
A REVIEW OF SANITATION PROGRAM …pdf.usaid.gov/pdf_docs/PNACB331.pdfEHP Activity Report No. 5 A...
79
EHP Activity Report No. 5 A REVIEW OF A REVIEW OF SANITATION PROGRAM EVALUATIONS SANITATION PROGRAM EVALUATIONS IN DEVELOPING COUNTRIES IN DEVELOPING COUNTRIES Anne K. LaFond February 1995 EHP Activity No. 016-CC Prepared for: ENVIRONMENTAL HEALTH DIVISION OFFICE OF HEALTH AND NUTRITION Center for Population, Health and Nutrition Bureau for Global Programs, Field Support and Research U.S. Agency for International Development & Water and Environmental Sanitation (Programme Division) Evaluation and Research Office Office of Social and Economic Policy UNICEF
Transcript of A REVIEW OF SANITATION PROGRAM …pdf.usaid.gov/pdf_docs/PNACB331.pdfEHP Activity Report No. 5 A...

EHP Activity Report No. 5
A REVIEW OF A REVIEW OF SANITATION PROGRAM EVALUATIONSSANITATION PROGRAM EVALUATIONS
IN DEVELOPING COUNTRIESIN DEVELOPING COUNTRIES
Anne K. LaFond
February 1995EHP Activity No. 016-CC
Prepared for:
ENVIRONMENTAL HEALTH DIVISIONOFFICE OF HEALTH AND NUTRITION
Center for Population, Health and NutritionBureau for Global Programs, Field Support and Research
U.S. Agency for International Development
&
Water and Environmental Sanitation(Programme Division)
Evaluation and Research OfficeOffice of Social and Economic Policy
UNICEF
UNICEF logo & motherEHP logoUNICEF logo & motherEHP logo
ENVIRONMENTAL HEALTH PROJECTENVIRONMENTAL HEALTH PROJECT
Activity Report # 5
A REVIEW OFSANITATION PROGRAM EVALUATIONS
IN DEVELOPING COUNTRIESby Anne K. LaFond
February 1995
Prepared jointly by UNICEF and EHP
Prepared for:
ENVIRONMENTAL HEALTH DIVISIONOFFICE OF HEALTH AND NUTRITIONCenter for Population, Health and Nutrition
Bureau for Global Programs, Field Support and ResearchU.S. Agency for International Development
&
WATER AND ENVIRONMENTAL SANITATIONProgramme Division
EVALUATION AND RESEARCH OFFICE

UNICEF

AN EVALUATION OF SANITATION PROGRAMSAN EVALUATION OF SANITATION PROGRAMSIN DEVELOPING COUNTRIES IN DEVELOPING COUNTRIES
A review of evaluation reportsA review of evaluation reportswith provisional draft program guidelines with provisional draft program guidelines

The principal challenges of the next decade will not be technological questions—thehardware of water supplies and sanitation—but the "software" issues: How are water andsanitation programs to be organized and financed? How can people be trained, organized,and motivated to install, use, and maintain the facilities? How can institutions develop thesector further and make improvements more sustainable? These are the questions for the1990s. [ REF 3]

i
CONTENTSCONTENTS
ACKNOWLEDGMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
EXECUTIVE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
1 INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.1 Purpose of this Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31.2 Framework for this Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31.3 Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.4 Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
2 SPECIFIC FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3 TOPIC RELATED FINDINGS: LESSONS OF EXPERIENCE . . . . . . . . . . . . . . . . . . . 11
3.1 Service Delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113.1.1 Technology Choice and Development . . . . . . . . . . . . . . . . . . . . . . 113.1.2 Organization and Management of the Intervention . . . . . . . . . . . . 12
3.2 Role of Sanitation Consumers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153.3 Influencing Behavior: Marketing, Promoting or Changing Hygiene Practices?16
3.3.1 Techniques for Stimulating Behavioral Change . . . . . . . . . . . . . . . 173.3.2 Techniques for Assessing Hygiene Behavior and Beliefs . . . . . . . . 18
3.4 Capacity Building . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183.4.1 Constraints to Capacity Building . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
3.5 Economic and Financing Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 3.5.1 To Subsidize or Not to Subsidize? . . . . . . . . . . . . . . . . . . . . . . . . . 21
3.6 Intra- and Inter-Sectoral Links . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223.6.1 Water and Sanitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223.6.2 Sanitation and Other Sectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
4 ISSUES FOR DISCUSSION AND DRAFT GUIDELINESFOR SANITATION PROGRAMMING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
4.1 Issues for Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 234.1.1 Summary of Lessons Learned . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
ii
4.1.2 Information Gaps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 244.1.3 Dispelling Myths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
4.2 A Basic Framework for Sanitation Programs . . . . . . . . . . . . . . . . . . . . . . . 254.3 Draft Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
4.3.1 Overall Aims and Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264.3.2 Program Aims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264.3.3 Guiding Principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264.3.4 Essential Program Activities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 274.3.5 Recommendations for Operational
Guideline Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
REFERENCES FOR EVALUATION DOCUMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
BIBLIOGRAPHY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
APPENDICES
A. Terms of Reference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45B. Summary Sheet for Review of Sanitation Evaluations . . . . . . . . . . . . . . . . 49C. Summary of Topics Included in Evaluation Documents . . . . . . . . . . . . . . . 53D. List of Inventory Respondents and Interview Guide . . . . . . . . . . . . . . . . . . 59
iii
BOXES, FIGURES, AND TABLESBOXES, FIGURES, AND TABLES
Box 1 Why Invest in Sanitation? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Box 2 Features of Sanitation Programming that Create Operational Problems . . . 8
Box 3 Components of Success: Stimulating and Sustaining Demand in Pakistan 16
Box 4 Components of Success: Linking Hardware and Software in Lesotho . . . . 16
Box 5 Hygiene Behavior and Latrine Use in Kenya . . . . . . . . . . . . . . . . . . . . . . . 20
Box 6 Current Changes in the Organization and Management of the Water and Sanitation Sectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Box 7 A Successful Sanitation Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Fig 1 Population in Developing Countries with Water and Sanitation Serviceby Year and Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Table 1 World Summit for Children: Goals Related to Sanitation . . . . . . . . . . . . . . . 2
Table 2 Summary of Evaluations by Topic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5

iv
v
ACKNOWLEDGMENTSACKNOWLEDGMENTS
I would like to thank Vanessa Tobin, Krishna Bose, Steven Esrey, and Gina Darcin-St Louisof UNICEF, and Eduardo Perez of the Environmental Health Project for their support andguidance in producing this document.
All errors remain the responsibility of the author.

vi

vii
Executive SummaryExecutive SummaryThe benefits of investing in sanitation indeveloping countries are improved healthand nutrition, particularly for children,reduced disease transmission in thecommunity, and greater privacy,convenience, and safety through access toappropriate facilities. Yet, sanitationprogramming falls far short of need, and bythe year 2000 may be proportionately lowerthan at the start of the International DrinkingWater Supply and Sanitation Decade.Sanitation is an important feature of thegoals set at the World Summit for Childrenin 1990 that are unlikely to be met withoutincreased sanitation investment and moreeffective programming.
UNICEF's global evaluation of sanitationprograms aims to analyze the experience ofdesigning and implementing sanitationinterventions in developing countries toascertain lessons for improving theeffectiveness of future investments. Thispaper is the first phase of this evaluation. Itconsists of a review and analysis ofsanitation program evaluations andsanitation program strategies of variousimplementing agencies, a summary oflessons learned, and provisional programguidelines for discussion among plannersand managers. The six topics under whichdata were collected and the findings arepresented are service delivery, the role ofsanitation consumers, influencing behavior,capacity building, economics and financing,and intra- and inter-sectoral links.
Investment in sanitation has beeninadequate for several reasons. Thedemand for sanitation is often low, andstimulating it takes time and money. Manydevelopment institutions are not attuned todemand-led programming, which mayexplain their unenthusiastic approach toinvesting in sanitation. Furthermore, keydecision-makers are not clear about anoverall strategy for sanitation programming,have not reached a consensus on adefinition of sanitation, and differ on theoptimal role for governments, NGOs,communities, the private sector, andexternal donors in program implementation.
Findings
Service Delivery. Choosing a technologyfor sanitation programs has become lessdifficult with the widespread acceptance of
the ventilated improved pit (VIP) latrine andthe pour flush toilet. However, an effectivetechnology must reflect consumerpreferences and local conditions. Cost,ease of operation and maintenance, andthe time taken to win acceptance are threeimportant considerations. High costs candeter acceptance. Planners should strike abalance between product sophistication,operation and maintenance requirements,and cost. Sometimes the choice of a low-cost technology may appear rational, butthe demand for a more attractive productrequiring less maintenance may be greater.Also, introducing a new technology takestime and effort on promotion. Projectmanagers must always be ready to learn.
The choice of implementing institution, thedivision of responsibilities in servicedelivery, and the coordination of theimplementation process are important forprogram success. Programs implementedby NGOs or the private sector - separatelyor in collaboration with government - aremore likely to succeed than programsimplemented by government alone.Sanitation programming often suffers in thehands of weak public institutions. However,projects that fail to 'build capacity' bybypassing these institutions only exacerbatethe shortcomings of the public sector. Theresponsibilities for building sanitationfacilities and for promoting a demand forsanitation often are assigned to differentactors. Because demand for sanitationgenerally is weak, success depends moreon promoting sanitation than on theefficiency of engineers and builders. Thecoordination of these two functions by asingle body facilitates programimplementation.
Role of Consumers. Involvingconsumers in project execution yieldsgreater community responsibility foroperation and maintenance and betterprospects for sustainability.
However, community participation shouldnot be limited to construction, as it often is.Four factors were found to enhance thecontribution of community participation toprogram success: the use of existingcommunity organizations rather thancreating new ones; improving theorganizational capacity of communitygroups and their problem solving skills;

viii
involving women; and includingcommunities in the design, management,and financing of projects.
Influencing Behavior. The failure ofsanitation projects is often attributed toexcessive emphasis on technology at theexpense of changing consumer attitudes tolatrine utilization and maintenance andgeneral hygiene. While there are signs thatprojects are increasingly emphasizingbehavioral change, they do not yetdifferentiate between the change needed toincrease demand and the change needed inhygiene practices. Different methods arenecessary depending on the purpose ofstimulating behavioral change. Mostevaluations noted a behavioral componentaimed at selling the idea of latrines; fewnoted the need to change hygiene-relatedbeliefs or practices. Moreover, becausebaseline surveys of hygiene behavior hadrarely been conducted, it was impossible todetermine what impact projects had made.Success in influencing behavioral changedepended on four factors: a clear sense ofpurpose, the use of participatorytechniques, the inclusion of women aspromoters/educators, and the simultaneousemployment of a range of techniques.Techniques for assessing hygiene beliefsand behavior must be more readilyavailable to program planners.
Capacity Building. Sanitation projectsshould enable local institutions and peopleto address sanitation problems on asustainable basis, a significant omissionfrom most evaluations. Undoubtedly, thedivision of responsibilities for sanitationprogramming is not conducive to capacitybuilding. Donors often establish separateunits to facilitate project implementation.However, in bypassing local institutions,they directly undermine national capacitybuilding, and by neglecting to improve localorganizations and management skillsthrough project implementation, actuallyimperil sustainability. Investing incommunity level institutions is morecommon than capacity building at thenational and district levels.
To facilitate capacity building, projectsshould be designed to fit in with sectoralneeds and conditions and should not beexcessively dependent on external supportand technical assistance. Another importantfactor is that trends towardsdecentralization and increased donor
pressure for accountability are changing thedemands on local institutions.
Economics and Financing. Economicsand financing did not figure prominently inthe evaluations. One mentioned the effectof cost on the access to latrines by differentincome groups. Without accessible methodsfor estimating demand as demonstrated byability and willingness of pay, planners havedifficulty gathering data to arrive atappropriate cost levels. The use ofsubsidies for financing sanitation programsreceived mixed reviews. Subsidization canmake expensive technology affordable andspeed up implementation, but it can alsocreate a dependence on externalresources. Finally, inadequate public sectorfinancing often impedes the realization ofcoverage and sustainability goals.
Intra- and Inter-sectoral links.Sanitation programs linked to water supplyprograms benefit from an increaseddemand and a greater health impact, butjoint coordination can be challengingbecause the construction and promotion ofwater programs generally outpace those ofsanitation programs. Some projectspromoted links between sanitation and thehealth and education sectors. Primaryhealth workers were employed to promotesanitation and hygiene education. In the linkwith the education sector, latrines were builtin schools and hygiene education wasintroduced in the curriculum.
The evaluations were deficient ininformation about the link betweenindividual sanitation projects and overallsector development, the place of sanitationin the national context, methods formeasuring demand for sanitation, indicatorsof facility utilization, financing, theidentification of beneficiary groups, baselinesurveys of hygiene beliefs and practices,and inter-sectoral linkages.
Planners are beginning to change theirperceptions of what constitutes a goodsanitation program, although as yet there isno single paradigm of the best ideas.Experience indicates that certaincombinations of factors must be present fora program to be considered successful.Based on the data gathered, a successfulprogram should: improve the health ofbeneficiary groups; be financially,organizationally, and politically sustainable;maximize the benefits of investment byreaching the greatest number of people;

ix
enhance local institutional and communitycapacity for organization and management;and protect the environment.

x

1
Box 1 Why Invest in Sanitation?
Health-related benefits
C Improves health status C Meets the responsibility of government to
promote preventive health care as a public goodC Reduces environmental degradation in
rapidly growing urban areas
Non health-related benefits
C Contributes to the economic and social well-being of thecommunityC Generates political mileage, especially in
urban areasC Effects immediate financial savings in
expanding peri-urban settlements; the later the investment, the costlier theintervention.
1 1 INTRODUCTIONINTRODUCTION
The experience gained by governments, aidagencies, and communities during theInternational Drinking Water Supply andSanitation Decade (1981-90) testifies to thebenefits of investing in sanitation indeveloping countries. Several studies haveshown that improved sanitation leads toimproved health and nutrition, particularlyamong children (Esrey and Habicht 1986;Habicht, DaVanzo, and Butz 1988; andEsrey, Feacham and Hughes 1985).Studies comparing the differential impactsof water and sanitation programs havefound that sanitation is a more importantdeterminant of child health than watersupply (Esrey 1994; Bateman and Smith1993; and Bateman and Smith 1991).Sanitation gives beneficiaries, particularlywomen, greater
convenience, privacy, and possibly safety(Elmandorf 1980; Water Aid 1993). It alsoprovides more than these individual benefitsby reducing the transmission of diseasethrough human contact and environmentalpollution in the community. Box 1 lists theadditional benefits from investing insanitation.
Despite this evidence, sanitationprogramming falls far short of need.Sanitation coverage currently lags behindwater supply, leaving 58 percent of ruralpopulations and 26 percent of urbanpopulations without access to facilities(UNICEF 1994). Moreover, it is estimatedthat coverage by the year 2000 may beproportionately lower than at the start of the
International Drinking Water Supply andSanitation Decade (van Wijk undated)
2
0
500
1000
1500
2000
2500
3000
1980 1990 2000 1980 1990 2000
POPULATION in DCs W ITH WATER W ITH SANITATION
u r b a n a r e a s r u r a l a r e a s
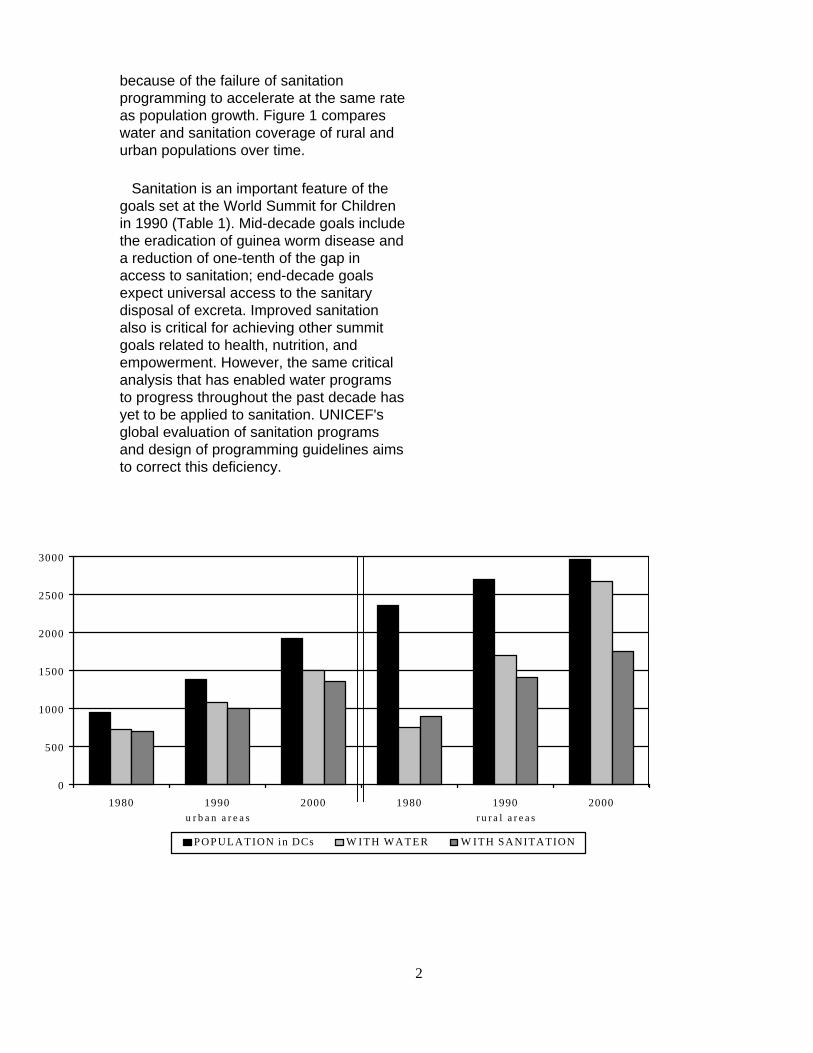
because of the failure of sanitationprogramming to accelerate at the same rateas population growth. Figure 1 compareswater and sanitation coverage of rural andurban populations over time.
Sanitation is an important feature of thegoals set at the World Summit for Childrenin 1990 (Table 1). Mid-decade goals includethe eradication of guinea worm disease anda reduction of one-tenth of the gap inaccess to sanitation; end-decade goalsexpect universal access to the sanitarydisposal of excreta. Improved sanitationalso is critical for achieving other summitgoals related to health, nutrition, andempowerment. However, the same criticalanalysis that has enabled water programsto progress throughout the past decade hasyet to be applied to sanitation. UNICEF'sglobal evaluation of sanitation programsand design of programming guidelines aimsto correct this deficiency.
3
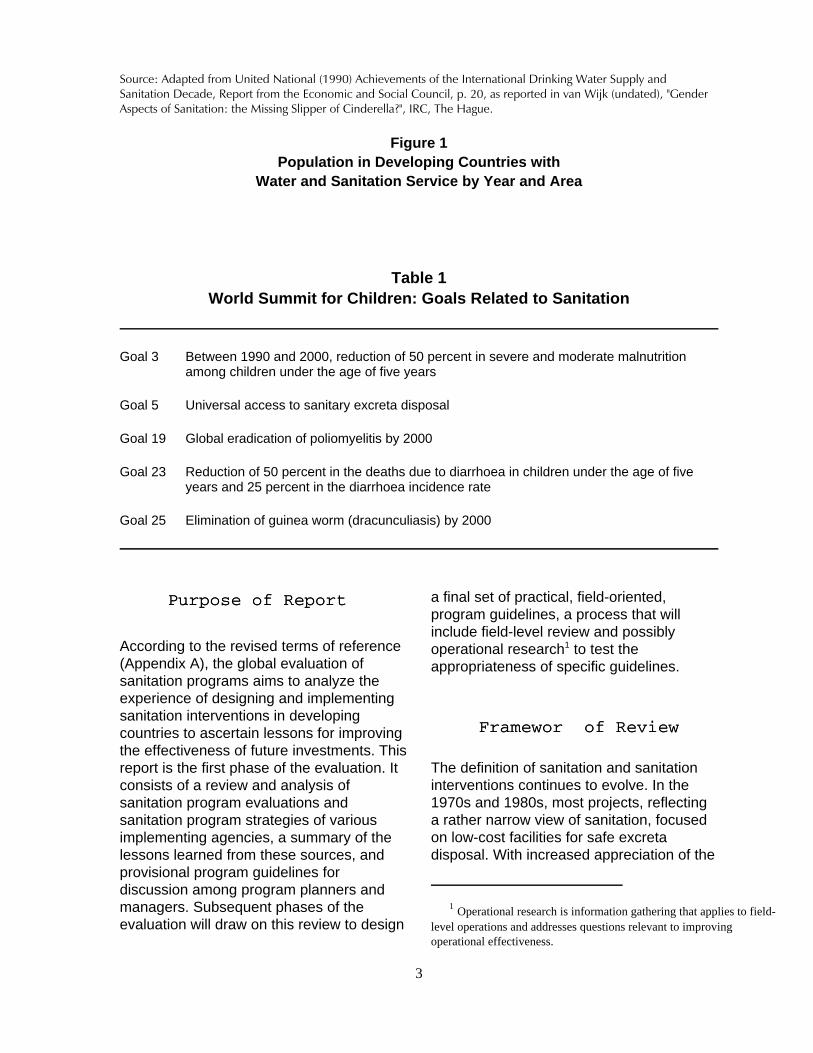
Source: Adapted from United National (1990) Achievements of the International Drinking Water Supply andSanitation Decade, Report from the Economic and Social Council, p. 20, as reported in van Wijk (undated), "GenderAspects of Sanitation: the Missing Slipper of Cinderella?", IRC, The Hague.
Figure 1Population in Developing Countries with
Water and Sanitation Service by Year and Area
Table 1World Summit for Children: Goals Related to Sanitation
Goal 3 Between 1990 and 2000, reduction of 50 percent in severe and moderate malnutritionamong children under the age of five years
Goal 5 Universal access to sanitary excreta disposal
Goal 19 Global eradication of poliomyelitis by 2000
Goal 23 Reduction of 50 percent in the deaths due to diarrhoea in children under the age of fiveyears and 25 percent in the diarrhoea incidence rate
Goal 25 Elimination of guinea worm (dracunculiasis) by 2000
1.11.1 Purpose of Report Purpose of Report
According to the revised terms of reference(Appendix A), the global evaluation ofsanitation programs aims to analyze theexperience of designing and implementingsanitation interventions in developingcountries to ascertain lessons for improvingthe effectiveness of future investments. Thisreport is the first phase of the evaluation. Itconsists of a review and analysis ofsanitation program evaluations andsanitation program strategies of variousimplementing agencies, a summary of thelessons learned from these sources, andprovisional program guidelines fordiscussion among program planners andmanagers. Subsequent phases of theevaluation will draw on this review to design
a final set of practical, field-oriented,program guidelines, a process that willinclude field-level review and possiblyoperational research1 to test theappropriateness of specific guidelines.
1.21.2 Framework of ReviewFramework of Review
The definition of sanitation and sanitationinterventions continues to evolve. In the1970s and 1980s, most projects, reflectinga rather narrow view of sanitation, focusedon low-cost facilities for safe excretadisposal. With increased appreciation of the
1 Operational research is information gathering that applies to field-level operations and addresses questions relevant to improvingoperational effectiveness.

4
importance of hygiene behavior in programsuccess, some planners currently areadvocating a broader definition of sanitationthat includes the promotion of facility useand a change in hygiene behavior.
But as yet there is no clear consensus onhow sanitation should be defined.2 UNICEFemploys the term environmental sanitation,implying a perspective that goes beyond theintroduction of technology. Nevertheless,based on the evaluations reviewed here,sanitation continues to be defined as theinstallation of hardware. While educationand behavioral change are increasinglyincorporated into projects, hardware is thedominant concern. The absence of a well-balanced view of sanitation may be one ofthe key constraints to programeffectiveness.
For the purpose of this report, sanitationrefers to the safe handling, treatment, anddisposal of excreta and wastewater, as wellas behavior that ensures these practices(adapted from WASH 1993, p 78). Thisdefinition guided the collection of data forthis review, and is reflected in the six topicsset out in the initial terms of reference andunder which the findings are presented:
C Service delivery - the ability of asanitation system to meet the needs ofbeneficiaries, as measured by the choice oftechnology and the organization andmanagement of service delivery;
C Role of sanitation consumers - in needsassessment, design, implementation, andfinancing of program activities;
C Influencing behavior - as manifested indemand for sanitation facilities, participationin latrine construction, proper usage and
maintenance of latrines, and changes inhygiene practices;
C Capacity building - evidence thatinvestment by government, communities,and external agencies has given localinstitutions and people the capacity toaddress sanitation problems on asustainable basis;
C Economics and financing - including thecost of sanitation and the financingmechanisms to meet it;
C Intra- and inter-sectoral links -coordination between sanitation and wateractivities, and between sanitation and othersectors (e.g., health, nutrition, education,agriculture).
1.31.3 MethodologyMethodology
A total of 38 evaluation documents orreviews, covering 54 sanitation projectsimplemented between 1980 and 1994,provided information on each of the sixtopics; 24 of these projects were supportedto some degree by UNICEF. Mostdocuments evaluated a single project, buttwo reviewed more than one project orprogram [REF 2, 24] and one was based on10 case studies of country experience [REF13]. A search of the UNICEF evaluationdatabase, the UNICEF WES library, and theWASH library produced a limited numberand variety of documents, reflecting ageneral scarcity of writing on sanitationprogramming experience. Thus, theevaluation reports reviewed here wereeventually selected on the basis of theiravailability. To increase the range ofinformation gathered, evaluations of entireprojects were given priority over evaluationsof specific aspects of projects (e.g., healthimpact). Documents focusing on the impactof hygiene education were excluded
2 Very few evaluations and project histories provided a precisedefinition of sanitation.

5
because a concurrent review of this subjectis being conducted by WHO.
At the outset, a standardized set ofquestions based on topics specified in theterms of reference was applied to eachevaluation. However, this was found to beunsuitable because very few of thedocuments covered all the topics orpresented findings in sufficient detail toanswer all the questions. For example,project-stimulated changes in hygienebehavior could not be determined withoutadequate baseline indicators. The datagathering guide was therefore revised toinclude general topics rather than specificquestions (Appendix B). The frequency ofoccurrence of each topic was recorded on asummary sheet, along with the findings ofthe evaluation. (Appendix C summarizesthe frequency of different topics in allevaluation documents.) Data were thensorted by topic and the dominant trends andpatterns of experience were noted.
1.41.4 LimitationsLimitations
In general, both the quantity and quality ofdata fell short of expectations. Instead of asample that represented a range ofgeographical and programming variables, itwas necessary to accept whatever wasoffered by the few appropriate documentsobtained within the given time frame. Whilethis was due partly to the general absenceof sanitation evaluations, it was also theresult of the limited time frame of thisreview. In addition, the unequal quality ofthe caliber of data gathering, analysis, andpresentation in the evaluation documentsaffected the reliability of the findingsreported here. There were twoconsequences of these shortcomings. First,the sample of evaluation documentsreviewed was smaller than planned. Theoriginal terms of reference specified 25UNICEF and 25 external evaluations, butmany of the more than 50 project
evaluations reviewed failed to provideuseful information. Thus, of the 36 UNICEFevaluations selected, only 25 could beused. Second, variations in the quality ofthe remaining evaluations made it difficult tosubstantiate findings or compareexperiences or lessons in sufficient detail.The results reported here are thereforemainly based on a smaller number of thebetter quality evaluations [see references 2,3, 4, 7, 13,16, 17, 20, 22, 23, 24, 25, 27, 30,32, 33, 36, and 38, which represent 37different projects]. In general, theevaluations in the UNICEF database wereless adequate than the external evaluationsin the following ways:
C about one-third lacked sufficient data onsanitation interventions (compared withwater);
C reports tended to emphasize hardware(e.g., latrine construction) over softwarecomponents;3
C most lacked rigorous indicators ofprogress apart from 'numbers of latrinesconstructed' and 'numbers of workerstrained' (i.e., few process indicators);
C comparison with pre-project status wasoften missing (i.e., no indication of baselinedata);
C results were reported withoutsubstantiation or lacked clarity.
3 Hardware refers to program activities such as the design andconstruction of sanitation facilities. Software describes less tangiblecomponents such as health and hygiene education, behavioral assessment,and interventions aimed at changing hygiene-related beliefs and practices.
6
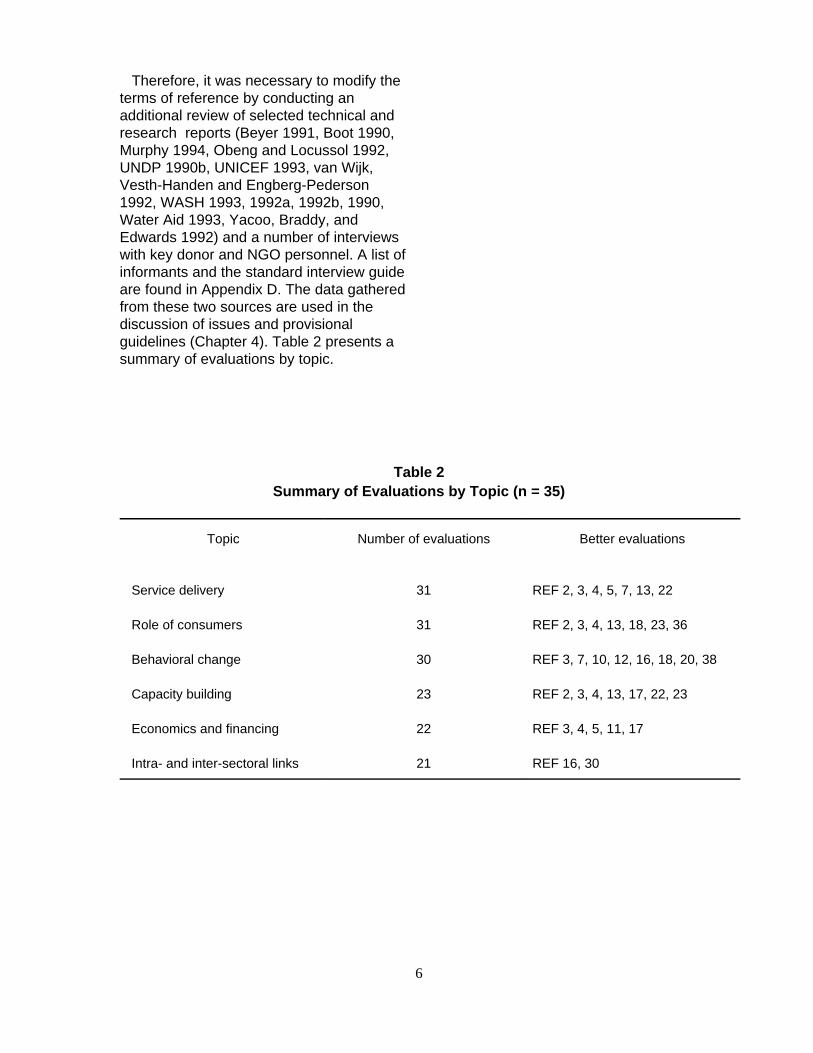
Therefore, it was necessary to modify theterms of reference by conducting anadditional review of selected technical andresearch reports (Beyer 1991, Boot 1990,Murphy 1994, Obeng and Locussol 1992,UNDP 1990b, UNICEF 1993, van Wijk,Vesth-Handen and Engberg-Pederson1992, WASH 1993, 1992a, 1992b, 1990,Water Aid 1993, Yacoo, Braddy, andEdwards 1992) and a number of interviewswith key donor and NGO personnel. A list ofinformants and the standard interview guideare found in Appendix D. The data gatheredfrom these two sources are used in thediscussion of issues and provisionalguidelines (Chapter 4). Table 2 presents asummary of evaluations by topic.
Table 2Summary of Evaluations by Topic (n = 35)
Topic Number of evaluations Better evaluations
Service delivery 31 REF 2, 3, 4, 5, 7, 13, 22
Role of consumers 31 REF 2, 3, 4, 13, 18, 23, 36
Behavioral change 30 REF 3, 7, 10, 12, 16, 18, 20, 38
Capacity building 23 REF 2, 3, 4, 13, 17, 22, 23
Economics and financing 22 REF 3, 4, 5, 11, 17
Intra- and inter-sectoral links 21 REF 16, 30

7

8
22 SPECIFIC FINDINGSSPECIFIC FINDINGS
Sanitation has not been accorded the sameimportance as water supply by national orinternational development institutions. Thisis apparent from coverage statistics,4
expenditure estimates, and the paucity ofproject evaluations conducted in the pastdecade. From the investor's standpoint,there are valid reasons for this neglect. Anumber of aspects of sanitation programsmake implementation particularlyproblematic and consequently more difficultto support than water programs and otherhealth-related interventions (see Box 2).
First, one of the most critical aspects ofsanitation programming is the centrality ofconsumer demand to program success.A World Bank review of 10 case studiesnotes that "the most fundamental lesson tobe drawn from low-cost sanitation programsof the last decade is that success or failureand rates of progress are determinedprincipally by consumer demand" [REF 13].Planners must therefore tailor sanitationinterventions to the needs and capacity ofbeneficiaries if they expect to make alasting impact on sanitation-related healthproblems.
Unfortunately, demand for sanitationamong target populations is often low.Communities are likely to prefer water oversanitation and may be reluctant to pay for afacility whose direct benefits are unclear. Tobe successful, however, sanitation
programs require individuals or householdsto make a significant commitment byagreeing to modify their homes or adoptnew technologies. Because sanitationprograms are rarely fully subsidized bygovernment, consumers are frequentlyexpected to pay for the installationsthemselves. Success also depends onconsumers' involvement in programmanagement, financing, and promotion.Moreover, for the intervention to make animpact on health, household members mustuse and maintain the facility properly andpossibly change some basic beliefs andpractices in their daily lives. Withoutconsumer demand for better sanitation,many of these fundamental steps ofprogram implementation are prone tofailure.
A second problem with sanitationprogramming is that the interest ofimplementing agencies in investing insanitation may also be low. Governmentsand donor agencies are deterred by a lackof good models for successful programs, ahigh cost per beneficiary, little institutionalenthusiasm for sanitation, the logisticaldemands of sanitation programs, and ageneral lack of awareness of health benefitsfrom improved sanitation (Murphy 1994).Thus, before sanitation interventions areconsidered, the need for services (and oftenan understanding that poor sanitationcontributes to poor health) must begenerated not only among beneficiaries, butalso among some implementing institutions.
4 From 1981-1990, it is estimated that 1.348 billion people wereprovided with water while only 748 million received sanitation, leaving1.7 billion unserved. (WASH 1992b: 1)
9
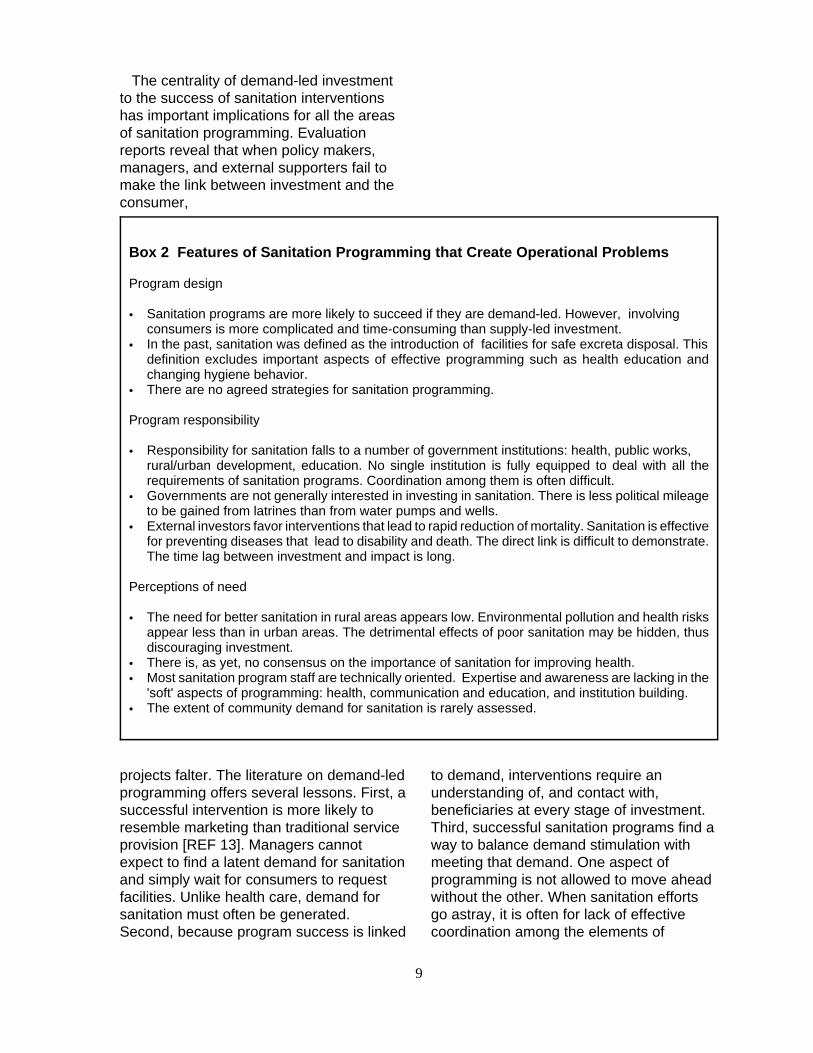
Box 2 Features of Sanitation Programming that Create Operational Problems
Program design
C Sanitation programs are more likely to succeed if they are demand-led. However, involvingconsumers is more complicated and time-consuming than supply-led investment.
C In the past, sanitation was defined as the introduction of facilities for safe excreta disposal. Thisdefinition excludes important aspects of effective programming such as health education andchanging hygiene behavior.
C There are no agreed strategies for sanitation programming. Program responsibility
C Responsibility for sanitation falls to a number of government institutions: health, public works,rural/urban development, education. No single institution is fully equipped to deal with all therequirements of sanitation programs. Coordination among them is often difficult.
C Governments are not generally interested in investing in sanitation. There is less political mileageto be gained from latrines than from water pumps and wells.
C External investors favor interventions that lead to rapid reduction of mortality. Sanitation is effectivefor preventing diseases that lead to disability and death. The direct link is difficult to demonstrate.The time lag between investment and impact is long.
Perceptions of need
C The need for better sanitation in rural areas appears low. Environmental pollution and health risksappear less than in urban areas. The detrimental effects of poor sanitation may be hidden, thusdiscouraging investment.
C There is, as yet, no consensus on the importance of sanitation for improving health. C Most sanitation program staff are technically oriented. Expertise and awareness are lacking in the
'soft' aspects of programming: health, communication and education, and institution building.C The extent of community demand for sanitation is rarely assessed.
The centrality of demand-led investmentto the success of sanitation interventionshas important implications for all the areasof sanitation programming. Evaluationreports reveal that when policy makers,managers, and external supporters fail tomake the link between investment and theconsumer,
projects falter. The literature on demand-ledprogramming offers several lessons. First, asuccessful intervention is more likely toresemble marketing than traditional serviceprovision [REF 13]. Managers cannotexpect to find a latent demand for sanitationand simply wait for consumers to requestfacilities. Unlike health care, demand forsanitation must often be generated.Second, because program success is linked
to demand, interventions require anunderstanding of, and contact with,beneficiaries at every stage of investment.Third, successful sanitation programs find away to balance demand stimulation withmeeting that demand. One aspect ofprogramming is not allowed to move aheadwithout the other. When sanitation effortsgo astray, it is often for lack of effectivecoordination among the elements of

10
implementation (e.g., building latrines fasterthan demand merits).
All the topics discussed in the nextchapter reflect the importance of consumerdemand in sanitation programming. Thelessons learned in these different areas alsopoint to a third finding of the review.Because sanitation programs benefit fromdemand-led design and implementation, theway in which programs are supported byimplementing agencies is critical.Nevertheless, the approach to investmentfollowed by many development institutionsis often not suited to demand-ledprogramming. While only a small number ofreports raised questions about the role ofdifferent actors in the programmingprocess, they often illustrated a mismatch ofthe skills, investment cycles, and pressuresof development institutions and consumer-focused programming. Donor adherence toa rigid project cycle and the desire for short-term outputs, for example, may hinder theeffectiveness of investment. Weak or poorlycoordinated government inputs werefrequently cited as a factor ofimplementation failure. Thus, successfulsanitation programming must be supportedby appropriate institutional mechanismsamong the main investors.
Finally, there is a lack of clarity amongkey decision makers concerning anoverall strategy for sanitationprogramming. This includes the failure toreach a consensus on a definition ofsanitation and on the optimal role forgovernments, NGOs, communities, theprivate sector, and external donors inprogram implementation.

11
12
33 TOPIC-RELATED FINDINGS: LESSONS OF EXPERIENCE
The division of sanitation programming intosix categories is an artificial analyticaldevice. In practice, these programcomponents combine in different ways toenhance or inhibit program success. Formanagers, the key is finding the right mix ofcomponents and balancing them withcritical program elements such asgenerating or meeting consumer demandand enhancing local capacity for addressingsanitation problems.
3.13.1 Service DeliveryService Delivery
The ability of a sanitation program to supplyan appropriate service to beneficiaries isinfluenced by two factors: the choice oftechnology, and the organization andmanagement of the program.
3.1.1 Technology3.1.1 TechnologyChoiceChoice
and Development and Development
Field work and research in the 1970s and1980s emphasized the development ofappropriate technology for water andsanitation (Kalbermatten et al. 1981). Twosanitation systems emerging from thisexperience met the criteria of widespreadapplicability and popularity: the ventilatedimproved pit (VIP) latrine and the pour flushtoilet. Of the evaluations reviewed, 75percent examined the technology used, andmost reported success with some variationof these two technologies. The Orangiproject in Pakistan, however, stands out asan exception. This project was no lesssuccessful, but involved the installation of
traditional water-borne sewerage systemsrather than latrines [REF 2, 36].
While the choice of basic technology nolonger poses problems for most sanitationprogram managers, all the cases evaluatedshowed that adapting technology toparticular circumstances is a critical elementof project success. Sanitation technologyrequires greater adaptation to localpreferences than water technology does.Again, the consumer plays a central role.Three factors of technology developmentemerged as important: C finding the right balance between costand consumer demand;C finding the right balance between capitalinvestment, operation and maintenance,and consumer demand;C allowing sufficient time for technologydevelopment and adoption.
Cost
Because consumers are often expected tocontribute in cash or in kind to theconstruction of sanitation facilities, the costof technologies is an important factor ofprogram success. The community's readyacceptance of responsibility for buildinglatrines in an integrated water andsanitation project in Baluchistan is attributedto the cheap and simple technologyemployed by the project [REF 2]. Costserved as a deterrent to communityinvolvement in Nepal, even with relativelyhigh subsidies from the project [REF 8]. Inaddition to materials and labor, consumersmay also consider the cost of the time spenton the upkeep of facilities. In the Busti

13
project in Baldia township, Karachi, programmanagers changed the design of sanitationtechnologies five times in six years in orderto lower the cost to consumers. But thesedesign changes resulted in decreasedutilization. Reducing the depth of the pit todecrease construction costs increased theneed for desludging. Moreover, the projectwent to great lengths to persuadebeneficiaries of the advantages of lower-cost 'pits plus soakaway' latrines, when thecommunity originally expressed a desire fora water-borne sewerage system. In the laterstages of the project, the water table beganto rise, requiring some soakpits to beconverted to septic tanks. Evaluatorssuggested that responding to thecommunity's preference for sewers at theoutset of the project might have been moreappropriate than persuading them of thebenefits of a lower-cost technology [REF 2].
Design and Maintenance
In addition to the consumer's willingness topay for facilities, it is necessary that thechoice of technology must also be suited tobeneficiary preference for convenience andproduct sophistication. Tradeoffs must oftenbe made between design sophistication andoperation and maintenance requirements.Consumer demand and utilization may behigher for a refined facility that requires lessmaintenance than for a simple, low-costlatrine. While the initial cost to theconsumer and the program (if subsidies areincluded) of a refined system may be high,the benefits resulting from proper utilizationand upkeep may exceed these costs. Someevaluations noted the availability and cost oflocal materials (and their transportation tothe building site) as significant programdesign factors. Local building andmaintenance capabilities were alsoimportant considerations in choosing amongdifferent technologies. These factors shouldalso be assessed with the consumer'sability to pay, although in some cases thethree cannot be coordinated successfully. In
Sudan, the demand for project latrines washigh, but dependence on imported materialsprevented the project from meeting thisdemand in a timely fashion. Replacement ofmaterials also posed a problem [REF 16].
Technology Development
One review of lessons of the past decaderecommends four steps before developingand adapting technology: find out what localsolutions already are available; inquireabout consumer design preferences;investigate consumer willingness and abilityto pay (the two are not necessarilycompatible); and estimate how muchpromotion might be needed to sell thetechnology to consumers [REF 13].Moreover, there is evidence that the timelag between the introduction and theadoption of new practices or technologiesmay be extremely long in somecommunities. Program managers should beaware that piloting technologies andpromotion may take up to 18 months. InMozambique, for example, sales of newlatrine floor slabs for low-incomehouseholds were slow because peoplewere waiting until their old latrine pits werefull. Programmers had to wait over twoyears to determine the demand for newfacilities. Although surveys reported thatdemand was high, sales increased onlywhen people were ready to buy andtransportation was made available to carrymaterials safely to their homes (Brandberg1985).
Sensitivity and adaptability to localpreferences ensure that investment insanitation is not wasted. Although few of theproject evaluations explained howtechnology choice was made, clearly theprocess requires project management to becreative and flexible. Managers shouldappreciate that technology developmentand refinement take time, although manyprograms ignore this learning approach toimplementation.

14
3.1.2 Program Organizationand Management
Many of the evaluations found that theorganization and management of a projectgreatly influenced its success. Amongseveral constraints to meeting operationalobjectives, the most frequent concerned thechoice of implementing institution, thedivision of responsibilities in servicedelivery, and coordination of theimplementation process. These three arediscussed below.
Choice of Implementing Institution
At the outset of a project, decisions aremade about the target population, projectdesign, and financing. However, one of themost critical factors for success is thechoice of implementing institution, whichcan be a government agency, anongovernmental body, the private sector,or a combination of the three. While theevaluations provided examples of bothsuccessful and less notable programexperiences for each of the three, theprograms implemented by governmentagencies alone generally accomplished theleast.
The apparent mismatch between sanitationprograms and government implementinginstitutions is mostly attributed to thenumber of agencies that are involved (e.g.,health, construction, education, socialmobilization). However, it also stems fromthe inability of public institutions to carry outmany of the functions required forsuccessful sanitation programming. Forexample, government is not usually skilledin the marketing techniques for promotinglocal participation in the construction andmaintenance of facilities. Manygovernments are centralized and localadministrative structures are weak, makingit difficult to encourage communityparticipation [REF 11, 30]. Moreover,conventional bureaucratic institutions rarely
display the sensitivity required forparticipatory programming.
Sanitation programs require a cadre ofwell-trained people in the field with a clearunderstanding of program needs, an abilityto deliver results, and a talent for convincingconsumers of the benefits of sanitation[REF 13]. Deficiencies in human resourcecapacity in the public sector were oftencited as a constraint to projectimplementation. In Botswana andIndonesia, program staff lacked the skillsand interest in promotion and healtheducation [REF 3,17]. In Nepal, poorsupervision of facility construction andinadequate followup of the constructionphase led to misuse of project materialsand low utilization and maintenance [REF8].
Rather than dealing with the weaknessesof public institutions, donors often bypassgovernment by establishing separateproject management units to ensure thetimely fulfillment of project plans. TheBaluchistan Integrated DevelopmentProgram (BIAD) employed thisimplementation strategy. BIAD was set upas an independent agency so it could adopta multi-disciplinary approach to watersupply and sanitation, and was staffed withseconded government personnel. Whilethese employees acquired skills they couldapply elsewhere once the project wascompleted, instituting a separatemanagement unit often caused friction withgovernment bureaucracies. This canthreaten the continuity of project benefits iffuture activities are subject to governmentcontrol [REF 2].
As an alternative to working directly withgovernment, donors can engageinternational and local NGOs to implementsanitation programs. The advantage ofNGOs is their experience in working withcommunities and the absence ofcumbersome bureaucratic procedures.

15
Nevertheless, problems can arise if theNGO focuses on community levelprogramming to the exclusion ofmaintaining effective links with government.CARE's WASHES project in Indonesia, forexample, attained remarkable coveragewith strong links to communities forged byCARE staff. However, once CARE'scontribution ended, the project faced asustainability problem because governmentwas unable to continue the same support inareas such as technical assistance andlogistics [REF 3].
The private sector as a third alternative forimplementation was involved in only a fewsanitation projects and mostly withconstruction [e.g., REF 2]. In Lesotho, thenational program boasts a successfulpartnership with the private sector. It hastrained local artisans in latrine constructionand some sanitation promotion andencouraged them to enter into contractswith consumers (see Box 4 at the end ofSection 3.2). A review of eight water andsanitation projects in Pakistan concludesthat the role of the private sector could beexpanded to encompass the marketing ofsanitation facilities. It also recommends thatgovernment and donors should invest incapacity building of private institutions tofacilitate their involvement in sanitationprogramming.
Division of Responsibilities
A second constraint on operationalobjectives can be the division ofresponsibilities among investment partners.In the simplest arrangement, projectimplementation can be split into buildingsanitation facilities and promoting sanitationactivities (including improved hygienebehavior). Different projects assign theseresponsibilities in different ways. As notedearlier, the varied tasks of sanitationprogramming do not fit easily under a singleline ministry. Health ministries are no moreaccustomed to supervising construction
than public works ministries are suited toproviding hygiene education. However,some successful examples were found inprojects that engaged other parties to fulfillconstruction contracts [e.g., REF 4].
Most schemes involved communities inbuilding part of a latrine, often providing theconstruction materials and labor for diggingand lining the pit and laying the slab, whilethe consumer built the superstructure [e.g.,REF 2]. Success depended on the fitbetween consumer demand and the design,cost, and perceived benefit from investing insanitation. A few programs also succeededwith other types of contractualarrangements. In the Orangi project inPakistan, for example, the community tookresponsibility for organizing the entireconstruction and maintenance of thesewerage system. In Botswana, districtcouncils engaged the labor for construction[REF 17]. And in Lesotho, consumers andlocal builders made their own financialarrangements for latrine building. All threeprograms have been highly successful ingenerating demand for latrine construction,perhaps because they have been able torespond to consumer demand in a timelyand innovative way [REF 4, 5].
The second task of implementation - thepromotion of sanitation facility construction,usage, and maintenance and improvedhygiene behavior - is normally assigned to adifferent group of people or a differentinstitution. This arrangement unfortunatelyoften results in the neglect of promotion, orpoor coordination between building andpromotion. Some projects elected to trainnew sanitation promoters [REF 2]. Othersrelied on health care workers to fulfill thepromotion role, with little success [REF 7].In Indonesia, the WASHES project wasdesigned to include a strong hygieneeducation component, but the managers'enthusiasm for latrine construction andcommunity-based resource mobilizationeventually overshadowed education

16
activities. The evaluation noted that "healtheducation was an afterthought toconstruction." Project technical andmanagerial staff were also unconvinced thatchanging hygiene behavior was importantfor lasting improvements in sanitation, andproject training failed to address thisnecessity [REF 3]. A second example ofweak coordination between building andpromotion comes from the BaluchistanIntegrated Area Development Program inPakistan. The labors of large teams ofengineers and community developmentworkers did not mesh despite training toorient staff to the benefits of communityinvolvement in programming [REF 2].
Because demand for sanitation must oftenbe generated, project success dependsmore on marketing than on the efficiency ofengineers and builders. The scope andpace of program development are definedby consumer demand. Two evaluationssuggested that successful promotionrequires extensive support and supervisionof the staff assigned to fulfill this task, whichis normally neglected by program managers[REF 2,13].
Coordination of Implementation
Whether government or private agenciesare responsible for implementation, there islikely to be a need for a coordinating bodyto ensure the effective working of differentelements, to prevent duplication andconflict, and to standardize practices andmaterials. Coordination is necessary atcentral as well as local levels.
There were few examples of national orlocal coordination. In Belize, theresponsibility for coordination wastransferred from the health to the publicwork ministry, upsetting a well-functioningprogram and causing friction between thetwo ministries [REF 7]. Lack of coordinationbetween different levels and areas ofgovernment in Bangladesh was cited as an
impediment to program implementation[REF 30].
3.23.2 Role of SanitationRole of SanitationConsumersConsumers
"The highest rates of coverage havegenerally been achieved by sanitationprograms in which the decision to installlatrines is made collectively and communityinstitutions are mobilized to ensure itsimplementation" [REF 13, p. 44].
The advantages of involving consumers inproject execution are legion. In Benin, thesustainability of project activities was linkedto the continuity of local committees [REF23].
In other countries, projects in whichcommunities had a hand in design andmanagement demonstrated a high level ofcommunity responsibility for operation andmaintenance. In both the WASHES projectin Indonesia and the Orangi project inPakistan, consumers have maintainedfacilities at a high standard because theyfelt they were part of the investmentprocess. Participation from the outset hasgiven them a sense of ownership andresponsibility for sustaining the flow ofproject benefits [REF 2, 3].
Program planners are becoming convincedof the necessity of community participation,as evidenced by 77 percent of theevaluations that noted some form of this inproject activities. However, few projectshave encouraged participation in all aspectsof programming. In most cases,participation was limited to the constructionphase and usually entailed a contribution oflabor, materials, or finance, rather thaninvolvement in planning or management[e.g., REF 4, 5, 8, 27]. Only 17 percent ofevaluations reported any direct involvementin needs assessment and project design,

17
but consumers did play an important role inpromotional and education activities and inproject financing.
The Busti program in Karachi, illustratingthe many ways in which communities cancontribute, attracted the support of 47community organizations, which performeda range of functions from generatingparticipation in the construction of facilitiesto social mobilization and the lobbying oflocal authorities. Households participated inpromotion by building demonstrationlatrines in 5 percent of the area's 25,000houses and inspiring the building of 14,000latrines more. A key to this success was theincorporation of women in promotionalactivities. Initially, two women were trainedas health educators to raise awarenessamong women and children of the linksbetween sanitation and health. This workedso well that it stimulated the introduction ofa basic education course for girls known asthe Home Schools project.
There were three factors that enhancedthe contribution of community participationto program success. The first was the useof existing community organizations insteadof creating new institutions. In Haiti, forexample, a sanitation project created villagecommittees for pump maintenance,hygiene, health, and women's welfare, buttheir roles in project activities were oftenunclear and their foundation in thecommunity was precarious [REF 21]. Thesecond factor for success was acommunity's organizational capacity, itsconfidence in problem solving, and theextent to which it invited women'sparticipation. In Indonesia, for example,local committees with management abilitieswere greatly responsible for the success ofcommunity financing schemes [REF 3]. Thethird factor was consumer participation inthe design, management, and financing of aproject, which generates a sense ofownership and responsibility for sustainingproject benefits.
18
Box 3 Components of Success: Stimulating and Sustaining Demand in Pakistan
The Baldia Township project in Pakistan succeeded in building 14,000 latrines in six years in response towidespread demand. Although the community was initially not convinced of the value of the proposedtechnology, promotional and educational efforts quickly generated sustained demand, encouraged propermaintenance, and helped the project capitalize on the high degree of dissatisfaction with existing facilities(bucket latrines) [REF 2].
Box 4 Components of Success: LinkingHardware and Softwarein Lesotho
Lesotho's national sanitation program, established in1983 initially as a single-district pilot project, isregarded as a model of integration of well-testedtechnologies, community involvement, andinnovative organization and management styles.Government now plays a largely organizational andfacilitative role, having successfully integrated theprivate sector and community groups into programimplementation. Health education and theinvolvement of women are the basis of the strategy.The high demand for latrines and the goodmaintenance levels are attributed to changes inpeople's belief about sanitation and an increasedsense of ownership from participation [REF 4, 5, 6].
Project success is rarely determined bychoice of technology, organization andmanagement, or consumer involvementalone. In most instances, it was acombination of the three that achieved highfacility coverage and utilization and thecontinuity of project benefits. The examplesdescribed in Box 3 and Box 4 illustrate this.
3.3 Influencing Behavior:3.3 Influencing Behavior:Marketing and Promoting, orMarketing and Promoting, orChanging Hygiene Practices?Changing Hygiene Practices?
The importance of changing hygiene-relatedbehavior for improving health is now widelyrecognized among sanitation programplanners (Yacoob et al. 1992). The previousassumption that latrine construction wouldlead to latrine use and that latrine use would
lead to better health meant thatinterventions often ended with thecompletion of facilities. Yacoob et al.ascribed the failure of many projects toexcessive emphasis on technology atthe expense of behavior modification.
Fortunately, there is evidence that achange in thinking is taking place. Agradual shift in program emphasis isreported by Beyer in a 1991 review of200 UNICEF water and sanitationevaluations, and is evident from the factthat 86 percent of the evaluationsexamined for this report—most of whichcovered projects implemented in thepast eight years—included a referenceto changing hygiene behavior (seeAppendix 3).
However, project designs do not yetdifferentiate between behavior associatedwith the demand for sanitation facilities andbehavior associated with health andhygiene practices. They may add abehavioral component, but only to enablelatrine construction to succeed. Projectsand evaluators generally betray a lack ofunderstanding of the complexities ofchanging hygiene practices. For example,programmers should clarify whetherbehavioral change is intended to promote

19
latrine construction, the use of latrines, orhand washing after use. Is it more akin tomarketing a facility, or stimulating a changein community beliefs about the link betweenhealth and sanitation? Different methodsare necessary for different purposes.
Many projects have learned through failurethe costs of neglecting the behavioralaspects of sanitation programming. InBelize, for example, no funds werebudgeted for health education in the firstphase of the project because managersassumed that health workers would do this.However, the assumption was provedwrong by a lack of enthusiasm, propertraining, and support for PHC workers, andrevised plans therefore added intensivetraining of health educators to the projectprofile. Even then, education made littleheadway because male health educatorswere found to be less effective thanfemales. By the time a team of womenhealth educators was trained, the projecthad been delayed by two years [REF 7].
Most of the evaluations that mentionedbehavioral change did so in the context ofstimulating demand for sanitation facilities(and thereby encouraging consumercontribution to building them) rather thanchanging hygiene practices. Some includeda hygiene education component to raiseawareness of the link between health andhygiene and encourage the proper use oflatrines, but few touched on such practicesas disposing of children's feces or handwashing.
Program success, therefore, was oftenmeasured by the numbers of latrines built.Moreover, it appeared that programs with abehavioral component had not surveyedhygiene beliefs and practices in thecommunity prior to project implementation,a fact that has two consequences. First,without baseline information, healtheducation cannot effectively modify existingpatterns of behavior. In Nepal, health
education raised awareness of the benefitsof safe excreta disposal, but the belief thatchildren's stools were harmless and that itwas unsafe for children to use the latrinediscouraged mothers from changing theirchildren's defecation habits. Latrines werebuilt but only some members of thehousehold were using them. The secondconsequence is that, without a clearunderstanding of attitudes to hygiene, it isvery difficult to discern whether anyappropriate behavioral change has takenplace as a result of project interventions.Only one evaluation assessed changes inhygiene behavior over time and attemptedto link these changes to project activities[REF 20]. A recent study in Kenya testifiesto the importance of looking beyondcoverage statistics for a betterunderstanding of hygiene-related behavior(Box 5).
3.3.1 Techniques for3.3.1 Techniques forStimulatingStimulating
Behavioral ChangeBehavioral Change
Success in influencing behavioral changedepends on four factors: a clear sense ofpurpose; the use of participatorytechniques;5 the inclusion of women aspromoters/ educators and targets; and thesimultaneous employment of a range oftechniques. In general, techniques that relyon demonstration rather than exhortationhave a better record of success [REF 13].
For promoting latrine construction,incentives in the form of price adjustmentsand availability of credit or subsidy weresuccessfully combined in Punjab, Pakistan[REF 2]. However, in Botswana, cost wasnot a factor when other conditions werefavorable. Promotion and education inducedrural households to pay an average of $110for a latrine, far exceeding theoretical
5 For a discussion of the advantages of participatory techniques seeSrinivasan 1990.

20
estimates of ability or willingness to pay[REF 17].
To change hygiene beliefs and practices, asmall project in Nepal successfullyemployed women sanitation workers toprovide intensive education on site invillages. Unfortunately, the national programmanagers, favoring construction overeducation, gave these women negligiblesupport. A project in Indonesia capitalizedon high levels of community involvement tobring about rapid and sustained latrineconstruction and use, but showed nounderstanding of the importance of hygieneeducation in project success. The staff andthe beneficiaries also displayed littleawareness of links between hygiene andwater-and-sanitation-related healthproblems. The evaluators of the projectconcluded that while traditional hygieneeducation through posters, films, or signson the latrines to encourage their use hasvalue,
experience in hygiene education showsthat just providing information to peopleencouraging them to change theirbehavior is usually not sufficient topromote change. Experiences in manycountries suggest that more effectiveways to promote sustained changes inindividual hygiene-related behavior areto change community norms and valuesregarding those practices. [REF 3, p.26]
One proven successful technique forchanging hygiene beliefs and practices is toengage 'gatekeepers,' or influentialcommunity leaders, in promotion andeducation. Gatekeepers can win communitysupport for new ideas and a commitment bythe community to solve hygiene-relatedproblems [REF 2].
3.3.2 Techniques for3.3.2 Techniques forAssessingAssessing
Hygiene Behavior andHygiene Behavior andBeliefsBeliefs
The absence of reporting on the relationshipbetween hygiene beliefs and behavior andproject activities may be attributed to a lackof available techniques for incorporatingsuch information into project planning andmonitoring. However, the increasedapplication of such techniques asparticipatory rural appraisal (PRA) tosanitation programming, as found in theSiaya project in Kenya, shows promise[REF 38]. Guidelines on hygiene educationand communication in sanitationprogramming are also becoming available(Boot 1990 and Boot and Cairncross 1993).
3.43.4 Capacity BuildingCapacity Building
Most evaluations failed to include capacitybuilding as a criterion, yet one question thatshould be asked in every evaluation iswhether projects are enabling localinstitutions and people to address sanitationproblems on a sustainable basis.Discussion of the effect of investment oncapacity building was implied rather thanreported directly, signifying either a lack ofconcern or a lack of understanding of thesubject. The term itself is variously definedby different implementing agencies.Moreover, because it encompasses a rangeof activities (e.g., system development,management support, organizationaltraining, public participation in operation andmaintenance), there are, as yet, nostandard methods or indicators formeasuring change in local capacity (Vesth-Handen and Engberg-Pederson 1992).Thus, the findings on capacity buildingreported here are based on personalexperience and interpretation of theconcept.
The earlier discussion of organization andmanagement noted that overall

21
responsibility for sanitation is often splitamong several agencies or institutions,which makes it difficult for investors todecide which institution to strengthen. Anatural response is to set up a separateimplementing unit that bypasses thegovernment altogether or to work directlywith nongovernmental groups and theprivate sector. Both approaches facilitateproject implementation but underminenational capacity building. In Baluchistan,the BIAD project set up a separatemanagement unit staffed with governmentengineers and other public sectoremployees, whom it trained in integratedand participatory management that could beapplied elsewhere once they returned to thepublic sector. Nevertheless, the donors thenengaged consultants and contractors todesign the first phase of the project. Wheregovernment staff could have benefited fromtaking responsibility for programming, theywere relegated to be workers whoseprimary task was fulfilling project objectives[REF 2]. Capacity was being built, but thedonors appeared more interested insafeguarding their investment thanempowering national agencies.
There were a number of examples ofprojects implemented through thegovernment, but here, too, capacity buildingwas often hindered by the implementationstyle. Evaluators attributed the failure of thesanitation component of a project inManshera district, Pakistan, to theinadequate training of district councilmembers in managing the software aspectsof programming. Consequently, theconstruction of water systems raced aheadwhile sanitation and hygiene educationwere left to flounder [REF 2]. A secondexample in Pakistan was the PunjabSanitation Program (1981-1986)implemented in collaboration with theprovincial government, which dealt withday-to-day administration while the donortook responsibility for formulating policy,coordination, funding, and training. Becausethe donor made no provision for handing
over these tasks to the government when itwithdrew, the program stopped abruptly andsanitation promoters and village sanitationcommittees, which had developed intoviable community organizations, weredisbanded.
By contrast, the Lesotho national sanitationprogram gradually grew from districtmanagement to management by twogovernment ministries. District officials andworkers were trained and in turn trainedothers who formed district sanitation teams.The intention of program planners was toavoid bypassing the national system inorder to keep costs down and promotesustainability. Evaluators noted twoimportant capacity building effects of theprogram: relations between the Ministry ofHealth and the Ministry of Works werestrengthened through the process ofimplementation, and this improvedrelationship changed the attitude ofdecision-makers toward sanitationprograms. For the first time, officials beganto appreciate the need to integrate thehardware and software components.
Projects were fairly consistent in theirattempts to build capacity at the communitylevel, often seeking to develop localinstitutions to facilitate projectimplementation. In the Punjab, for example,community leaders were trained to managesanitation projects [REF 2]. In Indonesia,community management and financingserved as the basis of the CARE water andsanitation project, which trained communityleaders to assume responsibility for waterand sanitation, thus ensuring the continuityof project benefits [REF 3].

22
Box 5 Hygiene Behavior and Latrine Use in Kenya [REF 38]
Evaluation of the health education component of the Siaya project in Kenya revealed that local hygiene-related beliefs and practices may be hindering the project's capacity to influence health status. Some of thefindings were as follows:
C Latrine use was found to be low for a number of reasons. First, social and cultural factors posedsignificant constraints on latrine construction, use, and maintenance. Digging the pit, building thesuperstructure, and making the roof are considered the man's responsibility. If the latrine is in need of repairand a male family member is not available, it will not be used; nor will it be used if a daughter-in-law, who isresponsible for cleaning it, has not done so.
Second, people were discouraged from using latrines because they were not readily accessible. Latrinesare built outside the compound because of local customs on privacy, social space, and kinship roles. If it isbuilt inside the compound, the latrine cannot be shared by in-laws. Using a latrine in the presence of in-laws is tantamount to being undressed in front of them.
Third, many latrines were not used because they were built to satisfy a Chief's order. These Chiefs'latrines are required by law every time there is a cholera outbreak. They are often of inferior quality and arebuilt only to satisfy the demands of the Chief. Figures of latrine coverage would therefore rise rapidly aftercholera epidemics, but real utilization will not have changed.
C Hand washing was perceived as good but not practical. Soap was used for washing after eating but notbefore.
C Mothers did not perceive the necessity of hand washing after handling children's stools, which areconsidered harmless. Mothers buried children's feces even when latrines were available.
3.4.1 Constraints to3.4.1 Constraints toCapacity BuildingCapacity Building
Two important aspects of sanitationprogramming were found to underminecapacity building. The first was an approachthat failed to place projects in a sectoralcontext, often designing them to function ina vacuum unconnected with other sectoralactivities. For example, while CARE'sproject in Indonesia built a successful modelof community management and financing, itdepended on technical assistance andlogistical support from CARE itself. Boththese functions could have been performedby government or another local institution,but no provision was made for transferringthese responsibilities. Successful capacitybuilding requires a sectoral perspective forinvestment.
The second constraint related to thechanging roles and responsibilities of thewater and sanitation sectors in developingcountries linked to decentralization anddemocratization and new approaches todonor assistance (Box 6). For example,decentralization dramatically changes theroles of central and local governments,giving the local government responsibilityfor planning and implementation andleaving the central government to set policyand oversee sectoral operations. InBangladesh, the early stages ofdecentralization began to blur the division ofresponsibility among district levelinstitutions, disrupting project activities [REF11]. Moreover, donors themselves arebeing pushed to show that aid funds haveachieved 'value for money' and aretransferring these pressures to theirinvestment partners in developing countries.These changes complicate the identification
23
Box 6 Current Changes in theOrganization and Management of theWater and Sanitation Sectors
C External implementing agencies arebeing pressured by their funding sources tobecome more efficient and are transferringthese expectations to developing countrygovernments and their NGO partners. To thisend, efforts are being made to change therole of government (particularly the centralgovernment) from service provider topromoter or regulator of sanitation activities.
C There is a general movement towarddecentralization of public sector responsibilityas a natural response to pressures forgreater efficiency. Decentralized structuresare often more responsive to sectoral needsand bring implementors closer to thecommunity, facilitating communityparticipation (Edwards et al 1992).
of capacity building needs and are rarelyconsidered in project evaluations.
3.53.5 Economics andEconomics andFinancingFinancing
Only a few evaluations reported economicand financing information and even fewerproffered any explanations of importancefor program success. It is not possible,therefore, to provide a comparativebreakdown of project financing by source(e.g., government, donor, and householdcontribution) or by expenditure category(e.g., construction, promotion,management, training).
The cost of erecting a single facility wassometimes compared with beneficiary abilityto pay, allowing some estimation of theeffect of project financing on the access tosanitation by different income groups. Forexample, in Lesotho, a VIP latrine wasestimated to cost $75 - $150, just less thanthe average monthly income, suggestingthat 45 percent of the target population
could afford to buy a latrine, 30 percentwould require credit, and 25 percent wouldrequire a substantial subsidy [REF 4].6
While the cost did not appear to haveadversely affected demand, the latrinedesign, which sought to avoid the need fora subsidy, probably denied people in thelowest income group access to sanitation.
3.5.1 To Subsidize or3.5.1 To Subsidize orNot to Subsidize?Not to Subsidize?
The choice of financing has an importantinfluence on capacity building andsustainability. Some projects have made it apolicy not to subsidize the cost of materialsand construction so as to avoid dependenceon external resources. Others choose costsharing by government, donors, andhouseholds. Despite the adverse effect onsustainability, donors and governments areoften tempted to resort to subsidies tospeed up implementation and makeexpensive technology affordable.
It was rarely clear how decisions aboutfinancing were made or whether theydepended on the community's willingnessor ability to pay. The Lesotho review notedthe necessity of proactively gatheringinformation on the ability and willingness ofconsumers to pay because estimates bygovernment and donors are oftenimprecise. Economists estimate that peoplein developing countries will spend two tothree percent of their income on sanitation,but each population and sub-population willdiffer.7 Until accurate methods of estimatingdemand are readily accessible to planners,trial and error is the only way to gauge theextent of financial support required forachieving a given level of coverage [REF13]. Nevertheless, the affordability of
6 While recurrent costs for sanitation are low, recurrent costs for waterare 20 percent to 40 percent of income.
7 This proportion is likely to be less in lower income groups.

24
sanitation to consumers, governments, anddonors should not be overlooked. WHO(1987) reports a median per capita cost of$120 for onsite urban sanitation and $60 forstandpipe water supply in the leastdeveloped countries, which may explain theslow pace of sanitation programming ingeneral.
The respective contributions of thegovernment and the donor are often spelledout in the project document. However, in anumber of countries, the government'sinability to meet its obligation often hinderedproject implementation [REF 2, 7]. TheWASHES project in Indonesia faced adifferent problem. The government's budgetcycles could not be adjusted to the slowerpace of community-led project expansion.Eventually the project lost financingbecause it could not spend its entireallocation in the specified period. Thesustainability and effectiveness of Lesotho'snational sanitation program testified to thebenefits of formulating sectoralimprovement plans that work within existingbudgetary constraints. However, while it hasmanaged to make sanitation facilitiesaccessible to the majority of the population(without an artificial dependency on externalresources), it still faces financial constraintsto achieving universal coverage.
3.6 Intra- and Inter-3.6 Intra- and Inter-Sectoral LinksSectoral Links
3.6.1 Water and3.6.1 Water andSanitationSanitation
Among the advantages of introducingsanitation along with water supply thatGlennie (1983) cites are greater healthbenefits and the ease of generating ademand for sanitation once the need forwater is met. Approximately 51 percent ofthe documents reviewed reported some linkbetween sanitation and water supply, and in
most cases the results were positive. Forexample, the Baluchistan Integrated AreaDevelopment Project succeeded ingenerating a demand for sanitation bybasing its promotion strategy on meetingthe community's demand for water [REF 2].Program mangers in Bangladesh wereequally successful by making watercontingent on acceptance of a sanitationfacility. In Lesotho, increased use of waterand altered health and hygiene were sold inone package as improved sanitation [REF4]. While the combination of improved watersupply and sanitation often has a greaterimpact on health than each on its own,there is some evidence of operationalproblems with integrating the two. A fewevaluations noted that the advantage of acombination was offset by the difficulties ofcoordination during implementation. Thepace of construction and promotion of waterprograms may exceed that of sanitationsimply because the demand for water isoften just waiting to be tapped. In contrast,failure to link up with a successful watercomponent limited the progress ofsanitation programming in Pakistan'sManshera district.
3.6.2 Sanitation and3.6.2 Sanitation andOther SectorsOther Sectors
The most common inter-sectoral link wasbetween sanitation and health. In manycases, use of a well-developed PHCinfrastructure proved a rewarding strategy,such as in Botswana [REF 17]. However,dependence on a poorly funded health caresystem or an overburdened cadre of healthworkers could be detrimental to educationand promotion activities [see Section 3.12and REF 7].
In Pakistan, extensive efforts at communityinvolvement, health education, andpromotion had positive spinoffs for theeducation and health sectors. Thesanitation program encouraged greaterinvestment in education for girls and health
25
44education for women and children [REF 2].Some programs also included theinstallation of sanitation facilities in schools[REF 7].
ISSUES FOR DISCUSSIONISSUES FOR DISCUSSIONAND DRAFT GUIDELINES FORAND DRAFT GUIDELINES FORSANITATION PROGRAMMINGSANITATION PROGRAMMING
Based on the evaluations reviewed and theinformation gleaned from interviews withagency personnel and existing programguidelines, this section presents a numberof issues for discussion and a basicframework for sanitation programming, andpreliminary program guidelines for fieldtesting and/or review.
4.14.1 Issues for DiscussionIssues for Discussion
4.1.1 Summary of4.1.1 Summary ofLessons LearnedLessons Learned
Service Delivery
Technology choice: Choosing atechnology has become less difficult withthe widespread acceptance of the VIPlatrine and the pour flush toilet. An effectivetechnology requires careful consideration ofconsumer preferences and local conditions.Cost, operation and maintenance, and thetimeframe for developing technologies arethree important considerations. High costscan deter acceptance of facilities. Plannersshould strike a balance between productsophistication and ease of operation andmaintenance. While the choice of a low-costtechnology may appear rational, thedemand for a more attractive productrequiring less maintenance may be higher.In addition, introducing and adapting a newtechnology to a particular population takestime. Project managers should have a
flexible approach to programimplementation.
Organization and management: Thechoice of implementing institution, thedivision of responsibilities in servicedelivery, and the coordination of theimplementation process are important forprogram success. Programs implementedby NGOs or the private sector - separatelyor in collaboration with the government - aremore likely to meet their objectives thanprograms implemented by the governmentalone. Sanitation programming often suffersat the hands of weak public institutions, andaid projects that fail to 'build capacity'through investment only exacerbate thisshortcoming. Inadequate coordination of theresponsibilities for building sanitationfacilities and promoting sanitation causescoverage to lag. Because demand forsanitation is often weak, program successdepends more on promoting and marketingthan on the efficiency of construction.Overall coordination of sectoral activities bya single body facilitates programimplementation.
Role of Consumers
Community participation in all phases of aproject yields a high level of communityresponsibility for operation andmaintenance and better prospects forsustainability. However, it is often limited tothe construction phase, a practice
26
frequently cited as an obstacle to effectiveimplementation. The four approaches tocommunity participation most likely toenhance program success are: the use ofexisting rather than new communityorganizations; improving the community'sorganizational capacity and its problemsolving skills; encouraging the involvementof women; and including the community inthe design, management, and financing of aproject.
Influencing Behavior
The failure of many sanitation projects isoften attributed to excessive emphasis ontechnology at the expense of changingbehavior and general hygiene practices.When programs do emphasize behavioralchange, they do not differentiate betweenbehavior to increase demand for newfacilities and behavior to change hygienepractices. Different methods are necessarydepending on the purpose of the desiredchange. Most evaluations noted abehavioral component designed to sellmore latrines; few found evidence of theneed to change hygiene-related beliefs orpractices. Baseline surveys of hygienebehavior were rare, making it impossible todetermine whether programs had beeneffective. Successful behavioral change isachieved by four factors: a clear sense ofpurpose, the use of participatorytechniques, the inclusion of women aspromoters/educators, and the simultaneousemployment of a range of techniques.Techniques for assessing hygiene beliefsand behavior must be made available toprogram planners.
Capacity Building
Most evaluations made no mention ofcapacity building as a criterion, despite itsimportance for sustainability. The division ofresponsibilities that frequently occurs insanitation programming makes capacitybuilding difficult, and donors often get
around the problem by setting up separateproject implementation units. However, inbypassing local institutions, they directlyundermine national capacity building. Bydenying local organizations the opportunityto acquire management skills throughproject implementation and by makinginadequate provisions for handing overmanagement, they in fact contribute to poorprospects for sustainability. Investing ininstitutions at the community level is morecommon than capacity building at thenational and district levels.
To facilitate capacity building, projectsshould reflect sectoral needs andconditions. If they are excessivelydependent on external support and fail tobuild local capacity, they are certain tofalter. Another important consideration isthat the trends towards decentralization andincreased donor demands for accountabilityare imposing new demands on localinstitutions.
Economics and Financing
Economics and financing did not figureprominently in the evaluations. Onementioned the effect of cost on the accessto latrines by different income groups.Without accessible methods for estimatingdemand as demonstrated by ability andwillingness to pay, planners have no way ofgathering data to determine appropriatecost levels. The use of subsidies forfinancing sanitation programs receivedmixed reviews. Subsidization can makeexpensive technology affordable and speedup implementation, but it can also create adependence on external resources. Finally,inadequate public sector financing oftenimpedes the realization of coverage andsustainability goals.
Intra- and Inter-Sectoral links
Sanitation programs linked to water supplyprograms benefit from an increased

27
demand and a greater health impact, butcoordinating the two can be challengingbecause the construction and promotion ofwater programs generally proceed moreswiftly. Some projects promoted linksbetween sanitation and the health andeducation sectors. Primary health workerswere employed to promote sanitation andhygiene education. In the link with theeducation sector, latrines were built inschools and hygiene education wasintroduced in the curriculum.
4.1.2 Information Gaps 4.1.2 Information Gaps
There are several subjects of importance insanitation programming that did not appearin the evaluations and that should beconsidered for inclusion in programguidelines. These subjects are discussedbriefly below:
CC The link between individualsanitation projects and overall sectordevelopment. Defining the relationshipbetween a project and national sanitationpolicy and program development,institutional changes taking place (e.g.,decentralization), and national humanresource development is necessary todetermine whether the project wasdesigned to complement the nationalprogram, inspire it, or change it. Withoutplacing a project in its institutional context, itis difficult to assess its contribution tooverall sector development andsustainability. C The link between sanitation and thenational context. The influence of landtenure, housing, democratization, andsimilar factors on sanitation programmingshould not be ignored. Urban sanitation inparticular should be approached in thewider context of urban planning and thesefactors.
C Methods for measuring demand forsanitation. Program managers should have
the tools to measure the demand forsanitation, an essential ingredient of anyreliable feasibility study.
C There should be some means tomeasure appropriate utilization ofsanitation facilities.
C Data on the financing of sanitationprograms are essential if cost-effectivenessand financial sustainability are to bedetermined.
C Indications of who benefited from asanitation project, which target groupswere selected, and who gained access tosanitation (e.g., by income, geographicalarea, gender) provide evidence of whetherthe neediest were reached by investment insanitation.
C A record of pre-project hygienepractices and project-linked changes inhygiene behavior should be constructed.
C Details of inter-sectoral linkages, inboth numbers and variety, must beprovided.
4.1.3 Dispelling Myths 4.1.3 Dispelling Myths
This report questions three common beliefsabout sanitation programming:
1. UNICEF Program Guidelines for Waterand Sanitation (UNICEF 1988) suggest thata sanitation program should be introducedafter a water program has been securelyestablished. Clearly, the proven benefits ofsanitation and the necessity of acceleratinginvestment in the sector refute this advice.More recent documents strongly advocate ahigher priority for sanitation than it waspreviously accorded, even if this entailsdelinking it from water and from traditionalconstruction style programs.
28
2. Contrary to the assumption that low-costtechnologies are always more appropriatein poor countries than higher cost,sophisticated facilities, there is evidencethat, in some cases, low-cost technologiesdiscourage demand. Programs are morelikely to succeed if they heed consumerpreferences.
3. Simply encouraging latrine constructionand use is not sufficient. To make an impacton health, programs must includebehavioral components designed to alterhygiene beliefs and practices unrelated tothe use of latrines.
4.2 Basic Framework for4.2 Basic Framework forSanitation ProgramsSanitation Programs
Planners are beginning to change theirperceptions of what constitutes a goodsanitation program, although as yet there isno single paradigm that incorporates all thebest ideas. Experience indicates that certaincombinations of factors must be present fora program to be considered successful.
Box 7 A Successful SanitationProgram will —
< Improve the health of beneficiary groups;< Be financially, organizationally, and
politically sustainable;< Maximize the benefits of investment by
reaching the greatest number of people;< Enhance local institutional and community
capacity for organization andmanagement; and
< Protect the environment.
4.34.3 Draft Guidelines Draft Guidelines
4.3.1 Overall Aims and4.3.1 Overall Aims andObjectivesObjectives
The general goal of UNICEF sanitationprograms is to ensure that all householdsbenefit from a healthy physical environmentfree from avoidable health hazards.According to the 1988 UNICEF programguidelines, environmental health risks willbe reduced "by establishing appropriatearrangements for the safe disposal ofhuman and other wastes, the control ofdisease vectors, hygienic food handling,and other practical environmental sanitationmeasures including, in particular, informingand educating the community." (UNICEF1988, section 4.1, page 2)
4.3.2 Program Aims4.3.2 Program Aims8
1. The fundamental aim of a sanitationprogram is to improve health status.
2. Programs should make sanitationfacilities more convenient, affordable,appropriate, and reliable.
3. Sanitation programs should enhance thecommunity's capacity to manage its ownenvironment.
4. Sanitation programs should enhance thecapacity of local institutions to addresssanitation problems.
4.3.34.3.3Guiding PrinciplesGuiding Principles
Based on the data gathered fromevaluations and interviews, there is aconsensus that sanitation programs shouldfacilitate:
CC Long-term self-reliance. They shouldaim for sustainable growth rather than rapidcoverage. The choice of sanitation systemshould be guided by the likelihood of
8 Partially adapted from UNICEF program guidelines.

29
sustainability not simply by technologicalmerit.
CC Cost-effectiveness. Investment shouldseek to deliver the greatest health (andother) benefits to the greatest number ofconsumers at the lowest cost.
CC Technical, organizational, political,and financial sustainability. Programsshould be designed for local capacities andconditions to ensure that the people canmaintain the flow of benefits frominvestment.
CC Expansion of sanitation activities.Programs should permit the expansion ofcoverage without risking effectiveness,efficiency, and sustainability.
CC Environmental protection. Programsshould not pollute the environment.
There is no general agreement on:
CC Dealing with demand: respond to itor generate it? There is somedisagreement about whether sanitationprograms should respond to demand orcreate it. The World Bank advocatesinvesting only where there is a demand, anapproach that ensures greater cost-effectiveness and demonstrates to skepticsthe benefits of improved sanitation. Otherorganizations, such as UNICEF, aremandated to assist the neediest segmentsof the population.
CC Targeting program activities. Arelated concern is the way beneficiaries areselected and whether the neediest groupsmust be given priority. Most evaluations didnot explain the methods for choosing theproject site or the target population, or whyone project area or community was chosenover another. In Pakistan, the decision wasleft to local government authorities, who
placed political considerations before need[REF 2].
If the purpose of investing in sanitation isto ensure that donor assistance achievesthe best results at the least cost, thenincreased access to sanitation for middle-income groups is considered a programsuccess. Alternatively, is it wise tocompromise financial sustainability or cost-effectiveness in order to improve access forthe poorest groups? The World Bank wouldargue that responding to existing demanddoes benefit the poor by establishing asustainable sanitation system that reducesdisease transmission and environmentalpollution, and that encourages demandcreation through demonstration andstimulating poorer groups to design theirown solutions to sanitation problems.
CC Financing arrangements: theadvantages and disadvantages ofsubsidies. Although it is often assumedthat subsidized construction will increasedemand, some evaluations suggested thatsubsidies can discourage utilization over thelong-term by creating dependence onexternal resources and weakeningcommunity responsibility for operation andmaintenance.
CC Integrating sanitation with water andother sectors. There are obvious healthbenefits from linking water, sanitation, andhealth education, as evidenced in WaterAid's program strategies. However, there issome concern about the ability of programmanagers and implementing institutions tocope with the demands of integratedprogramming.
CC Adequate coverage. Some considerthat coverage and utilization should reach90 percent for maximum health benefits[REF 13, p 5]; others conclude that 75percent coverage is adequate.

30
4.3.4 Essential Program4.3.4 Essential ProgramActivitiesActivities
The following program activities arerequired for the application of theseprinciples:
CC The maximum participation of thecommunity in program planning,implementation, operation, andmaintenance. This is important forgenerating demand, financing activities,designing program strategies and plans,stimulating behavioral change, choosingtechnologies, and developing maintenancestrategies.
CC The use of mechanisms to measureconsumer demand as the basis fordesigning program strategies and plans.
CC Capacity building of groups at all levelsof the system.
CC Selecting a technology based on localpreferences, the differences in the abilityand willingness to pay among communitygroups, capital and recurrent cost tradeoffs,availability of local building materials, andoperation and maintenance requirements.
CC Promoting behavioral change throughinformation and education.
CC Identifying a strong central agency toimplement a devolved program that plans,manages, and evaluates sanitationactivities. It would eventually change frombeing a direct provider of services to takingresponsibility for promotion, regulation,training, advocacy, and facilitation.
CC Establishing and supporting a cadre ofsanitation workers.
CC Placing sanitation program strategies inthe context of external economic, political,and institutional factors.
CC Exploring the comparative advantagesof public and private profit and nonprofitagencies in sanitation programming.
CC Developing appropriate financingmechanisms.
CC Promoting financial sustainabilitythrough cost-effective technologies andmanagement approaches, communitymanagement, community financing andcost sharing, standardization of equipment,increased utilization of the private sector,and improved monitoring and evaluation.
CC Promoting change in hygiene beliefsand practices.
4.3.5 Recommendations4.3.5 Recommendationsforfor
Operational Guideline Operational Guideline
General
1. Design and implement programs inresponse to local needs and conditions,using local people and local solutions.Improve existing facilities before introducingnew technologies.
2. Display flexibility in operational plans tomaintain responsiveness to local needs andconditions.
C Adjust programming time frames,strategies, implementation schedules, andbudgets to suit the pace at which localgroups and institutions can function anddevelop.
C Balance emphasis on production targetswith other program objectives (e.g.,capacity building, behavioral change, andsustainability).

31
C Identify and clearly define indicators toassess progress in capacity building,behavioral change, and sustainability.
3. Assess demand at the outset and tailorthe program to meet it.
4. Take a fresh approach in each locality.Avoid blueprints of project designs.
Technology choice and development
1. Examine local solutions to sanitationproblems before introducing a newtechnology.
2. Respect consumer design preferences.
3. Assess consumer willingness to pay fordifferent technologies, ensuring that variousincome groups are considered.
4. Estimate the extent of promotion neededto generate demand for differenttechnologies.
5. Allow sufficient time for testing andadapting technologies before going to scale.
Organization and management
1. Clarify the roles and responsibilities ofdifferent institutions involved inprogramming.
2. Use institutions in program activitiesaccording to their abilities; combining theskills of the public and the private sector isbetter than depending exclusively on one orthe other.
3. Adapt investment cycles, planning andbudgeting mechanisms, and implementationschedules to a community-based, demand-led strategy.
4. Implement the construction, promotion,and behavioral components of the programto facilitate the realization of programobjectives.
Behavioral change
1. Make an initial assessment of beliefs andpractices related to sanitation as the basisfor designing behavioral changes andmonitoring progress toward objectives.
2. Identify the aspects of beneficiarybehavior to be changed.
C Distinguish between the promotion ormarketing of facilities, the promotion ofappropriate utilization and maintenance,and changing behavioral practices andbeliefs affecting health and hygiene.Promotion of facilities may require socialmarketing, whereas encouraging newhygiene practices may require traditionaland nontraditional forms of health education(e.g., employing gatekeepers).
C Choose indicators for monitoring andevaluation that reflect desired changes inhygiene practice.
3. Maximize the impact of health educationand program activities aimed at behavioralchange by:
C employing participatory techniques,C targeting messages and activities towomen and children,C using women as facilitators, andC employing several techniquessimultaneously.
Involving sanitation consumers
1. Begin involving the community as earlyas the pre-project feasibility study.
2. Prepare the community beforeintroducing a new technology.
32
C Develop community awareness of thevalue of sanitation and the requirements foroperation and maintenance of facilities.
3. Assist government to develop aninstitutional framework that supportsparticipation. Government proceduresshould enable communities to play anactive role in planning, management, andevaluation.
C Encourage the establishment ofmechanisms and procedures for shareddecision making.
C Promote links between nationalinstitutions and communities.
4. Adjust program goals, the pace ofimplementation, and indicators to suitcommunity needs and capacity.
5. Focus program activities on women.
6. Engage existing community organizationsbefore creating new institutions.
C Train community groups to acquireorganizational skills.
C Build confidence in problem solving.
Capacity building
1. Clarify the roles and responsibilities ofimplementing agencies.
2. Define the human resource requirementsfor different levels of government and fordifferent implementing institutions. Supportthe development of skills through trainingand participatory programming.
3. Strike an appropriate balance betweenprogramming for immediate results andcapacity building for sustainability.
4. Avoid setting up independentmanagement units or excessive reliance onexternal technical assistance. Ensure thatimplementation through international orlocal NGOs complements, not undermines,the role of public sector institutions.
Financing
1. Choose financing mechanisms carefullyto complement consumer demand andfacilitate sustainability.
2. Target subsidies, where necessary, toaid lower-income groups.
3. Pay greater attention to the absolute costof facilities, the cost-effectiveness oftechnologies and implementation strategies,and the cost of operation and maintenance.
Monitoring and evaluation
1. Establish plans, mechanisms, andindicators for M & E at the outset of theprogram.
C Gather baseline information on allaspects of programming (e.g., coverage,utilization, demand, hygiene behavior).
C Specify the way in which evaluationresults will be employed by programmanagement. Set clear objectives forevaluations.
2. Involve sanitation consumers inevaluations where feasible.

33

34
REFERENCES FORREFERENCES FOREVALUATION DOCUMENTSEVALUATION DOCUMENTS
35
1 Evaluation Survey of Latrine Construction Project (1980) Union of Myanmar, CentralStatistical Organization, Ministry of Planning and Finance, March. U -
2 Pasha HA and McGarry MG, ed. (1989).Rural Water Supply and Sanitation in Pakistan,World Bank Technical Paper No 105, World Bank, Washington DC. E-Q29.254 Wo5812
3 McGowan R, Rahardjo S and Aubel J (1991) Final Evaluation Report ofCare/International's Water and Sanitation for a Healthier Environmental Setting(WASHES) Project, Care International, Indonesia. E-Q29.25 WO8050
4 UNDP/World Bank (1990) Rural Sanitation in Lesotho, From Pilot Project to NationalProgram, Water and Sanitation Discussion Paper Series No 3.
5 Blackett IC (1991) Low-cost Urban Sanitation in Lesotho, A Successful LatrinePromotion Program, unpublished. E-E68.10 WO8902c.2
6 Ministry of Health, Ministry of Interior, Chieftainship Affairs and Rural Development,Lesotho (1986) End of Project Evaluation Workshop Proceedings, Rural SanitationProject, Dec. E-Q29.25 WO5139
7 UNICEF (1990) Final Report, Toledo Water Supply and Sanitation Project, Belize,UNICEF. U - Belize office.
8 New Era (1990) A Comparative Evaluation of the UNICEF Assisted Semi-UrbanSanitation Pilot Program and the East Consult's Sanitation Action Program, Kathmandu,-U.
9 (1988) Joint Evaluation Sind Rural Water Supply and Environmental Sanitation Project,Phase II, UNICEF. - U.
10 Beyer M, (1984) India - Drinking Water Supply, Sanitation and Health Education: AnAssessment, UNICEF Travel Report. U.
11 UNICEF (1988) Rural Water Supply and Sanitation, 1987 - 1988, Annual ProgramReview and Report to Donors, UNICEF, 1988. U-BGD 3.2R AITR
12 Tobin V (1985) Evaluation for Sanitation Planning, A Field Investigation into theDevelopment of Suitable Methods for the Evaluation of the Sanitation Program in Nepal,unpublished MSc dissertation, London School of Hygiene and Tropical Medicine,London.
13 Cairncross, S (1992) Sanitation and Water Supply: Practical Lessons from The Decade,The World Bank, Washington DC.
14 New ERA (1991) Evaluation Report on Women's Involvement in Sanitation in CWSS,UNICEF, Nepal. U

36
15 National Institute of Health Sciences, Kalutara (1991) UNICEF Assisted Survey on TheUse and Maintenance of Latrines in Sri Lanka, UNICEF, Sri Lanka. Ref U116.0058
16 UNICEF (1989) Evaluation Report of North and South Kordofan Water and Sanitationand Health Education Projects, Government of Sudan and UNICEF, Khartoum.
17 Government of Botswana, UNICEF, World Bank, UNDP (1988) Self Help EnvironmentalSanitation Project, End of Project Evaluation Report, UNICEF, Botswana. U BOT 8.331988 AISF
18 Lewin E, Medine M, Sevilla M et al (1991) Water and Sanitation in Central America;Appraisal of UNICEF's Proposal for 1991-1995, A Study Commissioned by SIDA,Stockholm. U GA3.1 WA 1991 AIVV
19 Avaliacao Do Programa De Saneamento Rural (1991) Relatorio Interino, Vist ao CaboDelgado, UNICEF, Mozambique.
20 Loza S, Keller R and Plattenburg et al (1992) Assessment of the Impact of theCombined Water, Sanitation and Health Education Program in Upper Egypt: Draft FinalReport,SPAAC, Egypt. UNICEF-9990010
21 Foucoult H (1988) Rapport D'evaluation du Fonctionnement de 36 comites dedessources, leogane dans le cadre du projet integre eau, assainissement, educationsanitaire, UNICEF/SNEP, Haiti.
22 Roark P, Burns K, Daane J, et al (1993) Midterm Evaluation of Water and SanitationActivities in Malawi: A Review of Two Components of the Promoting HealthInterventions for Child Survival Project, WASH Field Report No 392, WASH, Virginia.
23 Roark P, LaPin D and Kleemeier E (1992) Sustainability Assessment for the Benin Rural
Water Supply and Sanitation Project, WASH Field Report No. 377, WASH, Virginia.
24 Larrea O, Scheider R, Duncan R et al (1988) Final Evaluation of USAID/Catholic ReliefServices Water and Sanitation Program in Ecuador, Peru, Guatemala, Honduras andthe Dominican Republic, WASH Field Report No. 201, Virginia.
25 Edwards D and Torres M (1993) Final Project Monitoring Report 1992-93; Water andSanitation for Health and Ecuadorian Development (WASHED), WASH Field Report No428, WASH. Virginia.
26 Barokas R, Leger P, Warner D et al (1983) Formulation of National Water Supply andSanitation Strategies in the Central African Republic, WASH Field Report No 72, WASHVirginia. U-CAF 3.1F 1983 AIVP
27 Turner J and Buzzard S (1987) Midterm Evaluation of the CARE Water Supply andSanitation Project in Belize, WASH Field Report No 206, WASH, Virginia.

37
28 Karp A, Martin P and Guild S (1990) Final Evaluation of the CARE/Bolivia Child Survivaland Rural Sanitation Project, WASH Field Report No 312, WASH, Virginia.
29 Requena L and de la Parra (1990) Environmental Assessment of the Public ServiceImprovement Project Component III - Water Supply, Sanitation and Health, El SalvadorWASH Field Report No. 229, WASH, Virginia.
30 Abdullah T and Boot M (1989) Progress Review of the Integrated Approach, RuralWater Supply and Sanitation Program, Bangladesh, Volume I: Report, InternationalWater and Sanitation Centre, The Hague.
31 Abdullah T and Boot M (1989) Progress Review of the Integrated Approach, RuralWater Supply and Sanitation Program, Bangladesh, Volume II: Data collection formats,International Water and Sanitation Centre, The Hague.
32 Imo State Evaluation Team (1989) "Evaluating Water and Sanitation Projects: Lessonsfrom Imo State, Nigeria," Health Policy and Planning, 4(1); 40-49.
33 Nordberg E and Winblad UNICEF (1990) Environmental Hygiene in SIDA-SupportedProgrammes in Africa, SIDA, Sweden.
34 Wurzel P (1988) Comments on Punjab Sanitation Program, UNICEF, New York.
35 Christmas J (1989) Report of a Watsan Program Mission to UNICEF Pakistan, UNICEF,New York.
36 Khan A (1992) Orangi Pilot Project Programs, OPP-RTI, Karachi.
37 (1993) Orangi Pilot Project, 56th Quarterly Report, Orangi Pilot Project, Karachi. 38 Almedom A, Mboya T, Moraa V et al (1994) Siaya Evaluation Study (Kenya), London
School of Hygiene and Tropical Medicine, London.

38

39
BIBLIOGRAPHY BIBLIOGRAPHY

40

9 The location and location code are indicated if available. U = UNICEF and E = Environmental Health Project, I = IRC
41
- Evaluations reviewed are indicated with (*)- Evaluations reviewed are indicated with (*)99
*Abdullah T and Boot M (1989) Progress Review of the Integrated Approach, Rural WaterSupply and Sanitation Program, Bangladesh, Volume I: Report, International Water andSanitation Centre, The Hague. I -
*Abdullah T and Boot M (1989) Progress Review of the Integrated Approach, Rural WaterSupply and Sanitation Program, Bangladesh, Volume II: Data collection formats,International Water and Sanitation Centre, The Hague. I -
*Almedom A, Mboya T, Moraa V et al (1994) Siaya Evaluation Study (Kenya), LondonSchool of Hygience and Tropical Medicine, London.
*Avaliacao Do Programa De Saneamento Rural (1991) Relatorio Interino, Vist ao CaboDelgado, UNICEF, Mozambique. U -
*Barokas R, Leger P, Warner D et al (1983) Formulation of National Water Supply andSanitation Strategies in the Central African Republic, WASH Field Report No 72, WASHVirginia. U-CAF 3.1F 1983 AIVP
Bateman, O. Massee and Smith S (1993) A Comparison of the Health Effects of WaterSupply and Sanitation in Urban and Rural Areas of Five African Countries, WASH FieldReport No 398, WASH,Virginia.
Bateman O. Massee and Smith S (1991) A Comparison of the Health Effects of WaterSupply and Sanitation in Urban and Rural Guatemala, WASH Field Report No 352. WASH,A Comparison of the Health Effects of Water Supply and Sanitation in Urban and RuralVirginia. .
Beyer M (1991) Water and Sanitation: A Summary of Evaluations Performed, UNICEF, NewYork.
*_______ (1984) India - Drinking Water Supply, Sanitation and Health Education: AnAssessment, UNICEF Travel Report. U -
*Blackett IC (1991) Low-cost Urban Sanitation in Lesotho, A Successful Latrine PromotionProgram, unpublished. E-E68.10 WO8902c.2
Boot M (1990)"Making the Links" - Guidelines for Hygiene Education in Community WaterSupply and Sanitation, Occasional Paper Series, IRC, The Hague.
42
Boot M and Cairncross S Eds (1993) Actions Speak, The study of hygiene behavior in waterand sanitation projects, IRC The Hague, and London School of Hygiene and TropicalMedicine.
Brandberg (1985) The Latrine Project, Mozambique, IDRC, Ottawa, cited in Cairncross(1992). *Cairncross, S (1992) Sanitation and Water Supply: Practical Lessons from The Decade,The World Bank, Washington DC.
*Christmas J (1989) Report of a Watsan Program Mission to UNICEF Pakistan, UNICEF,New York. U -
*Edwards D and Torres M (1993) Final Project Monitoring Report 1992-93; Water andSanitation for Health and Ecuadorian Development (WASHED), WASH Field Report No428, WASH. Virginia. E -
Elmandorf M (1980) Women, Water and Waste: Beyond Access, WASH, Virginia.
Esrey S (1994) "Multi-country Study to Examine the Relationships Between the Health ofChildren and the Level of Water and Sanitation Service, Distance to Water and Type ofWater Used". McGIll University, Montreal.
Esrey S et al (1990) Health Benefits from Improvements in Water Supply and Sanitation:Survey and Analysis of the Literature on Selected Disease, WASH, Virginia.
Esrey S, Feacham, R and Hughes J (1985) "Interventions for the Control of DiarrhoealDiseases Among Young Children: Improving Water Supplies and Excreta DisposalFacilities" Bulletin of the World Health Organization 63 (4):757-771.
Esrey S and Habicht J (1986) "Epidemiological Evidence for Health Benefits from ImprovedWater and Sanitation in Developing Countries"Epidemiologic Reviews 8:117-127.
*Evaluation Survey of Latrine Construction Project (1980) Union of Myanmar, CentralStatistical Organization, Ministry of Planning and Finance, March. U -
Feachem R, Bradley D, Garelick H et al (1983) Sanitation and Disease: Health Aspects ofExcreta and Waste Management, John Wiley and Sons, Chichester.
*Foucoult H (1988) Rapport D'evaluation du Fonctionnement de 36 comites de dessources,leogane dans le cadre du projet integre eau, assainissement, education sanitaire,NICEF/SNEP, Haiti. U -
Glennie C (1983) Village Water Supply in the Decade: Lessons from Field Experience, JohnWiley and Sons, Chichester.

43
*Government of Botswana, UNICEF, World Bank, UNDP (1988) Self Help EnvironmentalSanitation Project, End of Project Evaluation Report, UNICEF, Botswana. U - BOT 8.331988 AISF
Habicht J, DaVanzo J and Butz W (1988) "Mother's Milk and Sewage: Their InteractiveEffects on Infant Mortality," Pediatrics 81(3): 456-461.
*Imo State Evaluation Team (1989) "Evaluating Water and Sanitation Projects: Lessonsfrom Imo State, Nigeria," Health Policy and Planning, 4(1); 40-49. E -Q29.25 WO5352
Kalbermatten JM, Julius DS and Gunnerson CG, et al (1981) Appropriate Technology forWater Supply and Sanitation (12 vols), The World Bank, Washington DC.
*Karp A, Martin P and Guild S (1990) Final Evaluation of the CARE/Bolivia Child Survivaland Rural Sanitation Project, WASH Field Report No 145, WASH, Virginia. E -
*Khan A (1992) Orangi Pilot Project Programs, OPP-RTI, Karachi. E -
*Larrea O, Scheider R, Duncan R et al (1988) Final Evaluation of USAID/Catholic ReliefServices Water and Sanitation Program in Ecuador, Peru, Guatemala, Honduras and theDominican Republic, WASH Field Report No. 201, WASH, Virginia. E-
*Lewin E, Medine M, Sevilla M et al (1991) Water and Sanitation in Central America;Appraisal of UNICEF's Proposal for 1991-1995, A Study Commissioned by SIDA,Stockholm. U - GA3.1 WA 1991 AIVV
*Loza S, Keller R and Plattenburg et al (1992) Assessment of the Impact of the CombinedWater, Sanitation and Health Education Program in Upper Egypt: Draft Final Report,SPAAC, Egypt. U-9990010
*McGowan R, Rahardjo S and Aubel J (1991) Final Evaluation Report ofCare/International's Water and Sanitation for a Healthier Environmental Setting (WASHES)Project, Care International, Indonesia. E-Q29.25 WO8050
*Ministry of Health, Ministry of Interior, Chieftainship Affairs and Rural Development,Lesotho (1986) End of Project Evaluation Workshop Proceedings, Rural Sanitation Project,Dec. E-Q29.25 WO5139
Murphy H (1994) The Disease Burden of Sanitation-Related Diseases in Latin America,Working paper No. 121, WASH, Virginia, draft.
*National Institute of Health Sciences, Kalutara (1991) UNICEF Assisted Survey on TheUse and Maintenance of Latrines in Sri Lanka, UNICEF, Sri Lanka. Ref U -116.0058
*New Era (1991) Evaluation Report on Women's Involvement in Sanitation in CWSS,UNICEF, Nepal. U -
44
*________ (1990) A Comparative Evaluation of the UNICEF Assisted Semi-UrbanSanitation Pilot Program and the East Consult's Sanitation Action Program, Kathmandu, U -.
*Nordberg E and Winblad UNICEF (1990) Environmental Hygiene in SIDA-SupportedProgrammes in Africa, SIDA, Sweden. E -
Obeng L and Locussol A (1992) Sanitation Planning: A Challenge for the 90s, World Bank,Washington D.C.
*Orangi Pilot Project, 56th Quarterly Report (1993), Orangi Pilot Project, Karachi. E-
*Pasha HA and McGarry MG, ed. (1989).Rural Water Supply and Sanitation in Pakistan,World Bank Technical Paper No 105, World Bank, Washington DC. E-Q29.254 Wo5812
*Roark P, Burns K, Daane J, et al (1993) Midterm Evaluation of Water and SanitationActivities in Malawi: A Review of Two Components of the Promoting Health Interventions forChild Survival Project, WASH Field Report No 392, WASH, Virginia. E-
*Requena L and de la Parra (1990) Environmental Assessment of the Public ServiceImprovement Project Component III - Water Supply, Sanitation and Health, El Salvador,WASH Field Report No. 229, WASH, Virginia. E- *Roark P, LaPin D and Kleenmeier E (1992) Sustainability Assessment for the Benin RuralWater Supply and Sanitation Project, WASH Field Report No. 337, WASH, Virginia. E-
Srinivasan L (1990) Tools for Community Participation; a Manual for Training Trainers inParticipatory Techniques, PROWWESS/UNDP Technical Series, PROWWESS/UNDP, NewYork.
*Tobin V (1985) Evaluation for Sanitation Planning, A Field Investigation into theDevelopment of Suitable Methods for the Evaluation of the Sanitation Program in Nepal,unpublished MSc dissertation, London School of Hygiene and Tropical Medicine, London.U-
*Turner J and Buzzard S (1987) Midterm Evaluation of the CARE Water Supply andSanitation Project in Belize, WASH Field Report No 206, WASH, Virginia. E-
*UNDP/World Bank (1990a) Rural Sanitation in Lesotho, From Pilot Project to NationalProgram, Water and Sanitation Discussion Paper Series No 3. E -
UNDP/World Bank (1990b) Workshop on Goals and Indicators for Monitoring andEvaluation for Water Supply and Sanitation, June 25-29, 1990, Geneva.
UNICEF (1994) Terms of reference for global evaluation of sanitation, UNICEF, New York.

45
_______ (1993) Planning for Health Socio-Economic Benefits From Water andEnvironmental Sanitation Programmes, A Workshop Summary, April 21-22, 1993, UNICEF,New York.
* _______ (1990) Final Report, Toledo Water Supply and Sanitation Project, Belize,UNICEF. U - Belize office.
*_______ (1989) Evaluation Report of North and South Kordofan Water and Sanitation andHealth Education Projects, Government of Sudan and UNICEF, Khartoum. U -
*________(1988a) Joint Evaluation of Sind Rural Water Supply and EnvironmentalSanitation Project, Phase II, UNICEF. U -
_______ (1988b) Program Guidelines: Water Supply, Sanitation and Hygiene, Volume 3,UNICEF, New York.
* ________ (1988c) Rural Water Supply and Sanitation, 1987 - 1988, Annual ProgramReview and Report to Donors, UNICEF, 1988. U-BGD 3.2R AITR
van Wijk C (undated) "Gender Aspects of Sanitation, The missing slipper of Cinderella?'IRC, The Hague, mimeo. I -
Vesth-Handen K and Engberg-Pederson P (1992) Evaluation of UNICEF, Sector report:Water and Environmental Sanitation, Working Paper, publisher not indicated.
WASH (1993) Lessons Learned in Water, Sanitation and Health (Updated Edition)' ThirteenYears of Experience in Developing Countries, WASH, Virginia.
_______ (1992a) Making Choices for Sectoral Organization in Water and Sanitation,Technical Report No. 74, WASH, Virginia.
_______ (1992b) "Playing Catchup with Sanitation: Lessons Learned Forum; Information forAction from the Water and Sanitation for Health Project," September.
_______ (1990) Evaluation Guidelines for Community-Based Water and Sanitation Projects,Technical Report No. 64, WASH, Virginia.
United Nations (1990) Achievements of the International Drinking Water Supply andSanitation Decade 1981-1990, United Nations, New York.
Water Aid (1993) People and Water: Social Aspects of Community Water Supply andSanitation Programmes, Water Aid, London.
WHO (1987) The International Drinking Water Supply and Sanitation Decade: Review ofMid-Decade Progress, WHO, Geneva, cited in Cairncross (1992)
46
World Bank (1990) Water Supply and Sanitation in Africa: Laying the Foundation for the1990s, volume 1, Proceedings of the All Africa Rural Water Supply and SanitationWorkshop and Water Supply and Sanitation Sector Conference, World Bank, WashingtonD.C.
*Wurzel P (1988) Comments on Punjab Sanitation Program, UNICEF, New York. U -
Yacoob M, Braddy B and Edwards L (1992) Rethinking Sanitation: Adding BehavioralChange to the Project Mix, WASH Technical Report No. 72.
Yacoob M and Roark P (1990) Tech Pack: Steps for Implementing Rural Water Supply andSanitation Projects, WASH Technical Report No. 62, WASH, Virginia.
47
APPENDIX AAPPENDIX ATERMS OF REFERENCETERMS OF REFERENCE

48
49
Overall objective: To analyze the experience of designing and implementing sanitationinterventions in developing countries to ascertain lessons for improving the effectiveness offuture investments.
Specific objective: Conduct a literature search of relevant evaluations of sanitationprojects, including a representative sample from both within and outside UNICEF. Theliterature review is considered phase 1 of the global evaluation of sanitation programs.Phase 2 will examine in detail six countries where sanitation projects have been conducted.The final outcome of both phases will be a set of guidelines for country offices in the designand implementation of more successful sanitation programs and a set of succinct casestudies.
Approximately 30 studies should be reviewed from within UNICEF and 30 from otherorganizations, especially the WASH/USAID Project and IRC, the Netherlands.
Examine the following five aspects of sanitation program development in detail:
C Demand for servicesC Service delivery C User satisfactionC Economic factorsC Hygiene behavior and environmental awarenessC Intra- and inter-sectoral linkages
Analyze documents with reference to the six headings, review key lessons, and makerecommendations with respect to how these aspects could be improved in developmentprograms.
Produce a discussion paper to be used at a consultation to be held in May 1994.

50

51
APPENDIX BAPPENDIX BSUMMARY SHEET FOR REVIEW OFSUMMARY SHEET FOR REVIEW OF
SANITATION EVALUATIONS SANITATION EVALUATIONS
52

53
1. Objectives and project history
2. Definition or approach to sanitation
3. Lessons or information gaps related to
3.1 Service delivery: the ability of a sanitation intervention to supply an appropriateservice to beneficiaries.
3.11 Technology selection3.12 Management of service delivery
3.2 Role of the consumer
3.21 Needs assessment3.22 Planning, management, and financing3.23 Utilization/consumer satisfaction
What perceived benefit?
3.3 Behavioral change
3.31 Included in project strategy?3.32 Approach 3.33 Success rate3.34 Measurable health benefits
3.4 Capacity building and institutional linkages
3.41 Community level3.42 Subnational level3.43 National level
3.5 Economic and financing aspects
3.51 Costing data available3.52 Capital and recurrent costs breakdown (by source)3.53 Cost-effectiveness considered
3.6 Intra- and inter-sectoral links
3.61 Between water and sanitation3.62 Between sanitation and other sectors

54
4. Issues raised
4.1 Policy
4.2 Operations
4.3 Technical

55
APPENDIX CAPPENDIX CSUMMARY OF TOPICS INCLUDED INSUMMARY OF TOPICS INCLUDED IN
EVALUATION DOCUMENTSEVALUATION DOCUMENTS

56

57
SUMMARY OF TOPICS INCLUDED IN EVALUATION DOCUMENTS
Ref Tech-nology
Servicedeliv-ery
Commpartici-pation:needsassess-ment
Commpartici-pationplan,mgt,finance
Utiliza-tion
Usersatis-faction
Behav-ioralchange
Health benefit
Capa-citybldg
Cost-ing
Recur-rentcostsesti-mated
Cost effect-iveness
Linkswithwater
Links withothersectors
1 X X X X X X
2 X X X X X X X X X X
3 X X X X X X X X X X X X
4 X X X X X X X X X X X
5 X X X X X X X X X X X
6
7 X X X X X X X X
8 X X X X X X X X X
9
10 X X X X
11 X X X X
12 X X X X X X X
13 X X X X X X X X X X X X
14 X X X X X X
15 X X X
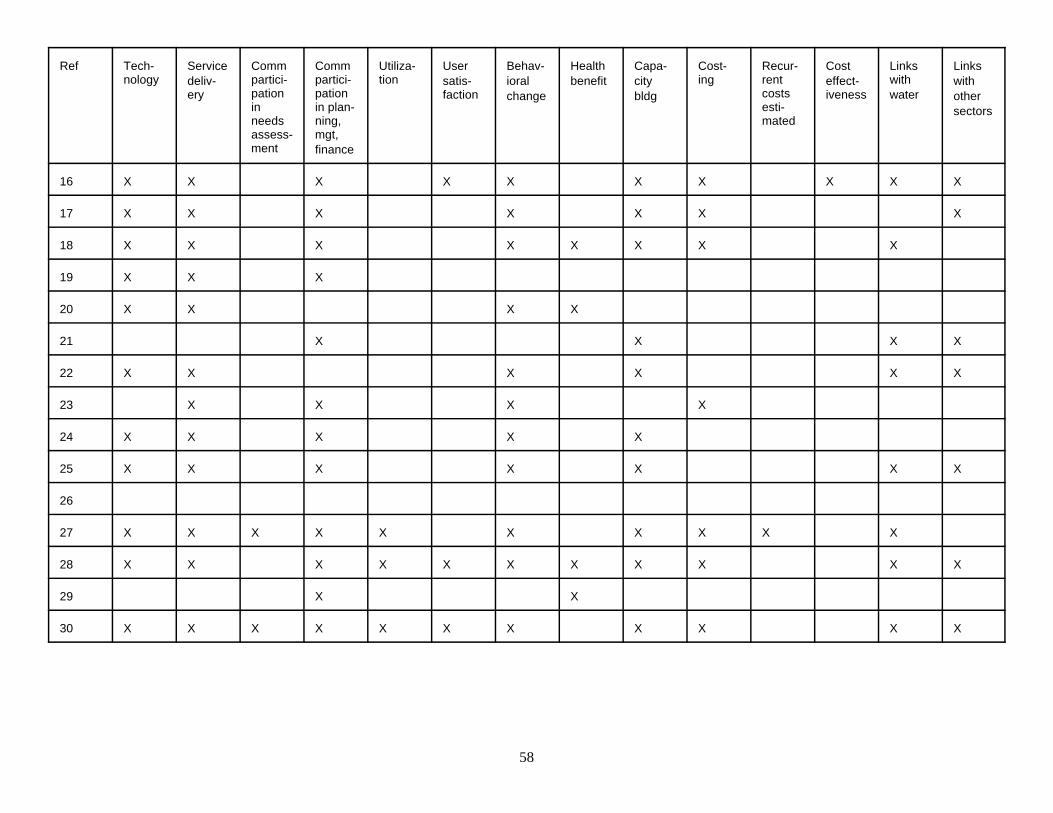
58
Ref Tech-nology
Servicedeliv-ery
Commpartici-pationinneedsassess-ment
Commpartici-pationin plan-ning,mgt,finance
Utiliza-tion
Usersatis-faction
Behav-ioralchange
Health benefit
Capa-citybldg
Cost-ing
Recur-rentcostsesti-mated
Cost effect-iveness
Linkswithwater
Links withothersectors
16 X X X X X X X X X X
17 X X X X X X X
18 X X X X X X X X
19 X X X
20 X X X X
21 X X X X
22 X X X X X X
23 X X X X
24 X X X X X
25 X X X X X X X
26
27 X X X X X X X X X X
28 X X X X X X X X X X X
29 X X
30 X X X X X X X X X X X

59
Ref Tech-nology
Servicedeliv-ery
Commpartici-pationinneedsassess-ment
Commpartici-pationin plan-ning,mgt,finance
Utili-zation
Usersatis-faction
Behav-ioralchange
Health benefit
Capa-citybldg
Cost-ing
Recur-rentcostsesti-mated
Cost effect-iveness
Linkswithwater
Links withothersectors
31
32 X X X X X X X
33 X X X X X X X X X
34 X X X X X X X X X X
35 X X X X X X X
36 X X X X X X X X X X X
37 X X X X X X X X X X X
38 X X X X X
Total 74% 86% 17% 77% 31% 49% 86% 46% 66% 57% 17% 26% 51% 46%
n = 35

60

61
APPENDIX DAPPENDIX DLIST OF INTERVIEW RESPONDENTS ANDLIST OF INTERVIEW RESPONDENTS AND
INTERVIEW GUIDEINTERVIEW GUIDE

62
63
RespondentsRespondents
Dr James Sarn Save the Children FederationMr. Ray Heslop Water Aid (UK)Mr. Albert Wright World Bank
Interview guideInterview guide
Date:Name:Organization:
1. Rough estimate of proportion of work devoted to sanitation
2. Approach to sanitation programming:
a. Standardized goals, strategies, framework?b. Process of designing sanitation interventionc. Are there guidelines available? If not, why not?
Specific issues:
DemandParticipationLinks with other sectorsIdentifying needReaching targetsHardware/software balance Behavioral change
3. Would the organization welcome guidelines?

64







![Wsp Tanzania Sanitation Review Draft Report Final Version[1][1]](https://static.fdocuments.in/doc/165x107/55cf9a72550346d033a1c64b/wsp-tanzania-sanitation-review-draft-report-final-version11.jpg)










