A Preliminary Evaluation of the Lunar Expert-XL for Bone Densitometry and Vertebral Morphometry
8
A Preliminary Evaluation of the Lunar Expert-XL for Bone Densitometry and Vertebral Morphometry* THOMAS LANG, MASAHIKO TAKADA, RICHARD GEE, CHUN WU, JIAO LI, CYNTHIA HAYASHI-CLARK, SUSAN SCHOEN, VESTA MARCH, and HARRY K. GENANT ABSTRACT We have evaluated the Lunar Expert-XL for standard bone mineral densitometry (BMD) and for morphometric imaging of the spine in the lateral projection. The short-term precision in vitro of the Expert-XL for BMD measurements was 0.7% for the Hologic and European spine phantoms, and the long-term stability (15-month) measurements had a 1.1% coefficient of variation. The precision in vivo for three operators examining a group of 10 premenopausal women was 0.9 –1.5% for lumbar spine (L2–L4), 1.7–2.2% for the femoral neck, and 0.9% for the total hip region of interest. For a group of nine postmenopausal women, the lumbar spine, femoral neck, and total femur precision ranges were 2.0 –2.4, 1.2–2.9, and 1.6 –1.7% respectively. For L2–L4, BMD comparison between the Expert-XL and DPX-L yielded a correlation coefficient of r 5 0.98, a slope of 0.86, and an intercept of 0.139 g/cm 2 . The femoral neck results were r 5 0.92, slope 5 1.00, and intercept 5 0.03 g/cm 2 . In an evaluation of the Expert-XL for lateral morphometry, we employed a group of 16 postmenopausal women. Comparison of vertebral dimensions between the Expert-XL and radiographic morphometry showed strong agreement (r 5 0.97), but the interobserver variability for vertebral height was higher for the Expert-XL than for radiographs (3–5% vs. 1–2%). In a subset of four women who had repeat scans, the interscan precision for measuring vertebral dimensions was 1.9, 4.1, and 4.3% for the L1–L4, T12–T8, and T7–T5 levels respectively. In the Expert-XL images, it was possible to identify clearly L4 –T4 in 10 of 16 patients and L4 –T6 in 15 of 16, indicating potential utility for vertebral fracture prescreening. (J Bone Miner Res 1997;12:136–143) INTRODUCTION S INCE ITS INCEPTION nearly a decade ago, dual-energy X-ray absorptiometry (DXA) has become a primary noninva- sive method for measurement of bone mineral density (BMD) for diagnosis and follow-up of metabolic bone dis- ease. (1– 6) The wide clinical use of DXA has been based on its low radiation dose, good precision, and the large number of skeletal sites it is capable of measuring. The technique has benefited from continual refinement, reducing both acquisition times and precision errors. (7,8) The newest gen- eration of DXA systems is embodied by the Lunar Ex- pert-XL (Lunar Corp., Madison, WI, U.S.A.) and the Ho- logic QDR-4500 (Hologic, Waltham, MA, U.S.A.). With both of these systems, a high-resolution detector array, coupled to an X-ray tube in a fanbeam geometry, is mounted on a rotateable C-arm gantry. In evaluating the impact of these changes, two major issues must be ad- dressed. On the one hand, densitometric precision errors may be reduced by improved definition of bone edges and intervertebral spaces, while on the other hand, they may be increased by the combination of a fanbeam geometry and the highly complex detector array and its associated elec- tronics. Also, in the lateral projection, these systems may resolve the vertebral endplates more clearly than previous *Part of this work was presented at the Meeting of the American Society for Bone and Mineral Research, Baltimore, MD, U.S.A., September 9 –13, 1995 (Lang T, Fan B, Wu C, et al. 1995 Assess- ment of vertebral deformation with a high-resolution fanbeam bone densitometer. JBMR 10:M461.) Osteoporosis Research Group, Department of Radiology, University of California–San Francisco, San Francisco, California, U.S.A. JOURNAL OF BONE AND MINERAL RESEARCH Volume 12, Number 1, 1997 Blackwell Science, Inc. q 1997 American Society for Bone and Mineral Research 136
-
Upload
thomas-lang -
Category
Documents
-
view
212 -
download
0
Transcript of A Preliminary Evaluation of the Lunar Expert-XL for Bone Densitometry and Vertebral Morphometry

A Preliminary Evaluation of the Lunar Expert-XL forBone Densitometry and Vertebral Morphometry*
THOMAS LANG, MASAHIKO TAKADA, RICHARD GEE, CHUN WU, JIAO LI,CYNTHIA HAYASHI-CLARK, SUSAN SCHOEN, VESTA MARCH, and HARRY K. GENANT
ABSTRACT
We have evaluated the Lunar Expert-XL for standard bone mineral densitometry (BMD) and for morphometricimaging of the spine in the lateral projection. The short-term precision in vitro of the Expert-XL for BMDmeasurements was 0.7% for the Hologic and European spine phantoms, and the long-term stability (15-month)measurements had a 1.1% coefficient of variation. The precision in vivo for three operators examining a group of10 premenopausal women was 0.9–1.5% for lumbar spine (L2–L4), 1.7–2.2% for the femoral neck, and 0.9% for thetotal hip region of interest. For a group of nine postmenopausal women, the lumbar spine, femoral neck, and totalfemur precision ranges were 2.0–2.4, 1.2–2.9, and 1.6–1.7% respectively. For L2–L4, BMD comparison between theExpert-XL and DPX-L yielded a correlation coefficient of r5 0.98, a slope of 0.86, and an intercept of 0.139 g/cm2.The femoral neck results were r5 0.92, slope5 1.00, and intercept5 0.03 g/cm2. In an evaluation of the Expert-XLfor lateral morphometry, we employed a group of 16 postmenopausal women. Comparison of vertebral dimensionsbetween the Expert-XL and radiographic morphometry showed strong agreement (r5 0.97), but the interobservervariability for vertebral height was higher for the Expert-XL than for radiographs (3–5% vs. 1–2%). In a subset offour women who had repeat scans, the interscan precision for measuring vertebral dimensions was 1.9, 4.1, and4.3% for the L1–L4, T12–T8, and T7–T5 levels respectively. In the Expert-XL images, it was possible to identifyclearly L4–T4 in 10 of 16 patients and L4–T6 in 15 of 16, indicating potential utility for vertebral fractureprescreening. (J Bone Miner Res 1997;12:136–143)
INTRODUCTION
SINCE ITS INCEPTION nearly a decade ago, dual-energy X-rayabsorptiometry (DXA) has become a primary noninva-
sive method for measurement of bone mineral density(BMD) for diagnosis and follow-up of metabolic bone dis-ease.(1–6) The wide clinical use of DXA has been based onits low radiation dose, good precision, and the large numberof skeletal sites it is capable of measuring. The techniquehas benefited from continual refinement, reducing both
acquisition times and precision errors.(7,8) The newest gen-eration of DXA systems is embodied by the Lunar Ex-pert-XL (Lunar Corp., Madison, WI, U.S.A.) and the Ho-logic QDR-4500 (Hologic, Waltham, MA, U.S.A.). Withboth of these systems, a high-resolution detector array,coupled to an X-ray tube in a fanbeam geometry, ismounted on a rotateable C-arm gantry. In evaluating theimpact of these changes, two major issues must be ad-dressed. On the one hand, densitometric precision errorsmay be reduced by improved definition of bone edges andintervertebral spaces, while on the other hand, they may beincreased by the combination of a fanbeam geometry andthe highly complex detector array and its associated elec-tronics. Also, in the lateral projection, these systems mayresolve the vertebral endplates more clearly than previous
*Part of this work was presented at the Meeting of the AmericanSociety for Bone and Mineral Research, Baltimore, MD, U.S.A.,September 9–13, 1995 (Lang T, Fan B, Wu C, et al. 1995 Assess-ment of vertebral deformation with a high-resolution fanbeambone densitometer. JBMR 10:M461.)
Osteoporosis Research Group, Department of Radiology, University of California–San Francisco, San Francisco, California, U.S.A.
JOURNAL OF BONE AND MINERAL RESEARCHVolume 12, Number 1, 1997Blackwell Science, Inc.q 1997 American Society for Bone and Mineral Research
136

densitometry systems, providing improved evaluation ofvertebral fracture.At our institution, over the last 15 months, we have
carried out a performance evaluation of the Lunar Ex-pert-XL bone densitometer. The Expert-XL features a cur-rent-integrating detector array with 288 0.8-mm elementsmounted on a C-arm opposite a rotating-anode X-ray tube.Dual-energy imaging is achieved by filtration of the X-raybeam and use of detector arrays sensitive to lower andhigher energy X-rays. The detector arrays and X-ray tubeare mounted on a C-arm gantry that can rotate 908 forsupine lateral examinations of the spine.Because this new system can perform both standard an-
teroposterior (AP) densitometry and high resolution spineimaging, our performance evaluation contains both densi-tometric and morphometric studies. To evaluate the impli-cations of this new system for BMD studies, we performedmeasurements in vitro and in vivo on both Expert-XL andDPX-L systems. Measurements in vitro included short-termand long-term precision as well as BMD response to vari-ations in lean and adipose soft-tissue thickness. In vivo, weevaluated the precision for AP-spine and femur studies aswell as the correlation between BMD measurements on theExpert-XL and DPX-L. To evaluate the capability of thissystem for lateral morphometry, we performed a study invivo comparing morphometric measurements on the Ex-pert-XL to morphometric measurements from lateralradiographs.
MATERIALS AND METHODS
BMD studies in vitro
Short-term precision of the Expert-XL was measured by10 repeat scans of a spine phantom (Hologic). Long-termprecision was evaluated by daily scans of the same spinephantom (Hologic) over a period of 15 months. Linearity ofBMD response for the Expert-XL was measured by 10repeat scans of the European Spine Phantom (QRM, Moh-rendorf, Germany) and calculated as the standard estimateof the error (SEE) of the regression between the measuredand the known BMD values of the three vertebral inserts.BMD response to variable soft-tissue thickness was evalu-ated on both the Expert-XL and DPX-L by imaging differ-ent thicknesses of water and acrylic placed uniformly overan aluminum spine phantom (Lunar). BMD response tochanges in vertebral fat content was determined on both theExpert-XL and DPX-L by imaging vertebral inserts with150 mg/cc BMD containing 0, 15, 30, and 50% fat by volumeand placed atop a 10-cm layer of acrylic.
Human subjects
For BMD studies, 10 young, healthy women (average age32 6 8 years, average BMD 1.18 6 0.12 g/cm2) and 9healthy postmenopausal women (average age 63 6 9 years,average BMD 1.036 0.14 g/cm2) were recruited. For lateralmorphometry studies, 16 postmenopausal women (averageage 67 6 14 years) were recruited. For all subjects, in-formed consent was obtained according to the policies and
procedures of the Committee on Human Research of theUniversity of California at San Francisco.
BMD studies in vivo
Subjects underwent repeat supine AP spine and femurimaging, with repositioning between scans, on both theExpert-XL and the DPX-L. On the Expert-XL, all scanswere performed in the “fast” mode. On the DPX-L, pa-tients were scanned in the “fast” or “medium” mode basedon body thickness according to the guidelines of themanufacturer.
Analysis of BMD image data
The duplicate AP spine and hip scans were analyzedusing Expert-XL software version 1.4 and DPX-L version1.3Z. Analysis of Expert-XL spine images was performed asfollows. The bone edges were first carefully evaluated andadjusted for appropriateness in one scan, and subsequentlythe edges in the second scan were adjusted, if necessary, forconsistency with the first scan. Next, the L1–L4 regions ofinterest (ROIs) in the first scan were placed with carefuladjustment of the intervertebral (IV) spaces. The ROIs ofthe first scan were then mapped to the second scan usingthe “compare” feature, but the IV spaces were adjusted ifnecessary. To determine the impact of automated edgedetection on the AP-spine precision values, the scans wereadditionally analyzed with careful adjustment of IV spacesbut without adjustment of the bone edges. For Expert-XLAP femur scans, the automated software was employed todetermine the bone edges and to place the standard ROIs(femoral neck, trochanter, Ward’s triangle, and total hip),but the ischium was manually “painted out” if the femoralneck ROI overlapped with it. To determine the componentof precision error due to inter-operator variation of theExpert-XL analysis software, the spine and hip images wereanalyzed separately and independently by three trainedobservers.
BMD precision measurements
In vitro, precision was determined as the percentagecoefficient of variation (%CV), defined as the standarddeviation (SD) of the n measurements normalized by themean value. In vivo, precision was calculated as the rootmean square (RMS) %CV of the pairwise scans as sug-gested by Gluer.(9) Interoperator variation was equivalentlycalculated as the RMS %CV of the three operators for oneset of scans.
Correlation of BMD measurements between theExpert-XL and DPX-L
Interdevice comparison of BMD was performed by linearregression of the means of the paired spine and hip scans onthe Expert-XL and DPX-L. The spine comparison wasbased on the L2–L4 ROI, and the hip comparison wasbased on the femoral neck ROI.
PERFORMANCE EVALUATION OF THE LUNAR EXPERT-XL 137

Acquisition and analysis of lateral spine images
Patients lay supine on the Expert-XL imaging table andhad lateral spine scans, which were performed in the “fastmode” (134 kVp, 5 mA, 10 mm/s scan speed) or the “me-dium mode” (134 kVp, 5 mA, 5 mm/s scan speed) depend-ing on the manufacturer’s guidelines for patient thickness.Four of the patients had duplicate Expert-XL scans forassessment of interscan precision. To determine vertebralheights from the Expert-XL images, two experienced ob-servers placed fiducial points at the inferior and superiormid-, anterior, and posterior locations on the vertebralendplates for levels T4–L4. These points were placed in-teractively on the terminal of the Expert-XL computerworkstation. The mid-, anterior, and posterior vertebralheights were then calculated as the distance between theinferior and superior points at each of the three locations.Where either observer determined that the vertebral levelwas not sufficiently visualized, that level was recorded andexcluded from further analysis. Following acquisition of theExpert-XL image, patients had conventional lateral tho-racic and lumbar radiographs in the decubitus projectionusing a technique of 80 kVp, 70 mA, and a 2-s exposure,with a film-to-focus distance of 100 cm. The lumbar andthoracic exposures were centered over L3 and T7, respec-tively. The radiographs were then placed on a digitizingtablet, and the two observers marked the locations of the sixvertebral fiducial points for L4–T4. The posterior mid- andanterior vertebral heights were then computed as before.Additionally, for both Expert-XL and radiographic datasets, the AP, mid-posterior (MP), and mid-anterior (MA)height ratios were calculated. Several comparisons betweenradiographs and Expert-XL were made.First, the interobserver variation was computed for each
vertebral level both on the radiographs and on the Ex-pert-XL images. For ratios and heights, for each vertebrallevel, the interobserver variance was computed as the RMSof the differences (RMSD) between the two observers. Tocompare vertebral heights between modalities, a linear re-gression was performed between Expert-XL images andradiographs. Comparison of vertebral height ratios was per-formed by computing the RMSD of height ratios betweenthe two modalities. Interscan precision for the Expert-XLvertebral heights was calculated as the RMS %CV of theduplicate scans on four volunteers. This was calculatedseparately for the lumbar vertebral levels (16 vertebrae),the lower-thoracic vertebral levels T12–T8 (20 vertebrae),and the upper thoracic levels T7–T5 (9 vertebrae). Finally,it should be noted that although the two observers prospec-tively agreed on general guidelines for evaluation of theimages, specific cases were analyzed separately without dis-cussion between them.
RESULTS
BMD studies in vitro
Short-term precision of the Expert-XL was 0.7% for boththe Hologic and European Spine Phantoms. The long-term(15-month) in vitro BMDmeasurements had a 1.1% overall
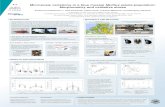
CV (Fig. 1), which was larger than normally observed forLunar DPX systems as monitored in clinical BMD trials byour laboratory. The variance could be attributed to signif-icant discontinuities, or shifts of the mean, in the BMDmeasurements as identified by a cumulative sum (CUSUM)analysis.(10) Scans of the European spine phantom showedthat the response of the Expert-XL to changes in BMD washighly linear, giving a 0.006 g/cm2 SEE. Response of Ex-pert-XL BMD measurements to differences in thicknessesof fat, water, and acrylic are demonstrated in Figs. 2–4. Thefat dependence of the two systems were almost identicaland were consistent with the 0.012 g/cm2 value reported byGluer for the QDR-1000 under identical conditions.(11)
There was a statistically significant dependence of BMD onthe thickness of acrylic but not on the thickness of water,and this held for both the DPX-L and the Expert-XL. Therewas no significant dependence of BMD on variation of tableheight.
BMD studies in vivo
Precision values obtained by each observer for Ex-pert-XL spine and hip ROIs are summarized in Table 1.
FIG. 1. Results of daily spine phantom scans acquiredover an 8-month period. Vertical dashed lines representdiscontinuities in BMD detected by a CUSUM statisticalanalysis program.
FIG. 2. Decrease of observed BMD with increasing %fatvolume as measured on the (a) Expert-XL and (b) DPX-L.
138 LANG ET AL.

Precision values for the corresponding measurements onthe DPX-L are summarized in Table 2. When the boneedges calculated by the Expert-XL spine software were notmodified, the L1–L4 precision values obtained by observers1 and 2 worsened from 0.9–1.1% to 1.5–1.8%. Interob-server variations for the Expert-XL spine and hip ROIs aresummarized in Table 3. Figures 5a and 5b represent thedegree of intersystem correlation observed for the L2–L4and femoral neck ROIs.
Lateral spine imaging
Figure 6 is an image of a 51-year-old volunteer in whichvertebral levels from L4 to T4 could be visualized. Gener-ally, the Expert-XL images showed clear definition of thelumbar and lower thoracic vertebral endplates, but theupper thoracic vertebral endplates could not be defined insome of the patients due to low contrast and the presence ofartifacts from overlying tissues. The effect of variable tho-racic image quality is described in Table 4, which summa-rizes the distribution of highest analyzable vertebral levelsfor the two observers. It should be noted that the twoobservers’ results agreed on identification of excluded levelsin 10 of 16 images. Interobserver variations for vertebralheights are compared for Expert-XL images and conven-tional radiographs in Tables 5 and 6. The correspondingvalues for vertebral height ratios were very similar. The
interobserver variation for the Expert-XL was generallyhigher than that for radiographs, but neither techniqueshowed a clear dependence on vertebral level. Regressionanalysis showed a highly linear correlation between verte-bral heights measured on the two modalities. AlthoughFig. 7 demonstrates this relationship for anterior heights,the same relation held true for posterior and mid-vertebraldimensions. Table 7 shows the RMSD for vertebral height
FIG. 3. Comparison of BMD response to varying thick-ness of water for the (a) Expert-XL and (b) DPX-L. Thevariation with water thickness may indicate the response ofthe systems to increasing lean body mass.
FIG. 4. Comparison of BMD response to varying thick-ness of acrylic on the (a) Expert-XL and (b) DPX-L. Theresponse to thickness of acrylic may indicate the variation ofBMD with more adipose soft tissue.
TABLE 1. PRECISION OF THE EXPERT IN VIVO FOR AP SPINEAND FEMUR REPORTED AS RMS %CV
Site Obs Pre (%) Post (%) Total (%)
L1–L4 Obs1 0.9 2.3 1.7Obs2 1.4 2.4 1.9Obs3 1.1 2.5 1.9
L2–L4 Obs1 1.2 2.0 1.7Obs2 1.4 2.1 1.8Obs3 1.2 2.4 1.8
Femoral neck Obs1 1.7 2.4 2.0Obs2 1.9 1.2 1.6Obs3 2.2 2.9 2.6
Ward’s triangle Obs1 2.4 1.7 2.1Obs2 2.5 3.4 2.9Obs3 2.2 3.1 2.9
Trochanter Obs1 2.0 3.5 2.8Obs2 2.5 1.7 2.0Obs3 2.5 1.9 2.2
Total Obs1 0.9 1.7 1.4Obs2 0.9 1.6 1.3Obs3 0.9 1.6 1.4
Pre, post, and total denote the premenopausal, postmenopausal,and summed subject groups, respectively.
TABLE 2. BMD PRECISION RESULTS FOR DPX-L
Site Pre (%) Post (%) Total (%)
L1–L4 0.6 1.7 1.3L2–L4 0.7 1.6 1.2Neck 2.2 2.8 2.4Ward’s 2.3 5.5 4.1Troch 3.6 3.5 3.5
Pre, post, and total denote the premenopausal, postmenopausal,and summed subject groups.
TABLE 3. INTEROBSERVER VARIABILITIES REPORTED AS THE
RMS %CV BETWEEN THE THREE OBSERVERS FOREXPERT-XL BMD MEASUREMENTS
Site IO Var (%)
L1–L4 0.7L2–L4 0.6Femoral neck 0.9Total hip 0.2
PERFORMANCE EVALUATION OF THE LUNAR EXPERT-XL 139

ratios measured on the Expert-XL and conventional radio-graphs. Again, the results were independent of vertebrallevel. Finally, the interscan precision for vertebral heightswas 1.9, 4.1, and 4.3% for the lumbar vertebrae, lower-thoracic, and upper-thoracic vertebrae, respectively.
DISCUSSION
Although the use of a fanbeam geometry for BMD andlateral spine measurements was introduced initially on theQDR-2000 (Hologic),(7,12) the design of the Expert-XL,particularly as regards the detector array, X-ray tube, andgantry, is sufficiently novel to merit a thorough review ofimplications of these changes for BMD and lateral mor-phometry measurements. The spatial resolution and noiseproperties of the Expert-XL densitometric images areunique to this system and have significant influence on theprecision of the BMD measurements. Thus, this report wasfocused on outlining key sources of precision error, such asedge detection and interoperator variation. To understandthe implications of replacing older systems with the Expert-XL, it is also important to compare Expert-XL BMD mea-surements with those of current technology. Thus, this workcompared in vivo AP spine and hip measurements betweenthe Expert-XL and the DPX-L, as well as in vitro responseto variations in fat and soft-tissue thickness. In addition toBMD measurements, the detector, X-ray tube, and gantrydesign of the Expert-XL permit supine examinations of thespine in the lateral projection on a 30-s timescale. Thecombination of short scan times and improved ability todelineate the vertebral endplates implies that the Ex-pert-XL has significant potential to perform vertebral frac-ture assessment and morphometry in a clinical setting.Thus, to understand the implications of using this newtechnology, it is important to assess how morphometricmeasurements made by the Expert-XL compare with thosemade from standard radiographs and to assess compara-tively the interoperator precision of the two techniques.Our BMD precision measurements showed that the per-
formance of the Expert-XL for AP hip scanning was com-parable to or better than the DPX-L, but that the spineprecision errors were somewhat larger than the DPX-L. Forthe whole study group, the Expert-XL had a L2–L4 preci-sion of 1.7–1.9% compared with 1.3% for the DPX-L. This
difference may originate from several factors. One majorfactor may be the need for further adjustment of the spineedge-detection algorithm. In evaluation of the spine data,we found that it was necessary to adjust the bone edges foraccuracy in most (approximately two-thirds) of the images.Because of the operator intervention thus required, theBMD precision results varied between observers and
FIG. 5. Correlation of Expert and DPX-L results for (a)L2–L4 and (b) femoral neck BMD.
FIG. 6. Expert-XL image of a 51-year-old postmeno-pausal volunteer. Vertebral levels from L4–T4 may be ad-equately visualized for fracture diagnosis.
TABLE 4. DISTRIBUTION OF HIGHEST ANALYZABLE VERTEBRALLEVELS FROM EXPERT-XL MORPHOMETRIC IMAGES ACQUIRED
OF THE 16 PATIENTS
Obs T4 T5 T6 T7 T8 T9 T10
Obs1 10 2 2 1 1Obs2 10 4 1 1
140 LANG ET AL.

ranged between 0.9 and 1.4% for young volunteers and2–2.5% for older women, with the result probably depend-ing on the degree of care in edge adjustment taken by eachoperator. That edge detection may be a key aspect of thespine precision error is supported by the interoperator pre-cision value of 0.6%. Another source of variability in thespine data may be the composition of the regions employedby the Expert-XL software as a soft-tissue baseline. Theshort (12-s) scan time may imply that these regions aremore sensitive to effects such as bowel gas or breathingartifacts, which may be smoothed over in longer acquisi-tions. Short-term variations in the scanner BMD measure-ments may also contribute, given our short-term in vitroprecision measurements of 0.7% on the Hologic and ESPspine phantoms.In the hip, where precision errors are dominated by
patient positioning and by variable placement of the neck
ROI, rather than by edge detection or variable soft-tissuecomposition, the Expert-XL was comparable to or betterthan the DPX-L. Of particular interest is the total hipmeasurement, which showed a precision better than 1% inyoung volunteers. This high precision value relates to thesize of the ROI and the ease of edge detection in the region.Finally, the long-term precision measurements, whichshowed significant variability in the measurement of BMDover time, represent an additional area of concern. Thelarge overall CV (1.1%) may be partly attributed to the factthat the Expert-XL in our laboratory was the first to beinstalled outside of the factory and was subject to severalrepairs and upgrades during its first year of operation.However, there were few outliers or resolvable short-termoscillations in these measurements, indicating that the cal-ibration system was successfully correcting short-term er-rors, but that the correction mechanism itself was driftingover time.There was a reasonable correspondence between the
Expert-XL and the DPX-L as evidenced by in vitro studiesas well as by comparison of in vivo spine and hip BMDmeasurements. The Expert-XL and DPX-L had similarresponses to variable fat- and soft-tissue thickness, and theresults for both systems point to the limitations in the use ofBMD measurements in obese subjects(13–15) or in subjectswho have experienced a large weight gain between visits ina longitudinal study. For AP spine studies, although themeasurements were highly correlated (r 5 0.98, CV 52.5%), there was a significant slope and intercept (slope 50.86, intercept5 0.14 g/cm), indicating a possible differencein calibration between the two machines. The hip resultsshowed more scatter (r 5 0.92, CV 5 5.2%) but a nonsig-nificant slope and intercept. The large CV may have beendue to the effect of variable positioning of the neck boxbetween the two systems. It should be noted that the com-parisons employed mean values of the paired scans ratherthan single measurements, thus increasing the correlationcoefficients by reducing the effect of precision errors. Thecorrelation results thus obtained are consistent with thegenerally accepted practice of not changing densitometersduring longitudinal evaluations of single patients or ofgroups of patients in clinical trials.The potential utility of the Expert-XL for lateral spine
imaging is based on the ability to use the same instrumentboth to perform standard densitometric examinations andto diagnose vertebral fractures at a lower radiation dosethan conventional spinal radiographs. Two questions mustbe comparatively assessed. The first issue is the ability of
TABLE 5. INTEROBSERVER VARIABILITY REPORTED AS RMS%CV BETWEEN TWO OBSERVERS FOR EXPERT VERTEBRAL
DIMENSION MEASUREMENTS
Site Post (%) Mid (%) Anterior (%)
L4–L1 5.3 4.0 5.1T12–T9 3.3 2.7 3.5T8–T5 4.9 4.1 4.2
TABLE 6. INTEROBSERVER VARIABILITY REPORTED AS RMS%CV BETWEEN TWO OBSERVERS FOR RADIOGRAPHIC
VERTEBRAL DIMENSION MEASUREMENTS
Site Post Mid Anterior
L4–L1 2.6 1.6 1.4T12–T9 1.9 1.4 1.6T8–T5 2.0 1.7 1.5
FIG. 7. Comparison of anterior heights measured withExpert and with standard radiographs. The slope of 1.25 isdue to the magnification inherent in the conebeam geom-etry of the radiographs.
TABLE 7. INTERMODALITY DEVIATIONS IN VERTEBRAL HEIGHTRATIOS REPORTED AS THE % RMS DIFFERENCE BETWEEN THE
CONVENTIONAL RADIOGRAPHIC AND EXPERT-XL LATERALMORPHOMETRY
Site Antero-posterior Mid-posterior Mid-anterior
L4–L1 3.2 3.0 3.2T12–T9 2.3 3.0 3.4T8–T5 3.0 2.2 2.7
PERFORMANCE EVALUATION OF THE LUNAR EXPERT-XL 141

the two techniques to diagnose qualitatively vertebral frac-tures. In our study, both observers could clearly visualizevertebral levels from L4–T4 from the spinal radiographs inall of the patients. In the Expert-XL images, it was possibleto visualize this range of levels in 10 of 16 patients and fromL4–T6 in 15 of 16 patients. The utility of the Expert-XL forqualitative diagnosis of vertebral fracture was also ad-dressed by Hans,(16) who found reasonable agreement, asevidenced by a k-score of 0.86, between consensus readingsof radiographs and qualitative assessment of fractures fromExpert-XL images in a group of 21 osteoporotic patients.The second issue that was addressed in this study is com-parison between quantitative vertebral measurements withthe two techniques. Our study, which assessed the inter-technique differences between quantitative morphometricmeasurements in a set of relatively healthy volunteers,showed that the differences between techniques, expressedas the RMSD of vertebral height ratios and the SEE ofregressions comparing vertebral height measurements, wereon the order of 2–5%. We found that interobserver andinterscan precision for the Expert-XL had a similar magni-tude, but also that the interobserver errors for conventionalradiographic morphometry were somewhat lower, rangingfrom 1–3%. It should be noted that the intertechnique andinterobserver variations for the Expert-XL are generallyconsistent with precision values reported in the literaturefor radiographic morphometry(17) and are small comparedwith the 20% reduction in height and/or height ratios, whichis often used as criteria for defining moderate vertebralfractures.However, it should be noted that the Expert-XL interop-
erator and precision errors documented here are probablylower than would be the case in routine clinical usage. Thisstudy was conducted in a group of healthy postmenopausalwomen, whereas in an osteoporotic population, low BMDwould result in both higher precision errors and weakercorrelations with conventional radiography due to reducedability to visualize the vertebral endplates. Another factorthat tended to reduce precision errors and increase thecorrelation with conventional morphometry was that verte-bral levels not identifiable by both observers on the Ex-pert-XL images were excluded from this analysis.In conclusion, the Expert-XL has advantages and limita-
tions as a clinical imaging system. The advantages are theshort examination times, which promote patient comfortand economy of usage, and the high image resolution,which permits detailed examination of the lateral spine. Thedensitometric precision errors are small compared with thepopulation variations in BMD, meaning that the system canbe effectively used for fracture risk screening. However, inlongitudinal BMD examinations of the lumbar spine, it isimportant to monitor carefully the bone edges to ensureacceptable precision. Thus, lumbar spine BMD measure-ments are an aspect of the system that will require furtherrefinement by the manufacturer.The use of the Expert-XL for lateral morphometry rep-
resents an interesting new dimension for densitometry inthat it offers the possibility to diagnose vertebral fracture ata substantially reduced radiation dose (40 mSv(18) vs. 700mSv(19)) compared with lateral lumbar radiographs. Our
preliminary measurements in a group of postmenopausalwomen indicate that it may be possible to employ theExpert-XL to screen for vertebral fracture in levels from L4to T4 in most of the population. However, in a significantnumber of cases, an additional radiographic measurementwould be required to establish the fracture status in theupper thoracic levels not visualized in the Expert-XL scan.Even so, use of the system would result in a substantialreduction of radiation dose for those cases in which theL4–T4 endplates were successfully visualized and a smallincremental dose for those cases where an additional radio-graph was necessary. While the Expert-XL system thus hasobvious promise for qualitative assessment of vertebralfracture, further research is required to establish the utilityof the system for more quantitative measurements. Due toreduced spatial resolution and higher image noise, the in-terobserver and interscan variabilities are higher for theExpert-XL than for radiography, and it is important tounderstand the impact of these errors both on the detailedclassification of vertebral fracture severity as well as onserial measurements of vertebral deformity. Advances inthese capabilities may result from improvements in imageprocessing and in scanning protocols, particularly as theyapply to the thoracic component of the Expert-XL scan.
ACKNOWLEDGMENTS
This research was partially supported by the Lunar Cor-poration. The authors thank Dr. Thomas Fuerst, Dr. ClausGluer, and Dr. Ying Lu for technical input. The authors aregrateful to Dr. James Hanson, Mr. Joseph Bisek, and Mr.Chris Fowler for technical support.
REFERENCES
1. Pocock NA, Sambrook PN, Nguyen T, Kelly P, Freund J,Eisman JA 1992 Assessment of spinal and femoral done den-sity by dual x-ray absorptiometry: Comparison of Lunar andHologic instruments. J Bone Miner Res 7:1081–1084.
2. Duboeuf F, Pommet R, Meunier PJ, Delmas PD 1994 Dual-energy x-ray absorptiometry of the spine in anteroposteriorand lateral projections. Osteoporosis Int 4:110–116.
3. Cleek T, Wahlen R 1993 Bone geometry, structure, and min-eral distribution using DXA. Calcif Tissue Int 52:154.
4. Genant HK, Engelke K, Gluer CC, Lang TF, Majumdar S 1995Recent advances in the non-invasive assessment of bone den-sity, quality and structure. J Jpn Soc Bone Morphom 5:93–108.
5. JergasM, Genant HK 1993 Current methods and recent advancesin the diagnosis of osteoporosis. Arthrit Rheumat 36:1649–1662.
6. Mazess R 1995 Dual-energy x-ray absorptiometry for the man-agement of bone disease. Phys Med Rehab Clin North Am6:507–537.
7. Steiger P, von Stetten E, Weiss H, Stein JA 1991 Paired APand lateral supine dual x-ray absorptiometry of the spine:Initial results with a 32 detector system. Osteoporosis Int 1:190.
8. Mazess R, Chesnut CH III, McClung M, Genant HK 1992Enhanced precision with dual-energy x-ray absorptiometry.Calcif Tissue Int 51:14–17.
9. Gluer CC, Blake G, Blunt BA, Jergas M, Genant HK 1995Accurate assessment of precision errors: How to measure the
142 LANG ET AL.

reproducibility of bone densitometry techniques. OsteoporosisInt 5:262–270.
10. Lu Y, Mathur A, Blunt B, Gluer C, Will A, Fuerst T, Jergas M,Andriano K, et al. 1996 Dual-energy X-ray absorptiometryquality control: Comparison of visual examination and processcontrol charts. J Bone Miner Res 11:626–637.
11. Gluer CC, Steiger P, Selvidge R, Elliesen-Kliefoth K, Hayashi C,Genant HK 1990 Comparative assessment of dual-photon-absorpti-ometry and dual-energy-radiography. Radiology 174:223–228.
12. Steiger P, Cummings S, Genant H, Weiss H 1994 Morphomet-ric X-ray absorptiometry of the spine: Correlation in vivo withmorphometric radiography. Osteoporosis Int 4:238–244.
13. Wahner HW, Dunn WL, Brown ML, Morin RL, Riggs BL1988 Comparison of dual-energy x-ray absorptiometry and dualphoton absorptiometry for bone mineral measurements of thelumbar spine. Mayo Clin Proc 63:1075–1084.
14. Tothill P, Pye DW 1991 Errors in DXA of spine due tonon-uniform fat distribution. Osteoporosis Int 1:199.
15. Johnson J, Dawson-Hughes B 1991 Precision and stability ofdual energy X-ray absortiometry measurements. Calcif TissueInt 49:174–178.
16. Hans D, Baiada A, Dubouef F, Vignot E, Bochu M, MeunierP 1995 Expert-XL: Clinical evaluation of a new morphometric
technique on 21 patients with verteral fracture. 11th Interna-tional Bone Densitometry Workshop, Gleneden Beach, OR,U.S.A.
17. Wu C, Li J, Jergas M, Genant H 1995 Comparison of quanti-tative and semi-quantitative techniques for the assessment ofvertebral fractures. Osteoporosis International 5:354–370.
18. Lunar 1996 Expert-XL Users Manual for software versionv1.52. Lunar Corp., Madison, WI, U.S.A.
19. Kalender WA 1992 Effective dose values in bone mineralmeasurements by photon absorptiometry and computed to-mography. Osteoporosis Int 2:82–87.
Address reprint requests to:Thomas F. Lang, Ph.D.
Osteoporosis Research GroupDepartment of Radiology
University of California–San Francisco533 Parnassus Avenue, Box 1250
San Francisco, CA 94143-1250 U.S.A.
Received in original form July 26, 1996; accepted August 29, 1996.
PERFORMANCE EVALUATION OF THE LUNAR EXPERT-XL 143