AAP Alabama State Chapter Shared Vision James C. Wiley, MD, FAAP Chapter Physician Project Leader.
16
AAP Alabama State Chapter Shared Vision James C. Wiley, MD, FAAP Chapter Physician Project Leader
-
Upload
asher-rogers -
Category
Documents
-
view
213 -
download
0
Transcript of AAP Alabama State Chapter Shared Vision James C. Wiley, MD, FAAP Chapter Physician Project Leader.

AAP Alabama State Chapter Shared Vision
James C. Wiley, MD, FAAPChapter Physician Project Leader

“I have the following financial relationships with the manufacturers(s) of any commercial products(s) and/or provider
of commercial services discussed in this CME activity:”
Research Support from: Speakers’ Bureau: Glaxo Smith Kline and Behavioral Diagnostics
Co.
It is my obligation to disclose to you (the audience) that I am on the Speakers Bureau for Glaxo Smith Kline and Behavioral Diagnostics Co. However, I acknowledge that today’s activity is certified for CME credit and thus cannot be promotional. I will give a balanced presentation using the best available evidence to support my conclusions and recommendations.”

State Quality Improvement Strategic Plan
• Alabama Chapter-AAP QI Committee created
• Collaboration with Alabama Medicaid – Alabama Healthcare Improvement and Quality Alliance (AHIQA)
• Alabama Chapter Aim Statement• Future Endeavors

CQN Impact MAINE
OHIO
OREGON
ALABAMA

• Learn about Alabama’s QI Committee• Understand the “gap” in care• Understand why this work is important• Become familiar with the goals for this
project
Goals

Global AimWe will build a sustainable quality improvement infrastructure within the Alabama Chapter-AAP to achieve measurable improvements in the health outcomes of children within our member practices.
Specific AimFrom April 2009 to November 2010, we will lead a quality improvement collaborative and achieve measurable improvements in asthma outcomes with the participating 10 to 15 practices by implementing the National Heart, Lund and Blood Institute (NHLBI) asthma guidelines.
Alabama Chapter-AAP Individualized Aim Statement
SECTION 1 (AIMS)

Goal: 90% of the CQN Asthma Pilot Practices will achieve 80% perfect care by September 2010.
Goal: 90% of the CQN Asthma Pilot Practices will use a structured encounter form 90% of the time by September 2010.
Outcome Goal: 90% of the CQN Asthma Pilot Practices will reach 80% of patients “well controlled” by September 2010.
What is Optimal Asthma Care?Optimal Asthma Care - % of patients with all of the following:•patients with assessment of asthma control using a validated instrument•patients which stepwise approach is used to identify treatment options or adjust therapy•patients with asthma action plan •patients 6 months and older with a flu shot or flu shot recommendation
Alabama Chapter-AAP Individualized Aim Statement
SECTION 2 (GOALS)

Long Term Goals
Goal: All CQN Asthma Pilot Practices will use a population based registry
Goal: 90% of the CQN Asthma Pilot Practices using a population based registry will achieve 90% perfect care by August 2012
Other Action Items: •The CQN Asthma Pilot Practices will submit annual follow-up data in August 2011 and August 2012, with the Chapter Team providing quarterly check-in/follow-up calls/emails.•The CQN Asthma Pilot Practices will host an Asthma QI Project sharing session/summit at the Chapter’s 2011 Spring Meeting in April 2011•The chapter will push out results of the CQN project and lessons learned on QI infrastructure to Chapter members through a variety of communication efforts: newsletter tips, case studies, etc.•The chapter will collaborate with Alabama Medicaid Agency and Blue Cross Blue Shield of Alabama to design and fund a second phase of pilot practices based on results of this quality improvement project.
Alabama Chapter-AAP Individualized Aim Statement
SECTION 3 (LONG TERM GOALS)

Optimal Care
>90% of patients have “optimal” asthma care (all of the following)
• assessment of asthma control using a validated instrument
• stepwise approach to identify treatment options and adjust therapy
• written asthma action plan • patients >6 mos. of age with flu shot (or
flu shot recommendation)

Asthma Admissions/10K
0
2
4
6
8
10
12
14
Baseline Post
As
thm
a A
dm
iss
ion
s/1
0K
PHO
Comparison Group
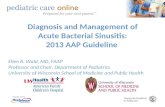
56%
36%
Baseline: 3 year average (10/1/00-9/30/03)
Post: 2 year average (10/1/06-9/30/08)
Commercial insurance only
CCHMC encounters only
Patients ≥ 2 yrs. of age
8 county primary service area
ICD-9 code of 493.xx in primary position
PHO vs. Comparison Group Asthma Admissions: Pre/Post Impact
Keith Mandel, MD; Cincinnati Children’s Hospital Medical Center
10

Change Concepts• Engaging Your Asthma QI Team and Your Practice *The QI team and practice is active and engaged in improving practice
processes and patient outcomes
• Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
• Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office *Care team is aware of patient needs and work together to ensure all
needed services are completed
• Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines implemented
• Providing Self management Support * Realized patient and care team relationship

Key Driver Diagram
GLOBAL CQN AIMWe will build a sustainable quality improvement infrastructure within our practice to achieve measurable improvements in asthma outcomesSpecific Aim From fall 2009 to fall 2010, we will achieve measurable improvements in asthma outcomes by implementing the NHLBI guidelines and making CQN’s key practice changes
Measures/Goals
Outcome Measures: >90% of patients well controlled
Process Measures >90% of patients have “optimal” asthma care (all of the following) assessment of asthma control using a validated instrument stepwise approach to identify treatment options and adjust therapy written asthma action plan patients >6 mos. Of age with flu shot (or flu shot recommendation)
>90% of practice’s asthma patients have at least an annual assessment using a structured encounter form
Engaging Your QI Team and Your Practice*The QI team and practice is active and engaged in improving practice processes and patient outcomes
Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office * CQN Encounter Form * Care team is aware of patient needs and
work together to ensure all needed services are completed
Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines
implemented
Providing Self management Support
* Realized patient and care team relationship
Key Drivers
Interventions
Form a 3-5 person interdisciplinary QI Team
Formally communicate to entire practice the importance and goal of this project
Meet regularly to work on improvement
All physicians and team members complete QI Basics on EQIPP
Collect and enter baseline data
Generate performance data monthly
Communicate with the state chapter and leaders within the organization
Turn in all necessary data and forms
Attend all necessary meetings and phone conferences
Select and install a registry tool
Determine staff workflow to support registry use
Populate registry with patient data
Routinely maintain registry data
Use registry to manage patient care & support population management
Select template tool from registry or create a flow sheet
Determine workflow to support use of encounter form at time of visit
Use encounter form with all asthma patients
Ensure registry updated each time encounter form used
Monitor use of encounter form
Select & customize evidence-based protocols for your office
Determine staff workflow to support protocol, including standing orders
Use protocols with all patients
Monitor use of protocols
Obtain patient education materials
Determine staff workflow to support SMS
Provide training to staff in SMS
Assess and set patient goals and degree of control collaboratively
Document & Monitor patient progress toward goals
Link with community resources
CQN Asthma Project Practice Key Driver Diagram Version 2.0

What is the Quality Gap?
• How QI came to me….
• The gap between the care we know is best and our ability to deliver it, every time, to every patient in the way they need it.

Defining the Gap: Asthma
• Affecting nine million children, childhood asthma is the most common serious pediatric chronic disease. The incidence of pediatric asthma continues to grow; it accounts for 14.7 million missed school days a year and 44% of all asthma hospitalizations[1]
• During August 2007, under the auspices of the National Heart, Lung, and Blood Institute (NHLBI) the National Asthma Education and Prevention Program (NAAEP) issued the first comprehensive update in a decade of asthma guidelines for the diagnosis and management of asthma (NHLBI asthma guidelines). The guidelines emphasize the importance of asthma control and introduce new approaches for monitoring asthma. The AAP recognizes that increased exposure to the new guidelines coupled with implementation support will decrease gaps in care and help move towards optimal care for children with asthma.
[1] American Academy of Allergy, Asthma and Immunology. http://www.aaaai.org/media/resources/media_kit/ asthma_statistics.stm

The Story of Improvement
Stephen Pleatman, MDPediatrician, Suburban Pediatric Associates, Inc.Board Member, Ohio Valley Primary Care Associates, L.L.C.Cincinnati, Ohio

Asthma Care a Year From Now
• Easier use of the asthma guidelines by physicians and staff
• Better understanding of asthma for patients and families
• Better systems so your office members can function as an efficient team
• Knowing your patients and being ready for their visits
• The best care for every patient, every time