
A PHASE 1B STUDY OF RXDX-105, A VEGFR-SPARING · PDF file1Alexander Drilon, 2Stephen V. Liu,...
14
esmo.org A PHASE 1B STUDY OF RXDX-105, A VEGFR-SPARING POTENT RET INHIBITOR, IN RET INHIBITOR NAÏVE PATIENTS WITH RET FUSION-POSITIVE NSCLC 1 Alexander Drilon, 2 Stephen V. Liu, 3 Robert Doebele, 4 Cristina Rodriguez, 5 Marwan Fakih, 5 Karen Reckamp, 6 Lyudmila Bazhenova , 7 Byoung Chul Cho, 8 Eric Kowack, 8 Denise Trone, 8 Rupal Patel, 8 Jennifer W. Oliver, 8 Pratik S. Multani, 9 Myung-Ju Ahn 1 Memorial Sloan Kettering Cancer Center, New York, NY; 2 Georgetown Lombardi Comprehensive Cancer Center, Washington, D.C.; 3 Anschutz Medical Campus, University of Colorado, Aurora, CO; 4 Seattle Cancer Care Alliance, Seattle WA; 5 City of Hope Comprehensive Cancer Center, Duarte, CA; 6 University of California San Diego, Moores Cancer Center, San Diego, CA; 7 Severance Hospital, Yonsei University Health System, Seoul, Korea; 8 Ignyta, Inc., San Diego, CA; 9 Samsung Medical Center, Seoul, Korea 10 September 2017
Transcript of A PHASE 1B STUDY OF RXDX-105, A VEGFR-SPARING · PDF file1Alexander Drilon, 2Stephen V. Liu,...

esmo.org
A PHASE 1B STUDY OF RXDX-105, A VEGFR-SPARING POTENT RET INHIBITOR, IN RET INHIBITOR NAÏVE
PATIENTS WITH RET FUSION-POSITIVE NSCLC
1Alexander Drilon, 2Stephen V. Liu, 3Robert Doebele, 4Cristina Rodriguez, 5Marwan Fakih, 5Karen Reckamp, 6Lyudmila Bazhenova, 7Byoung Chul Cho, 8Eric Kowack,
8Denise Trone, 8Rupal Patel, 8Jennifer W. Oliver, 8Pratik S. Multani, 9Myung-Ju Ahn
1Memorial Sloan Kettering Cancer Center, New York, NY; 2Georgetown Lombardi Comprehensive Cancer Center, Washington, D.C.; 3Anschutz Medical Campus, University of Colorado, Aurora, CO; 4Seattle Cancer Care Alliance, Seattle WA; 5City of Hope Comprehensive Cancer Center, Duarte, CA; 6University of California San Diego, Moores Cancer Center, San Diego, CA; 7Severance Hospital, Yonsei University Health System, Seoul, Korea; 8 Ignyta, Inc.,
San Diego, CA; 9Samsung Medical Center, Seoul, Korea
10 September 2017

2
• Advisory board: Takeda, Astra Zeneca, Eli Lilly, Novartis • Research support: BeyondSpring Pharmaceuticals
Disclosures

• Genomic alterations in RET, encoding the tyrosine kinase receptor RET (rearranged during transfection), lead to oncogenic signaling
• RET gene fusions are found predominantly in NSCLC and PTC, whereas activating mutations in the RET gene occur in MTC
• Activating RET gene fusions have been reported in 1-2% of lung adenocarcinomas; e.g., KIF5B-RET, CCDC6-RET, NCOA4-RET, EML4-RET
• More than half of the RET fusions in NSCLC involve the KIF5B gene as the fusion partner
3
Activating RET Alterations Are Oncogenic Drivers
1. AACR Project GENIE: Powering Precision Medicine Through An International Consortium. Cancer Discovery 2. Zehir, A., et al. Nature Medicine, 23(6), 703–713

• High potency against RET fusions and activating mutations • VEGFR-sparing, with ~500x higher potency against RET than
VEGFR in vitro • Strong anti-tumor activity in vivo, with tumor regression at clinically
achievable exposures in several PDX models harboring known activating RET fusions
4
RXDX-105 Is a VEGFR-Sparing, Potent RET Inhibitor
Target Kinase IC50 (nM)
RET 0.33
CCDC6-RET 0.33
NCOA4-RET 0.41
PRKAR1A-RET 0.81
RET (M918T) 4.34
FLT1/VEGFR1 141
KDR/VEGFR2 258
Gang G. Li et al. (2017), Clinical Cancer Research, Jun 15;23 (12):2981-2990

• Based on analysis of safety, efficacy and pharmacokinetics across multiple doses, 275 mg fed, administered orally once daily was selected as the RP2D
• Clinical exposures of RXDX-105 at the RP2D achieve target thresholds to inhibit RET, while remaining well below estimated threshold for VEGFR2 inhibition
5
275 mg (Fed) Orally Once Daily Regimen Maintains Exposures Above Projected Ceff

6
Patient Baseline Characteristics and Disposition
Patient Characteristics and Disposition, n (%) Phase 1 (N=55)
Phase 1b RET+ (N=47)
Phase 1b Other (N=50)
Total Subjects (N=152)
Dosing RP2D (275 mg Fed) Other
12 (22) 43 (78)
33 (70) 14 (30)
29 (58) 21 (42)
74 (49) 78 (51)
Ongoing Discontinued Treatment Disease Progression Adverse Event Death Withdrawal by Subject Other (e.g., Investigator decision, lost to follow-up)
2 53 40 7 3 3 0
27 20 15 1 0 2 2
4 46 21 11 1 6 7
33 119 76 19 4 11 9
Age, years, median (range) 61 (27, 81) 61 (33, 79) 69 (36, 90) 63 (27, 90) Sex, male/female % 45/55 50/50 50/50 48/52
Number of prior anti-cancer therapies, median (range) 3 (1, 17) 2 (0, 10) 3 (0, 7) 3 (0, 17)

• The majority of the treatment-related AEs continue to be ≤ Grade 2 and are reversible with dose modifications
• Thirteen patients (9%) experienced 19 treatment-related SAEs; all except 1 resolved by dose modification or discontinuation
• Toxicities commonly associated with VEGFR inhibition, such as hypertension, hypothyroidism, proteinuria, and neurotoxicity, were rarely observed
• RXDX-105 is not associated with QT/QTc prolongation
7
RXDX-105 Treatment-Related Adverse Events
* Rash, Rash erythematous, Rash generalized, Rash macular, Rash maculo-papular, Rash papular, Rash pruritic, Urticaria, Drug rash with eosinophilia and systemic symptoms, Drug hypersensitivity, Adverse drug reaction
The most common (>10%) treatment-related AEs as of August 1, 2017
Adverse Event Term RP2D (275 mg Fed) (n=74)
350 mg Fed (n=43)
All Doses (n=152)
≤G2 ≥G3 ≤G2 ≥G3 ≤G2 ≥G3
Rash* 16 (22) 9 (12) 11 (26) 6 (14) 37 (24) 15 (10)
Diarrhea 12 (16) 3 (4) 9 (21) 2 (5) 28 (18) 6 (4)
Fatigue 12 (16) 0 (0) 11 (26) 3 (7) 27 (18) 5 (3)
Hypophosphatemia 6 (8) 4 (5) 6 (14) 6 (14) 13 (9) 11 (7)
Elevated Alanine Aminotransferase 2 (3) 5 (7) 2 (5) 6 (14) 4 (3) 11 (7)
Elevated Aspartate Aminotransferase 5 (7) 3 (4) 4 (9) 3 (7) 9 (6) 6 (4)
Nausea 6 (8) 0 (0) 11 (26) 0 (0) 21 (14) 0 (0)
Muscle Spasms 5 (7) 0 (0) 10 (23) 0 (0) 19 (13) 0 (0)
Decreased Appetite 8 (11) 0 (0) 7 (16) 0 (0) 17 (11) 0 (0)
Vomiting 5 (7) 0 (0) 6 (14) 0 (0) 15 (10) 0 (0)
Blood Bilirubin Increased 1 (1) 1 (1) 5 (12) 0 (0) 6 (4) 1 (1)

8
Enrollment in Phase 1b RET Basket
RET Alterations
RET Fusion-Positive NSCLC
Fusion Partner RETi naïve Prior RETi KIF5B 20 7 Non-KIF5B-RET CCDC6 EML4 PARD3 NCOA4 CLIP1
9 6 2 1 -- --
2 -- -- -- 1 1
FISH+ (fusion partner unknown)
2 --
Total 31 9
Other RET Positive Histologies
Tumor type RETi naïve Prior RETi
mCRC 1 --
MTC 1 4
Sarcoma -- 1
Total 2 5

9
Anti-Tumor Activity of RXDX-105 in RETi-Naïve, RET Fusion-Positive NSCLC
Legend: * 0% Change, PD in Non-target lesions + NE due to AE # 200% change
Non-KIF5B KIF5B
• Non-KIF5B-RET fusion-positive NSCLC (n=8)
• 75% of these patients had a partial response
• KIF5B-RET fusion-positive NSCLC (n=14)
• 3 SD lasting 6+ months
• Additionally, a RETi naïve mCRC patient harboring CCDC6-RET fusion, achieved a CR and continues on study in C15
Note: Patients shown had measurable disease; fusions identified by NGS assay; at least one post treatment scan or discontinued due to an AE; and Investigator assessed by RECIST 1.1

Time of first response Discontinued due to AE or Progression RECIST Progression, continued on treatment On Treatment
10
Duration Of Treatment with RXDX-105
X
Non-KIF5B KIF5B
Median Duration of Response (DOR) has not been reached, with longest DOR at 10.2 months
11
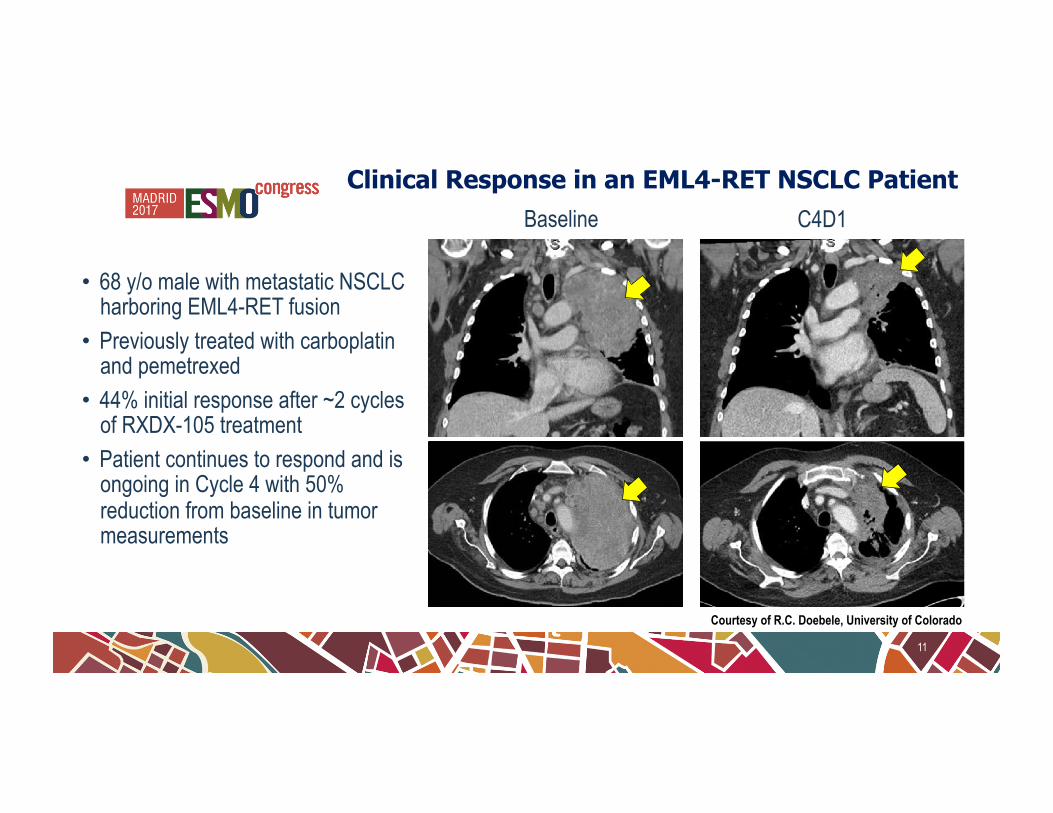
Courtesy of R.C. Doebele, University of Colorado
C4D1 Baseline Clinical Response in an EML4-RET NSCLC Patient
• 68 y/o male with metastatic NSCLC harboring EML4-RET fusion
• Previously treated with carboplatin and pemetrexed
• 44% initial response after ~2 cycles of RXDX-105 treatment
• Patient continues to respond and is ongoing in Cycle 4 with 50% reduction from baseline in tumor measurements

12
• 61 y/o female with metastatic NSCLC harboring CCDC6-RET fusion
• Previously treated with surgery and radiotherapy
• 40% initial response observed after ~2 cycles of RXDX-105 treatment, further response to 60% with resolution of hypermetabolism of multiple osseous and liver metastases
Clinical Response in a CCDC6-RET NSCLC Patient
Courtesy of A. Drilon, Memorial Sloan Kettering Cancer Center
Baseline C3D1

• RXDX-105 has demonstrated a manageable safety profile in patients with advanced or metastatic solid tumors
• 22 RET fusion-positive, RET inhibitor-naïve NSCLC patients treated at the 275 mg or 350 mg QD were evaluable for efficacy
• Of these, 8 patients harbored RET fusions partners other than KIF5B: CCDC6, EML4, and PARD3 • ORR of 75% (95% CI: 34.9% - 96.8%) in patients with non-KIF5B-RET fusions • Additionally, 1 patient had SD for ~6 cycles • Median DOR has not been reached, with the longest DOR at 10.2 months
• Of the other 14 patients harboring the KIF5B-RET fusion, none had a RECIST response, although 3 patients had SD lasting ≥ 6 months
• This disparity in response between tumors with the KIF5B and non-KIF5B fusion partners is consistent with previous pooled efficacy evidence with other RET-active agents, suggesting that KIF5B-RET fusion may be less susceptible to targeted inhibition
13
Conclusions
1. Drilon, A., et al. (2016), The Lancet Oncology, 17(12), 1653–1660
2. Yoh, K., et al. (2017), The Lancet Respiratory Medicine, 5(1), 42–50

The authors wish to thank the patients and their families, the investigators, and the site personnel
who participated in this study
14
Acknowledgements


















