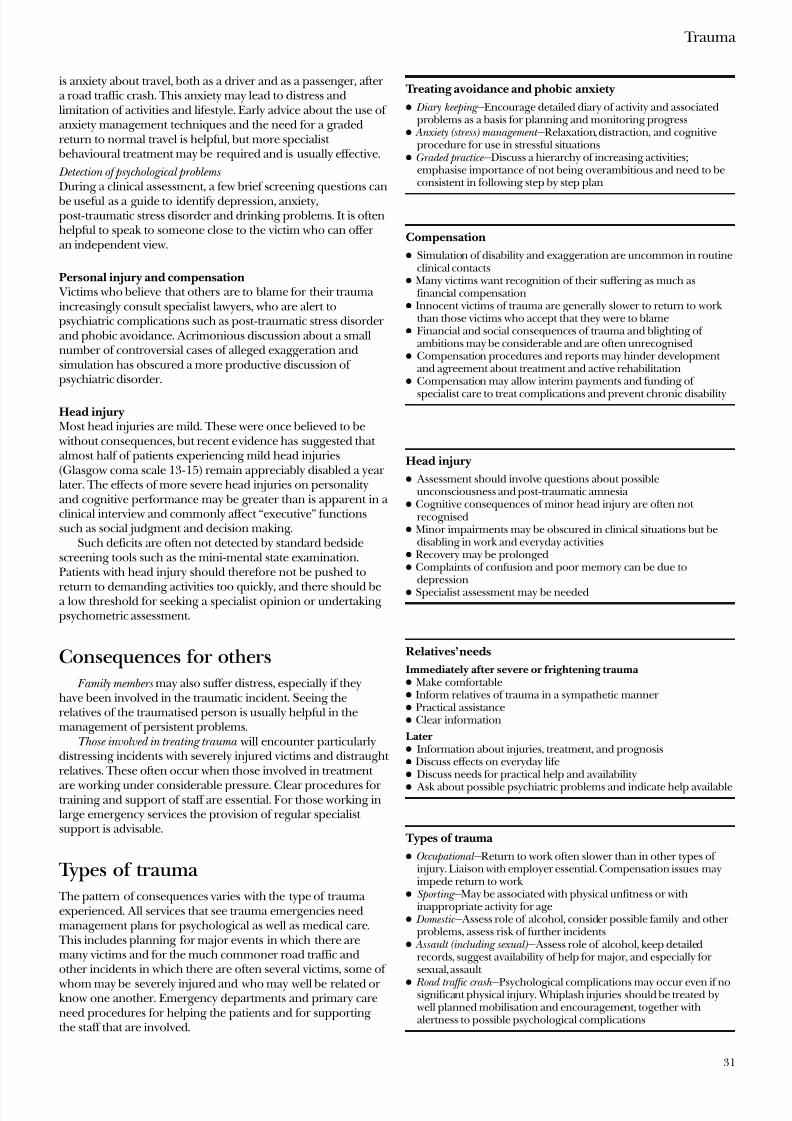
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 42/69
is anxiety about travel, both as a driver and as a passenger, after a road traffic crash. This anxiety may lead to distress andlimitation of activities and lifestyle. Early advice about the use of anxiety management techniques and the need for a gradedreturn to normal travel is helpful, but more specialist
behavioural treatment may be required and is usually effective.
Detection of psychological problems During a clinical assessment, a few brief screening questions can
be useful as a guide to identify depression, anxiety,post-traumatic stress disorder and drinking problems. It is oftenhelpful to speak to someone close to the victim who can offer an independent view.
Personal injury and compensation Victims who believe that others are to blame for their trauma increasingly consult specialist lawyers, who are alert topsychiatric complications such as post-traumatic stress disorder and phobic avoidance. Acrimonious discussion about a smallnumber of controversial cases of alleged exaggeration andsimulation has obscured a more productive discussion of psychiatric disorder.
Head injuryMost head injuries are mild. These were once believed to be
without consequences, but recent evidence has suggested that almost half of patients experiencing mild head injuries(Glasgow coma scale 13-15) remain appreciably disabled a year later. The effects of more severe head injuries on personalityand cognitive performance may be greater than is apparent in a clinical interview and commonly affect “executive” functionssuch as social judgment and decision making.
Such deficits are often not detected by standard bedsidescreening tools such as the mini-mental state examination.Patients with head injury should therefore not be pushed to
return to demanding activities too quickly, and there should bea low threshold for seeking a specialist opinion or undertaking psychometric assessment.
Consequences for others
Family members may also suffer distress, especially if theyhave been involved in the traumatic incident. Seeing therelatives of the traumatised person is usually helpful in themanagement of persistent problems.
Those involved in treating trauma will encounter particularlydistressing incidents with severely injured victims and distraught relatives. These often occur when those involved in treatment
are working under considerable pressure. Clear procedures for training and support of staff are essential. For those working inlarge emergency services the provision of regular specialist support is advisable.
Types of trauma The pattern of consequences varies with the type of trauma experienced. All services that see trauma emergencies needmanagement plans for psychological as well as medical care.
This includes planning for major events in which there aremany victims and for the much commoner road traffic andother incidents in which there are often several victims, some of
whom may be severely injured and who may well be related or know one another. Emergency departments and primary careneed procedures for helping the patients and for supporting the staff that are involved.
Treating avoidance and phobic anxiety
x Diary keeping— Encourage detailed diary of activity and associatedproblems as a basis for planning and monitoring progress
x Anxiety (stress) management— Relaxation, distraction, and cognitiveprocedure for use in stressful situations
x Graded practice— Discuss a hierarchy of increasing activities;emphasise importance of not being overambitious and need to beconsistent in following step by step plan
Compensation
x Simulation of disability and exaggeration are uncommon in routineclinical contacts
x Many victims want recognition of their suffering as much asfinancial compensation
x Innocent victims of trauma are generally slower to return to work than those victims who accept that they were to blame
x Financial and social consequences of trauma and blighting of ambitions may be considerable and are often unrecognised
x Compensation procedures and reports may hinder development and agreement about treatment and active rehabilitation
x Compensation may allow interim payments and funding of
specialist care to treat complications and prevent chronic disability
Head injury
x Assessment should involve questions about possibleunconsciousness and post-traumatic amnesia
x Cognitive consequences of minor head injury are often not recognised
x Minor impairments may be obscured in clinical situations but bedisabling in work and everyday activities
x Recovery may be prolongedx Complaints of confusion and poor memory can be due to
depressionx Specialist assessment may be needed
Relatives’ needs
Immediately after severe or frightening traumax Make comfortablex Inform relatives of trauma in a sympathetic manner x Practical assistancex Clear information
Laterx Information about injuries, treatment, and prognosisx Discuss effects on everyday lifex Discuss needs for practical help and availability
x Ask about possible psychiatric problems and indicate help available
Types of trauma
x Occupational— Return to work often slower than in other types of injury. Liaison with employer essential. Compensation issues mayimpede return to work
x Sporting— May be associated with physical unfitness or withinappropriate activity for age
x Domestic— Assess role of alcohol, consider possible family and other problems, assess risk of further incidents
x Assault (including sexual)— Assess role of alcohol, keep detailedrecords, suggest availability of help for major, and especially for sexual, assault
x Road traffic crash— Psychological complications may occur even if nosignificant physical injury. Whiplash injuries should be treated by
well planned mobilisation and encouragement, together withalertness to possible psychological complications
Trauma
31

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 43/69
Disasters All medical services and other institutions should have a disaster plan that is readily available and regularly reviewed. It should include a specification for immediate psychological careand information, together with proactive follow up so that psychological problems are identified early. Those involved incoping with disasters also require support and encouragement,and a minority may require specialist psychological help. The
disaster plan should also set out procedures for giving information to relatives and offering them practical help.
Conclusion
The psychological aspects of trauma may be important, even when injury seems trivial. Clear, sympathetic care, which takesaccount of patients’ needs, can do much to promote optimalrecovery. Specialist advice should be sought for persistent problems within the first few months of an injury. Long delaysin providing adequate assessment and treatment lead tounnecessary suffering and disability and may make suchproblems much more difficult to treat.
Evidence based summary
x Cognitive behaviour therapy is effective in treating post-traumaticstress disorder
x Early critical incident debriefing after trauma is potentially harmful
Sherman JJ. Effects of psychotherapeutic treatments for PTSD: a meta-analysisof controlled clinical trials. J Trauma Stress 1998;11:413-36
Wessely S, Rose S, Bisson J. Brief psychological interventions (“debriefing”) for trauma-related symptoms and the prevention of post traumatic stress disorder Cochrane Database Syst Rev 2999;(2):CD00050
Suggested reading
x Mayou RA, Bryant B. Outcome in consecutive emergencydepartment attenders following a road traffic accident. Br J
Psychiatry 2001;179:528-34x McDonald AS, Davey GCL. Psychiatric disorders and accidental
injury. Clin Psychol Rev 1996;16:105x NIH Consensus Development Panel on Rehabilitation of Persons
with Traumatic Brain Injury. Rehabilitation of persons withtraumatic brain injury. JAMA 1999;282:974-83
The print Very Slippy Weather is reproduced with permission of LeedsMuseum and Art Galleries and Bridgeman Art Library. The table of lifetime prevalence of traumatic events is adapted from Breslau et al. Arch Gen Psychiatry 1998;55:626-32. The graph of effect of immediatedebriefing on the psychiatric wellbeing of victims of road traffic injury isadapted from Mayou et al Br J Psychiatry 2000;176:590-4. The figureshowing reasons for people being offered help by Victim Support isadapted from Information in the Criminal Justice System in England and Wales.
Digest 4 , London: Home Office, 1999.
ABC of Psychological Medicine
32

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 44/69
10 FatigueMichael Sharpe, David Wilks
Fatigue can refer to a subjective symptom of malaise andaversion to activity or to objectively impaired performance. It
has both physical and mental aspects. The symptom of fatigueis a poorly defined feeling, and careful inquiry is needed toclarify complaints of “fatigue,” “tiredness,” or “exhaustion” andto distinguish lack of energy from loss of motivation or sleepiness, which may be pointers to specific diagnoses (see
below). Prevalence —Like blood pressure, subjective fatigue is
normally distributed in the population. The prevalence of continuously significant fatigue depends on the thresholdchosen for severity (usually defined in terms of associateddisability) and persistence. Surveys report that 5-20% of thegeneral population suffer from such persistent and troublesomefatigue. Fatigue is twice as common in women as in men but isnot strongly associated with age or occupation. It is one of thecommonest presenting symptoms in primary care, being themain complaint of 5-10% of patients and an important subsidiary symptom in a further 5-10%.
Fatigue as a symptom —Patients generally regard fatigue asimportant (because it is disabling), whereas doctors do not (because it is diagnostically non-specific). This discrepancy is a potent source of potential difficulty in the doctor-patient relationship. Fatigue may present in association withestablished medical and psychiatric conditions or be idiopathic.Irrespective of cause, it has a major impact on day to dayfunctioning and quality of life. Without treatment, theprognosis of patients with idiopathic fatigue is surprisinglypoor; half those seen in general practice with fatigue are still
fatigued six months later.
Causes of fatigue The physiological and psychological mechanisms underlying subjective fatigue are poorly understood. Fatigue may rather beusefully regarded as a final common pathway for a variety of causal factors. These can be split into predisposing,precipitating, and perpetuating factors.
Predisposing factors include being female and a history of either fatigue or depression.
Precipitating factors include acute physical stresses such asinfection with Epstein-Barr virus, psychological stresses such as
bereavement, and social stresses such as work problems. Perpetuating factors include physical inactivity, emotional
disorders, ongoing psychological or social stresses, andabnormalities of sleep. These factors should be sought as part of the clinical assessment.
Other physiological factors such as immunologicalabnormalities and slightly low cortisol concentration are of research interest but not clinical value.
Diagnoses associated with fatigue Among patients who present with severe chronic fatigue astheir main complaint, only a small proportion will be suffering from a recognised medical disease. In no more than 10% of patients presenting with fatigue in primary care is a disease
cause found. The rate is even lower in patients seen insecondary care.
Fatigue is a major symptom of many psychiatric disorders, but for a substantial proportion of patients with fatigue the
Medical conditions that may present withapparently unexplained fatigue
x General— Anaemia, chronic infection,autoimmune disease, cancer
x Endocrine disease— Diabetes, hypothyroidism,hypoadrenalism
x Sleep disorders— Obstructive sleep apnoea andother sleep disorders
x Neuromuscular— Myositis, multiple sclerosisx Gastrointestinal— Liver diseasex Cardiovascular— Chronic heart diseasex Respiratory— Chronic lung disease
Weary 1887 by Edward Radford (1831-1920)
Fatigue score
N o o f p a t i e n t s
00-4
146
-6
276
-8
625
-10
1288
-12
5127
-14
2287
-16
1968
-18
1387
-20
893
-22
541
-24
325
-26
163
-28
114
>28
84
2000
3000
4000
5000
6000
1000
Distribution of the complaint of fatigue in the population
33

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 45/69
symptom remains unexplained or idiopathic. In general, themore severe the fatigue and the larger the number of associatedsomatic (and unexplained) complaints, then the greater thedisability and the greater the likelihood of a diagnosis of depression.
Chronic fatigue syndromesChronic fatigue syndrome is a useful descriptive term for prominent physical and mental fatigue with muscular pain andother symptoms. It overlaps with another descriptive term,fibromyalgia, that has often been used when muscle pain ispredominant but in which fatigue is almost universal. There isalso substantial overlap of the diagnoses with other symptom
based syndromes, the so called functional somatic syndromes. The term myalgic encephalomyelitis (or encephalopathy)
has been used in Britain and elsewhere to describe a poorlyunderstood illness in which a prominent symptom is chronicfatigue exacerbated by activity. This is a controversial diagnosisthat some regard as simply another name for chronic fatiguesyndrome and that others regard as a distinct condition. Thisarticle will focus on chronic fatigue syndrome.
Prevalence and outcome —
Chronic fatigue syndrome can bediagnosed in up to 2% of primary care patients. Untreated, theprognosis is poor, with only about 10% of patients recovering ina two to four years. A preoccupation with medical causes seemsto be a negative prognostic factor.
Assessment and formulation History— The nature of the fatigue is an important clue todiagnosis, and it is therefore important to clarify patients’complaints. Fatigue described as loss of interest and enjoyment (anhedonia) points to depression. Prominent sleepinesssuggests a sleep disorder. The history should also cover x
Systematic inquiry for diseases and medications oftenassociated with fatiguex Symptoms of depression anxiety and sleep disorder x Patients’ own understanding of their illness and how theycope with it x Current social stresses.
Examination —Both a physical and mental state examinationmust be performed in every case, to seek medical andpsychiatric diagnoses associated with fatigue.
Routine investigations —If there are no specific indications for special investigations, a standard set of screening tests isadequate.
Special investigations —Immunological and virological testsare generally unhelpful as routine investigations. Sleep studies
can be useful in excluding other diagnoses, especiallyobstructive sleep apnoea and narcolepsy.
Psychological assessment —It is important to inquire fully about patients’ understanding of their illness (questions may include“What do you think is wrong with you?” and “What do youthink the cause is?”). Patients may be worried that the fatigue isa symptom of a severe, as yet undiagnosed, disease or that activity will cause a long term worsening of their condition.
Formulation — A formulation that distinguishes predisposing,precipitating, and multiple perpetuating factors is valuable inproviding an explanation to patients and for targeting intervention.
General management Persistent fatigue requires active management, preferably beforeit has become chronic. When a specific disease cause of fatigue
Psychiatric diagnoses commonly associatedwith fatigue
x Depressionx Anxiety and panicx Eating disordersx Substance misuse disordersx Somatisation disorder
Diagnostic criteria for chronic fatigue syndrome
Inclusion criteriax Clinically evaluated, medically unexplained fatigue of at least 6
months’ duration that isOf new onset (not life long)Not result of ongoing exertionNot substantially alleviated by rest
Associated with a substantial reduction in previous level of activitiesx Occurrence of 4 or more of the following symptoms
Subjective memory impairment, sore throat, tender lymph nodes,muscle pain, joint pain, headache, unrefreshing sleep,post-exertional malaise lasting more than 24 hours
Exclusion criteriax Active, unresolved, or suspected medical disease or psychotic,
melancholic, or bipolar depression (but not uncomplicated major depression), psychotic disorders, dementia, anorexia or bulimia nervosa, alcohol or other substance misuse, severe obesity
Screening tests for fatigue
x Full blood count x Erythrocyte sedimentation rate or C reactive
proteinx Liver function testsx Urea, electrolytes, and calciumx Thyroid stimulating hormone and thyroid
function testsx Creatine kinasex Urine and blood tests for glucosex Urine test for protein
Factors to consider in a formulation of chronic fatigue
Predisposing cause
Precipitating cause
Perpetuating cause
Biological Biological vulnerability
Acute disease PathophysiologyExcessive inactivitySleep disorder Side effects of drug treatment Untreated disease
Psychological Vulnerablepersonality
Stress DepressionUnhelpful beliefsabout causeFearful avoidance of
activitySocial Lack of support Life events
Social or work stress
Reinforcement of unhelpful beliefsSocial or work stress
ABC of Psychological Medicine
34
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 46/69
can be identified this should be treated. If no disease diagnosiscan be made, or if medical treatment of disease fails to relievethe fatigue, a broader biopsychosocial management strategy isrequired. A discussion with the patient about fatigue and itstreatment can be supplemented with written material (see
below).Patients should be told that they are suffering from a
common and treatable condition that the doctor takes seriously
and for which behavioural treatment can be helpful. Whilepatients may be concerned about possible disease and the needfor medical investigation and treatment, it can be explained that no disease has been found, and hence there is no disease basedtreatment, but that with help there is a great deal that thepatients can do themselves.
Identifying unhelpful beliefs —Potentially unhelpful beliefsshould be discussed. If a patient has a simple aetiological model(such as “It is all due to a virus”) an alternative approach basedon a biopsychosocial formulation can be outlined. This has theadvantage of highlighting potential perpetuating factors, asthese may be regarded as obstacles to recovery. Doctor andpatient can then work together to overcome these. It is rarely
productive to argue over the best name for the illness; instead,the emphasis should be on agreeing a positive and openminded approach to rehabilitation.
Managing activity and avoidance —Gradual increases in activitycan be advised unless there is a clear contraindication. It iscritical, however, to distinguish between carefully gradedincreases carried out in collaboration with patients and “forced”exercise. It is also important to explain that erratic variation
between overactivity on “good” days and subsequent collapsedoes not help long term recovery and that “stabilising” activityis a prerequisite to graded increases.
Depression and anxiety—If there is evidence of depression a trial of an antidepressant drug is worth while. Patients withfatigue are often sensitive to the side effects of antidepressants.However, if they are given adequate information about what toexpect when treatment begins, with small doses, most patientscan tolerate them. Randomised trials have shown psychologicaltherapies such as cognitive behaviour therapy to be equallyeffective for mild to moderate depression.
Managing occupational and social stresses —Patients whoremain in work may be overstressed by it. Those who have left
work may be inactive and demoralised and may not wish toreturn to the same job. These situations require a problemsolving approach to consider how to manage work demands,achieve a return to work, or to plan an alternative career.
Drug Treatments for Fatigue — A variety of pharmacologicaldrugs including stimulants and steroids have been advocated
for the treatment of fatigue. There is a limited evidence base for any of these pharmacological treatments, most of which maylead to substantial adverse effects. The role for these drugs istherefore limited and they should only be prescribed with great caution.
Referral for specialist management Most patients with fatigue are managed in primary care, but certain groups may require referral to specialist care:x Children with chronic fatiguex Patients in whom the general practitioner suspects occult
diseasex Patients with severe psychiatric illnessx Patients requiring specialist management of sleep disordersx Patients unresponsive to management in primary care.
Management of chronic fatigue
1 Assessment EmpathiseHistoryExaminationLimited investigationBiopsychosocial formulations
2 Treat treatable medical and psychiatric conditions
3 Help patient to overcome perpetuating factorsEducateReduce distressGradual increase in activitySolve social and occupational problems
4 Follow up
What is cognitive behaviour therapy?
x Brief pragmatic psychological therapy
x Targets beliefs and behaviours that might perpetuate symptomsx An established treatment for depression and anxietyx Has been adapted for somatic complaints of pain and fatiguex Requires a skilled therapist
Patients should be encouraged to gradually increase their activity (“MrsBradbury’s establishment for the recovery of ladies nervously affected”)
C h e c k l i s t i n d i v
i d u a l s t r e n g t h
( C I S ) -
f a t i g u e
0
35
40
45
50
55
60
30
Time since randomisation (months)
S i c k n e s s i m
p a c t p r o f i l e ( S I P ) - t o t a l
0 2 4 6
Functional impairment
Fatigue severity
8 10 12 140
1400
1200
1600
1800
Support groups
Natural course
Cognitive behaviour therapy
2000
1000
Efficacy of cognitive behaviour therapy for treating chronic fatigue syndrome
Fatigue
35

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 47/69
Referral may be to a physician or psychiatrist as is deemedmost appropriate. Psychologists may be able to offer cognitive behaviour therapy. Where available, joint medical andpsychiatric clinics are ideally suited to the assessment of chronicfatigue and related problems. It is essential there is close liaison between primary and specialist care to ensure a clear,consistent, and encouraging approach by all concerned.
RehabilitationRehabilitation based on behavioural principles is currently themost effective specialist treatment approach.
Cognitive behaviour therapy is a collaborative psychologicalrehabilitation that incorporates graded increases in activity but also pays greater attention to patients’ beliefs and concerns.
Graded exercise therapy is a structured progressive exerciseprogramme administered and carefully monitored by a therapist.
Both may be used in conjunction with antidepressant drugs.Both have been found to be effective in randomised trials of hospital referred cases of chronic fatigue syndrome. Somegeneral practitioners are able to provide graded exercise or
cognitive behaviour therapy in their practice or clinic. Othersmay wish to refer to a trained therapist.
Conclusion
Fatigue is a ubiquitous symptom that is important to patientsand has a major impact on their quality of life. It remains poorlyunderstood and has hitherto probably been not been givenadequate attention by doctors. Early and active management of fatigue in primary care may prevent progression to chronicity.Patients who have developed a chronic fatigue syndrome can benefit from specific treatments. Paying more attention to thesymptom of fatigue may help to avoid the distress and poor outcome that is associated with patients feeling that their problems are neither accepted nor understood. It may alsoreduce the numbers who turn to a variety of unproved, andeven harmful, alternative approaches.
What is graded exercise therapy?
x Explanation of fatigue as a physiologicalconsequence of inactivity, poor sleep, anddisturbed circadian rhythms
x Discussion, agreement, and implementation of graded exercise plans
x Monitoring of progress and setting of appropriate new targets
Evidence based summary
x Chronic fatigue syndrome is a descriptive term for a disabling syndrome that probably has multiple causes (physical andpsychological)
x Graded exercise and cognitive behaviour therapies are effective intreating chronic fatigue syndrome
Wessely S. Chronic fatigue: symptom and syndrome. Ann Intern Med 2001;134:838-43
Whiting P, Bagnall AM, Sowden AJ, Cornell JE, Mulrow CD, Ramirez G.Interventions for the treatment and management of chronic fatigue syndrome:a systematic review. JAMA 2001;286:1360-8
Further reading
x Wessely S, Hotopf M, Sharpe M. Chronic fatigue and its syndromes .Oxford: Oxford University Press, 1998
x Campling F, Sharpe M. Chronic fatigue syndrome: the facts . Oxford:Oxford University Press, 2000
x Reid S, Chalder T, Cleare A, Hotopf M, Wessely S. Chronic fatiguesyndrome. Clinical Evidence 2001 (Nov)
The painting Weary is held at Russell-Cotes Art Gallery and Museum,Bournemouth, and is reproduced with permission of Bridgeman Art Library. The graph of distribution of fatigue in the population is adaptedfrom Pawlikowska T, et al BMJ 1994;308:763-6. The box of diagnosticcriteria for chronic fatigue syndrome is adapted from Fukuda K, et al Ann
Intern Med 1994;121:953-9. The print of “Mrs Bradbury’s establishment for the recovery of ladies nervously affected” is reproduced with permission of Wellcome Library. The graph showing efficacy of cognitive behaviour therapy is adapted from Prins JB, et al Lancet 2001;357:841-7.
ABC of Psychological Medicine
36
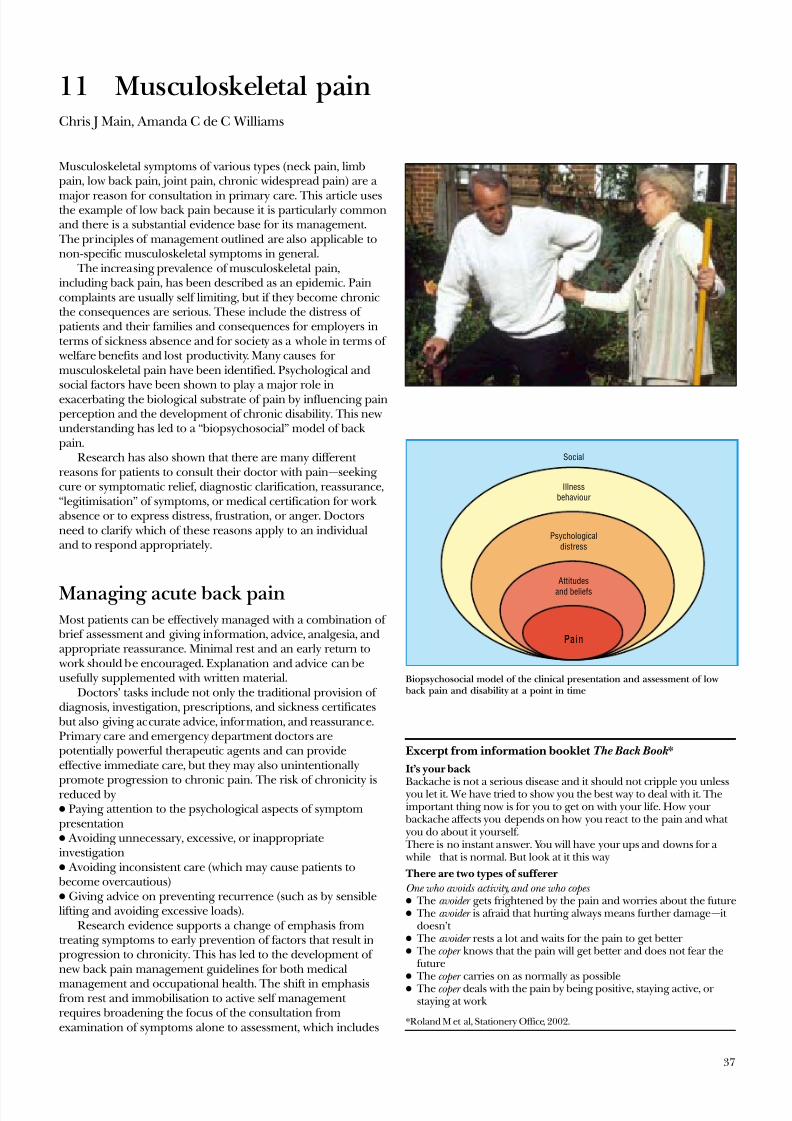
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 48/69
11 Musculoskeletal painChris J Main, Amanda C de C Williams
Musculoskeletal symptoms of various types (neck pain, limbpain, low back pain, joint pain, chronic widespread pain) are a
major reason for consultation in primary care. This article usesthe example of low back pain because it is particularly commonand there is a substantial evidence base for its management. The principles of management outlined are also applicable tonon-specific musculoskeletal symptoms in general.
The increasing prevalence of musculoskeletal pain,including back pain, has been described as an epidemic. Paincomplaints are usually self limiting, but if they become chronicthe consequences are serious. These include the distress of patients and their families and consequences for employers interms of sickness absence and for society as a whole in terms of welfare benefits and lost productivity. Many causes for musculoskeletal pain have been identified. Psychological andsocial factors have been shown to play a major role inexacerbating the biological substrate of pain by influencing painperception and the development of chronic disability. This newunderstanding has led to a “biopsychosocial” model of back pain.
Research has also shown that there are many different reasons for patients to consult their doctor with pain—seeking cure or symptomatic relief, diagnostic clarification, reassurance,“legitimisation” of symptoms, or medical certification for work absence or to express distress, frustration, or anger. Doctorsneed to clarify which of these reasons apply to an individualand to respond appropriately.
Managing acute back painMost patients can be effectively managed with a combination of brief assessment and giving information, advice, analgesia, andappropriate reassurance. Minimal rest and an early return to work should be encouraged. Explanation and advice can beusefully supplemented with written material.
Doctors’ tasks include not only the traditional provision of diagnosis, investigation, prescriptions, and sickness certificates but also giving accurate advice, information, and reassurance.Primary care and emergency department doctors arepotentially powerful therapeutic agents and can provideeffective immediate care, but they may also unintentionally
promote progression to chronic pain. The risk of chronicity isreduced byx Paying attention to the psychological aspects of symptompresentationx Avoiding unnecessary, excessive, or inappropriateinvestigationx Avoiding inconsistent care (which may cause patients to become overcautious)x Giving advice on preventing recurrence (such as by sensiblelifting and avoiding excessive loads).
Research evidence supports a change of emphasis fromtreating symptoms to early prevention of factors that result inprogression to chronicity. This has led to the development of new back pain management guidelines for both medical
management and occupational health. The shift in emphasisfrom rest and immobilisation to active self management requires broadening the focus of the consultation fromexamination of symptoms alone to assessment, which includes
Excerpt from information booklet The Back Book *
It’s your back
Backache is not a serious disease and it should not cripple you unlessyou let it. We have tried to show you the best way to deal with it. Theimportant thing now is for you to get on with your life. How your backache affects you depends on how you react to the pain and what you do about it yourself. There is no instant answer. You will have your ups and downs for a while—that is normal. But look at it this way
There are two types of sufferer
One who avoids activity, and one who copes x The avoider gets frightened by the pain and worries about the futurex The avoider is afraid that hurting always means further damage—it
doesn’t x The avoider rests a lot and waits for the pain to get better x The coper knows that the pain will get better and does not fear the
futurex
The coper carries on as normally as possiblex The coper deals with the pain by being positive, staying active, or staying at work
*Roland M et al, Stationery Office, 2002.
Pain
Attitudes
and beliefs
Psychological
distress
Illness
behaviour
Social
Biopsychosocial model of the clinical presentation and assessment of low back pain and disability at a point in time
37

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 49/69
patients’ understanding of their pain and how they behave inresponse to it. The shift towards self directed pain management recasts the role of primary care doctor to the more rewarding one of guide or coach rather than a mere “mechanic.”
Identify risk factors for chronicityGuidelines for primary care management of acute back painhighlight the identification of risk factors for chronicity. A useful
approach has been developed in New Zealand. It aims toinvolve all interested parties—patient, the patient’s family,healthcare professionals, and, importantly, the patient’semployer. Four groups of risk factors or “flags” for chronicityare accompanied by recommended assessment strategies, whichinclude the use of screening questionnaires, a set of structuredinterview prompts, and a guide to behavioural management.
The focus is on key psychological factors or “yellow flags” that favour chronicity:x The belief that back pain is due to progressive pathologyx The belief that back pain is harmful or severely disabling x The belief that avoidance of activity will help recoveryx A tendency to low mood and withdrawal from socialinteractionx The expectation that passive treatments rather than active self management will help.
The assessment of “red flags” will identify the small number of patients who need referral for an urgent surgical opinion.Similarly, patients with declared suicidal intent requireimmediate psychiatric referral. These two groups of patientsneed to be managed separately.
For the vast majority of patients, however, the identificationof contributory psychological and social factors should be seenas an investigation of the normal range of reactions to painrather than the seeking of psychopathology. Questions in theform of interview prompts have been designed to elicit potential psychosocial barriers to recovery in the “yellow flags”
system. They can be used at the time of initial presentation bythe general practitioner.
Establish collaborationRecent studies of miscommunications between doctors andpatients with pain show that adequate assessment andcollaborative management cannot be achieved without goodcommunication between doctors and patients: only then willpatients fully disclose their concerns.
The essence of good communication is to work towardunderstanding a patient’s problem from his or her ownperspective. In order to do this, the doctor must first gain thepatient’s confidence. A patient who has been convinced that thedoctor takes the pain seriously will give credence to what thedoctor says. Unfortunately, the converse is more common, andpatients who feel that a doctor has dismissed or under-ratedtheir pain are unlikely to reveal key information or to adhere totreatment advice.
Enhance accurate beliefs and self management strategiesIt is easy to overlook the value of simple measures. Manypatients respond positively to clear and simple advice, whichenables them to manage and control their own symptoms.
Factors associated with chronicity and outcome
Distressx Symptom awareness and concernx Depressive reactions; helplessness
Beliefs about pain and disabilityx Significance and controllabilityx Fears and misunderstandings about pain
Behavioural factorsx Guarded movements and avoidance patternsx Coping style and strategies
Structured interview promptsx What do you understand is the cause of your back pain?x What are you expecting will help you?x How are others responding to your back pain (employer,
coworkers, and family)?x What are you doing to cope with back pain?x Have you had time off work in the past with back pain?x Do you think that you will ever return to work? When?
Guidelines for collaborative management of patients withpain
x Listen carefully to the patient x Carefully observe the patient’s behaviour
x Attend not only to what is said but also how it is saidx Attempt to understand how the patient feelsx Offer encouragement to disclose fears and feelingsx Offer reassurance that you accept the reality of the painx Correct misunderstandings or miscommunications about the
consultationx Offer appropriate challenges to unhelpful thoughts and biases
(such as catastrophising)x Understand the patient’s general social and economic
circumstances
Examples of simple management strategies
x Explain the difference between “hurt” and “harm”x Reassure patients about the future and the benign nature of their
symptomsx Help patients regain control over painx Get patients to “pace” activities—that is, perform activities in
manageable, graded stages
x Advise that analgesic drugs be taken on a regular rather than a pain contingent basis
x Set realistic goals such as small increases in activityx Suggest rewards for successful achievement (such as listening
to some favourite music)
Clinical red flagsOrganic pathology
Concurrent medical problems
Iatrogenic factors
Beliefs
Coping strategies
Distress
Illness behaviour
Willingness to change
Family reinforcement
Work status
Health benefits and insurance
Litigation
Work satisfaction
Working conditions
Work characteristics
Social policy
Biomedical factors
Psychological orbehavioural factors(predictors)
Social and economicfactors
Occupationalfactors
Clinical yellow flags
Occupational blue flags
Socio-occupational blackflags
The clinical flags approach to obstacles to recovery from back pain andaspects of assessment
ABC of Psychological Medicine
38

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 50/69
Some of these strategies may seem self evident or eventrivial, but they are not. Only by building confidence slowly is it possible to prevent the development of invalidity. Occasionallypatients will seem to “get stuck” and become demoralised or distressed. Suggesting ways to enhance positive self management can help maintain progress towards a moresatisfactory lifestyle.
The success of the cognitive and behavioural approach
described below has stimulated the development of secondaryprevention programmes designed to prevent those with low
back pain from becoming chronically incapacitated by it.Intervention programmes based on cognitive behaviour therapy have also been shown to be effective in reducing disability.
Manage distress and angerIf patients show evidence of distress or anger, find out why.
Various strategies for dealing with distress and anger have beendeveloped.
Managing disabling chronic backpain
A minority of patients become increasingly incapacitated andrequire more detailed management of what has become a chronic pain problem. Research has shown that the most important influences on the development of chronicity arepsychological rather than biomechanical. The psychologicalfactors are high levels of distress, misunderstandings about painand its implications, and avoidance of activities associated with a fear of making pain worse.
For patients with established chronic disabling painspecialist referral is required. The treatment of choice is an
interdisciplinary pain management programme (IPMP). Inthese programmes the focus is changed from pain to function,
with particular emphasis on perceived obstacles to recovery. These pain management programmes address the clinical
flags. The most commonly used therapeutic approach is a cognitive-behavioural perspective with emphasis on self management. Treatment approaches based on cognitive and
behavioural principles have been found to be more effectivethan traditional biomedical or biomechanically orientedinterventions.
Specific chronic pain syndromesMany specific and more widespread pain syndromes have been
described—
such as “chronic pain,” late whiplash syndrome,chronic widespread pain, fibromyalgia, somatoform paindisorder, repetitive strain disorder. It seems unlikely that theseare distinct entities, and they are best seen as overlapping descriptive terms that do not have specific aetiologicalsignificance. Multidisciplinary treatment that includespsychological, behavioural, and psychiatric assessment andinterventions is usually required.
Conclusion There needs to be a revolution in the day to day management of musculoskeletal pain. Not only do we need to abandon
prolonged rest and enforced inactivity as a form of treatment, but we also need to appreciate that addressing patients’ beliefs,distress, and coping strategies must be an integral part of management if it is to be effective.
Ways of enhancing positive self management
Get patients tox Identify when they are thinking in unrealistic, unhelpful ways about
their pain (such as “It will keep getting worse”) and to change tomaking a more balanced positive evaluation
x Notice when they are becoming tense or angry and then take stepsto interrupt their thoughts and to use relaxation strategies
x Change how they respond when the pain gets bad (such as pauseand take a break)
x Document their progressx Elicit and use the help of others to establish and maintain
successful coping strategies
Key strategies for assessing and managing distress and anger
associated with painx Distinguish distress associated with pain and disability from more
general distressx Identify iatrogenic misunderstandingsx Identify mistaken beliefs and fearsx Try to correct misunderstandingsx Identify iatrogenic distress and anger x Listen and empathisex Above all, don’t get angry yourself
Defining characteristics of modern pain management programmes
x Focus on function rather than diseasex Focus on management rather than curex Integration of specific therapeutic ingredientsx Multidisciplinary management x Emphasis on active rather than passive methodsx Emphasis on self care rather than simply receiving treatment
DisabilityDisuse
Depression
Fear of movement
or injury No fear
Avoidance Painful experiences
Catastrophising
Back pain
Confrontation
Recovery
Effects of confrontation or avoidance of pain on outcome of episode of low
back pain: fear of movement and re-injury can determine how some people recover from back pain while others develop chronic pain and disability
Musculoskeletal pain
39

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 51/69
Lessons learnt in the management of chronic low back painhave direct relevance to the early and specialist management of musculoskeletal pain in general.
The photograph of a man with back pain is reproduced with permissionof John Powell/Rex. The figure showing the biopsychosocial model of low back pain is adapted from Waddell G, The back pain revolution , Edinburgh:Churchill Livingstone, 1998. The figure showing the clinical flagsapproach to assessing back pain and the box of defining characteristics of modern pain management programmes are adapted from Main CJ andSpanswick CC, Pain management: an interdisciplinary approach , Edinburgh:Churchill-Livingstone, 2000. The boxes of guidelines for collaborativemanagement of patients with pain, of key strategies for managing distressand anger associated with pain, of structured interview prompts, and of ways to enhance positive self management are adapted from Main CJ and Watson PJ, in Gifford L, ed, Topical issues in pain , vol 3, Falmouth: CNSPress (in press). The figure showing effects of confrontation or avoidanceof pain on outcome of episode of low back pain is adapted from Vlaeyen JWS et al, J Occup Rehabil 1995;5:235-52.
Evidence based summary
x Acute back pain is best treated with minimal rest and rapid returnto work and normal activity
x Psychological and behavioural responses to pain and social factorsare the main determinants of chronic pain disability
x Specialist psychological treatments and pain management programmes are effective in treating chronic pain
Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice topatients with back pain can have a positive effect. A randomised controlled trialof a novel educational booklet in primary care. Spine 1999;24:2484-91
Linton SJ. A Review of psychological risk factors in back and neck pain. Spine 2000;25:1148-56
Morley SJ, Eccleston C, Williams A. Systematic review and meta-analysis of randomised controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13
Further reading
x Clinical Standards Advisory Group. Clinical Standards AdvisoryGroup report on back pain . London: HMSO, 1994
x Kendall NAS, Linton SJ, Main CJ. Guide to assessing psychosocial yellow flags in acute low back pain: risk factors for long term disability and work loss . Wellington, NZ: Accident Rehabilitation and
Compensation Insurance Corporation of New Zealand and theNational Health Committee, 1997
x Royal College of General Practitioners. Clinical guidelines for the management of acute low back pain . London: RCGP, 1996
x Waddell G, Burton K. Occupational health guidelines for the management of low back pain at work—evidence review . London: Facultyof Occupational Medicine, 2000
x Roland M, Waddell G, Klaber-Moffett J, Burton AK, Main CJ. The back book. 2nd ed. Norwich: Stationery Office, 2002
ABC of Psychological Medicine
40

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 52/69
12 Abdominal pain and functional gastrointestinaldisordersElspeth Guthrie, David Thompson
Various functional gastrointestinal pain syndromes have beendefined, but there is substantial overlap between them. There isalso substantial overlap with other functional disorders such aschronic fatigue syndrome, fibromyalgia, and chronic pelvic pain.
The classification system for functional gastrointestinaldisorders (FGID) therefore remains controversial and is seldomused outside specialist and research settings. Furthermore, thepsychological management of these different syndromes isessentially similar.
In primary care about half of the patients seen with gut complaints have FGID, the most common disorder being irritable bowel syndrome. A UK general practitioner isestimated to see eight patients with irritable bowel syndrome
every week, one of whom will be presenting for the first time. The quality of life of patients with chronic FGID is far poorer than in the general population, and is even significantlylower than in patients with many other chronic illnesses. Thesepatients are not merely the “worried well.” It is also important toresist the temptation to think of FGID as exclusivelypsychological disorders. A biopsychosocial approach ispreferable. Physiological studies have suggested that patients
with FGID have abnormal visceral sensation and abnormalpatterns of bowel motility. Both psychological and physiologicalfactors are involved, with the relative contribution of these
varying among patients. Aetiological factors include physiological and psychological
predisposition, early life experience, and current social stresses.
It has been shown that a combination of psychological factorsand sensitisation of the gut after infection can trigger irritable
bowel syndrome in adults. Emotional distress — The degree of associated emotional
distress with FGID depends on the treatment setting. In thecommunity and general practice the prevalence of psychologicaldistress in patients with functional abdominal pain is about 10-20%, whereas in clinic and outpatient settings it is 30-40%, andis even higher for patients who are “treatment resistant.”
Abuse — Women with severe FGID often have a history of sexual and emotional abuse. This is as high as 30% in thoseattending gastroenterology clinics.
Initial management Most patients with FGID have relatively mild symptoms and can
be managed effectively in primary care. Only a third of patientsseen in primary care with irritable bowel syndrome are referredto gastrointestinal specialists for further assessment andtreatment.
Symptomatic treatment —Drug treatments for FGID are aimedat improving the predominant symptoms, such as constipation,diarrhoea, abdominal pain, or upper gastrointestinal symptoms.Standard treatments for lower bowel symptoms, depending onthe predominant symptom, include dietary fibre, laxatives,antispasmodic agents (including anticholinergics and direct
smooth muscle relaxants), and antidiarrhoeals. Treatment for upper gastrointestinal symptoms include H2 receptor antagonists and prokinetics. There are several useful reviews of the efficacy of these agents in FGID (see further reading).
Functional gastrointestinal disorders
x Functional dyspepsia x Ulcer-like dyspepsia x Dysmotility-like dyspepsia x Unspecified dyspepsia x Functional diarrhoea x Functional constipation
x Irritable bowel syndromex Functional abdominal bloating x Unspecified functional bowel disorder x Functional abdominal pain syndromex Unspecified functional abdominal
pain
Diagnostic criteria for irritable bowel syndrome
In preceding 12 months at least 12 weeks of abdominal discomfort with2 of 3 features: relieved with defecation, onset associated with change infrequency of stool, onset associated with change in form of stoolSupportive symptoms includex Fewer than 3 bowel movements a week x More than 3 bowel movements a dayx Straining during bowel movement x Urgent bowel movementsx Feeling of incomplete bowel movement
x Hard or lumpy stoolsx Loose or watery stoolsx Passing mucusx Abdominal fullness,
bloating, or swelling
Early lifeGenetics
EnvironmentAbuse
Outcome
MedicationsDaily function
Doctor visitsQuality of life
PhysiologySensationMotility
Life stressPsychiatric illness
CopingSocial support
SymptomsBehaviour
Biopsychosocial model for functional abdominal pain
Primary care• Physical and psychosocial assessment
• Link physical and psychological
• Detect and treat depression with antidepressants
• Refer for brief psychological treatment if psychosocial issues prominent
• Elicit concerns
• Reassure about cancer
• Advice about simple treatments
Not improved 70% improved
75% improved
60-80% improved
60% improved
Gastrointestinal clinic• Detailed assessment, including psychosocial
factors
• Appropriate limited investigations
• Clear explanation
• Brief treatment with standard agents
• Consider antidepressants for pain
Not improved
Brief psychological treatment• Cognitive therapy
• Interpersonal or relational therapies
• Hypnosis
• Behavioural therapy
Not improved
Review diagnosis• Consider hypnosis or interpersonal therapy if have not been tried
• Consider pain management programme
Implement long term management
• Close liaison between general practitioner and physician• Advice from liaison psychiatrist or psychologist may help
Not improved
Algorithm for treating patients with functional gastrointestinal disorders
41
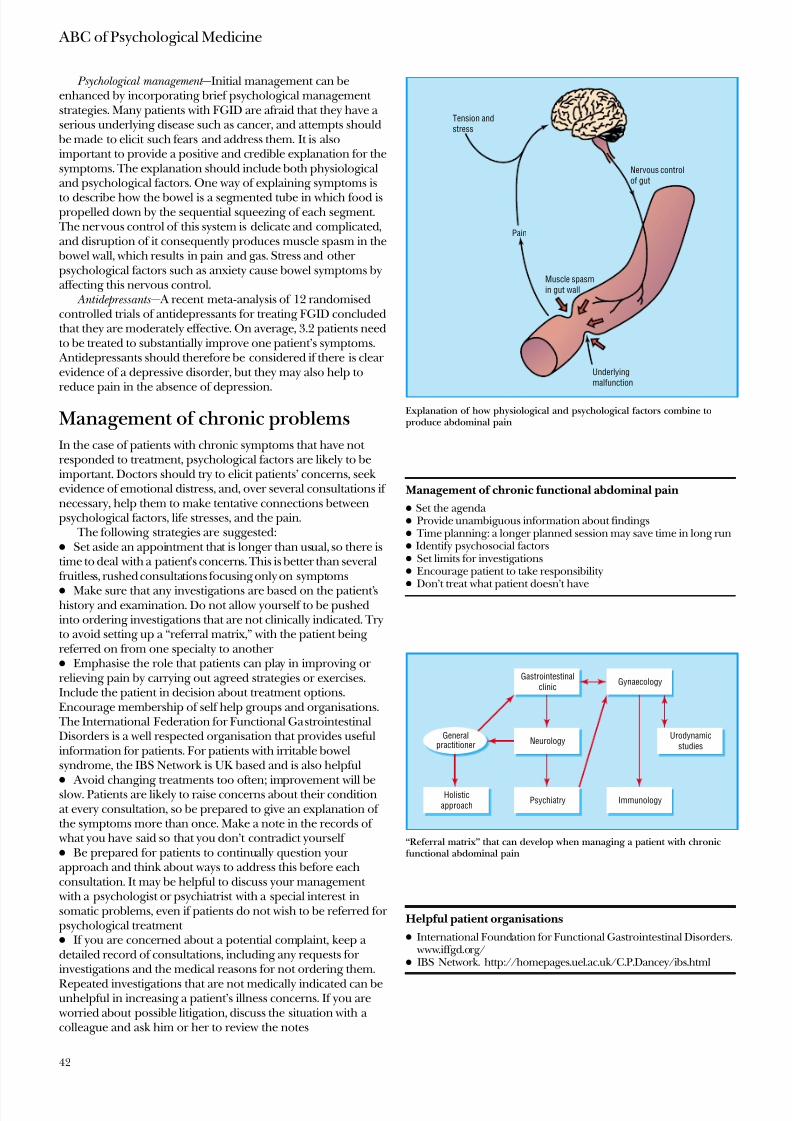
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 53/69
Psychological management —Initial management can beenhanced by incorporating brief psychological management strategies. Many patients with FGID are afraid that they have a serious underlying disease such as cancer, and attempts should
be made to elicit such fears and address them. It is alsoimportant to provide a positive and credible explanation for thesymptoms. The explanation should include both physiologicaland psychological factors. One way of explaining symptoms is
to describe how the bowel is a segmented tube in which food ispropelled down by the sequential squeezing of each segment.
The nervous control of this system is delicate and complicated,and disruption of it consequently produces muscle spasm in the
bowel wall, which results in pain and gas. Stress and other psychological factors such as anxiety cause bowel symptoms byaffecting this nervous control.
Antidepressants — A recent meta-analysis of 12 randomisedcontrolled trials of antidepressants for treating FGID concludedthat they are moderately effective. On average, 3.2 patients needto be treated to substantially improve one patient’s symptoms.
Antidepressants should therefore be considered if there is clear evidence of a depressive disorder, but they may also help to
reduce pain in the absence of depression.
Management of chronic problemsIn the case of patients with chronic symptoms that have not responded to treatment, psychological factors are likely to beimportant. Doctors should try to elicit patients’ concerns, seek evidence of emotional distress, and, over several consultations if necessary, help them to make tentative connections betweenpsychological factors, life stresses, and the pain.
The following strategies are suggested:x Set aside an appointment that is longer than usual, so there istime to deal with a patient’s concerns. This is better than severalfruitless, rushed consultations focusing only on symptoms
x Make sure that any investigations are based on the patient’shistory and examination. Do not allow yourself to be pushedinto ordering investigations that are not clinically indicated. Tryto avoid setting up a “referral matrix,” with the patient being referred on from one specialty to another x Emphasise the role that patients can play in improving or relieving pain by carrying out agreed strategies or exercises.Include the patient in decision about treatment options.Encourage membership of self help groups and organisations.
The International Federation for Functional GastrointestinalDisorders is a well respected organisation that provides usefulinformation for patients. For patients with irritable bowelsyndrome, the IBS Network is UK based and is also helpfulx
Avoid changing treatments too often; improvement will beslow. Patients are likely to raise concerns about their conditionat every consultation, so be prepared to give an explanation of the symptoms more than once. Make a note in the records of
what you have said so that you don’t contradict yourself x Be prepared for patients to continually question your approach and think about ways to address this before eachconsultation. It may be helpful to discuss your management
with a psychologist or psychiatrist with a special interest insomatic problems, even if patients do not wish to be referred for psychological treatment x If you are concerned about a potential complaint, keep a detailed record of consultations, including any requests for investigations and the medical reasons for not ordering them.
Repeated investigations that are not medically indicated can beunhelpful in increasing a patient’s illness concerns. If you are
worried about possible litigation, discuss the situation with a colleague and ask him or her to review the notes
Management of chronic functional abdominal pain
x Set the agenda x Provide unambiguous information about findingsx Time planning: a longer planned session may save time in long runx Identify psychosocial factorsx Set limits for investigationsx Encourage patient to take responsibilityx
Don’t treat what patient doesn’t have
Helpful patient organisations
x International Foundation for Functional Gastrointestinal Disorders. www.iffgd.org/
x IBS Network. http://homepages.uel.ac.uk/C.P.Dancey/ibs.html
Tension and
stress
Pain
Muscle spasm
in gut wall
Underlying
malfunction
Nervous control
of gut
Explanation of how physiological and psychological factors combine toproduce abdominal pain
Gastrointestinal
clinic
Holistic
approach
Urodynamic
studies
Gynaecology
ImmunologyPsychiatry
NeurologyGeneral
practitioner
“Referral matrix” that can develop when managing a patient with chronicfunctional abdominal pain
ABC of Psychological Medicine
42

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 54/69
x The aim of treatment should be to improve patients’symptoms and functioning rather than to abolish them. Althoughsome patients may remain chronically disabled despite treatment,appropriate and consistent management can prevent deterioration and protect patients from unnecessary surgery.
Referral for psychological treatment For patients who have not responded to initial management,four different kinds of psychological treatment have beenevaluated in FGID. They are cognitive therapies, behaviouraltherapies, interpersonal therapies, and hypnosis. Each therapyhas a different mechanism of action, but they have the commonaims of reducing symptoms and improving functioning. Most treatments are delivered on a one to one basis, once weekly,over a period of two to four months.
Although most trials indicate a positive outcome for psychological treatment, many have methodological flaws andfurther studies are required before definitive recommendationsabout treatment can be given. The most convincing evidencefor the efficacy of specific psychological treatments is for
patients with chronic or refractory abdominal symptoms.However, there may also be an important role for earlier intervention in order to prevent such long term difficulties.
Psychological treatments are not always available. As in anyother specialty, therapists need to have experience of treating chronic abdominal pain or chronic bowel disorders to developand retain competence. Psychological services based in primarycare are an option for patients with mild to moderatesymptoms, but counsellors are unlikely to develop the expertiseto enable them to treat patients with severe or refractoryabdominal symptoms. Similarly, referral to a psychiatrist or psychologist who is more used to managing severe mentalillness is unlikely to be fruitful. Dedicated medical liaisonservices with experience of somatic problems are more likely to be effective. If these do not exist consideration should be givento establishing a hospital based psychological medicine service.
The diagram of a biopsychosocial model for functional abdominal pain isadapted from Drossman DA et al, Gut 1999;45(suppl):II25-30.
Psychological treatments
Cognitive therapyx Modifies patients’ maladaptive beliefs about their pain and
symptomsx Encourages associated behaviour changesx Patients keep diaries to monitor pain and other symptoms,
associated thoughts, and behaviour x As therapy progresses, it may be possible to identify underlying
beliefs or fears about pain that drive preoccupation and worryx Therapeutic work directed at activating three change mechanisms:
1 Rational self analysis or self understanding (patients exploreidiosyncratic beliefs and fears and connect these to their pain)2 Decentring (patients gain distance from their selves by identifying their self talk and labelling it)3 Experiential disconfirmation (patients challenge their fears or irrational beliefs through planned behavioural experiments)
Behavioural therapiesx Focus on changing behaviour; they do not address motives or fearsx Patterns that reinforce abnormal behaviour are identified and
reversedx Activity is gradually increased, particularly for functional activities
such as social recreation and physical exercisex Pain behaviours are ignored and activity related behaviours are
reinforcedx Patients usually receive educational packages to increase their understanding of the condition
x Anxiety management strategies often included in treatment x Biofeedback can be used to teach patients to reduce tension in
affected muscles and to promote relaxation as a coping strategy
Interpersonal therapiesx Focus on resolving difficulties in interpersonal relationships that
underlie or exacerbate abdominal symptomsx Key problem areas include unresolved grief or loss, role transitions,
and relationship discordx Initial focus is on the patient’s abdominal symptoms, which are
explored in great detailx Emotional distress and abnormal feeling states arising from or
linked to physical symptoms are identifiedx Key problem areas in relationships and their link to physical and
psychological symptoms are understoodx Maladaptive relationship patterns, which may have developed after
key childhood experiences (such as sexual abuse) are identifiedx Solutions to interpersonal difficulties are tested out in therapy and
implemented in real world
Hypnosisx Directed at general relaxationx Hypnosis is induced using an arm levitation technique, which is
followed by deepening proceduresx General positive comments about health and wellbeing are madex Patients are asked to place their hand on abdomen, feel a sense of
warmth, and relate this to asserting control over gut functionx This is reinforced with visualisation (if patient has ability to do this)x Sessions are concluded with positive, ego strengthening suggestionsx After third session patients are given a tape for daily autohypnosis
Evidence based summary
x Treating functional gastrointestinal disorders with antidepressantsis effective even in the absence of depression
x Although several psychological treatments show promise intreating functional bowel disorders, no trial has yet providedunequivocal evidence of effectiveness
Jackson J, O’Malley PG, Tomkins G, Balden E, Santoro J, Kroenke K. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72
Talley NJ, Owen BKO, Boyce P, Paterson K. Psychological treatments for irritable bowel syndrome: a critique of controlled treatment trials. Am J
Gastroenterol 1996;91:277-86
Further reading
x Thompson WG, Heaton KW, Smyth GT, Smyth C. Irritable bowelsyndrome in general practice: prevalence, characteristics, andreferral. Gut 2000;46:78-82
x Drossman DA, Creed FH, Fava GA, Olden KW, Patrick DL, Toner BB, et al. Psychosocial aspects of the functional gastrointestinaldisorders. Gastroenterol Int 1995.1995:8:47-90
x Jailwala J, Imperiale TF, Kroenke K. Pharmacologic treatment of theirritable bowel syndrome: a systematic review of randomized,controlled trials. Ann Intern Med 2000;133:135-47
x Akehusrt R, Kaltenthaler E. Treatment of irritable bowel syndrome:a review of randomized controlled trials. Gut 2001;48:272
x Bytzer P. H2 receptor antagonists and prokinetics in dyspepsia: a
critical review. Gut 2002;50(suppl IV):58-62
Abdominal pain and functional gastrointestinal disorders
43
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 55/69
13 Chest painChristopher Bass, Richard Mayou
Chest pain is one of the commonest reasons for consultation inprimary care. Chest pain is usually mild and transient, but
further management is required in some cases. These are of twomain types—acute severe pain and persistent pain associated
with distress and functional limitation. Acute central chest painaccounts for 20-30% of emergency medical admissions.Chronic chest pain is the commonest reason for referral tocardiac outpatient clinics.
Management of chest pain The improved diagnosis and early treatment of ischaemic heart disease have not been accompanied by similar advances either in the delivery of long term rehabilitation of patients withischaemic heart disease or in the management of non-cardiaccauses of chest pain. Since at least half of those referred tocardiac outpatient clinics and about two thirds of emergencyadmissions have a non-cardiac cause for their chest pain, thereis a pressing need to address this problem.
Primary carePrimary care doctors have a major responsibility for thecontinuing care of patients with angina and those with chronicnon-cardiac chest pain, as well as a role in secondaryprevention. They therefore need good communication withspecialist cardiac services and access to appropriate resources,including psychological treatments.
Patients with a low risk of coronary disease (such as young women with no cardiac risk factors and atypical pain) do not usually need cardiac investigation. Some, however, especiallythose with chest pain who have a family history of heart diseaseor other risk factors, may need investigation. In such cases it isimportant that the possibility of a non-cardiac cause of thechest pain is explained before referral. If investigation revealsno cardiac cause for the pain patients need their worries to befully discussed, need advice about coping with symptoms, andshould be encouraged to maintain activity.
Patients with an intermediate or high risk (such as middle agedmale smokers) often require investigations even if the chest painis “not typical” of ischaemic pain. This will usually be achieved
by referral to a cardiology outpatient clinic or to an emergency
assessment service. When referring patients in whom the causeof chest pain is uncertain it is important to avoid giving themthe impression that the diagnosis of ischaemic heart disease isalready established (such as by prescribing anti-anginal drugs).
This is because, if patients come to believe that they haveischaemic heart disease, such beliefs can be difficult to changeeven if they are subsequently disproved by investigation.
Secondary care The best way to organise emergency care remains uncertain. Along wait for specialist investigations such as angiography islikely to increase anxiety and disability, as has been shown inpatients waiting for coronary artery surgery. Quicker access to
assessment (such as by rapid access clinics and observationunits) can be helpful but needs to be accompanied by a greater emphasis on aftercare for all patients assessed, not only those
who have had infarction or are undergoing cardiac surgery.
Assessment and management of chest pain in primary care
x History of pain, other symptoms and risk factorsx If at high risk of heart disease, refer for specialist assessment x If at low risk:
Identify non-cardiac causesGive a positive explanation
Advise how to cope with symptoms and return to normal activityDiscuss worriesOffer review if symptoms are persistent
Clinical priorities in managing patients with chest pain
Primary carex Recognise and refer possible heart diseasex Reassure minor chest painx Basic treatment of persistent non-cardiac painx Reassess chronic pain as required, monitor and coordinate
continuing carex Advise on secondary prevention need
Hospital emergency carex Immediate diagnosis and treatment plus initiating continuing care
of angina x Make a positive diagnosis; reassure if non-cardiac and arrange
follow up to determine investigation and treatment needsx Full and rapid communication with primary care
Cardiac outpatient carex Initiate immediate and continuing care of angina x
Reassure and advise if non-cardiac; plan treatment or reviewOther specialist carex Cardiac rehabilitation or aftercarex Psychological or psychiatric referral
British soldier admitted for observation with thediagnosis of “disordered action of the heart”—apost-combat syndrome in the first world warcharacterised by rapid heartbeat, shortness of breath,fatigue, and dizziness. (From Lewis T. The tolerance of physical exertion, as shown by soldiers suffering fromso-called ‘irritable heart.’ BMJ 1918;i:363-5)
44
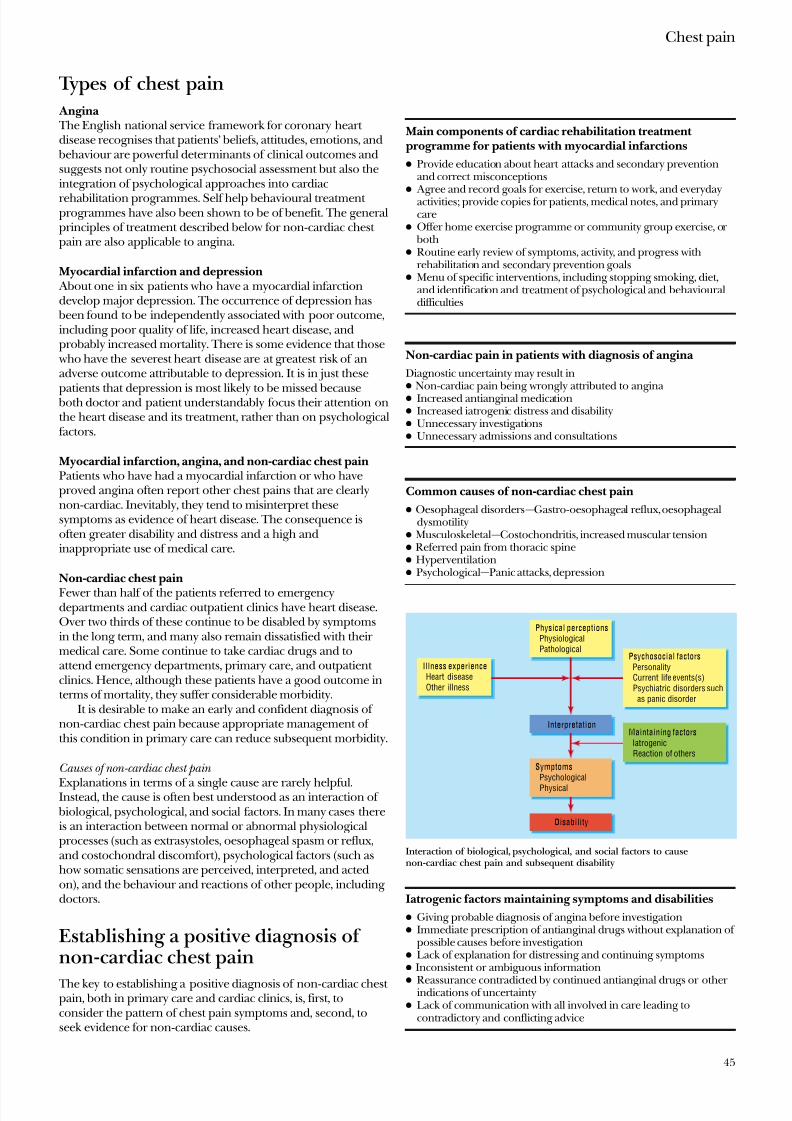
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 56/69
Types of chest pain
Angina The English national service framework for coronary heart disease recognises that patients’ beliefs, attitudes, emotions, and
behaviour are powerful determinants of clinical outcomes andsuggests not only routine psychosocial assessment but also theintegration of psychological approaches into cardiac
rehabilitation programmes. Self help behavioural treatment programmes have also been shown to be of benefit. The generalprinciples of treatment described below for non-cardiac chest pain are also applicable to angina.
Myocardial infarction and depression About one in six patients who have a myocardial infarctiondevelop major depression. The occurrence of depression has
been found to be independently associated with poor outcome,including poor quality of life, increased heart disease, andprobably increased mortality. There is some evidence that those
who have the severest heart disease are at greatest risk of anadverse outcome attributable to depression. It is in just these
patients that depression is most likely to be missed because both doctor and patient understandably focus their attention onthe heart disease and its treatment, rather than on psychologicalfactors.
Myocardial infarction, angina, and non-cardiac chest painPatients who have had a myocardial infarction or who haveproved angina often report other chest pains that are clearlynon-cardiac. Inevitably, they tend to misinterpret thesesymptoms as evidence of heart disease. The consequence isoften greater disability and distress and a high andinappropriate use of medical care.
Non-cardiac chest pain
Fewer than half of the patients referred to emergencydepartments and cardiac outpatient clinics have heart disease.Over two thirds of these continue to be disabled by symptomsin the long term, and many also remain dissatisfied with their medical care. Some continue to take cardiac drugs and toattend emergency departments, primary care, and outpatient clinics. Hence, although these patients have a good outcome interms of mortality, they suffer considerable morbidity.
It is desirable to make an early and confident diagnosis of non-cardiac chest pain because appropriate management of this condition in primary care can reduce subsequent morbidity.
Causes of non-cardiac chest pain
Explanations in terms of a single cause are rarely helpful.Instead, the cause is often best understood as an interaction of
biological, psychological, and social factors. In many cases thereis an interaction between normal or abnormal physiologicalprocesses (such as extrasystoles, oesophageal spasm or reflux,and costochondral discomfort), psychological factors (such ashow somatic sensations are perceived, interpreted, and actedon), and the behaviour and reactions of other people, including doctors.
Establishing a positive diagnosis of non-cardiac chest pain
The key to establishing a positive diagnosis of non-cardiac chest pain, both in primary care and cardiac clinics, is, first, toconsider the pattern of chest pain symptoms and, second, toseek evidence for non-cardiac causes.
Main components of cardiac rehabilitation treatment programme for patients with myocardial infarctions
x Provide education about heart attacks and secondary preventionand correct misconceptions
x Agree and record goals for exercise, return to work, and everydayactivities; provide copies for patients, medical notes, and primarycare
x Offer home exercise programme or community group exercise, or both
x Routine early review of symptoms, activity, and progress withrehabilitation and secondary prevention goals
x Menu of specific interventions, including stopping smoking, diet,and identification and treatment of psychological and behaviouraldifficulties
Non-cardiac pain in patients with diagnosis of angina
Diagnostic uncertainty may result inx Non-cardiac pain being wrongly attributed to angina x Increased antianginal medicationx Increased iatrogenic distress and disabilityx Unnecessary investigationsx Unnecessary admissions and consultations
Common causes of non-cardiac chest pain
x Oesophageal disorders—Gastro-oesophageal reflux, oesophagealdysmotility
x Musculoskeletal—Costochondritis, increased muscular tensionx Referred pain from thoracic spinex Hyperventilationx Psychological—Panic attacks, depression
Iatrogenic factors maintaining symptoms and disabilities
x Giving probable diagnosis of angina before investigationx Immediate prescription of antianginal drugs without explanation of
possible causes before investigationx Lack of explanation for distressing and continuing symptomsx Inconsistent or ambiguous information
x Reassurance contradicted by continued antianginal drugs or other indications of uncertainty
x Lack of communication with all involved in care leading tocontradictory and conflicting advice
Physical perceptions Physiological Pathological
Symptoms Psychological
Physical
Interpretation
Disability
Illness experience Heart disease Other illness
Psychosocial factors
Personality Current life events(s) Psychiatric disorders such as panic disorder
Maintaining factors
Iatrogenic Reaction of others
Interaction of biological, psychological, and social factors to causenon-cardiac chest pain and subsequent disability
Chest pain
45

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 57/69
Quality of chest pain Attempts to identify certain characteristics of chest pain that can help to establish a positive diagnosis of non-cardiac chest pain have been encouraging. For example, as few as threequestions can differentiate patients with chest pain but normalcoronary arteries from those with coronary heart disease.
Evidence for common non-cardiac causes
Oesophageal disorders are often associated with chest pain, but chest pain is poor correlated with objective oesophagealabnormalities. Symptomatic treatment (such as proton pumpinhibitors) can be useful. Psychological issues may needaddressing whether or not there is oesophageal pathology.Gastro-oesophageal reflux is an important cause of atypicalchest pain, but there is no convincing evidence that such chest pain is often related to disturbances of oesophageal motility.
Emotional disorders —Only a minority of patients who present to family doctors with non-cardiac chest pain are suffering fromconspicuous anxiety or depressive disorders. The rate of suchdisorders is, however, higher among those referred for specialist assessment in cardiac clinics, especially those who undergo
angiography and are shown to have normal coronary arteries. It is important to seek evidence of (a ) the key symptoms of depression (which include hopelessness; lack of interest,pleasure, and concentration; poor sleep; and irritability as wellas low mood) and (b) an association of the chest pain withanxiety and panic attacks.
Patients’ beliefs and worries Even if no definite psychiatric diagnosis can be made, it isessential to ask patients what goes through their mind whenthey experience chest pain.
Stressful life events Distressing life events can precipitate not only anxiety and
depressive disorders, but also functional symptoms such aschest pain. Events signifying loss, threat, and rejection are of particular importance. Open questions are most effective ineliciting these—such as: “Tell me about any changes or setbacksthat occurred in the months before your chest pain began.”
Treatment of non-cardiac painEarly and effective intervention is crucial, but how can this best
be provided? Because patients vary not only in the frequencyand severity of symptoms and associated disability but also intheir needs for explanation and treatment of their physical andpsychological problems, management needs to be flexible.
Avoiding iatrogenic worries —
A consultation for chest pain isinherently worrying. Inevitably, many patients assume that theyhave severe heart disease, which will have major adverse effectson their life. These concerns may be greatly increased by delaysin investigation, by comments or behaviours by doctors, and bycontradictory and inconsistent comments.
Symptomatic treatment —In some patients the pain is obviouslymusculoskeletal in origin and can be treated with non-steroidalanti-inflammatory drugs. Proton pump inhibitors provideeffective relief from the symptoms typical of gastro-oesophagealreflux, even in those with an essentially normal oesophagealmucosa. In some cases oesophageal function testing may reveal a motility disorder or acid reflux unresponsive to first line drugs.
These patients may require specialist gastroenterological referral.
Communication —
Problems in the care of patients with chest pain often arise from failures in communication between primaryand secondary care. Lack of information and contradictory or inconsistent advice makes it less likely that patients and their
Questions to differentiate patients with non-cardiac chest pain from those with coronary heart disease
Response
Question Typical Atypical
If you go up a hill (or other stressor) on 10 separateoccasions on how many do you get the pain?
10/10 < 10/10
Of 10 pains in a row, how many occur at rest? < 2/10 >2/10
How many minutes does the pain usually last? < 5 >5 When answers to all three questions are “atypical” the chance of coronarydisease is only 2% in patients aged < 55 years and 12% in those aged>55
Screening questions for panic attacks
x In the past six months have you ever had a spell or an attack whenyou suddenly felt frightened, anxious, or very uneasy?
x In the past six months have you ever had a spell or an attack whenfor no reason your heart suddenly began to race, you felt faint, or you couldn’t catch your breath?
If the answer is yes to either question then continuex Obtain descriptionx Did any of these spells happen when you were not in danger or the
centre of attention, such as in a crowd or when travelling?x
How many times have you had these spells in the past month?
Management of non-cardiac chest pain
General management x Explanation of the diagnosisx Reassurance that it is a real, common,
and well recognised problemx Advice on specific treatmentsx Advice on behaviour —such as not
avoiding exercisex Discussion of concernsx Provision of written informationx Involvement of relativesx Follow up to review
Specialist treatmentsx Cognitive behaviour
therapyx Antidepressant drugsx Psychosocial intervention
for associatedpsychological, family, and
social difficulties
Prevalence (%)
0
Patients given treadmillexercise test
Cardiac outpatient clinic
Psychiatric outpatient clinic
Primary care
General population
Patients given angiographyand with normal results
10 20 30 40
Prevalence of
panic disorder indifferent medicalsettings
C h e s
t p a in, pal p i t a t i o n s
P a n i c, ph o b i a
D y s th y m i a D y
s th y m i a
Time
Anxiety Anxiety Anxiety Anxiety
L i f e
e v e n t s c o r e
Life events and symptom reporting. Stress of adverse life events may result in increases in reporting of psychological and physical symptoms
ABC of Psychological Medicine
46
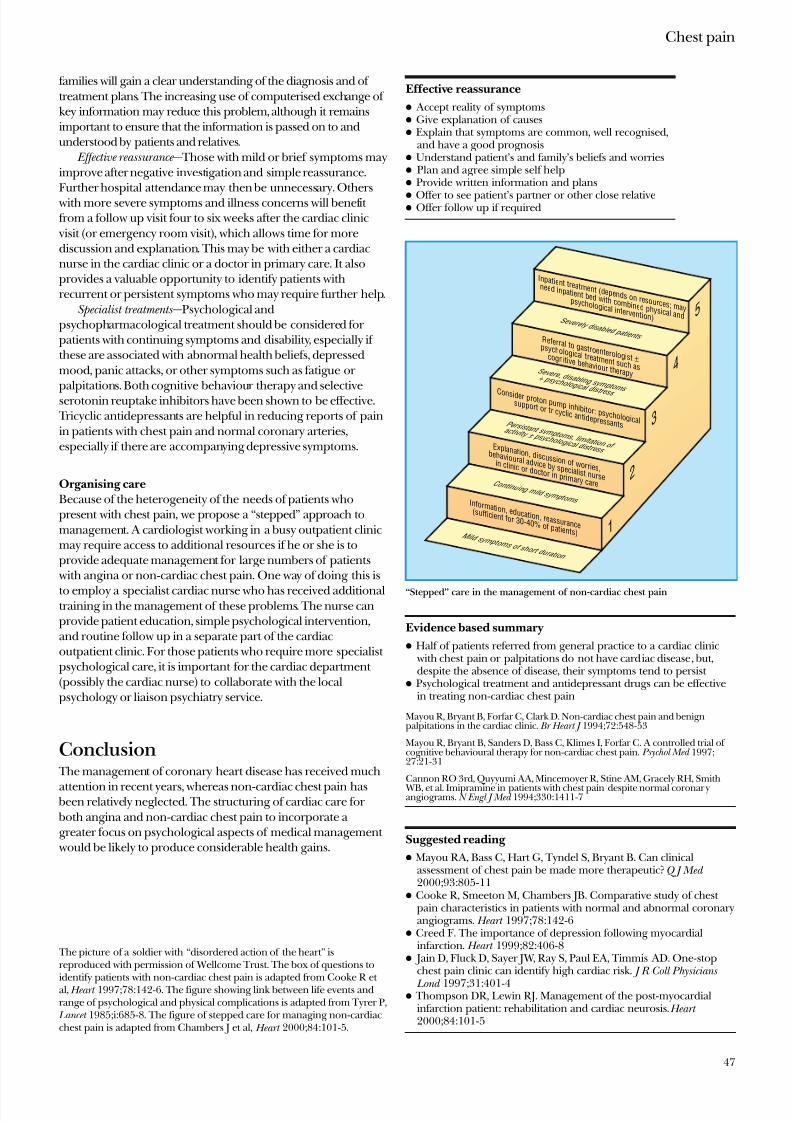
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 58/69
families will gain a clear understanding of the diagnosis and of treatment plans. The increasing use of computerised exchange of key information may reduce this problem, although it remainsimportant to ensure that the information is passed on to andunderstood by patients and relatives.
Effective reassurance — Those with mild or brief symptoms mayimprove after negative investigation and simple reassurance.Further hospital attendance may then be unnecessary. Others
with more severe symptoms and illness concerns will benefit from a follow up visit four to six weeks after the cardiac clinic
visit (or emergency room visit), which allows time for morediscussion and explanation. This may be with either a cardiacnurse in the cardiac clinic or a doctor in primary care. It alsoprovides a valuable opportunity to identify patients withrecurrent or persistent symptoms who may require further help.
Specialist treatments —Psychological andpsychopharmacological treatment should be considered for patients with continuing symptoms and disability, especially if these are associated with abnormal health beliefs, depressedmood, panic attacks, or other symptoms such as fatigue or palpitations. Both cognitive behaviour therapy and selectiveserotonin reuptake inhibitors have been shown to be effective.
Tricyclic antidepressants are helpful in reducing reports of painin patients with chest pain and normal coronary arteries,especially if there are accompanying depressive symptoms.
Organising care
Because of the heterogeneity of the needs of patients whopresent with chest pain, we propose a “stepped” approach tomanagement. A cardiologist working in a busy outpatient clinicmay require access to additional resources if he or she is toprovide adequate management for large numbers of patients
with angina or non-cardiac chest pain. One way of doing this is
to employ a specialist cardiac nurse who has received additionaltraining in the management of these problems. The nurse canprovide patient education, simple psychological intervention,and routine follow up in a separate part of the cardiacoutpatient clinic. For those patients who require more specialist psychological care, it is important for the cardiac department (possibly the cardiac nurse) to collaborate with the localpsychology or liaison psychiatry service.
Conclusion The management of coronary heart disease has received much
attention in recent years, whereas non-cardiac chest pain has been relatively neglected. The structuring of cardiac care for both angina and non-cardiac chest pain to incorporate a greater focus on psychological aspects of medical management
would be likely to produce considerable health gains.
The picture of a soldier with “disordered action of the heart” isreproduced with permission of Wellcome Trust. The box of questions to
identify patients with non-cardiac chest pain is adapted from Cooke R et al, Heart 1997;78:142-6. The figure showing link between life events andrange of psychological and physical complications is adapted from Tyrer P,
Lancet 1985;i:685-8. The figure of stepped care for managing non-cardiacchest pain is adapted from Chambers J et al, Heart 2000;84:101-5.
Effective reassurance
x Accept reality of symptomsx Give explanation of causesx Explain that symptoms are common, well recognised,
and have a good prognosisx Understand patient’s and family’s beliefs and worriesx Plan and agree simple self helpx Provide written information and plans
x Offer to see patient’s partner or other close relativex Offer follow up if required
Evidence based summary
x Half of patients referred from general practice to a cardiac clinic with chest pain or palpitations do not have cardiac disease, but,despite the absence of disease, their symptoms tend to persist
x Psychological treatment and antidepressant drugs can be effectivein treating non-cardiac chest pain
Mayou R, Bryant B, Forfar C, Clark D. Non-cardiac chest pain and benignpalpitations in the cardiac clinic. Br Heart J 1994;72:548-53
Mayou R, Bryant B, Sanders D, Bass C, Klimes I, Forfar C. A controlled trial of cognitive behavioural therapy for non-cardiac chest pain. Psychol Med 1997;27:21-31
Cannon RO 3rd, Quyyumi AA, Mincemoyer R, Stine AM, Gracely RH, Smith WB, et al. Imipramine in patients with chest pain despite normal coronar yangiograms. N Engl J Med 1994;330:1411-7
Suggested reading
x Mayou RA, Bass C, Hart G, Tyndel S, Bryant B. Can clinicalassessment of chest pain be made more therapeutic? Q J Med 2000;93:805-11
x Cooke R, Smeeton M, Chambers JB. Comparative study of chest pain characteristics in patients with normal and abnormal coronaryangiograms. Heart 1997;78:142-6
x Creed F. The importance of depression following myocardialinfarction. Heart 1999;82:406-8
x Jain D, Fluck D, Sayer JW, Ray S, Paul EA, Timmis AD. One-stopchest pain clinic can identify high cardiac risk. J R Coll Physicians
Lond 1997;31:401-4x Thompson DR, Lewin RJ. Management of the post-myocardial
infarction patient: rehabilitation and cardiac neurosis. Heart 2000;84:101-5
Inpatient treatment (depends on resources; may
need inpatient bed with combined physical and
psychological intervention)S e v e r e l y d i s a b l e d p a t i e n t s Referral to gastroenterologist ±
psychological treatment such as
cognitive behaviour therapyS e v e r e , d i s a b l i n g s y m p t o m s
+ p s y c h o l o g i c a l d i s t r e s s Consider proton pump inhibitor: psychological
support or tricyclic antidepressantsP e r s i s t a n t s y m p t o m s , l i m i t a t i o n o f
a c t i v i t y ± p s y c h o l o g i c a l d i s t r e s s Explanation, discussion of worries,
behavioural advice by specialist nurse
in clinic or doctor in primary careC o n t i n u i n g m i l d s y m p t o m s
M i l d s y m p t o m s o f s h o r t d u r a t i o n
Information, education, reassurance
(sufficient for 30-40% of patients)
5
4
3
2
1
“Stepped” care in the management of non-cardiac chest pain
Chest pain
47

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 59/69
14 Delirium Tom Brown, Michael Boyle
Delirium is a common cause of disturbed behaviour inmedically ill people and is often undetected and poorly
managed. It is a condition at the interface of medicine andpsychiatry that is all too often owned by neither. Although
various terms have been used to describe it —including acuteconfusional state, acute brain syndrome, and acute organicreaction—delirium is the term used in the current psychiatricdiagnostic classifications and the one we will use here.
Clinical featuresDelirium usually develops over hours to days. Typically, thesymptoms fluctuate and are worse at night. The fluctuation can
be a diagnostic trap, with nurses or relatives reporting that
patients had disturbed behaviour at night whereas doctors findpatients lucid the next day.Impaired cognitive functioning is central and affects
memory, orientation, attention, and planning skills. Impairedconsciousness, with a marked variability in alertness and inawareness of the environment is invariably present. A mistakenidea of the time of day, date, place, and identity of other people(disorientation) is common. Poor attention, and disturbedthought processes may be reflected in incoherent speech. Thiscan make assessment difficult and highlights the need to obtaina history from a third party. Relatives or other informants mayreport a rapid and drastic decline from premorbid functioning that is useful in distinguishing delirium from dementia.
Disturbed perception is common and includes illusions
(misperceptions) and hallucinations (false perceptions). Visualhallucinations are characteristic and strongly suggest delirium.However, hallucinations in auditory and other sensorymodalities can also occur.
Delusions are typically fleeting, often persecutory andusually related to the disorientation. For example, an elderlyperson may believe that the year is 1944, that he or she is in a prisoner of war camp, and that the medical staff are the enemy.Such delusions can be the basis of aggressive behaviour,
Delirium can have a profound effect on affect and mood. Apatient’s affect can range from apathy and lack of interest toanxiety, perplexity, and fearfulness that may sometimes amount to terror. A casual assessment can result in an erroneous
diagnosis of depression or anxiety disorder.Disturbances of the sleep-wake cycle and activity arecommon. A behaviourally disturbed patient with night timeagitation wandering around the ward is usually easy torecognise. However, presentations where a patient is hypo-alert and lethargic may go unrecognised.
Detection of deliriumDelirium often goes undiagnosed. Non-detection rates as highas 66% have been reported. Detection and diagnosis areimportant because of the associated morbidity and mortality:although most patients with delirium recover, some progress to
stupor, coma, seizures, or death. Patients may die because of failure to treat the associated medical condition or from theassociated behaviour —inactivity may cause pneumonia anddecubital ulcers, and wandering may lead to fractures from falls.
Diagnostic criteria for delirium*
x Disturbance in consciousness with reduced ability to focus, sustain,or shift attention
x Change in cognition (such as memory, disorientation, speech,disturbance) or development of perceptual disturbance not better accounted for by pre-existing or evolving dementia
x Disturbance develops over hours to days and fluctuates in severity
*Adapted from Diagnostic and Statistical Manual of Mental Disorders , 4th edition(DSM-IV)
Sensory misperceptions, including hallucinations and illusions, are commonin delirium. (Don Quixote and the Windmill by Gustave Doré, 1832-1883)
Alcohol addiction often goes undetected at the time of admission to hospital.All admitted patients should be asked about their alcohol consumption
48
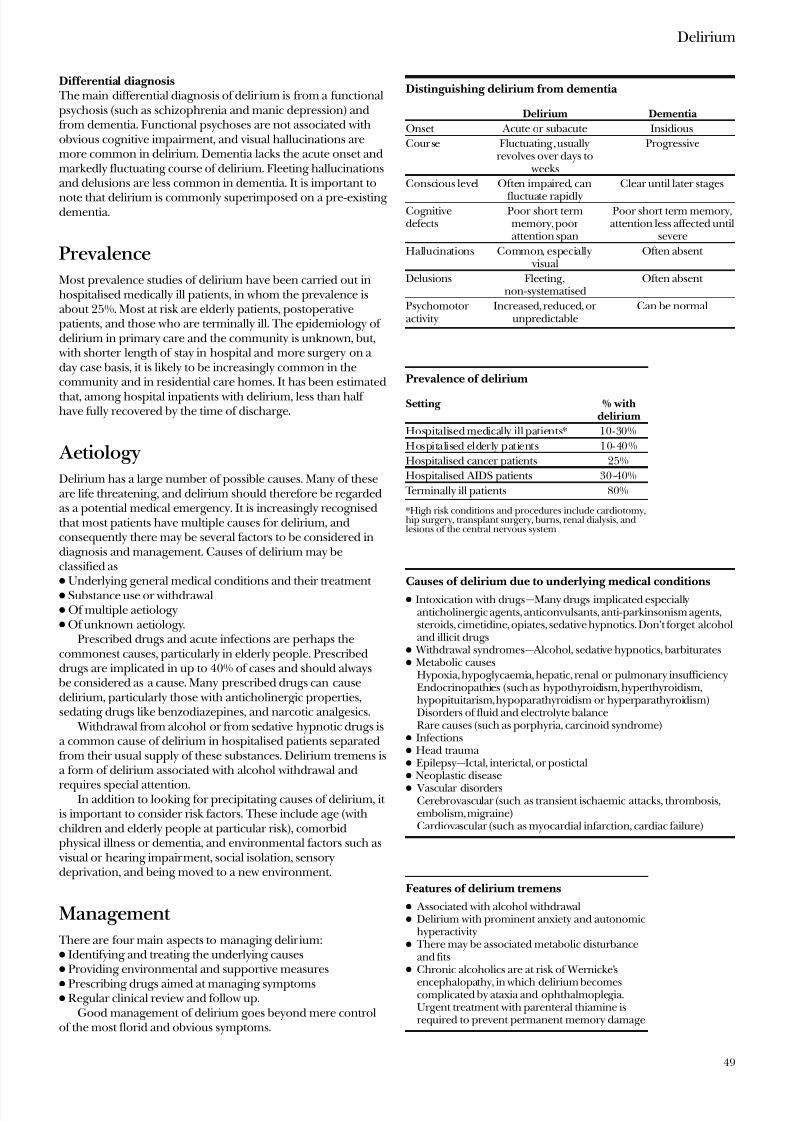
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 60/69
Differential diagnosis The main differential diagnosis of delir ium is from a functionalpsychosis (such as schizophrenia and manic depression) andfrom dementia. Functional psychoses are not associated withobvious cognitive impairment, and visual hallucinations aremore common in delirium. Dementia lacks the acute onset andmarkedly fluctuating course of delirium. Fleeting hallucinationsand delusions are less common in dementia. It is important to
note that delirium is commonly superimposed on a pre-existing dementia.
PrevalenceMost prevalence studies of delirium have been carried out inhospitalised medically ill patients, in whom the prevalence isabout 25%. Most at risk are elderly patients, postoperativepatients, and those who are terminally ill. The epidemiology of delirium in primary care and the community is unknown, but,
with shorter length of stay in hospital and more surgery on a day case basis, it is likely to be increasingly common in thecommunity and in residential care homes. It has been estimated
that, among hospital inpatients with delirium, less than half have fully recovered by the time of discharge.
AetiologyDelirium has a large number of possible causes. Many of theseare life threatening, and delirium should therefore be regardedas a potential medical emergency. It is increasingly recognisedthat most patients have multiple causes for delirium, andconsequently there may be several factors to be considered indiagnosis and management. Causes of delirium may beclassified asx Underlying general medical conditions and their treatment x Substance use or withdrawalx Of multiple aetiologyx Of unknown aetiology.
Prescribed drugs and acute infections are perhaps thecommonest causes, particularly in elderly people. Prescribeddrugs are implicated in up to 40% of cases and should always
be considered as a cause. Many prescribed drugs can causedelirium, particularly those with anticholinergic properties,sedating drugs like benzodiazepines, and narcotic analgesics.
Withdrawal from alcohol or from sedative hypnotic drugs isa common cause of delirium in hospitalised patients separatedfrom their usual supply of these substances. Delirium tremens isa form of delirium associated with alcohol withdrawal and
requires special attention.In addition to looking for precipitating causes of delirium, it
is important to consider risk factors. These include age (withchildren and elderly people at particular risk), comorbidphysical illness or dementia, and environmental factors such as
visual or hearing impairment, social isolation, sensorydeprivation, and being moved to a new environment.
Management There are four main aspects to managing delir ium:x Identifying and treating the underlying causesx Providing environmental and supportive measures
x Prescribing drugs aimed at managing symptomsx Regular clinical review and follow up.
Good management of delirium goes beyond mere controlof the most florid and obvious symptoms.
Distinguishing delirium from dementia
Delirium Dementia
Onset Acute or subacute Insidious
Cour se Fluctuating , usuallyrevolves over days to
weeks
Progressive
Conscious level Often impaired, can
fluctuate rapidly
Clear until later stages
Cognitivedefects
Poor short termmemory, poor attention span
Poor short term memory,attention less affected until
severe
Hallucinations Common, especially visual
Often absent
Delusions Fleeting,non-systematised
Often absent
Psychomotor activity
Increased, reduced, or unpredictable
Can be normal
Prevalence of delirium
Setting % withdelirium
Hospitalised medically ill patients* 10-30%
Hospitalised elderly patients 10-40%
Hospitalised cancer patients 25%
Hospitalised AIDS patients 30-40%
Terminally ill patients 80%
*High risk conditions and procedures include cardiotomy,hip surgery, transplant surgery, burns, renal dialysis, andlesions of the central nervous system
Causes of delirium due to underlying medical conditions
x Intoxication with drugs—Many drugs implicated especiallyanticholinergic agents, anticonvulsants, anti-parkinsonism agents,steroids, cimetidine, opiates, sedative hypnotics. Don’t forget alcoholand illicit drugs
x Withdrawal syndromes— Alcohol, sedative hypnotics, barbituratesx Metabolic causes
Hypoxia, hypoglycaemia, hepatic, renal or pulmonary insufficiencyEndocrinopathies (such as hypothyroidism, hyperthyroidism,hypopituitarism, hypoparathyroidism or hyperparathyroidism)Disorders of fluid and electrolyte balanceRare causes (such as porphyria, carcinoid syndrome)
x Infectionsx Head trauma x Epilepsy—Ictal, interictal, or postictalx Neoplastic diseasex Vascular disorders
Cerebrovascular (such as transient ischaemic attacks, thrombosis,embolism, migraine)Cardiovascular (such as myocardial infarction, cardiac failure)
Features of delirium tremens
x Associated with alcohol withdrawalx Delirium with prominent anxiety and autonomic
hyperactivityx There may be associated metabolic disturbance
and fitsx Chronic alcoholics are at risk of Wernicke’s
encephalopathy, in which delirium becomescomplicated by ataxia and ophthalmoplegia.Urgent treatment with parenteral thiamine isrequired to prevent permanent memory damage
Delirium
49
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 61/69
Making the diagnosisMost patients with delirium are identified only because of marked behavioural disturbance. It would be preferable for allolder patients to be screened for risk factors at admission tohospital. These would include substance misuse (particularlyalcohol) and pre-existing cognitive impairment (assessed withthe Hodkinson mental test or similar). Although such screening questions are part of the admission form in many hospitals, in
our experience junior doctors seldom complete them. Oncepatients are admitted, minor episodes of confusion, behaviouraldisturbance, or increasing agitation should be taken seriouslyand investigated as appropriate. They should not be simplydismissed as “old age” or psychological reactions tohospitalisation.
Identifying and treating the causeDelirium, by definition, is secondary to one or more underlying cause. Identifying such causes is often difficult, especially whenpatients are unable to give a coherent history or cooperate withphysical examination. On occasions, it can be necessary tosedate a patient before conducting an adequate assessment. The
interviewing of third parties is often helpful. Once a cause isfound, appropriate treatment should be started without delay.
The environment The aims of environmental interventions are, firstly, to createan environment that places minimum demands on a patient’simpaired cognitive function and, secondly, to limit the risk of harm to the patient and others that may result from disturbed
behaviour. Nursing should, as far as possible, be done by thesame member of staff (preferably one trusted by the patient).
This consistency should be supported with other strategiessuch as clear and if necessary repeated communication,adequate lighting, and the provision of clocks as aids tomaintaining orientation. Visits from family and friends andprovision of familiar objects from home can also be helpful.
The correction of sensory impairments (such as by providing glasses or hearing aids) to help patients’ grip on reality issometimes overlooked.
It is also be important to minimise any risk to a deliriouspatient, other patients on the ward, and staff by ensuring that the patient is in a safe and separate area and that potentiallydangerous objects are removed.
Drug treatment Drug treatment of delirium should only be used when essentialand then with care. This is because drugs such as antipsychoticsand benzodiazepines can make the delirium worse and can
exacerbate underlying causes (for example, benzodiazepinesmay worsen respiratory failure).
Antipsychotic drugs
Antipsychotics are the most commonly used drugs. Their onset of action is usually rapid, with improvement seen in hours todays. Haloperidol is often used because it has fewanticholinergic side effects, minimal cardiovascular side effects,and no active metabolites. As it is a high potency drug it is lesssedating than phenothiazines and therefore less likely toexacerbate delirium. It is, however, prone to causing parkinsonism, which may exacerbate a patient’s tendency to fall.Low dose haloperidol (1-10 mg/day) is adequate for most patients. In severe behavioural disturbance haloperidol may be
given intramuscularly or intravenously.It is preferable to use a fixed dose that is frequently reviewed
from the time of diagnosis rather than always giving the drug “as required” in response to disturbed behaviour. It is essential,
Hodkinson mental test
Score one point for each question answeredcorrectly and give total score out of 10
Question
x Patient’s agex Time (to nearest hour)x Address given, for recall at end of test (42 West
Street)x Name of hospital (or area of town if at home)x Current year x Patient’s date of birthx Current monthx Years of the first world war x Name of monarch (or president)x Count backwards from 20 to 1 (no errors
allowed but may correct self)
Environmental and supportive measures in delirium
x Education of all who interact with patient (doctors, nurses, ancillaryand portering staff, friends, family)
x Reality orientation techniquesFirm clear communication—preferably by same member of staff
Use of clocks and calendarsx Creating an environment that optimises stimulation (adequate
lighting, reducing unnecessary noise, mobilising patient whenever possible)
x Correcting sensory impairments (providing hearing aids, glasses, etc)x Ensuring adequate warmth and nutritionx Making environment safe (removing objects with which patient
could harm self or others)
Simple measures to help orientation (such as glasses, hearing aids, andclocks) are effective in the management of delirium
In postoperative patients judicious use of oxygen can treat deliriumeffectively
ABC of Psychological Medicine
50
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 62/69
yet often forgotten, to monitor patients for both adequateresponse and unacceptable side effects. While a patient is inhospital this consists of at least a daily assessment of symptoms,level of sedation, and examination for extrapyramidal and other unwanted drug effects.
Preliminary experience with new antipsychotics suggest theymay also be effective in delirium, but their advantages remainunestablished.
Benzodiazepines Benzodiazepines are usually preferred when delirium isassociated with withdrawal from alcohol or sedatives. They mayalso be used as an alternative or adjuvant to antipsychotics when these are ineffective or cause unacceptable side effects.Intravenous or intramuscular lorazepam may be given up toonce every four hours. In patients with delirium due to hepaticinsufficiency, lorazepam is preferred to haloperidol. Excessivesedation or respiratory depression from benzodiazepines isreversible with flumazenil.
ReviewOne of the most consistent failings in the management of
delirium is lack of review. The acute symptoms are usually dealt with “out of hours” by junior staff and are forgotten by the next day. It is essential to review management of delirium and of theunderlying causes for the duration of the hospital stay.
Patients’ capacity and consent Increasingly issues of capacity and informed consent may beraised in relation to the treatment of delirium. Urgent interventions needed to prevent serious deterioration or deathor necessary in the interests of a patient’s safety are deemed to be covered by common law in the United Kingdom. Althoughopinions differ, most agree that (a ) if medical colleagues woulddeem a treatment appropriate and (b) if reasonable people
would want the treatment themselves, then it can be given if urgently necessary.
Explaining the diagnosisEffective management requires that not only the doctors andnurses caring for a patient understand the condition, but that the patient’s family and friends appreciate the reasons for thedramatic change in the person’s behaviour and that it is usuallya reversible condition.
AftercareMany patients with delirium still have residual symptoms at thetime of discharge from hospital. There is therefore a need for continued vigilance about medication, environmental change,
and sensory problems during discharge planning and aftercare.Close liaison between hospital and primary care is an essentialpart of discharge planning.
Patients or their families will often need reassurance that anepisode of delirium is not the start of an inevitable progressionto dementia and that a full recovery can usually be expected.Delirious patients may erroneously be placed in long term careas “demented”: decisions to place patients in care should bemade only after an adequate assessment that differentiatesdelirium from dementia.
Key medicolegal judgments about patients’ capacity andconsent (English Law)
Re c (mental patients: refusal of treatment) [1994] 1 WLR 290 An adult has the capacity to consent to or refuse treatment if he or she canx Understand and retain the information relevant to the decision in
questionx Believe that informationx Weigh the information in the balance to arrive at an informed choice
Re f (mental health sterilisation) v West Berkshire HealthAuthority (1989) 2 WLR 1025: (1989) All ER 673“not only (1) must there be a necessity to act when it is not practicableto communicate with the assisted person but also (2) the action takenmust be such as a reasonable person would in all circumstances take,acting in the best interests of the assisted person.”“Action properly taken to preserve life, health or wellbeing of theassisted person (which) may well transcend such measures as surgicaloperations or substantial treatment and may extend to include suchhumdrum matters as routine medical or dental treatment, even suchsimple care as dressing and undressing and putting to bed.”
Evidence based summary
x A quarter of hospitalised elderly patients will have deliriumx Occurrence of delirium predicts poorer outcome and greater
length of stay even after controlling for other variables, including severity of illness
x Positive identification and management of risk factors can reduceincidence and severity of delirium in elderly patients
Francis J, Martin D, Kapoor WN. A prospective study of delirium in hospitalized
elderly. JAMA 1990;263:1097-101O’Keeffe S,.Lavan J. The prognostic significance of delirium in older hospitalpatients. J Am Geriatr Soc 1997;45:174-8
Cole MG, Primeau FJ, Elie LM. Delirium: prevention, treatment, and outcomestudies. J Geriatr Psychiatry Neurol 1998;11:126-37
Further reading
x American Psychiatric Association. Practice guideline for the treatment of patients with delirium . Washington, DC: APA, 1999
x Meagher DS. Delirium—optimising management. BMJ 2001;322:144-9
x Meagher DS, O’Hanlon D, O’Mahony E, Casey PR. The use of
environmental strategies and psychotropic medication in themanagement of delirium. Br J Psychiatry 1996;168:512-5
x Taylor D, Lewis S. Delirium. J Neurol Neurosurg Psychiatry1993;56:742-51
The picture of alcohol consumption is reproduced with permission of J Sutton and Rex Features. The picture of a patient receiving oxygen isreproduced with permission of Antonia Reeve and the Science PhotoLibrary. The picture of pills is reproduced with permission of AJHD/DHD Photo Gallery
Excessive use of sedative drugs often causes moreproblems that it solves
Delirium
51

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 63/69
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 64/69
53
blockers 16
Back Book, The 37
back pain 37biopsychosocial model 37clinical course 12
management of acute 37–9management of chronic 39–40
Beck depression inventory (BDI) 11behavioural therapies
anxiety disorders 16functional bowel disorders 43
hypochondriasis 20see also cognitive behaviour therapy
behaviour change, motivation 3beliefs 2, 4
back pain 38and chest pain 45, 46identifying unhelpful 35of relatives 5
benzodiazepines 16, 50, 51biopsychosocial models
functional gastrointestinal disorders 41
low back pain 37bipolar disorder 10brain metastases 25brief psychological therapies 16bronchodilators 15
buspirone 16
calcium channel blockers 15
cancer 25challenges of patient 25
distress 25 , 26–7psychological assessment and care 26–8psychological consequences 25–6recurrence 26risk of psychiatric illness 26
support organisations 27
treatments 26capacity, patient 51cardiac disease
and depression 10, 45functional symptoms 20, 45
cardiac nurse 47cardiac rehabilitation 20, 45
chemotherapy 26chest pain 20, 44
assessment and early management 44causes of non-cardiac 20, 45, 46
establishing a diagnosis 45–6treatment of non-cardiac 46–7types 45
chronic back pain 39–40
abdominal painexplanation of causes 42see also functional gastrointestinal disorders
abnormal illness behaviour see functional somaticsymptoms/syndromes
abuse, women 41active listening 1, 2
activity levelsin fatigue 35, 36
importance of 6, 16acute back pain 37–9acute stress disorder 29
adjustment disorders 10, 11alcoholism 48
alcohol withdrawal 42alprazolam 16
anger 3angina 45
assessment 44diagnostic uncertainty 45treatment 46–7
angiography 46, 46
anticonvulsants 15 antidepressants 12, 19
in cancer patient 27causing anxiety 15
for chest pain 47comparative studies 12for fatigue 35for functional gastrointestinal disorders 42
antimicrobials 15
antipsychotics 16 , 50–51anxiety 10
cancer patient 25, 26, 27characteristics of abnormal 14classification 14detection and assessment 15drugs causing 15medical conditions causing or mimicking 15
non-cardiac chest pain 46symptoms and signs 3, 14, 18treatment 15–16unpleasant procedures 16
anxious adjustment disorder 14 Aretaeus of Cappadocia 10
assault 29 , 31
assessment, as treatment 5–6attitudes 4, 5avoidance
in back pain 37 , 39in fatigue 35following trauma 31of threat 16
Index
Page numbers in bold refer to figures in the text; those in italics refer to tables or boxed material

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 65/69
Index
54
“chronic complainers” 21chronic fatigue syndromes 34chronic illness
care delivery skills 8changes in organisation of care 8–9effective management principles 7–8
chronic multiple functional symptomscommon management problems
23–4defined 21epidemiology and detection 21example of patient history 23 primary care management 21–2psychiatric referral 22–3see also factitious disorders
chronic painaetiological factors 18 following trauma 30lower back 39–40syndromes 39
clinical flags system in back pain 38cognitive assessment 50
cognitive behavioural approachback pain 39post-traumatic stress disorder 30
cognitive behaviour therapy anxiety disorders 16chest pain 47defined 35 depression 13fatigue 36functional bowel disorders 43 in functional syndromes 20
cognitive function 48, 49–50 collaborative management
chronic multiple functional symptoms 23depression 13musculoskeletal pain 38
collaborative self careback pain 37–8, 39 chronic illness 8–9
communication 1–3, 5, 38anxious patient 15–16between doctors 4 chest pain 46–7effective 5non-verbal 1
written 4 , 5community mental health services 13compensation claims 31consent, informed 51consultation 1–3
disease centred v patient centred 4 positive 6three function model 1
correspondence 4 , 5corticosteroids 15crime victim 29 , 30, 31critical incident debriefing 30cues, patients’ 1Cullen, William 14
Darwin, Charles 21debriefing, critical incident 30delirium
aetiology 49
in cancer 25clinical features 48detection and diagnosis 48–9, 50differential diagnosis 49management 49–51prevalence 49
delirium tremens 49delusions 48, 49
dementia 25, 49denial 2depression
in cancer 25, 26, 27classification 10clinical features 10drug treatment 12epidemiology 10and fatigue 35following trauma 30mental health services 13and myocardial infarction 10, 45non-cardiac chest pain 46physical symptoms 3, 11, 18psychological treatment 13recognition and diagnosis 11risk factors 11
Descartes, René 17
diabetes management 8 diagnosis, consultation 4digitalis 15 disaster plan 32disasters, debriefing 30disease registry 8disorientation 48distress
back pain 39
cancer 25 , 26–7functional gastrointestinal disorders 41linking to somatic symptoms 3
doctor-patient communication 1–3, 5, 38doctor-patient relationship 22
see also reassurancedomestic trauma 31
Don Quixote and the Windmill 48dopamine 15 Doré, Gustave 48
drugscausing anxiety 15causing delirium 49causing depression 10dependence 12, 16
withdrawal 16, 49see also named drugs and drug groups
dual focus 1dualism 17, 20dysthymia 10
emergency department 29emotional distress see distressemotions
detecting and responding to 1, 2–3linking to physical symptoms 3
exercise programme 36
expectations, and experience 4 expert patient programme 4, 7 explanations to patient
chronic multiple functional symptoms 22
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 66/69
Index
55
functional gastrointestinal disorders 42functional somatic symptoms 19
explanatory model, patient 2
factitious disorders 24family
cancer patient 27chronically ill patient 7delirious patient 51“thinking family” 2, 5trauma victim 31
“fat folder patient” 21fatigue 10
assessment 34causes 33–4general management 34–5medical conditions associated with 33prevalence 33specialist management 35–6
fear 3, 25fibromyalgia 34“flags”, clinical system in back pain 38
flumazenil 51follow up
in chronic illness 8 value of 6
functional gastrointestinal disordersbiopsychosocial model 41classification 41
explaining symptoms 42initial management 41–2management of chronic 42–3patient organisations 42psychological referral 43
functional somatic symptoms/syndromes
causal factors 18classification 17detection and diagnosis 18–19epidemiology 17management 19–20in medical disease 20see also chronic multiple functional symptoms
gastro-oesophageal reflux 46general health questionnaire 15
generalised anxiety disorder 14Gillray, James 29graded exercise therapy 36
hallucinations 48,49
haloperidol 16 , 50head injury 31health anxiety 16health beliefs see beliefsHippocrates 2Hodkinson mental test 50
hospital anxiety and depression scale (HADS)11, 15
hypnosis 51
hypocapnia 15
hypochondriasis 20hypoxia 15
iatrogenic factorsanxiety 15chest pain 45 , 46functional somatic symptoms 18, 21, 24
IBS Network 42imipramine 16
information, patient 1, 2, 4, 5, 15, 27informed consent 51injuries
compensation 31head 31see also trauma
inotropes 15 insulin 15
interdisciplinary pain management programme 39International Federation for Functional
Gastrointestinal Disorders 42interpersonal difficulties 24interpersonal therapy 16, 43
interview chronic multiple functional symptoms 22, 23style and techniques 1–2, 5
investigations see testsirritable bowel syndrome
diagnostic criteria 41
initial management 41–2
management of chronic 42–3patient organisations 42psychiatric referral 43
“irritable heart” 44
letters, primary/secondary care 4 , 5levodopa 15
liaison psychiatry services 13life events 46listening skills 1, 2
lorazepam 51
major depressive disorder 10
major incidents 29–30malingering 24management plan 2manic depressive (bipolar) disorder 10medical conditions
causing or mimicking anxiety 15
presenting with fatigue 33medical syndromes 17medicolegal judgments 51
ME (myalgic encephalomyelitis) 34mental assessment 43mental health services 13, 15metastases, brain 25mind-body dualism 17, 20motivation, for change 3multiple functional somatic symptoms see chronic multiple
functional symptomsMünchausen’s syndrome 24
musculoskeletal paincauses and prevalence 37management of acute 37–9management of chronic 39–40
myalgic encephalomyelitis (ME) 34myocardial infarction
and depression 10, 45non-cardiac chest pain 45rehabilitation programme 45
National Electronic Library of Health 5neuropsychiatric syndromes 25neurotic symptoms, epidemiology 10
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 67/69
Index
56
NHS Direct, online 5non-cardiac chest pain 20, 45
causes 45, 46establishing a diagnosis 45–6treatment 46–7
non-steroidal anti-inflammatory drugs 15 non-verbal cues 1nursing staff 5–6
occupational stresses 35occupational trauma 31oesophageal disorders 46oestrogen 15 organisation of care
chest pain 47chronic illness 8–9
paindistress and anger 39see also chronic pain
pain control 15
pain management programmes 39 panic disorder 10
detection 15features 14prevalence in medical settings 46 screening questions 46 treatment 15–16
paraneoplastic syndromes 25parkinsonism 50paroxetine 16 participatory management 2, 4, 7–8, 9patient
cues 1
expectations and experience 4 , 23explanatory model of problem 2participation in care 2, 4, 7–8, 9providing information 1, 2, 4, 5, 15, 27
patient centred consultation 4 patient information materials 5patient organisations
cancer 27 functional gastrointestinal disorders 42
personal injury claims 31phobia 10, 14phobic anxiety 30–1physiotherapists 30post-combat syndromes 19, 44postoperative patient 50post-traumatic stress disorder 30primary care team
depression management 13management of chronic illness 8–9stepped care approach 8, 47
problem solving 13 proton pump inhibitors 46psychiatric referral
cancer patient 28chronic multiple functional symptoms
22–3fatigue syndromes 35
functional bowel disorders 43psychiatric syndromes 17psychological therapies
brief 6 , 16
for functional bowel disorders 43see also named therapies
questionnairesanxiety 15 cancer patient 27depression 11panic attacks 46
questions 1, 2 , 15
Radford, Edward 31
radiotherapy 26reassurance 2, 5–6
anxiety 15–16chest pain 47chronic multiple functional symptoms 22complexity of 5 functional somatic symptoms 19
referrals see psychiatric referral; specialist referralreflux, gastro-oesophageal 46relationships, personal 16, 24relatives see family Resignation 26road traffic accident 29 , 30, 31Royal College of Psychiatrists 12
screening instrumentsanxiety 15depression 11
selective serotonin reuptake inhibitors(SSRIs) 12, 16 , 47
self care, collaborativeback pain 37–8, 39 chronic illness 8–9
self-report questionnaires
anxiety 15 cancer patient 27depression 11
shellshock 19
sleepiness 34sleep problems 10, 33 , 48sleep-wake cycle 48social support 27soldiers 19, 44somatic symptoms
anxiety disorders 14 cognitive model 6linking to emotional distress 3see also chronic multiple functional symptoms; functional
somatic symptoms/syndromessomatoform disorder 17specialist referral
cancer patient 27–8functional symptoms and syndromes 20letters 4see also psychiatric referral
squamous cell carcinoma 25
SSRIs (selective serotonin reuptake inhibitors) 12, 16 , 47state-trait anxiety inventory 15 stepped care 7, 8, 47stress 34 , 35, 46stroke 11
suicide risk 12, 25support organisations
cancer 27 functional gastrointestinal disorders 42
8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 68/69
Index
57
terminal disease 26tests
explaining negative 6psychological impact 6, 46unpleasant 16
“thinking family” 2, 5thyroxine 15 trauma
acute management 29–30consequences and care of patient 30–1family and carers 31head 31lifetime prevalence of events 29 personal injury and compensation 31types 29, 31
treadmill exercise test 46 treatment
anxiety about 26
communication with patient 4, 5compliance 16future planning 6principles 4–5
tricyclic antidepressants 12, 16 , 47
verbal cues 1Very Slippy Weather 29
Victim Support 30
war, functional symptoms/syndromes 19, 44Weary 33
Wilhelmson, Carl Wilhelm 26
withdrawal syndromes 16, 49 women 10, 21, 24, 33, 41 work stresses 35 World Health Organization 10, 17

8/21/2019 ABC_of_Psychological_Medicine.pdf
http://slidepdf.com/reader/full/abcofpsychologicalmedicinepdf 69/69


















