
A Summary of IAPT for Severe Mental Illness Demonstration ... · IAPT for Severe Mental Illness...
12
A Summary of IAPT for Severe Mental Illness Demonstration Site Data for Somerset Partnership Talking Therapies May 2015
Transcript of A Summary of IAPT for Severe Mental Illness Demonstration ... · IAPT for Severe Mental Illness...
A Summary of IAPT for Severe Mental Illness
Demonstration Site Data for Somerset Partnership
Talking Therapies
May 2015

2
Table of Contents
Executive Summary ............................................................. Page 3
Introduction ................................................................................... 4
Objectives ..................................................................................... 5
Findings ........................................................................................ 6
Discussion & Conclusions ........................................................... 11

3
Executive Summary
Background Somerset Partnership NHS Foundation Trust is a National demonstration site for personality disorders as part of the Improving Access to Psychological Therapies for Severe Mental Illness project. Primary and secondary care psychological therapies services in Somerset both offer treatment to people with personality disorders and those who have traits of PD, and work is continuing to ensure primary care staff, who traditionally have not worked with this client group, have awareness, knowledge and skills around working with personality disorder. This makes the Trust one of very few that are able to work with some consistency across both elements of service delivery. The service aims to ensure access to high quality and appropriate talking therapies, and interventions that are psychologically informed, for people with personality disorder or personality disorder traits at any point along their whole care pathway. This summary reports on outcomes assessed using the expanded minimum data set. A further summary will report on outcomes in secondary care. Aims This report aims to summarise the data collected in primary care from 1st November 2012 to 31st December 2014 and to present it for dissemination to local teams and practitioners. In line with the demonstration site project only outcomes for those people scoring above cut off on the SAPAS are included.1 Findings The sample included 63% of people who scored positively for personality disorder traits (had a SAPAS score >4). Overall the outcome measures show positive results. Across the measures, the majority of people show at least some improvement in their scores. On the depression and anxiety scales (PHQ9 and GAD7) most individuals show a reliable improvement, 60% and 50% respectively. The National standard recovery rates (50%) were nearly met for the PHQ9 (44%), and GAD7 (42%), for this group of people.
Patient experience, as assessed using the Patient Experience Questionnaire was positive, with the majority of individuals reporting the best possible score on all questions.
1 SAPAS The Standardised Assessment of Personality – Abbreviated Scale (SAPAS) identifies areas
such as difficulties in trusting others, forming relationships, understanding oneself and experiencing sudden changes in emotions.

4
Introduction
In 2008 the Department of Health launched the Improving Access to Psychological Therapies Programme (IAPT) to help increase public access to a range of psychological treatments for depression and anxiety that have been recommended by the National Institute for Health and Clinical Excellence (NICE). The IAPT programme, with the continued support of the Department of Health, is looking at how it can extend the benefits of improving access to psychological treatments to those with a severe mental illness. The programme’s long term aim is to ensure that all people with a psychosis, bi-polar and personality disorder, who could benefit from evidence based therapies, have access to them. To support this ambition the IAPT programme has set up the Severe Mental Illness (SMI) Project. Somerset Partnership NHS Foundation Trust has become a national demonstration site for IAPT for people with a personality disorder. This involves working with NHS England alongside two other mental health Trusts in central London in improving access to evidenced based psychological interventions for people with a personality disorder. Somerset is unique in its development and provision of a whole systems approach to working psychologically with people with personality disorder across primary and secondary care, as well as providing traditional psychological therapies in both settings within limited resources. As part of the demonstration site work we have provided a series of open days to share our practice. These open days have been used to share how we developed and implemented the Relational Recovery model and the training we have provided to all community and inpatient teams. We have set up a user forum and in collaboration with service users we have developed a website that includes information on local services, the national demonstration site work and personality disorder more generally. The Department of Health is keen for all demonstration sites to collect data and provide evidence and information regarding the impact on people’s health and wellbeing as a result of the treatment they have received. This has meant the introduction of data outcome and health utilisation booklets to the Personality Disorder Service and Psychological Therapies departments in secondary care, and the expansion of the data set collected within primary care including measures for quality of life and health and economics. Primary and secondary care psychological therapies services in Somerset both offer treatment to people with personality disorders and those who have traits of PD, and work is continuing to ensure primary care staff, who traditionally have not worked with this client group, have awareness, knowledge and skills around working with personality disorder. This makes the Trust one of very few able to work with some consistency across both elements of service delivery. We aim to ensure access to high quality and appropriate talking therapies, and interventions that are psychologically informed, for people with personality disorder or personality disorder traits at any point along their whole care pathway. As a demonstration site, we have been asked to share our good practice on how we currently work with people in

5
secondary care and how we have used this work to improve access to talking therapies and support for people experiencing emotional difficulties in primary care.
Objectives
The aim of this report is to provide a summary of the results for those people within Talking Therapies service who have a score of 4 or greater on the SAPAS.
Method
Data was pulled from IAPTUS, this included all data collected in the primary care service from 1st November 2012 to 31st December 2014. From this a sample of all people with a SAPAS score of 4 and above was extracted. The SAPAS can be used to screen for personality disorder with reasonable specificity (80% in secondary care with a cut off score of 3 and above). Although not formally validated in primary care settings it has been chosen by NHS England to screen for those with significant personality disorder traits who are being seen by primary care talking therapy services. Following discussions with the author it was agreed to be a valid measure within primary care settings with a cut off score of 4 and above. The data for each measure includes scores for all those who attended two or more appointments and who had paired scores for that particular outcome measure.
In addition, the outcomes for IAPT definitions for ‘reliable improvement’ and ‘reliable recovery’ are included for reference. It only includes people whose first scores reach ‘caseness’ (PHQ9: >/=10, GAD7: >/=8). IAPT standard recovery includes all people who move below ‘caseness’. Reliable improvement counts the number of people where both scores exceed the measurement error of the questionnaire. This currently only applies to the measures of PHQ9 (decrease by 6+ points) and GAD7 (decrease by 4+ points).
IAPT reliable recovery counts the number of people where both scores exceed the measurement error of the questionnaire and their score moves below the clinical cut-off. Currently this only applies to the measures of PHQ9 (score <10) and GAD7 (score <8).
For the other measures included, the statistical reliable change scores have yet to be determined, so the percentage improvement/ deterioration has been stated instead.
6
Findings
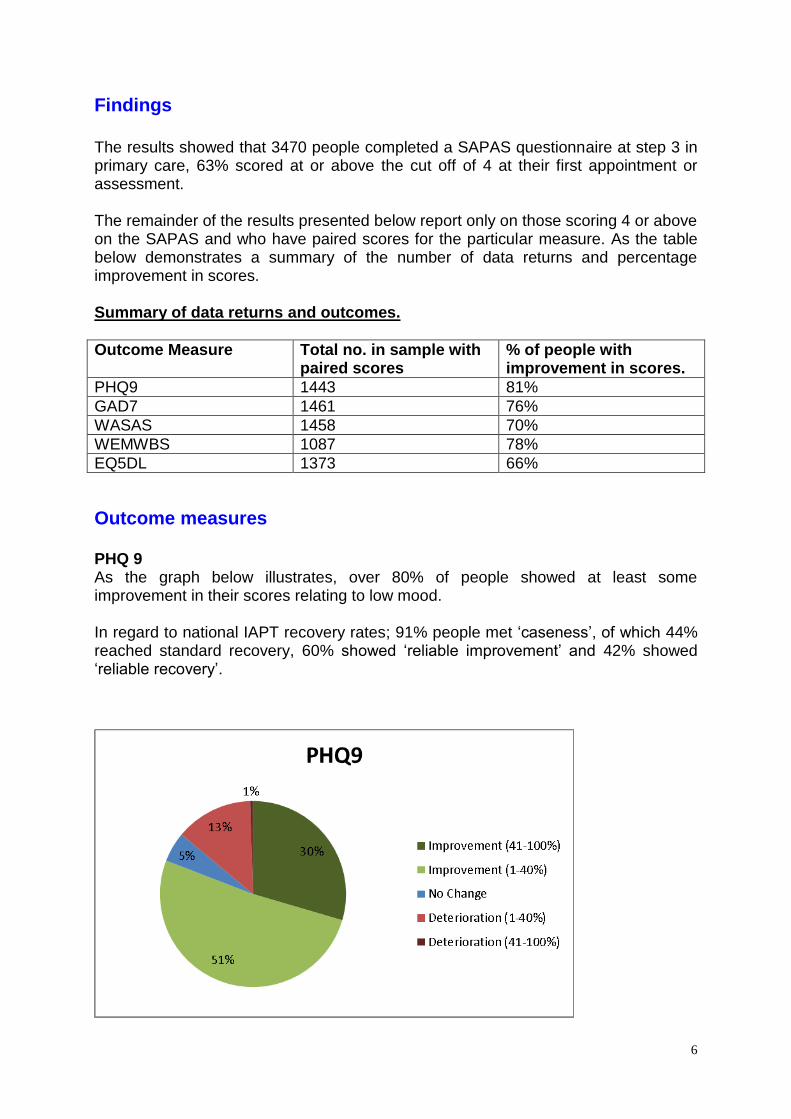
The results showed that 3470 people completed a SAPAS questionnaire at step 3 in primary care, 63% scored at or above the cut off of 4 at their first appointment or assessment. The remainder of the results presented below report only on those scoring 4 or above on the SAPAS and who have paired scores for the particular measure. As the table below demonstrates a summary of the number of data returns and percentage improvement in scores. Summary of data returns and outcomes.
Outcome Measure Total no. in sample with paired scores
% of people with improvement in scores.
PHQ9 1443 81%
GAD7 1461 76%
WASAS 1458 70%
WEMWBS 1087 78%
EQ5DL 1373 66%
Outcome measures
PHQ 9 As the graph below illustrates, over 80% of people showed at least some improvement in their scores relating to low mood. In regard to national IAPT recovery rates; 91% people met ‘caseness’, of which 44% reached standard recovery, 60% showed ‘reliable improvement’ and 42% showed ‘reliable recovery’.

7
GAD 7 Similarly to PHQ9 scores, the majority of people showed at least some improvement in their scores for generalised anxiety. In regard to national IAPT recovery rates; 92% met ‘caseness’, of which, 42% reached standard recovery, 50% showed ‘reliable improvement’ and 40% showed ‘reliable recovery’.
Work & Social Adjustment Scale (WASAS). As the graph below denotes, the majority of people showed slight to moderate improvement in scores relating to day-day functioning. Over a quarter showed some deterioration in scores.

8
Warwick & Edinburgh Mental Wellbeing Scale (WEMWBS) For the WEMWBS, the majority of people showed a slight to moderate improvement in their scores (between 1 and 40%). Only a small number showed significant improvement (greater than 41%). A notable proportion of people showed a slight to moderate deterioration, with no one showing a significant deterioration.
4%
74%
4%
18%
0%
WEMWBS
Improvement (41-100%)
Improvement (1- 40%)
No change
Deterioration (1-40%)
Deterioration (41-100%)
EQ5D5L As the graph below illustrates, more than half of people showed a slight-to-moderate improvement (1-40%) on the EQ5D5L. Some showed a slight deterioration in scores (1-40%) and very few people showed significant change (>40%) in either direction.

9
Patient Experience Questionnaire (PEQ) The graphs below show responses for the PEQ from those in the PD sample (SAPAS score 4+) who completed or dropped out of treatment. The free text feedback has not been included as this has already been reported on separately for the whole service. Friends and Family Test: The graph below demonstrates the responses (total no. 1032) to the Friends and Family Test: How likely are you to recommend this service to friends and family if they needed similar care or treatment? The vast majority of people reported being extremely likely to recommend the service.
The Friends and Family Test score was 63 on the continuum. This is calculated using a Department of Health tool where possible scores range from -100 to + 100; the nearer to +100, the more positive the response. This is slightly more positive in comparison to the result for the whole of Somerset Partnership Talking Therapies in 2013 of 57.

10
The Graph below shows the responses to each of the PEQ questions. Note only those questions reported for the national demonstration site are included, namely: Q2: Did staff listen to you and treat your concerns seriously? Q3: Do you feel that the service has helped you to better understand and address your difficulties? Q4: Did you feel involved in making choices about your treatment and care? Q6: On reflection, did you get the help that mattered to you? Q7: Did you have confidence in your therapist and his / her skills and techniques? Overall people responded very positively in regard to their experience with the service. The majority of people answered positively ‘at all times’ to each question. There were very few negative responses.

11
Discussion & Conclusions.
Overall the results presented above are positive. Across the measures, the majority of people showed at least some improvement in their scores, the scores for low mood and generalised anxiety showing the most positive results. It is heartening to see that the general IAPT national standard recovery targets (50%) are nearly met for the PHQ9 (44%), and GAD7 (42%), for this group of people. In addition, the results for reliable improvement (PHQ9 60%, GAD7 50%) and reliable recovery (42%, 40%), are positive in relation to the IAPT Year 1 results (Gyani et al 2013) who reported reliable improvement at 64% and reliable recovery rate at 40%. The patient experience questionnaire was more consistently positive with people reporting positive experiences in their responses to all questions. This was particularly true for individuals feeling listened to by staff and having confidence in therapists and their skills. It is also important to remember that the data only relates to paired scores, which can come from any point in a person’s course of treatment, thus it does not represent an actual pre and post result.

12
References
Clark, D., & Oates, M. (2014). Improving Access to Psychological Therapies. Measuring recovery in IAPT services. Version 2. NHS England. Gyani, A., Shafrana, R., Layard, R., & Clark, D. (2013). Enhancing recovery rates: Lessons from year one of IAPT. Behaviour Research and Therapy. Vol 51, 9, pg 597–606.


















