A Stepwise Approach to Acid Base Disorders in ICU
71
Rajesh Pande Senior Consultant & Head Senior Consultant & Head Department of Critical Care Medicine, Department of Critical Care Medicine, Fortis Hospital, Noida Fortis Hospital, Noida A stepwise approach to acid base disorders in ICU
-
Upload
vishal-prabhu -
Category
Documents
-
view
6 -
download
2
description
Acid Base Disorders in ICU
Transcript of A Stepwise Approach to Acid Base Disorders in ICU

Rajesh Pande
Senior Consultant & HeadSenior Consultant & HeadDepartment of Critical Care Medicine, Department of Critical Care Medicine,
Fortis Hospital, NoidaFortis Hospital, Noida
A stepwise approach to
acid base disorders in ICU

100
90
80
70
60
50
40
30
20
H+
(neq/L)
pH
7.0
7.05
7.1
7.3
7.4
7.7
7.5
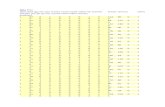
Relationship between hydrogen ion activity and pH
pH
Normal 7.35 – 7.45
Acidemia < 7.35
Alkalemia > 7.45

Daily Acid Load & acid-base Daily Acid Load & acid-base homeostasishomeostasis
Normal diet generates volatile acids (CO2) from carbohydrate & Non volatile acids ( H+) from protein metabolism.
Both lungs & kidneys are responsible for maintaining acid-base homeostasis by excreting these acids.
Alveolar ventilation allows for excretion of CO2.
Kidneys reclaim all filtered HCO3-. Any urinary loss
would lead to net gain of H+.
Kidneys must also excrete the daily protein load generated from protein intake.

Daily Acid LoadDaily Acid Load
Less than ½ of acid load is excreted as titrable acids ( phosphoric & sulfuric acids)
Remaining acid load is excreted as NH4+.
This process increases markedly in metabolic
acidosis.
Blood pH is determined by these physiological processes & the buffer systems present in body.

Buffers and respiration are temporary mechanisms.
Kidneys can make permanent adjustments.

Buffer systems of the bodyBuffer systems of the body
Bicarbonate- carbonic acid: (Extracellular
buffer) quantitatively the largest
Phosphate buffer: In RBC’s and kidney tubules (Ammonium is an important urinary buffer)
Protein buffer system: Tissues and plasma (Intracellular)
Hemoglobin buffer system: RBC’s

Bicarbonate- Carbonic acid Bicarbonate- Carbonic acid buffer systembuffer system
Principal extracellular buffer & the most important.
H2O + CO2 H2CO3 H+ + HCO3-
Adding acid load to the body consumes HCO3-: CO2 is maintained
within a narrow range via Resp. drive & HCO3- is regenerated by
the kidneys. Primary changes in PaCO2 lead to respiratory acidosis or
alkalosis. Primary changes in HCO3
- lead to metabolic acidosis or alkalosis.
In simple disorders, PaCO2 and HCO3- move in the same
direction
c.a
.c.a
.

Proximal Tubular cells
ca
CO2 + H2O H2CO3
H+ + HCO3-
Plasma
NaHCO3
Tubular Urine (glomerular
filtrate)
NaHCO3
+ HCO3-
H2CO3
H2O + CO2
Na+
Bicarbonate conservation by kidneys
ca

Excretion of H+ ions
After all HCO3- has been reclaimed, H+ secreted into renal
tubules can combine with phosphate ions (HPO4-) to form H2
PO4 which is eliminated in urine
Formation of Ammonia
After all HCO3- has been reclaimed, & phosphate buffer has
been utilized NH3/NH4 pair becomes the most important buffer. Ammonia comes from deamination of glutamine in proximal tubular cells. It combines with H+ and the NH4
+ is removed in urine

pH = 6.1 + log HCO3-
H2CO3
H2CO3 = PaCO2 .03
pH = 6.1 + log HCO3-
PaCO2 .03
Henderson Hasselbalch Equation
H+ = 24 PaCO2
HCO3-


Concept of anion gapConcept of anion gap
Metabolic acidosis High or Normal anion gap (Hyperchloraemia)
Normal Cl- (105) :Na+ (140) ratio = 1:1.4
Hyperchloraemia= Cl- : Na+ > 1:1.4

Na+
140
Cl-
105
HCO3-
25
Pr 16OA 4
PO4 -
SO4 -
2
Total anion (152) = Total cation (152)
Serum
Na+
140
Cl-
105
HCO3-
25
AG 15
Na (145) > Cl + HCO3 (130)
SerumK + 5K + 5Ca ++ 5
Mg ++ 2
UCUC
Mg + Ca +
K= 12
UAUA
Alb + PO4 +SO4+ organic
acids = 23

Concept of anion gapConcept of anion gap
It helps us in differentiating whether metabolic acidosis is due to H+ ions accumulation or loss of HCO3
- ions.
Anions gap: major plasma cations –major plasma anions
AG = (Na+) - (Cl-) + (HCO3-)
AG = 140 –(104 + 24) = 12 mEq / L
Normal range= 10 4 mEq / L

Anion gap & albumin Anion gap & albumin correctioncorrection
50% reduction in albumin will result in 75% reduction in AG.
2 methods to correct it:
Expected AG= (2 x albumin g/dl) +(0.5x PO4 mg/dl) Adjusted AG = Observed AG + 2.5 x (4.5 – meas alb)
AG 10, Serum albumin 2 Adjusted AG = 10 + 2.5 (4.5-2) = 16 meq/l

Copenhagen Approach: Copenhagen Approach: Concept of Base ExcessConcept of Base Excess
BE is the amount of acid (H+) or base (HCO3-)
that must be added to return blood pH to 7.40 and PaCO2 to 40 mmHg at full O2 saturation & 37C.
(Deviation of patient’s HCO3- from 24 mmol/
L after pH is corrected to 7.4)
It is usually derived from a monogram.
A negative value indicates Metabolic Acidosis and a positive value indicates metabolic alkalosis.

Standard Base ExcessStandard Base Excess
Copenhagen concept: An ideal metabolic index independent of PaCO2
SBE = 0.93 x ([HCO3-] + 14.48 x [pH-7.4]-
24.4 Ref Range: -3 to +3 mEq/L

Standard bicarbonate:Standard bicarbonate:
Standard bicarbonate is the bicarbonate concentration of a sample when the pCO2 has been adjusted (or ‘standardised’) to 40 mmHg at a temperature of 37oC.
This would remove the influence of changes in pCO2 by seeing what the [HCO3] would be if the respiratory component was made the same for all measurements.
Std HCO3- in metabolic acidosis,
in metabolic alkalosis
Buffer base is a measure of the concentration of all the buffers present in either plasma or blood.

Boston ApproachBoston Approach
Does not use BE, Std HCO3- or Base
Excess. The assessment of metabolic disturbances
is based on a comparison of the ‘actual’ (ie measured) and ‘expected’ values of [HCO3
-]. 6 Bedside rules e.g. Expected [HCO3] = 24 + { (Actual
pCO2 - 40) / 10 }

In vivo compensationIn vivo compensation
HCO3- + H+ H2CO3 H2O + CO2
(PaCO2 by 1mm Hg < 40 for each mmol/L of HCO3- < 24)
PFK is lactic acid production
Urea synthesis is ( HCO3- utilization)
CO3- is mobilized from bone to form plasma HCO3
- Intracellular buffering (50% of H+ load)
Renal compensation: HCO3- reabsorption, H+, NH4+
secretion, Cl- & HPO4 reabsorption)

Respiratory compensationRespiratory compensation
The central chemoreceptors: medulla respond to changes in H+ in the CSF.
They are stimulated by H+ and result in hyperventilation lowers PaCO2 & restores arterial pH to normal.
The peripheral chemoreceptors: aortic body, carotid body are sensitive to H+ , PaCO2, PaO2 & perfusion pressure. They communicate to Central receptors through glossopharyngeal nerve.

Metabolic acidosisMetabolic acidosis
It is a clinical disturbance characterized by an increase in total body acid.
It should be considered a sign of an underlying disease process.
Identification of the underlying condition is essential to initiate appropriate therapy.

PathophysiologyPathophysiology
An in the endogenous acid production (lactate, ketoacids): addition of H+
or Loss of bicarbonate (HCO3)
-) as in
diarrhea.
or Accumulation of endogenous acids
(kidneys unable to excrete the dietary hydrogen (H+) load: as in renal failure.

Systemic effects of metabolic Systemic effects of metabolic acidosisacidosis


Response of the body Response of the body
Extracellular buffering : Immediately
Respiratory compensation: Minutes
Intracellular and bone buffering: Hours
Renal excretion of the H+ ion load: Hours to days


Treatment of metabolic acidosisTreatment of metabolic acidosis

Alkali therapyAlkali therapy
Aim: pH 7.2, HCO3- 8 – 10 mmol/l
Take bicarbonate space to be 50% of body wt.
Base deficit Body wt. 0.3 (give 50% of the dose)
Difference between desired & measured HCO3
- wt. 0.5

Alternative alkalinizing agentsAlternative alkalinizing agents
Carbicarb: Equimolar conc. Of sodium bicarbonate & sodium carbonate
(It limits but does not eliminate generation of CO2)
THAM (0.3 N tromethamine): buffers both metabolic as well as respiratory acids.
(limits generation of CO2. Significant side effects)

Risks of NaRisks of NaHCOHCO33- - therapytherapy
Undiluted: Hypernatremia, hyperosmolality
ECF overload
Overshoot alkalosis
Stimulation of 6 phosphofructokinase activity
CO2 load

Treatment of metabolic Treatment of metabolic acidosisacidosis
Severe/ Refractory: Dialysis
DKA: Fluid resuscitation
Salicylate poisoning: Alkalinize urine with alkali to a pH > 7.0 ( helps in eliminating salicylate)
Methanol/ Ethylene glycol: Ethanol infusion: 8 – 10 ml/Kg 10% ethanol in 5D over 30 min. + Infusion 0.15 ml/kg/hr

Anaesthetic implicationsAnaesthetic implications
Depressant effect of sedatives/ anesthetics
Circulatory depressant effect of inhalational agent
Avoid halothane, suxamethonium

Metabolic AlkalosisMetabolic Alkalosis
Primary change is HCO3 / or H+ - pH
For each in HCO3 of 7-7.5 mEq/L - pH by 0.1
Respiratory compensation - PaCO2
(Not very common) Expected PaCO2 in Metabolic Alkalosis:
0.7 × HCO3 + 21 ( ±2)

Causes of Metabolic AlkalosisCauses of Metabolic Alkalosis
Nasogastric suction : Diuretics : Cl, K, Mg Loss. Volume depletion: Stimulates Renin -
Angiotensin – Aldosterone axis – promotes loss of K+, H+ , in the distal tubule.
Addition of Organic anions – Acetate in parenteral nutrition, Citrate in banked blood.
Post Hypercapnia



pH = 6.1 + log HCO3-
H2CO3
H2CO3 = PaCO2 .03
pH = 6.1 + log HCO3-
PaCO2 .03
Henderson Hasselbalch Equation
H+ = 24 PaCO2
HCO3-

Patient EvaluationPatient Evaluation
Step 1 Comprehensive history taking & evaluation. It gives us clues to underlying acid-base
disorder. E.g. Diarrhea- non anionic gap metabolic
acidosis E.g. COPD- Respiratory acidosis

Common clinical states & Common clinical states & associated acid-base disordersassociated acid-base disorders
Clinical state Acid-base disorder
Pulmonary embolus Respiratory alkalosis
Hypotension Metabolic acidosis
Vomiting Metabolic alkalosis
Severe diarrhea Metabolic acidosis
Cirrhosis Respiratory alkalosis
Renal failure Metabolic acidosis
Sepsis Respiratory alkalosis, metabolic acidosis
Pregnancy Respiratory alkalosis
Diuretic use Metabolic alkalosis
COPD Respiratory acidosis

Acid-Base disorder Compensation formulaThe 1 for 10 Rule for Acute Respiratory Acidosis
The [HCO3] will increase by 1 mmol/l for every 10 mmHg elevation in pCO2 above 40 mmHg.
Rule 2 : The 4 for 10 Rule for Chronic Respiratory Acidosis
The [HCO3] will increase by 4 mmol/l for every 10 mmHg elevation in pCO2 above 40mmHg.
Rule 3 : The 2 for 10 Rule for Acute Respiratory Alkalosis
The [HCO3] will decrease by 2 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg.
Rule 4 : The 5 for 10 Rule for a Chronic Respiratory Alkalosis
The [HCO3] will decrease by 5 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg.
Rule 5 : The One & a Half plus 8 Rule - for a Metabolic Acidosis
Expected pCO2 = 1.5 x [HCO3] + 8 (range: +/- 2)
Rule 6 : The Point Seven plus Twenty Rule for a Metabolic Alkalosis
Expected pCO2 = 0.7 [HCO3] + 20
(range: +/- 5)

Rule 1 : Rule 1 : The 1 for 10 Rule for Acute Respiratory Acidosis
The [HCO3] will increase by 1 mmol/l for every 10 mmHg elevation in pCO2 above 40 mmHg.
Expected [HCO3] = 24 + { (Actual pCO2 - 40) / 10 }
Comment:The increase in CO2 shifts the equilibrium between CO2 and HCO3 to result in an acute increase in HCO3. This is a simple physicochemical event and occurs almost immediately.
Example: A patient with an acute respiratory acidosis (pCO2 60mmHg) has an
actual [HCO3] of 31mmol/l.
The expected [HCO3] for this acute elevation of pCO2 is 24 + 2 = 26mmol/l.
The actual measured value is higher than this indicating that a metabolic alkalosis must also be present.

Rule 2 : Rule 2 : The 4 for 10 Rule for Chronic Respiratory Acidosis
The [HCO3] will increase by 4 mmol/l for every 10 mmHg elevation in pCO2 above 40mmHg.
Expected [HCO3] = 24 + 4 { (Actual pCO2 - 40) / 10}
Comment: With chronic acidosis, the kidneys respond by retaining HCO3, that is, renal compensation occurs. This takes a few days to reach its maximal value.
Example: A patient with a chronic respiratory acidosis (pCO2 60mmHg) has an
actual [HCO3] of 31mmol/l. The expected [HCO3] for this chronic elevation of pCO2 is 24 + 8 =
32mmol/l. The actual measured value is extremely close to this so renal
compensation is maximal and there is no evidence indicating a second acid-base disorder.

Rule 3 :Rule 3 : The 2 for 10 Rule for Acute Respiratory Alkalosis
The [HCO3] will decrease by 2 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg.
Expected [HCO3] = 24 - 2 { ( 40 - Actual pCO2) / 10 }
Comment: In practice, this acute physicochemical change rarely results
in a [HCO3] of less than about 18 mmol/s. (After all there is a limit to how low pCO2 can fall as negative
values are not possible!) So a [HCO3] of less than 18 mmol/l indicates a coexisting
metabolic acidosis.

Rule 4 : Rule 4 : The 5 for 10 Rule for a Chronic Respiratory Alkalosis
The [HCO3] will decrease by 5 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg.
Expected [HCO3] = 24 - 5 { ( 40 - Actual pCO2 ) / 10 } ( range: +/- 2)
Comments: It takes 2 to 3 days to reach maximal renal
compensation The limit of compensation is a [HCO3] of about 12 to
15 mmol/l

Rule 5 : Rule 5 : The One & a Half plus 8 The One & a Half plus 8 Rule - for a Metabolic AcidosisRule - for a Metabolic Acidosis
Expected pCO2 = 1.5 x [HCO3] + 8 (range: +/- 2) Comments: Maximal compensation may take 12-24 hours to reach The limit of compensation is a pCO2 of about 10 mmHg Hypoxia can increase the amount of peripheral chemoreceptor stimulation Example:
A patient with a metabolic acidosis ([HCO3] 14mmol/l) has an actual pCO2 of 30mmHg.
The expected pCO2 is (1.5 x 14 + 8) which is 29mmHg. This basically matches the actual value of 30 so compensation is maximal and
there is no evidence of a respiratory acid-base disorder (provided that sufficient time has passed for the compensation to have reached this maximal value).
If the actual pCO2 was 45mmHg and the expected was 29mmHg, then this difference (45-29) would indicate the presence of a respiratory acidosis and indicate its magnitude.

Rule 6 : The Point Seven plus Twenty Rule 6 : The Point Seven plus Twenty Rule for a Metabolic AlkalosisRule for a Metabolic Alkalosis
Expected pCO2 = 0.7 [HCO3] + 20
(range: +/- 5)

Illustrative CaseIllustrative Case
Paramedic brought a 20-yr old man to the ER.
He was found lying in an alley with an empty liquor bottle nearby.
BP 120/80, pulse rate 110/min, RR 28/min, Temp 98.6 F.
Unresponsive, pupils minimally reactive to light. DTR brisk, symmetrical, Plantars normal
Bilateral basal crepitations.
History suggestive of ingestion of toxin- may be associated with acid base disorder.

Step 2Step 2
Obtain ABG
pH 7.1 PaCO2 35 PaO2 90 HCO3
- 12 Cl- 97 Na 145 K 5 BUN 30 Cr 1.5 Glucose 110

Step 3: Verify the accuracy Step 3: Verify the accuracy of Dataof Data
Obtain ABG
pH 7.1 PaCO2 35 PaO2 90 HCO3
- 12 Cl- 97 Na 145 K 5 BUN 30 Cr 1.5 Glucose 110
H+ = 24 (PaCO2÷HCO3-)
H+=24 (35 ÷12) = 70
Increase in H+ = 70-40= 30
Formula: (PH 7.2-7.55) There is a 0.01 change from 7.4
in the opposite direction for every 1 nEq/l change in H+ from 40
pH = 30 0.01 = 0.3 7.4-0.3 = 7.1 Data is internally consistent

Step 4: Identify the primary Step 4: Identify the primary disturbancedisturbance
pH <7.35 Acidemia
pH > 7.45 Alkalemia
Primary process is metabolic: Changes in HCO3- or
respiratory (changes in PaCO2)
Looks like metabolic acidosis!

Step 5: Calculate the expected Step 5: Calculate the expected compensationcompensation
Acid-Base disorder Compensation formula
Metabolic acidosis Change in PaCO2 = 1.2 change in HCO3
-
Metabolic alkalosis Change in PaCO2 = 0.6 change in HCO3
-
Acute respiratory acidosis Change in HCO3- = 0.1 Change in
PaCO2
Chronic respiratory acidosis Change in HCO3- = 0.35 Change in
PaCO2
Acute respiratory alkalosis Change in HCO3- = 0.2 Change in
PaCO2
Chronic respiratory alkalosis Change in HCO3- = 0.5 Change in
PaCO2

Evaluation of ABGEvaluation of ABG
Both HCO3- & PaCO2 are low
Primary disorder- metabolic.
Compensation = Change in PaCO2 = 1.2 change in HCO3
-
= 1.2 (24 -12) = 14 mm Hg PaCO2 should have been
40-14 = 26. But it is 35
Concomitant Respiratory acidosis is also present
pH 7.1 PaCO2 35 PaO2 90 HCO3
- 12 Cl- 97 Na 145 K 5 BUN 30 Cr 1.5 Glucose 110
PaCO2= 1.5 x (HCO3-) + 8

Step 6: Calculate the gapsStep 6: Calculate the gaps
For D/d of metabolic acidosis: Anion Gap.
Unmeasured anions (PO4-, SO4
-, organic anions, proteins) > unmeasured cations (ca++, Mg ++)
Normal value: 10 4 mEq/l
High anion gap MA: Acid dissociates into H+ & an unmeasured anion. H+ is buffered by HCO3
-, & the unmeasured anion accumulates in the serum resulting in increase in AG.
Non anion gap acidosis: H+ is accompanied by Cl- a measurable anion, hence no change in the anion gap.

Evaluation of ABGEvaluation of ABG
AG = 145-97-12 AG = 36 High anion gap MA
Has limitations Normal AG does not
exclude presence of unmeasured anion
pH 7.1 PaCO2 35 PaO2 90 HCO3
- 12 Na 145 K 5 Cl- 97 BUN 30 Cr 1.5 Glucose 110

Delta anion gapDelta anion gap
Assess the elevation of the anion gap relative to the decrease in HCO3
-.
Normal 1-1.6
<1 indicates HCO3- has decreased out of proportion to the
elevation of AG. It suggests the presence of non anion gap metabolic acidosis.
>1.6 indicates that AG has increased out of proportion to the rise in HCO3
- & suggests the presence of concomitant metabolic alkalosis.

Concept of Delta Anion GapConcept of Delta Anion GapAG excess/HCOAG excess/HCO3 3 deficitdeficit
Anion - anion gap or Delta AG ( AG)
To assess of AG relative to a in HCO3
-
AG = (Observed AG – normal AG) / (24 - HCO3
-) Normal AG = 1 (1-1.6) AG < 1= HCO3
- has out of proportion to AG ( Suggest presence of non anionic gap MA)
It reflects the coexistence of a normal AG metabolic acidosis.
pH 7.1 PaCO2 35 PaO2 90 HCO3
- 12 Na 145 K 5 Cl- 97 BUN 30 Cr 1.5 Glucose 110

AG >1.6 = AG has out of proportion to in HCO3
- (Suggest presence of concomitant metabolic alkalosis)
AG = (36-10) / (24 -12) AG = 26/12 = 2.2 Additional metabolic alkalosis is also present

High AG Metabolic AcidosisHigh AG Metabolic Acidosis
Acidosis with Organic source ( Production of endogenous non volatile acids):Lactic Lactic acidosis Ketoacidosis Renal failure
Acidosis due to ingestion of toxins (Ingestion of exogenous non volatile acids) Methanol Ethylene glycol Salicylate

Lactic acidosisLactic acidosis
Serum lactate > 5 mEq/l Tissue hypoxia Shock & organ hypoperfusion
Tachycardia Tachypnoea Urine output Mentation

KetoacidosisKetoacidosis
Uncontrolled DM or alcohol intake with poor dietary intake
Insulin deficiency & glucagon excess enable release of FFA from fat cells, which are metabolized to ketoacids: acetoacetate, hydroxybutyric acid.
These are unmeasured anions. Both alcoholic & diabetic Ketoacidosis can
cause significant in AG whereas starvation Ketoacidosis does not to > 18 mEq/l

KetoacidosisKetoacidosis
Sweet odor- due to acetone
Diagnosis: Nitroprusside ketone reaction (Acetest)
It detects only acetone & acetoacetate in serum. Does not detect hydroxybutyric acid which makes up 70% of ketones in diabetics & about 90% in alcoholics.

Toxin IngestionToxin Ingestion
Methanol (varnish, automotive fluids) Metabolized to formaldehyde & formic acid Formic acid dissociates into H+ & unmeasured anion (formate). Weakness, nausea, vomiting, vision, altered mental status.
Ethylene glycol: component of antifreeze & some solvents. Its toxic metabolites include glycolic acid, oxalic acid. Both
dissociate into H+ & unmeasured anions. Neurological symptoms predominate followed by
cardiopulmonary and later acute renal failure Urine exhibits fluorescence under Wood’s light Urinalysis may reveal characteristic enveloped shaped calcium
oxalate crystals.

How to process suspected How to process suspected poisoning?poisoning?
Find out the Osmole gap.
It is difference between measured and calculated serum osmolarity.
Represents presence of unmeasured solute.
Substances with low mol. Wt. that can achieve high serum conc. Without causing death ( methanol, ethylene glycol, isopropyl alcohol).
They cause high AGMA with osmole gap.

Calculate the Osmole GapCalculate the Osmole Gap
pH 7.1 PaCO2 35 PaO2 90 HCO3
- 12 Na 145 K 5 Cl- 97 BUN 30 Cr 1.5 Glucose 110 Serum Osmolarity (measured)
350 mOsm/l Lactate 1 mEq/l Ketones negative Salicylates negative
Calculated Osmolarity= (2 × Na+) + (glucose ÷18)+ (BUN ÷2.8)
(2 × 145)+ (110/18) + (30/2.8) 307 mOsm/l
Measured- calculated= 350-307 = 43.
This Osmole gap in presence of high AGMA suggested the ingestion of methanol or ethylene glycol.

Interpretation of the ABGInterpretation of the ABG
Complex triple acid-base disorder
High anion gap metabolic acidosis secondary to ethylene glycol ingestion, respiratory acidosis & metabolic alkalosis, probably as a result of vomiting.

Non-anion gap acidosisNon-anion gap acidosis
When metabolic acidosis is caused by loss of HCO3
- from extracellular fluid, the HCO3- loss is
counterbalanced by a gain of chloride ions to maintain electrochemical neutrality.
As the in HCO3- proportional to Cl- gain the AG =
Na-(Cl-+ HCO3-) remains unchanged.
Therefore this non AG metabolic acidosis is also called Hyperchloremic MA.

Hyperchloremic Acidosis Hyperchloremic Acidosis (Normal Anion Gap)(Normal Anion Gap)
GI Losses of HCO3- : Diarrhea (20 – 50 mEq/L HCO3
-),
Renal Loss of HCO3- : Failure to reabsorb HCO3
- (Defect in prox. Tubules) Type 2 renal tubular acidosis (urine pH <5.5 , when serum HCO3
- is low)
Failure to excrete H+ ( Defect in Distal tubules) Type 1 renal tubular acidosis (urine pH >5.5)
Dilutional: Saline infused, Amino acid infusion, Large q. of NH4Cl infused.
Less common: Pancreatic fistula, small bowel syndromes, Acetazolamide infusion, fistulas between ureters & GI tract

Non-anion gapNon-anion gap
Diarrhea, renal tubular acidosis & hyperalimentation Calculate Urine anion gap Urine:
cations Na+, K+, Ca++, Mg++, NH4+
Anions Cl-, H2PO4-, SO4
—
Urinary anion gap is defined as the difference between the unmeasured anions and the unmeasured cations.
Normally NH4+ is the unmeasured cation (20-40 mEq/L/day)
Urinary anion gap is negative (-20 to 0 mEq/l)
Normal renal response to an acid load is an in generation of ammonia with an in NH4
+ excretion resulting in large negative anion gap (-20 to -50 mEq/l).
In renal tubular acidosis (Defect in renal acidification): NH4+ excretion is impaired and urine anion gap becomes positive.
Urine Anion Gap= Na+ + K+ - Cl-

FormulasFormulas
1. Modified Handerson- Hasselbalch equation H+=24 × PaCO2 /HCO3
- = 40 nEq/l
2. Law of electrical neutrality = Cl-+ HCO3-+ unmeasured
anions =Na+ + unmeasured cations
3. Anion Gap = Na+ - Cl- – HCO3- (10 4 mEq/l)
4. Delta anion gap= (anion gap-10) / (24 - HCO3-) (1-1.6)
5. Osmole gap= Diff between measured & calculated serum osmolarity (normal 10-20 mOsm/l)
6. Calculated osmolarity= (2 × Na+) + (glucose ÷18)+ (BUN ÷2.8)
7. Law of electrical neutrality (urine)= unmeasured anions +Cl- = Na++ K+
8. Urinary anion gap (normal= -20 to 0 mEq/l)= Na+ + K+- Cl-

Thank You