
A targeted oncology company developing a pipeline of ... V2 .pdf · A targeted oncology company...
31
JEFFERIES GLOBAL HEALTHCARE CONFERENCE CHARLES BAUM, M.D., PH.D., PRESIDENT AND CEO JUNE 2015 A targeted oncology company developing a pipeline of cancer therapies for select patient populations.
Transcript of A targeted oncology company developing a pipeline of ... V2 .pdf · A targeted oncology company...

JEFFERIES GLOBAL HEALTHCARE CONFERENCE
CHARLES BAUM, M.D., PH.D., PRESIDENT AND CEO
JUNE 2015
A targeted oncology company developing a pipeline of cancer therapies for select patient populations.

Safe harbor statement
2
Certain statements contained in this presentation, other than statements of fact that are independently verifiable at the date hereof, contain “forward-looking” statements, within the meaning of the Private Securities Litigation Reform Act of 1995, that involve significant risks and uncertainties. For more detailed disclosures and discussions regarding such forward looking statements, please refer to Mirati’s filings with the U.S. Securities and Exchange Commission (“SEC”), including without limitation Mirati’s filings on Forms 10-K, 10-Q, and 8-K. Forward looking statements are based on the current expectations of management and upon what management believes to be reasonable assumptions based on information currently available to it. Such statements can usually be identified by the use of words such as "may," "would," "believe," "intend," "plan," "anticipate," "estimate," “expect,” and other similar terminology, or by statements that certain actions, events or results "may" or "would" be taken, occur or be achieved. Such statements include, but are not limited to, statements regarding Mirati’s development plans and timelines, potential regulatory actions, expected use of cash resources, the timing and results of clinical trials, and the potential benefits of and markets for Mirati’s product candidates. Forward looking statements involve significant risks and uncertainties and are neither a prediction nor a guarantee that future events or circumstances will occur. Such risks include, but are not limited to, potential delays in development timelines or negative clinical trial results, reliance on third parties for development efforts, changes in the competitive landscape, changes in the standard of care, as well as other risks described in Mirati’s filings with the SEC. We are including this cautionary note to make applicable, and to take advantage of, the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 for forward-looking statements. The information in this presentation is given as of the date above and Mirati expressly disclaims any obligation to update or revise any forward-looking statements, whether as a result of new information, future events or otherwise, unless required by law.
Proven Targeted Oncology Strategy
Accelerated Development Approach
• Targeting genetic and epigenetic drivers of cancer
• Treating intrinsic and acquired mechanisms of resistance to targeted therapy
• Experienced and proven management team
• Creative and agile clinical development
ACCELERATED APPROVAL
FULL APPROVAL
Expanded indications
Genetically-defined patients
Mirati develops molecularly targeted oncology therapies for patients with cancer-driving genomic alterations
3

4 All programs owned by Mirati except certain Asian rights to Mocetinostat – Partnered with Taiho.
CANDIDATE/ INDICATION
PRIMARY TARGETS PRECLINICAL PHASE I PHASE 1b -
PHASE 2 REGISTRATION
TRIAL
MGCD265 Non Small Cell Lung Cancer (NSCLC) MET
Axl MGCD265 Solid tumors
MGCD516 Solid tumors
RET DDR Trk
Mocetinostat Bladder Cancer
HDAC 1,2,3,11 Mocetinostat
Diffuse Large B-Cell Lymphoma (DLBCL)
KIN
ASE
PRO
GR
AMS
EPIG
ENET
IC
PRO
GR
AM
Mirati is advancing multiple targeted oncology clinical pipeline programs

MGCD265 Multi-Targeted Kinase Inhibitor

6
MGCD265
MET plays a key role in NSCLC
*Raghav KPH, et al, Translational Lung Cancer Research 1.3 (2012):179-193. **Mirati data on file and Paik PH., et al. Cancer Discovery. Online May 13, 2015. Last accessed May 14, 2015 at http://cancerdiscovery.aacrjournals.org/content/early/2015/05/13/2159-8290.
• Higher MET expression rates correlate with advanced stages of tumor progression and poor clinical outcomes*
• Historical efforts to target MET generated inconsistent results due to incorrect development strategies as well as molecular challenges – MET protein overexpression by IHC versus MET genetic alterations – Driver alterations are more effectively targeted by small molecules
MET’s ROLE IN CANCER
• MET is a driver of tumor growth when it is genetically altered and activated by point mutations, exon 14 deletions and gene amplification in NSCLC patients** – MET mutations transform cell lines – Inhibition of MET mutations in xenograft models leads to tumor regression – MET mutations do not overlap with other drivers (e.g., ALK, ROS, EGFRm)
MET IN NSCLC
7
MGCD265
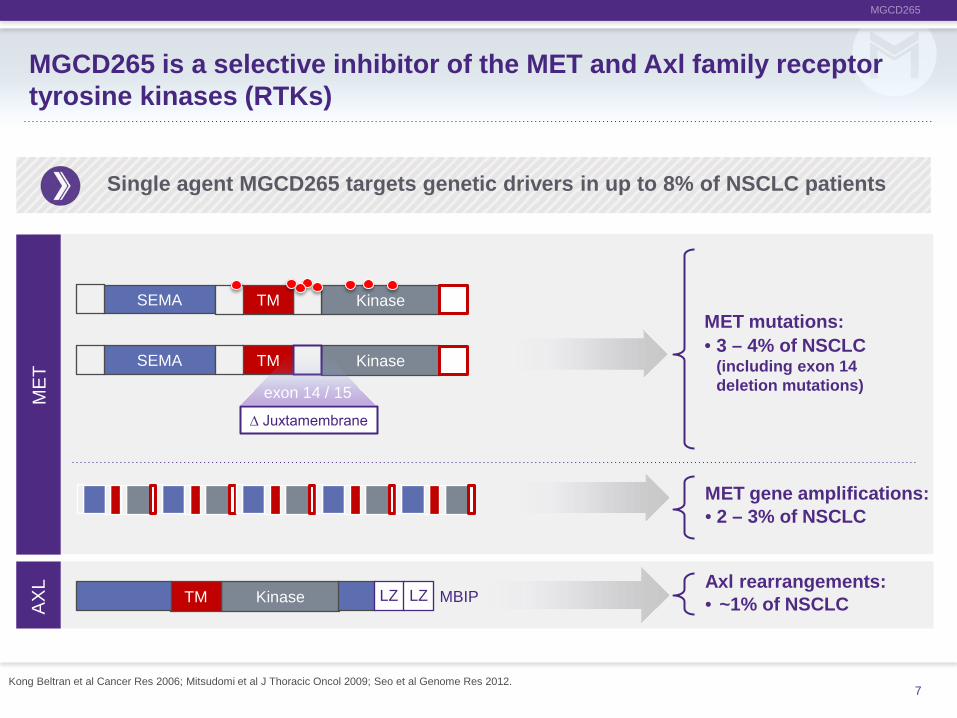
• 3 – 4% of NSCLC (including exon 14 deletion mutations)
MBIP
∆ Juxtamembrane
Kinase TM SEMA
• ~1% of NSCLC
MET mutations:
Kinase TM LZ LZ
MET
AX
L
Kinase TM SEMA
exon 14 / 15
• 2 – 3% of NSCLC MET gene amplifications:
Axl rearrangements:
MGCD265 is a selective inhibitor of the MET and Axl family receptor tyrosine kinases (RTKs)
Single agent MGCD265 targets genetic drivers in up to 8% of NSCLC patients
Kong Beltran et al Cancer Res 2006; Mitsudomi et al J Thoracic Oncol 2009; Seo et al Genome Res 2012.

8
MGCD265
ASCO 2015 abstract # 2589.
MGCD265 preclinical data in MET mutation and MET gene amplification xenograft models increase our confidence in targeted approach
MET Exon 14 Deletion PDX Lung Cancer Model
Start of treatment
MET Amplified Gastric Cancer Model
1000
2000
3000
0 8 16Treatment Day
Tum
or v
olum
e (m
m3 )
04 12
MGCD265 60 mg/kg QD
Vehicle
Start of treatment
Vehicle
MGCD265 60mg/kg QD
Start of treatment
Day Post Tumor Implantation
9
MGCD265
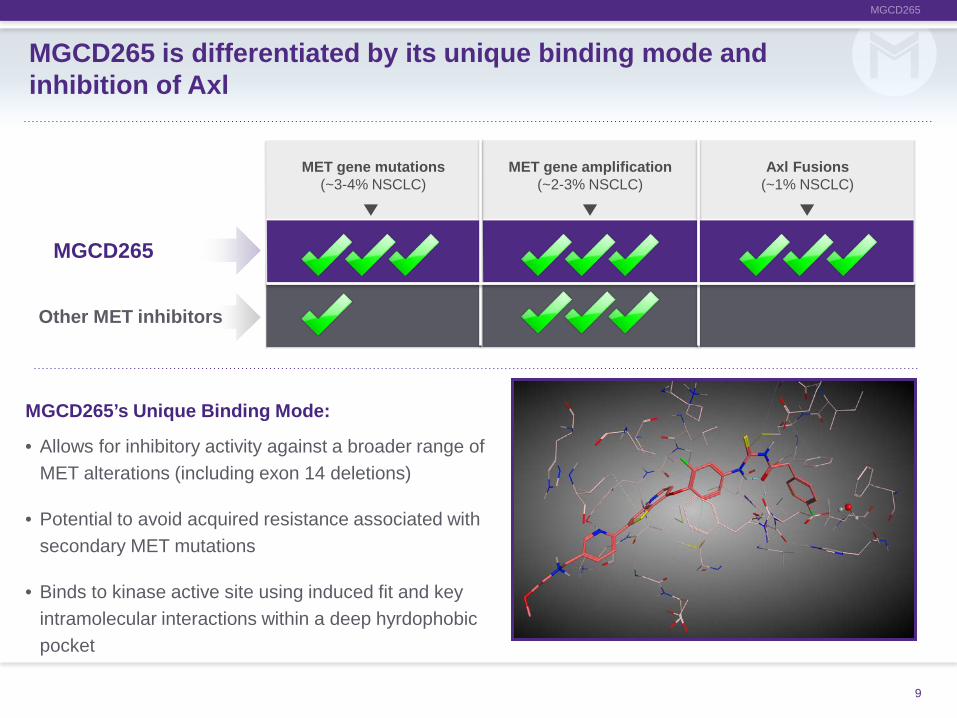
MGCD265 is differentiated by its unique binding mode and inhibition of Axl
MGCD265’s Unique Binding Mode:
• Allows for inhibitory activity against a broader range of MET alterations (including exon 14 deletions)
• Potential to avoid acquired resistance associated with secondary MET mutations
• Binds to kinase active site using induced fit and key intramolecular interactions within a deep hyrdophobic pocket
MGCD265
Other MET inhibitors
MET gene mutations (~3-4% NSCLC)
MET gene amplification (~2-3% NSCLC)
Axl Fusions (~1% NSCLC)

10
MGCD265
Phase 1 dose escalation study of MGCD265 achieved >90% inhibition of targets, and MTD of 1050 mg BID was well tolerated
Part 2: Dose expansion
• Patients with genetic alterations in MET or Axl
Cohort 1 N = 3 600mg BID
Cohort 2 N = 6 1200mg BID
Cohort 3 N = 3 1050mg BID
1050mg BID MTD / RP2D
• 2 DLTs • Grade 3 fatigue • Grade 3 diarrhea
• No DLTs
ClinTrials.gov identifier: NCT00697632.

11
MGCD265
MGCD265 dose expansion study is ongoing
Expansion Cohort 2 2nd-line Solid tumors (e.g., gastric cancer)
Expansion Cohort 1 2nd-line NSCLC
NGS screen for patients with:
•MET mutations •MET gene amplifications •Axl rearrangements
NSCLC
Other solid tumors
ASCO 2015 abstract #2589. ClinTrials.gov identifier: NCT00697632.
Initial clinical data confirm our targeted approach, resulting in tumor regression in NSCLC patients selected for MET genetic alterations.
12
MGCD265
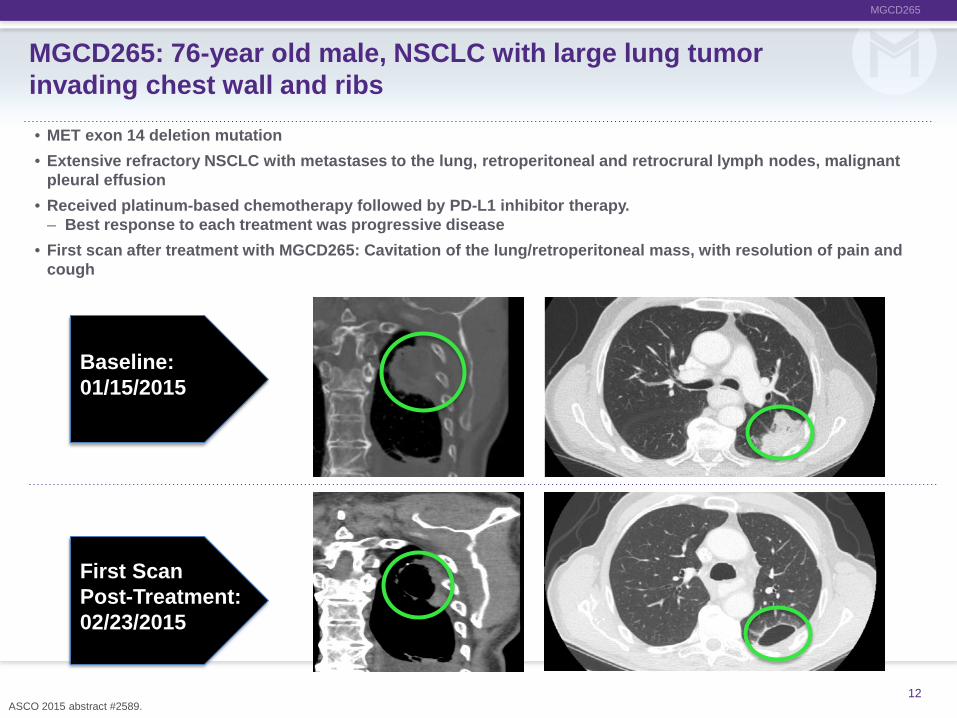
MGCD265: 76-year old male, NSCLC with large lung tumor invading chest wall and ribs
Baseline: 01/15/2015
First Scan Post-Treatment: 02/23/2015
• MET exon 14 deletion mutation
• Extensive refractory NSCLC with metastases to the lung, retroperitoneal and retrocrural lymph nodes, malignant pleural effusion
• Received platinum-based chemotherapy followed by PD-L1 inhibitor therapy. – Best response to each treatment was progressive disease
• First scan after treatment with MGCD265: Cavitation of the lung/retroperitoneal mass, with resolution of pain and cough
ASCO 2015 abstract #2589.

MGCD265
MGCD265: 70-year old female, NSCLC with liver metastases
ASCO 2015 abstract #2589. 13
Baseline: 12/15/14
First scan post-treatment: 1/29/15
• MET exon 14 deletion mutation
• Liver metastases and right pulmonary lesion
• Underwent neoadjuvant chemoradiation followed by radical pneumonectomy for T3N1 disease, received chemoradiation for pleural and bone metastases, Stereotactic Body Radiation Therapy (SBRT) for pulmonary metastasis and resection of recurrence in the colon
• First scan after treatment with MGCD265: Extensive tumor necrosis and regression

14
MGCD265
MGCD265: 51-year old female, NSCLC with large lung tumor, bone and brain metastases
• MET amplification
• Refractory metastatic lung cancer with extensive lung disease
• Received EGFR inhibitor, chemotherapy and whole brain radiation
• First scan after treatment with MGCD265: Tumors in the lung showed regression
Baseline: 3/5/2015
First scan post-treatment: 4/13/2015
ASCO 2015 abstract #2589.

Initial data show preliminary evidence of clinical efficacy in heavily pretreated NSCLC patients with MET gene alterations
15
CONCLUSIONS
• MGCD265 is tolerable at the MTD of 1050 mg BID. Exposures achieved with this dose result in >90% inhibition of MET and Axl based on preclinical predictions and the biomarkers sMET and sAxl
• The first 3 patients (two with MET exon 14 deletion mutations and one with MET amplification) demonstrated tumor regressions
• Enrollment continues: – Patients with NSCLC with MET exon 14 deletions or MET gene
amplification – Patients with other solid tumors with genetic alterations of interest

16
MGCD265
We anticipate initiating the Phase 2 registration-enabling study for MGCD265 monotherapy in NSCLC by the end of 2015
Tissue or blood NGS screen for patients with:
• MET mutations • MET gene amplifications
• Open label, parallel-arm study of MGCD265
• Target Population: Recurrent or metastatic NSCLC with activating genetic alterations of MET with at least one prior treatment with a platinum based combination therapy
• Multinational: U.S., Canada, Europe and Asia
• Primary Endpoint: Objective Response Rate (ORR)
• Secondary Endpoint: Progression Free Survival (PFS)
We believe ORR >40% could lead to accelerated approval in 2nd-line setting for NSCLC followed by a confirmatory trial in 1st-line.
2nd-line NSCLC: MET mutations
2nd-line NSCLC: MET gene amplifications

17
MGCD265
MGCD265 has significant single agent NSCLC market opportunity
Mirati data on file; TCGA; AACR 2015 abstract #1118.
NSCLC Driver Alterations
MET amplifications
MET mutations
Axl rearrangements 1%
3.5%
3%
ALK4%
BRAF4%
ROS1%Her21%
MET amp 3%
MET mut 3.5%
Axl 1%
Other & Unknown42%
KRAS25%
EGFR15%
US NSCLC Annual Incidence: 191,000 Target population: 15,300
MET and Axl genetic alterations comprise up to 7-8% of NSCLC
• MET mutations: ~3.5% • MET amplifications: ~3% • Axl rearrangements: 1% Axl rearrangements 1%
T790M+ 7.5%
T790M - 7.5%

18
MGCD265
• Resistance is mediated through mutation and/or overexpression of alternative RTK targets and pathways, including MET and Axl
• Research shows that EGFR kinase inhibitor resistance can be reversed in vivo by combined EGFR and MET/Axl inhibition, a finding that validates combination therapy with EGFR and MET/Axl inhibitors to address therapeutic resistance
All tumors eventually become resistant to EGFR therapy
MGCD265 plus an EGFR/T790m inhibitor combination could target the majority of EGFR resistance in NSCLC
*Turke AB, et al. Cancer cell 17.1 (2010): 77-88., Zhang Z. et al. Nature Genetics 44.8 (2012): 852-862., Byers L.A., Diao L., Wang J., et al. Clinical Cancer Res 19. (2013): 279-290. Published online first Oct. 22, 2012.
Adapted from Gibbons, DL. Cancer Discov, 2014

19
MGCD265
Single agent MGCD265, and in combination with a 3rd-generation EGFR inhibitor, could treat a significant NSCLC patient population
NCI SEER, Mirati Data on File. *30% in Asia.
Annual NSCLC Incidence
191,000**
AXL 1%
MET 7%
EGFRm >15%*
EGFRm positive
MET and/or Axl positive
T790m positive
T790m negative
• MGCD265
• Initial focus: Accelerated approval for 2nd-line, followed by 1st-line
• Patients:15,300
• T790m inhibitor
• Initial focus: Accelerated approval for 2nd-line
• Patients: ~14,300
• MGCD265 + T790m inhibitor
• Initial focus: Accelerated approval for 2nd-line
• Patients: ~14,300
• T790m inhibitor
• MGCD265 + T790m inhibitor
• 1st-line expansion potential
• Patients: 28,650
15%
8%
50%
50%

20
MGCD265
Single agent MGCD265 has the potential for accelerated approval in NSCLC, gastric cancer and in combination with EGFR inhibitor
2015 2016 2017 2018 Si
ngle
Age
nt
ACCELERATED APPROVAL
2nd Line NSCLC Dose Expansion POC
in NSCLC & Solid Tumors
NSCLC: 2nd Line Phase 2 Registration Trial (MET mutations and MET gene amplification)
Combination Dose Expansion POC in NSCLC
Combination Study NSCLC 2nd Line Trial C
ombi
natio
n w
ith T
790m
in
hibi
tors
NSCLC: Confirmatory Randomized Trial in 1st Line for Full Approval
Solid Tumors (e.g. gastric): 2nd Line Phase 2 Registration Trial
NDA SUBMISSION
2nd Line NSCLC

MGCD516 Multi-Targeted Kinase Inhibitor

22
MGCD516
POTENTIAL INDICATIONS
TRK
Kinase JM Ligand Binding
Kinase JM TPM3
Kinase JM TPR
Kinase ETV6 • Mutations in NSCLC (~1%)
TrkB/C mutations
TrkA/C fusions
RET
D
DR
• NSCLC fusions (2%)
• NSCLC (1%) (including 3-4% lung SCC)
Kinase Coiled Motor
Kinase Motor
Kinase JM Discoidin
KIF5B RET fusions
DDR2 mutations
Single agent MGCD516 targets genetic alterations in up to 4% of NSCLC patients
An et al 2012, Ding et al 2008, Doebele et al, 2014; Eguchi et al 1999, Euhus el al 2002, Greco et al 2010, Hammerman et al 2011, Harada et al 2011, Kohno et al 2012, Lipson et al 2012, Marchetti et al 2008, Phay et al 2010, Sheng et al 2001

23
MGCD516
Dose escalation study with MGCD516 in advanced solid tumors is ongoing
ClinTrials.gov identifier: NCT02219711.
Part 2: Dose expansion • NSCLC patients with genetic alterations in RET, DDR or Trk identified by NGS
• Expected to begin in second half of 2015
Cohort 1 10 mg QD
Cohort 2 20 mg QD
Cohort 3 40 mg QD
Cohort 4 80 mg QD
Cohort 5 110 mg QD
Unselected patients
Upon MTD

Mocetinostat Spectrum Selective Histone Deacetylase (HDAC) Inhibitor

25
MOCETINOSTAT
Indication Regimen Phase Patient Selection Strategy
DLBCL Single-agent
Phase 2 Ongoing
• Refractory patients with genetic alterations in CREBBP and EP300
Bladder Single-agent
Phase 2 Ongoing
• Refractory patients with genetic alterations in CREBBP and EP300
Mocetinostat’s novel HDAC development strategy centers on epigenetic patient selection
There is growing evidence that HDACs may be able to increase the efficacy of immuno-oncology therapies.* We are exploring combinations with checkpoint inhibitors. We are also exploring combinations with other epigenetic agents as a potential next step in the mocetinostat development program.
Sing
le A
gent
Po
tent
ial
Com
bina
tion
*Maeda T, et al. Blood, vol. 96., Skov et al. Cancer Research, vol.65,2005., West AC et al. Cancer Res 2013.

26
MOCETINOSTAT
Gui Y et al Nature Genetics 2011.
CH1 KIX Bromo CH2 CH3 CREBBP Acetyltransferase
EP300 Bromo KIX CH1
Splice site Insertion or deletion Nonsense Missense
CH2 CH3
CREBBP and EP300 are inactivated through loss of function mutations in a unique spectrum of cancers
Mocetinostat demonstrated complete tumor growth inhibition in non-clinical models exhibiting CREBBP and EP300 mutations
• Histone acetyltransferases (HATs), including CREBBP and EP300, are associated with gene transcription and are counterbalanced by HDACs, which are associated with gene silencing.
• Through their complimentary roles, they regulate the expression of other genes involved in cell growth, survival and differentiation.

27
MOCETINOSTAT
ClinicalTrials.gov Identifier: NCT02236195.
IF > 3 RESPONSES STAGE 1 N=15 *Patients
STAGE 2 N=33 *Patients
STAGE 3 N=100 *Patients
IF > 9 RESPONSES
Mocetinostat Phase 2 study in selected bladder cancer patients is ongoing
*Patients have inactivating mutations of histone acetyltransferase genes CREBBP and EP300.

28
MOCETINOSTAT
Sponsored Phase 2/3 Registration Study
N = 150 Patients
N = 27 *Patients
Cohort 2: Follicular Lymphoma
Cohort 1: DLBCL (Relapsed/refractory)
N = 27 *Patients
ClinicalTrials.gov Identifier: NCT02282358.
Investigator-sponsored mocetinostat Phase 2 study in selected Non-Hodgkins lymphoma patients is ongoing
*Patients have inactivating mutations of histone acetyltransferase genes CREBBP and EP300.

Summary

30
2015 is poised to be a transformational year for Mirati
*As of March 31, 2015.
PROGRAM UPDATE ESTIMATED TIMEFRAME
MGCD265
Provide additional data on efficacy and duration of response from Phase 1/1b study ONGOING
Initiate Phase 2 registration-enabling study END OF 2015
MGCD516 Identify optimal dose MID - 2015
Initiate dose expansion cohorts for Phase 1/1b study 2ND HALF - 2015
Mocetinostat Data from ongoing Phase 2 trials ONGOING
FIN
ANC
IAL*
• NASDAQ MRTX
• Shares Outstanding*: 16.1M
• Cash*: $68M

![Targeted therapies in oncology t a Serbian ... · Targeted therapies in oncology t a Serbian pharmacoeconomic perspective :}ÀvD]Zio}À] 1,2 1D]Zio}À] Health Analytics; 2Unit of](https://static.fdocuments.in/doc/165x107/5e529c79803c4c5149451c3e/targeted-therapies-in-oncology-t-a-serbian-targeted-therapies-in-oncology-t.jpg)

















