A PHARMACEUTICAL NEEDS ASSESSMENT FOR · PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY...
199
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011 1 A PHARMACEUTICAL NEEDS ASSESSMENT FOR NHS WANDSWORTH 2011-2013 Author: David Tamby Rajah, Community Pharmacy Lead NHS Wandsworth Date: 1 st February 2011 WANDSWORTH COMMUNITY PHARMACIES & NHS WANDSWORTH WORKING TOGETHER SERVING OUR PATIENTS
-
Upload
vuongtuyen -
Category
Documents
-
view
214 -
download
0
Transcript of A PHARMACEUTICAL NEEDS ASSESSMENT FOR · PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY...

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
1
A PHARMACEUTICAL NEEDS ASSESSMENT FOR NHS WANDSWORTH 2011-2013
Author: David Tamby Rajah, Community Pharmacy Lead NHS Wandsworth
Date: 1st February 2011
WANDSWORTH COMMUNITY PHARMACIES & NHS WANDSWORTH WORKING TOGETHER SERVING OUR PATIENTS

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
2
Abbreviations and Glossary AUR Appliance Use Review LPC Local Pharmaceutical Committee
BBV Blood Borne Viruses LPS Local Pharmaceutical Service
BLT Barts and London NHS Trust LSOA Lower Layer Super Output Area
BME Black and Minority Ethnicity MAS Minor Ailments Scheme
BMI Body Mass Index MMR Measles, Mumps and Rubella
CDT Community Drug Team MUR Medicine Use Review
CHD Coronary Heart Disease NCSP National Chlamydia Screening Programme
CKD Chronic Kidney Disease NHS National Health Service
COPD Chronic Respiratory Disease NHSIC NHS Information Centre
DAC Dispensing Appliance Contractor NRT Nicotine Replacement Therapy
DH Department of Health OCT Over the Counter
DOT Directly Observed Therapy ONS Office of National Statistics
DRS Directly Standardised Rate PCT Primary Care Trust
EHC Emergency Hormonal Contraceptive PDU Population of Problematic Drug Users
ELFT East London NHS Foundation Trust PGD Patient Group Direction
FTE Full-Time Equivalent PNA Pharmaceutical Needs Assessment
GLA Greater London Authority PPCG Planning for Population Change and Growth
GP General Practitioner PSA Public Service Agreement
GUM Genito-Urinary Medicine PSB Pharmacy Strategic Board
H1N1 Swine Flu Virus PWP Pharmacy White Paper
HIV Human Immunodeficiency Virus QOF Quality Outcomes Framework
INEL Inner North East London SAC Stoma Appliance Customisation
INR International Normalised Ratio STI Sexually Transmitted Infection
TB Tuberculosis Infection IVDU Intravenous Drug User
JSNA Joint Strategic Needs Assessment LAP Local Area Partnership
LINK Local Involvement Network WIC Walk-in Centre
NHS appeals authority A special health authority that was responsible for determining control of entry appeals. Subsequently replaced by the NHS Litigation Authority
Community pharmacy contract The community pharmacy contract is made up of three service levels: essential services, advanced services, and enhanced services.
Consultation facilities / area Most community pharmacies now have an area in the pharmacy where the patient and pharmacist can have a private consultation. The design and specification of these facilities varies from pharmacy to pharmacy.
Medicines Use Review A discussion between the pharmacist and patient with the aim of improving understanding and medicines used by the patient.
ONS Cluster PCTs that are grouped according to local social and economical factors
Pharmacist A registered pharmacist has typically completed five years of training which includes a degree and post-graduate training.
Pharmaceutical services These are services available from pharmacies and dispensing appliance contractors and dispensing GPs.
Pharmacy A registered pharmacy premises that is regulate by the Royal Pharmaceutical Society and appears on the PCT‟s list.
Prescription item (s) Each medicine on a prescription counted as one item. A prescription may have many items.
Quartile One of four divisions which divide a series of data into four equal parts
Quintile One of five divisions which divide a series of data into five equal parts
Repeat dispensing A mechanism by which the patient‟s GP may issue the pharmacist with a prescription to dispense at agreed intervals for ongoing treatment
Secondary care Hospital-based care
Tertiary care Specialist residential care

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
3
ACKNOWLEDGEMENTS
NHS Wandsworth would like to thank:
TONIA MICHAELIDES – Director of Performance & Primary Care Contracting
HOUDA AL SHARIFI – Director of Public Health
GRAHAM MACKENZIE- Director of Strategic Planning and Borough Commissioning
LAWRENCE GIBSON – Associate Director Public Health
YUI-BING YEUNG – Pharmaceutical Analyst MELISSA COTTINGTON - Public Health Information Analyst
SARAH CURTIS – Programme Manager Polysystems
SALLY BAHRI - Public Health Information Analyst
DR AMER SALIM – Local Medical Committee Representative
NICK BEAVON – Chief Pharmacist
ANDREW McCOIG CEO, Sutton, Merton & Wandsworth Local Pharmaceutical Committee
GARY BRADLEY – Prescribing Support Technician
RAJ PATEL – Chair, Sutton, Merton & Wandsworth Local Pharmaceutical Committee
CHRIS CAIRNS – Head of Pharmacy Kingston University
SANITA ELLIS – Primary Care Coordinator – Substance Misuse
ELLEN MUSHAMBI – Pharmacy Graduate Kingston University
RAYCHEL PETERS – Needle Exchange Facilitator
REBECCA MAYHEW – Copyeditor and Proof-reader
FADI DEXTER – Primary Care Support Manager

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
4
Table of Contents Executive Summary .................................................................................................... 7 1 Introduction ........................................................................................................... 10
1.1 The Pharmaceutical Needs Assessment Report ...................................................... 11 1.2 Development of the PNA ..................................................................................... 12 1.3 NHS Commissioning ............................................................................................ 13 1.4 Pharmaceutical Regulations and Control of Entry ................................................... 13
2 Community Pharmacy Contractual Framework ...................................................... 16 2.1 Harmonisation of Services ................................................................................... 17 2.2 Primary Care Contractual Differences .................................................................... 18 2.3 Community Pharmacy Funding ............................................................................. 19 2.4 Types of Pharmaceutical Commissioning ............................................................... 20 2.5 Stoma and Appliances – Direct Appliance Contractors ............................................ 21 2.6 Contractual Framework........................................................................................22 2.6.1 Essential Services............................................................................................22 2.6.2 Advanced Services..........................................................................................22
2.6.3 Funding ......................................................................................................... 22 3 Professional Standards and Statutory Documents ................................................. 24
3.1 Pharmacy White Paper ........................................................................................ 24 3.2 NHS White Paper ................................................................................................ 25
3.3 Health and Social Care Bill ...................................................................................26 3.3.1 Impact on Pharmacy.......................................................................................26
3.4 Conclusions ........................................................................................................28 4 Pharmaceutical Provision in NHS Wandsworth ...................................................... 29
4.1 Community Pharmacy in Wandsworth ................................................................... 29 4.2 Localities.............................................................................................................31
4.3 Prescription Analysis – National and Local ............................................................. 31 4.4 Advanced Services Medicine Use Reviews..............................................................32 4.5 Access by Private and Public Transport ................................................................. 33 4.6 Opening Hours ................................................................................................... 34
4.7 Community Pharmacies outside Wandsworth..........................................................35 4.8 Sector Analysis ................................................................................................... 36 4.9 Summary ........................................................................................................... 37 4.10 Pharmacy Services in Wandsworth ..................................................................... 38 4.11 NHS Wandsworth Community Pharmacy Resources .............................................. 43 4.11a Community Pharmacy Staffing Mix .................................................................. 43 4.11b Premises, IT and Medical Equipment Audit ...................................................... 44 4.11.1 Summary ..................................................................................................... 46
4.12 Acute and Specialist Pharmacy Providers in Wandsworth......................................46 5 Consultation, Patient View and Experience............................................................49
5.1 Street Interviews.................................................................................................49 5.1a Street Interviews Summary Findings.................................................................50
5.2 Patient Group Feedback.......................................................................................56 5.3 Overall Conclusions..............................................................................................56
6 Public Health in Wandsworth ................................................................................. 57 6.1 Population in Wandsworth ................................................................................... 57 6.2 Population Change...............................................................................................59
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
5
6.3 Population Density .............................................................................................. 59 6.4 Ethnic Breakdown of Wandsworth ........................................................................ 60 6.5 Socio-Economic Indicators ................................................................................... 64
7 Health in Wandsworth – Public Health and the Local Borough .............................. 66 7.1 Smoking Cessation .............................................................................................. 67 7.2 Disease States & Long Term Conditions ................................................................ 70 7.3 Cardiovascular Disease ........................................................................................ 74 7.4 Diabetes ............................................................................................................ 75 7.5 Cholesterol ......................................................................................................... 75 7.6 NHS Healthchecks ............................................................................................... 77 7.7 Respiratory Disease & COPD ................................................................................ 77 7.8 Sexual Health ..................................................................................................... 78 7.8.1 Emergency Hormonal Contraception through Community Pharmacy ................... 80 7.9 Drugs and Alcohol ............................................................................................... 85 7.9.1 Understanding General Prevalence...................................................................85 7.9.2 Services for Drug Misusers...............................................................................87 7.9.3 Geographical Spread.......................................................................................88 7.9.4 Supervised Administration and Needle Exchange...............................................90 7.10 Obesity ............................................................................................................ 98 7.11 Mental Health and Social Inclusion ..................................................................... 98 7.12 Cancer and Palliative Care.................................................................................. 99 7.13 Care Homes .................................................................................................... 100 7.14 Health Outcomes and Inequality in Wandsworth.................................................101
8 Locality Profiles and Polysystems ........................................................................ 106 8.1 Locality Commissioning Groups and Polysystems ................................................. 109 8.2 West Wandsworth ............................................................................................. 110
8.2.1 Roehampton ................................................................................................ 113 8.2.2 Putney, West Hill ......................................................................................... 115 8.2.3 West Wandsworth Needs Analysis and Local Pharmaceutical Commissioning Recommendations ................................................................................................ 116
8.3 Central Wandsworth .......................................................................................... 119 8.3.1 Services Provided ......................................................................................... 122
8.4 Balham, Tooting & Furzedown (BTF) .................................................................. 123 8.4.1 Services Provided ......................................................................................... 125
8.5 Battersea ......................................................................................................... 126 8.5.1 Battersea LCG Identified Workplans ............................................................... 131 8.5.2 Services Provided..........................................................................................136
9 NHS Wandsworth and Wandsworth Council ........................................................ 137 9.1 NHS Wandsworth Commissioning Strategic Plan NHS Wandsworth ........................ 137 9.2 Community Pharmacy Contractual Framework vs. NHS Wandsworth CSP ............... 137 9.3 Primary Care .................................................................................................... 139
9.3.1 General Practice ........................................................................................... 141 9.3.2 Tooting Walk in Centre/Minor Injuries Unit ..................................................... 144 9.3.3 Self-Care, Minor Conditions and Minor Ailments .............................................. 144 9.3.4 Virtual Health Wards .................................................................................... 146 9.3.5 Information Technology ............................................................................... 148
9.4 Public Health & Wandsworth Borough Council ..................................................... 149 9.4.1 NHS Public Health White Paper......................................................................150

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
6
9.4.2 Wandsworth Borough Council.........................................................................150 10 Prescribing and Medicines Management ............................................................ 152
10.1 Aims of the Strategy.........................................................................................152 10.2 Specials Medicines ........................................................................................... 158 10.3 Waste Medicines..............................................................................................158 10.4 Oral Nutritional Supplements.............................................................................159 10.5 Local Pharmaceutical Service Contracts ............................................................. 161 10.6 Monitored Dosage Service ................................................................................ 162 10.7 Non-Medical Prescribing ................................................................................... 162 10.8 Commissioning Recommendations.....................................................................162
11 Commissioning Strategy and Commissioning Recommendations ...................... 164 11.1 Key Commissioning Principles ........................................................................... 164 11.2 Gap Analysis and Commissioning Recommendations .......................................... 165
12 The Future............................................................................................................167 12.1 Emerging Organisations...................................................................................168 12.2 Changes and Updating.....................................................................................170
References .............................................................................................................. 171 Appendixes ...................................................................................................................
Appendix 1 Project Plan...........................................................................................174 Appendix 2 Prescription Demand London .................................................................. 176 Appendix 3 Population Breakdown of the Borough of Wandsworth .............................. 178 Appendix 4 Joint Strategic Needs Assessment Key Messages......................................180 Appendix 5 Attributes of a Good Pharmaceutical Service World Class Pharmacy – Pharmacy White Paper ............................................................................................ 184 Appendix 6 Patient Engagement .............................................................................. 185 Appendix 7 PNA briefing for Stakeholders ................................................................. 186 Appendix 8 NHS Wandsworth Commissioning Strategy .............................................. 187 Appendix 9 Joint letter from PSNC and BMA supporting improved collaboration between Community Pharmacy and General Practice .............................................................. 189 Appendix 10 Community Pharmacy Opening Hours ................................................... 189 Appendix 11 Community Pharmacy Enhanced Services...............................................195 Appendix 12 Commissioning Toolkit..........................................................................199

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
7
Executive Summary
The Pharmaceutical Needs Assessment is a statutory requirement for PCTs to have as a guide for the commissioning of pharmaceutical services and community pharmacy contract applications. Information presented about community pharmacies is based on data taken in September 2010. Wandsworth has a network of 63 community pharmacies and one dispensing appliance contractor within the borough, which serve both the resident population and patients who visit the borough. It should be noted there are pharmacies neighbouring Wandsworth in Lambeth, Sutton & Merton, Richmond and Kingston, and a 24 hour pharmacy in Earls Court which provides access to Wandsworth residents. Wandsworth is well served by the existing community pharmacy network within the borough and in areas neighbouring the borough. There is very good access to private and public transport. NHS Wandsworth has sought to develop the role of Community Pharmacy, which has a key role to play in public health, minor ailments, medicines management and long-term conditions. There are contractual differences between Community Pharmacy and other primary care contractor groups (General Medical Services contract, dental and ophthalmic contracts), which should be taken into account in commissioning. In Wandsworth there are other pharmaceutical providers such as the pharmacy team at St George‟s and the SW London Mental Health Trust. Their contribution to commissioned services should also be included in commissioning of services. In order to assess the adequacy of the provision of pharmaceutical services, NHS Wandsworth has defined the following as services to meet the current needs of Wandsworth:-
High volume services usually have between 25-40 pharmacies providing that service. These high volume services include:-
Minor Ailments
Emergency Contraception
Supervised Administration
Stop Smoking Some of the PCT-commissioned services in Wandsworth are lower volume or pilot services. Examples include asthma, needle exchange and medicines management, which have between 2-12 pharmacies covering the borough, which is sufficient to meet local needs. These services are commissioned on a smaller network basis.
Supervised Administration
Needle & Syringe Exchange
Palliative care Stop Smoking Minor Ailment Service
Out of Hours (Rota Service – Access to Medicines)
Emergency Contraception under PGD Targeted Medication use reviews Care Homes Monitored Dosage services Patient group Directions Medicines management Hepatitis C screening

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
8
It should be noted that stop smoking, needle exchange, access to emergency contraception (EHC), and chlamydia screening can also be provided by other providers, which the PCT will take into account in this needs assessment. NHS Wandsworth operates 11 local pharmaceutical services (LPS) and one essential small pharmacy service (ESPS). The whole of Wandsworth is designated with these contracts. NHS Wandsworth will commission pharmacies outside Wandsworth to provide locally enhanced services subject to the service criteria, close proximity to the border of Wandsworth, and compliance with contractual monitoring in their host PCT. In terms of service gaps, the care home service requires complete re-engineering, which involves a shared care arrangement between the care home, GP practice and community pharmacy focused on patient care and medicines. NHS Wandsworth fully supports the harmonisation of services and standardised accreditation to allow pharmacists to bring their experience of services from other PCTs. Patients The patient or customer service experience is fundamental to any service. The public in Wandsworth are generally satisfied with pharmacy services and there are opportunities to develop service skills, such as making better use of consultation rooms so the public can have private consultations, and ensuring that advice around minor conditions is robust and evidence-based. The PNA strongly recommends pharmacy engagement and representation at patient groups such as the Local Involvement Networks (LINks), Drug Misuse Forum, Young Persons‟ Forum and patient locality groups. This will support development and continual improvement of pharmacy services through patient feedback and relationships with the public.
Localities and Local Commissioning Groups Wandsworth has been divided into four localities for the purpose of the PNA:
Battersea
West Wandsworth
Central Wandsworth
Balham, Tooting and Furzedown The localities match the boundaries of the GP-led Local Commissioning Groups (LCGs). The pharmacies in the localities provide a range of locally enhanced services, which patients can access. Community pharmacy representation at the LCGs will be key to ensure better integration and increased professional engagement.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
9
Medicines management Community Pharmacy has a key role to play in medicines management. A dramatic reduction in the cost of specials medicines was achieved through the Local Pharmaceutical Committee, community pharmacy lead and Wandsworth community pharmacies working together to reduce this cost. At the time of writing this report costs have been reduced from £140k/month to £79k/month. Community Pharmacy still needs to be better integrated into the Medicines Management. Development and Commissioning Strategy The development and commissioning of high quality services will require joint-working with key stakeholder organisations such as the Royal Pharmaceutical Society, Southwest London Local Practice Forum, National Pharmacy Association and College of Pharmacy Practice. This will ensure standards in accreditation. The Future The PNA has been written during tremendous changes in the NHS. The NHS White Paper (July 2010) has seen a major change in NHS organisations:
The loss of PCTs by 2013
New organisations: GP consortia Public Health moving to local authorities and setting up the Health and
Wellbeing boards National/Local NHS Commissioning Board
The PNA will be the responsibility of the Health and Wellbeing board. Control of entry will be the responsibility of the NHS Commissioning Board who will use the PNA to determine applications to the pharmaceutical list. It is important that both groups communicate clearly and update on any service or regulatory changes that may affect the PNA.
Updating the PNA
The PNA for Wandsworth has sought to provide up-to-date information, but with time, changes will take place. It is important that the PNA is kept updated.
Regulatory changes will require consultation and appropriate revision
Changes to the pharmaceutical list, commissioned services and opening hours would result in minor changes and re-mapping of services and updating core data. This information could be printed as supplementary statements describing the changes, or an annual review where such revised data is amended in the core document.
The PNA must be reviewed every 3 years

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
10
1. INTRODUCTION It is now a regulatory requirement and statutory duty for PCTs to produce a Pharmaceutical Needs Assessment (PNA) report by 1st February 2011 (see reference 30). The regulations provide clarity over the structure and content of the document. Provisions in the Health Act 2009 will require Primary Care Trusts to develop and publish a mandatory Pharmaceutical Needs Assessment, which will then be used in the determination of applications for inclusion in a pharmaceutical list. In the current Pharmaceutical Regulations a PNA is defined as “The statement of the needs for pharmaceutical services [in its area] which each Primary Care Trust is required to publish”. The term pharmaceutical (pharmacy) service refers to the definitions in the NHS regulations around the services provided by community pharmacies under their contractual framework and by local pharmaceutical service contracts, appliance contractors and dispensing doctors. In Wandsworth there are community pharmacies and appliance contractors but not dispensing doctors as these are solely relevant to rural areas, so do not apply to Wandsworth.
The purpose of the Pharmaceutical Needs Assessment (PNA) is to identify the pharmacy services that NHS Wandsworth wishes to commission from various providers, such as Community Pharmacy, acute pharmacy, appliance contractors and access to medicines. For Community Pharmacy, the services that will be considered in the PNA are covered under their contractual framework (see Section 2).
This will be carried out by reviewing existing provision of pharmacy services and comparing with Wandsworth’s local needs. The report will take into account the current regulations and professional standards and strategy of the pharmacy profession. This report will support the following activities:- To be used as a guide in the determination of Community Pharmacy Contract Applications -
a process currently called Control of Entry (see reference 27 and 28), to be replaced by a Market Entry Test, anticipated in 2011
Commissioning and procurement of pharmacy services from various providers
Developing high quality pharmacy services to meet the needs of the population in Wandsworth
Including the role of appliance contractors
The PNA will now cover all aspects of pharmaceutical commissioning, which includes Community Pharmacy e.g. acute sector market management, access to medicines, community services.
PCTs must undertake a consultation process on the first draft of the PNA for a minimum of 60 days. Some of the key groups to be consulted are the Local Pharmaceutical Committee (LPC), the Local Medical Committee (LMC), patient groups such as the Local Involvement Network (LINk) and neighbouring PCTs. The PNA must slow divide the PCT area or borough into defined localities. The regulations also require the PCT to define localities around which the PNA will be making Control of Entry decisions. The needs of these localities will be taken into account.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
11
This document has to be updated every three years; annual revisions can be made in line with local developments or changing needs. The scope of this document is much wider, with respect to the importance of how it will fit into pharmacy commissioning and procurement. The current Control of Entry system will be replaced with a Market Entry Test (expected to be introduced through regulations in 2010 and 2011, determined by reference to local Pharmaceutical Needs Assessments). The PNA report will be used to identify where Community Pharmacy can add value through the service tiers of the new Pharmacy Contractual Framework. This will give the PCT an opportunity to review commissioning and service design through Community Pharmacy and other pharmaceutical providers. The Department of Health (DH) introduced new legislation and guidance to PCTs in April 2010 about key requirements for the PNA and how this document will be used in commissioning. This document sets out the vision for integration of Community Pharmacy and other pharmaceutical providers in the wider health economy in NHS Wandsworth Primary Care, Public Health and Wandsworth Borough Council. In addition the PNA for Wandsworth will integrate with the best practice of the Royal Pharmaceutical Society to ensure that professional standards and a code of ethics are maintained. 1.1 The Pharmaceutical Needs Assessment Report
The Pharmaceutical Needs Assessment (PNA) is drawn from various sources of information used to compile the report as shown below.
Pharmaceutical Needs Assessment
Report
NHS WANDSWORTH PUBLIC HEALTH
REPORT
NHS WANDSWORTH COMMISSIONING
STRATEGY
RPSGB PROFESSIONAL & NATIONAL POLICIES
PHARMACY WHITE PAPER REGULATIONS
LOCAL COMMISSIONING
GROUPS
PRIMARY CARE WORK STREAMS
POLYSYSTEM DEVELOPMENTS VIRTUAL WARDS
WANDSWORTH BOROUGH COUNCIL
DATA FROM EXISTING
PHARMACY SERVICES
JOINT STRATEGIC NEEDS ASSESSMENT
SERVICE NEEDS ASSESSMENT
e.g. DAAT, Sexual Health, stop smoking
BASELINE ANALYSIS –COMMUNITY
PHARMACY STAFFING
PRESCRIBING DATA& MEDICINES
MANAGEMENT POLICIES
There are differences between the PNA and other types of needs assessments as the PNA‟s content is set out in NHS regulations and there is a consultation process. There are similarities to Joint Strategic Needs Assessments (JSNAs). The PNA will derive information from the JSNA as well as other sources as listed above. The PNA is a standalone document that focuses purely on pharmaceutical services.
The PNA is the systematic method of identifying the unmet healthcare needs of a population and making changes to meet these needs. The PNA allows identification of the varying needs of the PCT‟s population and assists the prioritisation, planning and delivery of services in the most resource-effective way, linked to the needs of the local population, PCT and borough strategic commissioning plans.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
12
The PNA introduces openness and accountability into the process of service selection. In order to understand the pharmaceutical needs of its population, NHS Wandsworth has undertaken a comprehensive PNA exercise. Findings from the PNA will be used to:
Stipulate the full and prescribed range of services required to be provided for „exemption‟ applications submitted to the PCT
Inform the PCT Community Pharmacy Commissioning Strategy. The information for this report is primarily taken from two sources:-
Internal analysis – Current existing pharmaceutical provision by NHS Wandsworth community pharmacies through a baseline analysis of services, staffing and opening hours
External analysis – Reviewing Public Health data, data from Wandsworth Borough Council population information, and current PCT commissioning priorities to understand patient needs.
Under the DH regulations the views of stakeholders such as patients will be taken on board.
Patient view The views and comments of patients and healthcare professionals on existing pharmacy services.
From the PNA the information will be analysed and this will develop the commissioning strategy for pharmaceutical services within Wandsworth. This will be used to indicate where there is sufficient provision of pharmaceutical services and where there is a need for pharmaceutical services. The methods of commissioning will take into account the current regulatory framework, pharmacy professional standards and code of Ethics along with the available tools for commissioning pharmacy services. Within this report there are colour-coded summaries.
1.2 Development of the PNA The PCT set up a steering group consisting of the following members to develop the PNA: Strategic Group Board level sponsor – Director of Quality & Professional Practice (Chair) Consultant in Public Health Director of Commissioning – Primary Care & Performance Chief Pharmacist Strategic Planning Manager Operational Support – Commissioning Manager – Pharmacy External Champion – LPC member with responsibility for Pharmacy Patient and Public Involvement Development Manager Communications Manager
The blue box looks at commissioning intentions for Community Pharmacy and other pharmaceutical services that can be provided in Wandsworth.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
13
Polysystem support which covered the work streams in Practice-Based Commissioning Stakeholder Reference Group (see reference 2 and 5) A Stakeholder Reference Group was set up in June 2010. This group has been invited to make comments on draft versions of the PNA in April and June 2010. Membership consists of: PCT Local Pharmaceutical Committee Representative Local Medical Committee Representative PCT Public Health Directorate Process of developing the PNA
Any changes in pharmacies or commissioned services
Key data sets for the PNA agreed by June 2010
Update Public Health data by November 2010
Finalise service mapping by December 2010
Carry out stakeholder consultation to neighbouring PCTs, Local Pharmaceutical Committees between September 2010- November 2010
Carry out patient consultation by November 2010 and update draft PNA report
Update Medicines Management Strategy November 2010 A draft report was produced by mid November 2010 for consultation. The PNA report has to be signed off by the PCT Board by February 2011. 1.3 NHS Commissioning The PNA is central to taking forward the Pharmacy White Paper and Pharmaceutical Commissioning. The PNA can contribute towards all the commissioning competencies. As listed below:-
Competency 2: Work collaboratively with community partners to commission services that optimise health gains and reduce health inequalities.
Competency 4: Lead continuous and meaningful engagement of all clinicians to inform strategy and drive quality service design and resource utilisation.
Competency 5: Manage knowledge and undertake robust and regular needs assessments that establish a full understanding of current and future local health needs and requirements.
Competency 7: Effectively stimulate the market to meet demand and secure required clinical, and health and wellbeing outcomes.
The PNA will also guide and direct commissioning of pharmacy services at local borough level to develop innovative pharmacy services that support the needs of Wandsworth. 1.4 Pharmaceutical Regulations and Control of Entry
The current process of granting new pharmacy contract applications or relocations of existing contracts is called Control of Entry. This is set down in the Pharmaceutical Regulations of 2005. The regulations cover pharmacy contract applications which are made under the necessary or expedient route, and in addition four types of application were exempted from this ruling (see reference 21 and 28) :-

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
14
1. Wholly internet or mail-order pharmacies that provide a full professional service. 2. Pharmacies located in out-of-town shopping centres of more than15,000 sq metres. 3. Pharmacies that intend to open for more than 100 hours per week.
These pharmacies must demonstrate that they are open and available 100 hours per week
PCTs will be required to „de-list‟ any pharmacy that consistently fails to meet the terms of the exemption unless there is good cause.
4. Applications from members of a consortium establishing a new one-stop primary care centre.
The centre must offer a wide range of primary care and community-based services in addition to usual GP services e.g. dentistry, optometry, podiatry, other social or community-based services, to a registered population of around 18,000-20,000 patients.
This exemption only applies to centres that are part of the PCT‟s Strategic Service Development Plans (SSDP) or equivalent.
The Department of Health has published its proposals for legislative change for Pharmacy as part of the Health Bill. The Health Bill received Royal Assent on 12th November 2009. The Act contains a number of reforms to NHS pharmaceutical services. These will include:-
Market entry - Replacing the current Control of Entry system with a Market Entry system, based on PCTs‟ Pharmaceutical Needs Assessments
Quality and performance - PCTs will have new powers to take more effective action where providers are not delivering services, and will have the option to withhold funds to an acceptable level. This will in turn form part of a wider quality and performance programme, using existing and new legislation for providers of pharmaceutical services.
Local Pharmaceutical Services (LPS) - Amendments to the current LPS legislation to allow PCTs to provide pharmaceutical services directly in specific circumstances, such as national emergencies.
Expected timeframe for regulatory change:-
April-May 2011 – New regulations come into force, which will replace 2005 Control of Entry test with Market Entry
Feb 2011 – PCTs must have Pharmaceutical Needs Assessments in place
The PNA will be revised in accordance with the new NHS regulations and guidance from April 2011 onwards.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
15
Fig 1: Bill introduced Jan 11 and Royal Assent by December. Implementation in stages from April 12 when SHAs abolished

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
16
2. COMMUNITY PHARMACY CONTRACTUAL FRAMEWORK In April 2005 the Community Pharmacy Contractual Framework was launched by the DH (see reference 2) and a summary is presented below. Community pharmacies operate under Schedule 1 of the Pharmaceutical Service Regulations and the services listed below provided under Terms of Service. Community pharmacies:-
Have to dispense drugs
Can dispense appliances Table 1 Community Pharmacy Contractual Framework
ESSENTIAL ADVANCED ENHANCED
NATIONAL CONTRACT
LOCALLY ENHANCED
ES1 Dispensing of Medicines ES2 Repeat Dispensing ES3 Health Promotion ES4 Signposting ES5 Support for Self Care ES6 Disposal of Unwanted Medicines ES7 Support for Disabilities ES8 Clinical Governance
AS Medicines Use Review
& Interventions
(maximum of 400 MURs
can be completed)
EN1 Supervised Administration EN2 Needle & Syringe Exchange EN3 Palliative Care EN4 Stop Smoking EN5 Care Home EN6 Medicines Assessment & Compliance Support EN7 Medication Review (Full Clinical Review) EN8 Minor Ailment Service EN9 Out of Hours (Access to Medicines) EN10 Supplementary Prescribing by Pharmacists EN11 EHC via PGD EN12 Seasonal Influenza Vaccination EN13 Patient Group Directions EN14 Chlamydia Screening & Treatment EN15 NHS Healthchecks
Three tiers of service include:- Essential services, which every community pharmacy must provide and must be compliant with through annual contractual monitoring. Advanced services, Medicines Use Reviews (MURs), which pharmacies can choose to provide, if they meet the accreditation. Requires a suitable consulting room and completion of an accredited course. Enhanced services, which are commissioned locally by PCTs according to need. For essential and advanced services the specification and funding is agreed nationally. Enhanced services funding is agreed locally by PCTs. All services have national specifications which can assist PCTs in commissioning services. PCTs should apply the strategic commissioning tests with respect to the pharmacy contract (COMMUNITY PHARMACY STRATEGIC COMMISSIONING TESTS AND COMMUNITY PHARMACY ASSURANCE
FRAMEWORK 2007/08)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
17
The commissioning tests broadly represent a prompt in the following areas:-
1. National policy and priorities 2. Shared Strategic Needs Assessment 3. Planning, commissioning and contracting 4. Performance management
5. Workforce 6. IT (and other infrastructure) 7. Patient access, patient choice and patient
experience 8. Market development and market management
The purpose of the tests is:-
To establish a tool to be able to demonstrate that the PCT is maximising the value of primary care contracts and other arrangements by:
Ensuring Community Pharmacy is fully integrated into the commissioning process;
Ensuring that Community Pharmacy is used as an enabler in service redesign;
Ensuring that Community Pharmacy is delivering specific NHS outcomes;
Ensuring that a „fit for purpose‟ pharmacy-related infrastructure is in place to enable the above.
To provide a prompt for PCTs, GP consortia (local commissioning groups, borough councils and NHS Commissioning Board) to take account of relevant published documents
To set Community Pharmacy in the context of the operating framework, PBC guidance and commissioning framework
In NHS Wandsworth the following enhanced services have been commissioned:-
EN1 Supervised Administration EN2 Needle & Syringe Exchange EN3 Palliative Care EN4 Stop Smoking EN5 Care Home EN6 Medicines Assessment & Compliance Support
EN8 Minor Ailment Service EN9 Out of Hours (Access to Medicines) EN11 EHC via PGD EN14 Chlamydia Screening & Treatment Pharmacy Obesity Service Pharmacy Asthma Service Pharmacy Medicines Management Service
Generally NHS Wandsworth has complied with the strategic commissioning tests and has utilised most of the contractual framework. Further work is required to integrate Community Pharmacy into key PCT workstreams such as long-term conditions, medicines management strategy and NHS healthchecks. The framework can also be applied to local borough commissioning plans as possible commissioning options for health and social care services. 2.1 Harmonisation of Services Each PCT commissions their pharmacy locally enhanced services and this has resulted in different specifications and fees. While each service is meant to be designed to local need, there is no set standardisation or harmonised accreditation. This has a negative impact on the Community Pharmacy workforce, which is quite mobile as pharmacists trained and accredited to provide a service in one PCT may have to retrain in another PCT they move to. This has an impact on community pharmacy services that can lead to a loss of service provision. Many community pharmacies are now consolidating and are buying contracts in different PCTs and work across larger areas. The Department of Health has asked PCTs in London to support a common harmonisation of accreditation and work towards standardised services. An agreement has been in place from the

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
18
former SW London Strategic Health Authority for all SW London PCTs to have reciprocal accreditation agreements for services. Service harmonisation has the following benefits:-
Better standardisation of services results in pharmacists who are trained to provide services being able to transfer their skills and experience to different PCTs
Better integration of pharmacy professional standards
More cost-effective utilisation of the Community Pharmacy workforce
More opportunities for resource-sharing between commissioning organisations
Maintains service continuity across a sector. NHS Wandsworth is committed to professional consolidation and consistency around pharmacy services. PCTs are required under the PNA regulations to consult with stakeholders. One key feedback from Community Pharmacy Groups and bodies is for the need for standardised services and accreditation. Feedback is provided below:-
There is still the general issue of accreditation across PCTs when locum pharmacists are covering holidays or sickness and we are continually pressing for nationwide accreditation to make continuity of provision easier to manage. (National Cooperative Pharmacy Jan 2011) Commissioning for patients • Community and specialist pharmacy should be commissioned nationally; • A level playing field must be given to all providers, including pharmacy, by GP–led
commissioning consortia. (Royal Pharmaceutical Society Jan 2011)
2.2 Primary Care Contractual Differences
There are some key contractual differences between Community Pharmacy and other primary care contractor groups which will be an important consideration in commissioning.
Community Pharmacy has a National Contractual Framework, and there is no signed contract between the PCT and contractor. (This also applies to Dispensing Appliance Contractors (DACs)).
Pharmacy Premises o Pharmacy premises are registered with the RPSGB o A PCT-approved consulting room is required to conduct MURs, which is covered by
the NHS regulations o There are no clear „primary care‟ standards in the contractual framework or terms of
service. Infection control is not built into the core contractual framework.
Finance o Community pharmacists are not pensionable.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
19
o Only one PC system funded through the contract o No IMT DES (Directed Enhanced Service) o Community pharmacists provide their own IT, premises, CPD, staffing etc.
Breach of Terms of Service - referral to another PCT to review a pharmacy case.
Patients do not have to register with a pharmacy to receive a service. This has implications for commissioned services and for pharmacies located on the border with another PCT where the Community Pharmacy may see patients from different PCTs.
The above contractual differences between Community Pharmacy and Primary Care contractor groups will have an effect on commissioning of locally enhanced services (LES), and this will affect service contracting.
2.3 Community Pharmacy Funding Community pharmacy funding is remunerated through a national contractual framework. Before April 2010 PCTs were allocated a national budget for practice payments, Electronic Transfer of Prescription (ETP) payments and Medicines Use Reviews. The remainder of the Community Pharmacy Payment was allocated through the national Pharmacy Global Sum held by the Department of Health which covered ETP payments, establishment payments and dispensing fees. In April 2010 each PCT in England was allocated a portion of the Global Sum on a cash limited basis. The Global Sum portion of the community pharmacy contract funding has been divided and allocated to each PCT on a fair share basis calculation. Currently this funding is non-recurrent and is going through a test period. The Global Sum composition is shown below. Figure 2: Breakdown of Pharmacy Global Sum
PCTs have been advised by the Director of Finance in March 2010 to manage the transition, including building up data in 2010-11 and beyond using the new basis of charge. It is important that the PCT maintains steady state in terms of patterns and levels of activity. PCTs should not seek to extend prescription duration, with the aim of reducing the fees and allowances paid to Community Pharmacy and appliance contractors. There are major implications of significantly extending prescription duration, which include:-

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
20
Creating widespread shortages of medicines, with patients unable to obtain the essential medicines they need
Medicine prices increasing as a result
Associated increases to the cost of pharmaceutical services as pharmacists and their staff spend increased amounts of time trying to locate medicines
A likely increase in the wastage of medicines
Undermined financial viability of individual pharmacies, not just due to reductions in fees and allowances, but due to the delay in full reimbursement of drug costs (up to three months after dispensing).
Pharmacies could be affected indiscriminately and disproportionately, with no link to their standard of service provision or patients‟ ability to access their medicines. Furthermore, PCTs may then fail to meet their statutory duty to ensure the adequate provision of NHS pharmaceutical services.
It will not lead to cost savings. DH monitors fees and allowances to ensure payments deliver the agreed annual financial sum, as required under the national contractual framework. If there is a significant reduction in prescription volume and hence decrease in fees and allowances paid, upward adjustments to fees and allowances will need to be made in year, to ensure the contractual framework sum is delivered.
The financial implications are that the PCT has a cash-limited sum for the existing community pharmacy contracts. Any additional contract represents an extra cost. The PCT will work within its financial resource. 2.4 Types of Pharmaceutical Commissioning The commissioning of community pharmacy services can be delivered through the following (see appendix 12):-
Locally enhanced services – Within the contractual framework under the current regulations, community pharmacies must be compliant in provision of essential services. All locally enhanced services in Wandsworth will be offered through an expression of interest which will include :-
o Proof of delivering essential services to a high standard o Proof of delivering PCT-commissioned services to a high standard o NHS email o Stable staffing for the last three years.
Local pharmaceutical services – Under the current regulations and existing contractual framework community pharmacies cannot be tendered or subjected to local contractual redesign. The Local Pharmaceutical Service contract does allow for local contractual redesign and tendering. This type of contract does give a PCT a tool to locally innovate pharmaceutical services to meet local need (see reference 22 and 26).
From April 2010 the PNA will have a broader view of pharmaceutical commissioning and access to medicines and will have to take into account not just Community Pharmacy but also the following:-
Management of the PCT prescribing budget

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
21
Non-medical prescribing – Independent or supplementary prescribing allowing healthcare professionals to prescribe within their level of competence. This can be applied to opticians and podiatrists as well as nurses and community pharmacists
Pharmacists with special interest
Out of Hours access to medicines
Acute Pharmacy and Specialist Tertiary Care Pharmacy who could provide services to Primary Care
Patient Group Directions and Patient Specific Directions – allowing pharmacists, nurses, optometrists and podiatrists the ability to supply prescription-only medication against a direction
Pharmacists with Special Interest – Commissioning of Specialist Pharmacist roles
Appliance contractors – there will be a contractual framework for appliance contractors from April 2010.
Fig 3: Pharmacy Development Model
Figure 3 above shows the Pharmacy Professional Development Model which shows the different tiers of pharmacy practice. Pharmaceutical commissioning will have to reflect all sectors of the pharmacy profession and where skills can be fully utilised or developed and commissioned according to need. 2.5 Stoma and Appliances – Direct Appliance Contractors
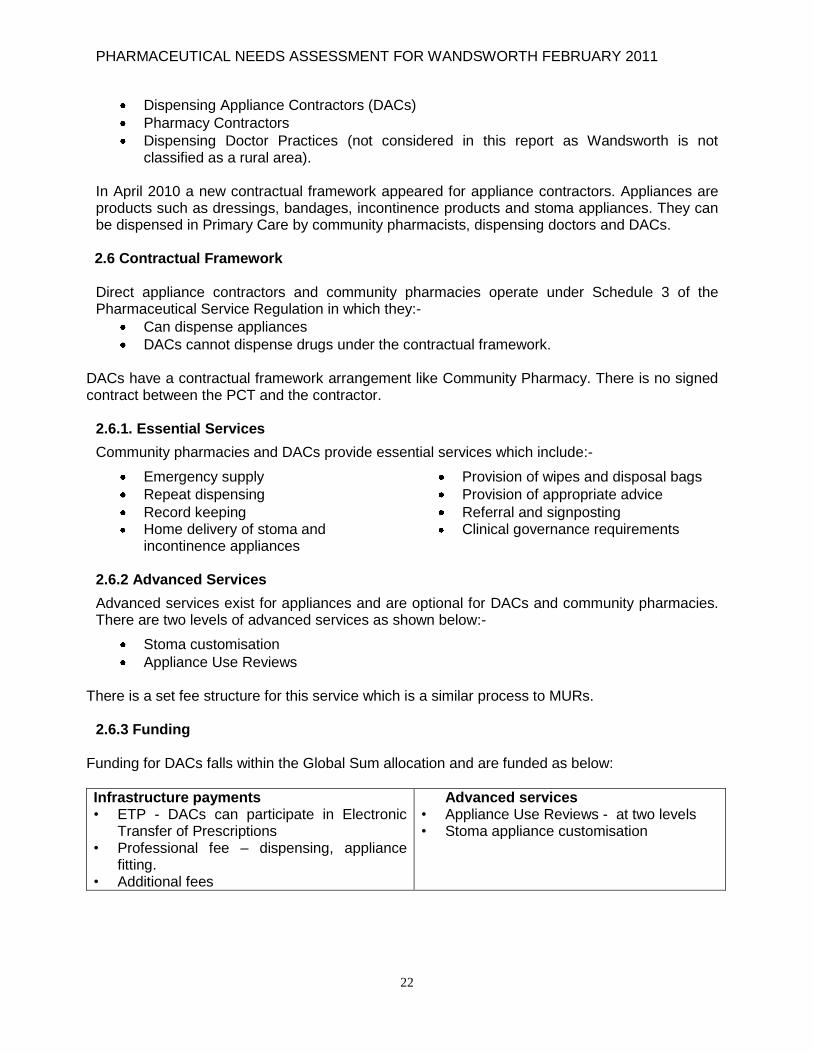
The PNA considers the role of the Direct Appliance Contractor (DAC) which is a supplier of appliances such as stomas and colostomies. In Wandsworth there is one DAC. The Department of Health recognised that due to the specialist nature of this service it was important to have a contractual framework and this should be considered in the Pharmaceutical Needs Assessment. Most community pharmacies and dispensing doctors would dispense and provide appliances to patients under prescription and in some cases provide a home delivery service. DACs can also dispense prescriptions for such products, usually employ stoma nurses, provide product customisation and starter kits. DACs will operate and provide services over a much wider geographical area. In 2010 new NHS regulations and a contractual framework was introduced for providers of appliances listed in Part IXA, B and C of the Drug Tariff. Appliances include ostomy and urology patients. There are three types of contractor that can provide this service:
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
22
Dispensing Appliance Contractors (DACs)
Pharmacy Contractors
Dispensing Doctor Practices (not considered in this report as Wandsworth is not classified as a rural area).
In April 2010 a new contractual framework appeared for appliance contractors. Appliances are products such as dressings, bandages, incontinence products and stoma appliances. They can be dispensed in Primary Care by community pharmacists, dispensing doctors and DACs.
2.6 Contractual Framework Direct appliance contractors and community pharmacies operate under Schedule 3 of the Pharmaceutical Service Regulation in which they:-
Can dispense appliances
DACs cannot dispense drugs under the contractual framework.
DACs have a contractual framework arrangement like Community Pharmacy. There is no signed contract between the PCT and the contractor.
2.6.1. Essential Services
Community pharmacies and DACs provide essential services which include:-
Emergency supply
Repeat dispensing
Record keeping Home delivery of stoma and
incontinence appliances
Provision of wipes and disposal bags
Provision of appropriate advice
Referral and signposting Clinical governance requirements
2.6.2 Advanced Services
Advanced services exist for appliances and are optional for DACs and community pharmacies. There are two levels of advanced services as shown below:-
Stoma customisation
Appliance Use Reviews There is a set fee structure for this service which is a similar process to MURs.
2.6.3 Funding Funding for DACs falls within the Global Sum allocation and are funded as below:
Infrastructure payments • ETP - DACs can participate in Electronic
Transfer of Prescriptions • Professional fee – dispensing, appliance
fitting. • Additional fees
Advanced services • Appliance Use Reviews - at two levels • Stoma appliance customisation

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
23
PNA Commissioning Intentions – There is one DAC in Wandsworth and the PCT will be working with the contractor to maximise and make best clinical use of the appliance use reviews and other services to ensure patients in Wandsworth receive the best use of their stoma and appliance products. Appliance use reviews have a key role to play in improved patient care and waste reduction. The DAC in Wandsworth will be expected to work with the NHS Wandsworth community stoma nurses, local commissioning groups and prescribing advisors around patient care and supply of appliances and stoma products. Increased use of repeat dispensing of products will improve patient care and reduce waste. Community pharmacies who wish to provide an appliance service would be expected to work in the same way. There are opportunities for the DAC to work with local pharmacies in order to have a robust and integrated appliance service. There are opportunities for training and development which will support collaborative working.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
24
3 PROFESSIONAL STANDARDS AND STATUTORY DOCUMENTS
The PNA will take into account professional standards and statutory documents. This is to ensure that high quality pharmaceutical services are developed which support ethical standards throughout pharmacy provision in Wandsworth and that strategic national changes are reflected. 3.1 Pharmacy White Paper
April 2008 saw the release of the Pharmacy White Paper (see reference 12, 16 and 17) promoting the Government‟s vision for community pharmacies to be Healthy Living Centres for screening, health promotion and to provide a range of services that complement General Practice. The White Paper should be read in conjunction with the Anne Galbraith Review on the Pharmacy Contract. The Pharmacy White Paper highlights the following:- Strengths of the current system*
A network of health professionals based in the community, offering health promotion, advice and easy access to medicines
Pharmacies open at times that suit patients and consumers
Quick, safe and efficient provision of prescribed medicines
A highly trained and experienced pharmacy workforce
Hospital pharmacists with specialist experience, including prescribing. Future potential – improvements could include*:
Pharmacies becoming „healthy living‟ centres, promoting health and wellbeing
Prescribing certain common medicines and being the first port of call for people with minor ailments – saving up to 57 million GP consultations a year
Expanding the range of medicines available over the counter
Providing support for people with long-term conditions
Screening for vascular disease and sexually transmitted diseases
Providing stop smoking services
Working more closely with hospitals to provide safe, seamless and clinically-focused care
Playing a bigger role in vaccination and contraception programmes
Increasing the number of independent and supplementary prescribers or pharmacists registered as defined specialists on the UK Public Health Register
Involvement in developing clinical pathways that support integrated care. *See reference 12
The Pharmacy White Paper has brought together the principles of World Class Commissioning, Public Health and Medicines Management (see Appendix 5). There is a need to expand access and choice through more help with medicines, including the need to provide access to medicines out of hours, improve the hospital / community pharmacy interface and proposals to extend emergency supplies to 28 days. It encourages the development of pharmacy services to support healthy living and better care, and specifically refers to minor ailment schemes and screening, including vascular risk assessments(NHS Healthchecks) for groups not registered with GPs, and the development of a more defined role in the management of long-term conditions. It recognises that access to Pharmacy is currently very good, with 99% of the population able to reach a pharmacy within 20 minutes. However, pharmacy contract applications are provider-

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
25
driven in terms of location and thus PCTs can have limited control. It encourages PCTs to strengthen their commissioning role to stimulate competition. This can be achieved by undertaking a more rigorous assessment of pharmaceutical needs and using its performance-monitoring powers to terminate contracts in cases of poor performance. The Control of Entry procedure, which is the process to manage new contract applications, is currently under review. It is thought that the outcome of the review is likely to be a move to an approach where applications are reviewed against commissioning priorities. Overall the White Paper provides an opportunity to review current service provision and ensure better integration into Primary Care Commissioning and Public Health development (see Appendix 5). 3.2 NHS White Paper The Community Pharmacy Contract, through payment for performance, will incentivise and support high quality and efficient services, including better value in the use of medicines through better informed and more involved patients. Pharmacists, working with doctors and other health professionals, have an important and expanding role in optimising the use of medicines and in supporting better health. Pharmacy services will benefit from greater transparency in NHS pricing and payment for services (see references 16 and 17). Consortia of GP practices will commission the great majority of NHS services for their patients at a local borough level. They will not be directly responsible for commissioning services that GPs themselves provide, but they will become increasingly influential in driving up the quality of general practice. They will not commission the other family health services of dentistry, community pharmacy and primary ophthalmic services. These will be the responsibility of the NHS Commissioning Board, as will national and regional specialised services, although consortia will have influence and involvement. The key drivers for this change are:-
Demographics – an ageing population making disproportionate use of NHS resources
Growth in prevalence of long-term conditions such as diabetes and heart disease
Relatively high level of errors at all stages in the use of medicines
Public health a priority for the new government
Funding restraints – the need to focus on productivity without compromising quality of patient care
Recognition by pharmacy employers and education providers of the need to co-operate more closely to deliver a pharmacy workforce fit for purpose.
There is a clear focus on efficiencies and outcomes-based services around medicines management. Key to this is a closer working relationship between Community Pharmacy and general practitioners.
PNA Commissioning Intentions – The Pharmacy White Paper has a detailed action plan which needs to be integrated into pharmaceutical commissioning. Since April 2010 there have been no changes to this paper and the principles will be adopted. This will be particularly important for service redesign and commissioning of pharmacy services.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
26
The PCT now has an opportunity to refocus services around outcomes-based medicines management services. This will support the following:-
Management of prescribing budgets
Support of patients around long-term conditions
Reduction of waste medication
Improved communication between general practitioners and pharmacists around medicines management
Overall improvement in management of the dispensing and prescribing process. 3.3 Health and Social Care Bill
The Health and Social Care Bill published in January 2011 will have implications for Pharmacy and will have a major impact on the NHS. The Bill confirms the measures in the NHS White Paper „Equity and Excellence: Liberating the NHS‟. The Bill lists the new organisations, changes to existing organisations, and the abolishment of other originations.
The key changes include:-
The abolition of Strategic Health Authorities and Primary Care Trusts
The transition of hospitals to Foundation Trusts
Establishment of an NHS Commissioning Board
Establishment of GP consortia
The PCT Public Health function moving to local authorities and the creation of the Statutory Health and Wellbeing Board
The National Institute for Health and Clinical Excellence (NICE) will be renamed the National Institute for Health and Care Excellence
The Independent Regulator of NHS Foundation Trusts, which was established to oversee Foundation Trusts, will be now known as Monitor
The Creation of HealthWatch to champion patient and service user voice at national and local levels
Lays the underpinnings for the creation of Public Health England as part of DH
Changes to Arm‟s Length Bodies (ALBs): ⁻ Place NICE on statutory footing and extend remit to social care ⁻ Re-establish Information Centre in primary legislation ⁻ Streamline Arm‟s Length Bodies involved in professional regulation ⁻ Streamline other DH ALBs, transferring their functions where appropriate. (Other
changes to DH ALBS are part of Public Bodies Bill) 3.3.1 Impact on Pharmacy
There will be an impact on Pharmacy as part of the introduction of the Bill which is as follows: • Transfer of functions which currently lie with PCTs to the Board in relation to the
commissioning of pharmaceutical services • Transfer of functions to the Board in relation to pharmaceutical remuneration (Secretary of
State to have powers to intervene on which elements are to be charged to the Board/consortia and to require information)
• Transfer of responsibility for developing and updating pharmaceutical needs assessments from PCTs to Health and Wellbeing Boards of upper-tier local authorities.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
27
Key pharmacy provisions – overview • Pharmaceutical services, including local pharmaceutical services for England will be
commissioned by the Board • Pharmaceutical Needs Assessments (PNAs) will be developed and published by Health
and Wellbeing Boards of upper-tier local authorities • The Board will take over responsibility for dealing with applications for Market Entry in
England • The Board will be given discretion that even if a PNA finds a gap in services, it will not be
obliged to fill that gap as there will be other factors it needs to take into account; • The Board will take over responsibility for fitness to practise matters including
performers‟ lists for pharmacies, including LPS performers (provisions in Act being streamlined)
• The Board will recognise local pharmaceutical (representative) committees • The administration of remuneration for pharmaceutical services for England will be the
responsibility of the Board. The Board will decide which elements of remuneration should be allocated between GP consortia and which should be retained by the Board (GP consortia will be responsible for meeting certain elements such as drugs costs). Secretary of State can direct the Board if desired. (Source DH presentation Overview for pharmacy stakeholders 21 January 2011)
Extracts from the Bill that affect pharmacy are shown below:
A104. The White Paper proposes that commissioning of pharmaceutical services be conferred directly on the NHS Commissioning Board and that it will be for the Board to determine how best it carries out its commissioning functions for pharmaceutical services under the Community Pharmacy Contractual Framework (CPCF). A105. Pharmaceutical contractors would wish to be assured that commissioning and market entry arrangements are sufficiently robust and objective so that no one profession has control or undue influence over the others. A106. Commissioning of pharmaceutical services by the Board increases patient choice. Pharmaceutical contractors can and do provide services which could also be commissioned and provided by GPs e.g. smoking cessation and weight management. A107. Entry to the pharmaceutical list is controlled through legislation. The regulations are there not only to ensure access to and choice of NHS pharmaceutical services but to also ensure that entry to the NHS pharmaceutical services market achieves the right balance between a regime which encourages enterprise and innovation with the requirement that the NHS plans service commissioning to meet identified local needs. A108. The transfer of commissioning to the NHS Commissioning Board would mean that responsibility for maintaining lists of pharmaceutical contractors and recognition of local pharmaceutical contractor representative committees will also lie with the Board. This will require significant professional input to achieve the above.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
28
General Pharmaceutical Council
Under the Bill‟s provisions, regulatory bodies could establish registers for unregulated healthcare professionals, and those studying to join a regulated or unregulated profession. In theory, this means the General Pharmaceutical Council (GPhC) could hold voluntary registers for pharmacy students, preregistration trainees, and non-practising and retired pharmacists. It could also open the door for the GPhC to hold voluntary registers for those practising homoeopathy or herbal medicine.
3.4 Conclusions There will be major organisational change over the next year, and local leadership will be required to ensure that the new emerging organisations work together and communicate to ensure that pharmacy commissioning and development is not lost. The NHS Commissioning Board will have financial and performance accountability for Primary Care independent contractors and responsibility for Control of Entry (changing to Market Entry). The NHS Commissioning Board will use the PNA to determine community pharmacy contract applications and the Health and Wellbeing Board will take responsibility to develop the PNA. Section 12 explores the futures changes and how this will impact the PNA and Pharmacy.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
29
4. PHARMACEUTICAL PROVISION IN NHS WANDSWORTH This section reviews the current pharmaceutical provision within NHS Wandsworth. This will cover Community Pharmacy and also refer to other pharmaceutical and appliance providers. Section 8 will look at the how Wandsworth has been divided into the localities as required by the 2010 Pharmaceutical Needs Assessment regulations. 4.1 Community Pharmacy in Wandsworth PCTs are required to include within their PNA a map that identifies the premises at which pharmaceutical services and dispensing services are provided (NHS Pharmaceutical Regulations paragraph 8, Schedule 3A). There are currently 63 community pharmacies and one appliance contractor in NHS Wandsworth. The distribution of pharmacies across NHS Wandsworth can be seen in Figure 4. There is a mixture of independently owned pharmacies, medium-sized companies and large corporate pharmacy companies. About 23 pharmacies are owned by large corporate chains and the rest are owned by medium-sized and independent pharmacies. Fig 4: Distribution of community pharmacies in NHS Wandsworth

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
30
Since the production of the draft PNA report the following changes of ownership took place in December 2010: Lloyds Pharmacy (no. 31 & 34) was sold to Paydens; Blaze Pharmacy (no. 51) has been sold and is now called Wellbeing Pharmacy. At the time of writing this report there are 63 pharmacies and one DAC in Wandsworth. In terms of availability there is already a very good distribution of pharmacies across Wandsworth. The 63 community pharmacies collectively are open for 3,500 hours a week; each pharmacy is open on average for 9 hours a day, 6 days a week (see appendix 10).
8 pharmacies open on Sunday
22 pharmacies open up to 7pm on weekdays
11 pharmacies have more than one pharmacist working on weekdays
One pharmacy is open 365 days a year.
Wandsworth Ward Analysis of Pharmacies
Table 2 Prescription item analysis by Wandsworth Borough ward population
Ward
No. of Pharmacies
Ward Population (April 2009)
Ward
No. of Pharmacies
Ward Population (April 2009)
Balham 3 14,238 Queenstown 1 16,807
Bedford 1 14,617 Roehampton 5 13,248
Earlsfield 4 14,351 St Mary‟s Park 4 15,791
East Putney 0 14,650 Shaftesbury 2 13,406
Southfields 7 16,141
Fairfield 1 13,878
Furzedown 4 14,367 Thamesfield 5 14,854
Graveney 4 14,325
Latchmere 1 13,785 Tooting 4 14,200
Nightingale 5
14,536
Wandsworth Common 1
14,467
Northcote 6 13,923 West Hill 2 16,229
West Putney 3 13,418
The analysis of prescription items by Wandsworth electoral ward is shown in Table 2 above.
Wandsworth has an average of one pharmacy per population of 4008.
Northcote and Southfields have the highest number of pharmacies.
PNA Commissioning Intentions – This distribution and spread of the existing community pharmacies provide the PCT and Wandsworth with increased service capacity. This provides opportunities for long-term conditions management, self-care and health promotion, which are all central to the Community Pharmacy Contractual Framework.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
31
This analysis can be used as part of the neighbourhood analysis when new contract applications and relocations are submitted to the PCT. There are clearly enough community pharmacies in Wandsworth to meet current patient need of prescriptions. These figures give a rough idea of demand for pharmacies; however it should be noted:-
Patients from outside NHS Wandsworth access pharmacies in Wandsworth
There are pharmacies in neighbouring PCTs that border some of the Wandsworth borough electoral wards. These pharmacies will serve Wandsworth patients and should be considered for any cross-border commissioning.
4. 2 Localities The PNA Regulation (paragraph 7(a), Schedule 3A) requires a PCT to divide into localities. NHS Wandsworth has been divided into four localities in line with the four Local Commissioning Groups (LCGs). Chapter 8 of this report will go further into localities and look at the needs of these localities. The localities are:-
West Wandsworth - (West Wandsworth Local Commissioning group)
Battersea (Battersea Local Commissioning group) SW11 and SW8 South Wandsworth Commissioning Group covers two localities:-
Central Wandsworth covering SW18 (Earslfield and Southfields)
Balham, Tooting and Furzdown (SW17, SW12 and SW16) 4.3 Prescription Analysis – National and Local The graph below shows the average dispensing items per month by all NHS Wandsworth community pharmacies over the last four financial years. Fig 4: Average items dispensed by NHS Wandsworth pharmacies

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
32
Table 3 Average prescription items/month 2009-2010 April 09-Oct 09*
2008-2009
Monthly average prescription item 4791
4596
% Change +4% +4.6%
National average
6129
London average 4509
Over the last three financial years, there has been a steady increase in the number of prescriptions being dispensed by community pharmacies of just less than 5% year on year. Most PCTs in London including NHS Wandsworth dispense 30% less than the UK average monthly prescription, which is 6,129 (see Appendix 2). There is clearly enough pharmaceutical capacity to manage and dispense. This average is the same for London. Wandsworth is also an inner London borough with areas of deprivation. Community pharmacies in Wandsworth have adjusted their opening hours to cope with demand and patient needs. Local prescription analysis showed that 85-90% of all prescriptions prescribed by NHS Wandsworth GPs are dispensed in Wandsworth pharmacies. This presents some opportunities for local Medicines Management to support the prescribing budget, reduce waste medicines, and ensure patients have a better understanding of their medication. 4.4 Advanced Services Medicine Use Reviews Nearly all pharmacies in Wandsworth undertake advanced services or Medicine Use Reviews (MURs). In the regulations for advanced services there is a requirement for a consulting room where the conversation between the pharmacist and the patient cannot be overhead. Each accredited pharmacy can undertake up to 400 MURs. Over the last few years the following number of MURs was undertaken:- In 2007/2008 – 11,362 44% of total MURs In 2009/2010 – 11,1335 42% of Total MURs In 2010/2011 - (8645- April 2011- December 2010)- 45% of Total MURs (Pro rata) Overall pharmacies have undertaken under 50% of MURs that they are allowed to do. MURS remain an area for potential development for the PCT; there are opportunities to develop this service and integrate improving patient medication compliance with long-term conditions, reducing waste medication through improved patient compliance and better integration with GP medication review. A more structured framework of working is required to develop the potential of this service. Local integration of this service at LCG level will support this development.
PNA Commissioning Intentions – There are opportunities for local medicines management to support the management of prescribing budget. Examples include non-medical prescribing, increasing repeat dispensing, prescription intervention and reduction in waste or unused medicines. There is a need to bring in NHS Wandsworth community pharmacies to supporting GP practices in managing the prescribing budgets and ensuring
the best possible quality of care for patients. (See Medicines Management Section 9.5)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
33
During the consultation process the Chief Pharmacist and PCT Prescribing team recommended more focused development of MURs linked to patient outcomes and focused in long term conditions. 4.5 Access to Community Pharmacies The public do not have to register with a community pharmacy and are free to access any pharmacy. The PNA analysed access within Wandsworth and outside Wandsworth. 4.5 Access by Private and Public Transport The Wandsworth network of pharmacies was mapped against access by private and public transport.
Fig 6: Access to pharmacy by private transport
PNA Commissioning Intentions – MURs do have a role to play in patient care but will require more development to be integrated into long-term conditions and focussed on locum outcomes in agreement with GP practices. MURs can support reduction of waste medicines. LCGs will provide an opportunity for this service to be developed further through closer communication between GP practices and community pharmacies.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
34
Fig 7: Access to pharmacy by public transport
Mapping showed that all community pharmacies in Wandsworth are accessible by either public or private transport within five minutes. This has been verified by a commissioned patient survey across Wandsworth in September 2010. 4.6 Opening Hours Community pharmacies are contracted to open for core hours, which are a minimum of 40 hours. They can provide additional or supplementary hours on top of their core hours. An analysis of the opening hours for community pharmacies over the last three years has shown an increase in supplementary hours (see Appendix 10). Figure 8: Supplementary opening hours across Wandsworth

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
35
Mapping of opening hours across Wandsworth postcodes showed a range of opening times where at least there was a minimum of pharmacies open 60 hours a week for more information. All polysystem areas in Wandsworth had most pharmacies open on Saturday and at least one pharmacy open on Sunday. (See Appendix 10.) It should be noted that GP practices have extended their opening hours through PCT-funded locally enhanced services (LES) and directed enhanced services (DES). The PCT does have a Pharmacy Rota Service which can be adjusted to different localities. Community pharmacies have the flexibility to adjust their supplementary hours. More research is required to monitor the prescription volume during these extended hours. It should be noted that community pharmacies have extended their opening hours in response to local need over the last few years. Section 8, which covers the locality profiles, will look at opening hours in these areas. Appendix 10 lists all the opening hours of community pharmacies (September 2010 data). PNA Commissioning Intentions – Community Pharmacy must to be factored into polysystem planning and access. The Pharmacy Rota Service should be adjusted according to local need. Further discussion and engagement is required with community pharmacy contractors. Other forms of access to medicines, particularly out of hours, should be explored e.g. patient group directions and medicines bags for medical out of hours service. 4.7 Community Pharmacy outside Wandsworth Wandsworth patients can access pharmacies outside Wandsworth especially if they live on the border with another borough. There are at least 40-50 pharmacies 0.5 to 5 miles around Wandsworth. There are 10 pharmacies less than 500m from the Wandsworth border. It is likely that these pharmacies serve NHS Wandsworth registered patients. Figure 9: Map of pharmacies open outside Wandsworth

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
36
Table 4: Number of pharmacies per 100,000 population
PCT Population No.
Pharmacies No. of
Pharmacies/100k
No. Of Pharmacies open > 70
hours
No. Of Pharmacies
open on Sunday
No. Of Pharmacies
open for 100 hours or more
Wandsworth 284,000 63 22.18 5 10 0
Croydon 342,800 72 21 6 15 4
Ealing 316,600 71 22.43 5 14 3
Hammersmith & Fulham 169,700 40 23.57 5 9 1
Hounslow 234,200 53 22.63 6 16 4
Sutton & Merton † 398,600 78 19.57 6 11 2
Richmond & Twickenham 189,000 46 24.34 3 4 0
Kingston 166,700 30 18 5 11 0
Lambeth 283,300 62 21.88 6 10 2
Kensington & Chelsea 169,900 38 22.37 12 20 3
† There will be a new pharmacy opening soon. This will increase to 79 pharmacies.
The following has been noted:-
There is a 24 hour pharmacy located in Earls Court
There is a 100 hour pharmacy in Raynes Park
There are 42 pharmacies open over 70 hours, 6-7 days a week neighbouring Wandsworth. 4.8 Sector Analysis
A comparison of pharmacies per 100,000 of borough population was analysed by comparing the number of pharmacies in Wandsworth against SW & SE London PCTs and the Office of National Statistics (ONS) cluster group that Wandsworth falls into.
Figure 10: Pharmacy distribution in South London PCT

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
37
Figure 11: Pharmacy distribution in ONS peer groups
The analysis of pharmacies per 100,000 borough population showed:-
SW London PCTs - NHS Wandsworth was the second highest after NHS Richmond. It should be noted NHS Richmond has a lower population and smaller number of pharmacies than NHS Wandsworth
In all South London PCTs NHS Wandsworth was the third highest
For the ONS grouping NHS Wandsworth is comparable with most PCTs, NHS Westminster being the exception as it has the largest numbers of pharmacies in Wandsworth.
4.9 Summary There is no access problem to pharmacies inside and outside Wandsworth; there are a good number of pharmacies open 70 hours or more in and around Wandsworth. For future development of polysystems, more discussion with local pharmacy contractors should be taken forward so they are part of the planning process in terms of opening hours. It should be also noted that there should be a consideration to other forms of out of hours access to medicines, which is covered later in this report. Wandsworth Council, as part of the consultation period, noted the following:- The conclusion of the PNA that there is no overall shortage of pharmacies in Wandsworth appears justified. However, particular attention must be paid to the retention of provision in those wards in which there is just a single pharmacy. The loss of these pharmacies would be a significant weakening of the network. Also, some of them form key components of secondary shopping parades, and their loss may threaten the viability of these parades. WANDSWORTH BOROUGH COUNCIL ADULT CARE AND HEALTH OVERVIEW AND SCRUTINY COMMITTEE –10TH JANUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
38
PNA Commissioning Intentions – A revised rota system would be more cost effective than additional pharmacy contracts where there is good existing provision. This can be linked to polysystem development and revised in line with GP opening hours. LPS could provide a suitable model of contracting. As the polysystem developments progress over the next few years, out of hours contracting would be a future service that could be commissioned subject to GP changes of demand. Existing locally enhanced services, such as Minor Ailments, EHC and Supervised Administration for drug misusers, could be aligned to a rota service. The Carson report has also identified ways to access medicines outside normal hours. 4.10 Pharmacy Services in Wandsworth This section will look at the type of community pharmacy services that are commissioned in Wandsworth. Information on patient and pharmacy eligibility and cross-border commissioning can be applied. (See Table 5a on following page.) The current regulations that govern the PNA require the PCT to assess the adequacy of the provision of pharmaceutical services. PCTs need to consider if the services fall into the following categories (schedule 3A.1, 2,3) :- Currently commissioned
Services currently commissioned that are necessary to meet a current need
Services that are currently commissioned which are relevant but do not constitute “necessary services”.
Future services/future commissioning
Services not currently commissioned that will be necessary in specified future circumstance
Services not currently commissioned that would secure improvements or better access to pharmaceutical services.
In NHS Wandsworth the following services have been commissioned:-
EN1 Supervised Administration EN2 Needle & Syringe Exchange EN3 Palliative Care EN4 Stop Smoking EN5 Care Home EN6 Medicines Assessment & Compliance Support
EN8 Minor Ailment Service EN9 Out of Hours (Access to Medicines) EN11 EHC via PGD EN14 Chlamydia Screening Pharmacy Obesity Service Pharmacy Asthma service Pharmacy Medicines Management Service through LPS
The following services are being revised and planned:-
Integrated Sexual Health Service linking EHC with chlamydia screening and testing
Cancer Screening Service
Hepatitis Screening Service
Revision of Care Home Service
Medicines Management

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
39
NHS Healthchecks
Vaccinations capacity through Community Pharmacy. The commissioning pharmacy contractor eligibility and patient eligibility for NHS commissioned pharmacy services are shown below. Table 5a: Breakdown of community pharmacy services by pharmacy and patient eligibility
NHS Pharmacy Service
Pharmacy Eligibility Patient Eligibility Cross-Border Commissioning Implication
Must be compliant with Essential services in WPCT or host PCT if a non WPCT pharmacy.
EN1 Supervised Administration
WPCT Pharmacies WPCT registered patients attending WPCT drug treatment agencies
Y
EN2 Needle & Syringe Exchange
WPCT Pharmacies Public health service offered to all patients
N
EN3 Palliative Care
WPCT Pharmacies & non-WPCT pharmacies serving a WPCT registered patient population
Public health service offered to all patients with a valid FP10
Y
EN4 Stop Smoking
WPCT Pharmacies & Non WPCT pharmacies serving a WPCT registered patient population
WPCT registered patients and patients who receive a service within Wandsworth
Y
EN5 Care Home WPCT Pharmacies & non-WPCT pharmacies serving a WPCT registered population
WPCT registered patients in a registered Wandsworth Care Home or Nursing home
Y
EN6 Medicines Assessment & Compliance Support
WPCT Pharmacies & non-WPCT pharmacies serving a WPCT registered population
WPCT registered patients living independently in their own home
Y
EN7 Medication Review (Full Clinical Review)
Not Commissioned yet WPCT registered patients ?
EN8 Minor Ailment Service
WPCT pharmacies & non-WPCT pharmacies serving a WPCT registered population
WPCT registered patients and patients resident in Wandsworth
Y
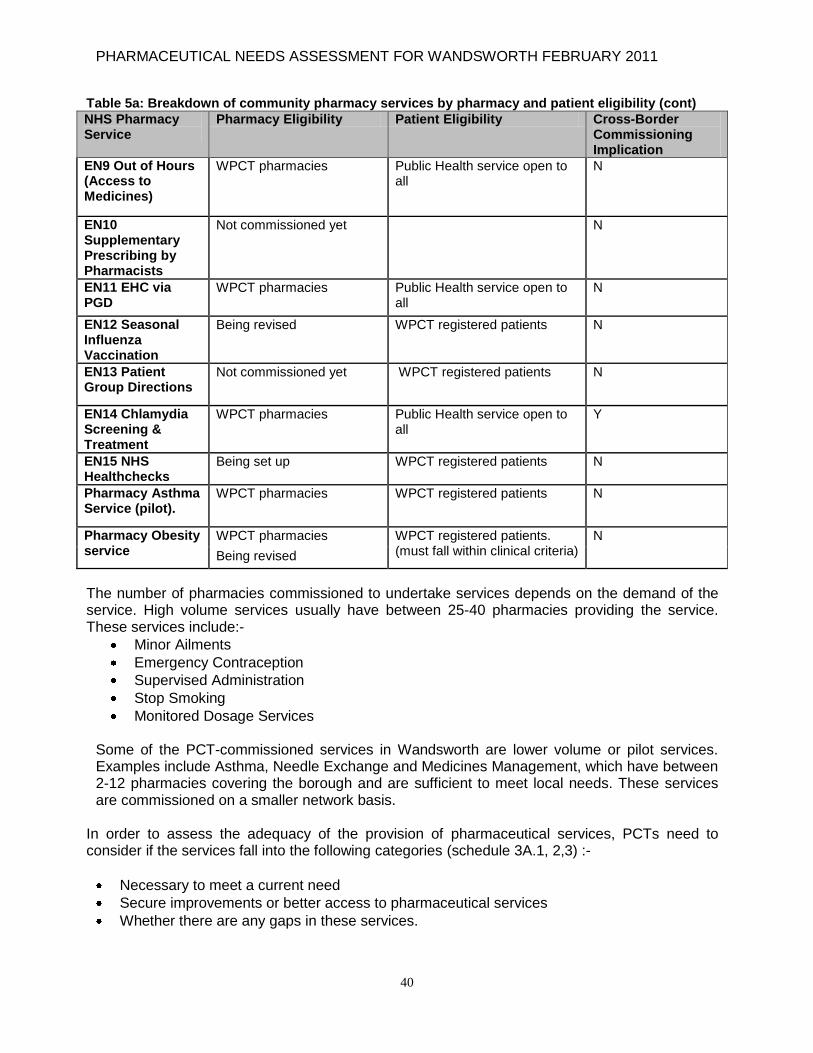
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
40
Table 5a: Breakdown of community pharmacy services by pharmacy and patient eligibility (cont)
NHS Pharmacy Service
Pharmacy Eligibility Patient Eligibility Cross-Border Commissioning Implication
EN9 Out of Hours (Access to Medicines)
WPCT pharmacies Public Health service open to all
N
EN10 Supplementary Prescribing by Pharmacists
Not commissioned yet N
EN11 EHC via PGD
WPCT pharmacies Public Health service open to all
N
EN12 Seasonal Influenza Vaccination
Being revised WPCT registered patients N
EN13 Patient Group Directions
Not commissioned yet WPCT registered patients N
EN14 Chlamydia Screening & Treatment
WPCT pharmacies Public Health service open to all
Y
EN15 NHS Healthchecks
Being set up WPCT registered patients N
Pharmacy Asthma Service (pilot).
WPCT pharmacies WPCT registered patients N
Pharmacy Obesity service
WPCT pharmacies WPCT registered patients. (must fall within clinical criteria)
N
Being revised
The number of pharmacies commissioned to undertake services depends on the demand of the service. High volume services usually have between 25-40 pharmacies providing the service. These services include:-
Minor Ailments
Emergency Contraception
Supervised Administration
Stop Smoking
Monitored Dosage Services
Some of the PCT-commissioned services in Wandsworth are lower volume or pilot services. Examples include Asthma, Needle Exchange and Medicines Management, which have between 2-12 pharmacies covering the borough and are sufficient to meet local needs. These services are commissioned on a smaller network basis.
In order to assess the adequacy of the provision of pharmaceutical services, PCTs need to consider if the services fall into the following categories (schedule 3A.1, 2,3) :-
Necessary to meet a current need
Secure improvements or better access to pharmaceutical services
Whether there are any gaps in these services.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
41
The services are stratified as follows – see Table 5b below. Table 5b: Services by adequacy, necessary provision, current provision
Service Assessment of Services
Essential Services Community Pharmacy & DACs
All the services as laid out in the essential part of the Community Pharmacy Contractual Framework are considered to be a necessary service to meet the current needs. With future changes in populations or in the local health economy a future update will be required. It should be noted that NHS Wandsworth community pharmacies and pharmacies bordering Wandsworth serve the Wandsworth population.
Advanced Services – Community Pharmacy & DACs
Medicine Use Reviews Appliance User Reviews/Stoma Customisation
These services are considered a necessary service to meet the current needs
Locally Enhanced Commissioned Services – Currently Commissioned
EN1 Supervised Administration
These services are considered a necessary service to meet the current needs across Wandsworth for WPCT registered patients
EN2 Needle & Syringe Exchange
These services are considered a necessary service to meet the current needs
EN3 Palliative Care
These services are considered a necessary service to meet the current needs
EN4 Stop Smoking
These services are considered a necessary service to meet the current needs
EN8 Minor Ailment Service
The Minor Ailments service is a necessary service to meet current need for NHS Wandsworth registered patients and patients resident in Wandsworth
EN9 Out of Hours (Rota Service Access to Medicines)
These services are considered a necessary service to meet the current needs.
EN11 EHC via PGD These services are considered a necessary service to meet the current needs
EN14 Chlamydia Screening & Treatment
The Chlamydia Screening service is considered relevant but it does not constitute a necessary service
EN15 NHS Healthchecks The Chlamydia Screening service is considered relevant but it does not constitute a necessary service
Pharmacy Asthma Service (targeted MURS)
This service is running on a pilot and is to be evaluated but the PCT believes this service is a necessary service

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
42
Services not yet Commissioned/to be Commissioned
EN5 Care Home
This service is currently being revised but would be deemed to be necessary
EN6 Medicines Assessment & Compliance Support
Services not currently commissioned that will be necessary
EN7 Medication Review (Full Clinical Review)
Services not currently commissioned that will be necessary in specified future circumstance
EN10 Supplementary Prescribing by Pharmacists
Services not currently commissioned that will be necessary in specified future circumstance
EN12 Seasonal Influenza Vaccination
Services not currently commissioned that will be necessary in specified future circumstance
EN13 Patient Group Directions These services are considered a necessary service to meet the current needs
Pharmacy Obesity Service
The PCT believes that this is a service that would secure improvements to pharmaceutical services
Pharmacy Medicines Management Service
The PCT believes that this is a service that would secure improvements to pharmaceutical services
Integrated Sexual Health Service linking EHC with Chlamydia Screening and Testing
The PCT believes that this is a service that would secure improvements to pharmaceutical services
Cancer Screening Service The PCT believes that this is a service that would secure improvements to pharmaceutical services
Medicines Management These services are considered a necessary service to meet the current needs
Hepatitis C Screening These services are considered a necessary service to meet the current needs
Targeted MURs MURS focused on long-term conditions and with locally agreed outcomes. However, given the intention to manage most long-term conditions through the care packages, the use of targeted MURs is considered to be necessary in the future to support these care packages.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
43
Cross-Border Commissioning In the recent DH Pharmaceutical Needs Assessment guidance on cross-border commissioning, it was noted:-
Cross Border Commissioning –Draft Guidance Draft Regulations to the Health Act 2009 – Pharmaceutical Needs Assessment 20. Community pharmacies deal with populations not just registered patients and therefore a pharmacy close to a PCT boundary may be serving patients from its own and its neighbouring PCT(s). PCTs will need to review their needs and PNAs to explore populations across boundary areas so there is common agreement around cross commissioning of services to meet population need. 21. In this regard, PCTs may wish to look to see how they handle cross border commissioning of services for patients registered with a GP practice that is in contract with the PCT, but the patient lives outside the PCT’s area (see reference 20).
NHS Wandsworth will commission from pharmacies outside Wandsworth subject to the above service criteria.
The service is appropriate for cross-border commissioning as identified in the above table 5a.
The service will be linked to patients registered with an NHS Wandsworth GP
The pharmacy is compliant with essential services with their host PCT
NHS Wandsworth registered patients are being served by that pharmacy outside Wandsworth and can demonstrate a significant volume
Subject to the appropriateness of the type of pharmacy service as listed in table 5a. Nearly all community pharmacies expressed interest in being commissioned to provide locally enhanced services. Currently all pharmacy services are paper-based. The PCT is now setting up an automation of pharmacy services. This will support faster and accurate data collection and invoicing. 4.11 NHS Wandsworth Community Pharmacy Resources The next section looks at the current resources available in Wandsworth community pharmacies through staffing and skill mix, IT, medical equipment and languages spoken. 4.11a Community Pharmacy Staffing Mix The graph below shows the breakdown of staffing in all pharmacies in Wandsworth (Baseline data July 2010). This gives an indication of the range of skill mix that is available through Community Pharmacy. Collectively, all community pharmacies in Wandsworth are employing up to 100 pharmacists and over 200 support staff which include technicians and front line pharmacy staff. Pharmacy

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
44
services need to take into account skill mix and the role that pharmacy technicians and front line staff could play in services.
Fig 12: Community Pharmacy staffing analysis July 2010
4.11b Premises, IT and Medical Equipment Audit A scoping study in July 2010, Pharmacy Scoping for Premises and Equipment, showed the following information: Table 6: Premises analysis
Questions Yes No
No Response
Planned for 2010 onwards
There is a separate room within the pharmacy for consultations with patients and customers
61 0 0 2
The consultation area/room is clearly signposted as a private consultation area within the pharmacy
57 2 3 1
Facilities in the consultation area
Yes No Nearby No Response
Sink 39 19 4 1
Computer access 39 18 5 1
Toilet 6 50 6 1
61 pharmacies have consulting rooms, out of which 26 pharmacies have hand-washing facilities in their consulting rooms
Two pharmacies are undergoing a refit for consulting rooms
Five Pharmacies are co-located within a GP practice. Since the pharmacy contract started in April 2005, over 30 pharmacies now have a built-in consulting room in their premises. This change has been due to the Contractual Framework.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
45
Fig 13: Number of consulting rooms in Wandsworth
IT Nearly all community pharmacies in Wandsworth are care compliant with Release 1 and all pharmacies have a dedicated Patient Medication Record system (PMR). Current funding requirements only allow for one IT system and broadband connections. All pharmacies have a mixture of corporate or personal emails.
13 pharmacies have additional IT i.e. additional laptop or computer in their consulting rooms.
Medical Equipment Audit Based on the July 2010 audit pharmacies had the following equipment:-
53 pharmacies have blood pressure machines
10 pharmacies have a cholesterol machine of varying manufacturers
49 pharmacies have weighing scales of various types
Over 49 pharmacies have carbon monoxide meters as they provide stop smoking services. Fig 14: Different equipment for services
The PCT Primary Care Estate Strategy should take into account the premises capacity offered through Community Pharmacy. This will support guidance for pharmacy contractors about development of premises and opportunities for investment. The Commissioners Investment Asset Management Strategy (CIAMS) methodology would be a suitable next step to review community pharmacy premises to meet future requirements for patient care. Across the whole borough nearly all pharmacies have consulting rooms and access to medical equipment.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
46
4.11.1 Summary In comparison to the GMS, contract Community Pharmacy does not receive similar levels of funding and there are no prescribed standards for premises, IT or medical equipment. For example, the Community Pharmacy Contractual Framework does not specify infection control standards in pharmacy premises and IT funding only allows for one computer per pharmacy. The Pharmacy White Paper (2008) has now recognised the importance of pharmacy premises and IT to deliver world class pharmacy services (see Appendix 5). Community Pharmacy can potentially hold or collect valuable health data to support better patient care. The PCT is now currently working with its Community Pharmacy contractors to set up NHS net email and automate pharmacy services. Some PCTs in London already have automated services which support faster data analysis and billing. 4.12 Acute and Specialist Pharmacy Providers in Wandsworth In Wandsworth there are other pharmacy providers as listed below:-
St George‟s Hospital Pharmacy Department providing pharmacy services in the acute sector
Queen Mary‟s Hospital Community Pharmacy service – provided under a service level agreement from Kingston Hospital
South West London & St George‟s Mental Health Trust, providing a specialist pharmacy service to patients with mental health needs at the Springfield site in Tooting and QMH in Roehampton (and other sites in the boroughs of Richmond, Kingston, Sutton & Merton)
Wandsworth Prison Pharmacy service. This is currently provided by Community Services Wandsworth as part of the wider contract for healthcare services at the prison. This service does not fall under the consideration of this report. There is no definitive timeframe agreed yet, but there will be a retender for the provision of healthcare services at HMP Wandsworth, including pharmacy, at some point in the future but not during 2010-11. The PCT would consider partnership bids from independent healthcare providers including independent pharmacy organisations as part of a consortium approach to delivery.
Pharmacist Nightingale Nursing Hospice – Part-funded PCT post for a pharmacist attached to Nightingale Hospice Nursing Home to support patient medication management
• Palliative Care – Trinity Hospice is located just outside Wandsworth but links to Wandsworth. The pharmacy service is under SLA from the Guys and St Thomas pharmacy team.
PNA Commissioning Intentions – Community pharmacies are a source of health data which needs to be integrated into local public health systems. The PCT will be automating pharmacy services. Pharmacy consulting rooms could provide the PCT with increased service capacity through use of premises and consulting rooms. There are opportunities to locate outreach services particularly in areas where communities are hard to reach. This information will be of key planning importance for polysystems as Community Pharmacy can provide additional primary care access and resources through skill mix, consulting rooms and medical equipment. CIAMS methodology should also be used to review pharmacy premises to support access to services.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
47
Figure 15: Acute pharmacies across SW London
Richmond
Kingston
Sutton &Merton
Croydon
Wandsworth
1
SW LONDONAcute & Specialist Pharmacy teams
Hospital
St Helier Hospital
Kingston Hospital
Mayday Hospital
St George'sSW London Metropolitan
Key
Specialist centre
SWL & St George's Mental Health Trust
Royal Marsden
CROYDON LPC
MSW LPC
K&R LPC
Queen Mary’s Hospital
Community Pharmacy Contractors
The above mapping shows the distribution of acute pharmacies against the six SW London boroughs. While the PNA will consider Community Pharmacy in terms of Control of Entry and future Market Entry, the Pharmaceutical Commission Strategy takes into consideration that acute pharmacy providers can provide services and specialist pharmaceutical expertise to patients and even practitioners such as general practitioners, nurses and community pharmacists. It is important that key PCT workstreams such as long-term conditions, virtual wards and polysystems, recognise there are other pharmacy providers within Wandsworth with specialist skills. There are examples where pharmacists from various sectors of pharmacy have collaborated:-
The community pharmacy palliative care services work closely with the specialist palliative care pharmacists from Guys and St Thomas‟s hospital to share specialist knowledge and skills to the community pharmacy palliative care network
St George‟s Hospital pharmacy team, NHS Wandsworth and Merton, Sutton & Wandsworth Local Pharmaceutical Committee have worked with local Wandsworth pharmacies to improve discharge of medicines from secondary care back to primary care, reciprocal exchange of pre-registration pharmacists.
The pharmacy asthma service involved the contribution of a member of the PCT prescribing team to update local participating community pharmacists on prescribing policies.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
48
PNA Commissioning Intentions – Further work is required to develop the links between these various pharmacy groups. The key area for joint working would be around:-
Safe administration of medicines
Discharge of medication
Commissioning of specialist pharmacy roles e.g. mental health, long-term conditions, review of specials formulations, care home advice
Pre-registration exchange. The roles of the different pharmaceutical providers should be reflected in polysystem development as specialist clinical skills could be commissioned in Primary Care. It is important that there is representation from and communication with other pharmaceutical providers in Wandsworth as part of polysystem and care plan commissioning. .

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
49
5 CONSULTATION, PATIENT VIEW AND EXPERIENCE
Under PNA regulations ( see reference 30, regulation 3F Consultation) and as part of the PNA, PCTs need to consult key stakeholders, including patient and public groups (service users) to ascertain their views on pharmacy services to ensure they are being developed and improved to support patient care. For NHS Wandsworth this process has been done by several methods. (See Appendixes 6 and 7.) 5.1 Street Interviews The views of the residents across Wandsworth were sought through a patient survey. 237 interviews were carried out and were conducted with members of the public across five areas in Wandsworth: Clapham Junction Putney Roehampton Tooting Wandsworth Town The research was to assess patient satisfaction with local pharmacies in Wandsworth. All respondents were screened to ensure that they had recently visited a Wandsworth pharmacy and had some interaction with the pharmacist. The demographic breakdown of the sample size was as follows:- 57% was female and 43% was male 90% lived in Wandsworth and 10% lived outside the borough 69% of the respondents were white, 16% were black/black British, 6% Asian British, 4%
were of mixed ethnicity and 1% Chinese/other The majority of respondents are generally in good health (84%), only 3% claiming to be of
poor health and 13% of fair health. The age breakdown of the sample size is shown below. Fig 16: Breakdown of sample size

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
50
5.1a Street Interviews Summary Findings Pharmacy usage
Older respondents (64% 65+ yrs) are like50ly to visit the pharmacy more frequently than younger respondents (20% 16-24yrs)
77% are more likely to use the same pharmacy, primarily for its location but also where respondents have an established relationship with the staff.
Fig 17: Same pharmacy usage
Over 90% of respondents visit the pharmacy for themselves. Those aged 25-44 years
are more likely than other age groups to visit the pharmacy for their children (44% cf. 20% overall). Over four-fifths walk to the pharmacy, very few will drive (6%). See figure 18 below. Fig 18: Pharmacy usage

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
51
Pharmacy Services
Unprompted, over two-fifths (41%) mentioned that pharmacies can be used to get advice or treatment without a prescription, and nearly a quarter (24%) were aware of stopping smoking clinics. However, almost a third (31%) could not specify any other services on offer at their pharmacy
Once prompted awareness of all services increased, however a fifth of those surveyed were still unaware of the listed services – see figure 19 below
Over a quarter of respondents sought advice or treatment from a pharmacist regarding a minor ailment or condition. 10% have used the collection and delivery service. Fig 19: Usage of pharmacy services
Overall, respondents are generally satisfied with the services used at a Wandsworth pharmacy.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
52
Fig 20: Satisfaction of pharmacy services
Over three-quarters (78%) of respondents would be either very or fairly likely to seek advice regarding a minor ailment from a pharmacist; this figure rises slightly amongst the 45-64 year old group
Ultimately, respondents feel it is very important that the pharmacy has their medicines in stock; the staff are friendly, helpful and offer a quick service. Over half (51%) feel that it is very important that they can usually see the same pharmacist. See figure 21 below. Fig 21: Satisfaction ratings
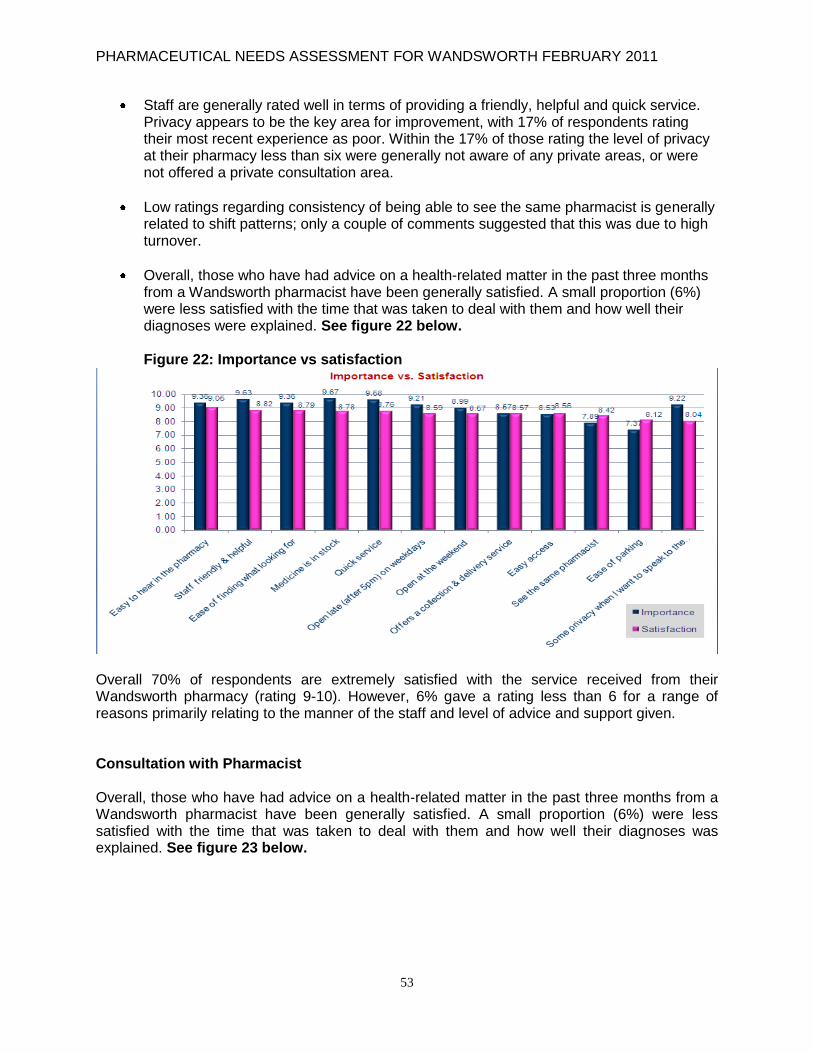
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
53
Staff are generally rated well in terms of providing a friendly, helpful and quick service. Privacy appears to be the key area for improvement, with 17% of respondents rating their most recent experience as poor. Within the 17% of those rating the level of privacy at their pharmacy less than six were generally not aware of any private areas, or were not offered a private consultation area.
Low ratings regarding consistency of being able to see the same pharmacist is generally related to shift patterns; only a couple of comments suggested that this was due to high turnover.
Overall, those who have had advice on a health-related matter in the past three months from a Wandsworth pharmacist have been generally satisfied. A small proportion (6%) were less satisfied with the time that was taken to deal with them and how well their diagnoses were explained. See figure 22 below. Figure 22: Importance vs satisfaction
Overall 70% of respondents are extremely satisfied with the service received from their Wandsworth pharmacy (rating 9-10). However, 6% gave a rating less than 6 for a range of reasons primarily relating to the manner of the staff and level of advice and support given. Consultation with Pharmacist Overall, those who have had advice on a health-related matter in the past three months from a Wandsworth pharmacist have been generally satisfied. A small proportion (6%) were less satisfied with the time that was taken to deal with them and how well their diagnoses was explained. See figure 23 below.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
54
Fig 23: Satisfaction of pharmacists
Two-thirds of those who have recently had a consultation with a pharmacist were not offered the option of having the discussion in a private area. 9% of respondents felt that the level of privacy was worse than expected – none were offered a private area for the consultation. Fig 24: Private consultation areas
Evidence from baseline assessment shows that the majority of pharmacies have built consulting rooms, yet pharmacists need to offer private consultations to patients.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
55
Key messages from the street surveys Satisfaction
The majority of patients appear to be satisfied with the level of service received from their Wandsworth pharmacy, with 70% saying they are extremely satisfied (rating 9-10) and a further 24% satisfied.
Comments suggest that high satisfaction is generally a result of a prompt, friendly and helpful service.
Conversely, those less satisfied (rating 6 or less) tend to have had experiences of unhelpful staff, poor advice or long waiting times.
Ratings highlight that stock levels and a prompt, friendly and helpful service are important to patients and that these are areas where there is potentially some room for improvement.
Patients appear to be less concerned with being able to see the same pharmacist or parking (as the vast majority walk to their pharmacy).
The widest gap between importance and satisfaction ratings is in relation to being able to
have some privacy when consulting with a pharmacist. Pharmacy Services
Overall, awareness of pharmacy services, both unprompted and prompted, is relatively low.
Once prompted over a third of patients confirmed that they were aware they could:
seek advice or treatment from a pharmacist
access a stop smoking clinic through their pharmacy
access a collection and delivery service
Even when prompted, very few were aware that they could access the following services at pharmacies in Wandsworth:
Out of hours medicine dispensing services (13%)
Advice on losing weight (22%)
Diabetes testing (22%) Consultation with pharmacist
Those who have had a consultation with a pharmacist appear to have generally been satisfied with the service.
There are only a small number of cases where the patient has felt rushed or that the wrong advice was given, which in one case could have had a very serious outcome.
Over two-thirds of patients were not offered a private consultation room to hold their discussion in private.
The vast majority (91%) of those who did use a private consultation room felt that the level of privacy was either as expected or better.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
56
5.2 Patient Group Feedback Joint Commissioning Group –Drug and Alcohol Misuse feedback: It is important that services for drug misusers should:-
Be non-judgmental
Not discriminate against drug misusers, but should treat this client group equitably.
Wandsworth LInk - The Wandsworth LInk recommended that future patient feedback should link into the primary care subgroup. There should be a better exploration of pharmacy opening hours in wards where there is poor access to health services. 5.3 Overall Conclusions The patient or customer service experience is fundamental to any service. The public in Wandsworth are generally satisfied with pharmacy services and there are opportunities to develop service skills, making better use of consultation rooms so the public can have private consultations and ensure that advice around minor conditions are robust and evidenced-based. The PNA strongly recommends pharmacy engagement and representation at patient groups such as the LINk, Drug Misuse Forum, Young Person‟s Forum and patient locality groups. This will support development and ensure continual improvement of pharmacy services that meet local need through patient feedback, and build relationships with the public.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
57
6. PUBLIC HEALTH IN WANDSWORTH This section looks at the population profile for Wandsworth. Under regulation 3G(1)(b) PCTs should take into account and reflect in their PNAs the needs of different patient groups. These attributes are age, disability, gender (including gender reassignment), race, religion or belief and sexual orientation. This section looks at this on a borough perspective. Public Health data is taken from the Joint Strategic Needs Assessment 2011 (see Appendix 4 and reference 9), Picture of Health 2009 (see reference 8), December 2009 Public Heath report (see reference 6), Wandsworth Council Profile August 2010 (www.londoncouncils.gov.uk), and the Greater London Authority Population Projection 2007. This section looks at the whole population, key areas of health, and makes strategic commissioning recommendations on pharmacy services. 6.1 Population in Wandsworth
The population of Wandsworth is estimated to be 284,000 (Wandsworth council profile) and has a unique age structure. The number of people that are registered with a Wandsworth GP is higher, at approximately 363,000. The population of Wandsworth is estimated to have stabilised between 2007 and 2009 with an increase of just 736 people (0.3%). (See Appendix 3) Table 7: Population of Wandsworth
Population of Wandsworth
Total 284,000
Under 16 45,200
Over pensionable age 31,500
Unemployment
Total unemployed benefit claimants 3.1%
It should be noted that the Office for National Statistics (ONS) estimates, and the GLA estimates are calculated differently - the ONS estimates are based on GP registrations, which in London can suppress population levels as they do not take into account highly mobile populations.
Wandsworth has a relatively young population profile reflecting both a transient renting population and a more established population of young families. The population of Wandsworth over pensionable age form only 12.6% of the local population, compared to 15.5% of London as a whole, and 21.1% nationally. Wandsworth has a different profile to many of its neighbours since 57% of the population are aged between 25 and 54. A large proportion of this population will also be working and may work and use services outside of the borough.
Seven out of the twenty wards in Wandsworth saw a decrease in their population between 2007 and 2009. The biggest decrease was seen in Roehampton ward, where the population is estimated to have decreased by 11%. The largest population increase was seen in Queenstown ward, where the population is estimated to have increased by 8%.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
58
Wandsworth has a much smaller proportion of older people and children compared to the UK. Wandsworth has a much larger proportion of residents in the 20-44 year age group compared to neighbouring boroughs. At a national level there are now more people aged 60 and over than there are under 16. The London picture differs, with still more people under 16 than aged 60 and over and Wandsworth also follows this pattern – 18% of the Wandsworth population are under 16 years and 12% are aged 60 and over.
The number of people aged over 60 in Wandsworth has reduced between 1991 and 2007 from around 45,000 to 34,000, a decrease of 24%. The population of those aged 85 and over has remained relatively stable and is expected to do so for the near future. Population projections suggest that between 2007 and 2013 there will be no overall increase in the number of residents aged 60 to 74. A significant reduction of 7% is expected in those aged 75 years and above.
The wards with the largest older population across all age bands are Roehampton and West Putney. Nightingale House Care Home may account for the high number of those aged over 85 in Nightingale ward. There are 3,566 people over the age of 65 living in Wandsworth who are receiving care as part of a community care package from the council.
Age structure
Wandsworth is the most populous Inner London borough and around 132,000 dwellings are home to a population of over 280,000 residents. The age structure of residents is skewed and differs significantly from both the national and the Greater London average. The 20-39 year old age group represents 48% of the population (see figure 25) compared to 27% nationally and 36% in Greater London.
Figure 25: Wandsworth age-sex pyramid
3.42
2.26
1.83
1.87
4.16
7.65
7.83
5.01
3.70
2.75
2.08
1.94
1.69
1.30
1.16
0.99
0.92
0.14
0.32
0.56
0.81
1.06
1.09
1.41
1.62
1.94
2.57
3.91
5.64
8.49
6.20
3.17
1.80
1.76
2.29
3.56
0.35
0.67
10 8 6 4 2 0 2 4 6 8 10
0-4
5-9
10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85-89
90+
Age G
roups
Percent
Males(%) Females(%)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
59
6.2 Population Change The population of Wandsworth was estimated to have stabilised between 2007 and 2009 with an increase of just 736 people (0.3%). Seven out of the twenty wards in Wandsworth saw a decrease in their population between 2007 and 2009. The biggest decrease was seen in Roehampton ward, where the population is estimated to have decreased by 11%. The largest population increase was seen in Queenstown ward, where the population is estimated to have increased by 8%. The population of the borough is set to increase to over 330,000 by 2030. Population change in the borough is a product of both natural change in the population and net migration. Natural change is the difference between the number of births and deaths in a given year, whilst net migration refers to the difference between people moving into and out of the borough. Natural change in the population is expected to increase, with an overall increase in the number of births, combined with a falling death rate. The largest increase in population by 2030 is projected in the 45-49, 50-54 and 55-59 year old age groups. This is likely to be reflective of the „ageing on‟ process in projection methodology. However, in practice Wandsworth is a borough which experiences high levels of population turnover year on year, and the movement of young adults into the borough is expected to continue. Although actual numbers remain small, the number of people aged 90 or over is projected to increase significantly by 2030, particularly for males. Significant increases in the number of children in the borough are also projected, reflecting the continuing upward trend in the number of births. In 2009 there were 5,335 live births, an increase of 31% since 2002 and the highest level for at least 20 years. Projection methodology „ages on‟ these births to increase the number of children in age groups 5-9, 10-14 and 15-19 by 2030.
6.3 Population Density Wards to the east and west of Wandsworth have a much lower population density compared to the rest of Wandsworth. Queenstown and Roehampton are the wards with lowest population density and with lowest service provision; however, residents in those wards are still making good use of services. Figure 26: Wandsworth community pharmacies mapped against population density

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
60
There is a good distribution of pharmacies within areas of high population density. At present there are enough community pharmacies to meet the needs of the population of NHS Wandsworth. Population growth is not anticipated to rise significantly over the next five years. Community pharmacies have adjusted their opening hours to meet need. 6.4 Ethnic Breakdown of Wandsworth
Table 8: Population of Wandsworth ethnicity breakdown
Ethnicity Breakdown of Wandsworth
White
White British 168,665 64.8%
White Irish 8,151 3.1%
White other 26,162 10.1%
Mixed
White & Black Caribbean 2,893 1.1%
White & Black African 1,252 0.5%
White & Asian 2,247 0.9%
Mixed other 2,336 0.9%
Asian or Asian British
Indian 7,412 2.9%
Pakistani 5,449 2.1%
Bangladeshi 1,099 0.4%
Other Asian 4,084 1.6%
Black or Black British
Caribbean 12,665 4.9%
African 10,013 3.9%
Black other 2,388 0.9%
Chinese or other
Chinese 2,227 0.9%
Other ethnic group 3,337 1.3%
The ethnic mix of the population of England has changed over the last 10 years and continues to do so. The population estimates by ethnicity of the residents living in London may reflect these overall changes. Wandsworth is home to a diverse range of communities and 20% of the borough‟s population is non-white, compared with 31% in Greater London and 12% nationally. In 2007, Wandsworth had the 27th largest non-white population of the 33 London boroughs.
Wandsworth, at 66.5%, has a greater proportion of White British residents. Ethnic differences in health vary across age groups, between men and women, as well as between geographic areas. Ethnic differences in health may vary between generations. In some Black and Minority Ethic (BME) groups, rates of ill-health are worse among those born in the UK than in first generation migrants. Although the overall non-white population in the borough has changed little since 2001, there has been a significant percentage increase in the number of residents of Asian or Asian British ethnicity, particularly Bangladeshi, with an estimated increase in population size of 92% to 2,300 from 2001 to 2007. In contrast, a decrease of more than 20%

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
61
has been observed in residents from Black or Black British Caribbean (-2,900), African (-2,100) and White Irish (-1,800) ethnic groups.
The ethnic distribution of Wandsworth‟s population is not predicted to change significantly over the next 10 years
The population aged 65+ who are of „Other‟ ethnic origin are predicted to increase by the largest percentage (48%)
The „White‟ population is approximately 78% and „Non-white‟ accounts for 22% (10% Black, 8% Asian, 4% Other)
Wandsworth has a more diverse community than SW London generally, but is similar to NHS Wandsworth‟s ONS peer group ethnic profile
Ethnic breakdowns by ward show a high Black Caribbean population in Latchmere (24%) and a high Asian population in Tooting (22%).
Fig 27: Percentage of “Non White” population by Wandsworth wards, 2001 (NHS Wandsworth Public Health report Nov 2009)
Mortality from coronary heart disease (CHD) is 46% higher for men and 51% higher for women of South Asian origin than in the non-Asian population in the UK.
The occurrence of diabetes is twice as frequent, and the occurrence of chronic kidney disease is six times higher in South Asian populations than the rest of the UK population (Bhopal et al, 1999).
People of African descent are more likely to have hypertension than the white population in the UK, and stroke is 2.2 times more common in people of African or Caribbean origin. Stroke is also thought to be more common in certain South Asian groups.
Alongside the direct increase in prevalence of the diseases, the prevalence of other risk factors varies between ethnic groups e.g. a disproportionately high number of Bangladeshi, Irish and Pakistani men smoke compared to the general population.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
62
Fig 28: Estimated hypertension and CHD growth by ethnic group NHS Wandsworth Public Health report Nov 2009
Fig 29: Estimated hypertension and CHD growth by ethnic group NHS Wandsworth Public Health report Nov 2009
Figures 28 and 29 demonstrate the importance of focusing on CHD prevention in the groups. This demonstrates how the estimated prevalence of both hypertension and CHD is predicted to change in Wandsworth ethnic groups up to 2020.
In comparison the majority of the community pharmacists reflect the diverse culture of Wandsworth residents. In a recent mapping exercise community pharmacists were asked what languages their staff and themselves spoke. The four major languages spoken in Wandsworth are Guajarati, Hindi, Urdu, and Punjabi. Most other language groups are represented. The survey factored in the whole pharmacy team, which are front line pharmacy support staff and pharmacy technicians(see fig 30) .
This language diversity in Pharmacies offers Wandsworth Council, Public health and the various health and social care agencies a valuable resource to support local communities.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
63
Fig 30: Languages spoken in Wandsworth pharmacies
PNA Commissioning Intentions – The Community Pharmacy Contractual Framework offers opportunities for signposting and self-care. The multilingual capabilities of the community pharmacy network could be enhanced to help develop bridges with local communities groups by providing more self-care, managing medicines and signposting for health and social care. Front line staff could provide a health trainer role, and support PCT health trainers with more focused health promotion and signposting. Community pharmacies should be able to access the multilingual translation support offered by the NHS to support patients. Community pharmacies need to link up with key community groups to explore their services and the needs of patients. Support should be tailored for various communities around improved use of medicines, signposting to health and social care services, and making use of pharmacy premises for community outreach support. CHD prevention in Wandsworth ethnic communities is a key priority and Community Pharmacy can support communities through understanding medication and improving compliance. NHS health checks and screening services around long-term conditions would assist in providing access for communities in hard-to-reach areas. Community Pharmacy has a role to play as a gatekeeper of local knowledge and this needs to be developed further with Public Health and Wandsworth Borough Council.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
64
6.5 Socio-Economic Indicators Unemployment – This is variable across the borough. Queenstown and Latchmere have the highest rates (over 5%) and Northcote the lowest (3.01%). The elders – Wandsworth has a smaller proportion of people over 60 years of age (13.8%) than the average for England and Wales (20.9%), but a slightly larger proportion than the average for London (12.4%). There is almost a twofold variation in the percentage of older people between wards in Wandsworth, from 10.44% in Northcote to 19.98% in West Putney. 11% of households in Wandsworth are of pensioners living alone. Single parents with children in Wandsworth – The percentage of children from single parent households is 30% (compared with 28.9% in London and 22.9% in England). There is a wide variation between the wards (e.g. 13.7% of households with dependent children are lone parent households in Thamesfield, compared to 47.5% in Latchmere). Research evidence shows that these children are more likely to be disadvantaged in relation to income, housing, nutrition, growth and educational achievement. These factors have a direct impact, both short and long-term, on their health.
Migration and turnover - With a young and mobile population, Wandsworth experiences high levels of turnover compared with other local authorities. Between 2001 and 2008 Wandsworth had the 9th highest volume of migration per 1,000 population in England and Wales. The borough has high levels of both internal (UK) and international migration and overall migration in Wandsworth has gradually increased from 244 migrants per 1,000 population in mid-2001 to 259 by mid-2008. Net migration is outward and increasing, but not enough to lead to an overall decrease in population. The main mobility in the Wandsworth population is around the two age groups, 15-29, and 30-44. From a starting point of 2002-3 to 2007-8, the number of people within the 15-29 age group moving in has remained stable at 14,000, and the numbers moving out has declined by approximately 600 people to 10,000. This reflects the increase in the number of students moving in to find their first jobs. For the 30-44 age group, the numbers moving in have increased by approximately 1,500 people from 2002-3 to 2007-8, whilst the number moving out has also increased by approximately 800 people, to 12,000.
Household composition – The number of households in the borough is projected to increase by 12% over the 15 year period 2011 to 2026. One person households account for 38% of all households and the proportion is increasing. Other multi-person households (e.g. occupied by unrelated adults) account for 16% of households in the borough. The proportion of households which are couple households (married and cohabiting) is projected to decrease over the next 15 years, whilst the number and proportion of lone parent households is set to increase. On average, there are 2.2 people per household in Wandsworth and average household size is projected to decrease to 2.1 persons by 2026.
Deprivation – Overall, Wandsworth has a relatively prosperous community and compares very well with other Inner London boroughs in terms of poverty. However, the wards of Latchmere, Roehampton, Queenstown and Tooting all exhibit significant disadvantage across most, if not all, dimensions of deprivation. These are the borough‟s priority neighbourhoods and are subject to continued specific and targeted action to reduce these inequalities. The map below (figure

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
65
31) shows the distribution of community pharmacies in Wandsworth against an index of deprivation. Fig 31: Map of distribution of community pharmacies vs. deprivation
There are at least 17-20 Wandsworth community pharmacies located in the highest areas of deprivation
Out of this total there are four community pharmacies located in or near housing estates where they represent the only form of health and social care.
PNA Commissioning Intentions – Community pharmacies with a consulting room could be used as mini citizens‟ advice bureaus in vulnerable areas by providing advice and signposting to appropriate health and social care. There are several community pharmacies that provide a more accessible route to healthcare in areas of deprivation. These pharmacies should be reviewed in terms of how they could support the local communities further. The locally enhanced service route could offer the PCT and Wandsworth Council opportunities to develop local social care services that could benefit the community. There are opportunities to develop pharmacies in those wards with higher deprivation to support health and social care.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
66
7. HEALTH IN WANDSWORTH – PUBLIC HEALTH AND THE LOCAL BOROUGH This section of reports presents a summary of the Public Health and borough population needs. This is based on the Picture of Health 2009 and the December 2009 Public Heath report. This section looks at key health areas such as long-term conditions, stop smoking, sexual health and patient needs. The 2011 JSNA has summarised the health inequalities across the borough where this report will present the Community Pharmacy commissioning response to meet those needs. Within Wandsworth, the ward which is most frequently worst performing in health outcomes is Roehampton. Other wards have particular factors that may account for high ill health outcomes, such as the presence of a long stay hospital, nursing home, or a high proportion of ethnic groups. Deprivation is not the sole key to understanding the data. West Putney is more affluent than most other wards in Wandsworth, yet it has some of the worst health outcome indicators. The prevalence data may mislead as it will have different data quality standards applied by each GP practice for legitimate organizational reasons. However, it is interesting to note that of the four wards with the highest levels of prevalence for long-term conditions (Roehampton, West Putney, East Putney, and Nightingale), Roehampton is the only ward which is also in the four wards with the highest levels of all age all cause mortality. This could indicate that a higher level of prevalence in primary care generally benefits the older population. Life expectancy is the average number of years of life remaining at a given age. Life expectancy at birth is the average expected lifespan of an individual. By looking at life expectancy at different ages, we are able to exclude the effect of high death rates in a specific age group e.g. if we look at life expectancy at age five, we can exclude the effect of infant death rates. Life expectancy at birth in the UK has increased over the period of 1992 to 2006, rising from 73.4 to 77.3 years for males and from 78.9 years to 81.5 years for females. In 2006, the local area within the UK with the highest life expectancy for both males and females was Kensington and Chelsea. The local area with the lowest life expectancy in 2006 was Glasgow City. Females continue to live longer than males, but the gap has been closing. Although both sexes have shown annual improvements in life expectancy at birth, over the past 25 years the gap has narrowed from six years to 4.3 years. Life expectancy at age of 65 is the number of further years someone reaching 65 could expect to live. It is also higher for women than for men. Based on the death rates in 2005-2007, a man aged 65 years could expect to live another 17.2 years and a woman another 19.9 years. Another concept that arises from life expectancy is health expectancies. While life expectancy provides an estimate of average expected life-span, healthy life expectancy divides total life expectancy into years spent in “good” or “not good” health. Thus health expectancies represent the period of time an individual might expect to remain in good or fairly good health or free from a limiting chronic illness or disability if he or she experienced the particular age-specific rates for that time period throughout their life. Health expectancies are powerful indicators of the interactions between health and mortality and can be used to monitor the health of the population in relation to increased life expectances over time. Based on 2004–2006 rates, on average, males in the UK could expect to live in good or fairly good health for 68.2 years at birth and 12.8 years at age 65. For females these figures are 70.4 years and 14.5 years.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
67
7.1 Smoking Cessation
Smoking remains the greatest cause of preventable illness and premature death in the UK. It causes short and long-term health, social and financial problems manifested in high morbidity and mortality from cardiovascular disease (CVD) and cancers. Smoking imposes a significant economic burden on the NHS society. It is estimated that there are over 70,000 (31%) smokers in Wandsworth. This is higher than the national average which is estimated at 27%. NHS Wandsworth is committed to reducing the prevalence of smoking among routine and manual workers to 26% or less by 2010. In Wandsworth approximately 35% of deaths are thought to be attributed to people aged over 35 who smoke. This is above the national average. According to national data approximately 450 young people start smoking every day. Smoking Cessation is one of the PCT‟s key priorities and Community Pharmacy has played a role in this. Figure 32 shows how practice data has been used to understand small area variations in smoking status. Patient level data regarding smoking status has been taken from EMIS web and has been used to create a thematic map showing geographical patterns in smoking status.
Figure 32: Map showing location of "current smokers" by lower super output area
Percentage of 'Current smokers'LSOA based smokers and list size
21.8 to 29.6 (36)
18.7 to 21.8 (35)
15.5 to 18.7 (33)
12.6 to 15.5 (34)
4.3 to 12.6 (36)
Source: EMIS Web & NSTS 2009
These findings and recommendations are being used to further build upon the service redesign that has already taken place during 2008/9. It should be noted for the purposes of the PNA that while this data relates to prevalence in the GP registered population, community pharmacy stop smoking providers will see patients from anywhere. This is an area where community pharmacies have proven success. The following has been taken forward since 2005:-

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
68
Increased the number of smoking cessation counsellors in community pharmacies from 12 to over 30 from 2004 to 2009
Increased the number of front line pharmacy staff (i.e. pharmacy technicians, front line pharmacy counter staff)
Provision of Nicotine Replace Therapy through Community Pharmacy – therefore providing a one-stop service where stop smoking counselling and pharmacotherapy support for clients motivated to stop smoking. Introduction of a Patient Group Direction for the supply of Nicotine Replacement Therapy in 2006
Revised stop smoking LES integrating counselling and the PCT smoking cessation pharmacotherapy policy
Introduction of automation so consultations can be recorded electronically. The PCT is now extending this to pharmacotherapy supply.
The current distribution of Community Pharmacy smoking cessation providers is shown below mapped against COPD. Fig 33: Map of community pharmacy stop smoking providers vs COPD
There are over 30 pharmacies contracted to provide stop smoking, and there are no access issues to this service through Community Pharmacy.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
69
Fig 34: Stop Smoking Quits 2010-2011
The 2010-2011 stop smoking data (see figure 34 above) showed that Community Pharmacy contributed nearly 34% of the PCT‟s total Stop Smoking Quits. This is an important contribution to the PCT‟s efforts towards stop smoking. A review on the stop smoking service was carried out by the Department of Health Tobacco Control National Support Team (NST) in July 2010. The team produced a comprehensive report to propose improvements and recommendations. The extract from the report below relates to pharmacy:- • There is enthusiasm and leadership within the Local Pharmaceutical Committee to further
develop capacity for provision of stop smoking support within the community pharmacy workforce
• NHS Wandsworth develops a consistent data collection mechanism across all Stop Smoking
Community Providers (CP).[ Quit Manager –requirement for GP & Pharmacy LES ] This will require a decision be taken on the appropriateness of the use of the current electronic system for collection of data from community providers
• The development of tailored interventions for key target groups as set out in DH Service and
Monitoring Guidance 2010/11[ Set target for BME/Pregnant women/RMW- LES – GP & pharmacy ]
The NST endorses the intention to further develop capacity within existing pharmacy-based stop smoking provision by: • Expanding Level 2 training to include dispensing and counter staff • Working with high performing providers to act as exemplars of best practice with regards to
client engagement and quality interventions • Using the opportunity provided by the review of the pharmacy LES to engage community
pharmacies not currently providing stop smoking support and to set more robust performance indicators
• Developing a varenicline PGD for pharmacists to ensure that all providers (and clients) have more immediate access to varenicline via pharmacy

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
70
7.2 Disease States and Long-Term Conditions The role of pharmacy in long-term conditions has been highlighted over the years. The report from the Royal Pharmaceutical Society on pharmacy and long-term conditions (2006) and Chapter 4 of the Pharmacy White Paper (see reference 16 and 17) identified the role community pharmacists can provide in terms of providing specific support for people who are starting out on a new course of treatment for long-term conditions e.g. high blood pressure, high cholesterol and diabetes. NHS health checks have been highlighted as part of pharmacy‟s role in the White Paper. Community pharmacy has several strengths for delivery of long-term conditions (see reference 14 and 16):
Acceptable to patients – Most patients don‟t mind going to the pharmacy, because they don‟t need an appointment, and there is less „social distance‟ between the „customer‟ and the pharmacist than there is between the „patient‟ and other healthcare professionals. This provides an excellent opportunity for planned as well as opportunistic interventions
Well-located – They are accessible and widely located, including in disadvantaged communities
Increased coverage – Those patients who do not attend GP or nurse clinics still collect prescriptions from their pharmacy, including those whose condition is less well controlled or might become uncontrolled. In addition pharmacies offer services when local surgeries are closed, including Saturdays
Skilled and willing – Pharmacists already have great expertise in medicines management, and, in a recent survey, 65% expressed an interest in specialising in the management of long-term conditions
Cost-effective – Most of the costs of the community pharmacy network are already met via the NHS contractual frameworks, so additional services can usually be provided cost-effectively.
See reference 15
PNA Commissioning Intentions – There are currently just over 35 pharmacies providing smoking cessation and there is a potential to expand this network further by increasing the number of counsellors who are second pharmacists, dispensers and sales assistants. The role of community pharmacists could be expanded in new areas such as group counselling, funding for Sunday treatments and access to key employment groups in Wandsworth e.g. Wandsworth Borough Council employees, the fire brigade, St George‟s Hospital and NHS Wandsworth employees. Most pharmacy premises have consulting rooms and could accommodate stop smoking counsellors. This would make better use of the access pharmacies provide particularly in areas of deprivation or trying to target hard-to-reach communities. A model of collaborative provision could see a drop in stop smoking services being co-located in a pharmacy. Pharmacists could provide the pharmacotherapy support and take responsibility for managing medication. Updated pharmacotherapy training in line with NICE guidance for pharmacists and front line staff should be developed. The stop smoking pharmacy service through pharmacy should be fully automated to include pharmacotherapy.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
71
NHS Wandsworth is undergoing a review of the way that long-term conditions are reviewed and managed. The key breakdown of disease in Wandsworth can be seen below in figure 35.
Fig 35: Percentage of residents with limiting long-term (Source NHS Wandsworth Public Health report Nov
2009 Source: Census 2001
Nationally the NHS spends £8 billion a year on prescription drugs in Primary Care in England. Expenditure on primary care drugs has increased by 60% in real terms over the last decade and the number of items dispensed has increased by 55%. The continued development of new drugs for use in the NHS, identification of new applications for existing drugs and England‟s ageing population means that further growth can be expected (National Audit Office, 2007).
In NHS Wandsworth around £30 million is spent on drugs in Primary Care. Large areas of expenditure are associated with long-term conditions such as cardiovascular disease, mental illness, respiratory diseases and diabetes. Prescribing is the most common intervention in healthcare and has led to improvements in the diagnosis, treatment and follow-up of patients. It has also played an important role in reducing morbidity and increasing life expectancy. Figure 36 shows annual trends in dispensed prescriptions for respiratory, mental health (including depression and severe mental illness e.g. including schizophrenia) and diabetes. There does not appear to be a significant change in the number of prescriptions for respiratory diseases. These trends may be considered as a proxy for disease management and should be viewed with local prevalence data in these disease areas.
Fig 36: Annual trends in CVD prescriptions 2005–2009 and annual trend in dispensed prescriptions (respiratory, mental health and diabetes), 2005–2009
There has been a rise in activity in terms of prescribing and dispensing over the last four years. Community pharmacists handle the most amounts of medicines in the PCT through dispensing; they are also in a position to make interventions in terms of medicines management and lifestyle intervention.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
72
The PCT has set up a Long-Term Condition working group. The purpose of this group is to steer a number of work programmes around long-term conditions ensuring integration of health and social care for these patients. Several working subgroups have been formed:-
COPD / Asthma
Cardio Vascular Disease (inc. Heart Failure)
Diabetes
Older People
Neuro Rehab
End of Life Care Long-term conditions delivered through polysystems will be managed through the model below. Medicines management and pharmacy needs to be integrated to support delivery of this model. Fig 37: Proposed long-term condition pathway for polysystems
PC
HAcute Exacerbatio
nMulti-complex
Complex
Simple
Screening and diagnosis
Prevention
Social Care
3rd
SectorGP
GP
Urgent
Care
PC
Proposed LTC Pathway
13/5/2010 NHS Wandsworth LTC Generic model
PCP
ers
on
alis
atio
nGP
GP
GPPC
GP
GP Practice
Polysystem – GP
Based/Primary
Care
Polyclinic
Home
Acute Hospital
Currently all polysystems are using the above service model. Pharmacy will link into all these workstreams as all long-term conditions involve medicines. The Community Pharmacy Contractual Framework offers a package of care that can be integrated into long-term condition care pathways. The National Contract can offer a great deal of value to patient care. This is shown below in a modified diagram of the Core Contractual Framework. There are opportunities to look at improved patient compliance around medicines and develop more structured medication reviews. The key driver for this will be with joined up planning through LCGs and with GPs. It is important to recognise there are contractual differences between the GMS and Community Pharmacy framework and professionally both groups will approach long-term conditions in a different way. Through joined up planning, integrated service design and improved communication Community Pharmacy can offer and provide services that can support patient care and be complimentary to general practice and avoid duplication.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
73
An example of how Community Pharmacy can support diabetic care is shown below. Fig 38: Community Pharmacy long-term condition service model (e.g. Diabetes)
NATIONAL CONTRACT ALIGNED TO DIABETIC CARE
ESSENTIAL ADVANCED
1. Dispensing of medicines
• PMR identity Diabetes patients .
2. Repeat Dispensing
• Patients medication managed
3. Public Health:-PCT stats Diabetes
4. Signposting-local Diabetic Network
5. Support for Self care
7. Support for disabilities
8. CLINICAL GOVERNANCE
• CPD, current prescribing issues in Diabetes
DIABETES MEDICATION
USE REVIEW
Link in with Repeat dispensing
Link in with GP Medication
reviews, other HCPs
The core contract can offer a tier 1 package of care around a long-term condition and can act as the foundation to locally enhanced services around long-term conditions. MURS can be locally developed with agreed outcomes with local GP practices. This will provide better value for money and develop community pharmacies in long-term conditions. There needs to be a consideration of other pharmacy providers who can offer specialist skills in long-term conditions. Specialist pharmacists working in acute trusts could offer more clinical input and advanced medication reviews. This could be useful for specialist review clinics in polysystem settings.
PNA Commissioning Intentions – More integration of the Community Pharmacy Contractual Framework in long-term conditions, particularly Medication Use Review, repeat dispensing and health promotion and signposting. The patient pathway for long-term conditions needs to factor in management of medicines at a community level. Prescribing and dispensing around long-term conditions need to be linked more closely together. A closer working approach with general practitioners, community pharmacists and prescribing advisors (attached to PBC groups) around long-term conditions. More joint planning with the long-term condition groups, GPs and nurses is required to ensure the role of Community Pharmacy is developed and enhanced. Pharmacists working in acute or tertiary care can offer specialist skills around long-term conditions in Primary Care.
Locally enhanced e.g Diabetic Screening Tier 3 Medication reviews

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
74
7.3 Cardiovascular Disease (CVD) Cardiovascular disease (CVD) (incorporating ischaemic heart disease, cerebrovascular disease and peripheral vascular disease) is the leading cause of death in the UK. CVD and its related conditions, diabetes and chronic kidney disease, are also a major cause of morbidity. Together, the conditions affect the lives of 6.2 million people and are responsible for a fifth of all hospital admissions. These diseases share common risk factors such as smoking, hypertension, hypercholesterolemia, lack of physical activity and obesity. Alongside this, they often serve as risk factors for each other e.g. a person with diabetes is much more likely to develop ischaemic heart disease than somebody who does not have diabetes. CVD is a major contributing factor to health inequalities within the borough of Wandsworth, as this differentially affects people from deprived socioeconomic populations and BME groups. It is thought that CVD accounts for more than half the variation in life expectancy between the rich and the poor. The burden of disease is clearly evident in our most deprived ward (Latchmere); the SMR is 196.4 for deaths under 75 years due to CVD (SMR=100 for England), compared to the most affluent ward (Thamesfield) which has an SMR of 74.2. Recent estimates in the USA indicate that one in four adults have high blood pressure. But with the lack of any specific symptom, nearly one third of these people are not aware they have it. Many people have high blood pressure for years without knowing it.
Fig 39: Map of Community Pharmacy Vs CHD rates
The map above compares the distribution of community pharmacies with coronary heart disease (CHD). This gives a rough indication where community pharmacies are located in terms of a disease state that includes cholesterol as one of its risk factors.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
75
7.4 Diabetes It is estimated that around 3% of adult men and women have diabetes, mainly type 2 diabetes. While there are no accurate estimates of the number of diabetics in Wandsworth, a study carried out in the mid 1990s (involving nine practices) found that: - Table 9: Percentage of adult population with diabetes.
% OF TOTAL GROUP MALE FEMALE
WHITE 6.7% 5.2%
ASIAN 25.4% 20.5%
BLACK 1.9% 14.9%
The 2009 PCT Public Health report identified the diabetes register rate has increased in 11 out of the 20 Wandsworth wards. The prevalence of diabetes across Wandsworth is shown below:- Fig 40: Prevalence of diabetes across Wandsworth
PNA Commissioning Intentions – Community Pharmacy can support CVD monitoring through open screening in pharmacies and medicines management. The key groups with CVD prevalence are the same groups that access community pharmacies with prescriptions of CVD medication or for self care. There are opportunities to link into specialist pharmacy skills such as pharmacists working in acute settings who could bring their specialist skills into the community. Further work is required to integrate their skills into this long-term condition pathway.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
76
The NHS Wandsworth Public Health report has identified several areas to manage diabetes across Wandsworth:-
• Use of health trainers to do specific work in the community on key health goals such as diabetes
• The importance of physical activity and weight loss. • The occurrence of diabetes is twice as frequent for South Asians.
The Community Pharmacy service model (figure 38, page 73) for diabetes demonstrates how the National Community Pharmacy Contractual Framework can be tailored and redesigned around a long-term condition. This model will help to focus community pharmacies around diabetes and work towards local outcomes.
7.5 Cholesterol It is estimated that the UK average blood cholesterol is about 5.5mmol/l for men and 5.6 mmol/l for women. There are no accurate figures on the prevalence of hyperlipidaemia and levels of HDL and LDL in Wandsworth. However, the mid-1990s‟ Wandsworth Heart Study showed the percentage of the adult population with a cholesterol reading of over 6.5 mmol/l. Table 10: Percentage of adult population with a cholesterol reading of over 6.5 mmol/l.
% OF TOTAL GROUP
MALE FEMALE
WHITE 37.3% 36.3%
ASIAN 22.4% 18.6%
BLACK 15.5% 21.9%
It is important that when taking readings for cholesterol the full lipid profile is carried out. Some pharmacy companies have gone ahead and offered free cholesterol testing to the public. These readings do not offer a full lipid profile and in some instances have resulted in incorrect referrals to primary care. The pharmacy companies who offer these services sometimes do not charge and this has caused queues, which reduces those pharmacies‟ capacity to offer other key services the PCT require, such as smoking cessation.
PNA Commissioning Intentions – Community pharmacies could play a role in diabetes management through screening, blood glucose testing, medicines management and health promotion. More integrated working between general practice and Community Pharmacy could support this. Diabetes figures more strongly among the Asian population. The majority of community pharmacies speak an Asian language; this represents more specialised opportunities for health promotion and improving medication for communities. NHS healthchecks through Community Pharmacy could be linked or developed into screening programmes to identify patients at risk and manage them back into Primary Care. According to areas of prevalence Roehampton, Tooting, Furzedown, Graveny and parts of Battersea are priority areas.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
77
7.6 NHS Healthchecks Community Pharmacy can support the NHS Healthcheck programme and support vascular screening in Wandsworth. The PCT has identified that up to six pharmacies will be selected to provide NHS healthchecks. At the time of writing this report the PCT is now going through the final stages of getting the services set up. 7.7 Respiratory Disease and COPD Figure 41 below shows the admission rate for respiratory disease in Wandsworth across three age bands.
There is an increase in admissions as age increases, with the rate of admission for males consistently being higher than that for females
Deprivation has an effect on the rate of admissions in the most deprived group of wards (Latchmere, Roehampton, Queenstown, Graveney)
The rates of admissions for respiratory conditions were greater in men than in women except for those wards in the highest deprivation category.
Fig 41: Admission rates by age group, respiratory disease in Wandsworth (ICD10 J00-j99
Chronic Obstructive Pulmonary Disease (COPD) The most important cause of COPD is smoking. Figure 42 shows COPD was responsible for 62% of all respiratory disease admissions. It also shows that there is a higher percentage of male admissions compared to female admissions for COPD.
PNA Commissioning Intentions – Community Pharmacy can offer and provide appropriate cholesterol testing by providing PCT approved services. Baseline data has shown most pharmacies have cholesterol machines. New technology means that there are take-home or onsite kits where samples can be sent to laboratories for a full lipid profile analysis. Community Pharmacy can provide access and extra capacity for cholesterol testing. Cholesterol testing can be built into other pharmacy services e.g. weight management, health screening and medication reviews.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
78
Figure 42: Percentage of COPD admissions to hospital (Wandsworth) Source: Clear net 2004
In Wandsworth there is a very good respiratory nursing network consisting of four specialist respiratory nurses. In addition there are some practice-based nurses who have some training in respiratory care. There has been a good working relationship between respiratory nursing and Community Pharmacy.
7.8 Sexual Health Wandsworth has increasing rates of some sexually transmitted infections (STIs) like chlamydia and genital warts, and a young population at risk of poor sexual health. Men who have sex with men and black or minority ethnic groups also tend to have poorer sexual health than the general population. Information for this section is taken from the 2009 Sexual Health Service Reconfiguration in Wandsworth Future Provision. For Wandsworth :
In 2008, in highest third of London boroughs for teenage pregnancy rates
In 2009, more than 70% of abortions took place at 10 weeks pregnant or earlier
In 2008, nearly three times the national HIV prevalence rate, but lower than the overall London rate
Syphilis has risen from one case in 1998 to 26 cases in 2008
In 2008 St George‟s Hospital diagnosed 30% of chlamydia and 51% of gonorrhoea cases in South West London
High number of cases of hepatitis B in south Asians
Nearly 60% of HIV cases accessing care in 2007 were infected by men having sex with men
Over a quarter of HIV cases accessing care in 2007 were from black African communities. 60% of these were women.
Wandsworth has a higher proportion of persons of reproductive age as shown below.
PNA Commissioning Intentions – Community pharmacists can support COPD and asthma by improving the use of medicines through compliance assessment and inhaler technique. This service will be suitable for patients who do not readily access Primary Care. There are opportunities to link this into GP medication reviews, and to provide updated information. The service should be integrated with smoking cessation, lifestyle advice and linked to the Wandsworth Council Airtext campaign, which alerts registered asthma/COPD patients to poor air quality through a text message. Spirometry testing can be build into these services. COPD can link into pharmacies offering stop smoking and supplying vitamin D.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
79
Fig 43: Reproductive age in Wandsworth
Sexually Transmitted Disease (STD) in Wandsworth has risen dramatically over the past few years and by more than the national average for chlamydia (112%) and gonorrhoea (104%). Under-16 conception rates have generally increased since 1998. The rate of terminations of pregnancy has remained constant from 1998 to 2002 with 88-90% of these terminations being funded by the NHS. The percentage of under-18 conceptions ending in termination is under 60%.
Table 11: Trends in teenage conception rates (under 18 years)
Area
1998 (baseline)
2002 (latest year)
Target reduction 50% by 2010 on 1998
baseline
Wandsworth 70.3 60.7 35.1
England 47.0 42.6 23.5
LONDON 51.0 52.0 25.5
Inner London 67.1 67.4 33.6
Outer London 41.9 43.4 21.0
Bottom quintile 79.1 78.5 39.6
(From the 2001 Trends in teenage conception rates (under 18 years))
Wandsworth is in the bottom quintile for teenage conception rates. The immediate and long-term consequences of STDs and unwanted pregnancies, especially teenage pregnancies, are enormous. If left untreated, chlamydia and gonorrhoea are common causes of pelvic infection, ectopic pregnancy, and infertility. Babies born to mothers infected with chlamydia can develop pneumonia. If left untreated, two out of three patients with syphilis will develop serious heart, nervous system, skin or bone problems, leading to disability or death. Infection with syphilis in mothers often leads to miscarriage. Babies born to infected mothers may have congenital syphilis. Furthermore, 85% of people infected with hepatitis C will develop chronic liver disease, with some also developing liver cancer. Nearly all STIs are preventable with the majority, if

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
80
recognised and diagnosed early, and responding well to treatment, which is why improving sexual health services is so important for Wandsworth. 7.8.1 Emergency Hormonal Contraception through Community Pharmacy There is currently a network of community pharmacies in Wandsworth that provides Emergency Hormonal Contraception (EHC) (see figure 44). The service was set up in 2005 and now community pharmacies commissioned by Wandsworth offer free EHC from 13 years and above by supplying the prescription-only Levenogesterol 1500mg, under Patient Group Direction. The service is a supervised administration where clients must take the EHC in the pharmacy. There is an over-the-counter Levenogesterol 1500mg, which is branded differently and is licensed for 16 years and above. The rationale for free EHC through community pharmacies is:-
The public value and frequently visit their local pharmacy
Development of pharmacist‟s role as part of an integrated sexual health network
Opportunities within Community Pharmacy Contractual Framework for self care, health promotion and signposting linked to sexual health
Improved access to EHC as need and demand exists
Assist in reducing pressure for uncomplicated EHC request on other services – GUM, Family Planning clinics and other forms of Primary Care.
Figure 44: Map of Community Pharmacy vs teenage conception data
EHC pharmacy

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
81
The service activity for EHC is listed below by postcode. Table 12: Service activity for EHC
Financial Year 09/10: EHC SUPPLY BY POSTCODE
SW11 710
SW12 1201
SW15 1117
SW16 19
SW17 786
SW18 554
SW19 4
Total EHC supply 4391
Financial Year 10/11 (April 2010-Dec 2010) : EHC SUPPLY BY POSTCODE
SW11 641
SW12 744
SW15 982
SW16 16
SW17 557
SW18 429
SW19 26
Number of EHC supplied 3395
The information in table 12 above has been revised into EHC activity for each polysystem area in figure 45 (below). It should be noted that figures for 2010/2011 are current EHC activity from April 2010- December 2010.
Figure 45: EHC supplied by polysystem area
The overall data shows that EHC is accessible through PCT-commissioned pharmacies, but there are local issues that have to be resolved.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
82
Service Continuity - Due to the nature of community pharmacy staffing, pharmacists are mobile and can move to different pharmacies as part of corporate changes or when changing jobs. The PCT commissions the pharmacy through the accredited pharmacist to provide the service. If the pharmacist were to leave then the service ceases until a new pharmacist can be trained. Each PCT has different service specifications and differs in training; therefore if an accredited pharmacist from one PCT wishes to practice in another PCT, they have to wait for PCT training. In response to the above, NHS Wandsworth has done the following:-
Locally NHS Wandsworth has supported harmonised accreditation across London so that pharmacy EHC services are standardised and accredited pharmacists can practice in different boroughs
The NHS Wandsworth community will accept training for pharmacists from other PCTs carried out in the last 18 months
Twice yearly training and updates are carried out to avoid service drop-out and to offer training to new pharmacists.
All community pharmacies can supply and sell EHC over the counter from 16 years and above. Promotion – This is an area of ongoing development but needs to be linked into family planning websites for these services to be made available. Sexual Health Network – For Community Pharmacy to play a significant role in sexual health provision, there needs to be professional integration and inclusion into the network of Reproductive Sexual Health (RSH) providers such as GUM and family planning clinics. While community pharmacies can deal with more uncomplicated requests for EHC and take pressure off these services, more clinical and social complex sexual health conditions could be referred to family planning clinics. There are opportunities to develop referrals, and pathways between Community Pharmacy and RSH. Locally the RSH providers could be commissioned to help deliver training and input development of local pharmacies. This would support local discussions about joint working and closer integration. Locally NHS Wandsworth community pharmacies will support teenage pregnancy initiatives through health promotion.
The South West London HIV & Sexual Health Clinical Services Network provides the structure for the collaboration and co-ordination between organisations and professional groups who deliver clinical services for HIV, GUM and Reproductive Sexual Health. The focus is on clinical governance, developing integrated care pathways and increased user choice, whilst ensuring that services are patient-focused, high quality, effective and equitable. Professional pharmacy representation at this level is required to ensure there are professional inclusion opportunities for joint working.
Professional Development – In response to the current NHS changes, the Royal Pharmaceutical Society has convened a workgroup on Sexual Health in Pharmacies (SHIP) to look at better integration of resources, developing best professional practice and harmonised

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
83
accreditation for pharmacies wishing to provide sexual health services. Stakeholders include the College of Pharmacy Practice and the British Association for Sexual Health and HIV (BASHH). It is anticipated this will lead to a harmonised training and development. The PCT emergency contraception training for pharmacists has been revised to include:-
A review of all types of contraceptive methods and long-acting contraception
The needs of young people and developing services to be young persons‟ friendly. Sexual Health Service Development – Community pharmacies commissioned through NHS Wandsworth provide EHC. This is emergency contraception only. There are opportunities to make use of this EHC supply through building in more interventional work to develop a broader sexual health service. The PCT is taking foreword a smaller number of community pharmacies to provide additional services. These include:-
Free condom supply for young people up to 25 in line with the PCT condom distribution scheme
Redevelopment of chlamydia screening and treatment
Supply of long-acting contraception under patient group direction.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
84
PNA Commissioning Intentions – The Community Pharmacy PCT EHC service is considered a necessary service to meet the current needs of Wandsworth. The Chlamydia Screening service and Integrated Sexual Health service are considered relevant but do not constitute necessary services. The existing Community Pharmacy EHC service should be developed to meet local needs and work with reproductive sexual health and local GP practices. Pharmacies commissioned to provide EHC should participate in the condom distribution scheme. The PCT is now developing an Integrated Sexual Health service that combines:- • EHC • Chlamydia screening and treatment • Condom distribution • Long-acting oral contraception through Patient Group Direction. This will be offered to a smaller number of pharmacies to be developed in providing more sexual health services. Further integration of community pharmacy sexual health services with the overall sexual health strategy is now required. This would support better professional development and improve patient signposting and patient referral between all providers. The SE London Modernisation initiative for sexual health service model (below) clearly stratified how Community Pharmacy fitted a local sexual health model. A similar approach is required for SW London and Wandsworth that looks at the different types of provision for sexual health services in an integrated care model.
This work must be underpinned by strong professional development, harmonised accreditation and local partnership working around patient care. Joint working with the Royal Pharmaceutical Society, College of Pharmacy Practice and SW London Local Practice Forum will ensure robust development and closer Community Pharmacy integration into sexual health in SW London.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
85
7.9 Drugs and Alcohol Information from this section is taken from the Wandsworth Drugs and Alcohol Misuse Needs Assessment 2011, Wandsworth Drug Treatment update 2009-10, Supervised Dispensing of Methadone and Buprenorphine April 2009-March 2010, and the Wandsworth Needle Exchange Annual Report April 2009-2010. This section will look at the wider health needs for drug misuse and alcohol prevalence and how Community Pharmacy can support these client groups. 7.9.1 Understanding General Prevalence Table 13: Illustrating prevalence of drug misuse, treatment uptake and penetration rates
Wandsworth is estimated to have 1,828 priority drug users (crack cocaine or opiate users). At 0.61% of the overall population this is slightly below the estimated prevalence for London (0.82%) but is similar to the national prevalence (0.62%). Overall the Wandsworth rate per 1000 of drug users in treatment, both PDUs and the wider drug using population, is lower than London or national rates. However, our penetration rate at 53.0% of estimated drug users in or known to treatment in the last two years is above the London average.
Rates per 1000 population of people engaged in treatment for substance misuse as of March 2010
Wandsworth London National
PDUs (in effective treatment during the year) 846 25,791 162,891
All Drug Users (in effective treatment during the year) 1,047 31,688 192,544
Primary Alcohol (in treatment during the year) 701 16,144 111,381
Population 290,260 7,683,866 51,809,700
PDUs/1000 2.91 3.36 3.14
All Drug Users/1000 3.61 4.12 3.71
Alcohol/1000 2.44 2.10 2.15
Sources: NDTMS.net, NDTMS Alcohol Needs Assessment Data, NDTMS Drugs Needs Assessment Data, GLA Population Projections 2009, ONS MYE 2009 Priority Drug Users – effective treatment penetration at end of 2009-10
Wandsworth London National
In effective treatment 31st March 2010 538 18,290 129,260
Otherwise, in effective treatment during 2009-10 246 7,501 33,631
Otherwise, in effective treatment during 2008-09 185 6,409 26,035
Prevalence estimate 1,828 62,769 321,229
Penetration Rate (%) 53.0% 51.3% 58.8%
Estimated Treatment Naïve PDUs 859 30,569 132,303
Sources: NDMTS Needs Assessment Data, NTA/Glasgow University Prevalence Estimates
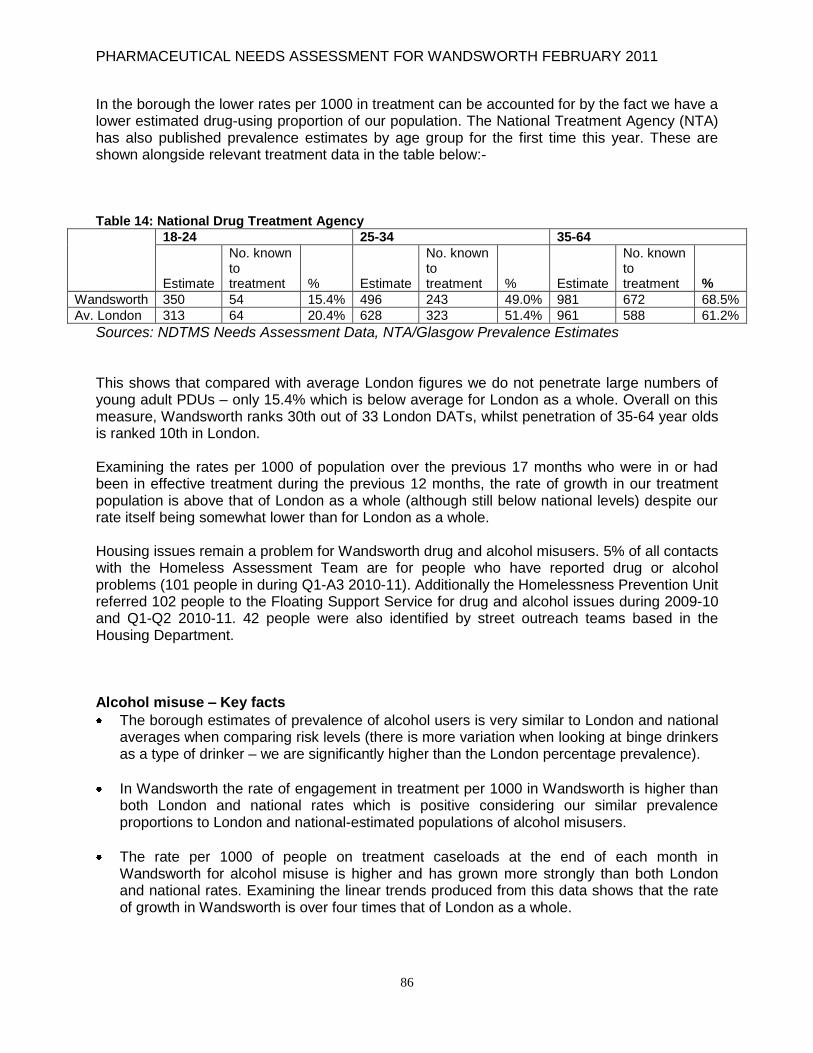
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
86
In the borough the lower rates per 1000 in treatment can be accounted for by the fact we have a lower estimated drug-using proportion of our population. The National Treatment Agency (NTA) has also published prevalence estimates by age group for the first time this year. These are shown alongside relevant treatment data in the table below:- Table 14: National Drug Treatment Agency
18-24 25-34 35-64
Estimate
No. known to treatment % Estimate
No. known to treatment % Estimate
No. known to treatment %
Wandsworth 350 54 15.4% 496 243 49.0% 981 672 68.5%
Av. London 313 64 20.4% 628 323 51.4% 961 588 61.2%
Sources: NDTMS Needs Assessment Data, NTA/Glasgow Prevalence Estimates This shows that compared with average London figures we do not penetrate large numbers of young adult PDUs – only 15.4% which is below average for London as a whole. Overall on this measure, Wandsworth ranks 30th out of 33 London DATs, whilst penetration of 35-64 year olds is ranked 10th in London. Examining the rates per 1000 of population over the previous 17 months who were in or had been in effective treatment during the previous 12 months, the rate of growth in our treatment population is above that of London as a whole (although still below national levels) despite our rate itself being somewhat lower than for London as a whole. Housing issues remain a problem for Wandsworth drug and alcohol misusers. 5% of all contacts with the Homeless Assessment Team are for people who have reported drug or alcohol problems (101 people in during Q1-A3 2010-11). Additionally the Homelessness Prevention Unit referred 102 people to the Floating Support Service for drug and alcohol issues during 2009-10 and Q1-Q2 2010-11. 42 people were also identified by street outreach teams based in the Housing Department. Alcohol misuse – Key facts
The borough estimates of prevalence of alcohol users is very similar to London and national averages when comparing risk levels (there is more variation when looking at binge drinkers as a type of drinker – we are significantly higher than the London percentage prevalence).
In Wandsworth the rate of engagement in treatment per 1000 in Wandsworth is higher than both London and national rates which is positive considering our similar prevalence proportions to London and national-estimated populations of alcohol misusers.
The rate per 1000 of people on treatment caseloads at the end of each month in Wandsworth for alcohol misuse is higher and has grown more strongly than both London and national rates. Examining the linear trends produced from this data shows that the rate of growth in Wandsworth is over four times that of London as a whole.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
87
Unlike amongst drug clients, a comparison of primary alcohol clients has not been conducted in previous years. It is worth highlighting significant trends within the data. First, Wandsworth has a much more even gender balance amongst alcohol clients than amongst drug clients. In Wandsworth 58.4% of clients are male and 41.6% female, which is a higher proportion than most other demographically similar boroughs (although overall the proportion of women is higher in all boroughs).
7.9.2 Services for Drug Misusers Community pharmacies in Wandsworth provide services to drug misusers through supervised administration of medication (primarily Methadone and Buprenorphine) and needle exchange services. There are 63 pharmacies in the Wandsworth area, of which 43 provide the supervised dispensing service of methadone and buprenorphine. This represents 64% of all pharmacies providing this enchanced service. The number of pharmacies signed up to provide the service can be broken down into local commissioning cluster localities:-
Battersea : 11 pharmacies West Wandsworth : 8 pharmacies Wandle : 24 pharmacies
The key highlights are presented below:-
Between 2008/09 and 2009/10 the number of clients in structured substance misuse treatment, as measured by National Drug Treatment Monitoring System (NDTMS), increased by 6.7%, from 983 to 1049 (PDUs up from 770 to 791)
In 2007/08 a number of clients on the caseload of the two statutory prescribing services were found to be long-term, inactive or incorrectly entered and had to be removed from the totals. In 2009/10 a number of clients at several agencies had to be removed as the records were found to be inaccurate. Furthermore, a data refresh exercise by NDTMS led to a further significant loss of records during the year.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
88
7.9.3 Geographical Spread
Figure 46: Map of deprivation based estimates of priority drug user numbers by ward and at risk lower level super output areas
Figure 46 shows ward estimates of the prevalence of Priority Drug Users (PDUs) in the borough, with small areas likely to have higher concentrations of PDUs. The estimates are weighted for age, gender and collated to deprivation levels in the borough as reported in the Index of Multiple Deprivation 2007. The estimates predict the highest concentration in Latchmere and Queenstown, followed by Roehampton. This pattern is largely held up by the distribution of clients testing positive for opiate or crack cocaine use as part of the Drugs Intervention Programme (DIP) during 2009-10. Latchmere, Fairfield and Queenstown come out as the most prominent areas. Roehampton and most of the southern wards, except Tooting, appear less concentrated but it must be remembered that they border non-intensive DIP areas so fewer of their residents may be entering the system as a result. Another measure available to look at potential drug misuse is finds of sharps (needles, drugs waste) by housing, street cleansing and parks maintenance teams. The final data for 2009-10 shows significant finds in Roehampton, confirming the existence of high levels of substance misuse in this part of the borough. Significant finds also exist all over Latchmere and the larger estates in Shaftesbury, St. Mary‟s Park and Queenstown wards, and also in the area of Southfields identified in the prevalence estimates as a significant area for predicted PDUs.
An analysis of raw data, extracted from NDTMS, of Wandsworth clients referred into structured treatment in 2009/10, provides some information on the geographical spread of problem drug users in treatment. From this, a very high proportion of those in treatment come from a relatively small number of postcode sectors. In the following maps, this is compared with data on the postcodes of those who underwent assessments under the Drug Interventions Programme in the same year.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
89
NDTMS Data
In 2009/10 there were 1269 unique clients in treatment during the year. Not all of these clients would have been in effective treatment. It is also possible that due to inaccurate entry of attributor data, some clients have still been double-counted. However, of these 1,269 clients, 1,060 (83.5%) had valid Wandsworth postcodes. The map below shows the distribution of these clients across the borough.
Figure 47: Number of clients in treatment per postcode
Drug Intervention Programme (DIP) data
This distribution can be compared to the number of clients being assessed by DIP. The data set used in this instance was for 2009-10. In total there were 491 clients with an initial assessment following a positive drugs test for opiates or crack/cocaine; of these there were 491 unique clients. 368 of these people had valid postcodes (88.7%) and 203 were Wandsworth residents (48.9%).

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
90
Figure 48: Number of clients per drug treatment programme
Data from both maps indicate that the Battersea region – Latchmere in particular but also the surrounding wards – has the highest concentration of drug users in the borough. However, in the DIP data map the area around Tooting/Graveney shows up as an area of significant concentration of drug users. The underrepresentation of this area in the map of drug users in treatment may relate to the lack of services in this particular area of the borough. Likewise, Roehampton shows up strongly as an area of drug users in treatment – a statutory drugs service is located at Queen Mary‟s hospital, but not on the DIP data map. This is likely to be the result of neighbouring Kingston, Richmond and Merton boroughs both being non-intensive DIP areas where routine drugs testing is not carried out.
Sharps finds show Queenstown as having a much higher association with drug use; in particular around the Doddington Estate. This is not inconsistent with these maps as the Doddington Estate is actually within the postcode sector that straddles Latchmere, Shaftesbury and also this small area of Queenstown ward. Sharps finds are also found in significant numbers in Roehampton in the Alton Estate and amongst several other housing estates in all areas of the borough. London Ambulance data for drug overdose-related callouts shows much the same pattern as the other data, although there is a concentration in Roehampton of callouts (other concentrations in Fairfield and Wandsworth Common wards can be related to the location of the main custody suite at Wandsworth police station and Springfield Hospital).
7.9.4 Supervised Administration and Needle Exchange The map below shows the distribution of drugs services in Wandsworth provided by pharmacies. There are at least 30 pharmacies providing supervised administration services and 11 pharmacies providing needle exchange.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
91
Fig 49: Map of community pharmacies providing needle exchange & supervised administration
Needle exchange pharmacy Supervised administration pharmacy
Supervised Administration In Wandsworth community pharmacies, drug misusers can receive Methadone, Buprenorphine, Naltrexone or Diazepam as part of a supervised administration programme. This service provided by community pharmacies is only available for those patients being prescribed by Wandsworth prescribing agencies. Pharmacies do treat supervised patients who are prescribed by out-of-borough agencies but we do not provide pharmacists‟ payment for this. Drug misusers can easily find or be referred to a pharmacy that provides supervised administration. Over the last four years the number of pharmacies providing supervised administration has grown from 15 pharmacies to over 30. Scoping studies carried out between 2005-2007 showed that about 200-250 clients visited pharmacies for supervised administration. Summarised below is key information relating to this service.
Referral source The three main prescribing sources within the Wandsworth area are:
Wandsworth Communtiy Drug Project, St John‟s Hill (WCDT)
Addiction Treatment Centre, Queen Mary‟s Hospital (ATC)
Referrals via general pracititioners (GPs)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
92
The number of clients per local commissioning group The graph below indicates the number of clients receiving the supervised dispensing service from pharmacies across the localities. Fig 50: Supervised dispensing client numbers per Local Commissioning Group
Substitution Treatment
Methadone is the main substitute drug prescribed for clients
In 2009-2010, 279 clients received a supervised prescription; this is a decrease of 10 clients compared to 2008-2009
39 clients received a supervised prescription of Buprenorphine; this is a decrease of two clients compared to 2008-2009
From 2009-2010 a total number of 25,311 supervisions were undertaken; this is an increase of 1,454, again compared to the year before, and only one client received supervised Diazepam.
The data below shows the number of clients who received supervised consumption for the first three months as per the recommended governmental guidelines:-
A total number of 203 clients received supervised dispensing for the first three months of the start of their prescription
A total number of 115 clients exceeded the recommended supervised period, this is an
increase of 19 clients compared to 2009-2010 (96 clients).
Key issues and developments to be taken forward for 2011/2012 Length of Supervision - Some clients have stayed on supervised consumption for longer lengths of time than is expected. Few patients can achieve abstinence rapidly, most require the support of prescribed medicines for longer than just a few months. The decision to maintain a patient on long-term opioid prescription should be reviewed at regular intervals, usually at least three-monthly and should be part of a broader programme of their care plan with ongoing social and psychological support. Further work is also being conducted during weekly team meetings with the Community Drug Teams (CDTs) to review all clients who are receiving supervised consumption prescriptions. Controlled Drugs - Medicines Act – Prescribing controlled drugs is subject to the Medicines Act-Drug Misuse Act, which has very strict criteria in terms of prescribing and handwriting

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
93
requirements for prescriptions. Future updates around these areas should involve community pharmacists, prescribers from the CDTs, and general practice to ensure there is improved understanding. Non-Judgemental Service – As part of the PNA consultation, patient groups were consulted. The Drug Misuse Forum has fed back the importance that clients are treated non-judgmentally as part of the service delivered in pharmacies. This will apply to front line pharmacy staff as well as pharmacists. Shared Care – The care of clients is key, and effective communication around client care, linking prescribers from the CDTs and GPs, client key worker and community pharmacies, is important to ensure that key clinical issues, client compliance issues and prescribing changes are transparent.
Needle Exchange
There are ten pharmacies currently providing a Needle Exchange service in Wandsworth and one fixed Needle Exchange site based at Wandsworth Drug Project, Garratt Lane. All pharmacies and the fixed Needle Exchange site provide a pick and mix system of needles, syringes and injecting paraphernalia. Pharmacists are also able to provide harm reduction information to service users; this is done by way of providing leaflets or signposting to the seven substance misuse services in Wandsworth. This report will refer to pharmacies in relation to LCGs, an overview of the pharmacies in relation to LCGs is seen below.
Battersea : 3 pharmacies
West Wandsworth : 2 pharmacies
Wandle : 5 pharmacies
There is a fixed site service provided by a Community Drug Team. This is not provided by a community pharmacy and therefore will not be considered as part of this report. From a commissioning point of view, other non-pharmacy providers could be commissioned to provide needle exchange.
Data Summary The data for this service is taken from April 2009 - March 2010. Each individual is counted only once in the same pharmacy for that month and only once for the quarter. Each individual counted may use more than one pharmacy in a month and also may use more than one alias name on a daily basis. As a result there may be duplication in the numbers of injecting drug users. However from April 2010 a new database will be used and this will provide us with a more accurate figure for 2011. The chart below shows the number of clients who have accessed the pharmacy exchange in the five clusters.
Apr-June 09 July-Sep 09 Oct-Dec 09 Jan-March 10
Battersea 434 353 467 507
Wandle 622 661 594 628
West Wandsworth 147 178 175 185

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
94
Client profile Based on analysis of returned needle exchange forms, the analysis of patient ethnicity is shown below: Figure 51: Ethic origin needle exchange users
Drug injection From Figure 52 below, the primary drug injected by the majority of needle exchange users is heroin. Figure 52: Primary drug injected by needle exchange users
Usage of Equipment Needles, syringes and swabs are distributed through the needle exchange service. In addition Vitamin C sachets and water for injection are supplied. It should be noted that water for injection should be provided to clients who have no source of running water and who are sleeping rough.
Needles The 1ml size needle is the preferred needle for injecting heroin, with Battersea showing the highest distribution, followed by West Wandsworth (see figure 53, below).

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
95
Fig 53: Syringe distribution
Swabs These are distributed in all needle exchanges. Clients are encouraged to swab the injecting site to remove any bacteria; however it was reported that alcohol swabs were often used in a variety of inappropriate ways, one of which is using the swab as a heat source for the preparation of drugs for injections. Battersea has distributed the majority of swabs. (See Figure 54 below.) Due to the increase of Anthrax all pharmacies in 2010 are encouraging clients to take note of the importance of swabbing the injecting site and are also providing harm reduction information around the serious bacterial infection of Anthrax. (Health Protection Agency HPA Cfi 05/02/2010). Figure 54: Distribution of swabs across Wandsworth
Steroids Users In addition to drug misusers, the needle exchange service has been extended to steroid users. This client group faces similar medical risks to drug misusers through not accessing sterile needles. All pharmacies and the fixed site have been advised on harm reduction issues and have been provided with information leaflets. Further work around steroid use in gyms will be carried out.
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
96
Patient Experience A mystery shopper campaign was carried out in 2009-2010 as part of the review of the pharmacy needle exchange service. A summary of the mystery shopper report on the community pharmacy needle exchange service and the fixed site service is as follows:-
All pharmacies responded well to the different scenarios
All the ten pharmacies within the borough provided an excellent service and complied with all the aims and objectives set out in the Service Level Agreement
The most vulnerable clients were signposted to other services and to A & E; this could be due to injecting infections or poor health
Pharmacist were polite and non-judgemental and treated the service user no differently to others customers accessing the pharmacy
The counter staff and pharmacist were respectful when issuing equipment and aware of the service users needs
All pharmacies were very knowledgeable with regards to providing supervised consumption and supplying clean injecting equipment, at the same time advising clients about overdose issues
There did seem to be some uncertainty with regards to information about treatments that are available including complimentary therapies for services users, and also living out-of-borough and still using the services.
All staff were professional, discreet and provided services users with as much information as possible, mainly via booklets and leaflets, with some pharmacies accessing the internet for the client.
Client feedback
In September 2010 consultation over the review of drug treatment services is taking place. At the time of writing of this report it was highlighted that Community Pharmacy had to be better integrated into service design.
Complimentary opening hours for clinics, pharmacies and GPs to ensure better communication around patient care
Ensure prescriptions for controlled drugs are written in compliance with the Medicines Act and are rectified if any errors occur
Shared care arrangement around the care and wellbeing of drug misusers, linking drug treatment clinics, general practitioners, community pharmacies and client drug workers
More health promotion awareness for drug misusers through hard reduction advice.
Overall Wandsworth Needle Exchange services are very well established and are growing from strength to strength. The Battersea cluster provided the most needles followed by West Wandsworth. The service has been extended to sterioid users.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
97
Moving Forward: Policy Issues
The new coalition government has a number of policies which will impact on the delivery of drugs and alcohol services in the future. Many policies of the last government have been continued and extended in this field, which we must also now implement and respond to. To summarise, the main policy issues identified by the DAAT as likely to have a significant impact on service delivery and treatment need within the borough, are:
The implementation of GP Commissioning Consortia and abolition of the Primary Care Trust
The development of integrated recovery models and the development of community budgets through schemes such as Integrated Offender Management and Family Intervention and Recovery Schemes
The increasing importance of alcohol treatment and the need to find or divert funds to pay for the expansion of this sector
The continued establishment of the polysystem model
The potential development of elected police commissioners The establishment of a polysystem model in the borough was fully examined in last year‟s needs assessment and it has been fully planned for in the commissioning process currently underway which will conclude later this year. The new provider will be expected to cover all three polysystem areas. The implementation of the new Integrated Drug and Alcohol Service, which will be commissioned as a result of the tender process, is currently underway. The new service will seek to better cover the borough to fulfil equal provision across all three polysystem areas and open up access to both drug and alcohol treatment at both structured and open access levels of provision across the borough. The nature of the new treatment system with fewer providers, although hopefully offering more services, will naturally lead to a very different treatment landscape once it is fully established. Assessing need and performance will be likely to be done at a whole system level rather than a service level, and problems around referrals and continuity of care will hopefully be reduced as a result of this switch in delivery models.
PNA Commissioning Intentions – The PCT deems supervised administration and needle exchange a necessary service to meet the current needs across Wandsworth. The number of pharmacies providing services for drug misusers has been in place over the last five years. There is an established network which presents opportunities to develop further and work is being done to expand supervision to include diazepam and naltrexone. Needle exchange is now being expanded to include steroid misusers. More development of pharmacies undertaking supervised administration to provide harm reduction advice has been identified. There are opportunities to now develop a few pharmacists who already provide supervised administration and needle exchange, and involve them in hepatitis screening. Community pharmacies could offer additional services such as minor ailments, minor injuries, focused health promotion and signposting to local support agencies. NHS Wandsworth will explore commissioning of supervised administration and needle exchange with pharmacies closely bordering NHS Wandsworth, who see Wandsworth drug misuse clients. NHS Wandsworth will be engaging with Lambeth PCT contractors to help meet the needs of drug misuse prevalence in Queenstown Road.
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
98
7.10 Obesity
From the November 2009 Public Health report little is known about the prevalence of obesity in adults in Wandsworth, however modeling of the Health Survey for England data estimates the prevalence in Wandsworth adults is 14.2% which is lower than the estimated average for London (18.4%). The Faculty of Public Health‟s obesity calculation tool estimates that there are as many as 70,000 people in Wandsworth with a BMI over 30 kg/m2 (weight indicator for obesity accounting for height) and 100,000 people with a raised waist circumference (additional indicator of obesity).
7.11 Mental Health and Social Inclusion Promoting the social inclusion and wellbeing of people with severe and enduring mental health problems, including those from Black and Minority Ethnic (BME) groups, is a key criteria. This can be achieved by increasing access to healthcare, employment, mainstream education and training opportunities and voluntary work. This will involve providing enhanced mental health promotion, annual physical health checks, the engagement of BME communities in improving their mental wellbeing, increasing significantly the number of people supported into paid employment, education/training and voluntary work.
All community pharmacies support the PCT Mood Manager Programme which is a health promotion DVD designed to help patients make the most of their medication, gives ideas on coping strategies around better health, and information about local services. This is prescribed by giving to patients diagnosed with depression on presentation of their first prescription. Patients with certain types of mental health conditions may also experience difficulties with compliance with their medication regime. Supervised administration for patients who do not comply with their medication would improve their therapy.
PNA Commissioning Intentions – Community Pharmacy is in an ideal position to provide public health and medicines management services in obesity and weight management. Community pharmacists already provide informal weight management advice and services through sales of vitamins, dietary supplements, and patient access to weighing scales. The Community Pharmacy Pilot Obesity Service is now being reviewed. NHS Wandsworth is setting up a pilot weight management service which will be offering counselling, lifestyle advice and, where appropriate, pharmacotherapy through supply of Orlistat on a Patient Group Direction. Community pharmacists could support patients receiving pharmacotherapy for obesity through monitoring BMI, blood pressure and dietary advice in addition to counselling around the patient‟s medication.
PNA Commissioning Intentions – Community pharmacies in Wandsworth have supported the Mood Manager DVD programme. This should continue as a programme of health promotion through all pharmacies.
There is an opportunity to set up supervised dispensing for those patients who have compliance problems with their medication. The model would be similar to the supervised administration model for drug misusers. A shared care approach between prescribers in treatment agencies, the patient‟s GP, the client‟s social care work, and the community pharmacist would improve care around the patient.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
99
7.12 Cancer and Palliative Care The cancer register rate has increased between 2007 and 2009 in 12 out of the 20 Wandsworth wards. Community pharmacists support the care of cancer patients and the terminally ill by providing palliative care. In Wandsworth a network of 11 community pharmacies has been in place over the last 12 months to keep a formulary of palliative care drugs during their normal hours of operation. This provides improved access for patients, their carers and community nurses who have a need of community pharmacies. The map below compares the cancer rates against the distribution of the palliative care pharmacies. There is a good distribution of pharmacies providing this service across Wandsworth.
Fig 55: Map of palliative care pharmacies vs cancer rates
Figure 56 below shows the annual number of palliative care items dispensed by the palliative care pharmacy over the last few years. Palliative care items dispensed have been around 1,300 items or more a year.
Palliative Care Pharmacy
Earls Court out of hours pharmacy

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
100
Figure 56: Palliative care dispensing activity over the last four years
Out of hours access to palliative care medication is provided under a service level agreement with a 24 hours pharmacy in Earls Court. This is an example of cross-border commissioning.
7.13 Care Homes Currently there are 73 registered care homes in NHS Wandsworth serving 1,812 people. These homes require medicines for their patients and advice on storage and administration of medication. Community pharmacies provide for care homes by dispensing prescriptions for care home clients and giving advice on Care Home Medicines Policy. Some homes may require validated training. In 2005 NHS Wandsworth, in collaboration with the Primary Care Support Service, Sutton & Merton and Wandsworth LPC, and NHS Sutton & Merton, revised the audit procedures for accredited community pharmacists who provide services to care homes. In Wandsworth there are 16 registered care homes (serving a total of 1,061 patients) that receive pharmaceutical services. Currently there is under-utilisation of Wandsworth pharmacy contractors as more work is required around better integration of Community Pharmacy with a care home and the responsible GP practice. Pharmacy commissioning of care homes in Wandsworth is an area where local contractors need further inclusion into planning around medicines management.
PNA Commissioning Intentions - There will be more work to increase integration of the community pharmacy network into the end of life care network. The commissioned development support from the palliative care specialist pharmacist at Guys and St Thomas hospital will carry on as this has added value to the clinical practice of the community pharmacists.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
101
7.14 Health Outcomes and Inequality in Wandsworth
The level of mortality in a population is the most obvious health outcome used to compare between populations, for example in Wandsworth in 2010 approximately 2,500 people died. In addition the number and type of admissions to hospital reflect the immediate or acute need of the population of medical consultant led care; for example the people of Wandsworth generated 60,000 emergency hospital attendances in 2009/10. Many conditions and lifestyle choices contribute to premature mortality or the need for care in a hospital, and these are described more fully within the life-stage chapters to which they are most appropriate.
Mortality
Wandsworth residents experience slightly lower life expectancy (76 years male, 81 years female) than London (77 years male and 82 years female). Life expectancy increased between 2001-2005 to 2003-2007 by 0.7 years in males and 0.3 years in females (Source: APHO 2009). However, the picture in different wards varies: in Graveney, life expectancy decreased for both males and females, by 1.3 years and 1.1 years respectively. Male life expectancy has increased by the largest amount in West Hill (2.3 years) and female life expectancy has increased by the largest amount in Earlsfield (3.2 years).
PNA Commissioning Intentions – The care home pharmacy services is a gap in terms of service redesign. There needs to be a shared care arrangement, (analogous to care around drug misuse) where an accredited community pharmacy, GP practice, care home and relevant NHS and borough commissioners work together around the care of patients in care homes. This shared agreement will support closer integrated working around patient care. Care homes that need pharmaceutical services and advice include registered elderly care homes, registered nursing homes and care homes that serve patients with mental health, learning difficulties and children. These organisations will have pharmaceutical needs in terms of training of staff, handling and administration of medicines. Community pharmacists are in a position to link their current services to care homes with medicines management and NSF for the elderly. There are opportunities to provides focused medication reviews based on agreed local outcomes with GP practices. Focussed Medication Use Reviews in agreement with the GP practice and where the patient is able to participate in a medication review, should be developed to support better care of patients. There are opportunities for pharmacists with specialist skills to undertake independent reviews of care home prescribing, reviewing special formulations and advanced medication reviews where appropriate. There are opportunities to provide specialist pharmacy advice for care homes from acute trusts.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
102
The Standardised Mortality Ratio (SMR) for all-cause mortality for all ages and for the under 75s in Wandsworth are in line with the England rates, but worse than the London figures. For some specific conditions (circulatory disease, cancer, and stroke) the SMRs for Wandsworth indicate a higher rate of mortality than in London or England. The level of suicide in Wandsworth is relatively low, with a better SMR than for both London and England. (Source: NCHOD 2006-08)
Two targets for under-75 mortality were set out under Our Healthier Nation; circulatory disease and cancer. The circulatory target of 99 (DSR) has already been reached with a 2006-8 actual of 89 (DSR). The cancer target of 107 (DSR) has not yet been reached, with a 2006-8 based actual of 126 (DSR).
Latchmere has the highest under-75 SMRs for both males (165.4) and females (152.2), closely followed by West Hill (males at 155.1 and females at 127.4). The rates in West Hill may be distorted by the presence of the Royal Hospital for Neuro-Disabilities. Roehampton also has high SMRs for under-75s.
The pattern of mortality changes when considering the all-age SMRs. Whilst Latchmere remains high, wards such as St Mary‟s Park (males at 125.5 and females at 171.9) and Nightingale (males at 138.2 and females at 140.4) are highlighted. The high SMRs for Nightingale may be attributable to the large nursing home in this ward, but there is no evident explanation for the high SMRs in St Mary‟s Park.
Inequality
There are specific wards with poorer health outcomes and economic and social disadvantage. These wards have high levels of social housing, lone parents with dependent children, benefit-claiming households and low levels of educational attainment. There are also higher levels of over-crowding, greater numbers of black and minority ethnic residents and higher levels of long-term limiting illness. These deprived wards generate disproportionate numbers of children who become looked after by the council, and higher numbers of children in need who require ongoing support from the council. Evidence of the impact of this deprivation on health outcomes is clearly demonstrated by looking at observed mortality rates throughout Wandsworth and the associated level of deprivation.
The Index of Multiple Deprivation (IMD) provides a composite score of deprivation and is available at a low level of geography. Figure 57 below shows the percentage contribution of various causes of death to the life expectancy gap between the most and the least deprived quintiles in Wandsworth. The largest cause of years of life lost is coronary heart disease which contributes to over one year of the life expectancy gap for males and five months for females.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
103
Fig 57: Breakdown of life expectancy gap between the most and least deprived quintiles in Wandsworth by
cause of death
Hospital (acute) Care
Attendance rates at hospital are indicative both of the absolute level of need within the community as well as the effectiveness of community-based services in providing treatment without the need for hospital admission. Recording of hospital activity provides a breakdown into Accident and Emergency attendances, outpatient attendances, and admissions.
The Directly Standardised Rate (DSR) allows a comparison of two populations with differing age structures, an important calculation given the young population of Wandsworth (see table 15 below). Generally the DSR for outpatients, A&E and emergency admissions in Wandsworth is lower than for London and England (the exception being outpatient attendances, for which Wandsworth has a higher rate than England). The DSR for outpatient attendances and admissions for mental health conditions in Wandsworth is higher than London and England, suggesting that mental wellbeing remains a key issue for Wandsworth.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
104
Table 15: Hospital care activity 2009/10, Directly Standardised Rate per 1000 population
Activity Wandsworth Rate (Value)
London Rate
England Rate
Outpatient attendances 1145 (379,168) 1181 1047
Accident and Emergency attendances 314 (114,949) 327 368
Emergency admissions 66 (20,783) 80 86
Admissions for alcohol-related harm 1489 (3,375) 1490 1582
Mental health outpatient attendances 26 (9167 ) 16 22
Mental health admissions 2.3 (851 ) 2.2 1.9
Source: NHS comparators 2009/10, HES 2008/9, Local Alcohol Profiles England 2008/09
Recommended key areas of need (in no order of priority) Key areas of need Community pharmacy commissioning
response
Relatively low or poor health outcomes • High teenage conceptions (NI 112)
• High number of falls and fractured neck of femurs • Wandsworth has relatively high levels of
chlamydia, gonorrhoea, and syphilis. In particular the incidence of chlamydia for people above and below 25 is higher than Inner London.
• High <75 mortality for cancer (particularly female) (NI 122)
• High childhood obesity levels (NI 055 / 056) • Low childhood immunity for measles, mumps, and
rubella
Community Pharmacy EHC service Integration of Community Pharmacy in falls prevention Integrated Community Pharmacy sexual health service Health promotion Pharmacy integration into PCT obesity service Community pharmacies to provide additional capacity for vaccination
Worsening trend • Numbers of children with physical and learning
disabilities admitted to Wandsworth special schools
• Under 75 all-cause and cancer mortality • Number of people accessing HIV related care • Number of alcohol related hospital admissions (NI
39)
Medicines management Health promotion Alcohol screening through Community Pharmacy
Equality & diversity (age, disability, gender, geography) • Smoking prevalence correlated with deprivation
Community Pharmacy stop smoking

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
105
• Adult Social Care provision and correlation with
deprivation
• Disproportionate rate of mental health admissions in BME groups
• Low representation of 15-34 age group in
substance misuse services • Relatively low level of flu immunisation in the over
65 age group and those at risk
• Low % of people with learning disabilities in
employment (NI 146)
• Low % of people with learning disabilities in settled accommodation (NI 145)
network Revised health and social care signposting Focused health promotion through community pharmacies. Supervised administration programmes for mental health patients with medication compliance problems Health promotion, recruitment into service Community pharmacies to provide additional capacity for vaccination Revised health and social care signposting Revised health and social care signposting
Failure to meet targets which may contribute to poor outcomes • Carers receiving needs assessment (NI 135) • Independence for older people through
rehabilitation and intermediate care (NI 125) • Enabling people to be able to choose to die at
home. (NI 129) • Screening for cervical, bowel, and breast cancer,
and AAA • Breast symptom two week wait • Childhood immunisations • Breast feeding at 6/8 weeks (NI 053) • Pregnant women attending a 12 week maternity
appointment (NI 126)
Focused health screening and health promotion programmes through pharmacies in areas of deprivation

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
106
8. LOCALITY PROFILES AND POLYSYSTEMS The PNA regulations (paragraph 7(a), Schedule 3A) require PCTs to divide its area into localities. This will be used as the basis for decisions made on future contract applications. The decision taken by NHS Wandsworth is to divide the borough in line with the four Local Commissioning Groups (LCGs). This is in line with the JSNA and borough commissioning plans. This section will look at the needs of these localities and current provision of pharmacy services with commissioning recommendations for each locality. The four localities are:-
West Wandsworth (West Wandsworth Local Commissioning group) - SW15 SW19. Divided into Putney and Roehampton – while both are part of the same postcode there are clear differences in terms of housing, health and population. Also included is part of SW19. There will be a hub at a GP practice in Putney and at Queen Mary‟s Hospital.
Battersea (Battersea Local Commissioning group) – SW11 and SW8
Central Wandsworth – covering SW18 (Earlsfield and Southfields)
Balham, Tooting and Furzdown (SW17, SW12 and SW16)
Note these last two localities are covered by Wandle Commissioning Group. Fig 58: Polysystems in Wandsworth
The four polysystems groups for NHS Wandsworth are shown below with the number of pharmacies in each polysystem. Table 16: Number of pharmacies per locality
PBC GROUPS - Local Commissioning Groups
Number of Pharmacies
Battersea 14
West Wandsworth 15
Central Wandsworth 13
Balham, Tooting Furzedown 21

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
107
Fig 59: Locality boundaries within Wandsworth
The NHS-commissioned services are available across all polysystems in Wandsworth. Table 17: Pharmacy enhanced and advanced services across Wandsworth Battersea BTF Central
Putney & Rosehill
EN1 Supervised Administration Yes Yes Yes Yes
EN2 Needle & Syringe Exchange Yes Yes Yes Yes
EN3 Palliative Care Yes Yes Yes Yes
EN4 Stop Smoking Yes Yes Yes Yes
EN5 Care Home Yes Yes Yes Yes
EN6 Medicines Assessment & Compliance Support (MDS or dossette box) Yes Yes Yes Yes
EN7 Medication Review (Full Clinical Review) (being revised) No No No No
EN8 Minor Ailment Service Yes Yes Yes Yes
EN9 Out of Hours (TAKE PART IN ROTA (Access to Medicines) Yes Yes Yes Yes
EN10 Supplementary Prescribing by Pharmacists Not Started
EN11 EHC via PGD Yes Yes Yes Yes
EN12 Seasonal Influenza Vaccination No No No No
EN13 Patient Group Directions No No No No
EN14 Chlamydia Screening Yes Yes Yes Yes
EN15 NHS Health Check (Vascular risk assessment and management service) Being revised No No No No
Pharmacy asthma service (NHS) Yes Yes Yes Yes
NHS Weight management (being revised) No No Yes Yes
Advanced Services Medicines Use Review. Yes Yes Yes Yes

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
108
Table 18: Number of pharmacies providing enhanced and advanced services across the localities Battersea BTF Central
Putney & Rosehill
EN1 Supervised Administration 11/15 14/21 6/12 10/15
EN2 Needle & Syringe Exchange 3/15 2/21 2/12 3/15
EN3 Palliative Care 2/15 4/21 4/12 1/15
EN4 Stop Smoking 13/15 15/21 10/12 13/15
EN5 Care Home (service being revised)
4/15 8/21 3/12 3/15
EN6 Medicines Assessment & Compliance Support (MDS or dossette box)
11/15 5/21 1/12 7/15
EN7 Medication Review (Full Clinical Review)
0 0 0 0
EN8 Minor Ailment Service 14/15 16/21 7/12 11/15
EN9 Out of Hours (TAKE PART IN ROTA (Access to Medicines)
4/15 6/21 4/12 8/15
EN10 Supplementary prescribing by Pharmacists (not commissioned yet)
0 0 0 0
EN11 EHC via PGD 13/15 18/21 8/12 10/15
EN12 Seasonal Influenza Vaccination 0 0 0 0
EN13 Patient Group Directions 0 0 0 0
EN14 Chlamydia Screening Being Revised
EN15 NHS Health Check (Vascular risk assessment and management service)
Not Started
Pharmacy asthma service (NHS) 3/15 4/21 3/12 2/15
NHS Weight management Being Revised
Tables 17 and 18 above show the pharmacies providing locally enhanced services across Wandsworth as of January 2011. For individual pharmacy services details please see Appendix 11. For the services that are deemed necessary to meet the current needs of Wandsworth, there is very good access across Wandsworth and good provision in each locality or polysystem area.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
109
8.1 Locality Commissioning Groups and Polysystems Information is taken from the four Local Commissioning Group (LCG) plans written in July 2010. It should be noted that there were some differences in the layout of the plans. To ensure consistency the PNA has not made any changes to the layout but has added how Community Pharmacy and pharmacy providers can meet the health needs indentified in each polysystem. NHS Wandsworth is currently working on four polysystems. These developments will offer a wider range of services closer to patients‟ homes, and both walk-in and bookable doctor‟s appointments for longer hours every day in line with what local people need. The LCGs are setting up virtual wards for improved management of patient care. These services will include those that have normally only been provided by a hospital, like blood tests, x-rays and ultrasounds. The PCT is working on several polysystem developments. The Pharmaceutical Needs Assessment will be revised and amended in line with future polysystem developments. The 2008 Pharmacy Commissioning Toolkit for Polyclinics goes into detail about the approach taken to commission pharmacy services. It should be noted that pharmacy services cover a wide range of areas and sectors and should be designed and commissioned according to need. The Community Pharmacy Contractual Framework can provide a useful care package of services to localities and patients. These include:-
Pharmacy core services
Repeat dispensing
Medication Use Reviews
Health promotion
Minor ailments
Stop smoking
Emergency contraception
Pharmacy rota service
Pharmacy capacity o Premises – use of pharmacy consultation
rooms. o Pharmacy skill mix – pharmacy and non-
pharmacy staff o Medical equipment – blood pressure meters
In February 2010 the DH launched a suite of commissioning toolkits for Primary Care including a toolkit for pharmaceutical services. As part of high quality, patient-centred care, pharmacy forms an important part of the overall strategy to ensure safe, effective, fairer and more personalised patient care. Pharmacy has much more to offer than the safe and effective dispensing of medicines and is increasingly expanding its provision of clinical services, becoming a persuasive force in improving health and wellbeing. Pharmacists working on medicines management and providing prescribing support are assisting patients to take medicines more safely and effectively, as well as supporting evidence-based use of medicines by prescribers. The increasing number of pharmacist supplementary and independent prescribers is having a direct role in the management of individual patients‟ treatment and care. The commissioning of pharmaceutical services effectively is as important as the PCT‟s role in commissioning other primary care services. However, this area of commissioning is complex with a number of distinctive features that are unique to pharmaceutical services. NHS and borough commissioners will need to develop and strengthen their commissioning of pharmaceutical services if they are to maximise the opportunities for contributing to their population‟s health that pharmacy can offer.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
110
It should be noted that before any form of pharmacy commissioning can take place, a robust options appraisal should be carried out. Traditional dispensing models are often proposed when other pharmaceutical options such as access to specialist advice, specialist medication review or pharmacy-led diagnoses services may be more suitable. Pharmaceutical models of provision must comply with the Medicines Act as pharmacy is very heavily legislated. Acute and community pharmacy providers have different legislation which means there are certain activities they cannot do. The use of community pharmacies to provide rent to health centres or polysystem development is not a justifiable need or use of a community pharmacy. The majority of prescriptions are repeatable and with NHS repeat dispensing, patients will visit their pharmacies more times than visiting the GP practice for a check up. Electronic transfer of prescriptions will allow patients to nominate pharmacies to receive their electronic prescriptions. In an LCG there are pharmacy implications for prescribing, medicines management, supporting long-term conditions, medication reviews, urgent care and virtual wards. In terms of service stratification the pharmacy integration service model below will be applied to future development of pharmacy services. Fig3 60: Tony Carson pharmacy polysystem model
Pharmacy services in polysystem settings provide opportunities for service redesign, bringing in specialist skills from acute or tertiary care, enhancing the role of acute pharmacy and community pharmacy provision.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
111
Each Local Commissioning Group will have a community pharmacy and pharmacy representative to ensure that:-
o Contractually - Working with the LCG to maximise the Community Pharmacy Contractual Framework and locally enhanced services so they are focused locally and linked to outcomes. Focus on local priorities for the LCG and link this to pharmacy services
o Professionally – Making sure the best professional standards are reflected in the work
pharmacists do and services that they provide. This links in with the English Pharmacy Board and local practice forum approach to develop the highest level of clinical practice.
For the Local Commissioning Groups in Wandsworth, consideration will have to go to other pharmacy providers such as acute and specialist pharmacists.
8.2 West Wandsworth The West Wandsworth area covers Putney, Roehampton and West Hill. The polysystem is characterised by two distinct areas: one of high deprivation in the West and an area of low to mid-deprivation in the North and East of the polysystem. The population in the more deprived areas experience higher rates of chronic illness and higher rates of under-75 years old mortality. The least deprived areas are characterised by a healthy population that are also a healthy seeking population where most health needs are dealt with in Primary Care resulting in a low number of referrals. Information is presented by polysystem area, ward and GP practice within the polysystem. There is a good network of local community pharmacies located throughout SW15 and SW19 (Inner Park Road). There are three LPS contracts in SW15, two in Putney and one in Roehampton that cover the whole locality. The population in this locality has access to pharmacy services and there are some pharmacies in Putney and Roehampton open seven days a week. Patients in the north of Wandsworth can access a 24 hour pharmacy in Earls Court through existing public transport or via the PCT out of hours service.
PNA Commissioning Intentions – Practice-based commissioning (PBC) Bulletin 5 highlighted the importance of community pharmacy engagement with PBC cluster groups to ensure that the local community pharmacy network in engaged and kept aware of local commissioning developments. The DH has produced a Commissioning Toolkit for pharmacy services in polyclinics. The toolkit also emphasises the importance of stakeholder engagement. The Community Pharmacy Contractual Framework needs to be integrated more into PBC and polysystem workstreams.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
112
Population The West Wandsworth polysystem area has a registered population of 84,298 (M- 42696 F-41602).
Largest population groups are aged 25-34.
However the wards of East and West Putney and Roehampton have the highest proportions in the borough of people aged 65 years and older.
The 65 and over population in Thamesfield is projected to increase by 15% in the next ten years while in East and West Putney the younger population. (20-29 and 40-59 years) is projected to increase
Socio-economic Status
There are two areas of high deprivation in Wandsworth. One of these is located in the West Wandsworth polysystem area.
As a result the polysystem is defined by two distinct areas, one of high deprivation and one of low deprivation.
The high deprivation area covers the ward of Roehampton and the surrounding areas in the northern part of West Hill and the south-eastern area of West Putney.
The areas of low deprivation include Thamesfield, East Putney, and the majority of West Putney and West Hill.
68% (44,777) of the West Wandsworth population is white British.
West Hill is the most ethnically diverse ward.
East Putney has the highest proportion of white British population.
Standardised mortality ratios by underlying cause and polysystem (2003-07)
West Wandsworth records the highest female all-cause standardised mortality ratio in the under 75 year olds.
West Wandsworth records the lowest cancer standardised mortality ratio for all persons of all ages.
CVD is the biggest cause of death in West Wandsworth.
Source: Greater London Authority
-20.0% -15.0% -10.0% -5.0% 0.0% 5.0% 10.0% 15.0% 20.0%
85+
80-84
75-79
70-74
65-69
60-64
55-59
50-54
45-49
40-44
35-39
30-34
25-29
20-24
15-19
10-14
5-9
0-4
Percentage
Ag
e g
rou
pPopulation Distribution by Age and Gender, 2010. West Wandsworth
West Wandsworth West Wandsworth Women London Men London
Source: Department of Communities & Local Government
0
20
40
60
80
100
120
Male all cause mortality, <75
Female all cause mortality, <75
CHD, Males and Females, All Ages
Cancer, Males and Females, All Ages
CVD, Males and Females, All Ages
SMR by underlying cause and polysystemCentral Wandsworth West Wandsworth Balham Tooting & Furzedown Battersea

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
113
Under 75 cardiovascular disease mortality
Roehampton (164.7) has an under 75 years old CVD SMR that is significantly higher than the national average (= 100).
The Mayfield, Roehampton and Alton practices record high admissions for CHD.
These GP practices are all located in the high deprivation ward of Roehampton.
This is confirmed by a recent health needs assessment on CVD that found the ward of Roehampton had the greatest need in relation to the improvement of heart health and primary prevention of CVD.
QRISK2 scores (20% or greater risk of developing CVD over the next ten years) show GP practices in Roehampton have the largest proportions at risk. These are Mayfield, Roehampton, the Alton and Danebury practices.
GP registered smokers 2009
GP smoking data shows a clear distinction between prevalence at GP practices located in high deprivation areas and those not.
Danebury, Inner Park Road, Alton, Roehampton, Mayfield and Tudor Lodge practices all record prevalence above 25%.
GP practices located in less deprived areas record prevalence below 20%.
Smoking prevalence is under-reported across the borough; therefore it is possible this pattern may change if all patients were questioned about their smoking status.
Mapping smoking prevalence by area confirms higher prevalence in West Wandsworth coincides with the high deprivation areas in north West Hill and Roehampton.
8.2.1 Roehampton Information for Roehampton is taken from the April 2006 Roehampton Needs Assessment report and the April 2009 Picture of Health. The key facts about Roehampton are:-
The Roehampton ward is one of the five most deprived wards in Wandsworth (IMD 2004).
It is surrounded by more affluent wards
It has the second highest reported rate of crime in Putney and Roehampton
There are five housing estates, which in order of size are Alton, Ashburton, Putney Vale, Lennox and Eastwood
Roehampton has a higher percentage of 20-24 year olds compared to Wandsworth, whose largest percentage of population falls in the 25-34 age group.
In addition there is a new housing development on Roehampton Lane providing 447 new and refurbished houses and apartments, of which 24 are luxury homes. Based on local council figures (July 2007) the projected population is not expected to rise above 1% of the current value.
Source: EMIS Web.
Source: London Health Observatory
Source: EMIS Web.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
114
The April 2009 Picture of Health shows that there are five pharmacies located in Roehampton. Three pharmacies are located close to four GP practices. There is one pharmacy located in a housing estate and another in a supermarket just before the A3. Currently most patients do not have to walk far to get to a local pharmacy. Pharmacies in the area are providing a mixture of services such as:-
Minor ailments
Emergency contraception and chlamydia screening
Monitored dosage services
Asthma service
Services to drug misusers which include needle exchange and supervised administration
Pharmacy rota service
Stop smoking There is one LPS contract in this area. NHS Wandsworth was exploring the establishment of a polyclinic at Queen Mary‟s Hospital Roehampton as part of our commitment to improving health and enhancing access to services for the local population. As part of the development, which would have included a GP service at the polyclinic available 8am to 8pm, seven days per week, it was necessary to consider the supply of pharmaceutical services in the area. In September 2009, after careful consideration it was felt that there were sufficient pharmaceutical services in the local area and the addition of another pharmacy was therefore not feasible at this time. The PCT will be monitoring the local demand for pharmacy services as the polyclinic develops and will continually review this position for future provision. More work is required to integrate Community Pharmacy with polysystem provision in this area.
1) Population Roehampton
Population in 2009 13,248 No of people <18 years old 3,185 No of people 20-44 years old 5,161 No of people over the age of 65+ 1,750
Projected Population in 2012 13,312
% of population classifed as "White" 79.3 Index of Multiple Deprivation 2007 (rank in brackets, 1 most, 20 least) 31.7 (2)
General Practice (% PCT Total) 4 (8%)
Pharmacy (% PCT Total) 5 (8%)
Dentists (% PCT Total) 5 (10%)
Table 19: Picture of Health, April 2009 Roehampton

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
115
8.2.2 Putney, West Hill Putney covers four electoral wards which contain some of the most affluent wards in Wandsworth.
Table20 : Picture of Health, Putney April 2009
1) Population West Hill
West Putney
East Putney Thamesfield
Population in 2009 16,229 13,418 14,650 14,854 No of people <18 years old 3,456 3,081 2,102 2,660 No of people 20-44 years old 8,042 5,736 8,498 8,244 No of people aged 65+ 1,206 1,602 1,583 1,152
Projected Population in 2012 16,260 14,281 14,872 15,455
% of population classified as "White" (i.e. White British, White Irish, White Other) 78.6 86.5 86.3 91.8 Index of Multiple Deprivation 2007 (rank in brackets, 1 most, 20 least)
21.6 (8) 18.8 (12) 14.9 (16) 10.4 (20) Source: GLA 2007 Round Population Projections (2009 projected), Census 2001, IMD 2007
Table 21: Primary care contractors in West Hill
Ward
No of Community Pharmacies (% of total in NHS Wandsworth )
No of GP Practices (% of total in
NHS Wandsworth)
Dental Practices (% of total in NHS Wandsworth)
Optometrists (% of total in NHS Wandsworth )
Registered Population
(April 2008)
Ward Population (April 2009)
East Putney 1 1 1 0 14,650
West Putney 3 2 1 0 13,418
West Hill 2 2 1 0 16,229
Thamesfield 4 1 2 3 14,854
Patients can access pharmacies in the area. Services offered by pharmacies in the area include: -
Minor ailments
Emergency contraception and chlamydia screening
Monitored dosage services
Asthma service
Services to drug misusers which include needle exchange and supervised administration
Pharmacy rota service
Stop smoking
Current needs assessments shows there is no need for additional pharmacies in Putney as there is adequate provision. There are two LPS contracts in this area.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
116
8.2.3 West Wandsworth Needs Analysis and Local Pharmaceutical Commissioning Recommendations The West Wandsworth Local Commissioning delivery plan has provided information on needs for the area. The Local Commissioning delivery plan through consultation with local GPs has identified any significant gaps in service provision. This is due to the already developed community hospital/Polyclinic at Queen Mary‟s - with care provided close to patients‟ homes. This is true for both the Putney and Roehampton populations in general. There is generally little wait for outpatient appointments and diagnostics, and communication between the referring GPs and acute/diagnostic services is good. However the Health Needs Analysis indicates significant issues mainly associated with the deprivation in the Roehampton area, where key health needs are not being adequately addressed and require review and development of service provision. These include long-term condition management, particularly in relation to management of patients with COPD and aspects of CVD. Cancer screening and childhood immunisations are also issues that significant parts of the West Wandsworth population are failing to access and a plan to address is as outlined. The significant deprivation in the area also means issues such as teenage pregnancy and substance misuse are higher than in other parts of the borough and these are addressed in our five year plan. The identified gaps and/or areas for improvement of current service provision are detailed below alongside the community pharmacy commissioning response. The gaps from the Local Delivery Plan are also listed below: Priority Health Needs Local Population Community Pharmacy Core Service
Commissioning Recommendation
Mental health to include – Community Mental Health Teams, Psychological Therapies in Primary Care (PTiPC) and Child and Adolescent Mental Health Services (CAMHS)
Supervised administration for chaotic or vulnerable patients who are at risk of poor compliance of medication through an assessment. Health promotion advice and local signposting for patients. Supporting the PCT Mood Manager DVD initiative.
Cancer screening – including breast and cervical screening
Health promotion advice and local signposting for patients (essential services)
Increase life expectancy by targeting CVD prevention measures – including NHS healthchecks
One community pharmacy to undertake NHS healthchecks. Targeted MURs in agreement with local GPs (advanced services) Tier 3 medication reviews through Community Pharmacy or specialist pharmacist linked to long-term conditions

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
117
Health promotion advice and local signposting for patients (essential services) linking into Choosing Health through Community Pharmacy
Reduce smoking prevalence
Ongoing development of existing community pharmacy network to provide stop smoking services
Reduce obesity in adults and children
One to two community pharmacies offering a NHS weight management/obesity service
Address health issues of older population including bone health
Targeted MURs in agreement with local GPs (advanced services)
Ensure needs of the learning disability population are met
Health promotion advice and local signposting for patients (essential services)
Promote breastfeeding Health promotion advice and local signposting for patients (essential services)
Management of substance misuse – focus particularly on alcohol
One to two community pharmacies already providing supervised services to offer alcohol screening Development of pharmacy network to provide advice to drug misusers on harm reduction and staying healthy One community pharmacy to support Hepatitis C screening
Supporting NHS Wandsworth operating plan with regard to teenage pregnancy, ensuring choice of access to contraceptive services
Ongoing development of community pharmacy sexual health services such as emergency contraception and chlamydia screening and treatment
Local Delivery Plans Community Pharmacy Core Service Commissioning Recommendation
Urgent care (GP-Primary Care Service)
Key features of service delivery of urgent care within the West Wandsworth hub include (some still under development):
Open seven days a week, 8am – 8pm
One single point of entry to capture all patients and ensure they are managed through the polyclinic as seamlessly as possible
GP access for registered and unregistered
Review of minor ailment service and self care through Community Pharmacy Review of access to medicines outside normal working hours delivered through:-
Patient group directions for the Minor Injuries unit
GP out of hours service provision of

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
118
walk-in patients (as triaged), improving access and supporting choice (in line with the GPLHC model of care)
Full range of primary care urgent care services including the ability to see patients under the age of two
Nearby pharmacy providing advice and treatment for minor ailments as well as dispensing – aligned with polyclinic hours
GP out of hours services aligned to this model using facilities and community links
medication through medicine bags
Review of pharmacy rota system.
Hub and spoke model The hub for the West Wandsworth polysystem is already functioning and is located in Queen Mary‟s Hospital, Roehampton. Review, evaluation and redesign of care pathways and the service provision will continue on an ongoing basis as we seek to ensure inter-operability of services, effective communication and overall a streamlined patient experience within the hub and between the hub and the range of spokes within West Wandsworth. The spokes within West Wandsworth will comprise all the GP practices and a range of other health and social care providers.
Development of Community Pharmacy Contractual Framework to link into local care pathways. Integration of Community Pharmacy into virtual wards around medicines management, long-term conditions and self-care through minor ailments.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
119
8.3 Central Wandsworth There are four wards within Central Wandsworth (Fairfield, Southfields, Earlsfield and Wandsworth Common). There are ten general practices and 12 pharmacies in the Central Wandsworth polysystem. Across Central Wandsworth there is a good distribution of pharmacies offering a wide range of pharmacy services. There are three LPS contracts covering this locality and an Essential Small Pharmacy LPS (ESPLPS) contract in this locality. Patients in this locality have access to some pharmacies that are open seven days a week. The Central LCG report noted “Pharmacies will provide a crucial role in the development of the polysystem and the provision of primary care services”. This report seeks to provide structure and commissioning strategies to take this forward. Table 22
Population
Ethnicity by Ward
Source: Census 2001
67.83% 68.96% 67.51%
75.63%
10.02%13.05% 14.52%
10.68%3.09%
2.92% 2.81%
2.63%6.72%
4.84% 6.51%3.87%
10.35% 8.07% 6.80% 5.97%1.99% 2.15% 1.85% 1.22%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Earlsfield Fairfield Southfields Wandsworth Common
OTHER
BLACK
ASIAN
MIXED
White Other
White British
The practices within the Central Wandsworth polysystem have a GP registered population of 67,779 of which 70% are White British, with the remainder being of Black and Ethnic Minority origin. It is unclear at present how many residents are unregistered with a GP, within the four wards. The detailed breakdown of ethnicity by ward is given in the table opposite. Based on the index of multiple deprivations (IMD), these wards do not fall within the 20% of most deprived wards in Wandsworth. The Wandsworth map in Figure 1 highlights areas of high deprivation (measures include life expectancy, health outcomes, numbers in receipt of Jobseekers Allowance).
Picture of Health, April 2009
1) Population Earlsfield Fairfield Southfields Wandsworth
Common
Population in 2009 14,351 13,878 16,141 14,467 No of people <18 years old 2,532 2,061 3,121 3,214 No of people 20-44 years old 8,356 8,894 9,082 7,211 No of people aged 65+ 1,239 835 1,264 1,024
Projected Population in 2012 15,402 13,903 16,194 14,533 % of population classified as " White" (i.e. White British, White Irish, White Other) 77.9 82.0 82.0 86.3 Index of Multiple Deprivation 2007 (rank in brackets, 1 most, 20 least) 19.4 (11) 16.5 (13) 14.1 (18) 14.8 (17) Source: GLA 2007 Round Population Projections (2009 projected), Census 2001, IMD 2007

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
120
Primary Care 10 GP practices 12 community pharmacies (19% of community pharmacies in Wandsworth) 8 NHS dentists 4 opticians
There are four wards within Central Wandsworth (Fairfield, Southfields, Earlsfield and Wandsworth Common); based on the index of multiple deprivations (IMD), these wards do not fall within the 20% of most deprived wards in Wandsworth. The Wandsworth map highlights areas of high deprivation (measures include life expectancy, health outcomes, numbers in receipt of Jobseekers Allowance). Areas highlighted in red indicate the areas of highest deprivation.
The identified gaps and/or areas for improvement of current service provision are detailed below. The priority health needs identified for West Wandsworth include the following: The Health Needs Analysis shows that recorded prevalence of major long-term conditions (i.e. Diabetes, COPD, CHD, Stroke, Hypertension and severe mental illness) are either lower or comparable to the Wandsworth average. In addition, life expectancy and standardised all-cause mortality for both sexes are either comparable or better than the Wandsworth average. However, there are significant gaps between the recorded and estimated prevalence for all these conditions. To address this issue, emphasis needs to be placed on working with GPs and primary care clinicians to ensure prevalence of long-term conditions are recorded and added to practice disease registers. (Central LCG Commissioning report July 2010.) The Community Pharmacy and commissioning recommendations are listed below alongside gaps from the Local Delivery Plan which can be seen on the following page:
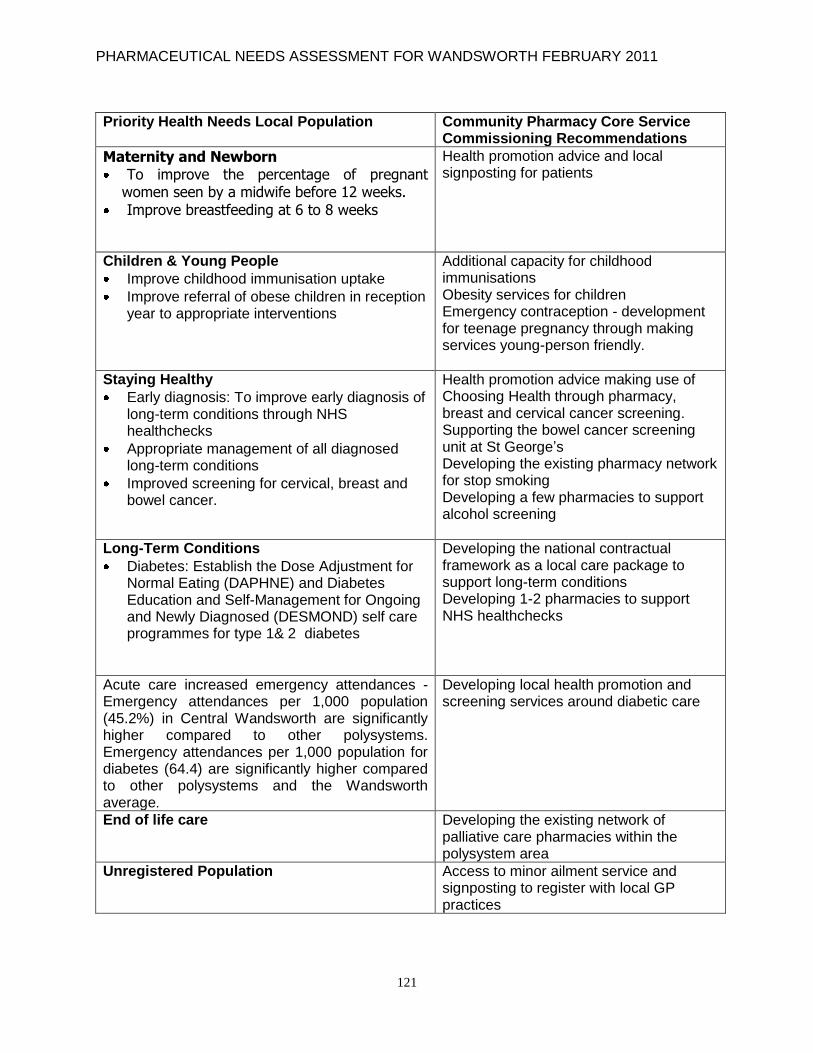
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
121
Priority Health Needs Local Population Community Pharmacy Core Service Commissioning Recommendations
Maternity and Newborn To improve the percentage of pregnant
women seen by a midwife before 12 weeks.
Improve breastfeeding at 6 to 8 weeks
Health promotion advice and local signposting for patients
Children & Young People
Improve childhood immunisation uptake
Improve referral of obese children in reception year to appropriate interventions
Additional capacity for childhood immunisations Obesity services for children Emergency contraception - development for teenage pregnancy through making services young-person friendly.
Staying Healthy
Early diagnosis: To improve early diagnosis of long-term conditions through NHS healthchecks
Appropriate management of all diagnosed long-term conditions
Improved screening for cervical, breast and bowel cancer.
Health promotion advice making use of Choosing Health through pharmacy, breast and cervical cancer screening. Supporting the bowel cancer screening unit at St George‟s Developing the existing pharmacy network for stop smoking Developing a few pharmacies to support alcohol screening
Long-Term Conditions
Diabetes: Establish the Dose Adjustment for Normal Eating (DAPHNE) and Diabetes Education and Self-Management for Ongoing and Newly Diagnosed (DESMOND) self care programmes for type 1& 2 diabetes
Developing the national contractual framework as a local care package to support long-term conditions Developing 1-2 pharmacies to support NHS healthchecks
Acute care increased emergency attendances - Emergency attendances per 1,000 population (45.2%) in Central Wandsworth are significantly higher compared to other polysystems. Emergency attendances per 1,000 population for diabetes (64.4) are significantly higher compared to other polysystems and the Wandsworth average.
Developing local health promotion and screening services around diabetic care
End of life care Developing the existing network of palliative care pharmacies within the polysystem area
Unregistered Population
Access to minor ailment service and signposting to register with local GP practices

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
122
Local Delivery Plans Community Pharmacy Core Service Commissioning Recommendations
Services for Ethnic Minorities – GPs have stated that lack of information in other languages (for example information about services available, and how to use choose & book) often causes difficulty in communication with BME groups
Making better use of languages spoken in community pharmacies. This will support compliance around medication.
Young Ethnic Minorities – Feedback has indicated that young ethnic minority groups would benefit from having information about sexual health issues available in a number of languages and in a format that is more accessible to both their age and ethnicity
Development of pharmacies proving EHC linking into pharmacies that can offer more than one language
Spirometry – There are gaps in service provision. GPs state this is due to the nurse time that it takes to perform a test (usually a 30 minute appointment). There is a risk that if funding via an LES (or equivalent) is taken away, the primary care service may cease, leading to patients attending hospital instead
Extension of LES to community pharmacies to provide additional capacity support
Health Visiting Clinics – Central Wandsworth only has three clinics at West Hill, Brocklebank and the Southfields Community College (the Aspire Centre), but large numbers of clients are seen at all of them
Improved integration and communication with local community pharmacies around medicines management, dressings and independent nurse prescribing.
Premises - A study of available estate across the PCT (an analysis of empty space in GP practices and PCT health centres) was commissioned and carried out in 2009, by the Strategic Services Partnership (SSP)
Inclusion of community pharmacies premises in terms of providing additional premises capacity
8.3.1 Services Provided
The services below are provided by local pharmacies. There is good coverage and access for patients in the Central Wandsworth locality.
Minor ailments
Emergency contraception and chlamydia screening
Monitored dosage services
Asthma service
Services to drug misusers which include needle exchange and supervised administration
Pharmacy rota service
Stop smoking

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
123
8.4 Balham, Tooting & Furzedown (BTF) BTF covers the postcodes of Balham Tooting and Furzedown. There are 21 community pharmacies in this locality. There are three LPS contracts covering this locality The Local Commissioning Plan acknowledged pharmacy and stated, “A pharmacy needs assessment [of pharmacies in Balham, Tooting and Furzedown] is currently underway and the outcomes from this work will identify the types of service they currently provide, in their respective locality. Details of the needs assessment for this locality are summarised below:-
Population
The practices within the Balham, Tooting and Furzedown [BTF] polysystem have a GP-registered population of 108,331 of which 54% are white British and the remainder from various black and ethnic minority [BME] groups. The number of non-registered residents living in the BTF district is unclear at present.
Area and Services
Two out of six wards in BTF (Tooting and Graveney) fall under 20% of the most deprived wards in Wandsworth based on the index of multiple deprivation 2007. Within the BTF districts there are in total 16 primary schools, two secondary schools and one special school.
Summary of Health Needs:
Maternity and Newborn
There were 1,780 singleton births in the BTF district, comprising 30.9% of the 5,759 singleton births in Wandsworth overall [Jan-Dec 2009].
Birth weight rate is low in BTF (9%) and comparable to the Wandsworth average.
The percentage of pregnant women seen by a midwife within 12 weeks of gestation (31.5%) is significantly lower in BTF, in comparison to other polysystems in the borough.
More often the actual delay in the system is the time it takes to be seen by a midwife, with an opportunity to review the post-referral process.
Breastfeeding prevalence at 6-8 week check (75.6%) is lower compared to Battersea (77.7%) but comparable to the Wandsworth average.
Children & Young People
Overall childhood immunisation uptake within the BTF district is comparable to other polysystems in the borough.
The uptake of DTaP/IPV/HiB at age one (92.6%) and MMR 1 at age two (87.6%) from 2009-10 data was better in comparison to Battersea and West Wandsworth.
However, the target for this financial year [2010-11] is 95% and further work is required to achieve this.
In the BTF district, especially in the ward of Tooting, obesity among reception-year children is very high (14%).
However, obesity among reception-year children in general across the BTF district is lower (8%) compared to the Wandsworth average (10%).
Obesity among children in Year 6 across the BTF district is 22%, which is 1% lower compared to the Wandsworth average (23%).
Teenage conception rate (61/1000) is significantly higher across the BTF district compared to other polysystems in the borough:
Central Wandsworth: 43

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
124
West Wandsworth: 45
Battersea: 75
However, it is comparable to the Wandsworth average (61).
Two wards within BTF (Nightingale (98) and Tooting (70), have a very high teenage conception rate.
Staying Healthy
Prevalence of smoking (22.46%) and binge drinking (15.3%) is lower in BTF compared to the Wandsworth average (22.9% and 16.5% respectively).
Majority of screening rates in BTF are comparable to the Wandsworth average, apart from breast screening:
Cervical: 70.3%, bowel: 38.5%, chlamydia: 1.1%, and retinal: 82.3% (compared to Wandsworth average (cervical: 72%, bowel: 40.4% , chlamydia:1.4%, retinal:86.5%))
Breast screening take-up is poorer in BTF (59.0%) compared to the Wandsworth average (58.2%).
Long-Term Conditions Recorded prevalence of major long-term conditions (i.e. Diabetes, COPD, CHD, Stroke, Hypertension and severe mental illness) are significantly higher compared to other polysystems and the Wandsworth average, as shown in the table below:-
Chronic conditions
Balham, Tooting & Furzedown
Central Wandsworth
West Wandsworth
Battersea Wandsworth average
Diabetes 48.13 35.33 28.75 32.26 36.65
COPD 7.05 8.28 10.51 7.55 8.24
CHD 17.36 14.38 18.10 13.34 15.74
Stroke 8.42 7.26 9.09 7.07 7.93
Hypertension 76.90 95.82 83.43 81.71 84.76
Severe Mental Illness [ Mental Health Register – prevalence]*
9.78 7.91 7.38 7.85 8.29
* Mental health indicator relates to number of people with schizophrenia, bipolar disorder and other psychoses.
Service Gaps
Local Developmental Plans Community Pharmacy Core Service Commissioning Recommendations
Diabetes - 7% of their local population are
diabetics, compared with the national average
of 3%.
Health promotion advice and local signposting for patients. Developing focused MURs according to local need

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
125
Developing a few community pharmacies to support diabetic screening through a screening service or through NHS healthchecks Commissioning of specialist roles through acute pharmacy. Developing local pharmacy network to support diabetic patients
Tuberculosis (TB) – Awareness within
general practitioners and allied healthcare
professionals. TB outreach activity in the
community
Extending TB screening through 1-2 community pharmacies
Teenage conception rate is significantly higher
across BTF
Emergency contraception development for teenage pregnancy through making services young-person friendly
Outreach clinic for hard-to-reach groups and
working in collaboration with 3rd sector and
community leaders
Exploring the premises and staffing capacity community pharmacy network could offer
Resource gaps:
Diabetics‟ resources within the community
Heart failure specialist nurses
HIV screening at registration
TB community outreach
Develop models of diabetic care through Community Pharmacy and specialist acute pharmacy services. Examples include developing NHS healthchecks, pharmacy screening services, and advanced medication reviews
8.4.1 Services Provided
The services below are provided by local pharmacies. There is good coverage and access for patients in this locality. There are some pharmacies that are open seven days a week.
Minor ailments
Emergency contraception and chlamydia screening
Monitored dosage services
Asthma service
Services to drug misusers which include needle exchange and supervised administration
Pharmacy rota service
Stop smoking

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
126
8.5 Battersea Battersea Local Commissioning Group covers SW11 and SW8 postcodes. It should be noted that one of the GP practices has opted out of this LCG and has joined Central LCG. One of the GP practices is located just within Lambeth but is registered to NHS Wandsworth. Fig 61: Map of the boundary of Battersea LCG
There are 14 pharmacies in Battersea, which compares well with the national average for the size of the population. There are two LPS contracts covering the locality. Pharmacies are well distributed across the area except for Northcote, which has double the number of pharmacies of any other ward in the area. The northern part of Queenstown ward has no pharmacies; however the area is bordered by Wandsworth Road in Lambeth which is home to a number of pharmacies. Services currently being provided by most pharmacies include minor ailments, smoking cessation, weight management, services for substance misusers, emergency contraception services and mental health promotion. It should be noted that as part of the needs assessment the PCT will explore commissioning of pharmacy services with Lambeth pharmacy contractors. As one GP practice is on the border with Wandsworth just within Lambeth, the NHS Lambeth pharmacies close to that practice could be commissioned to provide services for NHS Wandsworth.
NHS Wandsworth has been in regular contact with NHS Lambeth regarding pharmacies on the Lambeth side of the border whose custom could be mainly NHS Wandsworth patients. NHS Lambeth has replied to the PNA consultation making the following observations and recommendations:

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
127
NHS Lambeth Response to Consultation Jan 2011 'In terms of geographical distribution, there seems to be adequate provision along the Lambeth-Wandsworth border, with there being at least one pharmacy in the wards of Queenstown, Shaftesbury, Northcote, Balham, Bedford and Furzedown. In terms of opening hours, there seems to be sufficient access too with most of the pharmacies in Wandsworth, along the border with Lambeth, open late, until 6.00 pm Mondays to Fridays, and also open on Saturdays. With regards to service provision along the border, the services being commissioned in the Battersea, Balham, Tooting and Furzedown areas match those services commissioned widely in Lambeth, namely supervised administration, needle and syringe exchange, stop smoking, minor ailments, EHC via PGD and chlamydia screening, so this is to be welcomed. With regards to services commissioned by NHS Wandsworth and not NHS Lambeth, the services that we would like to commission, based on our PNA, and resources-permitting, include palliative care, advice to care homes, medicines assessment and compliance airs, and out of hours rota. With regards to services commissioned by NHS Lambeth and not NHS Wandsworth, resources-permitting NHS Wandsworth should consider commissioning a seasonal 'flu vaccination service to address service anomalies along the Lambeth-Wandsworth border in particular.'
Table 23: Primary care contractors in Battersea Source: GLA 2007 Round Population Projections 2009 projected), Census 2001, IMD 2007
Ward
Community Pharmacies (% of total in NHS Wandsworth)
GP Practices (% of total in NHS Wandsworth)
Dental Practices (% of total in NHS Wandsworth)
Optometrists (% of total in NHS Wandsworth)
Registered Population (April 2008)
Ward Population (April 2009)
Queenstown 1 2 1 16,807
St Mary`s Park 4 2 2 15,791
Latchmere
1 1 3
13,785
Shaftesbury 2 3 3 1 13,406
Northcote 5 2 2 4 13,923
Fairfield 1 1 1 0 13,878
Latchmere 1 1 1 0 13785

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
128
Table 24: Picture of Health, April 2009
1) Population Latchmere Queenstown St. Mary's
Park Shaftesbury Fairfield Northcote
Population in 2009 13,785 16,807 15,791 13,406 13,878 13,923 No of people <18 years old 3,299 3,127 2,487 1,929 2,061 3,176 No of people 20-44 years old 6,809 9,760 8,553 8,442 8,894 7,720 No of people aged 65+ 1,230 1,112 1,426 1,024 835 811 Projected Population in 2012 14,086 16,868 16,475 13,414 13,903 14,163 % of population classified as "White" (i.e. White British, White Irish, White Other) 63.8 70.8 77.5 85.0 82.0 86.3 Index of Multiple Deprivation 2007 (rank in brackets, 1 most, 20 least) 36.9 (1) 28.9 (3) 22.3 (7) 20.7 (9) 16.5 (13) 13.8 (19)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
129
Population demographics
Battersea has a population of 87,981 making it the second largest polysystem in Wandsworth. The population is young with 64% classified as White British, a similar proportion to Wandsworth as a whole. 57% of the population is described as a mobile group of well-educated single households or cohabiting couples without children, with little ill health except amongst older members. 17% are „urban professionals‟, a slightly younger version of the group described above, and 15% are „multicultural key workers‟ who are young parent families from minority ethnic groups, who are twice as likely as the national average to be unemployed, and amongst whom an above-average number of the working population have poor health or long-term illness.
Ethnic group
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Central Wandsworth West Wandsworth Balham, Tooting and Furzedown
Battersea Wandsworth
GLA 2007 Round Ethnic Group Projections by Polysystem
Other Ethnic Group
Chinese
Other Black
African
Caribbean
Other Asian
Bangladeshi
Pakistani
Indian
Mixed - Other Mixed
Mixed - White & Asian
Mixed - White & Black African
Mixed - White & Black Caribbean
White - Other White
White - Irish
White - British
168,000 people in Wandsworth are estimated to be white British, which represents 65% of the population. The percentage varies by polysystem, Central Wandsworth 70% (37,000) West Wandsworth 68% (45,000) Balham Tooting and Furzedown 59% (47,000), and Battersea 64% (40, 000). 14%, (9,000) of the population is black African/Caribbean/Black other. This rises to 25% of the population in Latchmere. Asians (Indian sub-continent and other) comprise approximately 4% of the population.
Socio-economic status Battersea has three of the six most deprived wards in the borough: Latchmere, Queenstown and St Mary‟s Park. The map of the 2007 version of the Index of Multiple Deprivation shows the pockets of highest deprivation in red throughout the borough. The average score for the borough is 20.4 and the polysystem with the highest IMD score is Battersea with a score of 23.3. There is considerable variation in practice deprivation score with Battersea Fields being the most deprived and Thurleigh Road the least.
-20.0% -15.0% -10.0% -5.0% 0.0% 5.0% 10.0% 15.0% 20.0%
85+
80-84
75-79
70-74
65-69
60-64
55-59
50-54
45-49
40-44
35-39
30-34
25-29
20-24
15-19
10-14
5-9
0-4
Percentage
Ag
e g
rou
p
Population Distribution by Age and Gender, 2010. Battersea
Battersea Battersea Women London Men London

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
130
Lifestyle Wards within this polysystem have the highest smoking prevalence rates within the borough. Wards in Battersea also have the highest rates of binge drinking and obesity across the borough. Smoking
0%
10%
20%
30%
40%
50%
60%
70%
Obesity (per 1000) Smoking Binge Drinking Sports Participation Fruit and Vegetable
Consumption
Pre
va
len
ce
Central Wandsworth
West Wandsworth
Balham Tooting & Furzedown
Battersea
Wandsworth
Mortality and causes of death
Circulatory disease and cancer are the major causes of death in Wandsworth. Battersea has the highest cancer and CVD standardised mortality ratios (SMRs all ages) in the borough. Latchmere ward has a much higher SMR than other wards in the polysystem and Queenstown ward has had a larger reduction in SMR than any other ward. There is also variation in cancer SMRs by ward, with a particularly high SMR in Latchmere ward.
Projections up to 2020 estimate that the prevalence of CHD and COPD is not likely to increase, but that diabetes prevalence will increase by 15% by 2025 and hypertension prevalence by 1.6% by 2020. The Quality and Outcomes Framework (QOF (GMS contract)) prevalence of long-term conditions within the polysystem does not vary significantly from the borough average. High proportions of patients with long-term conditions have either not been diagnosed or are not on the QOF registers: COPD 67%, diabetes 18%, CHD 41%, hypertension 56%.
0
20
40
60
80
100
120
Male all cause mortality, <75
Female all cause mortality, <75
CHD, Males and Females, All Ages
Cancer, Males and Females, All Ages
CVD, Males and Females, All Ages
SMR by underlying cause and polysystemCentral Wandsworth West Wandsworth Balham Tooting & Furzedown Battersea

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
131
8.5.1 Battersea LCG Identified Workplans.
Battersea LCG Identified Workplans Community Pharmacy Core Service Commissioning Recommendations
Drug Misuse Wandsworth‟s Drug and Alcohol Action Team (DAAT) currently has an accredited GP with Special Interest (GPSI) in post that is providing services to substance misusers. Most GP practices in Battersea have signed up to shared care of drug abusers working with the Substance Misuse Liaison Team and Wandsworth Drug and Alcohol Action Team. We will need to ensure all Battersea drug misuse patients are covered by this service.
Integrate the pharmacies providing needle exchange and supervised administration as part of a shared care agreement
Smoking Cessation
Targeting smoking cessation services at "at risk" communities
Recruit and train a network of stop smoking advisors in a variety of settings
Deliver Smoke Free Homes Project and Smoke Free Workplace Initiative, in line with national guidance
Improve availability of smoking cessation services in Primary Care and community services.
Actions
Coordinate, develop and sustain drop-in
clinics in deprived areas and areas with
high smoking prevalence (Latchmere,
Shaftsbury, Clapham Junction and
Fairfield)
Implement community mobilisation and
awareness campaigns for BME and other
communities
Pregnant smokers from low-income class
will be identified and supported to stop
smoking
Ensure that Battersea LCG Stop Smoking
Service has enough advisors, including
youth workers and key workers
Develop the existing pharmacy network further to work more flexibly Link community pharmacies into the Smoke Free Homes Project Develop closer integrated workings between community pharmacies and drop-in clinics Develop more local health promotion with BME communities and young people Explore co–location of drop-in clinics with local pharmacies Develop stop smoking services in pharmacies located in or near areas of deprivation Integrate the community pharmacy network into local stakeholder groups such as GPs, local councils and patient groups Increase pharmacy capacity further by contracting with NHS Lambeth pharmacies that see NHS Wandsworth patients

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
132
Work with council and local businesses
Provide information and in-house support, train staff
Work with pharmacy and dental teams to
increase the capacity for service provision
Roll out successful smoking cessation pilot
undertaken in the Lavender Hill practice to
the practices in the area of highest
smoking prevalence
Map area and practices with greatest
smoking prevalence and ensure service
delivered where there is greatest need
Develop smoking cessation service for
pregnant smokers and young smokers,
including working with school nurses
Train children, young people and health
visitors using Smoke Free Homes Toolkit
Reducing the proportion of undiagnosed CVD Actions Implement a Vascular Risk Assessment (VRA) programme across Wandsworth. Full implementation of programme by 2012/13 Ensure that the appropriate software is installed and used by GPs to develop GP information systems to enable the rapid identification of eligible patients. Governance and workforce development
Develop 1- 2 community pharmacies to provide NHS healthchecks Focus local community pharmacies around medicines management issues
Tackling Mental Health The proportion of patients from BME groups admitted to acute adult wards / detained under section in the last three years has been more than double that of the general population of Wandsworth. Actions Education programme for staff. Develop more appropriate and responsive services for BME population. Provide better response to disadvantaged groups e.g. BME, deaf people.
Develop local health promotion and make use of Mood Manager programme. Develop focused MURs and compliance and concordance for patients Explore supervised administration

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
133
Develop capacity in primary care to treat people with mental illness. Ensure adult Early Intervention service achieves target number of clients
Sexual Health Reducing undiagnosed HIV and increasing early diagnosis of HIV. Access to 48 hour GUM clinics Reduce late diagnosis of HIV and improve health and social care for people living with HIV Maintain 100% access target and increase availability of GUM services in community Increase awareness among professionals by promoting explicit criteria for HIV testing in primary care Increased access to EHC (emergency hormonal contraception) in community settings e.g. pharmacies Participate in SHS service development Develop sexual health services, and implement revised new model of family planning / community sexual health provision.
Integrate community pharmacies providing EHC and chlamydia screening into a local sexual health network Develop referral pathways between reproductive sexual health and local pharmacies stratified to patient and clinical risk Develop local health promotion and signposting
Long-Term Conditions The aim of Battersea LCG is to commission services that address the following population needs:
People enjoy improved quality of life, health and wellbeing and are more independent
People are supported and educated to care for themselves (self-care) and make decisions about their support
People have choice and control over their care and support with services built around their needs
People can design their care around health and social care services that are integrated, flexible, proactive and
Re-develop the Community Pharmacy Contractual Framework around each long-term condition Develop local health promotion programmes and signposting.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
134
responsive to individual needs
People are offered health and social care services that are high quality, efficient and sustainable.
Extended Hours The GP-led Junction Health Centre opened in April 2010, providing extended access 8.00am to 8.00pm seven days a week, and provides services for both registered and unregistered patients. Extended hours are also provided at BLHC and Thurliegh Road practices. Battersea LCG is committed to improving same-day „urgent‟ care access for our patients and plans to achieve this via three main goals: 1. Improve access for patients during „core‟
practice hours, thereby reducing A&E
attendances which peak at around
11:00am. This will be done via an initial
review of practice procedures,
benchmarked against nationally
recognised good practice (ref. Dr Carson,
Primary Care Foundation).
2. Target specific high users of A&E to
develop an effective primary care pathway.
This is expected to be paediatric patients
(those under 16, though target age group
may be refined down). Evidence has
shown that community paediatric clinics
can be effective, with the main enabler
being a targeted marketing campaign.
3. Review extended hours Mon-Fri (focus on
6.30-8.00pm) to reduce A&E attendances.
Presently, the access to LES and DES is
for booked appointments, which are a
different cohort to the type of patients who
require a walk-in / same-day appointment.
We will explore local options for providing
greater „extended‟ access for patients
requiring a walk-in or same-day
appointment.
The Community Pharmacy Rota will be adjusted to meet local needs. Develop pharmacy extended LES More planning is required for this locally Better use of the minor ailments service to shift minor conditions to pharmacies within and outside Battersea who serve the locality Link the minor ailments conditions to A&E. Explore other forms of pharmaceutical commissioning around access to medicines out of hours.
Pharmacy extended rota
Patient group directions for nurses working in walk-in centres.
GP medication bags for out of hours GP services.
Make best use of repeat dispensing.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
135
Battersea LCG Identified Gaps Community Pharmacy Core Service Commissioning Recommendations
A group of ten GPs and nurses considered where they perceived gaps in present service provision. This included where they identified a total lack of service in an area where they identified need as well as where greater screening and service could be developed in primary care if resources were available. The gaps identified are in no particular order:
Dementia – memory screening clinic
Speech and language therapy for adults without neurological condition
Psychosexual counselling
HIV counselling in community (possible dual role with service above?)
Perinatal mental health care
Psychiatric and psychology service that is integrated and comprehensive
Occupational therapy service for children
Outreach clinics for hard-to-reach groups in Asda, Battersea Park etc.
Resource Gaps
Alcohol screening (since LES stopped there has been a 30% reduction in referrals to Fresh Start Clinic)
HIV screening at registration in Primary Care
Identify patients at registration with smoking history who should be offered spirometry
Spirometry screening of asthmatics when at risk of COPD
Diabetes screening at registration for patients
Gaps Identified Throughout the Battersea LCG Document
Diagnostic services
Lack of robust community service providers for the shift of care
Lack of suitable premises to deliver extra activity
Community pharmacies to provide access through use of consulting rooms and premises Explore co-location of clinics in pharmacies in this locality by making use of counselling rooms Extend alcohol screening LES to 1-2 pharmacies in Battersea Link spirometry to pharmacies offering stop smoking as part of COPD Link NHS Health checks/ diabetic screening service. Scope out community pharmacy contribution to shift of care. Map community pharmacies with consulting rooms and link to local premises strategy

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
136
8.5.2 Services Provided
The services below are provided by local pharmacies. There is good coverage and access for patients in this locality. There are some pharmacies that are open seven days a week.
Minor ailments
Emergency contraception and chlamydia screening
Monitored dosage services
Asthma service
Services to drug misusers which include needle exchange and supervised administration
Pharmacy rota service
Stop smoking
There are two LPS contracts covering the whole of the locality. There are opportunities to commission pharmacies in Lambeth that are very close to the Wandsworth border, to provide minor ailments, supervised administration, needle exchange and stop smoking for NHS Wandsworth patients. It is recommended that NHS and borough commissioners covering Wandsworth and Lambeth work together to ensure that patients who live on the border area are not denied services and that the pharmacy network located either side of the border in both neighbouring areas are fully utilised to meet patient need.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
137
9. NHS WANDSWORTH AND WANDSWORTH COUNCIL The following section looks at NHS Wandsworth‟s strategy for primary care, public health and medicines management, and how Community Pharmacy can provide suitable pharmaceutical services. 9.1 NHS Wandsworth Commissioning Strategic Plan (CSP) NHS Wandsworth aims to achieve this vision through five goals within the Commissioning Strategic Priorities (CSP) (reference 10). 1. Improve life expectancy over and above the expected trends and focus on a greater health
gain for those in deprived wards. 2. Ensure young people enter adulthood in a state of health that enables them to reach their
full potential. 3. Improve the quality and responsiveness of services that address mental wellbeing, sexual
health, drugs, alcohol and obesity. 4. Improve access to, and the responsiveness of, GPs and other primary care services. 5. Improve the quality of services for people living with complex and long-term conditions. NHS Wandsworth‟s approach to the way patients are serviced is covered below.
(See Appendix 8). 9.2 Community Pharmacy Contractual Framework vs. NHS Wandsworth CSP The Community Pharmacy Contractual Framework has been mapped against the five NHS Wandsworth CSP goals. This shows the potential value and contribution Community Pharmacy can make to the commissioning plans of Wandsworth.
Our Vision NHS Wandsworth‟s vision is to transform the health of people living and working in
Wandsworth. We will work with local people, communities and our partners to deliver high quality services that are patient centred, safe and innovative. We want all our local
communities to be ambitious about their own health and to challenge us to commission the best possible care in the best possible environments within our resources.
Our Values In partnership with staff, key clinicians and partners we have developed our values to
underpin our commissioning approach: outward-looking, focused on high quality outcomes, based on honesty and integrity, trustworthy and open, person-centred and listening,
collaborative, innovative and professional.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
138
Table 25: Mapping of Community Pharmacy Contractual Framework vs CSP/PCT targets/Public Health
COMMUNITY PHARMACY CONTRACTUAL FRAMEWORK SERVICE
CSP Goals Public Health
National Target & Key Priorities e.g. accessing smoking BBV 18 weeks LCG delivery plans(LCG)
ES1 DISPENSING CSP1 Supporting Prescribing savings, LCG
ES2 REPEAT DISPENSING CSP1,4 Supporting Prescribing savings, improve access to medicines LCG
ES3 HEALTH PROMOTION CSP1,2,3,5 Y LCG
ES4 SIGNPOSTING CSP1,2,3,4,5 Y LCG
ES5 SUPPORT FOR SELF CARE CSP1,2,3,4,5 Y LCG
ES6 DISPOSAL OF UNWANTED MEDICINES
CSP1,3,5 Y Environmental Agency- regulations
ES7 – SUPPORT FOR DISABILITIES
ES8 CLINICAL GOVERANCE Quality Care Commission /NPSA alerts Safeguarding Children/Environmental waste/Contracting.
ADVANCED SERVICES CSP1,4,5 Y Developed with Long Term conditions/ service redesign/ LCG/Prescribing savings
COMMUNITY PHARMACY CONTRACTUAL FRAMEWORK LOCALLY ENHANCED SERVICE
CSP Goals Public Health
National Target & Key Priorities e.g. access smoking BBV 18 weeks LCG delivery plans(LCG)
EN1 Supervised Administration CSP1,2,3 Y LCG
EN2 Needle & Syringe Exchange CSP1, 2,3,5 Y LCG
EN3 Palliative Care CSP1,5 Y LCG, End of Life care
EN4 Stop Smoking CSP1,2,3,5 Y PCT target, LCG
EN5 Care Home CSP1,5 Care of Elderly/Medicines management
EN6 Medicines Assessment & Compliance Support
CSP1,5 Y Medicines management
EN7 Medication Review (Full Clinical Review)
CSP1 ,5 Y Medicines management
EN8 Minor Ailment Service CSP1 ,2 Y Access/demand management/urgent care
EN10 Supplementary Prescribing by Pharmacists
CSP1 Medicines management/Improving access to medicines
EN9 Out of Hours (Access to Medicines)
CSP1,5 Y Urgent care
EN11 EHC via PGD CSP1,2,3 Y Teenage pregnancy/Urgent care/LCG
EN12 Seasonal Influenza Vaccination CSP1,4 Y PCT Flu campaign/extra capacity
EN13 Patient Group Directions CSP1,2,3,4 Medicines management
EN14 Chlamydia Screening & Treatment
CSP1,3 Y PCT Chlamydia screening target/LCH
EN15 NHS Healthchecks CSP1,4 ,5 Y Pharmacy White paper/LCG
The CSP mapping exercise shows how each activity and service line of the Community Pharmacy Contractual Framework can support PCT objectives. This has major implications for any service redesign or pathway review; if medicines are involved as part of service redesign then there needs to be a consideration of the services that Community Pharmacy currently

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
139
provide. All NHS Wandsworth community pharmacy locally enhanced services are linked to the relevant CSP goal(s). 9.3 Primary Care This section looks at the key issues that Community Pharmacy support in Primary Care. Note that polysystems have already been discussed and linked to pharmacy localities. Fig 62: Map of NHS Wandsworth primary care contractors
The map above shows the four main Primary Care Contractor Groups which include general practice, high street dentists, community pharmacies and opticians. Table 26: Primary Care contractor groups in Wandsworth
Contractor Groups Number of Contracts
General Practice 48
High Street Dentists 49
Community Pharmacy Appliance Contractor –
63 1
Opticians 30 High Street/31 Domiciliary contracts

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
140
While dentists and opticians have specialist roles, general practitioners and community pharmacists have a more general role in healthcare, covering long-term conditions, sexual health, stop smoking and prescriptions. Other examples of Primary Care collaboration
In 2009 the minor ailment service was revised to include referral to an NHS dentist for patients presenting with mouth ulcers.
An NHS dentist presented at a community pharmacy forum on oral care and appropriate referral to dentists. The Local Pharmaceutical Committee has invited a Local Dental Committee Secretary to look at opportunities for joint-working.
Community pharmacies took part in Oral Health Promotion. It should be noted that dental practitioners can prescribe and opticians can be non-medical prescribers and will need to be considered in medicines management.
PNA Commissioning Intentions – More professional links need to be established between community pharmacists and dentists and opticians. Development of the minor ailment service could be expanded to include dispositions for oral and dental care in professional partnership with dentists and opticians. Agreed referral pathways between community pharmacies, dentists and opticians could be used to identify serious oral care conditions or optical conditions and refer patients appropriately to a professional.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
141
9.3.1 General Practice Fig 63: Map of community pharmacies and general practitioners
The above map shows community pharmacies mapped with GP practices. In Primary Care the biggest interface for Community Pharmacy is with general practice. In January 2009 NHS employers along with the British Medical Association (BMA) and the Pharmaceutical Services Negotiating Committee (PSNC) wrote an open letter to GP practices and community pharmacies to encourage better joint-working around the following (see Appendix 9):- Table 27: Areas for joint-working between GPs and Community Pharmacy
Polysystem commissioning
New service awareness and referral pathways
Vascular risk assessment checks developing care pathways to deliver care closer to home
Managing minor illness and care pathways for minor illness
Minimising medication waste, supporting patient adherence through the use of safe and appropriate compliance aids
Discussions on specific medicines e.g. warfarin, methotrexate or other high risk drugs where pharmacy and general practice can improve patient safety by working together
Repeat dispensing and robust repeat prescription ordering
Electronic prescription service
Medicines use reviews (MURs) and how to target patients in local priority groups
Locally organised multi-disciplinary audits

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
142
Further guidance has been produced on repeat dispensing and MURs for GPs and community pharmacies by NHS employers (see Appendix 9). This will support closer integrated working and will be of importance to support GP-led commissioning developments around medicines management and prescribing. There are opportunities to link the Community Pharmacy Contractual Framework and GMS contract to support patient care. It is important to make sure that there is no duplication between the contracts, but harmonisation. Community Pharmacy can support general practice and Primary Care through the following activities:-
Supporting the management of the prescribing budget through interventions, working with GPs to reduce the cost of special medicines, effective repeat dispensing and prescription systems
Taking pressure off general practice, thereby improving access e.g. minor ailments, patient group directions for emergency contraception and nicotine replacement therapy
Improving the recording of a patient‟s health status e.g. medications review, smoking cessation, weight management, screening services
Access and convenience to patients e.g. repeat dispensing, emergency contraception, screening and diagnostic services e.g. anticoagulation
Feedback from the Local Medical Committee/GP Practices There was substantive discussion and feedback from the Local Medical Committee. Key points are listed below:-
Strategic planning around the GP/Community Pharmacy interface in terms of referrals, communication and long-term conditions
Avoiding duplication of effort with GP practices and ensuring resources are utilised effectively
Contractual differences between the GMS contract and Community Pharmacy Contractual Framework
The importance of focusing on outcomes.
Communication back to GP practices regarding key clinical information and linking into EMIS (GP IT system used in NHS Wandsworth)
The PNA has already clarified that most pharmacy services are related to Community Pharmacy practice, but has made strong recommendations for more joint-working with GPs around patient care. For example:
Locally agreed outcomes with GP practices for MURs
Joint planning around long-term conditions
Robust repeat ordering systems for medication adhering to the local GP practice policy
Improving the use of medicines, which community pharmacists could support
Agreeing criteria for communication between community pharmacies and GP practices
Integration of pharmacy systems with EMIS to facilitate transfer of clinical information
Ensuring all pharmacy services are focused on local outcomes

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
143
GP practice – Key feedback
Managing repeat medication and ordering as part of controlling prescribing costs
Robust patient delivery services
Communication with practices – e.g. out of stock medicines, prices of special medicines, clinical information and feedback
Robust advice around minor ailments and conditions The key amendment to the PNA is for more joined-up work and planning around the GP and Community Pharmacy interface. It should be noted that the Local Pharmaceutical Committee made the following comments in their feedback on the PNA: “The LPC welcomes the comments made on better usage of the Community Pharmacy
Contractual Framework. A better understanding of how medicine use reviews can be
targeted and linked into the GPs GMS and PMS contract would be useful to build better
professional links with General Practice.”(MSW LPC response to Consultation Jan 2011)
There is clearly willingness from Community Pharmacy to work with general practitioners and to have a more meaningful discussion about integrated working around patient care. This discussion is now vital so that different professional groups are working together, which will improve communication and lead to a community pharmacy network in each local commissioning area that is an important contribution towards patient care.
PNA Commissioning Intentions – NHS Wandsworth is in an ideal position to facilitate partnerships and services between general practice and Community Pharmacy. This will support an integrated primary care vision, more collaboration between professions, efficient budgeting and funding. Local contractual changes are required to integrate the Community Pharmacy Contractual Framework and GMS contract, which can support the management of the prescribing budget and can look at where both professions can support patient care. Repeat dispensing and more developed and focused MURs need to be taken forward with GP practices. Community pharmacies have made a major contribution to a reduction in the cost of special medicines. There are more opportunities for GP practices to involve community pharmacies in patient care, and to work together and improve patient care and use of medicines.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
144
9.3.2 Tooting Walk-in Centre/Minor Injuries Unit Community Pharmacy can take pressure off walk-in centres in the same way as it can take pressure off GPs. Community pharmacies should also be regarded as walk-in centres as they show the following similarities:
Table 28: Comparison between walk-in centres and community pharmacies
Walk-in centre Community Pharmacy
Nurse-run Pharmacist-run
Primary care service Primary care service
Accessible service Accessible service
Patient access into the NHS Patient access into the NHS
Walk-in population Walk-in population
Minor ailments Minor ailments
Minor injuries and wound care Medication advice and counter prescribing
Health care advice Health care advice
Health promotion Health promotion
(See reference 11)
Both organisations are demand-led services. In addition, community pharmacists can supply emergency hormonal contraception (EHC) against a patient group direction. 9.3.3 Self Care, Minor Conditions and Minor Ailments The role of Community Pharmacy in managing minor conditions and minor ailments has been well documented. The Pharmacy White Paper April 2008 identified the following:-
Pharmacy’s ready availability in more deprived areas offers enormous potential on which to capitalise and expand access to healthcare services for more disadvantaged groups or those who do not regularly use other health services
From the survey of public use and attitudes conducted for this White Paper it is also clear that public knowledge and confidence in what pharmacy has to offer in terms of improved clinical services and facilities needs gradual build-up.
The recent Bow Group report on „Delivering Enhanced Pharmacy Services in a Modern NHS: Improving Outcomes in Public Health and Long-Term Conditions‟ (reference 20) identified the following: It is estimated annually that 57 million GP consultations concern minor ailments, which in large could be dealt with at a pharmacy. The average cost of a pharmacy consultation (£17.75) versus an average GP consultation (£32) is £14.25 less expensive. If all patients with minor ailments received pharmacy consultations, then over £812 million could potentially be saved from the NHS budget equating to over 4% of the Government’s pledged £20 billion efficiency savings target.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
145
In terms of shift of care, minor conditions and ailments managed through Community Pharmacy could make better use of pharmacies and free up more valuable time with local GPs who are also taking on shift of care for some acute services. Fig 64: A map of minor ailments pharmacies
The minor ailments service will be adapted to meet local needs and outcomes. Based on studies over the last few years:-
The majority of minor ailment consultations took place in areas of deprivation
Access to this service offered equitably across Wandsworth to support patient access
Support for drug misusers and rough sleepers who access the needle exchange service identified that access to certain treatments through minor ailments was required
More local development between GP practices and community pharmacies was needed to develop referral pathways.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
146
9.3.4 Virtual Health Wards
The Virtual Ward aims to reduce admissions to St George‟s Hospital by identifying patients who are at high risk and managing them more effectively in the community.
The Community Virtual Ward reproduces the strengths of a hospital ward in the community by using a multi-disciplinary team approach in healthcare provision. It is called "virtual" because the ward does not exist physically and patients remain in their home.
Dr Geraint Lewis originally conceived the idea in 2006 in Croydon. Many similar wards now exist in the UK and abroad but these do not include a GP. The Wandsworth Virtual Ward will involve the addition of a GP to the current community health team. This new concept was developed by Dr Seth Rankin (Project Clinical Lead) and Deborah Hoadley (PBC Management Lead for Battersea). The four wards in the project cover Wandle, Roehampton, Battersea and South Wandsworth.
PNA Commissioning Intentions – The minor ailments service is a necessary service to meet current need for NHS Wandsworth-registered patients and patients resident in Wandsworth. Community Pharmacy‟s role in minor ailments management needs to be factored into primary care demand management, urgent care and shift of care planning. The service should be focused around key patient groups and professions:-
Drug misusers – A basic minor ailments service could be provided through community pharmacies linked to improving general health, particularly of these clients
Homeless/rough sleepers – This group will not be registered to GP practices, so community pharmacies could provide access to support for minor ailments and self care for this group
Key ethnic communities – Community pharmacies could work more closely with Public Health outreach workers to improve access to minor conditions to key patient ethic groups who do not access Primary Care
Dental profession – High Street dentists and the community dental service could refer clients for oral care after diagnosis by a dentist e.g uncomplicated mouth ulcers, gingivitis and basic oral care. There are some dental products on the minor ailments formulary
Opticians – High Street opticians could refer minor eye conditions back to pharmacies through appropriate referral pathways.
The above changes will focus the minor ailment service on care where it is needed and improve outcomes.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
147
The core team consists of a GP, community matron and ward clerk who will do daily ward rounds and weekly MDT meetings, where all the community health professionals will be invited, including the district nurses, specialist nurses, physiotherapist, occupational therapist, social workers, intermediate care team, pharmacist etc. Information from these meetings would then be communicated directly to the patients‟ registered GP by updating their EMIS notes.
Appropriate patients for virtual wards
Above the age of 18 years at risk of readmission
Community Matron‟s current case load of patients
Patients selected using computer-generated predictive tools (Combined Model and PARR data)
GPs‟ referrals
Perceived benefits
More effective communication between GPs, secondary care and community services
Reduction of avoidable hospital admissions
Improved patient health and satisfaction with the health services
Avoidance of duplication of work and optimising use of resources
Increased support for healthcare professionals in the community Currently integration of community pharmacy in this development needs to be taken forward. Key areas where Community pharmacy could support virtual wards by working with identified high risk patients around medicines include through the following areas:-
Focussed Medicines Use reviews carried out in the pharmacy or in patient homes.
Medicines compliance assessment to monitor patients medication adherence
Medication waste reduction through compliance monitoring identifying unused medication, medication synchronisation and NHS repeat dispensing.
Focussing Medicines Use reviews around discharge of medication, The above areas would be at no additional cost as this makes better use of the National Contractual framework. There are opportunities to bring the skills of Pharmacists working in acute settings who may have experience around working with Long Term condition disease groups, mental health and Long Term care of the elderly.
PNA Commissioning Intentions – In Wandsworth all prescribing advisors are attached to virtual wards. Community Pharmacy and acute pharmacy need to be integrated more into the virtual ward setting. Areas that need to be considered include medicines management, integration of MURS and repeat dispensing. These systems would support the reduction of patient admission to hospital.
Further analysis of high risk patients and their associated care plans is required to produce a pharmaceutical service model to need the needs of this demanding patient group.
There needs to be clear communication and between the Primary care Virtual ward team and pharmacy provides working in acute and Community settings.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
148
9.3.5 Information Technology. There is a Primary Care IT strategy which focuses mainly around GPs. All GPs in Wandsworth use EMIS and have clear policies around information governance and data sharing. The community IT infrastructure has different arrangements:-
Community pharmacies must provide Release 1 and Release 2 compliant systems
Currently the majority of pharmacy services are still paper-based and, as has been discussed in this report, the PCT will be automating these services to speed up data analysis and billing
All community pharmacies are being encouraged to be moved onto NHS net email accounts to receive PCT communication, transfer patient sensitive data and to receive drug alerts
Experience of community pharmacy services has shown that minor ailments, emergency contraception and stop smoking generate the most paperwork. Automation to a paperless system will improve data collection, public health analysis and invoicing. Setting up an IT platform for community pharmacy services offers the opportunity for electronic communication with GP systems. PNA Commissioning Intentions – Automation of pharmacy services is urgently required to facilitate data collection, analysis and performance management. More scoping work is required to explore the communication and IT interface between GP IT systems and community pharmacies.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
149
9.4 Public Health and Wandsworth Borough Council The relationship between Public Health and pharmacy is a very important one. If the public health activity is mapped against the Community Pharmacy Contractual Framework (below), it can be seen that this framework has a very strong public health contribution. Under the current plans for the NHS White Paper, PCT Public Health departments will move to local boroughs. It is now important that there is an understanding of the pharmacy network and its role in the community. The responsibility of maintaining and developing the PNA will move to the Health and Wellbeing Board of the local council as part of current changes to the NHS. Fig 65: Map of Public Health activity across the Community Pharmacy Contractual Framework
New Pharmacy Contractual framework
-PUBLIC HEALTH CONTRACT
ESSENTIAL ADVANCED ENHANCED
NATIONAL CONTRACT LOCALLY
COMMISSIONED
1-Dispensing of medicines.
2-Repeat Dispensing.
3-Health Promotion
4-Signposting
5-Support for Self care
6-Disposal of unwanted
medicines
7-Support for disabilities
8-CLINICAL GOVERNANCE
Medicines use review
&
Interventions
Can be used for Long
Term Conditions
EN1 Supervised Administration
EN2 Needle & Syringe Exchange
EN3 Palliative care
EN4 Stop Smoking
EN5 Care Home
EN6 Medicines Assessment & Compliance
Support
EN7 Medication Review (Full Clinical
Review)
EN8 Minor Ailment Service
EN9 Out of Hours (Access to Medicines)
EN10 Supplementary Prescribing by
Pharmacists
EN11 EHC via PGD
EN12 Seasonal Influenza Vaccination
EN13 Patient Group Directions
EN14 Chlamydia Screening & Treatment
EN15 NHS Healthchecks
Community Pharmacy works as a Public Health model of provision as patients do not have to register with a pharmacy and do not have to make appointments. The Pharmacy White Paper has highlighted the Public Health role of pharmacy. There needs to be brief healthy lifestyle advice given out with medicines, and attention paid to lifestyle modification. This, in addition to stressing the importance of taking medicines for CHD and diabetes, could potentially result in improved health outcomes. Examples of community pharmacy public health strategies are shown below:
• Signposting • Health promotion • To help people with acute and long-term conditions, promoting self-care, linking to Public
Health Initiatives for helping people to stay healthy • To have skilled, knowledgeable, competent and considerate staff • To be part of local network of health improvement services and local leaders for health • To be a wider „information retailer‟ to improve patients‟ health where needed

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
150
• To be a primary source of accessible, up-to-date, trusted and reliable health advice and information
9.4.1 NHS Public Health White Paper The Government's Public Health White Paper, „Healthy Lives, Healthy People: Our Strategy for Public Health in England‟ was published on 30th November 2010. The document sets out the Government's long-term vision for the future of public health in England, and outlines plans which will transform public health and for the first time create a „Wellness Service‟ - Public Health England - to meet today's wide-ranging health challenges. The Government's view is that society, government and individuals share collective responsibility for public health and the new public health system will encourage all to play their part in improving and protecting the nation's health and wellbeing. There is recognition of the pharmacy's role in improving public health. The document states that „community pharmacies are a valuable and trusted public health resource' and identifies the potential to use pharmacy teams more effectively to improve health and wellbeing and to reduce health inequalities. Pharmacists are also explicitly recognised in the White Paper as part of a wider public health professional network. Opportunities for Community Pharmacy are highlighted and include NHS Healthchecks, long-term condition management, tackling drug and alcohol abuse, prevention of long-term illness (stop smoking and obesity services), and increased uptake of seasonal flu vaccination. 9.4.2 Wandsworth Borough Council Wandsworth Borough Council – The feedback from the Oversight and Scrutiny Committee of Wandsworth Borough Council as part of the Consultation is a s follows (Jan 2011):- “The demographic profile of the Wandsworth population means that community pharmacy services are likely to be of particular importance. The high level of population mobility, the high proportion of young adults who are not regular users of health services, and the very high proportion who are in full-time employment make the model of service offered by community pharmacies – requiring neither appointments nor registration, and frequently open for extended hours – particularly appropriate. It is important to build on the ad hoc nature of patient contact with pharmacists to ensure that service users are able to access the full range of services, including preventive and health promotion provision that are of most relevance to them. The PNA serves the intended purpose of detailing the profile of current services available in the borough and the immediately surrounding area, pulling together relevant needs assessment information. Through a gap analysis the PNA makes a number of commissioning recommendations covering the need for a range of enhanced services. It is Evident that Wandsworth has generally strong pharmacy provision, although there may be scope for increased Sunday opening. The recommended strengthening of enhanced service provision appears sensible and reflects local need. The conclusion of the PNA that there is no overall shortage of pharmacies in Wandsworth appears justified. However, particular attention must be paid to the retention of provision in those wards in which there is just a single pharmacy. The loss of these pharmacies would be a

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
151
significant weakening of the network. Also, some of them form key components of secondary shopping parades, and their loss may threaten the viability of these parades.”
Wandsworth Borough Council has identified the importance of community pharmacies in terms of the economy on the High Street and in areas of deprivation. There are opportunities for more local development with Wandsworth Borough Council‟s Economic Development Office. Community pharmacies in areas of deprivation and close to or within council estates are in an ideal opportunity for local development linked to a health and social framework of care. Community Pharmacy has a key role to play the council and Local Strategic Partnership's Community Strategy and Neighbourhood Renewal Strategy.
Recommendations Strategy for engagement with the Local Borough Council:
A review of pharmacies and their services in wards with significant deprivation
Exploring initiatives between the Borough Council and community pharmacies e.g signposting, making use of pharmacy premises for outreach work
Developing strong partnerships with key groups such as Borough Tobacco Alliance, teenage pregnancy steering groups, emergency and influenza pandemic planning.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
152
10 PRESCRIBING AND MEDICINES MANAGEMENT Information for this section is taken from the PCT Medicines Management Strategy October 2009. The PCT has a prescribing budget of c£34m representing just over 10% of the PCT budget. Management of this is provided by a prescribing team and is a key PCT corporate criteria. The PCT prescribing team provides support to the Local Commissioning Groups cluster and leads on the following areas:-
Exceptional circumstance high cost drugs
Clinical effectiveness and medicine management committee
Accountable officer for control drugs
Prescribing advice to LCG clusters
Pharmacy community services – advice for vaccinations, community nursing
Community Pharmacy – advice and service development, work with special medicines and waste medicine reduction.
Community Pharmacy is currently in the Primary Care contracting department and the community pharmacy lead reports to the chief pharmacist
10.1 Aims of the Strategy
General Principles
The use of medicines is one of the most frequently used interventions in healthcare and all healthcare professionals have a contribution to make to medicines management to deliver improvements in health outcomes. Community pharmacies handle and manage medicines more frequently. NHS Wandsworth recognises that medicines have the potential for harm, as well as for good, and is therefore committed to ensuring that medicines are used effectively and safely. This is in accordance with principles of clinical governance and Care Quality Commission. The medicines management strategy also provides a review of the medicines management work undertaken to date by the pharmacy team and describes how medicines management plans will integrate with other workstreams within NHS Wandsworth, including Community Services Wandsworth (CSW) and other partners including GP practices. The pharmacy team has links with pharmacy teams in HMP Wandsworth, St George‟s Hospital, Kingston Hospital and Primary Care Trusts in the SW London sector and across London. Clinical Effectiveness and Prescribing Demonstrable improvements in the quality of prescribing in Wandsworth have been made across a wide range of therapeutic areas including cardiovascular disease, antibiotics, diabetes, mental health and respiratory conditions. NHS Wandsworth has a prescribing team that provides GP prescribing support and a community pharmacy lead that links into the PCT community pharmacy network. The roles of the Public Health Clinical Effectiveness and Medicines Management Committee, along with non-medical prescribing activities, are still key to ensuring safe prescribing and evidenced-based practice.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
153
Medicines Management in NHS Wandsworth Expenditure on medicines in Wandsworth accounts for a significant proportion of overall resources (c£34 million prescribing spend for 2009-2010), and the possibility of rapid growth in prescribing costs and significant reduction in growth monies available from 2011 and beyond represents a significant risk in terms of impact on other services and development. There are also risks associated with prescribing and the use of medicines, so robust systems need to be in place to ensure the effective and safe used of medicines. It should be noted that while the PCT has responsibility for the prescribing budget, Community Pharmacy is reimbursed for drug costs through the prescriptions they dispense, as they handle the largest number of medicines. Community Pharmacy is therefore part of the prescribing budget and has a key role to play in medicines management, improving the use of medicines for patients, prescribing interventions, and closer working with GP practices. There are well-established systems in place for allocating and monitoring prescribing budgets. Regular budget updates are provided to all GP practices and PBC cluster groups. Improved disease prevalence and disease register information should enable a more sophisticated approach to budget setting in the future. There has been much guidance aimed at improving standards, which has had an impact on the medicines management agenda. There is now one main Core National Standard – C4d: “Medicines are Handled Safely ands securely”, although several others are also related (e.g. C1a: “Analysis of Incidents”; C1b: “Patient Safety Notices, Alerts”; C5d: “Clinical Audit”; C5a: “Conformation to NICE Technology Appraisals....take into account nationally agrees guidance”; C16: “Information Available to Patients”). http://www.cqc.org.uk/_db/_documents/Criteria_for_assessing_core_standards_in_2009-10_-_Primary_Care_Trusts_as_Providers.pdf The PCT should have access to advice about medicines management, prescribing and pharmacy issues. This advice will be required at both Board level and at Professional Executive Committee (PEC) level. Although it may be possible for the same person to provide all this advice, a range of knowledge and skills may be required to provide the full range of pharmaceutical advice required. The importance of this was reflected in the Audit commission report “A Spoonful of Sugar”. Therefore the PCT will need to work closely with Workforce Development Confederations to develop the PCT medicines management workforce to meet local needs. It can be seen that there is clearly a Board level responsibility of medicines management, which will support the achievement of the Trust‟s aims by ensuring the highest level of performance at all stages in the medicines management process. This may be facilitated by its approval of this Medicines Management Strategy and programme of development, with clearly defined objectives and feedback on progress. Existing Committee Structures:
Public Health Clinical Effectiveness and Medicines Management Committee
Non-Medical Prescribing Committee
Controlled Drugs Local Intelligence Network (CDLIN) to support the implementation of strengthened governance arrangement for the safe and secure management of Controlled Drugs.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
154
Priorities for Future Development Improving the quality of medicines management across the health economy has always been a key focus of work for the PCT. However, it is recognised that a number of areas need to be addressed to further improve medicines management services: Long Term Conditions (LTCs) Management Despite the availability of effective medicines it is accepted that many patients may still have poor control of their chronic condition. Patients should be involved in treatment choices and support should be provided to ensure that patients gain optimal benefit from their medication. Strategies should aim to reduce health inequalities and this strategy includes a plan for enhancing the care of patients with long-term conditions. It is proposed that a lead pharmacist supports the development of medicines management through the appropriate Local Implementation Team (LIT). Opportunities presented in the enhanced services of the Community Pharmacy Contractual Framework, acute pharmacy, and practice-based pharmacists may enable further support to assist with management of patients with LTCs. The Community Pharmacy Contractual Framework needs to be more integrated into LTCs as shown in section 7.2 of this report. Currently, patients will be supported by practice-based pharmacists (e.g. medication review clinics, chronic disease clinics) and community pharmacists (e.g. MURs are recommended for patients with long-term conditions). The expertise of pharmacists in acute settings could be brought into Primary Care to provide review clinics, services, specialist advice to prescribers, and access to medicines information. Governance and Medicines Safety Joint-working with governance colleagues has recently seen the development of an electronic system to disseminate and gather actions following medicines or device alerts. National Patient Safety Agency (NPSA) alerts and Medicines and Healthcare Products Regulatory Agency (MHRA) alerts need to be actioned promptly and the PCT, as the commissioner, needs to ensure that all providers and contractors are implementing NPSA and MHRA alerts. Further work should continue to reduce the number of avoidable hospital admissions caused by adverse drug reactions and healthcare-acquired infections. The PCT needs to demonstrate to the Care Quality Commission that medicines are handled safely and securely across all departments of the organisation. New controlled drugs regulations require improved governance arrangements to be in place to ensure safe management of controlled drugs. Commissioning Commissioning organisations need to assure themselves that all medicines management services provided to their patients through their various provider organisations are appropriate, safe, and address both financial and clinical risks to both patients and the wider health economy. In order to achieve this, a framework will be developed so that the PCT can assure itself that medicines management services are fit for purpose, continue to improve, and meet the needs of patients. Commissioning of services which involve supplying or prescribing medicines must ensure that such services comply with the Medicines Act.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
155
A proposed framework will incorporate the following criteria:
NHS Better Care Better Value and other prescribing indicators All organisations within the health economy should work together to achieve improvements in Better Care, Better Value indicators and other locally agreed prescribing objectives. Effective healthcare is efficient healthcare, and the NHS should demonstrate that effective use is made of public money to deliver quality healthcare. Compliance with national guidance e.g. NICE The PCT follows NICE guidance and provider organisations should action NICE guidance and should be able to demonstrate implementation. Health economy formulary / guidelines Provider organisations should actively participate in health economy discussions on prescribing and medicines management, and participate in a formulary agreed through the health economy Clinical Effectiveness & Medicines Management Committee. Support to Primary Care Practice-based pharmacists have demonstrated their effectiveness in promoting cost-effective and quality prescribing. Providers should utilise practice-based pharmacist support to ensure that prescribing is cost-effective and that prescribing budgets are used to deliver quality healthcare. There is a prescribing advisor attached to each LCG. Community Pharmacy can have a key role to play in the prescribing budget; this has been evidenced in NHS Wandsworth through the cost reduction programme in special medicine. Effective use of the contractual framework and better integration of long-term conditions and medicines management offers another cost-effective option to Primary Care. Acute pharmacy could also be brought to support Primary Care through specials advice. Acute pharmacy services and products is another cost effective option that Primary Care could explore. NSPA medicines safety alerts PCTs should assure themselves that their provider organisations comply with NPSA medicines safety alerts, are making good progress with implementation and are on target to achieve full implementation by stipulated times. Commissioners should ensure that providers are able to assure them that they are maintaining compliance with previous medicines safety alerts, for example through the annual medicines management audit programme. Where further NPSA medicines safety alerts are published, a similar approach should apply. Communications involving prescribed medicines Healthcare organisations should have good communication systems between primary and secondary care so that clinicians in each sector have up-to-date knowledge of medicines being currently prescribed and taken by patients. This should cover admission to hospital, discharge from hospital, as well as attendance at outpatients or specialist clinic appointments. This has been highlighted by the Care Quality Commission (CQC) as an area for improvement in the NHS. St George‟s pharmacy team and community pharmacies in Wandsworth have been involved in the discharge of medicines and improved communication between the secondary and primary care interface.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
156
Untoward incidents Provider organisations should provide timely information to their Primary Care Trusts of serious untoward incidents involving medicines (AIR forms and investigations). These should also include reports arising from investigations, lessons learned and recommendations so that improvements in medicines safety can be made by all NHS organisations.
Participation in national / local audits
The service provider achieves a score of „good‟ or „better‟ in the CQC and has an action plan agreed that will deliver further improvement in their overall CQC medicines management score. Community Services Wandsworth (CSW) Community Services Wandsworth is now part of St George‟s Hospital. Currently, pharmacy services such as dispensing and ward clinical pharmacy are provided at Queen Mary‟s Hospital pharmacy through a Service Level Agreement with Kingston Hospital NHS Trust. Community Pharmacy plays a very important role in medicines management and prescribing. Analysis of one year‟s worth of PCT prescribing data showed that between 85-90% of all NHS Wandsworth prescriptions were dispensed by NHS Wandsworth pharmacy contractors. This means that community pharmacies are ideally placed to support the management of the prescribing budget and work with GPs. Examples are given below:-
Prescription intervention – to support waste reduction, dose optimisation, generic switching
Review specials medicines
Increased repeat dispensing and robust repeat prescription service where the correct repeatable medicines are ordered.
Prescribing Data GP Surgeries
Period Name Prescriber Name BNF Name Total Items
cal year 2009 BALHAM HEALTH CENTRE BNF 24,875
cal year 2009 BALHAM HILL MEDICAL PRACTICE BNF 18,993
cal year 2009 BALHAM PARK SURGERY BNF 100,110
cal year 2009 BATTERSEA FIELDS PRACTICE BNF 92,766
cal year 2009 BATTERSEA RISE GROUP PRACTICE BNF 46,973
cal year 2009 BEDFORD HILL FAMILY PRACTICE BNF 88,744
cal year 2009 BRIDGE LANE GROUP PRACTICE BNF 151,621
cal year 2009 BROCKLEBANK GROUP PRACTICE BNF 178,050
cal year 2009 CHARTFIELD SURGERY BNF 89,588
cal year 2009 CHATFIELD MEDICAL CENTRE BNF 147,794
cal year 2009 CLAPHAM JUNCTION MEDICAL PRACTICE BNF 41,186
cal year 2009 DANEBURY AVENUE SURGERY BNF 57,546
cal year 2009 DR FREEMAN AND PARTNERS BNF 124,263

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
157
cal year 2009 DR NICHOLAS & PARTNERS BNF 139,661
cal year 2009 EARLSFIELD SURGERY BNF 163,107
cal year 2009 ELBOROUGH STREET SURGERY BNF 39,668
cal year 2009 FURZEDOWN PRIMARY CARE CENTRE BNF 54,033
cal year 2009 GRANVILLE ROAD SURGERY BNF 11,882
cal year 2009 INNER PARK ROAD HEALTH CENTRE BNF 70,330
cal year 2009 LAVENDER HILL GROUP PRACTICE BNF 87,945
cal year 2009 MAYFIELD SURGERY BNF 91,004
cal year 2009 OPEN DOOR SURGERY BNF 83,904
cal year 2009 PUTNEYMEAD MEDICAL CENTRE BNF 120,642
cal year 2009 QUEENSTOWN ROAD MEDICAL PRACTICE BNF 96,323
cal year 2009 SAI MEDICAL CENTRE BNF 9,608
cal year 2009 SOUTHFIELDS GROUP PRACTICE BNF 164,459
cal year 2009 ST PAUL'S COTTAGE PRACTICE BNF 43,458
cal year 2009 ST. JOHN'S HILL PRACTICE BNF 19,164
cal year 2009 STREATHAM PARK SURGERY BNF 96,239
cal year 2009 THE ALTON PRACTICE BNF 56,384
cal year 2009 THE FALCON ROAD MEDICAL CENTRE BNF 85,393
cal year 2009 THE GREYSWOOD PRACTICE BNF 92,229
cal year 2009 THE HAIDER PRACTICE BNF 18,241
cal year 2009 THE HEATHBRIDGE PRACTICE BNF 101,996
cal year 2009 THE HERITAGE MEDICAL CENTRE BNF 67,712
cal year 2009
THE JUNCTION HTH CTR-REGISTERED PATIENTS BNF 0
cal year 2009 THE ROEHAMPTON SURGERY BNF 127,893
cal year 2009 THE SURGERY BNF 33,965
cal year 2009 THURLEIGH ROAD PRACTICE BNF 65,619
cal year 2009 TOOTING BEC SURGERY BNF 8,288
cal year 2009 TOOTING SOUTH MEDICAL CENTRE BNF 41,465
cal year 2009 TRIANGLE SURGERY BNF 64,309
cal year 2009 TUDOR LODGE HEALTH CENTRE BNF 62,795
cal year 2009 WANDSWORTH MEDICAL CENTRE BNF 62,450
cal year 2009 WATERFALL HOUSE BNF 60,813
3,403,488
NHS Wandsworth Community Pharmacies dispense around 85% to 90% of all prescriptions produced by NHS Wandsworth GP practice. The core area of Medicines Management will be working with Community Pharmacies around supporting prescribing strategies, plans for reduction in waste medicines, supporting patients compliance and understanding of medicines and non medical prescribing. Community Pharmacies handle and manage most amount of medicines in Wandsworth.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
158
10.2 Specials Medicines Specials medicines are locally formulated and produced medicines, which are prescribed when there is no commercially licensed alternative. From the graph below the cost of specials in NHS Wandsworth rose from £60k/month to £140k/month. Figure 66: Cost of specials medicines
The issue of specials medicines is a rather complex and nebulous area with no clear NHS pricing and formularies. NHS Wandsworth is now working with pharmacy contractors to bring down the cost of specials medicines. This is a partnership between the community pharmacy lead and Local Pharmaceutical Committee to assist the PCT. More joined-up working between community pharmacies and GPs is being taken forward on this important matter. There is an opportunity for acute pharmacies that produce specials to provide a more integrated service around advice and procurement to prescribers and community pharmacies. 10.3 Waste Medicines Reduction of unused or over-ordered medication will be another part of the medicines management strategy. This is a multi-faceted approach requiring patient engagement and education, and co-working with prescribers and dispensers. Prescribing systems:
Shorter prescribing intervals e.g. 28 days, can result in less waste when medicines are stopped or changed
Improved synchronisation for all medicines on a prescription so they run out at the same time
Ensure that only medicines that are to be taken regularly for long-term conditions are allowed on repeat prescription
Ensure patients are stable on a medicine and are tolerating it well before it becomes „repeatable‟
Medicines that are required occasionally (e.g. analgesics, antihistamines, creams etc.) should remain as ‟acute‟ prescription items
Develop robust repeat prescribing policies that ensure repeat supplies are only made if set criteria are met. This should be communicated with community pharmacies
Timely clinical medication reviews, ideally involving the patient and the prescriber, to address issues around all prescribed medicines.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
159
Community pharmacy services:
The Medicines Use Review (MUR) service in the Community Pharmacy Contractual Framework is designed to support patients with practical aspects around their medicine-taking. Pharmacists can target patients whom they suspect may have problems. Other healthcare professionals can also signpost or refer to this service where appropriate.
The repeat dispensing service enables the day-to-day management of repeat prescribing to be undertaken by a patient‟s nominated community pharmacist. They are obliged to satisfy themselves that each medicine is required whenever medicines are dispensed. This presents an ideal opportunity to identify and address problems that lead to waste. (A similar check will be required when repeatable Electronic Prescriptions are introduced.)
Some PCTs have commissioned community pharmacy services aimed at reducing waste e.g. intervention schemes (pharmacists identify potentially wasteful prescribing) and „not-dispensed‟ schemes (pharmacists implement an extra check that the patient actually needs all the items on the prescription, and only dispense what is needed).
Publicity campaigns Raising public awareness of the issues around waste medicines in terms of cost and loss of money to the NHS is a key message. The public may have the misconception that the prescription charge covers the cost of a prescribed or unused medicine that is returned to a pharmacy, and that it can be reissued to other patients; in actual fact, the medicine has to be sent for waste.
Patient engagement concordance While these ideas can help reduce waste medicines, it is important to ensure that patients are actively involved in the decision-making processes around treatment options, and are motivated and enabled to comply with the regimen agreed. Working with patients and their carers around medicines management will be a key role for community pharmacists.
10.4 Oral Nutritional Supplements The 2010 London Procurement report reviewed the costs of nutritional feeds. Expenditure on oral nutritional supplements (ONS) is rising nationally by 10% per year. In London, PCTs spent just over £15million in 2009/10. Although Wandsworth has implemented strategies to improve ONS prescribing practice, expenditure has continued to rise, especially in the last two years. Evaluation of expenditure in 2009/10 in Wandsworth is complicated by the transfer of a very large, high spending GP practice due to boundary change. The PCT from which it transferred experienced a significant reduction in expenditure despite limited demand management initiatives being implemented in the same time frame. In the last five years (2005-2010), Wandsworth has spent just over £2.4million on oral nutritional supplements.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
160
Fig 67: Summary graph of potential ONS expenditure outcomes to 2014
Future cost projections
Based on current expenditure and ONS trends, it is predicated expenditure on ONS will increase to £1 million annually by 2013/14.
The average annual increase in spend in Wandsworth in the last five years was 12%, compared to the London average (8% increase) and the best performing trust (6% annual reduction). Data from Quarter 1 and 2 shows a 7% increase in 2010/11, indicating cost avoidance will be achieved this year.
Cost savings that could be realised
Introducing initiatives to reduce inappropriate ONS expenditure could result in cost avoidance savings
Based on the London average expenditure of 8%, this would equate to a cost avoidance of approximately £70,230 over four years
Implementing a robust framework to manage ONS could result in cash releasing savings
The best performing London PCT experienced savings of 6% per year. It is estimated up to £434,142 could be saved in the next four years in Wandsworth if a system to effectively manage ONS is fully implemented. In total, over £500,000 could be saved from a combination of cost avoidance and cash releasing. Savings strategies to mange ONS should be fully implemented.
Recommendations
Ensure greater engagement by acute services to address inappropriate ONS prescribing and utilisation within secondary care
Implement local care pathways across primary and secondary care to ensure best practice with regard to the treatment of malnutrition, throughout the whole patient journey
Malnutrition education and training embedded in local routine practice
Implementation of local ONS guidelines
Continued GP education, audit and training. There are opportunities for Community Pharmacy to support the implementation of the ONS NHS guidelines by carrying out patient reviews, developing patient education, and reducing

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
161
waste. There is an opportunity for self-care, which would have major implications in term of supporting prescribing and ONS strategy 10.5 Local Pharmaceutical Service Contracts Fig 68: Map of LPS and ESPLPS contracts
NHS Wandsworth operates 11 LPS contracts and one low dispensing ESPLPS contract. The LPS contracts are focused around medicines management. The results of the LPS contract include the following:-
Reduction in inappropriate prescribing.
Usage of a standard assessment template linked to dossette services
Managing patients with poor compliance into the service and move out once the patient is stabilised
Better communications with GP practices The current service could provide specific care for patients covered by the virtual ward. The ESPLPS contract has been revised in Wandsworth and linked to local needs:-
Will provide and offer stop smoking and emergency contraception
Will offer the use of consulting rooms for outreach services
Will take part in PCT pandemic planning or emergency services. This method of contracting could be applied to other services e.g. sexual health, services for drug misusers and medicines management to run alongside normal contracts.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
162
10.6 Monitored Dosage Service There is a PCT-funded service for monitored dosage services (MDS) for patients who have difficulties taking their medication. This is aimed at patients living independently in their own accommodation not supported by a care worker. The service is not meant for patients who live in registered care homes. The service is offered by the PCT or separately by pharmacies. In a recent PCT audit there was a wide variation of provision. Where the service was not commissioned by the PCT but offered to patients there was no proper compliance assessment methodology. The service should be focused on improving compliance. MDS is one of many options that could be used to support patient compliance through:-
Easy to read labels
Memory charts
Patient‟s informal carer support (not funded by the council)
Supervised administration e.g. patients with mental health difficulties where medication compliance is problematic
The service should be renamed Medicines Compliance Service that brings in the principles of supporting and improving patient compliance. 10.7 Non-Medical Prescribing Prescribing rights have been extended to more healthcare professionals and therefore the PCT will need to ensure that the benefits of extended prescribing are reflected in service development or redesign plans. There are opportunities for trained non-medical prescribers to work in parallel with doctors to increase access, capacity and choice for patients (Making the Connections – Using Healthcare Professionals as Prescriber to Deliver Organisational Improvements). However, performance management and competency frameworks needs to be in place to ensure effective use of non-medical prescribers. An infrastructure should be in place to support new prescribers, including systems to ensure that drug alerts and hazard warnings are received. New prescribers should be represented on appropriate PCT medicines management groups. Currently more nurses are developed as non-medical prescribers, Community pharmacists have yet to be developed as non-medical prescribers. There are opportunities for opticians to be non medical prescribers as part of service redesign. Currently in Wandsworth there are no non-medical prescribers in community pharmacies. There are opportunities to develop a few pharmacies in each of the polysystem areas with a non- medical prescriber. 10.8 Commissioning Recommendations The NHS White Paper has highlighted the role of pharmacy through payment for performance, and will incentivise and support high quality and efficient services including better value in the use of medicines through better informed and more involved patients. There are planned

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
163
changes to the Community Pharmacy Contractual Framework that will see services around MURs focused on long-term conditions and improving patients‟ usage of medicines. The core contractual framework needs to be fully integrated into this process. Repeat dispensing and more focused medication use reviews in agreement with local GPs could support the management of the prescribing budget and improve patient care. The medicines management component of the GMS contract and the community pharmacy contract have never been properly aligned and there is an opportunity to develop this. Merton, Sutton and Wandsworth Local Pharmaceutical Committee made the following
statement during the PNA consultation:
Merton, Sutton and Wandsworth Local Pharmaceutical Committee
The LPC welcomes the comments made on better usage of the Community Pharmacy
Contractual Framework. A better understanding of how MURs can be targeted and linked into
the GPs GMS and PMS contract would be useful to build better professional links with general
practice.
PNA Commissioning Intentions – Community Pharmacy handles more medicines on a higher volume than any other healthcare professional. To support effective prescribing and develop a wider medicines management network across Wandsworth, development and commissioning of existing models of medicine management is now required. At a local level, GP practices need to involve community pharmacies with prescribing decisions. Key areas for development are:-
Prescription intervention service
Focused MURs in agreement with local GP practices
Making better use of repeat dispensing and robust repeat prescription collection services
Redevelopment of LPS contracts around medicine management
Supporting the PCT on the prescribing and review of specials medicines
Waste medicines management policy
Exploring pathways for acute pharmacy providers to support medicines management in Wandsworth
The above solutions will require more local joint-working and regular communication between GP practices and community pharmacies. These recommendations are in line with the Joint letter from the PSNC and BMA in January 2009 about GPs and pharmacies working together (see Appendix 9).

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
164
11.0 COMMISSIONING STRATEGY AND COMMISSIONING RECOMMENDATIONS Pharmacy has an important role to play in the health and wellbeing of the population of Wandsworth. It is important that there is a robust commissioning process linked to strong professional standards and development to make good use of all pharmacy providers in order to develop high quality pharmaceutical services. 11.1 Key Commissioning Principles Community Pharmacy Locally Enhanced Services Before any community pharmacy is commissioned on a locally enhanced service:-
Pharmacies must deliver essential services to a high standard.
Pharmacies must demonstrate low staff turnover, which is key to continued care and safety around medicines management and dispensing
Pharmacies must demonstrate they are providing enhanced services in addition to dispensing
The PCT will commission pharmacies outside the PCT depending on the appropriateness of the locally enhanced service and the pharmacy being compliant with Community Pharmacist Assurance Framework in their host PCT
All pharmacies must use NHS net email accounts
All services will be developed to meet the needs of the population of Wandsworth with key outcomes
All pharmacy services will have an accreditation framework Other Pharmaceutical Providers
The PCT will ensure that other pharmaceutical providers are engaged and kept informed of LCG developments.
Service Redesign Where the PCT is reviewing service reconfiguration, attention must be paid to medicines and prescribing.
Additional services that require access to or supply of medication must be compliant with the Medicines Act
Robust options appraisals must be carried out, looking at the suitability, feasibility and acceptability of proposals along with value for money
Representation
All Local Commissioning Groups have a nominated community pharmacy and acute pharmacy representative
Both representatives will work together professionally around medicines management
Representation carries the responsibilities of selflessness, communication to the pharmacy network in the community, and articulating the community pharmacy viewpoint
All pharmacy providers are informed and updated when there are prescribing changes

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
165
Developmental Strategy
Professional development is critical to ensure robust pharmacy services of a high quality. The PCT and stakeholder commissioning organisations must engage with the key processional stakeholder organisations
The PCT will support SW London sector/pan London accreditation and ensure all pharmacy services are harmonised in line with national accreditation standards
The PCT will work with other PCTs in the sector to develop standardised services
The PCT will work with key national stakeholders such as the English Pharmacy Board, National Pharmacy Association, College of Pharmacy Practice and Education (CPPE) and Kingston University School of Pharmacy to develop high quality services
There will be engagement with the English Pharmacy Board‟s representation at sector level, the SW London Local Practice Forum, so there is professional engagement around local needs and development
The PCT will commission specialist pharmaceutical expertise to develop and enhance services and competencies required to deliver those services
11.2 Gap Analysis and Commissioning Recommendations Community Pharmacy Provision There is adequate coverage of community pharmacies within Wandsworth. Each polysystem locality has access to all commissioned pharmaceutical services and there are pharmacies open seven days a week in each of the polysystems. The PCT also takes into account community pharmacies outside Wandsworth for access to dispensing services and, where appropriate, commissioning of locally enhanced pharmacy services. The PCT does not currently require additional pharmacy contracts to meet prescription needs. Locally enhanced pharmacy services are accessible in all localities and there is a good coverage of LPS contracts across the whole of Wandsworth. Community Pharmacy Capacity The capacity offered through the community pharmacy network through premises, staffing and skill mix, medical equipment and IT needs to be leveraged. There are opportunities to locate outreach services within pharmacies. There needs to be a further review through the Primary Care estates strategy. There are opportunities for the council, public health and local groups to make use of the signposting and health promotion that pharmacy can offer.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
166
Pharmaceutical Providers There are opportunities to bring in other pharmaceutical providers such as acute pharmacy. The key areas identified are:-
Safe administration of medicines,
Discharge of medication
Commissioning of specialist roles e.g. mental health, long-term conditions, review of specials formulations.
The roles of the different pharmaceutical providers should be reflected in polysystem development as specialist clinical skills could be commissioned in Primary Care. Pharmacy Services Pharmacy services are available across the whole borough and there are generally no access problems. The key gap is to develop services further into the next tier of provision and developing specialist pharmacy services. The only main gap found was development of a revised and integrated care home service. The key gaps and commissioning recommendations are identified below.
Automation of services – An IT system to support data collection and performance management
Overall services should be developed and raised to the next levels located in each polysystem area
Care homes – This required complete overhaul and will require an engagement with stakeholders. Community pharmacies in Wandsworth have expressed interest in providing services
Sexual health – The majority of pharmacies provide EHC. There is a need for a smaller number to provide an integrated sexual health service consisting of chlamydia screening and treatment, condom distribution and access to oral contraception under PGD
Stop smoking – Increasing the range of pharmacotherapy and skill mix. Opportunities to locate drop-in clinics in pharmacies
Services for drug misusers – There are no access issues for supervised administration and needle exchange; however more development work is required for harm reduction training for pharmacies. Extension of supervision to include diazepam and naltrexone. Two pharmacies should be developed to support hepatitis C screening
Asthma and COPD – Development of the asthma pilot service and extension to COPD. This can link into pharmacies that provide stop smoking services. There are opportunities for focused medication reviews
Health and wellbeing – The PNA has identified that pharmacies need to be included in NHS sexual healthchecks and a few pharmacies will be taken forward. Pathfinder projects will be set up for pharmacies to deliver obesity services, support cancer screening and diabetic screening in each of the polysystem areas

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
167
Long-term conditions – Further involvement and integration of all pharmacy providers (community and acute) is required in long-term conditions around medicines management and patient care. A service model based on the Community Pharmacy Contractual Framework can be integrated into polysystem planning around long-term conditions
Mental health – Community pharmacies should carry on supporting the Mood Manager programme in Wandsworth. There are opportunities for supervised administration for patients with difficulties with compliance. The specialist pharmacy team at Springfield Mental Health Trust should be included in medication planning for mental health patients
The minor ailments service should be revised to support shift of care of minor conditions from general practice and urgent care to community pharmacies. Referral pathways should be developed for key patient groups e.g. drug misusers, unregistered patients, families on low income
Medicines management remains a key area for community pharmacy development and there are many opportunities for community pharmacies to work with general practitioners to support the management of the prescribing budget. The areas of focus will be:- o Reduction in waste medication and prescribing strategies. o Prescription Intervention service o Focused medicines reviews linked to agreed outcomes with GPs o Revised monitored dosage service o Development of non-medical prescribing advisors o Management and review of special medicines and waste medicines strategy o Increasing repeat dispensing and robust repeat prescription collection service o Involvement of acute sector pharmacy and specialist pharmacy to commission specialist
services.
A strategic review of the GP / Community Pharmacy interface, with recommendations for stakeholder groups to meet and aim for an agreed strategic plan around services, communication and clinical interface issues
Guide to the new emerging organisations, the interrelationships and communication required, and work together to deliver the Pharmaceutical Needs Assessment (See appendix 7)
Regulatory updates and summary of Health and Social Care Bill and impact on Pharmacy commissioning strategy.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
168
12 THE FUTURE 12.1 Emerging Organisations
The PNA has been written during a time of great change to the health service. For pharmacists this has proved to be an unsettling period and it is vitally important that the key emerging groups work together to ensure that progress made around community pharmacy development is not lost. They key groups are presented below:-
NHS Commissioning Board - The commissioning board will be responsible for managing primary care health services e.g. general practice, dentistry, optometry and Community Pharmacy, for arranging the provision of primary health services, and will be responsible for regulating GP consortia. The board will maintain lists of pharmaceutical contractors. In emergency circumstances such as an outbreak of pandemic influenza, the Bill states that the board will be expected to provide pharmaceutical services to cover any shortfall in the provision of services, but this will be a last resort and only where alternative providers are not available. Pharmacy contract applications are made through the current Control of Entry, which is anticipated to be replaced by the Market Entry Test. GP commissioning Consortia – Every GP practice in England will belong to a consortium. The Consortia will be responsible for commissioning almost all NHS services for their patients and the NHS Commissioning Board will allocate budgets to consortia. Local Authorities – The PCT Public Health departments will move to the local authorities and will be required to improve public health through commissioning and establish Health and Wellbeing boards. The board will take responsibility for developing and publishing Pharmaceutical Needs Assessments. In SW London the New SW London Transitional Contracting functions will be a precursor to a regional or national commissioning board and will have financial accountability for the community pharmacy contracts. The Wandsworth Health and Wellbeing Board, though Public Health at Wandsworth Council, will have the responsibility for the PNA. It is vitally important that these groups communicate clearly around the PNA so that needs assessments and finance should be balanced. The relationship between Community Pharmacy and the emerging organisations is shown in figure 69 and 70.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
169
Fig 69: Current organisation model in relation to Community Pharmacy
Chemist & Druggist January 2011 Fig 70: Funding, accountability and relationship links between the new organisations
(Interpretation by the Royal Pharmaceutical Society January 2011)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
170
12.2 Changes and Updating the PNA The PNA for Wandsworth has sought to provide up-to-date information, but with time, changes will take place. It is important that the PNA is kept updated The document should be updated as and when changes take place. The current document is valid until 2013. It is anticipated that minor changes will be made in the following areas:-
Additions or removals to the NHS Pharmaceutical List
Changes in pharmacies providing current or new locally enhanced services
Changes in Community Pharmacy core and supplementary hours
Minor regulatory changes and minor contractual changes around the Community Pharmacy Contractual Framework
Regulatory update when Market Entry is brought in. This information must be updated on a regular basis. Communication between NHS commissioning boards, Public Health, service providers and Local Pharmaceutical Committees will be crucial to this process. This information can be written as a PNA addendum with revised appendices and must be linked to the original PNA document.
.
PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
171
REFERENCES NHS Wandsworth
1. NHS Wandsworth 2005 Pharmaceutical Needs Assessment reports
2. NEW PHARMACY CONTRACT – Briefing paper to the NHS Wandsworth PEC
3. March 2005. J. Hameer, D. Tamby Rajah, S. Warren.
4. NHS Wandsworth community pharmacy baseline assessment reports March 2005.
5. D. Tamby Rajah, Executive Summary Reports to Local Pharmaceutical Committee, Local Medical Committee: Commissioning, Public Health and Wandsworth Council
6. Wandsworth Public Health Report Nov 2009
7. Greater London Authority Population Projections for the London Borough of Wandsworth
2007
8. Picture of Health April 2009
9. NHS Wandsworth Joint Strategic Needs Assessment 2011
10. NHS Wandsworth Primary Care Strategy 2009 Pharmacy
11. NHS walk-in centres: Implications for pharmacy The Pharmaceutical Journal Vol 265 No 7111 p305-307 August 26, 2000 Articles
12. NHS Confederation Briefing 160 May 2008
13. RPSGB report The role of Pharmacy in Long Term Condition (2006)
14. Choosing health through pharmacy - A programme for pharmaceutical public health
2005–2015
15. RPSBG Community Pharmacy and Long Term Conditions 2006
16. The Pharmacy White Paper consultation - “Pharmacy in England: Building on strengths – delivering the future – proposals for legislative change” 2008 http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Consultations/Responsestoconsultations/DH_093264
17. Pharmacy in England: building on strengths – delivering the future
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_083815
18. Primary and Community Care Services: Improving pharmaceutical service 2010

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
172
http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Dearcolleagueletters/DH_097654
19. Report on the Wandsworth Minor ailment service Kingston ELLEN MUSHAMBI –
Pharmacy Graduate Kingston University May 2010
20. Delivering Enhanced Pharmacy Services in a Modern NHS: Improving Outcomes in Public Health and Long-Term Conditions August 2010
Regulations
21. Pharmaceutical services
The NHS (Pharmaceutical Services) Regulations 2005, Statutory Instrument (SI) 2005/641
govern the provision of pharmaceutical services. The original Regulations can be found at: www.legislation.gov.uk/uksi/2005/641/made
www.opsi.gov.uk/stat.htm The relevant amending Regulations are: In 2005 – 1015, 1501, 3315 In 2006 – 552, 913, 1501, 3373 In 2007 – 674 In 2008 – 528, 683, 915, 1514 In 2009 – 309, 599, 2205, 3340 In 2010 – 22, 914
22. Local pharmaceutical services
The NHS (Local Pharmaceutical Services) Regulations 2006 govern the provision of Local Pharmaceutical Services (LPS) and can be found at: www.legislation.gov.uk/uksi/2006/552/contents/made
Directions
23. Provision of advanced and enhanced services (Gateway reference 4795) The Pharmaceutical Services (Advanced and Enhanced Services) (England) Directions 2005 www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsLegislation/ DH_4108209
24. Provision of appliance advanced services (Gateway reference 13187)
The Pharmaceutical Services (Advanced Services)(Appliances) (England) Directions 2009 www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsLegislation/ DH_110489

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
173
25. Pharmaceutical services application fees (Gateway reference 9517) National Health Service Act 2006: Pharmaceutical Services (Fees for applications) Directions 2008 www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsLegislation/ DH_083854
26. Provision of Essential small pharmacy LPS (Gateway reference 5733)
Local Pharmaceutical Services (Essential Small Pharmacies) Directions 2005 www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsLegislation/ DH_4122402 Amendments www.dh.gov.uk/en/Healthcare/Primarycare/Communitypharmacy/ Localpharmaceuticalservices/DH_4115335
Guidance – Control of Entry 27. Control of entry (Gateway reference 12573)
The NHS (Pharmaceutical Services) Regulations 2005: Information for primary care trusts (Control of entry) www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_105361
28. Exempt applications – approved retail areas
The list of retail areas approved by Secretary of State www.dh.gov.uk/en/Healthcare/Primarycare/Communitypharmacy/ NHSpharmaceuticalregulations/Controlofentry/index.htm
29. Guidance – local pharmaceutical services
LPS permanence guidance (Gateway reference 8808) www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_083442
30. Guidance – pharmaceutical needs assessment
DH information on pharmaceutical needs assessments (Gateway reference 14083) www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_114953

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
174
APPENDIX 1 Project Plan

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
175

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
176
APPENDIX 2 Prescription Demand London Source General Pharmaceutical Services in England 1999-2000 to 2008-09
England monthly prescription average
64,205,000items/10475 pharmacies =6129 items/month/pharmacy

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
177

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
178
APPENDIX 3 Population Breakdown of the Borough of Wandsworth
Population
Total 284,000
Under 16 45,200
Over pensionable age 31,500
Unemployment
Total unemployed benefit claimants 3.1%
Ethnicity
White
White British 168,665 64.8%
White Irish 8,151 3.1%
White other 26,162 10.1%
Mixed
White & Black Caribbean 2,893 1.1%
White & Black African 1,252 0.5%
White & Asian 2,247 0.9%
Mixed other 2,336 0.9%
Asian or Asian British
Indian 7,412 2.9%
Pakistani 5,449 2.1%
Bangladeshi 1,099 0.4%
Other Asian 4,084 1.6%
Black or Black British
Caribbean 12,665 4.9%
African 10,013 3.9%
Black other 2,388 0.9%
Chinese or other
Chinese 2,227 0.9%
Other ethnic group 3,337 1.3%
Housing tenure

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
179
Total number of households 130,533
Local authority 17,145
Registered social landlord 9,807
Other public sector 300
Private sector 103,281
Total public sector 21%
Total private sector 79%
Schools Number of schools Number of pupils
Nursery 3 191
Primary 56 17,558
Secondary 10 10,338
Special 8 609
Pupil referral units 4 114
Independent 30 9,334
City technology colleges 0 0
Academies 1 1,068

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
180
APPENDIX 4 Joint Strategic Needs Assessment (JSNA) Key Messages
Key Messages: Children and Young People
Relatively low or poor health outcomes
Worsening trend in health outcome
Equality & diversity
Failure to meet targets which may contribute to poor outcomes
Despite reductions, teenage pregnancy rates are still above national and London averages (and well short of the 55% target reduction from 1998) Levels of childhood obesity are high in comparison to national averages – especially for Year 6
Increasing numbers of children with physical and learning disabilities admitted to Wandsworth special schools Increasing numbers of children with autistic spectrum disorders Estimates indicate a high potential demand for Child and Adolescent Mental Health Services (CAMHS)
Overrepresentation of black and minority ethnic groups:
Levels of obesity
In treatment for drug misuse
Using Child and Adolescent Mental Health Services
With statements of special educational need
Percentage of teenage conceptions
Being excluded from school and in the criminal justice system
Prevalence of sickle cell anaemia Vulnerable groups and mental health problems including looked after children, young carers, teenage parents, youth offenders, lesbian, gay, bisexual and transgender (LGTB) and homeless young people Concern that substance misuse services may not be reaching the most vulnerable (e.g. older teenagers)
Childhood immunisation rates, whilst considerably improved, are below the level required to provide “herd immunity” (95% for MMR at Year 2) Percentage of pregnant women attending a maternity appointment at 12 weeks was below target

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
181
Key Messages: Young Adulthood
Relatively low or poor health outcomes
Worsening trend in health outcome
Equality & diversity
Failure to meet targets which may contribute to poor outcomes
Number of new diagnoses of chlamydia, gonorrhoea, and syphilis
Hospital admissions attributable to alcohol People accessing HIV-related care
Young women are more likely to be screened for chlamydia than their male peers Low representation of 15-34 age group in substance misuse services Alcohol-related admission to hospital has some correlation with deprivation
People with learning disabilities in employment
Key Messages: Mid Life
Relatively low or poor health outcomes
Worsening trend in health outcome
Equality & diversity Failure to meet targets which may contribute to poor outcomes
Wandsworth has a greater mental health need than the four other PCTs in South West London and England as a whole. (Mental Illness Needs Index 2000)
Increasing rates of HIV diagnoses in Wandsworth. South West London has a relatively high proportion of cases diagnosed late
Increasing rates of hospital admissions attributable to alcohol
Increasing rate of TB
Smoking prevalence is higher in more deprived areas, and cessation services show an underrepresentation of clients under 35 years
The number of people with a registered learning disability is expected to grow by approximately 520 people by 2020 Disproportionate rate of mental health admissions for black minority ethnic groups
Cervical screening
Breast screening target
Bowel screening target
Those with learning disabilities are currently below target for being in settled accommodation

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
182
Key Messages: Pre and Post Retirement
Relatively low or poor health outcomes
Worsening trend in health outcome
Equality & diversity Failure to meet targets which may contribute to poor outcomes
Life expectancy at 65 for females was 20.2 years, and for males was 17.2 years. Both were significantly lower for Wandsworth compared to London as a whole Relatively low percentage of patients who feel that they have enough support to manage their long-term condition. For those that are admitted to hospital they have longer than expected lengths of stay High level of undiagnosed long-term conditions: COPD, hypertension, and atrial fibrillation Independence for older people through rehabilitation and intermediate care
Mortality rates for all causes and all cancers are significantly higher for males and females than London and England; neither is higher than Inner London Female mortality trends, particularly where breast and lung cancer has been diagnosed
The levels of under-75 mortality in Wandsworth show some difference between males and females Mortality in the more deprived areas of Wandsworth is higher than expected (circulatory disease, cancer and chronic obstructive pulmonary disease). This largely accounts for the 6-7 year difference in life expectancy between the deprived and affluent in Wandsworth Emergency admissions to hospital are correlated with deprivation The percentage of carers whose needs were assessed or reviewed by the council was in the lowest quarter of all London Boroughs. This is recognised as a high priority and actions are in place; however, this historical position does not directly correlate to service support being provided to carers.
The breast symptom two-week wait target underperformed (87% against the target of 93%) and has been caused by new processed and insufficient capacity Flu immunisation in the over 65s was also significantly lower than Inner London, London and England Hospital discharge for COPD patients does not meet required standards Two targets for under-75 mortality were set out for 2010 under Our Healthier Nation: Circulatory Disease and Cancer. The circulatory target of 99 (DSR) was reached with a 2006-8 actual of 89, but the cancer target of 107 (DSR) has not yet been reached, with a 2006-8 actual of 126

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
183
Key Messages: Older Age
Relatively low or poor health outcomes
Worsening trend in health outcome
Equality & diversity Failure to meet targets which may contribute to poor outcomes
Wandsworth has a significantly higher rate of excess winter deaths than England
The number of people over 65 with dementia is expected to increase by 7% to 2,200 in 2020
The number of people over 65 with depression is expected to remain stable at 2,200 until 2020
The number of people over 65 with a bladder problem is expected to remain stable at 4,400 until 2020
The complexity of managing people in the community with long-term care needs is ever-increasing
Emergency
admissions for
fractured neck of
femur in the over
65s
Overrepresentation of minority ethnic groups receiving support from adult social services Adults social care provision is correlated with deprivation There are pockets of deprived older people largely correlated to the most deprived Wandsworth wards Council day service support for older people is used disproportionately by women Wandsworth has the second highest proportion of women aged 75+ living alone in London at 68.6% (HSE 2007)
The number of people aged 90+ is expected to increase by 20% over the next five years
Flu immunisation in the over 65s was significantly lower than Inner London, London and England. The percentage of people having access to appropriate end of life care and dying at home was 18.5% in 2008. This was within the lowest quarter of all Inner London boroughs

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
184
APPENDIX 5 Attributes of a Good Pharmaceutical Service World Class Pharmacy – Pharmacy White Paper

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
185
APPENDIX 6 Patient Engagement http://www.wandsworth.nhs.uk/gettherighttreatment/Pharmacists/Pages/Pharmacyneedsassessment.aspx

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
186
APPENDIX 7 PNA Briefing for Stakeholders
Briefing: The First Pharmaceutical Needs Assessment The PCT has a statutory duty to publish its first pharmaceutical needs assessment (PNA) by 1st February 2011. Failure to meet this duty could lead to a judicial review. Background The White Paper „Pharmacy in England: Building on Strengths – Delivering the Future‟ was published by the Department of Health in April 2008. It highlighted the variation in the structure and data requirements of PCT PNAs and confirmed that they required further review and strengthening to ensure they are an effective and robust commissioning tool which supports PCT decisions. The Health Act 2009 amended the National Health Service Act 2006 to include provisions for regulations to set out the minimum standards for PNAs. The regulations were consulted on in late 2009/early 2010, were laid in Parliament on 26 March 2010 and came into force on 24 May 2010. The Duty on the PCT The regulations place a statutory duty on each PCT to develop and publish their first PNA by 1 February 2011. The regulations set out the minimum requirements for the first PNA produced under this duty, and these include such things as data on the health needs of the PCT‟s population, current provision of pharmaceutical services, gaps in current provision and how the PCT proposes to close these gaps. The PNA will also consider the future needs for services. PCTs will be required to undertake a consultation on their first PNA for a minimum of 60 days, and the regulations list those persons and organisations that must be consulted, like the Local Pharmaceutical Committee, Local Medical Committee, LINKs and other patient and public groups. The PNA will be updated at least every three years. Market Entry In addition to being a tool to commission pharmaceutical services, subject to new regulations, PNAs will in future be used to determine applications from pharmacy and appliance contractors to open new premises in the PCT‟s area, or to move to new premises. This will replace the current system whereby the PCT decides if it is necessary or expedient to approve an application in order to secure access to pharmaceutical services in a particular area (also known as the control of entry system) and will help the PCT to commission pharmaceutical services to meet the health needs of its population. It is therefore important that the PNA is a robust document and that it links to the PCT‟s Joint Strategic Needs Assessment. For further information on the pharmaceutical needs assessment (PNA) in Wandsworth please contact David Tambyrajah, Community Pharmacy Lead, at [email protected] or on 020 8812 7770.

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
187
APPENDIX 8 NHS Wandsworth Commissioning Strategy
Our Vision
Our vision is to transform the health of people living and working in Wandsworth. We will work with local people,
communities and our partners to deliver high quality services that are patient centred, safe and innovative. We want all
our local communities to be ambitious about their own health and to challenge us to commission the best possible care
in the best possible environments within our resources.
Our Values
In partnership with staff, key clinicians and partners we have developed our values to underpin our commissioning
approach: outward looking, focused on high quality outcomes, based on honesty and integrity, trustworthy and open,
person centred and listening, collaborative, innovative and professional
1. Help people to live
longer and healthier
lives, particularly
those living in
Wandsworth’s most
deprived communities
2. Support young
people to take control
of their own health
earlier, so they
continue to make
healthier choices
throughout their lives
Average index of multiple
deprivation score
5. Improve the quality of life of people living with long term and complex health conditions and their carers by improving the quality, range and choice of services and giving them information to better manage their own health
Goals
Staying Healthy 1. Staying Healthy programme
4. Improve access, quality and choice of service provision across all care pathways and in appropriate settings.
3. Educate people
about mental
wellbeing, sexual
health, drugs, alcohol
and obesity. Help
prevent and diagnose
earlier and improve
services.
2. Delivering the Children and
Young People’s Plan
3. Maternity
4. Drugs and Alcohol Harm
reduction
5. Sexual Health
6. Mental Health Strategy
10. Long Term Conditions /
Disease Management
11. End of Life
7. Urgent Care
8. Secondary and tertiary care
Service redesign
9. Polysystems and Primary /
Community Service Redesign
Strategic Initiatives
Percentage of patients who spend less
than four hours in A&E.
Proportion of women aged 25 -64
screened for cervical cancer.
Life expectancy at time of birth
Under 18 conception rate.
Smoking quitters per 100,000
population.
Rate of hospital admissions per
100,000 for alcohol related harm.
Cardiovascular disease mortality rate.
Proportion of deaths that occur at home.
Links to WCC Outcomes Care pathway
Long term
conditions
Children and
young people
End of Life
Acute Care
Maternity and
newborn
Mental health
Planned Care
Proportion of children who complete
MMR immunisation by 2nd birthday.
Supporting Initiatives
12. Demand Management
13. Cost savings initiatives

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
APPENDIX 9 Joint letter from PSNC and BMA supporting improved collaboration between Community Pharmacy and General Practice

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
APPENDIX 10 Community Pharmacy Opening Hours Sept 2010

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
Commissioning Tools

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
APPENDIX 11 Community Pharmacy Enhanced Services Sept 2010

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
Community Pharmacy Enhanced Services (cont)

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011

PHARMACEUTICAL NEEDS ASSESSMENT FOR WANDSWORTH FEBRUARY 2011
APPENDIX 12 Commissioning Tools
These tools have been published and developed prior to the publication of the Government's White Paper, Equity and Excellence.
Polyclinics finance and commissioner model The tool aims to make provision of services more patient-focused by commissioning polyclinic services at the levels at which they are required.
June 2008 Provides PCTs with knowledge and tools to be able to provide
an affordable polysystem offering.
Draft commissioning guidance The tool sets out the various different sections of a commissioning specification for PCTs commissioning a polyclinic hub.
September 2008
Describes the ethos of a polyclinic so that potential providers understand how they would be expected to work within this new model of care.
Project planning framework A practical guide to help PCTs in the project management aspect of implementing a new polysystem.
September 2008
A practical guide to help PCTs in the project management aspect of implementing a new polysystem.
Polyclinics communications toolkit A practical tool for PCTs to use when communicating messages about polyclinics locally.
February 2009
Provides examples of innovative ways to promote this new service model that will appeal to different sections of the population.
Commissioning pharmacy services A step by step guide to the commissioning of pharmacy services within a polysystem.
March 2009 Provides PCTs with knowledge and tools to be able to provide pharmacy services within polysystem
Procurement and contracting guidance for clinical commissioners
A short reference guide detailing the different options PCTs have for procurement.
June 2009 Guidance for clinical commissioners unused to contracting and procurement
Super contract and guidance Draft super contract template to allow PCTs to deliver integrated working from multiple providers
June 2009 Provides PCTs with knowledge of how to utilise a super contract to govern existing contracts within the new framework of a polyclinic and how to still be able to achieve the outcomes of a polyclinic
Polyclinics consumerism toolkit: "Focusing on the person in the patient - Changing Healthcare to healthCare”
A practical guide for PCTs to understand how services can be commissioned in response to patient experience
July 2009 PCTs can commission in response to patient experience.
Evaluation outputs A two-year study of polysystem implementation Ongoing Practical outputs to support future GP commissioning, whilst providing practical insight to patent engagement.
Urgent care guidance - “Commissioning a new delivery model for unscheduled care in London”
Translation of the HfL unscheduled care commissioning guidance to include the role of polysystems
February 2010
Supporting PCTs to translate this guidance into tangible, local implementation plans