AAACN KHOLT FINAL - ennect Logingo.ennectmail.com/Resources... · · 2012-10-26!Research shows...
18
10/19/12 1 Nursing DEPARTMENT OF NURSING Kim P. Holt, BSN, RN, CPN Nurse Manager Ambulatory Infusion Center Developing a Successful Pediatric Ambulatory Infusion Center: From Concept to Expansion & Beyond Objectives 1. Identify essential elements to consider when developing a pediatric Ambulatory Infusion Center 2. Describe unique considerations for daily operations of a pediatric Ambulatory Infusion Center 3. Identify strategies to enhance operations & promote success in a pediatric Ambulatory Infusion Center Infusion Centers are a subspecialty in Ambulatory that offer accessible, cost-effective care for patient’s with acute illness or chronic disease. By implementing key strategies, Infusion Centers can provide safe, efficient, high-quality, evidence-based care that results in positive outcomes. Ambulatory Infusion Center Background • Patient throughput project • >900 outpatient infusions occurred in an inpatient setting • 300 outpatient infusions occurred in a surgery/procedural area • >1200 missed opportunities for inpatient admit or procedure • Consolidate infusion services into one outpatient location Allergy/ Immunology Bariatric Surgery Dermatology Endocrine Gene8cs Gynecology Nutri8on/ GI Neurology Pulmonary Renal Rheumatology Transplant services Infec8ous Disease
Transcript of AAACN KHOLT FINAL - ennect Logingo.ennectmail.com/Resources... · · 2012-10-26!Research shows...

10/19/12
1
Nursing
DEPARTMENT OF NURSING
Kim P. Holt, BSN, RN, CPN Nurse Manager
Ambulatory Infusion Center
Developing a Successful Pediatric Ambulatory Infusion Center:
From Concept to Expansion & Beyond
Objectives 1. Identify essential elements to consider when
developing a pediatric Ambulatory Infusion Center
2. Describe unique considerations for daily operations of a pediatric Ambulatory Infusion Center
3. Identify strategies to enhance operations & promote success in a pediatric Ambulatory Infusion Center
Infusion Centers are a subspecialty in Ambulatory that offer accessible, cost-effective care for patient’s with acute illness or chronic disease. By implementing key strategies, Infusion Centers can provide safe, efficient, high-quality, evidence-based care that results in positive outcomes.
Ambulatory Infusion Center Background • Patient throughput project
• >900 outpatient infusions occurred in an inpatient setting
• 300 outpatient infusions occurred in a surgery/procedural area
• >1200 missed opportunities for inpatient admit or procedure
• Consolidate infusion services into one outpatient location
ü Allergy/ Immunology ü Bariatric Surgery ü Dermatology ü Endocrine ü Gene8cs ü Gynecology ü Nutri8on/ GI
ü Neurology ü Pulmonary ü Renal ü Rheumatology ü Transplant services ü Infec8ous Disease
10/19/12
2
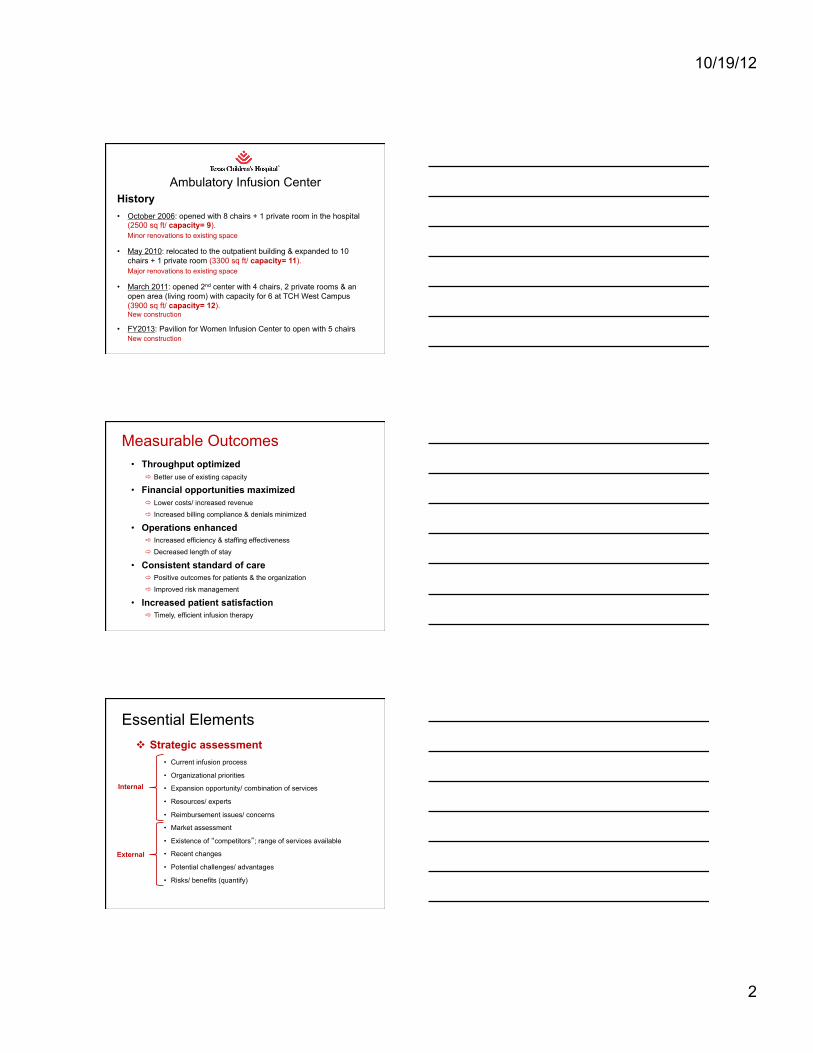
Ambulatory Infusion Center History
• October 2006: opened with 8 chairs + 1 private room in the hospital (2500 sq ft/ capacity= 9). Minor renovations to existing space
• May 2010: relocated to the outpatient building & expanded to 10 chairs + 1 private room (3300 sq ft/ capacity= 11). Major renovations to existing space
• March 2011: opened 2nd center with 4 chairs, 2 private rooms & an open area (living room) with capacity for 6 at TCH West Campus (3900 sq ft/ capacity= 12). New construction
• FY2013: Pavilion for Women Infusion Center to open with 5 chairs New construction
Measurable Outcomes
• Throughput optimized ð Better use of existing capacity
• Financial opportunities maximized ð Lower costs/ increased revenue
ð Increased billing compliance & denials minimized
• Operations enhanced ð Increased efficiency & staffing effectiveness
ð Decreased length of stay
• Consistent standard of care ð Positive outcomes for patients & the organization
ð Improved risk management
• Increased patient satisfaction ð Timely, efficient infusion therapy
Essential Elements v Strategic assessment
• Current infusion process
• Organizational priorities
• Expansion opportunity/ combination of services
• Resources/ experts
• Reimbursement issues/ concerns
• Market assessment
• Existence of “competitors”; range of services available
• Recent changes
• Potential challenges/ advantages
• Risks/ benefits (quantify)
Internal
External

10/19/12
3
Essential Elements
v Project Implementation
• Objectives/ Goals/ Priorities
• Organizational structure
• Project members
• Project plan
• Timeline & budget
• Marketing plan
• Scope of Services
ð Services offered
ð Capacity/ volume projections
ð Limitations/ exclusions
ð Staffing mix/ plan
ð Referral/ scheduling process
Essential Elements
v Space/ Design
• Desired capacity • Renovations or new construction • Best-practice design standards • Proximity to ancillary services • Type/ layout of environment • Workflow • Non-patient care areas
• Regulations/ Accreditation ð Federal/ State/ Local ð CMS (Medicare/ Medicaid) ð The Joint Commission ð OSHA/ United States
Pharmacopeia (USP) ð Internal: Facilities, Compliance,
Legal, Safety/ Infection Control
Essential Elements
v Human Resources • Complexity of services
• State board requirements
• Qualifications/ experience
• Training/ competency
• Physician supervision (“incident to”)
• Management (typically nurse managed)
• Resources/ Technology

10/19/12
4
Considerations for Daily Operations
v Staffing • Staff mix
• Volume/ Acuity/ workload
• Emergency needs
• Manager staffing expectations
• Physician supervision (availability)
• Physical layout/ workflow (direct observation vs closed-door)
Considerations for Daily Operations
v Appointment Scheduling • Patient initiated or limited to referring provider
• Treatment versus chair time
• Difficult to master scheduling of chairs
• Mismanaged schedule à delays
• 10%- 20% urgent walk-in appointments
• Benefits requirements (precert/ prior authorization)
Considerations for Daily Operations
v Orders/ Protocols/ Documentation • Various therapies/ services
• Reoccurring treatment
• Order process (requesting/ receiving/ storage)
• Billing/ reimbursement requirements
• Nursing documentation

10/19/12
5
Considerations for Daily Operations
v Billing issues/ concerns • Frequent changing codes & guidelines (CPT, HCPCS)
• COMPLICATED rules with specific criteria/ requirements
• Payer practices & reimbursement policies
• Capturing/ recording all services provided
• Urgent medically necessary visits
Considerations for Daily Operations
v Miscellaneous • New technology
• New drugs
• Pharmacy
o Inventory management (lead time to order/ storage)
o Expensive, hard to obtain drugs/ Non-formulary
o Preparation requirements/ time
o Payer practices (specialty pharmacy)
Strategy to Improve Efficiency v Space Design/ Layout
• Incorporate best-practice/ evidence-based design standards ü Open layout
– Timely detection of problems / diversion of untoward events
– 90% of drugs require frequent / continuous monitoring
ü Research shows patients prefer an open layout
– Study revealed 97% prefer direct observation
• Integrate workflow in the design
• EMR workstations throughout space &/or on wheels
• Identify services to consolidate (space redundancies eliminated & â costs)

10/19/12
6
Space/ Square Footage Initial Space/ Capacity= 9
New space
Blank canvas
Supply/ equip/ med storage
utility
Weigh/ measure
Nurse
Offi
ce
Private room
8 open infusion bays
Entrance Pharmacy 5 floors up (9th floor)
Pharmacy
= P-tube
Ini8al Space Capacity= 9
Nurses Station
New Space/ Capacity= 11 Open Concept 10 infusion bays + 1 Private Room
Patient Restroom
Staff Restroom
Waiting area Manager Office
Lounge
Supply/ Equiq Med storage Soiled
Utility
Nourishments
Private Room
Entrance
= P-tube = Pass-through
window

10/19/12
7
Open Infusion Bay
Workspace between Infusion Bays
Central Nurses Sta8on

10/19/12
8
Mixed Concept Infusion Center TCH West Campus
Open Living Room (6)
Closed Private Rooms (2)
Open
Infusion Bays (4)
Nurses StaFon
Restroom
Restroom
Storage
Waiting Room
Work area
Open Concept-‐ Living Room
Open Concept-‐ Infusion Bay

10/19/12
9
Closed-‐ Private Infusion Rooms
Strategy to Improve Efficiency
v Scheduling Process • Centralize scheduling/ benefits process
• Schedule chairs based on ordered treatment
• Standardize visit types ü Identify length of each visit by drug (chair time)
ü Include preparation, treatment and post observation time
ü Assign visit types based on drug/ length of visit (IV3, IV4, etc)
• Dedicated person to review medical necessity
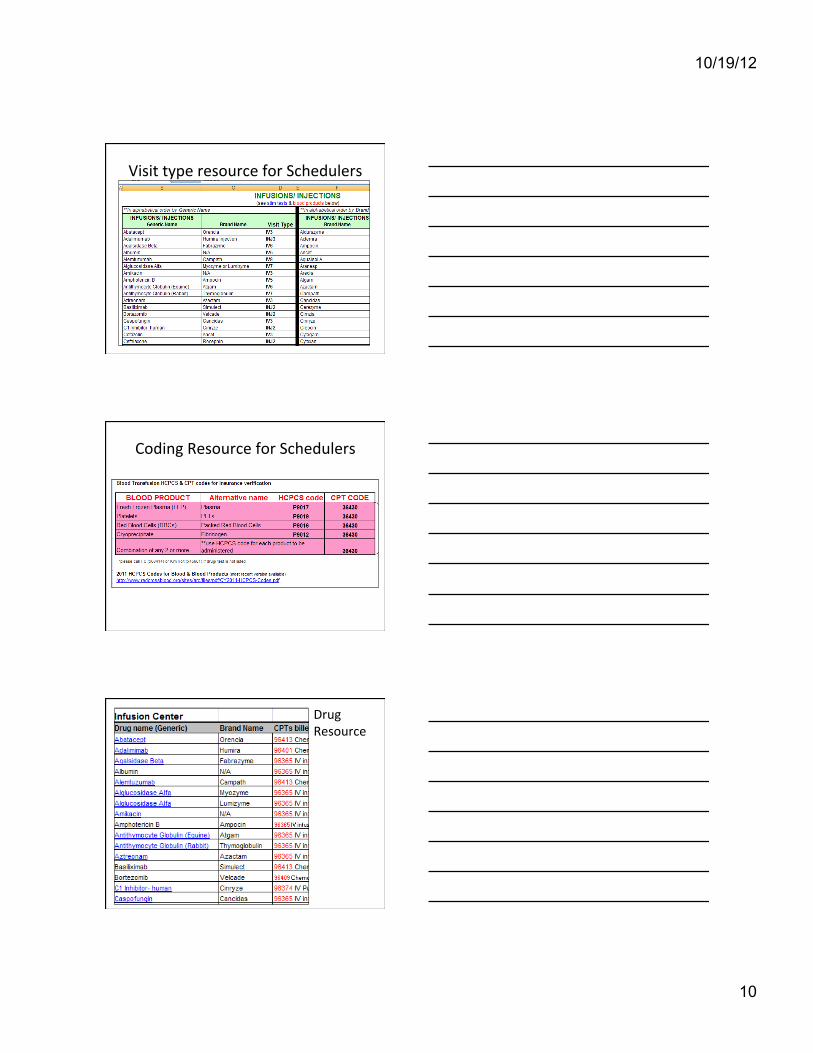
• Create resources for schedulers & update regularly
• Review orders 24-48 hours in advance
• Track length of stay & turnaround time/ delays
Visit type resource for Schedulers
10/19/12
10
Visit type resource for Schedulers
Coding Resource for Schedulers
Drug Resource
10/19/12
11
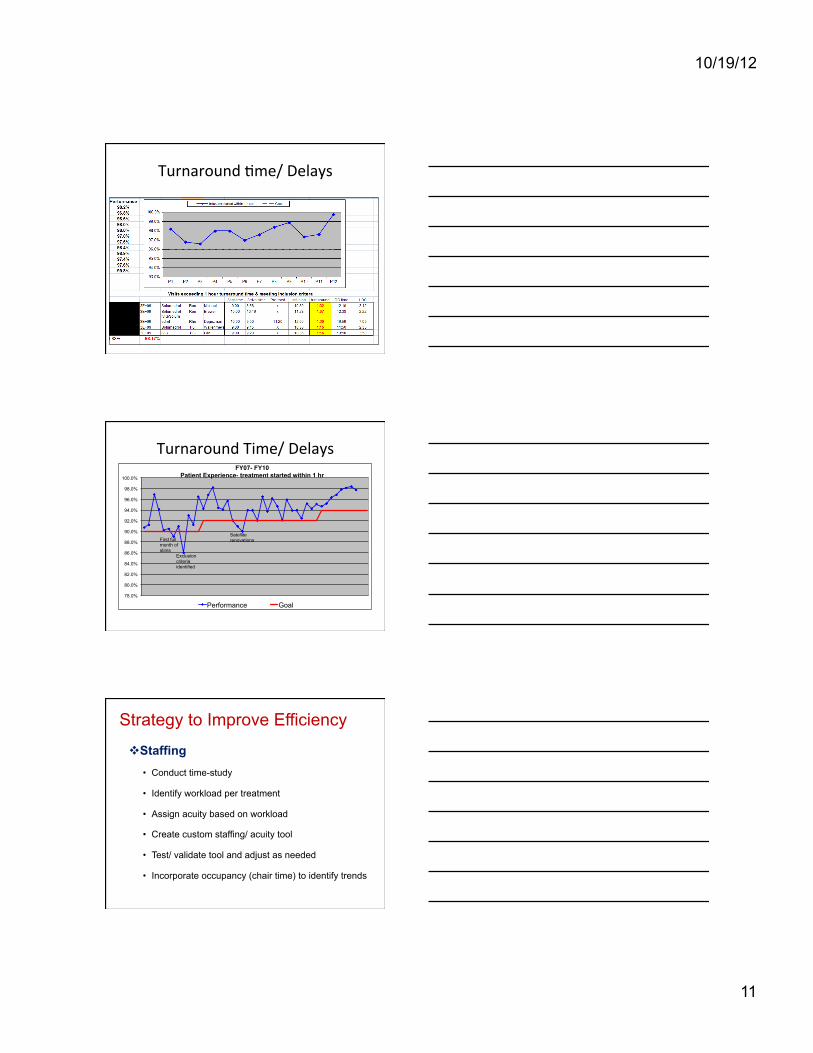
Turnaround 8me/ Delays
Turnaround Time/ Delays
78.0%
80.0%
82.0%
84.0%
86.0%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
FY07- FY10 Patient Experience- treatment started within 1 hr
Performance Goal
Exclusion criteria identified
First full month of stims
Satellite renovations
Strategy to Improve Efficiency
v Staffing • Conduct time-study
• Identify workload per treatment
• Assign acuity based on workload
• Create custom staffing/ acuity tool
• Test/ validate tool and adjust as needed
• Incorporate occupancy (chair time) to identify trends

10/19/12
12
Customized daily staffing/ acuity tool
Staffing Tool
Monthly Summary
Daily Infusion Chair Occupancy
0%
21%
41%
62%
82%
103%
123%
144%
165%
8/1/
2011
8/
2/20
11
8/3/
2011
8/
4/20
11
8/5/
2011
8/
6/20
11
8/7/
2011
8/
8/20
11
8/9/
2011
8/
10/2
011
8/11
/201
1 8/
12/2
011
8/13
/201
1 8/
14/2
011
8/15
/201
1 8/
16/2
011
8/17
/201
1 8/
18/2
011
8/19
/201
1 8/
20/2
011
8/21
/201
1 8/
22/2
011
8/23
/201
1 8/
24/2
011
8/25
/201
1 8/
26/2
011
8/27
/201
1 8/
28/2
011
8/29
/201
1 8/
30/2
011
8/31
/201
1
Daily occupancy rate Goal
*average industry standard is 80% productive time per chair

10/19/12
13
Strategy to Improve Efficiency v Standardize Orders/ Documentation
• Establish an acceptable timeframe for reoccurring orders
• Incorporate common orders (procedural pain prevention, flushes, pre-meds)
• Create protocols for adverse event management
• Standardize documentation per billing requirements
Standardized Orders (currently 43 protocols)
Infusion/ Injec8on Documenta8on & Billing
10/19/12
14
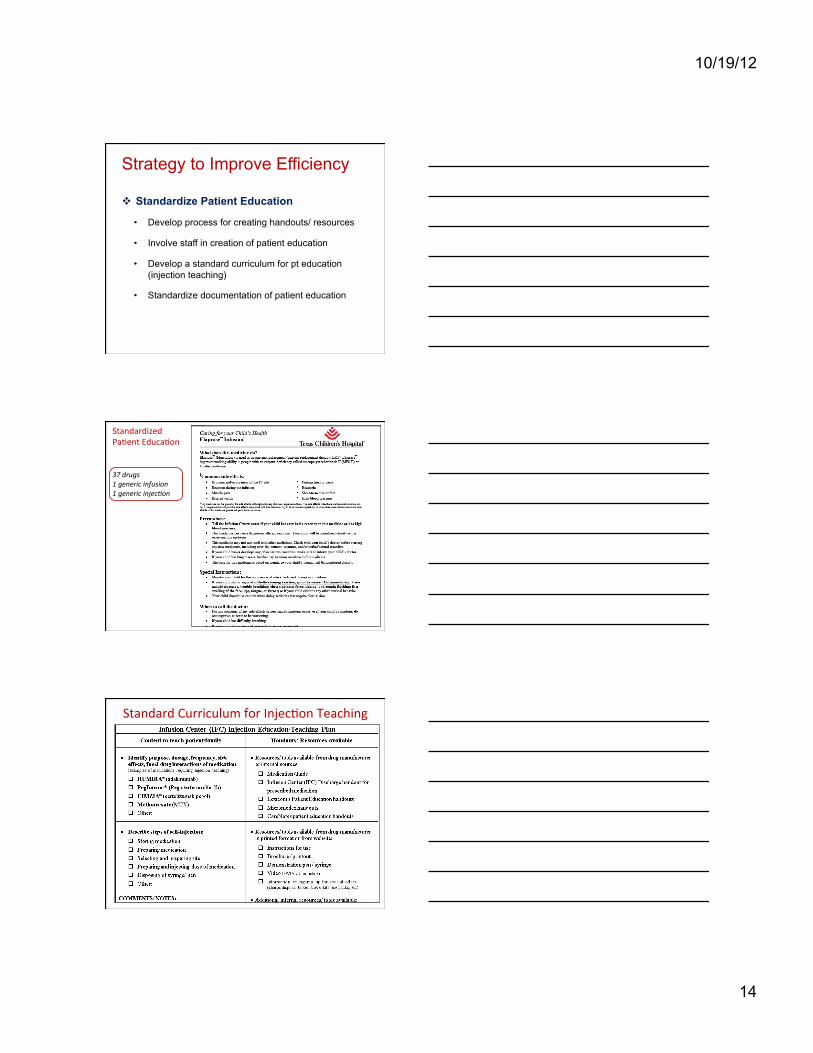
Strategy to Improve Efficiency
v Standardize Patient Education
• Develop process for creating handouts/ resources
• Involve staff in creation of patient education
• Develop a standard curriculum for pt education (injection teaching)
• Standardize documentation of patient education
Standardized Pa8ent Educa8on 37 drugs 1 generic infusion 1 generic injec1on
Standard Curriculum for Injec8on Teaching
10/19/12
15
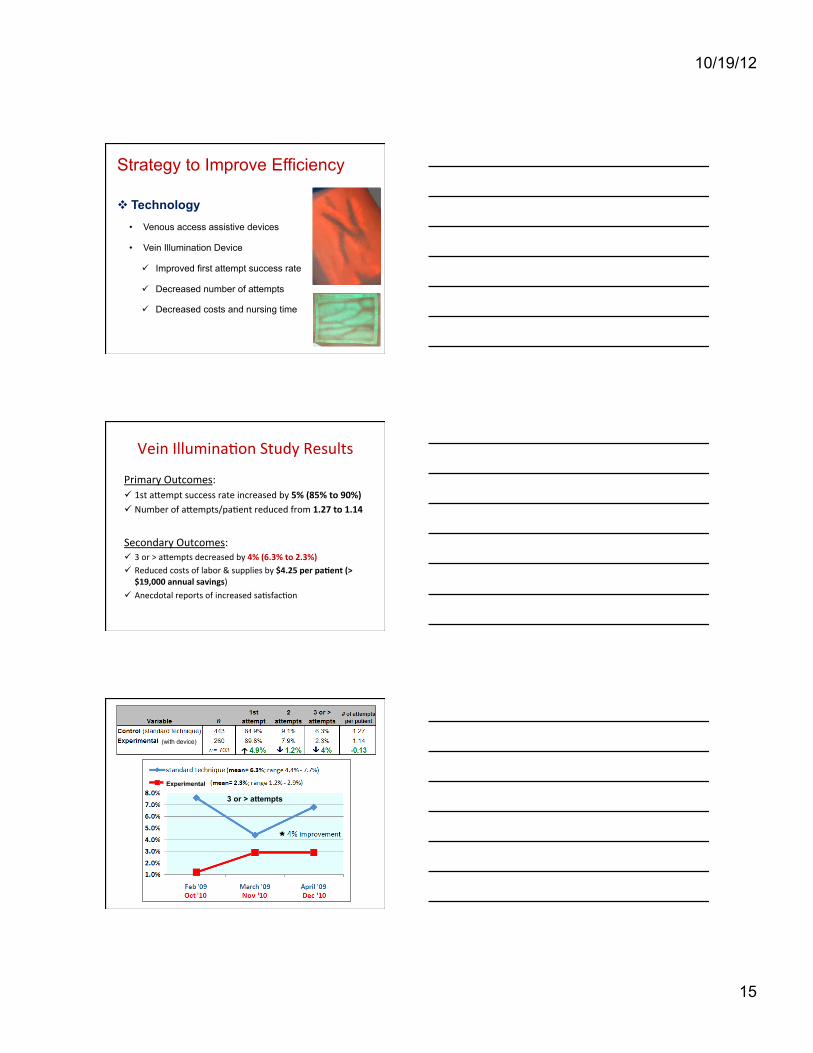
Strategy to Improve Efficiency
v Technology • Venous access assistive devices
• Vein Illumination Device
ü Improved first attempt success rate
ü Decreased number of attempts
ü Decreased costs and nursing time
Vein Illumina8on Study Results
Primary Outcomes: ü 1st a^empt success rate increased by 5% (85% to 90%) ü Number of a^empts/pa8ent reduced from 1.27 to 1.14
Secondary Outcomes: ü 3 or > a^empts decreased by 4% (6.3% to 2.3%) ü Reduced costs of labor & supplies by $4.25 per paFent (>
$19,000 annual savings) ü Anecdotal reports of increased sa8sfac8on
3 or > attempts
(with device)
Experimental

10/19/12
16
PURPOSE: assess impact of a vein illumination device on first attempt success rate & number of attempts required for insertion of a peripheral intravenous (IV) catheter in pediatric patients
Vein illumination: • Improves 1st attempt success • Decreases number of attempts • Preserves veins • Increases efficiency &
proficiency • Ensures proper & efficient use of
resources • Decreases unnecessary &
costly procedures • Improves satisfaction
Study Implica8ons
• Decreases costs
• Enhances the IV experience
• Promotes building of trust, cooperation & confidence
• Supports high-quality care & outcomes
• Complies with practice standards
Summary of Strategies for Success
v Evidence-based concepts • Space design
• Technology v Standardize / Customize
• Visit types • Scheduling/ Benefits verification
• Billing
• Identifying staffing needs (acuity tool)
• Orders
• Documentation (critical for reimbursement)
• Patient education
Additional Strategies for Success v Recruit the “right” staff
• Maximize experience
v Facilitate development of experts • Designate staff to specific tasks
v Market your services • If you build it they will come, BUT only if they know about it • Remain alert to changing needs
v Develop collaborative partnerships • Pharmacy • Referring services/ physicians • Home Health

10/19/12
17
1243 1454 1923
2259
3024 164
349
258
210
221
156
378
441
471
567
50
550
1050
1550
2050
2550
3050
3550
FY07 FY08 FY09 FY10 FY11
Infusions Blood Transfusions S8mula8on Test
20.2% á
30% á
1563 visits 2181 visits 2622 visits 2940 visits *3813 visits
Top 3 infusion visits: 1. Steroids 2. Biologics (MoAbs; IVIG) 3. Enzyme Replacement Therapy
*full year in expanded space
39.5% á
12% á
FY2012 acFvity= 4,581 visits: (25% á) v Infusions= 3,917 v Blood Transfusions= 127 v S8mula8on Tests= 537
System-‐wide Infusion Services Growth
References Carota, R. (2002). Plan before you Design. American Academy of Medical
Administrators. Retrieved 6/9/11 from h^ps://www.aameda.org/MemberServices/Exec/Ar8cles/winter2002carota.pdf
Dohse, L. (2005). The Infusion Nurses's Role in Precer8fica8on. Journal of Infusion Nursing. 28(1), 23-‐29.
Dohse, L. (2007). Nine ways to improve efficiency in an ambulatory infusion center. Community Oncology. 4(1), 33-‐34.
Ernst, D. (2009). Take the guesswork out of venipunctures. Medical Laboratory Observer. 41(4). April 2009. 18-‐21.
Founts, M., Gabay, D. (2008). Healing through Evidence-‐Based Design. Oncology Issues. May/June 2008. 28-‐32.
Franklin, David M. (2010). "Embarking on an AIS Venture: How to Start Up an Ambulatory Infusion Suite". 2010 NHIA Annual Conference & Exposi8on [Conference]. Dallas. 15 April 2010.
Gaits, V. (2005). Nurse Resource Alloca8on in Ambulatory Cancer Centers: Guidelines for Clinicians and Execu8ves. Oncology Issues. September/ October 2005. 36-‐42.

10/19/12
18
Garner, R. (2009). "Infusion centers: opportuni8es for financial and personal success". 2008 College of Americal Pathologists Futurescape of Pathology [Conference]. Rosemont. 7-‐8 June 2008.
Gruber, M., Hennessy, K., O'Neal, C. et al. (2008). Quality Improvement Project to Determine Outpa8ent Chemotherapy Capacity and Improve U8liza8on. Journal of Nursing Care Quality. 23(1), 75-‐83.
Health Facili8es Management (2008). Crea8ng Environments for Cancer Care. Retrieved 6/11/2011 from h^p://www.burthill.com/FILES/press/Crea8ng_Environments_for_Cancer_Care.pdf
Jewler, D. (2010). Cancer Center Design for the Future. Cancer Care ACCCBuzz. May 3, 2010 issue; retrieved 6/9/2011.
Rieger, P. (2005). The Crea8on of a Pa8ent-‐Classifica8on System in an Outpa8ent Infusion Center Setng. Oncology Nursing Forum. 32(3). 535-‐538.
Versel, N. (2005). Build Your Own Infusion Clinic. Biotechnology Healthcare. February 2005 issue. 35-‐40.
Wang, Z., Pukszta, M., Petzoldt, N. et al. (2011). Cancer Treatment Environments: From pre-‐design research to post-‐occupancy evalua8on. World Health Design. July 2011 issue. 68-‐74.
West, S. (2009). The “Right” Nurse Staffing Model. Oncology Issues. November/December 2009. 26-‐30.