A special region-specific The Newsmagazine as i-pacifc ... · Advances in pediatric imaging P 13...
12
EDUCATION PROGRAM IN MYANMAR : FIRST PET/CT INSTALLED JANUARY 2002 The Newsmagazine of Imaging Innovation & Economics SPRING 2013 asia-pacific Advances in pediatric imaging P 13 The diagnosis and monitoring of children using ultrasound comes with its own unique challenges CAD P 11 Promising advances in Computer Aided Detection of breast cancer Breast MRI P 16 A summary of recent data on the diagnostic performance of a high- relaxivity contrast agent A special region-specific publication from the editors of Diagnostic Imaging asia-pacific
Transcript of A special region-specific The Newsmagazine as i-pacifc ... · Advances in pediatric imaging P 13...

Education program in myanmar : First pEt/ct installEd
January 2002
The Newsmagazine of Imaging Innovation & EconomicsSpring 2013 asia-pacific
Advances in pediatric imaging P 13The diagnosis and monitoring of children using ultrasound comes with its own unique challenges
CAD P 11
Promising advances in Computer Aided Detection of breast cancer
Breast MRI P 16A summary of recent data on the diagnostic performance of a high-relaxivity contrast agent
A special region-specific publication from the editors of Diagnostic Imaging
asia-pacific

A Well-Balanced Contrast Medium
With a right mix of osmolality, viscosity and iodine concentration, Ultravist® delivers contrast for high-quality imaging results.1
www.bayer.co.ukEnquiries: 01635 563000Calls to and from Bayer HealthCare may be recordedDate of preparation: October 2012. L.GB.10.2012.0951All rights reserved. © Bayer plc 2012
Ultravist® (iopromide) Prescribing Information (Refer to Summary of Product Characteristics (SmPC) before prescribing) Presentation: Intravascular injections of non-ionic iopromide in strengths of 150mg, 240mg, 300mg and 370mg of iodine/ml. Indications: For diagnostic use only. Delineation of the vascular and renal systems and of body cavities. Posology and administration: Adults Intravenous urography: minimum doses: Ultravist 370: 0.8ml/kg body weight; Ultravist 300: 1ml/kg body weight; Ultravist 240: 1.3ml/kg body weight. Children Intravenous urography: see SmPC. Adults Computed tomography: Cranial CT: Ultravist 240: 1.5-2.5ml/kg body weight; Ultravist 300: 1-2ml/kg body weight; Ultravist 370: 1-1.5ml/kg body weight. Whole-body CT: Dosage and administration rate depend on investigation and scanner. Adults Angiography: depends on age, weight, cardiac output, general condition, clinical problem, examination technique and the nature and volume of the vascular region to be investigated. (see SmPC). Adults Checking function of dialysis shunt: Ultravist 150: 10ml. Paediatric population: young infants (age < 1 year) and especially newborns are susceptible to electrolyte imbalance and haemodynamic alterations. Care should be taken regarding the dose of contrast medium to be given, the technical performance of the radiological procedure and the patient status. Renal impairment: to reduce the risk of additional contrast media-induced renal impairment in patients with pre-existing renal impairment, the minimum possible dose should be used. Hepatic impairment: no dosage adjustment is necessary. Elderly: possibility of reduced renal function should be considered. Contra-indications: Uncontrolled thyrotoxicosis. Warnings and precautions: Can be associated with anaphylactoid/hypersensitivity reactions, ensure preparedness for institution of emergency measures. Allergy-like reactions from mild to severe possible, mostly within 30 min, but delayed reactions (hours to days) may occur. Particularly careful risk/benefit judgement required for patients with: known hypersensitivity to Ultravist or its excipients; previous reaction to any contrast medium or; history of bronchial asthma or allergic disorders (increased risk). Pre-medicate with corticosteroids if necessary. To minimise risk: administer Ultravist to recumbent patients; observe patients closely for 15 minutes and keep them in hospital for at least one hour after the last injection. Patients on beta-blockers may be resistant to the effects of beta agonists. If severe reaction occurs, patients with cardiovascular disease are more susceptible to serious or fatal outcomes. Caution in patients with: known/suspected hyperthyroidism or goitre, monitor thyroid function in neonates exposed via mother or during neonatal period. Caution in patients with cerebral arteriosclerosis, pulmonary emphysema, poor general health, renal insufficiency, dehydration, diabetes mellitus, multiple myeloma/ paraproteinaemia, repetitive and / or large doses of Ultravist. Nephrotoxicity may occur or rarely acute renal failure. Ensure adequate hydration of patients; correct water or electrolyte imbalances before administration. With cardiac or severe coronary artery disease, increased risk of haemodynamic changes or arrhythmia. Intravascular injection may precipitate pulmonary oedema in patients with heart failure. Increased risk of neurological complications in patients with seizure history or CNS disorders. Caution in patients with reduced seizure threshold. May aggravate the symptoms of myasthenia gravis. Flush intravascular catheters frequently with physiological saline (if possible with addition of heparin) and minimise procedure length to minimise procedure-related thromboembolism risk. Patients with phaeochromocytoma may be at increased risk of developing a hypertensive crisis. Minimise excitement, anxiety and pain. Do not use in myelography. Sensitivity testing is not recommended. Interactions: Consider interruption of biguanides treatment prior to Ultravist administration as a precaution against development of lactic acidosis. Prevalence of delayed reactions higher in patients who have received interleukin-2. Diagnosis and treatment of thyroid disorders with thyrotropic radioisotopes may be impeded for up to several weeks due to reduced radioisotope uptake. Pregnancy and lactation: Adequate and well-controlled studies in pregnant women have not been conducted. Safety for nursed infants has not been investigated. Effects on ability to drive and use machines: Driving or operating machinery is not advisable for 30 minutes after the last injection. Undesirable effects: Common: dizziness, headache, dysgeusia, blurred/disturbed vision, chest pain/discomfort, hypertension, vasodilatation, vomiting, nausea, pain, injection site reactions (e.g. oedema, soft tissue injury post extravasation), feeling hot. Serious side effects: cf – Warnings and Precautions – in addition: Hypersensitivity/anaphylactoid reactions (anaphylactoid shock§*, respiratory arrest§*, bronchospasm*, laryngeal*/pharyngeal* or mucosal oedema, laryngeal/pharyngeal spasm§, asthma§*, angioedema), vasovagal reactions, arrhythmia*, dyspnoea*, cardiac arrest*, myocardial ischaemia*/infarction*, thyrotoxic crisis, thyroid disorder, coma*, cerebral ischaemia/infarction*, stroke*, brain oedema*, convulsion*, transient cortical blindness (IV use only), loss of consciousness, amnesia, paresis/paralysis, hearing disorders, cardiac failure*, bradycardia*, tachycardia, cyanosis*, hypotension*, shock*, thromboembolic events (IV use), pulmonary oedema*, respiratory insufficiency*, aspiration*, bullous conditions (e.g. Stevens-Johnson syndrome or Lyell syndrome), compartment syndrome due to extravasation (IV use), renal impairment/acute renal failure (IV use). § Reactions identified only during post-marketing surveillance (frequency not known). *These adverse reactions may have a fatal or life-threatening outcome and are considered the most serious adverse drug reactions. Prescribers should consult the SmPC in relation to other side effects. Overdose: Symptoms may include fluid and electrolyte imbalance, renal failure, cardiovascular and pulmonary complications. Monitoring of fluids, electrolytes and renal function recommended in case of intravascular overdosage. Treatment of overdose should be directed towards the support of vital functions. Ultravist is dialysable. Incompatibilities: Because of possible precipitation, X-ray contrast media and prophylactic agents must not be injected as mixed solutions. Special Precautions for Storage: Protect from light and X-rays. Legal Classification: POM Package Quantities and Basic NHS Price: Ultravist 150 10 x 50ml bottles £101.57 Ultravist 240 10 x 50ml £145.86 Ultravist 300 10 x 20ml £124.63 10 x 50ml £182.03 1 x 100ml £36.16 1 x 200ml £71.98 Ultravist 370 10 x 50ml £224.94 1 x 100ml £44.68 1 x 200ml £88.78 MA Numbers: Ultravist 150: 00010/0564 Ultravist 240: 00010/0565 Ultravist 300: 00010/0566 Ultravist 370: 00010/0567 Further information available from: Bayer plc, Bayer House, Strawberry Hill, Newbury, Berkshire, RG14 1JA, Telephone: (01635) 563000 Date of preparation: August 2012 Ultravist® is a trademark of the Bayer Group.
Adverse events should be reported. Reporting forms and information can be found
at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Bayer plc.
Tel.: 01635 563500, Fax.: 01635 563703, Email: [email protected]
References1. For details and full range of indications please refer to the
Summary of Product Characteristics.
13667_bhc_uv_anz_uk_di_spc-right_bl.indd 1 05.02.13 18:42

COMING SOON IN the AutuMN ISSue: •Interventional radiology•Ultrasound•Tech update•Imaging News
INfORMAtICS
Radiology and the mobile device:. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
IMAGING NewS
Chinese research shows potential of MRI imaging of tumor angiogenesis using integrin αvβ3 probes . . . . . . . . . . . . . . . . . . . . . . . 5Improving outcome from breast cancer in low income countries: lessons from Bangladesh . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52013 RAD-AID Conference open for registration . . . . . . . . . . . . . . . . . . 6PET with or without CT is more accurate than bone scan for the detection of bone metastases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 INDuStRy NewS
Chinese Radiologist honored . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Toshiba enters into partnership for dementia research . . . . . . . . . . . . . 8New Zealand company candidate for Gold award . . . . . . . . . . . . . . . . . . 9SonoScape Receives FDA Clearance . . . . . . . . . . . . . . . . . . . . . . . . . . 9Affordability & Access to Breast Care in developing countries : a comparison of China and India with the United States . . . . . . . . . . 10
SPRING 2013
RePORtS
The need for easily operated ultrasound devices that produce high quality images is common across all radio-logical specialties. But the diagnosis and monitoring of children using ultrasound comes with its own unique challenges.
Page 13
An FDA study has shown that a new approach to CAD leads to improvements in radiologist sensitivity to breast cancer as well as in the radiologist’s ability to differentiate between breast cancer and non-cancer.
Page 11
ReGuLARS
4| fROM the eDItORDespite accounting for only a relatively small proportion of the total number of examinations carried out, CT is now responsible for the biggest part of the total collective radiation dose. Industry has a vital role in future dose reduction strategies
15| BOOk RevIewS
Review questions for MRI by C K Roth & W H Faulkner, Jr.
Neurovascular Examination: the Rapid Evaluation of Stroke Patients Using Ultrasound Waveform Interpretationby Andrei V. Alexandrov.
21| teChNOLOGy uPDAte
The optimization of breast MRI protocols has focussed on improvements in spatial resolution and the potential benefits of higher field strength. However, careful and appropriate selection of the MRI contrast agent can also significantly improve diagnostic performance.
Page 16
VisiT us AT
SPRING 2013 D I A G N O S T I C I M A G I N G A S I A P A C I F I C 3
asia-pacific
asia-pacificCOveR StORy
EDuCATIon PRogRAM FoR HEAlTH PRoFEssIonAls sTARTED In MyAnMARPhilips recently announced the start of a year-long program of clinical education in association with the Myanmar Radiological society. The company will also shortly introduce the first PET/CT imaging system to Myanmar, which will result in higher imaging capabilities and greater diagnostic confidence to improve management of cancers, neurological and cardiovascular diseases. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9

By Dr Alan Barclay
With the ever-increasing globalization of the inter-national radiology mar-ket, there is a tendency
to think that the main differences between various geographic and economic blocs are simply due to temporary differences in the positions of such blocs on some sort of uni-versally valid and applicable developmental time–scale. Thus, if it is accepted that it is in the United States that there are currently the largest numbers of radiology scans car-ried out each year and the largest number of installed systems, with Western Europe just behind, the feeling is that as emerging countries progress more or less inexorably along an economic development path, it is just a matter of time before the developing countries reach the same level of availability of radiology systems per head of popula-tion. The danger of such an over-simplified view of things is that it implies that devel-oping countries are almost by definition bound to encounter the same problems as already being seen in the so-called devel-oped world. Nowhere is this more so than in the dramatic increase in the number of CT scanners in the developing world. Although the data of course vary from country to country, the majority of examinations in the developing world are still carried out using basic radiography systems, frequently still with analog, film-based systems.
However, already this century there has been a sea-change in radiology. This is the astonishing development of MDCT scanners and the ever-increasing installed base of these systems. MDCT scanners enhance diagnostic capabilities immensely, and reduce the scanning time so that a single breath-hold is sufficient for chest CT. The result is that now CT is not only patient-friendly but also the physician’s preferred imaging tool. What’s more, CT has also been added to molecular imaging systems to create hybrid scanners such as PET/CT and SPECT/CT. In addition, cur-rently the actual usage pattern of CT is markedly different from that at the time of its original introduction three or four decades ago. Thus earlier practice used thick slices of 10mm with inter-slice gaps of 10 mm and a scan area restricted to either the pelvis or the abdomen rather than the
combined abdomen and pelvis routinely carried out today.
The outcome of all these developments is a huge rise in the contribution of CT to the total radiation dose used in medical practices. As pointed out in a recent review (Rehani, M, Challenges in radiation protec-tion of patients for the 21st century, Am J Roentgenology AJR 2013; 200 762) data from the United Nations Scientific Committee on the Effect of Atomic Radiation (UNSCEAR) show that CT contributes to 35% of the total collective radiation dose, even though it actually accounts for only 5% of all diag-nostic and interventional procedures. In comparison, conventional radiography and fluoroscopy only contribute 11% to the total collective dose.
What’s worse is that the trend in aver-age effective dose used in CT is actually increasing. Rehani cites data showing that the average effective dose of a CT exam in the 1970s was 1.3 millisieverts as against 7.4 millisievert in the decade from 1997 to 2007.
So are the developing countries con-demned to follow inexorably the same trend of increasing dose as they follow the trend to increased usage of CT systems with the development of their economies? The answer is not necessarily. Although it sounds suspiciously as having one’s cake and eating it, the future clinical advantages of CT may be achievable without an obligatory concomitant increase in dose. As Rehani points out several factors could contrib-ute to this ideal situation. These include increased awareness of, and reaction to, the issue of dose by radiation biologists, refer-ring physicians, radiologists, radiographers and medical physicists. However the most determining contribution looks likely to come from manufacturers. As they vie with each other to reduce dose, developments in detectors, electronics and software look likely to be able to make sub-millisievert dose CT a routine procedure — and not just for cardiac examination.
Equipment manufacturers look set to play the greatest role in making patients safer. n
Radiation protection of patients: industry’s vital contri bution
FROM THE EDITOREDITORIAL ADVISORY BOARDDr. Jennifer Cawson, Melbourne, AustraliaProf. Yi-Hong Chou, Taipei, TaiwanProf. Jiang-Ping Dai, Beijing, ChinaProf. Hiroshi Fujita, Gifu, JapanMr. Robert George, Sturt, S. AustraliaDr. Julian He, Boston, USAProf. Jung-gi Im, Seoul, KoreaDr. Bhavin Jankharia, Mumbia, IndiaProf. Mikund S. Joshi, Mumbai, IndiaDr. George Klempfner, Melbourne, AustraliaProf. Michio Kono, Kobe, JapanDr. K. Kulaveerasingam, Kuala Lumpur, MalaysiaDr. Lillian L.Y. Leong, Hong Kong, ChinaProf. Jae Hoon Lim, Seoul, KoreaProf. Quanfei Meng, Guangzhou, ChinaProf. Wilfred C. G. Peh, SingaporeDr. Tauqir Ahmed Rana, Riyadh, Saudi ArabiaDr. Zhonghua Sun, Curtin, AustraliaProf. Lenny K. A. Tan, SingaporeDr. Chui-Mei Tui, Taipei, TaiwanProf Dr. John George, Kuala Lumpur, Malaysia
EDITORIAL STAFF
Editor Alan Barclay, Ph.D. US Consulting Editor Greg Freiherr Editorial coordinator Denise Asbury
Publisher David Lansdowne Associate Publisher Bob Warren
EDITORIAL CONTACTRue des Noisetiers, 91421 Ophain, BelgiumTel. +32 479 370 364 E-mail: [email protected]: [email protected]
SUBSCRIBER SERVICESTelephone: +44 1442 877777; Fax: +44 1442 70617
E-mail: [email protected]
INTERNATIONAL SALES OFFICES
Europe & North America JapanDi Europe Ltd Orient Echo inc.
E-mail: [email protected]
Telephone: +(44) 1442 877777 Telephone: + (81) 3/3235-5961
Fax: +(44) 1442 870617 Fax: + (81) 3/3235-5852
Contact: David Lansdowne Contact: Masahiko Yoshikawa
Contact: Bob Warren
E-mail: [email protected]
Contact: Marika Cooper
E-mail: [email protected]
China KoreaAdept Marketing Young Media inc
unit B, 13/f, Por Yen Building, 407 Jinyang sangga
No 478 Castle Peak Road, 120-3 Chungmuro 4 ga
Cheung sha Wan, Kowloon, Hong Kong Chung-Ku, seoul, Korea 100-863
E-mail: [email protected] E-mail: [email protected]
Telephone: +852 2891 7117 Telephone: +82 2 2273 4819
Fax: +852 2893 2101 Fax: +82 2 2273 4866
Contact: Adonis Mak Contact: Young J. Baek
Article Reprint Sales DI Europe Ltd Tel: +44 1442 877777
Email: [email protected]
DIAGNOSTIC IMAGING ASIA PACIFIC is published by DI Europe Ltd. Printed by Manson, St-Albans, UK. Editorial Advisory Board members suggest topics for coverage and answer questions for the editors. They do not conduct a formal peer-review of all manuscripts submitted to DI Europe.
Copyright © 2013 DI Europe Ltd. All rights reserved. Reproduction in any form is forbidden without express permission of copyright owner.
DI ASIA PACIFIC2 Claridge CourtLower Kings RoadBerkhamsted, Herts HP4 2AFUKTelephone: +44 1442 877777Fax: +44 1442 870617
asia-pacific
SPRING 2013 D I A G N O S T I C I M A G I N G A S I A P A C I F I C 4

NewSiMaging Chinese research shows potential of MRI imaging of tumor angiogenesis using integrin αvβ3 probes
Improving outcome from breast cancer in low income countries: lessons from Bangladesh
Accurate detection and quantifica-tion of tumor angiogenesis is important for early diagnosis of cancers as well as post therapy assessment of antiangio-genic drugs. A recently published paper from Shanghai Jiao Tong University in Shanghai, China reviews the potential of MRI using integrin αvβ3 probes for imaging tumor angiogenesis. (Liu Y,
Yang Y, Zhang C, Int J of nanomedi-cine 2013; 8: 1083) The cell adhesion molecule integrin αvβ3 is a specific marker of angiogenesis, and is highly expressed on activated and proliferat-ing endothelial cells, but generally not on quiescent endothelial cells. Over recent years, many different approaches have been developed for imaging αvβ3
expression, for the detection and char-acterization of tumor angiogenesis. The Shanghai research group has now pro-vided an overview of the current status of magnetic resonance molecular imag-ing of integrin αvβ3, including the new development of highly sensitive contrast agents and strategies for improving the specificity of targeting probes and the biological effects of imaging probes on αvβ3 positive cells. In particular the authors describe MR molecular imaging of tumor angiogenesis by targeting inte-grin αvβ3 with RGD peptide-modified magnetic probes. For detection of the sparse angiogenic marker, the imaging probes have evolved from paramagnetic nanoparticles to high sensitive single superparamagnetic iron oxide nanopar-ticles (SPIONs). These are the most widely used T2 (or T2*) contrast agent in MRI. More recent research highlights the potential of ultrahigh sensitive SPION clusters which have been shown in experimental animals to be able to detect nascent tumors.http://tinyurl.com/Liu-et-al-paper
For the past five years, a group of US and Bangladeshi clinicians have been working in rural Bangladesh to under-stand what happens to women with breast cancer in the region. (Story HL et al. Improving Outcomes from Breast Can-cer in a Low-Income Country: Lessons from Bangladesh Int J Breast Cancer doi: 10.1155/2012/423562)
Women in low- and middle-income countries (LMICs) have yet to benefit from recent advances in breast cancer diagnosis and treatment now experi-enced in high-income countries. Their unique sociocultural and health sys-tem circumstances warrant a different approach to breast cancer management than that applied to women in high-income countries. The research team analyzed case and consecutive series data, carried out focus group and indi-
vidual interviews, and accumulated clinical care experience. The findings of the team support the idea that barriers to effective breast cancer management in the Khulna Division of Bangladesh are rooted in complex sociocultural, economic, and health systems issues which affect womens’ choices to seek and accept care and successful treat-ment. Most of these, including gender equity and human rights, are beyond the scope of the usual approach to can-cer control but have a profound influ-ence on effective care on a population level. Studies in other parts of South Asia and amongst immigrants to high-income countries from South Asia have suggested similarly complex issues. The authors believe that the general calls for “breast cancer awareness,” “early detec-tion and mammography” and “access to
drugs” are well intentioned but unlikely to result in a significant improvement on morbidity in these contexts. How-ever the team concluded that health system, human rights, and governance issues underlie high mortality from this relatively rare disease in Bangladesh. With a commitment to and prioritiza-tion of quality research, including the training and resources required, research outcomes can have a direct impact on productivity, prosperity, and quality of life of people in low and middle-income countries.http://tinyurl.com/Story-et-al-paperBody
SPRING 2013 D I A G N O S T I C I M A G I N G A S I A P A C I F I C 5

IMAGING NewS
RAD-AID International is a non-profit organization founded by a team of radiologists trained at Johns Hopkins University, Baltimore, MD, USA. A global network designed to assist developing countries to implement and optimize radiology and health imag-ing services while improving the role of radiology in global public health initia-tives. RAD-AID improves the provi-sion of radiology and health care ser-vices in the developing world through a sustained longitudinal legacy of dialog, education, resources, and collaboration.Each year since 2009, RAD-AID holds a free conference at Johns Hopkins on international radiology for developing
and emerging countries to improve global health services. The confer-ence brings together nongovernmental humanitarian organizations, academic medical centers, overnment, and busi-nesses with individuals of all back-grounds such as radiologists, public health officials, technology engineers, economists, medical technologists, nurses, physicians, and business leaders. The conference is a lively interactive forum with discussions of how medi-cal imaging can be improved to boost international health care. The RAD-AID conferences produce consensus white papers published in the Journal of the American College of Radiology
(JACR). Presentations at the confer-ence include new global community service programs, emerging research on clinical models for delivering imaging services to limited-resource regions, international economic devel-opment strategies, innovative technol-ogy approaches for building radiology abroad, and educational programs for those interested in serving internation-ally, such as residents, students, and practicing health personnel.
The 2013 RAD-AID Conference on Radiology for Developing Countries will be held Saturday, October 26, 2013 at Johns Hopkins Medical Campus in Baltimorewww.rad-aid.org
A team of clinicians from the Seoul National University College of Medi-cine have just published a paper (Lee et al Korean J Radiol 2013;14(3):510) show-ing that PET is more accurate than bone scans for detecting bone metastases. In the paper the team compared the diagnostic accuracies between bone PET and bone scan in cancer patients who underwent both imaging studies.
Na18F was introduced as a bone imag-ing agent in positron emission tomogra-phy (PET) as early as the 1960s. Na18F is
a very useful imaging agent for the evalu-ation of bone abnormality and thanks to its high bone affinity, rapid clearance, and low protein binding, is superior to 99mTc-labeled phosphate agents in terms of bone image quality. Furthermore, the fast kinet-ics of Na18F enables image acquisition as early as 30 minutes post injection.
Despite all these theoretical advantages, bone PET using Na18F was not routinely used in clinical practice in early years because of the relatively undeveloped status of PET imaging technology of the
period. In fact, the advent of gamma imag-ing technology and the development of 99mTc -labeled phosphate agents in the 1970s almost replaced bone PET with the bone scan.
Now recent innovative technologi-cal advances in the PET modality have allowed Na18F to resurface as a promising bone imaging agent. The resolution of PET is superior to that of gamma camera imaging and PET/CT further improves the lesion detection rate with the aid of anatomical information from the CT. Thanks to effective attenuation correction algorithms, PET generates a more accurate quantitative image data set than gamma camera imaging . Furthermore, the recent supply crisis of 99Mo, the parent radionu-clide of 99mTc meant that in 2010 many physicians began to focus more attention to the usefulness of bone PET using Na18F. Bone PET has been proven to be use-ful for a variety of bone diseases and is able to effectively evaluate not only malig-nant diseases, but also benign bone dis-eases The Seould team Na18F bone PET is more accurate than 99mTc-HDP bone scan for the evaluation of bone metastases. The authors consider that bone PET by itself has the potential to be a gold standard test for bone metastases. However, without sufficient confirmatory data in Korea, they only claim that, based on their findings, the accuracy of bone PET is superior to that of the bone scan.http://tinyurl.com/Lee-et-al-paper
2013 RAD-AID Conference open for registration
PET with or without CT is more accurate than bone scan for the detection of bone metastases
6 D I A G N O S T I C I M A G I N G A S I A P A C I F I C SPRING 2013
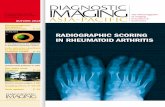
Findings of bone positron emission tomography (PET) and bone scan in 84-year-old male prostate cancer patient with numerous bone metastatic lesions. Left Panel. Anterior and posterior planar images of bone scan show multiple bone metastases. Right panel. Bone PET anterior and posterior maximum-intensity projection images reveal numer-ous metasatic bone leisons. Note that metastatic lesions on bone PET are more prominent than those on bone scan.

Radiology and the mobile device: radiology in motionThe impact of mobile devices is revolutionizing the way we communicate, inter-act, are entertained, and organize our lives. With healthcare in general and radiology in particular becoming increasingly digital, the use of such devices in radiology practice is inevitable. A very recent article [1] has evaluated the likely impact of mobile devices on radiology and the current limitations of the avail-able technologies. This article summarizes the main take-home messages.
The practise of radiology is evolving toward the universal adoption of teleradiology by radiolo-gists and radiology groups across the world, The most recent change in the dynamic has
been the introduction of portable handheld devices, such as tablet PCs and smartphones, which allow for on-the-go interpretation of medical images, as opposed to the use of an office-based workstation. Since its introduction in 2010, the iPad has been a game changer. In addition, there are several other tablets based on the Android system and there is now the Playbook from Blackberry. However, the iPad is clearly the leading force in the tablet market. The picture archiving and communica-tion system (PACS) applications that currently run on mobile handheld devices include Merge Mobile, OsiriX, iClarity, Mobile MIM, ResolutionMD, Fujifilm Synapse, and RadSpa.
It is important to understand and be aware of the benefits as well as potential pitfalls of the use of such technologies.
Speed of iMage download The availability of high-speed wireless bandwidth such as 2G and now 3G on mobile tablet devices allows for immediate transfer of images to tablets enabling “on the move” teleradiology, which is particularly of great benefit in the emergency setting.
iMage reSolution and diSplay Using a tablet PC, the radiologist is able to read scans in high resolution with very little panning. The web-based application allows the reader to zoom and adjust the window level, contrast, and brightness of the image. The radiologist will be evaluating actual raw DICOM image data and not just JPEG snapshots. Depending on the application, size, and density measurement tools, and annotation features may also be available, allowing for a complete evaluation.
The iPad’s 9.7-inch display provides 1024 × 768-pixel resolution at 132 pixels per inch (PPI). The larger display allows images to be displayed at or closer to their native resolution. The iPad has a maximum luminance of 270 cd/m2, which is much lower than the average primary interpretation workstation display with maximum lumi-nance of 500-600 cd/m2. The display of medical images on
an iPad is superior to that of an off-the-shelf workstation displays but below that of the medical grade monitors.
SecurityThe health insurance portability and accountability Act (HIPAA) requires that the images are transferred securely and are accessed by authenticated users. The iPad and tablet applications for radiology need to ensure they use the secure socket layer (SSL) protocol or virtual private network (VPN) for transferring the medical images and the access to these images is login controlled. The images are not actually stored on the iPad, but are always accessed from the server through the login-based interface. Login timeout restricts the amount of time that the images are physically displayed on the device’s monitor. Ultimately, it is of course the responsibility of the radiologist or physician to ensure the physical security of his/her portable device.
teaching toolWeb-based teaching is greatly facilitated by the use of technologies such as tablet PCs. In combination with the use of internet-based videoconferencing technologies, the iPad can greatly extend the reach of radiology training beyond the traditional classroom model.
current liMitationS While the extreme portability of the iPad is its greatest asset, it may at the same time be seen as a liability for those unused to touch screen technology and tablet-based keyboard typing. For advanced viewing, there need to be applications developed to render advanced imaging like 3D and MIP/MPR on iPad screens. These are currently in the development stage. However, mobile MIM’s applica-tion currently have the capability of rendering MPRs. At the time of writing, it is the only FDA- approved applica-tion for use on an iPad. This application can also measure standardized uptake values (SUVs) on positron emission tomography-computed tomography (PET-CT).
reference 1 Panughpath SG & Kalyanpur A. Radiology and the mobile device:
Radiology in motion. Indian J Radiol Imaging 2012;22:246-50. The article above is a much abridged summary of points expressed in more detail in the paper by Panughpath & Kalyanpur who are based at the Department of Radiology, Teleradiology Solutions Private Limited, Whitefield, Bangalore, Karnataka, India
INFORMATICS
SPRING 2013 D I A G N O S T I C I M A G I N G A S I A P A C I F I C 7

chinese radiologist honored
Prof. Qiyong Guo, MD, Presi-dent of the China Medical Univer-sity and head of the Department of Radiology in Shenjing hospital, was awarded with an honorary mem-bership of the German Radiology Society at the recent DRK congress held in Hamburg Germany. Profes-sor Qiyong Guo is an abdominal and interventional radiologist at one of the most prominent univer-sity hospitals in China and has an excellent reputation as editor of the Chinese Journal of Interventional radiology and the Chinese Journal of Radiology. Prof Guo is radiol-ogy representative in the Chinese Medical Association and is a past-president of the Chinese Society of Radiology, where currently he is the Vice President. During his time as President of the Chinese Society of Radiology an agreement was signed with the German Radiology Society according to which both societies agreed on exchange programmes for young mammograph specialists and radiologists
toshiba enters partnership for dementia research
Toshiba has unveiled a ground-breaking scientific cooperation with one of the world’s leading centres for research into dementia and neuro-degenerative conditions. The partnership with the Department of Radiology and the Department of neurology at the VU medisch cen-trum (VUmc) in Amsterdam, The Netherlands will see Toshiba provide
its latest MR system, the Titan 3T with pianissimo technology, for the next five years to support research into Dementia and Alzheimer’s disease.
MRI techniques have become of paramount importance in recent years in the investigation of the development of dementia. How-ever, the unique MR angiography techniques developed by Toshiba - combined with the features of the quiet and patient-friendly Titan 3T – could prove pivotal in the advance-ment of research in this field. Not only does the equipment allow the visualization of the cerebral micro-vasculature at a clinical MR field-strength, but these techniques are contrast-free and can be added to the protocol of longitudinal dementia studies where patients are scanned repeatedly over many years to study the onset and progression of the dis-ease. The scientific cooperation with VUmc comes at a time that health-care and financial systems are braced for a dramatic rise in the number of patients with dementia. Data show there are now some 36 million peo-ple worldwide living with dementia, with that figure expected to rise by 16 million a year between now and 2050, underlining the significance of the research and the importance of the Toshiba MR technology within that.
The Toshiba equipment was installed at VUmc at the beginning of May with the research being over-seen by Head of Neurology, Profes-sor Philip Scheltens and the Head of Neuroradiology, Professor Frederik Barkhof. Professor Scheltens, who is also head of the VUmc Alzheimer Center, said: “MR imaging is the cor-
nerstone of dementia diagnosis and working with Toshiba will enable us to dig deeper into the brains of demented people at the earliest stage and discover important clues that ultimately will improve management of these patients.”
Professor Barkhof, who is a senior consultant at the Alzheimer Center and the Director of the Image Analy-sis Center, explained that MRI is a critical tool in helping to show loss of brain volume in relevant struc-tures, such as the hippocampus, in Alzheimer’s disease. He added that their research in this area will help in obtaining more sensitive markers to diagnose Alzheimer’s and the role of vascular co-morbidity in dementia. A key advantage of the new Toshiba system is that it is wide bore and has been designed to offer the maxi-mum comfort to the most fragile and elderly patients. With the unique pianissimo technology, the 3T sys-tem is quiet and safe for a patient to be scanned for a continuous period of time using the most gradient demanding sequences. “The very low noise level will enhance acceptance of MRI in this very old and frag-ile population and the new Toshiba sequences will allow us to study the vascular pathology in dementia in more detail,” said Professor Barkhof. Throughout the study, the VUmc researchers expect to scan hundreds of patients with suspected demen-tia from its memory clinic, which is the largest in The Netherlands and screens 15-20 new patients a week. Professor Barkhof said the scientific cooperation with Toshiba will allow his team to focus on dementia using “patient-friendly equipment” in a “technically-advanced manner.”
He added: “As an academic centre we continuously strive to improve the care for our delicate patients. Toshiba’s Titan 3T Pianissimo scan-ner will allow us to better address the needs of vulnerable patient groups, including those less-oriented ones with cognitive decline and dementia, but also children with neurological diseases such as leukodystrophies.”TOSHIBA MEDICAL TOCHIGI, JAPANwww.toshibamedicalsystems.com
NewSinduStry
8 D I A G N O S T I C I M A G I N G A S I A P A C I F I C SPRING 2013

new Zealand company candidate for gold award
The New Zealand company Mat-akina Technology has been named as a finalist in the Discovering Gold award scheme organized to recognize outstanding performance by New Zea-land companies. Matakina was cited for their Volpara breast imaging software. The Discovering Gold category focuses on technological, scientific and innova-tive research and development projects and products that have come to the market in 2012.
Dr Ralph Highnam, CEO for Mat-akina said, “The Volpara software is faster and more robust with an easy to use intuitive interface. It has been widely accepted by the international breast imaging researcher community and is in clinical use across the world.”
Volpara was designed to help over-come the limitations of mammogra-phy to detect breast cancer in women with dense breasts, a known risk factor, generating objective, automatic mea-surement of volumetric breast density values along with a BI-RADS Breast Density Classification for mammo-grams acquired from any commercially available digital mammography system.MATAKINAWELLINGTON, NEW ZEALANDwww.matakoina.com
SonoScape receives fda clearance
SonoScape, the Shenzhen, China-based company specialized in provid-ing ultrasound systems and high-def-inition transducers for the worldwide healthcare industry, announced that the company has received FDA (510K) clearance for its outstanding portable color Doppler system S2. With its prac-tical design and stable performance, the S2 system has been developed to cater to the needs of healthcare professionals. The system has an intelligent patient file management system, and conve-nient user-definable settings suitable
SPRING 2013 D I A G N O S T I C I M A G I N G A S I A P A C I F I C 9
Front Cover Feature
Philips initiates education program for health professionals in Myanmar
Philips recently announced the start of a year-long program of clinical edu-cation in association with the Myan-mar Radiological Society. The program started off with a special symposium, to address the broad application of Posi-tron Emission Tomography (PET) and radio pharmacology in Myanmar. This program underscores Philips commit-ment to supporting the advancement of clinical practice in the country. Through a series of lectures and panel discussions with guest opinion lead-ers in the field of PET and Computed Tomography (CT) health professionals in Myanmar will have the opportunity to further their skills and knowledge in clinical applications of imaging tech-nology. Philips also announced that the company will shortly introduce the first PET/CT imaging system to Myan-mar, which will result in higher imag-ing capabilities and greater diagnostic confidence to improve management of cancers, neurological and cardiovascu-lar diseases. The PET/CT imaging sys-tem will be installed at Yangon General Hospital. Vincent Chan, General Man-ager, ASEAN, Philips Healthcare said “Philips is committed to improving the lives of patients and help clinicians in Myanmar with meaningful healthcare solutions. We do this by developing innovations across the entire contin-uum of care in partnership with clini-cians and our customers to improve patient outcomes, provide better value and expand access to care. Our clini-cal education program is an excellent example of how we will work in Myan-
mar and compliments the recently set-up ASEAN Non-Communicable Disease (NCD) Network which was initiated across the region to facilitate constructive debate and knowledge sharing, including in Myanmar”.
The education program will roll-out in three phases which will see par-ticipants begin with fundamentals of imaging technology, including PET/CT, before moving on to advanced multi-modality applications and finally complete clinical skills solu-tions. The first phase of the training will take place between May 2013 and March 2014 and focus on tech-nology essentials and specific trends and capabilities, including additional sessions on Nuclear Medicine, MRI and Ultrasound imaging. The Minis-try of Health, Republic of the Union of Myanmar, is pioneering the devel-opment of Nuclear Medicine in the country, beginning with the deploy-ment of the country’s first PET/CT facility and the localization of radio-nuclide production. Nuclear Medicine is a safe, painless and cost-effective way of diagnosing and treating dis-eases that would otherwise require surgery or more expensive diagnos-tic tests. The use of nuclear medicine imaging procedures can often identify medical problems long before they are apparent via other diagnostic tests.
In addition to regular symposia held in Myanmar, the Philips Educa-tion program will also seek to make available to Myanmar Radiological Society participants its CE-accredited distance learning platform, the Phil-ips Learning Center (www.theonline-learningcenter.com). This easy-to-use accredited continuing healthcare edu-cation platform offers access to over 1,200 quality medical courses and an extensive library of clinical cases - all via the Internet.PHILIPSEINDHOVEN THE NETHERLANDSwww.healthcare.philips.com/

INDuStRy NewS
for professional diagnostic applications. State-of-the-art technologies, such as μ-Scan, panoramic and 4D imaging etc. mean that high quality ultrasound is now available to a much broader range of clinicians. The FDA clearance of S2 is confirmation that SonoScape’s portable color Doppler system has reached the standard of the USA regu-
latory authorities and market. It will substantially help SonoScape consoli-date its brand influence and expand market share in this biggest ultrasound market. The FDA clearance of the S2 diagnostic system and a whole range of transducers is applicable for use in sev-eral fields, including abdomen, ob/gyn, cardiac, small organs, musculoskeletal and urology. SonoScape’s products are now available in over 130 countries. SONOSCAPESHENZHEN, CHINAwww.sonoscape.com
affordability & access to Breast care in developing countries : a comparison of china and india with the united States
Increasing awareness, affordability, and access to breast care are critical in developing countries. A new data visu-alization feature from GE Healthcare (http://newsroom.gehealthcare.com/) looks at these three issues, comparing the health burden, the trends in diagno-ses through routine screening and the cost of national screening programs in China and India with the United States.
The incidence of breast cancer is higher in the US than in developing countries. However, it is the most com-mon cancer among women in develop-ing regions and is expected to increase
at a faster rate than in the US. In major Indian cities, women aged
40 or older are advised to have mam-mograms at least every two years, which is similar to the guidelines in most Western countries. Surveyed physicians estimate that only 16% of cases are currently diagnosed through screening but that this rate will increase dramatically to 27% in five years and to 41% by 2018.
However, mammography availabil-ity is limited in India because of the shortage of facilities and well-trained staff. The high cost of screening is also a major factor.
In China, on average only 25% of patients currently diagnosed with breast cancer in the three major Chi-nese cities (Beijing, Shanghai and Guangzhou) are identified through routine screening. Surveyed physi-cians foresee that screening practices will change dramatically in the next five to ten years and estimate that in 2018, the percentage of patients identified through routine screening will more than double to 54%. Phy-
sicians in Shanghai reported much higher routine screening than in the other two cities. A possible reason for this difference is that the incidence of breast cancer in Shanghai is ris-ing quickly. Thus, breast cancer has garnered more attention from the general population in Shanghai in the past two years. The high cost of mam-mograms and scarcity of well-trained staff to interpret results, particularly in
community-based and rural hospitals, are cited by physicians as the primary limiting factors for routine mammog-raphy screening in China. In addition, physicians comment that the fear of radiation among Chinese women lim-its the popularity of mammography screening.
As part of its commitment to invest $1B in oncology research and devel-opment by 2016 to enhance the qual-ity and affordability of healthcare, GE Healthcare has recently launched a series of new, innovative technologies and solutions to help advance cancer diagnostics, molecular imaging and the patient experience.
A recent GE Healthcare data visu-alization on patient experience and breast cancer reveals why women may avoid regular mammograms, what vari-ables can affect patient pain levels dur-ing a scan and what hospitals can do to improve patient experience.
Compliance rates for yearly mam-mograms have long been an issue. One of the main reasons women avoid rou-tine mammograms is fear that the pro-
cess will be painful; however in one survey 43% of women said that their first mammogram wasn’t painful. One in every four women avoids mammo-grams because of worry and fear; fewer than 70% of women in the U.S. of age 40 and older have had a mammogram in the last two years. GE HEALTHCARE, CHALFONT ST GILES, UK http://tinyurl.com/GE-Visualization-data
10 D I A G N O S T I C I M A G I N G A S I A P A C I F I C SPRING 2013
FIGURE 1. A new data visualization feature from GE Healthcare compares the health burden of breast cancer, the trends in diagnoses through routine screening and the cost of national screening programs in China and india with the united states. http://tinyurl.com/GE-Visualization-data.

Refining technology, renewing hope: promising advances in Computer Aided Detection of breast cancer
The World Health Organization calls early detection “the cornerstone of breast can-cer control”[1]. After years of technological improvements, Computer Aided Detection
(CAD) systems are poised to build on that cornerstone: a new generation of CAD technology is currently improv-ing radiologists’ effectiveness in finding cancer and distinguishing cancer from non-cancer.
CAD systems help radiologists zero in on potential pathologies by automatically identifying areas of a mam-mogram that are consistent with breast cancer. Designed to detect suspicious masses, architectural distortions, and microcalcifications in breast tissue, some of these systems also employ comparisons with the contralateral breast to locate asymmetries. With their potential to save time and help to make radiologist more effective, they may soon become indispensable in the search for breast cancer.
Early CAD systems were the subject of controversy, with studies questioning their effectiveness [2]. How-ever, a comprehensive reader study of recently intro-duced CAD technology confirms a significant change for the better. For the first time, an FDA study has shown that a new approach to CAD leads to improvements in radiologist sensitivity to breast cancer as well as in radi-ologist ability to differentiate between breast cancer and non-cancerous states. These technological strides should translate directly into better health outcomes for women.
a Brief hiStory of cadLooking back to 1998, when CAD for mammogra-phy was making its debut, the technology seemed
both promising and problematic at the same time. The hope was that it would help radiologists to more effectively detect breast cancers and potentially save lives. That vision seemed unrealistic after an influen-tial study published in the New England Journal of Medicine stated that CAD interpretation of mammo-grams was less accurate than interpretation without a computer’s help [3].
by R. Bird
CAD
SPRING 2013 D I A G N O S T I C I M A G I N G A S I A P A C I F I C 11
the author :
rives Bird
is Director of Clinical Affairs
VuCOMP, Inc., Plano, Texas. USA
Rives Bird has a broad range of experience in engineering, R&D and clinical settings, spanning over 20 years. His background includes pivotal involvement in a variety of mammography tech-nologies as well as other clinical applications. Rives holds a BA is Physics from Wake Forest University, and did his graduate work at the Bowman Gray School of Medicine.
He can be reached at [email protected] FIGURE 1. A very small mass detection with associated architectural distortion.
«....For the first time, an FDA study has shown that a new approach to CAD
leads to improvements in radiologist sensitivity to breast cancer as well as in the radiologist’s ability to differentiate
between breast cancer and non-cancer...»

CAD
The U.S. Food and Drug Administration (FDA) responded strongly to such concerns.
In 2007, the FDA re-evaluated the process to clear a CAD device for market. After public comment and con-siderable deliberation, the FDA established guidance for “designing and conducting clinical performance assess-ment studies” that would support premarket submissions to the FDA [4]. The final guidelines, issued in July 2012, further specified that guidance. Recommending the use of comprehensive reader studies to demonstrate device effectiveness, they note that “performance metrics based on the receiver operating characteristic (ROC) curve or variant of ROC … in addition to sensitivity and specific-ity at a clinical action point will be likely candidates as study endpoints” [5].
recent reader Study ValidateS new generation of cad SySteMSDesigned and conducted according to the FDA’s final guidelines, a study of physicians using VuCOMP’s M-Vu CAD system has recently met its study endpoints. Led by principal investigator Dr. Etta Pisano of the University of North Carolina at Chapel Hill, the comprehensive reader study concluded that physicians using this CAD system
were more effective at reading mammograms, and that the system increased their ability to discriminate between cancer and non-cancer [6].
a different approach to iMage analySiSIn the past, CAD systems have typically depended on “black-box” learning technologies such as neural networks. By processing a vast number of examples and encoding the emergent patterns in a set of numbers, neural networks are ablke to “learn”. However the problem with this type of technology is that engineers do not precisely know what the computer is encoding—hence the term “black box.” With-out this knowledge, engineers have a hard time identifying the source of any problems arising during the development process. Are there hidden biases in the example cases, for instance? What if examples of non-cancer cases come from a clinic that overexposes its mammograms, and examples of cancer cases from another clinic that uses proper expo-sure? In that (admittedly simplified) scenario, since a black-box learns all it knows from the examples it is given, the system might learn that overexposure means “nor-mal,” while proper exposure means “cancer.” This would of course degrade actual performance—and without being able to clearly understand what was learned, the developer might never discover why. There is another option for CAD makers today.
In contrast to “black-box” systems, decision technol-ogy can be oriented towards the important types of visual structures that appear in mammograms. With this technol-ogy, developers can construct mathematical formulae that represent the concepts underlying these structures to map closely to our own human understanding. The automated intelligence thus performs its reasoning using mathematical constructs that an engineer can interpret more intuitively. The benefits of this approach are obvious: because a prob-lem can be traced to a particular concept flaw, the system can be improved more quickly and with relative ease. The net result is that the technology can be pushed to greater levels of performance than approaches based upon more obscure reasoning. Systems using decision technology are not only better equipped to adapt to clinical realities now; they will be more responsive to clinical needs in the future.
referenceS1. http://www.who.int/cancer/detection/breastcancer/en/index.html
2. “Study Refuting CAD Effectiveness in Mammography Sparks Debate,” Radiological Society of North America (1 Oct. 2011). http://www.rsna.org/NewsDetail.aspx?id=2535
3. Fenton JJ, Taplin SH, et al. Influence of Computer-Aided Detection on Performance of Screening Mammography. NEJM, Vol. 356, No. 14. April 5, 2007
4. “Draft Guidance for Industry and FDA Staff: Clinical Performance Assessment: Considerations for Computer Assisted Detection Devices Applied to Radiology Images and Radiology Device Data – Premarket Approval (PMA) and Premarket Notification [510(k)] Submissions” (21 Oct. 2009), 7.
5. Guidance for Industry and FDA Staff: Clinical Performance Assessment: Considerations for Computer-Assisted Detection Devices Applied to Radiology Images and Radiology Device Data - Premarket Approval (PMA) and Premarket Notification [510(k)] Submissions” (3 July 2012), 9.
6. SSED Data http://www.accessdata.fda.gov/cdrh_docs/pdf10/P100005b.pdf
12 D I A G N O S T I C I M A G I N G A S I A P A C I F I C SPRING 2013
FIGURE 2. A detected microcalcification cluster.
«...In the past, CAD systems have typically depended on “black-box” learning
technologies such as neural networks…there is another option for CAD today....”