A publication for pediatric caregivers from Children’s ...
5
www.childrenshospital.org Pediatric Views A publication for pediatric caregivers from Children’s Hospital Boston New Pediatric Specialist Guide T he 2006–2007 Pediatric Specialist Guide (PSG), an easy-to-use directory to assist you in con- tacting the appropriate specialist at Children’s Hospital Boston, is now available. The guide is organized by specialty/subspecialty and provides quick access to basic contact information for our spe- cialists, including telephone and fax numbers, email addresses, office locations and directions/maps to Children’s. In addition, the PSG provides department/ division descriptions, guidelines on how to refer a patient, accepted health insurance, and more. All PSG information is also available online by visiting www.childrenshospital.org and clicking on “Find a Specialist.” Additional information, such as a specialist’s education/training history, professional experience, curriculum vitae and community-based office locations, can be found as part of our online physician profiles. A “Print-On-Demand” feature allows you to gener- ate a PDF file of the most up-to-date information, whether you’d like to print the entire guide or just one department/division. We also offer a new op- tion to download the PSG—the entire directory or a particular department—to your personal digital assistant. You will receive a copy of the 2006-2007 PSG by mail. To request additional copies, send your mailing address to [email protected]. www.childrenshospital.org/views W hen 13-year-old Nichole Paone awoke one chilly morning in November, something just wasn’t right. She’d been lethargic for several days prior, experiencing a tingling sensation in her head and some mild vomiting. But that particular Tuesday, she was looking almost yellow. Nichole had been in and out of her pediatrician’s office all month, undergoing several tests to determine what was causing her symptoms. When the tests turned up empty, she was eventually referred to a neurologist, but the appointment wasn’t for another few days. But that wasn’t soon enough for her mother, Michelle, who had been watching her little girl’s symptoms change and get worse over the weeks. So, she brought Nichole to Children’s Hospital Boston’s emergency room later that day. A CT scan revealed that Nichole had a tumor the size of a baseball lodged in the back of her brain. “The tumor was a juvenile pilocytic astrocytoma (JPA),” says neurosurgeon Liliana Goumnerova, MD. “This is probably the most common tumor in that location in children. There are no known causes of JPA; it is believed to occur sporadically.” Nichole, who wants to be a veterinarian, took her diagnosis in stride. When told she had a brain tumor, she described, in great detail, a brain operation she had MR-OR in action ››› continued on page 6 Liliana Goumnerova, MD, gives patient Nichole Paone a clean bill of health. PSG with Neurosurgeon- in-Chief R. Michael Scott, MD, in our MR-OR.
Transcript of A publication for pediatric caregivers from Children’s ...

www.childrenshospital.org
Pediatric ViewsA publication for pediatric caregivers from Children’s Hospital Boston
New PediatricSpecialist Guide
The 2006–2007 Pediatric Specialist Guide (PSG),
an easy-to-use directory to assist you in con-
tacting the appropriate specialist at Children’s
Hospital Boston, is now available. The guide is
organized by specialty/subspecialty and provides
quick access to basic contact information for our spe-
cialists, including telephone and fax numbers, email
addresses, office locations and directions/maps to
Children’s. In addition, the PSG provides department/
division descriptions, guidelines on how to refer a
patient, accepted health insurance, and more.
All PSG information is also available online by
visiting www.childrenshospital.org and clicking on
“Find a Specialist.” Additional information, such as
a specialist’s education/training history, professional
experience, curriculum vitae and community-based
office locations, can be found as part of our online
physician profiles.
A “Print-On-Demand” feature allows you to gener-
ate a PDF file of the most up-to-date information,
whether you’d like to print the entire guide or just
one department/division. We also offer a new op-
tion to download the PSG—the entire directory or
a particular department—to your personal digital
assistant.
You will receive a copy of the 2006-2007 PSG by
mail. To request additional copies, send your mailing
address to [email protected].
www.childrenshospital.org/views
When 13-year-old Nichole Paone awoke one chilly morning in November, something just wasn’t right. She’d been lethargic for several days prior, experiencing a tingling sensation in her head and some mild vomiting. But
that particular Tuesday, she was looking almost yellow. Nichole had been in and out of her pediatrician’s office all month, undergoing several
tests to determine what was causing her symptoms. When the tests turned up empty, she was eventually referred to a neurologist, but the appointment wasn’t for another few days.
But that wasn’t soon enough for her mother, Michelle, who had been watching her little girl’s symptoms change and get worse over the weeks. So, she brought Nichole to Children’s Hospital Boston’s emergency room later that day.
A CT scan revealed that Nichole had a tumor the size of a baseball lodged in the back of her brain. “The tumor was a juvenile pilocytic astrocytoma (JPA),” says neurosurgeon Liliana Goumnerova, MD. “This is probably the most common tumor in that location in children. There are no known causes of JPA; it is believed to occur sporadically.”
Nichole, who wants to be a veterinarian, took her diagnosis in stride. When told she had a brain tumor, she described, in great detail, a brain operation she had
MR-OR in action
››› continued on page 6
Liliana Goumnerova, MD, gives patient Nichole Paone a clean bill of health.
PSG with Neurosurgeon-
in-ChiefR. Michael
Scott,MD, in our
MR-OR.

2 www.childrenshospital.orgPediatric Views | February 2006 3 Pediatric Views | February 2006www.childrenshospital.org
By Marc Laufer, MD
Surgeon Marc Laufer, MD, is chief of the Division of Gynecology, and co-director of the
Center for Young Women’s Health at Children’s Hospital Boston. He specializes in pediatric and
adolescent gynecology and gynecologic surgery.
What is endometriosis?Endometriosis is a condition that occurs when tissue similar to the lining of the uterus is found outside its normal location. Common locations of these endometrial implants, or lesions, include the ovaries, fallopian tubes, ligaments that support the uterus, and tissue covering the bladder and rectum. The location of the endometrial implants, and the way in which the lesions affect the pelvic organs, contributes to the symptoms adolescent and adult women may have. Some teens with a lot of lesions have very little pain, while others with a small amount have severe pain.
What causes endometriosis?Although we know that some young women may be slightly more likely to develop endometriosis because female relatives have it, the truth is, we don’t know the cause of this disease. Any woman, anywhere, can get endometriosis.
What symptoms are associated with endometriosis?The most common symptoms include occasional or constant pelvic pain and/or severe period cramps—often referred to as chronic pelvic pain. Pain can occur before, during or after a period and may be cyclic or acyclic. Teens may experience pain at rest, with exercise, sex or after a pelvic exam. Painful or frequent urination, diarrhea or constipation may accompany the pelvic pain, confusing the diagnosis of endometriosis with inflammatory bowel disease, recurrent urinary tract infection, appendicitis, pelvic inflammatory disease.
How is endometriosis diagnosed?The only way to be completely sure that the problem is endometriosis is to have a laparoscopy—a minimally invasive, outpatient surgery to examine the pelvic organs. Blood tests, cultures to check for infection, an ultrasound or an MRI may help rule out other diagnoses prior to laparoscopy. It is important to refer young women to gynecologists who specialize in treating teens with endometriosis as it can be more challenging to recognize endometriosis in teens than adult women.
How is endometriosis treated?Although we can’t cure endometriosis, there are many options for treating symptoms. The goals are to relieve pain, control the progression of the endometriosis and preserve fertility. Treatment can make a big difference in improving the quality of a young woman’s life, and early treatment may preserve a woman’s fertility. We recommend continuous treatment through child bearing years or until desired family size is reached.
Some common treatment methods include:
• Over-the-counter pain relievers, such as aspirin, acetaminophen, ibuprofen and naproxen sodium can offer relief for some. Others require prescription drugs.
• Oral contraceptives taken continuously relieve symptoms in eight out of 10 patients. GnRH agonists (gonadotropin releasing hormone drugs), such as Lupron, temporarily stop periods by lowering estrogen levels.
• During laparoscopy, doctors can use special instruments to laser or cauterize the endometriosis. Many teens find relief from symptoms after going through this procedure, although over time, some may experience pain again.
• Acupuncture, herbal remedies, homeopathy and healing touch are a few alternatives we’ve seen grow in popularity. We’ve also found many of these therapies to be effective. We encourage patients to speak with their
primary care doctor or gynecologist before pursuing alternative treatments, as research studies are limited and not every alternative approach has been proven to be safe and effective.
• Eating well and getting enough rest helps the body to manage pain. Exercise often helps to relieve or lessen pelvic pain and menstrual cramps. Practicing relaxation techniques, such as yoga and meditation, help ease pain too.
• Many centers work closely with other health care providers in programs that
provide treatment and support for acute and chronic pain. Following an evaluation, services such as biofeedback, physical therapy, TENS (transcutaneous electrical stimulation) and exercise programs, may be offered.
Is endometriosis being researched?Yes. A variety of research is underway around the world. At Children’s, we’ve just finished collecting data on a blood test for
endometriosis that may one day provide a less invasive way to diagnose it. We are also studying the way complementary and alternative therapies, such as acupuncture, may help manage symptoms alone or in conjunction with other forms of treatment.
Where can young women or parents find more information?The Center for Young Women’s Health is a great resource for young women, parents and health professionals. Their Web site (www.youngwomenshealth.org) includes pages on basic health, nutrition and fitness, emotional health, sexuality and reproductive health. Common questions about endometriosis are answered in sections specific to teens, parents and health professionals. The Endometriosis Association (www.endometriosisassn.org) is another good resource for more information on endometriosis.
Talking about endometriosis
Each month the CYWH hosts an on-line chat about en-dometriosis, inviting women anywhere in the world to partici-pate. Additional chats are held each month on a variety of topics. To learn more, visit www.youngwomenshealth.org.
Pediatric Health Care SummitsChildren’s Hospital Boston, in conjunction with the community hospitals listed below, presents the following Pediatric Health Care Summits. The summits are free, community-based continuing medical education seminars designed to inform primary pediatric providers of trends in the management of common pediatric health concerns.
Friday, April 7, 2006, 7:30 a.m. to 12:30 p.m. Beverly Hospital, Beverly, Mass.Topics include: Asthma Management • Pediatric Hypertension and Management of an Acute Crisis • Cardiac Evaluation of the Pediatric Athlete • Food AllergiesCME: 4 hours in category 1 credits
Thursday, May 6, 2006, 7:30 a.m. to 12:15 p.m. South Shore Hospital, Weymouth, Mass.Topics include: The Future of Pediatric Cardiac Surgery • Overuse Injuries in Children and Adolescents • Pediatric Hip DysplasiaCME: 3 hours in category 1 credits
Thursday, June 1, 2006, 7:30 a.m. to 12:30 p.m. MetroWest Medical Center, Framingham, Mass.Topics include: Advances in Radiology Imaging • Autism • Chlamydia • Sports Injuries in the Female AthleteCME: 4 hours in category 1 credits
Brochures for the individual conferences will be mailed. To register in advance, visit
www.childrenshospital.org/cme or call Physician Relations at (617) 355-2454.
Arthur mousepadsTo celebrate “Arthur’s Guide to Children’s Hos-
pital Boston” on the hospital’s new Web site,
we are offering free mousepads. To request a
mousepad, visit www.childrenshospital.org/
mousepad. In addition, to provide your patients
with information on the new resources
on our Web
site, as well as
the mousepad
offer, send an
email with your
mailing address
to marketing@
childrens.harvard.
edu, and we will send you a tear-off pad for
your waiting room.
Continuing Medical EducationCurrent Concepts in Pediatric Health CareAn online, lunch-time learning opportunity, which is part of a series sponsored by GE Healthcare and MESG. This complimentary, cutting-edge program featuring Children’s Hospital Boston specialists is intended for primary care physicians, pediatricians, family practitioners, pharmacists and nurses. Talks can be viewed online or through TiP-TV, where available.
April Update on Childhood Acute Lymphoblastic Leukemia by Lewis Silverman, MD.
May Pain Issues in Pediatric and Adolescent Gynecology: Ovarian Cysts, Tumors, Endometriosis and Congenital Anomalies of the Reproductive Tract by Mark Laufer, MD. (See related article on page 3.)
June Angiogenesis-dependent Diseasesby Judah Folkman, MD.
July Assessing and Treating Pediatric and Adolescent Scoliosis by John Emans, MD.
August What to Do When Seizures Won’t Stop by James Riviello, MD, and Joseph Madsen, MD.
September Evolving Management of Hypoplastic Left Heart Syndrome: From Fetal to Post-Natal Interventionby Roger Breitbart, MD, and Pedro del Nido, MD.
To register, visit: www.chbpediatriccme.com.
Frontiers in Pediatric SurgeryWednesday, March 15, 2006, 7:30 a.m. to 3:45 p.m.The Conference Center at Waltham Woods, 860 Winter Street, Waltham, Mass.
Topics include: Strabismus • Head Injuries • Management of Prenatally Diagnosed Hydronephrosis• Acute Abdominal Pain • Pigmented Nevi • Nocturnal Enuresis • Pictorial Guide to Pediatric and Adolescent Gynecology • Shoulder Injuries • Sinusitis and Its Treatment • Back Pain in Children
CME: 6 .0 category 1 credits. Fee: $50. To register, contact Anne Vaccaro at (617) 355-5186.
Tom Jaksic, MD, PhD, surgical director of
Children’s Hospital Boston’s Short Bowel
Syndrome (SBS) Program will perform
a serial transverse enteroplasty (STEP)
procedure to correct SBS in a pediatric
patient. (See related article on page 4.)
Steven Fishman, MD, co-director of the
Vascular Anomalies Center, will perform
a procedure to debulk tissue in a patient
with Klippel-Trenaunay Syndrome.
For more information, visit
www.childrenshospital/webcasts.Researchers at Children’s Hospital Boston have found that children with serious congenital heart defects
benefit from an exercise rehabilitation program. To read more about it, check out the article on page 5.
Two new, live surgical Webcasts
Cardiology multimedia library
The Department of Cardiology has created a web-based multimedia library that provides an unprecedented and unique review of congenital
heart disease. The site, edited by Children’s Hospital Boston cardiologist Robert Geggel, MD, includes im-ages (electrocardiograms, chest radiographs, diagrams, gross pathology), audio (phonocardiograms) and video (echocardiography, angiocardiography, magnetic reso-nance imaging, cardiac surgery) to help educate both physicians and families about congenital heart disease.
Visit www.childrenshospital.org/mml/cvp for more.
Cardiac Rehabilitation Week January 12 to18

4 www.childrenshospital.orgPediatric Views | February 2006 5 Pediatric Views | February 2006www.childrenshospital.org
Children with serious congenital heart defects are typically urged to restrict their activity, but a pilot
study at Children’s Hospital Boston, published in the December Pediatrics,indicates that most of these children can benefit from cardiac rehabilitation.
The study enrolled 19 children, ages 8 to 17, in a 12-week program of stretching, aerobics and light weight/resistance exercises. All the children had cardiac disease severe enough to consider restricting their activity, and all showed reduced function on exercise tests, but none had test findings that might raise a safety concern, such as arrhythmias or chest pain. Still, all 16 children who completed the program had undergone heart surgery or a nonsurgical procedure in the past, and 11 of the 16 had just one functional ventricle.
The hour-long sessions, held twice weekly, were tailored to the children’s interests and included dance, calisthenics, kick boxing and jump rope. Balls, music, games, relay races and age-appropriate prizes helped keep the kids motivated, and sessions were moved outdoors whenever possible. Heart rate was checked initially and two to three times during each session. A pulse oximeter and external defibrillator were available on site, but were never needed, since there were no adverse events.
At the program’s end, 15 of 16 children had significantly improved peak work rate, peak oxygen consumption, or
both—their hearts pumped more blood with each beat, and their muscles used more oxygen. Functional improvements were as high as 20 percent on some parameters.
Children’s cardiologist JonathanRhodes, MD, who led the study, believes that some of the reduced exercise capacity in children with congenital heart defects
is due to inactivity. In this pilot study, he notes, fewer than 10 percent of children with diminished exercise capacity had conditions that made it dangerous to exercise. “With the approval of a pediatric cardiologist, and after careful exercise testing, exercise is generally safe and tolerable,” he says.
Follow-up exercise testing, roughly
7 months after program completion, showed that participants’ cardiac benefits were sustained, whereas non-participating children had a slight decline in cardiac function. Participants reported exercising more than in the past and had higher behavioral, emotional and self-esteem scores.
Children’s plans to launch a formal cardiac rehabilitation program in fall 2006 or spring 2007, when facilities at Children’s Hospital Boston at Waltham are complete. Rhodes believes that some two-thirds of children with serious congenital heart disease will be eligible to participate.
Children with heart defects can benefit from exercise
When he was just one day old, Devin O’Bleanis had surgery at Long Island Jewish Hospital in New York to correct a twisting of his intestine. But when the
problem persisted, an additional surgery was required to remove the damaged segment of his intestine altogether.
As a result, Devin developed short bowel syndrome (SBS), a condition in which patients are without a significant length of their small intestine and are usually deficient in a range of important nutrients, because their intestine cannot absorb enough nutrition from regular food.
Treatment consists primarily of nutritional management to help the remaining intestines adapt and take on the absorption functions that were lost. Many SBS patients get nutrients delivered directly into their stomachs or small intestines via enteral nutrition. But in some cases, this is not possible, so patients must get nutrition intravenously through parenteral nutrition (PN). Depending on the length and health of the remaining intestine, nutritional support becomes a lifelong necessity for some patients.
As a newborn with SBS, Devin was put on PN immediately and did well enough to go home after four months. A few days after discharge, however, Devin’s parents noticed a yellow discoloration of his skin and eyes.
After consulting with their doctors at Long Island Jewish Hospital, the O’Bleanis’s were referred to nearby Mount Sinai Hospital, where doctors ran tests and found damage to Devin’s liver. But their recommendation of a liver and intestine transplant concerned the O’Bleanis’s. “He was a vivacious and high-spirited child, and we didn’t want to put him through that
trauma,” says Devin’s mother, Yvette. “So we began to explore other options.”
Their research led them to Children’s Hospital Boston’s pre-eminent program for treating SBS. A team of doctors evaluated Devin and concluded that the best course of action was not a transplant but a bowel lengthening procedure called a serial transverse enteroplasty, or STEP.
Developed at Children’s by Heung Bae Kim, MD, and Tom Jaksic, MD, PhD, the STEP procedure is based on the idea that stapling v-shapes into alternating sides of the bowel will
decrease its width and increase its length. Thus, the intestine eventually stretches out and becomes a normal tube, and food is propelled down the tube like a normal piece of intestine.
The O’Bleanis’s agreed to the surgery, and just
weeks later, Devin was back in Boston to undergo a STEP procedure. Following the STEP, his condition improved almost immediately. Devin’s bilirubin level, which was causing his yellow discoloration, began to recede. And while a biopsy taken during surgery revealed some damage to his liver, it was determined that proper nutritional care would be able to reverse it.
“Patients like Devin are complex, but they can be helped if they get the right kind of care,” says Dr. Jaksic, the Short Bowel Syndrome Program’s surgical director. “They present a number of challenges, primarily because their care involves so many different specialties.”
Delivering effective nutrition to patients like Devin demands important contributions from a multidisciplinary team, including gastroenterologists, dieticians, pharmacists and nurses. Christopher Duggan, MD, MPH, medical director of the Short Bowel Syndrome Program, helps direct how to best to keep kids with SBS growing.
“Devin was pretty malnourished when he got here,” says Dr. Duggan. “The first thing we did was an intensive assessment of his nutritional status and nutrient needs. We were also very aggressive in weaning him from parenteral to enteral nutrition.” Other team members involved in his care include: Clifford Lo, MD, PhD; Sharon Collier, RD; Julie Iglesias, CPNP; Kathleen Gura, Pharm D; and Denise Richardson, RN.
Today, Devin, an energetic 4-year-old, is back home in New York. Since his STEP surgery in 2003, he has gradually been taken off PN and is now eating everything by mouth. Although Devin sometimes requires extra fluid through his G-tube to supplement his oral diet, it’s a marked improvement for the O’Bleanis family. “The doctors at Children’s gave us our life back—which is Devin,” says Yvette.
For more information on Children’s Hospital Boston’s Short Bowel Syndrome Program, visit www.childrenshospital.org/sbs.
To schedule an appointment, call (617) 355-9600.
The Next STEP
Teenagers who think their mothers put a premium on thinness may be more likely to worry about their weight and diet frequently, suggest new findings from the Growing
Up Today Study, published in the December Archives of Pediatric Adolescent Medicine.
Investigators at Children’s Hospital Boston and Brigham and Women’s Hospital surveyed more than 9,000 U.S. adolescents and their mothers. Overall, 33 percent of girls, 8 percent of boys, and about half the mothers reported frequently thinking about wanting to be thinner. But girls who thought—correctly or not—that their mothers wanted them to be thin were two to three times more likely to worry about their weight. A similar trend was found among boys.
Among both sexes, teens, who accurately perceived that their weight was important to their mother, were about twice as likely to diet frequently (at least twice a week) than those who believed, correctly, that their weight wasn’t important to their mothers. In girls, this relationship held true even if they weren’t overweight.
“While there’s definitely reason for parental concern about a child’s weight, putting too much value on thinness can promote unhealthy behaviors,” says study author Alison Field, ScD, of Children’s Division of Adolescent Medicine. She cautions parents to avoid commenting too much about their own weight or other people’s, since teens can internalize negative messages, and instead, promote physical activity and sound nutrition.
Teens’ dieting may reflect mothers’ concerns
Illus
tratio
n: ©
Chr
isto
pher
Qui
nn, 2
006.
1
3
2
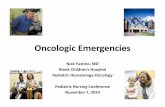
One STEP at a time1. Short bowel syndrome causes the bowel to grow wider to absorb nutrients. But this can cause life-threatening infections.
2. With the STEP procedure, the bowel is stapled on alternating sides.
3. When complete, the bowel is longer, making food digestion easier.

6 www.childrenshospital.orgPediatric Views | February 2006 7 Pediatric Views | February 2006www.childrenshospital.org
© C
hild
ren’
s H
ospi
tal B
osto
n, 2
006.
Thi
s pa
ge m
ay b
e re
prod
uced
for
edu
catio
na p
urpo
ses.
Rep
rint
perm
issi
on is
req
uire
d fo
r al
l oth
er u
ses.
ChildhealthThe facts on carbon monoxide poisoning by Aarthi Iyer, MPH, Education Coordinator, Regional Center for Poison Control and Prevention
New network services The Division of Genetics is now seeing patients at Children’s Hos-
pital Boston at Waltham. To schedule an appointment, call (781)
216-2100. In addition, geneticist Jonathan Picker, MBChB,
MSC, PhD, will begin seeing patients at South Shore Hospital
this March. To make an appointment, call (781) 331-4715.
The Hearing Technology Center opens at Children’s Hospital
Boston at Waltham on February 21. Headed by audiologist Mary
Ellen Curran, MA, CCC-A, the center will professionally fit and
sell hearing aids and assistive listening devices for teens and
adults with sensorineural hearing loss. To schedule an appoint-
ment, call (781) 216-2100.
Greg Young, MD, has been
named president and CEO of
the Pediatric Physicians of
Children’s (PPOC) and vice president of
Community Pediatrics at Children’s Hos-
pital Boston. Dr. Young previously served
as physician advisor for Utilization Manage-
ment at the hospital and has been a practicing pediatrician
at Longwood Pediatrics for 15 years (where he will continue
to practice part-time). He also completed his residency at
here and served as Chief Resident in 1990.
Dr. Young is fortunate to assume
leadership from the very talented and
committed Michael Grady, MD,
who has done a phenomenal job
building the PPOC from its humble
beginnings to one of the largest
networks of pediatricians in the
state.
When parents tuck their children into bed at night, they usually feel assured that they’re as safe as
can be. But a “silent killer” could be on the loose in some homes, putting the whole family at risk of illness or even death.
What is carbon monoxide?Carbon monoxide (CO) is a gas that is produced when fuel—gasoline, propane, natural gas, oil, wood, or coal—is burned. CO is extremely dangerous to people when emitted in an enclosed, unventilated area, such as a house, garage or car.
Why is it harmful?When CO is breathed, it is absorbed into the bloodstream and displaces oxygen necessary to vital organs. It can eventually cause permanent brain damage and death.
CO is especially dangerous because it cannot be seen or smelled. People may feel ill or become unconscious without realizing they are being poisoned and need to get to fresh air immediately.
How would someone be exposed to CO?Winter is when most CO poisoning incidents happen, because people use heaters, leave cars idling to warm up, and because snow drifts can block vents and tailpipes. Poisoning can happen when:
• A furnace, gas stove or water heater is faulty or installed improperly.
• The outside vent to a fuel-burning appliance becomes covered with snow.
• A fireplace chimney or stove pipe becomes clogged or blocked.
• A charcoal grill is used indoors.
• A car or gas-powered snow- or leaf-blower is left running in a closed garage.
• A car is running while parked with snow blocking the tailpipe.
With electric heaters and appliances, you do not need to worry about CO.
What happens during poisoning?Both children and adults can become very ill and even die within minutes or hours of exposure, depending on the level. Pregnant women, their unborn children, babies, heavy smokers, and people with anemia, heart or lung disease may be affected more quickly or seriously.Symptoms and effects vary between individuals, even at the same level of CO exposure, but people typically experience flu-like symptoms, including: dizziness, fatigue, weakness, headache or vomiting, trouble breathing, confusion, ringing in the ears, heart fluttering, gastrointestinal complaints, increased blood pressure, or bright red or pink skin, mucous membranes or nails.
However, death from CO poisoning can result even if none of these symptoms occur first. In some cases, people fall unconscious before ever feeling ill.
Some CO poisoning survivors have described drifting in and out of consciousness, but being completely immobilized and unable to get themselves out of the area.
How many people die from CO exposure?According to the Journal of the American
Medical Association, 1,500 Americans die each year from accidental
exposure to CO, and there are more than 10,000 injuries each year.
Although most CO poisoning happens during a one-time sudden incidence, it is possible to suffer from chronic CO
poisoning. This is when someone is exposed to low levels over weeks
or months (for instance, due to a faulty oil-burning furnace), and experiences symptoms over that time.
How can you prevent exposure?It’s important to have your fuel-burning appliances inspected by a qualified professional at least once each year. But the most important thing you can do is to have a CO detector in your home.
When a sleeping 10-year-old girl died in her home last year because a snow
drift blocked an outside vent, the state of Massachusetts passed “Nicole’s Law,” requiring all residential buildings to be equipped with CO detectors. Other states have passed similar laws.
How do detectors work?CO detectors, which can be purchased at most hardware stores, can be hardwired, battery-operated or plugged-in.
Most beep when levels have been at 70 ppm for an hour, or sooner if levels are higher. Although symptoms usually go unnoticed at that level, if the alarm sounds, immediately open windows and doors for ventilation, leave your home and call 911 immediately before symptoms or unconsciousness occur.
This article was adapted from content provided by Children’s Hospital Boston to the Health and Parenting sections of Yahoo! For more pediatric health information from Children’s, visit http://health.yahoo.com, and select “Parenting” under Healthy Living.
Source: Consumer Reports, 2005.
seen performed on a dog on one of her favorite TV shows, “Emergency Vets.” Once the doctor confirmed that she would be undergoing a similar procedure, she didn’t need any further explanation.
But what made Nichole’s operation much different than her four-legged friend’s was the use of Children’s new MR-OR—the world’s first-of-its-kind Intraoperative Magnetic Resonance Imaging (MRI) system in a pediatric hospital. Suspended from ceiling tracks, the 15,000-pound magnet travels from behind doors in the operating room’s wall to take images before, during and after an operation. With this technology, surgeons can determine the extent of a tumor while the patient is undergoing surgery and ensure its accurate removal.
Surrounded by a team of neurosurgeons, anesthesiologists, radiologists, radiology technicians and nurses, Nichole became the second patient at Children’s to undergo an operation in the MR-OR the very next morning.
While anesthesiologist Craig McClain, MD, managed Nichole’s anesthesia, Dr. Goumnerova removed Nichole’s tumor using her usual metal surgical tools instead of the non-metallic instruments that must be used in previous MR operating rooms. And before Dr. Goumnerova closed the wound, radiologist Caroline Robson, MB, ChB, deployed the MRI from its dock to scan Nichole’s brain to determine if the entire tumor had been resected. And in fact, it had.
“Nichole’s case is a perfect example of how the new MR-OR can be used to benefit our patients,” says Dr. Goumnerova, citing that 12 patients have now undergone procedures in the new unit. “The quality of the images we obtained during her surgery was very good, so we were able to interpret them accurately to see if the tumor has been completely removed, therefore avoiding additional procedures.”
By 11 a.m., Nichole was out of surgery and recovering in the ICU, and by 2 p.m. that afternoon, she was already up and walking to the restroom with the help of her mother and her nurse. She spent just three additional days in the hospital before returning home.
While she did experience a mild problem with coordination on her left side affecting her arm and leg after surgery, Nichole has since completely recovered. “She was out of school for about a month, but that mostly has to do with the holidays,” says Michelle. “And she’s already caught up on all of her school work. You look at her, and you’d never even know she’d just had brain surgery. It’s truly amazing.”
Nichole returned to Children’s in January for a follow-up visit with Dr. Goumnerova and was given a clean bill of health. “Nichole has recovered wonderfully from the surgery,” says Dr. Goumnerova. “Her examination was normal, and she can return to her usual activities without any restrictions. Generally, these tumors have about a 96 percent cure rate if completely removed, so Nichole’s long-term outcome is expected to be excellent.”
For more information on our MR-OR, visit www.childrenshospital.org/mr. To schedule an appointment in the Department of Neurosurgery, call (617) 355-6009.
MR-OR ››› continued on page 6
The MR-OR suite at
Children’s HospitalBoston.
as physician advisor for Utilization Manage- Greg Young, MD
Michael Grady, MD
PPOC welcomes new leader
((((((
Detecting CO • When buying a CO detector, check for
the UL approved label.
• Digital display models show the CO level,
rather than simply beeping.
• Install CO detectors in a central area on
every floor and near sleeping areas.
• Detectors should be placed at least five
feet above the ground, as CO rises.
• Hard-wired and plug-in models won’t
work during a power outage.
• Like smoke detectors, batteries need to
be replaced each year.
• CO detectors lose sen-
sitivity over time and
should be replaced
every five years.
can block vents and tailpipes. Poisoning can happen when:
The outside vent to a fuel-burning appliance becomes covered with snow.
Medical Association,die each year from accidental
poisoning. This is when someone is exposed to low levels over weeks
or months (for instance, due to a faulty
In an emergency, or for more information, call your local poison
center: 1-800-222-1222.
New CPR guidelinesIn November 2005, the American Heart Associa-
tion released new CPR guidelines. They now
recommend that all single rescuers
employ a chest compression-to-
breath ratio of 30:2 on all victims
from infants (excluding newborns)
to adults, aiming for increased
blood flow to the heart, brain and
other vital organs.
30:2New chest compression-
to-breath ratio.

Published by Children’s Hospital Boston Department of Public Affairs and Marketing.© Children’s Hospital Boston, 2006. All rights reserved.
The information in this newsletter should not be taken as medical advice, which can only be given to you by your personal health care professional.
Editors: Alison Dargie, Anna GonskiContributors: Michael Coyne, Beth DiPietro, Bryan Farrow, Nancy Fliesler, Rachel Pugh, Christopher QuinnDesigners: Javier Amador-Peña, Patrick Bibbins300 Longwood Avenue, AT 600Boston, MA 02115617-355-6000
www.childrenshospital.org/[email protected]
Pediatric Views NONPROFIT ORG.
U.S. Postage
PAID
Boston, Mass.
Permit No. 59240
serv
eth
ene
eds
ofin
fant
s to
adolescentscentss
com
mun
icat
ion,
and
spee
chan
d lang
uage pathology to
lesce
ologTh
ece
nter
com
bine
sfiv
epr
ogra
ms in
audio
logy, augmentativeis
now
seei
ngpa
tient
sat
Child
ren’s
Hospi
talBosto
n at Waltham.
adole
patho
ntativ
ofin
fant
s t
ad
nguaggee pa
auuggment
althamm.Th
eCe
nter
forC
omm
unic
atio
nDi
sord
ers,
unde
r the
lead
ersh
ipof Howard Shane, PhD,
ad
tsto
a
(and
som
ead
ults)
with
speaking or
hear
ingi
mpair
ments.
coTh
serv
eth
ene
eds
ofin
f
omm
unic
atio
n,an
dsp
eech
aanndd la
ng
hece
nter
com
bine
sfiv
epr
ogra
mmss in
audio
logy,y,y aais
now
seei
ngpa
tient
sat
Childd
rreen’s
Hospi
tallBBoosto
n att WWalTh
eCe
nter
forC
omm
unic
atio
nDi
sord
errss,
unde
r the
leeaad
ershh
iippof HHoowward Sha
DID
YO
UH
E A R ?
To schedule an appointment, call (781) 216-2100. For more information on services available, visit:
www.childrenshospital.org/ccd.