Processed Amniotic Membrane Allografts. Amniotic Membrane Allografts.
Upload
ricardo-gomezCategory
view
216download
4
American Journal of Obstetrics and Gynecology (2005) 192, 678–89
www.ajog.org
A short cervix in women with preterm labor and intactmembranes: A risk factor for microbial invasion of theamniotic cavity
Ricardo Gomez,a Roberto Romero,b,* Jyh Kae Nien,b Tinnakorn Chaiworapongsa,c
Luis Medina,a Yeon Mee Kim,c,d Bo Hyun Yoon,e Mario Carstens,a Jimmy Espinoza,b
Jay D. Iams,f Rogelio Gonzaleza
Center for Perinatal Diagnosis and Research (CEDIP), Sotero del Rıo Hospital, P Universidad Catolica de Chile,Puente Alto, Chile,a Perinatology Research Branch, National Institute of Child Health and Human Development, NIH,DHHS, Bethesda, Md, and Detroit, Mich,b Department of Obstetrics and Gynecology,c and Pathology,d Wayne StateUniversity School of Medicine, Detroit, Mich, Department of Obstetrics and Gynecology, Seoul National UniversityCollege of Medicine, Seoul, Korea,e and Department of Obstetrics and Gynecology, The Ohio State University,Columbus, Ohiof
KEY WORDSUterine cervixUltrasoundChorioamnionitis
AmniocentesisPreterm delivery
Objective: The purpose of this study was to determine whether there was a relationship betweensonographic cervical length and the presence of culture-proven microbial invasion of the amniotic
cavity in women with preterm labor and intact membranes.Study design: Ultrasonography and amniocentesis were performed in 401 patients admitted withpreterm labor (22-35 weeks) and cervical dilatation of %3 cm, as assessed by digital examination.Cervical length was determined by transvaginal ultrasound at admission. Outcome variables were
the presence of microbial invasion of the amniotic cavity (defined as a positive amniotic fluidculture) and the occurrence of preterm delivery before 35 weeks. Contingency tables, c2 test,receiver-operator characteristic (ROC) curves, and logistic regression were used for statistical
analysis.Results: The prevalence of microbial invasion of the amniotic cavity was 7% (28/401).Spontaneous preterm delivery (%35 weeks) occurred in 21.4% (82/384) of patients. ROC curve
analysis showed a significant relationship between the frequency of microbial invasion of theamniotic cavity and the length of the uterine cervix (area under the curve: 0.77; P ! .005).Patients with a cervical length !15 mm had a higher rate of a positive amniotic fluid culture than
patients with a cervical length R15 mm (26.3% [15/57] vs. 3.8% [13/344], respectively; P ! .05).Moreover, patients with a short cervix (defined as !15 mm) were more likely to deliverspontaneously before 35 weeks, 32 weeks, within 7 days, and within 48 hours of admission (P !.05 for all comparisons). Forty percent of patients (161/401) had a cervical lengthR30 mm. These
patients had a very low risk of microbial invasion of the amniotic cavity (1.9% [3/161]),spontaneous delivery %35 weeks (4.5% [7/154]), %32 weeks (2.6% [2/76]), within 7 days (1.9%[3/154]), and within 48 hours (0% [0/154]) of admission.
Presented at the 21st Annual Meeting of the Society for Maternal-Fetal Medicine, Reno, Nev, February 5-10, 2001.
* Reprints not available from the authors. Please address correspondence to: Roberto Romero, MD, Perinatology Research Branch, NICHD,
NIH, DHHS, 3990 John R Boulevard, Detroit, MI 48201.
E-mail: [email protected]
0002-9378/$ - see front matter � 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.ajog.2004.10.624

Gomez et al 679
Conclusion: Endovaginal ultrasonographic examination of the uterine cervix in women withpreterm labor identifies patients at increased risk for intrauterine infection.� 2005 Elsevier Inc. All rights reserved.
Microbial invasion of the amniotic cavity is present inapproximately 10% of patients with preterm labor, andis a risk factor for impending preterm delivery,1 clinicalchorioamnionitis,2-4 neonatal morbidity,2,5-7 broncho-pulmonary dysplasia,8-10 and cerebral palsy.11-14 Mater-nal clinical symptoms and signs of clinicalchorioamnionitis are insensitive predictors for the iden-tification of patients with microbial invasion of theamniotic cavity.15-17 Thus, amniocentesis and amnioticfluid analysis have been used for the detection of bothintra-amniotic infection and inflammation.18-22 We havepreviously reported that women with microbial invasionof the amniotic cavity present with a greater degree ofcervical dilatation than patients with a negative amnioticfluid culture,1 an observation confirmed by others.23
Thus, we propose that the likelihood of microbialinvasion of the amniotic cavity may also vary asa function of cervical length. This study was conductedto test this hypothesis.
Study design
Study population
Patients admitted between December 1997 and October2003 to the Sotero del Rio Hospital with the diagnosis ofpreterm labor and intact membranes were asked toparticipate in a prospective cohort study designed toexamine the relationship between clinical, biochemical,and biophysical parameters and the risk of pretermdelivery, intrauterine infection, and neurologic disabil-ities. For the purposes of this study, we selected patientsin this cohort who met the following criteria: (1)singleton gestation; (2) gestational age between 22 and35 weeks and a live fetus; (3) cervical dilatation %3 cmby digital examination; (4) intact membranes; and (5)signed informed consent approved by the InstitutionalReview Board of both the Sotero del Rio Hospital andthe National Institute of Child Health and HumanDevelopment, NIH. Seventy-nine patients in this studywere also included in another investigation, exploringthe relationship between cervical length, vaginal fetalfibronectin, and preterm delivery.24
Definitions, study procedures, and clinicalmanagement
Preterm labor was diagnosed in the presence of regularuterine contractions of at least 3 in 30 minutes. Beta-mimetic agents and/or magnesium sulfate were given
intravenously for tocolysis. Steroids were administeredbetween 24 and 34 weeks. Endovaginal ultrasonographywas performed shortly after admission, around the timeof amniocentesis, with a 5-7.5 MHz transvaginal probe.Patients were asked to empty their bladder beforeendovaginal sonography. Measurements were obtainedbetween contractions by orienting the transducer so thatthe endocervical canal and internal cervical os werevisualized in the same sagittal plane. Three images wereobtained, and the one demonstrating the shortestcervical length was used to generate cervical biometricparameters. An amniocentesis was performed trans-abdominally to assess the microbiologic state of theamniotic cavity. The fluid was transported to thelaboratory in a capped plastic syringe and cultured foraerobic and anaerobic bacteria, as well as genitalMycoplasmas. A white blood cell count, glucose con-centration, and Gram stain for microorganisms wereperformed in amniotic fluid. The results of these testswere used for patient management. The standard of careis to use tocolysis in patients without evidence ofinfection and inflammation of the amniotic cavity. Onthe other hand, in patients with evidence of intra-amniotic inflammation/infection (as determined bya combination of a positive amniotic fluid Gram stain,white blood cell count O50 cells/mm3, and/or a glucosedetermination %14 mg/dL), the management dependedupon gestational age and the results of the test(s). Thepresumptive diagnosis of microbial invasion of theamniotic cavity/intra-amniotic inflammation was anindication for discontinuation of tocolysis at all gesta-tional ages, as well as administration of parenteralantibiotics until delivery. Steroid administration (beta-methasone) was used regardless of the presumptivediagnosis of amniotic fluid inflammation, except inpatients who had evidence of fetal lung maturity, asdetermined by a shake test and/or lamellar body count.Tests such as a lecithin/sphingomyelin ratio and phos-phatidyl glycerol determination are not performed atour institution because their cost is prohibitive for ourhealth care system. After the 32nd week of gestation,patients with presumptive microbial invasion of theamniotic cavity/intra-amniotic inflammation who re-mained pregnant after 48 hours underwent augmenta-tion of labor, if required. Before the 32nd week,management consisted of antibiotic administrationwithout tocolysis. Clinical chorioamnionitis was anindication for augmentation of labor with oxytocin ormisoprostol. Clinical chorioamnionitis was defined ac-cording to the criteria proposed by Gibbs et al.25 The

680 Gomez et al
diagnosis required a temperature elevation to 37.8(Cand 2 or more of the following criteria: uterine tender-ness, malodorous vaginal discharge, maternal tachycar-dia, fetal tachycardia, and leukocytosis O15,000/mm3.
Analysis
Outcome variables were the presence of a positiveamniotic fluid culture and the occurrence of spontane-ous preterm delivery (%35 weeks, %32 weeks, within 7days, and within 48 hours of admission). We used theseoutcomes because previous reports differed in endpoints, making comparisons among studies difficult.Comparisons between proportions were performedwith chi-square or Fisher exact tests. Receiver-operatorcharacteristic (ROC) curves were constructed to de-scribe the relationship between the sensitivity and thefalse-positive rate (1–specificity) of cervical length in theprediction of microbial invasion of the amniotic cavityand preterm delivery. Diagnostic indices (sensitivity andspecificity), as well as positive and negative predictivevalues for the cervical length, were obtained. Likelihoodratios for positive and negative tests were also calcu-lated. Logistic regression analysis was used to explorethe relationship between the occurrence of microbialinvasion of the amniotic cavity and various explanatoryvariables, including the results of the ultrasonographicexamination of the uterine cervix. Patients with a condi-tion requiring delivery (abruption, fetal distress, clinicalchorioamnionitis, fetal death/malformations, severe ma-ternal conditions) were excluded from the analysis of therelationship between cervical length and spontaneouspreterm delivery. A Kaplan-Meier survival analysis wasperformed to assess the examination-to-delivery intervalaccording to the results of cervical length determinedby transvaginal ultrasonography. Patients who were
Table I Clinical characteristics of the study population
Maternal age (y [mean G SD]) 24 G 8Gestational age at admission(wk [mean G SD])
31.1 G 2.8
Nulliparous (%, n) 48.9% (196/401)Multiparous (%, n) 51.1% (205/401)Previous preterm delivery (%, n) 14.9% (60/401)Delivery %35 wk (%, n) 26.8% (103/384)*Delivery %32 wk (%, n) 14.7% (27/184)*Delivery within 7 d (%, n) 20.3% (78/384)*Delivery within 48 h (%, n) 11.9% (46/384)*Microbial invasion of theamniotic cavity (%, n)
7% (28/401)
Gestational age at delivery(wk [mean G SD])
36.5 G 3.3*
Admission to delivery interval(d [median, range])
34 (0-123)*
* Excludes patients who were lost to follow-up (n = 17).
delivered preterm for maternal or fetal indicationswere included in the analysis with a censored time equalto the examination-to-intervention interval.
Results
Clinical and ultrasonographic characteristics ofpatient population
Four hundred and one patients met the entry criteria forthe study. Forty-six were either lost to follow-up(n = 17) or had an indication for delivery (n = 29)and were, thus, excluded from the analysis of therelationship between cervical length and spontaneouspreterm delivery. Table I describes the clinical character-istics of patients. Mean gestational age at admission was31.1 weeks (G 2.8), while mean gestational age atdelivery was 36.5 weeks (G 3.3). The median cervicallength was 27 mm (range 0-58.5 mm). Fifty-sevenpatients (14.2%) had a cervical length !15 mm, while161 (40.1%) had a cervical length R30 mm.
Relationship between cervical length andmicrobial invasion of the amniotic cavity
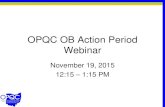
The prevalence of microbial invasion of the amnioticcavity was 7% (28/401), and the most common micro-organism isolated from amniotic fluid was Ureaplasmaurealyticum. Other microorganisms found were Myco-plasma hominis, Streptococcus viridans, Gardenerellavaginalis, Staphylococcus aureus, Listeria monocyto-genes, Candida albicans, and Prevotella sp. ROC curveanalysis showed that the curve constructed for cervicallength was above the 45-degree angle, indicating a sig-nificant relationship with the presence of a positiveamniotic fluid culture (area under the curve = 0.77,P ! .005, Figure 1). Patients with a cervical length !15mm had a higher rate of microbial invasion of theamniotic cavity than those with a cervical length R15mm (26.3% [15/57] vs 3.8% [13/344], respectively; P !.05). In contrast, patients with a cervical lengthR25 mm(n = 234) and R30 mm (n = 161) had a low risk ofmicrobial invasion of the amniotic cavity (2.6% [6/234]and 1.9% [3/161], respectively). Importantly, amongpatients with a gestational age at presentation %30weeks, those with a cervical length !15 mm had a 43%(9/21) risk of microbial invasion of the amniotic cavity,a rate significantly higher than those with a cervicallength R15 mm (3.9% [3/76], P ! .05] (see Table II).
A cut-off of 15 mm identified 54% (15/28) of patientswith microbial invasion of the amniotic cavity, witha specificity of 89% (331/373) and positive and negativepredictive values of 26% (15/57) and 96% (331/344),respectively. The likelihood ratios for a positive andnegative test were 4.7 and 0.5, respectively.

Gomez et al 681
Logistic regression analysis was performed to exam-ine the relationship between the occurrence of a positiveamniotic fluid culture and different clinical and ultraso-nographic variables. Univariate and multivariate anal-ysis demonstrated that cervical length was the strongestpredictor of microbial invasion of the amniotic cavity.When other clinical explanatory variables (gestationalage at admission, cervical status as assessed by digitalexamination, frequency of uterine contractions andothers) were added individually to the model, onlygestational age at admission and cervical length weresignificantly associated with the presence of microbialinvasion of the amniotic cavity (see Table III).
Therefore, in order to estimate the individual risk ofmicrobial invasion of the amniotic cavity in patientspresenting with preterm labor and intact membranes, wedeveloped a regression-based table that provides a spe-cific probability according to gestational age at admis-sion and the sonographic length of the uterine cervix(Table IV). The figures presented in the tables representestimates derived from mathematic modeling and notfrom empirical observations in each cell.
Relationship between cervical length andspontaneous preterm delivery
The prevalence of spontaneous preterm delivery %35weeks was 21.4% (82/384). Patients with an indicationfor preterm delivery were excluded from this analysis(see indications for delivery in Table VI). Patients witha cervical length !15 mm were more likely to deliverspontaneously before 35 weeks than those with a cervicallength R15 mm (66.7% [38/57] vs 13.5% [44/327],respectively; P ! .01). Also, patients with a cervicallength !15 mm had a higher frequency of delivery %32weeks, within 7 days, and within 48 hours of admissionthan those with a cervical length R15 mm (see Table V).On the other hand, patients with a cervical length R30mm (n = 154) had a very low risk of spontaneousdelivery %35 weeks (4.5% [7/154], %32 weeks (2.6% [2/76]), delivery within 7 days (1.9% [3/154]), and deliverywithin 48 hours of admission (0% [0/154]) (see Table V).
A cut-off of 15 mm had a sensitivity and specificity of46% (38/82) and 94% (283/302) for delivery%35 weeks,respectively, with positive and negative predictive valuesof 67% (38/57) and 87% (283/327), respectively. Likeli-hood ratios were 7.37 for a positive test and 0.57 fora negative test (similar indices were observed for delivery%32 weeks, within 7 days, and within 48 hours ofadmission) (see Table V).
Analysis of the duration of pregnancy accordingto cervical length results
A Kaplan-Meier survival analysis was performed toassess the examination-to-delivery interval according toresults of the cervical length, as determined by trans-
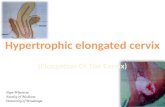
vaginal ultrasonography. Patients who were lost tofollow-up were excluded (n = 17). Patients with anindicated preterm delivery (n = 29) had their admis-sion-to-delivery interval censored. Indications for de-livery are described in Table VI. Patients with a cervicallength !15 mm had a significantly shorter admission-to-delivery interval than those with an endocervicalcanal R15 mm (median survival 4 days, 95% CI 2-6days vs median survival 39 days, 95% CI 36-42 days; P! .00001, log rank test, Figure 2, A). Similarly, patientswith a cervical length of R30 mm had a longeradmission-to-delivery interval than those with a cervicallength!30 mm (median survival 47 days, 95% CI 41-53days vs median survival 27 days, 95% CI 22-32 days,respectively; P ! .00001, log rank test, Figure 2, B).
Comment
Principal findings of this study:
This study demonstrates that (1) The shorter the cervixat presentation, the higher the likelihood of culture-proven microbial invasion of the amniotic cavity; and(2) Sonographic cervical length was the best parameterto assess the risk of intrauterine infection amongobstetrical clinical factors such as maternal temperature,digital examination of the cervix, frequency of uterinecontractions, and other historical information whichclinicians can elicit from patients (ie, history of pretermbirth and vaginal bleeding) in order to assess the risk of
Figure 1 ROC curve analysis showed that the curve con-structed for cervical length was above the 45-degree angle,
indicating a significant relationship with the presence ofa positive amniotic fluid culture (area under the curve = 0.77,P ! .005).

682 Gomez et al
Table II Risk of microbial invasion of the amniotic cavity (MIAC) according to cervical length and gestational age
Gestational age (wk)
Cervical length (mm) %35 %32 %30 %28
!15 26.3% (15/57) 33.3% (10/30) 42.9% (9/21) 45.5% (5/11)15-29 5.5% (10/183) 4.8% (4/84) 6.3% (2/32) 11.8% (2/17)R30 1.9% (3/161) 2.5% (2/79) 2.3% (1/44) 0% (0/24)Prevalence of MIAC 7.0% (28/401) 8.3% (16/193) 12.4% (12/97) 13.5% (7/52)
P ! .001 for all categories of gestational age (c2 for trend).
intrauterine infection (data can be provided upon re-quest).
The importance of microbial invasion of theamniotic cavity
Twenty-five percent of all preterm neonates are born towomen with microbial invasion of the amniotic cavity,as demonstrated by studies of amniotic fluid retrieved bytransabdominal amniocentesis and cultured with stan-dard microbiologic culture techniques.26 Patients withmicrobial invasion of the amniotic cavity are more likelyto develop maternal complications such as clinicalchorioamnionitis1 and pulmonary edema while receivingtocolysis,27as well as deliver a preterm neonate shortlyafter admission.1,28,29 Moreover, patients with microbialinvasion of the amniotic cavity show evidence ofhistologic chorioamnionitis (a maternal host response)and funisitis, the pathologic hallmark of the fetalinflammatory response syndrome (FIRS).30,31 FIRS isassociated with fetal multisystem involvement,32 includ-ing the hematologic system (increased number ofnucleated red blood cells, leukocytosis, etc),33 adrenalgland hyperactivity,34 cardiac dysfunction,35 and out-pouring of matrix degrading enzymes.36 Fetuses withFIRS are at increased risk not only for short-termmorbidity,5 but also long-term handicap such as cere-bral palsy13,14 and chronic lung disease.8,10 There is nowcompelling clinical2,37-39 and experimental40-43 evidencethat fetal exposure to infection and inflammation isassociated with adverse outcome. Thus, it would seemlogical that the optimal management of patients withpreterm labor would require knowledge of whether ornot there is intra-amniotic infection. Yet, some centerscontinue to treat patients with premature labor withoutthis determination. Reliance on clinical signs of infection
Table III Relationship between gestational age at admis-sion, cervical length, and microbial invasion of the amnioticcavity, analyzed by logistic regression
Odds ratio 95% CI
Gestational age at admission (wk) 0.87 0.76–0.99Cervical length (mm) 0.92 0.88–0.95
(eg, maternal chorioamnionitis) has been demonstratedfor over a decade to be insensitive.15-17
The optimal method to determine whether there isinfection/inflammation in the amniotic cavity is analysisof amniotic fluid.1,20,21 Thus, it is desirable to identifywomen at high risk for microbial invasion of theamniotic cavity. Maternal white blood cell count andC-reactive protein determinations have been demon-strated to have limitations, presumably because mostcases of amniotic fluid infection and fetal infection/inflammation may not be detected by these markers.16,17
Our study was conducted to determine if sonographiccervical length could assist in identifying women at riskfor intra-amniotic infection, and the results indicate thatsuch is the case.
Sonographic cervical length and microbialinvasion of the amniotic cavity
The main finding of this study, namely that a shortcervix is associated with an increased frequency ofmicrobial invasion of the amniotic cavity, confirms theobservations of Rizzo et al.44 They studied 144 patientswith preterm labor and intact membranes, and founda relationship between the cervical index (cervical funnellength C 1/cervical length) and the rate of positiveamniotic fluid culture for microorganisms. Our findingsextend these observations by comparing sonographiccervical length with other clinical parameters, and byproviding diagnostic indices, predictive values, andlikelihood ratios for the identification of microbialinvasion of the amniotic cavity. This information wasnot available in the literature.
It is noteworthy that the frequency of microbialinvasion of the amniotic cavity is higher the earlier thegestational age at presentation.1,45 Indeed, in 1992 wereported that microbial invasion of the amniotic cavitywas present in 55.1% (17/33) of patients presentingbetween 14 to 24 weeks of gestation with a cervicaldilatation R2 cm, intact membranes, and without activelabor.46 Other studies have subsequently confirmed thisobservation.47 The relationship between cervical lengthduring pregnancy and increased risk of perinatal in-fection has been the subject of study in the prediction ofprematurity. A short cervix has been considered to be an

Gomez et al 683
Table IV Estimated risk (%) of microbial invasion of the amniotic cavity in patients with preterm labor and intact membranes,according to gestational age and the cervical length as measured by transvaginal ultrasound
Gestational age (wk)
CL (mm) 22 23 24 25 26 27 28 29 30 31 32 33 34
1 59 56 53 50 46 43 40 37 34 31 28 26 232 57 54 51 48 44 41 38 35 32 29 27 24 223 55 52 49 45 42 39 36 33 30 28 25 23 214 53 50 47 43 40 37 34 31 29 26 24 21 195 51 48 45 41 38 35 32 30 27 24 22 20 186 49 46 43 39 36 33 31 28 25 23 21 19 177 47 44 40 37 34 32 29 26 24 21 19 17 168 45 42 38 35 33 30 27 25 22 20 18 16 159 43 40 37 34 31 28 25 23 21 19 17 15 1410 41 38 35 32 29 26 24 22 20 18 16 14 1311 39 36 33 30 27 25 22 20 18 16 15 13 1212 37 34 31 28 26 23 21 19 17 15 14 12 1113 35 32 29 27 24 22 20 18 16 14 13 11 1014 33 30 27 25 23 20 18 17 15 13 12 11 915 31 28 26 23 21 19 17 15 14 12 11 10 916 29 27 24 22 20 18 16 14 13 11 10 9 817 28 25 23 21 19 17 15 13 12 11 9 8 718 26 24 21 19 17 16 14 12 11 10 9 8 719 24 22 20 18 16 14 13 12 10 9 8 7 620 23 21 19 17 15 13 12 11 10 8 8 7 621 22 19 17 16 14 13 11 10 9 8 7 6 522 20 18 16 15 13 12 10 9 8 7 6 6 523 19 17 15 14 12 11 10 9 8 7 6 5 524 18 16 14 13 11 10 9 8 7 6 5 5 425 16 15 13 12 10 9 8 7 6 6 5 4 426 15 14 12 11 10 9 8 7 6 5 5 4 427 14 13 11 10 9 8 7 6 6 5 4 4 328 13 12 11 9 8 7 7 6 5 5 4 4 329 12 11 10 9 8 7 6 5 5 4 4 3 330 11 10 9 8 7 6 6 5 4 4 3 3 331 11 9 8 7 7 6 5 5 4 4 3 3 232 10 9 8 7 6 5 5 4 4 3 3 3 233 9 8 7 6 6 5 4 4 3 3 3 2 234 8 8 7 6 5 5 4 4 3 3 2 2 235 8 7 6 5 5 4 4 3 3 3 2 2 236 7 6 6 5 4 4 3 3 3 2 2 2 237 7 6 5 5 4 4 3 3 2 2 2 2 138 6 5 5 4 4 3 3 3 2 2 2 2 139 6 5 4 4 3 3 3 2 2 2 2 1 140 5 5 4 4 3 3 3 2 2 2 2 1 1
Based on a population with preterm labor and intact membranes, cervical dilatation of !3 cm, no clinical chorioamnionitis at admission, and a 7% rate
of microbial invasion of the amniotic cavity.
independent risk factor for the subsequent developmentof clinical chorioamnionitis and neonatal sepsis.48
The most common organism isolated from the amni-otic cavity is Ureaplasma urealyticum, which has beendemonstrated to be associatedwith a robust host responsein amniotic fluid, maternal and fetal compartments inpatients presenting with preterm labor or preterm pre-mature rupture of membranes (PROM).49-52 Comparedwith patients with sterile amniotic fluid, those who hada positive culture forUreaplasma urealyticum in amniotic
fluid had a higher amniotic fluid concentration of proin-flammatory cytokines, including tumor necrosis factor-alpha, interleukin (IL)-1 beta and IL-6, higher plasmaconcentration of IL-6 in umbilical cord blood, higherprevalence of histologic chorioamnionitis, higher risk ofimpending preterm delivery, and adverse perinatal out-come.49-52
In order to assist clinicians in assessing the risk ofmicrobial invasion of the amniotic cavity in patientspresenting with preterm labor and intact membranes, we

684 Gomez et al
Table V Frequency and likelihood ratio of spontaneous preterm delivery according to cervical length
Cervicallength (mm)
Delivery %35 wk Delivery %32 wk Delivery within 7 d Delivery within 48 h
% LR % LR % LR % LR
C / � C / � C / � C / �!15 66.7% (38/57) 7.37 56.7% (17/30) 7.60 59.6% (34/57) 7.39 38.6% (22/57) 5.72R15 13.5% (44/327) 0.57 6.5% (10/154) 0.40 9.2% (30/327) 0.51 4.9% (16/327) 0.47!30 32.6% (75/230) 1.78 23.1% (25/108) 1.75 26.5% (61/230) 1.81 16.5% (38/230) 1.78R30 4.5% (7/154) 0.18 2.6% (2/76) 0.16 1.9% (3/154) 0.09 0% (0/154) 0.03Prevalence 21.4% (82/384) 14.7% (27/184) 16.7% (64/384) 9.9% (38/384)
LR, Likelihood ratio. Prevalence was calculated excluding patients who were lost to follow-up. Indicated preterm delivery was not included in the
calculations of spontaneous preterm delivery rate.
have generated tables which include the calculatedprobability of microbial invasion according to gesta-tional age at presentation and cervical length, the twofactors strongly associated with the likelihood of a pos-itive culture (Table IV). The implications of thesefindings are straightforward. The shorter the cervixand the earlier the gestational age, the higher the riskof infection. For example, 43% of women with pretermlabor and a cervix of less than 15 mm presenting before30 weeks will have a positive amniotic fluid culture. Onthe other hand, patients with a long cervix (R30 mm)presenting with preterm labor late in pregnancy (eg,after 32 weeks) are unlikely to have microbial invasionof the amniotic cavity.
Why is microbial invasion of the amniotic cavitymore frequent in patients with a sonographically shortcervix? Two possibilities can be considered. First,patients could have microbial invasion of the amnioticcavity as a cause of preterm labor, and a short cervixsimply represents recruitment of the cervical componentof ‘‘the common terminal pathway of parturition’’53 (seebelow). The other alternative is that a short cervix maypredispose to ascending intrauterine infection.
The term ‘‘common terminal pathway of parturition’’describes the anatomic, biochemical, endocrinologic,and clinical events that occur in both mother and/or
Table VI Principal indications for delivery
Indication n
Preeclampsia/eclampsia 5Clinical chorioamnionitis 4Placental abruption 4Stillbirth 4Preterm PROM(near term, oligohydramnios, or with MIAC)
4
Abnormal fetalheart rate/umbilical Doppler
3
Chronic hypertension 2Appendicitis 1Symptomatic placenta previa 1Cord prolapse 1
fetus in term, as well as preterm labor.53 The uterinecomponents of this terminal pathway are: (1) increasedmyometrial contractility; (2) cervical ripening; and (3)membrane/decidual activation. Each component can bestudied through a different test. For example, a tocody-namometer has been used to determine the frequency ofmyometrial contractility,54,55 ultrasound to assess cervi-cal ripening,56-58 and fetal fibronectin as presumably anearly marker of membrane/decidual activation.59-62 Ashort cervix is the imaging equivalent to ‘‘an effacedcervix’’ or ‘‘ripened cervix.’’
It is now known that some women have microbialinvasion of the amniotic cavity at the time of mid-trimester amniocentesis. These patients can have a spon-taneous abortion or a spontaneous preterm deliveryweeks after the amniocentesis.63,64 It is likely that‘‘chronic intra-amniotic infection’’ is the cause of pre-term delivery for these patients. The clinical presenta-tion may be either conventional ‘‘preterm labor,’’ whichis the synchronous activation of the 2 or 3 componentsof the terminal pathway (such as increased myometrialcontractility and cervical ripening), or asynchronousactivation. We use the term asynchronous activationwhen patients present predominantly with one of thefollowing: preterm contractions, a dilated cervix, orpreterm PROM. In these cases, the predominant clinicalfeature can be linked to a single component of thepathway, although there may be subclinical activationof the others. For example, patients with preterm labormay have a positive fetal fibronectin and, hence, sub-clinical evidence of membrane/decidual activation with-out preterm PROM. Membrane rupture represents theextreme and generally irreversible form of membrane/decidual activation. The patient with chronic intra-amniotic infection can present with preterm labor withintact membranes with a short cervix. The higherfrequency of positive amniotic cultures in patients witha short cervix merely reflects the fact that patients withinfection have true preterm labor and, thus, recruitmentof the cervical component of the pathway.
Yet, other patients have a short cervix for days orweeks. The short cervix may result in loss of the mucus

Gomez et al 685
plug, which is not only a mechanical barrier but alsoa component of the innate immune system.65 Thecervical mucus has antimicrobial properties,66 and thecervical epithelium expresses a series of pattern recog-nition receptors67 that can sense the presence of micro-organisms and orchestrate an immune response.68,69
Patients with a short cervix and changes in themicrobial ecosystem of the lower genital tract couldhave ascending intra-amniotic infection.70 The fact thatintra-amniotic infection is a secondary event does notdecrease its importance as a mechanism of preterm labor,although we predict that the fetal attack rate for fetalinfection and FIRS is different for chronic infections,which may last weeks, and recent infection lasting onlyhours or days.
Clinical implications
Our observations suggest that it is possible to assess thelikelihood of microbial invasion of the amniotic cavitybased upon information easily obtained in clinical care:sonographic cervical length and gestational age. Pleasenote that Table IV is also freely accessible on thejournal’s web site. This information could be used toassess when to perform an amniocentesis. However, therisk of microbial invasion of the amniotic cavity remainsfinite even in patients with a long cervix and advancedgestational age.
A clinical challenge is the optimal management ofa patient with microbial invasion of the amniotic cavity.The difficulty derives from the risks that clinicians facewhile balancing the management (ie, immaturity vsprolonged exposure to infection/inflammation) withthe constraints to research in vulnerable patients (preg-nant women and fetuses).
Is there evidence that treating microbial invasion ofthe amniotic cavity could be beneficial? There is norandomized clinical trial specifically designed for pre-term gestation in which patients with microbial invasionof the amniotic cavity detected by amniocentesis havebeen randomized to antibiotics or continued exposure ofthe fetus to infection in utero (placebo or no treatment).However, this should not be interpreted as absence ofevidence that treatment of infection may not be bene-ficial. For example, two retrospective studies concludedthat the rate of neonatal sepsis was lower in patientswith clinical chorioamnionitis treated with antibioticsbefore delivery than in neonates treated immediatelyafter birth.71,72 The only randomized trial in whichpatients with clinical chorioamnionitis (preterm andterm neonates, but mostly term neonates O34 weeks)were randomized to either immediate intrapartumtreatment vs antibiotic treatment of the neonate afterclamping of the umbilical cord was stopped by a Dataand Safety Monitoring Committee because of a signifi-cant excess of neonatal sepsis in the group allocated to
delayed treatment.73 Gibbs et al concluded that treat-ment with antibiotics should be initiated immediatelyupon the diagnosis of clinical chorioamnionitis.73 Inaddition, there is evidence that parenteral antibioticadministration can cross the placenta.74,75 There is alsoexperimental evidence in several species that treatmentof intrauterine infection with antibiotics76 and other
Figure 2 Cumulative survival of patients according tocervical length measured by ultrasound (for cut-offs of 15
mm (A) and 30 mm (B). A Kaplan-Meier survival analysis wasperformed to assess the examination-to-delivery interval ac-cording to the results of the cervical length as determined by
transvaginal ultrasonography. Patients who were lost tofollow-up were excluded (n = 17). Patients with an indicatedpreterm delivery (n = 29) had their admission-to-deliveryinterval censored. Patients with a cervical length !15 mm
had a significantly shorter admission-to-delivery interval thanpatients with an endocervical canal R15 mm (median survival4 days, 95% CI, 2-6 days vs median survival 39 days, 95% CI,
36-42 days; P ! .00001, log rank test) (A). Similarly, patientswith a cervical length of 30 mm or greater had a longeradmission-to-delivery interval than patients with a cervical
length less than 30 mm (median survival 47 days, 95% CI, 41-53 days vs median survival 27 days, 95% CI 22-32 days,respectively; P ! .00001, log rank test) (B).

686 Gomez et al
biological response modifiers improves pregnancy out-come.77
It could be argued that the results of uncontrolledstudies and those of the randomized clinical trial citedabove are not applicable to preterm gestations withmicrobial invasion of the amniotic cavity because mostfetuses were at term rather than preterm. There are,however, problems with this line of reasoning. Thepreterm fetus and neonate have been widely consideredas ‘‘an immunocompromised host’’ in comparison withthe term fetus/neonate. This is based upon both clinicalstudies indicating that the lethality rate of neonatalsepsis is higher in preterm than term neonates,78,79 aswell as the examination of the immune response of thepreterm neonate.80,81 Therefore, arguing that antibioticsmay be beneficial to the term but not the preterm fetusesimplies that an immunocompromised host does notbenefit from early antibiotic treatment when exposedto microorganisms. This reasoning contradicts a largebody of evidence that has informed medical practice ofthe immunocompromised host. Thus, unless evidencethat prolonged exposure to bacteria is harmless topreterm fetuses is presented, withholding antibiotictreatment is contrary to medical practice. Indeed,experimental40,41,43,82 and clinical2,37-39 evidence sug-gests that acute and chronic intrauterine infection couldbe harmful to the fetus.
The argument could also be made that the results ofa trial of clinical chorioamnionitis should not beextrapolated to women with microbial invasion of theamniotic cavity without clinical chorioamnionitis. Thedifficulty here is that clinical chorioamnionitis is a ma-ternal and not a fetal host response, and it is the fetalinflammatory response that has been implicated in fetalinjury.5,10 There is no evidence at this time that the lackof a maternal host response protects the fetus from mi-crobial invasion of the amniotic cavity and the adverseconsequences of a fetal inflammatory response.
The optimal experimental approach required toanswer the question is to conduct a randomized clinicaltrial in which amniocenteses are used to identifymicrobial invasion of the amniotic cavity, with thepatients being randomized to either treatment withantibiotics or no treatment (or placebo). This trialwould be difficult to undertake as the current regula-tions state that fetuses should not be exposed to invasiveprocedures that are not directly beneficial to the in-dividual fetus. It is unclear whether the current frame-work governing research in fetuses could permit thata group of patients with infection be allocated to notreatment or placebo. It is not difficult to foreseemothers refusing to participate in such a trial afterbeing counseled that antibiotic treatment of term fetusesexposed to infection reduces the rate of neonatal sepsis.Thus, this question may need to be addressed by a clusterrandomized trial or another variation of this design.
An unanswered question: The relationshipbetween cervical length and intra-amnioticinflammation
The current study focused on the relationship betweenmicrobial invasion of the amniotic cavity and cervicallength. The rationale for our interest in intra-amnioticinfection is that the detection of microorganisms inamniotic fluid with culture techniques is the gold stan-dard for the diagnosis of intra-amniotic infection.However, there is now accumulating evidence thatintra-amniotic inflammation may be as important asmicrobial invasion detected by standard microbiologictechniques in determining adverse pregnancy and neo-natal outcome.83,84 Therefore, future studies need toexamine the relationship between cervical length andintra-amniotic inflammation, as well as cervical lengthand the detection of microbial footprints with sensitivemolecular microbiologic techniques.52,85,86
References
1. Romero R, Sirtori M, Oyarzun E, Avila C, Mazor M, Callahan R,
et al. Infection and labor: V. Prevalence, microbiology, and clinical
significance of intraamniotic infection in women with preterm labor
and intact membranes. Am J Obstet Gynecol 1989;161:817-24.
2. Hillier SL, Krohn MA, Kiviat NB, Watts DH, Eschenbach DA.
Microbiologic causes and neonatal outcomes associated with
chorioamnion infection. Am J Obstet Gynecol 1991;165:955-61.
3. Garite TJ, Freeman RK. Chorioamnionitis in the preterm gesta-
tion. Obstet Gynecol 1982;59:539-45.
4. Newton ER. Chorioamnionitis and intraamniotic infection. Clin
Obstet Gynecol 1993;36:795-808.
5. Gomez R, Romero R, Ghezzi F, Yoon BH, Mazor M, Berry SM.
The fetal inflammatory response syndrome. Am J Obstet Gynecol
1998;179:194-202.
6. Yoon BH, Romero R, Kim CJ, Jun JK, Gomez R, Choi JH, et al.
Amniotic fluid interleukin-6: a sensitive test for antenatal diagnosis
of acute inflammatory lesions of preterm placenta and prediction
of perinatal morbidity. Am J Obstet Gynecol 1995;172:960-70.
7. Seo K, McGregor JA, French JI. Preterm birth is associated with
increased risk of maternal and neonatal infection. Obstet Gynecol
1992;79:75-80.
8. Ghezzi F, Gomez R, Romero R, Yoon BH, Edwin SS, David C,
et al. Elevated interleukin-8 concentrations in amniotic fluid of
mothers whose neonates subsequently develop bronchopulmonary
dysplasia. Eur J Obstet Gynecol Reprod Biol 1998;78:5-10.
9. Watterberg K, Demers L, Scott S, Murphy S. Chorioamnionitis
and early lung inflammation in infants in whom broncho-
pulmonary dysplasia develops. Pediatrics 1996;97:210-5.
10. Yoon BH, Romero R, Kim KS, Park JS, Ki SH, Kim BI, et al. A
systemic fetal inflammatory response and the development of
bronchopulmonary dysplasia. Am J Obstet Gynecol 1999;181:
773-9.
11. Yoon BH, Romero R, Jun JK, Park KH, Yang SH, Kim IO, et al.
Amniotic fluid concentrations of interleukin 6 identify fetuses at
risk for the development of periventricular leucomalacia. Am J
Obstet Gynecol 1996;174:330.
12. Yoon BH, Romero R, Yang SH, Jun JK, Kim IO, Choi JH, et al.
Interleukin-6 concentrations in umbilical cord plasma are elevated
in neonates with white matter lesions associated with periventric-
ular leukomalacia. Am J Obstet Gynecol 1996;174:1433-40.

Gomez et al 687
13. Yoon BH, Jun JK, Romero R, Park KH, Gomez R, Choi JH, et al.
Amniotic fluid inflammatory cytokines (interleukin-6, interleukin-
1beta, and tumor necrosis factor-alpha), neonatal brain whitematter
lesions, and cerebral palsy. Am J Obstet Gynecol 1997;177:19-26.
14. Yoon BH, Romero R, Park JS, Kim CJ, Kim SH, Choi JH, et al.
Fetal exposure to an intra-amniotic inflammation and the de-
velopment of cerebral palsy at the age of three years. Am J Obstet
Gynecol 2000;182:675-81.
15. Carroll SG, Papaioannou S, Davies ET, Nicolaides KH. Maternal
assessment in the prediction of intrauterine infection in preterm
prelabor amniorrhexis. Fetal Diagn Ther 1995;10:290-6.
16. Yoon BH, Jun JK, Park KH, Syn HC, Gomez R, Romero R.
Serum C-reactive protein, white blood cell count, and amniotic
fluid white blood cell count in women with preterm premature
rupture of membranes. Obstet Gynecol 1996;88:1034-40.
17. Yoon BH, Yang SH, Jun JK, Park KH, Kim CJ, Romero R.
Maternal blood C-reactive protein, white blood cell count, and
temperature in preterm labor: a comparison with amniotic fluid
white blood cell count. Obstet Gynecol 1996;87:231-7.
18. Romero R, Emamian M, Quintero R, Wan M, Hobbins JC,
Mazor M, et al. The value and limitations of the Gram stain
examination in the diagnosis of intraamniotic infection. Am J
Obstet Gynecol 1988;159:114-9.
19. Romero R, Jimenez C, Lohda AK, Nores J, Hanaoka S, Avila C,
et al. Amniotic fluid glucose concentration: a rapid and simple
method for the detection of intraamniotic infection in preterm
labor. Am J Obstet Gynecol 1990;163:968-74.
20. Romero R, Quintero R, Nores J, Avila C, Mazor M, Hanaoka S,
et al. Amniotic fluid white blood cell count: a rapid and simple test
to diagnose microbial invasion of the amniotic cavity and predict
preterm delivery. Am J Obstet Gynecol 1991;165:821-30.
21. Romero R, Yoon B, Mazor M, Gomez R, Gonzalez R, Diamond
MP, et al. A comparative study of the diagnostic performance of
amniotic fluid glucose, white blood cell count, interleukin-6, and
Gram stain in the detection of microbial invasion in patients with
preterm premature rupture of membranes. Am J Obstet Gynecol
1993;169:839-51.
22. Romero R, Yoon B, Mazor M, Gomez R, Diamond MP, Kenney
JS, et al. The diagnostic and prognostic value of amniotic fluid
white blood cell count, glucose, interleukin-6, and Gram stain in
patients with preterm labor and intact membranes. Am J Obstet
Gynecol 1993;169:805-16.
23. Armer TL, Duff P. Intraamniotic infection in patients with intact
membranes and preterm labor. Obstet Gynecol Surv 1991;46:
589-93.
24. Gomez R, Romero R, Medina L, Nien JK, Chaiworapongsa T,
Carstens M, et al. Cervico-vaginal fibronectin improves the
prediction of preterm delivery based upon sonographic cervical
length in patients with preterm labor and intact membranes. Am J
Obstet Gynecol 2005;192:350-9.
25. Gibbs R, Blanco J, St Clair P, Castaneda Y. Quantitative
bacteriology of amniotic fluid from women with clinical intra-
amniotic infection at term. J Infect Dis 1982;145:1-8.
26. Romero R, Espinoza J, Chaiworapongsa T, Kalache K. Infection
and prematurity and the role of preventive strategies. Semin
Neonatol 2002;7:259-74.
27. Hatjis CG, Swain M. Systemic tocolysis for premature labor is
associated with an increased incidence of pulmonary edema in the
presence of maternal infection. Am J Obstet Gynecol
1988;159:723-8.
28. Hameed C, Tejani N, Verma UL, Archibald F. Silent chorioam-
nionitis as a cause of preterm labor refractory to tocolytic therapy.
Am J Obstet Gynecol 1984;149:726-30.
29. Romero R, Quintero R, Oyarzun E, Wu YK, Sabo V, Mazor M,
et al. Intraamniotic infection and the onset of labor in preterm
premature rupture of the membranes. Am J Obstet Gynecol
1988;159:661-6.
30. Yoon BH, Romero R, Park JS, Kim M, Oh SY, Kim CJ, et al. The
relationship among inflammatory lesions of the umbilical cord
(funisitis), umbilical cord plasma interleukin 6 concentration,
amniotic fluid infection, and neonatal sepsis. Am J Obstet Gynecol
2000;183:1124-9.
31. Pacora P, Chaiworapongsa T, Maymon E, Kim YM, Gomez R,
Yoon BH, et al. Funisitis and chorionic vasculitis: the histological
counterpart of the fetal inflammatory response syndrome. J
Matern Fetal Neonatal Med 2002;11:18-25.
32. Romero R, Chaiworapongsa T, Espinoza J. Micronutrients and
intrauterine infection, preterm birth and the fetal inflammatory
response syndrome. J Nutr 2003;133:1668S-73S.
33. Berry SM, Gomez R, Athayde N, Ghezzi F, Mazor M, Yoon BH,
et al. The role of granulocyte colony stimulating factor in the
neutrophilia observed in the fetal inflammatory response syn-
drome. Am J Obstet Gynecol 1998;178:S202.
34. Yoon BH, Romero R, Jun JK, Maymon E, Gomez R, Mazor M,
et al. An increase in fetal plasma cortisol but not dehydroepian-
drosterone sulfate is followed by the onset of preterm labor in
patients with preterm premature rupture of the membranes. Am J
Obstet Gynecol 1998;179:1107-14.
35. Romero R, Gomez R, Ghezzi F, Maymon E, Yoon BH, Mazor M,
et al. A novel form of fetal cardiac dysfunction in preterm
premature rupture of membranes. Am J Obstet Gynecol 1999;
180:S27.
36. Romero R, Athayde N, Gomez R, Mazor M, Yoon BH, Edwin S,
et al. The fetal inflammatory response syndrome is characterized
by the outpouring of a potent extracellular matrix degrading
enzyme into the fetal circulation. Am J Obstet Gynecol 1998;
178:S3.
37. Dammann O, Leviton A. Maternal intrauterine infection, cyto-
kines, and brain damage in the preterm newborn. Pediatr Res
1997;42:1-8.
38. Goldenberg RL, Hauth JC, Andrews WW. Intrauterine infection
and preterm delivery. N Engl J Med 2000;342:1500-7.
39. Yoon BH, Park CW, Chaiworapongsa T. Intrauterine infection
and the development of cerebral palsy. BJOG 2003;110(Suppl
20):124-7.
40. Dombroski RA, Woodard DS, Harper MJ, Gibbs RS. A rabbit
model for bacteria-induced preterm pregnancy loss. Am J Obstet
Gynecol 1990;163:1938-43.
41. Yoon BH, Kim CJ, Romero R, Jun JK, Park KH, Choi ST, et al.
Experimentally induced intrauterine infection causes fetal brain
white matter lesions in rabbits. Am J Obstet Gynecol 1997;177:
797-802.
42. Gravett MG, Haluska GJ, Cook MJ, Novy MJ. Fetal and
maternal endocrine responses to experimental intrauterine in-
fection in rhesus monkeys. Am J Obstet Gynecol 1996;174:
1725-31.
43. Gibbs RS, Davies JK, McDuffie RS Jr, Leslie KK, Sherman MP,
Centretto CA, et al. Chronic intrauterine infection and inflamma-
tion in the preterm rabbit, despite antibiotic therapy. Am J Obstet
Gynecol 2002;186:234-9.
44. Rizzo G, Capponi A, Vlachopoulou A, Angelini E, Grassi C,
Romanini C. Ultrasonographic assessment of the uterine cervix
and interleukin-8 concentrations in cervical secretions predict
intrauterine infection in patients with preterm labor and intact
membranes. Ultrasound Obstet Gynecol 1998;12:86-92.
45. Watts DH, Krohn MA, Hillier SL, Eschenbach DA. The
association of occult amniotic fluid infection with gestational age
and neonatal outcome among women in preterm labor. Obstet
Gynecol 1992;79:351-7.
46. Romero R, Gonzalez R, Sepulveda W, Brandt F, Ramirez M,
Sorokin Y, et al. Infection and labor: VIII. Microbial invasion of
the amniotic cavity in patients with suspected cervical incompe-
tence: prevalence and clinical significance. Am J Obstet Gynecol
1992;167:1086-91.

688 Gomez et al
47. Mays JK, Figueroa R, Shah J, Khakoo H, Kaminsky S, Tejani N.
Amniocentesis for selection before rescue cerclage. Obstet Gynecol
2000;95:652-5.
48. Iams JD, for the NICHD MFMU Network. MAternal Fetal
MedicineUnitNetwork,BM.ThePretermPredictionStudy: cervical
length and perinatal infection. Am J Obstet Gynecol 1997;176:S6.
49. Yoon BH, Romero R, Park JS, Chang JW, Kim YA, Kim JC, et al.
Microbial invasion of the amniotic cavity with Ureaplasma urealy-
ticum is associatedwith a robust host response in fetal, amniotic, and
maternal compartments. Am J Obstet Gynecol 1998;179:1254-60.
50. Yoon BH, Chang JW, Romero R. Isolation of Ureaplasma
urealyticum from the amniotic cavity and adverse outcome in
preterm labor. Obstet Gynecol 1998;92:77-82.
51. Yoon BH, Romero R, Kim M, Kim EC, Kim T, Park JS, et al.
Clinical implications of detection of Ureaplasma urealyticum in
the amniotic cavity with the polymerase chain reaction. Am J
Obstet Gynecol 2000;183:1130-7.
52. Yoon BH, Romero R, Lim JH, Shim SS, Hong JS, Shim JY, et al.
The clinical significance of detecting Ureaplasma urealyticum by
the polymerase chain reaction in the amniotic fluid of patients with
preterm labor. Am J Obstet Gynecol 2003;189:919-24.
53. ChaiworapongsaT,Espinoza J,KalacheK,GervasiMT,RomeroR.
Sonographic examination of the uterine cervix. In: Chervenak FA,
editor. The fetus as a patient. London (UK): Parthenon Publishing;
2002. p. 90-117.
54. Iams JD, Johnson FF, Hamer C. Uterine activity and symptoms as
predictors of preterm labor. Obstet Gynecol 1990;76:42S-6S.
55. Newman RB, Richmond GS, Winston YE, Hamer C, Katz M.
Antepartum uterine activity characteristics differentiating true
from threatened preterm labor. Obstet Gynecol 1990;76:39S-41S.
56. Andersen HF, Nugent CE, Wanty SD, Hayashi RH. Prediction of
risk for preterm delivery by ultrasonographic measurement of
cervical length. Am J Obstet Gynecol 1990;163:859-67.
57. Iams JD, Goldenberg RL, Meis PJ, Mercer BM, Moawad A, Das
A, et al. The length of the cervix and the risk of spontaneous
premature delivery. National Institute of Child Health and Human
Development Maternal Fetal Medicine Unit Network. N Engl J
Med 1996;334:567-72.
58. Hassan SS, Romero R, Berry SM, Dang K, Blackwell SC,
Treadwell MC, et al. Patients with an ultrasonographic cervical
length ! or =15 mm have nearly a 50% risk of early spontaneous
preterm delivery. Am J Obstet Gynecol 2000;182:1458-67.
59. Lockwood CJ, Senyei AE, Dische MR, Casal D, Shah KD, Thung
SN, et al. Fetal fibronectin in cervical and vaginal secretions as
a predictor of preterm delivery. N Engl J Med 1991;325:669-74.
60. Iams JD, Casal D, McGregor JA, Goodwin TM, Kreaden US,
Lowensohn R, et al. Fetal fibronectin improves the accuracy of
diagnosis of preterm labor. Am J Obstet Gynecol 1995;173:141-5.
61. Goldenberg RL, Mercer BM, Meis PJ, Copper RL, Das A,
McNellis D. The preterm prediction study: fetal fibronectin testing
and spontaneous preterm birth. NICHD Maternal Fetal Medicine
Units Network. Obstet Gynecol 1996;87:643-8.
62. Leitich H, Egarter C, Kaider A, Hohlagschwandtner M, Berg-
hammer P, Husslein P. Cervicovaginal fetal fibronectin as a marker
for preterm delivery: a meta-analysis. Am J Obstet Gynecol
1999;180:1169-76.
63. Cassell GH, Davis RO, Waites KB, Brown MB, Marriott PA,
Stagno S, et al. Isolation of Mycoplasma hominis and Ureaplasma
urealyticum from amniotic fluid at 16-20 weeks of gestation:
potential effect on outcome of pregnancy. Sex Transm Dis
1983;10:294-302.
64. Horowitz S, Mazor M, Romero R, Horowitz J, Glezerman M.
Infection of the amniotic cavity with Ureaplasma urealyticum in
the midtrimester of pregnancy. J Reprod Med 1995;40:375-9.
65. Hein M, Valore EV, Helmig RB, Uldbjerg N, Ganz T. Antimi-
crobial factors in the cervical mucus plug. Am J Obstet Gynecol
2002;187:137-44.
66. Hein M, Helmig RB, Schonheyder HC, Ganz T, Uldbjerg N. An in
vitro study of antibacterial properties of the cervical mucus plug in
pregnancy. Am J Obstet Gynecol 2001;185:586-92.
67. Kim YM, Kim M, Kim G, Chaiworapongsa T, Gomez R,
Camacho N, et al. The uterine cervix expresses the pattern-
recognition receptors: toll-like receptors-2 and -4. Am J Obstet
Gyn 2004;189:S103.
68. Svinarich D, Wolf N, Gomez R, et al. Detection of human
defensin-5 in reproductive tissues. Am J Obstet Gynecol
1997;176:470-5.
69. Quayle AJ, Porter EM, Nussbaum AA, Wang YM, Brabec C, Yip
KP, et al. Gene expression, immunolocalization, and secretion of
human defensin-5 in human female reproductive tract. Am J
Pathol 1998;152:1247-58.
70. Hillier SL, Nugent RP, Eschenbach DA, Krohn MA, Gibbs RS,
Martin DH, et al. Association between bacterial vaginosis and
preterm delivery of a low-birth-weight infant. The Vaginal
Infections and Prematurity Study Group. N Engl J Med
1995;333:1737-42.
71. Sperling RS, Ramamurthy RS, Gibbs RS. A comparison of
intrapartum versus immediate postpartum treatment of intra-
amniotic infection. Obstet Gynecol 1987;70:861-5.
72. Gilstrap LC III, Leveno KJ, Cox SM, Burris JS, Mashburn M,
Rosenfeld CR. Intrapartum treatment of acute chorioamnionitis:
impact on neonatal sepsis. Am J Obstet Gynecol 1988;
159:579-83.
73. Gibbs RS, Dinsmoor MJ, Newton ER, Ramamurthy RS. A
randomized trial of intrapartum versus immediate postpartum
treatment of women with intra-amniotic infection. Obstet Gynecol
1988;72:823-8.
74. Maberry MC, Trimmer KJ, Bawdon RE, Sobhi S, Dax JB.
Gilstrap LC III. Antibiotic concentration in maternal blood,
cord blood and placental tissue in women with chorioamnionitis.
Gynecol Obstet Invest 1992;33:185-6.
75. Heikkinen T, Laine K, Neuvonen PJ, Ekblad U. The trans-
placental transfer of the macrolide antibiotics erythromycin,
roxithromycin and azithromycin. BJOG 2000;107:770-5.
76. Fidel P, Ghezzi F, Romero R, Chaiworapongsa T, Espinoza J,
Cutright J, et al. The effect of antibiotic therapy on intrauterine
infection-induced preterm parturition in rabbits. J Matern Fetal
Neonatal Med 2003;14:57-64.
77. Gravett M, Sadowsky DW, Witkin S, Novy M. Immunomodula-
tors plus antibiotics to prevent preterm delivery in experimental
intra-amniotic infection (IAI). Am J Obstet Gyn 2004;189:S56.
78. Stoll BJ, Gordon T, Korones SB, Shankaran S, Tyson JE, Bauer
CR, et al. Early-onset sepsis in very low birth weight neonates:
a report from the National Institute of Child Health and Human
Development Neonatal Research Network. J Pediatr 1996;129:
72-80.
79. Holmgren PA, Hogberg U. The very preterm infantda popula-
tion-based study. Acta Obstet Gynecol Scand 2001;80:525-31.
80. Falconer AE, Carr R, Edwards SW. Impaired neutrophil phago-
cytosis in preterm neonates: lack of correlation with expression of
immunoglobulin or complement receptors. Biol Neonate
1995;68:264-9.
81. Kallman J, Schollin J, Schalen C, Erlandsson A, Kihlstrom E.
Impaired phagocytosis and opsonisation towards group B strep-
tococci in preterm neonates. Arch Dis Child Fetal Neonatal
1998;78:F46-50.
82. Gravett MG, Witkin SS, Haluska GJ, Edwards JL, Cook MJ,
Novy MJ. An experimental model for intraamniotic infection and
preterm labor in rhesus monkeys. Am J Obstet Gynecol
1994;171:1660-7.
83. Shim S, Yoon BH, Romero R, Hong JS, Kim G, Sohn Y, et al.
The frequency and clinical significance of intra-amniotic inflam-
mation in patients with preterm premature rupture of the
membranes. Am J Obstet Gynecol 2004;189:S83.

Gomez et al 689
84. Yoon BH, Romero R, Moon JB, Shim SS, Kim M, Kim G, et al.
Clinical significance of intra-amniotic inflammation in patients
with preterm labor and intact membranes. Am J Obstet Gynecol
2001;185:1130-6.
85. Yankowitz J, Weinter CP, Henderson J, Grant S, Towbin JA.
Outcome of low-risk pregnancies with evidence of intraamniotic
viral infection detected by PCR on amniotic obtained at second
trimester genetic amniocentesis. J Soc Gynecol Invest 1996;3:132.
86. Oyarzun E, Yamamoto M, Kato S, Gomez R, Lizama L, Moenne
A. Specific detection of 16 micro-organisms in amniotic fluid by
polymerase chain reaction and its correlation with preterm delivery
occurrence. Am J Obstet Gynecol 1998;179:1115-9.
Supplemental material
A complete version of this manuscript with an expandedset of references is available online at www.ajog.org.