A Toolkit for Ward Sisters and Charge Nurses
38
BCUHB Nutrition and Hydration Human Rights Project Group A Toolkit for Ward Sisters and Charge Nurses
Transcript of A Toolkit for Ward Sisters and Charge Nurses

BCUHB Nutrition and HydrationHuman Rights Project Group
A Toolkit forWard Sisters andCharge Nurses

© Betsi Cadwaladr University Health Board 2012.All rights reserved. Not to be reproduced in whole orin part without the permission of the copyright owner.
Supported by Awyr Las, Registered Charity No. 1138976


Putting Human Rights at the Heart of Nutrition and Hydration
is toassist Ward Sisters andCharge Nurses to developand use human rights based
approaches to the planning anddelivery of care. It has beenproduced by drawing on theexperiences of service users, staff,stakeholders and organisations withexpertise in both human rights andhealth. It is championed at Boardlevel by the Director of Nursing,Midwifery and Patient Services whois the strategic lead for Nutrition andPatient Services. It is built upon thework of the Nutritional Assessmentand Pathways TransformationalGroups at Betsi CadwaladrUniversity Health Board and hasbeen developed by a steeringgroup in collaboration withstakeholders, service users and staff.
High quality nutrition and hydrationare fundamental aspects of care andare basic prerequisites for the
effective management of patients'basic needs. Adequate hydrationand a balanced diet, appropriate toan individual's needs are importantfactors that influence patient clinicaloutcomes and also their satisfactionwith the quality of care providedand hospital stay overall. The lack ofthese factors can also have severeconsequences for a patient's healthand well being, and are likely toconstitute a violation of anindividual's human rights. Taking ahuman rights based approach canprovide a way for everyone in anorganisation to make realimprovements in people's lives.
Nationally and internationally therehave been a number of initiativesand documents that set thestandards for hospital catering andpatient nutrition. However there donot appear to be specific guidelineswhich make the direct link betweenhydration, nutrition and humanrights, particularly in relation to theobligations on service providerswhich follow from the
.
T

Putting Human Rights at the Heart of Nutrition and Hydration
This is important as we becomeincreasingly aware nationally ofincidences where patients' nutritionand hydration needs have beenneglected, to the point whereindividuals have been malnourished,dehydrated and in extreme painand suffering.
This toolkit attempts to provide acomprehensive account of measuresneeded to ensure that every patient'shydration and nutritional needs aremet. It is driven by the patient'sneed for basic human dignity in thecare environment, a right to whicheveryone is entitled, under nationaland international human rightslegislation. This human rights basedapproach seeks to ensure thatpatients and staff are treated asindividuals and that their dignity andrights are placed at the heart of alldecisions and services. Such anapproach will be of practical valueto our organisation and thoseindividuals within, providing betterservices for patients and theirfamilies.
'' aims to
enable WardSisters and Charge Nurses, usingtheir professional judgement, tobuild human rights into policy andpractice, particularly as these relateto nutrition and hydration in theward environment. Whilst the focusof the toolkit is on nutrition andhydration, a human rights basedapproach must take into account allaspects of care, and will have aneffect on how they are delivered.
1. Introduction

Putting Human Rights at the Heart of Nutrition and Hydration
● We will have a conscious approach to humanrights principles and values (fairness, respect,equality, dignity and autonomy)
● We will place the patient as an individual atthe centre of this work
● We will involve patients and staff in thisdevelopment
● We will identify, monitor and protect the rightsof the most vulnerable
● We will inform and empower patients andstaff about human rights
● We will embed this approach into day to dayactivity
● We will be innovative
● We will use service improvement methodology
● We will communicate the benefits of a humanrights based approach

Putting Human Rights at the Heart of Nutrition and Hydration
Human rights represent all thethings that are essential to us ashuman beings, such as beingable to choose how to live our lifeand being treated with dignityand respect.
Many of the rights in the HumanRights Act (2000) are relevant tohealthcare, among them, the rightto life, prohibition of torture andinhuman and degrading treat-ment, the right to liberty, to a fairtrial and respect for private andfamily life.
Our human rights basedapproach to hydration andnutrition places human rights atthe centre of our policies andpractice and the patient at thecentre of his or her own care.
Health organisations as a publicbody have a legal requirement toact in accordance with theHuman Rights Act (2000) andtheir core values should be at theheart of everything we do.
Human rights belong to everyone. They are the basic rights weall have simply because we are human, regardless of who weare, where we live or what we do.
F a i r n e s s
R e s p e c t
E q u a l i t yD i g n i t y
A u t o n o m y

Putting Human Rights at the Heart of Nutrition and Hydration
Almost everyone will come into contact with the NHS at some point in their lives,usually when they are at their most vulnerable. Human rights values are in many waysthe very same values that lie at the heart of good healthcare.
This means that putting humanrights at the heart of the wayhealthcare services are designedand delivered can make forbetter services for everyone, withpatient and staff experiencesreflecting the core values offairness, respect, equality,dignity and autonomy

Putting Human Rights at the Heart of Nutrition and Hydration

Putting Human Rights at the Heart of Nutrition and Hydration
● Ward Sister/Charge Nurse
● Doctors
● Matron
● RegisteredNurses
● SpecialistNurse
● Health CareSupportWorker
Accountable for the day to daymanagement of the patients’nutritional and hydrationrequirements and high standards ofcare. This is done through ensuringall patients receive Nutritional RiskScreening (identification of thedietary needs of patients) thatpatients receive appropriate, wellpresented food and assistance toeat where required. Implementingand managing protective mealtimesand referring to specialists asrequired.
Make an assessment of the patient'snutritional and hydration state,including an evaluation of their diet;general physical condition; andmeasurement of height, weight andbody mass index. Recognises theimpact of nutritional and hydrationissues on the clinical outcome ofdisease process and directs caremanagement plan. Leads the multi-disciplinary specialist nutritionsupport team, bringing together thecollective expertise for the provisionof coherent nutritional support.
Lead by example by providing anauthoritative and visible presence inward areas, setting and monitoringthe highest standards of care andensuring that patients nutritionalneeds are met. Ensuring thatpatients and their families aretreated with dignity and respect andthat the ward staff have the required
resources including staffing andequipment to deliver quality care.
Play a key role in providing patientcentred nutritional care, workingclosely with the widermultidisciplinary team, to ensure thenutritional needs of individualpatients are being met in a way thatis appropriate and safe. Undertakenutritional risk screening, weight,BMI and basic swallowingassessment, ensuring patientsreceive appropriate food and fluidsand assistance where necessary.Plan, monitor, evaluate anddocument nutritional and hydrationcare and communicating the clinicalreasons for adopting alternativefeeding options.
Member of the specialist nutritionsupport team, providing advancedknowledge, skills and advice on allaspects of enteral and parenteralnutritional care. Leads anddevelops operational policy,procedure and audit, providesspecialist advice, education andtraining for nurses, doctors, studentsand the multidisciplinary team.
Prepares the mealtime environment,ensuring patients are comfortableand have washed their hands. Assistpatients with food choice, servemeals, provide assistance forpatients that need help with eatingand drinking, monitor and document
4.1 WardsandDepartments

Putting Human Rights at the Heart of Nutrition and Hydration
food and fluid intake.
Assist with food choice and serving,ensuring ward area is clean andconducive to pleasant mealtimeenvironment for patients. Ensuresnacks available to patients outsideset mealtimes and work closely withcatering department to ensure wardprovisions meet patient need.
Member of the nutritional supportteam providing nutritional adviceand expertise on dietary changesidentifying appropriate foodchoices, nutritional supplements andtherapeutic diets and, wherenecessary, specialised forms ofartificial feeding. Undertakeindividual patient nutrition screening,develop and implement nutritionalcare plan and monitor and adjustthe patient's response to the nutritioncare delivered. Work closely withcatering department to ensure thatthe meals provided are nutritiousand meet the nutritional, cultural andreligious needs of all patients.
Work with patients who havedifficulty with feeding andswallowing. Provide specialistadvice to ward staff, undertakingspecialist swallowing assessmentand advising on textured modifieddiet and fluids specific to patientneed. Work across the
multidisciplinary framework toassess, diagnose, manage and treatpatients as well as offering advice,training and education tocolleagues, carers and families
Member of specialist NutritionSupport Team addresses the care ofpatients who receive specializednutrition support, includingparenteral and enteral nutrition,responsibility for promotingmaintenance and/or restoration ofoptimal nutritional status,designing and modifying treatmentaccording to the needs of thepatient.
Help patients whose independenceor ability to live a normal life hasbeen affected. Assisting patient tolearn new skills or adapt existingones to enable them to engage inall aspects of their lives. This mayinclude advice on adapting theirenvironments such as ensuringcorrect seating and positioning tosupport safe eating and enablingindependence by helping patients tofeed themselves, for example, byproviding adapted eating ordrinking utensils.
Help patients having surgery orcomplicated orthodontic treatment,or those with particular medicalconditions to maintain a healthymouth, thereby optimising ability tomeet nutrition needs.
● Housekeeper
● Dietician
● Speech andLanguageTherapist
● Pharmacist
● OccupationalTherapist
● DentalHygienist

Putting Human Rights at the Heart of Nutrition and Hydration
● Physiotherapist
● CateringManager
● Porters
● Procurementand SuppliesOfficers
● NHS Board
● ExecutiveBoardMember
Advises on appropriate and timelypositioning, including the provisionof suitable seating to enable thepatient to sit comfortably and withgood posture for eating andswallowing.
Responsible for catering servicesincluding procuring, choosing andordering food, menu planning takinginto account dietetic advice andpatients' needs; managing staffrestaurant, maintaining food safetyand hygiene standards, controllingcosts and monitoring waste, auditingpatient satisfaction and training anddevelopment of staff.
Delivering food to ward at agreedtimes, removal of trolleys aftermealtimes.
Liaise with multidisciplinary team toensure the procurement of food anddrinks from sustainable and safesources which meets the diverseneeds of hospital inpatients, staffand visitors.
The Board ensures there are clearaccountabilities and performancemanagement arrangements forcatering and patient nutritionthroughout the organisation up toBoard level. They obtain assurancethat the delivery of catering andpatient nutrition services meetsnational guidelines, legislation andrecognised best practice.
A designated board level directorwith lead responsibility for cateringservice and patient nutrition withinthe Health Board, ensuring that thereis a strategy in place to deliverhospital catering and patientnutrition, that services are of a highstandard and recognise bestpractice and that there areestablished performancemanagement arrangements tomonitor and achieve serviceimprovements.
4.2 Catering and Portering
4.3 The Board

Putting Human Rights at the Heart of Nutrition and Hydration
Safe
tyId
entif
y vu
lner
able
pat
ient
san
d th
ose
at r
isk
at th
ebe
ginn
ing
of e
very
shi
ft.Es
tabl
ish
an a
lert
syst
em
Envi
ron
men
tEn
sure
app
ropr
iate
envi
ronm
ent o
f car
ein
clud
ing
acce
ss to
equi
pmen
t
Au
dit
co
mp
lia
nce
an
dM
ea
sure
im
pro
vem
en
tM
UST
aud
it an
d Fu
ndam
enta
lsof
Car
e au
dits
. Ide
ntify
,m
onito
r an
d le
arn
from
conc
erns
Mea
l ti
mes
Ensu
re m
ealti
mes
are
prot
ecte
d. E
nabl
e an
d pr
omot
eap
prop
riate
invo
lvem
ent o
f car
ers
and
volu
ntee
rs
Ch
oic
eEn
able
and
pro
mot
e ch
oice
and
ensu
re 2
4 ho
ur a
cces
sto
food
and
drin
ks
Emp
ow
er
pa
tien
tsa
nd
th
eir
fa
milie
sEn
sure
and
ena
ble
regu
lar
com
mun
icat
ion.
Ens
ure
patie
nts
auto
nom
y an
ddi
gnity
is r
espe
cted

Putting Human Rights at the Heart of Nutrition and Hydration
Six Key
Areas
For
Intervention
Six key areas and arange of relatedinterventions have beenidentified bystakeholders at BetsiCadwaladr UniversityHealth Board to puthuman rights at theheart of hydration andnutrition
1. Safety
2. Environment
3. Audit and Compliance
4. Meal Times
5. Choice
6. EmpowermentIn this section (pages 11to 23) the 6 key humanrights are laid out inmore detail.
The Human Rights Act came intoforce in the UK on 2 October2000. The Act brought most ofthe rights contained in theEuropean Convention onHuman Rights into UK law. Italso placed a duty on
- to comply with theHuman Rights Act in everythingthat they do. Public authoritiesinclude health boards, localauthorities and centralgovernment departments amongother institutions.
A very few human rights areknown as . This meansthat they can never be limited orrestricted in any way. Publicauthorities - and theGovernment - need to ensurethat these rights are bothrespected and protected. Thereare very few absolute rights, butthey include the right to life andfreedom from torture, inhumanand degrading treatment.
A failure to respect these rights,whatever the reason, is unlawful
under UK law. However, thelevel of suffering or degradationwould need to be very high toclass as inhuman and degradingtreatment under the HumanRights Act.
The majority of rights areclassed as andcan be limited or restricted incertain circumstances,particularly when they conflictwith the rights of otherindividuals or the interests ofwider society. Embeddinghuman rights is about ensuringthat minimum certain standardsof care are respected forindividuals. Where restrictionson rights are necessary, theyshould be to theend that needs to be achievedand should ensure a properbalance between the needs andrights of other patients and staff.A proportionate action is onethat is reasonable and notexcessive in the circumstances.The principle of proportionalityis central to the human rightsframework. It helps to ensure
that any interference with a rightis kept to a minimum.
Certain questions can be askedto help decide whether arestriction on someone's rightscan be justified:
Is there an alternative approachto the problem that would allowfull respect for the person'srights?
Is there anything that we can doto minimise the restriction? Astraightforward way of thinkingabout proportionality is '
. The important pointis that any restriction of aperson's rights must be carefullyjustified, strictly necessary, andas small as possible.

Putting Human Rights at the Heart of Nutrition and Hydration
A hospital patient desperatefor a drink of water had totelephone the switchboard ofthe hospital he was beingtreated in to beg to see adoctor. He said that nurseswere refusing to give him anywater because he hadknocked over the first cup ofwater he had been given. Butwhen the doctor arrived hewas turned away by the wardnurse, who said he was overreacting and threatened toconfiscate his phone. Theman died eight hours later.His condition had not initiallybeen life-threatening, and aninvestigation concluded thathad it not been for thefailings of the ward nurse hewould have survived. Thiskind of situation couldbreach the right to life.
Source: Bexley Times
“This lady who is 100 yrs oldhas difficulty moving and yeton a previous visit to thehospital her food and drinks(especially water) was placedat the end of the bed, shecouldn’t reach and nobodycame to help her and as aresult was dehydrated, shewas glad to get back to hercare home”.
Source: BCUHB Picker Survey2011
.
Source: BCUHB Picker Survey2011
“Please help with food anddrink if the patients cannotdo it themselves.”
Source: BCUHB Dignity Survey2011

Putting Human Rights at the Heart of Nutrition and Hydration
The case study raises a number ofhuman rights issues, including:
Patients should always be givenenough to eat and drink to keepthem alive and well and shouldcertainly never be bywithdrawing these. If hospital stafffail to provide enough food / water,for whatever reason, they may bebreaching the right to life. This rightis absolute so there is never anyjustification for failing to respect it.
Staff are also obliged to step in toprotect someone's life, even where itis not through their own fault. Forexample, if a patient is brought intothe hospital suffering frommalnourishment they must addressthis as far as they are able. This isknown as a positive obligation. Itmeans that staff must takereasonable steps to protectsomeone's life where it is at risk.
If a patient with capacity is refusingdrink and food, the duty to protectlife does not extend to forcing thepatient to eat or drink. Patientchoice should be respected,otherwise this will itself raise issuesunder Article 8, respecting patient'sautonomy, or even Article 3, if forcefeeding were to lead to inhuman ordegrading treatment.
If patients' lives are put at riskthrough lack of food/drink, even ifthis does not lead to death, it is
likely to be extremely painful andhumiliating and may be a breach ofArticle 3. There is a positiveobligation under Article 3 to takereasonable steps to preventindividuals from inhuman ordegrading treatment or punishment.In the case study, the 'punishment'and the patient's suffering throughlack of water may both haveengaged Article 3.
If a patient's suffering is not severeenough to reach the high thresholdof Article 3, the lack of food/watermay engage Article 8. The right torespect for private life includes aright to physical and psychologicalintegrity, which may be violated by alack of food/water.
In the case study, the actions of theward nurse are most directlyresponsible for the patient's deathand suffering beforehand. But thedoctor may also have had anobligation to insist on seeing thepatient given the severity of theclaim. Other staff members, if theywitnessed the patient's sufferingshould have stepped in to assist him- even if this meant overriding theorders of the ward nurse. The rightto life and the right to be free frominhuman and degrading treatmentare more important than internalregulations or orders and staffmembers would be acting unlawfullyif they did not act to save life whenthey knew it was at risk.
Human Rights Act(2000)

Putting Human Rights at the Heart of Nutrition and Hydration
The All Wales Nutritional CarePathway is in place on the ward,with weight and nutritionalscreening undertaken for patientswithin 24 hours of admissions andthe care plan followed as per therisk status.
� Identify vulnerable patients atrisk of malnutrition anddehydration
� Intentional rounding forhydration and nutrition needstakes place by the teamleader during every shift
� The team leader will identifypatients at risk ofmalnutrition and/ordehydration andcommunicate this to thenurse in charge, team andhousekeeper at the safetybriefing at the beginning ofevery shift.
� Visual prompts will beinstigated by thehousekeeper/nurse in chargeto signify patients who needassistance/prompting i.e. redlids on jugs and symbolidentification on individualbed boards
� The identification of ‘at risk’patients will be highlightedon the ‘at a glance’ boardoutlining relevant referrals toappropriate healthcareprofessions e.g. Speech andLanguage Therapy, Dietetics,Occupational Therapist,Nutrition Support team
� Registered Nurse delegatesagreed nutrition andhydration care needs forpatients identified at risk aspart of nursing orders toHealthcare Support Workers
� During intentional roundingthe assessment of fluidbalance charts and foodcharts will be carried out bythe by nurse in charge atleast once a day
� During intentional roundingstaff will ensure that oralfluids are offered a minimumof 2 hourly (Supported IntakeProgrammes SIPS)
� All ward based staff willundertake the nutritionale-learning and equality andhuman rights training
� The nurse in charge will beaccountable for ensuringthat patients have enoughfood and water during theirstay to meet nutritional andhydration requirements

Putting Human Rights at the Heart of Nutrition and Hydration
Mrs S, aged 102, feltdisrespected andneglected while she was inhospital. Despite being blind,her meals and drinks were lefton a trolley - in most caseswithout even letting her knowthey were there. For the mostpart, staff also did not offerany assistance with eating ordrinking. As a result, many ofthe meals were removeduntouched. Mrs S alsosuffered a great indignitywhen she asked for acommode, but was told by anurse that she could use herincontinence pad. This kind oftreatment is unacceptableand could amount toinhuman or degradingtreatment.
Source: Age Concern: On the RightTrack?
Source BCUHB Picker Survey2011
"Nurses kept food for meso I could eat when I could;terrible Nausea problems."
Source: BCUHB Dignity Survey2011

Putting Human Rights at the Heart of Nutrition and Hydration
The case study raises a number ofhuman rights issues, including:
This right can be very relevant forolder or vulnerable people. Inhumantreatment means treatment causingsevere mental or physical suffering;degrading treatment meanstreatment that is grossly humiliatingand undignified. Not being able toaccess food or water, even if staffbelieve they have delivered it to thepatient, could result in dehydrationand malnutrition and may engageArticle 3.
As with the case study above, if the
patient's suffering is not severeenough to reach the high thresholdof Article 3, the lack of food/watermay engage Article 8.
This article prohibits discriminationwhere any other rights in the HRAare engaged. It recognises that toavoid discrimination or secure equalrights, it may sometimes benecessary to treat an individual orgroup differently because theirsituation is different from others. Inthe case study above, the hospitalstaff should have recognised thatbecause Mrs S was blind, sheneeded extra assistance with eatingand drinking.
Human Rights Act(2000)
The immediate environment should be preparedin order for patients to be able to enjoy theirfood in a dignified manner.
All members of the ward team should beinvolved in this as a mater of routine.
� Appropriate equipment will be availableincluding adapted cutlery, plates andcups, seating, tables; a designateddining area will be utilised whereavailable
� Assistance will be provided to patients toattend dining areas or to sit in a chair oradopt a suitable eating/drinking positionas appropriate
� Clearing and cleaning of tables will becarried out before and after mealtimes
� Hand washing is encouraged andfacilitated before and after meals
� Toileting is offered before meal times.Patients are encouraged and enabled toutilise toilet facilitates out of the wardbay environment where appropriate
� Patients receive their meals in anuninterrupted setting as possible
� The nurse in charge will ensure flexibilitywith visiting during protected mealtimesto enable relatives to assist patients

Putting Human Rights at the Heart of Nutrition and Hydration
� As part of the daily ward roundundertaken by the nurse in charge,nutrition and hydration managementplans will be evaluated to ensureassessments are up to date andmanagement plans are implemented anddocumented
� Registered nurses should ensure foodand fluid intake is documented, and thatfood charts are countersigned
� All Ward Sisters/Charge Nurses willundertake MUST audits monthly as arequirement of the Care metrics; andFundamentals of Care audits twice ayear
� Local Fundamentals of Care metrics willreflect the requirements of this documentand inform compliance reports
� Spot checks will be undertaken byWard Sisters/Charge Nurses andMatrons and any issues rectified
� Trends from on the spot concernsrelated to nutrition and hydrationwill be collated and action plansformulated by the Ward Sister inconjunction with the Matron
� Trends from allconcerns/complaints will becollated and action plansformulated by the Ward Sister inconjunction with the Matronoutlining clear responsibilities foraction.
� Compliance in relation to nutritionand hydration elements of this toolkit will be measured at a minimumon a monthly basis and displayedwithin the ward/units on runcharts.
Any instances of nutritional or hydration carethat falls below the expected standards will beinvestigated and appropriate action instigated.

Putting Human Rights at the Heart of Nutrition and Hydration
Key human rights raised by this caseinclude Articles 3 and 8.
Although patients do not haveautomatic access to food 24-hoursa day when in hospital, individualpatient requirements must be takeninto account and accommodatedwhen possible.
To ensure patients do not becomedehydrated, hospitals should ensurethey have constant access to water.
Allowing patients to have visitorsduring meal times may assisthospital staff as visitors may be ableto assist patients who need supportto eat. In other cases, visitors mayinhibit certain patients from eating.The policy should allow for flexibilityto meet individual needs..
I used to turn up specificallynear to lunchtimes to ensurethat my father would eat hisfood. Besides helping him, Iwould end up checkingseveral other patients whohad no visitors - which wasmost of them - to help themget something to eat. Therewere no NHS staff to assist theolder people.
Plates were put in the servingarea and left there oftenuntouched.
Usually the patient could notpick up both a knife and afork because they did nothave the strength to use twoutensils. More importantly theycould not cut up the meat etc.in to smaller sizes to get intotheir mouths.
Source: 'Still Hungry to Be Heard',Age UK 2010
Human Rights Act(2000)

Putting Human Rights at the Heart of Nutrition and Hydration
� The nurse in charge will ensure thatprinciples of protected mealtimes arepractised and every effort is made tominimise planned interruptions
� Ensure protected mealtime signage isdisplayed on the entrance to the ward
� On a daily basis a named member ofthe team will be responsible for themealtime experience and adopting therole of the 'maître D'
� All food and drink will be in easy reachfor patients who are able to help
� Assistance will be given to all patientswho are identified as unable to eat anddrink themselves. Allied healthprofessionals will provide support forpatients to maintain nutrition andhydration where appropriate
� The team leader, in conjunction with thehousekeeper and the team, will ensurethat families and carers who wish toassist with feeding during protected mealtimes are encouraged, enabled andsupported to do so. Family and carerswill be approached by the team leaderduring visiting to identify whether theywish to be involved or not
� Medical staff and professions allied tomedicine will be made aware of theprinciples of this toolkit and work withthe nurse in charge to ensure thatmealtimes are protected whereverpracticable to do so
� The Nurse in Charge will ensure thatstaff breaks are aligned to supportmealtimes for patients
� The ward roster will provide adequatestaff numbers during meal times tosupport patients requiring assistance.The Matron will be informed where this isnot the case and will be responsible forensuring adequate staffing to meetpatient needs
Putting Human Rights at the Heart of Nutrition and Hydration
"The food options for my diet(vegan) were awful. Dined onbaked potato and overcooked
baked beans"
Source: BCUHB Picker Survey 2011
Source: BCUHB Picker Survey2011
The food was disgustingeverything was cold. Myfamily brought mesandwiches everyday.Even the salads werewilted and not edible.Thank god for Weetabixand cheese & biscuits."
Source: BCUHB Picker Survey2011
The 'choice' ( ) aspects ofthe examples above are mostobvious in the case of the veganpatient - and this may also be anexample of discrimination. Patientswith particular dietary needs,resulting from strongly held beliefs,should not be made to eat anythingwhich goes against their principlesas this would be an infringement oftheir autonomy. They should beprovided with the same degree ofnutrition as other patients and thereshould also be an element of varietyin their diet - just as there should befor other patients.
Human rights may also be engagedby the examples above if they leadto malnutrition - for example, forlong-term patients. In extreme casesthis may be a case of inhuman anddegrading treatment (Article 3) or inlesser cases to a violation of apatient's physical integrity (Article 8)Autonomy is also important where apatient refuses to eat or refusesartificial nutrition and hydration. Thepatient's wishes should normally berespected if it is certain that thepatient has capacity to make thisparticular decision. However, sincethis may be a right to life concern,
Human Rights Act(2000)
Putting Human Rights at the Heart of Nutrition and Hydration
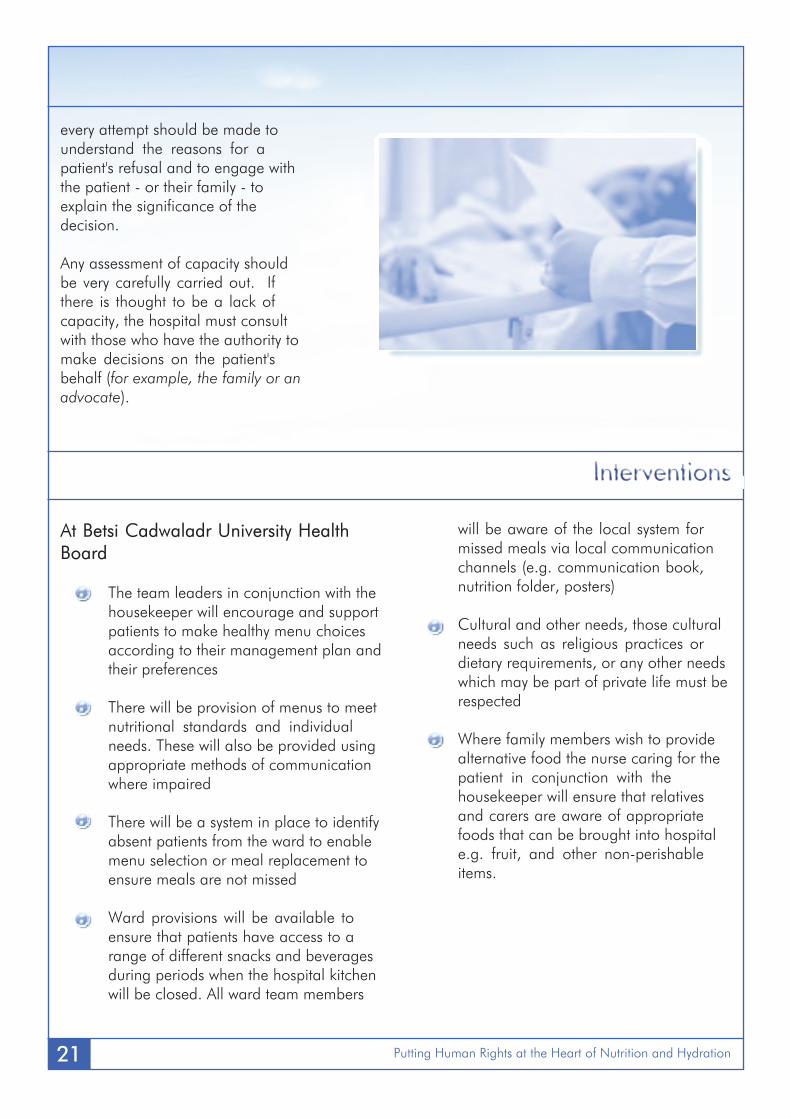
every attempt should be made tounderstand the reasons for apatient's refusal and to engage withthe patient - or their family - toexplain the significance of thedecision.
Any assessment of capacity shouldbe very carefully carried out. Ifthere is thought to be a lack ofcapacity, the hospital must consultwith those who have the authority tomake decisions on the patient'sbehalf (for example, the family or anadvocate).
� The team leaders in conjunction with thehousekeeper will encourage and supportpatients to make healthy menu choicesaccording to their management plan andtheir preferences
� There will be provision of menus to meetnutritional standards and individualneeds. These will also be provided usingappropriate methods of communicationwhere impaired
� There will be a system in place to identifyabsent patients from the ward to enablemenu selection or meal replacement toensure meals are not missed
� Ward provisions will be available toensure that patients have access to arange of different snacks and beveragesduring periods when the hospital kitchenwill be closed. All ward team members
will be aware of the local system formissed meals via local communicationchannels (e.g. communication book,nutrition folder, posters)
� Cultural and other needs, those culturalneeds such as religious practices ordietary requirements, or any other needswhich may be part of private life must berespected
� Where family members wish to providealternative food the nurse caring for thepatient in conjunction with thehousekeeper will ensure that relativesand carers are aware of appropriatefoods that can be brought into hospitale.g. fruit, and other non-perishableitems.

Putting Human Rights at the Heart of Nutrition and Hydration
"Mr W was 79 years old sufferedfrom dementia and depressions,was frail and recently widowed.He was admitted to hospital withdehydration and depression. Thehospital treated Mr W withintravenous fluids andantibiotics, which were stoppedwhen his chest infection clearedup. A week later, his daughter,herself a former nurse, told adoctor caring for Mr W of herconcerns that his generalcondition had deterioratedduring his admission and that hewould be better off receivingintravenous fluids. The doctorsaid he could not do this as itwould 'prevent his leavinghospital' and that 'he can meethis needs orally'. Mr W'sdaughter disagreed as hefrequently refused to eat anddrink more than very smallamounts"
Source: Ombudsman Careand Compassion 2011
Patients must be supported as far aspossible to make their own informedchoices about their care - includingwhere this relates to diet. Patientsmay need support to understandtheir rights.
There should be systems in place toallow them to complain if they feeltheir rights are not respected.
Too often a person may not realisethat they are able to do somethingabout their situation, or even thatthere is something wrong with theway they are being treated.
In cases such as the example above,patients and their families who maybe acting in their best interests,should feel able to insist on bettercommunication, advice and infor-mation.
It is vital that everyone isempowered and able to accessinformation about their humanrights so they can challenge poortreatment and demand betterservices.

Putting Human Rights at the Heart of Nutrition and Hydration
� The Nurse in Charge or team leaderdiscusses and agrees management planof high risk vulnerable patients with thepatients and relatives, this will includeensuring relatives are aware of theflexibility around visiting at mealtimes toprovide assistance
� Information is provided on lockers settingout Betsi Cadwaladr University HealthBoard’s commitment to meeting nutritionand hydration needs and encouragingpatients and families to highlightindividual requirements
� The housekeeper, or other ward staff,will undertake a daily ward round togather feedback relating to the quality ofthe mealtime experience, this will berelayed to the team leader and the Nursein Charge. On the spot concerns will becompleted and acted upon immediately
� Matrons will be available at mealtimes tooversee the mealtime experience
� Human rights information will bedisplayed on the ward and madeavailable to patients and their families
Putting Human Rights at the Heart of Nutrition and Hydration
1.
In other words, to make it possible for people todirectly raise or claim their human rights withincomplaints and legal systems here in the UK. It alsomeans that human rights issues are now interpretedby British courts, in addition to the European Court ofHuman Rights, giving greater domestic ownership tothe Convention.
2.
The Human Rights Act is about much more thancompliance with the law by public authorities. TheAct was intended to place human rights at the heartof public service delivery, and through this to makerights a reality for all people in the UK.
(DOH 2008)
♥ The to life
♥ The not to be tortured ortreated in an inhuman ordegrading way
♥ The to be free from slavery orforced labour
♥ The to liberty and security
♥ The to a fair trial
♥ The to no punishmentwithout law
♥ The to respect for private andfamily life, home andcorrespondence
♥ The to freedom of thought,conscience and religion
♥ The to freedom ofexpression
♥ The to freedom of assemblyand association
♥ The to marry and found afamily
♥ The not to be discriminatedagainst in relation to theenjoyment of any of the rightscontained in the EuropeanConvention
♥ The to peaceful enjoyment ofpossessions
♥ The to education
♥ The to free elections
The Human Rights Act cameinto force in the UK inOctober 2000.
The Act has two main aims:
What is the
trying to achieve ?

Putting Human Rights at the Heart of Nutrition and Hydration
Additional information for staff can be found on the Betsi Cadwaladr University Health Board intranetpage under ‘Clinical Resources’ page and then the ‘Nutrition’ link

Putting Human Rights at the Heart of Nutrition and Hydration
Safety Briefings are a simplecommunication tool for frontline staff on a face to facedaily basis in the clinicalenvironment for everydayconcerns / issues regardingsafety.
They are an opportunity for allstaff to be involved in raisingsafety awareness in the clinicalenvironment. Briefings helppromote a culture of safetyand can foster qualityimprovement.
The briefings are short and canlast from andneed to be concise.
The whole team areencouraged to contribute tothe briefing, this can includenon nursing staff e.g. WardClerks, Domestics,Housekeepers and the MedicalTeam.
m Led by the person designatedin charge of the clinical shift
m Held at the end of shifthandovers or during the shift
m Held at the patient status "at aglance" (PSAG) board
m Items discussed at the briefingcan be added to the computergenerated patient handoversheet
m Examples of items raisedduring briefings are:
○ Environmental issues withe.g. Ward area closed dueto infection
○ Manual handlingequipment
m Patient(s) deemed at risk offalls
m Patient(s) deemed at risk ofPressure Ulcers
m Patient(s) requiring assistancewith nutrition and hydration
m Patient(s) at risk of unsafeswallow
The briefing is an essential andeffective means of wardcommunication to improve thepatient and staff experience.

Putting Human Rights at the Heart of Nutrition and Hydration
SA
FETY
CA
LEN
DA
R –
Vul
nera
ble
Pat
ient
sas
sist
ed w
ith L
unch
Vul
nera
ble
Pati
ents
rec
eive
das
sist
ance
with
in…
…m
ins
of m
eal
arri
ving
GR
EEN
Mon
th:
War
d:
Vul
nera
ble
Patie
nts
did
not
rece
ive
assi
stan
ce w
ithin
……
…m
ins
ofm
eal a
rriv
ing
RED
Dat
eR
easo
n fo
r RE
D s
quar
e

Putting Human Rights at the Heart of Nutrition and Hydration
At A Glance Symbols to identifyPatients requiring assistance withtheir hydration and nutrition

Putting Human Rights at the Heart of Nutrition and Hydration
MON
Y / N
TUES
Y / N
WED
Y / N
THURS
Y / N
FRI
Y / N
SAT
Y / N
SUN
Y / N
Clear patients’ bed tables
Make sure corridors are free ofobstruction / clutter
Assist those patients that can tosit out in their chairs for theirmeal
Position those in bed comfortableready for their meal
Offer patient hand washing beforethe meal
Identify patients that requireassistance with eating
Were NOMINATED familymembers allowed to assis t withtheir relative’s meal
Did the Evening ORAL medica-tion round commence before thearrival of Meal trolley on the ward.
Ring the when themeal trolley arrives on the ward
Dim Ward lighting (switch downto your settings themain ward corridor)
Close Ward doors, lower blindsdisplay Protected Mealtime noticeoutside the door
Hand out meals
Feeding
Assist those that require help
Monitor the mealtime experiencefor the patients
Give encouragement andassistance for nominatedpersons to come in and help withtheir relative’s meal
The Protected Mealtime: Evening Meal
Please Completethis formDAILY

Putting Human Rights at the Heart of Nutrition and Hydration
MON
Y / N
TUES
Y / N
WED
Y / N
THURS
Y / N
FRI
Y / N
SAT
Y / N
SUN
Y / NThe completion of bedside chartsrelated to nutrition and hydration(eg )
If any Multi-Disciplinary Teammember come to ward make sureits for documentation work ONLYand
Were any Ward staff called awayfrom the patients during the meal
Did you have to POLITELYdiscourage any medicalintervention / reviews during themeal time( )
At the End of the Meal period,were the meal utensils andcrockery quietly removed andreturned to the meal trolley readyfor collection.
After the Meal period is complete,were the ward lightingrestored to normal operatinglevels, door opened, blinds
Was the administration of IVmedication — left until A FTERthe meal time
Did any ward visiting occurduring this protected meal timeperiod (
)
Page 2 of 2
The Protected Mealtime
Setting the Scene

Putting Human Rights at the Heart of Nutrition and Hydration
A human rights based approach is one where therealisation of human rights principles is a centralaim in policy and planning, where staff andpatients are empowered and involved inachieving these, where accountability is clearand the needs of the most vulnerable groups aretaken into account. It is the process by whichhuman rights principles are put into practice.
The European Convention on Human Rights is aregional human rights treaty passed after WorldWar II by the Council of Europe. TheConvention established a European Court ofHuman Rights, based in Strasbourg, France. TheUK signed up to the Convention in 1951.
The Human Rights Act came into force in the UKin October 2000. It brought most of the rightscontained in the European Convention onHuman Rights into UK law. The Act places a dutyon all public authorities in the UK to act inaccordance with the rights protected by theConvention.
The term 'public authority' is not fully defined inthe Human Rights Act, but it should beinterpreted broadly. It includes any person ororganisation 'whose functions are of a publicnature'. Strategic Health Authorities, NHS Trusts,Primary Care Trusts and NHS Foundation Trustsare all included. The term covers private
organisations such as companies or charities,when they are carrying out a public function.
These rights may never be interfered with, noteven in times of war or national emergency.There is no possible justification for interferenceand no balancing with any public interest. Thethreshold for finding a breach of absolute rights ishigh. An example is Article 3 (the prohibition oftorture, inhuman and degrading treatment).
These rights are not absolute. They may belimited in certain strictly defined circumstances.An example is Article 5 (the right to liberty andsecurity). Someone's liberty may be limited, forexample when they are lawfully detainedbecause they have committed a crime or if theyare suffering from serious mental health problems.However, there are very strict procedures whichmust be followed if someone's liberty is to berestricted.
These rights are not absolute. They may beinterfered with to protect the rights of others or inthe wider interests of the community. Theinterference must be in accordance with the law,it must be strictly necessary, and it must beproportionate (see 'proportionality' below). Anexample is Article 8 (the right to respect forprivate and family life, home andcorrespondence).

Putting Human Rights at the Heart of Nutrition and Hydration
A proportionate response to a problem is one thatis appropriate and not excessive in thecircumstances. The expression commonly used tocapture this meaning is 'you should not use asledgehammer to crack a nut'. You shouldremember that the 'nut' should only be cracked ifit is strictly necessary! If there is a way ofachieving a balance of rights and needs withoutrestricting the right at all, this path should befollowed.
These obligations require public authorities to takeproactive steps to protect human rights. Positiveobligations are often contrasted with negativeobligations, which require authorities to refrainfrom action that may violate human rights. Anexample includes the positive obligation underArticle 3 to protect individuals from inhuman ordegrading treatment where authorities know, orshould know, that there is a risk of this takingplace.

Putting Human Rights at the Heart of Nutrition and Hydration
1. All Wales Nutrition and Catering Standards for Food andFluids in Hospital (2011)
2. Hospital catering and Patient Nutrition (Wales Audit Office,2011)
3. Doing Well Doing Better - Standards for Health Services inWales, Standard 14 - Nutrition (2010)
4. Meeting Quality Standards in Nutritional Care (BritishAssociation for Parenteral and Enteral Nutrition, 2010)
5. Free to Lead Free to Care (Welsh Assembly Government,2008)
6. Fundamentals of Care, Improving the Quality of FundamentalAspects of Health and Social Care for Adults (2003)
7. Resolution on food and nutritional care in hospital (Council ofEurope, 2003)
8. Improving Health in Wales, a Plan for the NHS and Its Partners(2001)

Putting Human Rights at the Heart of Nutrition and Hydration
Thank you to the:
BCUHB Human Rights in Healthcare Project Group
, Ysbyty Glan Clwyd
, Ysbyty Gwynedd
, Ysbyty Maelor Wrexham
Mersey Care NHS Trust
The British Institute of Human Rights;
and all staff, stakeholders and service users that contributed to this project.