
A rapid scan of the literature · 2010-01-04 · A rapid scan of the literature 26 March 2009...
64
A rapid scan of the literature 26 March 2009 Screening for the early detection of acoustic neuroma in patients with asymmetric sensorineural hearing loss: a rapid literature scan of MRI and other surveillance methods Dan Paech Adele Weston
Transcript of A rapid scan of the literature · 2010-01-04 · A rapid scan of the literature 26 March 2009...
A rapid scan of the literature
26 March 2009
Screening for the early detection of acoustic neuroma in patients with asymmetric sensorineural hearing loss: a
rapid literature scan of MRI and other surveillance methods
Dan Paech Adele Weston
This report should be referenced as follows:
Paech, D, and Weston, A. Screening for the early detection of acoustic neuroma in
patients with asymmetric sensorineural hearing loss: a rapid literature scan of MRI
and other surveillance methods
HSAC Report 2009; 2(1).
2009 Health Services Assessment Collaboration (HSAC), University of Canterbury
ISBN 978-0-9582973-5-6 (online)
ISBN 978-0-9582973-6-3 (print)
ISSN 1178-5748 (online)
ISSN 1178-573X (print)

i
Screening in ASNHL for acoustic neuroma
Review Team
This review was undertaken by the Health Services Assessment Collaboration
(HSAC). HSAC is a collaboration of the Health Sciences Centre of the University of
Canterbury, New Zealand and Health Technology Analysts, Sydney, Australia. This
report was authored by Dan Paech who developed and undertook the literature search,
extracted the data, and prepared the report, and Dr Adele Weston who provided
guidance and reviewed the report.
The current review was conducted under the auspices of a contract funded by the New
Zealand Ministry of Health. This report was requested by Dr Sandy Dawson of New
Zealand’s Ministry of Health. We thank Dr Dawson for assisting in developing the
scope of the review and providing background material for the review.
Copyright Statement & Disclaimer
This report is copyright. Apart from any use as permitted under the Copyright Act
1994, no part may be reproduced by any process without written permission from
HSAC. Requests and inquiries concerning reproduction and rights should be directed
to the Director, Health Services Assessment Collaboration, Health Sciences Centre,
University of Canterbury, Private Bag 4800, Christchurch, New Zealand.
HSAC takes great care to ensure the accuracy of the information in this report, but
neither HSAC, the University of Canterbury, Health Technology Analysts Pty Ltd nor
the Ministry of Health make any representations or warranties in respect of the
accuracy or quality of the information, or accept responsibility for the accuracy,
correctness, completeness or use of this report.
The reader should always consult the original database from which each abstract is
derived along with the original articles before making decisions based on a document
or abstract. All responsibility for action based on any information in this report rests
with the reader.
This report is not intended to be used as personal health advice. People seeking
individual medical advice should contact their physician or health professional.
The views expressed in this report are those of HSAC and do not necessarily represent
those of the University of Canterbury New Zealand, Health Technology Analysts Pty
Ltd, Australia or the Ministry of Health.

ii
Screening in ASNHL for acoustic neuroma
Contact Details
Health Services Assessment Collaboration (HSAC)
Health Sciences Centre
University of Canterbury
Private Bag 4800
Christchurch 8140
New Zealand
Tel: +64 3 345 8147 Fax: +64 3 345 8191
Email: [email protected]
Web Site: www.healthsac.net

iii
Screening in ASNHL for acoustic neuroma
Executive Summary
Introduction
This report provides a brief scan of the literature available on the role of magnetic
resonance imaging (MRI) and comparative surveillance techniques in screening for
the early detection of acoustic neuroma (AN) in patients with asymmetric
sensorineural hearing loss (ASNHL). It was commissioned by the New Zealand
Ministry of Health.
Methods
A systematic method of literature searching and study selection was employed in the
preparation of this report. The literature was searched using the bibliographic
databases of EMBASE and Medline. The Cochrane Database of Systematic Reviews
and numerous health technology assessment websites were also searched to help
identify existing reviews or clinical practice guidelines. In addition, the bibliographies
of key included papers were examined for relevant studies. It is important to note that
as this was a brief scan of the evidence, and not a full systematic review, detailed
quality appraisal, data extraction and interpretation of the identified literature was not
performed. The review relies heavily upon material reported in each publication’s
abstract.
Key results
The search strategy identified a total of 451 citations, of which 289 were included for
title/abstract review. After consideration of titles and abstracts using the study
selection criteria, 53 citations were included in the review. Only the papers of the
citations considered most relevant to the topic of interest were retrieved for more in-
depth description. There was also one systematic review identified which is due for
publication in April 2009. All available details of this review are provided.
The literature gathered in this report suggests that MRI is considered the ‘gold
standard’ in detecting ANs in patients with ASNHL. Although auditory brainstem
response (ABR) testing is also widely used, it has been shown to have insufficient
sensitivity and specificity to be used as a sole screening test. There is particular
concern around its ability to identify small sized tumours. Nonetheless, there appears
to be significant variety in the way clinicians screen and manage patients presenting
with ASNHL. This may be due to the fact that there are no universally accepted
clinical practice guidelines, and because of the accessibility and cost issues of
screening all patients with MRI. Whether or not MRI maintains its superiority once
costs are taken into account has not been addressed in this report.
Conclusions
The review concludes with suggested directions of action and potential research
questions for this topic.
iv
Screening in ASNHL for acoustic neuroma
Table of Contents
Review Team ................................................................................................................. i
Copyright Statement & Disclaimer ............................................................................. i
Contact Details ............................................................................................................. ii
Executive Summary .................................................................................................... iii
Introduction ............................................................................................................... iii
Methods ..................................................................................................................... iii
Key results ................................................................................................................. iii
Conclusions ............................................................................................................... iii
Table of Contents ........................................................................................................ iv
List of Tables ................................................................................................................ v
Introduction .................................................................................................................. 1
Literature Search ......................................................................................................... 3
Results ........................................................................................................................... 7
Review of screening techniques ................................................................................. 7
Systematic review ...................................................................................................... 7
Prospective studies ..................................................................................................... 8
Retrospective studies ................................................................................................ 10
Reviews, patient management or clinical practice papers ....................................... 14
Cost based studies .................................................................................................... 17
Key publications ....................................................................................................... 20
Published audiological screening protocols ............................................................. 24
Summary and Recommendations ............................................................................. 27
Conclusions .............................................................................................................. 27
References ................................................................................................................... 29
Appendix A: HTA websites searched ....................................................................... 35
Appendix B: Excluded studies annotated by reason for exclusion ....................... 37

v
Screening in ASNHL for acoustic neuroma
List of Tables
Table 1 Summary of the literature search .............................................................. 4 Table 2 Criteria for inclusion/exclusion in review ................................................ 4 Table 3 Prospective studies identified through the literature search ..................... 9 Table 4 Summary of retrospective cohort studies ............................................... 11
Table 5 Summary of publications classified as a review, patient management or
clinical practice paper ............................................................................. 14 Table 6 Summary of cost based studies ............................................................... 17 Table 7 Results of MRI and ABR screening tests ............................................... 22 Table 8 A description of published decision-support protocols for acoustic
neuroma .................................................................................................. 25

1
Screening in ASNHL for acoustic neuroma
Introduction
Hearing loss is the most prevalent sensory deficit reported by patients. In Australia,
10–20% of Australians have some hearing impairment and approximately 50% of
those over 65 years of age are hearing impaired. Hearing loss can be conductive,
sensorineural or mixed, with sensorineural occurring most frequently in adults
(Angeli et al. 2005). Sensorineural hearing loss indicates defects in either the cochlea
or in the neural transmission to the central nervous system. Asymmetric sensorineural
hearing loss (ASNHL) is defined as binaural difference in conduction thresholds of
>10 dB at two consecutive frequencies or >15 dB at one frequency (0.25–8.0 kHz)
(Sabini and Sclafani 2000).
One pathology which may present as ASNHL is acoustic neuroma (AN), also known
as vestibular schwannoma. Acoustic neuroma is a benign tumour arising from the
Schwann cells in the vestibular portion of the eighth cranial nerve. However, the
majority of patients who present with ASNHL do not have AN, the reported incidence
being approximately 2% of all patients with ASNHL (Urben et al. 1999). As a result,
selecting patients with ASNHL for further investigation continues to pose challenges,
given the disparity between the number of symptomatic patients, and the low
incidence of AN as the underlying cause (Nouraei et al. 2007).
When patients present with symptoms that may indicate an AN, magnetic resonance
imaging (MRI) is often considered the diagnostic test of choice. However, there are
some patients for whom MRI is inappropriate (e.g. patients with implanted electrical
devices or a cerebral aneurysm clip), and increasingly there are cost and accessibility
issues associated with MRI (Prasad and Cousins 2008). Contention also surrounds the
most efficient MRI protocol to use in the investigation of suspected AN.
Electrophysiological measurement of the auditory brainstem response (ABR) is
another diagnostic technique which has been used to diagnose AN (National Institute
of Health Research 2007). This report will gather the evidence on MRI, and the place
of any other screening tests, in the early detection of AN.
An extensive literature search was conducted as is described below. The aim of the
literature search was to provide a rapid overview of the available evidence for
screening ASNHL patients for AN, with a particular focus on MRI.
The results of each identified study should be considered with the year of publication
in mind, as significant advances in technology have occurred in AN diagnosis over
the last 20 years.

2
Screening in ASNHL for acoustic neuroma

3
Screening in ASNHL for acoustic neuroma
Literature Search
A search of the EMBASE, Medline and Cochrane database as well as numerous HTA
websites (Appendix A) was conducted to identify any published guidelines,
systematic reviews or publications pertaining to the screening of patients with
ASNHL for the identification of acoustic neuromas. The literature source, search
terms, number of citations identified and date of the search is outlined in Table 1.
Many of the citations identified through the search of the Cochrane library and HTA
websites were duplicates already identified through the EMBASE/Medline search, or
were completely irrelevant to the topic of interest, and were therefore excluded before
downloading into the Reference Manager database.

4
Screening in ASNHL for acoustic neuroma
Table 1 Summary of the literature search
Source Search terms Citations Date
EMBASE.com (Includes EMBASE and Medline)
(('acoustic neuroma'/exp OR 'acoustic neuroma') OR 'vestibular schwannoma' OR ('neurinoma'/exp OR 'neurinoma')) AND ('asymmetric sensorineural hearing loss' OR 'asymmetric sensori-neural hearing loss' OR ('sensorineural hearing loss'/exp OR 'sensorineural hearing loss') OR 'sensori-neural hearing loss' OR 'asymmetrical sensorineural hearing loss' OR 'asymmetrical sensori-neural hearing loss' OR ('perception deafness'/exp OR 'perception deafness')) AND [english]/lim AND [humans]/lim
281 03/02/2009
Cochrane library ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
86 03/02/2009
CADTH ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
49 03/02/2009
EuroScan
‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
20 03/02/2009
National guideline clearinghouse
‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
7 03/02/2009
National Institute for Health Research
‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
6 03/02/2009
NICE ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
2 03/02/2009
INAHTA ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
0 03/02/2009
MSAC ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
0 03/02/2009
ANZHSN ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
0 03/02/2009
AHRQ ‘Sensorineural hearing loss’ OR ‘vestibular schwannoma’ OR ‘acoustic neuroma’
0 03/02/2009
Total 451 03/02/2009
Abbreviations: AHRQ, Agency for Healthcare Research and Quality; ANZHSN, Australia and New Zealand Horizon Scanning
Network; CADTH, Canadian Agency for Drugs and Technology in Health; INAHTA, International Network of Agencies for
Health Technology Assessment; MSAC, medical Services Advisory Committee; NICE, National Institute for Clinical Excellence.
In addition, a general internet search was performed to identify any additional
publications, clinical practice guidelines or systematic reviews. There were 289
citations downloaded into the reference manager database from the various sources
described above. The titles and abstracts (where available) were reviewed using the
inclusion and exclusion criteria outlined below in Table 2.
Table 2 Criteria for inclusion/exclusion in review
Reason for exclusion Number of citations excluded
Incorrect study type: case study (<10 patients), opinion piece, letter 69
Incorrect patient population: not ASNHL 68
Incorrect disease: not acoustic neuroma 27
Incorrect intervention/outcomes: does not examine relevant screening technique for acoustic neuroma
72
Included 53
Abbreviations: ASNHL, Asymmetric sensorineural hearing loss.

5
Screening in ASNHL for acoustic neuroma
After reviewing the citations, there were 53 that qualified for inclusion. One of these
was a systematic review which is due for publication in April 2009. Further details on
the types of publications retrieved and an in-depth description of the forthcoming
systematic review is provided below. The excluded citations and reasons for exclusion
are provided in Appendix B.

6
Screening in ASNHL for acoustic neuroma
7
Screening in ASNHL for acoustic neuroma
Results
Review of screening techniques
The identified studies assessed a number of different surveillance techniques. These
are discussed below.
The initial screening test for assessing patients with ASNHL was the pure tone
audiogram (PTA) (Wareing 2002). Whilst there is no characteristic shape of
audiogram, unexplained asymmetry between the ears warrants further investigation.
In the past, other audiological screening tests such as loudness recruitment, tone
decay, stapedial reflex thresholds and decay have been used as an initial screening
measure although these are now only of historical interest.
Auditory brainstem response testing was first introduced in 1970 and has been used to
identify retrocochlear lesions. It is a safe and painless test of the auditory pathway and
brainstem function in response to auditory stimuli. The ABR test is widely used by
audiologists as an initial screening tool in patients with sensorineural hearing loss.
However, its success rate in ASNHL has been shown to be dependent on tumour size,
with the test at its least sensitive in small and medially placed tumours, these being
the tumours that an early diagnostic strategy aims to detect (Wareing 2002).
Magnetic resonance imaging with gadolinium enhancement has been considered the
‘gold standard’ for detection of ANs since 1991. It has been shown to have a near
100% diagnostic accuracy, being able to detect tumours as small as 3mm. More
recently, screening scan procedures have been developed that either decrease the
gadolinium dose or remove the need for it all together, using T2 fast spin echo (FSE)
scanning protocols. However, some authors argue that using this approach is probably
not justified since other alternative diagnoses may be missed due to the lack of
contrast material. Nevertheless, high-resolution FSE T2-weighted MRI has proven to
be a cost-saving alternative to contrast-enhanced MRI (Vossough 2003). The
disadvantages of MRI relate to the cost of universal screening as well as access to the
scanner.
The use of contrast enhanced computerised tomography (CT) has also been reported
as useful in the diagnosis of AN. However, because bone has a positive signal, its
ability to diagnose intracanalicular tumours is limited and possibly no better than
ABR testing. Its role is currently limited to those patients in whom MRI is
contraindicated (Wareing 2002).
Systematic review
There was one systematic review identified through the literature search. It is
currently being undertaken by the National Institute of Health Research (NIHR) and is
due for publication in April 2009. According to the NIHR webpage, the project is in
the editorial review stage. The title of the systematic review is:
‘The role of magnetic resonance imaging in the identification of suspected acoustic
neuroma: systematic review of clinical and cost effectiveness, and natural history’

8
Screening in ASNHL for acoustic neuroma
The following summary of the project and proposed publication abstract are taken
from the NIHR webpage.
Summary
Some patients presenting to their general practitioner with unilateral hearing loss and/or tinnitus may have a small tumour called an acoustic neuroma growing on the hearing (acoustic) nerve; estimated to be 3-7.5%. How these tumours grow and the effect they have on an individual varies. Identification of such tumours and assessment of their rate of growth is important clinical information which contributes to decisions on whether or how to treat them.
There exist several different tests that can be used for this assessment, each of which has different accuracy and different costs. There are no current guidelines on which is the most clinically- and cost-effective to use.
We propose to identify existing published and unpublished literature and to extract all the relevant evidence which will contribute to answering questions on how acoustic neuromas grow and affect individuals, which diagnostic tests are better and what are the costs involved. Only by evaluating the existing evidence can we see if there are gaps in our knowledge which need to be answered by further research. The proposed research will not raise ethical issues and will not require NHS ethical approval.
The base for the research will be the University of Nottingham. Co-applicants are based in Birmingham, Liverpool, Cambridge, Belfast, and Athens. Our team comprises experts in various aspects of this field, including methodological experts who will reach a consensus based on the evidence. Each will review aspects of the evidence for which they have expert knowledge and each will contribute to the final report. The costs requested are to employ a research assistant to carry out the searches and identify the available evidence. In addition we are requesting funds for consultancy for the expert reviewers and co-ordinators to allow them to dedicate sufficient time to the project, travel costs for meetings of the whole team and for consultancy meetings between the researcher and the experts, and consumable costs of acquiring the literature that is not available on the internet.
Abstract
The aim of the study is to (i) evaluate the clinical- and cost-effectiveness of a range of diagnostic strategies for investigating patients with unilateral hearing loss and/or sudden-onset tinnitus with a view to confirming or eliminating a diagnosis of acoustic neuroma, (ii) to describe the natural history of acoustic neuroma and (iii) to synthesise the findings from these two elements of the study to formulate guidelines for clinical practice and to identify priorities for future primary research in this area.
We propose to identify existing published and unpublished literature and to extract all the relevant evidence which will contribute to answering the questions of how do acoustic neuromas grow and affect individuals, the diagnostic accuracy and performance (e.g. yield) of different tests and combinations of tests that investigate unilateral hearing loss/tinnitus (i.e. magnetic resonance imaging, hearing tests, computed tomography scans, auditory brainstem response testing) including the outcomes of interventions and the cost-effectiveness of MRI compared with other diagnostic tests for the investigation of unilateral hearing loss and/or tinnitus. These questions will be examined in terms of different case definitions, tumour size and different protocols of tests. Each review will be conducted in accord with contemporary methodological standards for systematic reviews (e.g. Cochrane diagnostic screening Methods Group, NHS Centre for Reviews & Dissemination systematic review guidelines).
Data source: National Institute of Health Research 2009
Abbreviations: MRI, magnetic resonance imaging; NHS, National Health Service
Prospective studies
There were eight prospective studies assessing a number of different surveillance
techniques identified through the literature search. The citation details for these, along
with a summary of each publication are provided in Table 3. Where possible,
publications are further grouped by screening intervention type.

9
Screening in ASNHL for acoustic neuroma
Table 3 Prospective studies identified through the
literature search
Reference Abstract / Summary
ABR
Cueva RA. (2004) Auditory brainstem response versus magnetic resonance imaging for the evaluation of asymmetric sensorineural hearing loss. Laryngoscope 114:1686-1692.
ABR vs MRI
ABR testing and MRI are compared for the evaluation of patients with ASNHL. This study is a prospective, nonrandomised comparison of ABR and MRI for the evaluation of patients with asymmetric SNHL. Further details are provided under the Key Publications section.
Ruckenstein MJ, Cueva RA, Morrison DH, and Press G. (1996) A prospective study of ABR and MRI in the screening for vestibular schwannomas. American Journal of Otology 17:317-320.
ABR vs ABR + MRI
This study reports on the preliminary results of an ongoing prospective study on the evaluation of patients with ASNHL. All patients with asymmetry in two or more pure-tone thresholds of (greater-than or equal to)15 dB or asymmetry in speech discrimination scores of (greater-than or equal to)15% or both entered the study and underwent both an ABR examination and an enhanced MRI scan. Further details are provided under the Key Publications section.
Swan IRC. (1989) Diagnostic vetting of individuals with asymmetric sensorineural hearing impairments. Journal of Laryngology and Otology 103:823-826.
ABR, acoustic reflex, alternative binaural loudness balance, ENG and caloric testing + CT
This study aimed to assess the efficiency of various tests in excluding CPA tumours with the minimum of unnecessary investigations. All patients received the full battery of ABR, acoustic reflex thresholds and decay, alternate binaural loudness balance and ENG and caloric testing. All patients who did not have normal ABR proceeded to high resolution CT scanning. The efficiency of these tests in a general ORL clinic is very much poorer than often suggested, due largely to the number of occasions on which the tests cannot be done, and to the very small proportion of the test population who have CPA tumours.
MRI
Annesley-Williams DJ, Laitt RD, Jenkins JPR, Ramsden RT, and Gillespie JE. (2001) Magnetic resonance imaging in the investigation of sensorineural hearing loss: Is contrast enhancement still necessary? Journal of Laryngology and Otology 115:14-21.
FSE-T2W MRI vs Gd-T1W MRI
Over a 22-month period the use of axial turbo-spin echo T2-weighted images (T2w) were prospectively compared with contrast-enhanced T1-weighted spin echo scans in the evaluation of 513 patients presenting with audiovestibular symptoms. With the 3-D sequence three ANs were all identified correctly with no false positive and only one false negative result. Authors concluded that mass lesions of the IAM/CPA can be reliably identified on T2w TSE imaging but labyrinthine lesions may be missed without contrast enhancement.
Zealley IA, Cooper RC, Clifford KM, Campbell RS, Potterton AJ, Zammit-Maempal I, Baudouin CJ, and Coulthard AJ. (2000) MRI screening for acoustic neuroma: a comparison of fast spin echo and contrast enhanced imaging in 1233 patients. The British Journal of Radiology 73:247.
Gd-T1W MRI vs FSE-T2W MRI
In order to determine the utility of fast spin echo imaging, both gadolinium enhanced T1 weighted images and fast spin echo T2 weighted images were acquired in 1233 consecutive patients referred for exclusion of AN. Thirty three ANs were identified. Only 56% were confidently identified on fast spin echo T2 weighted images alone; gadolinium enhanced T1 weighted images were required to confirm the diagnosis in 44% of the cases, including 9 of the 10 intracanalicular tumours. It was concluded that an imaging strategy intended to identify small intracanalicular ANs cannot rely on fast spin echo T2 weighted imaging alone.

10
Screening in ASNHL for acoustic neuroma
Table 3 Prospective studies identified through the
literature search (continued)
Reference Abstract / Summary
Adler J, Atlas M and Shnier R. (1998) High resolution MRI and asymmetric sensori-neural hearing loss. Australian Journal of Oto-Laryngology. FindArticles.com. 09 Feb, 2009.
FSE-MRI vs Gd-T1W MRI
The present study examined the suitability of a high resolution fast spin echo (FSE) sequence, combined with a whole head FSE sequence, in the screening evaluation of 39 consecutive patient's referred with a diagnosis of ASNHL. The efficacy of the sequences was compared with standard MRI which included T1 weighted gadolinium enhanced scans. Whilst there were no significant differences in the imaging diagnoses achieved with the FSE sequences when compared to standard protocols, the incidence of acoustic tumour in this unselected series (4%) was too low to allow a definitive judgement with respect to the value of the FSE sequences as a stand-alone screening tool.
Soulie D, Cordoliani YS, Vignaud J, and Cosnard G. (1997) MR imaging of acoustic neuroma with high resolution fast spin echo T2-weighted sequence. European Journal of Radiology 24:61-65.
FSE-T2W MRI vs Gd-T1W MRI
The aim of this study was to assess the value of high resolution 2D fast spin echo T2-weighted sequence (HR 2D-FSE T2W) for evaluating the internal auditory meatus in patients with asymmetric or unilateral sensorineural hearing loss, vs. gadolinium-enhanced T1-weighted (T1w) sequence; to suggest a screening protocol to exclude the diagnosis of AN in a patient with isolated unilateral sensorineural hearing loss. Normal images using HR 2D-FSE T2w sequence can rule out the diagnosis of AN. Using this protocol authors could exclude the diagnosis of AN in case of normal HR 2D-FSE images and no additional gadolinium-enhanced T1w sequence is necessary.
Bassi P, Piazza P, Cusmano F, Menozzi R, Gandolfi A, and Zini C. (1989) MR cisternography of the cerebello-pontine angle and internal auditory canal in diagnosis of intracanalicular acoustic neuroma. Neuroradiology 31:486-491.
T1W + T2W MRI
115 patients, suffering from SNHL were tested with a 1.5 T superconducting magnet. The authors describe utility of both T1-weighted multiple slice and T2-weighted multiple echo images for the evaluation of cerebello-pontine angle, internal auditory canal and their neurovascular content. In 73 cases MR cisternography was normal. The remaining 42 cases were subdivided into twenty extracanalicular masses, eleven small intra-extracanalicular and nine purely intracanalicular lesions. All the lesions were histologically proven ANs, except one intracanalicular mass which was a meningioma. Examination was inconclusive only in two cases and decision was then made to follow the clinical course. Advantages of MR cisternography over CT and air CT cisternography are pointed out.
Abbreviations: ABR, audio brainstem response; ASNHL, asymmetric sensorineural hearing loss; CPA, cerebellopontine angle
CT; computed tomography; ENG, electronystagmogram; FSE, fast spin echo; IAM, internal auditory meatus; MRI, magnetic resonance imaging; ORL, ;T2W, T-2 weighted; TSE, turbo spin echo.
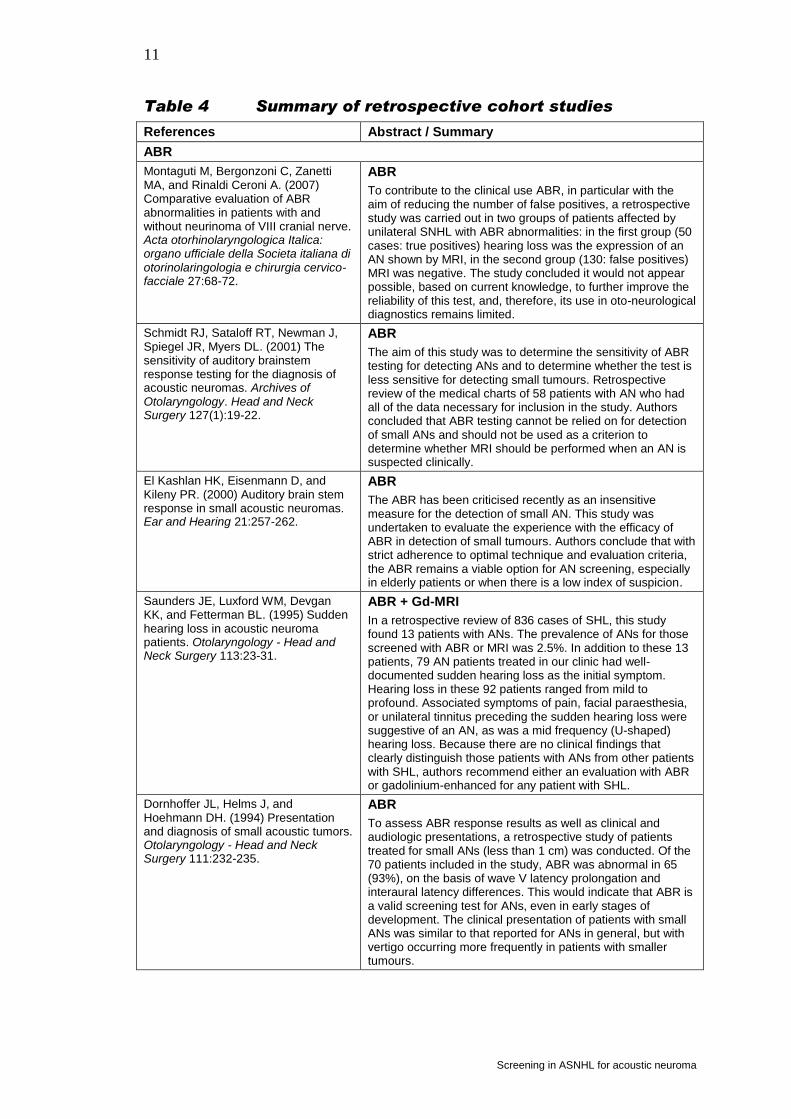
Retrospective studies
There were 17 studies which retrospectively assessed various surveillance techniques
for AN. The citation details and a summary for each are shown below in Table 4.
Again, publications have been grouped according to the screening intervention.
11
Screening in ASNHL for acoustic neuroma
Table 4 Summary of retrospective cohort studies
References Abstract / Summary
ABR
Montaguti M, Bergonzoni C, Zanetti MA, and Rinaldi Ceroni A. (2007) Comparative evaluation of ABR abnormalities in patients with and without neurinoma of VIII cranial nerve. Acta otorhinolaryngologica Italica: organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale 27:68-72.
ABR
To contribute to the clinical use ABR, in particular with the aim of reducing the number of false positives, a retrospective study was carried out in two groups of patients affected by unilateral SNHL with ABR abnormalities: in the first group (50 cases: true positives) hearing loss was the expression of an AN shown by MRI, in the second group (130: false positives) MRI was negative. The study concluded it would not appear possible, based on current knowledge, to further improve the reliability of this test, and, therefore, its use in oto-neurological diagnostics remains limited.
Schmidt RJ, Sataloff RT, Newman J, Spiegel JR, Myers DL. (2001) The sensitivity of auditory brainstem response testing for the diagnosis of acoustic neuromas. Archives of Otolaryngology. Head and Neck Surgery 127(1):19-22.
ABR
The aim of this study was to determine the sensitivity of ABR testing for detecting ANs and to determine whether the test is less sensitive for detecting small tumours. Retrospective review of the medical charts of 58 patients with AN who had all of the data necessary for inclusion in the study. Authors concluded that ABR testing cannot be relied on for detection of small ANs and should not be used as a criterion to determine whether MRI should be performed when an AN is suspected clinically.
El Kashlan HK, Eisenmann D, and Kileny PR. (2000) Auditory brain stem response in small acoustic neuromas. Ear and Hearing 21:257-262.
ABR
The ABR has been criticised recently as an insensitive measure for the detection of small AN. This study was undertaken to evaluate the experience with the efficacy of ABR in detection of small tumours. Authors conclude that with strict adherence to optimal technique and evaluation criteria, the ABR remains a viable option for AN screening, especially in elderly patients or when there is a low index of suspicion.
Saunders JE, Luxford WM, Devgan KK, and Fetterman BL. (1995) Sudden hearing loss in acoustic neuroma patients. Otolaryngology - Head and Neck Surgery 113:23-31.
ABR + Gd-MRI
In a retrospective review of 836 cases of SHL, this study found 13 patients with ANs. The prevalence of ANs for those screened with ABR or MRI was 2.5%. In addition to these 13 patients, 79 AN patients treated in our clinic had well-documented sudden hearing loss as the initial symptom. Hearing loss in these 92 patients ranged from mild to profound. Associated symptoms of pain, facial paraesthesia, or unilateral tinnitus preceding the sudden hearing loss were suggestive of an AN, as was a mid frequency (U-shaped) hearing loss. Because there are no clinical findings that clearly distinguish those patients with ANs from other patients with SHL, authors recommend either an evaluation with ABR or gadolinium-enhanced for any patient with SHL.
Dornhoffer JL, Helms J, and Hoehmann DH. (1994) Presentation and diagnosis of small acoustic tumors. Otolaryngology - Head and Neck Surgery 111:232-235.
ABR
To assess ABR response results as well as clinical and audiologic presentations, a retrospective study of patients treated for small ANs (less than 1 cm) was conducted. Of the 70 patients included in the study, ABR was abnormal in 65 (93%), on the basis of wave V latency prolongation and interaural latency differences. This would indicate that ABR is a valid screening test for ANs, even in early stages of development. The clinical presentation of patients with small ANs was similar to that reported for ANs in general, but with vertigo occurring more frequently in patients with smaller tumours.

12
Screening in ASNHL for acoustic neuroma
Table 4 Summary of retrospective cohort studies
(continued)
References Abstract / Summary
Hashimoto S, Kawase T, Furukawa K, and Takasaka T. (1991) Strategy for the diagnosis of small acoustic neuromas. Acta Oto-Laryngologica, Supplement 481:567-569.
ABR vs CT
ABR has been believed as the most reliable test for the diagnosis of AN despite several reports of false-negatives. In this series, 4 tumours out of 18 tested had normal ABR. The false-negative rate was 22%, which is much higher than expected. In CT, only 11 tumours were recognised. Although the total number is not large, present results clearly suggest the limits of these examinations. At present, HR-MRI is the most reliable diagnostic method for ANs with no false-negative reported; ordinary MRI may have false-negatives.
Telian SA, Kileny PR, Niparko JK, Kemink JL, and Graham MD. (1989) Normal auditory brainstem response in patients with acoustic neuroma. Laryngoscope 99:10-14.
ABR
ABR testing has been a major breakthrough in audiologic screening for AN because of its high degree of sensitivity. Although it is not uncommon for other cerebellopontine angle masses to present with normal ABR findings, reports of eighth nerve tumours with false-negative ABR tests are quite rare. A series of 120 ANs re-sected at the University of Michigan was reviewed and revealed two such patients. These two patients presented with ASNHL and unilateral tinnitus and were found to have completely normal ABR. The diagnosis of AN would have been delayed if a comprehensive evaluation had not been pursued.
Kanzaki J. (1986) Present state of early neurotological diagnosis of acoustic neuroma. ORL 48:193-198.
SR and ABR test
The incidence of cases of AN that are manifested as sudden deafness or progressive sensorineural hearing loss was investigated. The findings of the SR test, the ABR test and the caloric test were analysed, and the procedure for the diagnosis of AN was discussed.
MRI
Mahrous AK and Kalepu R. (2008) Positive findings on MRI in patients with asymmetrical SNHL. European Archives of Oto-Rhino-Laryngology 265:1471-1475.
MRI
This is a retrospective study of 100 consecutive patients who attended an ENT outpatient clinic in a 6 month-period. All of them presented with ASNHL. They were all investigated with MRI scan of the IAM and CPA. The pickup rate was 1% for CPA lesion which was vestibular schwannoma. Further details are provided under the Key Publications section.
Nouraei SAR, Huys QJM, Chatrath P, Powles J, and Harcourt JP. (2007) Screening patients with sensorineural hearing loss for vestibular schwannoma using a Bayesian classifier. Clinical Otolaryngology 32:248-254.
MRI
This study developed and validated a diagnostic model using a generalisation of neural networks, for detecting vestibular schwannomas from clinical and audiological data, and compared its performance with six previously published clinical and audiological decision-support screening protocols. The Gaussian Process Ordinal Regression Classifier increased the flexibility and specificity of the screening process for vestibular schwannoma when applied to a sample of matched patients with and without this condition. If applied prospectively, it could reduce the number of 'normal' magnetic resonance scans by as much as 30% without reducing detection sensitivity. Further details are provided under the Key Publications section.

13
Screening in ASNHL for acoustic neuroma
Table 4 Summary of retrospective cohort studies
(continued)
References Abstract / Summary
Baker R, Stevens-King A, Bhat N, and Leong P. (2003) Should patients with asymmetrical noise-induced hearing loss be screened for vestibular schwannomas? Clinical Otolaryngology and Allied Sciences 28:346-351.
MRI
Those patients with ASNHL are routinely screened for vestibular schwannomas by MRI scanning. Scan reports from the past 5 years have been reviewed and out of 152 scans, four revealed vestibular schwannomas giving a pick-up rate of 2.5%, which compares favourably with other published pick-up rates. Review of the audiograms in these cases suggests that they can be misleading in this context. The conclusion is that patients with noise-induced ASNHL should be screened for ANs.
Kubo T, Sakashita T, Kusuki M, Kyunai K, Ueno K, Hikawa C, Wada T, and Nakai Y. (2000) Evaluation of radiological examination for sensorineural hearing loss. Acta Oto-Laryngologica, Supplement -:34-38.
X-ray, CT and MRI
In this study, the clinical significance of radiological examinations for SNHL was evaluated and the value of their utilisation was reconsidered. A total of 1,276 ears of 724 patients who demonstrated unilateral or bilateral SNHL was studied retrospectively. Findings of radiological examinations such as plain X-ray (X-p), CT and MRI of the brain or the temporal bone were investigated. Temporal bone X-p was usually performed to rule out acoustic tumours. CT was further performed in 119 patients (16.4%) and MRI in 84 patients (11.6%) in total. Of five cases with AN, two with a small tumour exhibited normal findings for the internal auditory canal on temporal bone X-p. These small tumours were finally confirmed by MRI. These findings confirmed that MRI is very useful for detecting small acoustic tumours and suggested that MRI also reveals cerebral vascular insufficiency in patients with SNHL.
Manfre L, Angileri T, Ferrara S, Accardi M, Raineri R, and Lagalla R. (1997) The role of magnetic resonance imaging in central hearing deficits: Beyond the acoustic schwannoma. Rivista di Neuroradiologia 10:409-416.
MRI
This study retrospectively examined 72 patients complaining of different clinical syndromes and SNHL or different kinds of acoustic impairment who underwent MRI brain study excluding the presence of acoustic schwannoma and other CPA masses. In conclusion, although AN was the most common cause of acquired hearing deficit, a lesion involving the neural centres of the acoustic pathway can also determine SNHL. Considering the high sensitivity of MRI in the detection of acoustic intra-axial pathway lesions, an in-depth MRI examination of the brain stem and the temporal lobe is mandatory when SNHL occur in patients not affected by acoustic schwannoma.
Levy RA and Arts HA. (1996) Predicting neuroradiologic outcome in patients referred for audiovestibular dysfunction. American Journal of Neuroradiology 17:1717-1724.
Audiovestibular testing and MRI
This study retrospectively reviewed the neuroimaging studies, results of audiometric and vestibular testing, and medical records of 118 patients to rule out AN. Patients' presentation and results of audiometric and vestibular testing were associated with either a positive or negative neuroimaging outcome. Clinical presentation and audiovestibular testing could not sensitively predict the outcome of neuroimaging in our cohort of patients referred for audiovestibular dysfunction.
Stack JP, Ramsden RT, Antoun NM, Lye RH, Isherwood I, and Jenkins JP. (1988) Magnetic resonance imaging of acoustic neuromas: the role of gadolinium-DTPA. The British Journal of Radiology 61:800-805.
Gd-MRI
MRI was performed in 20 patients with evidence on CT of 21 ANs before and after intravenous administration of gadolinium-diethylene-triamine-pentaacetic acid (Gd-DTPA). The authors concluded that MRI with gadolinium-DTPA is a relatively quick, safe, well tolerated and effective method for the diagnosis of AN.

14
Screening in ASNHL for acoustic neuroma
Table 4 Summary of retrospective cohort studies
(continued)
References Abstract / Summary
Curati WL, Graif M, Kingsley D, King T, Scholtz C, and Steiner R. (1986) MRI in acoustic neuroma: a review of 35 patients. Neuroradiology 28:208-214.
MRI vs CT
This retrospective study is aimed to assess the diagnostic efficacy of MRI in relation to contrast enhanced CT and air-CT-cisternography. The results suggested that MRI was the best non invasive technique for demonstrating ANs.
Chaimoff M, Nageris BI, Sulkes J, Spitzer T, and Kalmanowitz M. (1999) Sudden hearing loss as a presenting symptom of acoustic neuroma. American Journal of Otolaryngology - Head and Neck Medicine and Surgery 20:157-160.
DISC test, ABR, acoustic reflex
This paper describes the incidence of AN presenting as sudden hearing loss (SHL) and the effectiveness of the discrimination (DISC) test, the brainstem-evoked response, and acoustic reflex (AR) test in predicting AN in patients with SHL. The DISC test is a useful screening tool for acoustic tumour, whereas the brainstem-evoked response test shows poorer results in affected patients with sensorineural hearing loss than in other subgroups with different signs of AN. Authors recommend that young patients presenting with mild SHL who have normal results on the AR and brainstem-evoked response tests undergo MRI to rule out CPA tumour.
Abbreviations: ABR, audio brainstem response; AN, acoustic neuroma; ASNHL, asymmetric sensorineural hearing loss; CPA,
cerebellopontine angle CT; computed tomography; DISC, discrimination; ENT, ear nose throat; IAM, internal auditory meatus; MRI, magnetic resonance imaging; SNHL, sensorineural hearing loss; SHL, sudden hearing loss; SR, stapedius reflex; X-p, X-
ray.
Reviews, patient management or clinical practice papers
Of the 53 included citations, 15 were grouped under review, patient management, or
clinical practice associated with the diagnosis of AN. The reference for the
publication and a brief summary of the study is provided below in Table 5. Where
possible, similar publications have been grouped together.
Table 5 Summary of publications classified as a review,
patient management or clinical practice paper
Reference Abstract/Summary
Monsell EM and Rock JP. (1990) Sensorineural hearing loss and the diagnosis of acoustic neuroma. Henry Ford Hospital Medical Journal 38:9-12.
AN management (R)
ANs can now be detected when they are small, and early microsurgical removal results in the lowest overall morbidity. These authors examine the historical development of AN management; discuss current diagnosis and treatment, and present illustrative cases from recent experience. Complaints of tinnitus and hearing loss, especially when unilateral, require appropriate medical evaluation.
Morley S and Beale TJ. (2007) Imaging of deafness and tinnitus. Imaging 19:55-70.
Imaging acoustic neuroma (R)
This paper reviews the clinical features of hearing loss which suggest that imaging is warranted. The imaging features of the main causes of sensorineural deafness are reviewed, with particular focus on imaging vestibular schwannoma. The pathologies that result in tinnitus overlap with those causing sensorineural deafness. This article pays particular attention to the imaging of tinnitus caused by glomus tumours and vascular causes, such as aberrant vessels and arteriovenous malformations.

15
Screening in ASNHL for acoustic neuroma
Table 5 Summary of publications classified as a review,
patient management or clinical practice paper
(continued)
Reference Abstract/Summary
Swartz JD. (2004) Lesions of the cerebellopontine angle and internal auditory canal: diagnosis and differential diagnosis. Seminars in ultrasound, CT, and MR 25:332-352.
Diagnostic review (R)
There is a wide variety of differential diagnostic possibilities that must be considered when viewing images of patients with sensorineural hearing loss, vertigo, and dizziness. This communication was intended to provide the reader with an approach to this problem. Detailed anatomy of the region is also included in this communication.
Isaacson JE and Vora NM. (2003) Differential diagnosis and treatment of hearing loss. American Family Physician 68:1125-1132.
Causes and diagnostic review (R)
This paper reviews causes of hearing loss, diagnostic techniques and treatment. It includes both conductive and sensorineural hearing loss.
Vossough A. (2003) Imaging evaluation of sensorineural hearing loss. Applied Radiology 32:6-14.
Diagnosis and management (PM)
This article reviews the diagnosis and management of hearing loss with a particular focus on imaging findings in patients with SNHL.
Spoelhof GD. (1995) When to suspect an acoustic neuroma. American Family Physician 52:1768-1774.
Diagnosis and treatment (PM)
This publication reviews diagnosis and treatment for patients with suspected AN. Patients with ASNHL or unilateral tinnitus should be evaluated expeditiously to prevent further neurologic damage. Gadolinium- enhanced MRI is the best tool for making the diagnosis of AN. Surgical removal using a translabyrinthine approach is the favoured treatment, although radiation therapy and expectant management may be chosen for patients at high surgical risk.
Obholzer RJ and Harcourt JP. (2004) Magnetic resonance imaging for vestibular schwannoma: analysis of published protocols. The Journal of Laryngology and Otology. 118:329-332.
Protocol for MRI selection (CP)
This study seeks to define the most appropriate guidelines for selection of patients for MRI to exclude a vestibular schwannoma. All MRIs of the internal auditory meatus, performed during 2000, were reviewed. Further details are provided under the Key Publications section.
Sheppard IJ, Milford CA, and Anslow P. (1995) MRI in the detection of acoustic neuromas- a suggested protocol for screening. Clinical Otolaryngology & Allied Sciences 21:301-304.
Protocol for MRI selection (CP)
Authors suggest, based on a retrospective review of AN cases, that the entry protocol for MRI screening be limited to patients up to 70 years of age presenting with unilateral audiovestibular symptoms in the absence of significant neurological symptoms or signs, with an average difference in hearing threshold of 15 dB between normal and symptomatic ears or unilateral tinnitus with normal hearing. Further details are provided under the Key Publications section.
Thomsen J and Tos M. (1993) Management of acoustic neuromas. Annales d'Oto-Laryngologie et de Chirurgie Cervico-Faciale 110:179-191.
Protocol for screening (CP)
A survey of the management of ANs in the broadest sense is given. The paper recommends all patients with hearing better than 70-80 dB should be subjected to ABR audiometry, and if there is any doubt about the normality of the response, the patient should proceed to MRI. Patients with poor hearing should go directly to MRI. The advantages and disadvantages of the different surgical approaches are described and an electric treatment algorithm is outlined.
Kanzaki J, Ogawa K, Tsuchihashi N, Yamamoto M, Ogawa S, and Uchi T. (1991) Diagnostic procedure for acoustic neuroma. Acta Oto-Laryngologica, Supplement 487:114-119.
Protocol for screening (CP)
The authors' diagnostic procedure for unilateral AN and the reasoning behind it are explained. At present, pure tone audiometry and simple radiographic imaging of the internal auditory canal are first carried out. Then, if the hearing level (average hearing at 4 kHz and 8 kHz) is 70 dB or lower, ABR audiometry is carried out. If it is 71 dB or higher, the patient is examined by MRI or CT. Contrast-enhanced CT is carried out when MRI is not available.

16
Screening in ASNHL for acoustic neuroma
Table 5 Summary of publications classified as a review,
patient management or clinical practice paper
(continued)
Reference Abstract/Summary
Smith IM, Turnbull LW, Sellar RJ, Murray JAM, and Best JJK. (1990) A modified screening protocol for the diagnosis of acoustic neuromas. Clinical Otolaryngology and Allied Sciences 15:167-171.
Protocol for screening (CP)
This paper reviews current protocol for preliminary screening for AN. The current method is a combination of caloric tests, tomography of the internal auditory meati and ABR audiometry with 2 positive results indicating the need for further investigation. This protocol, although sensitive, lacks specificity and results in a high incidence of normal CT air meatograms. Authors’ devised a weighted system of scoring to avoid subjecting large numbers of normal patients to CT air meatography. The proposed system was derived from screening 61 patients with unilateral sensorineural hearing loss, 24 of whom had an AN. This method reduced the false positive rate of CT air meatography from 68%, using the 2 out of 3 criteria, to 18%, whilst the false negative incidence remained at 8%.
Wright A and Bradford R. (1995) Management of acoustic neuroma. British Medical Journal 311:1141-1144.
Early detection techniques (CP)
This article reviews the investigation of patients presenting with unilateral auditory symptoms including the diagnosis and treatment of abnormalities.
Wareing MJ, Baguley D, and Moffat DA. (2002) Investigations for vestibular schwannoma. CME Bulletin Otorhinolaryngology Head and Neck Surgery 6:12-15.
Early detection techniques (CP)
This review looks at the early detection of vestibular schwannoma. Treatment of smaller tumours results in better outcomes. Advances in imaging, in particular the refinement of MRI techniques, have been responsible for the detection of smaller tumours with near 100% sensitivity. The ABR, previously the mainstay of screening, has been superseded in this role. The optimal protocol for patients suspected of a having a vestibular schwannoma is an MRI scan.
Dawes PJD. (1999) Screening for vestibular schwannoma: Current practice in New Zealand. Australian Journal of Otolaryngology 3:307-310.
Survey of clinical practice (CP)
A clinical practice study surveying New Zealand otolaryngologists was conducted. Results indicated the preferred initial screening modality for diagnosing vestibular schwannoma is MRI. 57% proceed direct to MRI, 24% use ABR audiometry and/or CT to select for MRI, and 17% rely upon their clinical judgement supported by investigations such as speech audiometry, acoustic reflex thresholds and ABR audiometry before requesting further investigation. Further details are provided under the Key Publications section.
Kanzaki J, Ogawa K, Ogawa S, Yamamoto M, Ikeda S, and Uchi T. (1991) Audiological findings in acoustic neuroma. Acta Oto-Laryngologica, Supplement 487:125-132.
Audiological examination (CP)
This paper discusses audiological examinations in the diagnosis of AN. This paper proposes the most sensitive audiological examination is ABR audiometry. Its most useful parameter is the IT5. A U-shaped audiometric configuration suggests AN, since it is seen in 10% of patients with small tumours. Psychological audiometric tests can be excluded from the battery of screening tests since they have low rates of positive diagnosis. Nevertheless, the SR test can be employed as a screening device in cases in which the hearing level at 2 kHz and lower is 70 dB or lower, even if it is 71 dB or higher at 4 kHz and 8 kHz.
Abbreviations: ABR, audio brainstem response; AN, acoustic neuroma; ASNHL, asymmetric sensorineural hearing loss; (CP) =
clinical practice; CT, computed tomography; dB, decibel; KHZ, kilohertz; MRI, magnetic resonance imaging; (PM) = patient management; (R) = review; SNHL, sensorineural hearing loss; SR, stapedius reflex.

17
Screening in ASNHL for acoustic neuroma
Cost based studies
Retrieved citations that mentioned costing, cost containment or cost-effectiveness in
the diagnosis of AN were grouped together. These papers were identified through the
clinical literature search and are shown below in Table 6. These studies have been
further grouped by the type of screening intervention. The country that the study was
conducted in has also been shown in the reference column of the table.
Table 6 Summary of cost based studies
Reference Abstract / Summary
ABR and MRI
Rupa V, Job A, George M, and Rajshekhar V. (2003) Cost-effective initial screening for vestibular schwannoma: auditory brainstem response or magnetic resonance imaging? Otolaryngology--head and neck surgery: official journal of American Academy of Otolaryngology-Head and Neck Surgery 128:823-828.
Country of study: United States of America
ABR + Gd-MRI
This study aimed to determine the cost-effectiveness of including ABR testing in a screening protocol for the diagnosis of vestibular schwannoma. Patients were investigated prospectively with both ABR and gadolinum-enhanced MRI (GdMRI). A protocol involving screening of all patients with asymmetric audiovestibular symptoms using ABR and only subjecting those patients with no responses or retrocochlear pathology to GdMRI would effect a savings of $1200 for every patient detected to have a VS. Further details are provided under the Key Publications section.
Cheng G, Smith R and Tan AK. (2003) Cost comparison of auditory brainstem response versus magnetic resonance imaging of acoustic neuroma. J Otolaryngol 32(6):394-399.
Country of study: United States of America
ABR + MRI/CT
The cost-effectiveness of current diagnostic approaches employed in patients with suspected AN was evaluated. Currently, patients with signs and symptoms suggestive of AN, such as sudden unilateral hearing loss and/or tinnitus, undergo ABR screening tests to rule out this condition. If the ABR is normal, AN can be ruled out. However, if the ABR is abnormal, MRI or CT is necessary to confirm the diagnosis. The total costs of this approach were compared with the estimated costs of straight MRI screening performed on the same patient population.
Robinette MS, Bauch CD, Olsen WO, and Cevette MJ. (2000) Auditory brainstem response and magnetic resonance imaging for acoustic neuromas: costs by prevalence (Brief record). Archives of Otolaryngology. Head and Neck Surgery 126:963-966.
Country of study: United States of America
Gd-MRI vs ABR + Gd-MRI
To compare hypothetical costs for identification of ANs when using MRI with gadolinium Gd 64 (MRI-(64)Gd) as a sole diagnostic test and when using ABR testing followed by MRI-( 64)Gd (ABR + MRI-(64)Gd) for those with positive ABR findings. Authors concluded decisions regarding assessment of patients at risk for ANs must be made on a case-by-case basis. Use of ABR + MRI-(64)Gd allows considerable savings when patients are in the intermediate- or low-risk subgroups. New MRI and ABR testing techniques offer promise for reducing costs.

18
Screening in ASNHL for acoustic neuroma
Table 6 Summary of cost based studies (continued)
Reference Abstract / Summary
Urben SL, Benninger MS, and Gibbens ND. (1999) Asymmetric sensorineural hearing loss in a community-based population. Otolaryngology - Head and Neck Surgery 120:809-814.
Country of study: United States of America
ABR vs ABR + radiological examination
A retrospective study of all patients with ASNHL who were evaluated in a community-based general otolaryngology practice was performed. ASNHL was present in 325 patients The charge of diagnosis per AN was more than $41,000. In summary, a small percentage of patients with ASNHL have retrocochlear pathology, and the charge of diagnosis per AN can be excessive. A cost-containment approach for the evaluation and management of patients with ASNHL is proposed. Further details are provided under the Key Publications section.
MRI
Murphy MR and Selesnick SH. (2002) Cost-effective diagnosis of acoustic neuromas: a philosophical, macroeconomic, and technological decision (Brief record). Otolaryngology. Head and Neck Surgery 127:253-259.
Country of study: United States of America
Gd-MRI
This study aimed to define the most sensitive techniques of AN diagnosis, to examine their relative costs, and to propose diagnostic modality selection given the rarity of AN incidence and given the other costs that society faces in more commonly encountered diseases. The review found that although MRI with gadolinium remains the most sensitive diagnostic modality in the discovery of AN, its cost may be prohibitive for some societies. The study suggested the modality to use in AN diagnosis is just as much a philosophical and macroeconomic question as a technological one. The cost of a timely diagnosis of ANs must be weighed against using resources for other, more pressing, health concerns.
Verret DJ, Adelson R, and Defatta R. (2006) Asymmetric sensorineural hearing loss evaluation with T2 FSE-MRI in a public hospital. Acta Oto-Laryngologica 126:705-707.
Country of study: United States of America
FSE-MRI vs Gd-MRI
The goal of this study was to determine if fast spin echo T2 MRI is similar to gadolinium-enhanced MRI in evaluating ASNHL in a county hospital population. This was a retrospective chart review of all outpatients who underwent gadolinium-enhanced MRI. Cost savings of over $100 000 would have been realised if only T2 FSE protocols had been used. Further details are provided under the Key Publications section.
Daniels RL, Shelton C, and Harnsberger HR. (1998) Ultra high resolution non-enhanced fast spin echo magnetic resonance imaging: Cost-effective screening for acoustic neuroma in patients with sudden sensorineural hearing loss. Otolaryngology - Head and Neck Surgery 119:364-369.
Country of study: United States of America
FSE-MRI
Cost analysis was done in the cases of 58 patients with sudden SNHL by comparing the costs for routine workup and screening of AN with the cost of fast spin echo MRI with the use of screening protocols based on literature review. The potential cost savings of evaluating patients with SSHL with fast spin echo MRI for AN was substantial, with a 54% reduction in screening costs. Authors state that fast spin echo MRI has become the most cost-effective method to screen suspected cases of AN at their institution. This is due to improved technology at reduced cost and through eliminating charges for impedance audiometry, ABR testing, and contrast- enhanced MRI.

19
Screening in ASNHL for acoustic neuroma
Table 6 Summary of cost based studies (continued)
Reference Abstract / Summary
Carrier DA and Arriaga MA. (1997) Cost-effective evaluation of asymmetric sensorineural hearing loss with focused magnetic resonance imaging (Structured abstract). Otolaryngology. Head and Neck Surgery 116:567-574.
Country of study: United States of America
T1 and T2 MRI
This paper developed a focused MRI sequence for evaluation of patients with ASNHL. The protocol includes a T1-weighted sagittal localizer, pregadolinium and postgadolinium T1-weighted 3-mm contiguous axial slices through the internal auditory canal and the region of the cerebellopontine angle, and T2-weighted axial images through the entire brain. Total scanning time was about 12 minutes, and the estimated cost was $300 to $500. Authors suggested that by eliminating the need for follow-up audiometric or electrophysiologic studies, a focused MRI-based diagnostic scheme is more cost-effective on a cost-per patient basis.
Ravi K, V and Wells SC. (1996) A cost effective screening protocol for vestibular schwannoma in the late 90s (Brief record). Journal of Laryngology. and Otology. 110:1129-1132.
Country of study: United Kingdom
MRI
In a retrospective study, the clinical records of all the patients who presented to the ENT department of Taunton and Somerset NHS Trust with suspected symptoms of VS during the year 1994 were analysed. The cost of confirming or refuting the diagnosis of VS in each patient ranged from £220.72 to £580.31 depending on the number of hospital visits and investigations performed. This study shows that the routine use of MR scanning for detection of VS is cost effective and more effective than the use of conventional tests.
Allen RW, Harnsberger HR, Shelton C, King B, Bell DA, Miller R, Parkin JL, Apfelbaum RI, and Parker D. (1996) Low-cost high-resolution fast spin-echo MR of acoustic schwannoma: An alternative to enhanced conventional spin-echo MRI American Journal of Neuroradiology 17:1205-1210.
Country of study: United States of America
FSE-MRI vs T1W-MRI
This paper reviewed the records of 25 patients with pathologically documented acoustic schwannoma and 25 control subjects, all of whom had undergone both enhanced conventional spin-echo MRI and unenhanced fast spin- echo MRI of the cerebellopontine angle/internal auditory canal region. They found no statistically significant difference in the sensitivity and specificity of unenhanced high-resolution fast spin-echo imaging and enhanced T1-weighted conventional spin-echo imaging in the detection of acoustic schwannoma. Authors concluded that the unenhanced high- resolution fast spin-echo technique provides a cost-effective method for the diagnosis of acoustic schwannoma.
Robson AK, Leighton SE, Anslow P, and Milford CA. (1993) MRI as a single screening procedure for acoustic neuroma: a cost effective protocol. Journal of the Royal Society of Medicine 86:455-457.
Country of study: United Kingdom
Audiovestibular investigations vs MRI
A prospective study was set up in a specially designated screening session to audit the cost effectiveness and accuracy of audiovestibular investigations compared to MRI. The total cost of the audiovestibular protocol was £12,545 compared to £12,900 for the MRI protocol, which is a diagnostic and well-tolerated procedure. This study shows that MRI can be cost effective, as well as accurate, when used as a single screening procedure for ANs.

20
Screening in ASNHL for acoustic neuroma
Table 6 Summary of cost based studies (continued)
Reference Abstract / Summary
OTHER
Bance ML, Hyde ML, Malizia K. (1994) Decision and cost analysis in acoustic neuroma diagnosis. J Otolaryngol 23: 109-120
Country of study: Canada
Variety of diagnostic tests
This study seeks to determine the most efficient testing strategy for patients with AN. They develop analytic techniques to allow analysis of diagnostic strategies that included multi-test protocols.
Mangham CA and Welling DB. (1992) Acoustic neuroma: Cost-effective approach [1]. Otolaryngology - Head and Neck Surgery 106:315-316.
Country of study: NA
NA
Abbreviations: ABR, audio brainstem response; AN, acoustic neuroma; ASNHL, asymmetric sensorineural hearing loss; CT;
computed tomography; dB, decibel; ENT, ear nose throat; FSE, fast spin echo; GdMRI, gadolinium enhanced MRI; MRI,
magnetic resonance imaging; NA = not available; NHS, National Health Service; SNHL, sensorineural hearing loss; VS, vestibular schwannoma.
Key publications
A selection of citations, which appeared to have the most relevance for the topic of
interest were requested in full text. Further detail of each study is provided below.
Positive findings on MRI in patients with asymmetrical SNHL (Mahrous and Kalepu 2008)
This was a retrospective study of 100 patients who attended an ENT outpatient clinic
in a six month period in 2006. All patients presented with ASNHL. The case notes of
patients audiograms and symptoms, on which the decision to scan with MRI was
made, were reviewed. There were no guidelines or protocols employed as to when to
request MRI. The mean age of participants was 53 years and there were 53% males
and 47% females. There was one patient diagnosed with acoustic neuroma which
equates to a pick up rate of 1%, a figure lower than that published in other series. The
patient diagnosed with AN was a 61 year old male, with gradual right SNHL for 3
years. The patient had audiogram asymmetry of >15 dB in the frequencies 500-4 kHz.
The MRI showed a 18 x 16mm lesion in the right internal acoustic meatus displacing
the cerebellum and pons. The authors suggest universal screening for AN is debatable
due to the low pick up rate and high expense of MRI. They suggest applying a
protocol to select patients for MRI is worth considering.
Screening patients with sensorineural hearing loss for vestibular schwannoma using a Bayesian classifier (Nouraei et al. 2007)
This study retrospectively examined records of 129 patients with a proven diagnosis
of vestibular schwannoma based on MRI scans, and an equal number of patients in
whom this diagnosis was suspected, but excluded on MRI. There were 130 males and
128 females and the average age at presentation was 53 ± 15 years (± sd; range 16–97
years). On direct questioning, 121 patients (46%) reported unilateral tinnitus and 79
(30%) episodic vertigo. There were significant overlaps in the degree of hearing
threshold asymmetry between patients with and without a vestibular schwannoma
across all frequencies. A Gaussian Process Ordinal Regression Classifier was used to
predict the likelihood of a patient having or not having a vestibular schwannoma on

21
Screening in ASNHL for acoustic neuroma
the basis of clinical and audiological data. Variables used for analysis included pure
tone thresholds at 250 Hz, 500 Hz, 1 kHz, 2 kHz, 4 kHz and 8 kHz at the time of
presentation, as well as patient age and sex, and the presence or absence of unilateral
tinnitus or episodic vertigo. The study proved it possible to pre-select sensitivity and
specificity, with an area under the curve of 0.8025. At 95% sensitivity, the trained
system had a specificity of 56%, 30% better than audiological protocols with closest
sensitivities. Authors concluded that if applied prospectively, it could reduce the
number of ‘normal’ MRI scans by as much as 30% without reducing detection
sensitivity.
Asymmetric sensorineural hearing loss evaluation with T2 FSE-MRI in a public hospital (Verret et al. 2006)
The records of patients with ASNHL presenting in a country hospital who underwent
MRI evaluation were examined. As part of the screening process, a GD-enhanced
MRI scan sequence was obtained; however this also included a non-GD-enhanced
FSE T2 sequence. A total of 146 patients were identified with patients ranging from
20–84 years with a mean age of 55 years. There were 56 male and 90 female patients.
Of the 146 MRI scans performed, abnormalities were seen on 71 of them, the majority
of which were inconsequential (e.g. sinonasal disease, gray/white matter changes, and
previous cerebrovascular disease or intracranial procedures). However, none of the
abnormalities were retrocochlear or explained the etiology of the audiological
findings. The authors estimated that the cost of GD-enhanced MRI was US$1200,
with a T2 FSE protocol costing about $415. For this study population, a saving of
US$114 610 would have been realised if only a T2 FSE protocol had been used. The
authors concluded that T2-weighted FSE can be economically beneficial for screening
patients with ASNHL without other neurological findings in a public hospital
population.
Magnetic resonance imaging screening for vestibular schwannoma: analysis of published protocols (Obholzer and Harcourt 2004)
This was a retrospective review of radiology reports from all MRIs of the internal
auditory meatus, performed during the year 2000 at Charing Cross Hospital. The
notes of all patients who had vestibular schwannoma and those of the last 100
‘negative’ scans were requested. The presenting symptoms and pure tone audiograms
were extracted and data were analysed comparing the sensitivity and specificity of
differences in hearing loss at each specific frequency, at any two and any three
frequencies, and utilising six published protocols. Thirty-six patients with vestibular
schwannomas were included and 92 without, eight case notes were unavailable.
Thirty two of the 36 presented with ASNHL, 19 of whom also had tinnitus. Four
criteria had a sensitivity of > 95%; of these the highest specificity (49%) utilised an
interaural difference at two adjacent frequencies of 15 dB in unilateral hearing loss
and 20dB in bilateral asymmetric loss. The most sensitive criterion was a difference
of 15 dB at any frequency (sensitivity 100% and specificity 29%). The optimal
combination of sensitivity and specificity was achieved using a criterion of >15 dB
difference at two adjacent frequencies if the mean threshold in the better ear was ≤30
dB, and 20 dB if greater than 30 dB. This produced 97% sensitivity and 49%
specificity. The application of the best protocol would have reduced the number of
MRI scans requested from 392 to 168, saving 224 patients’ scans.

22
Screening in ASNHL for acoustic neuroma
Magnetic resonance imaging for the evaluation of asymmetric sensorineural hearing loss (Cueva 2004)
This was a multi-institutional, prospective, non-randomised comparison of ABR and
MRI with gadolinium for the evaluation of patients with ASNHL (defined as ≥15 dB
in 2 or more pure tone thresholds or an asymmetry of ≥15% on speech discrimination
score). There were 312 patients (between the ages of 18 and 87 years) who completed
the study. Patients prospectively underwent both ABR and MRI with the primary
outcome being the presence or absence of retrocochlear pathology. The results of the
two screening tests are shown below in Table 7.
Table 7 Results of MRI and ABR screening tests
MRI
+ Causative lesion - Causative lesion Total
ABR
Abnormal 22 73 95
Normal 9 208 217
Total 31 281 312
Thirty-one (9.94%) patients of the study population of 312 were found on MRI to
have lesions causing their SNHL. Of the 31 patients with causative lesions on MRI
there were 24 vestibular schwannomas. Twenty-two of the 31 patients had abnormal
ABRs, whereas 9 patients (7 with small vestibular schwannomas) had normal ABRs.
This gives an overall false-negative rate for ABR of 29%. The false-positive rate was
found to be 77%. Sensitivity of ABR as a screening test was 71%, and specificity was
74%. The ABR positive predictive value was 23% and negative predictive value was
96%. ABR was been demonstrated to have low sensitivity and specificity in the
evaluation of these patients and cannot be relied on as a screening test for patients
with asymmetric SNHL. Keeping the use of MRI conditional on the results of ABR
will annually result in missed or delayed diagnosis of causative lesions in 29 patients
per 1,000 screened. The author recommends abandoning ABR as a screening test for
asymmetric SNHL and adoption of a focused MRI protocol as the screening test of
choice.
Screening for vestibular schwannoma: current practice in New Zealand (Dawes 1999)
This study reported the results of a questionnaire survey of New Zealand
otolaryngologists. Sixty seven questionnaires were sent. Forty-two replies were
received, three other replies indicated that the member had retired from clinical
practice. The results indicated that 41 clinicians preferred MRI testing for screening
for AN. However, only 29 had locally available imaging equipment. Twenty-four
clinicians used MRI as their first screening test, 10 used ABR and then MRI, 7 used
clinical judgement and other investigations and one used CT scanning only. The
survey also indicated that many clinicians still use ABR and CT as a preliminary
screen to select for MRI because of financial or local political reasons. The author
believes New Zealand would be best served by a single set of vestibular schwannoma
screening guidelines.

23
Screening in ASNHL for acoustic neuroma
MRI in the detection of acoustic neuromas- a suggested protocol for screening (Sheppard 1996)
During the period September 1990 to September 1993, 920 requests for MRI imaging
of the IAM or cerebellopontine angle were made within the Oxford region. A total of
892 scans were successfully carried out. The symptoms of ENT patients scanned from
the Oxford Department of Otolaryngology included sudden and gradual sensorineural
hearing loss, tinnitus, vertigo, otalgia. Facial numbness and facial palsy. The decision
to scan was based on the presence of asymmetrical audiovestibular symptoms as
outlined by Robson et al. (1993). Initially, all patients had sagittal and axial T,
weighted interleaved images performed after the administration of gadolinium. The
current scanning protocol involves only 3 mm interleaved fast spin echo T, weighted
axial scans. Four millimetres T, weighted images with gadolinium-DTPA
enhancement are used if there is diagnostic doubt.
Of the total number of patients scanned (n = 892), an acoustic neuroma was detected
in 38 (4.26%). Of these patients, 16 were men and 22 women. Of the 38, 18 were
from non-Oxford clinics, 20 from oxford clinics. Those from the Oxford clinic all had
a degree of ASNHL ranging from 15 dB to 92 dB between normal and abnormal ears.
The study suggested a protocol for the selection of MRI which was: those patients up
to 70 years of age presenting with unilateral audiovestibular symptoms in the absence
of significant neurological symptoms or signs, with an average difference in hearing
threshold of 15 dB between normal and symptomatic ears or unilateral tinnitus with
normal hearing.
A prospective study of ABR and MRI in the screening for vestibular schwannomas (Ruckenstein et al. 1996)
This was a prospective study of 47 patients with ASNHL. Adult patients (18 years or
older) with asymmetry in two or more pure-tone thresholds of ≥15 dB were included.
The mean age of patients was 56 years with 19% older than 65 years. All patients
underwent an ABR and enhanced MRI scan. ABRs were considered abnormal if they
demonstrated asymmetric IT5 latencies (asymmetry >0.2ms), abnormal absolute wave
V latencies, or absent or poor waveform morphology. All MRI scans were reviewed
by a neuroradiologist for the presence or absence of retrocochlear disease. The
authors obtained a sensitivity of 63%, specificity of 64%, positive predictive value of
26%, and negative predictive value of 89% for the ABR test. The 3 ANs missed were
all less than 2 cm. The authors concluded that ABR testing was not an ideal screening
test, cautioning, however, that a larger sample size would be required for confirmation
of this assertion.
Cost-effective initial screening for vestibular schwannoma: auditory brainstem response or magnetic resonance imaging? (Rupa et al. 2003)
This study aimed to determine the cost-effectiveness of including ABR testing in a
screening protocol for the diagnosis of AN in patients with asymmetric auditory
symptoms at the Christian Medical College and Hospital, Vellore, India, where,
commonly, patients with AN have tumours greater than 2 cm at the time of diagnosis.
Ninety patients who presented to the ENT Department with asymmetric auditory
symptoms of hearing loss and tinnitus were prospectively evaluated by pure tone
audiometry, ABR testing, and gadolinium-enhanced MRI (GdMRI) of the temporal
bone and brain. Of a total of 90 patients enrolled in the study, 56 were males and 34

24
Screening in ASNHL for acoustic neuroma
females (age range, 15 to 66 years). Of the 30 patients who were found to have
retrocochlear pathology on ABR, 4 patients were diagnosed as having AN.
The study indicated that the cost of GdMRI was approximately 15 times the cost of
ABR. Thus, if all 90 patients had undergone GdMRI alone, the total cost of
investigation would have been $18,000. If only the 48 patients who had either no
response or evidence of retrocochlear pathology on ABR underwent GdMRI, the cost
of screening would have been $9,600. Therefore, a protocol involving screening all
patients with ABR and only subjecting those patients with no response or
retrocochlear pathology on ABR to MRI would save up to $7,200 in total. Because 6
patients with AN were identified, the saving in cost per patient diagnosed correctly
was $1,200. This would be the approximate total cost of having the tumour surgically
excised at this hospital. The authors concluded that the financial burden of identifying
patients with AN could be considerably reduced with a screening protocol including
ABR.
Asymmetric sensorineural hearing loss in a community-based population (Urben et al. 1999)
This was a 5-year retrospective study that examined patients older than 17 years with
ASNHL (defined as an interaural difference in pure-tone thresholds ≥10 dB at 2
frequencies or ≥15 dB at 1 frequency. The study also conducted a cost analysis for
diagnosing AN. All patients’ medical records and audiograms were reviewed for
demographic, historic, and audiologic data and results from ABRs and radiologic
studies. Of all the audiograms reviewed, 193 (21%) met the audiological criteria for
ASNHL. Patients with ASNHL were a median age of 51 years, with 66% male and
34% female.
Among the 193 patients who had diagnostic studies, 4 were found to have ANs, for a
prevalence of 2.1%. ABR tests were performed in 179 patients (55%), and 92% (164
of 179) were normal. Patients with abnormal or inconclusive ABR and patients with
severe SNHL were evaluated with radiologic studies (46 patients). Of the 34 who had
an MRI, 30 were normal and four were abnormal. All 19 CT scans were judged as
normal.
To assess the cost of diagnosis per AN, the study determined the charges for
diagnostic studies. Charges may differ from patient costs. Because audiograms were
used in the inclusion criteria for the study, the charge for audiograms was excluded.
The charges for diagnostic studies were multiplied by the number of studies
performed, and a charge of $166,955 was incurred in identifying 4 patients with AN
and ASNHL. The charge of diagnosis per AN was more than $41,000. The authors
suggest a cost containment protocol for screening AN.
Published audiological screening protocols
Acoustic neuromas produce patterns of audiovestibular symptoms and in particular
ASNHL, which tends to be different between patients with and without an AN. This
difference has been used to develop a number of different decision-support protocols
for clinicians, to assist in risk-stratifying patients, with those at higher risk being
referred for an MRI. A brief description of published audiological screening protocols
for AN is shown in Table 8.

25
Screening in ASNHL for acoustic neuroma
Table 8 A description of published decision-support
protocols for acoustic neuroma
Name Clinical criteria Asymmetry of thresholds
Seattle (Mangham 1991) Nil ≥15 dB between the average of 1-8 KHz
Charing cross (Obholzer et al. 2004)
Nil ≥15 dB in any two neighbouring frequencies if the average hearing threshold of the better ear ≤30
dB≥20 dB in any two neighbouring frequencies if the average hearing threshold of the better ear >30 dB
Nashville (Welling et al. 1990) Nil ≥15 dB at any frequency between 0.5 and 4 KHz
Oxford (Sheppard et al. 1996) Unilateral tinnitus, age < 70 years
≥15 dB between the average of 0.5 to 8 KHz
UK Department of Health (2002) Vertigo ≥ 20 dB at any frequency between 0.5 and 4 KHz
Sunderland (Dawes et al. 1998) Unilateral tinnitus or Meniere’s disease symptoms
≥ 20 dB between two neighbouring frequencies
Source: Nouraei et al. (2007), Table 1 page 251.
None of these protocols are universally accepted for screening AN in patients with
ASNHL.

26
Screening in ASNHL for acoustic neuroma
27
Screening in ASNHL for acoustic neuroma
Summary and Recommendations
Conclusions
This preliminary report presents the evidence for the early detection of AN using MRI
or other comparative diagnostic techniques in patients with ASNHL, albeit without
critical appraisal. It appears there is a significant clinical argument to support the
routine use of MRI. The test has been reported to have high sensitivity and specificity,
higher than that of the ABR test. However, the widespread use of MRI in this patient
population is problematic due to the high cost per diagnosis of AN (attributed to the
high cost of MRI and low incidence rate of AN in ASNHL presenting patients), and
issues surrounding accessibility to MRI equipment. Most papers suggest a protocol or
guidelines be implemented to help select patients for MRI screening. However this
approach accepts that there is a trade-off between cost efficiency, and the risk of
missing some tumours.
Points to consider
As mentioned previously there is a systematic review due for publication by the
NIHR in April 2009 titled:
‘The role of magnetic resonance imaging in the identification of suspected acoustic
neuroma: systematic review of clinical and cost effectiveness, and natural history’
Alternatively a full systematic review could be considered on the use of MRI in
screening patients with ASNHL for the early detection of AN.

28
Screening in ASNHL for acoustic neuroma

29
Screening in ASNHL for acoustic neuroma
References
Adler JR, Atlas M, and Shnier R. (1998) High resolution MRI and asymmetric
sensori-neural hearing loss. Australian Journal of Otolaryngology 1:1-5.
Allen RW, Harnsberger HR, Shelton C, King B, Bell DA, Miller R, Parkin JL,
Apfelbaum RI, and Parker D. (1996) Low-cost high-resolution fast spin-echo MR of
acoustic schwannoma: An alternative to enhanced conventional spin-echo MR?
American Journal of Neuroradiology 17:1205-1210.
Angeli S, Yan D, Telischi F, and et al. (2005) Etiologic diagnosis of sensorineural
hearing loss in adults. Archives of Otolaryngology– Head & Neck Surgery 132:890-
895.
Annesley-Williams DJ, Laitt RD, Jenkins JPR, Ramsden RT, and Gillespie JE. (2001)
Magnetic resonance imaging in the investigation of sensorineural hearing loss: Is
contrast enhancement still necessary? Journal of Laryngology and Otology 115:14-
21.
Baker R, Stevens-King A, Bhat N, and Leong P. (2003) Should patients with
asymmetrical noise-induced hearing loss be screened for vestibular schwannomas?
Clinical Otolaryngology and Allied Sciences 28:346-351.
Bance ML, Hyde ML, and Malizia K. (1994) Decision and cost analysis in acoustic
neuroma diagnosis. The Journal of Otolaryngology 23:109-120.
Bassi P, Piazza P, Cusmano F, Menozzi R, Gandolfi A, and Zini C. (1989) MR
cisternography of the cerebello-pontine angle and internal auditory canal in diagnosis
of intracanalicular acoustic neuroma. Neuroradiology 31:486-491.
Carrier DA and Arriaga MA. (1997) Cost-effective evaluation of asymmetric
sensorineural hearing loss with focused magnetic resonance imaging (Structured
abstract). Archives of Otolaryngology– Head & Neck Surgery 116:567-574.
Chaimoff M, Nageris BI, Sulkes J, Spitzer T, and Kalmanowitz M. (1999) Sudden
hearing loss as a presenting symptom of acoustic neuroma. American Journal of
Otolaryngology - Head and Neck Medicine and Surgery 20:157-160.
Cheng G, Smith R, and Tan A-KW. (2003) Cost comparison of auditory brainstem
response versus magnetic resonance imaging screening of acoustic neuroma (Brief
record). The Journal of Otolaryngology. 32:394-399.
Cueva RA. (2004) Auditory brainstem response versus magnetic resonance imaging
for the evaluation of asymmetric sensorineural hearing loss. The Laryngoscope
114:1686-1692.
Curati WL, Graif M, Kingsley D, King T, Scholtz C, and Steiner R. (1986) MRI in
acoustic neuroma: a review of 35 patients. Neuroradiology 28:208-214.

30
Screening in ASNHL for acoustic neuroma
Daniels RL, Shelton C, and Harnsberger HR. (1998) Ultra high resolution
nonenhanced fast spin echo magnetic resonance imaging: Cost-effective screening for
acoustic neuroma in patients with sudden sensorineural hearing loss. American
Journal of Otolaryngology - Head and Neck Medicine and Surgery 119:364-369.
Dawes PJD. (1999) Screening for vestibular schwannoma: Current practice in New
Zealand. Australian Journal of Otolaryngology 3:307-310.
Dawes PJD and Jeannon JP. (1998) Audit of regional screening guidelines for
vestibular schwannoma. The Journal of Laryngology and Otology 112:860-864.
Dornhoffer JL, Helms J, and Hoehmann DH. (1994) Presentation and diagnosis of
small acoustic tumors. American Journal of Otolaryngology– Head & Neck Surgery
111:232-235.
El Kashlan HK, Eisenmann D, and Kileny PR. (2000) Auditory brain stem response
in small acoustic neuromas. Ear and Hearing 21:257-262.
Fortnum H, Nikolopoulos T, O'Neill C, Taylor R, Baguley D, Lenthall R, et al. (2007)
The role of magnetic resonance imaging in the identification of suspected acoustic
neuroma: systematic review of clinical- and cost- effectiveness, and natural history.
National Institute of Health Research.
Hashimoto S, Kawase T, Furukawa K, and Takasaka T. (1991) Strategy for the
diagnosis of small acoustic neuromas. Acta Oto-Laryngologica, Supplement 481:567-
569.
Isaacson JE and Vora NM. (2003) Differential diagnosis and treatment of hearing
loss. American Family Physician 68:1125-1132.
Kanzaki J, Ogawa K, Ogawa S, Yamamoto M, Ikeda S, and Uchi T. (1991)
Audiological findings in acoustic neuroma. Acta Oto-Laryngologica, Supplement
487:125-132.
Kanzaki J, Ogawa K, Tsuchihashi N, Yamamoto M, Ogawa S, and Uchi T. (1991)
Diagnostic procedure for acoustic neuroma. Acta Oto-Laryngologica, Supplement
487:114-119.
Kanzaki J. (1986) Present state of early neurotological diagnosis of acoustic neuroma.
Journal for Oto-rhino-laryngology and its Related Specialities 48:193-198.
Kubo T, Sakashita T, Kusuki M, Kyunai K, Ueno K, Hikawa C, Wada T, and Nakai
Y. (2000) Evaluation of radiological examination for sensorineural hearing loss. Acta
Oto-Laryngologica, Supplement -:34-38.
Levy RA and Arts HA. (1996) Predicting neuroradiologic outcome in patients
referred for audiovestibular dysfunction. American Journal of Neuroradiology
17:1717-1724.

31
Screening in ASNHL for acoustic neuroma
Mahrous AK and Kalepu R. (2008) Positive findings on MRI in patients with
asymmetrical SNHL. European Archives of Otolaryngology-Rhino-Laryngology
265:1471-1475.
Manfre L, Angileri T, Ferrara S, Accardi M, Raineri R, and Lagalla R. (1997) The
role of magnetic resonance imaging in central hearing deficits: Beyond the acoustic
schwannoma. Rivista di Neuroradiologia 10:409-416.
Mangham CA and Welling DB. (1992) Acoustic neuroma: Cost-effective approach
[1]. Archives of Otolaryngology– Head & Neck Surgery 106:315-316.
Mangham CA. (1991) Hearing threshold difference between ears and the risk of
acoustic tumour. Archives of Otolaryngology– Head & Neck Surgery 105:814-817.
Monsell EM and Rock JP. (1990) Sensorineural hearing loss and the diagnosis of
acoustic neuroma. Henry Ford Hospital Medical Journal 38:9-12.
Montaguti M, Bergonzoni C, Zanetti MA, and Rinaldi Ceroni A. (2007) Comparative
evaluation of ABR abnormalities in patients with and without neurinoma of VIII
cranial nerve. Acta Oto-Laryngologica 27:68-72.
Morley S and Beale TJ. (2007) Imaging of deafness and tinnitus. Imaging 19:55-70.
Murphy MR and Selesnick SH. (2002) Cost-effective diagnosis of acoustic neuromas:
a philosophical, macroeconomic, and technological decision (Brief record). Archives
of Otolaryngology– Head & Neck Surgery 127:253-259.
Myrseth E, Pederson PH, Moller P, and Lund-Johansen M. (2007) Treatment of
vestibular schwannomas. Why, when and how? Acta Neurochirurgica 49:647-660.
National Institute of Health Research. (2009) The role of magnetic resonance imaging
in the identification of suspected acoustic neuroma: systematic review of clinical and
cost effectiveness, and natural history. UK Department of Health.
Nouraei S, Huys Q, Chatrath P, Powles J, and Harcourt J. (2007) Screening patients
with sensorineural hearing loss for vestibular schwannoma using a Bayesian
classifier. Clinical Otalaryngology 32:248-254.
Obholzer RJ and Harcourt JP. (2004) Magnetic resonance imaging screening for
vestibular schwannoma: analysis of published protocols. The Journal of Laryngology
and Otology. 118:329-332.
Prasad J and Cousins VC. (2004) Asymmetrical hearing loss. Australian Family
Physician 37(4):312-320.
Ravi K, V and Wells SC. (1996) A cost effective screening protocol for vestibular
schwannoma in the late 90s (Brief record). The Journal of Laryngology and Otology.
110:1129-1132.

32
Screening in ASNHL for acoustic neuroma
Robinette MS, Bauch CD, Olsen WO, and Cevette MJ. (2000) Auditory brainstem
response and magnetic resonance imaging for acoustic neuromas: costs by prevalence
(Brief record). Archives of Otolaryngology. Head and Neck Surgery 126:963-966.
Robson AK, Leighton SE, Anslow P, and Milford CA. (1993) MRI as a single
screening procedure for acoustic neuroma: a cost effective protocol. Journal of the
Royal Society of Medicine 86:455-457.
Ruckenstein MJ, Cueva RA, Morrison DH, and Press G. (1996) A prospective study
of ABR and MRI in the screening for vestibular schwannomas. American Journal of
Otology 17:317-320.
Rupa V, Job A, George M, and Rajshekhar V. (2003) Cost-effective initial screening
for vestibular schwannoma: auditory brainstem response or magnetic resonance
imaging? Otolaryngology– Head & Neck Surgery 128:823-828.
Sabini P and Sclafani AP. (2000) Efficacy of serologic testing in asymmetrical
sensorinerual hearing loss. Otolaryngology– Head & Neck Surgery 122:469-476.
Saunders JE, Luxford WM, Devgan KK, and Fetterman BL. (1995) Sudden hearing
loss in acoustic neuroma patients. Otolaryngology– Head and Neck Surgery 113:23-
31.
Schmidt RJ, Sataloff RT, Newman J, Spiegel JR, and Myers DL. (2001) The
sensitivity of auditory brainstem response testing for the diagnosis of acoustic
neuromas. Archives of Otolaryngology– Head & Neck Surgery 127:19-22.
Sheppard IJ, Milford CA, and Anslow P. (1995) MRI in the detection of acoustic
neuromas- a suggested protocol for screening. Clinical Otolaryngology & Allied
Sciences 21:301-304.
Smith IM, Turnbull LW, Sellar RJ, Murray JAM, and Best JJK. (1990) A modified
screening protocol for the diagnosis of acoustic neuromas. Clinical Otolaryngology
and Allied Sciences 15:167-171.
Soulie D, Cordoliani YS, Vignaud J, and Cosnard G. (1997) MR imaging of acoustic
neuroma with high resolution fast spin echo T2-weighted sequence. European
Journal of Radiology 24:61-65.
Spoelhof GD. (1995) When to suspect an acoustic neuroma. American Family
Physician 52:1768-1774.
Stack JP, Ramsden RT, Antoun NM, Lye RH, Isherwood I, and Jenkins JP. (1988)
Magnetic resonance imaging of acoustic neuromas: the role of gadolinium-DTPA.
The British Journal of Radiology 61:800-805.
Swan IRC. (1989) Diagnostic vetting of individuals with asymmetric sensorineural
hearing impairments. Journal of Laryngology and Otology 103:823-826.

33
Screening in ASNHL for acoustic neuroma
Swartz JD. (2004) Lesions of the cerebellopontine angle and internal auditory canal:
diagnosis and differential diagnosis. Seminars in Ultrasound, CT, and MRI 25:332-
352.
Telian SA, Kileny PR, Niparko JK, Kemink JL, and Graham MD. (1989) Normal
auditory brainstem response in patients with acoustic neuroma. The Laryngoscope
99:10-14.
Thomsen J and Tos M. (1993) Management of acoustic neuromas. Annales d'Oto-
Laryngologie et de Chirurgie Cervico-Faciale 110:179-191.
UK Department of Health. (2002) Clinical effectiveness guidelines: acoustic neuroma
(vestibular schwannoma). UK Department of Health.
Urben SL, Benninger MS, and Gibbens ND. (1999) Asymmetrical sensorineural
hearing loss in a community-based population. Otolaryngology– Head & Neck
Surgery 120:809-814.
Verret DJ, Adelson R, and Defatta R. (2006) Asymmetric sensorineural hearing loss
evaluation with T2 FSE-MRI in a public hospital. Acta Oto-Laryngologica 126:705-
707.
Vossough A. (2003) Imaging evaluation of sensorineural hearing loss. Applied
Radiology 32:6-14.
Wareing MJ, Baguley D, and Moffat DA. (2002) Investigations for vestibular
schwannoma. CME Bulletin Otorhinolaryngology Head and Neck Surgery 6:12-15.
Welling DB, Glassock ME, Woods CI, et al. (1990) Acoustic neuroma: a cost-
effective approach. Otolaryngology– Head & Neck Surgery 103:364-370.
Wright A and Bradford R. (1995) Management of acoustic neuroma. British Medical
Journal 311:1141-1144.
Zealley IA, Cooper RC, Clifford KM, Campbell RS, Potterton AJ, Zammit-Maempal
I, Baudouin CJ, and Coulthard AJ. (2000) MRI screening for acoustic neuroma: a
comparison of fast spin echo and contrast enhanced imaging in 1233 patients. The
British Journal of Radiology 73:247.

34
Screening in ASNHL for acoustic neuroma
35
Screening in ASNHL for acoustic neuroma
Appendix A: HTA websites searched
HTA and systematic review databases to be searched for this project are:
Health Technology Assessment Database (via the Cochrane Library):
http://www3.interscience.wiley.com/cgi-bin/mrwhome/106568753/HOME
INAHTA website database:
http://www.inahta.org/Search2/?pub=1
Note: Can search database and gain access to individual member websites.
Individual HTA groups:
MSAC: http://www.msac.gov.au/
ANZHSN: http://www.horizonscanning.gov.au/
NZHTA: http://nzhta.chmeds.ac.nz/
NICE: http://www.nice.org.uk/
AHRQ/USPSTF: http://www.ahrq.gov/
CADTH: http://www.cadth.ca/

36
Screening in ASNHL for acoustic neuroma

37
Screening in ASNHL for acoustic neuroma
Appendix B: Excluded studies annotated by reason for exclusion
Farrell III JT. (1983) Radiographic
evaluation of acoustic neuromas:
Comparison of high-resolution
computed tomography and
polytomography. Journal of the
American Osteopathic Association
83:61-66.
Reason for exclusion: Incorrect study
type
Adelman S. (1983) Identification of
acoustic neuroma in noise-exposed
workers. Scandinavian Audiology
12:247-250.
Reason for exclusion: Incorrect study
type
Flood LM and Brightwell AP. (1984)
Cochlear deafness in the presentation
of a large acoustic neuroma. Journal of
Laryngology and Otology 98:87-92.
Reason for exclusion: Incorrect study
type
Terry RM. (1985) An unusual
presentation of acoustic neuroma.
Journal of Laryngology and Otology
99:593-595.
Reason for exclusion: Incorrect study
type
David M and Trehub SE. (1989)
Perspectives on deafened adults.
American Annals of the Deaf 134:200-
204.
Reason for exclusion: Incorrect study
type
(1990) Docs' Discussion at OMG.
American Journal of Otology 11:141-
143.
Reason for exclusion: Incorrect study
type
Farrell ML, Harries MLL, Baguley
DM, and Moffat DA. (1991) Bilateral
acoustic schwannoma: Post-operative
hearing in the contralateral ear.
Journal of Laryngology and Otology
105:769-771.
Reason for exclusion: Incorrect study
type
Moon HH, Jabour BA, Andrews JC,
Canalis RF, Chen FH, Anzai Y, Becker
DP, Lufkin RB, and Hanafee WN.
(1991) Nonneoplastic enhancing
lesions mimicking intracanalicular
acoustic neuroma on gadolinium-
enhanced MR images. Radiology
179:795-796.
Reason for exclusion: Incorrect study
type
House H, Sheehy J, De la Cruz A,
House J, Nelson R, Luxford W,
Shelton C, and Linthicum J. (1991)
Docs' discussion at HEC. American
Journal of Otology 12:147-149.
Reason for exclusion: Incorrect study
type
Vellutini EAS, Cruz OLM, Velasco
OP, Miniti A, and Almeida GM.
(1991) Reversible hearing loss from
cerebellopontine angle tumors.
Neurosurgery 28:310-313.
Reason for exclusion: Incorrect study
type
Berenholz LP, Eriksen C, and Hirsh
FA. (1992) Recovery from repeated
sudden hearing loss with corticosteroid
use in the presence of an acoustic
neuroma. Annals of Otology,
Rhinology and Laryngology 101:827-
831.
Reason for exclusion: Incorrect study
type
Quester R, Menzel J, and Thumfart W.
(1993) Radical removal of a large

38
Screening in ASNHL for acoustic neuroma
glossopharyngeal neurinoma with
preservation of cranial nerve functions.
Ear, Nose and Throat Journal 72:600-
611.
Reason for exclusion: Incorrect study
type
Ghobashy A and Van Loveren H.
(1993) Acoustic schwannoma
presenting as acute posterior fossa
hematoma: Case report and review of
the literature. Skull Base Surgery
3:136-140.
Reason for exclusion: Incorrect study
type
Kingdom TT, Lalwani AK, Pitts LH,
Chandler WF, and Salcman M. (1993)
Isolated metastatic melanoma of the
cerebellopontine angle: Case report.
Neurosurgery 33:142-144.
Reason for exclusion: Incorrect study
type
Van Leeuwen JPPM, Cremers CWRJ,
Thijssen HOM, and Meyer HE. (1993)
Unchanged unilateral hearing loss and
ipsilateral growth of an acoustic
neuroma from 1 to 4 cm. Journal of
Laryngology and Otology 107:230-
232.
Reason for exclusion: Incorrect study
type
Shelton C. (1993) Doc's Discussion at
HEC. American Journal of Otology
14:199-202.
Reason for exclusion: Incorrect study
type
O'Donoghue GM. (1993) Acoustic
neuroma: triumph and disaster. British
Journal of Hospital Medicine 49:85-
87.
Reason for exclusion: Incorrect study
type
Levine RA, Bu-Saba N, and Brown
MC. (1993) Laser-Doppler
measurements and
electrocochleography during ischemia
of the guinea pig cochlea: Implications
for hearing preservation in acoustic
neuroma surgery. Annals of Otology,
Rhinology and Laryngology 102:127-
136.
Reason for exclusion: Incorrect study
type
Kawaguchi T, Tanaka R, Kameyama
S, and Yamazaki H. (1994) Full
recovery from deafness after removal
of a large acoustic neurinoma
associated with neurofibromatosis 2:
Case report. Surgical Neurology
42:326-329.
Reason for exclusion: Incorrect study
type
Downie AC, Howlett DC, Koefman
RJ, Banerjee AK, and Tonge KA.
(1994) Case report: prolonged contrast
enhancement of the inner ear on
magnetic resonance imaging in
Ramsay Hunt syndrome. British
Journal of Radiology 67:819-821.
Reason for exclusion: Incorrect study
type
Linstrom CJ, Krajewski MJ, Shapiro
AL, and Caruana S. (1994) Outer table
graft in middle fossa surgery.
Otolaryngology - Head and Neck
Surgery 111:70-75.
Reason for exclusion: Incorrect study
type
Sakakibara A, Aoyagi M, and Koike
Y. (1994) Acoustic neuroma presented
as repeated hearing loss. Acta Oto-
Laryngologica, Supplement 511:77-80.
Reason for exclusion: Incorrect study
type
Donnelly MJ, Daly CA, and Briggs
RJS. (1994) MR imaging features of an
intracochlear acoustic schwannoma.
Journal of Laryngology and Otology
108:1111-1114.

39
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect study
type
Sells JP and Hurley RM. (1994)
Acoustic neuroma in an adolescent
without neurofibromatosis: case study.
Journal of the American Academy of
Audiology 5:349-354.
Reason for exclusion: Incorrect study
type
Schneider ML, Walker GB, and
Dormer KJ. (1995) Effects of magnetic
resonance imaging on implantable
permanent magnets. American Journal
of Otology 16:687-689.
Reason for exclusion: Incorrect study
type
Wall MP and Block R. (1995) Annual
meeting of the American
Laryngological, Rhinological, and
Otological Society. Archives of
Otolaryngology - Head and Neck
Surgery 121:1065-1066.
Reason for exclusion: Incorrect study
type
Saeed SR, Woolford TJ, Ramsden RT,
and Lye RH. (1995) Magnetic
resonance imaging: A cost-effective
first line investigation in the detection
of vestibular schwannomas. British
Journal of Neurosurgery 9:497-503.
Reason for exclusion: Incorrect study
type
Minor LB. (1995) Neuro-otology:
Hearing. Current Opinion in
Neurology 8:89-94.
Reason for exclusion: Incorrect study
type
Peh WC and Yuen AP. (1995) Clinics
in diagnostic imaging. Singapore
medical journal 36:433-436.
Reason for exclusion: Incorrect study
type
Judkins RF and Rubin AM. (1995)
Sudden hearing loss and unstable
angina pectoris. Ear, Nose and Throat
Journal 74:96-99.
Reason for exclusion: Incorrect study
type
Gaffney RJ and McShane DP. (1996)
Bilateral acoustic neurofibromatosis
camouflaged by corticosteroid
treatment of sudden sensorineural
hearing loss. Leukemia 10:151-152.
Reason for exclusion: Incorrect study
type
Nishizawa S, Yokoyama T, Hinokuma
K, and Uemura K. (1997) Unilateral
sensori-neural hearing disturbance
caused by intramedullary cerebellar
tumors. Neurologia Medico-
Chirurgica 37:701-707.
Reason for exclusion: Incorrect study
type
Ishikawa K, Yasui N, Monoh K, Tada
H, Mineura K, Sasajima H, and
Togawa K. (1997) Unilateral acoustic
neuroma in childhood. Auris Nasus
Larynx 24:99-104.
Reason for exclusion: Incorrect study
type
Fitzgerald DC, Mark AS, and Shelton
C. (1999) Cost-effective screening for
acoustic neuroma [1] (multiple letters).
Otolaryngology - Head and Neck
Surgery 121:846.
Reason for exclusion: Incorrect study
type
Shamboul KM and Grundfast K.
(1999) Hearing loss in
neurofibromatosis type 1: Report of
two cases. East African Medical
Journal 76:117-119.
Reason for exclusion: Incorrect study
type
Selesnick SH, Deora M, Drotman MB,
and Heier LA. (1999) Incidental
discovery of acoustic neuromas.

40
Screening in ASNHL for acoustic neuroma
Otolaryngology - Head and Neck
Surgery 120:815-818.
Reason for exclusion: Incorrect study
type
Tripathy LN, Forster DMC, and
Timperley WR. (1999) Adult primitive
neuroectodermal tumour. A case report
and review of the literature. British
Journal of Neurosurgery 13:90-92.
Reason for exclusion: Incorrect study
type
Michaels L, Lee K, Manuja SL, and
Soucek SO. (1999) Family with low-
grade neuroendocrine carcinoma of
salivary glands, severe sensorineural
hearing loss, and enamel hypoplasia.
American Journal of Medical Genetics
83:183-186.
Reason for exclusion: Incorrect study
type
Hasegawa T, Kobayashi T, Kida Y,
Tanaka T, Yoshida K, and Osuka K.
(1999) Two cases of facial neurinoma
successfully treated with gamma knife
radiosurgery. Neurological Surgery
27:171-175.
Reason for exclusion: Incorrect study
type
Indira Devi B, Panigrahi M, Jaiswal
VK, Bhat DI, Das S, and Das BS.
(2000) Facial nerve neurinoma
presenting as middle cranial fossa and
cerebellopontine angle mass: A case
report. Neurology India 48:385-387.
Reason for exclusion: Incorrect study
type
Maeta M, Saito R, and Nameki H.
(2001) False-positive magnetic
resonance image in the diagnosis of
small acoustic neuroma. Journal of
Laryngology and Otology 115:842-
844.
Reason for exclusion: Incorrect study
type
Scott A, D'Souza A, Henderson J, and
Morgan DW. (2001) Intracochlea
acoustic neuroma: A case report and
discussion. European Archives of Oto-
Rhino-Laryngology 258:557-559.
Reason for exclusion: Incorrect study
type
Joseph BV and Rajshekhar V. (2002)
Facial myokymia as a presenting
symptom of vestibular schwannoma.
Neurology India 50:369-370.
Reason for exclusion: Incorrect study
type
Chee NWC and Tong HMH. (2002)
Acoustic neuroma presenting as
exercise-induced vertigo. Journal of
Laryngology and Otology 116:630-
632.
Reason for exclusion: Incorrect study
type
Branch MP and Hirsch BE. (2002)
Management of unilateral acoustic
neuroma in a 72-year-old patient with
contralateral congenital deafness.
Otolaryngology - Head and Neck
Surgery 127:483-486.
Reason for exclusion: Incorrect study
type
Meiteles LZ, Liu JK, and Couldwell
WT. (2002) Hearing restoration after
resection of an intracanalicular
vestibular schwannoma: A role for
emergency surgery? Case report and
review of the literature. Journal of
Neurosurgery 96:796-800.
Reason for exclusion: Incorrect study
type
Hegarty JL, Patel S, Fischbein N,
Jackler RK, and Lalwani AK. (2002)
The value of enhanced magnetic
resonance imaging in the evaluation of
endocochlear disease. Laryngoscope
112:8-17.
41
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect study
type
Yuksel H, Odabasi AR, Kafkas S,
Onur E, and Turgut M. (2003)
Clitoromegaly in type 2
neurofibromatosis: A case report and
review of the literature. European
Journal of Gynaecological Oncology
24:447-451.
Reason for exclusion: Incorrect study
type
Ahsan S, Telischi F, Hodges A, and
Balkany T. (2003) Cochlear
implantation concurrent with
translabyrinthine acoustic neuroma
resection. Laryngoscope 113:472-474.
Reason for exclusion: Incorrect study
type
Aarnisalo AA, Suoranta H, and
Ylikoski J. (2004) Magnetic resonance
imaging findings in the auditory
pathway of patients with sudden
deafness. Otology and Neurotology
25:245-249.
Reason for exclusion: Incorrect study
type
Laudadio P, Berni Canani F, and
Cunsolo E. (2004) Meningioma of the
internal auditory canal. Acta Oto-
Laryngologica 124:1231-1234.
Reason for exclusion: Incorrect study
type
Gupta T, Sarin R, Jalali R, and Juvekar
S. (2005) Posterior fossa ependymoma:
Unusual extension into the internal
auditory canal in a 32-year-old woman.
Journal of the Hong Kong College of
Radiologists 8:109-111.
Reason for exclusion: Incorrect study
type
Karagama YG, Bridges LR, and van
Hille PT. (2005) Angioleiomyoma of
the internal auditory meatus: a rare
occurrence in the internal auditory
canal. Ear, nose, & throat journal
84:216, 218.
Reason for exclusion: Incorrect study
type
Deb P, Sharma MC, Gaikwad S, Gupta
A, Mehta VS, and Sarkar C. (2005)
Cerebellopontine angle paraganglioma
- Report of a case and review of
literature. Journal of Neuro-Oncology
74:65-69.
Reason for exclusion: Incorrect study
type
Singh K and Kharrubon B. (2006)
Neurofibromatosis type 2: A case
report. JMS - Journal of Medical
Society 20:153-155.
Reason for exclusion: Incorrect study
type
Wang MT, Chen JC, Tsai TC, Chen
TY, Tzeng WS, Mak CW, Tsai JM,
and Wu TC. (2006) CT and MR
imaging manifestation of
lipochoristomas in internal auditory
canal: A case report. Chinese Journal
of Radiology 31:35-38.
Reason for exclusion: Incorrect study
type
Kernohan MD, Blackmore KJ,
Johnson IJM, and Zammit-Maempel I.
(2006) Magnetic resonance imaging: Is
a single scan ever enough for the
diagnosis of acoustic neuroma?
Journal of Laryngology and Otology
120:1061-1063.
Reason for exclusion: Incorrect study
type
Fayad JN, Don M, and Linthicum J.
(2006) Distribution of low-frequency
nerve fibers in the auditory nerve:
Temporal bone findings and clinical
implications. Otology and Neurotology
27:1074-1077.
Reason for exclusion: Incorrect study
type

42
Screening in ASNHL for acoustic neuroma
Halefoglu AM. (2007)
Neurofibromatosis type 2 associated
with multiple cranial nerve
schwannomas: a case report. Kulak
burun bogaz ihtisas dergisi : KBB =
Journal of ear, nose, and throat
17:171-175.
Reason for exclusion: Incorrect study
type
Zhang J, Kaga K, and Zheng QY.
(2007) Small papillary tumor in the
saccule. International Journal of
Pediatric Otorhinolaryngology Extra
2:107-110.
Reason for exclusion: Incorrect study
type
Nascentes SM, Paulo EADO, De
Andrade EC, Da Silva AL, Vassoler
TMF, and Scanavini ABA. (2007)
Sudden deafness as a presenting
symptom of acoustic neuroma: Case
report. Brazilian Journal of
Otorhinolaryngology 73:713-716.
Reason for exclusion: Incorrect study
type
Amit A, Achawal S, and Dorward N.
(2008) Pituitary macro adenoma and
vestibular schwannoma: A case report
of dual intracranial pathologies. British
Journal of Neurosurgery 22:695-696.
Reason for exclusion: Incorrect study
type
Zanetti D, Campovecchi CB, Pasini S,
and Nassif N. (2008) Simultaneous
translabyrinthine removal of acoustic
neuroma and cochlear implantation.
Auris Nasus Larynx 35:562-568.
Reason for exclusion: Incorrect study
type
Prasai A, Jones SEM, Cross J, and
Moffat DA. (2008) A facial nerve
schwannoma masquerading as a
vestibular schwannoma. Ear, Nose and
Throat Journal 87:E4.
Reason for exclusion: Incorrect study
type
Bush ML, Jones RO, and Shinn JB.
(2008) Auditory brainstem response
threshold differences in patients with
vestibular schwannoma: A new
diagnostic index. Ear, Nose and
Throat Journal 87:458-462.
Reason for exclusion: Incorrect study
type
Prasad J and Cousins VC. (2008)
Asymmetrical hearing loss. Australian
Family Physician 37:312-320.
Reason for exclusion: Incorrect study
type
Schaedler A and Hawkins D. (2008)
Audiologic management of a patient
with a sudden hearing loss and
vestibular Schwannoma in the
contralateral ear. Journal of the
American Academy of Audiology
19:210-214.
Reason for exclusion: Incorrect study
type
Martinez Del Pero M, Moffat D, and
Sudhoff H. (2008) Unusual
presentation of temporal bone
involvement in Churg-Strauss
syndrome. Journal of Laryngology and
Otology 122:425-427.
Reason for exclusion: Incorrect study
type
Shin YR, Choi SJ, Park K, and Choung
YH. (2009) Intralabyrinthine
schwannoma involving the cochlea,
vestibule, and internal auditory canal:
'Canalolabyrinthine schwannoma'.
European Archives of Oto-Rhino-
Laryngology 266:143-145.
Reason for exclusion: Incorrect study
type
Borg E and Lofqvist L. (1982)
Auditory brainstem response (ABR) to
rarefaction and condensation clicks in
43
Screening in ASNHL for acoustic neuroma
normal and abnormal ears.
Scandinavian Audiology 11:227-235.
Reason for exclusion: Incorrect
patient population
Hinojosa R and Marion M. (1983)
Histopathology of profound
sensorineural deafness. Annals of the
New York Academy of Sciences Vol.
405:459-484.
Reason for exclusion: Incorrect
patient population
Jerger S and Jerger J. (1983)
Evaluation of diagnostic audiometric
tests. Audiology 22:144-161.
Reason for exclusion: Incorrect
patient population
Hirsch A. (1983) The stapedius reflex
tests in retrocochlear hearing disorders.
Audiology 22:463-470.
Reason for exclusion: Incorrect
patient population
Mafee MF, Kumar A, and Valvassori
GE. (1985) Diagnostic potential of CT
in neurotological disorders.
Laryngoscope 95:505-514.
Reason for exclusion: Incorrect
patient population
Bergenius J. (1985) Vestibular findings
in sensorineural hearing disorders.
Acta Oto-Laryngologica 99:83-94.
Reason for exclusion: Incorrect
patient population
Campbell KCM and Abbas PJ. (1987)
The effect of stimulus repetition rate
on the auditory brainstem response in
tumor and nontumor patients. Journal
of Speech and Hearing Research
30:494-502.
Reason for exclusion: Incorrect
patient population
Jerger J and Johnson K. (1988)
Interactions of age, gender, and
sensorineural hearing loss on ABR
latency. Ear and Hearing 9:168-176.
Reason for exclusion: Incorrect
patient population
Bonfils P, Uziel A, and Pujol R. (1988)
Evoked oto-acoustic emissions from
adults and infants: Clinical
applications. Acta Oto-Laryngologica
105:445-449.
Reason for exclusion: Incorrect
patient population
Tsirulnikov EM, Vartanyan IA,
Gersuni GV, Rosenblyum AS, Pudov
VI, and Gavrilov LR. (1988) Use of
amplitude-modulated focused
ultrasound for diagnosis of hearing
disorders. Ultrasound in Medicine and
Biology 14:277-285.
Reason for exclusion: Incorrect
patient population
Silverstein H, Norrell H, Smouha E,
and Haberkamp T. (1988) The singular
canal: A valuable landmark in surgery
of the internal auditory canal.
Otolaryngology - Head and Neck
Surgery 98:138-143.
Reason for exclusion: Incorrect
patient population
Dolan KD and Yuh WTC. (1989)
Gadolinium-enhanced facial nerves:
Accompanying bilateral acoustic
tumors in a patient with
neurofibromatosis. Annals of Otology,
Rhinology and Laryngology 98:747-
748.
Reason for exclusion: Incorrect
patient population
Almqvist U, Almqvist B, and Jonsson
KE. (1989) Phase audiometry - A rapid
method for detecting cerebello-pontine
angle tumours? Scandinavian
Audiology 18:155-159.
Reason for exclusion: Incorrect
patient population

44
Screening in ASNHL for acoustic neuroma
Tos M, Trojaborg N, and Thomsen J.
(1989) The contralateral ear after
translabyrinthine removal of acoustic
neuromas: is there a drill-noise
generated hearing loss? Journal of
Laryngology and Otology 103:845-
849.
Reason for exclusion: Incorrect
patient population
Bauch CD and Olsen WO. (1989)
Wave V interaural latency differences
as a function of asymmetry in 2,000-
4,000 Hz hearing sensitivity. American
Journal of Otology 10:389-192.
Reason for exclusion: Incorrect
patient population
Ohlms LA, Lonsbury-Martin BL, and
Martin GK. (1991) Acoustic-distortion
products: Separation of sensory from
neural dysfunction in sensorineural
hearing loss in human beings and
rabbits. Otolaryngology - Head and
Neck Surgery 104:159-174.
Reason for exclusion: Incorrect
patient population
Ogawa K, Kanzaki J, Ogawa S,
Tsuchihashi N, and Yamamoto M.
(1991) Acoustic neuromas with normal
hearing. Acta Oto-Laryngologica,
Supplement 487:144-149.
Reason for exclusion: Incorrect
patient population
Ogawa K, Kanzaki J, Ogawa S,
Tsuchihashi N, and Inoue Y. (1991)
Acoustic neuromas presenting as
sudden hearing loss. Acta Oto-
Laryngologica, Supplement 487:138-
143.
Reason for exclusion: Incorrect
patient population
Souliere J, Kava CR, Barrs DM, and
Bell AF. (1991) Sudden hearing loss as
the sole manifestation of
neurosarcoidosis. Otolaryngology -
Head and Neck Surgery 105:376-381.
Reason for exclusion: Incorrect
patient population
Thompson ME and Abel SM. (1992)
Indices of hearing in patients with
central auditory pathology. II. Choice
response time. Scandinavian
Audiology, Supplement 35:17-22.
Reason for exclusion: Incorrect
patient population
Gstoettner W, Neuwirth-Riedl K,
Swoboda H, Mostbeck W, and Burian
M. (1992) Specificity of auditory
brainstem response audiometry criteria
in acoustic neuroma screening as a
function of deviations of reference
values in patients with cochlear
hearing loss. European Archives of
Oto-Rhino-Laryngology 249:253-256.
Reason for exclusion: Incorrect
patient population
Pappas J, Hoffman RA, Cohen NL,
Holliday RA, and Pappas S. (1993)
Petrous jugular malposition
(diverticulum). Otolaryngology - Head
and Neck Surgery 109:847-852.
Reason for exclusion: Incorrect
patient population
Dufour JJ, Michaud LA, Mohr G,
Pouliot D, and Picard C. (1994)
Intratemporal vascular malformations
(angiomas): Particular clinical features.
Journal of Otolaryngology 23:250-
253.
Reason for exclusion: Incorrect
patient population
Moffat DA, Baguley DM, Von
Blumenthal H, Irving RM, and Hardy
DG. (1994) Sudden deafness in
vestibular schwannoma. Journal of
Laryngology and Otology 108:116-
119.
Reason for exclusion: Incorrect
patient population

45
Screening in ASNHL for acoustic neuroma
Silverstein H, Wanamaker HH,
Rosenberg SI, Crosby N, and Flanzer
JM. (1994) Promontory testing in
neurotologic diagnosis. American
Journal of Otology 15:101-107.
Reason for exclusion: Incorrect
patient population
Jacobson GP, Butcher JA, Newman
CW, and Monsell EM. (1995) When
paroxysmal positioning vertigo isn't
benign. Journal of the American
Academy of Audiology 6:346-349.
Reason for exclusion: Incorrect
patient population
Hulka GF, Bernard EJ, and Pillsbury
HC. (1995) Cochlear implantation in a
patient after removal of an acoustic
neuroma: The implications of magnetic
resonance imaging with gadolinium on
patient management. Archives of
Otolaryngology - Head and Neck
Surgery 121:465-468.
Reason for exclusion: Incorrect
patient population
Lonsbury-Martin BL, Martin GK,
McCoy MJ, and Whitehead ML.
(1995) New approaches to the
evaluation of the auditory system and a
current analysis of otoacoustic
emissions. Otolaryngology - Head and
Neck Surgery 112:50-63.
Reason for exclusion: Incorrect
patient population
Chakrabarti KB, Doughty D, and
Plowman PN. (1996) Stereotactic
multiple arc radiotherapy. II--Cranial
neuroma. British Journal of
Neurosurgery 10:577-583.
Reason for exclusion: Incorrect
patient population
Tono T, Ushisako Y, and Morimitsu T.
(1997) Cochlear implantation in an
intralabyrinthine acoustic neuroma
patient after resection of an
intracanalicular tumor. Advances in
oto-rhino-laryngology 52:155-157.
Reason for exclusion: Incorrect
patient population
Weber PC, Zbar RI, and Gantz BJ.
(1997) Appropriateness of magnetic
resonance imaging in sudden
sensorineural hearing loss.
Otolaryngology - Head and Neck
Surgery 116:153-156.
Reason for exclusion: Incorrect
patient population
Aslan A, De Donato G, Balyan FR,
Falcioni M, Russo A, Taibah A, and
Sanna M. (1997) Clinical observations
on coexistence of sudden hearing loss
and vestibular schwannoma.
Otolaryngology - Head and Neck
Surgery 117:580-582.
Reason for exclusion: Incorrect
patient population
Welling DB, Miles BA, Western L,
and Prior TW. (1997) Detection of
viral DNA in vestibular ganglia tissue
from patients with Meniere's disease.
American Journal of Otology 18:734-
737.
Reason for exclusion: Incorrect
patient population
Swartz JD, Harnsberger HR, and
Mukherji SK. (1998) The temporal
bone: Contemporary diagnostic
dilemmas. Radiologic Clinics of North
America 36:819-853.
Reason for exclusion: Incorrect
patient population
Ravikumar A, Singh P, and Batish VK.
(1999) Vestibular schwanomma with
normal hearing. Indian Journal of
Otolaryngology and Head and Neck
Surgery 51:71-76.
Reason for exclusion: Incorrect
patient population
Sugimoto T, Tsutsumi T, Noguchi Y,
Tsunoda A, Kitamura K, and

46
Screening in ASNHL for acoustic neuroma
Komatsuzaki A. (2000) Relationship
between cystic change and rotatory
vertigo in patients with acoustic
neuroma. Acta Oto-Laryngologica,
Supplement 542:9-12.
Reason for exclusion: Incorrect
patient population
Driscoll CLW, Jackler RK, Pitts LH,
and Brackmann DE. (2000) Lesions of
the internal auditory canal and
cerebellopontine angle in an only
hearing ear: Is surgery ever advisable?
American Journal of Otology 21:573-
581.
Reason for exclusion: Incorrect
patient population
Shaida AM, McFerran DJ, Da Cruz M,
Hardy DG, and Moffat DA. (2000)
Cavernous haemangioma of the
internal auditory canal. Journal of
Laryngology and Otology 114:453-
455.
Reason for exclusion: Incorrect
patient population
Sheykholeslami K, Murofushi T,
Kermany MH, and Kaga K. (2000)
Bone-conducted evoked myogenic
potentials from the
sternocleidomastoid muscle. Acta Oto-
Laryngologica 120:731-734.
Reason for exclusion: Incorrect
patient population
Lesinski-Schiedat A, Frohne C, Illg A,
Rost U, Matthies C, Battmer RD,
Samii M, and Lenarz T. (2000)
Auditory brainstem implant in auditory
rehabilitation of patients with
neurofibromatosis type 2: Hannover
programme. Journal of Laryngology
and Otology 114:15-17.
Reason for exclusion: Incorrect
patient population
Adams WM. (2002) Imaging of the
cerebellopontine angle. CME Journal
Radiology 3:58-65.
Reason for exclusion: Incorrect
patient population
Anyanwu E, Campbell AW, and High
W. (2002) Brainstem auditory evoked
response in adolescents with acoustic
mycotic neuroma due to environmental
exposure to toxic molds. International
Journal of Adolescent Medicine and
Health 14:67-76.
Reason for exclusion: Incorrect
patient population
Al Sebeih K and Zeitouni A. (2002)
Vestibular-evoked myogenic potentials
as a test of otolith function. Medical
Principles and Practice 11:136-140.
Reason for exclusion: Incorrect
patient population
Hilton MP, Kaplan DM, Ang L, and
Chen JM. (2002) Facial nerve paralysis
and meningioma of the internal
auditory canal. Journal of Laryngology
and Otology 116:132-134.
Reason for exclusion: Incorrect
patient population
Eckhardt-Henn A, Breuer P,
Thomalske C, Hoffmann SO, and Hopf
HC. (2003) Anxiety disorders and
other psychiatric subgroups in patients
complaining of dizziness. Journal of
Anxiety Disorders 17:369-388.
Reason for exclusion: Incorrect
patient population
Lonsbury-Martin BL and Martin GK.
(2003) Otoacoustic emissions. Current
Opinion in Otolaryngology and Head
and Neck Surgery 11:361-366.
Reason for exclusion: Incorrect
patient population
Larson TL. (2003) Understanding the
posttreatment imaging appearance of
the internal auditory canal and
cerebellopontine angle. Seminars in
Ultrasound CT and MRI 24:133-146.

47
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect
patient population
Huang MY and Vermeulen S. (2003)
Clinical perspectives regarding patients
with internal auditory canal or
cerebellopontine angle lesions:
Surgical and radiation oncology
perspectives. Seminars in Ultrasound
CT and MRI 24:124-132.
Reason for exclusion: Incorrect
patient population
Baguley DM, Jones SEM, and Moffat
DA. (2003) A small vestibular
schwannoma arising from the inferior
vestibular nerve. Journal of
Laryngology and Otology 117:498-
500.
Reason for exclusion: Incorrect
patient population
Chandrasekhar SS. (2003) Updates on
methods to treat sudden hearing loss.
Operative Techniques in
Otolaryngology - Head and Neck
Surgery 14:288-292.
Reason for exclusion: Incorrect
patient population
Kania RE, Herman P, and Tran Ba
Huy P. (2004) Vestibular-like facial
nerve schwannoma. Auris Nasus
Larynx 31:212-219.
Reason for exclusion: Incorrect
patient population
Abdelkader M, McEwan M, and
Cooke L. (2004) Prospective
evaluation of the value of direct
referral hearing aid clinic in
management of young patients with
bilateral hearing loss. Clinical
Otolaryngology and Allied Sciences
29:206-209.
Reason for exclusion: Incorrect
patient population
Jombik P and Bahyl V. (2005) Short
latency disconjugate vestibulo-ocular
responses to transient stimuli in the
audio frequency range. Journal of
Neurology, Neurosurgery and
Psychiatry 76:1398-1402.
Reason for exclusion: Incorrect
patient population
Shah RK, Blevins NH, and Karmody
CS. (2005) Mid-frequency
sensorineural hearing loss: Aetiology
and prognosis. Journal of Laryngology
and Otology 119:529-533.
Reason for exclusion: Incorrect
patient population
Choi KD, Cho HJ, Koo JW, Park SH,
and Kim JS. (2005) Hyperventilation-
induced nystagmus in vestibular
schwannoma. Neurology 64:2062.
Reason for exclusion: Incorrect
patient population
Sauvaget E, Kici S, Kania R, Herman
P, and Huy PTB. (2005) Sudden
sensorineural hearing loss as a
revealing symptom of vestibular
schwannoma. Acta Oto-Laryngologica
125:592-595.
Reason for exclusion: Incorrect
patient population
Cadoni G, Agostino S, Scipione S,
Ippolito S, Caselli A, Marchese R, and
Paludetti G. (2005) Sudden
sensorineural hearing loss: Our
experience in diagnosis, treatment, and
outcome. Journal of Otolaryngology
34:395-401.
Reason for exclusion: Incorrect
patient population
Amiridavan M, Nemati S, Hashemi
SM, Jamshidi M, Saberi A, and Asadi
M. (2006) Otoacoustic emissions and
auditory brainstem responses in patiens
with sudden sensorineural hearing loss.
Do otoacoustic emissions have
prognostic value? Journal of Research
in Medical Sciences 11:263-269.

48
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect
patient population
Cadoni G, Cianfoni A, Agostino S,
Scipione S, Tartaglione T, Galli J, and
Colosimo C. (2006) Magnetic
resonance imaging findings in sudden
sensorineural hearing loss. Journal of
Otolaryngology 35:310-316.
Reason for exclusion: Incorrect
patient population
Khrais T and Sanna M. (2006) Hearing
preservation surgery in vestibular
schwannoma. The Journal of
laryngology and otology. 120:366-370.
Reason for exclusion: Incorrect
patient population
Chen CC, Cheng PW, Tseng HM, and
Young YH. (2006) Posterior cranial
fossa tumors in young adults.
Laryngoscope 116:1678-1681.
Reason for exclusion: Incorrect
patient population
Lenarz T, Lim HH, Reuter G, Patrick
JF, and Lenarz M. (2006) The auditory
midbrain implant: A new auditory
prosthesis for neural deafness-concept
and device description. Otology and
Neurotology 27:838-843.
Reason for exclusion: Incorrect
patient population
Sone M, Katayama N, Otake N, Sato
E, Fujimoto Y, Ito M, and Nakashima
T. (2007) Characterizing the auditory
changes in tumor metastasis to the
bilateral internal auditory canals.
Journal of Clinical Neuroscience
14:470-473.
Reason for exclusion: Incorrect
patient population
Poh ACC and Tiong YT. (2007)
Sudden deafness due to
intralabyrinthine haemorrhage: A
possible rare late complication of head
and neck irradiation. Annals of the
Academy of Medicine Singapore
36:78-82.
Reason for exclusion: Incorrect
patient population
Tringali S, Grayeli AB, Bouccara D,
Sterkers O, Chardon S, Martin C, and
Dubreuil C. (2008) A survey of
satisfaction and use among patients
fitted with a BAHA. European
Archives of Oto-Rhino-Laryngology
265:1461-1464.
Reason for exclusion: Incorrect
patient population
Wenzel GI, Gotz F, Lenarz T, and
Stover T. (2008) HIV-associated
cerebral lymphocyte infiltration
mimicking vestibular schwannoma.
European Archives of Oto-Rhino-
Laryngology 265:1567-1571.
Reason for exclusion: Incorrect
patient population
Tringali S, Marzin A, Dubreuil C, and
Ferber-Viart C. (2008) Bone-anchored
hearing aid in unilateral inner ear
deafness: Electrophysiological results
in patients following vestibular
schwannoma removal. Acta Oto-
Laryngologica 128:1203-1210.
Reason for exclusion: Incorrect
patient population
Balbani AP and Montovani JC. (2008)
Mobile phones: influence on auditory
and vestibular systems. Revista
brasileira de otorrinolaringologia
(English ed. ) 74:125-131.
Reason for exclusion: Incorrect
patient population
Djupesland G, Flottorp G, Modalsli B,
Tvete O, and Sortland O. (1981)
Acoustic brain stem response in
diagnosis of acoustic neuroma.
Scandinavian Audiology, Supplement
13:109-112.
Reason for exclusion: Incorrect
disease

49
Screening in ASNHL for acoustic neuroma
Sataloff RT. (1986) Sensorineural
hearing loss. Otolaryngologic Clinics
of North America 19:3-37.
Reason for exclusion: Incorrect
disease
Dauman R, Aran JM, and Portmann M.
(1988) Limits of ABR and contribution
of transtympanic electrocochleography
in the assessment of cerebellopontine
angle tumours. Clinical
Otolaryngology and Allied Sciences
13:107-114.
Reason for exclusion: Incorrect
disease
Papsin BC and Abel SM. (1988)
Temporal summation in hearing-
impaired listeners. Journal of
Otolaryngology 17:93-100.
Reason for exclusion: Incorrect
disease
Gleeson MJ, Cox TCS, and Strong AJ.
(1989) Aneurysm of the anterior
inferior cerebellar artery mimicking an
intracanalicular acoustic neuroma.
Journal of Laryngology and Otology
103:107-110.
Reason for exclusion: Incorrect
disease
Martin GK, Ohlms LA, Franklin DJ,
Harris FP, and Lonsbury-Martin BL.
(1990) Distortion product emissions in
humans. III. Influence of sensorineural
hearing loss. Annals of Otology,
Rhinology and Laryngology 99:30-42.
Reason for exclusion: Incorrect
disease
Litt AW, Mirsky P, Berson BD, and
Kricheff II. (1991) Screening protocol
for MR imaging of the internal
auditory canal. Journal of Computer
Assisted Tomography 15:930-933.
Reason for exclusion: Incorrect
disease
Anand VT, Byrnes DP, Walby AP, and
Kerr AG. (1993) Bilateral acoustic
neuromas. Clinical Otolaryngology
and Allied Sciences 18:365-371.
Reason for exclusion: Incorrect
disease
Mark AS, Seltzer S, and Harnsberger
HR. (1993) Sensorineural hearing loss:
More than meets the eye? American
Journal of Neuroradiology 14:37-45.
Reason for exclusion: Incorrect
disease
Mukerji B, Estrem SA, and O'Sullivan
FX. (1994) The challenge of
sensorineural hearing loss in
rheumatoid arthritis. Journal of
Rheumatology 21:1753-1757.
Reason for exclusion: Incorrect
disease
Lustig LR, Jackler RK, and Chen DA.
(1995) Contralateral hearing loss after
neurotologic surgery. Otolaryngology -
Head and Neck Surgery 113:276-282.
Reason for exclusion: Incorrect
disease
Weissman JL. (1996) Hearing loss.
Radiology 199:593-611.
Reason for exclusion: Incorrect
disease
Baguley DM, Beynon GJ, Grey PL,
Hardy DG, and Moffat DA. (1997)
Audio-vestibular findings in
meningioma of the cerebellopontine
angle: A retrospective review. Journal
of Laryngology and Otology 111:1022-
1026.
Reason for exclusion: Incorrect
disease
Zbar RIS, Megerian CA, Khan A, and
Rubinstein JT. (1997) Invisible culprit:
Intralabyrinthine schwannomas that do
not appear on enhanced magnetic
resonance imaging. Annals of Otology,
Rhinology and Laryngology 106:739-
50
Screening in ASNHL for acoustic neuroma
742.
Reason for exclusion: Incorrect
disease
Daniels RL, Swallow C, Shelton C,
Davidson HC, Krejci CS, and
Harnsberger HR. (2000) Causes of
unilateral sensorineural hearing loss
screened by high- resolution fast spin
echo magnetic resonance imaging:
Review of 1,070 consecutive cases.
American Journal of Otology 21:173-
180.
Reason for exclusion: Incorrect
disease
Ramsden R and Saeed S. (2000) The
future of ORL-HNS and associated
specialities series: The future of neuro-
otology. Journal of Laryngology and
Otology 114:89-92.
Reason for exclusion: Incorrect
disease
Huang TW and Young YH. (2002)
Differentiation between
cerebellopontine angle tumors in
cancer patients. Otology &
neurotology : official publication of the
American Otological Society,
American Neurotology Society [and]
European Academy of Otology and
Neurotology 23:975-979.
Reason for exclusion: Incorrect
disease
Mendez JC, Saucedo G, Ruiz P, Vega
A, and Nombela L. (2002) Lipoma of
the internal auditory canal: MR
findings [2]. European Radiology
12:703-704.
Reason for exclusion: Incorrect
disease
Glastonbury CM, Davidson HC,
Harnsberger HR, Butler J, Kertesz TR,
and Shelton C. (2002) Imaging
findings of cochlear nerve deficiency.
American Journal of Neuroradiology
23:635-643.
Reason for exclusion: Incorrect
disease
Rebol J, Munda A, and Tos M. (2004)
Hyperpneumatization of the temporal,
occipital and parietal bones. European
Archives of Oto-Rhino-Laryngology
261:445-448.
Reason for exclusion: Incorrect
disease
Oghalai JS, Ramirez AL, Hegarty JL,
and Jackler RK. (2004) Chronic
pachymeningitis presenting as
asymmetric sensorineural hearing loss.
Otology and Neurotology 25:616-621.
Reason for exclusion: Incorrect
disease
Crummer RW and Hassan GA. (2004)
Diagnostic Approach to Tinnitus.
American Family Physician 69:120-
126+127.
Reason for exclusion: Incorrect
disease
Marcucci R, Liotta AA, Cellai AP,
Rogolino A, Berloco P, Leprini E,
Pagnini P, Abbate R, and Prisco D.
(2005) Cardiovascular and
thrombophilic risk factors for
idiopathic sudden sensorineural
hearing loss. Journal of Thrombosis
and Haemostasis 3:929-934.
Reason for exclusion: Incorrect
disease
Sen A, Khan MIJ, Ramsden RT, and
Gillespie JE. (2005) Stenosis of the
internal auditory meatus masquerading
as bilateral vestibular schwannomas: A
cautionary tale. Journal of
Laryngology and Otology 119:995-
997.
Reason for exclusion: Incorrect
disease
Gonul E, Izci Y, and Onguru O. (2007)
Arachnoid cyst of the cerebellopontine
angle associated with gliosis of the

51
Screening in ASNHL for acoustic neuroma
eighth cranial nerve. Journal of
Clinical Neuroscience 14:700-702.
Reason for exclusion: Incorrect
disease
Preuss M, Stein M, Huegens-Penzel
M, Kuchelmeister K, and Nestler U.
(2008) Metastatic tumours mimicking
vestibular schwannoma. Acta
Neurochirurgica 150:915-919.
Reason for exclusion: Incorrect
disease
Muzzi E, Rinaldo A, and Ferlito A.
(2008) Meniere disease: diagnostic
instrumental support. American
Journal of Otolaryngology - Head and
Neck Medicine and Surgery 29:188-
194.
Reason for exclusion: Incorrect
disease
Neely JG, Britton BH, and Greenberg
SD. (1976) Microscopic characteristics
of the acoustic tumor in relationship of
its nerve of origin. Laryngoscope
86:984-991.
Reason for exclusion: Incorrect
intervention/outcomes
Mathew GD, Facer GW, Suh KW,
Houser OW, and O'Brien PC. (1978)
Symptoms, findings, and methods of
diagnosis in patients with acoustic
neuroma. Laryngoscope 88:1893-1903,
1921.
Reason for exclusion: Incorrect
intervention/outcomes
Nager GT. (1984) Neurinomas of the
trigeminal nerve. American Journal of
Otolaryngology - Head and Neck
Medicine and Surgery 5:301-333.
Reason for exclusion: Incorrect
intervention/outcomes
Valvassori GE. (1984) Radiologic
evaluation of eighth nerve tumors.
American Journal of Otolaryngology -
Head and Neck Medicine and Surgery
5:270-280.
Reason for exclusion: Incorrect
intervention/outcomes
Sturzebecher E, Kevanishvili Z, and
Werbs M. (1985) Interpeak intervals of
auditory brainstem response, interaural
differences in normal-hearing subjects
and patients with sensorineural hearing
loss. Scandinavian Audiology 14:83-
87.
Reason for exclusion: Incorrect
intervention/outcomes
Mikaelian DO, Eyyunni U, Osterholm
J, Fariello R, and Jassal SP. (1985)
Hearing preservation in surgery for
acoustic neuroma. Transactions -
Pennsylvania Academy of
Ophthalmology and Otolaryngology
37:255-258.
Reason for exclusion: Incorrect
intervention/outcomes
Jay WM and Williamson MR. (1987)
Incidence of subcortical lesions not
increased in nonarteritic ischemic optic
neuropathy on magnetic resonance
imaging. American Journal of
Ophthalmology 104:398-400.
Reason for exclusion: Incorrect
intervention/outcomes
Symon L, Sabin HI, Bentivoglio P,
Cheesman AD, Prasher D, and Barratt
H. (1988) Intraoperative monitoring of
the electrocochleogram and the
preservation of hearing during acoustic
neuroma excision. Acta
Neurochirurgica, Supplement 42:27-
30.
Reason for exclusion: Incorrect
intervention/outcomes
Clemis JD, Toriumi DM, and Gavron
JP. (1988) Otosclerosis masking
coexistent acoustic neuroma. American
Journal of Otology 9:117-121.
Reason for exclusion: Incorrect
intervention/outcomes

52
Screening in ASNHL for acoustic neuroma
Armington WG, Harnsberger HR,
Smoker WRK, and Osborn AG. (1988)
Normal and diseased acoustic
pathway: Evaluation with MR
imaging. Radiology 167:509-515.
Reason for exclusion: Incorrect
intervention/outcomes
Tos M, Thomsen J, and Harmsen A.
(1988) Is preservation of hearing in
acoustic neuroma worthwhile? Acta
Oto-Laryngologica, Supplement
452:57-68.
Reason for exclusion: Incorrect
intervention/outcomes
Moffat DA, Baguley DM, Hardy DG,
and Tsui YN. (1989) Contralateral
auditory brainstem response
abnormalities in acoustic neuroma.
Journal of Laryngology and Otology
103:835-838.
Reason for exclusion: Incorrect
intervention/outcomes
Benecke J. (1989) Diagnosis and
management of acoustic tumors: An
overview. Seminars in Hearing
10:307-312.
Reason for exclusion: Incorrect
intervention/outcomes
Ohlms LA, Lonsbury-Martin BL, and
Martin GK. (1990) The clinical
application of acoustic distortion
products. Otolaryngology - Head and
Neck Surgery 103:52-59.
Reason for exclusion: Incorrect
intervention/outcomes
Hutman S. (1991) New approaches to
acoustic neuroma surgery. Journal of
clinical laser medicine & surgery
9:168-175.
Reason for exclusion: Incorrect
intervention/outcomes
Ogawa K, Kanzaki J, Ogawa S,
Tsuchihashi N, and Ikeda S. (1991)
Progression of hearing loss in acoustic
neuromas. Acta Oto-Laryngologica,
Supplement 487:133-137.
Reason for exclusion: Incorrect
intervention/outcomes
Hoffman RA, Kohan D, and Cohen
NL. (1992) Cochlear implants in the
management of bilateral acoustic
neuromas. American Journal of
Otology 13:525-528.
Reason for exclusion: Incorrect
intervention/outcomes
Shusterman D, Handler SD, Marsh
RR, Bilaniuk L, and Tom LWC.
(1992) Usefulness of computed
tomographic scan in the evaluation of
sensorineural hearing loss in children.
Archives of Otolaryngology - Head
and Neck Surgery 118:501-503.
Reason for exclusion: Incorrect
intervention/outcomes
Helms J. (1992) Hearing preservation
in acoustic neurinoma surgery.
Otolaryngologia Polska 46:533-537.
Reason for exclusion: Incorrect
intervention/outcomes
Shaan M, Vassalli L, Landolfi M,
Taibah A, Russo A, and Sanna M.
(1993) Atypical presentation of
acoustic neuroma. Otolaryngology -
Head and Neck Surgery 109:865-870.
Reason for exclusion: Incorrect
intervention/outcomes
Florentine M, Reed CM, Rabinowitz
WM, Braida LD, Durlach NI, and
Buus S. (1993) Intensity perception.
XIV. Intensity discrimination in
listeners with sensorineural hearing
loss. Journal of the Acoustical Society
of America 94:2575-2586.
Reason for exclusion: Incorrect
intervention/outcomes
Bu-Saba NY, Rebeiz EE, Salman SD,
Thornton AR, and West C. (1994)
Significance of false-positive auditory

53
Screening in ASNHL for acoustic neuroma
brainstem response: A clinical study.
American Journal of Otology 15:233-
236.
Reason for exclusion: Incorrect
intervention/outcomes
Mark AS. (1994) Contrast-enhanced
magnetic resonance imaging of the
temporal bone. Neuroimaging Clinics
of North America 4:117-131.
Reason for exclusion: Incorrect
intervention/outcomes
Moller A, Mytseth E, Jensen O, and
and-Pedersen PH. (1995) Acoustic
Neuroma: Observation, Surgery or
Gamma-knife treatment. 2nd.
International Conference on Acoustic.
Neuroma. Surgery and 2nd. European
Skull. Base. Society Congress. . Paris,
France, 22. 26. April. , 1995.68,
Abstract.
Reason for exclusion: Incorrect
intervention/outcomes
Walsted A, Salomon G, Thomsen J,
and Tos M. (1996) Cerebrospinal fluid
loss and threshold changes. 1. Hearing
loss in the contralateral ear after
operation for acoustic neuroma: an
analysis of the incidence, time course,
frequency range, size and
pathophysiological considerations.
Audiology & neuro-otology 1:247-255.
Reason for exclusion: Incorrect
intervention/outcomes
Tanaka H, Komatsuzaki A, and
Hentona H. (1996) Usefulness of
auditory brainstem responses at high
stimulus rates in the diagnosis of
acoustic neuroma. ORL 58:224-228.
Reason for exclusion: Incorrect
intervention/outcomes
Nadol J, Diamond PF, and Thornton
AR. (1996) Correlation of hearing loss
and radiologic dimensions of
vestibular schwannomas (acoustic
neuromas). American Journal of
Otology 17:312-316.
Reason for exclusion: Incorrect
intervention/outcomes
Held P, Fellner C, Fellner F, Seitz J,
Graf S, Hilbert M, and Strutz J. (1997)
MRI of inner ear and facial nerve
pathology using 3D MP-RAGE and
3D CISS sequences. The British
Journal of Radiology 70:558-566.
Reason for exclusion: Incorrect
intervention/outcomes
Hung TY, Litofsky NS, Smith TW,
and Megerian CA. (1997) Ganglionic
hamartoma of the intracanalicular
acoustic nerve causing sensorineural
hearing loss. American Journal of
Otology 18:498-500.
Reason for exclusion: Incorrect
intervention/outcomes
Davis NL, Rappaport JM, and
MacDougall JC. (1997) Cochlear and
auditory brainstem implants in the
management of acoustic neuroma and
bilateral acoustic neurofibromatosis.
McGill Journal of Medicine 3:115-120.
Reason for exclusion: Incorrect
intervention/outcomes
Heier LA, Comunale J, and Lavyne
MH. (1997) Sensorineural hearing loss
and cerebellopontine angle lesions. Not
always an acoustic neuroma - A
pictorial essay. Clinical Imaging
21:213-223.
Reason for exclusion: Incorrect
intervention/outcomes
Mangham CA. (1997) Expert opinion
on the diagnosis of acoustic tumors.
Otolaryngology - Head and Neck
Surgery 117:622-627.
Reason for exclusion: Incorrect
intervention/outcomes
Qiu WW, Stucker FJ, and Welsh LW.
(1998) Clinical interpretations of
transient otoacoustic emissions.

54
Screening in ASNHL for acoustic neuroma
American Journal of Otolaryngology -
Head and Neck Medicine and Surgery
19:370-378.
Reason for exclusion: Incorrect
intervention/outcomes
Ross GJ. (1998) Acoustic neuroma
(vestibular schwannoma). New
England Journal of Medicine
339:1440.
Reason for exclusion: Incorrect
intervention/outcomes
Marple BF, Milchbrub S, Meyerhoff
WL, and Roland PS. (1998)
Necrotizing granulomatous
inflammation of the superior vestibular
nerve mimicking an acoustic neuroma.
Otolaryngology - Head and Neck
Surgery 118:862-865.
Reason for exclusion: Incorrect
intervention/outcomes
Poen JC, Golby AJ, Forster KM,
Martin DP, Chinn DM, Hancock SL,
Adler JR, Gutin PH, Lunsford LD,
Friedman WA, Samii M, and Matthies
C. (1999) Fractionated stereotactic
radiosurgery and preservation of
hearing in patients with vestibular
schwannoma: A preliminary report.
Neurosurgery 45:1299-1307.
Reason for exclusion: Incorrect
intervention/outcomes
Yokoyama K, Nishida H, Noguchi Y,
and Komatsuzaki A. (1999) Hearing
impairment in patients with acoustic
neuroma - Analysis by
electrocochleography. Auris Nasus
Larynx 26:401-409.
Reason for exclusion: Incorrect
intervention/outcomes
Hellman RP. (1999) Cross-modality
matching: A tool for measuring
loudness in sensorineural impairment.
Ear and Hearing 20:193-213.
Reason for exclusion: Incorrect
intervention/outcomes
Haapaniemi J, Laurikainen E,
Johansson R, Miettinen S, and Varpula
M. (2000) Cochleovestibular
symptoms related to the site of
vestibular schwannoma. Acta Oto-
Laryngologica, Supplement 543:14-16.
Reason for exclusion: Incorrect
intervention/outcomes
Quaranta A, Gandolfi A, Fava G,
Quaranta N, and Zini C. (2000)
Paradoxical effects of contralateral
white noise on evoked otoacoustic
emissions in ears with acoustic
neuroma. Acta Oto-Laryngologica
120:227-230.
Reason for exclusion: Incorrect
intervention/outcomes
Eisenman DJ and Arts HA. (2000)
Effectiveness of treatment for sudden
sensorineural hearing loss. Archives of
Otolaryngology - Head and Neck
Surgery 126:1161-1164.
Reason for exclusion: Incorrect
intervention/outcomes
Harner SG, Fabry DA, and Beatty CW.
(2000) Audiometric findings in
patients with acoustic neuroma.
American Journal of Otology 21:405-
411.
Reason for exclusion: Incorrect
intervention/outcomes
Noguchi Y, Komatsuzaki A, and
Nishida H. (2000)
Electrocochleographic study in patients
with vestibular schwannomas and U-
shaped audiograms. Audiology 39:19-
23.
Reason for exclusion: Incorrect
intervention/outcomes
Klingebiel R, Bockmuhl U, Werbs M,
Freigang B, Vorwerk W, Thieme N,
and Lehmann R. (2001) Visualization
of inner ear dysplasias in patients with
sensorineural hearing loss. Acta
Radiologica 42:574-581.

55
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect
intervention/outcomes
Kallinen J, Laurikainen E, Bergroth L,
and Grenman R. (2001) A follow-up
study of patients suffering from sudden
sensorineural hearing loss. Acta Oto-
Laryngologica 121:818-822.
Reason for exclusion: Incorrect
intervention/outcomes
Friedman RA, Kesser BW, Slattery
3rd. WH, Brackmann DE, and
Hitselberger WE. (2001) Hearing
preservation in patients with vestibular
schwannomas with sudden
sensorineural hearing loss.
Otolaryngology - Head and Neck
Surgery 125:544-551.
Reason for exclusion: Incorrect
intervention/outcomes
Zubay G and Porter RW. (2001)
Preoperative assessment of patients
with acoustic neuromas. Operative
Techniques in Neurosurgery 4:11-18.
Reason for exclusion: Incorrect
intervention/outcomes
Kothari P and Kukreja N. (2001)
Intratympanic dexamethasone for
sudden sensorineural hearing loss:
Clinical and laboratory evaluation.
Chandrasekhar SS. Otology &
Neurotology 2001; 22: 18-23. CME
Bulletin Otorhinolaryngology Head
and Neck Surgery 5:108-109.
Reason for exclusion: Incorrect
intervention/outcomes
Magliulo G, Zardo F, Bertin S,
D'Amico R, and Savastano V. (2002)
Meningiomas of the internal auditory
canal: Two case reports. Skull Base
12:19-26.
Reason for exclusion: Incorrect
intervention/outcomes
Jereczek-Fossa BA, Zarowski A,
Milani F, and Orecchia R. (2003)
Radiotherapy-induced ear toxicity.
Cancer Treatment Reviews 29:417-
430.
Reason for exclusion: Incorrect
intervention/outcomes
Magliulo G, Gagliardi M, Appiani GC,
and D'Amico R. (2003) Preservation of
the saccular nerve and of the vestibular
evoked myogenic potential during
vestibular schwannoma surgery.
Otology and Neurotology 24:308-311.
Reason for exclusion: Incorrect
intervention/outcomes
Niparko JK, Cox KM, and Lustig LR.
(2003) Comparison of the bone
anchored hearing aid implantable
hearing device with contralateral
routing of offside signal amplification
in the rehabilitation of unilateral
deafness. Otology and Neurotology
24:73-78.
Reason for exclusion: Incorrect
intervention/outcomes
Nikolopoulos TP and Kiprouli K.
(2004) Cochlear implant surgery in
challenging cases. Cochlear Implants
International 5:56-63.
Reason for exclusion: Incorrect
intervention/outcomes
Hol MKS, Bosman AJ, Snik AFM,
Mylanus EAM, and Cremers CWRJ.
(2004) Bone-anchored hearing aid in
unilateral inner ear deafness: A study
of 20 patients. Audiology and Neuro-
Otology 9:274-281.
Reason for exclusion: Incorrect
intervention/outcomes
Mawman DJ, Bhatt YM, Green KMJ,
O'Driscoll MP, Saeed SR, and
Ramsden RT. (2004) Trends and
outcomes in the Manchester adult
cochlear implant series. Clinical
Otolaryngology and Allied Sciences
29:331-339.

56
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect
intervention/outcomes
Rutherford SA and King AT. (2005)
Vestibular schwannoma management:
what is the 'best' option? (Brief
record). British Journal of
Neurosurgery 19:309-316.
Reason for exclusion: Incorrect
intervention/outcomes
Magliulo G, D'Amico R, Celebrini A,
and Cuiuli G. (2005) Postoperative
Ramsay-Hunt syndrome after acoustic
neuroma resection. Viral reactivation.
Anales otorrinolaringologicos ibero-
americanos 32:253-259.
Reason for exclusion: Incorrect
intervention/outcomes
Moller AR. (2006) History of cochlear
implants and auditory brainstem
implants. Møller AR (ed): Cochlear
and Brainstem Implants. Adv
Otorhinolaryngoll 64:1–10
Reason for exclusion: Incorrect
intervention/outcomes
Sazgar AA, Akrami K, Akrami S, and
Karimi Yazdi AR. (2006) Recording of
vestibular evoked myogenic potentials.
Acta Medica Iranica 44:13-16.
Reason for exclusion: Incorrect
intervention/outcomes
Mazzoni A, Dubey SP, Poletti AM,
and Colombo G. (2007) Sporadic
acoustic neuroma in pediatric patients.
International Journal of Pediatric
Otorhinolaryngology 71:1569-1572.
Reason for exclusion: Incorrect
intervention/outcomes
Mackle T, Rawluk D, and McConn
Walsh R. (2007) Atypical clinical
presentations of vestibular
schwannomas. Otology and
Neurotology 28:526-528.
Reason for exclusion: Incorrect
intervention/outcomes
Neff BA, Wiet RM, Lasak JM, Cohen
NL, Pillsbury HC, Ramsden RT, and
Welling DB. (2007) Cochlear
implantation in the neurofibromatosis
type 2 patient: Long-term follow-up.
Laryngoscope 117:1069-1072.
Reason for exclusion: Incorrect
intervention/outcomes
Ubell ML, Ho KC, Meyer GA, and
Friedland DR. (2007) Simultaneous
astrocytoma and vestibular
schwannoma arising from the
vestibulocochlear nerve. Otology and
Neurotology 28:286-287.
Reason for exclusion: Incorrect
intervention/outcomes
House JW and Kutz J. (2007) Bone-
anchored hearing aids: Incidence and
management of postoperative
complications. Otology and
Neurotology 28:213-217.
Reason for exclusion: Incorrect
intervention/outcomes
Penido NDO, Tangerina RP, Kosugi
EM, De Abreu CEC, and Vasco MB.
(2007) Vestibular Schwannoma:
Spontaneous tumor involution.
Brazilian Journal of
Otorhinolaryngology 73:867-871.
Reason for exclusion: Incorrect
intervention/outcomes
Liu JK, Sayama CM, Shelton C, and
MacDonald JD. (2007) Transient facial
nerve palsy after topical papaverine
application during vestibular
schwannoma surgery: Case report.
Journal of Neurosurgery 107:1039-
1042.
Reason for exclusion: Incorrect
intervention/outcomes
Shelfer J, Zapala D, and Lundy L.
(2008) Fall risk, vestibular
schwannoma, and anticoagulation
therapy. Journal of the American
Academy of Audiology 19:237-245.

57
Screening in ASNHL for acoustic neuroma
Reason for exclusion: Incorrect
intervention/outcomes
Margolis RH and Saly GL. (2008)
Asymmetric hearing loss: definition,
validation, and prevalence. Otology &
neurotology : official publication of the
American Otological Society,
American Neurotology Society [and]
European Academy of Otology and
Neurotology 29:422-431.
Reason for exclusion: Incorrect
intervention/outcomes
Toh EH and Luxford WM. (2008)
Cochlear and Brainstem Implantation.
Neurosurgery Clinics of North
America 19:317-329.
Reason for exclusion: Incorrect
intervention/outcomes
Bischoff B, Romstock J, Fahlbusch R,
Buchfelder M, and Strauss C. (2008)
Intraoperative brainstem auditory
evoked potential pattern and
perioperative vasoactive treatment for
hearing preservation in vestibular
schwannoma surgery. Journal of
Neurology, Neurosurgery, and
Psychiatry 79:170-175.
Reason for exclusion: Incorrect
intervention/outcomes
Dell'Aringa AHB, Sena LFP, Teixeira
R, Dell'Aringa AR, and Nardi JC.
(2008) The importance of the auditory
evoked potential in acoustic neuromas.
Brazilian Journal of
Otorhinolaryngology 74:639.
Reason for exclusion: Incorrect
intervention/outcomes


















