AAO CONVO 2019 - American Academy of...
25
AAO CONVO 2019 : student presentations Edward G. Stiles, D.O., FAAODist. Prof. of OPP University of Pikeville Kentucky College of Osteopathic Medicine Sturgill Distinguished Professor University of Pikeville Where do I start my O.M.T. Treatment ? Finding the Key S/D !
Transcript of AAO CONVO 2019 - American Academy of...

AAO CONVO 2019: student presentations
Edward G. Stiles, D.O., FAAODist.Prof. of OPP
University of PikevilleKentucky College of Osteopathic Medicine
Sturgill Distinguished ProfessorUniversity of Pikeville
Where do I start myO.M.T.
Treatment ?
Finding the Key S/D !

“YOUR THEORY DETERMINES
WHAT YOU WILL SEE”ALBERT EINSTEIN
“YOUR PARADIGM DETERMINES . . .
ROBERT DAVIS
Sometimes when you learnsomething new,
you need a new paradigm

Paradigm Shift:2018
looking at familiar data, come to new understanding &new way of explaining old observations
“Learn the principles and
get them to work for you.”Paul E. Kimberly, DO, FAAO
• Anatomical design• OMT mechanisms

The Meso-Kinetic System
Musculo-Skeletal System a
21st. Century Design Perspective
BioTensegrity4

Tensegrity structures: human design•Light weight
•Much stronger than experts had predicted•Multi / Omni - directional
•Whole system adapts to stressors•Protects the “weakest link” / the A.G.R.
• defy gravity•Non-metallic materials, organized in a
Tensegrity arrangement, can conduct electricity
• ‘wired’: keep eyes level, evenly distributeweight among all 4 quadrants.•Conduct vibratory information
• appropriate design for whole body •Would it not make sense to identify,
the A.G.R. - H( area of greatest restriction - hindrance )
in thisflexible & adaptive system ?
7

BioTensegrity:21st Century
Paradigm
Components: derived from mesoderm / middle layer / “innerness”( posture & locomotor appartus / Pr. Machinery - I.M. Korr PhD )
•Non-touching compression struts – skeletal structures• Straight struts: traditional Tensegrity – systems contract when stressed• Curved struts: systems expand when stressed
•Body wide continuous network of tension system - muscles & fascia• Tensegrity: non-living wires or bungie like cords• BioTensegrity: living - fascia & muscles – Dynament design ( van der Waal )
•Remaining human body components:• Ectodermal derived: on the “out side” of middle layer• Endodermal derived: on the “inside” of middle layer - visceral / 2d machinery
The Fascia is the “Organ of Innerness” –A Holistic approach based upon phenomenological embryology & morphology.
van der wal, MD, PhD 2014
6

TENSEGRITYvan der Wal: brought architectural concepts to anatomy
•Tensional Integrity - Floating Compression
• “The skeleton is an
island of compression floated
in a balanced sea of tension”.
Tom Myers I.O.C. 2014 Berlin( total body )
•Fascia “is a fibrous collagenous tissue
which is part of a body wide tensional force transmission system”
( FRC 2009 definition )Mesodermal origin: in between layer / “innerness”
KEY: Dynament organization / dynamic functional potentialEnables postural & locomotion system function. 5

MESOKINETIC SYSTEM COMPLEXITYMeso ( mesoderm ): gives rise to
•Connective tissues & fascia•Cartilage
•Bone•Striated and smooth muscle
•Myocardium and pericardium•Blood and lymph vessels
•Kidneys and ureters•Adrenal cortex
•Gonads•Tubes, uterus and upper vagina
•Serous membranes lining the body cavities ( T, A & P )•GI fascial support system
•Spleen
Kinetic:Related to movement of physical objects
NOTE:S/D might impact both musculo-skeletal & visceral structures.
Netter’s Atlas of Human Embryology 8

MESOKINETIC SYSTEM COMPLEXITYMeso ( mesoderm ): gives rise to
•Connective tissues & fascia•Cartilage
•Bone•Striated and smooth muscle
•Myocardium and pericardium•Blood and lymph vessels
•Kidneys and ureters•Adrenal cortex
•Gonads•Tubes, uterus and upper vagina
•Serous membranes lining the body cavities ( T, A & P )•GI fascial support system
•Spleen
Kinetic:Related to movement of physical objects
NOTE:S/D might impact both mysculo-skeletal & visceral structures.
Netter’s Atlas of Human Embryology 9

Biomechanical paradigm shift to Biodynamics / Tensegrity:•Challenges the traditional block / column model of spine ( biomechanics )
•Block / column model proven to be unable to explain a lot of biological phenomena ( biodynamics needed )
•Same “tensegrity organized tissues” can bear up to 100% increased load !
Are D.O.’s / E.C.O.P. teaching E.B.M. spinal / bio-mechanics ?
10

Musculo-skeletal System: only SNS innervation !Mesokinetic System components: SNS and PNS innervation:
inc. complexity since combines both Pr. & Sec. machinery componentsplus serous lining of T, A & P . . . Think about visceral impact !
“Netter”: S.N.S & P.N.S. CHART expanded
X
X
X X
XX
X
11

“innerness” of van der Wal, MD, PhDMesodermal layer = inner layer ( “innerness” )
The system of posture and locomotion + some visceraDynament concept makes a BioTensegrity system very dynamic
“Netter”: S.N.S & P.N.S. CHART expanded
X
X
X X
XX
X
12

Passing on the TraditionAlan Becker, DO, FAAO 2010Journal of AAO – fall edition
•“Dr. Still was keen on being very specific.•He looked at the patient as a Totality.
•He looked for the Elusive Key Lesion – Hindrance ( somatic dysfunction )
that people have discussed for years”.
•That is what He looked for and
when He found it, He fixed it and then left it alone.He said that once done,
the body will do its own work because it is designed to do its own work.
•Our job is to find the Key Restriction – Hindrance
to homeostatic integrity,
and once restored to normalcy, to rest assured that the body will take care of the rest of the work”.
13

LBP patientA.G.R.
( Key somatic dysfunction )
( Stiles: 100 patients )• T/RC = 60%
• Lumbar = 24%• L.E. = 11%Total: 95%
Note:Sacrum
andinnominates were not the #1 A.G.R. !
( where many would start treating )
may have been treated later in the
treatment sequence
L.B.P.
Other possible A.G.R.s•Cranial: dural tube
•U.E.•L.E.
•Note: ever see a LBP research strategy which considered S/D
in T/RC, UE, LE or cranial ?
14
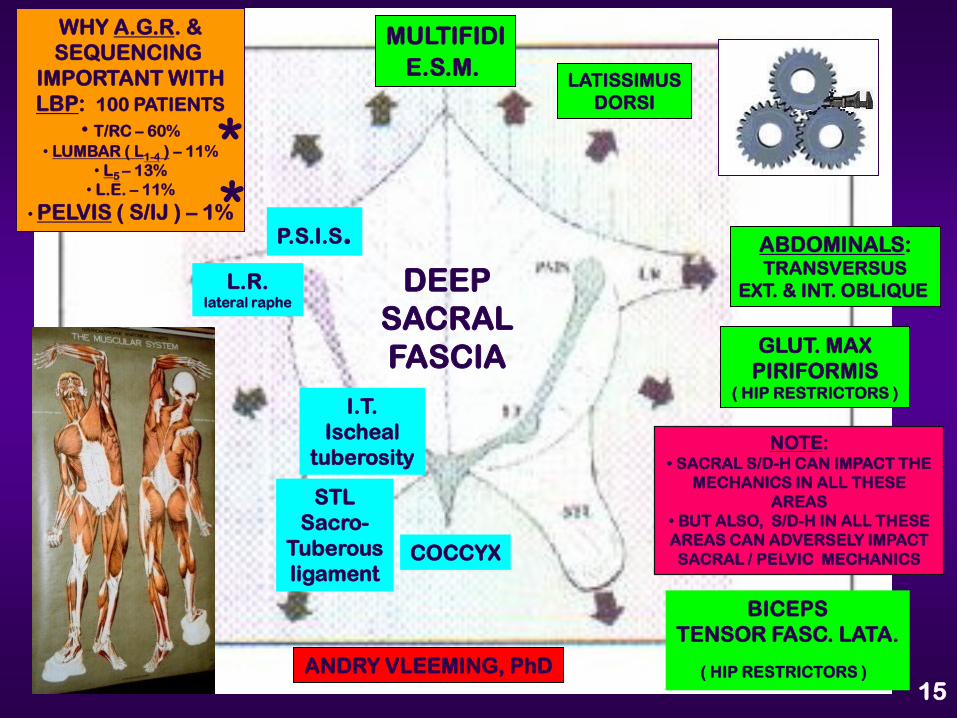
MULTIFIDIE.S.M.
LATISSIMUSDORSI
ABDOMINALS:TRANSVERSUS
EXT. & INT. OBLIQUE
GLUT. MAXPIRIFORMIS
( HIP RESTRICTORS )
P.S.I.S.
I.T.Ischeal
tuberosity
STLSacro-
Tuberousligament
BICEPSTENSOR FASC. LATA.
( HIP RESTRICTORS )
WHY A.G.R. &SEQUENCING
IMPORTANT WITHLBP: 100 PATIENTS
• T/RC – 60%• LUMBAR ( L1-4 ) – 11%
• L5 – 13%• L.E. – 11%
• PELVIS ( S/IJ ) – 1%
ANDRY VLEEMING, PhD
DEEPSACRALFASCIA
COCCYX
L.R.lateral raphe
15
NOTE:• SACRAL S/D-H CAN IMPACT THE
MECHANICS IN ALL THESE AREAS
• BUT ALSO, S/D-H IN ALL THESE AREAS CAN ADVERSELY IMPACT SACRAL / PELVIC MECHANICS
**

In light of this complexity,how do you clinically view your patients ?
Stiles’ Current Perspectivecomplex, dynamic,
inter-connected, inter-woven,containing multiple, simultaneously functioning systems,
non-linear,autopoietic
functional unit.
LBP
16

the Meso-Kinetic System
is acomplex non-linear system.
Biomechanics ( is linear ) whereas Biodynamic ( is non-linear )
EXAMPLE: a common joint
can take on unpredicted motion characteristics once inserted into a tensegrity system. 17

Fascia Research Congress
Berlin, Germany
Nov. 13-15, 2018also
International Osteopathic
and
Inter-DisciplinaryKongress
BerlinNov. 16-18, 2018
FRC abstract reviewer’s comments:“good, well conceived study,
innovative & valuable.”Over 300 abstracts submitted
( 70 selected for posters )
18

CLINICAL RESEARCH DATASUPORTING
THE
SCREENINGAND
A.G.R. – HSTRATEGY
•Gracovetsky – SpinoScope: inter-segmental motion improvement
•sEMG & “butterfly”& C.O.P.: M.A.P.’s / “firing patterns” improvement.
•Ground Reactive Force: total body motion evaluation changes.
•Statistical & Fractal significance: 80% during 1st visit
•Golfers: performance immediately improved
• 3 elite female runners: < strike force by av. 7-10 lbs.
•DARI: Tampa 8/10-12/2018
2018 FRC committee: “good, well designed, innovative & valuable.”26

elite female runner # 1• Cc: B/L tight , painful gluts
x 4 yrs.• Left upsheared innominate
• L3 FRSL• T8 ERSL
• L. posterior innominate• Right on right gait
restriction• “my gluts are relaxed”• “my glut pain is gone”
If there is any whitebetween the lines:
it is statisticallySignificant
( 2 SD )Green = pre – seq. OMTGray = post – seq. OMT

Data Significance:• Both pre and post sequenced curves represent the mean of 60 gait
cycles: therefore they represent a lot of data !• Comparable dots of each curve are compared for both
statistical and fractal significance. If any white exists between 2 curves,
it means it is a statistically significant change.• Immediate post AGR-H / sequencing OMT changes documented.
• Post protocol OMT or exercise did not produce significant changes.• Have not been able to identify any other studies showing
immediate post intervention changes.
Mean of 60 gait cycles

elite female runner # 2•For 2 years, felt like “could not get
her left hip to glide forward as much as her right hip”
•When checked gait, she could not go into right on right torsional
movement•Tensegrity PT had been doing a lot
of retaining exercises. “Help somewhat”•L R6-10 exhaled
•L4 FRSL•L. posterior innominate
•Right on right gait restriction•“ I move freely now”
•“I can get that left hip forward without effort”

elite female runner # 3•cc: LBP while running
•B/L wrist fractures as a young gymnast•Old fracture of thoracic R. TP
•AGR: T8 ERSL•L. upsheared innominate
•L3 & 5 FRSL
•L. S/T “counterfeit”corrected when L5 ERSL treated
•left on left gait restriction•L. posterior innominate
•L. FH posterior•L. talus anterior
•B/L RH externally rotated could not pronate both forearms.
•“I feel taller”
Remember:any white betweenthe lines means it
is statisticallySignificant
( over 2 SD )


Osteopathic management:Host + Disease = Illness presentation
host + DISEASE = ILLNESSHOST + disease = ILLNESSHOST + DISEASE = ILLNESS
Additional mechanisms: to explain • S/D: physiological impact & clinical presentation
• OMT: once observe post OMT clinical outcome ( hindrances removed )
•Cybernetics: ( dynamic “feedback” loop )•Gen. Adaptive Systems: ( 1 system )•Complex Systems: ( multiple systems )•Fractal Geometry: ( distribution issues )•Autopoiesis: ( dynamic S/F changes )•Multi-Agent Modeling: ( S/D < resistance > susceptibility ) + virus / CA•Network of Networks: ( simultaneous multiple system networks )•Emergent Properties:
• Whole is greater / more dynamic than sum of the parts !• Non-linear systems ( non-Newtonian ). Can’t predict the outcome but
can explain it backwards once observe the outcome !
7 Competencies: using P/P “mirror” strategy• Osteopathic Integration• Medical Knowledge• Patient Care / Management• Inter-Personal Communications• professionalism• Practice-Based Care and Learning• Systems-Based care and Learning
S/D
S/D can impact:1,all, any combo
of arms
ACGME / E.E.M.• Action
• Reflection• Abstraction
• Application 43