A study of 10 cases of velopharyngeal incompetence treated by flap pharyngoplasty
6
ORIGINAL / MAIN ARTICLE A STUDY OF 10 CASES OF VELOPHA RYNGEAL INCOMPETENCE TREATED BY FLAP PHARYNGOPLASTY MAHENDRA NAIK ANIL CHADHA NAYAN PAREKH VATSAL PATEL. • • :'- . ~fi :~ ~ : : ~ ~ ' ~ .~-°~- 5" -', ' '~ . " .'~ ' " " ~ /,~:~'~ --".: -" i':~ ,~''~-~'~: ~, ~" .... " - ,',.-~=~ "~":J~"~,/" .':" ' . ~ " ,~'-"~ " ~"',~ :~!.-.. ,~-! ~ .mPetence: :~vp.!o, ~s~.a ~~n?bf ~-~f~fi.Port areal!:::. i:~ " ~ !:i~; ~ : ~ ~ by Yearn and. poste~ ph~geal: ~i !~ ~ ~b~t~o~ ~a~n~ : r~lts m .. ( ~ :,~i~ ~ ~us: iy~s ~speech d~'ects, which form; t~ main : ~ ~ af ~: ~a~e~t: Wc have" ;:i !i:: :~~died O,¢ase~of - V.pI due toiPario~ caus~:~;t~..~ ~ m ! p r 6 y e n i e . nt~o~tab~ied by flap! ~ ~clopharyngeal incompetence (VPI) is a multifaceted problem, primarily caused by a wide gap between soft palate and posterior pharyngeal wall and secondarily causing upto severe degree of speech defects along with hearing defects and feeding problems. The solution to this is only a well organised multidisciplinary approach involving not only E.N.T. and plastic surgeons but also speech pathologists, linguistic experts and even dentists. Although a vast majority of causes of VPI fall under the perview of plastic surgeon, a considerable number of patients present primarily to ENT specialists, also for their nasal twang, hearing defects or similar speech problems. However, till today many E.N.T. specialists are reluctant to tackle this problem themselves. Our present study consists of 10 cases of VPI treated by flap pharyngoplasty in conjunction with plastic surgeon, speech pathologists and linguistic experts at the Department of E.N.T., Civil Hospital, Ahmedabad, India, over a period of 1. I/z years (1986 - 87). Out of limited surgical options available, either a superior or inferior based flap pharyngoplasty was done in each case. While speech was assessed by speech pathologists and linguistic experts for nasality, articulation defects and oral consonant air pressure with its recording on audio tapes. All our patients have been followed up for a minimum period of six months. We have studied 10 cases of VPI, randomly selected from ENT or Plastic O.P.D. Full assessment by detailed history and complete ENT examination was done. Radiographic cephalometry, taking standard fixed distance lateral view X-rays of skull, first in resting condition of palate and then while phonating "e...e...e..."; was done in each case. (as shown in x-ray photograph and line diagram). It helped in a unidimentional measurement of defect of V.P. port area. Nasopharyngogram was done in selected few cases to outline the defect with a radio opaque dye. Speech pathologists and linguistic experts assessed the speech and hearing of each patient preoperatively, 1 month post operatively after intensive speech therapy and 6 months post operatively. Speech records were maintained on audiotapes. The speech defects were classified and graded as shown in footnote below table, which helped in comparative evaluation of results. Two linguistic experts combindly and two speech pathologists separately evaluated each case every time before tabulating the results. Each patient was followed up for a minimum period of 6 months. VPI is an incomplete closure of V.P.port area, normally formed by velum and posterior pharyngeal wall. Mahendra Naik Honorary Professor of E.N.1 Anil Chadha Professor of Plastic Surgery Nayan Parekh Assistant Professor of E,N.T Vatsal Patel 4th Year Resident in E.N.T. BJ. MediccJi,'_allege& Civil Hospital, Ahmedabad. Address for Reprints Dr. Mahendra Naik Honorary Professor of E.N.T., Ward E-6, Civil Hospital, Asarwa, Rhmedab~d-38001< Indian Journal of Otolaryngologv, Volume 43, No. 1, March, 1991 ~]
-
Upload
mahendra-naik -
Category
Documents
-
view
215 -
download
0
Transcript of A study of 10 cases of velopharyngeal incompetence treated by flap pharyngoplasty

ORIGINAL / MAIN ARTICLE
A STUDY OF 10 CASES OF VELOPHA RYNGEAL INCOMPETENCE
TREATED BY FLAP PHARYNGOPLASTY M A H E N D R A NAIK ANIL CHADHA NAYAN PAREKH VATSAL P A T E L .
• • : ' - . ~ f i : ~ ~ : : ~ ~ ' ~ . ~ - ° ~ - 5 " - ' , ' ' ~ . " . ' ~ ' " " ~ / , ~ : ~ ' ~ - - " . : - " i ' : ~ , ~ ' ' ~ - ~ ' ~ : ~ , ~ " . . . . " - , ' , . - ~ = ~ " ~ " : J ~ " ~ , / " . ' : " ' . ~ " ,~ ' - "~ " ~ " ' , ~ : ~!.-.. ,~-! ~ .mPetence: :~vp.!o, ~s~.a ~ ~ n ? b f ~ - ~ f ~ f i . P o r t areal!:::. i:~ " ~ !:i~; ~ : ~ ~ by Yearn and. p o s t e ~ ph~geal: ~ i !~ ~ ~b~t~o~ ~ a ~ n ~ : r~ l t s m .. ( ~ :,~i~ ~ ~ u s : iy~s ~speech d~'ects, which form; t ~ main : ~ ~ af ~ : ~a~e~t: Wc have" ;:i !i:: : ~ ~ d i e d O,¢ase~of - V.pI due toiPario~ c aus~:~;t~.. ~ ~ m ! p r 6 y e n i e . nt~o~tab~ied by flap! ~
~ c l o p h a r y n g e a l incompetence (VPI) is a multifaceted problem, primarily caused by a wide gap between soft palate and posterior pharyngeal wall and secondarily causing upto severe degree of speech defects along with hearing defects and feeding problems. The solution to this is only a well organised multidisciplinary approach involving not only E.N.T. and plastic surgeons but also speech pathologists, linguistic experts and even dentists.
Although a vast majority of causes of VPI fall under the perview of plastic surgeon, a considerable number of patients present primarily to ENT specialists, also for their nasal twang, hearing defects or similar speech problems. However, till today many E.N.T. specialists are reluctant to tackle this problem themselves.
Our present study consists of 10 cases of VPI treated by flap pharyngoplasty in conjunction with plastic surgeon, speech pathologists and linguistic experts at the Department of E.N.T., Civil Hospital, Ahmedabad, India, over a period of 1. I/z years (1986 - 87). Out of limited surgical options available, either a superior or inferior based flap pharyngoplasty was done in each
case. While speech was assessed by speech pathologists and linguistic experts for nasality, articulation defects and oral consonant air pressure with its recording on audio tapes. All our patients have been followed up for a minimum period of six months.
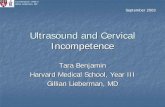
We have studied 10 cases of VPI, randomly selected from ENT or Plastic O.P.D. Full assessment by detailed history and complete ENT examination was done. Radiographic cephalometry, taking standard fixed distance lateral view X-rays of skull, first in resting condition of palate and then while phonating "e...e...e..."; was done in each case. (as shown in x-ray photograph and line diagram). It helped in a unidimentional measurement of defect of V.P. port area. Nasopharyngogram was done in selected few cases to outline the defect with a radio opaque dye. Speech pathologists and linguistic experts assessed the speech and hearing of each patient preoperatively, 1 month post operatively after intensive speech therapy and 6 months post
operatively. Speech records were maintained on audiotapes. The speech defects were classified and graded as shown in footnote below table, which helped in comparative evaluation of results. Two linguistic experts combindly and two speech pathologists separately evaluated each case every time before tabulating the results. Each patient was followed up for a minimum period of 6 months.
VPI is an incomplete closure of V.P.port area, normally formed by velum and posterior pharyngeal wall.
Mahendra Naik Honorary Professor of E.N.1
Ani l Chadha Professor of Plastic Surgery
Nayan Parekh Assistant Professor of E,N.T
Vatsal Patel 4th Year Resident in E.N.T.
BJ. MediccJi ,'_allege & Civil Hospital, Ahmedabad. Address for Reprints
Dr. Mahendra Naik Honorary Professor of E.N.T., Ward E-6, Civil Hospital, Asarwa, Rhmedab~d-38001<
Indian Journal of Otolaryngologv, Volume 43, No. 1, March, 1991 ~ ]

A study of 10 cases of velopharyngeal incompetence treated by flap pharyngoplasty - ~ Naik el al.
N
A N
- - - - v - -
P
B
Fig. I..
CEPHALOMETRIC MEASUREMENTS
This leads to inability to establish a normal intra-oral pressure necessary for normal production of non-nasal consonants and vowels. It leads to following changes in speech.
i. Weak pressure for all vowels and consonants.
2. Unclear articulation mainly for pressure sounds.
3. Nasal Emission. 4. Hypernasality.
Due to thes~ defects, attempted correction but in fact faulty, 'maladjustments' in the speech tract leads to production of secondary compensating speech defects in form of 'Glottal stops' and 'Pharyngeal Fricatives'.
All these defects ultimately leads to production of week, unclear and unitelligible nasal speech. The main cause of VPI are as follows:
(1) Congenital short soft palate. (2) Cleft palate of various types and
degree. (3) Submucous cleft palate. (4) Acquired palato pharyngeal
disproportion following adenoidectomy.
(5) Pharyngomegaly, i.e. an overly large pharynx in 0resence of palate of normal length and mobility. The management of VPI includes :
Surgical Procedure
(A) (a)
(b)
Surgical line of treatment :
Palatal push back or lenghthening procedure. Various types of phm3,ngoplasties- 1. Pharyngeal flap : Inferior or
superior based. 2. Sphincter pharyngoplasty 3. Augraentation pharyngoplasty. 4. Combination of above.
(B) Non-surgical line of treatment : (a) Prosthetic device. (b) Speech therapy including
training of muscle movements.
With limited options at hand we went only for the most accepted procedure of flap pharyngoplasty in all cases. Each patient underwent either superior or inferior based flap pharyngoplasty by an ENT or plastic surgeon. Both procedures are shown by line drawings in figure (2&3), with important details explained below the respective figures.
The merits and demerits of these proccdures are as follows :
Inferior based [ Superior based m
pharyhgoplasty. [ pharyngoplasty.
1. This type of flaps draw the palate j downward and backward.
1This typeof flaps will draw the palate upward and backward which ix mor~ Physiological moventcn t.
~ Indian Journal of Otolaryngology, Volume 43, No. 1, March, 1991

A s tudy of 10 cases of ve lopha ryngea l i n c o m p e t e n c e t r e a t ed by f lap p h a r y n g o p l a s t y - Naik et al.
2. It is not necessary ~ 2. Repaired palate has to completely deride / divided in the midline a repaird palate. Ilence not a good . Hence, a good procedure for secondary procedure for surgery but definitely secondary surgery superior when associ-
ated with primary palate repair.
3. Less incidence of hyponasality and snoring, postopera- tively.
3. tligher reported inci- dence of hyponasality and snoring.
A l l ten pa t ien t s were be low 25 years
o f age while 8 were be tween 16 to 25 years . Ou t of 10 pa t ien ts , 3 were with r e p a i r e d cleft pa la te , 5 with s u b m u c o u s clef t p a l a t e and 2 with congen i t a l shor t soft pa la te . Al l had nasa l and d i s t o r t e d speech while
re
C
_._1 t k O (.3 Z >- r.o
6 Q- z a .
._~
tU O'1
O m
I11 u _
Z
(Inferior base flap pharyngoplasty)
A After retracting the soft palate ( velum ) forwards, two lateral incisions for the pharyngeal flap are put in the fossa o~ Rosenmullcr, depending cn the .length required.
B After dissecting the flap further from the underlying prevertebral fascia the tip
(proximal end ) is cut and the donor defect area is closed with catgut sutures.
C By pulling the flap forward on the velum, its area of attachment on the velum is
marked and then a trap door type semicircular flap is raised from the velum.
Pharyngeal flap is sutured to the velum as the flap raised from the velum goes behind it.
I nd i an Journa l of Oto la ryngology , V o l u m e 43, No. 1, March , 1991 [ ]

A study of 10 cases of velopharyngeal incompetence treated by flap pharyngoplasty - Naik el al.
t a b t
°
(Fig. NO. 3)
SUPERIOR BASE FLAP PHARYNGOPLASTY
( Superior base flap pharyngoplasty ) prevent its tubing. Two lining flaps (b) are marked on nasal surface of the soft palate. A catheter is placed in the lateral port on one side of the pharyngeal flap.
A.
B.
Soft .palate is d iv ided in the midline. Superior pharyngeal flap is marked along the full width of the poster ior pharyngeal wall, incised and di.~ected from the prever tebta l russia
The lx~ te r io r pharyngeal wall gap is sutured, bu t not till the base of the flap to
C. The lining flaps (b) are retracted laterally after elevation. The pharyngeal flap is now sutured to the mucosa of the nasal surface of the soft palate. The lining flaps
(b) are to be rotated ( as shown by arrows
over the raw surface of pharyngeal flap.
D. The lining flaps (b) are sutured to cover the raw surface of the pharyngeal flap in the midline. The or'41 side of the soft palate is sutured beginning from u-u till infer ior end of incision.
Indian Journal of Otolaryngology, Volume 43, No. 1, March, 1991

A study of 10 cases of velopharyngeal incompetence treated by flap pharyngoplasty - Naik et al.
X-ray skull {lateral view) showing gap between posterior pharyngeal wall and velum {shown by arrow} while speaking 'e-e-C_.
nasal regurgitation and hearing defects were other complains. Radiographic cephalomatric findings showed a maximum velopharyngeal gap of 12 mm and minimum of 6 mm.
As mentioned earlier, the subjective speech assessment results by two speech oathologists individually and two linguistic experts combindly giving 3 total results were tabulated individually and then mean was taken as final result. The selected speech samples remained constant for each patient during each evaluation, thereby making comparison of speech assessment easy and reliable. Pre-operative speech samples were compared in each case with results after surgery and one month of intensive speech therapy and then final assessment was done again at 6 months interval. 8 patients were operated by inferior based flap pharyngoplasty while 2 by superior based flap pharyngoplasty.
The improvement in various types of speech defects were as shown in table. Accordingly nasality showed' maximum and the earliest improvement with as many as 9 patients falling in grade O to 1 at six
months follow-up. Acceptable speech rating also improved markedly with 8 patients showing grade O to 1. However, articulation defects got corrected only in 2 patients out of 8 in whom it was present preoperatively. The table also shows that the oral consonant air pressure is changed markedly after surgery and improves further after continuous speech therapy to reach the final results.
All these results emphasise not olfly on the role of surgery but more firmly on the part played by continuous and intensive speech therapy in all cases of VPI for achieving fmal improvements in speech defects. Active involvement of speech therapist and co-operation of the patient played a vital role in the outcome.
Though a few complications llke bleeding, airway obstruction, oro-nasal fistula, etc have been
TABLE SHOWING IMPROVEMENT IN SPEECH DEFECTS
Criteria used and its Pre-operative 1 month, post-opet:~ 6. months post-oper- gradation, tively after speech tively after speech
therapy therapy No. of cases. No. of cases No. of cases.
(A)
(B)
(C)
(D)
NASALITY 0 0 1 2 1 1 6 7 2 2 2 0 3 3 1 1
ACCEPTABLE SPEECH RATING 0 0 1 2 1 1 6 6 2 2 3 2 3 3 0 0
ARTICULATION DEFECTS Present 8 7 6 Absent 2 3 4
ORAL CONSONENT AIR PRESSURE P + 3 6 8 P - - 7 4 2
i i i
Indian Journal of Otolaryngology, Volume 43, No. 1, March, 1991 @

A study of 10 cases of velopharyngeal incompetence treated by flap pharyngoplasty - , Naik e, al.
(A) NASALITY: Grades : 0 Normal 1 Mild; probable not
perceptable to layman. 2 Moderate : consistingly
perceptable to layman. 3. Severe : Generally
unitelligible.
(B) ACCEPTABLE SPEECH RATING: 0 Indistinguishing from
normal speech. 1 Noticable deviation
but not difficult in understanding speech sample.
2. Speech was understand- able if topic was known.
3. Speech onintelligible.
(c) ARTICULATION DEFECTS: Present : Articulation defect present. Absent : Articulation defect absent.
(D) CONSONANT ORAL AIR PRESSURE: P + : Air pressure good. P- : Air pressure poor.
occasionally reported in the 4. literature to be associated with pharyngoplasqr, including flap separation as a delayed problem, we didn't encounter any of these in our 5. study.
The study shows highly encouraging 6. results for flap pharyngoplasty m velopharyngeal incompetence. It is
safe, simple and highly effective surgical method and all E.N.T. surgeons should be familiar with it. Along with intensive speech therapy, it gives significant improvement in speech defects; particularly nasality and acceptable speech rating, along with achieving better oral consonant air pressure in a majority. 9.
All 10 patients had some improvement in speech were subjectively very happy with the 10. results and none had any complications. 1t.
Bardly, Doris P. (1971): Congenital and acquired palatopharyngeai insufficiency. Cleft, Lip and Palate, 42:658.
Bardly, Doris P. (1971~ Congenital and acquired palatophat3,ngeal insufficiency. Cleft, Lip and Palate 42:668.
Calnan James S. : (1971): Surgery for speech. Recent advances in Plastic surgery. Vol. I, 3:39.
Cainan James S. (1971) : Permanent nasal escape in speech after adenoidectomy. British Journal of Plastic surgery, 24: 197- 204.
Dibbell David G. (1965)" A modification of combined push back and pharyngeal
flap operation. Plastic and reconstructive Surgery, 34: 170.
lsshiki Nobuiko (1975): A new folded pharyngeal flap. Plastic and reconstructive surgery. 55: 461.
7. M. Coy FJ. (1972): A new approach to the elusive dynamic pharyngeal flap. Plastic and reconstructive surgery, 49:160.
8. Michel Hogan, V. : Valopharyngeal
incompetence. Plastic surgery by John Macqals Converse, 52: 2268.
12.
13.
14.
15.
Owslay J.A. (1976) : The Re-do pharyngeal flap. Plastic and Reconstructive surgery. 57: 180.
Sommerland Brain (1975): A synopsis of surgical anatomy (ll.lh EA) 2 31 240.
Sullivan, D.E. (1961) : Bilateral phatyngoplasty as aid to V.P. closure. Plastic Reconstructive surgery. 23:32.
Supriestersbach D.C. and Morris H.L(1977): Speech problems of patients with cleft lip' and palate RecenL PL Surgery by John Marquis Converss. 4:2246.
William Laworthy, G. (1975): ttearing acuity before and after pharyngeal flap procedure. Plastic Reconstructive surgery. 56:49.
William Porterfieio H (1966) : Hyperaasality in noncleft patients. Plastic and Reconstructive surgery. 37 : 216.
Yules 1LD. (1971) : Secondary techniques for correction of palatopharyneeai incompetence. Cleft Lip and Palate. 32 451-83.
Indian Journal of OtUaryngology, Volume 43, No. 1, March, 1991