A Prospective, Randomized Comparison of Paclitaxel- eluting TAXUS Stents vs. Bare Metal Stents...
37
A Prospective, Randomized Comparison of Paclitaxel-eluting TAXUS Stents vs. Bare Metal Stents During Primary Angioplasty in Acute Myocardial Infarction – One Year Results – HORIZONS AMI Trial Gregg W. Stone MD For the HORIZONS-AMI Investigators, TCT 2008
-
Upload
roy-sutton -
Category
Documents
-
view
224 -
download
2
Transcript of A Prospective, Randomized Comparison of Paclitaxel- eluting TAXUS Stents vs. Bare Metal Stents...
A Prospective, Randomized Comparison of Paclitaxel-eluting TAXUS Stents vs. Bare Metal Stents During Primary Angioplasty in Acute Myocardial Infarction
– One Year Results –
HORIZONS AMI Trial
Gregg W. Stone MDFor the HORIZONS-AMI Investigators, TCT 2008
Background
● No consensus exists regarding the safety and efficacy of drug-eluting stents in pts with STEMI undergoing primary PCI– TLR and restenosis rates tend to be lower in STEMI vs.
elective PCI patients because of less plaque burden and non viable myocardium
– The safety of implanting DES in ruptured plaques with thrombus has been questioned
● Outcomes from registry studies of DES vs. BMS in STEMI have been conflicting, and no large-scale randomized trials have been performed
Stone GW. TCT 2008.
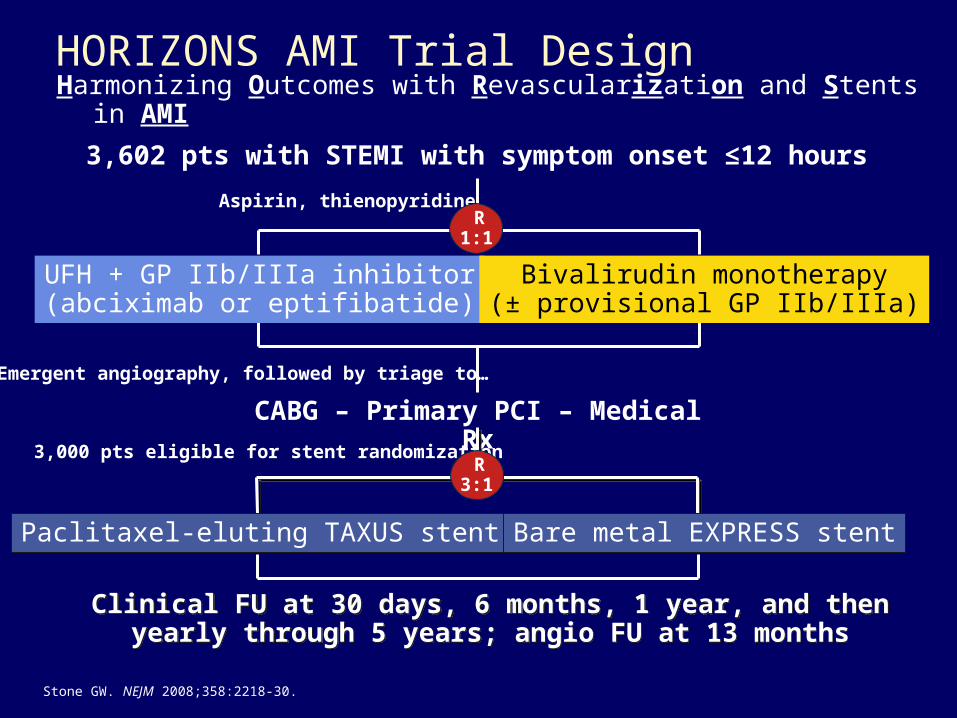
CABG – Primary PCI – Medical Rx
Aspirin, thienopyridine R 1:1
3,000 pts eligible for stent randomization R 3:1
Paclitaxel-eluting TAXUS stent Bare metal EXPRESS stent
HORIZONS AMI Trial DesignHarmonizing Outcomes with Revascularization and Stents in AMI
3
UFH + GP IIb/IIIa inhibitor(abciximab or eptifibatide)
Bivalirudin monotherapy(± provisional GP IIb/IIIa)
3,602 pts with STEMI with symptom onset ≤12 hours
Emergent angiography, followed by triage to…
Clinical FU at 30 days, 6 months, 1 year, and thenyearly through 5 years; angio FU at 13 months
Clinical FU at 30 days, 6 months, 1 year, and thenyearly through 5 years; angio FU at 13 months
Stone GW. NEJM 2008;358:2218-30.
Stent Randomization Hypotheses
● In patients with STEMI undergoing primary PCI, the use of paclitaxel-eluting TAXUS stents rather than bare metal EXPRESS stents will be:– Efficacious, as evidenced by reduced rates of ischemia-driven
target lesion revascularization at 1-year and angiographic binary restenosis at 13 months; and
– Safe, with non-inferior rates of the composite measure of death, reinfarction, stent thrombosis or stroke at 1-year
Stone GW. TCT 2008.
Clinical Inclusion Criteria
● STEMI >20 mins and <12 hours in duration– ST-segment elevation of 1 mm in 2 contiguous leads; or– Presumably new left bundle branch block; or– True posterior MI with ST depression of 1 mm in 2
contiguous anterior leads– Patients with cardiogenic shock, left main disease, etc., were
not excluded
● Age ≥18 years
● Written, informed consent
Stone GW. NEJM 2008;358:2218-30.
Principal Clinical Exclusion Criteria
● Contraindication to any of the study medications
● Prior administration of thrombolytic therapy, bivalirudin, GP IIb/IIIa inhibitors, LMWH or fondaparinux for the present admission (prior UFH allowed)
● Current use of coumadin
● History of bleeding diathesis or known coagulopathy (including HIT), or will refuse blood transfusions
● History of intracerebral mass, aneurysm, AVM, or hemorrhagic stroke; stroke or TIA within 6 months or any permanent neurologic deficit; GI or GU bleed within 2 months, or major surgery within 6 weeks; recent or known platelet count <100,000 cells/mm3 or hgb <10 g/dL
● Planned elective surgical procedure that would necessitate interruption of thienopyridines during the first 6 months post enrollment
Stone GW. NEJM 2008;358:2218-30.

Angiographic Inclusion Criteria
● The presence of least 1 acute infarct artery target vessel* in which:– a) ALL significant lesions are eligible for stenting with study
stents, and– b) ALL such lesions have a visually estimated reference
diameter ≥2.25 mm and ≤4.0 mm
● Expected ability to deliver the stent(s) to all culprit lesions (absence of excessive proximal tortuosity or severe calcification)
● Expected ability to fully expand the stent(s) at all culprit lesions (absence of marked calcification)
*Arteries containing multiple lesions may be randomized if all lesions are study stent eligible; multiple vessels may be randomized if all lesions in each vessel are study stent eligible
Stone GW. TCT 2008.
Angiographic Exclusion Criteria
● Bifurcation lesion definitely requiring implantation of stents in both the main vessel + side branch
● Infarct related artery is an unprotected left main
● >100 mm of study stent length anticipated
● Infarction due to stent thrombosis, or infarct lesion at the site of a previously implanted stent
● High likelihood of CABG within 30 days anticipated
Stone GW. TCT 2008.
Study Medications (i)
● Unfractionated heparin– 60 U/kg IV*; subsequent boluses titrated by nomogram to ACT
200-250 secs; terminated at procedure end unless prolonged antithrombin needed
● Bivalirudin– Bolus 0.75 mg/kg IV**, infusion 1.75 mg/kg/h, not titrated to
ACT; terminated at procedure end unless prolonged antithrombin needed (0.25 mg/kg/hr infusion)
● Glycoprotein IIb/IIIa inhibitors– Routine use in UFH arm; recommended only for giant
thrombus or refractory no reflow in bivalirudin arm– Abciximab or double bolus eptifibatide as per investigator
discretion – dosing per FDA label, renal adjusted; continued for 12 (abciximab) or 12-18 (eptifibatide)
* If pre randomization UFH administered, ACT is checked first** If pre randomization UFH administered, started 30’ after last bolus
Stone GW. NEJM 2008;358:2218-30.
Study Medications (ii)
● Aspirin– 324 mg chewed non enteric coated or 500 mg IV in the ER,
followed by 300-325 mg/day in-hospital and 75-81 mg/day as out patient indefinitely
● Thienopyridines– Clopidogrel 300 mg or 600 mg loading dose (per investigator
discretion) in the ER followed by 75 mg PO QD for at least 6 months (1 year or longer recommended)– Ticlopidine load + daily dose permissible if clopidogrel
is unavailable or patient is allergic
● Other– Beta blockers: IV pre procedure followed by PO QD in the
absence of contraindications; ACE inhibitors for HTN, CHF or LVEF <40%; Statin if LDL >100 mg/dl
Stone GW. NEJM 2008;358:2218-30.
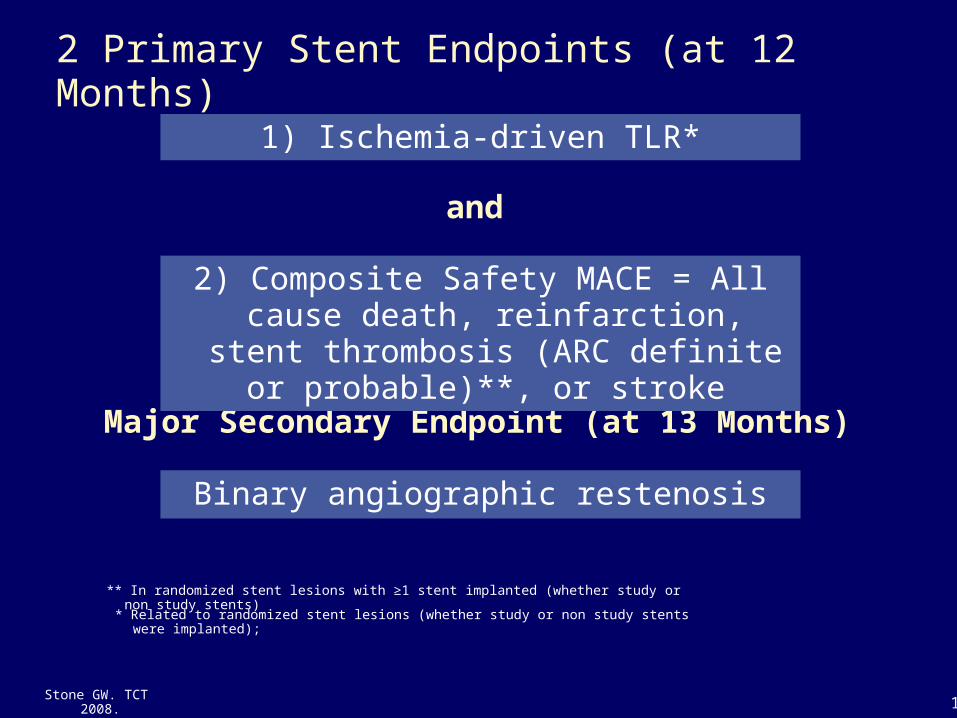
2 Primary Stent Endpoints (at 12 Months)
and
Major Secondary Endpoint (at 13 Months)
Binary angiographic restenosis
2) Composite Safety MACE = All cause death, reinfarction, stent thrombosis
(ARC definite or probable)**, or stroke
1) Ischemia-driven TLR*
11
* Related to randomized stent lesions (whether study or non study stents were implanted);
** In randomized stent lesions with ≥1 stent implanted (whether study or non study stents)
Stone GW. TCT 2008.
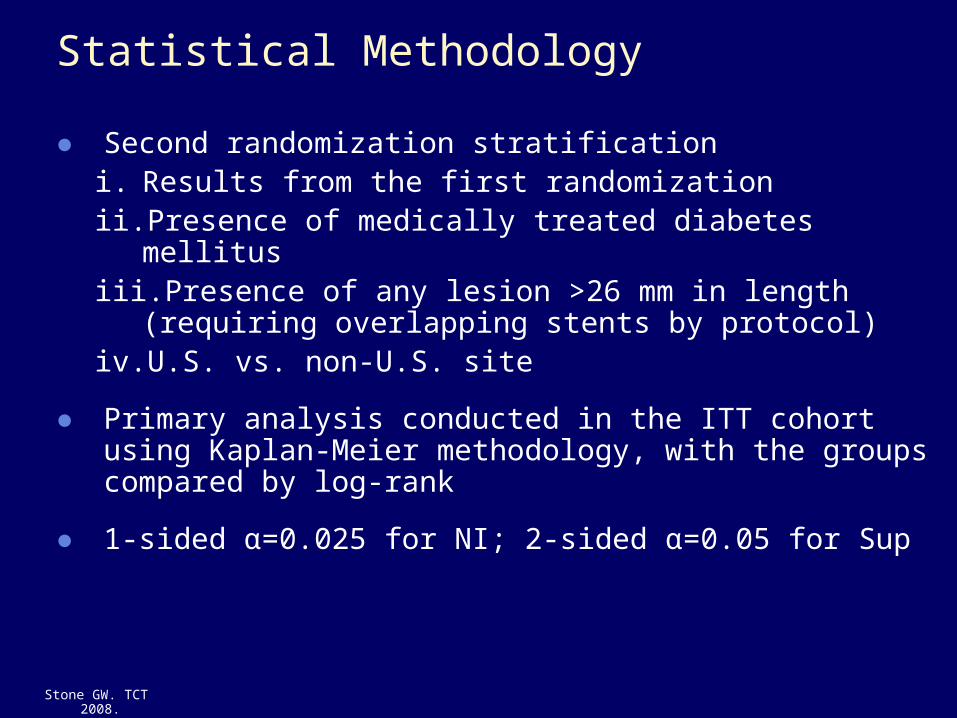
Statistical Methodology
● Second randomization stratification i. Results from the first randomization ii. Presence of medically treated diabetes mellitus iii. Presence of any lesion >26 mm in length (requiring
overlapping stents by protocol)iv. U.S. vs. non-U.S. site
● Primary analysis conducted in the ITT cohort using Kaplan-Meier methodology, with the groups compared by log-rank
● 1-sided α=0.025 for NI; 2-sided α=0.05 for Sup
Stone GW. TCT 2008.
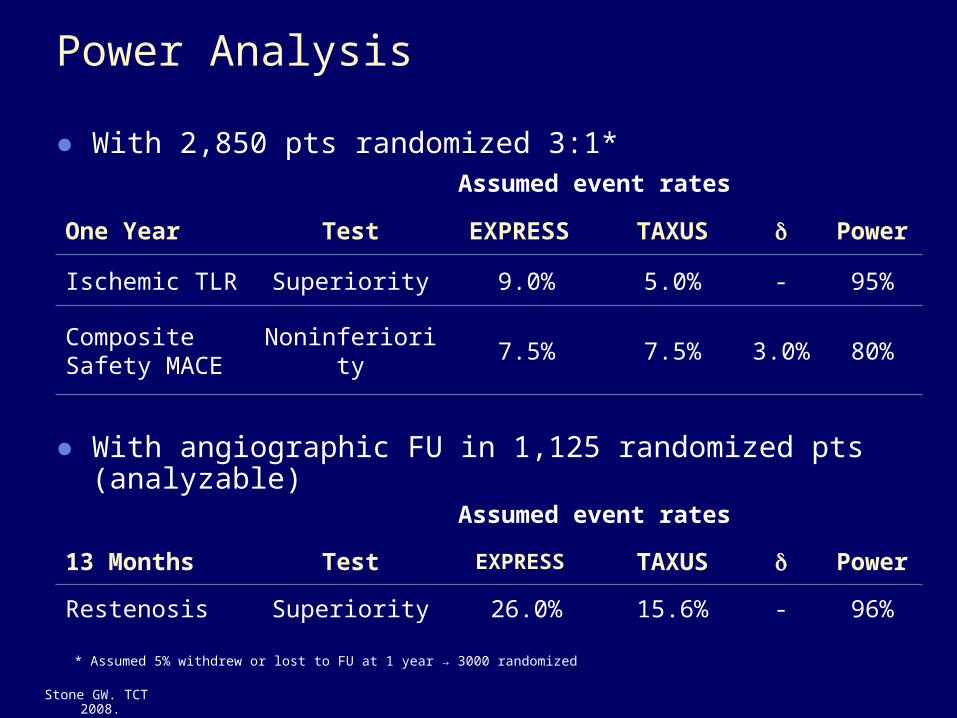
Power Analysis
● With 2,850 pts randomized 3:1*Assumed event rates
One Year Test EXPRESS TAXUS Power
Ischemic TLR Superiority 9.0% 5.0% - 95%
Composite Safety MACE
Noninferiority 7.5% 7.5% 3.0% 80%
Assumed event rates
13 Months Test EXPRESS TAXUS Power
Restenosis Superiority 26.0% 15.6% - 96%
● With angiographic FU in 1,125 randomized pts (analyzable)
* Assumed 5% withdrew or lost to FU at 1 year → 3000 randomized
Stone GW. TCT 2008.
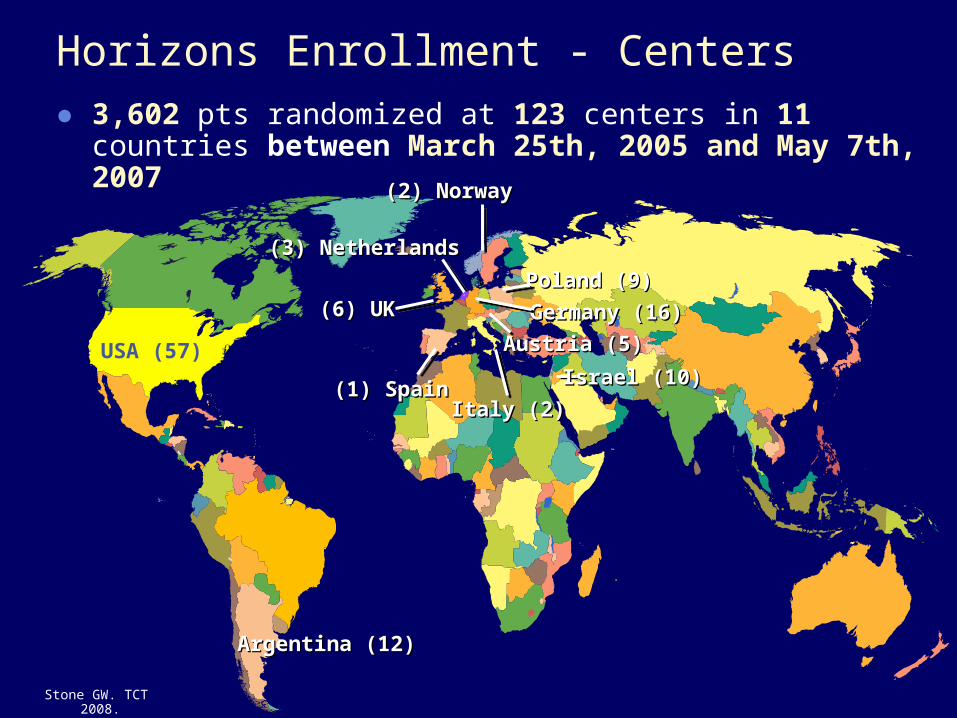
Horizons Enrollment - Centers● 3,602 pts randomized at 123 centers in 11 countries between
March 25th, 2005 and May 7th, 2007
USA (57)
(1) Spain(1) Spain
(6) UK(6) UK
(2) Norway(2) Norway
Poland (9)Poland (9)
Germany (16)Germany (16)
Austria (5)Austria (5)
(3) Netherlands(3) Netherlands
Italy (2)Italy (2)
Argentina (12)Argentina (12)
Israel (10)Israel (10)
Stone GW. TCT 2008.
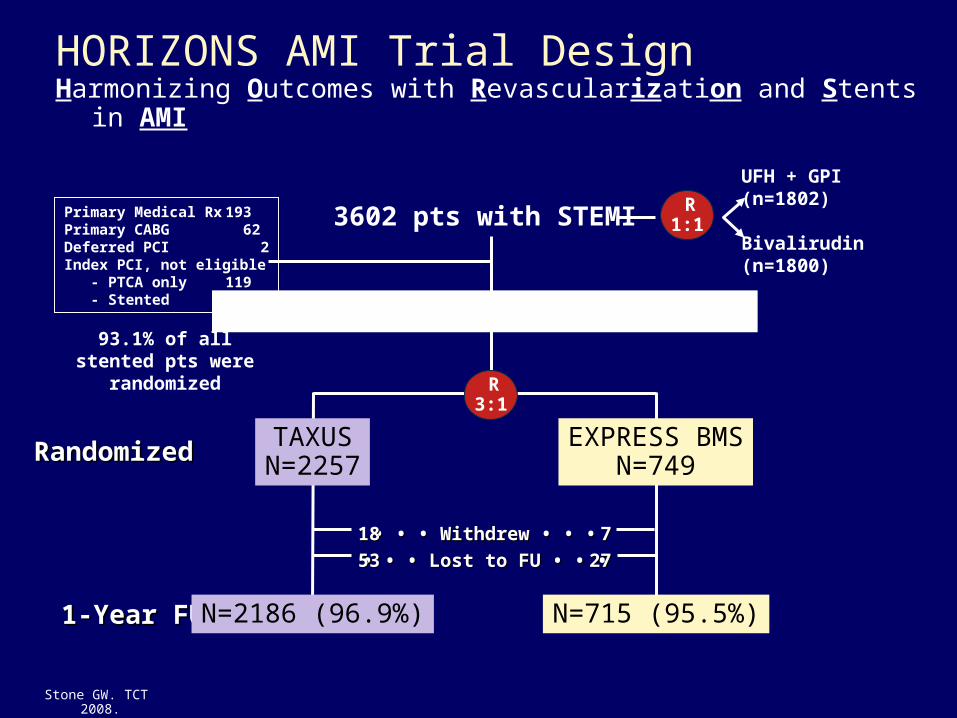
R 1:1
HORIZONS AMI Trial DesignHarmonizing Outcomes with Revascularization and Stents in AMI
UFH + GPI (n=1802)
Bivalirudin(n=1800)
• • • • • • Withdrew • • •Withdrew • • •
• • • • • • Lost to FU • • •Lost to FU • • •1818
535377
2727
3602 pts with STEMI
RandomizedRandomized
1-Year FU1-Year FU
TAXUSN=2257
N=2186 (96.9%)
EXPRESS BMSN=749
N=715 (95.5%)
R 3:1
Primary Medical Rx 193Primary CABG 62Deferred PCI 2Index PCI, not eligible - PTCA only 119 - Stented 220
3006 pts eligible for stent rand.93.1% of all stented
pts were randomized
Stone GW. TCT 2008.
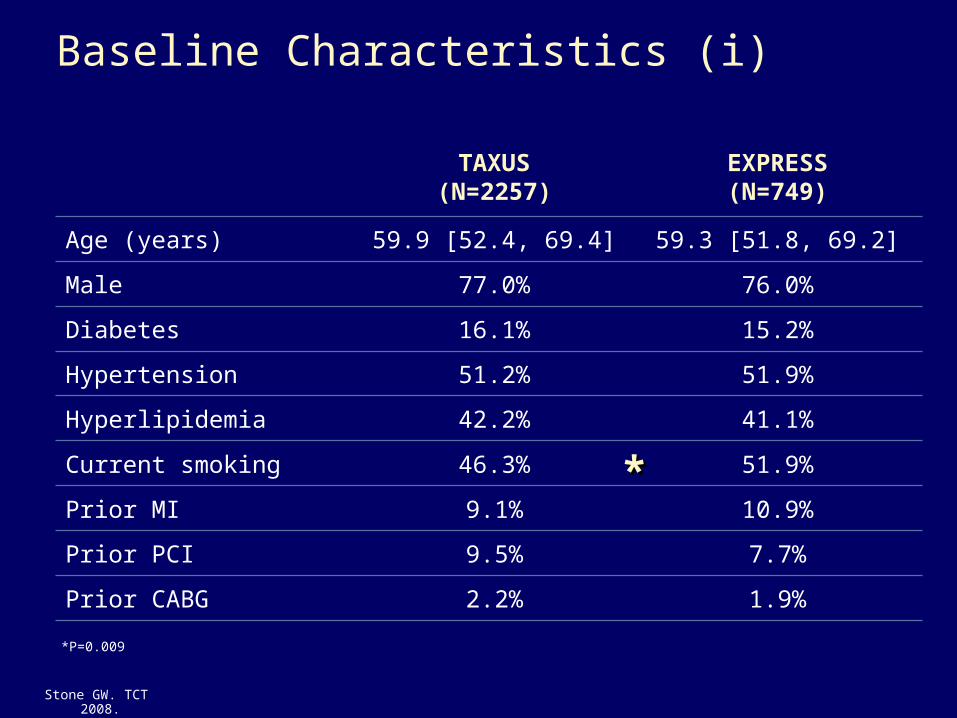
Baseline Characteristics (i)
TAXUS(N=2257)
EXPRESS(N=749)
Age (years) 59.9 [52.4, 69.4] 59.3 [51.8, 69.2]
Male 77.0% 76.0%
Diabetes 16.1% 15.2%
Hypertension 51.2% 51.9%
Hyperlipidemia 42.2% 41.1%
Current smoking 46.3% 51.9%
Prior MI 9.1% 10.9%
Prior PCI 9.5% 7.7%
Prior CABG 2.2% 1.9%
*P=0.009
**
Stone GW. TCT 2008.
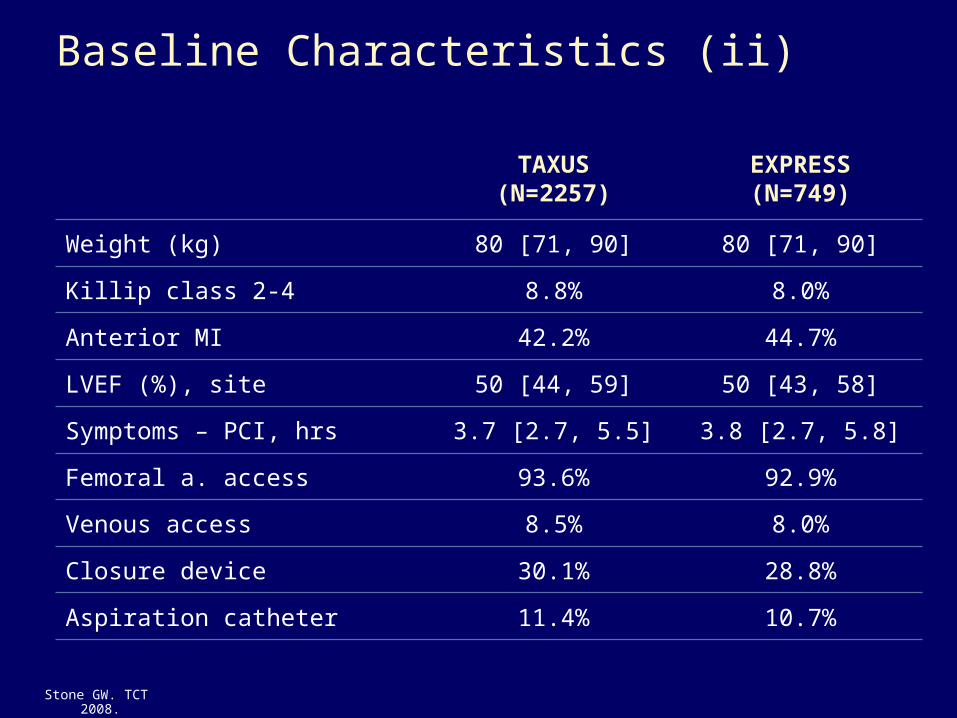
Baseline Characteristics (ii)
TAXUS(N=2257)
EXPRESS(N=749)
Weight (kg) 80 [71, 90] 80 [71, 90]
Killip class 2-4 8.8% 8.0%
Anterior MI 42.2% 44.7%
LVEF (%), site 50 [44, 59] 50 [43, 58]
Symptoms – PCI, hrs 3.7 [2.7, 5.5] 3.8 [2.7, 5.8]
Femoral a. access 93.6% 92.9%
Venous access 8.5% 8.0%
Closure device 30.1% 28.8%
Aspiration catheter 11.4% 10.7%
Stone GW. TCT 2008.
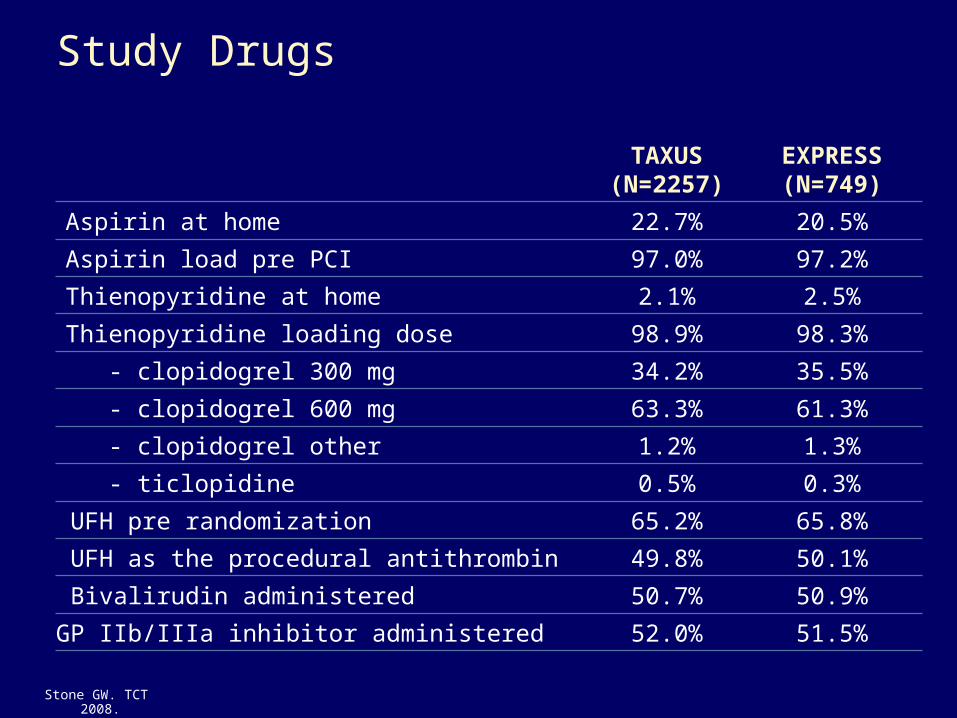
Study Drugs
TAXUS(N=2257)
EXPRESS(N=749)
Aspirin at home 22.7% 20.5%
Aspirin load pre PCI 97.0% 97.2%
Thienopyridine at home 2.1% 2.5%
Thienopyridine loading dose 98.9% 98.3%
- clopidogrel 300 mg 34.2% 35.5%
- clopidogrel 600 mg 63.3% 61.3%
- clopidogrel other 1.2% 1.3%
- ticlopidine 0.5% 0.3%
UFH pre randomization 65.2% 65.8%
UFH as the procedural antithrombin 49.8% 50.1%
Bivalirudin administered 50.7% 50.9%
GP IIb/IIIa inhibitor administered 52.0% 51.5%
Stone GW. TCT 2008.
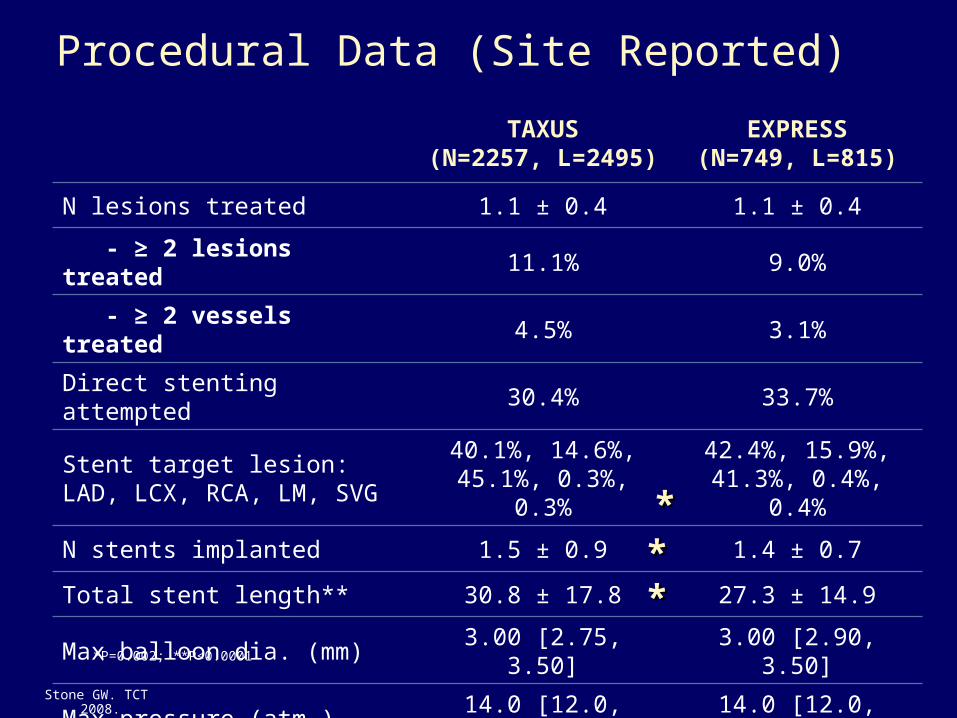
Procedural Data (Site Reported)
TAXUS(N=2257, L=2495)
EXPRESS(N=749, L=815)
N lesions treated 1.1 ± 0.4 1.1 ± 0.4
- ≥ 2 lesions treated 11.1% 9.0%
- ≥ 2 vessels treated 4.5% 3.1%
Direct stenting attempted 30.4% 33.7%
Stent target lesion:LAD, LCX, RCA, LM, SVG
40.1%, 14.6%, 45.1%, 0.3%, 0.3%
42.4%, 15.9%, 41.3%, 0.4%, 0.4%
N stents implanted 1.5 ± 0.9 1.4 ± 0.7
Total stent length** 30.8 ± 17.8 27.3 ± 14.9
Max balloon dia. (mm) 3.00 [2.75, 3.50] 3.00 [2.90, 3.50]
Max pressure (atm.) 14.0 [12.0, 16.0] 14.0 [12.0, 16.0]
*P=0.002; **P<0.0001
******
Stone GW. TCT 2008.
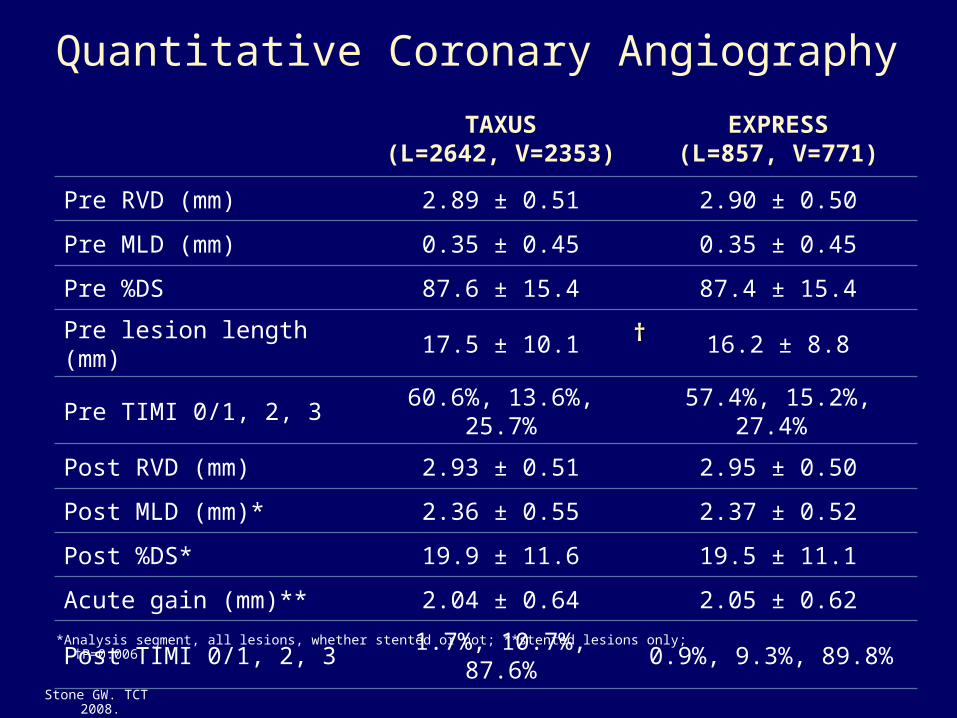
Quantitative Coronary Angiography
TAXUS(L=2642, V=2353)
EXPRESS(L=857, V=771)
Pre RVD (mm) 2.89 ± 0.51 2.90 ± 0.50
Pre MLD (mm) 0.35 ± 0.45 0.35 ± 0.45
Pre %DS 87.6 ± 15.4 87.4 ± 15.4
Pre lesion length (mm) 17.5 ± 10.1 16.2 ± 8.8
Pre TIMI 0/1, 2, 3 60.6%, 13.6%, 25.7% 57.4%, 15.2%, 27.4%
Post RVD (mm) 2.93 ± 0.51 2.95 ± 0.50
Post MLD (mm)* 2.36 ± 0.55 2.37 ± 0.52
Post %DS* 19.9 ± 11.6 19.5 ± 11.1
Acute gain (mm)** 2.04 ± 0.64 2.05 ± 0.62
Post TIMI 0/1, 2, 3 1.7%, 10.7%, 87.6% 0.9%, 9.3%, 89.8%
*Analysis segment, all lesions, whether stented or not; **stented lesions only; †P=0.006
††
Stone GW. TCT 2008.
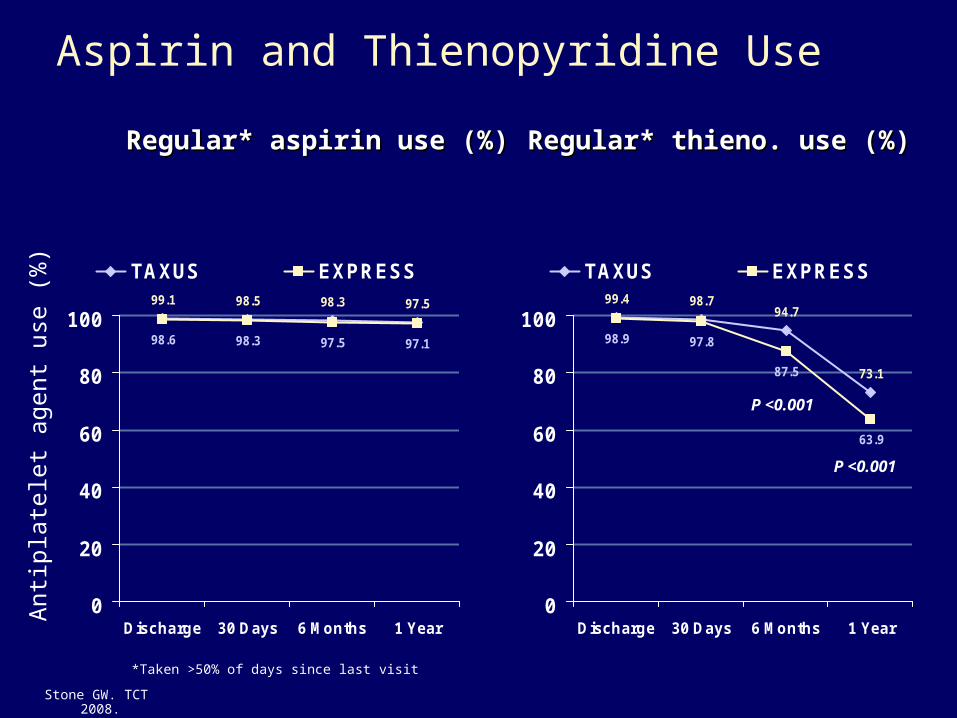
Aspirin and Thienopyridine Use
Regular* aspirin use (%)Regular* aspirin use (%) Regular* thieno. use (%)Regular* thieno. use (%)
*Taken >50% of days since last visit
99.1 98.5 98.3 97.5
98.6 98.3 97.5 97.1
0
20
40
60
80
100
Discharge 30 Days 6 Months 1 Year
TAXUS EXPRESS99.4 98.7
94.7
73.1
98.9 97.8
87.5
63.9
0
20
40
60
80
100
Discharge 30 Days 6 Months 1 Year
TAXUS EXPRESS
Ant
ipla
tele
t ag
ent
use
(%)
P <0.001
P <0.001
Stone GW. TCT 2008.
Time in Months
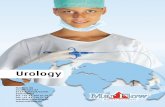
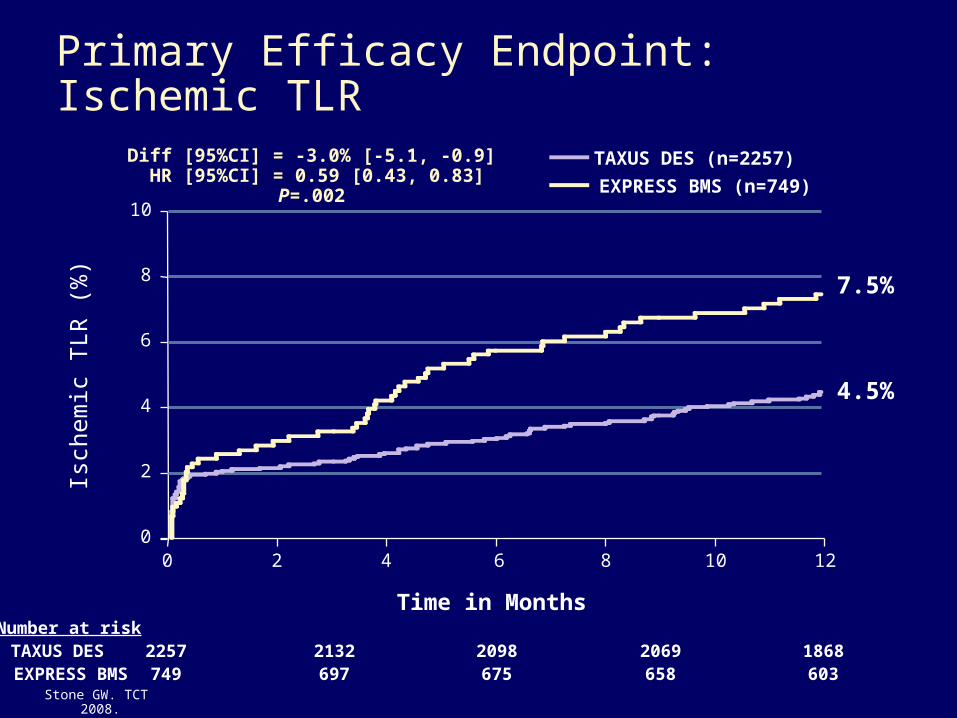
Primary Efficacy Endpoint: Ischemic TLR
Isch
emic
TLR
(%
)
0
4
8
10
0 2 4 6 8 10 12
Diff [95%CI] = -3.0% [-5.1, -0.9] HR [95%CI] = 0.59 [0.43, 0.83]
P=.002
TAXUS DES (n=2257)
EXPRESS BMS (n=749)
6
2
7.5%
4.5%
2257 2132 2098 2069 1868749 697 675 658 603
Number at riskTAXUS DESEXPRESS BMS
Stone GW. TCT 2008.
Time in Months
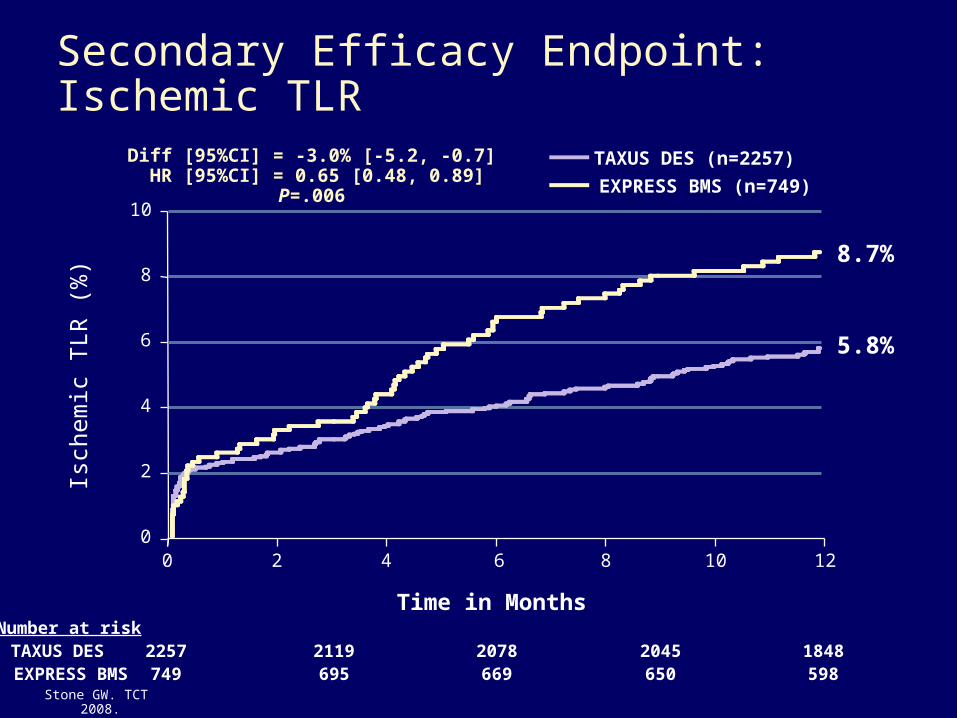
Secondary Efficacy Endpoint: Ischemic TLR
Isch
emic
TLR
(%
)
0
4
8
10
0 2 4 6 8 10 12
Diff [95%CI] = -3.0% [-5.2, -0.7] HR [95%CI] = 0.65 [0.48, 0.89]
P=.006
TAXUS DES (n=2257)
EXPRESS BMS (n=749)
6
2
8.7%
5.8%
2257 2119 2078 2045 1848749 695 669 650 598
Number at riskTAXUS DESEXPRESS BMS
Stone GW. TCT 2008.
Time in Months
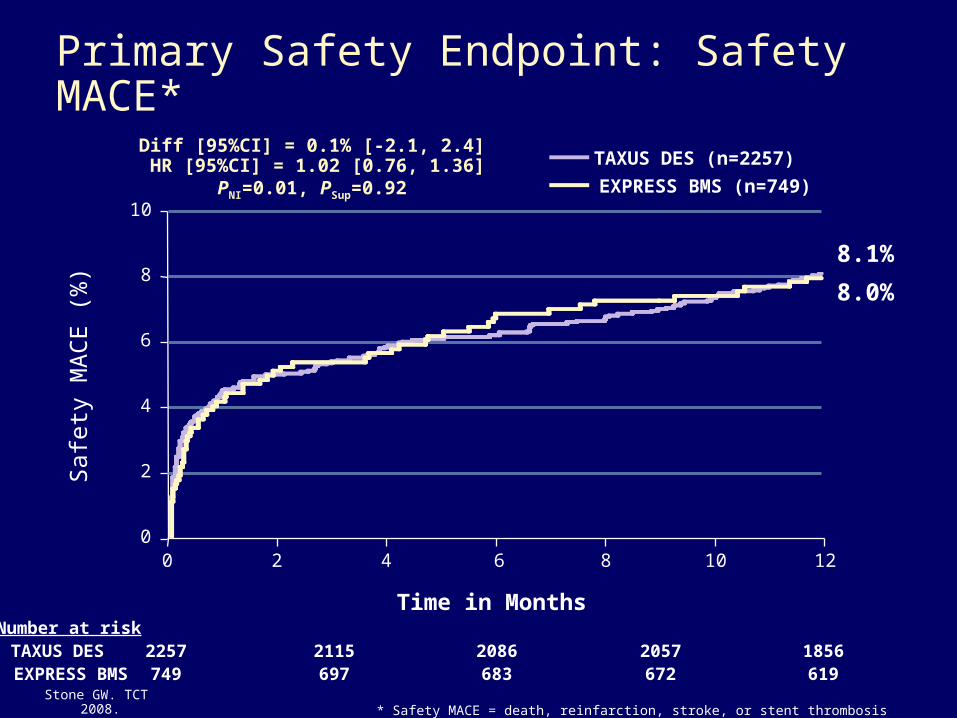
Primary Safety Endpoint: Safety MACE*S
afet
y M
AC
E (
%)
0
4
8
10
0 2 4 6 8 10 12
Diff [95%CI] = 0.1% [-2.1, 2.4] HR [95%CI] = 1.02 [0.76, 1.36]
PNI=0.01, PSup=0.92
TAXUS DES (n=2257)
EXPRESS BMS (n=749)
6
2
8.1%
8.0%
2257 2115 2086 2057 1856749 697 683 672 619
Number at riskTAXUS DESEXPRESS BMS
* Safety MACE = death, reinfarction, stroke, or stent thrombosisStone GW. TCT 2008.
Time in Months
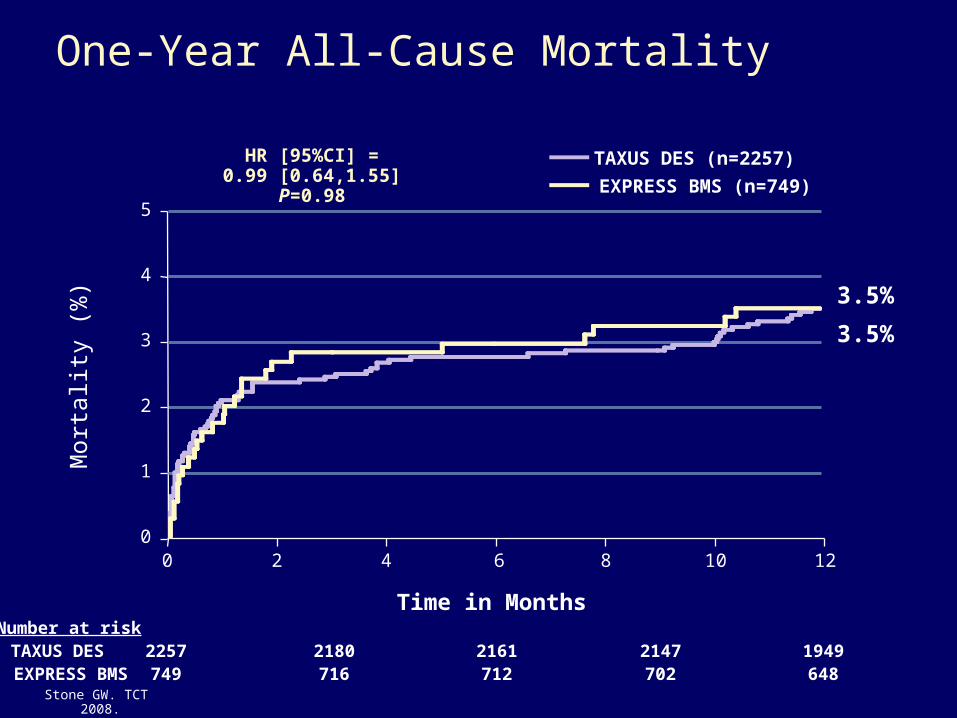
One-Year All-Cause MortalityM
orta
lity
(%)
0
2
4
5
0 2 4 6 8 10 12
HR [95%CI] =0.99 [0.64,1.55]
P=0.98
TAXUS DES (n=2257)
EXPRESS BMS (n=749)
3
1
3.5%
3.5%
2257 2180 2161 2147 1949749 716 712 702 648
Number at riskTAXUS DESEXPRESS BMS
Stone GW. TCT 2008.
Time in Months
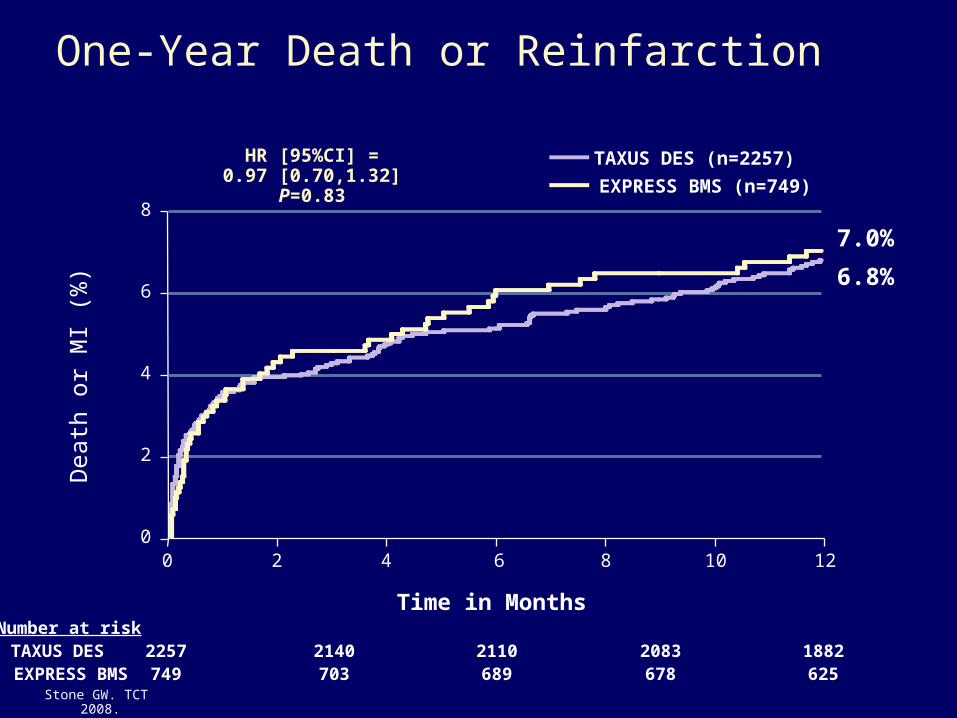
One-Year Death or ReinfarctionD
eath
or
MI
(%)
0
2
6
8
0 2 4 6 8 10 12
HR [95%CI] =0.97 [0.70,1.32]
P=0.83
TAXUS DES (n=2257)
EXPRESS BMS (n=749)
4
7.0%
6.8%
2257 2140 2110 2083 1882749 703 689 678 625
Number at riskTAXUS DESEXPRESS BMS
Stone GW. TCT 2008.
Time in Months
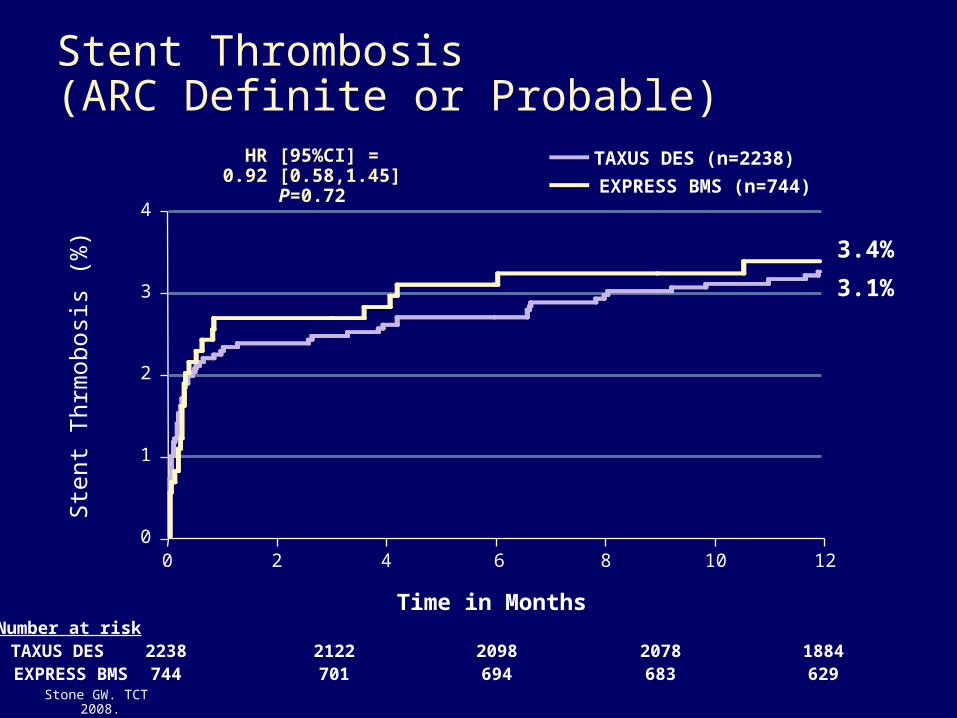
Stent Thrombosis (ARC Definite or Probable)
Ste
nt T
hrm
obos
is (
%)
0
1
3
4
0 2 4 6 8 10 12
HR [95%CI] =0.92 [0.58,1.45]
P=0.72
TAXUS DES (n=2238)
EXPRESS BMS (n=744)
2
3.4%
3.1%
2238 2122 2098 2078 1884744 701 694 683 629
Number at riskTAXUS DESEXPRESS BMS
Stone GW. TCT 2008.
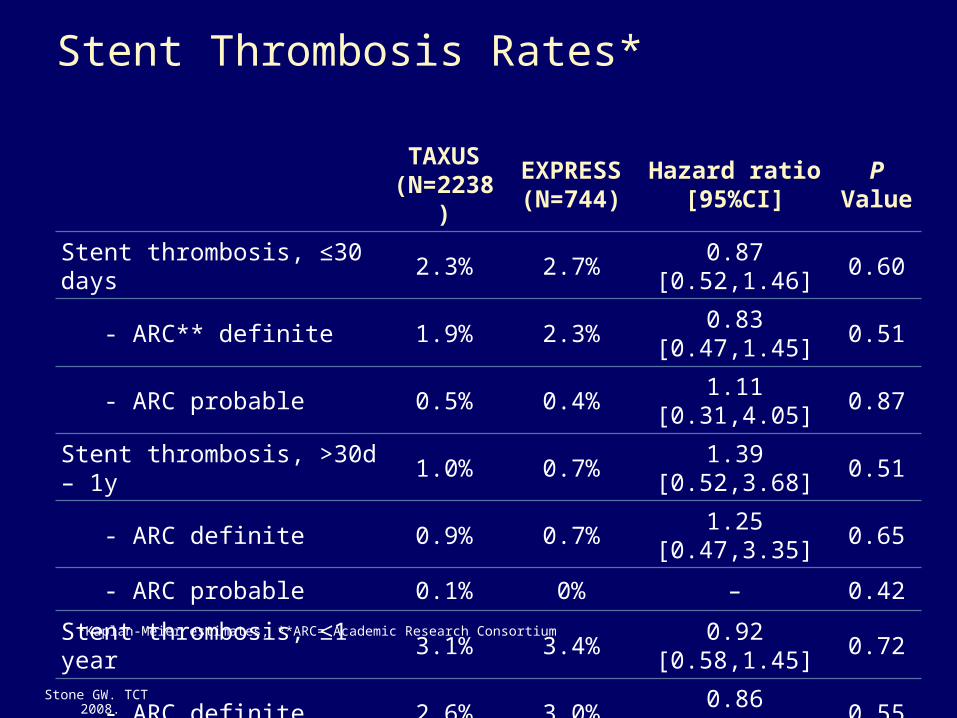
Stent Thrombosis Rates*
TAXUS(N=2238)
EXPRESS(N=744)
Hazard ratio[95%CI]
P Value
Stent thrombosis, ≤30 days 2.3% 2.7% 0.87 [0.52,1.46] 0.60
- ARC** definite 1.9% 2.3% 0.83 [0.47,1.45] 0.51
- ARC probable 0.5% 0.4% 1.11 [0.31,4.05] 0.87
Stent thrombosis, >30d – 1y 1.0% 0.7% 1.39 [0.52,3.68] 0.51
- ARC definite 0.9% 0.7% 1.25 [0.47,3.35] 0.65
- ARC probable 0.1% 0% – 0.42
Stent thrombosis, ≤1 year 3.1% 3.4% 0.92 [0.58,1.45] 0.72
- ARC definite 2.6% 3.0% 0.86 [0.53,1.41] 0.55
- ARC probable 0.5% 0.4% 1.33 [0.38,4.73] 0.65
*Kaplan-Meier estimates, **ARC= Academic Research Consortium
Stone GW. TCT 2008.
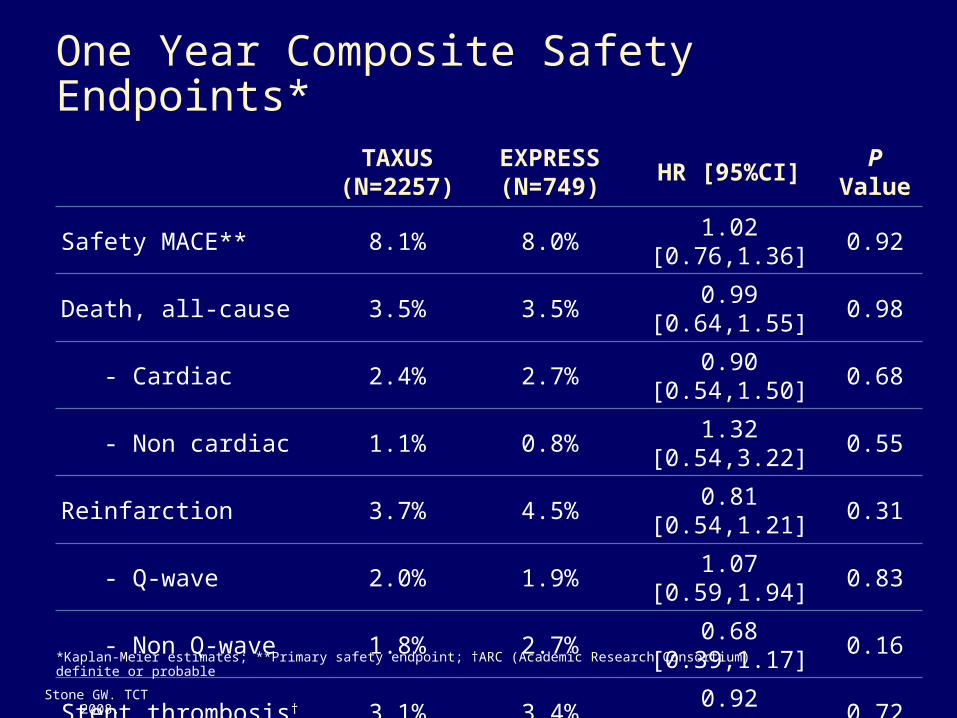
One Year Composite Safety Endpoints*
TAXUS(N=2257)
EXPRESS(N=749)
HR [95%CI]P
Value
Safety MACE** 8.1% 8.0% 1.02 [0.76,1.36] 0.92
Death, all-cause 3.5% 3.5% 0.99 [0.64,1.55] 0.98
- Cardiac 2.4% 2.7% 0.90 [0.54,1.50] 0.68
- Non cardiac 1.1% 0.8% 1.32 [0.54,3.22] 0.55
Reinfarction 3.7% 4.5% 0.81 [0.54,1.21] 0.31
- Q-wave 2.0% 1.9% 1.07 [0.59,1.94] 0.83
- Non Q-wave 1.8% 2.7% 0.68 [0.39,1.17] 0.16
Stent thrombosis† 3.1% 3.4% 0.92 [0.58,1.45] 0.72
- ARC definite 2.6% 3.0% 0.86 [0.53,1.41] 0.55
- ARC probable 0.5% 0.4% 1.33 [0.38,4.73] 0.65
Stroke 1.0% 0.7% 1.52 [0.58,4.00] 0.39
*Kaplan-Meier estimates; **Primary safety endpoint; †ARC (Academic Research Consortium) definite or probable
Stone GW. TCT 2008.
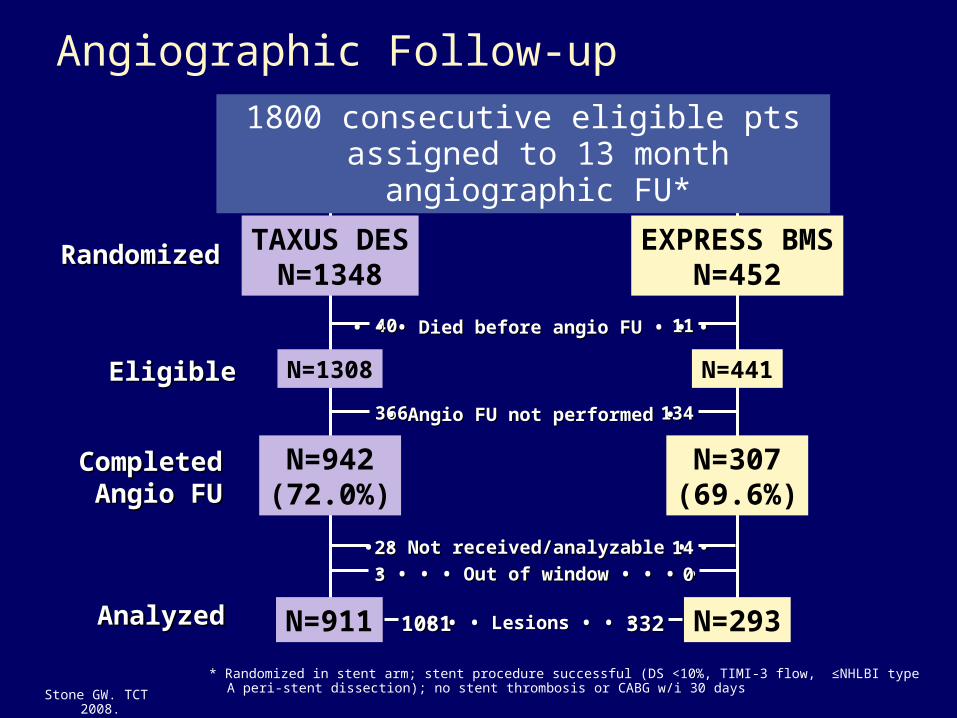
Angiographic Follow-up
TAXUS DESN=1348
EXPRESS BMSN=452
RandomizedRandomized
EligibleEligible N=1308 N=441
1800 consecutive eligible pts assigned to 13 month angiographic FU*
* Randomized in stent arm; stent procedure successful (DS <10%, TIMI-3 flow, ≤NHLBI type A peri-stent dissection); no stent thrombosis or CABG w/i 30 days
4040 1111• • • • • • Died before angio FU • • • Died before angio FU • • •
N=942(72.0%)
N=307(69.6%)
CompletedCompletedAngio FUAngio FU
366366 134134 • • Angio FU not performed • Angio FU not performed •
• • • • Not received/analyzable • •Not received/analyzable • •
• • • • • • • • Out of window • • • •Out of window • • • •2828
331414
00
N=911 N=293AnalyzedAnalyzed • • • • • • Lesions • • • Lesions • • • 10811081 332332
Stone GW. TCT 2008.
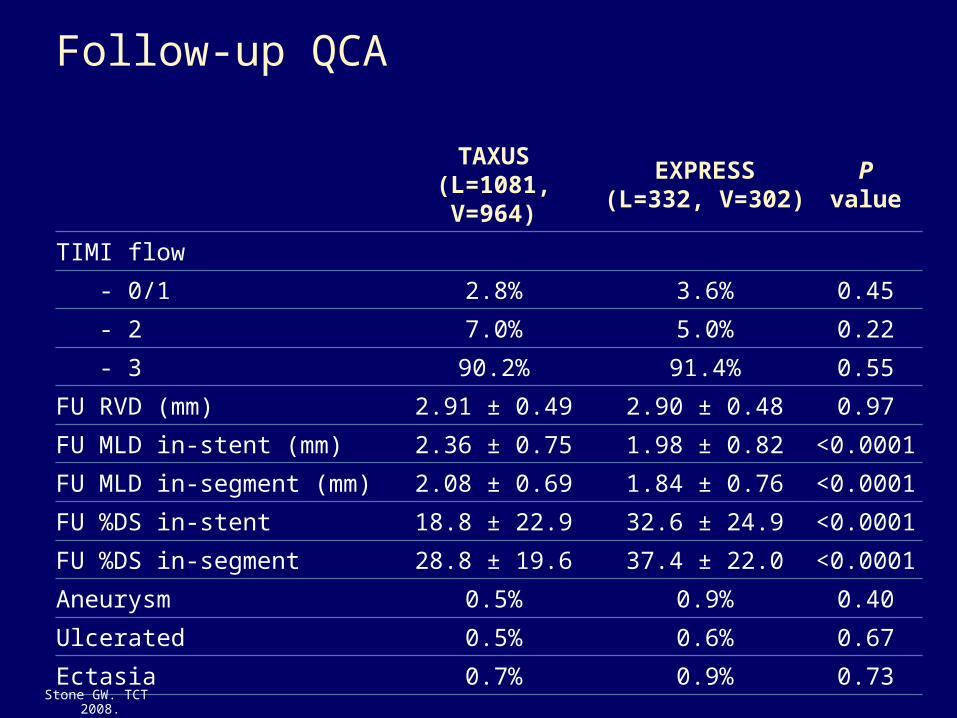
Follow-up QCA
TAXUS(L=1081, V=964)
EXPRESS(L=332, V=302)
Pvalue
TIMI flow
- 0/1 2.8% 3.6% 0.45
- 2 7.0% 5.0% 0.22
- 3 90.2% 91.4% 0.55
FU RVD (mm) 2.91 ± 0.49 2.90 ± 0.48 0.97
FU MLD in-stent (mm) 2.36 ± 0.75 1.98 ± 0.82 <0.0001
FU MLD in-segment (mm) 2.08 ± 0.69 1.84 ± 0.76 <0.0001
FU %DS in-stent 18.8 ± 22.9 32.6 ± 24.9 <0.0001
FU %DS in-segment 28.8 ± 19.6 37.4 ± 22.0 <0.0001
Aneurysm 0.5% 0.9% 0.40
Ulcerated 0.5% 0.6% 0.67
Ectasia 0.7% 0.9% 0.73
Stone GW. TCT 2008.
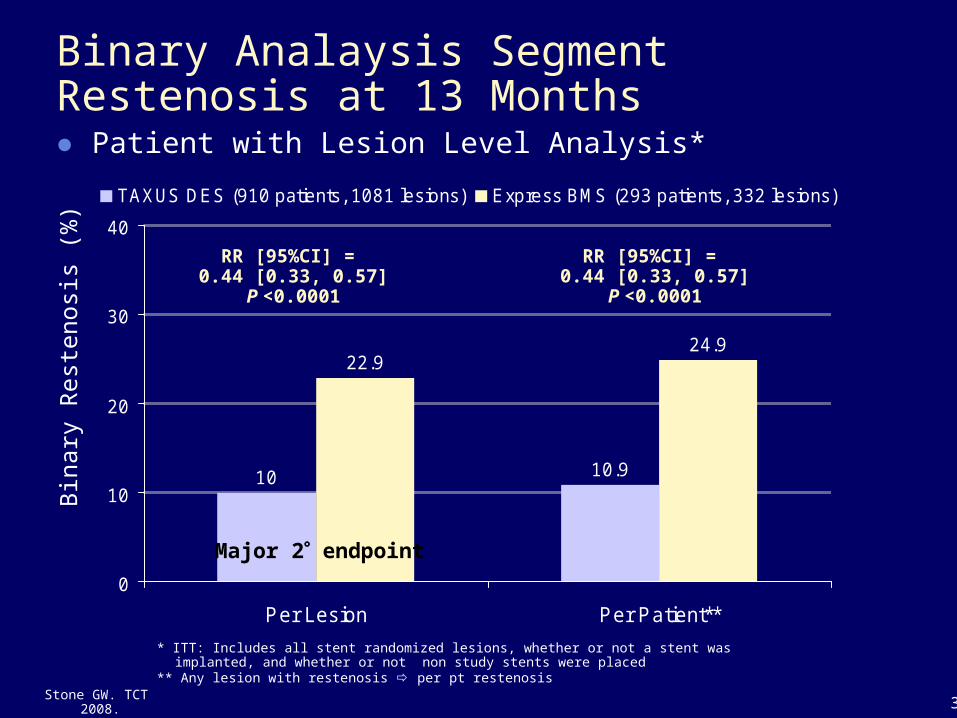
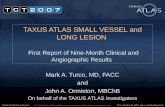
10 10.9
22.924.9
0
10
20
30
40
Per Lesion Per Patient**
TAXUS DES (910 patients, 1081 lesions) Express BMS (293 patients, 332 lesions)
Binary Analaysis Segment Restenosis at 13 Months● Patient with Lesion Level Analysis*
Bin
ary
Res
teno
sis
(%)
32
* ITT: Includes all stent randomized lesions, whether or not a stent was implanted, and whether or not non study stents were placed
** Any lesion with restenosis per pt restenosis
RR [95%CI] = 0.44 [0.33, 0.57]
P <0.0001
RR [95%CI] = 0.44 [0.33, 0.57]
P <0.0001
Major 2 endpoint
Stone GW. TCT 2008.
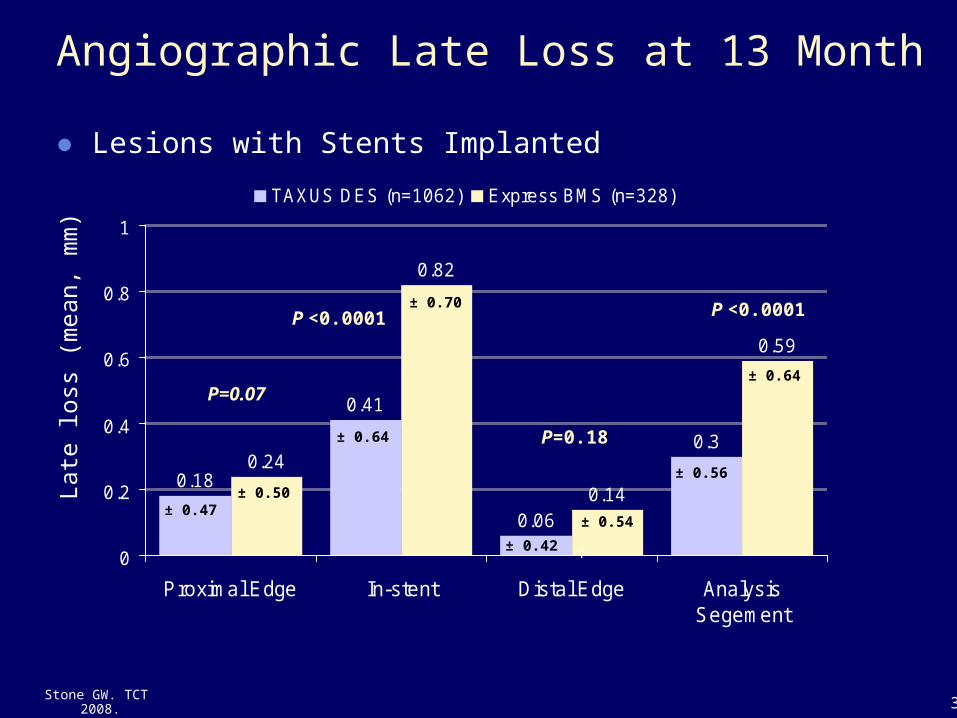
0.18
0.41
0.06
0.30.24
0.82
0.14
0.59
0
0.2
0.4
0.6
0.8
1
Proximal Edge In-stent Distal Edge AnalysisSegement
TAXUS DES (n=1062) Express BMS (n=328)
Angiographic Late Loss at 13 Month
● Lesions with Stents Implanted
P <0.0001
P=0.07
Late
loss
(m
ean,
mm
)
†
33
P=0.18
P <0.0001
± 0.42
± 0.54
± 0.64
± 0.70
± 0.56
± 0.64
± 0.47 ± 0.50
Stone GW. TCT 2008.
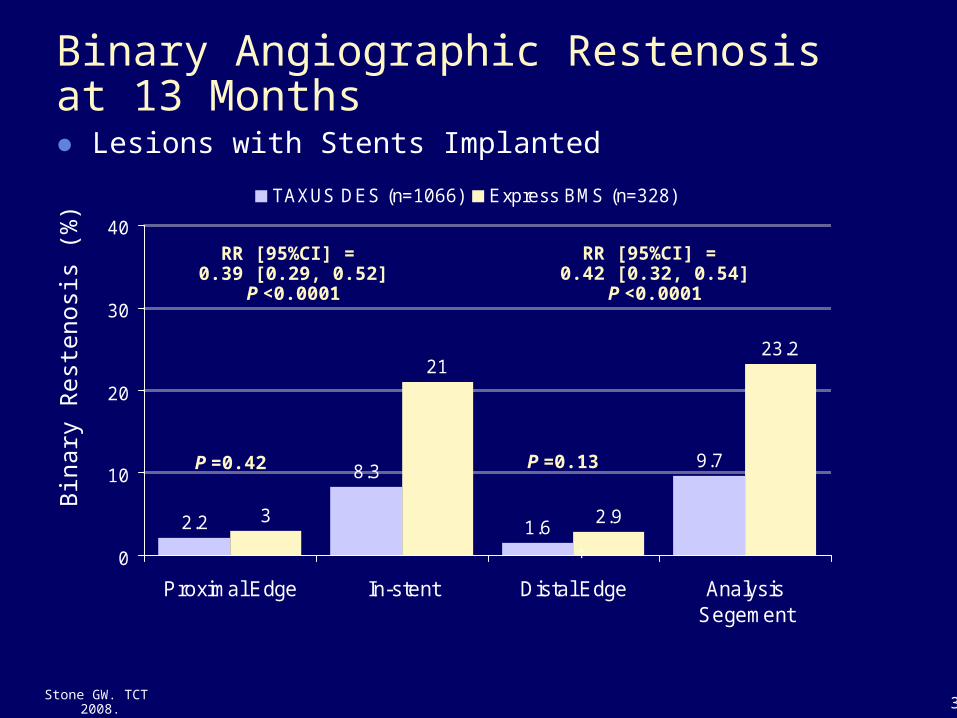
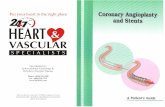
2.2
8.3
1.6
9.7
3
21
2.9
23.2
0
10
20
30
40
Proximal Edge In-stent Distal Edge AnalysisSegement
TAXUS DES (n=1066) Express BMS (n=328)
Binary Angiographic Restenosisat 13 Months● Lesions with Stents Implanted
†
34
Bin
ary
Res
teno
sis
(%)
RR [95%CI] = 0.42 [0.32, 0.54]
P <0.0001
RR [95%CI] = 0.39 [0.29, 0.52]
P <0.0001
Stone GW. TCT 2008.
P =0.13P =0.42
Limitations
● Open label design– Potential bias was mitigated by high protocol procedure
compliance and use of blinded clinical event adjudication committees and core laboratories
● Underpowered for stent thrombosis and death– The virtually identical rates of MACE in the TAXUS and
EXPRESS groups makes it unlikely that major safety differences exist favoring either stent type at 1-year
Stone GW. TCT 2008.
Conclusions
● In this large-scale, prospective, randomized trial of pts with STEMI undergoing primary stenting, the implantation of paclitaxel-eluting TAXUS stents compared to bare metal EXPRESS stents resulted in:– A significant 41% reduction in the 1-year primary efficacy
endpoint of ischemia-driven TLR, and a significant 56% reduction in the 13 month major secondary efficacy endpoint of binary restenosis
– Non inferior rates of the primary composite safety endpoint of all cause death, reinfarction, stent thrombosis or stroke at 1-year
Stone GW. TCT 2008.
Conclusions
● The long-term safety and efficacy profile of paclitaxel-eluting TAXUS stents compared to bare metal EXPRESS stents in STEMI will be determined by the ongoing 5 year follow-up of patients randomized in the HORIZONS-AMI trial
Stone GW. TCT 2008.