A Way Forward - Denver Foundation...A Way Forward How Colorado’s Behavioral Health Leaders Can...
16
A Way Forward How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs A Report Made Possible by The Colorado Health Access Fund APRIL 2018
Transcript of A Way Forward - Denver Foundation...A Way Forward How Colorado’s Behavioral Health Leaders Can...

A Way ForwardHow Colorado’s Behavioral Health Leaders
Can Address Colorado’s Most Pressing Needs
A Report Made Possible by The Colorado Health Access Fund
APRIL 2018

A Way ForwardHow Colorado’s Behavioral Health Leaders
Can Address Colorado’s Most Pressing Needs
CHI staffers contributing to this report
• Alex Caldwell, Lead Author
• Jeff Bontrager, Lead Author
• Brian Clark
• Cliff Foster
• Deborah Goeken
• Jalyn Ingalls
• Michele Lueck
• Liana Major
• Ian Pelto
Special Thanks
This report is made possible by the Colorado Health Access Fund, a field of interest fund of The Denver Foundation. Established in 2014 with an anonymous gift of $40 million, the Fund is dedicated to improving health outcomes for underserved Coloradans.
3 Introduction
4 Our Recommendation
4 Guiding Principles for Behavioral Health Leaders
5 Strategic Funding Priorities in Behavioral Health
6 STRATEGIC FUNDING AREA ONE: Support Programs Offering Direct Services
8 STRATEGIC FUNDING AREA TWO: Strengthening the Behavioral Health Workforce
10 STRATEGIC FUNDING AREA THREE: Improve the System
12 Colorado's Behavioral Health Workforce
14 Looking Ahead
14 Endnotes

Colorado Health Institute 3
APRIL 2018
A Way Forward: How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs
Colorado continues to struggle with behavioral health challenges.
Almost 12 percent of Coloradans report poor mental health, according to
the 2017 Colorado Health Access Survey, up from about 10 percent in 2015.1
Colorado ranks 43rd of the 50 states plus the District of Columbia on a 2018
mental health index from Mental Health America, based on 15 measures.2
As these leaders look to the future, they face several challenges:
• Where should they focus their efforts to address these needs — while at the same time promoting innovation and health equity so that the change is lasting and it equitably benefits all Coloradans?
• What innovative, scalable and sustainable services or initiatives — beyond treatment — could Colorado’s behavioral health leaders support to address our most pressing needs and barriers to care?
• How can they best leverage their individual strengths to effectively tackle this big problem?
The Colorado Health Institute (CHI) was asked by the Colorado Health Access Fund at The Denver Foundation to conduct an analysis to help answer these questions to inform Colorado’s behavioral health leaders.
We interviewed key informants, analyzed the literature and reviewed guidance from other behavioral health philanthropies. Together, the quantitative and qualitative data we gathered helped us create a list of more than 50 potential funding strategies to help address the state’s most pressing behavioral health needs. We vetted each strategy by asking: Will this create measurable impact? Promote health equity? Capture patient stories? Leverage policy opportunities? Foster innovation while ensuring sustainability?
The result was a curated list of best-in-class funding strategies that we settled on as actionable proposals for the community to consider. This report explains those strategies.
The Colorado Health Access Fund made this work possible. But this report is for all Colorado behavioral health leaders who want to collaborate and tackle these problems head-on.
The substance use problem has brought new attention to the issue. An estimated half million Coloradans are dependent on alcohol or have used illicit drugs. In fact, drugs are killing more Coloradans than ever. The state saw 912 Coloradans lose their lives in 2016 to overdoses, setting another record with 959 deaths in 2017 according to early estimates.3
Colorado’s behavioral health care system is struggling to keep up with the increased need. About one of 13 Coloradans (7.6 percent) did not get needed mental health services in 2017.4
The rate was double for Medicaid clients, with one of six (15 percent) failing to get needed care. Race and ethnicity matter, too. Colorado’s Hispanic, African-American, multiracial, American Indian and Alaska Native residents report not getting needed mental health services at higher rates than white Coloradans.
Thankfully, Colorado benefits from a rich community of leaders from foundations, state agencies and community organizations who are committed to tackling this important issue together. These leaders have developed a crisis system of hotlines, walk-in centers, and mobile response teams that serve everyone regardless of ability to pay. Their work has led to law enforcement and other first responders being equipped with Naloxone, the opioid overdose reversal medication.
And committed philanthropic leaders have provided millions of dollars in support of sustainable, innovative, equitable investments in our state’s behavioral health system — improving the lives of many Coloradans in the process.
INTRODUCTION

4 Colorado Health Institute
Our RecommendationAccording to CHI’s analysis, Colorado’s behavioral health needs fall along a continuum — from care for individuals on one end to social, systemic and policy solutions on the other.
We could argue that all of these areas deserve additional attention and resources. But opportunities emerged as areas that are still underfunded.
Colorado’s behavioral health leaders — foundations, governments and community organizations — could focus their behavioral health investments in three strategic approaches:
• Support Programs Offering Direct Services. Substance use treatment, crisis services, and child
and youth mental health issues are top priority needs for Colorado.
• Strengthen the Behavioral Health Workforce. Behavioral health leaders can build the behavioral health workforce by integrating providers into primary care environments, investing in community-based care, and extending the existing behavioral health workforce using telehealth and other technologies.
• Improve the System. Address systemic issues such as policy change and social challenges by investing upstream in advocacy efforts, data infrastructure and the social determinants of behavioral health.
This document outlines the biggest funding needs and potential funding strategies to meet those needs.
The Colorado Health Access Fund’s Guiding PrinciplesCHI used the Colorado Health Access Fund’s Guiding Principles to synthesize the most impactful, sustainable funding opportunities that will address Colorado’s pressing behavioral health needs. These principles are specific to the Fund — but we believe they can inform the funding practices of any behavioral health leader in Colorado.
We assessed each of the more than 50 funding opportunities against the guiding principles listed below. That assessment resulted in a list of top tier investment opportunities illustrated in Figure 1: Strategic Funding Priorities in Behavioral Health.
The priorities that emerged reflect today’s behavioral health context. For example, providing housing ranked near the top. But another recommendation we assessed — investing in outreach to increase insurance coverage — did not end up on this list. This may be thanks to the aggressive efforts Colorado has pursued in outreach and enrollment since the Affordable Care Act implementation.
Acknowledge Lived Experiences
• Promotes racial equity in health;
• Generates personal stories that convey impact.
Promote Complementary Philanthropy
• Does not increase “demand” for other philanthropic support in the future;
• Contributes to the collective philanthropic knowledge base;
• Does not duplicate the efforts of other organizations.
Pursue Policy
• Informs and strengthens policies around behavioral health care;
• Leverages possible new legislative opportunities or funding sources.
Ensure Legacy
• Scales innovative services that address behavioral health care needs;
• Supports a high spend rate;
• Supports sustainable programs.

Colorado Health Institute 5
APRIL 2018
A Way Forward: How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs
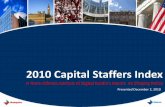
Strategic Funding Priorities in Behavioral HealthTo meet the most pressing behavioral health needs in Colorado — while championing innovative and sustainable models of health equity — CHI recommends that behavioral health leaders in Colorado consider focusing together on three strategic funding areas.
These strategic funding areas fall along a
Promising Investment Opportunities
Substance Use Disorder Treatment
• Residential substance use disorder treatment• Medication-assisted treatment
Crisis Services• Co-responder model• Crisis response services
Child and Youth Mental Health
• Early childhood and youth-focused behavioral health promotion programs• Trauma-informed care for justice-involved youth
Behavioral Health Integration
• Culturally competent providers• Practice transformation efforts• Nontraditional integration models
Care in the Community
• Mental Health First Aid• Peer specialists model
Telehealth Capacity• Tele-mental health services• Psychiatric e-consults in rural areas
Social Determinants of Health
• Housing support such as social impact bonds• Employment support for people with behavioral health issues• Medical-legal partnerships
Data Infrastructure • Social information exchange
Policy Change • Advocacy efforts
continuum that includes care for individuals on one end to social and policy solutions on the other:
• Support Programs Offering Direct Services.
• Strengthen the Behavioral Health Workforce.
• Improve the System.
Following are brief introductions to each funding priority and the short list of investment opportunities — projects, models and approaches — that rose to the top to help meet those priority needs. (See Figure 1.)
Figure 1: Strategic Funding Priorities in Behavioral Health
Sup
po
rt P
rog
ram
s
Off
erin
g D
irec
t Se
rvic
es
Stre
ng
then
the
B
eha
vio
ral H
ealt
h
Wo
rkfo
rce
Imp
rove
th
e Sy
stem

6 Colorado Health Institute
STRATEGIC FUNDING AREA ONE:
Support Programs Offering Direct ServicesWhen it comes to addressing the state’s behavioral health needs, the most direct path for Colorado’s behavioral health leaders is to invest in infrastructure and services that go straight to those who need them. Investments might include capital projects to expand residential treatment facilities and mobile crisis units, or youth-focused health promotion programs.
Since foundations are not limited by reimbursement rules or policy barriers, they can play a unique role supporting treatment services and building the infrastructure necessary to meet these needs.
Which services could Colorado’s behavioral health leaders focus on? Substance use treatment, crisis services, and child and youth mental health services rise to the top as areas of greatest need and investment potential.
Funding Priority One: Substance Use Disorder Treatment
What is the Gap?
In 2017, 67,000 Coloradans reported that they did not get needed services for alcohol or drug use. CHI estimates that many more Coloradans need treatment but do not know it or are not ready to seek help.5
Medication-assisted treatment, which pairs medication with counseling to treat opioid addition, is clinically proven but not available to everyone who needs it. An average of 22,000 Coloradans annually report abuse or dependence on opioids, while 4,000 — or about one of five — received treatment annually at a specialty facility between 2011 and 2014.6 Colorado won a federal State Targeted Response grant to develop this model of care, but the need continues to outstrip capacity.7,8
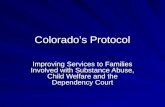
For patients who need long-term support and recovery from all forms of substance abuse disorder, residential treatment provides a safe and stable 24-hour environment. But 28 counties in Colorado do not have these kinds of treatment facilities. Much of the San Luis Valley, southeastern and northern Colorado continue to go without care (see Map 1).9
Where Are the Opportunities?
Make investments that serve high-acuity patients who need long-term or in-patient treatment. These services are expensive and difficult to sustain in low-income or low-population areas. Medication-assisted treatment and residential substance abuse treatment expansions rank at the top.
Potential Investment Strategies
1. Medication-assisted treatment. Expand access using Vermont’s Hub-and-Spoke model as an example.10 The state weaved together existing care infrastructure — like Federally Qualified Health Centers, methadone clinics, and office-based opioid treatment centers to offer regional intensive addiction care center “hubs” and primary care “spokes” to provide long-term support for patients as they get back on their feet.
2. Residential substance use disorder treatment. Colorado needs more beds for long-term substance abuse treatment. Mind Springs Health, the Western Slope’s largest behavioral health provider, is building the West Springs Hospital in Grand Junction to provide psychiatric care to a 23,000 square mile area from Routt to Summit to Mesa counties.11 But many regions remain without a facility, and transportation to the facility is necessary for people who need this level of care but live hours away.
Funding Priority Two: Crisis Services
What is the Gap?
Behavioral health crisis services are critical parts of a comprehensive behavioral health system. Despite Colorado’s investments in a statewide system, CHI’s research has revealed critical opportunities to strengthen these services, especially in rural parts of the state.
Though Colorado’s system includes all the elements of an effective response system — mobile crisis teams and walk-in centers for stabilization and emergency observation, for example — challenges exist in how the services are monitored and delivered.12
In rural areas with few patients, it’s expensive to recruit providers and offer transition care. Key informants identified several parts of the system that are weak: short-term psychiatric services, withdrawal management, connections with local Community

Colorado Health Institute 7
APRIL 2018
A Way Forward: How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs
Mental Health Centers, mobile crisis support and crisis transport.
Where Are the Opportunities?
Invest in crisis services provided to people when and where they need them. The two approaches that rose to the top were the co-responder model of behavioral health care delivery alongside police, and mobile crisis response teams to address needs in underserved areas.
Potential Investment Strategies
1. Co-responder model. Pair trained police officers with mental health professionals to divert individuals with low-level offenses from the criminal justice system and towards treatment and
social services.13 Colorado’s Office of Behavioral Health awarded grants to eight primarily urban communities in 2018.14 Foundations can build on these investments in rural and underserved areas.
2. Crisis response services. Research has revealed a variety of needs related to the state’s crisis services. These include challenges related to provider recruitment, fragmentation of regional services, transportation to post-crisis care, and data infrastructure. The state’s Department of Human Services has convened groups of stakeholders to evaluate and strengthen the system.15 Their recommendations will become available in June 2018. Behavioral health leaders could align with these efforts to address gaps and increase efficiencies in the state’s crisis services.
MAP 1: Mental Health and Substance Use Services Combined
Source: Colorado Office of Behavioral Health, 2017

8 Colorado Health Institute
Funding Priority Three: Child and Youth Mental Health
What is the Gap?
Nearly one of three high school students (30 percent) reported feeling so sad for at least two weeks in a row that they stopped engaging in normal activities.16 But according to school data, resources are lacking, with 29 percent of elementary schools in Colorado without a school counselor, 11 percent without a school psychologist, and 47 percent without access to a school social worker.17
Where Are the Opportunities?
Promote good behavioral health early in life, and provide responsive, trauma-informed care throughout childhood and adolescence. Decades of prevention science have identified the contextual factors that predict health outcomes for youth — such as community and family connectedness, school participation and social skills.18 Invest in approaches that address these factors.
Potential Investment Strategies
1. Early childhood and youth-focused behavioral health promotion programs. One example is Project LAUNCH (Linking Actions for Unmet Needs in Children’s Health) — a federally funded project to promote the wellness of young children to address all aspects of development — including behavioral health. Seven Colorado communities were awarded LAUNCH Together grants, inspired by Project LAUNCH, to promote the social and emotional health of children. A national cross-site evaluation of the program found that participants were on a positive trajectory.19
2. Trauma-informed youth behavioral health care. Especially for justice-involved youth, this treatment approach addresses complex needs for people who have experienced chronic trauma like abuse, homelessness, and neglect. Evidence basis is still growing for this approach.20 Behavioral health leaders could leverage the work of Colorado’s Trauma Informed System of Care (COACT Colorado), which is serving 17 counties with wraparound services like technical assistance, facilitators, and family advocates to increase access to trauma-informed care for the highest-needs kids in the state.21
STRATEGIC FUNDING AREA TWO:
Strengthen the Behavioral Health WorkforceMany Colorado communities — especially those in rural areas — struggle to provide behavioral health services because they lack behavioral health professionals.
We provide a deeper exploration of this complex issue on pages 12 and 13. The solutions are wide-ranging — from policy change to telehealth to loan repayment — but all speak to the underlying theme of increasing or optimizing the use of a scare resource.
While leaders in behavioral health can help in a variety of ways, our analysis suggests that the most promising opportunities for investment include integrating care into primary care environments, investing in community-based care, and extending the existing behavioral health workforce using telehealth and other technologies.
Funding Priority One: Behavioral Health Integration
What is the Gap?
A growing body of evidence shows that integrating behavioral health services and primary care services leads to better health outcomes, better transitions in care, and better quality of care.22 It is a strategy that can increase access to needed services by offering them in a place where patients are already visiting and may address the potential stigma of going to a mental health provider.
Where Are the Opportunities?
Investing in integrated care can mean many things. The three options below take a broad view of integration by identifying how providers can augment the care of a clinician to better meet the needs of patients.
Potential Investment Strategies
1. Culturally competent providers. Mental Health America released a position statement identifying the importance of providers being able to be culturally and linguistically responsive to the needs of their patients.23 The Eugene S. Farley, Jr. Health Policy Center of Colorado developed a set of core

Colorado Health Institute 9
APRIL 2018
A Way Forward: How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs
APRIL 2018
competencies for behavioral health providers working in primary care.24 Training culturally competent behavioral health workers is a critical step in Colorado’s efforts to promote health equity.
2. Practice transformation efforts. Research shows that “whole person” care leads to better health outcomes, lower costs and more efficiency.25 Leaders could build on Colorado’s State Innovation Model efforts to help clinics apply value-based payment structures and strengthen information technology to improve behavioral health outcomes.26
3. Nontraditional integration models. Instead of bringing behavioral health services to primary care environments, nontraditional integration models bring services to other areas of care. For example, Oregon has piloted a program called Project Nurture to provide prenatal care, inpatient maternity care, and postpartum care for women who struggle with addictions.27 The model engages women in prenatal care and drug treatment early in pregnancy. The Institute for Healthcare Improvement highlights successes and lessons learned from Project Nurture.28 The number of newborns born with neonatal abstinence syndrome in Colorado has spiked since 2000, indicating the need for a more complete treatment program for mothers with substance use treatment needs.29
Funding Priority Two: Care in the Community
What is the Gap?
Neither the number nor the distribution of licensed behavioral health professionals meets Colorado’s needs. But evidence suggests that an unlicensed workforce can be as effective for patient care, especially when it comes to early identification of mental illness, reducing stigma, and connecting people to care.30
Where Are the Opportunities?
Train unlicensed community members to provide care through approaches like Mental Health First Aid and Peer Specialists.
Potential Investment Strategies
1. Mental Health First Aid. Mental Health First Aid trainings teach community members how to
identify and react to the signs of a mental health challenge or crisis. Mental Health First Aid Colorado provides trainings throughout Colorado, with modules that provide tailored training for specific populations, such as law enforcement officials. And the evidence basis of Mental Health First Aid is growing to show that trained community members are more confident and able to help others facing a crisis — and had increased mental wellness themselves.31
2. Peer Specialists Model. Peer support programs allow people who have successfully overcome addiction or other mental health conditions to assist others with treatment and recovery. Peer support programs are considered a best practice, and have been shown to reduce symptoms, decrease hospital stays, and improve well-being.32 Mental Health America has developed a national certification for peer support.33
Funding Priority Three: Telehealth Capacity
What is the Gap?
Most of Colorado’s behavioral health workforce is disproportionately located in the state’s population centers. This leaves rural areas and urban underserved areas lacking needed behavioral health resources.
For example, Boulder County boasts 2,009 psychiatrists, psychologists, counselors, licensed clinical social workers, and other behavioral health providers — about one provider for every 160 residents. But Conejos County in southern Colorado landed on the other end of the spectrum with just one provider serving 8,000 residents.34
Where Are the Opportunities?
Investments in technological solutions — such as telehealth — can help diminish the maldistribution of behavioral health providers by delivering care via live video over long distances.
Potential Investment Strategies
1. Tele-mental health services. Tele-mental health providers can increase telehealth capacity by working directly with clinics on best practices, integration into existing workflow, and selection and purchasing of video equipment.35 Some states have built virtual care teams to address social and

10 Colorado Health Institute
behavioral health needs using distant providers in a team arrangement.36
2. Psychiatric e-consults in rural areas. E-consults, or providing clinical advice electronically from a distant specialist like a psychiatrist to a primary care provider in need, have been proven to increase access to care and reduce unnecessary referrals while maintaining quality and reducing costs.37 Though some Colorado providers are participating in this model, there is significant room to expand and reimburse for these services.38
STRATEGIC FUNDING AREA THREE:
Improve the System Systemic issues continue to prevent Coloradans from maintaining good behavioral health or getting care when they need it. These systemic issues include policies, such as lack of Medicaid reimbursement for certain behavioral health services, and social challenges such as inadequate housing. They will only be addressed through collaborative investment approaches.
These issues are especially complex because they both affect and are affected by behavioral health status. One example is the link between homelessness and substance use. A Keystone Policy Center report, “Bridging the Divide: Addressing Colorado’s Substance Use Disorder Needs,” identified housing as a substance use treatment priority for all seven regions of the state.39
As funding leaders shift from a health disparities lens to a health equity framework, investing upstream — before treatment is required — becomes even more important. To be healthy, Coloradans need stable employment and housing.40, 41 They need to live free from legal battles related to immigration, legal status, insurance and other issues — and the associated financial burden. And they need a health care system that can monitor and use data on these critical factors to inform the care they receive.
These are the levers behavioral health leaders can use to enhance the way Colorado’s behavioral health system promotes health equity. Doing this requires investments in advocacy efforts, data infrastructure and the social determinants of behavioral health.
Funding Priority One: Social Determinants of Health
What is the Gap?
Research shows that social, economic and environmental factors have a major impact on behavioral health outcomes.42 Literature has established an association between income and mental health and education and mental health. These two examples indicate the need to address the social determinants of health to improve mental health.43
Key informant interviews with 11 of Colorado’s behavioral health experts reinforced the need to provide social supports for patients during treatment and recovery. Many key informants stated homelessness as being a barrier to achieving good mental health.
A holistic approach is critical for treating mental health issues and maintaining good mental health throughout life.
Where Are the Opportunities?
Behavioral health philanthropic leaders could focus on approaches that are “upstream” from treatment by investing in a community’s well-being — from adequate housing to stable employment to reduced inequities.
Potential Investment Strategies
1. Housing support such as social impact bonds. Research shows that housing has a direct impact on behavioral health, especially for kids.44 Social impact bonds provide financing for a program that results in improved social outcomes and public-sector savings. The funders are repaid with the money that is saved from the program. Denver currently has a Social Impact Bond program to provide housing for 250 homeless individuals who have mental health needs. The Urban Institute is evaluating the Housing Social Impact Bond initiative and an early report suggests there is promising evidence the program will meet its goals.45
2. Employment support for people with behavioral health issues. The Substance Abuse and Mental Health Administration Services (SAMHSA)recognizes Supported Employment as an evidence-based approach to addressing the needs of people with serious mental illnesses.46 This model supports patients seeking jobs with

Colorado Health Institute 11
APRIL 2018
A Way Forward: How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs
follow-up support as needed. Behavioral health leaders could consider building on the efforts of several of Colorado’s community mental health centers implementing this approach.47
3. Medical-legal partnerships. A partnership between medical providers and a legal team can provide pro-bono legal services for low-income patients in situations that may be impacting their health — like experiencing eviction, intimate partner violence or something else. The Colorado Health Equity Project currently provides medical-legal partnership services in three Colorado health care facilities. While the evidence for this model is still building, early reviews show promise in improving health outcomes.48
Funding Priority Two: Data Infrastructure
What is the Gap?
Strengthening the connection between mental health and medical health providers is critical to coordinating efficient, high-quality patient care. As highlighted above, research suggests social determinants of health — where and how people are born, live, work and age — are just as important predictors of behavioral health as physical health.49
SAMHSA recognizes the importance of treating behavioral health through integrated systems that also address a patient’s social needs, such as housing and employment. Integrated systems of care promote a holistic approach by improving information-sharing among data systems.
Where Are the Opportunities?
Invest in systems that integrate different data sets impacting health — like access to adequate housing, exposure to intimate partner violence, and food security.50 These are known as social information exchanges.51
Potential Investment Strategy
1. Social information exchange. A social information exchange is a data collection system that integrates information on a patient’s social determinants of health into their electronic health record. Health care providers can use the data to better track, prevent and address issues by using community-based services before the issues lead to poor patient outcomes such as substance use disorder or serious mental illness. Colorado maintains some of the largest health information
exchanges in the country, including the Colorado Regional Health Information Organization (CORHIO), and Quality Health Network (QHN) on the Western Slope. The data infrastructure networks collectively capture information from millions of Coloradans — offering a big opportunity for data collection on social determinants of health.
Funding Priority Three: Policy Change
What is the Gap?
Investing in treatment alone will not address the underlying issues that keep Colorado’s behavioral health system from performing at its best. Systemic and unjust policies can create barriers to accessing mental health — even if the policy was implemented with good intentions.
Policies to regulate health insurance systems can create barriers to accessing mental health services. One of five Medicaid clients in Colorado (21 percent) report poor mental health, a higher proportion than any other coverage group in the state. Yet Medicaid clients report not getting needed mental health services more frequently than other insured Coloradans. Medicaid policies — such as a lack of reimbursement for certain services — may be hindering members’ ability to get necessary mental health care.
Changing policies that hinder access to mental, social, and economic health can address mental health inequities in Colorado.
Where Should Funders Focus?
Foundations have an opportunity to take the long view and invest in policy change.52 Advocacy services funders could provide legislator education or lobbying, policy development, grassroots mobilization, awareness campaigns and research and dissemination.53
Potential Investment Strategy
1. Advocacy efforts. Key informants supporting this report repeatedly raised the need for policy change to meaningfully address needs in behavioral health, from strengthening the workforce to building crisis capacity to integrating services into primary care. They called for systemic investments in advocacy to increase the number of billable Medicaid behavioral health codes, enforce payment parity between physical and behavioral health care services, and promote harm reduction efforts like a supervised injection site.

12 Colorado Health Institute
Colorado’s behavioral health workforce — from psychiatrists to social workers to substance abuse counselors — is not meeting the needs of Colorado residents. Why?
Here is a deeper dive into this critical, complex issue.
What is keeping Colorado from developing and maintaining the right number of behavioral health care providers?
Is it noncompetitive salaries? Insufficient training programs or recruitment and retention efforts? Undeveloped workforce planning
infrastructure? Inadequate use of behavioral health integration and technology solutions like e-consults and telehealth?
Colorado’s Behavioral Health Workforce
Providers Are Concentrated in Urban Areas
Colorado has many rural counties, but most mental health providers are located in urban areas. This creates a challenge for rural residents looking for providers close to home.
With one mental health care provider serving about 330 residents, Colorado is in the 90th percentile for per capita providers.54 That compares with about one mental health care provider for every 470 Americans nationally.
But Colorado’s mental health care providers are mostly located along the Front Range. A handful of rural counties — San Juan, Mineral, Conejos, Costilla, and Baca — have either one or no therapist, psychiatrist, counselor or other behavioral health provider, according to the National Provider Identification registry.54
Planning Infrastructure is Lacking
Though Colorado maintains licensure data on providers like psychiatrists and licensed
clinical social workers, the data do not provide crucial information for leaders in behavioral health to use in workforce planning, including:
• Whether behavioral health providers are practicing;
• What their patient capacity is;
• What insurance providers are accepting;
• Whether providers represent the diverse demographics of their patients; and
• The extent to which they are integrated into primary care.55
It’s Hard to Get Paid
Only slightly more than half of psychiatrists nationally take any sort of insurance,
whether private or public insurance like Medicare or Medicaid.56 By contrast, about four of five physicians of other specialties take insurance — which means more people have to pay out-of-pocket for mental
Q:The answer: All of the above. CHI’s research reveals that there is no single or even handful of solutions that will solve Colorado’s behavioral health workforce challenges. But Colorado’s leaders can start with these sustainable, promising strategies profiled in this report (see page 8):
• Integrate behavioral health care into primary care environments;
• Invest in nontraditional providers to offer community-based care; and
• Extend the existing behavioral health workforce using telehealth and other technologies.
The Issues Colorado Faces in Developing its Behavioral Health Workforce

health care compared with other types of health care. And this problem is even worse for Medicaid clients. Only 43 percent of psychiatrists accept Medicaid, compared with about three of four other doctors.
In addition, insurance reimbursement is comparably low for behavioral health providers. One analysis showed that in 2015, Colorado’s private insurers paid primary care providers 40.9 percent more than behavioral health care specialists for the same types of services — like “evaluation and management” visits for patients with low or moderate behavioral health needs.57
Substance Use Treatment is Especially Difficult
Other barriers are more complex. One example is the shortage of physicians trained to provide medication-assisted treatment (MAT) — a clinically proven opioid treatment approach that combines medication and social support services. Though about 482 Colorado providers are trained to prescribe buprenorphine — one of the drugs used in MAT — estimates suggest that less than half of them do.58, 59
The reasons are varied, including not having enough nursing or office support, problems getting federal authorization, reimbursement challenges, lack of parallel counseling services, expensive rural recruitment efforts, regulations on which provider types can deliver the treatment, and limits on patient loads. And some providers have negative perceptions of addiction medications or the patients that come to their offices to receive them.60
The Pipeline Needs Work
Education and training of a new generation of behavioral health providers — and
recruitment and retention of those providers — are not sufficient to meet Colorado’s needs.
Incentive-based programs like education loan repayment for working in rural areas have mixed evidence.61 Providers are only required to repay their loan and then they can leave the region. So it’s unclear whether these individuals stay in underserved parts of the state.
And though demographics of the workforce are not consistently collected, anecdotall report suggest behavioral health providers do not reflect Colorado’s racial and ethnic character.55 Programs that identify potential students and help them pursue a career in behavioral health — known as pipeline programs — are not sufficient to recruit a diverse set of workers.
What is Colorado Doing Already?Colorado is working on the issue. Here are some examples: • A handful of peer specialist programs in Colorado train
mental health care consumers in peer counseling to help others manage mental illness.
• Mental Health First Aid uses an evidence-based curriculum to teach consumers how to respond to the first signs of mental illness and substance abuse in their community.62
• Scholarship and loan repayment programs for health and behavioral health providers, like the federally funded National Health Service Corps and legislative efforts like Senate Bill 18-24, help incentivize providers to work in underserved areas.63
Where Are the Opportunities?
Key informant interviews and a review of the literature provided a list of other possible solutions that behavioral health leaders could pursue. These are below. The ones that emerged as most impactful, sustainable, and scalable based on our guiding principles are noted with an asterisk.
Planning and Policy
• Open new Medicaid behavioral health service codes to make behavioral health more billable to ensure adequate salaries for providers.*
• Ensure payment parity across physical and behavioral health services.
• Create statewide collaborative to develop a behavioral health workforce strategic plan.
• Provide salary support for rural providers.
Build the non-traditional workforce
• Mental Health First Aid*
• Peer support services*
• Train non-behavioral health providers like PCPs but also social workers, chronic disease managers, health navigators, community health workers, and clergy to address behavioral health needs.
Other recruitment efforts
• Loan repayment programs
• Strengthen pipeline programs
Extend current workforce
• E-consults* • Telehealth* • Crisis text services*

14 Colorado Health Institute
Looking AheadThe need for behavioral health care is great in Colorado. And despite many ongoing efforts, we’re still far away from a comprehensive system of care that promotes equity and good health for all Coloradans.
But our leaders are well positioned to address the needs. Foundations, state agencies, community organizations and private companies can
build momentum by investing in treatment and infrastructure but also advocacy and learning about emerging models of care. And their stewardship can stimulate others to come forward with resources and innovative ideas.
With a collaborative approach, Colorado’s behavioral health leaders can address our state’s most pressing needs.
Endnotes1 Colorado Health Institute. (2017). "Colorado’s New Normal: State Maintains Historic Health Insurance Gains." Available at: https://www.colorado-
healthinstitute.org/sites/default/files/file_attachments/2017%20CHAS%20DESIGN%20FINAL%20for%20Web.pdf 2 Mental Health America. (2018). "The State of Mental Health in America 2018." Available at: http://www.mentalhealthamerica.net/sites/default/
files/2018%20The%20State%20of%20MH%20in%20America%20-%20FINAL.pdf 3 Colorado Department of Public Health and Environment (CDPHE). "Vital Statistics Program." (Retrieved April 23, 2018 , from: https://www.colo-
rado.gov/pacific/cdphe/vital-statistics-program. 4 Colorado Health Institute. (2017). "Colorado’s New Normal: State Maintains Historic Health Insurance Gains." Available at: https://www.colorado-
healthinstitute.org/sites/default/files/file_attachments/2017%20CHAS%20DESIGN%20FINAL%20for%20Web.pdf5 Colorado Health Institute. (2017). "Colorado’s New Normal: State Maintains Historic Health Insurance Gains." Available at: https://www.colorado-
healthinstitute.org/sites/default/files/file_attachments/2017%20CHAS%20DESIGN%20FINAL%20for%20Web.pdf6 Substance Abuse and Mental Health Services Administration. (2014). Center for Behavioral Health Statistics and Quality, National Survey on
Drug Use and Health. (Retrieved April 23, 2018, from: https://www.coloradohealthinstitute.org/blog/abcs-mat-medication-assisted-treatment).7 Colorado Department of Human Services (CDHS). (2018). “Conference to Focus on Model Used in OBH Opioid Grant.” (Retrieved April 23, 2018,
from: https://www.colorado.gov/pacific/cdhs/article/conference-focus-model-used-obh-opioid-grant). 8 Brown, J. (2018). “Methadone clinics in Colorado have doubled in three years, but the state is still short on treatment options.” The Denver Post.
(Retrieved April 23, 2018, from: https://www.denverpost.com/2018/02/04/colorado-methadone-clinics-drug-treatment-options/). 9 Colorado Department of Health Care Policy & Financing. (2017). “Exploring Options for Residential and Inpatient Treatment of Substance Use
Disorder in Health First Colorado.” (Retrieved April 23, 2018, from: https://www.colorado.gov/pacific/sites/default/files/HCPF%202017%20Inpa-tient%20SUD%20Treatment%20Report.pdf ).
10 Addiction Policy Forum, Center for Health & Justice and National Criminal Justice Association. (2017). “Spotlight: Care Alliance for Opioid Addic-tion the Hub and Spoke Model.” (Retrieved April 23, 2018, from: http://docs.wixstatic.com/ugd/bfe1ed_ac5aeb89fca841118306dda74d2e50d3.pdf).
11 Fayhee, MJ. (2018). “West Springs psychiatric facility secures matching grant in fundraising effort.” Aspen Daily News. (Retrieved April 23, 2018, from: https://www.aspendailynews.com/news/west-springs-psychiatric-facility-secures-matching-grant-in-fundraising-effort/article_b0fc47f8-32ff-11e8-951d-3b4c842399fa.html).
12 National Alliance on Mental Illness. “Getting Treatment During a Crisis.” (Retrieved April 23, 2018, from: https://www.nami.org/Learn-More/Treatment/Getting-Treatment-During-a-Crisis).
13 CDHS. “Co-Responder Programs.” (Retrieved April 23, 2018, from: https://www.colorado.gov/pacific/cdhs/co-responder-programs).14 CDHS. (2018). “CDHS Announces New Community Behavioral Health Partnerships with Local Law Enforcement.” (Retrieved April 23, 2018, from:
https://www.colorado.gov/pacific/cdhs/2018-01-10-cdhs-new-behavioral-health-partnerships-law-enforcement).15 CDHS. (2018). “Committee to Evaluate, Improve Colorado’s Crisis System.” (Retrieved April 23, 2018, from: https://www.colorado.gov/pacific/
cdhs/2018-01-05-crisis-system-committee). 16 Healthy Kids Colorado Survey. (2015). (Retrieved April 23, 2018, from: https://drive.google.com/file/d/0B2nM-3jK5N8pa2c5Uy1tTUZ6NlU/view). 17 Colorado Education Initiative. “Colorado Health Schools Smart Source.” (Retrieved April 23, 2018, from: http://www.coloradoedinitiative.org/
our-work/health-wellness/smart-source/). 18 Centers for Disease Control and Prevention. (2014). “Connecting the Dots: An Overview of the Links Among Multiple Forms of Violence.” Preven-
tion Institute. (Retrieved April 24, 2018, from: https://www.cdc.gov/violenceprevention/pdf/connecting_the_dots-a.pdf ).

Colorado Health Institute 15
APRIL 2018
A Way Forward: How Colorado’s Behavioral Health Leaders Can Address Colorado’s Most Pressing Needs
19 National Resource Center for Mental Health Promotion & Youth Violence Prevention. “Project LAUNCH.” (Retrieved April 24, 2018, from: https://healthysafechildren.org/grantee/project-launch).
20 County Health Rankings & Roadmaps. (2017). “Trauma-informed juvenile justice systems.” (Retrieved April 24, 2018, from: http://www.county-healthrankings.org/take-action-to-improve-health/what-works-for-health/policies/trauma-informed-juvenile-justice-systems).
21 COACT Colorado. “What is COACT?” (Retrieved April 24, 2018, from: https://coactcolorado.org/about).22 County Health Rankings & Roadmaps. (2018). “Behavioral health primary care integration.” (Retrieved April 24, 2018, from: http://www.county-
healthrankings.org/take-action-to-improve-health/what-works-for-health/policies/behavioral-health-primary-care-integration).23 Mental Health America. (2016). “Position Statement 18: Cultural and Linguistic Competency in Mental Health Systems.” (Retrieved April 24, 2018,
from: http://www.mentalhealthamerica.net/positions/cultural-competence). 24 Miller, B et al. (2016). “Core Competencies for Behavioral Health Providers Working in Primary Care.” (Retrieved April 24, 2018, from: http://farley-
healthpolicycenter.org/wp-content/uploads/2016/02/Core-Competencies-for-Behavioral-Health-Providers-Working-in-Primary-Care.pdf ). 25 Patient-Centered Primary Care Collaborative. “Benefits of Integrating Behavioral Health in PCMH.” (Retrieved April 24, 2018, from: https://www.
pcpcc.org/content/benefits-integration-behavioral-health). 26 University of Colorado Anschutz Medical Campus. “About SIM.” (Retrieved April 24, 2018, from: http://www.ucdenver.edu/anschutz/about/prac-
ticetransformation/about/Pages/default.aspx). 27 Health Share of Oregon. “Project Nurture: A Center of Excellence Model Integrating Maternity Care and Addiction Treatment for Pregnant
Women with Substance Use Disorders.” (Retrieved April 24, 2018, from: http://www.projectnurtureoregon.org/projectnurture.)28 Rakover, J. (2016). “Project Nurture: Two Approaches to Integrating Perinatal Care with Substance Use Treatment.” Institute for Health-
care Improvement. (Retrieved April 24, 2018, from: http://www.ihi.org/communities/blogs/_layouts/15/ihi/community/blog/itemview.aspx?List=7d1126ec-8f63-4a3b-9926-c44ea3036813&ID=226).
29 Ko, JY et al. (2016). “Incidence of Neonatal Abstinence Syndrome – 28 States, 1999-2013.” Morbidity and Mortality Weekly Report 65(31): 799-802.
30 National Academies of Sciences, Engineering, and Medicine. (2016). “Ending Discrimination Against People with Mental and Substance Use Disorders: The Evidence for Stigma Change.” Chapter 4. (Retrieved April 24, 2018, from: https://www.nap.edu/read/23442/chapter/1#ii).
31 Mental Health First Aid. “Research & Evidence Base.” (Retrieved April 24, 2018, from: https://www.mentalhealthfirstaid.org/about/research/).32 Mental Health America. “Peer Support In Behavioral Health: The Evidence Is In.” (Retrieved April 24, 2018, from: https://www.mentalhealthameri-
ca.net/sites/default/files/Evidence%20for%20Peer%20Support.pdf ).33 Mental Health America. “MHA National Certified Peer Specialist Certification – Get Certified!” (Retrieved April 24, 2018, from: http://www.men-
talhealthamerica.net/mha-national-certified-peer-specialist-certification-get-certified).34 County Health Rankings & Roadmaps. “Telemental Health Services.” (Retrieved April 24, 2018, from: http://www.countyhealthrankings.org/take-
action-to-improve-health/what-works-for-health/policies/telemental-health-services).35 Arizona Telemedicine Program. “Telemedicine and Telehealth Service Provider Directory.” (Retrieved April 24, 2018, from: http://telemedicine.
arizona.edu/servicedirectory).36 Klein, S. (2014). “Behavioral Health Integration: Approaches from the Field.” Commonwealth Fund. (Retrieved April 24, 2018, from: http://www.
commonwealthfund.org/publications/newsletters/quality-matters/2014/august-september/profiles). 37 Lowenstein, M et al. (2017). “Psychiatric Consultation at Your Fingertips: Descriptive Analysis of Electronic Consultation from Primary Care to
Psychiatry.” Journal of Medical Internet Research 19(8): e279. 38 Blue Shield California Foundation. (2016). “Electronic Consult Reimbursement Roadmap.” (Retrieved April 24, 2018, from: https://www.
blueshieldcafoundation.org/sites/default/files/u19/eConsult%20GPS_032916.pdf). 39 Keystone Policy Center. (2017). “Bridging the Divide: Addressing Colorado’s Substance Use Disorder Needs.” (Retrieved April 24, 2018, from:
https://www.keystone.org/wp-content/uploads/2017/03/Keystone-SUD-final.pdf ). 40 Pearsall, CC. (2013). “Lessons for Strategic Health Equity Grantmaking.” Grantmakers in Health. (Retrieved April 24, 2018, from: http://www.gih.
org/files/FileDownloads/Issue_Focus_Health_Equity_Grantmaking_9-23-13.pdf ). 41Mitchell, F. (2016). “Innovations in Health Equity and Health Philanthropy.” Stanford Social Innovation Review. (Retrieved April 24, 2018, from:
https://ssir.org/articles/entry/innovations_in_health_equity_and_health_philanthropy). 42 World Health Organization. (2014). “Social Determinants of Mental Health.” (Retrieved April 24, 2018, from: http://apps.who.int/iris/bitstream/
handle/10665/112828/9789241506809_eng.pdf;jsessionid=581AAC7EB88F4D42EC9A211A0CDA03C1?sequence=1). 43 Compton, M and RS Shim. (2015). “The Social Determinants of Mental Health.” Focus 13(4): 419-425. 44 How Housing Matters. “How Housing Quality Affects Child Mental Health.” (Retrieved April 24, 2018, from: https://howhousingmatters.org/
articles/housing-quality-affects-child-mental-health/). 45 Gillespie, S, et al. (2017). “Denver Supportive Housing Social Impact Bond Initiative: Housing Stability Outcomes.” Urban Institute. (Retrieved
April 24, 2018, from: https://www.urban.org/sites/default/files/publication/94141/denver-sib-outcome-report_0.pdf).

The Colorado Health Institute is a trusted source of independent and objective health information, data and analysis for the state’s health care leaders. The Colorado Health Institute is funded by the
Caring for Colorado Foundation, Rose Community Foundation, The Colorado Trust and the Colorado Health Foundation.
303 E. 17th Ave., Suite 930, Denver, CO 80203 • 303.831.4200 coloradohealthinstitute.org
OUR FUNDERS
46 U.S. Department of Health and Human Services. (2009). “Building Your Program: Supported Employment.” (Retrieved April 24, 2018, from: https://store.samhsa.gov/shin/content/SMA08-4365/BuildingYourProgram-SE.pdf ).
47 Colorado Department of Human Services. “Individual Placement and Support (IPS) – Supported Employment.” (Retrieved April 24, 2018, from: https://www.colorado.gov/pacific/cdhs/individual-placement-and-support-ips-supported-employment).
48 Beeson, T, et al. (2013). “Making the Case for Medical-Legal Partnerships: A Review of the Evidence.” The George Washington School of Public Health and Health Services. (Retrieved April 24, 2018, from: http://medical-legalpartnership.org/wp-content/uploads/2014/03/Medical-Legal-Partnership-Literature-Review-February-2013.pdf).
49 Monica, K. (2017). “Evidence Supports Push for Social Determinants in EHR Data.” EHR Intelligence. (Retrieved April 24, 2018, from: https://ehrin-telligence.com/news/evidence-supports-push-for-social-determinants-in-ehr-data).
50 Robert Wood Johnson Foundation. (2016). “Using Social Determinants of Health Data to Improve Health Care and Health: A Learning Report.” (Retrieved April 24, 2018, from: https://healthleadsusa.org/wp-content/uploads/2016/06/RWJF-SDOH-Learning-Report.pdf ).
51 Monica, K. (2018). “Texas HIE to Link Social Determinants of Health to Patients EHRs.” EHR Intelligence. (Retrieved April 24, 2018, from: https://ehrintelligence.com/news/texas-hie-to-link-social-determinants-of-health-to-patient-ehrs).
52 Center for Lobbying in the Public Interest. (2010). “Foundations for Civic Impact: Advocacy and Civic Engagement Toolkit for Private Founda-tions.” (Retrieved April 24, 2018, from: https://www.councilofnonprofits.org/sites/default/files/documents/pf_toolkit_complete.pdf ).
53 The Atlantic Philanthropies. (2011). “Catalytic Philanthropy: Investing in Policy Advocacy.” (Retrieved April 24, 2018, from: https://www.atlan-ticphilanthropies.org/news/catalytic-philanthropy-investing-policy-advocacy).
54 County Health Rankings & Roadmaps. “Colorado Mental Health Providers.” (Retrieved April 24, 2018, from: http://www.countyhealthrankings.org/app/colorado/2018/measure/factors/62/data).
55 Western Interstate Commission for Higher Education. (2010). “The Behavioral Healthcare Workforce in Colorado: A Status Report.” (Retrieved April 24, 2018, from: https://www.wiche.edu/info/publications/bhWorkforceColorado2010.pdf).
56 Bishop, TF, et al. (2014). “Acceptance of Insurance by Psychiatrists and the Implications for Access to Mental Health Care.” JAMA Psychiatry 71(2): 176-181.
57 Melek, S, and D Perlman. (2017). “Addiction and Mental Health vs. Physical Health: Analyzing Disparities in Network Use and Provider Reim-bursement Rates.” Milliman Research Report. (Retrieved April 24, 2018, from: http://www.milliman.com/uploadedFiles/insight/2017/NQTLDis-parityAnalysis.pdf ).
58 Substance Abuse and Mental Health Services Administration. “Buprenorphine Treatment Practitioner Locator.” (Retrieved April 24, 2018, from: https://www.samhsa.gov/medication-assisted-treatment/physician-program-data/treatment-physician-locator).
59 Colorado Health Institute. (2017). "Miles Away from Help: The Opioid Epidemic and Medication-assisted Treatment in Colorado." Available at: https://www.coloradohealthinstitute.org/sites/default/files/file_attachments/2017%20MAT%20report.pdf
60 Volkow, N, et al. (2014). “Medication-assisted Therapies – Tackling the Opioid-Overdose Epidemic.” New England Journal of Medicine 370(22): 2063-2066.
61 County Health Rankings & Roadmaps. “Higher Education Financial Incentives for Health Professionals Serving Underserved Areas.” (Retrieved April 24, 2018, from: http://www.countyhealthrankings.org/take-action-to-improve-health/what-works-for-health/policies/higher-education-financial-incentives-for-health-professionals-serving-underserved-areas).
62 Jorm, AF, et al. (2004). “Mental Health First Aid Training of the Public in a Rural Area: A Cluster Randomized Trial.” BMC Psychiatry 4(33): 1-9. 63 Colorado General Assembly. “Expand Access to Behavioral Health Care Providers.” (Retrieved April 24, 2018, from: http://leg.colorado.gov/bills/
sb18-024).