ABC of Psychological Medicine - R. Mayou, M. Sharpe, A. Carson (Eds) (BMJ, 2003) WW

ABC of burnsIntroductionShehan Hettiaratchy, Peter Dziewulski
Burns are one of the most devastating conditions encounteredin medicine. The injury represents an assault on all aspects ofthe patient, from the physical to the psychological. It affects allages, from babies to elderly people, and is a problem in boththe developed and developing world. All of us have experiencedthe severe pain that even a small burn can bring. However thepain and distress caused by a large burn are not limited to theimmediate event. The visible physical and the invisiblepsychological scars are long lasting and often lead to chronicdisability. Burn injuries represent a diverse and varied challengeto medical and paramedical staff. Correct management requiresa skilled multidisciplinary approach that addresses all theproblems facing a burn patient.
This series provides an overview of the most importantaspects of burn injuries for hospital and non-hospitalhealthcare workers.
How common are burns?In the United Kingdom about 250 000 people are burnt eachyear. Of these, 175 000 attend accident and emergencydepartments, and 13 000 of these are admitted to hospital.Some 1000 patients have severe enough burns to warrantformal fluid resuscitation; half of these are children aged under12 years. In an average year 300 burn deaths occur. These UKfigures are representative of most of the developed worldcountries, although some, such as the United States, have ahigher incidence.
Burns are also a major problem in the developing world.Over two million burn injuries are thought to occur each yearin India (population 500 million), but this may be a substantialunderestimate. Mortality in the developing world is muchhigher than in the developed world. For example, Nepal hasabout 1700 burn deaths a year for a population of 20 million,giving a death rate 17 times that of Britain.
What are the causes of burns?Most burns are due to flame injuries. Burns due to scalds arethe next most common. The most infrequent burns are thosecaused by electrocution and chemical injuries. The type ofburns suffered is related to the type of patient injured. It istherefore useful to break down burn aetiology by patientgroups as this reveals the varying causes of injury. In mostgroups there is a male predominance. The only exception is inelderly people, among whom more women are injured becauseof the preponderance of women in that population.
Who gets burnt?Young children—Children aged up to 4 years comprise 20% of
all patients with burn injuries. Most injuries (70%) are scaldsdue to children spilling hot liquids or being exposed to hotbathing water. These mechanisms can lead to large area burns.Because of changes in the design and material of nightclothing, flame burns are less common than they were. Boys aremore likely to be injured, a reflection of the behaviouraldifferences between boys and girls.
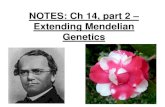
Top: Child with 70% fullthickness burns, whichrequired resuscitation,intensive care support,and extensivedebridement and skingrafting. Left: The samechild one year later at aburns camp, having madea good recovery. Areasonable outcome ispossible even with severeburn injuries
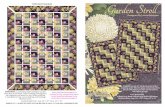
Incidence of burns by ageCauses of burns
20%
10%
10%
55%
Flame
1-4 years old
5-14yearsold
15-64 years old
>65 yearsold
Scalds
Chemical andelectrical
5%
40%
60%
Causes of burns (left) and incidence of burns by age (right)
Scald in young child caused byspilling hot liquid. Most of theburn is superficial, except for thepatch on the shoulder, whichrequired a skin graft and whichhealed well
This is the first in a series of 12 articles
Clinical review
1366 BMJ VOLUME 328 5 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Older children and adolescents—10% of burns happen tochildren between the ages of 5 and 14. Teenagers are ofteninjured from illicit activities involving accelerants, such as petrol,or electrocution.
Working age—Most burns ( > 60%) occur in patients aged15-64. These are mainly due to flame burns, and up to a thirdare due to work related incidents.
Elderly people—Some 10% of burns occur in people agedover 65. Various effects of ageing (such as immobility, slowedreactions, and decreased dexterity) mean elderly people are atrisk from scalds, contact burns, and flame burns.
Compromising factors—Burn victims’ health is oftencompromised by some other factor, such as alcoholism,epilepsy, or chronic psychiatric or medical illness. All suchproblems need to be addressed when managing patients inorder to speed recovery and prevent repetition of injury.
Care of a major burn injuryThe main aims of burn care are to restore form, function, andfeeling, and burn management can be divided up into sevenphases—rescue, resuscitate, retrieve, resurface, rehabilitate,reconstruct, and review.
Rescue—The aim is to get the individual away from thesource of the injury and provide first aid. This is often done bynon-professionals—friends, relatives, bystanders, etc.
Resuscitate—Immediate support must be provided for anyfailing organ system. This usually involves administering fluid tomaintain the circulatory system but may also involve supportingthe cardiac, renal, and respiratory systems.
Retrieve—After initial evacuation to an accident andemergency department, patients with serious burns may needtransfer to a specialist burns unit for further care.
Resurface—The skin and tissues that have been damaged bythe burn must be repaired. This can be achieved by variousmeans, from simple dressings to aggressive surgicaldebridement and skin grafting.
Rehabilitate—This begins on the day a patient enters hospitaland continues for years after he or she has left. The aim is toreturn patients, as far as is possible, to their pre-injury level ofphysical, emotional, and psychological wellbeing.
Reconstruct—The scarring that results from burns often leadsto functional impairment that must be addressed. Theoperations needed to do this are often complex and may needrepeating as a patient grows or the scars re-form.
Review—Burn patients, especially children, require regularreview for many years so that problems can be identified earlyand solutions provided.The complexity of the injury and the chronic nature of thesequelae of burns require an integrated multidisciplinaryapproach with long follow up. Only such management can leadto the best outcomes for burn patients.
Prognostication in major burnsDetermining whether someone will survive a severe burn injuryis not simple but is important. Aggressive treatment forsomeone with a non-survivable injury is inhumane, and it isinappropriate not to treat a patient who has a severe butpotentially survivable injury. Unfortunately, there is no exactway to predict who will survive a burn injury. Several formulaehave been devised to estimate the risk of death after burn injury.None has been evaluated prospectively in large trials, however,and so they should be used only for audit purposes. It is alsoinappropriate to apply generic formulae to individuals. Eachpatient should be considered individually.
Burn incurred by an adolescent boy while inhaling butane gas.There was full thickness damage to the lower lip, which requireddebridement and extensive reconstruction
Aims of burn care
Restore form—Return the damaged area to as closeto normality as is possible
Restore function—Maximise patient’s ability toperform pre-injury activities
Restore feeling—Enable psychological and emotionalrecovery
Bitumen burns to face in work related incident
Contact burns in an elderly patient after a collapse andprolonged contact with a radiator. Treatment required excisionand split skin grafting as well as investigation into the cause ofthe collapse
Clinical review
1367BMJ VOLUME 328 5 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Certain factors increase the risk of death. The mostimportant are increasing age, increasing burn size, and thepresence of an inhalational injury. Exactly how these factorsinterrelate is not clear. Evidence suggests that a patientaged over 60 with a burn covering more than 40% of bodysurface area and an inhalational injury has a > 90% chance ofdying.
As well as assessing the injury, it is also important to makesome estimation of the patient’s quality of life before the burn.This can be obtained from relatives, carers, or the patient.Deciding not to resuscitate a patient is difficult. It is often usefulto get a consensus opinion from the whole burn team.
Burn prevention and fire safetyThe fact that 90% of burn injuries are preventable has led tomany attempts to decrease their incidence. These attempts fallinto two main categories—education and legislation. Educationis an “active” process that requires a change in an individual’sbehaviour. Legislation is “passive” and is independent of aperson’s actions. Both have advantages and disadvantages.
Education—The most successful campaigns have targetedspecific burn aetiologies or populations. A good example of thisis the campaign to reduce chip pan fires in Britain during thelate 1970s. This led to a 30% reduction in the incidence ofburns due to chip pan fires. The main problem with educationalprevention is that it relies on changing the way individualsbehave. This means the message must be repeated regularly, asshown by the UK government launching a second chip pan firecampaign in 1999. However, a successful educational campaignhas an instantaneous and widespread impact.
Legislation—Legislation (such as the compulsory fitting ofsprinklers in commercial buildings) has led to substantialdecreases in burn injury. The main problem with legislation isthat it takes time to pass and to have an effect. Compliance mustalso be obtained and maintained. However, as it does not rely ona change in individuals’ actions, legislation can be effective.
Effective prevention requires both passive and activeelements. The basis for all prevention is good epidemiologicaldata to reveal specific causes of burns and at risk populations,both of which can be targeted. The UK government is currentlyrunning the “Fire kills” campaign, which covers all aspects ofdomestic fire prevention and safety. The related website,www.firekills.gov.uk, is an excellent source of information.
Some risk factors for burns are not easy to change.Overcrowding, poor housing, and the other attributes ofpoverty are major contributors to the risk of burn injuries.
Shehan Hettiaratchy is specialist registrar in plastic and reconstructivesurgery, Pan-Thames Training Scheme, London; Peter Dziewulski isconsultant burns and plastic surgeon, St Andrews Centre for PlasticSurgery and Burns, Broomfield Hospital, Chelmsford.
The ABC of burns is edited by Shehan Hettiaratchy; Remo Papini,consultant and clinical lead in burns, West Midlands Regional BurnsUnit, Selly Oak University Hospital, Birmingham; and PeterDziewulski. The series will be published as a book in the autumn.
Competing interests: RP has been reimbursed by Johnson & Johnson,manufacturer of Integra, and Smith & Nephew, manufacturer of Acticoatand TransCyte, for attending symposiums on burn care.
Death
Increasingage
Increasingburn size
Inhalationalinjury Factors that increase the risk
of death after a major burn
FIREKILLS
YOU CANPREVENT IT
UK government’s “Fire kills”campaign started in 2002
Information in UK government’s “Fire kills” campaign
“Top 10 safety tips”
How to make your house a safe homex Fit a smoke alarm and check it regularlyx Make a fire action plan so that everyone in your house knows how
to escape in the event of firex Take care when cooking with hot oil and think about using
thermostatically controlled deep fat fryersx Never leave lit candles unattendedx Ensure cigarettes are stubbed out and disposed of carefullyx Never smoke in bedx Keep matches and lighters away from childrenx Keep clothing away from heating appliancesx Take care in the kitchen. Accidents while cooking account for 59%
of fires in the homex Take special care when you are tired or when you’ve been drinking.
Half of all deaths in domestic fires occur between 10 pm and 8 am
On finding a fire in the homex Get out x Stay out x Call 999 (telephone number
for UK emergency services)
Key points
x Burns are a major cause of injury and death worldwidex Flame burns are the most common typex Young children, elderly people, and those who are mentally or
physically compromised are at particular riskx Death is more likely with increasing age, increasing burn size, and
presence of inhalational injuryx 90% of burns are preventable
BMJ 2004;328:1366–8
Further reading
x Wilkinson E. The epidemiology of burns in secondary care, in apopulation of 2.6 million people. Burns 1998;24:139-43
x Ryan CM, Schoenfeld DA, Thorpe WP, Sheridan RL, Cassem EH,Tompkins RG. Objective estimates of the probability of death fromburn injuries. N Engl J Med 1998;338:362-6
x Fire kills. You can prevent it. www.firekills.gov.ukx Herndon D. Total burn care. 2nd ed. London: WB Saunders, 2002x National Community Fire Safety Centre Toolbox.
www.firesafetytoolbox.org.ukx Liao C-C, Rossignol AM. Landmarks in burn prevention. Burns
2000;26:422-34
Clinical review
1368 BMJ VOLUME 328 5 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsPathophysiology and types of burnsShehan Hettiaratchy, Peter Dziewulski
Understanding the pathophysiology of a burn injury isimportant for effective management. In addition, differentcauses lead to different injury patterns, which require differentmanagement. It is therefore important to understand how aburn was caused and what kind of physiological response it willinduce.
The body’s response to a burnBurn injuries result in both local and systemic responses.
Local responseThe three zones of a burn were described by Jackson in 1947.
Zone of coagulation—This occurs at the point of maximumdamage. In this zone there is irreversible tissue loss due tocoagulation of the constituent proteins.
Zone of stasis—The surrounding zone of stasis ischaracterised by decreased tissue perfusion. The tissue in thiszone is potentially salvageable. The main aim of burnsresuscitation is to increase tissue perfusion here and preventany damage becoming irreversible. Additional insults—such asprolonged hypotension, infection, or oedema—can convert thiszone into an area of complete tissue loss.
Zone of hyperaemia—In this outermost zone tissue perfusion isincreased. The tissue here will invariably recover unless there issevere sepsis or prolonged hypoperfusion.
These three zones of a burn are three dimensional, and lossof tissue in the zone of stasis will lead to the wound deepeningas well as widening.
Systemic responseThe release of cytokines and other inflammatory mediators atthe site of injury has a systemic effect once the burn reaches30% of total body surface area.
Cardiovascular changes—Capillary permeability is increased,leading to loss of intravascular proteins and fluids into theinterstitial compartment. Peripheral and splanchnicvasoconstriction occurs. Myocardial contractility is decreased,possibly due to release of tumour necrosis factor �. Thesechanges, coupled with fluid loss from the burn wound, result insystemic hypotension and end organ hypoperfusion.
Respiratory changes—Inflammatory mediators causebronchoconstriction, and in severe burns adult respiratorydistress syndrome can occur.
Metabolic changes—The basal metabolic rate increases up tothree times its original rate. This, coupled with splanchnichypoperfusion, necessitates early and aggressive enteral feedingto decrease catabolism and maintain gut integrity.
Immunological changes—Non-specific down regulation of theimmune response occurs, affecting both cell mediated andhumoral pathways.
Mechanisms of injuryThermal injuries
Scalds—About 70% of burns in children are caused by scalds.They also often occur in elderly people. The commonmechanisms are spilling hot drinks or liquids or being exposed
Clinical image of burn zones. There is central necrosis,surrounded by the zones of stasis and of hyperaemia
Zone ofcoagulation
Zone ofcoagulation
Epidermis
Dermis
Zone ofstasis
Zone ofhyperaemia
Inadequateresuscitation
Adequateresuscitation
Zone of stasis preserved Zone of stasis lost
Jackson’s burns zones and the effects of adequate and inadequateresuscitation
CardiovascularReduced myocardialcontractility
ImmunologicalReduced immune
response
Increased capillarypermeability
Peripheral and splanchnicvasoconstriction
RespiratoryBronchoconstriction
MetabolicBasal metabolic rateincreased threefold
Adult respiratorydistress syndrome
Systemic changes that occur after a burn injury
This is the second in a series of 12 articles
Clinical review
1427BMJ VOLUME 328 12 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

to hot bathing water. Scalds tend to cause superficial tosuperficial dermal burns (see later for burn depth).
Flame—Flame burns comprise 50% of adult burns. They areoften associated with inhalational injury and other concomitanttrauma. Flame burns tend to be deep dermal or full thickness.
Contact—In order to get a burn from direct contact, theobject touched must either have been extremely hot or thecontact was abnormally long. The latter is a more commonreason, and these types of burns are commonly seen in peoplewith epilepsy or those who misuse alcohol or drugs. They arealso seen in elderly people after a loss of consciousness; such apresentation requires a full investigation as to the cause of theblackout. Burns from brief contact with very hot substances areusually due to industrial accidents. Contact burns tend to bedeep dermal or full thickness.
Electrical injuriesSome 3-4% of burn unit admissions are caused by electrocutioninjuries. An electric current will travel through the body fromone point to another, creating “entry” and “exit” points. Thetissue between these two points can be damaged by the current.The amount of heat generated, and hence the level of tissuedamage, is equal to 0.24×(voltage)2×resistance. The voltage istherefore the main determinant of the degree of tissue damage,and it is logical to divide electrocution injuries into thosecaused by low voltage, domestic current and those due to highvoltage currents. High voltage injuries can be further dividedinto “true” high tension injuries, caused by high voltage currentpassing through the body, and “flash” injuries, caused bytangential exposure to a high voltage current arc where nocurrent actually flows through the body.
Domestic electricity—Low voltages tend to cause small, deepcontact burns at the exit and entry sites. The alternating natureof domestic current can interfere with the cardiac cycle, givingrise to arrhythmias.
“True” high tension injuries occur when the voltage is 1000 Vor greater. There is extensive tissue damage and often limb loss.There is usually a large amount of soft and bony tissue necrosis.Muscle damage gives rise to rhabdomyolysis, and renal failuremay occur with these injuries. This injury pattern needs moreaggressive resuscitation and debridement than other burns.Contact with voltage greater than 70 000 V is invariably fatal.
“Flash” injury can occur when there has been an arc ofcurrent from a high tension voltage source. The heat from thisarc can cause superficial flash burns to exposed body parts,typically the face and hands. However, clothing can also be setalight, giving rise to deeper burns. No current actually passesthrough the victim’s body.
A particular concern after an electrical injury is the need forcardiac monitoring. There is good evidence that if the patient’selectrocardiogram on admission is normal and there is nohistory of loss of consciousness, then cardiac monitoring is notrequired. If there are electrocardiographic abnormalities or aloss of consciousness, 24 hours of monitoring is advised.
Chemical injuriesChemical injuries are usually as a result of industrial accidentsbut may occur with household chemical products. These burnstend to be deep, as the corrosive agent continues to causecoagulative necrosis until completely removed. Alkalis tend topenetrate deeper and cause worse burns than acids. Cement is acommon cause of alkali burns.
Certain industrial agents may require specific treatments inaddition to standard first aid. Hydrofluoric acid, widely used forglass etching and in the manufacture of circuit boards, is one ofthe more common culprits. It causes a continuing, penetrating
Examples of a scald burn (left) and a contact burn from a hot iron (right) inyoung children
Flash injuryTrue high tension injury
Current arcs, causing flashNo current goes through patient
Current passesthrough patient
Differences between true high tension burn and flash burn
Electrocardiogram after electrocution showing atrialfibrillation
Chemical burn due to spillage of sulphuric acid
Clinical review
1428 BMJ VOLUME 328 12 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

injury and must be neutralised with calcium gluconate, eitherapplied topically in a gel or injected into the affected tissues.
The initial management of all chemical burns is the sameirrespective of the agent. All contaminated clothing must beremoved, and the area thoroughly irrigated. This is often bestachieved by showering the patient. This has been shown to limitthe depth of the burn. Litmus paper can be used to confirmremoval of alkali or acid. Eye injuries should be irrigatedcopiously and referred to an ophthalmologist.
Non{accidental injuryAn estimated 3-10% of paediatric burns are due tonon{accidental injury. Detecting these injuries is important asup to 30% of children who are repeatedly abused die. Usuallyyoung children ( < 3 years old) are affected. As with othernon{accidental injuries, the history and the pattern of injurymay arouse suspicion. A social history is also important. Abuseis more common in poor households with single or youngparents. Such abuse is not limited to children: elderly and otherdependent adults are also at risk. A similar assessment can bemade in these scenarios.
It is natural for non{accidental injury to trigger angeramong healthcare workers. However, it is important that allmembers of the team remain non-confrontational and try toestablish a relationship with the perpetrators. The time aroundthe burn injury is an excellent opportunity to try to break thecycle of abuse. In addition, it is likely that the patient willeventually be discharged back into the care of the individualswho caused the injury. As well as treating the physical injury, theburn team must try to prevent further abuse by changing therelationship dynamics between victim and abuser(s).
Any suspicion of non{accidental injury should lead toimmediate admission of the child to hospital, irrespective ofhow trivial the burn is, and the notification of social services.The team should carry out the following:x Examine for other signs of abusex Photograph all injuriesx Obtain a team opinion about parent-child interactionx Obtain other medical information (from general practitioner,health visitor, referring hospital)x Interview family members separately about the incident(check for inconsistencies) and together (observe interaction).
It should be remembered that the injury does not have to becaused deliberately for social services to intervene; inadequatesupervision of children mandates their involvement.
Shehan Hettiaratchy is specialist registrar in plastic and reconstructivesurgery, Pan-Thames Training Scheme, London; Peter Dziewulski isconsultant burns and plastic surgeon, St Andrews Centre for PlasticSurgery and Burns, Broomfield Hospital, Chelmsford.
The ABC of burns is edited by Shehan Hettiaratchy; Remo Papini,consultant and clinical lead in burns, West Midlands Regional BurnUnit, Selly Oak University Hospital, Birmingham; and PeterDziewulski. The series will be published as a book in the autumn.
Competing interests: See first article for series editors’ details.
Specific chemical burns and treatments
Chromic acid—Rinse with dilute sodium hyposulphiteDichromate salts—Rinse with dilute sodium
hyposulphiteHydrofluoric acid—10% calcium gluconate applied
topically as a gel or injected
Injury pattern of non{accidental burns
x Obvious pattern from cigarettes, lighters, ironsx Burns to soles, palms, genitalia, buttocks, perineumx Symmetrical burns of uniform depthx No splash marks in a scald injury. A child falling into a bath will
splash; one that is placed into it may notx Restraint injuries on upper limbsx Is there sparing of flexion creases—that is, was child in fetal position
(position of protection) when burnt? Does this correlate to a “tideline” of scald—that is, if child is put into a fetal position, do theburns line up?
x “Doughnut sign,” an area of spared skin surrounded by scald. If achild is forcibly held down in a bath of hot water, the part in contactwith the bottom of the bath will not burn, but the tissue around will
x Other signs of physical abuse—bruises of varied age, poorly kempt,lack of compliance with health care (such as no immunisations)
History of non-accidental burns
x Evasive or changing historyx Delayed presentationx No explanation or an implausible mechanism
given for the burnx Inconsistency between age of the burn and age
given by the historyx Inadequate supervision, such as child left in the
care of inappropriate person (older sibling)x Lack of guilt about the incidentx Lack of concern about treatment or prognosis
“Doughnut sign” in a child with immersion scalds. Anarea of spared skin is surrounded by burnt tissue. Thetissue has been spared as it was in direct contact withthe bath and protected from the water. This burnpattern suggests non{accidental injury
Key points
x A burn results in three distinct zones—coagulation, stasis, andhyperaemia
x The aim of burns resuscitation is to maintain perfusion of the zoneof stasis
x Systemic response occurs once a burn is greater than 30% of totalbody surface area
x Different burn mechanisms lead to different injury patternsx Identification of non{accidental burn injury is important
BMJ 2004;328:1427–9
Further reading
x Kao CC, Garner WL. Acute burns. Plast Reconstr Surg 2000;105:2482{93
x Andronicus M, Oates RK, Peat J, Spalding S, Martin H.Non-accidental burns in children. Burns 1998;24:552-8
x Herndon D. Total burn care. 2nd ed. London: WB Saunders, 2002x Luce EA. Electrical burns. Clin Plast Surg 2000;27:133-43x Kirkpatrick JJR, Enion DS, Burd DAR. Hydrofluoric acid burns; a
review. Burns 1995;21:483-93x Burnsurgery.org. www.burnsurgery.org
Clinical review
1429BMJ VOLUME 328 12 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsFirst aid and treatment of minor burnsJackie Hudspith, Sukh Rayatt
Some 250 000 burns occur annually in the United Kingdom.About 90% of these are minor and can be safely managed inprimary care. Most of these will heal regardless of treatment, butthe initial care can have a considerable influence on thecosmetic outcome. All burns should be assessed by taking anadequate history and examination.
First aid
The aims of first aid should be to stop the burning process, coolthe burn, provide pain relief, and cover the burn.
Stop the burning process—The heat source should be removed.Flames should be doused with water or smothered with ablanket or by rolling the victim on the ground. Rescuers shouldtake care to avoid burn injury to themselves. Clothing can retainheat, even in a scald burn, and should be removed as soon aspossible. Adherent material, such as nylon clothing, should beleft on. Tar burns should be cooled with water, but the tar itselfshould not be removed. In the case of electrical burns the victimshould be disconnected from the source of electricity beforefirst aid is attempted.
Cooling the burn—Active cooling removes heat and preventsprogression of the burn. This is effective if performed within20 minutes of the injury. Immersion or irrigation with runningtepid water (15°C) should be continued for up to 20 minutes.This also removes noxious agents and reduces pain, and mayreduce oedema by stabilising mast cells and histamine release.Iced water should not be used as intense vasoconstriction cancause burn progression. Cooling large areas of skin can lead tohypothermia, especially in children. Chemical burns should beirrigated with copious amounts of water.
Analgesia—Exposed nerve endings will cause pain. Coolingand simply covering the exposed burn will reduce the pain.Opioids may be required initially to control pain, but once firstaid measures have been effective non-steroidalanti-inflammatory drugs such as ibuprofen or co-dydramoltaken orally will suffice.
Covering the burn—Dressings should cover the burn areaand keep the patient warm. Polyvinyl chloride film (cling film)is an ideal first aid cover. The commercially available roll isessentially sterile as long as the first few centimetres arediscarded. This dressing is pliable, non-adherent, impermeable,acts as a barrier, and is transparent for inspection. It isimportant to lay this on the wound rather than wrapping theburn. This is especially important on limbs, as later swellingmay lead to constriction. A blanket laid over the top will keepthe patient warm. If cling film is not available then any cleancotton sheet (preferably sterile) can be used. Hand burns canbe covered with a clear plastic bag so as not to restrict mobility.Avoid using wet dressings, as heat loss during transfer tohospital can be considerable.
Use of topical creams should be avoided at this stage asthese may interfere with subsequent assessment of the burn.Cooling gels such as Burnshield are often used by paramedics.These are useful in cooling the burn and relieving pain in theinitial stages.
A superficial scald suitable for management in primary care
Benefits of cooling burn injuries with water
x Stops burning processx Minimises oedema
x Reduces painx Cleanses wound
Cling film for dressing burn wounds
x Essentially sterilex Lay on wound—Do not wrap aroundx Non-adherentx Pliablex Transparent for inspection
Burnshield is a cooling gel used to cover burn andreduce pain
This is the third in a series of 12 articles
Clinical review
1487BMJ VOLUME 328 19 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Management of minor burnsThe cause of injury and depth and extent of burn should beassessed in the same way as for more major burns andrecorded. Similarly, associated illness or injuries must beconsidered (such as small burns as a result of fits, faints, or falls).Burns suitable for outpatient management are usually smalland superficial and not affecting critical areas. Homecircumstances should be considered, as even small injuries tothe feet will progress if the legs are not elevated for at least48 hours; this is rarely possible at home. Always consult a burnsunit if in doubt about management
Once the decision has been taken to treat a burn patient asan outpatient, analgesia should be given and the woundthoroughly cleaned and a dressing applied (except on the face).Ensure that a follow up appointment is made.
There are a vast range of acceptable options in theoutpatient management of minor burns. The following shouldbe used as a guide
Cleaning the burnIt is important to realise that a new burn is essentially sterile,and every attempt should be made to keep it so. The burnwound should be thoroughly cleaned with soap and water ormild antibacterial wash such as dilute chlorohexidine. Routineuse of antibiotics should be discouraged. There is somecontroversy over management of blisters, but large ones shouldprobably be de-roofed, and dead skin removed with sterilescissors or a hypodermic needle. Smaller blisters should be leftintact.
DressingsMany different dressings are in use, with little or no data tosupport any individual approach. We favour covering the cleanburn with a simple gauze dressing impregnated with paraffin(Jelonet). Avoid using topical creams as these will interfere withsubsequent assessment of the burn. Apply a gauze pad over thedressing, followed by several layers of absorbent cotton wool. Afirm crepe bandage applied in a figure of eight manner andsecured with plenty of adhesive tape (Elastoplast) will preventslippage of the dressing and shearing of the wound.
An elastic net dressing (Netelast) is useful for securingawkward areas such as the head and neck and chest. Limbburns should be elevated for the duration of treatment.
Dressing changesThe practice of subsequent dressing changes is varied. Ideallythe dressing should be checked at 24 hours. The burn wounditself should be reassessed at 48 hours and the dressingschanged, as they are likely to be soaked through. At this stagethe depth of burn should be apparent, and topical agents suchas Flamazine can be used.
Depending on how healing is progressing, dressing changesthereafter should be every three to five days. If the Jelonetdressing has become adherent, it should be left in place to avoiddamage to delicate healing epithelium. If Flamazine is used itshould be changed on alternate days. The dressing should bechanged immediately if the wound becomes painful or smellyor the dressing becomes soaked (“strike through”).
Any burn that has not healed within two weeks should beseen by a burn surgeon.
Specialist dressingsMany specialist dressings are available, some developed forspecific cases, but most designed for their ease of use. Thefollowing are among the more widely used.
Minor burns suitable for outpatientmanagement
x Partial thickness burns covering < 10% of totalbody surface area in adults
x Partial thickness burns covering < 5% of bodysurface area in children
x Full thickness burns covering < 1% of bodysurface
x No comorbidity
Large blister onthenar eminencerestricting movementof hand (top). Blisteris de-roofed usingaseptic technique(bottom)
Superficial scald burn on side of neck (top left) is cleaned and then alayer of Jelonet applied over it (top right). Gauze square dressings on topof the Jelonet (bottom left) are held in place with a Netelast type ofdressing (bottom right)
Dressing changes for burns
x Use aseptic techniquex First change after 48 hours, and every 3-5 days
thereafterx Criteria for early dressing change:
Excessive “strike through” of fluid from woundSmelly woundContaminated or soiled dressingsSlipped dressingsSigns of infection (such as fever)
Clinical review
1488 BMJ VOLUME 328 19 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Flamazine is silver sulfadiazine cream and is applied topicallyon the burn wound. It is effective against gram negative bacteriaincluding Pseudomonas. Infection with the latter will cause thedressing to turn green with a distinctive smell. Apply the creamin a 3-5 mm thick layer and cover with gauze. It should beremoved and reapplied every two days. There is a reported3{5% incidence of reversible leucopenia.
Granulflex is a hydrocolloid dressing with a thinpolyurethane foam sheet bonded onto a semipermeable film.The dressing is adhesive and waterproof and is therefore usefulin awkward areas or where normal dressings are not suitable. Itshould be applied with a 2 cm border. By maintaining a moistatmosphere over the wound, it creates an environment suitablefor healing. It usually needs to be changed every three or fourdays, but it can be left for seven days. A thinner version(Duoderm) is also available.
Mepitel is a flexible polyamide net coated with soft siliconeto give a Jelonet-type of dressing that is non adhesive. It is auseful but expensive alternative to Jelonet when easy removal isdesirable, such as with children.
Facial burnsFacial burns should be referred to a specialist unit. However,simple sunburn should be left exposed as dressings can beawkward to retain on the face. The wound should be cleansedtwice daily with mild diluted chlorohexidine solution. The burnshould be covered with a bland ointment such as liquid paraffin.This should be applied every 1-4 hours as necessary tominimise crust formation. Men should shave daily to reducerisk of infection. All patients should be advised to sleeppropped up on two pillows for the first 48 hours to minimisefacial oedema.
Follow upBurns that fail to heal within three weeks should be referred toa plastic surgery unit for review. Healed burns will be sensitiveand have dry scaly skin, which may develop pigmental changes.Daily application of moisturiser cream should be encouraged.Healed areas should be protected from the sun with sun blockfor 6-12 months. Pruritis is a common problem.
Physiotherapy—Patients with minor burns of limbs may needphysiotherapy. It is important to identify these patients earlyand start therapy. Hypertrophic scars may benefit from scartherapy such as pressure garments or silicone. For thesereasons, all healed burns should be reviewed at two months forreferral to an occupational therapist if necessary.
Support and reassurance—Patients with burn injuries oftenworry about disfigurement and ugliness, at least in the shortterm, and parents of burnt children often have feelings of guilt.It is important to address these issues with reassurance.
Jackie Hudspith is clinical nurse lead, Burns Centre, Chelsea andWestminster Hospital, London. Sukh Rayatt is specialist registrar inplastic and reconstructive surgery, West Midlands Training Scheme,Birmingham.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burn Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrews Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.
Competing interests: See first article for series editors’ details.
BMJ 2004;328:1487–9
Flamazine
x Silver sulfadiazine creamx Covers gram negative bacteria including
Pseudomonasx Needs to be changed every 24-48 hoursx Makes burn seem white and should be avoided if
burn needs reassessment
Management of facial burns
x Clean face twice a day with dilute chlorohexidinesolution
x Cover with cream such as liquid paraffin onhourly basis
x Men should shave dailyx Sleep propped up on two pillows to minimise
oedema
Pruritis
x Common in healing and healed burn woundsx Aggravated by heat, stress, and physical activityx Worst after healingx Massage with aqueous cream or aloe vera creamx Use antihistamines (such as chlorphenamine)
and analgesics
Key points
x Initial first aid can influence final cosmetic outcomex Cooling with tepid tap water is one of the most important first aid
measuresx Routine use of antibiotics should be discouragedx Simple dressings sufficex Aseptic technique should be used for dressing changesx If in doubt, seek advice from regional burns unit or plastic surgery
department
Further reading
x Wilson G, French G. Plasticized polyvinylchloride as a temporarydressing for burns. BMJ 1987;294:556-7
x Davies JWL. Prompt cooling of the burned area: a review ofbenefits and the effector mechanisms. Burns 1982;9:1-6
x Slater RM, Hughes NC. A simplified method of treating burns ofthe hands. Br J Plast Surg 1971;24:296-300
x Herndon D. Total burn care. 2nd ed. London: Harcourt, 2002x Settle J, ed. Principles and practice of burns management. Edinburgh:
Churchill Livingstone, 1996x National Burn Care Review. National burn injury referral
guidelines. In: Standards and strategy for burn care. London: NBCR,2001: 68-9
Clinical review
1489BMJ VOLUME 328 19 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsInitial management of a major burn: I—overviewShehan Hettiaratchy, Remo Papini
A major burn is defined as a burn covering 25% or more oftotal body surface area, but any injury over more than 10%should be treated similarly. Rapid assessment is vital. Thegeneral approach to a major burn can be extrapolated tomanaging any burn. The most important points are to take anaccurate history and make a detailed examination of the patientand the burn, to ensure that key information is not missed.
This article outlines the structure of the initial assessment.The next article will cover the detailed assessment of burnsurface area and depth and how to calculate the fluidresuscitation formula.
History takingThe history of a burn injury can give valuable informationabout the nature and extent of the burn, the likelihood ofinhalational injury, the depth of burn, and probability of otherinjuries. The exact mechanism of injury and any prehospitaltreatment must be established.
A patient’s history must be obtained on admission, as thismay be the only time that a first hand history is obtainable.Swelling may develop around the airway in the hours afterinjury and require intubation, making it impossible for thepatient to give a verbal history. A brief medical history shouldbe taken, outlining previous medical problems, medications,allergies, and vaccinations. Patients’ smoking habits should bedetermined as these may affect blood gas analyses.
Primary surveyThe initial management of a severely burnt patient is similar tothat of any trauma patient. A modified “advanced trauma lifesupport” primary survey is performed, with particular emphasison assessment of the airway and breathing. The burn injurymust not distract from this sequential assessment, otherwiseserious associated injuries may be missed.
A—Airway with cervical spine controlAn assessment must be made as to whether the airway iscompromised or is at risk of compromise. The cervical spineshould be protected unless it is definitely not injured. Inhalationof hot gases will result in a burn above the vocal cords. Thisburn will become oedematous over the following hours,especially after fluid resuscitation has begun. This means that anairway that is patent on arrival at hospital may occlude afteradmission. This can be a particular problem in small children.
Direct inspection of the oropharynx should be done by asenior anaesthetist. If there is any concern about the patency ofthe airway then intubation is the safest policy. However, anunnecessary intubation and sedation could worsen a patient’scondition, so the decision to intubate should be made carefully.
B—BreathingAll burn patients should receive 100% oxygen through ahumidified non-rebreathing mask on presentation. Breathingproblems are considered to be those that affect the respiratorysystem below the vocal cords. There are several ways that a burninjury can compromise respiration.
Initial assessment of a major burn
x Perform an ABCDEF primary surveyA—Airway with cervical spine control, B—Breathing,C—Circulation, D—Neurological disability, E—Exposure withenvironmental control, F—Fluid resuscitation
x Assess burn size and depth (see later article for detail)x Establish good intravenous access and give fluidsx Give analgesiax Catheterise patient or establish fluid balance monitoringx Take baseline blood samples for investigationx Dress woundx Perform secondary survey, reassess, and exclude or treat associated
injuriesx Arrange safe transfer to specialist burns facility
Key points of a burn history
Exact mechanismx Type of burn agent (scald,
flame, electrical, chemical)x How did it come into contact
with patient?x What first aid was performed?x What treatment has been
started?
x Is there risk of concomitantinjuries (such as fall from height,road traffic crash, explosion)?
x Is there risk of inhalationalinjuries (did burn occur in anenclosed space)?
Exact timingsx When did the injury occur?x How long was patient exposed
to energy source?
x How long was cooling applied?x When was fluid resuscitation
started?
Exact injuryScaldsx What was the liquid? Was it
boiling or recently boiled?x If tea or coffee, was milk in it?x Was a solute in the liquid?
(Raises boiling temperatureand causes worse injury, suchas boiling rice)
Electrocution injuriesx What was the voltage (domestic
or industrial)?x Was there a flash or arcing?x Contact time
Chemical injuriesx What was the chemical?
Is there any suspicion of non-accidental injury?x See previous article
Airway management
Signs of inhalational injuryx History of flame burns or burns in
an enclosed spacex Full thickness or deep dermal burns
to face, neck, or upper torsox Singed nasal hairx Carbonaceous sputum or carbon
particles in oropharynx
Indications for intubationx Erythema or swelling of
oropharynx on directvisualisation
x Change in voice, withhoarseness or harsh cough
x Stridor, tachypnoea, ordyspnoea
Carbonaceous particlesstaining a patient’s face aftera burn in an enclosed space.This suggests there isinhalational injury
This is the fourth in a series of 12 articles
Clinical review
1555BMJ VOLUME 328 26 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Mechanical restriction of breathing—Deep dermal or fullthickness circumferential burns of the chest can limit chestexcursion and prevent adequate ventilation. This may requireescharotomies (see next article).
Blast injury—If there has been an explosion, blast lung cancomplicate ventilation. Penetrating injuries can cause tensionpneumothoraces, and the blast itself can cause lung contusionsand alveolar trauma and lead to adult respiratory distresssyndrome.
Smoke inhalation—The products of combustion, thoughcooled by the time they reach the lungs, act as direct irritants tothe lungs, leading to bronchospasm, inflammation, andbronchorrhoea. The ciliary action of pneumocytes is impaired,exacerbating the situation. The inflammatory exudate created isnot cleared, and atelectasis or pneumonia follows. The situationcan be particularly severe in asthmatic patients. Non-invasivemanagement can be attempted, with nebulisers and positivepressure ventilation with some positive end-expiratory pressure.However, patients may need a period of ventilation, as thisallows adequate oxygenation and permits regular lung toileting.
Carboxyhaemoglobin—Carbon monoxide binds todeoxyhaemoglobin with 40 times the affinity of oxygen. It alsobinds to intracellular proteins, particularly the cytochromeoxidase pathway. These two effects lead to intracellular andextracellular hypoxia. Pulse oximetry cannot differentiatebetween oxyhaemoglobin and carboxyhaemoglobin, and maytherefore give normal results. However, blood gas analysis willreveal metabolic acidosis and raised carboxyhaemoglobin levelsbut may not show hypoxia. Treatment is with 100% oxygen,which displaces carbon monoxide from bound proteins sixtimes faster than does atmospheric oxygen. Patients withcarboxyhaemoglobin levels greater than 25-30% should beventilated. Hyperbaric therapy is rarely practical and has notbeen proved to be advantageous. It takes longer to shift thecarbon monoxide from the cytochrome oxidase pathway thanfrom haemoglobin, so oxygen therapy should be continueduntil the metabolic acidosis has cleared.
C—CirculationIntravenous access should be established with two large borecannulas preferably placed through unburnt tissue. This is anopportunity to take blood for checking full blood count, ureaand electrolytes, blood group, and clotting screen. Peripheralcirculation must be checked. Any deep or full thicknesscircumferential extremity burn can act as a tourniquet,especially once oedema develops after fluid resuscitation. Thismay not occur until some hours after the burn. If there is anysuspicion of decreased perfusion due to circumferential burn,the tissue must be released with escharotomies (see next article).
Profound hypovolaemia is not the normal initial responseto a burn. If a patient is hypotensive then it is may be due todelayed presentation, cardiogenic dysfunction, or an occultsource of blood loss (chest, abdomen, or pelvis).
D—Neurological disabilityAll patients should be assessed for responsiveness with theGlasgow coma scale; they may be confused because of hypoxiaor hypovolaemia.
E—Exposure with environment controlThe whole of a patient should be examined (including the back)to get an accurate estimate of the burn area (see later) and tocheck for any concomitant injuries. Burn patients, especiallychildren, easily become hypothermic. This will lead tohypoperfusion and deepening of burn wounds. Patients shouldbe covered and warmed as soon as possible.
Acute bronchoscopy being performed to assess amount of damage to thebronchial tree. Patient has been covered in a blanket and a heat lamp placedoverhead to prevent excessive cooling
Signs of carboxyhaemoglobinaemia
COHb levels Symptoms
0-10% Minimal (normal level in heavy smokers)
10-20% Nausea, headache
20-30% Drowsiness, lethargy
30-40% Confusion, agitation
40-50% Coma, respiratory depression
> 50% DeathCOHb = Carboxyhaemoglobin
Airway
Compromised or at
risk of compromise?
No
Yes
Yes
No
Yes
Yes
Circulation
Compromised perfusion
to an extremity?
Neurological disability
Impaired score on
Glasgow coma scale?
No
Breathing
Compromised?
Cause:
Mechanical
Carboxyhaemoglobin
Smoke inhalation
Blast injury
Consider:
Hypoxia (carboxyhaemoglobin level?)
Hypovolaemia
Escharotomies
Intubate and ventilate
Nebulisers
Non-invasive ventilation
Invasive ventilation
Invasive ventilation
Chest drains
Intubate
Escharotomies
Go back and re-evaluate
No
Exposure
Fully assess burn area and depth
Full examination for concomitant injuries
Keep warm
Fluids
Calculate resuscitation formula based on
surface area and time since burn
Algorithm for primary survey of a major burn injury
Clinical review
1556 BMJ VOLUME 328 26 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

F—Fluid resuscitationThe resuscitation regimen should be determined and begun.This is based on the estimation of the burn area, and thedetailed calculation is covered in the next article. A urinarycatheter is mandatory in all adults with injuries covering > 20%of total body surface area to monitor urine output. Children’surine output can be monitored with external catchment devicesor by weighing nappies provided the injury is < 20% of totalbody area. In children the interosseous route can be used forfluid administration if intravenous access cannot be obtained,but should be replaced by intravenous lines as soon as possible.
AnalgesiaSuperficial burns can be extremely painful. All patients withlarge burns should receive intravenous morphine at a doseappropriate to body weight. This can be easily titrated againstpain and respiratory depression. The need for further dosesshould be assessed within 30 minutes.
InvestigationsThe amount of investigations will vary with the type of burn.
Secondary surveyAt the end of the primary survey and the start of emergencymanagement, a secondary survey should be performed. This isa head to toe examination to look for any concomitant injuries.
Dressing the woundOnce the surface area and depth of a burn have been estimated,the burn wound should be washed and any loose skin removed.Blisters should be deroofed for ease of dressing, except forpalmar blisters (painful), unless these are large enough torestrict movement. The burn should then be dressed.
For an acute burn which will be referred to a burn centre,cling film is an ideal dressing as it protects the wound, reducesheat and evaporative losses, and does not alter the woundappearance. This will permit accurate evaluation by the burnteam later. Flamazine should not be used on a burn that is to bereferred immediately, since it makes assessment of depth moredifficult.
Referral to a burns unitThe National Burn Care Review has established referralguidelines to specialist units. Burns are divided into complexburns (those that require specialist intervention) andnon{complex burns (those that do not require immediateadmission to a specialist unit). Complex burns should bereferred automatically. If you are not sure whether a burnshould be referred, discuss the case with your local burns unit.It is also important to discuss all burns that are not healedwithin two weeks.
Shehan Hettiaratchy is specialist registrar in plastic and reconstructivesurgery, Pan-Thames Training Scheme, London; Remo Papini isconsultant and clinical lead in burns, West Midlands Regional BurnUnit, Selly Oak University Hospital, Birmingham.
The ABC of burns is edited by Shehan Hettiaratchy; Remo Papini;and Peter Dziewulski, consultant burns and plastic surgeon, StAndrews Centre for Plastic Surgery and Burns, Broomfield Hospital,Chelmsford. The series will be published as a book in the autumn.
Competing interests: RP has been reimbursed by Johnson & Johnson,manufacturer of Integra, and Smith & Nephew, manufacturer of Acticoatand TransCyte, for attending symposia on burn care.
BMJ 2004;328:1555–7
Investigations for major burns*
Generalx Full blood count, packed cell volume, urea and electrolyte
concentration, clotting screenx Blood group, and save or crossmatch serum
Electrical injuriesx 12 lead electrocardiographyx Cardiac enzymes (for high tension injuries)
Inhalational injuriesx Chest x rayx Arterial blood gas analysis
Can be useful in any burn, as the base excess is predictive of theamount of fluid resuscitation requiredHelpful for determining success of fluid resuscitation and essentialwith inhalational injuries or exposure to carbon monoxide
*Any concomitant trauma will have its own investigations
Indications for referral to a burns unit
All complex injuries should be referredA burn injury is more likely to be complex if associated with:x Extremes of age—under 5 or over 60 yearsx Site of injury
Face, hands, or perineumFeet (dermal or full thickness loss)Any flexure, particularly the neck or axillaCircumferential dermal or full thickness burn of limb, torso, or neck
x Inhalational injuryAny substantial injury, excluding pure carbon monoxide poisoning
x Mechanism of injuryChemical injury > 5% of total body surface areaExposure to ionising radiationHigh pressure steam injuryHigh tension electrical injuryHydrofluoric acid burn >1% of total body surface areaSuspicion of non-accidental injury
x Large size (dermal or full thickness loss)Paediatric ( < 16 years old) > 5% of total body surface areaAdult ( ≥ 16 years) > 10% of total body surface area
x Coexisting conditionsAny serious medical conditions (cardiac dysfunction,immunosuppression, pregnancy)Any associated injuries (fractures, head injuries, crush injuries)
Key points
x Perform a systematic assessment as with anytrauma patient (don’t get distracted by the burn)
x Beware of airway compromisex Provide adequate analgesiax Exclude any concomitant injuriesx Discuss with a burns unit earlyx If in doubt, reassess
Further reading
x Sheridan R. Burns. Crit Care Med 2002;30:S500-14x British Burn Association. Emergency management of severe burns
course manual, UK version. Wythenshawe Hospital, Manchester,1996
x Herndon D. Total burn care. 2nd ed. London: WB Saunders, 2002x Kao CC, Garner WL. Acute burns. Plast Reconstr Surg 2000;105:
2482-93x Burnsurgery.org. www.burnsurgery.org
Clinical review
1557BMJ VOLUME 328 26 JUNE 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsInitial management of a major burn: II—assessment and resuscitationShehan Hettiaratchy, Remo Papini
Assessment of burn areaAssessment of burn area tends to be done badly, even by thosewho are expert at it. There are three commonly used methodsof estimating burn area, and each has a role in differentscenarios. When calculating burn area, erythema should not beincluded. This may take a few hours to fade, so someoverestimation is inevitable if the burn is estimated acutely.
Palmar surface—The surface area of a patient’s palm (includingfingers) is roughly 0.8% of total body surface area. Palmar surfaceare can be used to estimate relatively small burns ( < 15% of totalsurface area) or very large burns ( > 85%, when unburnt skin iscounted). For medium sized burns, it is inaccurate.
Wallace rule of nines—This is a good, quick way of estimatingmedium to large burns in adults. The body is divided into areasof 9%, and the total burn area can be calculated. It is notaccurate in children.
Lund and Browder chart—This chart, if used correctly, is themost accurate method. It compensates for the variation in bodyshape with age and therefore can give an accurate assessmentof burns area in children.
It is important that all of the burn is exposed and assessed.During assessment, the environment should be kept warm, andsmall segments of skin exposed sequentially to reduce heat loss.Pigmented skin can be difficult to assess, and in such cases itmay be necessary to remove all the loose epidermal layers tocalculate burn size.
Resuscitation regimensFluid losses from the injury must be replaced to maintainhomoeostasis. There is no ideal resuscitation regimen, andmany are in use. All the fluid formulas are only guidelines, andtheir success relies on adjusting the amount of resuscitationfluid against monitored physiological parameters. The mainaim of resuscitation is to maintain tissue perfusion to the zoneof stasis and so prevent the burn deepening. This is not easy, astoo little fluid will cause hypoperfusion whereas too much willlead to oedema that will cause tissue hypoxia.
The greatest amount of fluid loss in burn patients is in thefirst 24 hours after injury. For the first eight to 12 hours, there isa general shift of fluid from the intravascular to interstitial fluidcompartments. This means that any fluid given during this timewill rapidly leave the intravascular compartment. Colloids haveno advantage over crystalloids in maintaining circulatoryvolume. Fast fluid boluses probably have little benefit, as a rapidrise in intravascular hydrostatic pressure will just drive morefluid out of the circulation. However, much protein is lostthrough the burn wound, so there is a need to replace thisoncotic loss. Some resuscitation regimens introduce colloidafter the first eight hours, when the loss of fluid from theintravascular space is decreasing.
Burns covering more than 15% of total body surface area inadults and more than 10% in children warrant formalresuscitation. Again these are guidelines, and experienced staffcan exercise some discretion either way. The most commonlyused resuscitation formula is the Parkland formula, a purecrystalloid formula. It has the advantage of being easy to
Adult Child
Back= 18%
Back= 18%
Head = 9%(front and back)
Head = 18%(front and back)
Right arm= 9%
Perineum= 1%
Perineum= 1%
Left arm= 9%
Left arm= 9%
Right leg= 18%
Right arm= 9%
Right leg= 13.5%
Left leg= 18%
Left leg= 13.5%
Chest = 18%
Chest = 18%
Wallace rule of nines
% Total Body Surface Area Burn
Be clear and accurate, and do not include erythema(Lund and Browder)
REGION PTL
%
FTL
Head
Neck
Ant. trunk
Post. trunk
Right arm
Left arm
Buttocks
Genitalia
Right leg
Left leg
Total burn
AREA
A = 1/2 OF HEAD
B = 1/2 OF ONE THIGH
C = 1/2 OF ONE LOWER LEG
Age 0
91/2
23/4
21/2
1
81/2
31/4
21/2
5
61/2
4
23/4
10
51/2
41/2
3
15
41/2
41/2
31/4
Adult
31/2
43/4
31/2
A
13
1
11
22
11/2 11/2
11/2 11/2
13/413/4
B B
C C
A
13
22
11/2
21/2 21/2
11/2
11/2 11/2
13/413/4
B B
C C
Lund and Browder chart
This is the fifth in a series of 12 articles
Clinical review
101BMJ VOLUME 329 10 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

calculate and the rate is titrated against urine output. Thiscalculates the amount of fluid required in the first 24 hours.Children require maintenance fluid in addition to this.The starting point for resuscitation is the time of injury, not thetime of admission. Any fluid already given should be deductedfrom the calculated requirement.
At the end of 24 hours, colloid infusion is begun at a rate of0.5 ml×(total burn surface area (%))×(body weight (kg)), andmaintenance crystalloid (usually dextrose-saline) is continued ata rate of 1.5 ml×(burn area)×(body weight). The end point toaim for is a urine output of 0.5-1.0 ml/kg/hour in adults and1.0-1.5 ml/kg/hour in children.
High tension electrical injuries require substantially morefluid (up to 9 ml×(burn area)×(body weight) in the first 24hours) and a higher urine output (1.5-2 ml/kg/hour).Inhalational injuries also require more fluid.
In Britain Hartman’s solution (sodium chloride 0.6%,sodium lactate 0.25%, potassium chloride 0.04%, calciumchloride 0.027%) is the most commonly used crystalloid.Colloid use is controversial: some units introduce colloid aftereight hours, as the capillary leak begins to shut down, whereasothers wait until 24 hours. Fresh frozen plasma is often used inchildren, and albumin or synthetic high molecular weightstarches are used in adults.
The above regimens are merely guidelines to the probableamount of fluid required. This should be continuously adjustedaccording to urine output and other physiological parameters(pulse, blood pressure, and respiratory rate). Investigations atintervals of four to six hours are mandatory for monitoring apatient’s resuscitation status. These include packed cell volume,plasma sodium, base excess, and lactate.
Burns units use different resuscitation formulas, and it isbest to contact the local unit for advice.
EscharotomiesA circumferential deep dermal or full thickness burn is inelasticand on an extremity will not stretch. Fluid resuscitation leads tothe development of burn wound oedema and swelling of thetissue beneath this inelastic burnt tissue. Tissue pressures riseand can impair peripheral circulation. Circumferential chestburns can also cause problems by limiting chest excursion andimpairing ventilation. Both of these situations requireescharotomy, division of the burn eschar. Only the burnt tissueis divided, not any underlying fascia, differentiating thisprocedure from a fasciotomy.
Incisions are made along the midlateral or medial aspects ofthe limbs, avoiding any underlying structures. For the chest,longitudinal incisions are made down each mid-axillary line tothe subcostal region. The lines are joined up by a chevronincision running parallel to the subcostal margin. This creates amobile breastplate that moves with ventilation. Escharotomiesare best done with electrocautery, as they tend to bleed. Theyare then packed with Kaltostat alginate dressing and dressedwith the burn.
Although they are an urgent procedure, escharotomies arebest done in an operating theatre by experienced staff. Theyshould be discussed with the local burns unit, and performedunder instruction only when transfer is delayed by severalhours. Initially, at risk limbs should be elevated and observed.
Assessment of burn depthThe depth of burn is related to the amount of energy deliveredin the injury and to the relative thickness of the skin (the dermisis thinner in very young and very old people).
Parkland formula for burns resuscitation
Total fluid requirement in 24 hours =4 ml×(total burn surface area (%))×(body weight (kg))50% given in first 8 hours50% given in next 16 hours
Children receive maintenance fluid in addition, at hourly rate of4 ml/kg for first 10 kg of body weight plus2 ml/kg for second 10 kg of body weight plus1 ml/kg for > 20 kg of body weight
End pointUrine output of 0.5-1.0 ml/kg/hour in adultsUrine output of 1.0-1.5 ml/kg/hour in children
Worked examples of burns resuscitation
Fluid resuscitation regimen for an adultA 25 year old man weighing 70 kg with a 30% flame burn wasadmitted at 4 pm. His burn occurred at 3 pm.
1) Total fluid requirement for first 24 hours4 ml×(30% total burn surface area)×(70 kg) = 8400 ml in 24 hours
2) Half to be given in first 8 hours, half over the next 16 hoursWill receive 4200 ml during 0-8 hours and 4200 ml during 8-24 hours
3) Subtract any fluid already received from amount required for first8 hoursHas already received 1000 ml from emergency services, and so needsfurther 3200 ml in first 8 hours after injury
4) Calculate hourly infusion rate for first 8 hoursDivide amount of fluid calculated in (3) by time left until it is 8 hoursafter burnBurn occurred at 3 pm, so 8 hour point is 11 pm. It is now 4 pm, soneed 3200 ml over next 7 hours:
3200/7 = 457 ml/hour from 4 pm to 11 pm
5) Calculate hourly infusion rate for next 16 hoursDivide figure in (2) by 16 to give fluid infusion rateNeeds 4200 ml over 16 hours:
4200/16 = 262.5 ml/hour from 11 pm to 3 pm next day
Maintenance fluid required for a childA 24 kg child with a resuscitation burn will need the followingmaintenance fluid:4 ml/kg/hour for first 10 kg of weight = 40 ml/hour plus2 ml/kg/hour for next 10 kg of weight = 20 ml/hour plus1 ml/kg/hour for next 4 kg of weight = 1×4 kg = 4 ml/hourTotal = 64 ml/hour
Escharotomy in aleg with acircumferentialdeep dermal burn
Line ofescharotomies
Diagram ofescharotomies forthe chest
Clinical review
102 BMJ VOLUME 329 10 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Classification of burn depthsBurns are classified into two groups by the amount of skin loss.Partial thickness burns do not extend through all skin layers,whereas full thickness burns extend through all skin layers intothe subcutaneous tissues. Partial thickness burns can be furtherdivided into superficial, superficial dermal, and deep dermal:x Superficial—The burn affects the epidermis but not thedermis (such as sunburn). It is often called an epidermal burnx Superficial dermal—The burn extends through the epidermisinto the upper layers of the dermis and is associated withblisteringx Deep dermal—The burn extends through the epidermis intothe deeper layers of the dermis but not through the entiredermis.
Estimation of burn depthAssessing burn depth can be difficult. The patient’s history willgive clues to the expected depth: a flash burn is likely to besuperficial, whereas a burn from a flame that was not rapidlyextinguished will probably be deep. On direct examination,there are four elements that should be assessed—bleeding onneedle prick, sensation, appearance, and blanching to pressure.
Bleeding—Test bleeding with a 21 gauge needle. Briskbleeding on superficial pricking indicates the burn is superficialor superficial dermal. Delayed bleeding on a deeper pricksuggests a deep dermal burn, while no bleeding suggests a fullthickness burn.
Sensation—Test sensation with a needle also. Pain equateswith a superficial or superficial dermal burn, non-painfulsensation equates with deep dermal injury, while full thicknessinjuries are insensate. However, this test is often inaccurate asoedema also blunts sensation.
Appearance and blanching—Assessing burn depth byappearance is often difficult as burns may be covered with sootor dirt. Blisters should be de-roofed to assess the base. Capillaryrefill should be assessed by pressing with a sterile cotton bud(such as a bacteriology swab).x A red, moist wound that obviously blanches and then rapidlyrefills is superficialx A pale, dry but blanching wound that regains its colourslowly is superficial dermalx Deep dermal injuries have a mottled cherry red colour thatdoes not blanch (fixed capillary staining). The blood is fixedwithin damaged capillaries in the deep dermal plexusx A dry, leathery or waxy, hard wound that does not blanch isfull thickness. With extensive burns, full thickness burns canoften be mistaken for unburnt skin in appearance.
Most burns are a mixture of different depths. Assessment ofdepth is important for planning treatment, as more superficialburns tend to heal spontaneously whereas deeper burns needsurgical intervention, but is not necessary for calculatingresuscitation formulas. Therefore, in acute situations lengthydepth assessment is inappropriate. A burn is a dynamic wound,and its depth will change depending on the effectiveness ofresuscitation. Initial estimates need to be reviewed later.
Shehan Hettiaratchy is specialist registrar in plastic and reconstructivesurgery, Pan-Thames Training Scheme, London; Remo Papini isconsultant and clinical lead in burns, West Midlands Regional BurnUnit, Selly Oak University Hospital, Birmingham.
The ABC of burns is edited by Shehan Hettiaratchy; Remo Papini;and Peter Dziewulski, consultant burns and plastic surgeon, StAndrews Centre for Plastic Surgery and Burns, Broomfield Hospital,Chelmsford. The series will be published as a book in the autumn.
Competing interests: RP has been reimbursed by Johnson & Johnson,manufacturer of Integra, and Smith & Nephew, manufacturer of Acticoatand TransCyte, for attending symposiums on burn care.
BMJ 2004;329:101–3
Epidermis
SuperficialSuperficial
dermalDeep
dermalFull
thickness
Dermis
Subcutaneous
Diagram of the different burn depths
Full thickness burn in a black patient. In a white patient with extensiveburns, such full thickness burns can easily be mistaken for unburnt skin
Assessment of burn depth
Burn type
SuperficialSuperficial
dermalDeep
dermalFull
thickness
Bleeding onpin prick
Brisk Brisk Delayed None
Sensation Painful Painful Dull None
Appearance Red,glistening
Dry, whiter Cherry red Dry, white,leathery
Blanching topressure
Yes, briskreturn
Yes, slowreturn
No No
Key points
x Accurate assessment of burn area is crucial to calculateresuscitation formula
x Resuscitation formulas are only guidelines—monitor the patientx Discuss resuscitation with a burns unitx Be aware of the need for escharotomiesx Burn depth is difficult to estimate and changes with resuscitation
Further information
x Clarke J. Burns. Br Med Bull 1999;55:885-94x Herndon D. Total burn care. 2nd ed. London: WB Saunders, 2002x Kao CC, Garner WL. Acute burns. Plast Reconstr Surg 2000;105:
2482{93x Yowler CJ, Fratianne RB. The current status of burn resuscitation.
Clin Plast Surg 2000;1:1-9x Collis N, Smith G, Fenton OM. Accuracy of burn size estimation
and subsequent fluid resuscitation prior to arrival at the YorkshireRegional Burns Unit. A three year retrospective study. Burns 1999;25: 345-51
x Burnsurgery.org (see www.burnsurgery.org)
Clinical review
103BMJ VOLUME 329 10 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsManagement of burn injuries of various depthsRemo Papini
Accurate assessment of burn depth on admission is importantin making decisions about dressings and surgery. However, theburn wound is a dynamic living environment that will alterdepending on both intrinsic factors (such as release ofinflammatory mediators, bacterial proliferation) and extrinsicfactors (such as dehydration, systemic hypotension, cooling). Itis therefore important to review the wound at regular intervalsuntil healing.
Optimum treatment of the wound reduces morbidity and, inlarger injuries, mortality. It also shortens the time for healingand return to normal function and reduces the need forsecondary reconstruction.
When epithelialisation is delayed beyond three weeks, theincidence of hypertrophic scarring rises. Hypertrophic scarsoccur in 60% of burnt children aged under 5 years. Earlygrafting of those burns that have not healed at three weeks hasbeen shown to improve the result, but because of delays in thereferral process, all injuries, which show no sign of healing by10 days, should be referred for assessment.
TreatmentEpidermal burnsBy definition these affect only the epidermis and are typified bysunburn. Blistering may occur but is not common. Supportivetherapy is usually all that is required, with regular analgesia andintravenous fluids for extensive injuries. Healing occurs rapidly,within a week, by regeneration from undamaged keratinocyteswithin skin adnexae.
Superficial partial thickness burnsThese affect the upper dermis and the epidermis. Blistering iscommon. The exposed superficial nerves make these injuriespainful.
Healing is expected within two weeks by regeneration ofepidermis from keratinocytes within sweat glands and hairfollicles. The rate of regeneration depends on the density ofthese skin adnexae: thin hairless skin (inner arm, eyelids, etc)heals more slowly than thick or hairy skin (back, scalp, and face).Progression to a deeper burn is unlikely but can occur if thewound dries out or becomes infected or the patient becomessystemically unwell or hypotensive.
Treatment is aimed at preventing wound progression by theuse of antimicrobial creams and occlusive dressings, sinceepithelialisation progresses faster in a moist environment.Hypafix applied directly to superficial wounds can be useful topreserve mobility and allow washing of the affected part withthe dressing intact. It must be soaked in oil (such as olive oil) foran hour before removal, and should be changed at least weeklyuntil the burn has healed.
Alternatively, tulle gras dressing or Mepitel (a siliconedressing) can be applied with or without silver sulfadiazinecream, or Acticoat and gauze, and changed on alternate days.Some burns units treat difficult wounds such as facial burns byleaving them exposed and applying antimicrobial ointment.
If a burn has not healed by two weeks, the depth hasprobably been assessed incorrectly and referral should be madeto a burns unit.
Deep dermal
Full thickness
Superficialpartialthickness
Flame injury showing all burn depths
Hypertrophic scar in a child
Hypafix dressing applied to a burn wound allowsmovement and washing
This is the sixth in a series of 12 articles
Clinical review
158 BMJ VOLUME 329 17 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Deep partial thicknessThese injuries are the most difficult to assess and treat. Theymay initially seem superficial, with blanching on pressure, buthave fixed capillary staining on re-examination after 48 hours.The density of skin adnexae (and hence islands of regeneration)is lower at this depth, and healing is slower and associated withcontraction. Therefore, if these injuries are extensive or infunctional or cosmetically sensitive areas, they are better excisedto a viable depth and then skin grafted to reduce morbidity andto accelerate return to normal function.
Some deep partial thickness injuries will heal if the woundenvironment is optimised to encourage endogenous healing.This includes keeping it warm, moist, and free of infection.Some of the newer tissue engineered dressings are designed toencourage this by supplying exogenous cytokines. An exampleis TransCyte, which contains allogeneic non-viable fibroblaststhat have produced wound healing factors during manufacture.However, these dressings are highly expensive and need to beapplied by trained staff in theatre.
Full thickness injuriesAll regenerative elements have been destroyed in these injuries,and healing only occurs from the edges and is associated withconsiderable contraction. All such injuries should therefore beexcised and grafted unless they are < 1 cm in diameter in anarea where function would not be compromised.
Timing of surgeryIdeally, all wounds should have epithelial cover within threeweeks to minimise scarring, but in practice the decision whetherto refer a patient must be made by day 10 to achieve this.
The burn eschar is shaved tangentially or excised to deepfascia. From the surgical viewpoint, the best time to graft burnsis within five days of injury to minimise blood loss, and injuriesthat are obviously deep at presentation must be referred early.
With major burns, treatment is skewed towards preservationof life or limb, and large areas of deep burn must be excisedbefore the burnt tissue triggers multiple organ failure orbecomes infected. In such cases more superficial burns may betreated with dressings until healing occurs late or fresh skindonor sites become available.
The ideal covering is split skin autograft from unburnt areas.Thickness is usually tailored to the depth of excision to obtaingood cosmesis, although thinner grafts are thought to contractmore. Donor sites should ideally be harvested adjacent to theinjury to improve colour match, and sheet graft is preferred toimprove the cosmetic result.
If donor sites are sparse, however, or the wound bed is likelyto bleed profusely (because excision is carried out late, forinstance) then the graft is perforated with a mesher to allowexpansion. Although this improves graft “take” where thewound bed is bleeding after tangential excision, the meshpattern is permanent and unsightly. Unmeshed sheet graft isused on hands and faces, and over any future site forintravenous central lines and tracheostomies to obtain rapidcover. Where unburnt split skin donor sites are in very shortsupply, there are two possible solutions:x Rotation of donor sites is practised, and unexcised burncovered with antimicrobial creamsx The excised wound is resurfaced with a temporary coveringuntil donor sites have regenerated and can be re-harvested.
Examples of a temporary covering are cadaveric allograftfrom an unrelated donor, xenograft (such as pigskin), syntheticproducts, and cultured epithelial autograft. Development ofsynthetic products (such as Integra dermal regeneration
Shave excision to healthy tissue
Thick and thin split skin grafts
Meshed graft
Persistent mesh pattern in patient whose extensiveburns were covered with meshed skin grafts
Clinical review
159BMJ VOLUME 329 17 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

template) has allowed us to excise extremely large burns andstill achieve physiological closure, with potentially lowermortality in these injuries. Cultured epithelial autografts alsopermits us to extend the available donor sites. The cultured cellscan be applied as sheets (available after three weeks) or insuspension (available within one week). A few burns units usethese cells for superficial skin loss or in combination with meshgraft to improve the cosmetic result.
Major burnsThese include injuries covering more than 20% of the totalbody surface area, and represent a real challenge to burnsurgeons. Survival depends on accurate assessment and promptresuscitation initially, as well as on patients’ premorbidconditions and associated injuries such as smoke inhalation.
Subsequently, constant attention to wound cleanliness and tonutritional, respiratory, cardiovascular, and renal support isnecessary. Relentless but carefully timed removal of burnt tissueand replacement with definitive wound cover is the key to survivaland return to function. Such injuries are best managed in largecentres where the necessary expertise is concentrated. Earlyexcision and grafting have been shown to reduce pain, shortenhospital stay, and accelerate return to normal function inmoderate injuries. It is more difficult to show that this approachimproves survival in massive injuries because these areuncommon and many factors other than surgery play a part.
Most major centres treating burns believe early aggressiveexcision is the treatment of choice, and advances in intensive careand the development of skin substitutes have facilitated this.
Summaryx Full thickness injuries have no regenerative elements left.Unless they are very small they will take weeks to heal andundergo severe contraction. They should be referred forsurgery as early as possible.x Deep dermal injuries are unlikely to heal within three weeks.The incidence of unsightly hypertrophic scarring rises from33% to 78% if healing is delayed from three to six weeks.Therefore these injuries should also be excised and graftedwithin the first 5-10 days.x Superficial wounds should heal by regeneration within twoweeks. They should be cleaned, dressed, and reviewed onalternate days to optimise the wound healing environment. Anyburn not healed within two weeks should be referred forassessment.x Clean wounds can be dressed with a non-adherent primarydressing such as tulle gras or Mepitel and an absorbentsecondary dressing such as gauze or Gamgee Tissue.Antimicrobial agents are added where infection is likely(perineum, feet) or heavy colonisation is evident on thedressings or invasive infection is suspected.
Remo Papini is consultant and clinical lead in burns, West MidlandsRegional Burn Unit, Selly Oak University Hospital, Birmingham.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini; and Peter Dziewulski, consultantburns and plastic surgeon, St Andrews Centre for Plastic Surgery andBurns, Broomfield Hospital, Chelmsford. The series will be publishedas a book in the autumn.
Competing interests: RP has been reimbursed by Johnson & Johnson,manufacturer of Integra, and Smith & Nephew, manufacturer of Acticoatand TransCyte, for attending symposia on burn care.
BMJ 2004;329:158–60
Top: Deep dermalinjury from bath scald.Bottom: Six weeks aftertangential excision andgrafting with 3:1 meshand cultured epithelialautograft in suspension.Note biopsy site for cellculture on buttock
Major burn in elderly patient
Depth assessed (appearance, bleeding, capillary refill, sensation)
Superficial
(epidermal)
Dress with tulle
gras and gauze if
extensive until
healed (usually
within 1 week)
Superficial
partial thickness
Deep partial
thickness
Full
thickness
Dress with tulle
gras and gauze,
reassess at
48 hours
May be suitable for
Hypafix; wash
dressing daily and
take off with
oil in 1 week
Continue with tulle gras or Bactigras
and review every 2 days until healed
Contaminated
or signs
of infection?
Likely to heal
within 2-3 weeks?
Signs of improvement
or healing?
Dress with tulle
gras and gauze,
reassess at 48 hours
Apply antimicrobials (such as silver
sulfadiazine cream, antibiotics) Need to refer
Obvious deep
dermal injury?
Re-dress and review
every 2 days
Requires surgery -
refer to burns unit
Unhealed at
2 weeks?
No
No Yes
Yes
Yes No
Low exudate? High exudate?
Yes
No
Requires surgery,
preferably within
5 days, unless
<1 cm2 in area in a
non-essential area
Algorithm for assessing depth of burn wounds and suggested treatment
Clinical review
160 BMJ VOLUME 329 17 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsIntensive care management and control of infectionMark Ansermino, Carolyn Hemsley
Intensive care management
The goal in management of an acute burn is to limit the extentof the systemic insult. Intensive care management should not beseen as rescue for failed initial treatment but as a preventivemeasure in patients at high risk of organ failure. Intensive careunits have the resources for improved monitoring and expertisein managing acute physiological changes. Intensive caremanagement should not, however, become an obstacle to earlyaggressive surgical excision of the burn wound, which isassociated with improved outcome.
Airway burnsThe term “inhalational injury” has been used to describe theaspiration of toxic products of combustion, but also moregenerally any pulmonary insult associated with a burn injury.Patients with cutaneous burns are two to three times more likelyto die if they also have lower airway burns. Death may be adirect result of lung injury but is usually due to the systemicconsequences of such injury. It may be impossible to distinguishlung injury caused at the time of the burn directly to the lungsby a burn from injury due to the systemic consequences of theburn.
Diagnosis of lower airway burns is largely based on thepatient’s history and clinical examination. Clinicians shouldhave a high index of suspicion of airway burns in patients withone or more of the warning signs. Special investigations willsupport clinical suspicion. However, severity of injury orprediction of outcome is not aided by additional tests.
The pathophysiology of airway burns is highly variable,depending on the environment of the burn and the incompleteproducts of combustion. The clinical manifestations are oftendelayed for the first few hours but are usually apparent by 24hours. Airway debris—including secretions, mucosal slough, andsmoke residue—can seriously compromise pulmonary function.
There is no specific treatment for airway burns other thanensuring adequate oxygenation and minimising iatrogenic lunginsult. Prophylactic corticosteroids or antibiotics have no role intreatment.
Control of the airway, by endotracheal intubation, isessential before transporting any patient with suspected airwayburn. Rapid fluid administration, with inevitable formation ofoedema, may lead to life threatening airway compromise ifcontrol of the airway is delayed. Endotracheal intubation beforeoedema formation is far safer and simpler. Oxygen (100%)should be given until the risk of carbon monoxide toxicity hasbeen excluded, since high concentrations of oxygen will clearcarbon monoxide from the body more rapidly thanatmospheric concentrations. Importantly, carbon monoxidetoxicity may result in a falsely elevated pulse oximetrysaturation.
Airway burns are associated with a substantially increasedrequirement for fluid resuscitation. Reducing the fluid volumeadministered, to avoid fluid accumulation in the lung, results ina worse outcome. Invasive monitoring may be required to guidefluid administration, especially with failure to respond toincreasing volumes of fluid. Adequate oxygen delivery to all thetissues of the body is essential to prevent multi-organ failure.
Patient with burns in intensive care unit. Note the bilateral slings raising theburnt hands, air fluidised mattress, warm air heater, haemofiltration, andventilator
Warning signs of airway burns
Suspect airway burn if:x Burns occurred in an enclosed spacex Stridor, hoarseness, or coughx Burns to face, lips, mouth, pharynx, or nasal mucosax Soot in sputum, nose, or mouthx Dyspnoea, decreased level of consciousness, or confusionx Hypoxaemia (low pulse oximetry saturation or arterial oxygen
tension) or increased carbon monoxide levels ( > 2%)
Onset of symptoms may be delayed
Mechanisms of pulmonary insult after lower airway burns
x Mucosal inflammationx Mucosal burnx Bronchorrhoeax Bronchospasm
x Ciliary paralysisx Reduced surfactantx Obstruction by debrisx Systemic inflammatory response
Bronchoscopy image showing mucosal inflammation
This is the seventh in a series of 12 articles
Clinical review
220 BMJ VOLUME 329 24 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Aggressive airway toilet is essential. Diluted heparin andacetyl cystine nebulisation may be helpful. Early surgicaldebridement, enteral feeding, mobilisation of the patient, andearly extubation are desirable. Antibiotics should be reservedfor established infections and guided by regular microbiologicalsurveillance.
Several ventilatory strategies have been proposed toimprove outcome following airway burns. Adequate systemicoxygenation and minimising further alveolar injury is theprimary clinical objective. Prolonging survival will permitspontaneous lung recovery.
Intensive monitoring—The intensive care environmentfacilitates rapid, graded response to physiological disturbance.Frequent reassessment, based on a range of clinical andmonitored parameters, should guide treatment. Fluidadministration should not be guided by calculated fluidrequirements alone. Failure to respond to treatment shouldtrigger an escalation in the invasiveness of the monitoring.
Heart failureMyocardial dysfunction is a potential consequence of majorburn injury. It has been attributed to a circulating myocardialdepressant factor, primarily causing myocardial diastolicdysfunction. It may also be caused by myocardial oedema.
Administration of an inotropic agent is preferable tooverloading a failing myocardium with large volumes of fluid.However, the inotropic drug can produce vasoconstriction inthe burn wound, reducing the viability of critically injuredtissue. Inotropic drugs should not be used until adequate fluidresuscitation has been ensured (usually by invasive monitoring).Inotropic drugs that do not produce vasoconstriction (such asdopexamine or dobutamine) will preserve wound viability,providing they do not produce unacceptable hypotension.
Kidney failureEarly renal failure after burn injury is usually due to delayed orinadequate fluid resuscitation, but it may also result fromsubstantial muscle break down or haemolysis. Delayed renalfailure is usually the consequence of sepsis and is oftenassociated with other organ failure.
A reduced urine output, despite adequate fluidadministration, is usually the first sign of acute renal failure.This will be followed by a rise in serum creatinine and ureaconcentrations. Early renal support (haemodialysis orhaemodiafiltration) will control serum electrolytes andaccommodate the large volumes of nutritional supplementationrequired in a major burn.
Cerebral failureHypoxic cerebral insults and closed head injuries are notuncommonly associated with burn injuries. Fluid administrationfor the burn injury will increase cerebral oedema andintracranial pressure. Monitoring intracranial pressure may helpin minimising the adverse effects of trying to achieve twocontradictory treatment goals.
NutritionBurn injury is associated with a considerable hypermetabolicresponse, mediated by the systemic response to the burn andrelated to the extent of the burn injury. The hypermetabolismmay result in a resting energy expenditure increase in excessesof 100% of basal metabolic rate. Even small burns can beassociated with hyperpyrexia directly due to hypermetabolism.
Only limited success has been achieved in reducing thehypermetabolic state, which may persist for many months.Close attention to nutritional needs is critical to prevent proteinbreakdown, decreased wound healing, immune suppression,and an increase in infective complications.
Airway burns—key clinical points
x Restricting fluids increases mortalityx If in doubt, intubatex Give 100% oxygen until carbon monoxide
toxicity excludedx Ventilatory strategies to avoid lung injury (low
volume or pressure)x Aggressive airway toiletx Early surgical debridement of woundsx Early enteral feeding
Possible ventilatory strategies for patientswith airway burns
x Low volume ventilationx Permissive hypercapniax High frequency percussive ventilationx Nitric oxidex Surfactant replacementx Partial liquid ventilation (experimental)x Extracorporeal membrane oxygenation (limited
application)
End points to guide fluid administration
x Vital signs (blood pressure, heart rate, capillaryrefill)
x Urine outputx Peripheral perfusion (temperature gradient)x Gastric mucosal pHx Serum lactate or base deficitx Central venous pressure or pulmonary capillary
wedge pressurex Cardiac output—oxygen delivery and
consumption
Myoglobinuria in patient after receiving high tensionelectrical burns
Management of the hypermetabolic response
x Reduce heat loss—environmental conditioningx Excision and closure of burn woundx Early enteral feedingx Recognition and treatment of infection
Clinical review
221BMJ VOLUME 329 24 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Energy requirements are proportional to the size of theburn and should be met by enteral nutrition, and this should beestablished as soon as possible after the burn injury. Totalparenteral nutrition is associated with immunosuppression, anincrease in infective complications, and reduced survival.Glutamine, arginine, and omega 3 fatty acid supplementationmay improve immunity and gut function.
Infection in burns patientsAfter the initial resuscitation, up to 75% of mortality in burnspatients is related to infection. Preventing infection, recognisingit when it occurs, and treating it successfully presentconsiderable challenges. Infective pulmonary complications arenow the commonest types of infection seen in burns patients,but infection is common in many other sites. Several factorscontribute to the high frequency and severity of infection atmultiple sites in burns patients:x Destruction of the skin or mucosal surface barrier allowsmicrobial accessx Presence of necrotic tissue and serosanguinous exudateprovides a medium to support growth of microorganismsx Invasive monitoring provides portals for bacterial entryx Impaired immune function allows microbial proliferation.
Deciding whether infection is present can be difficult. Burnspatients have an inflammatory state from the injury itself thatcan mimic infection. Extensive microbial colonisation ofwounds makes interpretation of surface cultures difficult.Patients may have open wounds and repeated episodes ofinfection over weeks. Excessive use of antibiotics will encouragethe appearance of resistant colonising organisms. A sensibleapproach is to limit antibiotic use to short courses of drugs withas narrow a spectrum of activity as is feasible.
PathogenesisThe burn injury destroys surface microbes except for Grampositive organisms located in the depths of the sweat glands orhair follicles. Without prophylactic use of topical antimicrobialagents, the wound becomes colonised with large numbers ofGram positive organisms within 48 hours. Gram negativebacteria appear from three to 21 days after the injury. Invasivefungal infection is seen later.
The microbiology reflects the hospital environment andvaries from centre to centre. In general there has been a changein the main infective organisms over time from � haemolyticstreptococci to resistant Gram negative organisms includingpseudomonas, resistant Gram positive organisms, and fungi.
Tube feeding in burns patients
x In all patients with burns covering more than20% of total body surface area
x Established during initial resuscitationx Early enteral feeding improves success in
establishing feedingx Nasojejunal feeding will bypass gastric stasis
Risk factors for pneumonia
x Inhalational injury:a) Destruction of respiratoryepithelial barrierb) Loss of ciliary function andimpaired secretion clearancec) Bronchospasmd) Mucus and cellular plugging
x Intubation
x Circumferential, full thicknesschest wall burnsDecreased chest wall compliance
x Immobilityx Uncontrolled wound sepsis
Can lead to secondarypneumonia from haematogenousspread of organisms from wound
Eyes
Secondary infection
of corneal burns
Sinuses and middle ear
Complications of
nasogastric feeding
Supparative chondritis
Ear commonest site
Intra-abdominal
Rare
Infective endocarditis
Risk from transient
bacteraemias secondary
to manipulation of burn
wound and line placement
Septic thrombophlebitis
Complications of long
line placement
Pneumonia
Burn wound
Urinary tract infection
Common with urinary
catheters and for
burns to perineum
Sites of potential infection in a burns patient
Streptococcal cellulitis in a superficial burn wound
Pseudomonal colonisation of a grafted burn wound ona thigh (note vivid green coloration of dressing)
Causative agents of wound infection
Bacteria� haemolytic streptococci—Such as Streptococcus pyogenes. Cause acute
cellulitis, and occasionally associated with toxic shock syndromeStaphylococci—Such as methicillin resistant Staphylococcus aureus
(MRSA). Cause abscesses and subeschar pusGram negative bacteria—Such as Pseudomonas aeruginosa, Acinetobacter
baumanii, Proteus species. Mini epidemics seen in specialisedcentres secondary to antibiotic pressure
FungiCandida—Most common fungal isolate, act as surface colonisers but
have low potential for invasionFilamentous fungi—Such as Aspergillus, Fusarium, and phycomycetes.
Can be aggressive invaders of subcutaneous tissues. Treatmentmust include debridement of infected tissue
VirusesHerpes simplex—Characterised by vesicular lesions
Clinical review
222 BMJ VOLUME 329 24 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Preventing invasive wound infectionOne aim of initial wound management is to prevent invasiveinfection. To this end, aggressive surgery and the use of topicalantimicrobial agents are effective. Topical antimicrobialtreatment slows wound colonisation and is of use early, beforedefinitive surgery. A wide selection of agents are available: silversulfadiazine is the most frequently used. Early closure of theburn wound by surgical techniques then lessens the surfacearea available for further microbial colonisation and subsequentinfection.
Prophylactic use of systemic antibiotics is controversial. Mostagree that prophylactic penicillin against group A streptococcalsepsis is not indicated, and broad spectrum antibiotics to coverwound manipulation are not required in patients with burnscovering less than 40% of total body surface area.
Diagnosing invasive wound infectionSurface swabs and cultures cannot distinguish wound infectionfrom colonisation. Wound biopsy, followed by histologicalexamination and quantitative culture, is the definitive method.However, it is time consuming and expensive, making itimpractical as a routine diagnostic technique. Diagnosis ofinfection therefore relies heavily on clinical parameters, with theaid of blood, surface, or tissue cultures to identify likelypathogens.
TreatmentWhen invasive infection of a burn wound is suspected, empiricalsystemic antimicrobial treatment must be started. Topicaltreatment alone is not sufficient, as it does not effectivelypenetrate the eschar and damaged tissue. The choice ofantibiotic depends on the predominant flora on the unit. Thiscan be adjusted later depending on culture and sensitivityresults of relevant specimens. Necrotic and heavily infectedmaterial must be removed by surgical excision.
Infection controlInfection control measures help to minimise cross infectionbetween patients and acquisition of nosocomial pathogens(such as MRSA or multiresistant Gram negative bacteria). Strictisolation of every patient is impractical, but universalprecautions are an absolute necessity.
Mark Ansermino is paediatric anaesthesiologist, British Columbia’sChildren’s Hospital, Vancouver, Canada. Carolyn Hemsley is specialistregistrar in infectious diseases and microbiology, John RadcliffeHospital, Oxford.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burns Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrew’s Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.
Competing interests: See first article for series editors’ details.
BMJ 2004;329:220–3
Advantages and adverse effects of topical antimicrobials
Silver sulfadiazinex Water soluble creamx Advantages—Broad spectrum, low toxicity, painlessx Adverse effects—Transient leucopenia, methaemoglobinaemia (rare)
Cerium nitrate-silver sulfadiazinex Water soluble creamx Advantages—Broad spectrum, may reduce or reverse
immunosuppression after injuryx Adverse effects—As for silver sulfadiazine alone
Silver nitratex Solution soaked dressingx Advantages—Broad spectrum, painlessx Adverse effects—Skin and dressing discoloration, electrolyte
disturbance, methaemoglobinaemia (rare)
Mafenidex Water soluble creamx Advantages—Broad spectrum, penetrates burn escharx Adverse effects—Potent carbonic anhydrase inhibitor—osmotic
diuresis and electrolyte imbalance, painful application
Signs of wound infection
x Change in wound appearance:a) Discoloration of surrounding skinb) Offensive exudate
x Delayed healingx Graft failurex Conversion of partial thickness wound to full
thickness
Key points
x Fluid resuscitation must be based on frequent reassessment.Formulas are only a guide
x Pulse oximetry readings may be normal in carbon monoxidetoxicity
x Unnecessary intubation is preferable to systemic hypoxiax Early enteral nutrition in major burns may improve survivalx Burn patients are at high risk of infection, and there are many sites
for infective complicationsx Antibiotics should be used wisely to limit emergence of
multiresistant organisms: close liaison with a clinical microbiologistis crucial
Further reading
x Still JM Jr, Law EJ. Primary excision of the burn wound. Clin PlastSurg 2000;27:23-8
x Desai MH, Mlcak R, Richardson J, Nichols R, Herndon DN.Reduction in mortality in pediatric patients with inhalation injurywith aerosolized heparin/N-acetylcystine [correction ofacetylcystine] therapy. J Burn Care Rehabil 1998;19:210-2
x Pruitt BA, Mc Manus AT, Kim SH, Goodwin MD. Burn woundinfections. World J Surg 1998;22:135-45
x Monafo WM, West MA. Current treatment recommendations fortopical therapy. Drugs 1990;40:364-73
x Warren S, Burke JF. Infection of burn wounds: evaluation andmanagement. Curr Clin Top Infect Dis 1991;11:206-17
Clinical review
223BMJ VOLUME 329 24 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsBurns reconstructionJuan P Barret
The basic concerns in burns reconstruction are for function,comfort, and appearance. Normal and hypertrophic scarring,scar contracture, loss of parts of the body, and change in colourand texture of injured skin are processes common to allseriously burnt patients and yet unique to each.
A realistic approach is necessary to harmonise patients’expectations (which are very high) with the probable outcomesof reconstructive surgery. Burn reconstruction starts when apatient is admitted with acute burns and lasts until the patient’sexpectations have been reached or there is nothing else to offer.However, even when this time has come, the patient-surgeonrelationship may still continue and can last a lifetime.
Any surgeon undertaking burn reconstruction must havegood understanding of wound healing and scar maturation toplan the time of reconstruction, and sound knowledge of allsurgical techniques and all the aftercare required (usually inconjunction with a burn team). A strong patient-surgeonrelationship is necessary in order to negotiate a master plan andagree on priorities.
Time of reconstruction
Definitive correction of burn scarring should generally bedelayed for a year or more after scar healing. Unsightly scarsmature over time, and, with the help of pressure and splints,many of them do not require surgery once the acute phase ofscar maturation is over. Patience is often the best tool of areconstructive surgeon. However, certain problems must bedealt with before scar maturation is complete. In burnreconstruction there are urgent procedures, others that areessential, and many that are desirable. It is for the last groupthat a good patient-surgeon relationship is necessary fornegotiation on which procedures take priority.
Urgent procedures—Waiting for scar maturation isinappropriate when it is certain that an operation is needed tocorrect a deformity or if vital structures are exposed or can beseverely damaged. Urgent procedures should be restricted tothose needed to correct function for injuries that are notsuitable for other treatments. Examples include an eyelidrelease to protect an exposed cornea, correction of distracted orentrapped neurovascular bundles, severe fourth degreecontractures, and severe microstomia.
Essential procedures—Although they are not urgent since noimportant structure or the patient’s overall health is challenged,essential procedures may, if performed early, improve thepatient’s final appearance and rehabilitation. Such proceduresinclude operations for all burn scar contractures that do notrespond to rehabilitation, and hypertrophic scarring andcontractures that prevent a patient from eating, bathing,moving, or performing everyday activities.
Desirable reconstructive procedures—Most of the problems thatpatients may present fall in this category. These are oftenaesthetic problems and scars contractures that, although notprominent, produce great discomfort. For all desirableprocedures, it is good practice to wait until all red and immaturescars have disappeared before starting any kind of surgery. Anearly operation is often unnecessary in these circumstances.
Top: Burn scarcontracture on theanterior axillary line.Planned Z-plasties forcontracture release areshown.Middle: The scar hasbeen incised and allflaps raised.Bottom: Closure of theZ-plasties after rotationof all flaps. Note that thescar contracture hasbeen released and thescar lengthened. Thismethod increases thetissue availability in thereconstructed area andincreases the range ofmotion
Techniques for use in acute phase of scar maturation todiminish reconstructive needs
x Use of darts in escharotomies whencrossing joints
x Use sheet grafts when possiblex Use aesthetic units to face and
hands with medium thickness splitskin grafts
x Use of splints, face masks, andsilicone inserts as soon as possible
x Place seams following skintension lines
x Place grafts transverselyover joints
x Early pressure therapyx Early ambulation and
exercise
Timing of burn reconstructive surgery
Urgent proceduresx Exposure of vital structures (such as eyelid releases)x Entrapment or compression of neurovascular bundlesx Fourth degree contracturesx Severe microstomia
Essential proceduresx Reconstruction of function (such as limited range of motion)x Progressive deformities not correctable by ordinary methods
Desirable proceduresx Reconstruction of passive areasx Aesthetics
This is the eighth in a series of 12 articles
Clinical review
274 BMJ VOLUME 329 31 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Patient-surgeon relationshipThe relationship between a burns patients and a reconstructiveburn surgeon is normally long lasting, often continuing for alifetime. Patients not only require a surgeon’s professionalexpertise, but also time, a good dose of optimism, andcompassion.
The initial meeting is one of the most important events. Thepatient presents a set of problems, and the reconstructive surgeonhas to evaluate these and the patient’s motivation for surgery andpsychological status. We have to remember, though, that thepatient will also evaluate the surgeon’s attitude and conduct.
Although deformities or chief complaints will often beapparent and ready for surgery, it is preferable to have furthervisits before surgery, to allow new queries to be addressed andunhurried preparation for surgery. Photographic workup isextremely important to assist in definitive preoperativeplanning and for documentation.
Patients need frequent reassurance. A reconstructivesurgeon needs to know a patient’s fears and feelings as thereconstructive plan goes on. A burn reconstruction projectcommonly requires more than 10 operations and many clinicvisits over a long period before a final assessment is made. Inthe case of a small child, this may take more than 18 years.Patients’ feelings and impressions must be addressedcontinuously, and any trouble, minor disappointment, ordepression detected early and treated as needed.
Burn reconstructive visitOne of the most important events during burn reconstructionis the burn reconstructive visit. At that time, a complete andaccurate overview of the problems and possible solutions isperformed in the following step wise manner:x Obtain as complete a record of the acute hospitalisation aspossiblex Take a thorough history and make a full physical examinationx Make a complete record of all encountered problems. Notequality and colour of the skin in the affected areas—abnormalscars, hyperpigmentation or hypopigmentation, contractures,atrophy, and open woundsx Consider function. Explore all affected joints and note rangesof motion. Outline any scar contracture extending beyond jointsx Consider skeletal deformities. Scar contractures may distractjoints and the body maintain an abnormal position toovercome the deformity. This is particularly true in children; theeffect of traction on a growing joint and bone can create longterm deformitiesx Consider needs for physiotherapy, occupational therapy, andpressure garments. If any of these devices will be needed aftersurgery the patient must be referred to the rehabilitationdepartment for considerationx Make an inventory of all possible sites for donor tissue.
Once a patient has voiced all his or her chief complaintsand a thorough examination of the patient has been done, amaster plan is developed. All reconstructive possibilities arediscussed with the patient, and the timing and order of suchprocedures are outlined.
Surgical proceduresBurn reconstructive surgery has advanced in recent decades,though not as dramatically as in other areas of plastic surgery.For many years, burn reconstructive surgery comprisedincisional or excisional releases of scars and skin autografting.Nowadays, however, the first approach that should beconsidered is use of local or regional flaps. These provide new
Top: Unstable burn scars with chronic open wounds on medial malleolus.Bottom: The scars were excised and the defect reconstructed with a freevascularised perforator based skin flap. In this case skin from the thigh wastransplanted to the ankle with microsurgical vascular anastomosis. Thesetechniques allow the transplantation of any tissue (skin, fascia, fat, functionalmuscle, and bone) in the same patient
Essentials of burn reconstruction
x Strong patient-surgeon relationshipx Psychological supportx Clarify expectationsx Explain prioritiesx Note all available donor sitesx Start with a “winner” (easy and quick operation)x As many surgeries as possible in preschool yearsx Offer multiple, simultaneous proceduresx Reassure and support patient
Incisional release of a severe neck contracture. Scar releases leave substantialtissue losses that require extensive skin autografting. Although scar releaseis still the first choice for some difficult contractures, flap reconstruction andmobilisation of adjacent tissues should be attempted to decrease the size ofthe defect to be grafted
Clinical review
275BMJ VOLUME 329 31 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

and vascularised tissue to the area, they grow in children, andthey give the best functional and cosmetic results. Such flapscan be raised either with normal skin or with burn scar. Eventhough burnt tissue generally has a high tendency tocongestion, ischaemia, and necrosis, it can be used as a reliableflap if extreme care is taken while raising the flap and theinjured skin is left attached to the underlying tissues.
When planning surgery for a burnt patient, a surgeon mustconsider what is the patient’s primary complaint, what tissuesare left, what parts are missing, and what sort of donor sites areavailable. This will help to determine the techniques availablefor burn reconstruction. The patient’s chief complaint orcomplaints need to be carefully evaluated. If immature scars oran increasing deformity is present, and no urgent or essentialprocedure is required, pressure garments and occupational andphysical therapy are indicated. If the deformity is stable andthere is a need for reconstruction, an inventory of donor sitesand priorities should be made.
Dealing with deficiency of tissueAt this point, the burn injury must be assessed for deficiency intissue. If there is no deficiency and local tissues can be easilymobilised, excision and direct closure or Z-plasties can beperformed.
If, however, there is a deficiency in tissue, the problem ofhow to reconstruct underlying structures must be addressed. Ifthe deformity affects the skin and subcutaneous tissues, skinautografting, Z-plasties, and all the modifications of them (suchas trident flaps) are advised. When reconstruction of underlyingstructures is necessary, flaps should be considered, includingdirect cutaneous, musculocutaneous, perforator based, andexpanded flaps and microvascular transfer of tissues (free flaps).The precise choice is made on an individual basis.
In addition, composite grafts and bone or cartilage grafts areoften necessary in order to perform a complete reconstruction.The use of alloplastic materials in these circumstances is notadvisable because of their tendency to extrusion.
SummaryEven though incisional or excisional release and skinautografting (with or without use of dermal templates) are stillthe main techniques used in burn reconstruction, flaps shouldbe used when possible (remember that Z-plasty and itsmodifications are transposition flaps). The burn reconstructionplan needs to be tailored to the individual patient and thepatient’s chief complaint, since certain anatomical areas arebetter suited to some techniques than others.
Juan P Barret is consultant plastic and reconstructive surgeon, StAndrews Centre for Plastic Surgery and Burns, Broomfield Hospital,Chelmsford.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burn Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrews Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.Competing interests: See first article for series editors’ details.
BMJ 2004;329:274–6
Techniques for burn reconstruction
Without deficiency of tissuex Excision and primary closurex Z-plasty
With deficiency of tissuex Simple reconstructionx Skin graftx Dermal templates and skin grafts
Transposition flaps (Z-plasty and modifications)x Reconstruction of skin and underlying tissues
Axial and random flapsMyocutaneous flapsTissue expansion
x Free flapsx Prefabricated flaps
1 2
A
B
A
B
3
Traditional Z-plasty to release a burn scar contracture. (1) The burn scar,showing the skin tension lines. (2) Z-plasty is performed by rotating twotransposition flaps with an angle of 60° with the middle limb of the Z on thescar. (3) Final appearance after insetting of flaps. Note the lengthening ofthe tissue and the change of scar pattern. Z-plasties can be combined withother flaps (five limb Z-plasty, seven limb Z-plasty, etc)
Expansion of normal skin by means of inflatable prostheses implanted insubcutaneous tissue. These are inflated with saline over several weeks untilenough extra skin has been created. The expanded skin is then mobilised asfull thickness skin grafts, regional advancement flaps, or free flaps. Theseprovide large amounts of normal skin to resurface scarred areas
Further readingx Herndon DN, ed. Total burn care. 2nd ed. London: WB Saunders, 2002x Engrav LH, Donelan MB. Operative techniques in plastic and
reconstructive surgery. Face burns: acute care and reconstruction. London:WB Saunders, 1997
x Achauer BM. Burn reconstruction. New York: Thiene, 1991
x Barret JP, Herndon DN. Color atlas of burn care. London: WBSaunders, 2001
x Brou JA, Robson MC, McCauley RL. Inventory of potentialreconstructive needs in the patient with burns. J Burn Care Rehabil1989;10:555-60
Clinical review
276 BMJ VOLUME 329 31 JULY 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsRehabilitation after burn injuryDale Edgar, Megan Brereton
Prevention of scarring should be the aim of burn management.For every member of the burn team, rehabilitation must startfrom the time of injury. Having a substantial burn injury isfrightening, particularly as patients will not know what to expectand will be in pain. Consistent and often repetitive education isa vital part of patient care. Oedema management, respiratorymanagement, positioning, and engaging patients in functionalactivities and movement must start immediately. Patients needto be encouraged to work to their abilities and acceptresponsibility for their own management. Functional outcome iscompromised if patients do not regularly engage in movement.
Pain controlIn order to achieve desired outcomes and movement habits,ensuring adequate pain control is important. The aim ofanalgesic drugs should be to develop a good baseline paincontrol to allow functional movement and activities of dailyliving to occur at any time during the day. The use of combinedanalgesics such as paracetamol, non-steroidal anti-inflammatorydrugs, tramadol, and slow release narcotics reduces the need forincreasing doses of narcotics for breakthrough pain. Codeineshould be avoided if possible because of its negative effects ongut motility. Other pain control methods that may be helpfulinclude transcutaneous electrical nerve stimulation (TENS).
Inhalational injuryAggressive, prophylactic chest treatment should start onsuspicion of an inhalational injury. If there is a history of burnin a closed space or the patient has a reduced level ofconsciousness then frequent, short treatments should begin onadmission. Treatment should be aimed at removing lungsecretions (oedema), normalising breathing mechanics, andpreventing complications such as pneumonia.
Initial treatment should include:x Normalisation of breathing mechanics—such as using apositive expiratory pressure device, intermittent positivepressure breathing, sitting out of bed, positioningx Improving the depth of breathing and collateral alveolarventilation—such as by ambulation or, when that is not possible,a tilt table, facilitation techniques, inspiratory holds.
Movement and functionMovement is a habit that should be encouraged from admissionto the burns unit. If a patient can accept the responsibility of selfexercise and activities of daily living then the most difficultaspects of rehabilitation are easily achieved. If there is suspectedtendon damage from the burn, then protected movement isappropriate and resting splints may be necessary.
Oedema managementOedema removal should be encouraged from admission. Theonly body system that can actively remove excess fluid anddebris from the interstitium is the lymphatic system. Oedema
Functional use of a positive expiratory pressure deviceto improve breathing mechanics (top) and practisingactivities of daily living to exercise a burnt limb(bottom)
Strengthening exercise for a patient who had sustained a high tensionelectrical flash burn to the right upper limb and right lateral trunk.Rehabilitation to restore function focuses on upper limb strength and trunkcore stability
This is the ninth in a series of 12 articles
Rehabilitation starts onthe day of injury
Clinical review
343BMJ VOLUME 329 7 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

collection in the zone of stasis of a burn may promote theprogression of depth of a burn. The principles of reduction ofoedema should be adhered to in totality and not just in part:x Compression—such as Coban, oedema glovesx Movement—rhythmic, pumpingx Elevation or positioning of limbs for gravity assisted flow ofoedema from themx Maximisation of lymphatic functionx Splinting does not control oedema except to channel fluid toan immobile area.
ImmobilisationStopping movement, function, and ambulation has its place. Itshould be enforced only when there is concomitant injury totendon or bone or when tissues have been repaired (includingskin reconstruction). If a body part must be immobilised—toallow skin graft adherence, for example—then the part shouldbe splinted or positioned in an anti-deformity position for theminimum time possible.
Skin reconstructionSkin reconstruction is tailored to the depth of burn found at thetime of surgery. The application and time frames ofreconstruction techniques utilised will be dependent onattending surgeon’s preference. Other factors influencingchoice of management include availability and cost ofbiotechnological products.
Scar managementScar management relates to the physical and aestheticcomponents as well as the emotional and psychosocialimplications of scarring.
Hypertrophic scarring results from the build up of excesscollagen fibres during wound healing and the reorientation ofthose fibres in non-uniform patterns.
Keloid scarring differs from hypertrophic scarring in that itextends beyond the boundary of the initial injury. It is morecommon in people with pigmented skin than in white people.
Scarring is influenced by many factors:x Extraneous factors—First aid, adequacy of fluid resuscitation,positioning in hospital, surgical intervention, wound anddressing managementx Patient related factors—Degree of compliance withrehabilitation programme, degree of motivation, age,pregnancy, skin pigmentation.
Management techniquesPressure garments are the primary intervention in scarmanagement. Applying pressure to a burn is thought to reducescarring by hastening scar maturation and encouragingreorientation of collagen fibres into uniform, parallel patternsas opposed to the whorled pattern seen in untreated scars.
Garments need to be tailored to patients’ requirements andare often influenced by the type of surgery completed. Patientsshould generally be measured for garments at five to seven daysafter grafting surgery, and these should be fitted as soon as theyare available. A pressure garment lasts for about three months;after that time it is helpful to re-measure patients frequently toaccommodate the changing dimensions of the scar.
If people have moderate to severe burns around the neck orface, an acrylic face mask must be considered. This providesconforming pressure over the face and neck. Material maskscan also be made for patients to wear at night.
Compression glove (Coban)
Immobilisation times for different types of skinreconstruction
Reconstruction method Depth of burnLength of
immobilisation
Biological dressings (such asBiobrane, TransCyte)
Any (preferably notfull thickness)
< 24 hours
Cultured epithelial autograft(suspension)
Superficial tointermediate
24-48 hours
Split skin graft Intermediate todeep partial
thickness
3-5 days
Dermal substitutes (such asIntegra, Alloderm)
Deep partialthickness to full
thickness
5-7 days
Fasciocutaneous ormyocutaneous flaps
Full thickness 7-14 days
Example of hypertrophic scarring
Acrylic face mask providing conforming pressure overburns to the face and neck
Clinical review
344 BMJ VOLUME 329 7 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

For areas of persistent scarring that have not responded wellto pressure garments, further scar management techniquesmust be considered. These include the use of massage,moisturising creams, and contact media.
Team education of scar managementBecause of the altered functions of the skin after a burn,patients should be continually encouraged to maintain a goodmoisturising regimen. Moisturising is important as it preventsthe skin from drying out and then splitting and cracking, whichmay lead to secondary infection and breakdown of the skin.
Education on sun protection is also important for patients.Patients must be made aware that they need to protectthemselves from the sun for up to two years and that they willneed to keep their skin protected and covered in sun screen(and appropriate clothing) if working or playing outside.
Outpatient follow upA burns unit team should offer outpatients regular andcomprehensive follow up reviews. The type of follow uprequired obviously depends on the severity of the burn, but interms of movement and function, patients require regularmonitoring and updating of their prescribed exercise regimenand home activity programme.
Therapists who do not regularly treat burns patients requireexperienced support to achieve the expected outcomes. Thisshould include written, verbal, and visual communications aswell as monitoring of management plans.
ConclusionThe rehabilitation of burns patients is a continuum of activetherapy. There should be no delineation between an “acutephase” and a “rehabilitation phase”—instead, therapy needs tostart from the day of admission (and before if possible).Education is of paramount importance to encourage patients toaccept responsibility for their rehabilitation. A consistentapproach from all members of the multidisciplinary teamfacilitates ongoing education and rehabilitation.
Dale Edgar is senior physiotherapist in Burns and Plastic Surgery andMegan Brereton is occupational therapist in the Upper LimbRehabilitation Unit, Royal Perth Hospital, Perth, Australia.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burn Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrew’s Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.
Competing interests: See first article for series editors’ details.
BMJ 2004;329:343–5
Scar management techniques in addition to pressure
x Massage—Helps to soften restrictive bands of scar tissue, makes scarareas more pliable
x Silicone gel sheets (contact media)—Mode of action not known;possibly limits the contraction of scars through hydration,occlusion, and low molecular weight silicone
x Elastomer moulds (contact media)—Used to flatten areas ofscarring where it is difficult to encourage silicone to mouldeffectively (such as toes and web spaces between them)
x Hydrocolloids (contact media)—As for silicone sheets, except thatthese may be left in situ for up to 7 days. Massage can be giventhrough thin sheets
x Moisturising creams—Combined with massage to compensate forlost secretory functions of skin; protect against complications fromskin cracking
x Ultrasound—Low pulsed dose aimed at progressing theinflammatory process more rapidly
Endurance training by a burns outpatient
Further reading
x Schnebly WA, Ward RS, Warden GD, Saffle JR. A nonsplintingapproach to the care of the thermally injured patient. J Burn CareRehabil 1989;10:263-6
Clinical review
345BMJ VOLUME 329 7 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsPsychosocial aspects of burn injuriesShelley A Wiechman, David R Patterson
With the increased survival of patients with large burns comes anew focus on the psychological challenges and recovery thatsuch patients must face. Most burn centres employ socialworkers, vocational counsellors, and psychologists as part of themultidisciplinary burn team. Physiological recovery of burnpatients is seen as a continual process divided into threestages—resuscitative or critical, acute, and long termrehabilitation. The psychological needs of burn patients differ ateach stage.
Resuscitative or critical stageThe psychological characteristics of this stage include stressorsof the intensive care environment, uncertainty about outcome,and a struggle for survival. The intensive care environment canbe both overstimulating and understimulating with themonotony of lying in a hospital bed for weeks.
Cognitive changes such as extreme drowsiness, confusion,and disorientation are common during this phase. More severecognitive changes such as delirium and brief psychotic reactionsalso occur, usually as a result of infections, alcohol withdrawal,metabolic complications, or high doses of drugs. Patients mayalso be intubated, which greatly limits direct communication.
TreatmentIn depth psychological intervention is of minimal value at thisphase, since physical survival is the primary goal. Patientsshould be encouraged to cope with the frighteningly unusualcircumstances of the intensive care unit through whateverdefences are available to them, even primitive strategies such asdenial and repression. Supportive psychological interventionsshould focus on immediate concerns, such as sleep, paincontrol, and protecting patients’ coping strategies.Non{pharmacological approaches to pain control, such ashypnosis and relaxation, can be effective.
Medical staff can also effectively intervene during this earlystage of recovery by working with a patient’s family members.Family members may be anxious and distressed while observingthe patient undergo treatment, which fosters the same responsein the patient. It is important to help family membersunderstand this effect and help them to convey a sense of hopeand calmness to the patient.
Acute stageThe acute phase of recovery focuses on restorative care, butpatients continue to undergo painful treatments. As patientsbecome more alert during this phase, they face theseprocedures with less sedation. Also, patients are more aware ofthe physical and psychological impact of their injuries.
Depression and anxiety—Symptoms of depression and anxietyare common and start to appear in the acute phase of recovery.Acute stress disorder (occurs in the first month) andpost{traumatic stress disorder (occurs after one month) aremore common after burns than other forms of injury. Patientswith these disorders typically have larger burns and more severepain and express more guilt about the precipitating event. Theseverity of depression is correlated with a patient’s level ofresting pain and level of social support.
With the increased survival of patients with large burns, there is increasedfocus on the psychological challenges and recovery that such patients mustface
Psychological characteristics of critical stageof recovery from a burn
Challengesx Overstimulationx Understimulationx Delirium, confusion, and disorientationx Impaired communicationx Sleep disturbancex Pain
Treatmentsx Protect patient’s natural defences and coping
strategiesx Drug management for pain control and to help
with sleepx Non-pharmacological techniques for pain
managementx Educate and provide support to family membersx Educate and provide support to staff
Prevalence of depression and anxiety ininpatients with burns
Condition Prevalence
Depression 23-61%
Generalised anxiety 13-47%
Post-traumatic stress disorder 30%
This is the 10th in a series of 12 articles
The psychological needs ofpatients with burn injuriesare unique at each stage ofphysical recovery
Clinical review
391BMJ VOLUME 329 14 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Sleep disturbance—Central to both anxiety and depression issleep disturbance. The hospital environment can be loud, andpatients are awakened periodically during the night foranalgesia or for checking vital signs. Patients’ mood, agitation,and nightmares can all affect sleep.
Premorbid psychopathology—Compared with the generalpopulation, burn patients have a high rate of premorbidpsychopathology. Patients with pre-existing psychopathologytypically cope with hospitalisation through previouslyestablished dysfunctional and disruptive strategies. The mostcommon premorbid psychiatric diagnoses are depression,personality disorders, and substance misuse. Priorpsychopathology can have an adverse impact on outcomes,including longer hospitalisations and the development of moreserious psychopathologies after injury.
Grief—Patients may now begin the grieving process as theybecome more aware of the impact of the burn injuries on theirlives. Family members, friends, or pets may have died in theincident, and patients may have lost their homes or personalproperty. In addition to these external losses, patients may alsogrieve for their former life (such as job, mobility, physical ability,appearance). Mental health professionals and other staff shouldhelp patients to grieve in their own way and at their own pace.
TreatmentBrief psychological counselling can help both depression andanxiety, but drugs may also be necessary. When offeringcounselling, it is often helpful to provide reassurance thatsymptoms often diminish on their own, particularly if thepatient has no premorbid history of depression or anxiety.
Drugs and relaxation techniques may also be necessary tohelp patients sleep. Informing patients that nightmares arecommon and typically subside in about a month can help allayconcerns. Occasionally patients will benefit from being able totalk through the events of the incident repeatedly, allowingthem to confront rather than avoid reminders of the trauma.Staff often make the mistake of trying to treat premorbidpsychopathology during patients’ hospitalisation. Referrals tocommunity treatment programmes should be made oncepatients are ready for discharge.
Pain controlBoth procedural and background pain can be challenging forpatients and staff. Some patients report that procedural pain iseasier to cope with because of its transient nature, whereas withbackground pain there is no clear end in sight. It is importantto conduct a thorough pain assessment in order to determinewhich type of pain is the greatest problem.
A pain treatment plan that provides pharmacological andnon-pharmacological approaches should be established. Opioidagonists are the most commonly used analgesics. Long actingopiates are used for background pain, and short acting opiatesare used for painful procedures such as wound care. It is crucialthat drugs for background pain are provided on a fixed doseschedule to maintain control of the pain. Opioid analgesics maybe supplemented with other drugs, including inhaled nitrousoxide and anxiolytics. Lorazepam has recently been found tolessen burn pain, largely by treating acute anxiety.
Non-pharmacological pain control techniques includecognitive{behaviour therapy and hypnosis. These have beenshown to be effective in treating procedural pain. One excitingnew distraction technique is virtual reality. Since attentionalfocus is limited and a person cannot attend to more than onestimulus at a time, virtual reality creates a realistic environmentfor patients to absorb themselves in during painful procedures,thus taking focus away from the discomfort.
Psychological characteristics of acute stage of recovery froma burn
Challengesx Pain—both background and proceduralx Anxiety—both acute stress disorder and post-traumatic stress
disorderx Depressionx Sleep disturbancex Premorbid psychopathology becomes more apparentx Grief
Treatmentsx Drug management of anxiety, pain, sleeplessness, and depressionx Brief counsellingx Teach non-drug approaches to pain management (relaxation,
imagery, hypnosis, virtual reality)
Time (hours)
Dru
g c
on
cen
trat
ion
in b
loo
d
0 6 12 18 24
No pain ormental clouding
Mental clouding andother side effects = Injection of opiate
Pain
Effects of fixed dose schedule of analgesic drugs for pain control
A patient’s attention is taken up with “SnowWorld” via a water-friendlyvirtual reality helmet during wound care in the hydrotub
Clinical review
392 BMJ VOLUME 329 14 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Long term rehabilitationThe long term stage of recovery typically begins after dischargefrom hospital, when patients begin to reintegrate into society.For patients with severe burns, this stage may involve continuedoutpatient physical rehabilitation, possibly with continuation ofprocedures such as dressing changes and surgery. This is aperiod when patients slowly regain a sense of competence whilesimultaneously adjusting to the practical limitations of theirinjury. The first year after hospitalisation is a psychologicallyunique period of high distress.
Physical problems—Patients face a variety of daily hasslesduring this phase, such as compensating for an inability to usehands, limited endurance, and severe itching. Severe burninjuries that result in amputations, neuropathies, heterotopicossification, and scarring can have an emotional and physicaleffect on patients.
Psychosocial problems—In addition to the high demands ofrehabilitation, patients must deal with social stressors includingfamily strains, return to work, sexual dysfunction, change inbody image, and disruption in daily life. Many people continueto have vivid memories of the incident, causing distress. Patientsmay also develop symptoms of depression. There is evidencethat adjustment to burn injuries improves over timeindependent of the injury size. Social support is an importantbuffer against the development of psychological difficulty.
TreatmentIt can be helpful to make follow up telephone calls to patientsafter discharge or to continue to see patients in an outpatientclinic to screen for symptoms of distress and to providepsychotherapy.
Adjustment difficulties that persist more than a year afterdischarge usually involve perceptions of a diminished quality oflife and lowered self esteem. Some studies suggest that burndisfigurement in general leads to decreased self esteem inwomen and social withdrawal in men. “Changing Faces” is asuccessful programme for enhancing self esteem. This includesa hospital based programme for image enhancement and socialskills plus a series of publications for patients dealing withaspects of facial disfigurement.
Many patients face a lengthy period of outpatient recoverybefore being able to return to work. Some patients go throughvocational challenges. In a recent study of patients hospitalisedfor burn injury 66% returned to work within six months of theirinjury, and 81% had returned by one year. As expected, patientswho sustained larger burns took longer to return to work.About half of the patients required some change in job status.
Ancillary resources such as support groups and peercounselling by burn survivors can also be important services toburn survivors. Major burn centres ideally have a network of burnsurvivors who are willing to talk with patients in the hospital.
SummaryA burn injury and its subsequent treatment are among the mostpainful experiences a person can encounter. The emotionalneeds of patients with burns have long been overshadowed bythe emphasis on survival. Patients undergo various stages ofadjustment and face emotional challenges that parallel thestage of physical recovery. Adjustment to a burn injury seems toinvolve a complex interplay between the patient’s characteristicsbefore the injury, moderating environmental factors, and thenature of the injury and ensuing medical care.
The picture of a patient with burnt head and shoulders is reproduced withpermission of Science Photo Library.
Psychological characteristics duringrehabilitation stage of recovery from a burn
ChallengesPhysical—Itching, limited endurance, decrease in
functionSocial—Changing roles, return to work, body image,
sexual issuesPsychological—Anxiety, depression
Treatmentsx Outpatient counsellingx Social skills trainingx Support groupsx Peer counsellingx Vocational counselling
Changing Faces (United Kingdom) and the PhoenixSociety (United States) are excellent sources ofinformation and support for burn survivors
Further reading
x Patterson DR, Everett JJ, Bombardier CH, Questad KA, Lee VK,Marvin JA. Psychological effects of severe burn injuries. Psychol Bull1993;113:362-78
x Patterson DR, Ford GR. Burn injuries. In: Frank RG, Elliott TT, eds.Handbook of rehabilitation psychology. Washington DC: AmericanPsychological Association, 2000:145-62
x Partridge J. When burns affect the way you look. London: ChangingFaces, 1997
Shelley A Wiechman is acting assistant professor and David RPatterson is professor in the Department of Rehabilitation Medicine,University of Washington School of Medicine, Seattle, USA.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burn Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrew’s Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.
Competing interests: See first article for series editors’ details.
BMJ 2004;329:391–3
Clinical review
393BMJ VOLUME 329 14 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsBurns in the developing world and burn disastersRajeev B Ahuja, Sameek Bhattacharya
Burns in the developing worldDeveloping countries have a high incidence of burn injuries,creating a formidable public health problem. High populationdensity, illiteracy, and poverty are the main demographic factorsassociated with a high risk of burn injury. The exact number ofburns is difficult to determine: judicious extrapolation suggeststhat India, with a population of over 1 billion, has 700 000 to800 000 burn admissions annually. The high incidence makesburns an endemic health hazard. Social, economic, and culturalfactors interact to complicate the management, reporting, andprevention of burns.
EpidemiologyThe epidemiology of burn injuries is different from that in thedeveloped world. Most burn injuries are sustained by womenaged 16-35 years. Women of this age group tend to be engagedin cooking, and most work at floor level in relatively unsafekitchens and wear loose fitting clothes such as saris, dupatta, etc.Children and elderly people are at relatively less risk becausemany households still exist as joint families, and the systemsafeguards these age groups to some extent.
The commonest mode of burn injury is a flame burn. Mostsuch incidents are related to malfunctioning kerosene pressurestoves. These are cheap contraptions without safety features,and burns occur when carbon deposits block the kerosenevapour outlets. Unsupervised and careless handling offirecrackers during the festival of Diwali lead to an increasedincidence of injuries during the festival period. Fire is also usedin homicide and suicide.
Problems in managementBurn management in developing countries is riddled withdifficulties. Lack of government initiative and low literacy ratespreclude effective prevention programmes. Many uneducatedhouseholds are fraught with superstition, taboos, weird religiousrituals, and faith in alternative systems of “medicine,” whichcomplicates management.
Most burn centres are situated in large cities and areinadequate for the high incidence of injuries. Resuscitation isoften delayed as patients have to travel long distances andtransport facilities are poor. Many burn centres are also plaguedwith lack of resources, lack of operating time, and shortage ofblood. Often there are no dedicated burn surgeons, and generalsurgeons without formal training are involved in burn care.Burn nursing is also not a recognised concept. These conditionsmake excisional surgery impossible for a large percentage ofpatients. There is generally no coordination between districthospitals and tertiary burn centres.
Strategies for effective burn care in developing countriesThe approach to burn management has to be radically differentfrom that in Western countries.
Prevention programmesPrevention programmes should be directed at behavioural andenvironmental changes which can be easily adopted intolifestyle. The programmes need to be executed with patience,persistence, and precision, targeting high risk groups.
Cooking at floor level in loose fitting clothes such as“dupatta” places women at increased risk of burn injury
Cheap kerosene cooking stoves, which are prone tomalfunction, are a common cause of burns
Unsupervised use of fireworks by children duringfestivals such as Diwali increases the incidence of burnsduring the festival period
Burn management problems in developingcountries
x High incidence of burnsx Lack of prevention programmesx Inadequate burn care facilitiesx Lack of resourcesx Lack of trained staffx Poor infrastructure and coordinationx Social problems
This is the 11th in a series of 12 articles
Clinical review
447BMJ VOLUME 329 21 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Depending on the population of the country, burnsprevention could be a national programme. This can ensuresufficient funds are available and lead to proper coordination ofdistrict, regional, and tertiary care centres. It could also providefor compulsory reporting of all burn admissions to a centralregistry, and these data could be used to evaluate strategies andprevention programmes. There should be adequate provisionby law to set manufacturing standards for heating and electricalequipment, fire safety standards for high rise buildings, andprocedures for storage and transportation of hazardousmaterials, explosive chemicals, and firecrackers. A national bodyof burn professionals should be constituted to educate allhealthcare staff involved in burn care.
Providing treatmentTo provide optimal burn care to a large population with limitedresources, it is imperative to strengthen the existinginfrastructure. A few regional burn centres should be developedto provide tertiary management and training to burn care staff.General surgeons working in district hospitals should form thenucleus of the burn care service and decide on referralprocedures.
If it is not possible to keep referred patients at burn centresfor six to eight weeks of treatment, they can be discharged aftertwo or three weeks of stabilisation. Such patients can then betreated at district hospitals or at home with the help of primaryhealth centres. Thus, primary health centres can act as liaisonbetween burn patients and district hospitals. The incidence ofburn wound septicaemia with domiciliary treatment isremarkably low. These patients can be readmitted as necessaryfor blood transfusions, treating septicaemia, and skin grafting.
Certain well tested and cost effective treatment proceduresneed to be adopted to conserve resources: these include usingParkland formula for resuscitation, pursuing conservative burnwound management, and using amnion as a biological dressing.
Burn disastersA disaster is a situation that is unpredictable, massive, and posesan immediate threat to public health. A burn disaster is “anevent resulting in mass burn casualties and severe loss ofhuman lives and material from a known thermal agent.”Disasters normally exceed the resources of local healthcarefacilities.
Disaster management involves coordinating the activities ofvarious health disciplines to prevent disasters, provide animmediate response to a disaster, and help in rehabilitation ofvictims.
Disaster planAn organised disaster plan can reduce loss of property, socialdisruption, and suffering. A disaster plan should be specificallytailored for a particular region and nature of fire disaster.Ultimately, a coordinated system must be developed thatincludes medical and public safety organisations, law and orderagencies, and transport agencies.
The communication lines from the central command shouldbe fast and multilingual. It should be able to advise workers at thedisaster site, direct transport agencies, and simultaneously relaythe information to surrounding hospitals. All the regional anddistant hospitals must be incorporated in a multi-tier system asthe number of cases may overwhelm local facilities.
Hospitals play a pivotal role in providing trained staff. Alldoctors and nurses, irrespective of their specialties and whetherthey are included in the plan, should be educated about thebasics of burn care. With a burn specialist at the core, the
Strategies for burn management indeveloping countries
x Effective prevention programmesx Burns as national health agendax Central registry of burnsx Create a professional burn groupx Adequate safety legislationx Induct district hospitals and primary health
centresx Encourage patient management at homex Cost effective treatment proceduresx Develop regional centres of excellence
Cost effective burn treatments to conservescare resources
Parkland formula for fluid resuscitationThis is cost effective and ensures proper compliance
Conservative burn wound managementThis involves using closed dressings, eschar
separation, and skin grafting. This takes thepressure off operating facilities and providescomparable results to surgery
Amnion as a biological dressingThis is easily available, is free of cost, and can be
comfortably preserved for a week
Characteristics of a burn disaster
x Large number of patients withextensive burn injuries
x A high incidence of seriousassociated injuries
x Site of the disaster is not alwaysaccessible
x Immediate care andassistance may not be adequate
x Response time may beprolonged
x Local infrastructure may beaffected by fire
Principles of disaster management
x Preventionx Disaster profilesx Disease patternsx Risk assessmentx Post-emergency phase
x Effective multidisciplinary responsex Mobilisation of workforce resourcesx Local community or national
involvementx Reconstructive phase
Factors to be considered while developing a disaster plan
x Unpredictabilityx Characteristics (explosion,
building fire, toxic fumes, etc)x Type of building (dwelling, hotel,
office, etc)x Type of trauma (burn, associated
injury, inhalational injury)
x Time (day, night, duringfestivities, etc)
x Area (city, non-urban,accessibility, etc)
x Number of people injuredx Degree of preparedness to
manage a disaster
Burn centremedical staff
Supervise careat disaster site
Treat casesin hospital
Provideambulances
Control patientflow by triage
Role of hospital in disaster management
Clinical review
448 BMJ VOLUME 329 21 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

hospital disaster management team also includes a respiratoryphysician and an anaesthetist. There should be prompt andjudicious deployment of staff. Teams of psychologists shouldmanage panic among disaster victims and their relatives both atthe disaster site and at hospitals. Accurate triage by cliniciansexperienced in burns must guide the flow of patients from thesite to the inner circle of healthcare facilities (primary andsecondary care hospitals) and then to the outer circle (tertiarycare hospitals and burn centres).
Transportation needs are guided by the number of victims,their condition, the nature of the fire disaster, and geographicalconsiderations. Possible modes of transport includeambulances, local transport vehicles, military vehicles,helicopters, fixed wing aircraft, and rescue boats.
Managing a disasterImmediate care is provided by people present at the scene ofthe disaster, who may be survivors or passers by. These firstresponders are later guided by trained healthcare workers whoarrive at the site. On site management includes first aid, patienttriage, and ambulance staging with a basic aim of maximal useof resources.
TriageTriage is the cornerstone of effective burn disaster managementand is done at the disaster site by staff with knowledge of burntreatment. Triage takes into consideration the total number ofpatients, bed availability, and transportation capacity.
Triage should be prognostic, and patients should becategorised on the basis of age, extent of burns, site of burnsand presence of inhalational injury:x Group I—Minor burns (< 10% of total surface area in
children, < 20% in adults) to non-critical areasAssigned to—Outpatient care, dressing, tetanus prophylaxis
x Group II—Minor burns to critical sites (face, hands, genitalia)Assigned to—Short hospital stay, special wound care oroperation
x Group III—Major burns (20-60%)Assigned to—Admission to burn unit, intravenousresuscitation
x Group IV—Extensive burns ( > 60%)Assigned to—Lower priority for transfer
x Group V—Minor burns with inhalational injury or associatedinjuryAssigned to—Oxygen, intubation, transfer to intensive careunit.The patients in groups III and V are evacuated first,
followed by group IV. Group II cases are evacuated at the end.Group I cases are either discharged after first aid or asked tomake their own way to the nearest primary care centre.
Further treatmentInitial care is in the line of ABC of resuscitation. An adequateairway and respiration must be ensured. All patients exceptthose with minor burns must receive fluid resuscitation basedon a simple formula. Wounds should be covered with a sterilesheet until they are dressed. Dressings should be simple, withonly antimicrobial pads and Gamgee Tissue. Effort should bemade to detect and treat associated injuries.
Secondary triage may also be done at this time. If necessary,seriously injured patients can be sent to centres of higherlevel while less serious patients who reach the tertiary centresare referred back to primary care centres. The success ofsuch a plan lies in accurate triage at every level, so that allcentres are used optimally and best possible treatment isdelivered to all according to the severity of injury, withminimum delay.
Central commandand communication
Immediatecare
Coordinatetransport
Furthertreatment
Furthertreatment
Triage
Relay information
Provide trained staff
Burncentre
Secondarycare hospital
Major arms of a disaster plan
First aid at the site of a burn disaster
x Quantitative assessment of burnsx Qualitative assessment of burnsx Commence intravenous resuscitationx Catheterisationx Analgesiax Hospital transfer
Further reading
Burns in the developing worldx Davies JWL. The problem of burns in India. Burns 1990;17(suppl
1):S2-22x Sawhney CP, Ahuja RB, Goel A. Burns in India: epidemiology and
problems in management. Ind J Burns 1993;1:1-4x Ahuja RB. Managing burns in India—focussing on newer strategies.
Ind J Burns 1995;3:1-7x Ahuja RB, Bhattacharya S. An analysis of 11 196 burn admissions
and evaluation of conservative management techniques. Burns2002;28:555-61
Burn disastersx Watchel TL, Dimick AR. Burn disaster management. In: Herndon
DN, ed. Total burn care. Philadelphia: WB Saunders, 1998:19-32x Hadjiiski O. Behaviour during a mass industrial burn disaster. Ann
Burn Fire Disaster 1996;9:232-7x Masellis M, Gunn SWA. Thermal agent disaster and burn disaster:
definition, damage, assessment and relief operation. Ann Burn FireDisaster 1991;4:215-9
Rajeev B Ahuja is head of department and Sameek Bhattacharya isspecialist in the Department of Burns, Plastic, Maxillofacial, andMicrovascular Surgery, Lok Nayak Hospital and associated MaulanaAzad Medical College, New Delhi, India.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burn Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrew’s Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.
Competing interests: See first article for series editors’ details.
BMJ 2004;329:447–9
Clinical review
449BMJ VOLUME 329 21 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

ABC of burnsWhen we leave hospital: a patient’s perspective of burn injuryAmy Acton
At the age of 18, I thought I had the best summer job possible,working outside at the local marina, with the prospect of goingto college in a few months to become a nurse. In an instanteverything changed. While moving a boat on a trailer, a groupof us sustained electrical injuries when the mast hit a hightension power line. I found myself fighting for my life in a burnscentre and mourning the loss of a friend. The physical healingwas gruelling and at times overwhelming for me and my family,and the medical team was a great support for me. However, thisarticle focuses on the problems I faced once I left the hospital,two and a half months later, because that was toughest part ofmy journey.
My comments are both personal and from the perspectiveof having been a burn nurse for over 13 years. It is a sharedstory of healing the emotional scars of burn injuries because Ihave learnt so much from others. One such person is BarbaraKammerer Quayle, a fellow burn survivor and colleague I metafter I became a burn nurse. She taught me how healthcareprofessionals could make a difference for survivors strugglingto regain a place in their family and society. Many of thestrategies I discuss are her life’s work and are used with herpermission. For some burn survivors these strategies are naturalresponses, but for others they have to be learnt and practised.
Facing the worldWhile in the secure cocoon of the burn centre, I receivedextraordinary social support and acceptance from staff. Aftermy discharge and return to my community, however, I feltsurprised, shocked, and sometimes completely overwhelmed asI realised I would face the curious stares of strangers. I hadremained focused on my physical healing and had neverthought about how my burns would affect my life long term.Addressing this issue with patients and families must becomepart of the discharge process from burns centres.
Before my burn injury, I passed through shops, restaurants,churches, and social occasions with minimal interest fromothers. Now, wearing splints and pressure garments, I found allof that had changed. I was not prepared for this and had noidea of how to cope with people’s reactions. It was not untilalmost two years later that I felt comfortable in social settings, asI learnt to love my body again and realised that I could make abig difference to how others responded by my attitude.
Attitudes about appearanceFrom childhood onward, we develop our attitudes aboutappearance. We possess a complex set of beliefs about whatappearance means in our life. These beliefs are the result of ourthoughts and influences by parents, teachers, friends,magazines, films, and television.
When my appearance was altered by my burns it threatenedmy existing thoughts and beliefs about my appearance and whoI was. Over time, I and many other burn survivors do accept thealteration in our appearance, and incorporate the changes intoa healthy body image, and go on to live successful lives. Thistakes time, support, self love, and learning new behaviouralskills. For some, it is a lifelong struggle.
Pressure garments stimulate reactions such as staresand questions
This is the last in a series of 12 articles
Clinical review
504 BMJ VOLUME 329 28 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

Staring: a fact of lifeStaring is part of human nature. Heads turn to look atteenagers with tattoos and body piercing, people with hearingimpairments signing, those using wheelchairs. It is a fact of lifethat looking different gets attention. Staring has power andmeaning only to the degree to which we give it meaning andpower over our lives.
I gradually found that most people stare because they areunfamiliar with burn injuries and feel compassion and concern.Others are simply curious. A few stare because they areoverwhelmed by such a traumatic injury, and the fewest starebecause they are rude.
What we see depends on what we are looking forThe way we choose to interpret and perceive stares willinfluence our ability to cope with them. If we focus ourattention on staring and perceive stares as evil and threatening,then that will be our experience. If, however, we diminish theimportance of staring and interpret stares as a mildinconvenience, that will be our experience. Our interpretationsand perceptions either defeat or enhance our social success.
Faulty assumptionsIn his book The Body Image Workbook Thomas Cash states that itis flawed thinking to assume that, simply because they noticeyou, people will dislike you: “friendliness, kindness, andconversational skills” are “more influential than whatever mightbe different about your looks.” Instead, the truth is that “you arethe one noticing what you don’t like about your appearance.”Other people usually do not care because they are thinkingabout other things.
In the first months after my burn injury, I wore clothing tohide my injuries and continually looked to see if people were“looking” at me. People staring and seeing my scars became thefocus of my attention, and I felt uncomfortable in social settings.I spent much of my energy worrying what others thought. Manyburn survivors have reported the same behaviour.
Cash also points out that “first impressions don’t always last”and “our initial reactions to someone’s appearance are notfrozen forever in our minds.” A person may focus on a burnsurvivor’s appearance initially. I consider this pretty normal.When I meet another burn survivor for the first time, I oftentake a few minutes to “get used to” the new and unique skinpatterns I am seeing. After we have established a relationship,however, the burns become less important, and personal traitssuch as intelligence, humour, integrity, and sensitivity are themost defining characteristics. Often I forget exactly where aperson’s burns are located—which side of the face, which hand,etc. By strengthening our social skills, we can overcome thechallenge of looking “different.”
So what do I do?Barbara Quayle has developed some simple strategies to helpthose with physical differences respond in a positive way toquestions and staring. By practising these strategies, many burnsurvivors have become more comfortable in social settings.These techniques are easily taught to patients before dischargefrom hospital, and they should be part of the care plan for allburn survivors.
“STEPS”If you find yourself being stared at, Barbara suggests standingup straight, looking directly into the person’s eyes, smiling, and,with a friendly tone of voice, saying “Hi, how are you doing?” or“Hi, how’s it going?” or even “Hi, great day, isn’t it?” Looking at
Reasons why people stare at burn survivors
Clinical review
505BMJ VOLUME 329 28 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from

and speaking to the person shows social awareness and selfconfidence. When you project confidence and poise the personstaring usually responds in a friendly manner, looks away, andgoes on with his or her business. When a stare triggers acomfortable and confident response, the person is sometimessurprised and often a little embarrassed about staring.Remember, you are in control, not the person staring. Becomeconscious of your own behaviour.
If eye contact, smiling, and speaking seem like too much atfirst, simply “look ’em in the eye” and smile. Energy and warmthradiate from faces wearing smiles. People who smile at othershave advantages in forming relationships because a smile oftendispels the fear and apprehension of strangers. In newsituations a smile can break barriers or end prejudicialjudgments. It sends a message of being approachable and atease. A smile also diminishes the visual intensity of scarring andskin discoloration. The STEPS acronym will help you rememberto take control and not “act like a victim.”
Another alternative is simply to ignore the person staringand go about your business. Sometimes this may be preferableif you are tired or not bothered by the stare. I never advocatereacting to staring with an angry response. Anger at othersoften hurts most the person who is angry. When you respondwith anger it is usually out of fear and says more about you thanthe person staring. There will be times when you or a protectivefamily member want to lash out verbally at someone staring, butbeing abusive does not reflect well on you or your family andmay leave you feeling frustrated, resentful, and bitter.
“Rehearse your responses”Another helpful technique that Barbara teaches is to beprepared for people’s questions. Often burn survivors and theirfamilies feel awkward, uncomfortable, angry, or embarrassedwhen strangers ask questions about their burns. If survivors candevelop a two or three sentence response to such questions andthen practise this in privacy with family and healthcareprofessionals, they will have greater confidence in new socialsituations.
It first must be a conscious effort. Then, as you “rehearseyour responses,” you find it becomes second nature, andeventually you become proud of your positive attitude and howyou handle social situations.
Healthcare professionals can helpIt is the responsibility of healthcare professionals to discussstaring with burn survivors and their families before discharge.They need to know that some people will stare, ask questions;and helping them to practise specific strategies to use in publicand in social situations can only assist them in making thesuccessful transformation to a person who thrives aftersurviving a burn injury.
Amy Acton is executive director of the Phoenix Society for BurnSurvivors, East Grand Rapids, MI, USA.
The ABC of burns is edited by Shehan Hettiaratchy, specialistregistrar in plastic and reconstructive surgery, Pan-Thames TrainingScheme, London; Remo Papini, consultant and clinical lead in burns,West Midlands Regional Burn Unit, Selly Oak University Hospital,Birmingham; and Peter Dziewulski, consultant burns and plasticsurgeon, St Andrews Centre for Plastic Surgery and Burns,Broomfield Hospital, Chelmsford. The series will be published as abook in the autumn.
Competing interests: AA is executive director of the Phoenix Society forBurn Survivors. See first article for series editors’ details.
BMJ 2004;329:504–6
Further reading
x Cash TF. The body image workbook. Oakland CA: New HarbingerPublications,1997
x Quayle BK. When people stare. Burn Support News2001;2(summer).
To learn more about support for burnsurvivors and to obtain articles by BarbaraKammerer Quayle and the PhoenixSociety, visit the society’s website atwww.phoenix-society.org
The picture of a pressure garment is used with permission of GottfriedMedical.
Clinical review
506 BMJ VOLUME 329 28 AUGUST 2004 bmj.com
on 30 September 2006 bmj.comDownloaded from
![A smart artificial bee colony algorithm with distance-fitness-based …hebmlc.org/UploadFiles/201872983541770.pdf · 2018. 7. 29. · abc. [] abc abc abc [] abc [abc abc [] abc [abc](https://static.fdocuments.in/doc/165x107/5febef9cecac5951281b206e/a-smart-artificial-bee-colony-algorithm-with-distance-fitness-based-2018-7-29.jpg)