A task analysis of laparoscopic surgery : requirements for...
235
A Task Analysis of Laparoscopic Surgery: Requirements for Remote Manipulation and Endoscopic Tool Design by Caroline G. L. Cao B. Sc. (Biochemistry) Simon Fraser University, 199 1 A THESIS SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE (KINESIOLOGY) in the School of Kinesiology O Caroline G. L. Cao Simon Fraser University April 1996 All rights reserved. This work may not be reproduced in whole or in part, by photocopy or other means, without permission of the author.
Transcript of A task analysis of laparoscopic surgery : requirements for...

A Task Analysis of Laparoscopic Surgery: Requirements for
Remote Manipulation and Endoscopic Tool Design
by
Caroline G. L. Cao
B. Sc. (Biochemistry)
Simon Fraser University, 199 1
A THESIS SUBMITTED IN PARTIAL FULFILMENT OF
THE REQUIREMENTS FOR THE DEGREE OF MASTER
OF SCIENCE (KINESIOLOGY)
in the School of Kinesiology
O Caroline G. L. Cao
Simon Fraser University
April 1996
All rights reserved. This work may not be reproduced in whole or in part, by photocopy or other means, without permission of the author.

APPROVAL
NAME: Caroline Cao
DEGREE: Master of Science
TITLE OF THESIS: A Task Analysis of Laparoscopic Surgery: Requirements for Remote Manipulation and Endoscopic Tool Design
EXAMINING COMMllTEE:
Chair Dr. John Dickinson
Dr. Christine ~ a c ~ e n z i e Senior Supervisor School of Kinesiology
Dr. Ron Marteniuk Dean Faculty of Applied Science
--
Dr. Shahram Payandeh School of Engineering Science
Dr. Barry Wills Systems Design Engineering University of Waterloo External Examiner
Date Approved: /Sw w

PARTIAL COPYRIGHT LICENSE
I hereby grant to Simon Fraser Universi the right to lend my
2 B thesis, pro'ect or extended essay (the title o which is shown below) to users o the Simon Fraser University Library, and to make partial or single copies only for such users or in response to a request from the library of any other university, or other educational institution, on its own behalf or for one of its users. I further agree that permission for multiple copying of this work for scholarly purposes may be granted by me or the Dean of Graduate Studies. It is understood that copying or publication of this work for financial gain shall not be allowed without my written permission.
Title of Thesis/Project/Extended Essay
Author: (signature)

ABSTRACT
Minimally invasive surgery, or endoscopic surgery is an alternate surgical technique to the
conventional open technique in general surgery, such as for gall bladder removal, hernia
repair, and appendectomy. It requires surgeons to operate using an endoscope and
specially designed endoscopic tools. The instrumentation for this technique imposes
additional visual, spatial, tactual and motoric constraints on the surgeons.
This exploratory study, examining three laparoscopic procedures,
Cholecystectomy, Appendectomy, and Fundoplication, is based on a human-centred,
information processing approach. The task analysis included an analysis of selected
surgical tasks, and the endoscopic manipulators used, as well as a survey of the surgeons'
views about the tasks and tools. Dissecting, suturing, knotting, and cutting tasks were
decomposed into subtasks and analyzed by timeline and motion analysis. Scissors,
graspers and needle drivers/holders were analyzed and evaluated for their usability. User
feedback on all three aspects of the study (user, task, and tool) were obtained through
personal interviews, and a questionnaire survey of registered general surgeons in British
Columbia, Canada.
Task analysis results and user feedback agreed that suturing and knotting are the
most difficult tasks in laparoscopic surgery. Surgeons require more time and movements
to suture and tie knots than other tasks. Surgeons also considered the needle
drivers/holders that were used for these tasks to be more difficult than other tools to use.
As tools were evaluated with respect to the task requirements, the perceived difficulty in
using the tools was associated with both the physical and information processing
constraints arising from performing the tasks. Surgeons' performance of basic surgical
skills reflect these constraints. Remote manipulation in laparoscopic surgery exhibits the
characteristic motions of natural human prehension, such as reaching and grasping.
However, contrary to the parallel arrangement of transport and grasp components in direct

manipulation, the results of motion analysis suggest that these reaching and grasping
components are organized serially for remote manipulation in endoscopic surgery.

ACKNOWLEDGEMENTS
The completion of this thesis would not have been possible without the support and
encouragement of many people. For all their patience and understanding throughout my
endeavour, I thank them.
I thank my family for the love and emotional support I needed to achieve my goal,
feeding me when I was hungry, entertaining me when I needed a distraction from my video
analysis, and keeping me on track when I strayed. I thank my good friends, for humoring
me by listening to my monologues when I demanded their attention and participation as a
naive audience to my research, and I thank my not-so-good friends for adding to my
determination to work hard, as well as for strengthening my character.
Most importantly, I thank my senior supervisor/mentor, Dr. Christine MacKenzie,
for opening the door, for me, to the wonderful world of motor control research. I am
eternally indebted to her for her enthusiastic guidance and mentorship. I especially thank
my supervisory committee members: Dr. Shahram Payandeh for introducing me to this
area of research and for his constant support and encouragement thereafter; and, Dr. Ron
Marteniuk for his expert advice and keeping things in perspective. My external examiner,
Dr. Barry Wills from the Department of Systems Engineering at the University of
Waterloo, deserves special thanks for his thorough examination of my thesis and insightful
feedback.
To my friends in the Human Motor Systems Lab, who were the most likely
recipients of my free-flowing emotions through the most intensive periods of my research,
I extend my most sincere appreciation for their help and support. Many thanks to the
Kinesiology office staff for always having an answer to my questions.
Lastly, I thank Dr. A. Nagy for helpful discussion and for permitting me to
videotape his laparoscopic training workshops at the Jack Bell Research Centre in
Vancouver, and Matt Hanley of Ethicon for providing us with the endoscopic tools. This

research was supported by IRIS-PRECARN (through Dr. S. Payandeh) and the Natural
Sciences and Engineering Research Council of Canada (through Dr. C. MacKenzie).

Table of Contents . . ....................................................................................... APPROVAL u ... ....................................................................................... ABSTRACT UI
...................................................................... ACKNOWLEDGEMENTS v TABLE OF CONTENTS ......................................................................... vii
................................................................................ LIST OF TABLES ix .............................................................................. LIST OF FIGURES x
INTRODUCTION ................................................................................ 1 Objectives of Thesis ...................................................................... 1 Layout of Thesis .......................................................................... 4 Literature Review ......................................................................... 5
Human Manipulation ............................................................ 5 .................................. Requirements for Successful Manipulation 8
........................................................... Remote Manipulation 10 .............................. Remote Manipulation in Laparoscopic Surgery 11
............................................... Vision in Laparoscopic Surgery 12 ............................................ Endoscopic Tools or Manipulators 12
....................................................... Applications of Research 13 METHODS ......................................................................................... 15
Data Collection ........................................................................... 15 Direct Observation ............................................................... 15
...................................................................... Videotaping 16 ............................................................................ Survey 18
............................................... Surgical Manuals & Videotapes 19 ........................................................... Instrument Catalogue 19
............................................................................. Data Analysis 19 ............................................................... Analysis of Tasks 19
................................................................ Analysis of Tools 21 .................................................... Analysis of User Response 22
RESULTS .......................................................................................... 24 Tasks ....................................................................................... 24
....................................................... Laparoscopic Procedures 24 Procedural Steps ................................................................. 30
................................................................... Surgical Tasks 33 ............................................................... Dissecting 33
................................................................. Suturing 36 ............................................................. Tying knots 40
........................................................... Cutting suture 43 Contrasting cutting suture and dissecting tissue .................... 45 Reliability check ........................................................ 47
Task Motion Analysis ........................................................... 48 ................................ Dissecting tissue -- motions involved 51
......................................... Suturing -- motions involved 55 ..................................... Tying knots -- motions involved 65
................................... Cutting suture -- motions involved 70 ................... Contrasting cutting suture with dissecting tissue 73
Analysis of Tools ......................................................................... 75 Laparoscopic Manipulators ..................................................... 75
................................................. Laparoscopic graspers 75 .................................................. Laparoscopic scissors 76
................................. Laparoscopic needle driverslholders 77 ........................................................... Tool Motion Analysis 79
......................................... Graspers -- motions involved 79
vi i

Scissors .. motions involved .......................................... 81 ......................... Needle drivers/holders .. motions involved 82
............................................................. Analysis of User Response 85 ........................................................ Questionnaire Response 85 ........................................................... Demographics 85
................................................................. On tasks 90 On instruments .......................................................... 91
................................................................ On attitude 98 .................................................. On general comments 99
............................................................. Interview Response 100 .............................................. Laparoscopic workshops 100
.................................................. Follow-up interviews 103 ..................................................................................... DISCUSSION 106
....................................................................... Triangular Strategy 106 ................................................................................ Constraints 107
............................................................ Physical Constraints 108 ............................................................... Safety Constraints 109
........................................................... Precision Constraints 111 .................................................................. Effects on Performance 112
Serial Order of Motions ......................................................... 112 .............................................. Epistemic vs . Pragmatic Motions 115
....................................................... Implications for Training 116 ................................................. Requirements for Tool Design 117
................................................................. Visuomotor Constraints 122 .......................................................................... Future Research 124
................................................................... . APPENDIX I Questionnaire 125 .................................................... . APPENDIX 11 Raw Data from Tirnelines 133
............................. . APPENDIX III Tests of Agreement between Two Observers 193 ............................................ . APPENDIX IV Survey Questionnaire Response 197
.................................................................................... REFERENCES 220
... V l l l

List of Tables
1 . Summary of key features in cholecystectomy. appendectomy. and . . ................................................................................ fundophcahon -25
2 . Summary of major surgical steps for cholecystectomy. appendectomy. and ................................................................................. fundoplication 26
3 . Operational definition of subtask initiation and termination for dissecting tissue ...... 34
............... 4 . Operational definition of subtask initiation and termination for suturing 37
5 . Operational definition of subtask initiation and termination for tying knots ............ 41
6 . Operational definition of subtask initiation and termination for cutting suture ......... 43 .................................... 7 . Description of motion and movement coordinate axes 50
..................................... 8 . Summary of survey questionnaire response analysis 86

List of Figures
........................................................ 1 . Triangular strategy of task analysis 4 ............................................... 2 . A model of human information processing 7
............................. 3 . A model of information processing in endoscopic surgery 9 4 . Dimensions of freedom of a conventional instrument in endoscopic surgery ........ 14 5 . Layout of workshop operating room and video camera position ....................... 17
............................................... 6 . Placement of trocars in a Cholecystectomy 27 ................................................ 7 . Placement of trocars in an Appendectomy 28
8 . Placement of trocars in a Fundoplication .................................................. 29 9 . Hierarchical Analysis: breakdown of Cholecystectomy into major procedural
..................................................................... steps and surgical tasks 30 10 . Hierarchical Analysis: breakdown of Appendectomy into major procedural
..................................................................... steps and surgical tasks 31 1 1 . Hierarchical Analysis: breakdown of Fundoplication into major procedural
..................................................................... steps and surgical tasks 32 .................................................... 12 . Timeline analysis for dissecting tissue 35
.............................................................. 13 . Timeline analysis for suturing 39 .......................................................... 14 . Timeline analysis for tying knots 42
15 . Timeline analysis for cutting suture ........................................................ 44 ............................................................... 16 . Cut suture vs . dissect tissue 45
..................................................... 17 . Motions involved in dissecting tissue 52 18 . Motions in dissecting tissue ................................................................ 54
............................................................... 19 . Motions involved in suturing 57
.............................................................. 20 . Motions involved in suturing 63 ........................................................... . 2 1 Motions involved in tying knots 66
22 . Motions involved in tying a simplified square knot ...................................... 68 . ......................................................... 23 Motions involved in cutting suture 71 . ......................................................... 24 Motions involved in cutting suture 72
25 . Contrasting the motions involved in the tasks cutting suture and dissecting tissue .......................................................................................... 74
.................................................. 26 . Conventional laparoscopic manipulators 78 27 . Rating of task difficulty by 79 B.C. General Surgeons who perform
laparoscopic surgery ......................................................................... 90 28 . Type of tool handles used and preferred by 79 B.C. General Surgeons who
performed laparoscopic surgery ............................................................ 93 29 . Rating of tool difficulty by 79 B . C. General Surgeons who perform
laparoscopic surgery ......................................................................... 94 30 . Actual design modifications suggested by a surgeon who responded to our
................................................................................. questionnaire 95 ........... . 3 1 Reported emotions when dealing with difficulties in laparoscopic surgery 98
. .................. 32 Reported frequency of error while performing laparoscopic surgery 99 3 3 . Contrasting the motions involved in the tasks cutting suture and dissecting
.......................................................................................... tissue 110 34 . Comparison of reaching and grasping in natural prehension and prehension
......................................... with a tool in laparoscopic remote manipulation 114

INTRODUCTION
Obiectives of Thesis
Humans are complex, biological information processing systems, capable of
learning and adapting to new environments and additional informational processing
demands. Taking advantage of their adaptability, humans have developed technology to
change the way we work in an attempt to improve the quality of life. For example, the
innovative use of a miniature video camera attached to the eyepiece of an endoscope started
the new era of minimally invasive surgery (MIS) (Soper, 1993). Also called minimal
access surgery (MAS), endoscopy offers an alternative to the traditional open technique in
performing routine, general surgical operations. The advantages include shortened
recovery time and reduced post-operative pain and suffering for the patients. For the
surgeons, however, the surgical procedures are more complex to perform endoscopically.
Surgeons are faced with unfamiliar instrumentation, altered visual feedback, reduced tactile
sensation, and limited degrees of freedom in manipulation, which result in longer learning
and performance time, as well as a great deal of frustration for the surgeon. A routine
bowel-resection is at least three times longer to perform and much more demanding to learn
and master (Dr. A. Nagy, personal communication, November 24,1994). The realization
that there are increased information processing demands, tool and task constraints being
placed on the surgeons using this technique motivates this study.
This research examines remote manipulation by humans in the context of
endoscopic surgery (ES). The objectives of this study on laparoscopic surgery are to:
1. Identify the task requirements and task constraints in laparoscopic surgery;
2. Evaluate the effectiveness of several endoscopic tools currently in use;
3. Make some general recommendations for redesigning these tools; and
4. Study the interaction between the task and the tools, from the user's perspective.
Without analyzing all endoscopic procedures which include specialties such as
orthopedic, urological, gastroentological, vascular, cardiovascular, thoracic, obstetrics and

2
gynecological, and general, we limit our study to laparoscopic procedures. Laparoscopic
surgery (Gk. lapara means flank) refers to general procedures such as Cholecystectomy
(gallbladder removal), Appendectomy (removal of appendix), Fundoplication (anti-reflux
procedures), inguinal and hiatal hernia repair, etc., which are performed within the
abdomen.
In spite of the fact that endoscopic surgery has become the preferred technique for
some operations in the last ten years, very little is known about the effect of task constraints
and physical constraints on the surgeon's performance in this environment. We observe
that the inherent constraints in endoscopy appear to be due to restricted access to the
operative site within the respective body cavity, visually, tactually and motorically. Also,
the very tools which allow surgical operations to be performed with minimal invasiveness
are a major physical constraint. These constraints could be altered with improved design of
instsumentation to better interface the operators with their tools for the task goals. Thus,
we need to better understand the task requirements, task constraints, information-
processing demands on the surgeons in remote manipulation, as well as the interaction
between the surgeon and their tools in performing endoscopic surgery.
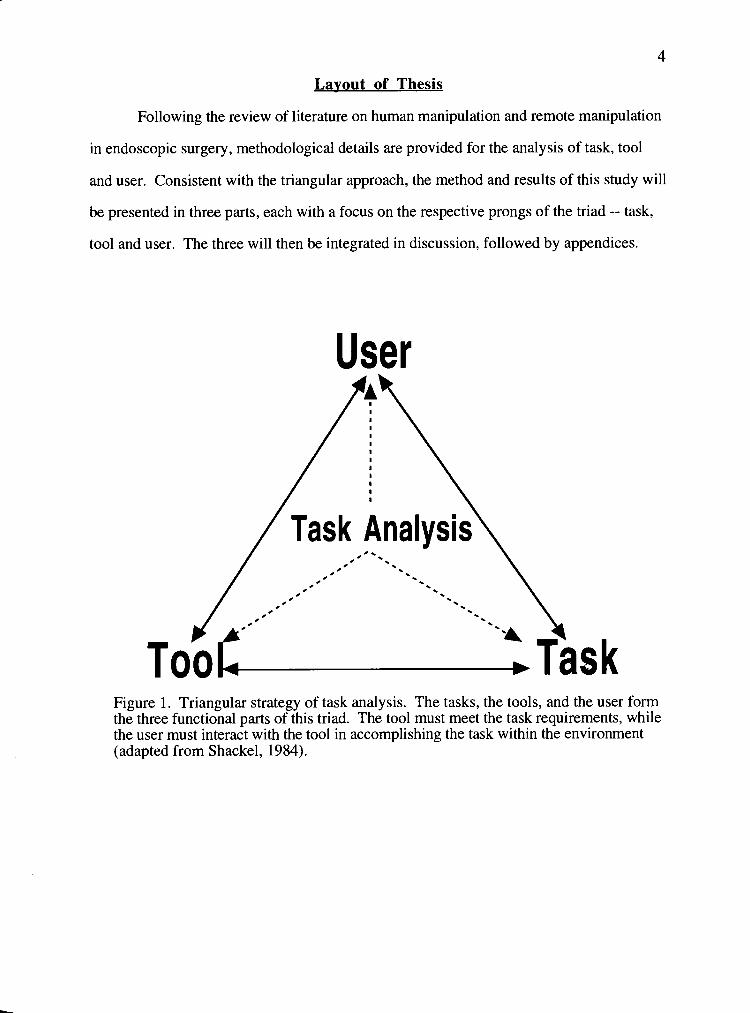
In order to achieve our objectives, a comprehensive study included all three
components of the triangular interrelationship among the task, the tool, and the user (see
Figure 1). This triangular strategy was achieved through a systematic analysis of task
requirements, systems/instrumentation and operator behaviour in surgery --- a task
- , analysis. The purpose of a task analysis is to compare the demands of a system on an
operator with operator capabilities, and when necessary, to alter these demands to reduce
error and achieve successful performance. Task analysis can also reveal the underlying
requirements of the skill, as well as trade-offs in the underlying information processing
requirements. Therefore, a task analysis would yield information relevant to the evaluation
of the existing design and to the design of new endoscopic manipulators.

3
An analysis of surgical tasks based on observations and videotape analysis can
reveal the task requirements; as well, the underlying information processing requirements
of the motor skills can be inferred. It can also provide a better understanding of the
constraints associated with the tasks and instrumentation in use. '~nformation regarding the
surgeons' interaction with the tools and their views on the use of the tools can be obtained
most directly from the surgeons themselves. This information, gathered through survey
questionnaires and interviews, could be very useful for evaluating the effectiveness of the
tools.
4
Layout of Thesis
Following the review of literature on human manipulation and remote manipulation
in endoscopic surgery, methodological details are provided for the analysis of task, tool
and user. Consistent with the triangular approach, the method and results of this study will
be presented in three parts, each with a focus on the respective prongs of the triad -- task,
tool and user. The three will then be integrated in discussion, followed by appendices.
User
Figure 1. Triangular strategy of task analysis. The tasks, the tools, and the user form the three functional parts of this triad. The tool must meet the task requirements, while the user must interact with the tool in accomplishing the task within the environment (adapted from Shackel, 1984).

Literature Review
Human Manipulation
The following sections outline the current state of understanding about human
manipulation, and the requirements for successful manipulation in terms of the information-
processing demands on the operator.
Manipulation may be the most complex task that the hand is capable of performing.
Manipulation is the skillful control of the hands or of some mechanical device with the
hands, in interacting with an object. It involves coordinated movements of the hand with
motions of the object to be manipulated. Manipulation is an activity which occurs after the
hand has contacted the object. Grasping involves the fingers or arms in taking, seizing,
clasping or embracing an object. Manipulation, in addition, involves imparting motion to
an object by applying forces to match anticipated forces acting on the object. An object can
be transported from one location in space to another, without changing its relation to the
fingers and hand during the task. Thus, the hand maintains a static posture and constant
contact points on the object in counteracting the forces acting on the object. Alternatively,
the object can be made to rotate, flip, oscillate, or vibrate while maintaining stable grasp.
The fingers and hand manipulate the object using dynamic hand movements, or dynamic
grasps (Kapandji, 1982 in MacKenzie & Iberall, 1994).
Two types of manipulative hand movements can be observed, based on task
requirements: 'exploratory-type' movements and 'performatory-type' movements
(Kunesch , Binkofski, and Freund, 1989). Exploratory hand movements are used to
extract object properties through active touch. Lederman and Klatzky (1987) described
stereotypical hand movement patterns that are used in acquiring knowledge about objects.
These hand movement patterns include rubbing or lateral motion over a small area of the
surface to acquire texture information, contour-following for object shape and volume
information, etc.. Other researchers (e.g., Gibson, 1962) have also shown that people are
more likely to identdj a felt object correctly through exploration of the object with the

6
hand. Without relying on vision, somatosensory information about the physical world is
gathered through haptics or 'active touch', which combines tactile and kinesthetic sensory
inputs with motor activities of the hand.
Performatory hand movements, on the other hand, use touch (or contacts) for
action with objects. Four forms of contacts have been classzed (MacKenzie and Iberall,
1994, p. 269):
1. fixed contacts. The hand imparts motion to the object using coordinated
movement of the hand. The contacting areas between the hand and object remain constant.
This is distinct from the static grasp of holding and transporting an object, where the object
is immobilized within the hand. In dynamic grasping with fixed contacts, the object can
move in the hand through coordinated movement of the digits. For example, when
removing a splinter, the index finger and thumb can move the grasped splinter with respect
to the stationary palm, while keeping the contact points fixed on the splinter.
2. rolling contacts. The hand imparts a rolling motion to the object. The
contacting areas between the hand and object roll over one another. For example, when
rolling up paper or winding a watch, the fingers roll on the object, or the object rolls in the
fingers.
3. sliding contacts. The hand imparts sliding motion to the object. The contacting
areas between the hand and object slide past one another. For example, in squeezing a
syringe, the object slides past the fingers as the hand squeezes.
4. repositioning or regrasping. The hand imparts motion to the object by releasing
grasp and relocating the hand's contacting points on the object. The hand and object are
not usually in contact between the grasp changes. For example, in turning a dial, the hand
changes the grasp posture on the object by repositioning the grasp between each turn of the
dial.
Proprioceptive and somatosensory inputs from the hand are used to monitor
motion. Specific mechanical events at the object-skin contact areas provide afferent

7
information to update the internal representations related to the object's physical properties
(Johansson & Westling, 1984). For example, at initial contact, frictional representations
are updated by Meissner corpuscle afferents. Small frictional slips during grasp also elicit,
through tactile afferents, motor responses to maintain stable grasp and update the frictional
representation.
st imul i i
sensory processing I
perception responses decision and response selection
response execution
L memory
4 feedback
Figure 2. A model of human information processing (from Wickens, 1992, p. 17).

8
Reauirements for Successful Manipulation
Humans are complex information processing systems (Figure 2). When engaging
in interactive tasks, such as manipulation, they are active, generative, intentional and
biological/biomechanical systems capable of integrating perceptual motor systems
(MacKenzie and Iberall, 1994). Sensory-motor memory systems play an important part in
this integration. Memory is involved in several processes which include identification and
classification of incoming sensory information. For example, object properties are
identified based on visual and haptic inputs; task goal and task features, initial state of
effectors are identified and compared with the sensory-motor memory based on previous
experience to effect planning and execution of motor commands (Johansson and Cole,
1992). During task progress, discrete sensory events are also used to update the internal
7 representation of the sensory-motor memory. Therefore, in information-processing terms,
information processing involves recognition encoding, transformation, decoding and
comparison, integrated with anticipation, past experience and feedback. We can associate
processing efficiency with the amount of information an operator can process per unit time.
Also, task difficulty can be associated with the rate at which information is presented. In
general, the processing limitations inherent in performing motor tasks are (Salthouse,
1991):
- A 1. not knowing what to expect from one's own action,
2. insensitivity to sensory/perceptual discrimination, and,
3. lack of proficiency in performing appropriate actions.
Schueneman and Pickleman (1993) analyzed surgical skills in an effort to evaluate
the demands and limiting factors in acquiring proficient surgical skills. They suggest that,
in addition to manual dexterity, the surgeon's ability to 'see' the relevant anatomy of the
operative site, is important. The 'expert' surgeon quickly identifies important landmarks in
the incision, mentally organizes multisensory data and action during the course of the
surgical procedure to produce smooth and efficient sequence of responses. Therefore,

9
perceptual-based cognition about complex spatial and anatomical relations is important for
surgical success.
Although our research is focused primarily on issues surrounding the manipulation
of the endoscopic instruments, it is important to keep in mind the issues of visualization
when dealing with the overall task constraints in endoscopic surgery. We begin with the
assumption that task requirements in terms of task goals for remote manipulation are the
same as in direct manipulation. Thus, performance degradation in endoscopic surgery can
be associated with additional task constraints, or additional physical constraints. The
constraints may impose information processing demands on the operator. Therefore, once
the constraints are identified, additional requirements for remote manipulation can be
inferred in terms of information processing (see Figure 3).
sti -
memory w
attention -@
w feedback 1
Figure 3. A model of information processing in endoscopic surgery. Perceived stimuli may not accurately represent actual stimuli and actual responses.
filtered actual stimuli
tool
sensory processing
- A
perception decision and response selection
response execution
end-effector motor
processing - responses
Remote Mani~ulation
The following sections idenbfy some problems encountered in remote manipulation
in the context of endoscopic surgery, and more specifically, in laparoscopy. Laparoscopy
is the examination of the abdomen using endoscopes. Common laparoscopic procedures
include hernia repairs, cholecystectomies (gallbladder removals), and bowel resections.
For the purpose of this study, remote manipulation is distinguished from direct
manipulation and telemanipulation. The most basic level of manipulation is by direct
contact of the hands with the object to be manipulated. For example, in order to achieve the
goal of dividing a sheet of paper in halves, the hands grasp the sheet and tear it in half.
Direct manipulation allows the performer to feel through direct touch of the texture and
weight of the object being manipulated, as well as the forces applied by the hand or fingers.
If, in addition to dividing the sheet of paper into halves, the goal is to divide the
sheet into equal halves with the edges straight, then the hands can either fold the sheet and
tear along the crease, or, use a pair of scissors to cut. The latter alternative -- using the
scissors as a tool or aid -- is considered remote manipulation. The hands manipulate the
paper remotely through the scissors, which physically separate the hand and the object to
be manipulated. In remote manipulation, physical properties of the object being
manipulated may not be obtained through direct touch. In addition, the tool may or may
not accurately transmit the forces from the object to the hands. Also, the action of the hand
on the handle of the tool may not map directly onto the tool end-effector. Therefore, the
requirements for successful manipulation in terms of demands on the performer are likely
to be different from those in direct manipulation.
Furthermore, if the task requirements were to become more demanding, such as
dividing a sheet of paper which has been contaminated with radioactive agents, the need to
withdraw the human operator from the immediate workspace becomes apparent. Under
such circumstances, a mechanical arm or a robot may be controlled from outside the
radioactive chamber to accomplish the task. This involves telemanipulation. In addition to

11
problems similar to those encountered in remote manipulation, technological problems in
designing control systems are important issues to be considered. Issues surrounding
telemanipulation are not within the scope of this study, and so will not be discussed further
in this proposal.
Remote Manipulation in Laparoscopic Surgery
In laparoscopic surgery, the need to cut open the patient to expose the internal
abdominal environment for visual inspection is eliminated. An endoscope is introduced
into the abdominal cavity through a small incision (about 2 cm wide), usually near the
umbilicus. The image from the endoscope is enlarged and viewed on a video monitor
mounted before the surgeon who is performing the operation. Endoscopic
manipulators/tools are inserted through small incision in the abdominal wall and act to
extend the capabilities of the hands in performing surgical work at a distance. It is possible
to grasp, clip, hold and cut tissue with these tools. Therefore, with practice, entire surgical
procedures, which may include cutting, suturing, and knotting, can be performed
successfully via remote manipulation.
In general, tools are helpful in performing more demanding tasks. However, in
endoscopic surgery, the tools also introduce additional demands on the surgeons using
them. These demands may involve increased task constraints and physical constraints,
such as limited vision of the operative site, loss of depth perception, decreased tactile sense
and force feedback, and restricted movement in manipulating tissues. Other demands may
be related to the interaction of the hand with the tool handle in achieving the desired motion
and orientation in the tool end-effector. The most obvious general areas for improvement
in endoscopic surgery have been identified as visual imaging systems, sensory feedback
from the instruments to the surgeon, and freedom of motion in the endoscopic instruments
(Tendick et al, 1993, Satava, 1993, Rininsland, 1993, Melzer et al, 1993, and Nagy &
Payandeh, 1994).

1 2
Vision in Laparoscopic Surgerv
The image of the abdominal environment on the video monitor is two-dimensional.
This affects the perception of relative positions of the organs and tissues, compared to
direct viewing in open surgery. The lack of stereoscopic view and adequate depth cues
result in longer performance time (Tendick et al, 1993). Surgeons must grope forward and
backward with instruments to gauge the relative depths of objects by touching them slowly,
so as not to damage the tissues in contact. Also, the motion represented on the monitor and
that of the hand controlling the tools are frequently mirror images. As the hand moves the
tool handle to the right, the image of the tool end-effector moves to the left on the video
monitor. This mirror reflection is further affected by magnification and camera point-of-
view. The orientation and viewing perspective of the endoscope, with respect to the
endoscopic tool may add to the mismatch in mapping between the position of the tool
handle and the seen position of the end-effector.
As the camera is controlled by an assistant to the surgeon, it often requires some
adjustments guided verbally by the operating surgeon. This requires experience on the part
of the assistant. The orientation of the endoscope is restricted by the fixed port of entry,
such that the only possible positions for the camera is within a conical volume ascribed by
the rotation of the proximal end of the endoscope. A 30•‹ scope is used sometimes based
on surgical site and preference of the surgeon.
Endosco~ic Tools or Mani~ulators
Presently, the tools available to endoscopic surgeons are crude and awkward to
use. In place of the direct 'hands-on' contact at the operative site, the surgeon's hands now
remotely manipulate a handle resembling that of scissors or pliers. Contact with the
operative site is at the distal end of a long slender rod attached to the handle. The tips of the
rods are equipped with various functional tools, such as forceps, clippers, and staplers,
etc. These tools can be divided generally into two classes: manipulation tools (such as
grippers, needle drivers, and cutters), and stapling tools. For the purpose of this thesis,
1 3
only manipulators are analyzed. Simple opening and closing of the forceps or clippers are
controlled via opening and closing of the hand as in operating a pair of scissors, or a pair of
pliers. More complex tasks such as suturing require coordinated action of two or more of
these grippers.
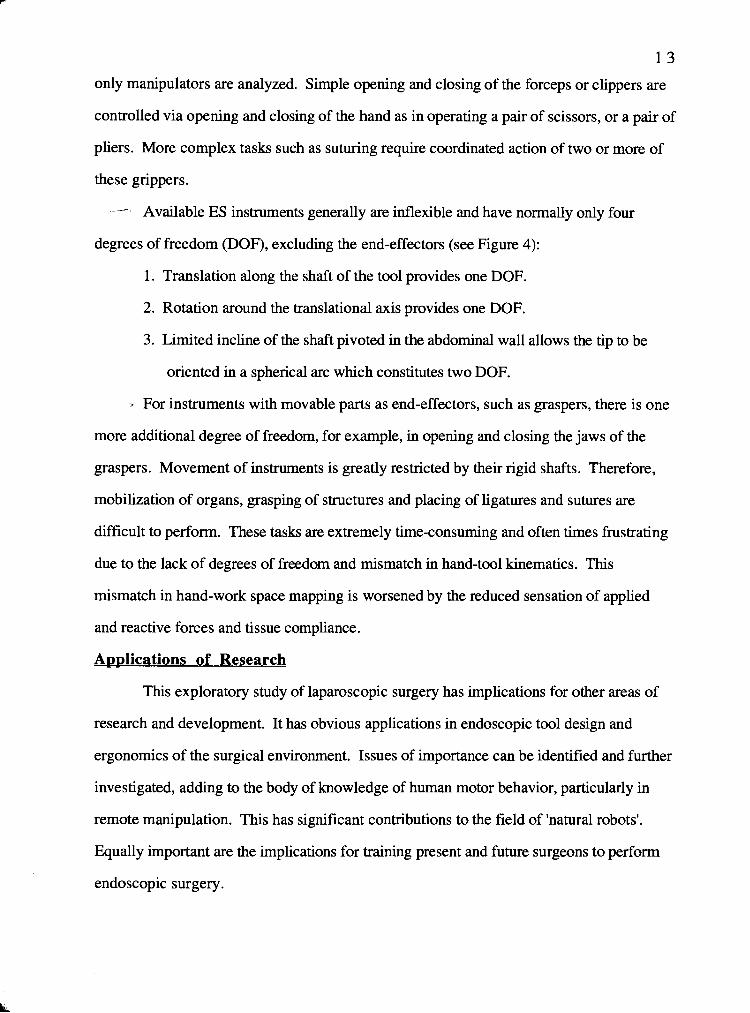
- Available ES instruments generally are inflexible and have normally only four
degrees of freedom (DOF), excluding the end-effectors (see Figure 4):
1. Translation along the shaft of the tool provides one DOF.
2. Rotation around the translational axis provides one DOF.
3. Limited incline of the shaft pivoted in the abdominal wall allows the tip to be
oriented in a spherical arc which constitutes two DOF.
- For instruments with movable parts as end-effectors, such as graspers, there is one
more additional degree of freedom, for example, in opening and closing the jaws of the
graspers. Movement of instruments is greatly restricted by their rigid shafts. Therefore,
mobilization of organs, grasping of structures and placing of ligatures and sutures are
difficult to perform. These tasks are extremely time-consuming and often times frustrating
due to the lack of degrees of freedom and mismatch in hand-tool kinematics. This
mismatch in hand-work space mapping is worsened by the reduced sensation of applied
and reactive forces and tissue compliance.
A~plications of Research
This exploratory study of laparoscopic surgery has implications for other areas of
research and development. It has obvious applications in endoscopic tool design and
ergonomics of the surgical environment. Issues of importance can be identified and further
investigated, adding to the body of knowledge of human motor behavior, particularly in
remote manipulation. This has significant contributions to the field of 'natural robots'.
Equally important are the implications for training present and future surgeons to perform
endoscopic surgery.

Figure 4. Dimensions of freedom of a conventional instrument in endoscopic surgery (from Melzer et al., 1992, p. 15).

1 I/
- METHODS
As we know very little about the nature of the constraints in endoscopic surgery and
the effects these constraints have on the surgeons, it was necessary to build a knowledge
base through exploratory research. In this study, the task analysis consists of three parts.
Part one is a comprehensive description and functional analysis of some of the tasks
involved in performing laparoscopic surgery. The second part of the task analysis is a
detailed analysis of several most commonly used endoscopic manipulators. Part three of
this study focuses on the user of these manipulators--- the surgeons' and their perspectives
on the use of endoscopic tools and the tasks performed.
- Data Collection
Data were collected from direct observations, videotapes of laparoscopic
workshops, personal interviews, questionnaire survey, surgical manuals and videotapes,
and product literature (Ethicon of Johnson & Johnson).
Direct Observation
A total of 4 site visits were arranged with Dr. Alex Nagy at the Jack Bell Research
Centre in Vancouver, to observe his monthly Laparoscopy Workshops. There were
usually at least two surgeons in attendance at each workshop, in addition to Dr. Nagy, and
an ES products representative from Ethicon (Johnson & Johnson). Dr. Nagy conducted
the workshop by demonstrating specific tasks in certain procedures, to be practiced by the
other surgeons, while the Ethicon representative provided instruction on the proper use of
the ES tools. The surgeons attending these workshops were either residents or practicing
surgeons who were learning the new technique.
Partial or whole laparoscopic procedures were performed on pigs that were kept
under general anesthesia throughout the procedure. During these workshops, activities
were videotaped and informal discussion with the participants was conducted. Comments
made by the surgeons during surgery were noted. Each surgeon was also given a copy of
a questionnaire to be completed and returned by mail to ensure anonymity (see Survey).

1 6
Videota~ing
At each laparoscopy workshop held at the Jack Bell Research Centre, a Sony video
camera was set up in the operating room to record the action of the surgeons' hands in
operation. Simultaneously, the endoscopic camera image of the tool end-effectors within
the abdominal cavity (viewed by the surgeons), was recorded on the same videotape in a
split-screen fashion. This was accomplished by feeding both images into a Panasonic
Digital AV Mixer WJ-AVES with a Picture-in-Picture feature. The signal from our Sony
camera fed directly into the mixer and was displayed as a full-screen image on a Sony
Trinitron color TV monitor. The signal taken from the endoscopic system monitor, fed
directly into the mixer, and was displayed as an inset picture, against the background of the
first image. This inset could be moved around on the screen as required. The combined
image was recorded at the standard play speed (SP) on a HQ-VHS Sony Hi-Fi Stereo
VCR. See Figure 5 for setup and connection.
Due to space restrictions within the operating room, the video camera was
positioned at an angle in front of the operating table (see Figure 4). As a result, the split-
screen image showed the surgeon facing the camera with histher left hand on the right side
of the screen, while the tool end-effectors were shown as from the perspective of the
surgeons. Thus, the action of the hand and the tool end-effector were mirrored in the two
images. For right-left consistency, one of the images would need to be flipped along its
vertical axis. The different viewing perspectives of the two cameras imposed limitations on
the nature, extent and accuracy of the video analysis. Three-dimensional motion analysis
was not possible from a two-dimensional image; nor was it possible to measure
quantitatively the magnitude and direction of movement.

surgeon operating
/ video camera
I nicrophone
video monito
view
digital mixer
Figure 5. Layout of workshop operating room and video camera position. Signals from the video camera and endoscopic system monitor feed into the mixer and display on the monitor as one picture set in the other. The VCR records the 2 pictures as one image onto a VHS tape with simultaneous audio input.

1 8
Survev
In addition to face-to-face interviews with surgeons at the laparoscopy workshops,
data were also collected by surveying registered general surgeons in British Columbia by
questionnaire. The list of 252 surgeons was obtained from the l994/95 BC Medical
Directory published by the College of Physicians and Surgeons of British Columbia.
Questions on the questionnaire asked surgeons to evaluate the tools they used, as well as
rank the difficulty of the tasks they performed in laparoscopic procedures. Other questions
elicited information regarding physical or psychological conditions and how they envision
improvement in the tools (see sample Questionnaire attached as Appendix I). The
questions on the questionnaire were pretested with Dr. Nagy during the design stage.
Modifications to the wording of each question were made based on feedback from Dr.
Nagy and others with expertise in questionnaire design.
The questionnaire was mailed out to the 252 B.C. general surgeons with a
personalized cover letter, a stamped return envelope and a stamped reply card. The reply
card was mailed back to us under separate cover and at the same time as the completed
questionnaire. This ensured anonymity for respondents while allowing us to keep track of
non-respondents. Non-respondents, after one month of the first mailing, were sent another
copy of the same questionnaire, with a follow-up letter and another return envelope and
reply card. A 20% response rate was expected. Therefore, a response rate of over 37%
was a pleasant surprise.
Some surgeons responded to the questionnaire with invitations for further
discussion by phone or face-to-face interviews. These were acknowledged by letters and
followed-up with phone calls and personal interviews, respectively. A few surgeons also
called with questions for clarification and feedback for survey questionnaire design.

1 9
Surgical Manuals & Videota~es
Videotapes of laparoscopic Cholecystectomy from the Television Learning Channel
(TLC) were available for public viewing. These videotapes were used in conjunction with
surgical manuals and medical texts (Ballie, 1992, Hunter & Sackier, 1993, Pearl, 1984,
Cuschieri, Buess and Perissat, 1992) for the breakdown of surgical procedures.
Instrument Catalogue
Product catalogues supplied by the manufacturer (Ethicon of Johnson & Johnson)
were used to compare the specifics of the tools of interest. Product catalogues from other
companies became available later from surgeons with access to literature from overseas
markets. However, they were not used for analysis in this study but for purposes of
contrasting alternative tool designs only.
Data Analysis
Analvsis of Tasks
In order to identify the task requirements and task constraints, the analysis of the
task component took the form of an hierarchical structure: procedures, steps, tasks,
subtasks, and motions. Three common laparoscopic procedures were analyzed:
Cholecystectomy (gallbladder removal), Appendectomy (appendix removal), and
Fundoplication (anti-reflux procedure). For each procedure, we noted the clinical signs
and symptoms for diagnosis and indications for surgery. A necessary step in our analysis
was to understand the operating room environment in which the surgeons work. Each
surgical procedure was different in the following ways: the relative positions of patients
and the surgeons, the relative placement of the video monitors within the operating room
(OR), the patient's posture and placement of incisions on the patient. All these were
included in the analysis of each procedure. Surgical manuals and videotapes (TLC) were
used to extract this information. For each surgical procedure, an hierarchical task analysis
yielded a general description of the procedural steps and procedural goals.

2 0
Once the high level goals of the procedure had been identified, selected procedural
steps were decomposed to yield a sequence of activities or tasks. The steps selected were
only those which contained surgical tasks of interest, such as cutting tissues, suturing,
tying knots and cutting suture. These tasks, which require the use of endoscopic
manipulators (scissors, forceps, and graspers, etc.), were further decomposed into a series
of subtasks.
For each task, a timeline analysis of subtasks and a motion analysis were
conducted. Characterization of the subtasks were based on ihe videotape recordings of
surgical tasks performed in the laparoscopic workshops at Jack Bell Research Centre.
Four sessions of the workshops were videotaped. Dr. Nagy, who conducted all four
workshops, was the expert surgeon, while all other surgeons who attended the workshop
were considered novice surgeons in our analysis of the videotapes. A total of five novice
surgeons were videotaped at the workshops. Results from one expert were compared with
those from five novices. Because only complete video segments of each task were
analyzed, the number of trials by each surgeon, and the number of novice surgeons for
each task, were not constant. Therefore, in our timeline and motion analyses, mean values
and variability are based on the data available for each task. Our statistics are descriptive,
not inferential.
Video recordings were annotated using 'Tirnelines' (Harrison, Owen, Baecker,
1994). 'Tirnelines' is a computer software system for video annotation which allows the
reduction of qualitative data such as recurring events, intervals, and comments, to
quantitative data. All task segments on the videotapes with clearly identifiable, and
complete sequences of subtasks were annotated. Beginnings and endings for these action
sequences were operationally defined and strictly followed when annotating the videotapes.
Durations of each subtask ~erformed within the task were averaged for each surgeon. An
average timeline was then created for each task.

2 1
Analysis of motion within each subtask was based on repeated viewing of the
motion sequence played forward at regular and reduced speeds. Characterization of the
motion was also based on operational definitions of beginnings and endings of the
movements. The two-dimensional video images limited the extent and accuracy of motion
analysis. Thus, motion analysis was limited to a qualitative description of the movement
characteristics and simple scoring of the number of repeated attempts made by the
surgeons.
Reliability of videotape annotation of subtask durations for three surgical tasks was
checked. A naive individual working as a research associate in another area, performed the
validation procedure. A brief explanation of the basic functions of the hardware system
preceded the actual video annotation. The individual, based on the provided criteria for
determining the time of sequence initiation and termination of subtasks (as presented later in
Table 4,5, and 6), analyzed randomly selected segments of video. Each segment was
analyzed twice without the presence of the experimenter. Data from the first trial were
considered practice, and were disgarded. Data from the second trial were compared with
our results for variance in scoring.
Analvsis of Tools
To evaluate the endoscopic manipulators, we analyzed the tool functions and how
the tools are controlled by the surgeons for a given task. Product catalogues (Ethicon of
Johnson & Johnson) were used to identify the relevant hardware features and associate
them to the function of the tools. Focus was on the handle and end-effector characteristics
of only endoscopic manipulators, namely, graspers, scissors, and needle driversholders.
The endoscopic viewing systems were outside the scope of this thesis.
A more detailed analysis of the tools in operation was based on the videotapes made
at the laparoscopic workshops. While the tools were in use, their motions were analyzed
using 'Timelines' (Harrison et al, 1994), to yield a more detailed description of tool
functions and manipulability. Movements of the tools, specifically, the end-effectors, were

2 2
characterized in terms of their intended functions. Movements were described with respect
to the object to be manipulated. Motions were functionally defined with beginning and end
physical states, and served as guidelines for the motion analysis. As in the analysis of
tasks and subtasks, a timeline for manipulating each tool in a particular surgical task was
constructed from the average durations of tool movements obtained by 'Timelines'. Other
descriptors of tool manipulability such as sequence of motion for orientation, number of
repeated attempts for a given manipulation were also obtained from the video analysis.
Due to limitations of a two-dimensional video image, it was not possible to extract
exact measures of motion from the video images. Also, motion analysis was done only if
the endoscope and video camera appeared to be stationary. This limited the amount of
videotape to be analyzed, because the endoscope was frequently repositioned to follow the
movement of the tools during surgery. Only complete sequences of motion were analyzed.
Note that the data used for the motion analysis of tool end-effectors are the same as those
for the motion analysis by tasks and subtasks.
Analvsis of User Response
An examination of the relationship between task and tool from the perspective of the
user was based on surgeons' responses to the questionnaire. A summary of the
questionnaire responses, question by question, was compiled. Answers to multiple-choice
questions were coded and analyzed. Answers to open-ended questions were treated in the
same manner as feedback from surgeons and summarized to illustrate trends in surgeons'
attitudes and behaviours. As well, any discussions with surgeons by phone or through
face-to-face interviews, including observations made during the laparoscopy workshops
with respect to difficulties encountered and errors made, were summarized and analyzed.
Results of the three analyses (tasks, tools, user response) are presented separately.
In so doing, overlaps will become apparent and the need for integrating the components for
a more meaningful interpretation of the data obvious. Interpretation of the results will be in

2 3
terms of the human-centred triangular strategy, integrating information obtained from task,
tool, and user response analyses in the environment of laparoscopic surgery.

RESULTS
The results are presented for the analysis of tasks, analysis of tools, and analysis of
users' response.
Tasks
Based on the hierarchical analysis of tasks, results are presented for laparoscopic
procedures, procedural steps, surgical tasks, subtasks, and finally motion analysis.
Laparoscopic Procedures 0 : ' ."\ ,,7 (0
From surgical manuals, medical texts and teaching videotapes, three laparoscopic
procedures were analyzed: Cholecystectomy, Appendectomy, and Fundoplication. Each
procedure has its own particular characteristics which make it unique in the operating room
(Cuschieri, 1993, Cuschieri, Nathanson, and Shimi, 1992, Perissat, 1992, Pier & Gotz,
1992, Pollak, 1984, Sackier, 1993, Szabo, 1993). These characteristics include the nature
and severity of the disease, such as clinical signs and symptoms, which demand surgical
intervention; the location of the diseased organ; and the procedural goals. These
characteristics affect the posture of the patient on the operating table, the placement of the
trocars for instrument and camera insertion into the patient, the relative positions of the
surgeon and the video monitors, as well as the performance of the surgical procedures.
The key features are summarized in Tables 1 and 2.
For all three procedures, patient preparation involves cleaning and depilating the
patient's abdominal skin, anaesthetizing the patient, emptying the urinary bladder by
catheterization, and insufflating the abdomen with C02. Because patients are under the
effect of general anesthesia for the duration of the surgery, they are also connected to a
respirator. For a Fundoplication procedure, the patient is also fitted with an endotracheal
tube and a nasogastric tube. The patient's stomach is kept deflated. Once the patient is
prepared, a sterile drape hangs over the abdomen, ready for the first incision.

Table 1 Summary of Key Features in Cholecy stec tomy, Appendectomy , and Fundoplication.
Cholecystectomy jaundice cholangitis frequent and severe
biliary colic
symptomatic cholelithiasis
large gallbladder polyps
acalculus cholecystitis diabetic patients
pregnancy pacemaker obesity cirrhosis previous surgery acute cholecystitis porcelain gallbladder carcinoma gallbladder
remove gallbladder
anaesthetize patient clean and disinfect
abdominal skin empty urinary bladder insufflate abdomen insert cannulae insert endoscopic
camera and instruments
Appendectomy anorexia nausea vomiting pain and tenderness
in lower right abdomen
psoas spasm
appendicitis
obesity
appendix
remove appendix
anaesthetize ~atient clean and dis'infect
abdominal skin empty urinary
bladder insufflate abdomen insert cannulae insert endoscopic
camera and instruments
Fundoplication heart burn dysphagia painful swallowing obstructed
swallowing non-cardiac chest
pain regurgitation hemorrhage failure of medical
therapy development of
complications reflux with motility
disorders and/or oesophageal chest pain
reflux in infants and children
reflux after upper abdominal surgery
previous (failed) antireflux surgery
obesity shortened
oesophagus
cardio-oesophageal junction
increase length of intra-abdohnal segment
anaesthetize patient clean and disinfect
abdominal skin insert endotracheal
and nasogastric tubes
deflate stomach empty urinary bladder insufflate abdomen insert cannulae insert endoscopic
camera and instruments

Table 2 Summary of Major Sur~ical Steps for Cholecystectomy, Apvendectomv. and Fundoplication.
Procedure Patient posture
Surgeon position Major surgical steps
Final steps
Surgical steps analyzed
Basic surgical tasks
Cholecystectomy supine
10-15' head-up tilt legs apart
between the legs of vatient
locate gallbladder isolate gallbladder
from surrounding adhering tissue
dissect from liver clip cystic duct and cut tie cystic duct stump clip artery dissect gallbladder free
of liver remove gallbladder
remove trocars desufflate abdomen close dissect attachments to
liver cut clipped cystic duct dissect gallbladder free
of liver
dissect
Appendectomy supine slight head-down,
lateral tilt to the left side
left side of patient
locate appendix isolate appendix
from surrounding organs and tissue
ligate base of appendix
close lumen of appendix by cautery
cut and remove appendix
disinfect stump
remove trocars desufflate abdomen close cut surrounding
adhering tissue cut base of
appendix
dissect
Fundoplication supine
10-15' head-up tilt
left side of patient
divide peritoneum expose lower
oesophagus and OC junction
lift up the abdominal oesophagus with a sling
pull the fundus of the stomach under and up to the right of thc oesophagus
repair the crura wrap fundus around
the oesophagus suture together remove sling and
orogastric tube remove trocars desufflate abdomen close divide ~eritoneum cut thhhreno-
oesophageal membrane
suture stomach and fundus together
dissect suture tie knot cut suture

27 -- : Generally, the first incision is made at the umbilicus for inserting the endoscopic
camera into the abdominal cavity. The camera is first inserted to inspect the operative site
and locate the diseased organ.' Then, other incisions for the working endoscopic
manipulators are made in the abdomen under visual control. Incisions in the abdominal
wall are maintained open with short cylindrical tubings called cannulae or trocars, which
allow endoscopic tools to be inserted easily into the abdomen without allowing the C02 gas
to escape. Working trocars for instruments are placed in strategic locations for ease of
reach and manipulation during surgery.
-.., For a Cholecystectomy, the procedural goal is to remove the gallbladder which is
located in the right upper region of the abdomen, inferior and medial to the liver.
Therefore, to reach the gallbladder, three working trocars are inserted in the abdominal
wall: One in the left hypochondrium, one in the right hypochondrium, and one in the lower
right hypochondrium (Figure 6).
head
Figure 6. Placement of trocars in a Cholecystectomy. The endoscopic camera is inserted through the cannula at the umbilicus, position 1. Working instruments are inserted at position 2,3, and 4.

2 8
In Appendectomy, the procedural goal is to remove the appendix, which is situated
in the right lower region of the abdomen. One trocar is placed in the left lower abdomen,
and another in the right lower abdomen (Figure 7).
head I
Figure 7. Placement of trocars in an Appendectomy. The endoscopic camera is inserted through the cannula at the umbilicus, position 1. Working trocars are at position 2 and 3.
Fundoplication, on the other hand, is a more involved procedure. The fundus is
wrapped around the oesophagus at the OG junction, and sutured to act as a flutter valve
which closes with apposition of the anterior and posterior walls when the intra-abdominal
pressure rises. A total of five cannulae are required for a Fundoplication. Unlike in the
Cholecystectomy and appendectomy procedures, the cannula for the insertion of the
endoscopic camera in this procedure is located in either of two positions. The two trocars
are placed just above the level of the umbilicus, but laterally along the linea semilunaris on
either side. The remaining three cannulae are placed, one below the right of the xiphoid,
one to the right of the linea alba, and one close to the lower end of the left costal margin
(Figure 8). These positions are such that manipulation of the stomach fundus at the
oesophagus-gastric junction is best achieved.

head
Figure 8. Placement of trocars in a Fundoplication. The endoscopic camera is inserted at position 1 or 2. Working trocars are place at positions 3,4, and 5.

3 0
Procedural Steps
The hierarchical analysis yielded a set of procedural steps for each operation. The
breakdown of the high level goals into a series of steps is presented in Figures 9, 10, and
11. The major surgical steps in a Cholecystectomy (Figure 9) are locate and isolate the
gallbladder from the surrounding tissue and the liver, clip and dissect cystic duct and
artery, and remove the gallbladder.
locate isolate from clip and cut clip cystic gallbladder adhesions cystic duct ar tery
dissect 0 Figure 9. Hierarchical Analysis: breakdown of Cholecystectomy into major procedural steps and surgical tasks.
The steps in an appendectomy (Figure 10) are similar to those in Cholecystectomy.
Once the organ has been located, the surgeon must isolate it from the surrounding tissues,
clipping arteries, sealing the lumen, and removing the organ without spilling its contents.

- locate isolate from ligate base close lumen
appendix adhesions of appendix by cautery
dissect 0 dissect El Figure 10. Hierarchical Analysis: breakdown of Appendectomy into major procedural steps and surgical tasks.
Fundoplication does not involve extraction of an organ, but wrapping the fundus of
the stomach around the oesophagus (Figure 11). This requires cutting the peritoneum to
expose the oesophago-gastric (OG) junction, freeing the oesophagus from the surrounding
organs, wrapping the fundus around and suturing the wrap around the oesophagus to
secure it. A row of continuous stitches running around the wrap, and a column of stitches
attaching the two ends of the wrap (stomach and fundus), are needed. Care must be
exercised when taking bites from the stomach, the oesophagus, the hiatus margin and the
fundus, etc. The underlying tissue to the wrap, such as the OG junction, may or may not
be attached by suture, depending on the extent of the approximation.

dissect n Figure 11. Hierarchical Analysis: breakdown of Fundoplication into major procedural steps and surgical tasks.

3 3
Surgical Tasks
Considerable time and effort was spent in viewing and analyzing the videotapes to
break the tasks down to subtasks with operational definitions of beginnings and endings.
These videotapes were of laparoscopic training workshops in the Animal Research
Laboratory at the Jack Bell Research Centre in Vancouver.
Dissectinp. i -
f ' si'G
p Of the four surgical tasks analyzed, dissecting tissue is the most basic and essential d
skill within the surgeon's performance repertoire. Most, if not all, surgical procedures
require dissection of tissue to expose the operative site, and to extract diseased tissue or
organs. In laparoscopic surgery, the dissection of tissue planes (e.g., peritoneum)
involves lifting the tissue with an atraurnatic forceps using the non-preferred hand, and
dissecting the tissue with scissors using the preferred hand. Similarly, dissection of
specific arteries or organs (e.g., appendix or gallbladder) involves lifting the tissue distal to
the point of dissection with forceps and cutting with scissors.
The task of dissecting was decomposed into two smaller tasks, or subtasks (see
Table 3):
1) lift and pull tissue taut, and
2) cut tissue.
The point of dissection must be visible and accessible by the scissors to be dissected safely
and accurately. Thus, these two subtasks are performed sequentially, with the latter
dependent on the success of the former. It is important that the surgeon exercise care in
gentle handling of the tissue, precise grasping and accurate cutting, especially when
working in regions adjacent to arteries and the common bile duct (in cholecystectomies).
These requirements become the task constraints that govern the way in which the surgeons
perform.

Table 3 Operational Definition of Subtask Initiation and Termination for Dissecting Tissue.
tissue tissue
Begin 1 End first movement of the I termination of
2. snip tissue
1 scissors
Tirneline analysis showed that the expert surgeon, with practice and experience,
was able to coordinate the timing of the two subtasks and achieve proficiency and speed in
dissecting. Novice surgeons, however, spent relatively more time in each phase of the task
(see Figure 12). The average time spent dissecting tissue per cut (n=5), as defined
operationally in Table 3, is 14.60 seconds for an expert surgeon, while the novice surgeons
spent an average of 20.24 seconds per cut (n=35). The novice surgeon spent over twice as
much time as the expert in the first phase of the task, lifting and pulling taut the tissue with
the graspers (9.27 seconds over 4.00 seconds), while the second phase of cutting with
scissors was almost equal for the novice and the expert surgeons (10.97 seconds and 9.27
seconds, respectively).
graspers toward tissue to be cut
first movement of scissors toward tissue
pulling movement; tissue taut
closure of scissors jaws; successful separation of tissue

Task , - I dissect I
\ t
Su btask I pull taut tissue snip tissue I I Figure 12(a). Decomposition of dissecting tissue into two subtasks: 1) pull taut tissue, and 2) snip tissue.
Timeline for Dissecting Tissue -- expert vs. novice
dissect tissue
- pull taut tissue
snip tissue -
Time (seconds)
novice
expert
Figure 12(b). Tirneline for dissecting tissue. The tirneline compares the average times spent in each subtask for an expert surgeon and novice surgeons who were learning the laparoscopic technique in the workshops. The times were averaged over 5 trials for the expert, and 35 trials for five novices. The error bars represent within subject variabilities. For the expert surgeon, the subtask of pull taut tissue contained data from only one trial. Therefore, no variability was calculated. For the novice surgeons, the variability was an average of the within subject variability of four surgeons who performed more than one trial of each subtask. Therefore, it is not reflective of the variability in all novice surgeons.

3 6
Suturing.
Tissue approximation by suturing is a basic and much practiced surgical task. It is
used in laparoscopic procedures where stapling is insufficient to approximate and hold
sections of tissue together, such as in a Fundoplication, or a bowel resection (not analyzed
in this study). Laparoscopic suturing involves passing a needle held by a needle driver
through the tissue, grasping the needle with a needle holder and pulling, then regrasping
with the needle driver to apply another stitch in the tissue. The two stitches, one on either
side of the approximation, constitute one cycle of the suturing task.
Suturing was decomposed into seven subtasks, which are performed in sequence
(see Table 4):
1) position needle,
2) bite tissue,
3) pull needle through,
4) re-position needle,
5) re-bite tissue,
6 ) re-pull needle through, and,
7) pull suture through.
For good approximation of openings in tissue, the placement of the individual
stitches are important. Accuracy is required to place the stitches on both sides of the
approximation for a tight junction when the suture is pulled through. Also, the size of the
bites must be precise to ensure that no tearing of the tissue will occur from too small a bite,
or injury of underlying organs from too deep a bite. It is a relatively difficult and complex
task with its many subtasks.

Table 4 Operational Definition of Subtask Initiation and Termination for Timeline Analysis.
Task Suture
I I I 1 needle 1 2. bite tissue
holder
3. pull 1 needle holder, 1 needle
through driver
Subtasks 1. position
needle holder
1 needle driver,
4. re- 1 needle driver, position 1 needle
holder 5. re-bite 1 needle driver,
tissue 1 needle
Tool 1 needle driver,
1 needle
I holder I
I I through I driver I 6. re-pull
needle
suture 1 needle through holder
1 needle holder, 1 needle
needle driver toward I with tissue
Begin first movement of
the needle or suture contact of needle with
End contact of needle
tissue; end of ~ositibn and orient heedle
first movement of needle holder toward tip of needle
emergence of tip of needle on other side of tissue
end of first pulling movement with needle through tissue
first movement of I contact of needle needle driver toward the needle or suture I with tissue
- - - ~
contact of needle with I emergence of tip of tissue; end of position and orient *
needle first movement of
needle holder toward tip of needle
first movement of needle driverlholder toward suture
needle on other side of tissue
end of pulling movement with needle through tissue
release of suture after adjusting for appropriate
Timeline analysis of suturing and its subtasks, based on operationally defined
beginnings and endings of each subtask (see Table 4), revealed that suturing is a long and
involved surgical task. Even without consideration for the accuracy of suture placement
and bite size in the tissue during workshop practice, novice surgeons took almost twice as
long, on the average, to suture as the expert surgeon (Figure 13). While the average time
spent in six out of seven subtasks was greater for the novice surgeons, the most notable
difference in mean duration between the novices and the expert surgeons were in the needle
position subtasks (1 and 4). For the first positioning subtask in suturing, the expert
surgeon spent, on average (n=7), 5 1.14 seconds orienting the needle such that it was
poised to be passed through the tissue. The four novice surgeons spent an average (n=9)
of 103.25 seconds doing the same. In the subsequent positioning subtask to put in the

3 8
second stitch, which is a repeat of the first, the differences are more remarkable. The
expert surgeon was able to accomplish the positioning subtask in 12.00 seconds while the
novices spent 41.88 seconds on average. The novice surgeons reduced the duration of the
second positioning subtask by over one-half that of their first positioning subtask. The
expert surgeon was able to reduce it by one-fourth. It seemed that for the expert, the needle
corning out the first bite of tissue was in a position and orientation very close to that
desired, such that less time was required to manipulate it. A major difference between the
expert and novice surgeons seemed to lie in proficiency at grasping the needle and moving
it to a desired position and orientation, without slipping or dropping it. More importantly,
it seemed that the expert surgeon was able to coordinate the movement of both graspers to
skip the subtask of the second positioning altogether by immediately taking a second bite of
tissue, without pulling the needle out of the tissue after the first bite. Therefore, the expert
surgeon was able to cut down the overall time spent in suturing, though not the average
time of each subtask. This was possible as there was no accuracy requirement on the
location and size of the second stitch in the workshop context.
Completion of each subtask in the sequence is a prerequisite for the subsequent
subtask, with the exception of step 3. The second bite of tissue, which constitutes the latter
half of a stitch, can be performed directly after the first bite of the tissue has been taken.
That is, the 2 bites of tissue can be taken consecutively without pulling the needle and
suture through after the first bite. This usually happened when the surgeon had a secure
grip of the needle and the pieces of tissue to be sutured together. This may not be realistic
in an operation with a human patient, as precision of bite location and bite size are
important.

Task
position bite pull needle re- re-bite re-pull pull suture Subtask I needle I t i s s u e l t h r u position t i s s u e needle t h r u
Figure 13(a). Decomposition of suturing into seven subtasks: 1) position needle, 2) bite tissue, 3) pull needle through tissue, 4) re-position needle, 5) bite tissue again, 6) pull needle through tissue, and 7) pull suture through tissue.
Timeline for Suturing -- expert vs. novice
suture
pull suture
re-pull needle
re-bite tissue
re-position
pull needle
novice
expert
Time (seconds)
Figure 13(b). Timeline for suturing. The timeline compares the average times spent in each subtask for an expert surgeon over 7 trials, and for five novice surgeons over 10 trials. The error bars represent within subject variabilities. For the novice surgeons, the variability was an average of the within subject variability of three surgeons who performed more than one trial of each subtask. Therefore, it is not reflective of the variability in all novice surgeons.

4 0
Tvine knots.
Tying knots is usually performed after suturing to secure the suture in tissue
approximation. In laparoscopic surgery, both internal and external knotting techniques are
available for the skilled surgeon. External knots are tied free-hand outside the abdominal
cavity and can be accomplished by following a set of procedural steps. These are not
analyzed in this study. Internal or intracorporeal knots are used in relation to suturing.
They are more difficult to execute as the hands are not free to manipulate the needle and
suture. Instead, the knots are tied within the abdominal cavity using a needle driver and
needle holder. The technique for tying a knot is similar to that used in microsurgery.
There are different knot styles depending on the type of suture and the structures
being sutured together. In the laparoscopic workshops, a modified version of the square
knot was practiced. It consisted of wrapping the long suture with needle attached around
the grasperslneedle holder. Then, with the graspers, the short tail is pulled through the
loops to form a knot. The knot is complete when tightened, unlike a square knot, which
forms a loose knot on the first knot, and uses that to adjust and tighten the second knot.
The modified version of tying a knot in laparoscopy were divided into four subtasks (see
Table 5):
1) position needle and suture,
2) form loops,
3) pull short tail through loops, and,
4) pull knot tight.
The best results are achieved if the suture tails are positioned at strategic locations
before the start of tying. That is, the subtasks 2,3, and 4 can be performed smoothly in
sequence, if the surgeon set up the short tail of the suture to be in line with the long-axis of
the free needle holder.

Table 5 Operational Definition of Subtask Initiation and Termination for Timeline Analysis.
Task Tie knot
Subtasks 1 Tool 1 Begin 1. position I 1 needle driver, I first movement of
2. form 1 needle driver, loops 1 needle
holder ! needle and suture
1 needle holder
needle driver toward the needle or suture
3. pull short tail through loops
4. pull knot tight
first movement of driver
1 needle driver, 1 needle holder
1 needle driver, 1 needle holder
with needle and suture in grasp, to loop around holder
end of loop; first movement of holder toward short tail of suture
first movement of needle driver toward the needle or suture
End needle holder is in
position to have suture loop around it; begin of loop
completion of loops; before begin of pull I
through hops
release of suture after tightening
Indeed, timeline analysis showed that a large portion of time was spent in
positioning (see Figure 14). The expert surgeon spent, on average, 15.47 seconds (n=15)
in this subtask, or 32.05% of the total time spent in tying knots. The novice surgeons, on
the other hand, spent about twice the time (30.65 seconds, n=23) positioning, or 35.55%
of total task duration. Novice surgeons seemed to spend about twice as much time
performing each subtask as the expert surgeon. This disproportionate time between the
expert and novice surgeons is consistent for all but the last subtask, pulling knot tight. The
surgeons spent approximately the same time pulling the knot tight (17.00 seconds for
expert, and 19.04 seconds for novices). The time difference between the two groups of
surgeons seemed to be a reflection of the requirements and constraints of the subtasks. In
three of the four subtasks, accuracy in position which required some degree of orientation
seemed to cause the novice surgeons to slow down. Interestingly, the proportions of total
task duration in each subtask are similar for both groups. Again, the larger proportion of
time spent in the last subtask for the expert surgeon seemed to be a reflection of the short
total task duration.

Task
Subtask I position needle pull short tail pull knot & suture thru loops I t ight I
Figure 14(a). Decomposition of tying knots into four subtasks: 1) position needle and suture, 2) form loops, 3) pull suture through loops, and 4) pull knot tight.
Timeline for Tying Knots -- expert vs. novice
tie knot
pull tight
pull thru
form loops
position
Time (seconds)
Figure 14(b). Timeline for tying knot. The timeline compares the average times spent in each subtask for an expert surgeon and five novice surgeons who were learning the laparoscopic technique in the workshops. The times were averaged over 15 trials for the expert and a total of 23 trials for the novice surgeons. The error bars represent within subject variabilities. For the novice surgeons, the variability was an average of the within subject variabilities of five surgeons.

4 3
Cutting suture.
In laparoscopic surgery, this task is similar to dissecting tissue. Thus, the results
are briefly presented, followed by a contrast with the task of dissecting tissue.
The surgical task of cutting suture follows logically from suturing and tying knots.
Suture and needle are removed by cutting the long and short tails of suture near the knot.
The suture is grasped by forceps using the non-preferred hand, and cut with scissors using
the preferred hand. The task of cutting suture was decomposed into two subtasks (see
Table 6):
1) pull suture taut, and
2) snip suture.
The subtask of 'pulling taut suture' can be made easier and faster if, after tying a knot, the
surgeon keeps one of the suture tails in grasp while changing the other graspers for
scissors. All that is required, then, is simply a tug on the suture to pull it taut. The exact
amount /length of suture left attached to the knot is not important, as long as the excess
suture is not too short for the knot to untie or too long to interfere with other structures in
the abdomen. However, it is still important for the point of separation to be visible and
accessible by the scissors to be cut without injuring surrounding structures.
Table 6 ODerational Definition of Subtask Initiation and Termination for Tirneline Analysis.
1. pull taut suture suture
2. snip
Tool 1 graspers
1 scissors
Begin 1 End first movement of the I termination of
Tirneline analysis showed that the expert surgeon was able to complete the task of
cutting suture in 8.67 seconds (see Figure 15). The novice surgeons, on average,
completed the task in 17.00 seconds. A comparison of the times spent in each subtask of
graspers toward suture to be cut
first movement of scissors toward suture
pulling movement; suture taut
closure of scissors jaws; successful separation of suture

4 4
cutting suture showed that novices spent relatively more time than the expert in the subtask
of snipping suture, but not in pulling taut the suture. The times for pulling suture taut were
very similar for both the expert and the novice surgeons, perhaps because the surgeons,
based on instructions from the expert, did not release the suture after tying the knots
previously. Snipping suture took 3.00 seconds for the expert surgeon, while the novice
surgeon, on average, required 10.00 seconds. The longer time may reflect the novice
surgeons' unfamiliarity with the instrumentation, as well as other constraints which affect
performance. - Task I cut suture I
Subtask pull taut suture
Figure 15(a). Decomposition of cutting suture into two subtasks: 1) pull taut suture, and 2) snip suture.
Timeline for Cutting Suture -- expert vs. novice
cut suture
snip suture
pull taut suture
Time (seconds)
- -
Figure 15(b). Tirneline for cutting suture. The timeline compares the average times spent in each subtask for an expert surgeon and four novice surgeons who were learning the laparoscopic technique in the workshops. The times were averaged over 3 trials for the expert and a total of 8 trials for the novices. The error bars represent within subject variabilities. For the novice surgeons, the variability was an average of the within subject variability of each novice surgeon.
novice
expert

4 5
Contrasting cutting suture and dissect in^ tissue.
The two tasks of cutting suture and dissecting tissue are similarly decomposed into
two subtasks:
1) pull taut object, and
2) snip object.
The object, in each task, determines the relative difficulty of the task. The lower degree of
precision requirement for cutting suture compared to dissecting tissue is apparent from the
timeline analysis (see Figure 16(a)). Overall, novice surgeons spent more time in each
tasks than the expert surgeon. All surgeons spent more time dissecting tissue than cutting
suture.
Cut Suture vs. Dissect Tissue --- expert vs. novice
h 3 0 4 U a 2 0 novice III V
B expert
F 10
0
cut suture dissect tissue
Task
Figure 16(a). Cut suture vs. dissect tissue. Comparison of task durations for the expert and 4 novice surgeons. For the task of cutting suture, the mean durations were averaged over 3 trials for the expert surgeon, and a total of 8 trials for the four novice surgeons. For the task of dissecting tissue, mean durations were averaged over 5 trials for the expert surgeon, and a total of 35 trials for five novice surgeons. Variabilities represent within-subject variability for the expert surgeon, and average within-subject variability for the novice surgeons. In the task of dissecting tissue, the average within- subject variability for novice surgeons was calculated from the variabilities of four surgeons. One surgeon only performed one trial of the task.

Pull Taut
n o v i c e expert
Snip
20 1
Q suture E: o
tissue - i lold .... . . . . . . . . . . . . .... ....
B . . . . . . . . .... 5 :.:.:.:. .... .... ... . .... . . . . .... . . . . .... .... .... . . . . .... .... . ... .... .... . . . . . . .. .... 0 .... ........
novice expert
sut,
tissue
Figure 16(b). Comparison of average times for subtasks pull taut and snip. The novice surgeons spent more time than the expert surgeon in the same subtasks. They also spent slightly more time in each subtask when the object being manipulated is tissue. They expert surgeon showed a more pronounced difference in the time spent in snipping. The time spent in snipping tissue was significantly longer than the time spent in snipping suture.
The proportion of time spent in each of the two subtasks reveals the effect of object
properties on the performance of surgical tasks. Figure 16(b) compares the times the
surgeons spent in each subtask for the two tasks of cutting suture and dissecting tissue. In
both subtasks, novice surgeons spent slightly more time manipulating tissue than suture.
Also, the times spent in each subtask are longer than that seen for the expert surgeon. The
expert surgeon, on the other hand, spent less time pulling taut tissue than suture, and
significantly more time in snipping tissue than in snipping suture.
The proportionately greater time duration spent by the expert surgeon in snipping
tissue over snipping suture may be due to the greater precision and safety constraints
required in handling tissue compared to suture. The effect of precision and safety
constraints on performance is not as pronounced for the novice surgeons. Perhaps the
effect of precision and safety constraints due to object properties is masked by the novice
surgeons' unfamiliarity with the new surgical technique. Other constraints may have a
more dominant effect on unskilled surgeons.

Reliabilitv check.
For inter-observer reliability of videotape analysis, one randomly selected video
segment of each of the tasks (suturing, tying knots and cutting suture), was analyzed by a
naive subject. The subject followed explicitly the operational definitions for beginnings
and endings of subtasks, as specified by the researcher. The operational definitions for
suturing, tying knots and cutting suture are presented in Tables 4,5, and 6, respectively.
The test was to show that the system we established for video analysis yields the
same results with different operators/observers. Timeline analysis results for the three
selected video segments obtained by the naive subject were compared to the researcher's
results for the same video segments. Because of the small number of subtasks, and likely
violation of distribution assumptions, two nonparametric tests were conducted (see
Appendix EI). First, Kendall's Rank-Order Correlation Coefficient, T (the nonparametric
analogue of the Pearson Product-Moment Correlation Coefficient, r), revealed that there are
no differences (T= 0.96, a < 0.01) between the two observers' subtask durations.
Second, the Freidman's Rank Test for Correlated Samples (the nonparametric analogue of
matched pairs t-test) showed that there are no differences ( x ~ ~ = 0.267, x~~ < x ~ . ~ ~ (I),
a=0.05) between the two observers' mean subtask durations, based on the set of
operational definitions for tirneline analysis. We are confident that the video analysis
results based on the established criteria are reliable for the purpose of subtask analysis.

I Task Motion Analvsis
Detailed motion analysis revealed that all of the tasks and subtasks could be broken
down to five distinct, basic motions (see Table 7 for descriptions):
ml) reach & orient ,
m2) grasp & holdcut,
m3) push,
m4) pull, and
rn5) release.
This important result was not anticipated when the motion analyses were planned.
Reach & orient was seen whenever the surgeon reached with a tool to grasp or cut a
piece of tissue. Reaching was operationally defined as positioning of the tool end-effector
physically closer to the target by translation along the long axis of the tool, in an inlout
fashion through the trocar, or by rotation of the tool as a lever, using the point of insertion
as the fulcrum. Orienting was seen as a rotational movement of the tool end-effector about
the long axis to orient the jaws of the tool to the object. Occasionally, the surgeon was able
, to coordinate the reach component with the orient component in one smooth motion. More m
; often, the reach occurred separately from the orient, such that the tool was rotated to the 2' <\
correct orientation after the end-effector has reached its target.
, In grasp & holdcut, the end-effectors of the graspers or scissors opened and closed
upon the tissue. Frequently, the open and close action occurred after the reach and orient
motion had occurred. Less frequently, the jaws of the end-effector opened during the reach
and orient motion. Because the chances of cutting or snagging other tissues and arteries
during this movement were high, the scissors were usually closed as they moved
physically closer to the target. Also, the jaws had to be rotated in orientation after the
reach, it was safer to have the jaws closed until the surgeon was ready to close the end-
effectors. This behavior was observed in all the surgeons, and was especially apparent in
cutting with the scissors. With the endoscopic scissors, the grasp & hold m o t i o ~ is

actually a cutting motion. The jaws of the scissors open and close upon the tissue or
7 suture, as with graspers. The closing action of the scissors result in a separation of the
object (tissue or suture), instead of a stable hold on the object.
. Pushing motions were observed in suturing tasks when the surgeon pushed the ." needle through the target tissue. These motions were also observed in other tasks when the
surgeons appeared to be struggling with the tools. Pushing was defined operationally as
any movement of the tool end-effector in a direction that is into the bulk of the target tissue.
The movements made by the tools for this motion were similar to those for reach & orient,
with translation of the tool along the long axis of the shaft, and rotation about the shaft, as
well as about the point of insertion. The end-effector, however, was in contact with the
object in pushing, while this was not the case in the motion of reach & grasp.
- Pulling was observed with the graspers and needle driversholders in all four
surgical tasks analyzed. It was defined as any movement of the tool away from the work
surface while holding suture or tissue that was still connected to the operative site.
Movement directions were opposite to those defined by pushing. Therefore, the same
translation and rotations of the tools were observed.
- Release was noted when the end-effectors of graspers or needle driversholders
opened to release the object in grasp, either intentionally or not. This motion was defined
as the opposite of grasp & hold. The observed movements made by the tools were an open
and close movement of the jaws of the end-effector. Instead of obtaining tissue or suture
into grasp, the object was released from grasp. Therefore, slips of suture or tissue from
the closed jaws after seemingly stable grasp, resulting in a re-opening of the jaws to re-
grasp, were also considered releases. By the same token, scissors actions which did not
cut when the end-effectors closed, resulting in a re-opening of the jaws to re-cut, were also
considered to be release motions.

Table 7 Description of motion and movement coordinate axes. Results of motion analysis revealed that all tasks and subtasks could be reduced to the same elemental motions: reach & orient, grasp & holdcut, push, pull and release motions. Graspers and needle drivers/holders grasp & hold objects with the end-effectors. Scissors, their end-effectors being two blades, grasp & cut the objects with the end-effectors.
Motion Description
Reach & Orient (ml) movement of tool in any direction toward or away from target rotational movement of
Grasp & HoldCut (m2)
Movement Coordinates
tool about tool insert point open and close movement of iaws
Release (m5)
translation along z-axis rotation about z-axis x and y axes
with object in stable gasp open jaws
opedclose about the jaw coordinate system translation along z-axis rotation about z-axis x and y axes translation along z-axis rotation about z-axis xandyaxes opedclose about the jaw ciirdinate svstem -
Below, motions are described for each task in an 'ideal' situation. This 'ideal'
description provides a baseline against which the motion analysis of surgeons' performance
can be compared. The 'ideal' situation is one where all six degrees of freedom are available
for manipulation, and where all attempts of the motions involved in a task are successful.-'

\
:b Dissecting tissue -- motions involved. I\ .\ "
Ideally, the motions required to perform the task of dissecting tissue are ordered as
follows (see also Figure 17):
Subtask 1 : ~ u l l taut tissue
1. reach & orient (graspers),
2. grasp & hold (tissue with graspers),
3. pull (tissue with graspers), and
Subtask 2: s n i ~ tissue
4. reach & orient (scissors),
5. grasp & cut (tissue with scissors), and
6 . release (graspers).
The total number of reach & orient in the pull taut tissue subtask is one, as with grasp &
hold and pull. No push or release motions were required in this subtask. In the snip
subtask, one of each of the reach & orient, grasp & hold (or cut, in the case of scissors),
and release motions was required. Other motions are not necessary for an unconstrained
'ideal'.

Subtask 1: pull taut tissue
Subtask 2: s n i ~ tissue
2. grasp & hold (tissue with
graspers)
3. pull (tissue with graspers)
6. release (graspers)
1. reach & orient
(graspers)
4. reach & orient
(scissors)
5. grasp & cut (tissue with
scissors)
Figure 17. Motions involved in dissecting tissue.

5 3
In practice, the number of motions actually made were generally more than the ideal
minimum. The expert surgeon made about the same number of movements as required, or
additional movements. In the subtask snip, it requires only one grasp & cut motion to
dissect tissue in our 'ideal' description. The surgeons made two attempts at cutting, which
suggests that the first attempt was not successful. This led to extra motions such as push
and pull motions which indicated that some adjustments were necessary when the first
attempts at snipping were not successful. These additional movements are results of
unsuccessful attempts, as well as of the limited degrees of freedom in manipulating the
tools. Other constraints which arise from the altered visual information may also be the
cause.
The effects of the constraints manifest themselves in the performance of novice
surgeons. With less experience and skill, the novice surgeons made a higher repetition of
both the required motions, and other 'additional' ones, than the expert surgeon (see Figure
18). More unsuccessful attempts of goal-directed movements were made due to lack of
skill. The novice surgeons' 'additional' movements included all five motions with the
tools. They resembled groping and exploration rather than goal-directed movements,
suggesting that they were trying to sort out the visuomotor mapping between the video
image and their hands. This suggests that some 'additional' motions may also be required,
given the constraints of laparoscopic surgery, as is evidenced by their observation in the
expert surgeon's performance.

(a) Histogram of Motions in Dissecting
reach grasp push pull release & &
orient hold
motion
(b) pull taut tissue
- 1
5 1 &
0 reach & grasp & push pull release orient hold
motion
ideal
H expert
novice
(c) snip tissue
reach & grasp push pull release orient & hold
motion
Figure 18. Motions in dissecting tissue. The average number of motions made by the expert and the novice surgeons are compared against the 'ideal' situation, where all six
i degrees of freedom for manipulation are available, and all movement attempts are successful. The numbers of motions per dissection were averaged over 5 trials for the expert surgeon, and a total of 35 trials for five novice surgeons. (a) is a comparison of the overall frequency of each motion. Note that no push motions are required in dissecting tissue, as specified by the 'ideal' description. There was no release motion for the expert surgeon as the surgeon did not let go of the tissue and went on to the next task. (b) and (c) are frequencies of motions in the subtasks, pull taut tissue, and snip tissue, respectively.

Suturing -- motions involved.
With no constraints, the task of suturing, with its seven subtasks, could be
accomplished as follows (see also Figure 19):
Subtask 1 : position needle
1. reach & orient (needle driver),
2. grasp & hold (needle with driver),
3. reach & orient (needle with driver),
Subtask 2: bite tissue
4. reach & orient (needle holder),
5. grasp & hold (tissue with holder),
6. pull (tissue with holder),
7. push (needle into tissue with driver),
Subtask 3: ~ u l l needle through
8. release (tissue from holder),
9. reach & orient (needle holder),
10. grasp & hold (needle with holder),
1 1. release (needle from driver)
12. pull (needle out of tissue with needle holder),
Subtask 4: re-position needle
13. reach & orient (needle driver),
14. grasp & hold (needle with driver),
15. release (needle from holder),
16. reach & orient (needle with driver),
Subtask 5: re-bite tissue
17. reach & orient (needle holder),
18. grasp & hold (tissue with holder),
19. pull (tissue with holder),

20. push (needle into tissue with driver),
Subtask 6: re-~ull needle through
2 1. release (needle from driver),
22. reach & orient (needle holder),
23. grasp & hold (needle with holder),
24. release (needle from driver),
25. pull (needle out of tissue with holder),
Subtask 7: vull suture through
26. reach & orient (needle driver),
27. grasp & hold (suture with driver),
28. release (needle from holder),
29. pull (suture with driver).
The total ideal numbers of the five motions are nine reach & orient motions, seven grasp &
hold, two push motions, five pull, and six releases. These motions enable the hands and i
r $ 4 tools to coordinate and approximate tissue. ! - I -

Subtask 1: position needle
Subtask 2: bite tissue
2. grasp & hold (needle with
dr iver)
1. reach & orient (needle driver)
/ (needle with driver)
3. reach & orient
1 (needle holder)
/8\
5. grasp & hold (tissue with
holder)
4. reach & orient
6. pull (tissue with holder)
1 tissue with driver)
b Figure 19. Motions involved in suturing.
7. push (needle into

Subtask 3: ~ u l l needle throu~h
8. release (tissue from holder)
9. reach & orient (needle holder)
10. grasp & hold (needle with holder)
1 1. release (needle from driver)
12. pull (needle out of tissue with needle holder)
Figure 19 (cont'd). Motions involved in suturing.

Subtask 4: re-~osition needle
Subtask 5: re-bite tissue
13. reach & orient (needle driver)
grasp & hold (needle with driver)
release (needle from holder)
16. reach & orient (needle with driver)
17. reach & orient (needle holder)
18. grasp & hold (tissue with holder)
19. pull (tissue with holder)
I driver)

Subtask 6: re-pull needle throu~h
21. release (tissue from holder)
22. reach & orient (needle holder)
grasp & hold (needle with holder)
release (needle from driver)
25. pull (needle out of tissue with holder)
Figure 19 (cont'd). Motions involved in suturing.

Subtask 7: pull suture throu~h
I (needle driver)
27. grasp & hold (suture with driver)
28. release (needle from holder)
Figure 19 (cont'd). Motions involved in suturing.

6 2
Surgeons at the workshops required more attempts in all five categories of motion
to accomplish the task of suturing. Figure 20 compares the number of motions ideally
required to suture, with the average numbers per suture made by expert and novice
surgeons in the workshops (see Figure 20a). Again, 'additional' movements, over and
above the number specified by the 'ideal' description, may be due to the many constraints
in laparoscopic surgery. The expert surgeon seemed to be able to suture using fewer
movements than the novice surgeons, which indicates that skill and experience can help to
reduce the number of 'additional' movements required. The most notable difference in the
number of motions between expert and novice surgeons is seen in the positioning tasks
(subtasks 1 and 4, Figure 20b and 20e).
In positioning the needle (subtask I), the novice surgeons used 15 reach & orient
motions, 12 grasp & hold, 13 pushes, 1 pull, and 8 releases (see Figure 20b). The expert
surgeon, on the other hand, was able to accomplish the same task with 30 fewer motions.
This accounts, in part, for the difference of 52.11 seconds in the average times spent
between expert and novice surgeons to complete the suturing task (refer to Figure 13,
tirneline for suturing).
Within the two subtasks of positioning needle, the most noticeable difference
between the expert and novice surgeons in number of motions is seen in the reach & orient
motion and the grasp & hold motion (see Figure 20b and 20e). These two motions are
usually performed in sequence such that each reach & orient precedes grasp & hold for the
purpose of grasping the object. If the latter was unsuccessful, either due to slippage, or an
incorrect orientation, then the two must be repeated in sequence. Thus, it appeared that the
need to orient in the second needle positioning subtask is decreased compared to the first,
as the needle is already in the general area and direction of the next stitch. In these two
subtasks, all other motions were performed at about the same frequency. Therefore, the
reach & orient, grasp & hold motions seemed to be the most time-consuming components
of the subtasks. Indeed, this is true across all subtasks.

6 3
There was a similar difference in the relative number of motions made in the
repositioning of the needle (subtask 4, Figure 20e). The expert surgeon made fewer
movements than the novice surgeons. However, the total number of movements for both
expert and novice surgeons are lower than in the first positioning subtask. This is also
reflected in the shorter times spent in performing this repositioning, compared to subtask 1,
positioning the needle (refer to timeline for suturing, Figure 13).
(a) Histogram of Motions in Suturing
reach grasp push pull release
& & hold
orient
motion
ideal
expert
[7 novice
Figure 20. Motions involved in suturing. The average number of motions made by the expert and the novice surgeons are compared against the 'ideal' situation, where all six degrees of freedom for manipulation are available, and all movement attempts are successful. The numbers of motions per suture were averaged over 7 trials for the expert surgeon, and a total of 10 trials for five novice surgeons. (a) is a comparison of the overall frequency of each motion.

(b) position needle
reach& grasp & push pull release orient hold
motion
(d) pull needle through
reach & grasp & push pull release orient hold
motion
(f) re-bite tissue
- . reach& grasp & push pull release orient h o l d
motion
( c ) bite tissue
reach & grasp & push pull release orient hold
motion
(e) re-position needle
reach& grasp & push pull release orient hold
motion
(g) re-pull needle through
k 4 7
e 2 * w k
" 0 reach& grasp & push pull release orient hold
motion
(h) pull suture through
I.ldeal 4 expert
5 2 k a O novice
- . reach & . grasp & push pull release I orient hold
motion
Figure 20 (cont'd). Motions involved in suturing. (b) through (h) are comparisons of the motions in each of the seven subtasks in suturing for surgeons against the 'ideal'.

6 5
T y i n ~ knots -- motions involved.
Given the full six degrees of freedom for unconstrained manipulation, a simplified
laparoscopic square knot can be tied quickly and efficiently with a total of five reach &
orient motions, two grasp & holds, two pulls, and one release motion, executed as follows
(see also Figure 21):
Subtask 1 : vosition needle
1. reach & orient (needle driver),
2. grasp & hold (needle with driver),
3. reach & orient (needle holder),
Subtask 2: loop
4. reach & orient (driver with needle),
5. reach & orient (driver with needle),
Subtask 3: vull through loops
6. reach & orient (needle holder),
7. grasp & hold (suture tail with holder),
8. pull (suture tail through loops with holder),
Subtask 4: pull knot tight
9. pull (suture with both needle driver and holder),
10. release (suture from driver and holder).
However, motion analysis showed that the surgeons required more movements to
accomplish the task (see Figure 22). As discussed, although these motions are additional
with respect to the 'ideal' situation, they may be necessary to accommodate the additional
constraints in laparoscopic surgery.

Subtask 1: position needle
Subtask 2: loop
2. grasp & hold (needle with
dr iver)
1. reach & orient (needle
driver)
3. reach & orient (needle
holder)
4. reach & orient (driver with needle)
5. reach & orient (driver with needle)
Figure 21. Motions involved in tying knots.

Subtask 3: pull through loom
Subtask 4: pull knot tipht
6. reach & orient (needle 1 holder)
7. grasp & hold (suture tail with
holder)
8. pull (suture tail through loops with
holder)
9. pull (suture with both driver and
holder)
10. release (suture from driver and
holder)
Figure 21 (cont'd). Motions involved in tying knots.

(a) Histogram of Motions in Tying Knots
reach grasp push pull release & &
orient hold
motion
(b) position needle
reach & gasp & push pull release orient hold
motion
(d) pull thru
reach & gasp & push pull release orient hold
motion
- h ; 4 1 z 2 b LI
0 reach & grasp & push pull release orient hold
motion
(e) pull tight
- . reach & grasp & push pull release orient hold
motion
Figure 22. Motions involved in tying a simplified square knot. The frequencies of the five motions in each subtask made by the expert and novice surgeons are compared with the 'ideal' numbers. Note that there are no pushing motions required in tying a knot.

6 9
In the workshops, the expert surgeon used nine reach & orient movements, eight
grasp & holds, eight pulls, and seven releases, while the novice surgeons used an average
of fourteen reach & orient motions, ten grasp & holds, five pulls, and eight releases for
tying a knot. The novice surgeons required more movements than the expert surgeon to tie
a knot, in all but the pulling motion. The greater number of pulling motions for the expert
was seen in the subtasks of positioning needle, looping, and pulling knot tight (see Figure
22b, 22c, and 22e). In spite of the extra pulling movements, the overall duration of the
subtasks were still shorter for the expert than the novice surgeons (refer to tirneline for
tying knots, Figure 14).
A comparison of the frequencies of other motions in each subtask revealed
inconsistencies between the expert and the novice surgeons. In some instances, the novice
surgeons performed more movements in one motion category, while in other instances, the
expert surgeon performed more movements within one motion category. However, the
duration of each subtask for the expert surgeon remained shorter than that for the novices.
Therefore, it seems that the expert surgeon was able to perform the motions, and hence
subtasks, with greater speed and proficiency.

7 0
Cutting suture -- motions involved.
The task of cutting a piece of suture theoretically could be accomplished simply
with two reach & orient motions, two grasp & hold/cut, one pull motion, as follows (see
also Figure 23):
Subtask 1 : pull taut suture
1. reach & orient (graspers),
2. grasp & hold (suture with graspers),
3. pull (suture with graspers), and
Subtask 2: sniv suture
4. reach & orient (scissors), and
5. grasp & cut (suture with scissors).
Motion analysis reveals that surgeons performed more movements within each category of
motion than the ideal description for cutting suture (see Figure 24). This, again, may be
due to the increased constraints with the instrumentation and viewing perspectives in
performing laparoscopic surgery.
Surprisingly, the expert surgeon made more movements than novice surgeons in
cutting suture. Overall, there were more reach & orient, grasp & hold, and release motions
in handling suture. Although the expert surgeon used more movements to cut suture, he
was able to accomplish the task in significantly less time than the novice surgeons (refer to
tirneline for cutting suture, Figure 15). In decomposing the individual subtasks, it became
apparent that most of the expert surgeon's 'additional' motions were performed in pulling
taut the suture before snipping. The expert surgeon performed more reach & orient, grasp
& hold, and release motions than the novice surgeon. The greater number of release
motions would suggest that the surgeon dropped the suture, or adjusted the length of the
suture in grasp by regrasping.

Subtask 1: pull taut suture
2. grasp & hold (suture with
graspers)
3. pull (suture with graspers)
1. reach & orient
(graspers)
4. reach & orient
(scissors)
5. grasp & cut (suture with
scissors)
Figure 23. Motions involved in cutting suture.

(a) Histogram of Motions in Cutting Suture
m h &
orient
ideal
El expert
I7 novice
grasp push pull release &
hold
motion
(b) pull taut suture
motion I motion
(c) snip suture
R 3 0
2 2 a ," 1 L
" 0 reach & grasp & push pull release orient hold
Figure 24. Motions involved in cutting suture. The frequencies of motions made by the surgeons in the laparoscopic workshops are compared with the 'ideal' situation. Note there are no push motions involved. (a) overall frequency of motions, (b) frequency of motions in pulling taut the suture, (c) frequency of motions in snipping suture. The expert surgeon performed more motions in pulling taut the suture, presumably dropping the suture or regrasping to adjust the length.
3 3
2 a 5 1 L
" 0 reach & grasp push pull release orient & hold
Contrasting cut tin^ suture with dissectinp tissue.
In essence, the two tasks of cutting suture and dissecting tissue have similar
subtasks, which consist of similar motion sequences. However, a comparison of the
surgeons' performance in these two tasks reveals marked differences. Figure 25 compares
the number of movements made for the two tasks of cutting suture and dissecting tissue.
The number of attempts in grasping suture to pull taut was greater for the expert surgeon
than for novice surgeons. This is contrary to the general pattern seen in other subtasks.
More interesting is the observation that the expert surgeon made more movements in the
subtask of pulling taut suture than in pulling taut tissue. The surgeon seemed to either
misjudge the location of the suture, or drop it. In general, the total number of attempts
made in each motion category is higher in grasping suture than tissue for the expert surgeon
(see Figure 24a and 24c). This may be due to the difference in accuracy constraints of the
object being grasped. Both subtasks require that the graspers approach the object with
care, so as not to penetrate into the underlying structures. However, the tissue plane has a
larger surface for grasping, with less demand on the precise location and orientation of
grip. The suture, on the other hand, is thinner and requires that the graspers' jaws be
oriented to close precisely upon the suture. Thus, object properties also affect the
performance of remote manipulation in laparoscopic surgery.

(a) pull taut suture
I reach & grasp push pull release onent & hold
I mot ion
(c) pull taut tissue
I reach & grasp push pull release onent & hold
I mot ion
(b) snip suture
Unovice u reach & grasp & p u s h . pull . release ' orient hold
m o t i o n
(d) snip tissue
'reach & ' gracp & ' push ' pull ' release ' orient hold
m o t i o n
Figure 25. Contrasting the motions involved in the tasks cutting suture and dissecting tissue. Note that in subtasks snip suture (b) and snip tissue (d), the motion grasp & hold is equivalent to the cut motion of the scissors.
The opposite pattern in performance differences is seen in the subtasks snipping
suture and tissue (Figure 25b and 25d). Overall, surgeons made fewer motions in snipping
suture than in snipping tissue. Clearly, surgeons were able to cut the suture in a
straightforward fashion, without too many other motions such as pushing or pulling, as
seen in snipping tissue. The repeated cutting motion in snipping suture by the novice
surgeons were most likely due to dull scissors which did not cut the suture with the first
closure. Tissue, in contrast, was not snipped in a straightforward fashion. Surgeons
appeared to manipulate the tissue with the scissors before making the final cut. This
behavior may be a double-checking performed to ensure the location of dissection is
absolutely precise. It is clearly more important to locate the cut precisely when cutting
tissue than when cutting suture. Therefore, safety constraints also affect the performance
of remote manipulation in laparoscopic surgery.

Analvsis of Tools
Results for the analysis of tools are presented in this section. A descriptive analysis
of the physical and functional characteristics of each tool is followed by a tool motion
analysis.
La~aroscopic Mani~ulators
The endoscopic tools analyzed in this study are manipulators used to perform the
surgical tasks of dissecting tissue, suturing, tying knots, and cutting tissue. They are the
straight graspers, curved scissors, and needle drivers/holders (Figure 26). Although other
tools are also used in laparoscopic surgery, such as the scissors with unipolar cautery to
dissect tissue, or the stapler to approximate, they are used only under special conditions.
The graspers, scissors and needle driverslholders, on the other hand, are basic mechanical
manipulators which are used under all conditions. As seen in the workshops, all surgeons
must learn to be proficient with them in order to perform the surgical tasks successfully. In
general, the endoscopic tools examined (Ethicon, Johnson & Johnson) have a long rigid
shaft with a standard 5 rnrn or 10 mm diameter. The longer tools have a 32 cm long shaft,
while the shorter ones are 21 cm long. The end-effectors are similar to traditional
microsurgical instruments, such as scissors and graspers. They are typically two jaws
joined by a simple hinge joint. The hinge is connected by cables running along the shaft to
the handles. The handles of the endoscopic tools are most commonly two-ringed handles,
like scissors. The handles are joined with a pin joint such that the opening of the handles
opens the jaws at the end of the shaft. The handle is rigid and is at right angles to the
length of the shaft, much like the configuration of a pistol. The tool is held at the handle by
inserting the thumb in one ring and two or three fingers in the other ring, as in holding a
pair of scissors.
Laparoscopic praspers.
Graspers are used to grasp tissue or suture for cutting. The graspers examined are
straight graspers with standard 32-cm or 21-cm long shafts. The graspers have, as end-

7 6
effectors, two jaws connected by a hinge joint which allows the jaws to open and close
with equal range of motion from the central axis along the shaft of the instruments. The
end-effectors of the graspers are all similar in shape with varying sizes in the teeth for grip
on the inside surface of the jaws. The jaws are opened and closed by a two-ringed handle
which is held by inserting the thumb into one ring, two or three fingers in the other ring.
To operate the tool, the fingers and thumb flex and extend in opposition to close and open
the jaws. The hand grips and applies pressure on the handle to maintain stable grasp of the
object by the tool. Most modern graspers are made with a ratcheted handle which may be
switched on with a finger when the graspers are in a closed position. This allows the
surgeons to release the hand's grip on the handle with the object held securely in grasp.
The hand can thus manipulate the tool more freely without constantly applying pressure to
keep the graspers closed.
The proximal end of the shaft is fitted with a pin-wheel which allows the index
finger to rotate the shaft 360-degrees about its long axis. Orientation of the graspers, with
jaws open or closed, can be accomplished by spinning this wheel, or simply by rotating the
handle along the tool shaft with a twist of the wrist. Other movements of the tool, such as
in and out of the trocar in the abdomen, or sweeping around to reach for tissue or suture,
must be accomplished through movements of the arm. The trocar acts as a fulcrum for the
circular sweeping of the tool, as well as an anchor for the surgeon to steady the tool. This
aids in accuracy by guiding the graspers towards and away from objects in a straight line.
Laparoscopic scissors.
At the workshops, the scissors used to dissect and cut suture were similar in design
to the graspers (Ethicon, Johnson & Johnson). The only difference between endoscopic
graspers and endoscopic scissors are the end-effectors. In place of a pair of straight, flat
jaws with varying gradation of teeth for grasping, the scissors have, as their end-effectors,
miniaturized scissors. The two blades of the scissors are connected by a hinge joint which
is either single or twin action. In single action hinge joints, one blade moves to open and

7 7
close the scissors, whereas in twin action hinge joints, both blades are movable. There are
variations in the design of the blades. The 'curved scissors', which are the ones used to
dissect and cut suture, have their blades tapered to the tips and slightly curved along the
length of the blades. Other variations of endoscopic scissors are 'hook scissors' and
'micro scissors'.
The endoscopic scissors are operated by the hand, opening and closing with the
two-ringed handle. The handle of endoscopic scissors are not equipped with a ratchet, as it
is not possible to maintain stable grasp of the object with scissors. Other movements of the
tool can be made as with the endoscopic graspers. The long shaft of the scissors can be
rotated on its long axis, independent of the handle, by rotating the pin-wheel at the
proximal end of the shaft. The tool, as a unit, can be inserted and withdrawn from the
abdomen along the cannulae, as well as rotated in a circular sweeping motion using the
insertion point at the abdominal wall was a fulcrum. Most endoscopic scissors are
disposable. This eliminates the problem of dull scissors blades with repeated use.
La~arosco~ic - needle driverslholders.
Needle driversfholders work as a pair to suture and tie knots. In suturing, one acts
as the driver to drive the needle through the tissue, while the other acts as the receiver to
receive the needle as it comes out of the tissue. When tying knots after suturing, the needle
driverslholders act as simple grasping forceps to manipulate the needle and suture.
These tools have similar designs as the graspers and scissors described above. The
handles are two-ringed scissor-type handles with a ratchet on the driver, but no ratchet
mechanism for the holder. Because the needle for suturing has a curved tip, it is important
that the needle be maintained in the appropriate orientation while biting into the tissue.
Therefore, the ratchet on the driver handle allows the needle to be locked in one orientation
once in stable grasp, and prevents the needle from rolling and changing orientation when it
pushes against and into the tissue. The holder receives the needle and transfers it to the

7 8
driver without regard for the orientation. Therefore, a ratchet is not necessary as the holder
does not apply and maintain great forces on the needle.
The difference in function between the needle driver and needle holder can also be
seen in the grasping surfaces of the end-effectors. The grasping surface of the driver has
finely serrated groves for better hold, while the holder has a smoother, more even lattice
texture grasping surface. Outwardly, the end-effectors look identical, both a pair of jaws
joined by a hinge joint with single action. One jaw is fixed and in-line with the long axis of
the shaft. The other jaw is the only movable part of the end-effector that is joined by the
hinge to the tool. Opening and closing of the movable jaw upon the fixed jaw is controlled
by the opening and closing of the hand at the handle.
The long shaft of the needle driversholders are fixed at right angles to the handle.
Unlike the endoscopic graspers and scissors, the needle driverskolders do not have an
independently rotatable shaft. Therefore, it can only be rotated about its long axis by
rotating the whole instrument by the hand and arm. Other movements of the tools are also
thus constrained. The other degrees of freedom for tool movement are rotating the tool as
one unit, about the point of entry, as well as translation in and out of the abdomen along the
trocars.
Tools
Graspers Scissors
Figure 26. Conventional laparoscopic manipulators.

Tool Motion Analysis
The motion analysis of each endoscopic manipulator was based on the motion
analysis of surgical tasks which used the tools.
Graspers -- motions involved.
In tissue dissection, the role of the graspers is to lift up the tissue from the
underlying structures and keep it taut, while the scissors cut. The surgeons perform the
subtask 'pull taut tissue' entirely with the graspers using the non-preferred hand. The
surgeon's hand holds the tool handle by inserting the thumb in one of the two rings at the
handle, and two or more fingers into the other ring. Upon inserting the tool into the
abdominal cavity through a trocar, the tool stands vertical with the handle horizontal above
the patient's abdomen. With the hand holding onto the handle, the surgeon's elbow is
flexed and the shoulder elevated. The hand is flexed and adducted at the wrist. The hand
is lowered when the tool is pushed further into the abdominal cavity; and when the tool is
rotated at the point of entry into the abdomen. Taller surgeons are able to hold the tools
without too much elevation of the shoulders and elbows in a relaxed posture. Under the
stress of surgery, their posture may become more tense with elevated shoulders and
elbows. For surgeons with a smaller physical stature, this awkward posture becomes more
extreme . Once the end-effector of the graspers is in view on the video monitor, the surgeon
moves the graspers towards the operative site. The arm and hand pushes the tool into the
abdominal cavity in a straight line, using the trocar as a guide and anchor. The hand tilts
and sweeps the tool in circular motions, using the point of insertion in the abdominal wall
as a fulcrum. These hand movements controlling the handle are small motions with the
biggest hand movement no more than 10 cm in length. They are rigid and discrete
movements with pauses between them, much as movements of a robot or mechanical doll.
Near the site of dissection, the hand holding the tool handle starts making even smaller
movements. These smaller movements are not to bring the tool end-effector closer to the

8 0
tissue. Rather, they orient the tool end-effector for grasping tissue. The hand opens the
handle by extending the fingers and thumb to open the graspers at the end of the tool.
Then, the wrist flexes the hand around to rotate the tool about its long axis. The hand is
now acutely flexed or extended at the wrist. The graspers rotation can also be achieved by
spinning the pin-wheel at the proximal end of the shaft using the index finger, while
keeping the handle stationary. However, it was noted that the most frequently observed
mode of control is with the wrist. In fact, only one surgeon (the expert surgeon in our
study) used the pin-wheel, but only rarely. The pin-wheel is often too stiff to be turn with
one finger, and requires two hands to operate.
The end-effector of the graspers, once opened and oriented, is moved toward the
tissue with even smaller movements of the hand. At this point in the task performance,
only minute adjustments are made with the hand to 'home-in' on the tissue. When the
surgeon perceives the graspers to be close to the tissue, he advances the graspers slowly
until he just touches the tissue with the graspers. This extra degree of care is taken to avoid
injury to the underlying structures. When the end-effector is in contact with tissue, the
surgeon flexes the thumb and fingers of the hand to close the handle, and consequently, the
graspers. If the surgeon was unsuccessful with the first attempt at grasping the tissue, the
process is repeated with even more care and longer pauses after each adjustment.
Once the tissue is in grasp, the hand applies pressure on the handle to maintain a
secure grip on the tissue. Keeping the orientation of the tool, the arm moves to withdraw
the tool slightly out of the trocar, or to tilt the tool slightly in the opposite direction to pull
the tissue taut. The scissors then move in to cut.
It is interesting to note that each movement made was of one or two degrees of
freedom, and as a discrete motion, with long pauses between consecutive motions. This
may presumably be for visual feedback processing, and visuomotor transformations to plan
for the next movement.

8 1
For the duration of the task of dissecting tissue (20.24 seconds for novice
surgeons, 14.60 seconds for the expert surgeon), the surgeon's shoulders, arms and hands
were put in an awkward posture, allowing only minute movements, one at a time. For the
novice surgeons, inexperience, anxiety, and unfamiliarity with the instrumentation and
visual cues seemed to add tension to the awkward posture for the upper limbs. This is
highly conducive to fatigue, frustration, errors in performance, and injury to the surgeon as
well as to the patient.
In cutting suture, the role of the graspers is to pick up the suture tail from the
surface of the operative site, so that the scissors can cut near the knot without inadvertently
cutting the adjacent tissue. The graspers are used to perform the subtask of 'pull taut
suture'. The procedure for manipulating the graspers to grasp suture is identical to that for
grasping tissue. The non-preferred hand is used to handle the tool. Manipulation of the
pin-wheel to rotate the shaft independent of the handle may be awkward due to the less
dexterous hand. Therefore, the preferred method of rotating the graspers is with wrist
movement. The awkward posture with the elevated shoulder, elbow and wrist is adopted.
This awkward posture is held for the duration of the task. Minute, discrete movements
with the hand and arm adjusts the orientation of the tool to 'home-in' on the suture.
Scissors -- motions involved.
The laparoscopic scissors are used to perform the subtasks 'snip tissue' and 'snip
suture', in the tasks dissection and cutting suture, respectively. These subtasks follow the
subtask of 'pull taut', performed by the graspers using the non-preferred hand. The
surgeons hold the scissors in the preferred hand. Postures for holding the scissors are
similar to those described for holding the graspers. Motions of the hand controlling the
scissors are also similar to those for controlling the graspers, as the two tools are similar in
their structural design of the handle, the shaft, and the end-effector.
The arm, first of all, pushes the tool into the abdominal cavity along the trocar.
Then, it positions the end-effector of the tool near the location of the object to be cut.

8 2
These positioning movements are performed relatively quickly compared to the reaching &
grasping motions of the graspers. Surgeons seemed to have a good sense of the target
position, after having spent a great deal of time placing the graspers with the other hand.
Once the scissors are near the target, the arm stops and the hand opens the handle to open
the end-effector. Some adjustments are made at this point to orient the scissors to the
object. In the laparoscopic workshops, these adjustments were sometimes made by
rotating the handle with the hand. At other times, the other hand was used to turn the pin-
wheel which rotates the shaft only, keeping the handle stationary. As a result, the surgeon
must re-orient with the graspers afterwards. It seemed that the more intuitive response to
rotate the tool end-effector was to rotate the handle in the same direction, as described,
rather than to use the pin-wheel for orienting the scissors end-effector.
In general, the subtask of snipping took less time to perform in cutting suture than
in dissecting, especially for the expert surgeon. Therefore, the awkward posture need not
be held as long in the task of cutting suture, as with dissecting tissue.
Needle drivers/holders -- motions involved.
In both surgical tasks of suturing and tying knots, the needle drivers/holders act as
grasping forceps. In suturing, the needle drivers are used to push the needle through
tissue, while the needle holders are used to receive the needle and pull it out of the tissue.
Because of the greater force required to push the needle through tissue, and the greater
precision required in placing the stitches, surgeons usually perform suturing tasks with the
needle driver held in the dominant hand, and the needle holder in the non-dominant hand.
The hands hold the tool handles by inserting the thumb into one of the two rings at the
handle, and two or more fingers into the other ring. The tips of these two tools meet at the
operative site inside the abdominal cavity, usually forming a right angle. The surgeon's
body posture adopts the same posture as described for using the graspers and scissors.
The surgeon's elbows and wrists are flexed, and the shoulders are elevated. In the

8 3 workshops, it was observed that surgeons' shoulders become more elevated and tense with
time, when suturing and tying knots.
Once the needle driver, with the needle and suture, and holder are in view on the
video monitor, the surgeon moves the tools toward the operative site along the trocars.
Near the suture site, the hand rotates the driver to orient the needle tip with the tissue to be
sutured. As the needle drivers and holders are not built with a pin-wheel to rotate the shaft
independently of the handle, the only option for the surgeon to rotate the jaws of the drivers
and holders is to rotate the entire tool. Therefore, the hand holding the needle driver is
flexed at the wrist while applying pressure on the handle to maintain grasp of the needle.
At the extreme of the wrist's range of motion, the holder moves toward the needle to grasp
the needle. To do this, the hand holding the needle holder may pronate and flex at the wrist
to orient the jaws to grasp the needle and maintain its orientation. As the needle driver jaws
open to release the needle, effected by the hand opening the handle, the hand supinates and
extends its wrist to turn the end-effector jaws to regrasp the needle from the needle holder.
This procedure is repeated until the needle tip is in the correct orientation to pass through
the tissue. Thus, the number of reaching & orienting, grasping & holding, and releasing
motions in needle positioning outnumber the reach & grasp motions in other tasks (see
Figure 20). These precise positioning and orientation tasks are more affected by reduced
degrees of freedom in tool manipulation than other tasks which do not require much
precision.
With the needle tip in the desired orientation, the two hands with their tools must
work together to push the needle tip into and through the tissue. If the needle tip is not
directed in an appropriate angle, the bite size would be affected. Also, the needle may roll
and swivel the tip into an undesirable orientation. The hand holding the needle driver
squeezes the handle to apply more pressure on the needle in grasp, to maintain stable grasp
and orientation. At the same time, the hand pushes the needle into the tissue.

8 4
In the context of the laparoscopic workshop, it was not critical for the surgeons to
take precise bite size of the tissue, nor was it essential to place the stitch in an exact
location, therefore, the needle was pushed into the tissue with great force, in an haphazard
manner with respect to location. The aim was to pass the needle through some tissue.
Precise location and bite size would be essential in the operating room.
Pulling the needle and suture through the tissue is relatively more simple than
positioning the needle. Once the needle is in grasp, the hand and arm simply withdraws the
tool away from the operative site. In this subtask, the needle holder acts as simple
graspers.
Tying knots with the needle drivers and holders also involve positioning of the
needle and suture. As with the subtask of positioning needle in suturing, there are many
rotational movements made by the hands. However, it is not important to orient the needle
tip in a specific angle, but in a general direction. Forming loops with the suture requires
coordination between the two hands and tools. The tips of the tools must be moving in
opposite directions in a circular fashion with respect to the long axis of the tools.
However, this is too complex to perform in the limited volume of space within the
abdomen. Therefore, the tip of one tool, with the suture in grasp, is rotated about the tip of
the other tool which is held fixed in position. The wrist of the hand holding the rotating
tool is usually held fixed. Circular movements of the end-effector are effected by the
movements of the arm. The arm moves slowly with tiny movements primarily about the
shoulder joint.

8 5
Analysis of User Res~onse
An examination of the relationship between task and tool, from the perspective of
the user, was based on surgeons' responses to the questionnaire, as well as any discussion
with surgeons by phone or through face-to-face interviews. A summary of the surgeons'
responses to the questionnaire will be presented, followed by comments made by surgeons
during interviews. Surgeons' views on laparoscopic task performance and tool use are
presented with selected comments quoted directly from the surgeons to exemplify the
general responses. All responses to the open-ended questions on the questionnaire are
compiled in Appendix IV. Comments have been transcribed directly from the
questionnaires to ensure surgeons' anonymity.
Questionnaire Response
Demogravhics.
A total of 252 questionnaires were mailed out to B.C. general surgeons. The
number of responses to the questionnaire was 94, or 37% response rate. Of those who
responded by returning the questionnaire, sixteen surgeons were retired, were not of the
general surgery discipline, or did not practice endoscopic surgery. Therefore, the
questionnaires were returned unmarked. The remainder of the returned questionnaires
(n=78) were sorted for completeness and analyzed. Questionnaires with answers for all
questions were considered complete. Those with any number of unanswered questions
were considered partially complete. Interpretation of user response were based on these 78
complete and partially complete questionnaires only. Results from the questionnaire
analysis are presented in Table 8.

Table 8 Sumrnarv of survev auestionnaire response analysis. Only completed and partially completed questionnaires were analyzed (n=78). Blank questionnaires returned by retired surgeons or non-general surgeons with fellowship in the B.C. General Surgeons Registry were not included in the analysis. Calculation of percent- response was based on the total number of questionnaires analyzed.
)emographics rota1 questionnaires rota1 response f completed questionnaire f partially completed questionnaire f blank questionnaire rota1 questionnaires analyzed
Sender of Surgeons Female Male Undeclared
4ge of Surgeons Minimum Maximum Range Mean Median Mode
fears of Practice Minimum Maximum
Range Mean Median Mode
Years of ES Experience Minimum Maximum Range Mean Median Mode
Number % Response

Table 8 (cont'd)
Surnrnarv of survey yuestionnaire response analysis.
Number
# of Surgeries Per Month Minimum Maximum
Range Mean Median Mode
# Teaching Demonstrations Per MOI Minimum Maximum
RaKP Mean
First Choice of Techniques Prefer Open Prefer ES Undeclared
Techniques Used in Practice ES only Open only Both
Types of Tool Handle Used Scissors Palm Both Undeclared
Types of Tool Handle Preferred Scissors Palm Undeclared
Tool Handle Size Appropriate for Hand Yes No Undeclared
6 Response
7.69% 88.46% 3.85%
0.00% 1.28%
98.72%
75.64% 19.23% 1.28% 3.85%
52.56% 20.51% 26.92%
79.49% 17.95% 2.56%

Table 8 (cont'd)
Summary of survey questionnaire response analvsis.
Number
Laparoscopic Procedures Most Per Cholecystectomy Inguinal Hernia Repair Appendectomy Hiatal HerniaIFundoplicati Diagnostic Laparoscopy Tubal Ligation Bowel Resection Splenectomy Thoracoscopic Procedures Others
-low Surgeons Feel Performing Lap; Challenged Frustrated Tired Angry Other or Undeclared
lived Error Frequency Often Sometimes Rarely Undeclared
rmed
YO Response
'oscopic SUI 4 7 44 2 C 1 1 1 4
Ranking of Ease of Use of Tool 1 TOOIS 1 ~ r a s ~ e r s 1 Scissors 1 Needle ~r ivers l Easy Medium Difficult
Ranking of Ease of Performance of Task
51 -30% 35.90%
5.10%
Task Most easy Easy Moderate Difficult Most Difficult Undeclared
51.30% 33.30%
7.70%
Grasp 44.90% 34.60% 10.00% 2.60% 2.60% 5.00%
Cut 57.70% 16.70% 16.70% 2.60% 2.60% 3.80%
12.80% 10.30% 62.80•‹h
Position 25.60% 30.80% 32.00% 2.60% 3.80% 5.00%

8 9
Of the seventy nine surgeons whose responses were analyzed, over 93% of them
were male. The ages of practicing surgeons ranged from 29 to 66, with a range of 37
years. These surgeons have been practicing surgery for an average of 18 years, with the
youngest surgeon having 2 years of experience, and the oldest 38 years. The amount of
experience in laparoscopic surgery is significantly less. The minimum amount of
experience was reported by one surgeon who newly acquired the technique and
incorporated endoscopy into his practice four months ago. The most extensive amount of
experience was reported by a teaching surgeon who has been doing laparoscopic surgery
for 21 years. Obviously, not all surgeons are in the latter position. As at 1995, the
majority of BC general surgeons have, on average, 3 to 4 years of laparoscopic experience.
While only one surgeon reported to practice only open techniques, all other
surgeons practice both open and endoscopic surgery. However, for 6 surgeons, open
surgery would be their first choice of technique to perform a particular procedure. Still,
over 88% of surgeons indicated that endoscopic surgery would be their first choice of
technique, unless contraindicated.
From the surgeon's reported number of years practicing laparoscopic surgery, it is
apparent that this technique has only come into wide-spread practice in the last 4 years.
Therefore, the number of different procedures that the surgeons are competent to perform
are still limited to the simple procedures. The most common laparoscopic procedures
performed are Cholecystectomy, Inguinal hernia repair, and Appendectomy. In fact,
reported figures show that 86% of surgeons perform Cholecystectomy on a regular basis.
The more complex procedures, such as Fundoplication and bowel resection, are performed
currently by only a small number of surgeons (13% and 5%, respectively).
Most surgeons perform an average of 10 surgeries per month, with one surgeon
reporting as many as 80 cases per month, and another 60 cases per month, while others as
few as four per month. It was also noted that the two surgeons who performed a

9 0
significantly greater number of surgeries per month are teaching surgeons. The majority of
surgeons, however, do not participate in teaching demonstrations.
On tasks.
Surgeons were asked to rank five surgical tasks for task difficulty. The tasks were:
cutting, positioning, grasping, suturing, and knotting. On a five-point scale, a ranking of
(1) would mean that the task is the most easy to perform, while a ranking of (5) would
mean that the task is the most difficult. Some surgeons ranked more than one task with the
same degree of difficulty. Other surgeons who had no experience with suturing and
knotting did not rank these tasks with the other tasks. A majority of surgeons ranked
suturing as 'difficult' (50%), and tying knots as 'the most difficult' (56%). In contrast,
58% of surgeons ranked cutting as the 'easiest' task. Grasping and position were ranked
as easiest, easy and moderate by the majority of surgeons (see Figure 27).
Task rating
easiest
easy
medium
difficult
most difficult
cut grasp position suture knot
tasks
Figure 27. Rating of task difficulty by 79 B.C. General Surgeons who perform laparoscopic surgery.

9 1
On instruments.
In general, the difficulties with instrumentation encountered by surgeons during
laparoscopic surgery concern primarily poor visualization of the operative field,
unresponsive instruments, and difficulty with maneuvering inside the abdominal cavity.
Poor visualization issues are mostly concerned with the lack of depth perception on a two-
dimensional image for complex manipulative tasks. Other difficulties with visualization are
technical, such as fogging lens, poor lighting, and limited field of view. Surgeons also
indicated that the angle of the endoscopic camera with the operative site, relative to the
surgeon's body centre is a major source of orientation difficulty. The difference in view
perspective creates a discrepancy in the direction of movements made by the surgeons, and
those seen on the monitor. 'It is difficult to work perpendicular (or at any other angles), to
the camera. I am better if I'm lined up to the image'. This may be a reason for surgeons
feeling 'insecure at dividing tissues'.
Difficulties with unresponsive instruments during surgery were a result of wear-
and-tear from overuse. The delicate instruments break and wear out quickly. Scissors
become dull, and graspers and needle driverslholders lose their grip. The jaws of the tools
often become stiff, resulting in the hands applying excess pressure to operate the
instruments. Also, the lack of feedback from the end-effector may result in 'overuse of
gripping pressure' by the hand, leading to tissue tear.
Many surgeons reported that they have no tactile feedback at all with the endoscopic
tools. The lack of tactile feedback regarding the feel of tissue is a problem which can lead
to injury, for example, to the bowel or the common bile duct. Other surgeons claimed that
although feedback from the tissue is limited, they still have a good feel of the tissue. They
'can tell if tissue is inflamedwoodnot', 'but not as good as in open surgery, not as
"sensitive"'. It appears that surgeons learn to relate the altered sensation to what they
would feel in open surgery, based on what they see on the video image. That is, they
'learn to recognize "feel" of tissue over 3-4 months'. Some say that it is 'not really a

9 2
"feel", more a correlation between force applied and visual tissue changes', and this can be
'easily related to open feel if experienced in both types of surgery'. 'After a while, [the
feel] is same as open surgery'. Therefore, 'both visual and tactile [feedback] are relevant.
A few surgeons go as far as saying that the feel of tissues with the endoscopic tools is
'realistic, like with handslin open'.
In general, the tools are difficult to manipulate within the abdominal cavity. They
have a rigid shaft which may be too long or too short. When working in a small area, the
long tools and the trocars interfere with one another, making positioning tasks very
difficult. In particular, the instruments are too large and clumsy for pediatric use, and for
delicate tasks. Surgeons suggested that the shaft should be rotating and flexible to go
around corners. In addition, the poor angle between the handle and the shaft of the tool
forces the surgeons' wrist to be flexed acutely and maintained in this posture for some
time. The surgeons' hands often become fatigued. This may be conducive to cumulative
trauma disorder. One surgeon suggested that the handle should be angled to allow the
wrist to be neutral while operating the tools. Another surgeon suggested complete re-
design of the tools. 'At present, the instruments are too much like the standard open
instruments. They will need to take on their own unique character and appearance, rather
like the car of today which bear little resemblance to the original "horseless carriages". The
latter however were similar to horse drawn carriages without the horses'.
The endoscopic manipulators available today have two different types of handles.
The most common one seems to be the traditional 'scissors' handle with two rings for
thumb and fingers insertion, as 76% of surgeons use this type. The other less widely used
handle is the newly designed 'palm' handle which resembles the handle of a pair of pliers.
More than 52% of surgeons claim to prefer the 'scissors' handle, while 21% claim to prefer
the 'palm' handle (see Figure 28). The remainder were undecided, as most of them have
never used the palm handle.

Endoscopic Manipulators
scissors palm handle handle
Type used
Type preferred
both
Handle type
Figure 28. Type of tool handles used and preferred by 79 B.C. General Surgeons who performed laparoscopic surgery.
Of note is the fact that about 18% of the surgeons complain that the tool handles were not
of an appropriate size for their hands. As all endoscopic tools are manufactured with one
standard handle size, no provisions are made for different hand sizes. Most surgeons are
able to adjust their grips on the 'scissors' handle by varying the number of fingers inserted
into one of the rings. However, hand grip on the 'palm' handle can not be adjusted as
easily. A smaller hand would not be able to wrap the fingers around the handle in order to
apply pressure on the handle. Conversely, a larger hand would have to squeeze the fingers
tight in a palmar grasp to apply sufficient pressure on the handle. Thus, for surgeons who
do not have a good grasp on the handle, their tasks can not be performed properly with
these tools.
Surgeons were asked to rank the laparoscopic tools they use, independent of the
tasks, for ease of use. The tools were graspers, scissors, and needle drivers/holders. A
ranking of (1) on a 3-point scale would mean that the tool is easy to use, whereas a ranking

9 4
of (3) would mean that the tool is difficult to use. Some surgeons ranked more than one
tool, such as the graspers and the scissors, as having the same degree of usability.
Surgeons who have had no experience with using the needle driversholders did not include
this tool in the ranking. Results show that most surgeons ranked the needle driversholders
as 'difficult' to use, while the graspers and scissors were considered approximately equally
easy to use (see Figure 29).
Tool Rating easy
medium
graspers scissors needle drivers
Figure 29. Rating of tool difficulty by 79 B.C. General Surgeons who perform laparoscopic surgery.
The problem, according to surgeons, with the needle driversholders seems to be
the lack of manipulability. Surgeons complain of difficulties in grasping the needle and
holding it in the desired position, taking appropriate bite size of tissues, holding the suture,
and keeping the jaws in the closed position with the drivers. 'The drivers have an
awkward sense of gravity'. The most limiting feature of the needle driversholders is
undoubtedly their poor grip on the needle. Other limiting features listed by the surgeons
included the 'handle design', 'lack of pivoting jaws', 'lack of flexibility of tip', 'lack of

9 5
accuracy' and 'angle of tying'. Interestingly enough, when asked what they considered to
be the best feature of the needle driverslholders they use, some surgeons responded by
naming the best feature of their ideal tool: 'easy to use', 'can hold needle on angle',
'secure tip', 'touch', and 'centre of gravity'. However, the fact that most surgeons left the
question unanswered indicated that they could not name one good feature of the tool.
Otherwise, responses were vague: 'palm grasp', 'feel', 'resemblance to open instrument',
'make MAS [minimal access surgery] feasible', 'or need re-inventing'.
Appropriately, suggestions for tool re-design, from surgeons themselves, tried to
eliminate the problem of securing the needle in grasp, and allowing the tool to rotate more
easily, with pivoting heads. Even automated devices for suturing were suggested. The
handle design also deserves attention. One surgeon suggested that the tools should have a
palm handle which makes a 300 to 45O with the shaft (see Figure 30).
Current instruments:
'good angle for your hand but poor tactile-tissue sensation'
'palm -- better tactile feel but poor angle for your hand unless the table is very low or you stand on a stool'
'What I wish they'd make -- forcep like handles at 300 - 450'
Figure 30. Actual design modifications suggested by a surgeon who responded to our questionnaire. Accompanying comments have been transcribed.

9 6
The graspers have similar problems as the needle driversholders. They do not hold
tissue well, especially if the tissue is thickened or inflamed. Graspers tend to slide off the
tissues, or they perforate the tissues. They are difficult 'to hold fixed for a prolonged
period', with their 'awkward release and grasp mechanism at [the] handles'. The small
jaws make grasping thick tissue difficult. Their lack of force feedback and poor tactile
sensation of the tissue in grasp are also on the list of most limiting features of the tool. The
ratchet mechanism which allows the graspers to be locked for holding pause was identified
as the best feature of the tool. Surgeons also indicated that the light-weight graspers
provided 'some tactile feel', and that the new ones allow for tissue to 'bunch up' and be
held secure. Most importantly, it was remarked that the best feature is the fact that 'they
make MAS feasible'.
Again, the question in search of the best feature of the present graspers resulted in a
list of desirable features for ideal graspers. The list includes rotating feature,
maneuverability and self-holding ability. Some surgeons were not able to name any good
features, while others suggested 'totally redesigning' or 're-inventing' the tool. Many
more specific suggestions were offered regarding a modified design of the graspers.
Surgeons want an improved grasping mechanism that does not damage tissue. For
example, make wider and more teeth on larger grasping surface to hold the tissue with
varying thickness. That means making longer jaws with more motion that have graded
response to pressure. To accommodate the different tissue types, different tissue graspers
with different weights should be available. They should all have rotating features. The
grasping end needs redesigning -- 'Don't use scissor type mechanisms'. Overall, they
should be sturdier, provide stronger grip, but atraumatic to tissue.
The problem with scissors is that they are often too dull to cut properly. Thus, they
require repeated cutting to separate the object, often sawing instead of cutting. Their sizes
are sometimes not appropriate for delicate dissections. As the scissors are not used as
manipulators, they do not have the same problems as with the needle driversholder and

9 7
graspers. Rather, the most limiting features reported by the surgeons are mainly those
concerning the sharpness of the blades for cutting. The scissors become dull too quickly
from wear and tear, as well as from use in cautery. Some surgeons complain of not being
able to see the tip when using the scissors; curved blades may help. Others indicated that
the scissors are good, particularly the disposable ones. One surgeon suggested that the
scissors be color-coded, such that they would not be used as graspers by mistake.
The best feature of the scissors for some surgeons is that the scissors work, and
have the same action as open instruments. The list of best features as provided by the
surgeons includes sharp, rotatable, curved thin blades that have size variations. These
features seem more likely to be desirable ones to include in a new design of the tool, rather
than existing ones which should be kept in the modified design. Surgeons stress
maneuverability as a best feature of the tool, as with the needle driverslholders, and the
graspers.
Specific suggestions were offered by the surgeons to improve the design of the
scissors. Other than the general push for better quality material for the blades, it was
suggested that the blades could be exchanged or replaced. To prevent tissue from slipping
while being cut, the blade may need to be finely serrated. Also, 'the blades could be 20%
longer', and stronger, with different angulation and improved degrees of freedom.
The constant changing of instruments for different tasks during surgery is a source
of nuisance. It sometimes requires a change of the trocar reducers to maintain an air-tight
seal for different tool diameters. The surgeons are forced to break their attention to change
instruments, which then requires re-orienting and re-calibrating with respect to the image
on the video monitor, each time they return to the task at hand. Most importantly, the break
in attention for changing tools during surgery creates the potential for the inadvertent use of
scissors for graspers or clamps. The result may be irreparable damage to tissues or organs.
One surgeon suggested that the tools may be color-coded to differentiate the scissors from
the other tools.

On attitude.
Surgeons were asked about how they feel when dealing with difficulties
encountered while performing laparoscopic surgery (see Figure 31). Given a choice of
'challenged', 'frustrated', 'tired', or 'angry', most surgeons responded feeling both
'challenged' and 'frustrated'. Some surgeons admitted to feeling 'tired' and 'angry', while
others reported feeling all of these emotions. Additions to the list were: 'satisfied when
difficulties are overcome', and 'exhilarated'. Some of the more candid comments were
'scared', 'slightly aggravated at incompetence', and 'very aggravated as often you can see
what you need to do but instrument doesn't go around corner!'.
Surgeons Feel ...
challenged frustrated angry tired other
Emotion
Figure 3 1. Reported emotions when dealing with difficulties in laparoscopic surgery, from 79 B.C. General Surgeons who responded to the survey questionnaire.
The feelings of being 'tired' are mostly experienced as muscular fatigue in the
hands, having to maintain pressure on tool handles for a long time. One surgeon in
particular developed carpal tunnel syndrome. He reported that after having had his carpal
tunnel syndrome repaired, he now tries 'not to flex [his] wrist as acutely' during surgery.

9 9
Others felt that new instruments are needed to explore the operative site, and that changing
strategies may help.
As far as errors were concerned, 45% of the surgeons reported that they only
'sometimes' made errors, while 39% claimed that they 'rarely' made errors (see Figure
32). Only 9% of the surgeons admitted to making errors 'often'. Obviously, most
surgeons do not consider the unsuccessful attempts at performing manipulative tasks in
laparoscopic surgery as errors. Rather, 'errors' to the surgeons would constitute gross
mistakes such as cutting the wrong artery, or removing the wrong organ, etc.
Surgeons' Perceived Error Frequency
often sometimes rarely
Frequency
Figure 32. Reported frequency of error while performing laparoscopic surgery, from 79 B.C. General Surgeons who responded to the survey questionnaire.
On general comments.
The expectation that three-dimensional vision systems will have a great impact on
the future of minimally invasive surgery, and make laparoscopic surgery more widely
practiced, is a common belief among the surgeons. 'I am certain a 3-D camera system will
eliminate most problems and also eliminate accidents'. Most surgeons are in support of the

100
idea of improving tool design to make their job of performing laparoscopic surgery easier.
For example, better cutting and coagulating instruments, such as laser, ultrasonic scalpels,
etc. can help. However, they do not believe that the amount of time spent in learning the
technique can be reduced. 'If anything, the time learning should be increased'. Most
surgeons feel that practice is the key to mastering the technique of performing laparoscopic
surgery. 'Much is dependent on an individual's own learning curve and aptitude' in
dealing with the new technology, such as orientation 'with the screen and hands, and
lighting, and how to expose the operative site; the rest of dissection, cut, etc. do not need to
learn, the feeling is the same as open surgery'. Therefore, it was suggested that surgeons
practice on inanimate models, animal models, or computer simulated models. 'Proper
introduction of instruments prior to performing surgery' is important. Surgeons should be
familiar with the tools and their functions, before having to use them in surgery. Also,
surgeons should be able to choose the endoscopic tools based on their preference, instead
of having 'non-surgeons choose the instruments that are purchased by the hospitals'.
Interview Res~onse
Informal discussions with surgeons at the laparoscopic workshops and follow-up
discussions from questionnaire responses were insightful and encouraging. Surgeons
appreciate the diffxulty of laparoscopic surgery and the importance of understanding the
perceived constraints of minimally invasive surgery from the surgeons' perspective. It was
the general agreement that laparoscopic surgery is more difficult than open surgery. The
source of the increased difficulty is the instrumentation involved. This includes the tools
which make minimally invasive surgery possible, and the vision system which makes
shared viewing of the remote operative site possible.
Laparoscopic workshops.
During practice at the laparoscopic workshops, surgeons were first introduced to
the special endoscopic tools, then practiced basic surgical skills such as dissecting,
suturing, and tying knots. Because the manipulators were simple and straight forward to

101
operate, only a few minutes were spent examining the various features of the tools. The
remaining time in the four-hour workshop was devoted to learning to perform the surgical
tasks, and practicing them.
It was noted that the endoscope had to be withdrawn and the lens cleaned
frequently. When the endoscope was re-inserted, it took some time for the surgeon to
position and focus the camera to the operative site. If the camera was positioned at a
different angle than it was previously, the operating surgeon had to spend more time re-
calibrating the tool position to the camera position.
It was also noted that surgeons were struggling with the tools to manipulate them
based on the video screen image. It appeared that the direction of movement seen on the
screen from the endoscopic camera perspective, was not always the same as the direction of
tool movement from the surgeon's point of view. Furthermore, the movement direction of
the hand holding the tool was always opposite to the direction of the tool due to the lever
system created by the port of entry. Therefore, the visuomotor transformations needed to
manipulate the tools to the desired position are at these two levels. Surgeons seemed to
have no trouble with the reversal of directions at the hand-tool level, but a great deal of
trouble matching the direction of the movements of their tools with that seen on the video
monitor.
When questioned about the apparent struggle with the altered viewing perspective,
one surgeon responded that he did not think about moving to the left or right, but watched
how the gripper moved on the screen as he moved it about in the operative site. As the
viewing perspective depends on the camera position, surgeons must learn to work with the
camera before learning to perform the actual procedure. Therefore, surgeons first assist in
surgeries by holding the camera, then they graduate to be assisting surgeons to hold the
tools which keep the tissues from obstructing the camera view. Then, once they are
familiar with the instrumentation, the are allowed to perform the surgery themselves,
provided that they are competent with the technique.

102
Another surgeon who appeared to have a great deal of difficulty manipulating the
tools was acutely aware of the changed viewing perspective, and talked himself through the
task. He worked with the endoscope pointed toward him, giving a mirror image of his
actions such that moving the tool to the left is seen as a rightward movement on the video
screen. 'Something about this camera, ..., it's reversed.' 'It's your brain, ..., your brain
doesn't allow you to move your arm anywhere else,...'. The surgeon did not realize that
the problem could be solved by repositioning the endoscope to point in the same direction
as his point of view. In subsequent discussion, the ES products representative from
Ethicon (Mr. Matt Hanley) used the analogy of the baseball diamond to describe the
preferred positions for the endoscope and the working tools. The endoscopic camera is at
the home position, the port for the right hand tool is at first base, the left at third base, the
task is performed at second base, while the surgeon looks out to centre field, 'not working
against the brain now'.
Surgeons spent the majority of time in the workshop practicing suturing and tying
knots. According to Dr. Nagy, the teaching surgeon conducting the workshop, the time
taken for surgeons to learn to tie knots depends on the individual. Some surgeons seem to
have an easier time adjusting to performing surgical tasks laparoscopically. It was
suggested that surgeons having experience with playing video games (the Nintendo
Generation) seemed to do better. They seemed better able to 'find themselves on the
screen'. Other surgeons seemed to have a great deal of difficulty just getting the tools into
the field of view. One of the many strategies used to get the tool into the field of view
quickly is to slide the tool down the shaft of one that is already in view, until both tools are
seen on the screen. This is a useful strategy especially for suturing. The needle is passed
from the needle driver to the needle holder during suturing, when the wrist is no longer
able to twist and rotate past the point of maximal range of motion.
For simple procedures such as gall bladder removal or hernia repair, the time of the
operations are similar to open techniques (one to one and one-half hours). For procedures

103
such as bowel resection which requires suturing, the procedures can last up to two or three
times as long as open technique.
Follow-up interviews.
In addition to feedback similar to those obtained from the questionnaire survey
regarding the tools and tasks in laparoscopic surgery, follow-up interviews with surgeons
yielded insight into how the surgeons use their tools, and how tools can be modified to
meet the needs of different surgical tasks.
Because of the long procedures, and the scheduling of surgeries by hospital,
surgeons spend hours standing in the operating room, performing one procedure after
another. 'We are working a lot of the time like this --- elbows up, wrist and hands
supinated'. This posture results from holding the instruments 'the classical way --- not a
good way of holding, not ergonomically desirable'. Some surgeons complain of digital
nerve palsy, which is a numbness where instrument presses on the lateral edge of the
thumb, proximal to the DIP joint. Surgeons are also prone to developing carpal tunnel
syndrome, as reported by a surgeon whose left (non-dominant) hand was constantly flexed
acutely while performing surgery.
With respect to the design of the instruments, modification at both ends of the
instruments are needed. 'The actual design of instrument handles still leaves a lot to be
desired.' New instruments with palm handles are not the solution to the problems
mentioned above. The posture of elevated elbows still exists, if not worsened. One
surgeon suggested that an angled handle would be desirable, as it would allow the elbows
to be lowered, with the hands and wrists maintained in the neutral position while operating
the tool.
Some tool handles have a ratchet mechanism. Different companies have different
mechanisms and some are more easy to use than others. The simple ones wear out quickly
and do not hold. When holding the body of the gall bladder with graspers, the hand must

104
be squeezing to keep the grip on it. Disposable ones are good, as they do not have a
chance to wear out.
End-effector design depends on the tool's intended function. The challenge for
designing graspers is to design an end-effector that will grasp something like the gall
bladder securely and pull on it without putting a hole in it. When grasping something that
is to be removed, it does not matter whether it is damaged by the graspers, unless
contamination from spilled contents is a concern. For example, spilling bowel contents is a
contamination concern. The rotating shaft on the graspers is a good feature. However, it
may be problematic if the graspers rotate when it is not desirable.
For scissors, the end-effector mechanism is 'fragile'. Straight scissors are not very
useful, but the curved ones are good. The curved tips on the scissors make their use easier
in procedures such as hernia repair or Fundoplication, which require more dissections. A
desirable feature on the scissors is a rotatable shaft. The earlier designs of scissors do not
have a rotating wheel built in, as for the graspers. The new design of scissors allow the
shaft to be rotated along its long axis. They are, however, not re-usable. Disposable
surgical instruments are not environmentally sound, as they can not be recycled.
Therefore, designing good reusable instruments that can be cleaned easily is a challenge.
Needle drivers are very difficult to use. With a straight shaft, the end-effector is not
seen by the endoscope's point of view ('For effective view, the endoscope must be coming
from the same direction as you are. If opposite, can't work. Therefore, with the
endoscope from behind the straight instruments, can't see tip when working in the same
angle'). A curved end would help. Storz has developed a curved instrument which is
good for reaching back and grasping. However, curved tips create a problem for tool
insertion through the cannulae. A flexible trocar for curved instruments has also been
designed by Storz. It has a coiled body which breaks the seal by leaking gas from the
insufflated abdomen.

105
Another design, by Surgical Innovations, is a curved shaft which can be
straightened before insertion, so that it can go through a straight cannulae. The shaft is
segmented with a cable inside that can be tightened to create a curve in the shaft. There are
standard curves into which the shaft can be bent: 75 degrees, 45 degrees, etc. The handle
of the tool also allows the hand to operate with the palm facing downward.
Although this particular instrument is not yet available in Canada, it is expected that
it will help with handling the needle in suturing tasks. The interface between the needle and
the tool is an important aspect for design modification. The ski needle (with a curved tip) is
difficult to hold and maintained in one orientation. One solution may be to flatten the shaft
of the needle so that it does not rotate in grasp. Alternatively, automated suturing devices
can be used, and are appearing on the market (e.g. autostitchs, staplers, etc.).

DISCUSSION
Trian~ular Strate~v
Based on our triangular strategy, the task analysis of laparoscopic surgery yielded
results on the task, the tool and the user. The results, when interpreted separately, give us
focused but limited information about the overall picture. The interaction between the
human and the tool, in the context of the task, is the crucial element which links these three
parts into one meaningful whole. Therefore, in our interpretation of the results, we need to
take a human-centred approach to surgical performance. Starting with surgeons' feedback
regarding the tasks and tools, we can find support for their claims and evaluation in our
systematic analysis of surgical tasks and endoscopic tools in the appropriate context.
For example, user feedback from the questionnaire survey indicated that the tools
are a major limitation to surgeons' performance of laparoscopic procedures. Another
limitation to surgeons' performance includes the degraded depth perception with a two-
dimensional video display of the operative site. According to the surgeons, the tools make
the tasks of laparoscopic suturing and tying knots so difficult that some surgeons avoid
these tasks by using clips or staples whenever possible. Most surgeons do not perform
laparoscopic procedures which require suturing at all. This implies that surgeons would be
able to perform their tasks better, if the tools were designed to be easier to use. In fact,
surgeons' responses to our questionnaire reflect this belief: Presently, the tools are too
long and rigid; the right angle between the shaft and the handle is too much; tools can not
go around corners, they can not flip and orient freely for more complex manipulations such
as in suturing. Most surgeons agree that graspers and scissors are relatively easy to use,
but needle driversholders are difficult to use. It seems that graspers and scissors allow
surgeons to perform their tasks of positioning and cutting well, whereas the needle
driversholders make the tasks of suturing and tying knots more difficult.
Our systematic task analysis reveals that while it is true that the design of the needle
drivers/holders create difficulties for surgeons' performance of suturing and tying knots,

107 the relative usability of the tools is a reflection of the task difficulty, per se. Suturing and
tying knots are more difficult than dissecting and cutting tasks because there are more task
constraints that impose greater demands on the surgeons. Therefore, improvement in the
surgeons' performance will result only from understanding the task requirements and
constraints that affect performance.
Constraints
In our attempt to iden* the task constraints which affect performance in remote
manipulation, we assume that constraints exist if task demands are not met as easily as in
an unconstrained, 'ideal' situation. That is, when a task requirement needs to be met by
additional information processing by the performer, or when a performance decrement
results from a task that is more difficult. In laparoscopic surgery, for example, constraints
are perceived by the surgeon when the task at hand requires the coordination of movements
of many degrees of freedom by the tools, which can be accomplished only by the
coordination of many single degree-of-freedom movements. This forces the surgeons to
slow down, and perform more single-dimensional movements with the tools, which they
could otherwise do with their hands faster, with fewer movements, and in parallel.
There are four major types of constraints that affect surgeons' performance of
laparoscopic surgery: physical, precision, safety, and visuomotor constraints. Precision
and safety constraints are determined by the task requirements. The instrumentation for
minimally invasive surgery (i.e., endoscopic viewing perspective of the operative site as a
two-dimensional image, and long, rigid tools) impose mainly physical and visuomotor
constraints on the surgeon's performance. The degree to which these constraints affect
performance is task-specific. Our discussion of the effects of constraints on performance
will focus mainly on those related to the physical, precision, and safety constraints.
Visuomotor constraints, although equally important, were not a focus of the task analysis
in this research. Visuomotor constraints will be dealt with briefly in the section on 'Other
Issues'.

1 0 8 Phvsical Constraints
In laparoscopy, physical constraints are constant, and stem from the very nature of
minimally invasive surgery (or minimal access surgery). Its minimal invasiveness restricts
the surgeon's access to the surgical field. Surgical tools can reach the operative site
through trocars, but with reduced degrees of freedom for subsequent maneuvers. Physical
constraints are due to the single, small port of entry for each tool, and the crude design of
the tool itself. In order for the tool to reach the operative site within the abdominal cavity, it
has a long shaft which extends the reach of the effector from the hand. The very nature of
minimal invasiveness dictates the small opening for tool insertion, and hence the reduced
degrees of freedom of the tool.
In general, endoscopic manipulators have been designed to resemble their
counterparts in open surgery. The end-effectors of graspers, scissors, and needle
driversholders have one function: open and close to grasp, for graspers and needle
driverslholders, or open and close to cut, for scissors. This function can be identified as an
elemental prehension movement, grasping. Forces are applied, in opposition, by the jaws
of the tool end-effectors to the target object. The scissors end-effectors, with their sharp
edges, shear the object with their closing motion. The gripping jaws of the graspers and
needle driversholders, on the other hand, afford only one type of fixed contact with the
object in grasp. The tool maintains a static gripping posture with constant contact points on
the object. Motion can be imparted to the object by translation/rotation movements of the
entire tool, or by releasing grasp and relocating the tool's contact points on the object,
much like turning the steering wheel of a large truck by repositioning the hands with each
one-quarter turn of the wheel. Thus, according to the four classified forms of contacts in
performatory hand movements (MacKenzie and Iberall, 1994, p. 269), these endoscopic
manipulators are able to perform only one type of manipulative movements: repositioning
or regrasping.
109
A few regrasping movements are usually sufficient for positioning tasks using
graspers, in laparoscopic surgery. When the task demands that the object be manipulated
using movements other than regrasping, such as involving sliding and rolling contacts,
surgeons perceive more difficulties. For example, the ski needle, used in suturing, can not
be rotated into the desired orientation by rolling the needle on its side between the jaws of
the needle holders. The surgeon must perform many incremental regrasping movements to
achieve the desired orientation of the needle. This process is more time consuming and
requires that the surgeon perform a series of additional motions to reach the task goal.
These additional motions are discrete, single or two degree-of-freedom motions that are
restricted by the tool's reduced degrees of freedom. These motions, in combination,
achieve the same result as a movement made with all six degrees of freedom, under what
we call the 'ideal' situation. Therefore, the more complex the manipulative movements that
are required in a task, the more additional motions, each with limited degrees of freedom
are performed to overcome the physical constraints, and thus, the more difficult the task.
This becomes obvious when suturing or tying knots are compared with cutting
tasks. Given the same degrees of freedom in tool manipulability, the task which requires
the greater number of subtasks and motions is perceived by the surgeons as more difficult.
Therefore, suturing and tying knots and more difficult than cutting tasks, while dissecting
is more difficult than cutting suture. However, other constraints also contribute to the
overall perception of task difficulty. Safety requirements and precision constraints are
often defined by task requirements and task goals.
Safetv Constraints
Safety constraints in laparoscopic surgery vary with task requirements. For
example, over and above the basic safety concerns inherent in performing laparoscopic
surgery, the task of dissecting tissue imposes a greater safety constraint than the task of
cutting suture, even though these two surgical tasks are similar in subtasks. They both
have two subtasks: 1) pull object taut, and 2) snip object. The object (tissue or suture) to

110
be divided in each task determines the degree of difficulty. Looking at the number of
motions in each subtask of snipping (see Figure 33), the greater number of motions in
snipping tissue over snipping suture may reflect a greater safety constraint perceived by the
surgeons. In snipping tissue, the location and size of the cut needs to be controlled. As
well, the risk of snipping the wrong tissue or surrounding tissues and arteries is a major
safety concern. Because of these safety constraints, snipping tissue is more difficult than
snipping suture.
In contrast, the motions in the subtasks of 'pulling taut the suture' and 'pulling taut
the tissue' indicate that it is more difficult to grasp suture. There are more motions
performed in pulling taut the suture than in pulling taut the tissue (see Figure 33). This can
be explained by examining the precision requirements in the subtasks.
(a) pull taut suture
reach & grasp push pull release orient & hold
motion
(c) pull taut tissue
reach & grasp push pull release orient & hold
motion
(b) snip suture
rcach & grasp & push pull release orlent hold
motion
(d) snip tissue
reach & 'grasp & ' push ' pull ' release ' orient hold
motion
Figure 33. Contrasting the motions involved in the tasks cutting suture and dissecting tissue.

11 1
Precision Constraints
In the subtasks of grasping tissue or suture to pull taut, for the purpose of dividing,
the same basic safety constraints underline both subtasks. However, grasping suture
seems to be more difficult than grasping tissue. In this case, the object to be grasped is
both a physical constraint and a precision constraint. As the suture is smaller and requires
greater precision to grasp with the tool, more motions are performed by the surgeons (see
Figure 33). Tissue or organ, on the other hand, is larger in surface area, such that the same
degree of precision to grasp is not required. As well, the orientation of the jaws need not
be in-line with the direction of the object, as for a piece of suture. There appears to be
more 'release' motions in grasping for suture, which may suggest that the suture is difficult
to hold in stable grasp. Also, if the suture is long, it may require regrasping to adjust the
length of the suture to be pulled.
These additional precision constraints add to the perceived difficulty of the surgical
tasks. In suturing, the precision required to place stitches in the tissue, to take an
appropriate bite size of the tissue by the needle, and to line up the second stitch with the
first stitch, increases the level of difficulty of the task. These precision constraints become
more significant as they can also be perceived as safety constraints in the task of
approximating tissue. For tying knots, precision is required to handle and manipulate
suture which is thin and slippery. Again, the physical constraints presented by the size of
the suture also increase the precision constraints for tying knots.

112
Effects on Performance
Surgeons' performance in laparoscopic surgery is affected by the combination of
physical constraints, safety constraints, precision constraints and visuomotor constraints,
each contributing in various amounts. The effects of these constraints can be seen in the
surgeons' motor performance.
Serial Order of Motions
The surgeons' movements with the endoscopic tools were reduced to five elemental
manipulation motions:
1. reach & orient,
2. grasp & hold,
3. push,
4. pull, and
5. release.
These motions, in various combinations, are observable in natural human prehension and
direct manipulation. Reaching and grasping (preshaping and enclosing, prior to contact)
are typically performed in parallel when humans perform goal-directed prehension
movements (Jeannerod, 1984), and are characterized by a transport component of the
wrist, and a grasp component of the hand. The hand typically opens during the transport
of the hand in space towards the object to be grasped, and closes around the object at the
end-point of the transport trajectory. These same movement components are observed in
laparoscopic surgery, but in series. The jaws are closed while the tool is being transported.
At the endpoint of the transport trajectory, the jaws open to grasp (see Figure 34).
However, motion analysis of tasks and tools revealed performance characteristics that can
be likened to simple robotic single-jointed movements. Simple robotic movements are
sometimes seen to be a sequential series of uni-directional motions that lack the appearance
of smooth coordination between multi-joints.

113
In laparoscopic surgery, the surgeons' movements appeared to be carried out in
slow motion. It also appeared that motions are controlled one at a time. For example,
reaching and grasping of a piece of suture is seen as a series of motions with limited
degrees of freedom: transport graspers toward suture; orient end-effector; open end-
effector; then close end-effector. The components of transport and grasp are performed
separately and in sequential order (see Figure 34). This is similar to the motor behavior of
patients who suffer brain injury (Ada, Canning, Cam, Kilbreath, and Shephard, 1994).
Ada and colleagues reported that a patient, after a head injury which resulted in upper limb
dysfunction, showed a complete dissociation of the reach and grasp components. When
reaching for an object, the transport phase was completed before the patient opened his
hand. Also, the overall movement time is at least three times that of normal (Ada et al.,
1994).
It is interesting to see the parallel in these two scenarios. It may be that surgeons
are forced to slow down and perform the motions in sequential order due to various
constraints. The slow motion in task performance may be a result of uncertainty in position
and orientation within the abdominal cavity. Motions that are performed one at a time may
be one way to minimize the many constraint variables for maneuvering in the operative field
by reducing the degrees of freedom. Therefore, it suggests that constraints in laparoscopic
surgery impose additional information processing demands on the surgeons, such that
motions that are normally executed in parallel in natural prehension must now be planned
and executed in serial order.

'Natural ' Prehension (After Jeannerod, 1984)
'Remote' Prehension
Figure 34. Comparison of reaching and grasping in natural prehension and prehension with a tool in laparoscopic remote manipulation. The parallel ordering of the transport and hand formation components were described by Jeannerod (1984). The same components of reaching and grasping are also seen in laparoscopic remote manipulation. However, the two components are performed in serial order.

Epistemic vs. Pra~matic Motions
From the previous discussion, it is reasonable to expect a skilled surgeon to
perform surgical tasks with fewer movements and in a shorter time than unskilled
surgeons. Our results from timeline and motion analyses support this expectation. In
addition to the many regrasping motions made to accommodate complex manipulations in
surgical tasks, novice surgeons performed more repetitions of the same motions than the
expert surgeon. These motions included repetitions of unsuccessful attempts at the
intended movements, as well as some probing, exploratory-type motions. The exploratory
motions did not bring the tool physically any closer to the target. Instead, they appeared to
be 'extra' movements that resulted in a longer task performance time. However, they were
not errors in the manner that an error would be made as a result of, for example,
misjudging the location of a target.
In fact, expert surgeons also make these exploratory movements during surgery,
sometimes by design (Dr. Laurence Turner, personal communication, April 21,1995).
Surgeons sometimes make small movements with their tools to verify their position and
orientation within the surgical field. It seems that by seeing the movement on the video
screen, surgeons obtain cues to enhance spatial and depth perception, to obtain orientation
information and to re-calibrate the visuomotor mapping between the image and the hand.
These movements are similar to movements reported by Kirsh and Maglio (1994) as
'epistemic' actions. In their report, epistemic actions were made by players in a real-time,
interactive video game, to 'reduce the space, time, or unreliability of the computations'
occurring in cognition. Unlike 'pragmatic' actions which bring one physically closer to a
goal, such as the regrasping to orient the needle in suturing, 'epistemic' actions, like the
probing motions made by the surgeons, help to uncover information to solve cognitive and
perceptual problems more quickly than by mental computations alone. This is especially
important for surgeons to re-orient after breaking their attention from the video monitor to

116 change instruments. This, in effect, serves to save time and effort, as well as reduce
errors, in the long run.
Implications for Training
At present, the training of surgeons for laparoscopic surgery does not follow a
standardized program. The most common course of action for these surgeons is
participation in workshops and practicing with animal or inanimate models. Their progress
in learning and acquiring the proficiency necessary to perform surgery on human patients
depends on the quality of instruction, the amount of practice, experience in open surgery,
as well as the surgeons' ability to learn and perform.
Our timeline and motion analysis results showed great within-subject variability.
The expert surgeon's performance varied with patients, with procedures, with tasks and
with trials of the same task. These within-subject variability are larger for novice surgeons,
implying that with practice, surgeons may become more consistent and thus more proficient
at performing surgical tasks. As observed in the laparoscopic workshops, novice surgeons
learned to perform laparoscopic tasks at different rates. Some seemed to have better hand-
eye coordination in performing remote manipulation based on a displaced two-dimensional
image, suggesting experience with playing video games.
To learn the laparoscopic surgical tasks that have significantly different constraints
from those performed in open techniques, surgeons can take advantage of the ordered
series of sequential motions for each subtask, as delineated in our task decomposition, and
use it as a guide for practice in training. This can be implemented in training programs for
surgeons to learn new laparoscopic skills. A similar strategy has been suggested by Szabo
and colleagues (Szabo, Hunter, Berci, Sackier, and Cuschieri, 1994). Surgeons can learn
to suture by following a 'choreographed sequence of repetitious steps and by memorizing
them'. This notion of a choreographed sequence of repetitious steps organized in 'nodes'
is based on the principle of 'economy of motion' to eliminate extraneous motions and
shorten operating time.

1 1 7 If all surgical situations were identical or predictable, surgeons would be able to
follow pre-choreographed routines to perform laparoscopic procedures, and new surgeons
can be trained to perform surgery by rote practice of these routines. In fact, a robot or a
computer could be programmed to carry out the operation once the instruments are placed at
the appropriate start position. In reality, this is not yet possible because of individual
differences in patients' internal anatomy. Furthermore, each case recommended for
surgery has its own unique set of characteristics. Therefore, the implementation of a
standardized routine to learning and training in surgical tasks should include such
considerations.
-- As suggested by surgeons responses to the questionnaire, practice is the only way
to master laparoscopic skills. This can be done by practicing on an inanimate model,
animal model, or computer simulated models. The inanimate model only allows the
surgeon to practice under one set of conditions. It does not provide variations similar to
those which the surgeon must face in reality, when operating on a real patient. The animal
model is realistic, but expensive. Many cases with different 'conditions' are needed to
allow the surgeon to become proficient. Computer generated models may be the ideal
training vehicle. Computer programs can simulate various conditions under which the
surgeon must alter the choreographed routine for surgical task performance to suit the
specific task requirements. Virtual laboratories could be developed. These could train the
surgeons to respond to real life conditions that an inanimate model, or an animal model
could not.
Reauirements for Tool Desicrn
Considerable work has been done to develop guidelines for the ergonomic design
of hand tools for industrial use. Studies on power grip, the effect of handle size and design
on grip strength, and on exerted forces have been conducted for this purpose.
The ideal state for a hand tool, according to the Man-Machine System design
philosophy (Greenberg & Chaffin, 1977), is the following:

1 1 8
The hand tool is light, easy to hold and grasp, requires minimal force of
actuation, simple to operate, reliable, provides minimal risk to the operator
and has a low cost. It can be used for many repeated applications with no
undue stress to any of its parts and with minimal need for adjustment,
maintenance or replacement.
In general, tool design can be divided into three categories: general principles,
grips, and tool geometry (Konz, 1974). The general principles in designing hand tools
suggests the use of specialized tools that save time; and that dual-function or multiple-
function tools that do not require switching tools are more efficient. Two grip types that
are common in industrial applications are the power grip and the precision grip. For power
grips, force should be applied along the axis of the forearm, with a grip diameter of 1.5
inches. The precision grip requires accurate control. The grip diameter should be at least
0.25 inches. Provided that a grip gives enough contact area to the hand, precise shape of
the handle is not important. The handle should have a compressible surface with high
coefficient of friction. As for tool geometry, the tool should bend instead of the wrist, to
avoid tenosynovitis.
Endoscopic surgery has its unique set of requirements and constraints that must be
taken into consideration when following the general guidelines for tool design.
Modifications to the present design of laparoscopic manipulators can be made based on
results from the task analysis. In designing tools for laparoscopic surgery, one must
consider using the tool as an extension of the hand. One of the most important
considerations is that the motion of the hand on the tool handle should reflect the motion of
the end-effector. The handle shape should be consistent with the function of the tool. That
is, closing or opening of the handle with the fingers should bring about the same actions in
the end-effector jaws. When this control-actuator relationship is natural and
straightforward, the surgeon can direct attention to performing the task, and not at the
operation of the tool.

119
The fact that all manipulators have the same basic design allows for tool evaluation
based on how well the tools meet the task requirements. This can be inferred by the
number of movements made with the tools. The greater the number of movements, the
more complex is the task, and the greater the need for improvement to the tool.
'The key requirements of any remote surgical manipulation or telemanipulation are
safety, responsiveness to the surgeon's desires, dexterity, and precision in executing the
tasks.' (Rininsland, 1993). Based on surgeons' feedback, the tools can be improved many
ways. With respect to the end-effectors of endoscopic manipulators, design modifications
should be specific for the tool's function for each task. A task which requires more
complex manipulations should have a tool equipped with a more functional end-effector.
For example, the needle driverslholders used in suturing and tying knots should be
modified to offer a similar increase in degrees of freedom, or the potential for differing
types of contacts (e.g., rolling and sliding contacts), such that regrasping movements are
minimized. This means that each tool would have its own unique features, rather than the
uniform structure seen in the current generation of laparoscopic tools.
We do not suggest that a fully automated device, which is capable of performing
one or all of the basic surgical tasks with the push of one button, would be the solution.
Basic surgical tasks are not always rigidly duplicated from one patient to the next.
Differences in patients' conditions, tissue properties, surgeons; approaches, and numerous
other factors, as discussed in this study, dictate the performance of one surgical task. One
single fully automated device can not appropriately accommodate all possible conditions
affecting the execution of a task (for example, the stapler can not replace sutures in
Fundoplication or Bowel Resection). Therefore, modifications to existing tools should
target specific aspects of the tools to more easily meet the task requirements.
With respect to handle design, we agree that in general, the angle that the tool
handle makes with the shaft, whether of the scissors handle type or the palm handle type,
should take into account the position of the tool in use, and the posture of the hand

120
operating it. At present, the right angle between the handle and the shaft of common
scissors handle manipulators forces the surgeons to adopt awkward postures, especially
when rotating the tool to orient the needle in suturing. This awkward posture is intensified
under the stress of surgery, and is a contributing factor to carpal tunnel syndrome. The
phenomenon of 'white knuckle' grip resulting from the stress of physical and mental
tension has been documented in the ergonomics literature. The hand exerts an excessive
grip force on the handle over that required for normal operation of the tool. When this
excessive grip force is maintained for a long period of time, the muscles and ligaments in
the hands are held in the stretched position.
These postural problems can be alleviated by lowering the height of the working
surface, thereby reducing the elevation of the elbows and shoulders. The surgeon should
be working in a more neutral posture. A 'reference position' is described by ergonomists
as one in which the upper arms hang down, elbows at right angles, forearms horizontal and
extended forward, with the wrists straight. From this 'reference position', movements
required to perform the tasks should be within a small work volume. Within this 'preferred
manipulation space', fast, accurate movements can be made comfortably without putting
undue stress on the body. The upper arms should be kept in its vertical plane most of the
time.
Adaptive strategies are seen with some skilled surgeons who stabilize the hand by
using the port of entry as a fulcrum for the tool in a lever system arrangement. Thus, the
posture is more relaxed. Also, instead of hyper-flexing the wrist to rotate the tool about its
long axis, the fingers release their scissors-type grip on the handle by changing the grip
posture on the handle to rotate the tool. The tool is then held without using the rings
putting less stress on the wrist. However, these adaptations are not common. It may take
a long time before surgeons learn to handle the tool differently from that function that is
suggested by its form. This indicates a need for modifying the tool handle, based on the
adaptive postures adopted. A handle with a uniform shape which has no particular

1 2 1
orientation implied or indicated may be desirable. It would allow the hand to change its
grip on the handle easily such that the wrist remains neutral while operating the tool.
The size and shape of the handles can be modified to accommodate different hand
sizes and shape preference. In general, the handle should fit the contours of the hand.
With the tool held securely in a suitable wrist and arm posture, it should be operated
comfortably utilizing the surgeon's natural strength and energy capabilities without
overloading the body.
Other issues in endoscopic tool design concern the material used in making the parts
of the tools, maintenance, re-usability, and cost. Present endoscopic manipulators have
metallic end-effectors which sometimes produce a glare in the visual field, from the light
source in the endoscope. This may be a nuisance when the surgeon is performing a
delicate task which requires continuous visual tracking. Glare can be reduce by using non-
reflective material for the tool shaft and end-effectors. This material must also be strong,
durable and light-weight. For reusable tools, the material must be autoclavable which
allows for appropriate cleaning and sterilization of the tools. Costs of material and
manufacturing must be weighted against the cost of maintenance. Disposable tools do not
have maintenance costs. However, they must be disposed appropriately, as they can not be
recycled.

1 2 2
Visuomotor Constraints
Although issues related to visuomotor constraints were not examined in this study,
they are important for understanding the overall effect of increased information processing
demands on the surgeons' performance. The new technology places the surgeon in
unfamiliar surroundings, with constantly changing relations between the surgeon's visual
field and the operative field. Restricted field of view afforded by the endoscopic camera
forces surgeons to rely on their memory and knowledge of the abdominal anatomy to orient
themselves. The camera's changing point of view, magnification of the image on the
monitor with movement of the endoscope, and altered spatial relationship between display
space and operative space, also require the surgeon to mentally orient and re-calibrate the
operative field.
Mapping between visual and motor directions of movement is fast and accurate
under normal circumstances (Poulton, 1956). When abnormal circumstances are
introduced, which changes the correspondence between visually perceived and motorically
specified positions in space, accuracy of visually guided hand movements is decreased.
This is true especially when the endoscope is at an angle with respect to the surgeon's point
of view, resulting in a rotated visual map of the operative field The longer time taken to
perform surgical tasks laparoscopically can be indicative of the increased difficulty in
visuomotor transformations to match the visual feedback with the motor map during hand
movements. Effects of unfamiliarity show up in comparisons between an expert surgeon
and novice surgeons. More motions are made when the surgeon is unsure of the situation.
This can also explain the greater number of epistemic motions discussed earlier.
Cunningham and Welch (1994) showed that a rotated visual-motor mapping can be
learned over time. They suggest that this learning is not entirely conscious. When subjects
were asked about their strategy to map visual movements directions to the hand, subjects
mostly had no idea. Some did specify the opposite direction and rotation. They mostly
reported behavioral strategies like making rotational movements, arcs, etc. Therefore, the

1 2 3
researchers concluded that it was not a mental strategy. The strategy seems similar to the
strategy surgeons and video games use by making epistemic motions.

124
Future Research
Several questions arise from this exploratory study of laparoscopic surgery. Issues
related to visuomotor constraints within the minimally invasive surgical environment need
to be examined more thoroughly. As technology is rapidly advancing to provide surgeons
with three-dimensional vision systems for performing laparoscopic surgery, studies are
now being conducted to evaluate the cost and benefit of two versus three-dimensional
visual feedback (Pietrabissa, Scarcello, Carobbi, and Mosca, 1994, Crosthwaite, Chung,
Dunkley, Shimi, and Cuschieri, 1995). Preliminary results suggest that 3-D is not better
than 2-D for many surgeons in tying knots laparoscopically (Crosthwaite et al., 1994).
However, our user response analysis seems to indicate that surgeons would prefer using
3-D systems to perform laparoscopic surgery. 3-D systems may reduce the degree of task
difficulty perceived by the surgeon, by reducing 'past-point' effects, and 'false grabs'
which are attributed to the reduced depth perception in 2D systems.
A question which concerns the nature of additional movements and need for
epistemic motions can be explored in future studies. If constraints which result in the need
for these motions can be identified and resolved, perhaps it would be possible to establish
an optimal number of motions used for each task. If these constraints result from
visuomotor transformations, our hypothesis that epistemic motions enhance the surgeons'
spatial orientation and depth perception can be tested.
At present, surgeons are not evaluated by standardized means for their competence
at performing laparoscopic surgery. The only means of training and evaluating
laparoscopic skills is subjective acceptance by their peers. An extension of our timeline and
motion analysis may be used to establish a basis for training and evaluation of surgeons'
laparoscopic skills, and the difficulties of specific operations.

APPENDIX I. Questionnaire

Sample Cover Letter
March 29, 1995
Dear Dr.
I am a graduate student in the School of Kinesiology at Simon Fraser University, Burnaby, B.C., working under the supervision of Drs. C. MacKenzie, S. Payandeh, and R. Marteniuk in the Faculty of Applied Science to study endoscopic manipulators. This project is sponsored by the Institute for Robotics and Intelligent Systems (IRIS), a Federal Network of Centres of Excellence. We are conducting an analysis of the instruments currently in use for laparoscopy. Specifically, we will evaluate the manipulators for their effectiveness and where necessary, recommend changes in design. We feel that you, as an end-user of these instruments, have invaluable input for this endeavor. The results will ultimately benefit present and future surgeons in performing endoscopic surgery.
The success of this project depends heavily upon your responses to reflect your views and opinions of the instruments you use in surgery. We would appreciate your help and need 10- 15 minutes of your time to complete the enclosed survey form. Most of the questions can be answered with a check mark or a brief phrase of two or three words. This questionnaire is designed to gather information regarding the effectiveness of the instruments used in laparoscopy. This questionnaire is a supplement to other research tools in this project, including a task analysis of laparoscopic surgery. Completion of the questionnaire is entirely voluntary. You may choose to answer all or parts of the questionnaire. Please return the completed form in the enclosed reply envelope. Please be assured that anonymity is ensured. There are no identification marks on the survey and envelope. Therefore, we request that you also fill out and return the enclosed postcard, separately, to tell us that you have completed the survey and do not need a reminder.
If you have concerns about this survey, you may contact my supervisor, Dr. Christine MacKenzie, or Dr. Andy Hoffer, Director of Kinesiology at Simon Fraser University (604- 291-3141). Copies of the results of this study may be obtained by contacting Dr. C. MacKenzie, Kinesiology, S.F.U., or Dr. S. Payandeh, Engineering Sciences, S.F.U.
Your prompt cooperation and participation in this important survey is appreciated. Please complete the questionnaire today and return it me in the return envelope provided. Thank you for your time.
Sincerely,
Caroline Cao Graduate Student, Kinesiology Simon Fraser University

Sample Reply Card
Dear Researcher:
I am sending this postcard at the same time that I am putting my completed questionnaire in
the mail. Since my questionnaire is completely anonymous, this postcard will tell you that
you need not send me a further reminder to participate in your study.
Dr.
(please print clearly)

Section I. General Information.
1. Age M- F-
2. How long have you been a surgeon? years.
3. How long have you been performing endoscopic surgery? years.
4. How often do you perform surgery? /month
5. If you are also involved in teaching or research, how often do you perform such
surgeries? /month
6. In general, would your first choice be endoscopic surgery, unless open surgery is more
appropriate? Yes No-
7. Please check the appropriate box(es).
You are presently practicing
both open surgery and endoscopic surgery
open surgery only
endoscopic surgery only
8. What are your most frequently performed laparoscopic procedures?
9. Are there certain procedures for which you prefer the open technique, and others for
which you prefer to use the minimally invasive technique (endoscopic)? Please list below.
Prefer Prefer
Open Surgery Endoscopic Surgery

Section 11. Endoscopic Manipulators.
10. What is the most common type of handle on the endoscopic manipulators (not staplers)
you use?
scissors handle - palm handle other
11. If you use different types, which do you prefer most?
scissors handle palm handle other
12. Are the handles an appropriate size for your hands?
Yes No
13. Do you have a feel of the tissues being manipulated through the instruments? How
would you describe the feel?
14. What do you think is the most limiting feature of the following endoscopic
manipulators?
a. graspers
b. needle drivers
c. scissors
15. What do you think is the best feature of the following endoscopic manipulators?
a. graspers
b. needle drivers
c. scissors
16. Please rank the following instruments in order of their difficulty to operateluse (from 1
for easy to 3 for difficult).
graspers
needle drivers
scissors

Section 111. Manipulators and Tasks.
17. Please rank the following tasks in order of their difficulty to perform (from 1 for easy
to 5 for difficult).
cut
suture
tie knots
position
- grasplgrip
18. Describe and explain some of the difficulties you have experienced using endoscopic
instruments in laparoscopy.
19. How did you feel when dealing with these difficulties?
choices).
challenged
frustrated
- angry tired
(please check all appropriate
other
20. How often are errors in the above tasks made due to restrictions in tool manipulability
and feel?
rarely - sometimes often
21. Give examples of the errors associated with each task (please be specific).
a. cut
b. suture
c. tie knots
d. position
e. grasplgrip
1 3 1
22. How did you correct these errors and why did you choose to resolve them that way?
23. In your opinion, how can the instruments be redesigned to improve performance
during surgery?
a. graspers
b. needle drivers
c. scissors
24. Do you think the amount of time spent in learning to use the instruments in endoscopic
surgery could be reduced? How?
25. Additional comments about endoscopic instruments for performing surgical tasks?
Thank you for your participation in this survey.

Sample Reminder Letter
April 5, 1995
Dear Dr. :
This is a follow-up letter to an earlier letter dated March 10, 1995 which included a survey questionnaire. The questionnaire was to solicit your expert knowledge of laparoscopic surgery and your views on the usability of laparoscopic instruments. I would like to urge you to take a few moments of your time to fill out this questionnaire.
As you know, we are conducting an analysis of the instruments currently used in laparoscopic surgery. Specifically, we will evaluate the manipulators for their effectiveness and where necessary, recommend changes in design. This project is sponsored by the Institute for Robotics and Intelligent Systems (IRIS), a Federal Network of Centres of Excellence.
The success of this project depends heavily upon your responses to reflect your views and opinions of the instruments you use in laparoscopic surgery. We would greatly appreciate your help and need 10-15 minutes of your time to complete the enclosed survey form. Completion of the questionnaire is entirely voluntary. You may choose to answer all or parts of the questionnaire. Please return the completed form in the enclosed reply envelope, and be assured that anonymity is ensured. There are no identification marks on the survey and envelope. Therefore, we request that you also fill out and return the enclosed postcard, separately, to tell us that you have completed the survey and do not need a reminder.
If you have concerns about this survey, you may contact my supervisor, Dr. Christine MacKenzie, or Dr. Andy Hoffer, Director of Kinesiology at Simon Fraser University (604- 291-3141). Copies of the results of this study may be obtained by contacting Dr. C. MacKenzie, Kinesiology, S.F.U., or Dr. S. Payandeh, Engineering Sciences, S.F.U.
Your prompt cooperation and participation in this important survey is much appreciated. Please complete the questionnaire today and return it in the return envelope provided. If you have already filled out and returned the questionnaire, please discard the enclosed questionnaire and accept our sincere thanks for your time and participation.
Sincerely,
Caroline Cao Graduate Student, Kinesiology Simon Fraser University

APPENDIX 11. Raw Data from Timelines

Dissect Tissue
Tape times lexpert 8371 33:50:43
0:06:52 0:07:26 0:08:09 0:08:35
0:07: 14 0:07:34 0:08: 1 5 0:08:43
cut tissue cut tissue cut tissue cut tissue

Tape times /novice 8371 34:27:47
I 0:30:511 0:31:041cut tissue 1
0:30:05 0:30:21
0:30:20 0:30:50
0:31:04 - 0:31:25 0:32:16
cut tissue cut tissue
0:32:31 0:32:38 0:32:49 0:33:01
0:31:24 0:32: 1 5 0:32:31
0:33:20 0:36:33 0:36:49
I 0:38:281 0:38:39/cut tissue
cut tissue cut tissue cut tissue
0:32:38 0:32:49 0:33:00 0:33: 19
0:37: 10 0:37:20 0:38: 16
cut tissue cut tissue cut tissue cut tissue
0:36:33 0:36:47 0:37:10
cut tissue cut tissue cut tissue
0:37:20 0:38:15 0:38:27
0:38:45 0:30:05
cut tissue cut tissue cut tissue
0:39:02 0:30:12
cut tissue ct 1

ct2 ctl ct2 ctl ct2 ctl ct2
0:30:26 0:30:51 0:30:54 0:31:04 0:31:11 0:31:25 0:32:02
0:32:34 0:32:38
0:30:50 0:30:55 0:31:04 0:31:12 0:31:24 0:32:01 0:32:15
0:38:07 0:38:16
0:32:38 0:32:45
ct2 ctl
0:38:15 0:38:18
ct2 ctl



I 0:33:531 I m l I

0:37:06 0:37:08
rnl rn2
0:37:12 0:37: 13
rnl m2
0:37:35 0:37:36
m5 rnl
0:37:37 0:37:38 0:37:41
rn4 rnl rn3
0:37:44 0:37:46
rnl m3
0:37:49 0:37:49 0:37:54
m5 m l rnl
0:37:58 0:38:02
rnl rn2
0:38:07 0:38:11 0:38: 13 0:38:15 0:38:16 0:38:17 0:38:18 0:38:19 0:38:22 0:38:25
m l rn2 rnl rn5 rnl rn2 m4 rnl rn2 rnl

I
Tape times /novice 837071 :09:20
0:15:11 0: 16:08 0: 17:24 0:16:32 0:29:30 0:29:53 0:15:11 0: 15:29
0: 15:53 0: 1 6:30 0: 17:43 0:16:51 0:29:53 0:30:20
0:16:15 0: 17:24
cut tissue cut tissue cut tissue cut tissue cut tissue cut tissue
0:15:27 0:15:53
ctl ct2
0:16:30 0:17:31
ct2 ctl

I 011 6:351 I m l I

1 :26:16 1 :26:25 1 :26:30 1 :26:36
1 :26:17 1 :26:26
- -
1 :02:44 1:14:39
cut tissue cut tissue
1 :26:31 1 :26:37
cut tissue cut tissue
1 :02:57 1:14:57
cut tissue ct1

1 :25:511 1 :25:571cut tissue
1 :24:59 1 :25:22
m2 rnl
Tape times ]novice 837071 :51:58
1 :26:04 1 :26:12
1 :26:05 1 :26: 1 3
0:06:37 0: 12:50 0:46:07
cut tissue cut tissue
0:07:10 0:13:05 0:47:29
cut tissue cut tissue cut tissue

Tape times novice 8371 58:07:45
I

Tape - - -- times expert -




times novice - -- - - - - - - -- -- -- - - -- - - -
- -- - -- - -- -

~~ -. ~ 1:18:35 . - -~ -- . m5 -- -- - -- - - . - ~
1:18:37 m l ------A ---------A--- ~ -- - - - - - p- -
1 :18:40 m2 ~ ~
- -A. - -- --
1 : l8:4O - ~ . - ~
m4 ~ ~ -. ~
1 :18:42 m l A -- A------ -- - ~ - - ~ ~
1:18:50 m3 ~ A - - - - - . - ~ - ~ ~.
1 : l8:52 ~ -~ --.-----A ~ m 5~ ~ -
1:18:53 m l ~ ----A -~ . .- -- -- ~~~~
1:18:54 m2 -p -- -- - .- - ~ ~
.- 1 : 18:56 m5 ~
1 : l8:57 - .. - .. - - m l - -
1:19:00 rn2 -- -~ -- -~ --A- -
1 :19:05 m4 - -
1 :19:07 m l -~ --~p~ -- - -- -- -
1 - 3 - 0 9 m2 . ---
1:19:10 m5 - -. - --.. -. - . - --- - -
1:19:12 m l 1:19:16 m2 1:19:16 m5 -- -
1:19:17 m l 1 :19:23 -. m2 1 :19:24 m5
.. -
1 :19:25 m l .- . --A_----
--
1 : 19:27 - m2 ___~
A -- 1:19:28 -- .. m5 - -
1 : l9:29 p~ --- . - -- m1 ~
1:19:42 m2 ._ ~ ~
. - 1 :19:47 . . - - - m l _ - . __-_ -
~- 1:19:51 ~.-~ - - -- m2 --
1:19:51 --- m5 1:19:52 -- -- m l 1 : 19:57 -- -
m2 -
1:19:59 m5 -- -- --.A-
-- 1 :20:01 rnl p- - -.
1 :20:07 . - , m2 .. ----_A- - --
1 :20:08 - - m5 .,-
1 :20:09 .. m l -- . -- - -
1 :20:13 m2 -- A - - --
1 :20: 14 --
m5 -- -. . . -
1 :20: 15 ~ ..~ .. - - - -.
m l _- - -.
m2 -A---p--p. - ~ - ~ -
1 :20:29 m4 -pp-. . - -- -
-
1 :20:32 -- -
m l -- -. -- - A-p - -- - -- -. . - - - - -- -
1 :21:01 A -- -- -- ~ - ----- ~
1 :21:08 ~ ~ m l -~ ~ - - . .- - - - -- - -- -
. 1:21:20 m3


1 :56: 15 suture - - --


0:00:01 -- -
start suturing - - --
0:OO:Ol 0:00:18 st1 - -- -- - - - - - -
0:00:20 0:00:29 st2 -- - - - -- - - - - -
0:00:31 0:00:56 st3 - - - - -
0:00!58 0:01:11 st5 -- -
0:01:14 0:01:37 st6 --
0:01:38 --
0:01:56 st7 -- --- - -
0:01:56 - end suture 1 -- - --
0:01:56 -- - start suture 2 0:01:56 0:02:32 st1
-- -- - - - -- - - --
0 : G : 17 0:03:30 st2
-- 0:04:10 st3 0:03:32 - --- - - - - - -
0:04: 13 0:04:17 st4 -- - - - - -- - - -
0:04: 18 0:04:21 st5 - - - - -- - - - -
0:04:24 - - - - 0:04:36 st6
0:04:37 - - 0:05:05 - - -- st7 - end suture - 2 -- - - -
0?E:05 start suture 3
- - 0:05:07 0:05: 18 st 1 --
0:05: 19 -- 0:05:47 st2 -- -- - --
0:05:49 - - - - - 0:06:08 st3 - - --
0:06:39 st4 0:06:14_ --_ - -- --
0:06:41 0:06:49 st5 --
0:06:51 0:07:07 st6 -- --
0:07:23 st7 -- --
-- end suture 3
-- - - -- - - -- start suture 4 0:07:27 0:07:31 st2 - -- - -- - -
0:07:34 0:08:23 st3 -- --- - - - - - - - -
0:08:24 -- 0:09: 13 st4 - - --- - -- -
O:O9: 14 --- -
0:09:33 st5 - - - -
0:09:34 -- - - 0:09:48 - st6 - -- -- -- -- - -
0:09:48_ -
0:10:14 st7 -- -- - - - - - --
0:OO:Ol start motion

0:02:05 -- rnl -
-- m2 --



0:08:31 m2 - - -- - - -- -
0:08:38 m 1 -- - - --- - - -- -- - - - -- -
0:08:40 m2 - - - - --- - p-pp - --- -
0:08:44 - -- - -- - - - -- m4 - -
0:08:46 m 1 -- --- -- ------- - - - - -
0:08:50 m2 -- - -- -- - A - - -- - -
- - - 0:08:53 m4 - - - - -- - - - -
0:09:00 ---- - m 1 - - - - - -- - - - -- - - - - - -- - -
0:09:04 - pp - -
m2 - - - - -
0:09:06 - -- m 1 - - - -- - - -- - --
0:09:09 m2 -- - -- - - A - - -
O:O9: 14 - --
m 1 -- A - -- - - --
0:09: 15 - - - -
m3 - - - - - -
O:O9: 18 - -- -- -
m l -- -- - - - --
0:09: - -- 19 - -- -- m2 - -- - ---
0:09:21 -- m3
- - -- - - -
0:09:28 -- - - - -- - - - m3 p---p-p --
0:09:35 -- - - - - m 1
-.- -
0:09:38 m2 -- -- 0:09:39 -- m2 --
0:09:41 m4 -- --
0:09:42 -- m l - --
0:09:46 .- - m2 --
0:09:50 - --
m4 -- -
0:09:51 m 1 _ _ _ - 0:09:52 m2 --
0:09:55 - - - m2
-- -- - --- - --
0:09:57 - - -
m4 - - -
0: 10:Ol - - ---- m4 - --
0:10:16 m 1 0:10:18 m2 -- - -
0: 10:20 m4 -- ---- - - - -
---
Tapetimes - expert - - - -- - - - -
83701 6:1 0:39-_- _- -- -- -
0:52:26 0:53:57 suture - 0:55:52 - --
0:57:02 suture 0:58:41 _ _ - 0:58:50 suture -- --
0:52:26 - - 0:52:41 st1 -- -- - -- -
0:52:41 0:52:53 st2 - - - - -, - --
- --- - -- -
0:52:54 -
0:53:08 st3 - - -- - -- - -- -- --
O:53: 15 - -
0:53:17 st4 - - - - -- -- - --
-- - 0:53:18 -- -- -- 0:53:23 st5 -- -- -- --
0:53:24 0:53:34 st6



-- --
1 :02:38 1 :06:35 suture motion -- -
1 :02:38 1:0419 st1 - - --
1 :04:20 1 :04:33 st2 - -
1 :04:35 . - -, - 1 :04:44 st3 - -
1 :04:44 - - 1 :04:52 - -- st4 - - - - - -
1 :04:53 1 :04:59 st5 - .- - - -- -- - - - - -- - -- -
1 :05:00 1 :05:21<t6 - -- -- - - - -- - - -- - -- --
1 :05:22 1 :06:35 st7 - - - - - - - --- -- -
1:02:17 motion


0: 18:29 - - - 0:18:39 - st3 - -- - - --- -
O:l8:4l -- -- -- 0: 1 8 : ~ 8 G 4 -- -
0: 18:59 0: 19:28 st5 start motion

0: -- 19:29 - ~. -- - ~ o:?o:O! .st!! - - -- -
0:20:02 0:20:51 st7 - - .~ -~ ~ - - - - ~ - - --
0: 14:35 start motion -- --- . . - -- -~ -
0: 14:40 m 1 .- .-- -~~ -- - -- - - - . ~ . . ---
0: 14:44 - - m2 ~ - -
0: 14:47 -. - -- - . - -~ -~
m 1 - - - -- - ~ - - - -- - - ~ - -
0: 14:48 m2 - ~-~
0: 14:54 l-nl - - .- ----A . - . - - - - - -- --
0: 14:56 m l ~ .- -~ . . . -- -- - ppp-
0: 1 5:03 m2 ~ - ---pp-.-.-----..p. --
0: 1 5:O7 - -. -- . -- m l
-- --- -~ .- -
- -- 0:15:16 m2 --
0: 1 5:20 m 1 - - .. - - - -. -- - . ..
0:15:32 .. . - - -- m3 ---p-pp--..--.-.--. ~ -.
0: 15:34 m l -. - ~ - ~ . . ---- ~
0:15:37 -
m2 - . - .- - - - . -
0: 1 5:42 -- m4 --- -- - - - - . --
0: 15:45 m3 0:15:51 m 1 - .-
0: 15:55 - - .- -. m3 . .- -
0:16:01 -- - - m ! 0: 16:05 m3 -. - .-
0:16:10 m l 0:16:17 -- - m3 ~- -- -
0: 16:23 m 1 --
0: l6:25 --- -- -. - m2 - ~. - --
0: 16:27 m3 . -- -- -.
0: 16:29 . m l - - --
0: 16:35 -- m3 -
0: 16:36 m3 0: 16:39 -. . - - J!??---- 0: 16:45 m l -- p- -. - -- - 0: 16:47 m3
-. -- - -. - . . -. . .-
0: 16:50 ~ ---- .- m l 0:16:51 - -- m3 ~ -- - -
0: 16:59 m l --..- - .
A 0: 17:Ol m2 .- -- 0: l7:O3 - . . m 3 -
0:17:11 m 1 _ . - _ ~ _---_.-.p._. --
0:17:13 m2 ---a- A --
0:17:14 ~ ~ ~ m3 ~ - -- - . --
0: 17:20 m l - _ -- - -- - --
0: 17:22 m2 ~ ~- -- -- - - - - - --
0: 17:26 m 1 - - - - .~ - --- -
0: 17:31 m 1 ~ - . -. - -- - --- ~~~ --
. 0:17:34 m2



---- - -- - - -- - - - -- -
Tape times expert I - - -- . .- - -- -- .- --
--- -
1 :06:05 --
1 :07:46 tie knot - - -- - - - -
1 :07:47 1 : 1 0:46 tie knot -- - - - -- -
1:13:15 - - -- - - 1 : 13:58 tie knot
--- -
1 : 14:24 1:15:13 tie knot ---
-. 1 :06:05 1 :06:26 kt 1 --
1 :06:26 1 :06:34 k t2 -- - -- -
1 :06:35 -- --
1 :06:47 k t3
- -- 1 :06:49 - -- - 1 :07:46 k t4 -- -- 1 :07:47 1 :09:00 k t 1 - --
1 :09:00 1 :09:06 k t2 --
1 :09:07 - 1:09:13 k t3 _
1 :09:47 1 :G:46 k t4 - -- - -- -
1:13:15 - - 1:13:22 k t1 - - - --
-- 1 : 13:22 1 :13:28 k t2 1 : 13:30 1:13:42 k t3 - - -
1 : 14:24 1:14:36 k t1 - -- -
1:14:37 --
1 :14:40 k t2 -- -
1:14:40 1:14:46 k t3 - -- -- . - - - -- - --
1:14:46 1:15:13 k t4
- - 1:13:42 1 :13:58 k t4 --
--- 1 :05:50 - -
motion
1 :06:07 -- - - - - - -- m 1 - --


m4 - 1:13:08 motion 1:13:15 - -- m 1 - ---
1:13:20 m2

rape -- -- times novice 337087:00:41 - - - -- - - --
1 :23:51 1 :24:47 tie knot -- 1 :24:55 1 :25:29 tieknot 1 :25:35 1 :26:07 tie knot - - - - - --
1:56:13 -- - - 1 :57:34 tie knot --
1 :57:35 - - -51 - - - tie knot - -- - ---
1 :23:55 1 :24:06 - kt 1 - -
1 :24:07 1 :24:23 kt2




0:29:48 - -- -- - 0:30:22 - kt - 1 -- - -- - -
0:30:23 - -- 0:31:01 kt2 -- - -- - -
0:31:02 0:31:14 kt3 - - - - - - --
0:31:14 0:31:28 kt4 - - - - -- - ,
-
0:29:48 0:31:28 tie knot -- - -- -- -- -- - -
0:31:32 0:34:38 tie knot - - -- -- - - -- - -- -- -- -- -- -- 0:34:44 0:35:59 tie knot
- - --
0:36:04 0:37: 1 7 tie knot , ---- -
0:31:32 - --- - 0:32:53 -- kt 1 - - pp -
0:32:53 0:33:37 kt2 - . -- - - --
0:33:38 0:33:53 kt3 - - -- - -
0:40:25 0:40:37 kt3 -_-- 0:40:37 0:40:41 kt4
-- - - -- 0:37:20 0:40:41 tie knot
- -- - -- - --
0:42:23 - -- -- 0:43: -- 19 tie knot - ---
0:42:23 0:42:38 kt 1 - - - - -- - .- --
0:42:39 - 0:42:49 kt2 -- - -
0:42:49 0:43:00 kt3 --- --
0:43:00 0:43: 19 kt4 - --A- --
0:29:35 m l -
0:29:51 m 1 -- --- - --- -
0:29:57 m2 -- - -- -- - - - --
0:29:59 m l - - - - -- - - 0:30:10 m l - -- - --- -
0:30: 1 4 - -- m 1 - - --- -- ----
0:30:23 - - - - --
m 1 - -. - - - --
0:30:27 - -- - - m 1 -- ---- -- - - - -
0:30:39 m l




--
Tape times expert -- --
8371 13: 1 1 :48 I 0:53:58 0:54:20 tie -- knot -1 0:54:20 0:54:45 tie knot - - --- -- .-. -
0:54:46 0:55:27 tie knot - -- -- -- - - -- -
- - 0:55:28 0:55:43 tie knot -- - -- - - - - - -- --
0:53:58 --
0:54:05 kt 1 -- - 0:54:05 0:54:07 kt2 ___ -- , -- - -- -
0:54:07 -- -
O:54:17 kt3 -
0:54: 17 0:54:20 kt4 - -- - --- -- - - - - -


0:56:00 - -- - -- -- m2
0:56:01 m5 0:56:02 m 1 --
0:56:03 m2 --
0:56:04 m5 - -- --
0:56:05 -- -- - -- m 1 0:56:59 - - - 0:57:20 - tie knot - -.
0:57:21 0:57:40 tie knot --- -
0:56:59 0:57:03 kt 1 - -
0:57:03 -- - -- -- 0:57:06-kt2 - -- --
0:57:06 - - 0:57: 11 k t3 - 0:57: 1 1 0:57:20 -- kt4 - --
0:57:21 - 0:57:23 -- k t 1 -- -
0:57:24 -- 0:57:26 -- kt2 - - -- -- - - 0:57:26 -- - 0:57:33 k t3 - - - -
0:57:33 0:57:40 k t4 -
0:58:50 -- 0:59: 19 tie knot - - ---
0:58:50 -.- 0:58:52 k t 1 -- -
0:58:52 0:58:53 -- k t2 --
0:58:54 - - - pp 0:58:57 kt3 -
0:58:57 - -- - O:59: 19 kt4
- - 0:56:59 -- - -- m 1 -- - -
0:57:03 - - -- -- m 1
- -- --
0:57:05 -- m 1 A -- --

Tape -- times novice -- --- 835357:24:01 - -
-- - - - -
-- -
1 :06:36 1 :08: 19 tie knot intern 1 -
1:08:19 1:1 1:52 tie
-- 1:11:59 - - . - -- 1 -- : 13:32 tie knot - -- -- - intern 1 1:13:33 1 : 15:55 tie knot





-- - - --- - - -- - - -- - - -
0:21 :00 0:23:50 tie knot -- - -- - - - - - - -
intern 2 -- - - ---
0:24:02 0:25: 19 tie knot intern 2
-- 0:21 :00 0:21:55 kt1 - - 0:21:55 0:22: 17 kt2


- - - - -- -- --
1:15:25 1 : 1 5:26 ,- pull taut -- 1:15:26- 1 : 15:29 snip
- - - - -- -- - - -
1:15:30 1 :15:32 snip - - - - - -
1:15:30 1 : 1 5:32 cut suture -- -- - - -- --- -- --
1 :26:26 1:26:31 pull taut -- -- - -. --
1 :26:32 ---- - 1 :26:43 snip 1 :26:44 1 :26:46 snip
- - ---- - - -- 1 :26:26 1 :26:43 cut suture
-- 1 :26:44 1 :26:46 cut suture -- ---
1 :26:33 -- -- - m 1 - -
1 :26:27 --
m4 - - -
1 :26:33 - --
m 1 - - -
- - 1 :26:43 m2
- -
1 :26:45 m 1 1 :26:46 - --
m2 - --
837071 - - :44:38 expert - -
0: 18:40 - 0: 19:OO -- cut suture- -
-- 0:19:16 0: 19:28 cut suture 0: 18:40 0:18:41 c s l

rape times novice 337095: 15: 12 -- .- -- -
- -- - 0 : G : 19 0:46:32 cut suture
- -- -
0:46:46 0:47:03 cut suture -- - -- - - - - - O:46: 19 ---- - 0:46:26 cs l 0:46:26 0:46:32 cs2 - 0:46:46 0:46:59 cs l -- - --
0:46:59 0:47:03 cs2 - 0 : G : 19 -- m 1 0:46:21 -- - m2
- - - - - ---
0:46:22 - - - - m4 0:46:27 - m 1 0:46:32 -- - - -- m2 0:46:45 - m 1 - -- - ---
0:46:49 - -- -- m2 - -
0:46:51 m 1
-- - - -- -- -
Tape times novice - - -
937072:08:53


1 9 3
APPENDIX 111. Tests of Agreement between Two Observers

1 9 4 Kendall Rank-Order Correlation Coefficient T
Subtasks Researcher's Rank (A) Naive Rank (B) duration (A) Subject's
duration (B) cs 1 5 1 4 1 cs2 6 2 6 2 kt 3 7 3 7 3 st2 1 0 4.5 1 0 4.5 st3 1 0 4.5 1 0 4.5 kt 2 1 3 6 1 3 6 st4 1 7 7 2 3 9 kt 1 2 2 8 1 9 7 st5 2 9 9 2 2 8 st6 3 2 1 0 3 0 1 0 kt 4 3 5 1 1 3 9 1 1 st7 4 9 1 2 4 8 1 2 st1 5 4 1 3 4 9 1 3 st1 5 6 1 4 5 9 1 4 st2 107 1 5 109 1 5
b: There is no association between the observers in the durations assigned for each subtask.
cs l cs2 k t 3 st2 st3 kt2 st4 k t1 st5 st6 k t4 st7 st1 st1 A 1 2 3 4.5 4.5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 B 1 2 3 4 . 5 4 . 5 6 9 7 8 1 0 1 1 1 2 1 3 1 4
I + + + + + + + + + + + + + 2 + + + + + + + + + + + +
3 + + + + + + + + + + + 4 . 5 0 + + + + + + + + +
4 . 5 + + + + + + + + + 6 + + + + + + + +
9 - - + + + + + 7 + + + + + +
8 + + + + + 1 0 + + + +
1 1 + + + 1 2 + +
1 3 + 1 4

S = the number of agreements in order minus the number of disagreements in order, for ranking B with A. N = the number of subtasks. TA = Zt(t-1), where t is the number of tied observations in each group of ties in A.
TB = B(t-1), where t is the number of tied observations in each group of ties in B.
T = 0.96 P[T > 0.961 < 0.01; for H, to be true, the probability of T = 0.96 is less than 0.01.
Z = 4.99, a(2-tailed) < 0.00001; H, is true with a probability of p < 0.00001.
Reject I+&,. There is no difference between the two observers' results for subtask
durations, using the same set of criteria for video analysis. T = 0.96 means that we have very good inter-observer reliability ( a < 0.01). Therefore, the timeline analysis results
from the videotape analysis based on the operational definitions of beginnings and endings
for each subtask are reliable.

1 9 6 Freidman's Rank Test for Correlated Samples
Subtasks Researcher's Rank Naive Rank duration Subject's
duration kt 1 22 2 19 1 k t2 13 1.5 13 1.5 k t3 7 1.5 7 1.5 k t4 35 1 39 2 st1 54 2 49 1 st2 107 1 109 2 st1 56 1 59 2 st2 10 1.5 10 1.5 st3 10 1.5 10 1.5 st4 17 1 23 2 st5 29 2 22 1 st6 32 2 30 1 st7 49 2 48 1 csl 5 2 4 1 cs2 6 1.5 6 1.5
Rank total 23.5 21.5 (Ri) Mean 30.1 29.9 duration
Ho: On average, subtask durations obtained by a naive subject are the same as those obtained by the researcher, using the same criteria for video analysis.
k = the number of observers N = the number of subtasks Ri = the sum of the ranks for observer i
x~~ < x ~ . ~ ~ (I), cannot reject Ho.
There are no differences between the two observers' results for subtask durations, using the same set of criteria for video analysis. Therefore, the timeline analysis results from the videotape analysis based on the operational definitions of beginnings and endings for each subtask are reliable.

1 9 7
APPENDIX IV. Survey Questionnaire Response

Section 11. Endoscopic Manipulators
13. Do you have a feel of the tissues being manipulated through the instruments? How would you describe the feel?
-very limited, instrument cannot be used for tactile sensation -I think i can imagine the feel more than actually feeling it -distant -0k -usual sensation via instruments -feel is appropriate -yes, can tell if tissue is inflamed /woody/ not -yes, but not as good as in open surgery, not as 'sensitive' -awkward, not good extension of my hands, don't stay on tissue or remain in place when I let go -good -yes, reasonable --- with some area less sensitive. Difficult to walk around vessels. -wooden -good feel, comparable with open surgery -of course, after a while, same as open surgery -yes, instruments do transmit the feel or 'texture' of the tissue quite well -more or less dense, soft, sound of calcified tissue -reasonable once you get used to it, I like blunt ended instruments as I feel they are safer. -moderate sensitivity considering distance and instrumentation -light tool -tactile stimulation minimal with lap. instruments, useful in groin surgery to identify cooper's ligament -fair to moderate sensitivity only -somewhat displaced centre of gravity or fulcrum distance -yes, relatively 'gross', instruments 'clumsy' and 'stiff -yes, the feel is two directional with no depth -moderate idea of firmness and extent of tension and strength of tissue. not nearly as good as open procedure -no. only very few instruments give a positivelsafe feel. this may of course be reflection of view in 2 d, new camera system will surely address that problem -yes. varies. -yes, feels a good coordination with my eye -no. for the most part. occasionally, very 'tense' gallbladder will feel that way. but most tissue handling does not give a sense of friability or toughness. -both visual and tactile are relevant -poor feeling if any at all. lOmm instruments give better feedback than 5mm instruments -more of a visual assessment -good. easily relate to open feel if experienced in both types of surgery -satisfying -fine, have nothing to compare it with except open -no direct appreciation of texture of tissue possible with instrument -indirect feel of tissue strength -variable feel depending on maintenance and wear -not a big factor -not as responsive as with open instruments, the instrument in endoscopic surgery works as a lever the fulcrum being the ab. wall -learned to recognize 'feel' of tissue over 3-4 months -almost none at all -yes, but difficult to describe

199 -not really a 'feel'. more a correlation between force applied and visual tissue changes -no -little tactile sensation except for lighter instruments -yes.---tissue or resistance -adequate, appropriate for the tissue, very similar to open surgery' -poor -yes, distant but distinct -fairly realistic -feeling of remote manipulation, i miss the tactile sensation and lack of 3-D vision -yes. one is able to detect the degree of elasticity of the tissue -not unusual -yes -not really -can only feel degree of in direction and pliability -yes -yes -moderate -yes, same as would feel open -no. very limited feedback of 'tissue feel' -feel only bluntly -the biggest problem is deciding with thiodiened, adherent, chronically inflamrned structures. For example dissecting the bowel off the gall bladder. lack of feel can lead to injury to bowel or common bile duct. -varies depending on the tissue -0k -yes, ie. woody (inflamrned), dense, scarred, descriptive terms -almost like feeling with the hands -yes. moderate -yes -yes -yes, you can feel the tissue but the lever-arm ratio makes the feel very rudimentry. again, I believe a palm action (like forceps) may offer better tactile input

200 14. What do you think is the most limiting feature of the following endoscopic manipulators?
14a. Graspers: -crude -tear grip -must be more gentle but able to grip -tearing -always coming off -graspers do not grasp tissue securely -doesn't grasp securely -diffult to hold large inflarnrned organs -holds tissue -v. good -hard to hold fmed for a prolonged period -don't have an angle -holding tissue finny yet not damaging it. -loose grasp -slip off tissue, or tear wall of organ -size of grasping -can tear tissue -don't hold -tend to slip -pull off -too traumatic -weak joints, not designed for appropriat muscle groups -don't grasp gb well -strength -varies--occasionally too sharp causing tissue injury -limited degrees of freedom, limited grasp of thick tissue -injuring tissue -inadequate for accute inflammatory conditions -they slip off tissue -tendency to slip from thick walled gb -soft touch -sometimes don't hold well -slip, damage tissue -they slip a lot -they fall off -awkward release and grasp mechanism at handles -insulation break down -they don't usually grasp -working at angles -slip off -none -often unable to grasp thick walled tissues, eg. chronically inflammed gallbladder, poor tactile sensation -no feel -either too week and slip off, or too strong and tear -grasping ability vs. tendency to tear tissues -either slipping off edematous tissue or perforation of thin tissue -often tear tissue -lack of force feedback -cannot rotate, the new models do rotate

-slipping -work well -often slip -can perforate the gall bladder -limited jaw opening
14b. Needle drivers:
-difficulty positioning needle in driver -crude --- grip -not firm in their grasp -0k -awkward to pass -poor grip on needle -holds needle -good -really awkward to hold needle in desired position -not holding needle -holding the neelde 'true' -need modify -angle of tying -needle slipping -holding needles to prevent rotation -neelde slips -awkward -lack accuracy -fussy to use -weak joints, not designed for appropriate muscle groups -orientation -not much experience -handle design -360 degrees -acuity to use -need adjustment -needle rnanipulation/positiionign -jaw straight -difficult because of the angle of the needle on the insbxernnt -pronation -visual depth perception -can be rigid to grasping -lack of flexibility of tip -work well -lack of pivoting of jaws
14c. Scissors:
-crude -don;t cut with gentle manipulation -no complaints -need a slightly finer touch when doing cholangiogram -get blunt -adequate -oft& fail to cut (disposables) accurately

-become dull quickly -sharp -pretty good -very good -0k -staying sharp and tight so as to cut clearly -get dull easily -good instrument -dull quickly -good -no significant problem -jaws too small, sharpness -weak joints, not designed for appropriate muscle groups -size -sharpness -become blunt easily -these seen to work well -sharpness, blade size -prefer one blade fixed -shears and hook type work fine -blade visualization -good. particularly the disposable. no problem -wear out at blade -don't cut as well -difficult to see tip at scissors -some are dull and dont' cut -curve of blades -sometimes not sharp enough and 'pinch' rather than cut -should be color marked so sicssors will not be used as graspers by mistake -hook scissors---no problem -don't always cut -visualization of the tip -fairly good -no feel -become dull too easily -dull quickly & cautery -lack of sharpness -same edge when used for cautery -all work well

2 0 3 15. What do you think is the best feature of the following endoscopic manipulators?
15a. Graspres:
-fm grip -easy to use -atramtic -can be locked for holding pause -if light-weight, allow some tactile feel -locking -very easy to clear -Maryland? --nice shape, feel -wide variety already available -basically are adequate -variable size -good ratchet, good grab, no damage -generally easy to hold -variety -atraurnatic -self-holding, can use for retraction -small -trigger lock -varies, dep on type and manufacturer -blunt -multi purpose and safe for dissection -rotate -make minimal access surgery feasible -totally need re designing -need reinventing -manoeuverability -able to rotate -the new nones allows tissue for 'bunch up' and hold securely -feel

15b. Needle drivers :
-easy to use -can hold needle on angle -palm grasp -small, compact -rotation difficult -generally good grasp of needle -feel -good grasp needed -hold needle securely -good feel -small --- to use -resemblence to open instruemtns -the features vary. depends on type and manufacturer -rotate -make MAS feasible -secure tip -centre of gravity adequate -need re-inventing -touch
15c. Scissors:
-easy to use -satis tissue feel -precise cutting -can be rotated -curved type, sharp points -0k -versatile -they work! -if sharp, noproblem -sharp, swivel, fine -generally good feel, cut well when sharp -easy dissection -sharpness -rotable -sharp -same action as open instruemnts -rotation, cautery -size -sharp, precise -can usually cut and easy -ease of operation -the features vary. depends on type and manufacturer -good generally -make MAS feasible -rotate -cutting blades may be thinner -manoeuverability -need re-inventing -scissor rotation -sharpness

205 Section 111. Manipulators and Tasks.
18. Describe and explain some of the difficulties you have experienced using endoscopic instruments in laparoscopy.
-It is difficult to work perpendicular (or at any angle) to the camera--I'm better if I'm lined up to the image. Knot tying in 2 dimensions is difficult -mostly equipment problems (insufflation, leaking valves, dull scissors) -crudeness of the instruments, poor optics, poor position of trocars -exposure, trocar site placement, losing pneumoperitoneum -graspers slip, scissor won't cut, constant chaning of reducers-- nuisance, insertion of instruments usually too stiff-- too much resistance -graspers sliding off tissue, scissor thickness too thick, drivers have awkward sense of gravity -occasional tearing of tissue, occasional sticking and insufficient grasp with graspers, dulling of scissors -grasping, positioning and accurate 3D view -narrow access -2D, grasping, tying -bleeding and its controlis worst, usually not as bad as it looks, spilling stones from a fragile gallbladder, visibility problems especially with fogging -the small instruments frequently break, instruments with ratcheted mechanism for maintaining instrument closure frequently fail, cholangiogram catheter clamps heavy and slip from position -handle does not have an angle, though -- it is quite uncomfortable for the finger and hand to hold for long time -mainly coordination--e.g. reverse movements, camera for visualization (Asst.) improves with practice -lack of good grasp with graspers, tissue sliding off, etc. -I developed a left hand carpal tunnel syndrome (dominant right), first noticed the symptoms during long laparoscopic procedures, many difficulties are due to improper port placement. I had my carpal tunnel syndrome repaired. Now I try not to flex my wrist as acutely. -the angle you are at can be difficult, ie., angled scope, and trying to get straight instrument into desired position around corner -to expose the operative site -mostly don't hold well, suction of clots impossible -suturing and knot tying, grasping needles. Occasionally equipment becomes stiff with use (opening and closing) -lack of exposure because of technical difficulties (unable to collapse lung), convert to open because of inability to feel deep lung lesion -scissors won't cut, instruments delicat and wear out quickly -2D viewing-- lack of depth perception, smoother release of needle driver, poor grasp of OB, esp. if inflamed -graspers not holding, scissors not cutting -trauma to tissue -breakages-- esp screws in handles falling off, stiff action-- frozen cables -suturing, knot tying, line station of trocar ports -getting to areas where an angled or flexible instrument would be helpful -hands tire -seem too large and clumsy for a delicate task. Needle holders difficult to keep closed at handles, limited degrees of freedom -2D visualization -exposure

206 -I do pediatric surgery only. Instruments too large and heavy, even those designed for pediatric use -limited field, limited angle, lack of 3D -graspers slipping -position and repositioning -depth perception is poor, different instrument (ie grasperslscissor) should have different colorlmarking so inadvertant use of scissors as clamps is circumvented -holding on to a gallbladder with thickend wall without tearing the gallbladder. Cutting dissection of gallbladder (remove off of liver bed) when the hooked dissector grounds out on the surrounding gallbladder -grasper slips off the tissue -failure of graspers to hold onto tissue, perforation of tissue by graspers -poor seals allowing C02 to leak rapidly -graspers slip off, scissors do not always cut, coagulation often not working -- connections -frankly, most of the problems have been with the visual aspects (lights, camera) and not with instruments -loss of depth perception -lack of feedback results in tearing and perforation of tissues, poor 'angles' between shaft and handles occasionally results in difficulty, applying appropriate pressure to operate instruments -grasping, visualization -insturments need to be rotating -difficulty manipulating, insecurity at dividing tissues, graspers slip, clips slip or cannot be put in place precisely as desired -keeping the lens and light source clear -length of instruments including trocars-- too long or too short, when working in a small area-- the instruments and ports interfere with one another -rigidity -instrument life not too long, not as responsive as with open instruments, the instrument in endoscopic surgery works as a lever, the fulcrum being the abdominal wall -rigid, long, small instrument, jaws inflexible -it is a new and entirely different dexterity which has to be learned -the camera and screen on occasion do not function well -lots -fogging of lens -visualization to position, access issues -poor visability because of 'fogging' of laparoscope lens -some technical problems with suction - aspirator parts not assembled properly, camera not working, cautery cables falling off instrument (too loose fitting) dull scissors -retrieval bags difficult to manipulate -some instruments don't grab well, some are not insulated distally enough so they short out on the hole -positioning of trocars most difficult, difficult to grasp and retract tissues without damaging them
to maneuver at times

207 21. Give examples of the errors associated with each task (please be specific).
-errors due to poor technique rather than problems with design of instruments
21a. Cut:
-saw instead of cut -only done when 100% sure of expected results -dull scissors occasionally a problem -cut tissue behind that desired -no problem -occasional cuts beyond desired structure -bleeding -no problem -poor visibility behind object (? taking too much with bite) -wrong tissue -angle difficult to see, large blades if disposable -cutting extra tissue at the tip -difficult to cut in correct position -none -curve of blades doesn't fit the approach, or dull blades -cut too far -not complete -won't cut -bleeding -too big a cut -none -few -scissors become loose and don't cut cleanly -blunt scissors, angle -entering GB, annoying, possible ligation or cutting adj . structures (adhesions) eg., artery, duct, bowel, etc. -cannot see clearly what you cut -dull scissors -- multiple cuts in cystic duct to perform cholangiograrn -cut too long, too short -dull scissors -tight space feeling -too deep -- tissue behind cystic duct -dull instruments -dull scissors -- difficulty cutting, more 'chewing'
21b. Suture:
-retying -difficult (no experience) -difficulty in placement as desired -rotation of needle -needle tip hard to position, can't always get smooth needle movement -done rarely -awkward at times -needle too short -don't do -depth of bite difficult to access

-needle manipulation -difficult to appreciate thickness of tissue -difficult to pass needle through tissue -none -needle slips -not secure -2D viewing-- lack of depth perception -awkward to grasp needle -bleeding-- suture slips -unable to place in desired location -none -difficult to aim needle and get both sides -needle slipping in grasper -position of instruments, size of the needles -entering GB, annoying, possible ligation or cutting adj. structures (adhesions) eg., artery, duct, bowel, etc. -accurate insertion in tissue difficult -staplers that catch mesh during hernia repair -3-D -needle turning -need re-doing -cumbersome instruments -- drops sutures -difficulty
21c. Tie Knots:
-retying -difficult (no experience) -improved with the latest Autosuture suturing device -knots not secure -hard to tie knots tightly -done rarely -slipping -don't do -slipping of knot -2D -just plain hard -difficult to maneouvre suture to correct position -knots not secure -none -difficulty approximating tissue -not secure -smooth release of needle driver -sometimes awkward to grasp suture -bleeding-- suture slips -difficult to tie secure knots -takes time to do it correctly -awkward-- extra-corporeal easier, suture may catch and get knotted -not tied tight enough, requires many throws -angle of instruments -uncomfortable -2D vision disadvantageous, instruments do not hold suture well to secure knot -avoid where possible, use clips -3-D

-need re-doing -thick instruments, won't pick up sutures -not easy to do
21d. Position:
-clips slip -lack of depth perception in 2D systems -no real difficulty except for tearing of gallbladder with grasping forceps -challenging in obese patients -only if non rotatable kind -poor visualization -limits of ports -not too much of a problem -injury to tissue -malposition-- wrong angle -angle of approach -- port placement -retraction not optimal -- poor visualization -retractor slipping and loss of exposure -need more instrument (new) to help to position instrument and lighting -trocars in wrong place to get good access -this is often difficult-- particularly if port are not optimal - ? -good to have a proper view -? triangle may be obscured by malposition -not usually a problem unless you position trocars incorrectly -assistants tired -wrong angle feeling -poor trocar placement -necessary to make more ports -operator problems, eg. port placement
-tear gallbladder wall -making holes in organ -slips off the gallbladder -difficulty in exposure, difficulty grasping GB -slippage with the desired tissue -loose retraction and therefore exposure -slippage, tearing of tissues -no real difficulty except for tearing of gallbladder with grasping forceps -occasional slippage from jaws or slippage of lock mechanism -tissue slipping -tear of gallbladder wall or perforation of gall bladder -perforation of hollow objects-- gallbladder with grasper -loss vision -GB perforation with tip of grasper -too rough or too soft -perforation -often do not grip tissue adequately -may cut into tissue -injury to tissue -can tear tissue

-swollen tissue can't be held (acute cholecystites) -trauma to gallbladder during cholecystectomy -poor grasp of OB esp if inflamed -slips off -instrument slipping, loss of exposure -slips -rarely -tiring if position maintained for long time -tissue slipping -tissue sliding from jaws -tool does not hold the object -slipping of grip, reach to loss of position of gallbladder during cranial retraction -slipping of cannula from cystic duct -too much tension on the hand -mostly tearing of tissue, or angle problem -slipping -tear hole in GB occasionally -slipping -slipping grip (ratchet releases or grip insufficient)

211 22. How did you correct these errors and why did you choose to resolve them that way?
-'I rarely make errors -- but at the expense of increased time to accomplish the task properly' -'practice learning the "feel" of the different instruments. Learning to allow for the limited degrees of freedom. Slow Down, move slowly and carefully like operating on a butterflies wing.' -'Changed the position and graspers' -'knots -- multiple throws, graspers -- different type or open' -'practice, palm grip the gall bladder grasper handle and squeeze the hell out of it' 'Apply endoleeps and clips for better security' 'was able to use less traumatic grasper, draining distended gall bladder' 'keep working. Ports replaced, or new instrument used; when all else fails, open pt' 'use different grasper' 'avoid using those techniques and use alternatives such as stapling.' 'either re-establish exposure by repositioning retractors correctly. Technical problems such as misplacement of --- tube. Convert to open' 'use disposable scissors, more retractors, graspers with better teeth, better exposure' 'make sure you know the anatomy and tissues behind your dissection or grasper site. Same as open surgery.' 'patience! Sometimes changing instruments' 'I try to take extra care in positioning the ports. I practice tying using the black box' 'Be really careful where you place the trocars and avoid intra-corporeal suturing where possible. Why? to make the procedures as easy as possible. Easy surgery is good surgery' 'open completion if any problems (no other option)' 'just ongoing effort to do things' 'sharp scissors--- accurate cutting, suturinglknot tying--keep practicing! Reposition slipped structures/instruments frequently to prevent injury etc.' 'training and experience' 'Don't be afraid to use more trocars or reposition them if standard or recommended ones don't seem to be working' 'time' 'continue to reapply' 'better maintenance' 'I have not altogether eliminated these problems. However, newer instruments appear to be more user friendly' 'New instruments' 'suction and wash, and re-apply. Weak clips. Open operation (rarely), pressure with bleeding--then cliplsuture' 'error delay procedures but technical equipment failures difficult to resolve intraoperatively' 'Better instruments which are sharper. Practice. Practice. Make as many ports as necessary. Better instruments' 'There is no correction. You accept a certain amount of injury' 'Open surgery. Persistence' 'Precise dissection' 'it takes time to learn the skills' 'avoid suturing (use staples). Tried 3D system (expensive)' 'Proper instrumentation helps-- but our Children's Hospital can't afford all the proper equipments' 'Experience or lack of it is usually the problem' 'Try again' 'Drain gall bladder .. .'

2 1 2 'increase awareness and with increased care, practice, practice, and practice. Practice, practice, practice, practice, practice, practice. Increase care and different graspers.' 'check errors repeatedly' 'Changing endoscope into different port position.' 'swivel scissors help. Deliberate moves, don't rush helps; instrument position or adddition of retractors helps.'

2 1 3 23. In your opinion, how can the instruments be redesigned to improve performance during surgery?
23a. Graspers:
-already much improved -more like vascular clamps (non-crushing0 -different instruments (ie. graspers/scissors) should have different colorlmarking so inadvertent use of scissors as clamp is circumvented -wider and more teeth -basically all instruments need to have rotation features -improve mechanism to improve grasp without tearing -better grasp -longer jaws with more motion, graded response to pressure -durability -find the best type of jaws -- Debalcey? forceps may be the answer -better grip on tissue-- graduated pressure -better teeth and lock mechanisms -better locking devices to accommodate varying tissue thickness -re-design the grasping end--Don't use scissor type mechanisms -better tips that would grasp without cutting through -better efforts by product companies -better teeth, more reliable ratchets -need to be stronger -- less 'slip off (but not rough) -finer -instrument that does not damage and grasps -use small multiple teeth for enough surface to hold tissue -wider and deeper surface area -more M.A. for better surer grip -lighter touch -more sturdy construction/better self-retaining mechanisms -adjustable curve for handling -There is always personal preference, and there is always room for refinements in design (to date have been improvements) -stronger and with teeth that work for prolonged holding -instruments should be designed so that the operator can hold and use these instruments with his hands and the arms in a position which is comfortable. -closing angle on jaws. {with space near the joint) -more --- of teeth -better interaction between jaws -bigger f m e r jaws -different tissue graspers -better jaws -sturdier -longer jaws, deeper but blunt teeth -relate to muscle groups performing function, new materials -make them less traumatic, different angulation -larger grasping surface in certain situations -need two types of graspers, light weight for maximum feel, heavy for tougher tissues -presently ok -serrated grasping surface, longer blades, better locking -change the shape, different types of teeth, and insulate to the tip -broader, less traumatic

23b. Needle drivers:
-better handle design -relate to muscle groups performing function, new materials -palmer grip best -rotation and angualtion -better grasp of needle -to hold needles more securely -easier manipulation -needles do not slip -instruments should be designed so that the operator can hold and use these instruments with his hands and the arms in a position which is comfortable. -to hold needle better is main problem -firmer grip on needle -better grasp -new auto-suture needle driver eliminates many previous difficulties -change centre of gravity -may be these need completely new designs, eg. 2-3 curves -finer -need to be strong but easy to 'work' -perhaps a groove for easier needle grasping -better effort by product companies -use staples -manoeuverability -0k -autosuturer, new one is --- -pivoting heads -improve driver to avoid rotation of needle -need to have rotating feature -sewing machine stapes -adequate -presently ok
23c. Scissors:
-no fault -finer quality of disposables -more curve -rotating features -fine -finer apposition of blades -better forging so they stay sharp -no problems -the biggest problem is maintaining sharpness -maintain sharp -sharpen them -presently ok -adequate -better effort by product companies -maintain sharpness -need to be sharp but respond to get the taugh -finer -these may need to be finely serrated that tissue does not slip while being cut -may help if scissors could be angled along with rotation

-thinner blades -better quality materials, exchangeable parts -disposable/reusable combination with economical replacement of I--- end' -nothing special -instruments should be designed so that the operator can hold and use these instruments with his hands and the arms in a position which is comfortable. -blades that can be sharpened or replaced -current are fine -0k -about 20% longer blades -stronger -relate to muscle groups performing functions, new materials -different angulation -improved degrees of freedom

2 1 6 24. Do you think the amount of time spent in learning to use the instruments in endoscopic surgery could be reduced? How?
-simulation -use animal lab regularly -no -no -no -no -no -probably with the introduction of 3D technology -yes, with improved designs of instrument, better visibility with 3D cameras, better cutting and coagulating instruments, eg. laser, ultrasonic scalpels, etc. -no -no. If anytlung the time learning should be increased. Some of the setups used at courses--for example suturing and knot tying, should be available in hospitals for practicing skills. No instrument manufacturer has shown us anything to date that would be helpful. -no -games using spatial orientation -more practice -no -more visiting surgeons with large experience -no -no. Perhaps computer generated tasks would make learning less time-consuming -no -yes, computer simulation -not really. Coordination is more important than the instruments -no -not sure -proper introduction of instruernnts prior to performing surgery. Sample instruments for practice. Surgeon, and not a 'non surgeon' should choose instruments that are purchased by hospitals. -interprofessional experience -no -no -camera and other models -endoscopic trainers -no -by practicing on a good inanimate model (not yet been developed) by 'choreographed' key or 'nodal' movements derived from careful task anlaysis, particularly important for suturing. -I feel the of time needed to use the instruments cannot be reduced as it is individual aptitude, but it can be helped with designing them to reach the tissue level easier. -lab time, virtual reality -no -no -no -no -no, learning comes necessary ---better trainees for OR'S to learn the techniques in the inanimate lab -yes, by --- or interactive technology, virtual reality -self learning with black box
217 -once you oriented well with the screen and hands and lighting, also know how to expose the op. site-- the rest of dissection, cut, etc. do not need to learn, the feeling is the same as open surgery -no, time and learning curve cannot be 'cheated'. -no. It is only by practice that you can become proficient and develop a feel of the tissue. -only constent practice helps-- no real shortcuts that I can think of. -probably no. the techniques are not easily learned by some surgeons. distant manipulation is troublesome for others, although those taking training are interested in using techniques (also nowadays patient preference is 80% in favour of small incisions and early mobility -- ie. thus almost mandatory for young surgeons. -question is incorrect! One has to create a sterotype, and thus require time, work is different for people -perform basic skills-- video endoscopy useful in establishing video laparoscopic skills, master basic skills with lap. choyappend. -yes. better instruments, easier exposure (in training) -probably not,-- teach young -no, more time required -practice and experience displays slight technical advantages and placement of instruemtns -I am certain a 3D camera system will eliminate most problems and also eliminate accidents! -no. It takes time to accommodate, patience is a virtue -no. young surgeons/residents need time and volume of cases. -much is dependent on an individual's own learning curve and aptitude. Good equipment and access to labs to practice is probably the best way to reduce learning time -no

2 1 8 25. Additional comments about endoscopic instruments for performing surgical tasks?
-they are constantly being improved by the instrument companies--some are 'overdesigned' -good luck. Money seems to be the limiting factor in pediatric laparoscopic surgery -major ongoing evolution in endoscopic surgery, which itself is only a few years old (as we know it now) -usually a poor carpenter blames his tools. A good carpenter can do good work with basic instruments -- not too fancy and not too high tech. and expensive! -good suction devices! -I believe that we are at the beginning of the age of endoscopic surgery. The instruments available now, I think, are crude and there is a long way to go in terms of refinement and development -I am sorry but the structure of this survey does not allow the most appropriate response -universal tool is required to do all tasks. It should be powered. 3D visual -the purpose of this questionnaire evades me. Some questions really have no application or appropriate answer -this is a very poorly designed questionnaire. What on earth can you possibly learn from this? -there is a great deal of money to be made in selling these instruments. Therefore, the instrument companies are making great efforts to perfect these instruments and have hired expert design personnel. You appear to be competing with well funded private enterprise. The new instruments now available are much superior to the instruments which we purchased at the beginning of laparoscopic cholecystectomies. -Tragically, I find the questions ambiguous and poorly worded. Has a laparoscopic surgeon been involved in the design of the questionnaire? I would like to help but I find the ambiguities too difficult to understand. -You should come and observe some procedures -time consuming-- particularly for hernias and bowel work. -get to know the instruments helpful using in vivo -the 'wave of the future', but must be tempered by judgements and constant assessment and compared always to open technique--esp in ---? -too many companies out there trying to make a quick 'buck' but in reality, know very little about our needs! Your help in designing instruments with input from 'operating' surgeons and Nurses will go a long way to produce better instrument. The New Third Generation instruments are certainly an improvement -I read about the AESOP ergometric camera holder which sounds like a great improvement. I feel that most endoscopic procedures can accomplish more if a singer operator had more control -some place for automation and ---? -better suction -- irrigation -- cautery combinations would make dissection much cleaner and safer. -self-cleaning endoscopes, laparoflators with exhaust circuit to remove smoke, robotic insturments to hold scopes, retractors, etc. -certainly is a major advance in mobilization (early discharge) of patients (fees beds). Well accepted by patients and finally surgeons. Patients (who are will) are able to return to work much earlier that after open surgery. Generally, I believe less morbidity with endoscopy (complications not withstanding) -I believe the use of endoscopy is limited to a few dey specific procedures except in experimental development surgery. Lap gall bladder, Nissen, reconstruction of Hartman, recurrent or primary hernia, appendectomy all good -- not take too long or are not safe or compromise cure (ie. cancer)

2 19 -need new instrument to help to expose operative site--eg. hold up or retract liver away; push and hold small bowel away, etc.--IN fact, I am interest to participate and develope instruments the endo-surgery -better carneralinsufflation -they are slowly improving -at present the instruments are too much like the standard open instruments. They will need to take on their own unique character and appearance, rather like the cars of today which bear little resemblance to the original 'horseless carriage'. The latter however were similar to horse drawn carriages without the horses -I am of the opinion that laparoscopic surgery by well trained people is the way to go. However young surgeons who have not done much open surgery should have enough experience here or mistakes will be made. It is an entirely different technique

2 2 0
REFERENCES
Ada, L., Canning, C. G., Carr, J. H., Kilbreath, S. L., and Shepherd, R. B. (1994).
Task-specific training of reaching and manipulation. In K. M. B. Bennett & U.
Castiello (Eds.), Insights into the reach and grasp movement (pp. 239-265).
Amsterdam: Elsevier Science.
Ballie, J. (1992). Gastrointestinal endoscopv: basic principles and practice. Oxford:
Buttenvorth-Heinemann Ltd.
College of Physicians and Surgeons of British Columbia. (1994). BC Medical directory.
Crosthwaite, G., Chung, T., Dunkley, P., Shimi, S, and Cuschieri, A. (1995).
Comparison of direct vision and electronic two- and three-dimensional display
systems on surgical task efficiency in endoscopic surgery. British Journal of
Surgery, 82, 849-85 1.
Cunningham, H. A. & Welch, R. B. (1994). Multiple concurrent visual-motor mappings:
implications for models of adaptation. Journal of Experimental Psvchologv:
Human Perception and Performance. 20 (3,987-999.
Cuschieri, A. E. (1993). Hiatal hernia and reflux esophagitis. In J. G. Hunter & J. M.
Sackier (Eds.), Minimally invasive surgery (pp. 87-1 12). New York: McGraw-
Hill, Inc.
Cuschieri, A., Buess, G., and Perissat, J. (Eds.). (1992). Operative manual of
endoscopic surgery. Germany: Springer-Verlag.
Cuschieri, A., Nathanson, L. K., and Shimi, S. M. (1992). Laparoscopic antireflux
surgery. In A. Cuschieri, G. Buess, and J. Perissat (Eds.), Operative manual of
endoscopic surgery (pp. 280-297). Germany: Springer-Verlag.

2 2 1 Cutkosky, M. R., & Howe, R. D. (1990). Human grasp choice and robotic grasp
analysis. In S.T. Venkatararnan, & T. Iberall (Eds.), Dexterous Robot Hands (pp.
5-3 1). New York: Springer-Verlag.
Ethicon Endo-Surgery (1993). Product catalog and mice list. Johnson & Johnson
Company.
Gibson J. J. (1962). Observations on active touch. Psychological Review, 69,477-491.
Greenberg, L. & Chaffin, D. B. (1977). Workers and their tools: a guide to the ergonomic
design of hand tools and small presses. Pendell, Midland, Michigan.
Harrison, B. L., Owen, R. and Baecker, R. M. (1994). Timelines: an interactive system
for the collection and visualization of temporal data. Proceedings of the Graphics
Interface '94 Conference (pp. 17 1 - 178). Banff, Alberta.
Hunter, J. G. & Sackier, J. M. (Eds.). (1993). Minimally invasive surgery. New York:
McGraw-Hill, Inc.
Jeannerod, M. (1984). The timing of natural prehension movements. Journal of Motor
Behavior. 16, 235-254.
Johansson, R. S., & Cole, K.J. (1992). Sensory-motor coordination during grasping and
manipulative actions. Current O~inion in Neurobiol0&,815-823.
Kirsh, D. & Maglio, P. (1994). On distinguishing epistemic from pragmatic action.
Cognitive Science, 18,513-549.
Konz (1974). Design of hand tools. In Human Factors Society, Proceedings of the
Human Factors Society 18th Annual Meeting (pp. 292-300). California: Santa
Monica.

2 2 2 Kunesch, E., Binkofski, F., & Freund, H. J. (1989). Invariant temporal characteristics of
manipulative hand movements. Ex~erimental Brain Research. 78,539-546.
Lederman, S.J., & Klatzky, R.L. (1987). Hand movements: a window into haptic object
recognition. Cognitive Psychology,19,342-368.
MacKenzie, C.L., & Iberall, T. (1994). The grasping hand. Amsterdam: Elsevier
Science.
J Melzer, A., Buess, G., & Cuschieri, A. (1992). Instruments for endoscopic surgery. In
A. Cuschieri, G. Buess, & J. Perissat (Eds.), Operative manual of endoscopic
surgery (pp. 15). Springer-Verlag.
Mital, A. (1991). Hand tools: injuries, illnesses, design, and usage. In A. Mital & W.
Karwowski (Eds.), Workspace, eauipment and tool design (pp. 219-256).
Amsterdam: Elsevier Science.
Nagy, A. G. & Payandeh, S. (1994). Endoscopic end-effectors. The American Societv of
Mechanical Engineers National Design Engineering Conference, March 1994.
Napier, J. R. (1980). Hands. Nevk York: Pantheon Books.
Pearl, R. K. (Ed.). (1984). Gastrointestinal endoscopy for surgeons. Little, Brown and
Company.
Perissat, J. (1992). Laparoscopic cholecystectomy. In A. Cuschieri, G. Buess, and J.
Perissat (Eds.), 0 erative manual of endoscopic surgery @p. 209-232). Germany:
Springer-Verlag.
Pier, A. & Gotz, F. (1992). Laparoscopic appendectomy. In A. Cuschieri, G. Buess,
and J. Perissat (Eds.), 0 erative manual of endoscopic surgery (pp. 194-208).
Germany: Springer-Verlag.

2 2 3 Pietrabissa, A., Scarcello, E., Carobbi, A., and Mosca, F. (1994). Three-dimensional
versus two-dimensional video system for the trained endoscopic surgeon and the
beginner. Endoscopic Surgery. 2, 3 15-3 17.
Pollak, R. (1984). Laparoscopy. In R. K. Pearl (Ed.), Gastrointestinal endoscopy for
surgeons (pp. 8 1-90). Little, Brown and Company.
Poulton, E. C. (1956). The precision of choice reactions. Journal of Experimental
Psvchologv, 5 1, 98-102.
Rininsland, H. H. (1993). Basics of robotics and manipulators in endoscopic surgery.
Endoscopic Surgery, 1, 1-3.
Sackier, J. M. (1993). Laparoscopic cholecystectomy. In J. G. Hunter & J. M. Sackier
(Eds.), Minimally invasive surgery (pp. 213-230). New York: McGraw-Hill, Inc.
Salthouse, T. S. (1991). Expertise as the circumvention of human processing limitations.
In K.A. Ericssons, & J. Smith (Eds.), Toward a general theory of expertise:
prospects and limits (pp. 286-300). New York: Cambridge University Press.
Satava, R. M. (1993). High tech surgery: speculation on future directions. In H.G.
Hunter, & J.M. Sackier (Eds.), Minimally invasive surgery (pp. 339-348). New
York: McGraw-Hill, Inc..
,, Schueneman, A. L. & Pickleman, J. (1993). Neuropsychological analyses of surgical
skills. In J. L. Starkes & F. Allard (Eds.), Cognitive issues in motor expertise
(pp. 189- 197). Amsterdam: Elsevier Science Publisher.
Shackel, B. (1984). The concept of usability. In J. Bennett, D. Case, J. Sandelin, and M.
Smith (Eds.), Visual dis~lav terminals. Usability issues and health concerns (pp.
1-29). Englewood Cliffs, NJ: Prentice Hall.

224 Soper, N. J. (1993). Laparoscopic general surgery -- past, present, and future. Surgery,
Szabo, Z. (1993). Laparoscopic suturing and tissue approximation. In J. G. Hunter & J.
M. Sackier (Eds.), Minimally invasive surgery - (pp. 14 1 - 156). New York:
McGraw-Hill, Inc.
Szabo, Z., Hunter, J., Berci, G., Sackier, J., and Cuschieri, A. (1994). Analysis of
surgical movements during suturing in laparoscopy. Endoscopic Surgery. 2, 55-
61.
Tendick, F., Jennings, R. W., Tharp, G., and Stark, L. (1993). Sensing and
manipulation problems in endoscopic surgery: experiments, analysis, and
observation. Presence. 2 (I), 66-81.
Wickens, C. D. (1992). Engineering Psychologv and Human Performance (2nd Ed.) (pp.
17). New York: Harper Collins Publishers.
Wilson, J. R. & Corlett, E. N. (Eds.). (1990). Evaluation of human work: a practical
ergonomics methodolow. London: Taylor & Francis.