Combat Stress Kieran Dhillon, PsyD, ABPP Military Psychology.
Upload
marjorie-simonCategory
view
215download
0
A Population Health Approach to Managing Obesity Using a Primary Care Behavioral
Health Clinical Pathway
Anne C. Dobmeyer, PhD, ABPP, Chief Psychologist, PCBH Directorate, Deployment Health Clinical Center
Jennifer L. Bell, MD, Associate Director, PCBH Directorate, Deployment Health Clinical Center
Christopher L. Hunter, PhD, ABPP, DoD Program Manager for Behavioral Health in Primary Care
Collaborative Family Healthcare Association 17th Annual ConferenceOctober 15-17, 2015 Portland, Oregon U.S.A.
Session # G1aOctober 16, 2015

Faculty Disclosure
The presenters of this session have NOT had any relevant financial relationships during the past 12 months.

Learning Objectives
At the conclusion of this session, the participant will be able to:
• Identify two key conclusions of outcome literature on treatment of obesity in primary care settings.
• Discuss the rationale for implementing a primary care-based, population health approach to obesity using the primary care behavioral health (PCBH) model of service delivery.
• Describe three key elements in a PCBH clinical pathway for obesity.

Bibliography / References
1. Dobmeyer, A. C., Goodie, J. L., & Hunter, C. L. (2014). Health care provider and systems interventions promoting health behavior change. In K. A. Riekert, J. K. Ockene, & L. Pbert (Eds.), The Handbook of Health Behavior Change (4th ed.). New York: Springer (pp. 417-436).
2. Thompson, C. A., & Foster, G. D. (2014). Dietary behaviors: Promoting healthy eating. In K. A. Riekert, J. K. Ockene, & L. Pbert (Eds.), The Handbook of Health Behavior Change (4th ed.). New York: Springer (pp. 139-154).
3. Moyer, V. A., on behalf of the U.S. Preventive Services Task Force (2012). Screening for and management of obesity in adults: U.S. Preventive Services Task Force recommendation statement. Annals of Internal Medicine, 157 (5), 1-7.
4. Wadden, T. A., Butryn, M. L., Hong, P. S., & Tsai, A. G. (2014). Behavioral treatment of obesity in patients encountered in primary care settings: A systematic review. JAMA, 312 (14), 1779-1791.
5. Alexander, S. C., Cox, M.E., Boling Turer, C. L., Lyna, P., Østbye, T., Tulsky, J. A., Dolor, R. J., & Pollak, K. I.(2011). Do the five A’s work when physicians counsel about weight loss? Family Medicine, 43 (3), 179-184.

Learning Assessment
• A learning assessment is required for CE credit.
• A question and answer period will be conducted at the end of this presentation.

Disclaimer
The views expressed are those of the authors and do not reflect the official policy of the Department of Defense (DoD), the United States Public Health Service (USPHS) or the U.S. Government.

Acknowledgements
The authors would like to acknowledge the following individuals who were instrumental in the development of the DoD PCBH Obesity Clinical Pathway:
Kent Corso, PsyDMeghan Corso, PsyDJay Earles, PsyDMatthew Nielsen, PhDNicholas Polizzi, PhDKathryn Waggoner, PhD

Overview
• Obesity treatment in primary care‒ Health behavior change and obesity treatment in primary care‒ Role of Behavioral Health Consultants (BHCs)
• Primary Care Behavioral Health (PCBH) obesity pathway‒ Key processes‒ Supports needed‒ Specific pathway content
• Future directions‒ Program evaluation‒ Pathway expansion and modification

What Do We Know about Improving Health Behaviors in Primary Care?
Intervention elements associated with improved health behavior outcomes1
• Assessment of patient characteristics and needs and subsequent tailoring of intervention elements to address assessment
• Behavioral interventions (especially those that include self-monitoring, collaborative goal setting and active problem solving)
• Combined behavioral and pharmacologic interventions• Supportive elements (both within and outside of intervention)• Use of multiple modalities• Multiple contacts• Inclusion of organizational or system elements to prompt patients and
clinicians
1. Goldstein, Michael G., Evelyn P. Whitlock, Judith DePue, and Planning Committee of the Addressing Multiple Behavioral Risk Factors in Primary Care Project. "Multiple behavioral risk factor interventions in primary care: summary of research evidence." American Journal of Preventive Medicine 27, no. 2 (2004): 61-79.

What Do We Know about Primary Care Providers (PCPs) and Obesity Treatment?
• PCPs are reluctant to address weight management, especially among those who are not extremely overweight
‒ Less than half of obese individuals are advised by their physicians to lose weight1
• Weight counseling declined from 1995–1996 to 2007–20082
‒ Rates of diet, exercise, and weight-related counseling similarly declined.
• PCP attitudes about obesity and its treatment3
‒ View obesity as largely a behavioral problem‒ Share negative stereotypes about the personal attributes of obese
people‒ View obesity treatment as less effective than treatment of most other
chronic conditions1. Galuska, Deborah A., Julie C. Will, Mary K. Serdula, and Earl S. Ford. "Are health care professionals advising obese patients to lose weight?." JAMA 282, no. 16 (1999): 1576-1578.2. Kraschnewski, Jennifer L., Christopher N. Sciamanna, Heather L. Stuckey, Cynthia H. Chuang, Erik B. Lehman, Kevin O. Hwang, Lisa L. Sherwood, and Harriet B. Nembhard. "A silent response to the obesity epidemic: decline in US physician weight counseling." Medical Care 51, no. 2 (2013): 186-192.3. Foster, Gary D., Thomas A. Wadden, Angela P. Makris, Duncan Davidson, Rebecca Swain Sanderson, David B. Allison, and Amy Kessler. "Primary care physicians’ attitudes about obesity and its treatment." Obesity Research 11, no. 10 (2003): 1168-1177.

Physicians and the “5 As”
• Ask: Physician asks about weight, nutrition, and/or exercise.
• Advise: Physician provides the patient with clear, strong advice.‒ “You need to get 30 minutes of exercise a day, 5 days a week.”‒ “Because of your diabetes, it is important for you to exercise.”
• Assess: Physician verbally assesses patient’s readiness to change.‒ “Is losing weight something you want to do in the near future?”‒ “Do you see yourself getting more exercise in the coming months?”
• Assist: Physician provides brief counseling or self-help materials.‒ “What might get in the way of your plan to exercise three times a week?”‒ “How are you feeling about being able to make this change?”‒ “Is your family supportive of your attempts to eat better?”
• Arrange: Physician arranges for follow-up with physician or nutritionist.‒ “Why don’t you call me in 2 weeks to let me know how the weight loss plan is going?”‒ “I will schedule an appointment for you to see our nutritionist.”
Alexander, Stewart C., Mary E. Cox, Christy L. Boling Turer, Pauline Lyna, Truls Østbye, James A. Tulsky, Rowena J. Dolor, and Kathryn I. Pollak. "Do the five A’s work when physicians counsel about weight loss?” Family Medicine 43, no. 3 (2011): 179 – 184.
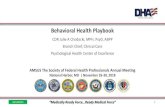
77%
63%
13%
5%
4%

“Do the Five A’s Work When Physicians Counsel About Weight Loss?”
Ask and Advise are more common, but they do not help physicians learn what patients are actually willing to do, so don’t help the physicians help patients formulate an action plan for change. The results…
Associations Between Five A’s and Dietary Fat and Fiber Intake• Advised: Increased motivation to change dietary fat and fiber intake. • Advised: Increased confidence to improve diet.• Assisted and Arranged: Patients were more likely to report improving their diet.
Association Between Five A’s and Weight Loss• Advised: Patients had significantly higher improvements in confidence to lose weight. • Assessed: Patients were more likely to improve their confidence.• Arranged: Patients had a significant difference in measured weight loss.
Alexander, Stewart C., Mary E. Cox, Christy L. Boling Turer, Pauline Lyna, Truls Østbye, James A. Tulsky, Rowena J. Dolor, and Kathryn I. Pollak. "Do the five A’s work when physicians counsel about weight loss?." Family medicine 43, no. 3 (2011): 179-184.

Date of download: 2/21/2015
From: Screening for and Management of Obesity in Adults: U.S. Preventive Services Task Force Recommendation Statement
Ann Intern Med. 2012;157(5):373-378. doi:10.7326/0003-4819-157-5-201209040-00475
Screening for and management of obesity in adults: clinical summary of U.S. Preventive Services Task Force recommendation.
Figure Legend:
Copyright © American College of Physicians. All rights reserved.

"Effectiveness of primary care–relevant treatments for obesity in adults: a systematic evidence review for the USPSTF”
• Behaviorally based treatments are safe and effective for weight loss and maintenance‒ Behavioral treatment trials providing 12 to 26 intervention sessions
during the first year lost 4- 7 kg (average, 6% of baseline weight) at 12 to 18 months, compared with little to no weight loss in control groups.
‒ Adding Orlistat to intensive behaviorally based intervention resulted in a 5-10 kg loss (avg, 8% of baseline weight), compared with 3- 6 kg in the placebo groups.
‒ Most trials showed that behavioral interventions had a statistically significant effect on weight loss at 12 to 18 months
LeBlanc, Erin S., Elizabeth O'Connor, Evelyn P. Whitlock, Carrie D. Patnode, and Tanya Kapka. "Effectiveness of primary care–relevant treatments for obesity in adults: a systematic evidence review for the US Preventive Services Task Force." Annals of Internal Medicine 155, no. 7 (2011): 434-447.

Do We Really Need All Those Appointments?
• More appointments associated with greater weight loss‒ Behavioral interventions lasting longer (24 to 54 months) continued to
show greater weight loss (2 to 4 kg) compared with controls ‒ Weight loss could be maintained for an additional year or more after
completion of an active weight-loss phase, particularly with additional support
• Higher intensity interventions associated with greater loss ‒ Most higher-intensity interventions included self-monitoring, setting
goals, addressing barriers to change, and strategizing about maintaining long-term changes.
‒ No component was associated with degree of weight loss in meta-regression. Specific articulation of essential elements of effective interventions was not possible.
LeBlanc, Erin S., Elizabeth O'Connor, Evelyn P. Whitlock, Carrie D. Patnode, and Tanya Kapka. "Effectiveness of primary care–relevant treatments for obesity in adults: a systematic evidence review for the US Preventive Services Task Force." Annals of Internal Medicine 155, no. 7 (2011): 434-447.

How Might BHCs Help in Obesity Treatment?
• Train PCPs on 5As for obesity‒ Formal teaching‒ Consultative feedback over time
• Provide intervention for obese patients‒ Ensure patients receive all of the 5As (especially Assist and Arrange)‒ Provide “higher intensity interventions”
‒ Evidence-based, brief behavioral interventions‒ Self-monitoring, goal setting, behavior change
‒ Increase overall number of appointments patients receive‒ Patients may receive appointments with PCP, BHC, nurse, dietician…‒ Provide care over time/relapse prevention
• Improve care coordination‒ Ensure patients and PC team have shared treatment goals and plan
• Advocate for organizational/system elements to prompt clinicians

PCBH Obesity Clinical Pathway

Overview of Key Processes in Pathway
• Identify‒ Methods to identify patients‒ Criteria for pathway inclusion
• Connect‒ Ways to link patients to BHC
• Intervene‒ Evidence-based assessment and
intervention from BHC
• Measure Outcomes‒ Type of outcome data to collect
Identify
Connect
Intervene
Measure
Outcomes

Supports Needed
• Interdisciplinary team support‒ Clinic leaders‒ Behavioral Health Consultant (BHC)‒ Primary Care Providers (PCP)‒ Nurses‒ Administrative personnel
• Pathway materials‒ Outline for primary care staff‒ Assessment and intervention materials for BHC‒ Patient handouts
• System supports‒ Registries (or ability to pull patient lists)‒ Secure messaging between patients and providers (desired, but not required)‒ Clinical reminders/prompts in electronic health record (EHR)‒ “Mineable” data entry fields in EHR

Identify
• Criteria for inclusion‒ BMI > 30‒ Patients with a diagnosis of obesity
• Processes for identification‒ Morning huddle review of PCP’s patient roster for the day‒ Weight screening at PCP appointment (by nurse/technician)‒ PCP identification during appointment‒ Data pull from Electronic Health Record (EHR) – BMI or obesity diagnosis‒ Self-referral‒ Referral from other providers/clinics

Connect
• When identified during PCP appointment:‒ Same-day appointment (warm hand-off) with BHC‒ Scheduled future appointment with BHC
• When identified through data pull:‒ Primary care staff (nurse, technician) calls patient to schedule a future
BHC appointment. Uses standard pathway telephone script‒ Primary care staff sends secure message to patient (using standard
pathway language) encouraging a BHC appointment• If patients declines BHC appointment:
‒ PCP may ask BHC to review available medical information and provide recommendations for care based on the available data

Connect: Standard Telephone Script
“Hello. I am Mr./Ms. _______________, a nurse/technician at ________ Clinic. Your PCP, Dr. __________, wanted me to give you a call about some of the details she noticed in your record related to your weight. As part of good comprehensive care for you, she would like you to schedule an appointment with our clinic’s Behavioral Health Consultant, who assists Dr. ___________ by providing recommendations and strategies for better weight management. The appointments are 30 minutes long and are right here in our clinic. Can I get you scheduled for an appointment within the next week or two?
If the patient has questions about how a BHC appointment might be helpful for weight management, please provide one or two examples of interventions that the BHC might recommend. “The IBHC might work with you on:
Making eating behavior changes that fit with your lifestyle that can make it easier lose weight and keep it off
Setting a physical activity plan that fits with your preferences that can make it easier lose weight and keep it off
Setting a plan to help manage stress. For many people being able to effectively manage stress makes it easier to lose weight and keep it off”

Intervene: Initial BHC Appointment
• Biopsychosocial assessment questions specific to obesity‒ Describe your typical eating habits.‒ Describe your typical exercise habits.‒ How long have you been overweight?‒ How long have you been trying to address your weight?‒ Factors related to onset (or worsening) of weight problem.‒ Course of weight gain and weight loss efforts.‒ Which prior weight loss efforts have been most/least successful?‒ How is weight impacting: work performance, relationships, social and/or
recreational activities, physical activities, health?
• Assessment measures‒ Weight/Height, BMI‒ Behavioral Health Measure-20 (BHM-20), a broad-spectrum measure of
health and behavioral health

Intervene: Initial BHC Appointment (cont’d)
• Intervention options: BHC and patient collaboratively select the evidence-based intervention(s) most appropriate for the patient’s difficulties and readiness for change
‒ Education on healthy weight loss with a focus on healthy eating and physical exercise
‒ Motivational interviewing to determine importance and readiness for change
‒ Identifying and problem-solving barriers to change‒ Goal setting for improved health behaviors (e.g., changes to eating,
increases to physical activity)‒ Instruction in use of a food and activity diary‒ Education and goal setting for behavior modification strategies for weight
management‒ Linking to other PCMH team members or external resources (e.g.,
dietician, etc.)




Intervene: Follow-Up Appointments
• Follow-up intervals‒ Tailored to patient, based on:
‒ Readiness to change‒ Likelihood of successfully making changes with self-management‒ Nature of intervention selected
‒ Often, follow-up interval is between 2 to 4 weeks
• Number of appointments‒ Some patients may improve aspects of weight management in 1 to 4
appointments‒ Many patients will need continuity consultation (> 4 appointments,
spaced at longer intervals) to maintain behavior changes ‒ Consider monthly or every other month appointments‒ Consider alternating appointments with BHC, PCP, dietician

Intervene: Follow-Up Appointments (cont’d)
• Assessment‒ BMI and BHM-20‒ Interview
‒ Adherence to behavior change plan‒ Identify barriers to success‒ Change in symptoms (weight) and functioning
• Intervention options‒ Motivational interviewing‒ Problem solving around identified barriers‒ Goal setting‒ Food/activity diary‒ Calorie reduction plan‒ Replacing high calorie meals or snacks‒ Changing how one eats (e.g., stimulus control, behavior modification)‒ Avoiding or managing high risk situations

Measure Outcomes
Process outcome examples
• Does pathway implementation lead to improved rates of collaborative care?
‒ Compare: % of enrolled population with BMI > 30 who have seen BHC in 6 months prior to pathway, with % who have had > 1 appointment with BHC for obesity during first 6 months of implementation
‒ Do pathway patients (those seeing BHC for obesity) accept a referral to nutritional medicine (and keep their scheduled appointments) more frequently than those not seeing BHC?
• Do patients enrolled in the pathway receive appropriate care from BHC?
‒ Minimum of 3 appointments with BHC for obesity‒ Content of intervention appropriate (record review of select charts). Use
of at least 2 specified evidence-based interventions must be documented

Measure Outcomes
Clinical outcome examples
• Do patients enrolled in the pathway demonstrate improved clinical outcomes?
‒ Change in BMI‒ Percent of total weight lost
• Do patients enrolled in the pathway show improved health indicators?
‒ Decreased blood pressure‒ Decreased cholesterol‒ Decreased A1C (if diabetic)
• Do patients who show a significant decrease in weight maintain that weight over time? (6 month and 12 month follow-up)
‒ 6 month follow-up on above‒ 12 month follow-up on above

Future Directions
• Conduct program evaluation‒ Consider evaluating standard clinical pathway package +
minimal training, versus enhanced implementation support
• Modify pathway to also target overweight population
• Tailor pathway for comorbid obesity and diabetes
• Incorporate shared medical appointments into pathway intervention options

Q & A/Summary
• What are two key conclusions of outcome literature on treatment of obesity in primary care settings?
• What is a rationale for implementing a primary care-based, population health approach to obesity using the PCBH model of service delivery?
• What are some key elements in a PCBH clinical pathway for obesity?

Session Evaluation
Please complete and return theevaluation form to the classroom monitor before
leaving this session.
Thank you!