A Petition to the Board of Pharmacy Specialties Requesting - ACCP
416
A Petition to the Board of Pharmacy Specialties Requesting Recognition of Pediatric Pharmacy Practice as a Specialty Prepared by: Marcia L. Buck Lea S. Eiland Matthew R. Helms Peter N. Johnson Patti G. Manolakis Mitchel C. Rothholz Chasity M. Shelton Jann B. Skelton C. Edwin Webb David R. Witmer Sponsored by: American College of Clinical Pharmacy (ACCP) American Pharmacists Association (APhA) American Society of HealthSystem Pharmacists (ASHP) Pediatric Pharmacy Advocacy Group (PPAG) November 2012
Transcript of A Petition to the Board of Pharmacy Specialties Requesting - ACCP
A13 Petition13 to13 the13 13
Board13 of13 Pharmacy13 Specialties13 13
Requesting13 Recognition13 of13 13
Pediatric13 Pharmacy13 Practice13
as13 a13 Specialty13 13
Prepared13 by13
Marcia13 L13 Buck13 13 13
Lea13 S13 Eiland13
Matthew13 R13 Helms13
Peter13 N13 Johnson13
Patti13 G13 Manolakis13
Mitchel13 C13 Rothholz13
Chasity13 M13 Shelton13
Jann13 B13 Skelton13
C13 Edwin13 Webb13
David13 R13 Witmer13 13
Sponsored13 by13
American13 College13 of13 Clinical13 Pharmacy13 (ACCP)13
American13 Pharmacists13 Association13 (APhA)13
American13 Society13 of13 Health-shy‐System13 Pharmacists13 (ASHP)13
Pediatric13 Pharmacy13 Advocacy13 Group13 (PPAG)13 13
November13 201213
Table13 of13 Contents13 13 Task13 Group13 on13 Pediatric13 Pharmacy13 Practice13 Member13 Rosterhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip313
13 Definition13 of13 Pediatric13 Pharmacy13 Practicehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip413
13 Executive13 Summaryhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 513
13 Criterion13 A13 13 Needhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 1413
13 Criterion13 B13 13 Demandhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip2813
13 Criterion13 C13 13 Number13 and13 Timehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip3813
13 Criterion13 D13 13 Specialized13 Knowledgehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip4413
13 Criterion13 E13 13 Specialized13 Functionshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 5613
13 Criterion13 F13 13 Education13 andor13 Traininghelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 6513
13 Criterion13 G13 13 Transmission13 of13 Knowledgehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 7513
13 13 Appendices13 13 Appendix13 B-shy‐113 Letters13 of13 Supporthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip8813 13 Appendix13 C-shy‐113 Pediatric13 Pharmacist13 Surveyhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip10613
13 Appendix13 D-shy‐113 Report13 of13 the13 Role13 Delineation13 Study13 of13 Pediatric13 Pharmacyhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip11113 13 Appendix13 D-shy‐213 NAPLEX13 Blueprinthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip20913
13 Appendix13 F-shy‐113 ASHP13 Educational13 Outcomes13 Goals13 and13 Objectives13 for13 Postgraduate13 Year13 Two13 (PGY2)13 Pharmacy13 13 13 13 Residencies13 in13 Pediatricshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip21313
13 Appendix13 F-shy‐213 ACCP13 Guidelines13 for13 Clinical13 Research13 Fellowship13 Training13 Programshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip24113
13 Appendix13 G-shy‐113 Pediatric13 Pharmacy13 Bibliographyhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip24413
13 Appendix13 G-shy‐213 Selected13 Pediatric13 Pharmacy13 Literaturehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip26413
13 Appendix13 G-shy‐313 ACPE13 PLAN13 Programming13 ndash13 Live13 Forum13 Knowledge13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip31913
13 Appendix13 G-shy‐413 ACPE13 PLAN13 Programming13 ndash13 Live13 Forum13 Application13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip35213
13 Appendix13 G-shy‐513 ACPE13 PLAN13 Programming13 ndash13 Home13 Study13 Knowledge13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip35913
13 Appendix13 G-shy‐613 ACPE13 PLAN13 programming13 ndash13 Home13 Study13 Application13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip37313
13 Appendix13 G-shy‐713 Sample13 Educational13 Program13 Materialshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip37513
13 Signatures13 of13 Supporthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip38713
Task13 Group13 on13 Pediatric13 Pharmacy13 Practice13 Member13 Roster13
13 Marcia13 L13 Buck13 PharmD13 FCCP13 FPPAG13 Clinical13 Pharmacy13 Coordinator13 UVA13 Childrens13 Hospital13 Associate13 Professor13 Pediatrics13 School13 of13 Medicine13 Clinical13 Associate13 Professor13 School13 of13 Nursing13 University13 of13 Virginia13 Department13 of13 Pharmacy13 Services13 Box13 80067413 Charlottesville13 VA13 2290813 (434)13 760-shy‐484413 mlb3uvirginiaedu13 13 Lea13 S13 Eiland13 PharmD13 BCPS13 FASHP13 Associate13 Clinical13 Professor13 13 Associate13 Department13 Head13 13 Department13 of13 Pharmacy13 Practice13 13 Auburn13 University13 Harrison13 School13 of13 Pharmacy13 13 Clinical13 Associate13 Professor13 of13 Pediatrics13 13 University13 of13 Alabama13 at13 Birmingham13 School13 of13 13 Medicine13 Huntsville13 Regional13 Medical13 Campus13 UABDivision13 of13 Pediatrics13 30113 Governors13 Drive13 SW13 Huntsville13 AL13 3580113 (256)13 551-shy‐444513 eilanlsauburnedu13 13 Matthew13 R13 Helms13 MA13 CAE13 13 Executive13 Director13 13 Pediatric13 Pharmacy13 Advocacy13 Group13 13 795313 Stage13 Hills13 Boulevard13 Suite13 10113 13 Memphis13 TN13 3813313 13 (901)13 380-shy‐361713 matthewhelmsppagorg13 13 13 Peter13 N13 Johnson13 PharmD13 BCPS13 Associate13 Professor13 of13 Pharmacy13 Practice13 PGY113 Pharmacy13 Residency13 Director13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 Clinical13 Pharmacy13 Specialist13 ndash13 Pediatric13 Critical13 Care13 Childrens13 Hospital13 at13 OU13 Medical13 Center13 111013 North13 Stonewall13 CPB13 20613 Oklahoma13 City13 OK13 7311713 (405)13 271-shy‐273013 Peter-shy‐Johnsonouhscedu13 13 13 13 13
Patti13 G13 Manolakis13 PharmD13 President13 PMM13 Consulting13 LLC13 1672613 Hammock13 Creek13 Place13 Charlotte13 NC13 2827813 (704)13 588-shy‐398113 pmanolakispmmcsolutionscom13 13 Mitchel13 C13 Rothholz13 RPh13 MBA13 Chief13 Strategy13 Officer13 American13 Pharmacists13 Association13 221513 Constitution13 Avenue13 NW13 Washington13 DC13 2003713 (202)13 429-shy‐754913 mrothholzaphanetorg13 13 Chasity13 M13 Shelton13 PharmD13 BCPS13 BCNSP13 Assistant13 Professor13 13 Department13 of13 Clinical13 Pharmacy13 13 The13 University13 of13 Tennessee13 13 Health13 Science13 Center13 88113 Madison13 Avenue13 Memphis13 TN13 3816313 (901)13 448-shy‐207413 csheltonuthscedu13 13 Jann13 B13 Skelton13 RPh13 MBA13 President13 Silver13 Pennies13 Consulting13 1713 Spruce13 Road13 North13 Caldwell13 NJ13 0700613 (973)13 228-shy‐328513 jskeltonsilverpenniescom13 13 C13 Edwin13 Webb13 PharmD13 MPH13 Associate13 Executive13 Director13 13 Director13 Government13 and13 Professional13 Affairs13 13 American13 College13 of13 Clinical13 Pharmacy13 13 145513 Pennsylvania13 Avenue13 NW13 Suite13 40013 13 Washington13 DC13 2000413 13 (202)13 621-shy‐182013 ewebbaccpcom13 13 David13 R13 Witmer13 PharmD13 Senior13 Vice13 President13 Chief13 Operating13 Officer13 13 American13 Society13 of13 Health-shy‐System13 Pharmacists13 727213 Wisconsin13 Avenue13 Suite13 219213 Bethesda13 MD13 2081413 (301)13 664-shy‐865913 dwitmerashporg13 13
Disclosure Patti Manolakis and Jann Skelton are under contract with the petitioning organizations to coordinate the development and submission of this petition They received payment for their work on this initiative
13 13 13
13
Definition13 of13 Pediatric13 Pharmacy13 Practice13 13 Pediatric13 pharmacy13 practice13 specializes13 in13 the13 delivery13 of13 patient13 care13 services13 by13 pharmacists13 that13 ensures13 the13 safe13 and13 effective13 use13 of13 medications13 for13 all13 children13 from13 neonates13 through13 adolescents13 The13 practice13 includes13 direct13 patient13 care13 for13 children13 often13 provided13 through13 interprofessional13 health13 care13 teams13 as13 well13 as13 advocacy13 and13 education13 for13 children13 and13 their13 families13 wellness13 and13 health13 promotion13 and13 activities13 that13 advance13 knowledge13 and13 skills13 in13 pediatric13 pharmacy13
13
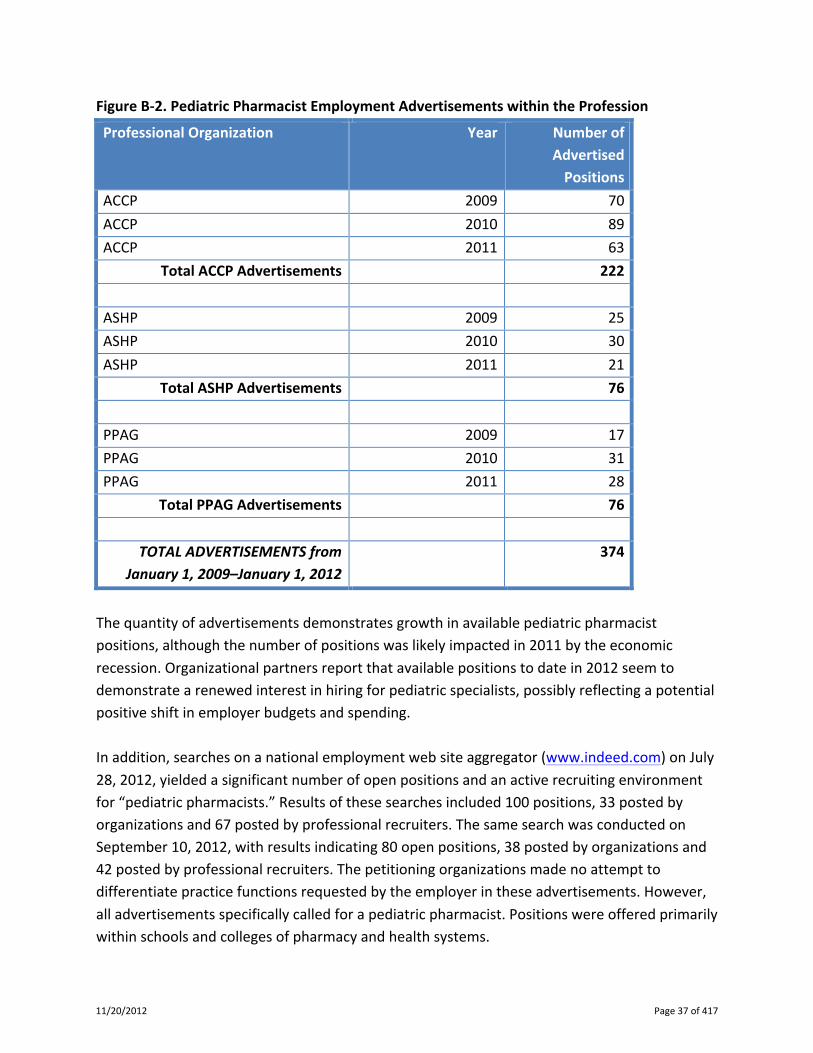
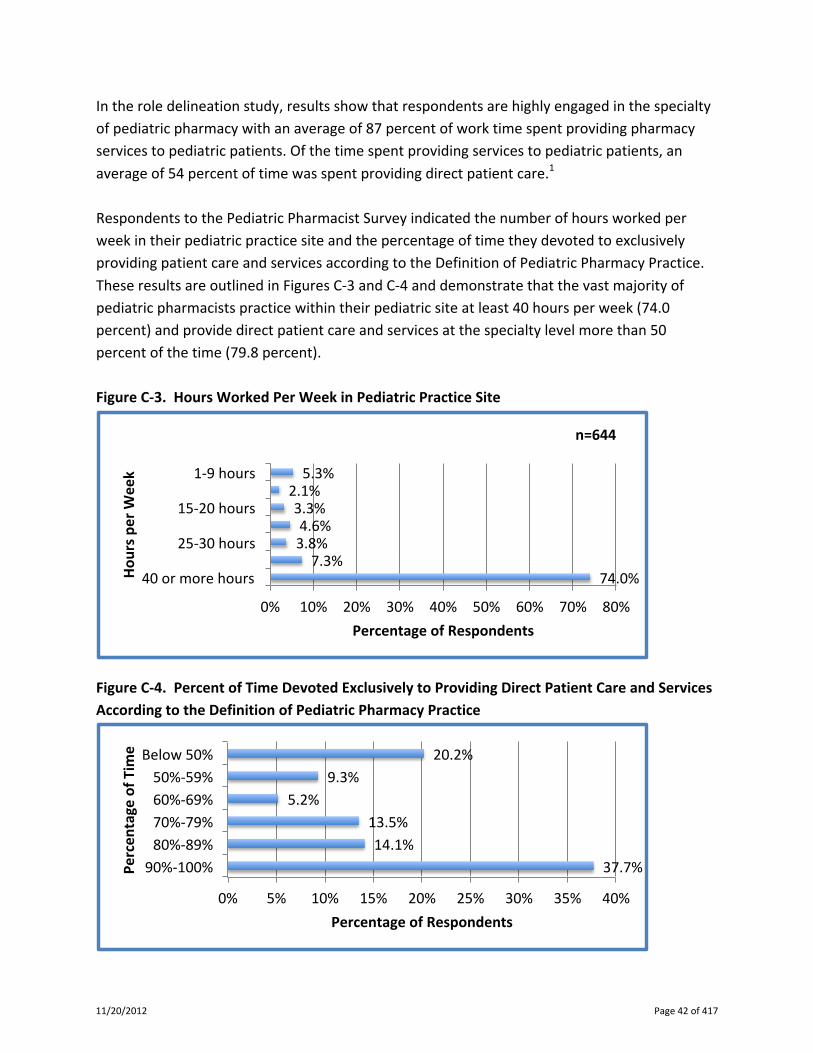
282 May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
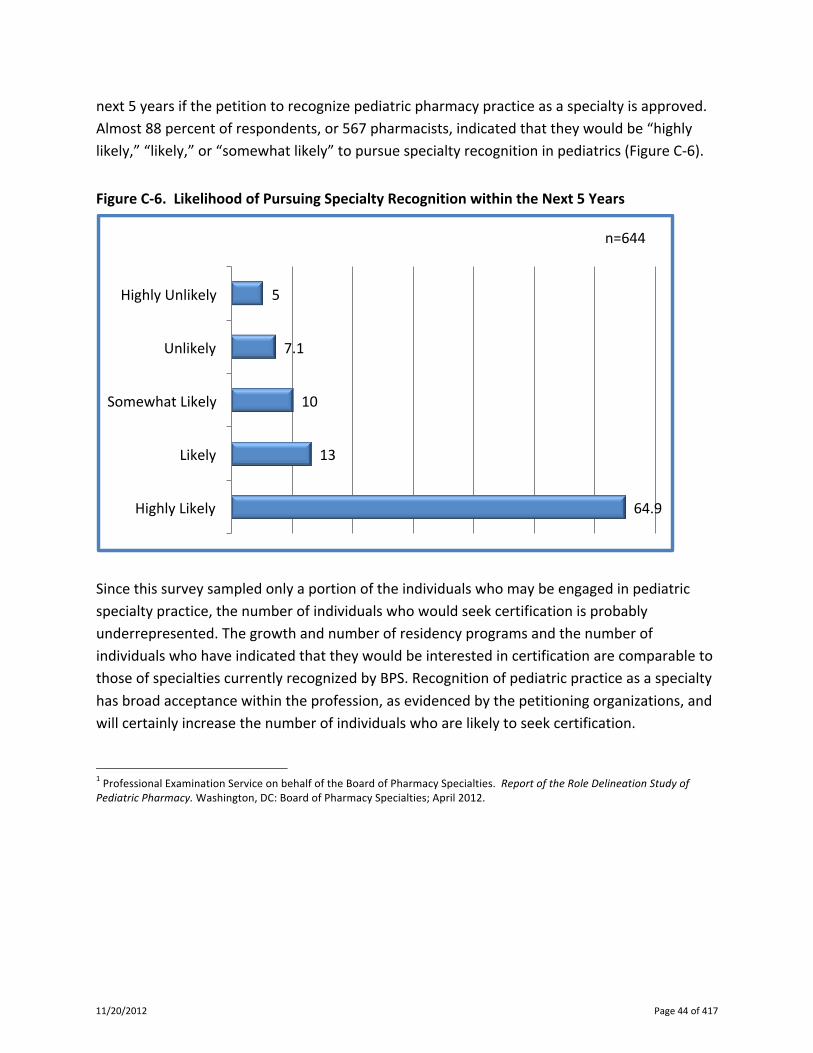
admission medication history can be obtainedHospital leadership is fully committed to 100 compliance
with complete medication reconciliation To meet this andother pharmacy initiatives one pediatric pharmacist shift wasadded per day during this time period The 567 medication rec-onciliationndashrelated clinical interventions performed by pharma-cists indicate that the time and effort of performing medicationreconciliation activities leads to positive benefit for patients
Pharmacist involvement in Mayorsquos medication reconciliationprogram has improved the accuracy of the admit medicationlist with one-quarter of PPML flow sheets corrected during thefirst five weeks As a result of these interventions the comput-er-assisted medication reconciliation process which has contin-ued as described has improved patient care by aiding pharm-acists to complete more thorough medication reconciliation
References1 Bates DW et al The costs of adverse drug events in hospitalized patientsAdverse Drug Events Prevention Study Group JAMA 277307ndash311 Jan 22ndash291997 2 Carter M et al Pharmacist-acquired medication histories in a university hos-pital emergency department Am J Health Syst Pharm 632500ndash2503 Dec 1520063 Bond CA Raehl CL Interrelationships among mortality rates drug coststotal cost of care and length of stay in United States hospitals Summary and rec-ommendations for clinical pharmacy services and staffing Pharmacotherapy21129ndash141 Feb 20014 Bond CA Raehl CL Clinical pharmacy services hospital pharmacy staffingand medication errors in United States hospitals Pharmacotherapy 22134ndash147Feb 20025 Bond CA Raehl CL Clinical pharmacy services pharmacy staffing andadverse drug reactions in United States hospitals Pharmacotherapy 26 735ndash747Jun 20066 The Joint Commission Comprehensive Accreditation Manual for Hospitals 2009The Official Handbook Oakbrook Terrace IL Joint Commission Resources 2008 7 Nester T Hale L Effectiveness of a pharmacist-acquired medication history inpromoting patient safety Am J Health Syst Pharm 592221ndash2225 Nov 15 2002J
Brian Gardner PharmD is Clinical Pediatric Pharmacist Mayo
Eugenio Litta Childrens Hospital Rochester Minnesota and
Kevin Graner RPh is Pharmacy Services Supervisor Please
address correspondence to Brian Gardner GardnerBrian
mayoedu
Online-Only Content
See the online version of this article for Appendix 1 Medication
History Printout
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012
AP1May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
Online-Only ContentAppendix 1 (PCARE) Program Patient Detailed Report Screen and Contained Information
A screen shot of the top of this window is shown along with a description of the information contained in each section of the Patient
Detailed Report PCARE Mayo Eugenio Litta Hospitalrsquos Web-based pharmaceutical care program CC-HPI-PMH Chief Complaint-
History of Present Illness-Past Medical History BMI body mass index BSA body surface area HB Harris Benedict PCR
Polymerase chain reaction BUN blood urea nitrogen INR international normalized ratio APTT activated partial thromboplastin time
CSF cerebrospinal fluid
Demographic information age sex actual weight ideal and aminoglycoside dosing weight body surface area
Hospital room location primary service and pager number
Dates of recent hospitalizations
Infection Control status and isolation requirements
CC-HP-PMH note documentation
Calculations HB equation BMI BSA aminoglycoside dosing weight
Infectious disease service consultations and pager number
Drug allergies
Renal functionstatus
Estimated amp measured creatinine clearance
Dialysis (if applicable) intermittent dialysis peritoneal dialysis or continuous renal replacement therapy (CRRT)
Medication reconciliation history and documentation
All medications within desired time range on a timeline grid andor a drug detail grid
Parenteral nutrition composition and calculations (total calories calories as fatprotein deviation from HB equation)
Microbiology data cultures stains and PCR assays
Selected laboratory data blood counts electrolytes liver enzymes creatinine BUN bilirubin international normalized ratio activated
partial thromboplastin time acidbase status etc
Antimicrobial and other drug assaysserum drug levels
Surgical operative reports
Rule flag information with link to intervention documentation form
Intervention information history and intervention outcomes
Monitors (including links to reference documents) and pharmacist communication notes
Nonformulary drug documentation and nonformulary order history
Urinalysis
CSF results
Warfarin protocol history
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012 Page 277 of 417
Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-

Table13 of13 Contents13 13 Task13 Group13 on13 Pediatric13 Pharmacy13 Practice13 Member13 Rosterhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip313
13 Definition13 of13 Pediatric13 Pharmacy13 Practicehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip413
13 Executive13 Summaryhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 513
13 Criterion13 A13 13 Needhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 1413
13 Criterion13 B13 13 Demandhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip2813
13 Criterion13 C13 13 Number13 and13 Timehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip3813
13 Criterion13 D13 13 Specialized13 Knowledgehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip4413
13 Criterion13 E13 13 Specialized13 Functionshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 5613
13 Criterion13 F13 13 Education13 andor13 Traininghelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 6513
13 Criterion13 G13 13 Transmission13 of13 Knowledgehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip13 7513
13 13 Appendices13 13 Appendix13 B-shy‐113 Letters13 of13 Supporthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip8813 13 Appendix13 C-shy‐113 Pediatric13 Pharmacist13 Surveyhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip10613
13 Appendix13 D-shy‐113 Report13 of13 the13 Role13 Delineation13 Study13 of13 Pediatric13 Pharmacyhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip11113 13 Appendix13 D-shy‐213 NAPLEX13 Blueprinthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip20913
13 Appendix13 F-shy‐113 ASHP13 Educational13 Outcomes13 Goals13 and13 Objectives13 for13 Postgraduate13 Year13 Two13 (PGY2)13 Pharmacy13 13 13 13 Residencies13 in13 Pediatricshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip21313
13 Appendix13 F-shy‐213 ACCP13 Guidelines13 for13 Clinical13 Research13 Fellowship13 Training13 Programshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip24113
13 Appendix13 G-shy‐113 Pediatric13 Pharmacy13 Bibliographyhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip24413
13 Appendix13 G-shy‐213 Selected13 Pediatric13 Pharmacy13 Literaturehelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip26413
13 Appendix13 G-shy‐313 ACPE13 PLAN13 Programming13 ndash13 Live13 Forum13 Knowledge13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip31913
13 Appendix13 G-shy‐413 ACPE13 PLAN13 Programming13 ndash13 Live13 Forum13 Application13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip35213
13 Appendix13 G-shy‐513 ACPE13 PLAN13 Programming13 ndash13 Home13 Study13 Knowledge13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip35913
13 Appendix13 G-shy‐613 ACPE13 PLAN13 programming13 ndash13 Home13 Study13 Application13 Activityhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip37313
13 Appendix13 G-shy‐713 Sample13 Educational13 Program13 Materialshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip37513
13 Signatures13 of13 Supporthelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip38713
Task13 Group13 on13 Pediatric13 Pharmacy13 Practice13 Member13 Roster13
13 Marcia13 L13 Buck13 PharmD13 FCCP13 FPPAG13 Clinical13 Pharmacy13 Coordinator13 UVA13 Childrens13 Hospital13 Associate13 Professor13 Pediatrics13 School13 of13 Medicine13 Clinical13 Associate13 Professor13 School13 of13 Nursing13 University13 of13 Virginia13 Department13 of13 Pharmacy13 Services13 Box13 80067413 Charlottesville13 VA13 2290813 (434)13 760-shy‐484413 mlb3uvirginiaedu13 13 Lea13 S13 Eiland13 PharmD13 BCPS13 FASHP13 Associate13 Clinical13 Professor13 13 Associate13 Department13 Head13 13 Department13 of13 Pharmacy13 Practice13 13 Auburn13 University13 Harrison13 School13 of13 Pharmacy13 13 Clinical13 Associate13 Professor13 of13 Pediatrics13 13 University13 of13 Alabama13 at13 Birmingham13 School13 of13 13 Medicine13 Huntsville13 Regional13 Medical13 Campus13 UABDivision13 of13 Pediatrics13 30113 Governors13 Drive13 SW13 Huntsville13 AL13 3580113 (256)13 551-shy‐444513 eilanlsauburnedu13 13 Matthew13 R13 Helms13 MA13 CAE13 13 Executive13 Director13 13 Pediatric13 Pharmacy13 Advocacy13 Group13 13 795313 Stage13 Hills13 Boulevard13 Suite13 10113 13 Memphis13 TN13 3813313 13 (901)13 380-shy‐361713 matthewhelmsppagorg13 13 13 Peter13 N13 Johnson13 PharmD13 BCPS13 Associate13 Professor13 of13 Pharmacy13 Practice13 PGY113 Pharmacy13 Residency13 Director13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 Clinical13 Pharmacy13 Specialist13 ndash13 Pediatric13 Critical13 Care13 Childrens13 Hospital13 at13 OU13 Medical13 Center13 111013 North13 Stonewall13 CPB13 20613 Oklahoma13 City13 OK13 7311713 (405)13 271-shy‐273013 Peter-shy‐Johnsonouhscedu13 13 13 13 13
Patti13 G13 Manolakis13 PharmD13 President13 PMM13 Consulting13 LLC13 1672613 Hammock13 Creek13 Place13 Charlotte13 NC13 2827813 (704)13 588-shy‐398113 pmanolakispmmcsolutionscom13 13 Mitchel13 C13 Rothholz13 RPh13 MBA13 Chief13 Strategy13 Officer13 American13 Pharmacists13 Association13 221513 Constitution13 Avenue13 NW13 Washington13 DC13 2003713 (202)13 429-shy‐754913 mrothholzaphanetorg13 13 Chasity13 M13 Shelton13 PharmD13 BCPS13 BCNSP13 Assistant13 Professor13 13 Department13 of13 Clinical13 Pharmacy13 13 The13 University13 of13 Tennessee13 13 Health13 Science13 Center13 88113 Madison13 Avenue13 Memphis13 TN13 3816313 (901)13 448-shy‐207413 csheltonuthscedu13 13 Jann13 B13 Skelton13 RPh13 MBA13 President13 Silver13 Pennies13 Consulting13 1713 Spruce13 Road13 North13 Caldwell13 NJ13 0700613 (973)13 228-shy‐328513 jskeltonsilverpenniescom13 13 C13 Edwin13 Webb13 PharmD13 MPH13 Associate13 Executive13 Director13 13 Director13 Government13 and13 Professional13 Affairs13 13 American13 College13 of13 Clinical13 Pharmacy13 13 145513 Pennsylvania13 Avenue13 NW13 Suite13 40013 13 Washington13 DC13 2000413 13 (202)13 621-shy‐182013 ewebbaccpcom13 13 David13 R13 Witmer13 PharmD13 Senior13 Vice13 President13 Chief13 Operating13 Officer13 13 American13 Society13 of13 Health-shy‐System13 Pharmacists13 727213 Wisconsin13 Avenue13 Suite13 219213 Bethesda13 MD13 2081413 (301)13 664-shy‐865913 dwitmerashporg13 13
Disclosure Patti Manolakis and Jann Skelton are under contract with the petitioning organizations to coordinate the development and submission of this petition They received payment for their work on this initiative
13 13 13
13
Definition13 of13 Pediatric13 Pharmacy13 Practice13 13 Pediatric13 pharmacy13 practice13 specializes13 in13 the13 delivery13 of13 patient13 care13 services13 by13 pharmacists13 that13 ensures13 the13 safe13 and13 effective13 use13 of13 medications13 for13 all13 children13 from13 neonates13 through13 adolescents13 The13 practice13 includes13 direct13 patient13 care13 for13 children13 often13 provided13 through13 interprofessional13 health13 care13 teams13 as13 well13 as13 advocacy13 and13 education13 for13 children13 and13 their13 families13 wellness13 and13 health13 promotion13 and13 activities13 that13 advance13 knowledge13 and13 skills13 in13 pediatric13 pharmacy13
13
282 May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
admission medication history can be obtainedHospital leadership is fully committed to 100 compliance
with complete medication reconciliation To meet this andother pharmacy initiatives one pediatric pharmacist shift wasadded per day during this time period The 567 medication rec-onciliationndashrelated clinical interventions performed by pharma-cists indicate that the time and effort of performing medicationreconciliation activities leads to positive benefit for patients
Pharmacist involvement in Mayorsquos medication reconciliationprogram has improved the accuracy of the admit medicationlist with one-quarter of PPML flow sheets corrected during thefirst five weeks As a result of these interventions the comput-er-assisted medication reconciliation process which has contin-ued as described has improved patient care by aiding pharm-acists to complete more thorough medication reconciliation
References1 Bates DW et al The costs of adverse drug events in hospitalized patientsAdverse Drug Events Prevention Study Group JAMA 277307ndash311 Jan 22ndash291997 2 Carter M et al Pharmacist-acquired medication histories in a university hos-pital emergency department Am J Health Syst Pharm 632500ndash2503 Dec 1520063 Bond CA Raehl CL Interrelationships among mortality rates drug coststotal cost of care and length of stay in United States hospitals Summary and rec-ommendations for clinical pharmacy services and staffing Pharmacotherapy21129ndash141 Feb 20014 Bond CA Raehl CL Clinical pharmacy services hospital pharmacy staffingand medication errors in United States hospitals Pharmacotherapy 22134ndash147Feb 20025 Bond CA Raehl CL Clinical pharmacy services pharmacy staffing andadverse drug reactions in United States hospitals Pharmacotherapy 26 735ndash747Jun 20066 The Joint Commission Comprehensive Accreditation Manual for Hospitals 2009The Official Handbook Oakbrook Terrace IL Joint Commission Resources 2008 7 Nester T Hale L Effectiveness of a pharmacist-acquired medication history inpromoting patient safety Am J Health Syst Pharm 592221ndash2225 Nov 15 2002J
Brian Gardner PharmD is Clinical Pediatric Pharmacist Mayo
Eugenio Litta Childrens Hospital Rochester Minnesota and
Kevin Graner RPh is Pharmacy Services Supervisor Please
address correspondence to Brian Gardner GardnerBrian
mayoedu
Online-Only Content
See the online version of this article for Appendix 1 Medication
History Printout
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012
AP1May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
Online-Only ContentAppendix 1 (PCARE) Program Patient Detailed Report Screen and Contained Information
A screen shot of the top of this window is shown along with a description of the information contained in each section of the Patient
Detailed Report PCARE Mayo Eugenio Litta Hospitalrsquos Web-based pharmaceutical care program CC-HPI-PMH Chief Complaint-
History of Present Illness-Past Medical History BMI body mass index BSA body surface area HB Harris Benedict PCR
Polymerase chain reaction BUN blood urea nitrogen INR international normalized ratio APTT activated partial thromboplastin time
CSF cerebrospinal fluid
Demographic information age sex actual weight ideal and aminoglycoside dosing weight body surface area
Hospital room location primary service and pager number
Dates of recent hospitalizations
Infection Control status and isolation requirements
CC-HP-PMH note documentation
Calculations HB equation BMI BSA aminoglycoside dosing weight
Infectious disease service consultations and pager number
Drug allergies
Renal functionstatus
Estimated amp measured creatinine clearance
Dialysis (if applicable) intermittent dialysis peritoneal dialysis or continuous renal replacement therapy (CRRT)
Medication reconciliation history and documentation
All medications within desired time range on a timeline grid andor a drug detail grid
Parenteral nutrition composition and calculations (total calories calories as fatprotein deviation from HB equation)
Microbiology data cultures stains and PCR assays
Selected laboratory data blood counts electrolytes liver enzymes creatinine BUN bilirubin international normalized ratio activated
partial thromboplastin time acidbase status etc
Antimicrobial and other drug assaysserum drug levels
Surgical operative reports
Rule flag information with link to intervention documentation form
Intervention information history and intervention outcomes
Monitors (including links to reference documents) and pharmacist communication notes
Nonformulary drug documentation and nonformulary order history
Urinalysis
CSF results
Warfarin protocol history
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012 Page 277 of 417
Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-
Task13 Group13 on13 Pediatric13 Pharmacy13 Practice13 Member13 Roster13
13 Marcia13 L13 Buck13 PharmD13 FCCP13 FPPAG13 Clinical13 Pharmacy13 Coordinator13 UVA13 Childrens13 Hospital13 Associate13 Professor13 Pediatrics13 School13 of13 Medicine13 Clinical13 Associate13 Professor13 School13 of13 Nursing13 University13 of13 Virginia13 Department13 of13 Pharmacy13 Services13 Box13 80067413 Charlottesville13 VA13 2290813 (434)13 760-shy‐484413 mlb3uvirginiaedu13 13 Lea13 S13 Eiland13 PharmD13 BCPS13 FASHP13 Associate13 Clinical13 Professor13 13 Associate13 Department13 Head13 13 Department13 of13 Pharmacy13 Practice13 13 Auburn13 University13 Harrison13 School13 of13 Pharmacy13 13 Clinical13 Associate13 Professor13 of13 Pediatrics13 13 University13 of13 Alabama13 at13 Birmingham13 School13 of13 13 Medicine13 Huntsville13 Regional13 Medical13 Campus13 UABDivision13 of13 Pediatrics13 30113 Governors13 Drive13 SW13 Huntsville13 AL13 3580113 (256)13 551-shy‐444513 eilanlsauburnedu13 13 Matthew13 R13 Helms13 MA13 CAE13 13 Executive13 Director13 13 Pediatric13 Pharmacy13 Advocacy13 Group13 13 795313 Stage13 Hills13 Boulevard13 Suite13 10113 13 Memphis13 TN13 3813313 13 (901)13 380-shy‐361713 matthewhelmsppagorg13 13 13 Peter13 N13 Johnson13 PharmD13 BCPS13 Associate13 Professor13 of13 Pharmacy13 Practice13 PGY113 Pharmacy13 Residency13 Director13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 Clinical13 Pharmacy13 Specialist13 ndash13 Pediatric13 Critical13 Care13 Childrens13 Hospital13 at13 OU13 Medical13 Center13 111013 North13 Stonewall13 CPB13 20613 Oklahoma13 City13 OK13 7311713 (405)13 271-shy‐273013 Peter-shy‐Johnsonouhscedu13 13 13 13 13
Patti13 G13 Manolakis13 PharmD13 President13 PMM13 Consulting13 LLC13 1672613 Hammock13 Creek13 Place13 Charlotte13 NC13 2827813 (704)13 588-shy‐398113 pmanolakispmmcsolutionscom13 13 Mitchel13 C13 Rothholz13 RPh13 MBA13 Chief13 Strategy13 Officer13 American13 Pharmacists13 Association13 221513 Constitution13 Avenue13 NW13 Washington13 DC13 2003713 (202)13 429-shy‐754913 mrothholzaphanetorg13 13 Chasity13 M13 Shelton13 PharmD13 BCPS13 BCNSP13 Assistant13 Professor13 13 Department13 of13 Clinical13 Pharmacy13 13 The13 University13 of13 Tennessee13 13 Health13 Science13 Center13 88113 Madison13 Avenue13 Memphis13 TN13 3816313 (901)13 448-shy‐207413 csheltonuthscedu13 13 Jann13 B13 Skelton13 RPh13 MBA13 President13 Silver13 Pennies13 Consulting13 1713 Spruce13 Road13 North13 Caldwell13 NJ13 0700613 (973)13 228-shy‐328513 jskeltonsilverpenniescom13 13 C13 Edwin13 Webb13 PharmD13 MPH13 Associate13 Executive13 Director13 13 Director13 Government13 and13 Professional13 Affairs13 13 American13 College13 of13 Clinical13 Pharmacy13 13 145513 Pennsylvania13 Avenue13 NW13 Suite13 40013 13 Washington13 DC13 2000413 13 (202)13 621-shy‐182013 ewebbaccpcom13 13 David13 R13 Witmer13 PharmD13 Senior13 Vice13 President13 Chief13 Operating13 Officer13 13 American13 Society13 of13 Health-shy‐System13 Pharmacists13 727213 Wisconsin13 Avenue13 Suite13 219213 Bethesda13 MD13 2081413 (301)13 664-shy‐865913 dwitmerashporg13 13
Disclosure Patti Manolakis and Jann Skelton are under contract with the petitioning organizations to coordinate the development and submission of this petition They received payment for their work on this initiative
13 13 13
13
Definition13 of13 Pediatric13 Pharmacy13 Practice13 13 Pediatric13 pharmacy13 practice13 specializes13 in13 the13 delivery13 of13 patient13 care13 services13 by13 pharmacists13 that13 ensures13 the13 safe13 and13 effective13 use13 of13 medications13 for13 all13 children13 from13 neonates13 through13 adolescents13 The13 practice13 includes13 direct13 patient13 care13 for13 children13 often13 provided13 through13 interprofessional13 health13 care13 teams13 as13 well13 as13 advocacy13 and13 education13 for13 children13 and13 their13 families13 wellness13 and13 health13 promotion13 and13 activities13 that13 advance13 knowledge13 and13 skills13 in13 pediatric13 pharmacy13
13
282 May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
admission medication history can be obtainedHospital leadership is fully committed to 100 compliance
with complete medication reconciliation To meet this andother pharmacy initiatives one pediatric pharmacist shift wasadded per day during this time period The 567 medication rec-onciliationndashrelated clinical interventions performed by pharma-cists indicate that the time and effort of performing medicationreconciliation activities leads to positive benefit for patients
Pharmacist involvement in Mayorsquos medication reconciliationprogram has improved the accuracy of the admit medicationlist with one-quarter of PPML flow sheets corrected during thefirst five weeks As a result of these interventions the comput-er-assisted medication reconciliation process which has contin-ued as described has improved patient care by aiding pharm-acists to complete more thorough medication reconciliation
References1 Bates DW et al The costs of adverse drug events in hospitalized patientsAdverse Drug Events Prevention Study Group JAMA 277307ndash311 Jan 22ndash291997 2 Carter M et al Pharmacist-acquired medication histories in a university hos-pital emergency department Am J Health Syst Pharm 632500ndash2503 Dec 1520063 Bond CA Raehl CL Interrelationships among mortality rates drug coststotal cost of care and length of stay in United States hospitals Summary and rec-ommendations for clinical pharmacy services and staffing Pharmacotherapy21129ndash141 Feb 20014 Bond CA Raehl CL Clinical pharmacy services hospital pharmacy staffingand medication errors in United States hospitals Pharmacotherapy 22134ndash147Feb 20025 Bond CA Raehl CL Clinical pharmacy services pharmacy staffing andadverse drug reactions in United States hospitals Pharmacotherapy 26 735ndash747Jun 20066 The Joint Commission Comprehensive Accreditation Manual for Hospitals 2009The Official Handbook Oakbrook Terrace IL Joint Commission Resources 2008 7 Nester T Hale L Effectiveness of a pharmacist-acquired medication history inpromoting patient safety Am J Health Syst Pharm 592221ndash2225 Nov 15 2002J
Brian Gardner PharmD is Clinical Pediatric Pharmacist Mayo
Eugenio Litta Childrens Hospital Rochester Minnesota and
Kevin Graner RPh is Pharmacy Services Supervisor Please
address correspondence to Brian Gardner GardnerBrian
mayoedu
Online-Only Content
See the online version of this article for Appendix 1 Medication
History Printout
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012
AP1May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
Online-Only ContentAppendix 1 (PCARE) Program Patient Detailed Report Screen and Contained Information
A screen shot of the top of this window is shown along with a description of the information contained in each section of the Patient
Detailed Report PCARE Mayo Eugenio Litta Hospitalrsquos Web-based pharmaceutical care program CC-HPI-PMH Chief Complaint-
History of Present Illness-Past Medical History BMI body mass index BSA body surface area HB Harris Benedict PCR
Polymerase chain reaction BUN blood urea nitrogen INR international normalized ratio APTT activated partial thromboplastin time
CSF cerebrospinal fluid
Demographic information age sex actual weight ideal and aminoglycoside dosing weight body surface area
Hospital room location primary service and pager number
Dates of recent hospitalizations
Infection Control status and isolation requirements
CC-HP-PMH note documentation
Calculations HB equation BMI BSA aminoglycoside dosing weight
Infectious disease service consultations and pager number
Drug allergies
Renal functionstatus
Estimated amp measured creatinine clearance
Dialysis (if applicable) intermittent dialysis peritoneal dialysis or continuous renal replacement therapy (CRRT)
Medication reconciliation history and documentation
All medications within desired time range on a timeline grid andor a drug detail grid
Parenteral nutrition composition and calculations (total calories calories as fatprotein deviation from HB equation)
Microbiology data cultures stains and PCR assays
Selected laboratory data blood counts electrolytes liver enzymes creatinine BUN bilirubin international normalized ratio activated
partial thromboplastin time acidbase status etc
Antimicrobial and other drug assaysserum drug levels
Surgical operative reports
Rule flag information with link to intervention documentation form
Intervention information history and intervention outcomes
Monitors (including links to reference documents) and pharmacist communication notes
Nonformulary drug documentation and nonformulary order history
Urinalysis
CSF results
Warfarin protocol history
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012 Page 277 of 417
Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-

13 13 13
13
Definition13 of13 Pediatric13 Pharmacy13 Practice13 13 Pediatric13 pharmacy13 practice13 specializes13 in13 the13 delivery13 of13 patient13 care13 services13 by13 pharmacists13 that13 ensures13 the13 safe13 and13 effective13 use13 of13 medications13 for13 all13 children13 from13 neonates13 through13 adolescents13 The13 practice13 includes13 direct13 patient13 care13 for13 children13 often13 provided13 through13 interprofessional13 health13 care13 teams13 as13 well13 as13 advocacy13 and13 education13 for13 children13 and13 their13 families13 wellness13 and13 health13 promotion13 and13 activities13 that13 advance13 knowledge13 and13 skills13 in13 pediatric13 pharmacy13
13
282 May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
admission medication history can be obtainedHospital leadership is fully committed to 100 compliance
with complete medication reconciliation To meet this andother pharmacy initiatives one pediatric pharmacist shift wasadded per day during this time period The 567 medication rec-onciliationndashrelated clinical interventions performed by pharma-cists indicate that the time and effort of performing medicationreconciliation activities leads to positive benefit for patients
Pharmacist involvement in Mayorsquos medication reconciliationprogram has improved the accuracy of the admit medicationlist with one-quarter of PPML flow sheets corrected during thefirst five weeks As a result of these interventions the comput-er-assisted medication reconciliation process which has contin-ued as described has improved patient care by aiding pharm-acists to complete more thorough medication reconciliation
References1 Bates DW et al The costs of adverse drug events in hospitalized patientsAdverse Drug Events Prevention Study Group JAMA 277307ndash311 Jan 22ndash291997 2 Carter M et al Pharmacist-acquired medication histories in a university hos-pital emergency department Am J Health Syst Pharm 632500ndash2503 Dec 1520063 Bond CA Raehl CL Interrelationships among mortality rates drug coststotal cost of care and length of stay in United States hospitals Summary and rec-ommendations for clinical pharmacy services and staffing Pharmacotherapy21129ndash141 Feb 20014 Bond CA Raehl CL Clinical pharmacy services hospital pharmacy staffingand medication errors in United States hospitals Pharmacotherapy 22134ndash147Feb 20025 Bond CA Raehl CL Clinical pharmacy services pharmacy staffing andadverse drug reactions in United States hospitals Pharmacotherapy 26 735ndash747Jun 20066 The Joint Commission Comprehensive Accreditation Manual for Hospitals 2009The Official Handbook Oakbrook Terrace IL Joint Commission Resources 2008 7 Nester T Hale L Effectiveness of a pharmacist-acquired medication history inpromoting patient safety Am J Health Syst Pharm 592221ndash2225 Nov 15 2002J
Brian Gardner PharmD is Clinical Pediatric Pharmacist Mayo
Eugenio Litta Childrens Hospital Rochester Minnesota and
Kevin Graner RPh is Pharmacy Services Supervisor Please
address correspondence to Brian Gardner GardnerBrian
mayoedu
Online-Only Content
See the online version of this article for Appendix 1 Medication
History Printout
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012
AP1May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
Online-Only ContentAppendix 1 (PCARE) Program Patient Detailed Report Screen and Contained Information
A screen shot of the top of this window is shown along with a description of the information contained in each section of the Patient
Detailed Report PCARE Mayo Eugenio Litta Hospitalrsquos Web-based pharmaceutical care program CC-HPI-PMH Chief Complaint-
History of Present Illness-Past Medical History BMI body mass index BSA body surface area HB Harris Benedict PCR
Polymerase chain reaction BUN blood urea nitrogen INR international normalized ratio APTT activated partial thromboplastin time
CSF cerebrospinal fluid
Demographic information age sex actual weight ideal and aminoglycoside dosing weight body surface area
Hospital room location primary service and pager number
Dates of recent hospitalizations
Infection Control status and isolation requirements
CC-HP-PMH note documentation
Calculations HB equation BMI BSA aminoglycoside dosing weight
Infectious disease service consultations and pager number
Drug allergies
Renal functionstatus
Estimated amp measured creatinine clearance
Dialysis (if applicable) intermittent dialysis peritoneal dialysis or continuous renal replacement therapy (CRRT)
Medication reconciliation history and documentation
All medications within desired time range on a timeline grid andor a drug detail grid
Parenteral nutrition composition and calculations (total calories calories as fatprotein deviation from HB equation)
Microbiology data cultures stains and PCR assays
Selected laboratory data blood counts electrolytes liver enzymes creatinine BUN bilirubin international normalized ratio activated
partial thromboplastin time acidbase status etc
Antimicrobial and other drug assaysserum drug levels
Surgical operative reports
Rule flag information with link to intervention documentation form
Intervention information history and intervention outcomes
Monitors (including links to reference documents) and pharmacist communication notes
Nonformulary drug documentation and nonformulary order history
Urinalysis
CSF results
Warfarin protocol history
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012 Page 277 of 417
Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-

282 May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
admission medication history can be obtainedHospital leadership is fully committed to 100 compliance
with complete medication reconciliation To meet this andother pharmacy initiatives one pediatric pharmacist shift wasadded per day during this time period The 567 medication rec-onciliationndashrelated clinical interventions performed by pharma-cists indicate that the time and effort of performing medicationreconciliation activities leads to positive benefit for patients
Pharmacist involvement in Mayorsquos medication reconciliationprogram has improved the accuracy of the admit medicationlist with one-quarter of PPML flow sheets corrected during thefirst five weeks As a result of these interventions the comput-er-assisted medication reconciliation process which has contin-ued as described has improved patient care by aiding pharm-acists to complete more thorough medication reconciliation
References1 Bates DW et al The costs of adverse drug events in hospitalized patientsAdverse Drug Events Prevention Study Group JAMA 277307ndash311 Jan 22ndash291997 2 Carter M et al Pharmacist-acquired medication histories in a university hos-pital emergency department Am J Health Syst Pharm 632500ndash2503 Dec 1520063 Bond CA Raehl CL Interrelationships among mortality rates drug coststotal cost of care and length of stay in United States hospitals Summary and rec-ommendations for clinical pharmacy services and staffing Pharmacotherapy21129ndash141 Feb 20014 Bond CA Raehl CL Clinical pharmacy services hospital pharmacy staffingand medication errors in United States hospitals Pharmacotherapy 22134ndash147Feb 20025 Bond CA Raehl CL Clinical pharmacy services pharmacy staffing andadverse drug reactions in United States hospitals Pharmacotherapy 26 735ndash747Jun 20066 The Joint Commission Comprehensive Accreditation Manual for Hospitals 2009The Official Handbook Oakbrook Terrace IL Joint Commission Resources 2008 7 Nester T Hale L Effectiveness of a pharmacist-acquired medication history inpromoting patient safety Am J Health Syst Pharm 592221ndash2225 Nov 15 2002J
Brian Gardner PharmD is Clinical Pediatric Pharmacist Mayo
Eugenio Litta Childrens Hospital Rochester Minnesota and
Kevin Graner RPh is Pharmacy Services Supervisor Please
address correspondence to Brian Gardner GardnerBrian
mayoedu
Online-Only Content
See the online version of this article for Appendix 1 Medication
History Printout
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012
AP1May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
Online-Only ContentAppendix 1 (PCARE) Program Patient Detailed Report Screen and Contained Information
A screen shot of the top of this window is shown along with a description of the information contained in each section of the Patient
Detailed Report PCARE Mayo Eugenio Litta Hospitalrsquos Web-based pharmaceutical care program CC-HPI-PMH Chief Complaint-
History of Present Illness-Past Medical History BMI body mass index BSA body surface area HB Harris Benedict PCR
Polymerase chain reaction BUN blood urea nitrogen INR international normalized ratio APTT activated partial thromboplastin time
CSF cerebrospinal fluid
Demographic information age sex actual weight ideal and aminoglycoside dosing weight body surface area
Hospital room location primary service and pager number
Dates of recent hospitalizations
Infection Control status and isolation requirements
CC-HP-PMH note documentation
Calculations HB equation BMI BSA aminoglycoside dosing weight
Infectious disease service consultations and pager number
Drug allergies
Renal functionstatus
Estimated amp measured creatinine clearance
Dialysis (if applicable) intermittent dialysis peritoneal dialysis or continuous renal replacement therapy (CRRT)
Medication reconciliation history and documentation
All medications within desired time range on a timeline grid andor a drug detail grid
Parenteral nutrition composition and calculations (total calories calories as fatprotein deviation from HB equation)
Microbiology data cultures stains and PCR assays
Selected laboratory data blood counts electrolytes liver enzymes creatinine BUN bilirubin international normalized ratio activated
partial thromboplastin time acidbase status etc
Antimicrobial and other drug assaysserum drug levels
Surgical operative reports
Rule flag information with link to intervention documentation form
Intervention information history and intervention outcomes
Monitors (including links to reference documents) and pharmacist communication notes
Nonformulary drug documentation and nonformulary order history
Urinalysis
CSF results
Warfarin protocol history
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012 Page 277 of 417
Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-

AP1May 2009 Volume 35 Number 5
The Joint Commission Journal on Quality and Patient Safety
Online-Only ContentAppendix 1 (PCARE) Program Patient Detailed Report Screen and Contained Information
A screen shot of the top of this window is shown along with a description of the information contained in each section of the Patient
Detailed Report PCARE Mayo Eugenio Litta Hospitalrsquos Web-based pharmaceutical care program CC-HPI-PMH Chief Complaint-
History of Present Illness-Past Medical History BMI body mass index BSA body surface area HB Harris Benedict PCR
Polymerase chain reaction BUN blood urea nitrogen INR international normalized ratio APTT activated partial thromboplastin time
CSF cerebrospinal fluid
Demographic information age sex actual weight ideal and aminoglycoside dosing weight body surface area
Hospital room location primary service and pager number
Dates of recent hospitalizations
Infection Control status and isolation requirements
CC-HP-PMH note documentation
Calculations HB equation BMI BSA aminoglycoside dosing weight
Infectious disease service consultations and pager number
Drug allergies
Renal functionstatus
Estimated amp measured creatinine clearance
Dialysis (if applicable) intermittent dialysis peritoneal dialysis or continuous renal replacement therapy (CRRT)
Medication reconciliation history and documentation
All medications within desired time range on a timeline grid andor a drug detail grid
Parenteral nutrition composition and calculations (total calories calories as fatprotein deviation from HB equation)
Microbiology data cultures stains and PCR assays
Selected laboratory data blood counts electrolytes liver enzymes creatinine BUN bilirubin international normalized ratio activated
partial thromboplastin time acidbase status etc
Antimicrobial and other drug assaysserum drug levels
Surgical operative reports
Rule flag information with link to intervention documentation form
Intervention information history and intervention outcomes
Monitors (including links to reference documents) and pharmacist communication notes
Nonformulary drug documentation and nonformulary order history
Urinalysis
CSF results
Warfarin protocol history
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
11202012 Page 277 of 417
Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-

Training Pediatric Clinical Pharmacology and TherapeuticsSpecialists of the Future The Needs the Reality andOpportunities for International Networking
Paediatric DrugsJanuary 1 2009 | Gazarian Madlen
Abstract
In recent years there has been a rapid and marked increase in global recognition of theneed for better medicines for children with various initiatives being implemented atglobal and regional levels These exciting developments are matched by recognition ofthe need to build greater capacity in the field of pediatric clinical pharmacology andtherapeutics to help deliver on the promise of better medicines for children A range ofpediatric medicines researchers educators clinical therapeutics practitioners andexperts in drug evaluation regulation and broader medicines policy are needed on alarger scale in both developed and developing world settings The current and likelyfuture training needs to meet these diverse challenges the current realities of trying tomeet such needs and the opportunities for international networking to help meet futuretraining needs are discussed from a global perspective
Pediatric clinical pharmacology and therapeutics (PCPT) can be broadly described asthe discipline concerned with the evaluation and use of medicines in the pediatricpopulation although many different descriptions of the specialty exist[12] The last fewyears have seen a rapid and marked increase in global recognition of the need for
11202012 Page 278 of 417
better medicines for children and pediatric clinical pharmacologists have been leadingthis effort[34] The key challenges PCPT specialists now face in delivering on thepromise of better medicines for children include (i) doing high-quality medicinesresearch relevant to meeting actual child health needs at a global level (ii) timelyevaluation collation and dissemination of new research evidence about the efficacyand safety of medicines to all clinicians involved in using medicines in the pediatricpopulation (iii) timely access to appropriate medicines and (iv) effective use ofresearch evidence from appropriate pediatric studies in the routine care of pediatricpatients (rational use of medicines or quality use of medicines) This includes theeffective application of knowledge translation research to improving medicines use andoutcomes an emerging field of expertise that is of great importance to achieving optimaltherapeutics in actual practice[5]
There is increasing recognition of the need to build greater capacity in PCPT to meetthese challenges A range of pediatric medicines researchers educators clinicaltherapeutics practitioners and experts in drug evaluation regulation and broadermedicines policy are needed on a larger scale The need for greater efforts at training tomeet the increasing need for expertise is recognized by a number of professionalbodies at global and regional levels[13] with several initiatives already underway[4]
This article discusses the current and likely future training needs from a globalperspective the current realities of trying to meet such needs and the opportunities forinternational networking to help meet training needs in the future
What is Needed for Training in Pediatric Clinical Pharmacology and Therapeutics
Content of Training Programs
Defining core content for PCPT training with some consistency at a global level hasbeen problematic[67] although a recent comparison of current Canadian and UKprograms found considerable similarities[2] In considering future training needs itmakes sense to look at the key challenges of delivering better medicines to children and
11202012 Page 279 of 417
design training around the skills needed to address them Some core generalcompetencies that are needed are listed in figure 1 A range of specialized clinical andresearch skills together with expertise in teaching and learning at many levels areneeded Perhaps much more so than any other specialty PCPT experts need to behighly skilled in the public health and social and political dimensions of healthcareincluding expertise in drug development medicines evaluation regulation andreimbursement issues and evidence-based therapeutic decision-making skills to informboth clinical practice and broader medicines policy They also need sophisticatedknowledge of and skills in ethical interactions with the pharmaceutical industrywhether through involvement in the design conduct or review of ethical medicinesresearch or through playing a key role in helping achieve rational use of medicines inclinical practice across a range of settings
Traditionally most PCPT experts have undertaken some type of specialty or sub-specialty pediatric clinical training with the content and duration varying betweendifferent countries21 Although most are medical specialists some have arrived atPCPT through pediatric pharmacy clinical training Yet others have trained in adultmedicine as their clinical base In the future it is likely that more trainees from a diversedisciplinary background may wish to train in PCPT Irrespective of the professionaldiscipline in which clinical training may have originated a core set of clinicalcompetencies in PCPT is needed by all experts in the field These include specializedknowledge and skills relevant to clinical care and therapeutic decision makingspecifically in the pediatric population (figure 2) In addition to the classically definedcompetencies in pharmacology and toxicology high-level expertise in the criticalevaluation of clinical research and application to evidence-based therapeutic decisionmaking is needed Such expertise is increasingly being valued and sought for exampleby various bodies concerned with rational therapeutics medicines access andreimbursement or with evidence-based therapeutic guidelines or medicines informationdevelopment at local national and global levels Indeed highlighting the importance ofsuch expertise to optimizing medicines use in healthcare settings has been suggestedas critical to the survival of the specialty itself[8]
11202012 Page 280 of 417
In addition to skills relevant to using research evidence PCPT experts must also behighly skilled in doing high-quality research to generate the needed evidence Formalresearch training in a basic science field andor in clinical research methods is optimallyacquired through a higher degree in research (eg masters or doctorate) Although thisis strongly encouraged there is insufficient dedicated time within most PCPT trainingprograms currently in existence so trainees need to devote additional time to acquiringa higher degree Given the central role most PCPT experts have played11 and willcontinue to play in the design and conduct of medicines research these are core skillsrelevant to all trainees This is especially so in the current context of increased demandfor pediatric medicines research globally A range of high-level expertise in thecomprehensive scientific evaluation of medicines including the design and conduct ofhigh-quality preand post-marketing clinical trials and observational studies relevant tothe pediatric population is needed (figure 3) Specialized expertise in the ethics ofclinical research in children including skills to appropriately address any possible ethicalissues in pharmaceutical industry-funded studies is vital[910]
Expertise in teaching and learning at both undergraduate and postgraduate levels isneeded by all PCPT experts In addition to teaching trainees within the field of PCPTthere will be an increasing need to provide effective cross-disciplinary teaching about avariety of topics relevant to pediatric medicines and therapeutics to a wide variety ofhealth professionals scientists and others from academia pharmaceutical industryand government agencies in the developed and developing worlds
Structure and Duration of Training Programs
The structure and duration of training can be variable with total durations ranging from5 to 10 years in existing programs[211] This is partly due to differences betweencountries in requirements for training in the foundation clinical discipline[1211] andpartly to differences in the duration of specialty training for the PCPT componentdespite similar content of some programs[2] The required duration of dedicatedresearch training can also vary (eg at least 6 months in Canada and at least 12
11202012 Page 281 of 417
months in the UK) although most programs emphasize that longer periods of researchare highly desirable
As the field continues to grow it should be possible to eventually develop some globalconsistency about the content and duration of the specialized pediatric CPTcomponent of any training program This could then be integrated into an overalltraining program structure taking into account differences in foundation disciplinarytraining requirements which vary between countries Defining minimum criteria for thenature duration and structure of formal research training would be highly desirableInnovative ways of delivering the needed training should be explored These mayinclude for example enrolment in a higher degree research program concurrent withclinical specialty training as a feasible model
Who Needs Training
Potential trainees may come from a range of medical pharmacy or other backgroundsMedical trainees could include pediatricians pediatric sub-specialists or those whohave initially trained in adult medicine Increasingly scientists and health professionalsfrom a range of settings including the pharmaceutical industry academia governmentand non-government organizations will need to acquire training in various aspects ofPCPT either in whole or in part Flexible and tailored programs to meet these diverseneeds will be vital to delivering relevant training and building a larger pool of expertise inthe field globally Balancing such diversity against maintaining high standards in corePCPT competencies will be challenging
The Realities How and Where can Training Needs be Met
Although there are indications and expectations of increasing demand for training inPCPT at a global level the current reality is that the capacity to meet that need issuboptimal in many parts of the world A recent survey of European Society forDevelopmental Perinatal and Paediatric Pharmacology (ESDP) members found thatonly four European countries had more than one pediatric clinical pharmacologist and
11202012 Page 282 of 417
the total number of trainees (n = 23) exceeded the number of pediatric clinicalpharmacologists (n = 18) Four trainees were in centers where there was no pediatricclinical pharmacologist111 The limited availability of PCPT experts to act as trainers isalso the reality in many other parts of the world with the possible exception of NorthAmerica
Even in centers where there may be a pediatric clinical pharmacologist the capacity ofa single center to deliver all of the diverse training needs is often limited This may bedue to limitations in the facility (eg limited infrastructure or access to an appropriatemix of patients) limitations in the ability to provide adequate supervision (eg numberexpertise or availability of senior staff) or limitations in the range of educational orresearch opportunities available In many instances funding for such training positionsmay not be available A shift from the traditional approach to training might help addresssuch challenges Ultimately the appropriateness of training may need to be determinedby acquisition of required core competencies through innovative and flexible models ofdelivery which may include multi-site training delivered by different trainers rather thanthe traditionally defined location- and duration-based training programs This will beespecially relevant to building capacity in areas of greatest need such as thedeveloping world A key determinant of the success of such an approach will bedeveloping consensus on a core curriculum for PCPT that is globally relevant While thishas proved challenging in the past the desirability of globally transferable skills in a fieldsuch as PCPT is an increasingly relevant need for the future
International networking in training and capacity building to help meet this need iscurrently under discussion and its success will be vital to the future viability of the fieldKey professional organizations such as the International Union of Basic and ClinicalPharmacology (IUPHAR) and the ESDP are actively collaborating to develop newresources and innovative modes of delivery to support training in PCPT at a globallevel[4] There are also a number of excellent training resources that are currently inexistence and which could be more widely utilized by trainees from different parts of theworld These include the annual ESDPEudipharm course in Evaluation of Medicinal
11202012 Page 283 of 417
Products in Children the biannual International Workshop on Paediatric Clinical Trialsrun by the Association of Clinical Research Professionals and the Journal of Pediatricand Perinatal Drug Therapym and education days in association with regular scientificmeetings such as those of the ESDP and the American Society for ClinicalPharmacology and Therapeutics (ASCPT) In addition training opportunities availablethrough local universities and relevant other organizations could be more widely utilizedFor example formal programs in clinical epidemiology and pharmacoepidemiologyclinical trials methodology or drug development[12] offer excellent generalopportunities that can be integrated with PCPT training
Accreditation of Programs and Assessment of Trainees
Currently trainees spend defined periods of time undertaking specified activities ataccredited training sites Not all sites have undergone an independent or formalaccreditation process Assessment of competencies is usually through a combination offormative and summative evaluations performed by the same experts who provided thetraining which has obvious drawbacks Although none of the existing programs has sofar had an exit examination at a national level this will be a requirement in the Canadianprogram soon (Ito S personal communication)[13]
A potential future model of flexible training programs built around acquisition of corecompetencies through a variety of sites trainers and learning modes will increase theneed for independent competency-based assessments With site-based trainingmodels processes need to be established for independent evaluation of the suitabilityof training programs and sites especially as new ones emerge It is also highlydesirable to have a separation of assessment from the delivery of training Similarlyindependent processes to address potential problems arising during training are neededto ensure high-quality training experiences and outcomes Given the current limitationsin numbers of available experts in most countries the need for independentassessments (of trainers and trainees) presents additional challenges These might alsobe addressed by innovative approaches in international networking
11202012 Page 284 of 417
Acknowledgments
Thanks to Prof Shinya Ito and Prof Imti Choonara for providing access to the Canadianand UK training curriculum documents Dr Gazarian trained in pediatrics in Australiaand in pediatric clinical pharmacology pediatric rheumatology and clinical epidemiologyin Canada This article is informed partly by personal experience and reflections (astrainee and trainer) and personal communications over a number of years withcolleagues from different countries whose input is gratefully acknowledged Specialthanks to Profs Gideon Koren Shinya Ito Imti Choonara and Kalle Hoppu for sharingtheir insights on training in pediatric clinical pharmacology No sources of funding wereused to assist in the preparation of this article The author has no conflicts of interestthat are directly relevant to the content of this article
[Reference]
References
1 Boriati M Breitkreutz J Choonara I et al Paediatric clinical pharmacology in EuropePaediatr Perinat Drug Ther 2006 7 (3) 134-7
2 Anderson M Choonara I Ito S et al Paediatric clinical pharmacology trainingprogrammes in Canada and the UK a comparison Paediatr Perinat Drug Ther 2007 8(1) 26-30
3 MacLeod S Peterson R Wang Y et al Challenges in international pediatricpharmacology a milestone meeting in Shanghai Pediatr Drugs 2007 9 (4) 215-8
4 Hoppu K Paediatric clinical pharmacology at the beginning of a new era Eur J ClinPharmacol 2008 64 (2) 201-5
5 Gazarian M Evidence-based medicine in practice paediatrics Med J Aust 2001174 586-7
11202012 Page 285 of 417
6 Koren G MacLeod SM The state of pediatric clinical pharmacology an internationalsurvey of training programs Clin Pharmacol Ther 1989 46 489-93
7 Koren G Kriska M Pons G et al The network of pediatric pharmacology trainingprograms Clin Pharmacol Ther 1993 54 1-6
8 Maxwell SRJ Webb DJ Clinical pharmacology too young to die Lancet 2006 367799-800
9 European Commission Educai considerations for clinical trials on medicinal productsconducted with die paediatric population [online] Available from URLhttpeceuropaeuentefrisephaGmaceuticalseudralexvol-10ethical_considerationspdf [Accessed 2008 Dec 1]
10 Field MJ Behrman R editors Ethical conduct of clinical research involving children[online] Washington DC The National Academies Press 2004httpwwwnapeducatalog10958html [Accessed 2008 Dec 1]
11 The Royal Australasian College of Physicians 2008 requirements for physiciantraining adult medicine and paediatrics (Australia) [online] Available from URLhttpwwwracpeduaupagephysician-educationtraining-requirements [Accessed 2008Dec 1]
12 The University of New South Wales Pharmaceutical medicine and drugdevelopment programs [online] Available from URLhttpwwwdrugdevmedunsweduau [Accessed 2008 Dec 1]
13 The Royal College of Physicians and Surgeons of Canada Specialty trainingrequirements in clinical pharmacology [online] Available from URLhttpwwwrcpscmedicalorginformationindexphp7specialty=410ampsubmit=Select[Accessed 2008 Dec 1]
[Author Affiliation]
11202012 Page 286 of 417
Mathen Gazarian
Paediatric Therapeutics Program School of Womens and Childrens Health Universityof New South Wales and Sydney
Childrens Hospital Randwick New South Wales Australia
[Author Affiliation]
Correspondence Dr Mathen Gazarian Paediatric Therapeutics Program School ofWomens and Childrens Health University of New South Wales Level 3 EmergencyWing Sydney Childrens Hospital High Street Randwick NSW 2031 Australia
E-mail MGazarianunsweduau
Gazarian Madlen
Copyright Wolters Kluwer Health Adis International 2008
httpwwwhighbeamcomdoc1P3-1638228481html
HighBeam Research is operated by Cengage Learning copy Copyright 2012 All rightsreserved
wwwhighbeamcom
11202012 Page 287 of 417
ORIGINAL ARTICLE
Medication Dosing and Renal Insufficiency in a Pediatric CardiacIntensive Care Unit Impact of Pharmacist Consultation
Brady S Moffett AElig Antonio R Mott AEligDavid P Nelson AElig Karen D Gurwitch
Received 2 October 2007 Accepted 17 November 2007 Published online 14 December 2007
Springer Science+Business Media LLC 2007
Abstract Pediatric patients who have undergone cardiac
surgery are at risk for renal insufficiency The impact of
pharmacist consultation in the pediatric cardiac intensive
care unit (ICU) has yet to be defined Patients admitted to
the pediatric cardiac ICU at our institution from January
through March of 2006 were included Patient information
collected retrospectively included demographics cardiac
lesionsurgery height weight need for peritoneal or he-
modialysis need for mechanical support highest and
lowest serum creatinine ICU length of stay (LOS) renally
eliminated medications pharmacist recommendations
(accepted or not) and appropriateness of dosing changes
There were 140 total admissions (131 patients age
30 plusmn 63 years) during the study period In total
14 classes of renally eliminated medications were admin-
istered with 326 plusmn 564 doses administered per patient
admission Thirty-seven patient admissions had one or
more medications adjusted for renal insufficiency the most
commonly adjusted medication was ranitidine Patients
who required medication adjustment for renal dysfunction
were significantly younger compared to those patients not
requiring medication adjustment Pharmacist recommen-
dations were responsible for 96 of medication
adjustments for renal dysfunction and the recommenda-
tions were accepted and appropriate all of the time The
monetary impact of pharmacist interventions in doses
saved was approximately $12000 Pharmacist consulta-
tion can result in improved dosing of medications and cost
savings The youngest patients are most at risk for inap-
propriate dosing
Keywords Renal insufficiency Pediatric Cardiac surgery Intensive care Pharmacist interventions Medication adjustment
Introduction
Renal function is integrally involved in the disposition of
medications in the human body Because renal dysfunction
is common in patients undergoing cardiac surgery medi-
cations often require adjustment for changes in renal
clearance [26] In adult patients failure to adjust medica-
tion doses and schedules often results in possible adverse
effects and inappropriate dosing [20] Interventions to
identify patients at risk for inappropriate medication dosing
secondary to renal dysfunction have been shown to
improve medication utilization [6 12]
Patients in the pediatric cardiac intensive care unit (ICU)
are at considerable risk for the development of renal insuf-
ficiency Factors contributing to renal insufficiency include
low cardiac output medications cardiopulmonary bypass
pathophysiology surgical procedure and young age [2 3
7 10] Use of peritoneal dialysis and hemodialysis is there-
fore not uncommon [5] A pharmacist review of medications
is likely to prevent inappropriate dosing secondary to renal
dysfunction [1 14 15] There is currently no literature
describing the impact of a pharmacist review of medications
for renal dosing in the pediatric cardiac ICU
The purposes of this study were (1) to identify the
medications in the pediatric cardiac ICU that most
B S Moffett (amp) K D Gurwitch
Department of Pharmacy Texas Childrenrsquos Hospital
6621 Fannin St MC 2-2510 Houston TX 77030 USA
e-mail bsmoffettexaschildrenshospitalorg
A R Mott D P Nelson
Department of Pediatrics Lillie Frank Abercrombie Section of
Pediatric Cardiology Baylor College of Medicine
Houston TX USA
123
Pediatr Cardiol (2008) 29744ndash748
DOI 101007s00246-007-9170-3
11202012 Page 288 of 417
frequently require adjustment for renal dysfunction (2) to
characterize the population of patients requiring medica-
tion adjustment secondary to renal insufficiency and (3) to
characterize pharmacist consultation for adjustment of
medications due to renal insufficiency in the pediatric
cardiac ICU
Materials and Methods
A renal dosing program was initiated in the pediatric car-
diac ICU at our institution in August 2003 The pharmacy
computer system was configured to automatically calculate
creatinine clearance (CrCl) from serum creatinine (SCr)
values according to the modified Schwartz equation for
pediatric patients or the Cockroft-Gault equation for adult
patients [8 22] The pharmacy staff in the ICU was required
to evaluate patient medication profiles relative to patient
CrCl on a daily basis As indicated pharmacists made
recommendations to the medical team in accordance with
guidelines for medication dosing in renal dysfunction
located in the institutional medication formulary which was
adapted from Pediatric Dosage Handbook 13th ed [23]
Patients admitted to the pediatric cardiac ICU at our
institution from January through March of 2006 were
identified and a waiver of consent was obtained from the
investigational review board Patients were included in the
study if they were admitted to the pediatric cardiac ICU for
greater than 24 h during the study period received at least
one medication and had at least one SCr level drawn
Patients were excluded if they spent less than 24 h
admitted to the ICU did not receive any medications while
admitted to the ICU or did not have a SCr level Medi-
cations that are monitored by serum concentrations (eg
aminoglycosides enoxaparin vancomycin) were not
included in the evaluation as renal insufficiency is not the
only factor affecting their disposition Angiotensin-con-
verting enzyme (ACE) inhibitors such as captopril or
enalapril are initiated at very low doses and titrated to
effect over a period of days and therefore are not adjusted
in patients with decreased renal function in our institution
Patient information collected retrospectively included
demographics cardiac lesionsurgery height weight use
of peritoneal or hemodialysis need for mechanical circu-
latory support high and low SCr and CrCl ICU length of
stay (LOS) medications that are renally eliminated
response to pharmacist recommendations and appropri-
ateness of dosing changes according to CrCl
Appropriateness of pharmacist recommendations was
assessed by the accuracy of the recommendation according
to institutional guidelines Monetary impact of pharmacist
interventions was determined by calculating the number of
doses that were saved by appropriately decreasing
medication doses or schedules for renal insufficiency
Patient charge determined from current medication buying
contracts and pricing was used as the basis for determining
cost savings
Data are presented as mean plusmn standard deviation unless
otherwise noted Comparisons between groups were per-
formed with the Wilcoxon rank sum test for nonparametric
data and Fisherrsquos exact test for categorical data
Results
There were 140 admissions (131 patients) to the pediatric
cardiac ICU during the study period and the mean patient
age on the day of admission was 30 plusmn 63 years (median
168 days range 1 dayndash44 years) The mean length of stay
in the ICU was 63 plusmn 88 days (median 40 days range
1ndash65 days) Twenty-four (171) admissions did not
involve surgical intervention Of the remaining 116
(828) surgical admissions 100 (862) required car-
diopulmonary bypass Peritoneal dialysis was utilized in a
small number of patients (19 admissions 136) and no
patients underwent hemodialysis Three (21) admissions
were on a form of mechanical circulatory support Six
(43) admissions underwent delayed sternal closure
The mean low and high calculated CrCl for the study
cohort was 740 plusmn 376 mlmin173 m2 and 1155 plusmn
565 mlmin173 m2 respectively A reduced CrCl
(50 mlmin173 m2) was observed in 40 (286)
admissions a CrCl 35 mlmin173 m2 was observed in
21 (150) admissions and no patients had a CrCl 10
mlmin173 m2
Fourteen classes of medications requiring adjustment in
renal dysfunction according to institutional guidelines
were prescribed during the study period (Table 1) A
median of 18 doses (range 1ndash414) of renally eliminated
medications were administered per patient admission Two
patients did not receive any renally eliminated medications
Patients who required medication adjustment for renal
dysfunction were significantly younger and smaller than
those patients who did not require medication adjustment
However patients were not more likely to have undergone
cardiopulmonary bypass or to have a single ventricle
physiology (Table 2)
Thirty-seven (264) patient admissions required
adjustment of one or more medications due to renal dys-
function Thirty-six (973) of these admissions had one or
more medications appropriately adjusted for renal dys-
function according to institutional guidelines and
ranitidine was the most common medication adjusted for
renal dysfunction (34 admissions 918) (Fig 1 Table 3)
Nine patients required readjustment of medications for
improved renal function
Pediatr Cardiol (2008) 29744ndash748 745
123
11202012 Page 289 of 417
Seventy-seven (916) of 84 courses of medication
were appropriately adjusted for renal dysfunction Phar-
macists were responsible for 74 (96) adjustments and
physicians were responsible for 3 (4) adjustments for
renal dysfunction Pharmacist recommendations for
adjustment of medications were accepted 100 of the
time The monetary impact of pharmacist interventions in
doses saved was $1248254
Discussion
Renal dysfunction can be a common occurrence in cardiac
intensive care Reports have documented the incidence of
renal insufficiency according to the RIFLE criteria in
adults after cardiac surgery as high as 196 [19] Subse-
quently programs to improve the use of medications in
adult patients with renal insufficiency have been adopted
In our study population 15 (21140) of the admissions
had renal insufficiency during ICU admission Appropriate
dosing of medications for critically ill patients with renal
insufficiency is important for therapeutic safety and cost-
effective reasons
Although the Schwartz and Cockroft-Gault equations
are the current standard for calculation of CrCl in the
clinical setting most publications evaluating the Schwartz
equation have identified an overestimation in the calcula-
tions [8 13 22] Harrison et al demonstrated that the
Schwartz equation overestimates CrCl in neonates after
surgery for hypoplastic left heart syndrome or transposition
of the great arteries which could lead to toxic concentra-
tions of drugs eliminated by the kidneys [16] If a more
accurate method for estimation of CrCl is developed there
will likely be a larger incidence of patients requiring
medication adjustments for renal dysfunction
Due to significant renal insufficiency in some patients
our study population had instances of peritoneal dialysis
use Elimination of medications might be affected by per-
itoneal dialysis However there are very little data on the
removal of medications due to peritoneal dialysis and
medications were not adjusted for the effects of peritoneal
dialysis in our cohort [11 17 21] Similarly medications
were not adjusted solely due to mechanical circulatory
support which might or might not include hemodialysis or
hemofiltration [4]
Medication adjustment was more common in younger
patients Decreased renal function after cardiac surgery is a
common occurrence in neonates [2 3 7 9 10] This likely
is due to the developmental changes in the kidney
Table 1 Classes of renally eliminated medications prescribed
Medication class Total no of doses administered
Antibiotics 1530
Histamine-2 antagonists 1375
ACE inhibitors 821
Diuretics 167
Beta-blockers 138
Antihypertensives 140
Prokinetic agents 125
Immunosuppressants 49
Antifungal agents 43
Antiviral agents 42
Antiepileptics 28
Digoxin 27
Antiarrhythmics 27
Colchicine 5
Uricosuric agents 5
Table 2 Patient factors associated with adjustment of medications
for renal dysfunction
Category Medications
adjusted
(n = 37)
Medications
not adjusted
(n = 103)
p-Value
Length of stay (days) 112 plusmn 136 45 plusmn 49 00001
Weight (kg) 59 plusmn 151 145 plusmn 186 00001
Height (cm) 519 plusmn 219 781 plusmn 306 00001
Age (months) 09 plusmn 11 365 plusmn 764 00001
Presence of CPB 648 757 NS
[18 years of age 27 58 NS
Univentricular
anatomy
20 262 NS
Ranitidine65
Ganciclovir5
Fluconazole2
Digoxin2
Ceftazidime4
Cefotaxime6
Cefazolin14
Ampicillin2
Fig 1 Medications adjusted secondary to renal dysfunction
746 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 290 of 417
occurring early in life in addition to the inflammatory
pathophysiology associated with cardiopulmonary bypass
[2 3 7 9 10] Additionally younger patients might have
had a higher acuity of illness as reflected by the increased
mean LOS
Ranitidine was the medication most frequently requiring
adjustment for renal dysfunction in our study group
Ranitidine is the standard for stress ulcer prophylaxis after
cardiovascular surgery at our institution Although the
clinical risks associated with overdosing of ranitidine are
not great the cost benefit associated with appropriate
ranitidine dosing was significant in our cohort [24]
Pharmacist involvement in pediatric patient pharmaco-
therapy has been documented to be beneficial [1 14 15
18 25] Additionally in pediatric intensive care patients
pharmacist involvement has been noted to decrease the cost
of care decrease medication errors and optimize medical
therapies via several types of activities [18] This is the first
account of pharmacist interventions focusing solely on
medication adjustment in renal insufficiency in patients in a
cardiac ICU The extrapolated cost savings of $50000
per year is substantial demonstrating the benefit of a
multidisciplinary approach to pediatric critical care
Conclusions
Patients in the pediatric cardiac ICU receive many medi-
cations that require adjustment for renal insufficiency with
the youngest patients most at risk for inappropriate dosing
Pharmacist consultation can result in improved dosing of
medications and substantial cost savings
Acknowledgments The authors would like to thank the CV phar-
macy team for their help in the study Susan Abraham Michael
Allegrino Roy Chacko Robert Chin Lizy Josekutty and David Ung
References
1 Ariano RE Demianczuk RH Danziger RG Richard A Milan H
Jamieson B (1995) Economic impact and clinical benefits of
pharmacist involvement on surgical wards Can J Hosp Pharm
48(5)284ndash289
2 Asfour B Bruker B Kehl HG Frund S Scheld HH (1996) Renal
insufficiency in neonates after cardiac surgery Clin Nephrol
46(1)59ndash63
3 Baskin E Saygili A Harmanci K et al (2005) Acute renal failure
and mortality after open-heart surgery in infants Renal Fail
27(5)557ndash560
4 Buck ML (2003) Pharmacokinetic changes during extracorporeal
membrane oxygenation implications for drug therapy of neo-
nates Clin Pharmacokinet 42(5)403ndash417
5 Chan K Ip P Chiu CSW Cheung Y (2003) Peritoneal dialysis
after surgery for congenital heart disease in infants and young
children Ann Thorac Surg 761443ndash1449
6 Chertow GM Lee J Kuperman GJ et al (2001) Guided medi-
cation dosing for patients with renal insufficiency JAMA
2862839ndash2844
7 Chesney RW Kaplan BS Freedom RM Haller JA Drummond
KN (1975) Acute renal failure an important complication of
cardiac surgery in infants J Pediatr 87(3)381ndash388
8 Cockroft DW Gault MH (1976) Prediction of creatinine clear-
ance from serum creatinine Nephron 1631ndash41
9 Daschner M (2005) Drug dosage in children with reduced renal
function Pediatr Nephrol 20(12)1675ndash1686
Table 3 Guidelines for
adjustment of medications in
patients with renal dysfunction
Medication Creatinine clearance
(mlmin173 m2)
Adjustment schedule
Ampicillin 10ndash30 Administer every 8ndash12 h
10 Administer every 12 h
Cefazolin 10ndash30 Administer every 12 h
10 Administer every 24 h
Cefotaxime 10ndash50 Administer every 12 h
10 Administer every 24 h
Ceftazidime 30ndash50 Administer every 12 h
10ndash29 Administer every 24 h
10 Administer every 48ndash72 h
Digoxin 10ndash50 Reduce dose 25ndash75 or administer every 36 h
10 Reduce dose 75ndash90 or administer every 48 h
Fluconazole 21ndash50 Reduce dose 50
11ndash20 Reduce dose 75
Ganciclovir 50ndash69 25 mgkgdose every 24 h
25ndash49 125 mgkgdose every 24 h
10ndash24 0625 mgkgdose every 24 h
10 0625 mgkgdose 3 timesweek following hemodialysis
Ranitidine 50 Administer every 18ndash24 h
Pediatr Cardiol (2008) 29744ndash748 747
123
11202012 Page 291 of 417
10 Dittrich S Kurschat K Dahnert I et al (2000) Renal function
after cardiopulmonary bypass surgery in cyanotic congenital
heart disease Int J Cardiol 73173ndash179
11 Elwell RJ Bailie GR Manley HJ (2000) Correlation of intra-
peritoneal antibiotic pharmacokinetics and peritoneal membrane
transport characteristics Perit Dial Int 20(6)694ndash698
12 Falconnier AD Haefell WE Schoenenberger RA Surber C
Martin-Facklam M (2001) Drug dosage in patients with renal
failure optimized by immediate concurrent feedback J Gen Intern
Med 16369ndash375
13 Filler G Lepage N (2003) Should the Schwartz formula for
estimation of GFR be replaced by cystatin C formula Pediatr
Nephrol 18(10)981ndash985
14 Folli HL Poole RL Benitz WE Russo JC (1987) Medication
error prevention by clinical pharmacists in two childrenrsquos hos-
pitals Pediatrics 79(5)718ndash722
15 Golightly LK OrsquoFallon CL Moran WD Sorocki AH (1993)
Pharmacist monitoring of drug therapy in patients with abnormal
serum creatinine levels Hosp Pharm 28(8)725-7ndash730-2
16 Harrison AM Davis S Eggleston S Cunningham R Mee RB
Bokesch PM (2003) Serum creatinine and estimated creatinine
clearance do not predict perioperatively measured creatinine
clearance in neonates undergoing congenital heart surgery
Pediatr Crit Care Med 4(1)55ndash59
17 Keller E (1988) Peritoneal kinetics of different drugs Clin
Nephrol 30(Suppl 1)S24ndashS28
18 Krupicka MI Bratton SL Sonnenthal K Goldstein B (2002)
Impact of a pediatric clinical pharmacist in the pediatric intensive
care unit Crit Care Med 30(4)919ndash921
19 Kuitunen A Vento A Suojaranta-Ylinen R Pettila V (2006)
Acute renal failure after cardiac surgery evaluation of the RIFLE
classification Ann Thorac Surg 81(2)542ndash546
20 Nash IS Rojas M Hebert P et al (2005) Reducing excessive
medication administration in hospitalized adults with renal dys-
function Am J Med Qual 2064ndash69
21 Paton TW Cornish WR Manuel MA Hardy BG (1985) Drug
therapy in patients undergoing peritoneal dialysis Clinical
pharmacokinetic considerations Clin Pharmacokinet 10(5)
404ndash425
22 Schwartz GJ Haycock GB Edelmann CM Spitzer A (1976) A
simple estimate of glomerular filtration rate in children derived
from body length and plasma creatinine Pediatrics 58(2)
259ndash263
23 Taketomo CK Hodding JH Kraus DM (2006) Pediatric Dosage
Handbook 13th ed Lexi-Comp Inc Hudson OH
24 Wade EE Rebuck JA Healey MA Rogers FB (2002) H(2)
antagonist-induced thrombocytopenia is this a real phenomenon
Intensive Care Med 28(4)459ndash465
25 Wang JK Herzog NS Kaushal R Park C Mochizuki C Wein-
garten SR (2007) Prevention of pediatric medication errors by
hospital pharmacists and the potential benefit of computerized
physician order entry Pediatrics 119(1)e77ndashe85
26 Wijeysundera DN Karkouti K Beattie S Rao V Ivanov J (2006)
Improving the identification of patients at risk of postoperative
renal failure after cardiac surgery Anesthesiology 10465ndash72
748 Pediatr Cardiol (2008) 29744ndash748
123
11202012 Page 292 of 417
Practice rePorts Medication errors
1254 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Rainu Kaushal MD MPh is Associate Professor Departments of Public Health and Pediatrics Weill Cornell Medical College New York NY DaviD W Bates MD Msc is Chief Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School Boston MA eRiKa l aBRaMson MD is Instructor Depart-ment of Pediatrics Weill Cornell Medical College Jane R souKuP Msc is Senior ProgrammerAnalyst Division of General Internal Medicine Brigham and Womenrsquos Hospital Harvard Medical School DonalD a GolDMann MD is Senior Vice President Institute for Healthcare Improvement Cambridge MA
Address correspondence to Dr Kaushal at Weill Cornell Medi-cal College 411 East 69th Street New York NY 10021 (rak2007medcornelledu)
Supported by a grant from the National Patient Safety Foundation
Copyright copy 2008 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082080701-1254$0600
DOI 102146ajhp070522
P R A C t i C e R e P O R t s
Unit-based clinical pharmacistsrsquo prevention of serious medication errors in pediatric inpatients
Rainu Kaushal DaviD W Bates eRiKa l aBRamson Jane R souKup anD DonalD a GolDmann
Purpose Rates of serious medication errors in three pediatric inpatient units (intensive care general medical and gen-eral surgical) were measured before and after introduction of unit-based clinical pharmacistsMethods Error rates on the study units and similar patient care units in the same hospital that served as controls were deter-mined during six- to eight-week baseline periods and three-month periods after the introduction of unit-based clinical phar-macists (full-time in the intensive care unit [ICU] and mornings only on the general units) Nurses trained by the investigators reviewed medication orders medication administration records and patient charts daily to detect errors near misses and adverse drug events (ADEs) and determine whether near misses were intercepted Two physicians independently reviewed and rated all data collected by the nurses Serious medication errors were defined
as preventable ADEs and nonintercepted near missesResults The baseline rates of serious medi-cation errors per 1000 patient days were 29 for the ICU 8 for the general medical unit and 7 for the general surgical unit With unit-based clinical pharmacists the ICU rate dropped to 6 per 1000 patient days In the general care units there was no reduc-tion from baseline in the rates of serious medication errorsConclusion A full-time unit-based clini-cal pharmacist substantially decreased the rate of serious medication errors in a pediatric ICU but a part-time pharmacist was not as effective in decreasing errors in pediatric general care units
Index terms Clinical pharmacists Clinical pharmacy Errors medication Hospitals Interventions Pediatrics Pharmaceutical servicesAm J Health-Syst Pharm 2008 651254-60
In 1999 the Institute of Medicine (IOM) report To Err Is Human es-timated that 44000ndash98000 people
die each year at least in part because of medical error1 This galvanized the patient safety movement in the United States although a number of previous studies had documented the frequency and serious consequences of medication errors2-6 Errors occur in about 5 of medication orders for adult patients approximately 1 out of 7 of these errors has significant potential for harm7 Less is known about the frequency of errors in pe-diatric patients but children may be at even greater risk Medication er-ror rates in pediatric inpatients have been reported to be as high as 1 in every 64 orders8 In a previous study in pediatric inpatients we found that although medication error and pre-ventable adverse drug event (ADE) rates were similar to those in adults the rate of potentially harmful er-rors (potential ADEs or near misses) was almost three times higher in children9
Most current efforts to reduce medication error rates focus on
information technology (IT)-based interventions Computerized pre-scriber order entry (CPOE) has re-ceived the greatest publicity largely because of its strong theoretical rationale and early studies showing
notable reductions in errors10-13 For example CPOE reduced noninter-cepted serious medication errors by 86 from baseline in a large tertiary-care hospital14 CPOE decreased medication errors by 40 in a tertiary-
11202012 Page 293 of 417
Practice rePorts Medication errors
1255Am J Health-Syst PharmmdashVol 65 Jul 1 2008
care pediatric hospital ADEs were reduced by 41 in a pediatric critical care unit1516 More recently studies have suggested that CPOE like any intervention can lead to new types of errors especially during the early phase of technology deployment and dissemination17 Furthermore CPOE is expensive to install and update
It is important therefore to evaluate other non-IT approaches to reducing medical error For example standardized protocols education programs and initiatives that ad-dress institutional culture may be efficacious in reducing medication error rates although the evidence base for these interventions is quite limited1819 The use of unit-based clinical pharmacists is perhaps the most promising non-IT-based in-tervention Leape et al20 found that having a clinical pharmacist participate on physician rounds in an adult intensive care unit (ICU) decreased preventable ADEs at the prescription-writing stage by 66 while Kucukarslan et al21 found that unit-based clinical pharmacists reduced preventable ADEs at the same stage by 78 These studies conducted on adult units in single institutions focused primarily on errors in ordering medications Few studies have focused on errors at all stages of the medication-use process in children
We hypothesized that unit-based clinical pharmacists might be able to reduce rates of serious medica-tion errors in pediatric inpatients in both ICU and general care unit settings Our study was designed to test this hypothesis in pediatric in-patient units of an academic medi-cal center
MethodsStudy site The prospective cohort
study was conducted at a freestand-ing pediatric teaching hospital locat-ed in an urban area with a socioeco-nomically diverse patient population Fewer than 5 of the patients treated
are adults most of whom have com-plex long-term medical and surgical conditions At the time of this study physicians wrote orders on paper charts Copies were sent to the phar-macy and nurses transcribed orders into the medication administration record (MAR) Before the study in-tervention dispensing pharmacists sent ready-to-administer doses to the patient care units but participated only intermittently in unit-based rounds
We studied the error rates before and after pharmacist intervention in two general medical units two general surgical units the pediatric ICU and the cardiac ICU The pairs of general units were selected be-cause of their similar characteristics and patient populations The ICUs however had differences in case mix whereas the cardiac ICU served pri-marily patients with heart diseases the pediatric ICU had patients from the general surgery neurosurgery or-thopedic craniofacial reconstruction otolaryngology and medicine servic-es One of the medical units and one of the surgical units were randomly selected as experimental groups and the others served as controls The pediatric ICU was randomly selected as an experimental group the cardiac ICU served as its control Despite the differences between cardiac ICU patients and pediatric ICU patients these were the most similar patient populations in terms of severity and complexity of disease The hospitalrsquos human subjects research committee approved the study protocol
Definitions We used IOM defi-nitions for the study1 Medication errors were defined as errors in drug ordering transcribing dispensing administering or monitoring Medi-cation errors with significant poten-tial for injuring patients were defined as near misses or potential ADEs Near misses were further subdivided into intercepted and nonintercepted potential ADEs Whereas intercepted near misses were corrected before the
medication reached the patient non-intercepted near misses were admin-istered but did not cause any harm ADEs were defined as injuries that resulted from the use of a drug22 An ADE was considered preventable if it was associated with a medication er-ror and nonpreventable if it was not For example a rash due to penicillin in a known penicillin-allergic patient was considered a preventable ADE whereas a penicillin-related rash in a patient with no known allergies was a nonpreventable ADE Serious medication errors were defined as preventable ADEs and noninter-cepted near misses An effective patient safety intervention should decrease serious medication error rates but it may increase rates of intercepted near misses These same definitions have been used in previ-ous studies1314
We used the term ldquounit-based clinical pharmacistrdquo to describe a pharmacist whose duties include making rounds with physicians as well as monitoring drug dispensing storage and administration The unit-based clinical pharmacists all had earned the Doctor of Pharmacy degree and had comparable skill lev-els In contrast the primary role of ldquodispensing pharmacistsrdquo at our in-stitution is to dispense medications
Data collection Before collecting data we enlisted the support of staff members and educated them on the studyrsquos purpose and methods We trained nurse data collectors for two weeks to develop a comprehensive uniform approach to error detection Interrater reliability was verified in the month before formal data col-lection and again every other month during the study period
Baseline data were collected for six to eight weeks in each unit during a six-month period from March to August 2000 After the introduction of unit-based clinical pharmacists data were collected concurrently in each intervention and control ICU or general unit pair
11202012 Page 294 of 417
Practice rePorts Medication errors
1256 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
for three months between June and November 2000
Medication errors near misses and ADEs were identified through detailed review of all medication orders MARs and patient charts by a nurse data collector randomly as-signed to each study unit on a daily basis These reviews were performed each weekday and on Mondays for the previous weekend To compile as complete a list as possible we also solicited reports of errors from house officers nurses and pharmacists Reporting a medication error did not trigger a review of clinical data rather all clinical data were reviewed daily for all patients enrolled in the study All reported errors had previ-ously been identified in the review process
Data collected for each error near miss or ADE included the drug name dose route and category the point in the system at which the error occurred the type of error medi-cal teams involved and additional work resulting from the error The data collectors evaluated whether near misses had been intercepted Data on the complexity of individual drug regimens including number and types of drugs were recorded Clinical and demographic data were collected from patient records and institutional administrative data-bases Morbidity and disability data were collected until discharge for all patients with an ADE
Two physicians independently reviewed each suspected ADE and near miss and classified them as ADEs near misses or medication errors The reviewers were blinded to the time period (ie before or after intervention) and the unit loca-tion of events in order to minimize potential bias The reviewers used a four-point Likert scale to rate the severity of injury for ADEs and near misses Preventability of ADEs was rated on a five-point Likert scale and attribution (ie the likelihood that an incident was due to the specific
drug) was rated with the algorithm of Naranjo et al23 Disagreements between reviewers were resolved through discussion and consensus
Intervention After baseline error rates were obtained for all six units a unit-based clinical pharmacist was added to the team in one medical unit one surgical unit and one ICU These pharmacistsrsquo primary role was to provide physicians with timely information and advice on ADEs drug interactions and appropriate dosages dose intervals and routes of administration In addition they facilitated communication between the medical care team and the phar-macy and assisted nurses with drug preparation by providing informa-tion on administration and moni-toring They also helped monitor the order transcription process and the medication preparation stor-age and distribution systems The pharmacist was an integral part of the unit-based continuous quality-improvement (CQI) team which in-cluded a unit nurse administrator a unit attending physician a member of the unit nursing staff a member of the house staff and one of the studyrsquos principal investigators or coinvestigators The CQI team met bimonthly to review serious medi-cation errors and to design process changes and system improvements to be implemented after the comple-tion of data collection
In the ICU the pharmacist was present full-time (40 hours per week) and participated daily in physician rounds In the general medical and surgical units the pharmacist was available only on a part-time basis during morning hours The pharma-cist in the general surgical unit often had difficulty attending rounds with surgeons which occurred in the early morning before the start of daytime pharmacist shifts and before sched-uled surgeries In the general medical unit the pharmacist tended to leave shortly after physician rounds were completed
Statistical methods We report preintervention and postinterven-tion rates of serious medication er-rors (nonintercepted near misses and preventable ADEs) per 1000 patient days assuming a Poisson distribu-tion Measures of interrater reliabil-ity (before discussion and consensus) were calculated using the kappa statistic with moderate-to-excellent levels of agreement (075 for incident classification) The a priori level of significance was 005
ResultsDuring the study period we ex-
amined a total of 1249 admissions in the ICUs 1690 admissions in the general medical units and 1924 admissions in the general surgical units Table 1 summarizes patient de-mographics Preintervention patients were generally similar to postinter-vention patients in all studied units with most variation occurring in age distribution
Table 2 summarizes serious medi-cation error rates The ICU with the full-time unit-based clinical pharma-cist had a decrease in serious medica-tion errors from 29 per 1000 patient days before the intervention to 6 per 1000 patient days after the interven-tion (p lt 001) On the other hand during the intervention period the rate of intercepted near misses in the intervention ICU increased from 32 to 57 per 1000 patients (p = 008) There was no significant difference between the two ICUs in the prein-tervention rates of serious medica-tion errors There were 33 fewer net serious medication errors per 1000 patient days in the intervention ICU (where the reduction was 23 errors per 1000 patient days) than in the control ICU (where the rate increased by 10 errors per 1000 patient days) (p lt 0001) There was no reduction in the rate of serious medication errors with pharmacist participation in the general units In both ICUs a ma-jority of detected errors occurred at the drug ordering stage (67ndash100)
11202012 Page 295 of 417
Practice rePorts Medication errors
1257Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Intensive Care Units n 209 401 280 359 Mean LOS (days) (95 CI) 594 (412ndash776) 650 (480ndash819) 545 (429ndash662) 628 (492ndash765) No () female 79 (38) 179 (45) 128 (46) 169 (47) Race (no []) White 129 (62) 253 (63) 190 (68) 221 (62) Black 18 (9) 36 (9) 17 (6) 19 (5) Asian 6 (3) 9 (2) 6 (2) 8 (2) Hispanic 15 (7) 31 (8) 14 (5) 26 (7) Other 7 (3) 23 (6) 22 (8) 32 (9) Unknown 34 (16) 49 (12) 31 (11) 53 (15) Age (no []) 0ndash1 mo 17 (8) 34 (8) 44 (16) 78 (22) 2 mondash1 yr 39 (19) 81 (20) 64 (23) 100 (28) 2ndash5 yr 37 (18) 78 (19) 47 (17) 58 (16) 6ndash12 yr 54 (26) 87 (22) 54 (19) 55 (15) 13ndash19 yr 52 (25) 86 (21) 55 (20) 35 (10) gt19 yr 10 (5) 35 (9) 16 (6) 33 (9) No () with Medicaid 51 (24) 83 (21) 52 (19) 85 (24)General Medical Units n 56 296 383 955 Mean LOS (days) (95 CI) 449 (321ndash577) 570 (473ndash666) 289 (247ndash331) 288 (252ndash324) No () female 26 (47) 143 (48) 172 (45) 428 (45) Race (no []) White 29 (53) 182 (61) 187 (49) 485 (51) Black 10 (18) 37 (13) 51 (13) 140 (15) Asian 2 (4) 4 (1) 16 (4) 30 (3) Hispanic 6 (11) 35 (12) 57 (15) 161 (17) Other 1 (2) 15 (5) 31 (8) 47 (5) Unknown 7 (13) 23 (8) 41 (11) 92 (10) Age (no []) 0ndash1 mo 2 (4) 20 (7) 56 (15) 187 (20) 2 mondash1 yr 17 (30) 37 (13) 176 (46) 289 (30) 2ndash5 yr 5 (9) 50 (17) 76 (20) 204 (21) 6ndash12 yr 18 (32) 96 (32) 58 (15) 168 (18) 13ndash19 yr 12 (21) 73 (25) 15 (4) 98 (10) gt19 yr 2 (4) 20 (7) 2 (1) 9 (1) No () with Medicaid 17 (30) 81 (27) 89 (23) 188 (20)General Surgical Units n 369 745 279 531 Mean LOS (days) (95 CI) 353 (288ndash418) 374 (333ndash414) 446 (368ndash524) 660 (410ndash910) No () female 188 (51) 370 (50) 112 (40) 223 (42) Race (no []) White 286 (78) 557 (75) 195 (70) 388 (73) Black 16 (4) 48 (6) 18 (6) 36 (7) Asian 9 (2) 13 (2) 5 (2) 7 (1) Hispanic 19 (5) 45 (6) 27 (10) 39 (7) Other 13 (4) 20 (3) 10 (4) 23 (4) Unknown 26 (7) 62 (8) 24 (9) 38 (7)
Table 1Demographic Characteristics of Study Patientsa
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
Continued on next page
11202012 Page 296 of 417
Practice rePorts Medication errors
1258 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
Interception of errors by unit-based clinical pharmacists occurred at all stages of the medication process with most intercepted errors (79) occurring at the physician ordering stage
The increase in the serious medi-cation error rate in the control ICU was largely attributable to an incor-rect preprinted order template for acetaminophen that resulted in the ordering of significant overdoses After excluding these acetamino-phen errors from our data analysis there would still be a net of 30 fewer serious medication errors per 1000 patient days in the intervention ICU than in the control ICU (p = 001) The acetaminophen template error was recognized and rectified through review of data by the CQI team
DiscussionOur results suggest that the in-
troduction of a full-time unit-based clinical pharmacist was associated with a 79 reduction in the serious medication error rate in critically ill pediatric inpatients However we found no apparent effect from adding part-time unit-based clinical pharmacists to the general medical and surgical units Because of the low baseline error rates on these units the study may have been underpow-ered to detect a difference associated with the intervention We speculate however that the primary reason for efficacy of the intervention only in
the ICU may have been the full-time presence of the pharmacist in the ICU and only part-time involvement in the general medical and surgical units
Some patient care units appear to have organizational characteristics that either facilitate or impede col-laboration with a clinical pharmacist For example rounds in the ICU were conducted with a multidisciplinary team at the bedside whereas rounds in the general medical and surgical units were often conducted away from the bedside and orders were not entered during rounds Such proce-dural differences may have mitigated the ability of the pharmacist to cor-rect errors in real time In addition the ICU tends to treat fewer patients and house staff physicians usually are in or near the unit and easily acces-sible to staff including unit-based clinical pharmacists In the general units patients are more spread out and each physician is responsible for more patients often on multiple floors In addition surgeons spend a considerable portion of each day in the operating room although the surgeons had a covering nurse practitioner it has been previously demonstrated that opportunities for error increase when decision-making responsibilities are ldquohanded off rdquo from one provider to another2425
Further research is necessary to determine if the addition of a full-time unit-based clinical pharmacist
and increased physicianndashpharmacist interaction decrease medication errors in the general medical or surgical unit setting A recent study by Kucukarslan et al21 suggests that pharmacist participation on a general medicine unit may indeed contribute to a significant reduc-tion in preventable ADEs Our study supports the conclusion that adding pharmacists to medical and surgi-cal rounds is challenging Altering the shifts of clinical pharmacists so that they are available early for sur-geonsrsquo rounds having them available throughout the day and having them make rounds with covering nurse practitioners are strategies for im-proving their effectiveness on general medical or surgical units
The benefit of unit-based clinical pharmacists in the pediatric ICU in this study is similar to what has been observed in adult ICUs We found a 79 decrease in the rate of serious medication errors in the pediatric ICU while Leape et al20 using a very similar method found a 66 decrease in preventable ADEs at the ordering stage in an adult ICU Our study showed a decrease in serious medication error rates at all stages whereas Leape et al were concentrat-ing on errors at the ordering stage
Like many previous studies our study documented higher rates of serious medication errors in the pe-diatric intensive care setting922 This is likely the result of greater patient
aData are reported for preintervention and postintervention periods although no intervention occurred in the control units LOS = length of stay CI = confidence interval
Age (no []) 0ndash1 mo 0 2 (0) 32 (11) 59 (11) 2 mondash1 yr 18 (5) 33 (4) 139 (50) 253 (48) 2ndash5 yr 46 (13) 72 (10) 93 (33) 155 (29) 6ndash12 yr 129 (35) 273 (37) 15 (5) 56 (11) 13ndash19 yr 143 (39) 287 (39) 0 8 (2) gt19 yr 33 (9) 78 (10) 0 0 No () with Medicaid 55 (15) 117 (16) 41 (15) 75 (14)
Table 1 (continued)
CharacteristicIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
11202012 Page 297 of 417
Practice rePorts Medication errors
1259Am J Health-Syst PharmmdashVol 65 Jul 1 2008
morbidity and medication complex-ity Implementing error prevention strategies such as the use of unit-based clinical pharmacists in ICUs is particularly efficacious because of these higher baseline error rates
Despite a growing body of data demonstrating the potential of unit-based clinical pharmacists to decrease medication errors only 30 of hos-pitals nationwide have pharmacists participating in physician rounds26 Pharmacists actively participating in rounds provide real-time advice to physicians in the same way that CPOE systems provide real-time computer-ized decision support Studies have demonstrated that physicians are much more amenable to changing therapeutic direction when advice is given before rather than after order completion27 Since about 80 of near misses in pediatric inpatients occur during medication ordering9 unit-based clinical pharmacists can intercept errors and inform clinical choices before orders are finalized They can also intercept other types of medication errors by independently monitoring the transcription drug preparation storage and dispensing of medications
In addition to being effective unit-based clinical pharmacists are practical and financially justifiable Both adult and pediatric ICUs have shown significant cost savings from implementation of a unit-based clinical pharmacist program2829 Unit-based clinical pharmacists are generally less expensive than most IT-based patient safety interven-tions which can cost millions of dollars to implement and main-tain30 By restructuring existing pharmacist resources from central-ized to unit-based positions hospi-tals can quickly decrease errors and perhaps the overall cost of care
Our study has several limitations First it was performed in a single freestanding academic pediatric hospital which limits its generaliz-ability Ideally unit-based clinical pharmacists would have been pres-ent full-time on all study units but this was not achieved It also seems likely that the individual attributes of clinical pharmacists have an im-portant impact on their efficacy in reducing error rates However given the single-institution design of this study we were unable to assess such factors
ConclusionA full-time unit-based clinical
pharmacist substantially decreased the serious medication error rate in the pediatric intensive care setting but a part-time pharmacist was not as effective in general care pediatric units
References
1 Kohn LT Corrigan JM Donaldson MS To err is human building a safer health system Washington DC National Acad-emy Press 1999
2 Brennan TA Leape LL Laird NM et al Incidence of adverse events and negli-gence in hospitalized patients Results of the Harvard Medical Practice Study I N Engl J Med 1991 324370-6
3 Cook R Woods D Miller C A tale of two stories contrasting views of patient safety Chicago National Patient Safety Foundation 1998
4 Leape LL Brennan TA Laird N et al The nature of adverse events in hospitalized patients Results of the Harvard Medical Practice Study II N Engl J Med 1991 324377-84
5 Thomas EJ Studdert DM Burstin HR et al Incidence and types of adverse events and negligent care in Utah and Colorado Med Care 2000 38(3)261-71
6 Thomas EJ Studdert DM Newhouse JP et al Costs of medical injuries in Utah and Colorado Inquiry 1999 36(3)255-64
7 Bates DW Boyle DL Vander Vliet MB et al Relationship between medication er-
Intensive Care Units No patient days 311 835 1062 759 No SMEs 9 5 21 23 SMEs1000 patient days 29 6 20b 30c
General Medical Units No patient days 660 1163 604 1319 No SMEs 5 10 4 10 SMEs1000 patient days 8 9 7d 8e
General Surgical Units No patient days 573 1109 737 1253 No SMEs 4 10 6 12 SMEs1000 patient days 7 9 8f 10g
Table 2Occurrence of Serious Medication Errors (SMEs) in Study Unitsa
VariableIntervention Unit
Preintervention PostinterventionControl Unit
Preintervention Postintervention
aData are reported for preintervention and postintervention periods although no intervention occurred in the control unitsbp = 038 for comparison with intervention unitcp lt 001 for comparison with intervention unitdp = 084 for comparison with intervention unitep = 078 for comparison with intervention unitfp = 081 for comparison with intervention unitgp = 089 for comparison with intervention unit
11202012 Page 298 of 417
Practice rePorts Medication errors
1260 Am J Health-Syst PharmmdashVol 65 Jul 1 2008
rors and adverse drug events J Gen Intern Med 1995 10(4)199-205
8 Marino BL Reinhardt K Eichelberger WJ et al Prevalence of errors in a pediatric hospital medication system implications for error proofing Outcomes Manag Nurs Pract 2000 4(3)129-35
9 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
10 AHA guide to computerized order entry application Washington DC American Hospital Association 2000
11 Sittig DF Stead WW Computer-based physician order entry the state of the art J Am Med Inform Assoc 1994 1108-23
12 Metzger J Turisco F Computerized order entry a look at the vendor marketplace and getting started Oakland CA Cali-fornia Healthcare Foundation and First Consulting Group 2001
13 Bates DW Leape LL Cullen DJ et al Effect of computerized physician order entry and a team intervention on preven-tion of serious medication errors JAMA 1998 2801311-6
14 Bates DW Teich JM Lee J et al The impact of computerized physician order entry on medication error prevention J Am Med Inform Assoc 1999 6313-21
15 King WJ Paice N Rangrej J et al The effect of computerized physician order entry on medication errors and adverse
drug events in pediatric inpatients Pedi-atrics 2003 112(3 pt 1)506-9
16 Potts AL Barr FE Gregory DF et al Computerized physician order entry and medication errors in a pediatric criti-cal care unit Pediatrics 2004 113(1 pt 1)59-63
17 Koppel R Metlay JP Cohen A et al Role of computerized physician order entry systems in facilitating medication errors JAMA 2005 2931197-203
18 Trooskin SZ Low-technology cost-efficient strategies for reducing medica-tion errors Am J Infect Control 2002 30351-4
19 Healthcare leaders urge adoption of methods to reduce adverse drug events National Patient Safety Partnership 1999 News release
20 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA 1999 282267-70
21 Kucukarslan SN Peters M Mlynarek M et al Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units Arch Intern Med 2003 163 2014-8
22 Bates DW Cullen DJ Laird N et al In-cidence of adverse drug events and po-tential adverse drug events Implications for prevention ADE Prevention Study Group JAMA 1995 27429-34
23 Naranjo CA Busto U Sellers EM et al A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther 1981 30239-45
24 Gandhi TK Fumbled handoffs one dropped ball after another Ann Intern Med 2005 142352-8
25 Petersen LA Brennan TA OrsquoNeil AC et al Does housestaff discontinuity of care increase the risk for preventable adverse events Ann Intern Med 1994 121866-72
26 Peterson CA Schneider PJ Santell JP ASHP national survey of pharmacy prac-tice in hospital settings prescribing and transcribingmdash2001 Am J Health-Syst Pharm 2001 582251-66
27 Bates DW Kuperman GJ Wang S et al Ten commandments for effective clinical decision support making the practice of evidence-based medicine a reality J Am Med Inform Assoc 2003 10523-30
28 Montazeri M Cook DJ Impact of a clinical pharmacist in a multidisciplinary intensive care unit Crit Care Med 1994 221044-8
29 Crowson K Collette D Dang M et al Transformation of a pharmacy depart-ment impact on pharmacist interven-tions error prevention and cost Jt Comm J Qual Improv 2002 28324-30
30 Kaushal R Jha A Franz C et al Return on investment for a computerized physician order entry system J Am Med Inform As-soc 2006 13261-6
11202012 Page 299 of 417
NOTES Medication-error reporting
1422 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
JENNIFER L COSTELLO PHARMD is Pediatric Clinical Pharmacist Childrenrsquos Hospital of New Jersey at Newark Beth Israel Medical Center (NBIMC) Newark DEBORAH LLOYD TOROWICZ MSN RN PHD(C) is Pediatric Nurse Practitioner Childrenrsquos Hospital of Philadelphia at the time of this study she was Nursing Director Pediatric Critical Care and Cardiac Nursing Childrenrsquos Hospital of New Jersey at NBIMC TIMOTHY S YEH MD is Chairman Depart-ment of Pediatrics and Division Director Pediatric Critical Care
Childrenrsquos Hospital of New Jersey at NBIMCAddress correspondence to Dr Costello at Childrenrsquos Hospital of
New Jersey Newark Beth Israel Medical Center 201 Lyons Avenue Newark NJ 07112 (jcostellosbhcscom)
Copyright copy 2007 American Society of Health-System Pharma-cists Inc All rights reserved 1079-2082070701-1422$0600
DOI 102146ajhp060296
Effects of a pharmacist-led pediatrics medication safety team on medication-error reporting
JENNIFER L COSTELLO DEBORAH LLOYD TOROWICZ AND TIMOTHY S YEH
Purpose The effects of a pharmacist-led pediatrics medication safety team (PMST) on the frequency and severity of medica-tion errors reported were studied Methods This study was conducted in a pediatric critical care center (PCCC) in three phases Phase 1 consisted of retrospective collection of medication-error reports be-fore any interventions were made Phases 2 and 3 included prospective collection of medication-error reports after several interventions Phase 2 introduced a pedi-atrics clinical pharmacist to the PCCC A pediatrics clinical pharmacist-led PMST (including a pediatrics critical care nurse and pediatrics intensivist) a new reporting form and educational forums were added during phase 3 of the study In addition education focus groups were held for all intensive care unit staff Outcomes for all phases were measured by the number of medication-error reports processed the number of incidents error severity and the specialty of the reporter
Results Medication-error reporting in-creased twofold threefold and sixfold be-tween phases 1 and 2 phases 2 and 3 and phases 1 and 3 respectively Error severity decreased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors were classified as category D or E respectively Conversely the reporting of near-miss errors increased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3 Conclusion An increase in the number of medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
Index terms Clinical pharmacists Docu-mentation Education Errors medication Forms Health professions Hospitals Inter-ventions Pediatrics Reports TeamAm J Health-Syst Pharm 2007 641422-6
Medication errors have been recognized as one of the major causes of iatrogenic disease in
the United States and have risen to the forefront of safety initiatives in health care institutions12 It has been estimated that 44000ndash98000 people die each year in the United States as a result of a medication error3 Medication errors are prevalent in both adult and pediatric populations Errors have the capacity to result in harm and can occur during any phase of the medication-use process Although medication errors occur at similar rates in the adult and pediat-ric populations errors in pediatric patients have three times the poten-tial to cause harm4 Compared with errors that occur in adults medica-tion errors in children are understud-ied and most likely underreported5
Medication errors have been re-ported in a variety of pediatric set-tings including general pediatrics wards pediatric intensive care units (PICUs) neonatal intensive care units and pediatric emergency de-partments13-6 Children in intensive care settings are at greatest risk for iatrogenic complications most likely a result of environmental intensity clinical symptoms severity of illness
comorbidities and an inability to communicate178
Multiple studies have analyzed error-prevention strategies utiliz-ing a clinical pharmacist1-49 Several reports have shown that ward-based clinical pharmacists reduce medica-tion errors9-12 Other studies have ad-
dressed collaboration between nurs-ing and other disciplines but only a limited number of articles have been published regarding nursendashpharmacy collaboration13 An extensive review of the literature did not produce any studies evaluating the effects of a nursendashpharmacist team on medi-
11202012 Page 300 of 417
NOTES Medication-error reporting
1423Am J Health-Syst PharmmdashVol 64 Jul 1 2007
cation errors in a PICU However intensive care outcomes resulting from interdisciplinary collaboration among nursing medicine and other disciplines have been reported1415 We hypothesized that the use of an interdisciplinary team including a nurse pharmacist and physician would reduce the severity of medi-cation errors through nonpunitive reporting and increased awareness through staff education The objec-tives of the study were to increase medication-error reporting and reduce the severity of medication er-rors reported in the pediatric critical care center (PCCC) by implementing a pediatrics medication safety team (PMST) comprising a pediatrics clinical pharmacist a pediatrics criti-cal care nurse and a pediatrics medi-cal intensivist
MethodsThe study was approved by the
hospitalrsquos institutional review board and conducted in three phases in a 19-bed PCCC Phase 1 conducted between September and December of 2004 involved a retrospective analysis of medication-error re-ports retrieved from the institutionrsquos medication-incident database The reports were sorted by number of incidents error type severity and specialty of reporter (ie nurse physi-cian pharmacist or dietitian) During phase 2 conducted between February and May of 2005 a clinical pharmacist was introduced to the PCCC The pharmacistrsquos effect on medication errors was analyzed prospectively utilizing the existing medication- error reporting system When phase 2 was completed three variables were introduced to the pediatrics critical care staff a PMST a new reporting system and monthly focus groups The PMST included a nurse leader medical director and clinical phar-macist all of whom had expertise in pediatrics critical care
The new medication-incident reporting form was adapted from
Cimino et al16 (Figure 1) When a medication incident was identified the form was completed and placed in a labeled box kept in the medica-tion room of the PCCC Staff were not required to sign the form or identify themselves in any manner Inservice education on the report-ing process was provided to all staff At the end of each month the nurse leader and pharmacist reviewed the medication-incident reports Each incident was subsequently entered into the medication-incident data-base by the clinical pharmacist The database classifies incidents by sever-ity (appendix)
Education was provided to health care providers during patient care rounds and during monthly open forums with the critical care staff and the PMST All monthly forums were interactive At the beginning of each meeting the prior monthrsquos medica-tion incidents were addressed using root-cause analysis This method was used to discover and address system flaws instead of focusing on individual staff members During the second part of each meeting the new reporting process was reviewed and staff brainstormed to develop innovative ways to prevent future medication errors The outcomes of these interventions were measured prospectively in phase 3 (Junendash September 2005)
ResultsA total of 109 medication-error
reports were identified between June and September of 2005 Over the three phases of the study patient vol-ume remained constant in the PCCC The total numbers of reported errors for each phase of the study are shown in Figure 2 There was a twofold in-crease in medication-error reporting between phase 1 (baseline) and phase 2 and a sixfold increase between phases 1 and 3 A threefold increase was observed between phases 2 and 3 Table 1 shows the occurrence of medication errors during phase 3 by
error type and discipline (nursing medicine pharmacy) Medication omission (dispensing delay in service or error in administration time) wrong medication and wrong dose accounted for the highest number of reported errors Error severity de-creased over the three time periods In phases 1 2 and 3 46 8 and 0 of the errors reported were cate-gory D or E respectively Conversely the reporting of near-miss errors in-creased from 9 in phase 1 to 38 in phase 2 and to 51 in phase 3
DiscussionMedication-error reporting was
increased and the severity of medi-cation errors reduced in the PCCC after the implementation of a PMST educational forums and the addi-tion of a clinical pharmacist Over-all medication-error reporting in-creased during phases 2 and 3 We anticipated that the increase in phase 2 would result from the introduction of a clinical pharmacist who would raise staff awareness of medication safety and encourage reporting of all incidents However the increased reporting in phase 2 did not demon-strate the anticipated change since the increase was almost entirely ac-counted for by incidents captured during rounds and chart review by the clinical pharmacist These find-ings demonstrated that the intro-duction of a clinical pharmacist did not change the existing culture of medication-incident reporting dur-ing the study period Reports made by nursing staff remained relatively constant and physician reports de-creased The dramatic increase in reporting during phase 3 was most likely due to several intervening factors including the vigilance of the team leader during rounds and continued presence in the unit the nonpunitive reporting form and the open forums with the intensive care staff If medication incidents were discovered during rounds staff were encouraged to report them The in-
11202012 Page 301 of 417
NOTES Medication-error reporting
1424 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
Figure 1 Medication-incident reporting form16
Patient Name _________________________________________________ MR _________________________________
Date of Suspected Error _________________________________________ UnitDepartment Occurred ________________
Medication NameDoseRoute __________________________________________________________________________________________
Level of Staff That Made Initial Error Pharmacy Nursing Attending ResidentIntern Other________________
Error Type ( all that apply for type and subtype)
Delay in Service DuplicationExtra Dose Expired Medication Given
Given without Orders Given without Proper Storage Given without Checking Parameters
Mislabeled Omission Procedure Error
Wrong Dose Wrong Dosage Interval Wrong Dose Form
Wrong Patient Wrong Infusion Rate Wrong MedicationIV
Wrong Route Wrong Duration of Therapy Wrong Patient WeightAge
Incomplete Order
Monitoring
Other___________________________________________________________________________________________________
Brief Description of Event and Patient Outcome
__________________________________________________________________________________________________________
Did Medication Reach Patient No Yes
If Medication Reached Patient in Error mdash Notify Physician
Was Order Reconciled with Prescriber No Yes
Could Medication Error Have Been Prevented No Yes
___________________
Was the Medication Accessed from
Pyxis Cassette Pharmacy Code Cart
If Accessed from Pyxis Was It an Override No Yes
Medication Error Identified by ( all that apply)
Pharmacy Nursing Attending ResidentIntern
Other _______________________________________
Patient Name ID Number Patient Weight Medication
Dose Dosage Form Dosing Interval Route
Transcription Error Handwriting Illegible
Allergy Information Not Checked Clinical Information DrugndashDrug Interaction
DrugndashFood Interaction IV Incompatibility Laboratory
11202012 Page 302 of 417
NOTES Medication-error reporting
1425Am J Health-Syst PharmmdashVol 64 Jul 1 2007
terventions that resulted in a predic-tive change in behavior and culture were the anonymous medication- error reporting form and nonpuni-tive action by unit leadership
Before the initiation of the anony-mous medication-error reporting form unit leadership addressed medication errors by counseling staff in the traditional method in which staff received an oral warning for the first incident a written warning for the second incident and pos-sible suspension and termination for the third incident Therefore staff perceived any medication- error reporting as a ldquoblack markrdquo on their personnel file that could poten-tially lead to termination In phase 3 unit leadership dealt with all errors through root-cause analysis focusing on education and systems changes to prevent future errors
We believe that the reduction in error severity over the three study phases most likely resulted from in-creased staff awareness through tar-geted medication-error education the global process of medication delivery administration and the reporting of errors earlier in the medication-use
Figure 2 Number of errors reported during study period No errors were reported by medical residents during any phase of the study
No
Err
ors
Study Phase
80
Attending Physician
70
60
50
40
30
20
10
0Phase 1 Phase 2 Phase 3
Total
Nursing
Pharmacy
Dietitian
process For example if a category D or E error resulted from a pre-scribing transcribing dispensing or administration error staff would have a heightened awareness of the error and thus be more diligent when performing the first three steps of the medication-use process Thus the error severity would be reduced be-cause it would be discovered earlier in the process
Education appeared to reach all members of the medical team as exemplified by an instance in which the clinical dietitian reported an er-ror related to an order for total par-enteral nutrition Medication-error reporting by attending physicians did not increase in fact it decreased There were no reports made by at-tending physicians in the last phase of the study Further examination of the data revealed that physicians reported incidents that resulted in temporary or permanent harm to the patient and incidents that required the patient to have increased monitoring There were no category D or higher inci-dents reported during phase 3
In all phases there was a lack of reporting by medical residents
even though they were specifically targeted at educational forums We did observe a dramatic increase in nursesrsquo reports Overall nursing staff became more proactive over the study period which we attribute to the nonpunitive reporting form im-proved pharmacyndashnursing interac-tion and improved communication and feedback through focus groups
Improvements in medication- error reporting and reductions in the severity of medication errors can be achieved through planned inter-ventions such as the introduction of a PMST Changing the hospital culture and environment is essential but it must include an integrative approach Increased communica-tion through education forums the presence of a clinical pharmacist as a team leader and a nonpunitive ap-proach by medical and nursing lead-ership can produce culture changes that positively affect patient out-comes One area that requires further attention is the effort to change the behavior of medical residents since they are responsible for prescribing many medication regimens in teach-ing hospitals
11202012 Page 303 of 417
NOTES Medication-error reporting
1426 Am J Health-Syst PharmmdashVol 64 Jul 1 2007
An unexpected observation dur-ing the study was that the current pharmacy services could not meet the demands of a pediatric critical care unit The study provided sup-port that led to the development of a pediatrics pharmacy satellite and improved pharmacy services
ConclusionAn increase in the number of
medication errors reported and a decrease in the severity of errors reported were observed in a PCCC after implementation of a PMST provision of education to health care providers and addition of a clinical pharmacist
References1 Ross LM Wallace J Paton JY Medication
errors in a paediatric teaching hospital in the UK five years operational experience Arch Dis Child 2000 83492-7
2 Stucky ER American Academy of Pedi-atrics Committee on Drugs American Academy of Pediatrics Committee on Hospital Care Prevention of medication errors in the pediatric inpatient setting Pediatrics 2003 112431-6
3 Kohn LT Corrigan JM Donaldson MS eds To err is human building a safer health system Washington DC National Academy Press 1999
4 Fortescue EB Kaushal R Landrigan CP et al Prioritizing strategies for prevent-ing medication errors and adverse drug events in pediatric inpatients Pediatrics 2003 111722-9
5 Slonim AD LaFleur BJ Ahmed W et al Hospital-reported medication errors in children Pediatrics 2003 111617-21
6 Fernandez CV Gillis-Ring J Strategies for the prevention of medical error in pediat-rics J Pediatr 2003 143155-62
7 Portnoy JD Dominguez TE Lin RJ et al Epidemiology of medication errors in the pediatric intensive care unit Crit Care Med 2003 31A14 Abstract
8 Kaushal R Bates DW Landrigan C et al Medication errors and adverse drug events in pediatric inpatients JAMA 2001 2852114-20
9 Leape LL Cullen DJ Clapp MD et al Pharmacist participation on physi-cian rounds and adverse drug events in the intensive care unit JAMA1999 282267-70 [Erratum JAMA 2000 2831293]
10 Folli HL Poole RL Benitz WE et al Medication error prevention by clinical pharmacist in two childrenrsquos hospitals Pediatrics 1987 79718-22
11 Krupicka MI Bratton SL Sonnenthal K et al Impact of a pediatric pharmacist in the pediatric intensive care unit Crit Care Med 2002 30919-21
12 Kane SL Weber RJ Dasta JF The impact of critical care pharmacists on enhancing patient outcomes Intensive Care Med 2003 29691-8
13 Merrow S Segelman M Nursendashpharma-cist collaboration in clinical nursing edu-cation Nursingconnections1989 255-62
14 Hospitalists pharmacists partner to cut errors Healthcare Benchmarks Qual Im-prov 2005 12(2)18-9 Letter
15 Taylor JA Brownstein D Christakis DA et al Use of incident reports by physicians and nurses to document medical errors in pediatric patients Pediatrics 2004 114729-35
16 Cimino M Kirschbaum MS Brodsky L et al Assessing medication prescrib-ing errors in pediatric intensive care units Pediatr Crit Care Med 2004 5 124-32
Circumstance or event had the capacity to cause an error
An error occurred but did not reach the patient (an ldquoerror
of omissionrdquo reaches the patient)
An error occurred that reached the patient but did not
cause patient harm
An error occurred that reached the patient and required
monitoring to confirm that it resulted in no harm to the
patient or required intervention to preclude harm
An error occurred that may have contributed to or re-
sulted in temporary harm to the patient and required
intervention
An error occurred that may have contributed to or resulted
in temporary harm to the patient and required initial or
prolonged hospitalization
An error occurred that may have contributed to or resulted
in permanent patient harm
An error occurred that required intervention necessary to
sustain life
An error occurred that may have contributed to or resulted
in the patientrsquos death
Type of Error Category Description
No error
Error no harm
Error harm
Error death
A
B
C
D
E
F
G
H
I
AppendixmdashDefinitions of error severity
Omission errorWrong medication or dosageWrong patientPyxis errorWrong or incomplete orderTranscription errorWrong rateUnauthorized drug
Table 1Number and Type of Medication Errors Reported during Phase 3 by Discipline
Type of Error
Discipline
Prescriber Pharmacy Nursing
016
00
10000
3128
210000
01001653
11202012 Page 304 of 417
THE ANNALS 40-YEAR EVOLUTION
1170 n The Annals of Pharmacotherapy n 2006 June Volume 40 wwwtheannalscom
2006 marks the 40th year of publication for The Annals Over that time The Annals has been an important contributor to the
development of clinical pharmacy Throughout 2006 we are publishing articles reflecting on the history of clinical pharmacy
through the eyes of practitioners including those pioneering clinical pharmacy as well as those who have more recently en-
tered the profession and a well-established specialty In addition we are also presenting articles and editorials from the early
history of The Annals that have given direction and shape to the practice of clinical pharmacy (see page 1174)
Nearly 42 years ago Harry Shirkey (a pediatrician fromCincinnati) termed infants and children as ldquotherapeu-
tic orphansrdquo He was concerned that drugs may be given tothese patients without adequate studies on their efficacyand safety Although progress has been made many drugscontinue to be used in young pediatric patients when theyhave been approved by the Food and Drug Administration(FDA) only for adults For the first time the FDA Mod-ernization Act provides a ldquocarrotrdquo of 6 months of marketexclusivity for drugs under patent if the manufacturer con-ducts studies in children The Best Pharmaceuticals forChildren Act of 2002 directs the Secretary of the Depart-ment of Health and Human Services (through the NationalInstitutes of Health Director and the FDA Commissioner)to develop and prioritize a list of drugs that need to bestudied Table 1 provides a list of drugs requiring pediatricstudies
This suggests that the need for pharmacokinetic phar-macodynamic pharmacogenetic efficacy and safety stud-ies in pediatric patients continues Since most drugs not la-
beled for this population are not available in appropriatedosage forms the need for the development of suitable pe-diatric drug formulations also exists
What Has Changed in Terms of PediatricPharmacy Practice
Robert Levin described clinical pharmacy practice in apediatric clinic in the pages of this journal in 1972 (seepage 1175) Pharmacistsrsquo clinical responsibilities at thattime included counseling patients and families about medi-cations by obtaining complete family and medication his-tory identifying adverse drug reactions and monitoringdrug therapy as well as teaching physicians and pharmacystudents about drug therapy
John Piecoro began an inpatient pediatric clinical phar-macy practice at the University of Kentucky Medical Cen-ter in 1969 His recollection of major accomplishments in-cluded establishment of a well-defined role in patientcare involvement with making rounds with pediatricteams provision of unit dose dispensing dose standardiza-tion parenteral nutrition resuscitation medications andclinical pharmacy services through a satellite pharmacyand training of pharmacy residents as well as pharmacy
Evolution of Pediatric Clinical Pharmacy
Milap C Nahata
Author information provided at the end of the text
Dr Nahata is Editor-in-Chief of The Annals
11202012 Page 305 of 417
students He also was aware of pediatric pharmacy ser-vices offered by Roger Klotz in Chicago
In 1979 I was the first clinical pharmacist at ColumbusChildrenrsquos Hospital and faced similar challenges I can re-member my first day on the infectious disease ward whenall of the physicians seemed to wonder why a pharmacistwas on the 6th floor rather than in the basement I was theinterface between the dispensing pharmacist and the physi-cians and offered clinical pharmacy services and therapeu-tic drug monitoring My other responsibilities included de-veloping a research program (writing grants abstracts andarticles) and teaching physicians pharmacists and medicaland pharmacy students at the hospital as well as at OhioState University (OSU) Soon other specialties includingneonatology hematologyoncology and critical care start-ed requesting clinical pharmacy services Today there are7 clinical pharmacy specialists at Childrenrsquosmdash6 funded bythe hospital and 1 funded by the college
Pediatric Pharmacy Advocacy Group (PPAG) devel-oped pediatric pharmacy practice guidelines in 1991American Society of Health-System Pharmacists [ASHP]Guidelines for Providing Pediatric Pharmaceutical Ser-vices in Organized Health Care Systems were published in1993 These included general principles orientation andtraining programs inpatient services ambulatory care ser-vices drug information therapeutic drug monitoring phar-macokinetic services patient and caregiver educationmedication errors adverse drug reactions drug use evalua-tions and research We are able to treat most illnessesmore effectively today than before and yet new challengesamong children and adolescents include rising rates ofobesity type 2 diabetes primary hypertension and psychi-atricbehavioral disorders
How Has Pediatric Pharmacy Education andTraining Changed Over the Past 40 Years
The majority of schools of pharmacy during the 1960sthrough the 1980s offered a BS (Pharmacy) degree PharmDis now the sole entry-level degree Both didactic education
and clerkship experiences are now being provided for ev-ery pharmacy student The required number of lecturehours has increased and many schools including OSUoffer an elective course in pediatric drug therapy Clerkshipexperience in pediatrics is required by the AccreditationCouncil for Pharmacy Education
Residencies and fellowships have been instrumental inpreparing practitioners and scholars There are 19 specialtyresidency programs in pediatric pharmacy practice current-ly accredited by the ASHP Additional general pharmacypractice residencies with emphasis in pediatrics may alsobe offered to PharmD graduates Seven pediatric fellow-ship programs are listed in the American College of Clini-cal Pharmacy (ACCP) database We have provided fellow-ship training to 25 fellows over the past 20 years Howev-er the number of residency and fellowship programsappears to be too low to meet future needs The funding of13 pediatric pharmacology research units by the NationalInstitute of Child Health and Human Development hasstimulated research in pediatric pharmacotherapy
Summary
Pediatric drug therapy has definitely improved over thepast 40 years Activities in practice research and educa-tion have all expanded The Pediatric Special InterestGroup of ASHP was the main venue for pharmacistsACCPrsquos Practice and Research Network and PPAG arenow additional venues for pediatric practitioners to sharetheir knowledge and skills with colleagues The future ofpediatric pharmacotherapy indeed looks bright
Milap C Nahata MS PharmD Professor and Division Chair Col-lege of Pharmacy Professor of Pediatrics and Internal MedicineCollege of Medicine Ohio State University (OSU) Associate Direc-tor of Pharmacy OSU Medical Center Columbus OH
I appreciate the input from John Piecoro MS PharmD at the University of Kentucky
Published Online 30 May 2006 wwwtheannalscomDOI 101345aph1G459
The Annals of Pharmacotherapy n 2006 June Volume 40 n 1171wwwtheannalscom
AcyclovirAmpicillinAmpicillinsulbactamAzithromycinBaclofenBumetanideBupropion ClonidineCyclosporineDactinomycin
DaunomycinDexrazoxaneDiazoxideDobutamineDopamineEletriptanEthambutolFlecainideFurosemideGriseofulvin
HeparinHydrochlorothiazideHydrocortisone valerate ointment and cream
HydroxychloroquineHydroxyureaIsofluraneIvermectinKetamineLindane
LithiumLorazepamMeropenemMethadoneMethotrexateMetoclopramideMetolazoneMorphinePiperacillintazobactamPralidoxime
PromethazineRifampinSevelamerSodium nitroprussideSpironolactoneVincristineZonisamide
Table 1 Drugs Listed by Department of Health and Human Services Requiring Studies in Pediatric Patientsa
aApril 25 2006
11202012 Page 306 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
httpwwwpediatricsorgcgicontentfull113159located on the World Wide Web at
The online version of this article along with updated information and services is
rights reserved Print ISSN 0031-4005 Online ISSN 1098-4275 Grove Village Illinois 60007 Copyright copy 2004 by the American Academy of Pediatrics All and trademarked by the American Academy of Pediatrics 141 Northwest Point Boulevard Elkpublication it has been published continuously since 1948 PEDIATRICS is owned published PEDIATRICS is the official journal of the American Academy of Pediatrics A monthly
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 307 of 417
Computerized Physician Order Entry and Medication Errors in aPediatric Critical Care Unit
Amy L Potts PharmD Frederick E Barr MD MSCIDagger David F Gregory PharmD BCPSLorianne Wright PharmD and Neal R Patel MD MPHDaggersect
ABSTRACT Objective Medication errors are a majorconcern of health care professionals and medical institu-tions especially errors involving children Studies inadults have shown that computerized physician orderentry (CPOE) systems reduce medication errors and ad-verse drug events (ADEs) The effect of CPOE implemen-tation in a pediatric population has not been reportedThe objective of this study was to evaluate the impact ofCPOE on the frequency of errors in the medication or-dering process in a pediatric critical care unit (PCCU)
Methods A prospective trial was conducted of 514pediatric patients who were admitted to a 20-bed PCCUin a tertiary-care childrenrsquos hospital before and after im-plementation of CPOE Medication errors were identi-fied after review of all orders during the study periodand then further classified as potential ADEs medicationprescribing errors (MPE) and rule violations (RV)
Results A total of 13 828 medication orders were re-viewed Before implementation potential ADEs occurredat a rate of 22 per 100 orders MPEs at a rate of 301 per100 orders and RVs at a rate of 68 per 100 orders Afterimplementation the rate of potential ADEs was reducedto 13 per 100 orders MPEs to 02 per 100 orders and RVsto 01 per 100 orders The overall error reduction was959 Potential ADEs were reduced by 409 and MPEsand RVs were reduced by 994 and 979 respectively
Conclusions The implementation of CPOE resultedin almost a complete elimination of MPEs and RVs and asignificant but less dramatic effect on potential ADEsPediatrics 200411359ndash63 medication errors critical carepediatrics clinical decision support systems computer-assisted drug therapy
ABBREVIATIONS ADE adverse drug event CPOE computer-ized physician order entry IOM Institute of Medicine PCCUpediatric critical care unit MPE medication prescribing error RVrules violation
Medication errors are a major concern ofhealth care professionals and medical insti-tutions especially errors involving chil-
dren Children have significant differences in both
pharmacokinetics and pharmacodynamics comparedwith adults that can make this population more sus-ceptible to medication errors and related injuriesSeveral factors make children in a critical care settingespecially vulnerable to medication errors and ad-verse events These factors include weight-baseddosing significant weight changes over a relativelyshort period of time lack of commercially availableproducts leading to dilution of stock medicationsand the decreased communication ability of criticallyill patients12 These problems are magnified by theuse of vasoactive infusions and the emergent use ofdrugs during cardiopulmonary resuscitation Eachpatient requires complex calculations to determinethe concentration of many drugs including vasoac-tive agents to be mixed by the pharmacy and the rateof delivery to achieve a desired dose The process ofprescribing medications for critically ill children iscomplex and lacks standardization which can in-crease the risk of medication errors and adverseevents
The significance of medication errors in pediatricinpatients has only recently been described Kaushalet al1 studied 1120 pediatric patients who were ad-mitted to 2 hospitals during a 6-week period Theauthors analyzed 10 000 medication orders andfound 616 medication errors resulting in an errorrate of 57 This error rate is consistent with the ratereported in adults3 In addition this study evaluatedthe frequency at which medication errors occurred atdifferent points in the medication system1 Seventy-nine percent of potential adverse drug events (ADEs)occurred at the time of physician ordering whereas asmaller percentage occurred at the point of transcrip-tion or administration
Recent trends toward cost containment standard-ization and accessibility of common medicationshave led to the implementation of various entities ofautomation and technology Computerized physi-cian order entry (CPOE) has been identified by theInstitute of Medicine (IOM) Leapfrog Group Insti-tute for Safe Medication Practices American MedicalAssociation American Academy of Pediatrics andothers as a tool that may prevent errors that occurduring the medication ordering process14ndash10 TheLeapfrog Group has also identified CPOE as 1 of 3initial hospital safety standards and has describedseveral benefits of CPOE that may result in improvedquality of care and reduced health care costs5 Thesebenefits may include enhanced communication be-
From the Department of Pharmaceutical Services Vanderbilt ChildrenrsquosHospital Nashville Tennessee DaggerDivision of Pediatric Critical Care andAnesthesia Department of Pediatrics Vanderbilt Childrenrsquos HospitalNashville Tennessee and sectDepartment of Biomedical Informatics Vander-bilt University Nashville TennesseeReceived for publication Oct 28 2002 accepted Apr 8 2003Reprint requests to (NRP) Department of Pediatrics Anesthesiology andBiomedical Informatics Division of Pediatric Critical Care and AnesthesiaVanderbilt Childrenrsquos Hospital 714 Medical Arts Bldg Nashville TN37212-1565 E-mail nealpatelvanderbilteduPEDIATRICS (ISSN 0031 4005) Copyright copy 2004 by the American Acad-emy of Pediatrics
PEDIATRICS Vol 113 No 1 January 2004 59 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 308 of 417
tween health care professionals through the elimina-tion of illegible or incomplete orders and the in-creased efficiency of order processing throughinstantaneous transmission of orders to other hospi-tal systems Computerized decision support associ-ated with CPOE systems such as displaying age-specific dosing regimens to the user checking fordoses above or below the usual range providingwarnings if current laboratory values indicate thatthe drug or regimen would be inappropriate for aparticular patient and screening for allergies anddrugndashdrug interactions may also improve the order-ing process
The role of CPOE in preventing medication errorsand ADEs has been noted in the adult literatureBates et al6 evaluated the medication error rates of 3medical units before and after CPOE during a 4-yearperiod The authors concluded that CPOE substan-tially decreased the rate of medication errors withadditional reductions observed after the addition ofdecision support and other features Another studyevaluated the use of CPOE in an adult populationand found that serious medication errors were re-duced by 557
The development of CPOE systems that are adapt-able to pediatric critical care environments has beenproblematic Developing systems that provideweight-based dosing as well as age-specific algo-rithms is difficult and applicable only to a smallproportion of the overall health care market Thereare limited data on the impact of CPOE on medica-tion errors in pediatric patients Most literature hasevaluated medication errors and ADEs that haveresulted in patient injury regardless of the point inthe system at which the error occurred We evaluatedmedication errors that occurred specifically at thetime of prescribing rather than administration ordispensing The objective of this study was to deter-mine the impact of CPOE on the frequency of med-ication errors at the point of physician ordering in apediatric critical care unit (PCCU)
METHODS
Study SettingThe study was conducted in a 20-bed multidisciplinary PCCU
at an academic institution located in a major metropolitan areaThe institution provides services to a diverse socioeconomic pa-tient population The PCCU has an average daily census of 163patients and the average length of stay is 41 days The hospitalcares for both adult and pediatric patients but pediatric servicesare both geographically and administratively distinct
Patient PopulationThis study included all patients who were admitted to the
PCCU during the designated study periods and encompassedboth medical and surgical patients Disease states represented inthis patient population included postoperative congenital heartdefect repair metabolic disorders trauma respiratory diseasesbone marrow and solid organ transplantation and other child-hood illnesses
Study DesignIn this prospective cohort study a comparison was made be-
tween the occurrences of errors in the medication ordering processbefore and after implementation of a CPOE system in the PCCUApproval from the Institutional Review Board at Vanderbilt Uni-versity Medical Center was obtained Data were collected before
CPOE implementation for a 2-month period from October 4 2001to December 4 2001 There was a 1-month period when no datawere collected to allow for CPOE implementation and training ofall attendings fellows residents and staff Post-CPOE data col-lection then occurred for a 2-month period from January 4 2002 toMarch 4 2002
Computer SystemsWizOrder is a CPOE system developed in 1994 by the faculty in
the division of Biomedical Informatics at Vanderbilt University11
WizOrder is the precursor to the commercially available HorizonExpert Order system (McKesson Atlanta GA) and currently in-terfaces with the Pyxis Medstation 2000 system (Pyxis Corp SanDiego CA) and the pharmacy computer system McKesson SeriesWizOrder provides clinicians with several types of decision sup-port including drug allergy alerts dose checking drug interactionalerts and US Food and Drug Administration alerts In additionWizOrder includes clinical pathways using 900 preprogrammedindividual order sets and links to drug monographs evidence-based literature sites and the National Library of MedicinePubMed site This system also interfaces to a computerized ar-chive of medical records that serves as a clinical data repository sothat order-related and laboratory-related alerts can be generatedfor each individual patient The depth of clinical decision supportcan be adjusted on the basis of predetermined criteria such as ageor patient location Recommendations for medication dosage ad-justment for impaired renal function for example varies betweenadult and pediatric patients Adjustments are recommended foradult patients on the basis of estimates of creatinine clearanceusing standard formulas Unfortunately these formulas cannotreliably be used in pediatric patients For these patients clinicaldecision support provides only recent laboratory values and analert to take renal function into account during the ordering pro-cess Another aspect of clinical decision support that has beenimplemented is information on varying medication dosage byclinical indication The system calculates the dose once the clini-cian selects 1 of the recommendations WizOrder had been imple-mented on all adult units and the general medicalsurgical pedi-atric wards before its implementation in the PCCU
Review ProcessAll medication orders were included in this analysis except for
the following fluids dialysate total parental nutrition (TPN)lipids and chemotherapeutic agents TPN and lipids had not beenadded to the CPOE system at the time of the study Fluidsdialysate and chemotherapy orders were entered in the CPOEsystem but will be evaluated at a later date A designated clinicalpharmacist reviewed all eligible orders Errors were entered into adatabase that included information such as patient name ageweight drug presence of error dose interval and route Errorswere identified and further classified into categories on the basisof the definitions and classifications listed in Table 1 and reviewedfor accuracy and relevance by a second clinical pharmacist Aphysician reviewer independently evaluated all original medica-tion orders for 10 of randomly selected patients in both thepre-CPOE and post-CPOE groups to determine level of agreementwith clinical pharmacists
Main Outcome MeasuresThis study focused on errors that occurred during the medica-
tion ordering process An error was determined to have occurredwhen an order was found to be incomplete incorrect or inappro-priate at the time of physician ordering Errors were classified aspotential ADEs medication prescribing errors (MPEs) or ruleviolations (RVs) A potential ADE was defined as any error that ifallowed to reach the patient could result in patient injury Poten-tial ADEs are those errors in which the ordering physician pro-vided incorrect or inappropriate information They also includeinstances in which the ordering physician failed to account forpatient-specific information (eg allergy) MPEs were defined aserrors in which inadequate information was provided or furtherinterpretation (eg illegibility) was required for the order to beprocessed RVs were defined as errors that were not compliantwith standard hospital policies (eg abbreviations)
60 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 309 of 417
Statistical AnalysisA 2 analysis and Fisher exact test for smaller sample sizes were
used for pre-CPOE and post-CPOE data comparison The STATAstatistical program was used for analysis (Stata Corp CollegeStation TX) The interrater reliability was calculated using thepercentage of agreement and the statistic The statistic forinterrater reliability between the physician reviewer and clinicalpharmacist was 096 This corresponds to excellent reliability
RESULTSA total of 13 828 medication orders involving 514
patients were analyzed throughout the study periodA total of 268 patients were evaluated during thepre-CPOE study period and 246 patients were eval-uated during the post-CPOE period The mean age ofpatients in the pre-CPOE group was 65 120 yearsand in the post-CPOE group was 54 103 yearsThis was not a significant difference between the 2groups Overall length of stay in the PCCU for bothgroups was also not significantly different The meanlength of stay was 42 107 days for the pre-CPOEgroup and 41 66 days for the post-CPOE group
During pre-CPOE 6803 orders were analyzed Atotal of 2662 (391 per 100 orders) errors and RVswere identified and are described in further detail inTable 2 After additional classification 22 per 100orders were identified as potential ADEs 301 per100 orders were identified as MPEs and 68 per 100orders were identified as RVs The most commonerrors in the last 2 categories were missing informa-tion and abbreviations
During post-CPOE 7025 orders were analyzedand a total of 110 (16 per 100 orders) overall errorsand RVs were identified (Table 2) Of those 13 per100 orders were categorized as potential ADEs Therate for MPEs and RVs was only 02 per 100 ordersand 01 per 100 orders respectively CPOE signifi-cantly reduced the rate of MPEs and RVs (P 001Table 2) Because of almost a complete elimination ofMPEs and RVs potential ADEs became the mostcommon level of error in the post-CPOE periodErrors involving medication dosage and interval
TABLE 1 Error Classifications and Definitions
Medication error Any order that was incomplete incorrect or inappropriate at the time ofphysician ordering
Potential ADEs Any error that if allowed to reach the patient could result in patient injuryDuplicate therapy Same drug prescribed twice or 2 or more drugs from the same class with
no evidence-based medicine to prove benefit from bothInappropriate dose12 Based on a 10 difference in published dosing guidelines or our PCCU
standards of practiceInappropriate interval12 Based on differences found from published dosing guidelinesInappropriate route12 Drug not available or not recommended to be given in the route orderedWrong drug Incorrect drug orderedWrong units Units are not correct for drug diagnosis or dose used (eg unitskgmin
vs mcgkgmin)Drug interaction Documented drug interaction between 2 medications that deems drug
ineffective or contraindicated (eg beta-blocker with beta-agonist)Allergy Documented allergy to drug ordered
MPEMissing information Missing route interval concentration rate or dose that results in an
incomplete orderNo weight Patientrsquos weight not availableIllegible Unable to read required further interpretation
RVsAbbreviation Shortened or symbolized representation of a drug name (eg dopa epi
MSO4) Does not include CaCl2 or NaHCO3Trailing zeros Zeros to the right of the decimal point (eg 10 mg)
TABLE 2 Overall Medication Error Analysis Before and After CPOE
Pre-CPOE (n 6803) Post-CPOE (n 7025) P Value
TotalNumber
Number Per100 Orders
TotalNumber
Number Per100 Orders
Potential ADEs 147 22 88 13 0001Duplicate therapy 4 006 0 0 001Inappropriate dose 53 078 59 084 69Inappropriate interval 24 035 19 027 39Inappropriate route 6 009 0 0 01Wrong drug 6 009 1 001 07Allergy 1 001 0 0 49Drug interaction 1 001 0 0 49Wrong units 52 076 9 013 001
MPEs 2049 301 12 02 001Weight not available 22 032 0 0 001Missing Information 1979 2909 12 017 001Illegible 48 071 0 0 001
RVs 466 68 10 01 001Trailing zeros 55 081 10 014 001Abbreviation 411 604 0 0 001
ARTICLES 61 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 310 of 417
were the most prevalent potential ADEs The reduc-tion in error rates for dosing (P 69) and interval(P 39) after CPOE implementation was not signif-icant
Overall CPOE resulted in a 959 (P 001) re-duction in all types of errors associated with medi-cation ordering Figure 1 shows a significant reduc-tion in MPEs (994 P 001) and RVs (979 P 001) A smaller but still significant reduction wasfound with potential ADEs (409 P 001) afterCPOE implementation
DISCUSSIONDuring the past decade the prevention of medica-
tion errors and ADEs has become a major focus ofmedical institutions Public knowledge regarding thefrequency and seriousness of medication errors andthe steps that patients can take to prevent suchevents from happening has increased accordingly Inaddition improving patient safety through reduc-tion of medication errors and ADEs has received theattention of government officials at both state andnational levels
In 1999 the impact of medical errors was dramat-ically publicized by an IOM report which estimatedthat between 44 000 and 98 000 people die each yearpartly as a result of medical errors8 This report laidout a comprehensive strategy by which governmenthealth care providers and consumers could reducemedication errors Another report of the IOM re-leased in March 2001 Crossing the Quality Chasm ANew Health System for the 21st Century focused onimproving and redesigning the health care system13
Prepared by the IOMrsquos Committee on the Quality ofHealth Care in America this report recommends theuse of automated systems for order processing andthe elimination of handwritten clinical informationby the end of this decade
ADEs are associated with significant morbidityand mortality and are often preventable Classen etal14 reported a 2-fold increase in death associated
with ADEs as well as prolonged hospitalization Inanother study Bates et al15 found that 28 of ADEswere preventable and that 56 of those occurred atthe point of medication prescribing The overall costof ADEs has been estimated to exceed $2000 perevent with preventable ADEs associated with anannual national cost of $2 billion1416 The Ameri-can Academy of Pediatrics has also stated that med-ication errors in particular are associated with signif-icant morbidity and mortality and increased healthcare costs by an estimated $1900 per patient917 Thisfigure does not reflect the additional emotional costsincurred by patients and their families
Most guidelines that address methods to reducemedication errors recommend that institutions im-plement CPOE systems However there are limiteddata evaluating the impact of CPOE on medicationerrors in the pediatric population In this study weevaluated errors that occur only during the medica-tion ordering process In addition the separation ofpotential ADEs MPEs and RVs provides for a de-tailed analysis of the specific impact of CPOE ondifferent types of errors
In this study CPOE significantly reduced all cate-gories of errors MPEs and RVs were virtually elim-inated and potential ADEs were reduced by 409In addition during the study there were no reportsof errors caused by the CPOE system including noreports of orders being entered on the wrong patientMPEs and RVs often lead to confusion and lack ofefficiency as a result of incorrect or missing informa-tion that requires interpretation and clarification bypharmacy and nursing personnel Our study dem-onstrated that a major benefit of CPOE is the en-hancement of communication between health careprofessionals that subsequently decreases the possi-ble misinterpretation of medication orders
Potential ADEs were significantly reduced (P 001) but not nearly to the extent of MPEs and RVsPotential ADEs were identified as errors in whichincorrect or inappropriate information was providedor patient-specific factors were not taken into ac-count and potential injury could occur to the patientif the medication were received as ordered Overallmost types of potential ADEs including duplicatetherapy wrong drug wrong units allergy and druginteractions were eliminated or significantly re-duced This error reduction when extrapolated an-nually would equate to a decrease of approximately300 instances per year in which a potential ADE wasprevented However errors involving dose and in-terval showed no significant difference between pre-CPOE and post-CPOE This may be explained by thelack of decision support on initial CPOE implemen-tation that would assist the prescriber in choosing anage- and indication-specific dose and interval for thepatient This is an area in which additional enhance-ments to CPOE systems are needed Targeted deci-sion support associated with CPOE was shown to beeffective in adult inpatients with renal insufficiencyby Chertow et al18 Decision support tools focused onpediatric issues such as weight-based calculations forinfusions and age-specific dosing guidelines may re-sult in additional reductions in these types of errors
Fig 1 Comparison of rates of potential ADEs MPEs and RV isbetween pre-CPOE and post-CPOE phases All categories of errorsdecreased significantly (P 001) after CPOE implementation Theoverall reduction was 409 (P 001) for potential ADEs 994(P 001) for MPEs and 979 (P 001) for RVs
62 CPOE AND MEDICATION ERRORS IN A PCCU by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 311 of 417
Our study evaluated medication errors that occurat the time of physician ordering The prevention ofactual ADEs involves multiple facets of the medica-tion delivery process Kaushal et al1 showed that thefrequency of preventable ADEs is very low (005 per100 orders) Despite the significant number of errorsin the ordering phase of medication delivery ourstudy was not appropriately powered to evaluate theimpact of CPOE on overall preventable ADEs Anappropriately powered study would require a sam-ple size that is 20 times the number evaluated in ourstudy Another limitation of our study is that we didnot investigate how these errors were detected byother components of the medication use system suchas verification of the order by a pediatric pharmacistor review of the order by nursing staff before admin-istration
Medication error rates have not been well studiedin pediatrics The rate reported in this study mayseem elevated because of our conservative definitionof errors in the medication ordering process Limiteddata are available on error rates associated with med-ication ordering in the pediatric critical care settingWith this study we have established an error rate fora multidisciplinary PCCU that serves a patient pop-ulation that is broad in both age and disease state
Although CPOE offers significant advantages inalmost eliminating MPEs and RVs CPOE is not thesole solution for preventing potential ADEs The ad-dition of decision support has previously beenshown to increase the effectiveness of CPOE in pre-venting medication errors in adult patients618 De-veloping features that accommodate the wide rangeof ages and weights found in pediatric patients iscomplex Incorporating pediatric-specific dosingguidelines and calculators for continuous infusionsmay prove to reduce the incidence of these types oferrors Additional evaluation is needed to determinethe benefits of enhancing CPOE with additional de-cision support designed for the pediatric populationSpecifically the issues of gestational age postnatalage and rapid weight changes in neonatal patientsare currently being incorporated into WizOrder inpreparation for implementation in our neonatal in-tensive care unit Unfortunately pediatrics is a smallportion of the overall CPOE market and limited fi-nancial rewards may prevent commercial vendorsfrom committing the necessary resources for devel-opment of these tools
CONCLUSIONSIn conclusion CPOE significantly reduced and al-
most completely eliminated MPEs and RVs whilestill demonstrating a significant reduction in the fre-quency of potential ADEs CPOE offers significant
benefits including ensuring legible and completephysician orders Incorporation of pediatric-specificdecision support tools into CPOE systems may resultin even further reductions of potential ADEs leadingto improved patient safety Additional evaluation ofthese safety features is needed and will be the focusof future studies
ACKNOWLEDGMENTSWe do not have any financial ties or obligations to the com-
mercialization process of WizOrder This study was not supportedin any manner by McKesson (Atlanta GA)
We acknowledge Fred R Hargrove RPh for valuable technicalassistance with the CPOE WizOrder system and data retrieval
REFERENCES1 Kaushal R Bates DW Landrigan C et al Medication errors and adverse
drug events in pediatric inpatients JAMA 20012852114ndash21202 Kaushal R Barker KN Bates DW How can information technology
improve patient safety and reduce medication error in childrenrsquos healthcare Arch Pediatr Adolesc Med 20011551002ndash1007
3 Bates DW Boyle DL Vander Vliet MB Schneider J Leape L Relation-ship between medication errors and adverse drug events J Gen InternMed 199510199ndash205
4 Leape LL Bates DW Cullen DJ et al Systems analysis of adverse drugevents ADE Prevention Study Group JAMA 199527435ndash43
5 The Leapfrog Group Computer physician order entry (CPOE) factsheet Available at wwwleapfroggrouporg Accessed June 11 2002
6 Bates DW Teich JM Lee J et al The impact of computerized physicianorder entry on medication error prevention J Am Med Inform Assoc19996313ndash321
7 Bates DW Leape LL Cullen DJ et al Effect of computerized physicianorder entry and a team intervention on prevention of serious medica-tion errors JAMA 19982801311ndash1316
8 The Institute of Medicine (US) To Err is Human Building a Safer HealthSystem Washington DC National Academy Press 1999
9 American Academy of Pediatrics Committee on Drugs and Committeeon Hospital Care Prevention of medication errors in the pediatricinpatient setting Pediatrics 1998102428ndash430
10 Teich JM Merchia PR Schmiz JL Kuperman GJ Spurr CD Bates DWEffects of computerized physician order entry on prescribing practicesArch Intern Med 20001602741ndash2747
11 Geissbuhler A Miller RA A new approach to the implementation ofdirect care-provider order entry Proc AMIA Annu Fall Symp 1996689ndash693
12 Taketomo CK Hodding JH Kraus DM Pediatric Dosage Handbook 8thed Hudson OH Lexi-Comp Inc 2001
13 The Institute of Medicine (US) Crossing the Quality of Chasm A NewHealth System for the 21st Century Washington DC National AcademyPress 2001
14 Classen DC Pestotnik SL Evans RS Lloyd JF Burke JP Adverse drugevents in hospitalized patients excess length of stay extra costs andattributable mortality JAMA 1997277301ndash306
15 Bates DW Cullen J Laird N et al Incidence of adverse drug events andpotential adverse drug events implications for prevention ADE Pre-vention Study Group JAMA 199527429ndash34
16 Bates DW Spell N Cullen DJ et al The costs of adverse drug events inhospitalized patients Adverse Drug Events Prevention Group JAMA1997277307ndash311
17 Physician Insurers Association of America Medication Error StudyWashington DC Physician Insurers Association of America 1993
18 Chertow GM Lee J Kuperman GJ Burdick E Horsky J Seger DL LeeR Mekala A Song J Komaroff AL Bates DW Guided medicationdosing for inpatients with renal insufficiency JAMA 20012862839ndash2844
ARTICLES 63 by guest on April 19 2011 wwwpediatricsorgDownloaded from
11202012 Page 312 of 417
200411359-63 PediatricsPatel
Amy L Potts Frederick E Barr David F Gregory Lorianne Wright and Neal R Critical Care Unit
Computerized Physician Order Entry and Medication Errors in a Pediatric
amp ServicesUpdated Information
httpwwwpediatricsorgcgicontentfull113159including high-resolution figures can be found at
References
httpwwwpediatricsorgcgicontentfull113159BIBLat This article cites 12 articles 11 of which you can access for free
Citationshttpwwwpediatricsorgcgicontentfull113159otherarticlesThis article has been cited by 58 HighWire-hosted articles
Subspecialty Collections
httpwwwpediatricsorgcgicollectionoffice_practice Office Practice
following collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwpediatricsorgmiscPermissionsshtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
Reprints httpwwwpediatricsorgmiscreprintsshtml
Information about ordering reprints can be found online
by guest on April 19 2011 wwwpediatricsorgDownloaded from 11202012 Page 313 of 417
Pediatric Critical Care
Impact of a pediatric clinical pharmacist in the pediatric intensivecare unit
Marianne I Krupicka PharmD Susan L Bratton MD MPH Karen Sonnenthal MS FNPBrahm Goldstein MD FAAP FCCM
I n recent years changes in healthcare financing have necessitatedthat health care providers delin-eate and justify both a medical and
an economic basis for their involvementin patient care Numerous studies haveevaluated the role of the clinical pharma-cist in adult intensive care units (1ndash7)Few have addressed the role of the clini-cal pharmacist in the pediatric intensivecare unit (ICU) (8) Our intent was tostudy the medical and economic impactof a clinical pediatric pharmacist in ourpediatric ICU
The goals of the study were to deter-mine the type and quantity of patient careinterventions recommended by a clinicalpharmacist and to specifically examine
cost savings (or loss) that resulted fromclinical pharmacist recommendations inthe pediatric ICU We hypothesized thatthe pediatric ICU clinical pharmacistwould have a positive impact on patientcare and medical staff education andwould prove to be cost effective
METHODS
Doernbecher Childrenrsquos Hospital is a 124-bed comprehensive pediatric hospital includ-ing pediatric intensive care general medicalsurgery hematologyoncology and neonatalcare units Pharmacy services are provided 24hrs a day 7 days a week from a centralizedpharmacy Clinical pharmacy services are pro-vided directly on the units 5 days a week by apediatric clinical pharmacist who reviewsmedication records for all patients Weekendservices are provided in a centralized locationAt the time of this study the pediatric ICUpharmacist (MIK) had worked at the institu-tion as the pediatric clinical pharmacist forapproximately 4 yrs
The study took place in the 10-bed medi-calsurgical pediatric ICU at DoernbecherChildrenrsquos Hospital OR Health Sciences Uni-
versity The study was approved by the Insti-tutional Review Board The study was con-ducted from November 19 1996 to May 61997 and included 24 consecutive 4-dayweeks (79 days) excluding days that the pedi-atric clinical pharmacist was off duty
The following data were recorded for allpediatric ICU patients enrolled in the studysubject number age gender daily PediatricRisk of Mortality Index (PRISM) score (as ameasure of severity of illness) (9) and totalnumber and specific type of medications theyreceived During the study the pediatric clin-ical pharmacist (MIK) documented all inter-ventions that occurred during the shift (700am to 330 pm) attributable to recommenda-tions made on rounds or from a private dis-cussion with the physicians The clinical phar-macist attended morning rounds with thepediatric ICU service approximately two timesper week
Drug acquisition costs were used to calcu-late drug cost savings Drug acquisition costswere multiplied by 24 days of therapy (theaverage length of stay for pediatric ICU pa-tients) to obtain the total cost savings fordiscontinued drugs if treatment began on day1 of the patientrsquos pediatric ICU stay If the
From the Department of Pharmacy (MIK) and theDivision of Pediatric Critical Care (SLB KS BG) De-partment of Pediatrics Doernbecher Childrenrsquos Hospi-tal amp Oregon Health Sciences University Portland OR
Supported in part by a grant from the AmericanSociety of Health-System Pharmacists (AHSP) Re-search and Education Foundation Bethesda MD
Copyright copy 2002 by Lippincott Williams amp Wilkins
Objective To study the impact of a clinical pharmacist in apediatric intensive care unit The goals of the study were todetermine the type and quantity of patient care interventionsrecommended by a clinical pharmacist and to specifically exam-ine cost savings (or loss) that resulted from clinical pharmacistrecommendations
Design A prospective case seriesSetting Ten-bed pediatric intensive care unit in a university-
affiliated childrenrsquos hospitalPatients All patients admitted to the pediatric intensive care
unit during the study periodInterventions NoneMeasurements and Main Results During the 24-wk study
period the pediatric clinical pharmacist documented all interven-tions that occurred during her shift She rounded with the pedi-atric intensive care unit team approximately two times a weekand reviewed medication lists daily Drug acquisition costs wereused to calculate drug cost savings Demographic information
was collected on all the patients in the pediatric intensive careunit during the study period
There were 35 recommendations per 100 patient days Themost common interventions were dosage changes (28) druginformation (26) and miscellaneous information (22) Theaverage time spent per day by the clinical pharmacist in thepediatric intensive care unit was 073 hrs or 002 full-time equiv-alent The total cost direct savings for the study period was$1977 Extrapolated to direct cost savings per year the totalamount saved was $9135year or 015 full-time equivalent Indi-rect savings from educational activities avoidance of medicationerrors and optimization of medical therapies represent an addi-tional nonquantifiable amount
Conclusion We conclude that a clinical pharmacist is animportant and cost-effective member of the pediatric intensivecare unit team (Crit Care Med 2002 30919ndash921)
KEY WORDS pediatric clinical pharmacist cost savings pediat-ric intensive care
919Crit Care Med 2002 Vol 30 No 4
11202012 Page 314 of 417
patient had already stayed in the pediatric ICU24 days the cost was calculated for 1 day Ifthe drug was changed to a more or less expen-sive counterpart the difference in drug costsbefore and after the change was determined Ifthe more expensive medication was therapeu-tically superior then the costs was not addedinto the calculation Labor supplies or anyother indirect costs were not included
The database was managed by usingGraphPad Prism PPC (GraphPad SoftwareSan Diego CA) Descriptive statistics for theanalysis including means standard deviationsmedians and 25th and 75th quartiles werecalculated Subjects who received at least onerecommendation from the pharmacist werecompared with those who did not by using theMann-Whitney U test for continuous data andthe chi-square test for categorical data Wealso examined correlations between patient di-agnosis severity of illness (PRISM) and totaland specific pharmaceutical interventionsSignificance was defined as p 05
RESULTS
Two hundred and one children wereadmitted to the pediatric ICU during thestudy days Twelve were readmitted to thepediatric ICU during the study and onechild was admitted three times duringthe study days for a total of 215 patientadmissions to the pediatric ICU Childrenwho received recommendations duringan admission had significantly longer pe-diatric ICU stays as well as total hospitalstay (Table 1) They also tended to bemore severely ill with higher medianPRISM scores although this was not sta-tistically significant The longer length ofstay and PRISM scores suggest that thechildren with recommendations weremore severely ill compared with the chil-dren who did not have pharmacy inter-ventions
As expected the pharmacist spent sig-nificantly more time in both rounds andin total time devoted to a patient in chil-dren who received a recommendationcompared with those who did not have arecommendation from the pharmacistAmong children who received recom-mendations from the pharmacist themedian number of recommendations was1 (25th and 75th quartiles 1 and2) Thegroups did not differ significantly by ageor gender
There were 493 total patient daysstudied The pharmacist made 172 rec-ommendations for 77 patients either dur-ing rounds or when reviewing their med-ication lists during the study periodThere were 35 recommendations per 100patient days We found the most commoninterventions were dosage changes druginformation and miscellaneous informa-tion (Table 2)
The average time spent per day by theclinical pharmacist in the pediatric ICUwas 073 hrs The total cost savings forthe study period was $1977 Extrapolatedto cost savings per year the total amountsaved was $9135year if the pharmacistwas employed full-time
DISCUSSION
This study documents a major educa-tional role for the clinical pharmacist inthe pediatric ICU and demonstrates aneconomic savings from decreases in drugcost Critically ill patients frequently re-quire multiple drug therapy and mayhave multiple-system organ dysfunctionthat alters drug pharmacokinetics andpharmacodynamics In addition to thesechallenges patients in the pediatric ICUhave a wide range of age and weightadding to the complexity of pharmacy
interventions compared with adult ICUpatients
Our study demonstrated that changesin drug dosing were the most commoninterventions that the clinical pharmacistmade in our pediatric ICU The potentialmedical benefit and economic savingsfrom avoidance of medication error at-tributable to over- or underdosing al-though not possible to accurately calcu-late are likely substantial The presenceof a pediatric clinical pharmacist in thepediatric ICU also improved staff educa-tion regarding pharmacologic therapyTwo of the most common recommenda-tions involved drug information and gen-eral information to the physicians andnurses Other reports on activities of aclinical pharmacist in adult ICUs alsoconfirm the importance of staff education(10ndash11)
We found that even in a relativelysmall pediatric ICU (average census dur-ing the study 49 patients) interventionsby the clinical pharmacist resulted insubstantial drug costs savings and pro-vided the medical staff with importantdrug education The average time spentper day was 1 hr allowing the pharma-cist time to attend to other duties
The cost savings that we estimated areconservative because discontinued medi-cation costs were calculated on 24-hrsupply of drug labor materials andother cost savings were not includedFurthermore improvements in dosingefficiency were not included the pharma-cist did not round daily with the service(although the pharmacist did review pa-tient medications daily) and the cost oferrors that were avoided could not beaccurately estimated Even so our resultssuggest that the direct cost savings fromthe pediatric ICU pharmacist activitiesmay account for up to 015 full-timeequivalent of the average starting salaryfor a hospital-based pharmacist in 1997($62400) (12) This direct amount morethan justifies the average time spent inthe pediatric ICU of 073 hrsday or 002full-time equivalent In addition this cal-culation does not take into account thepotential indirect savingsbenefits fromthe avoidance of medical errors benefitsfrom ongoing education and optimiza-tion of patient medical therapies Avoid-ance of medical errors recently has re-ceived intense scrutiny by both thefederal government and general public(13ndash15) Furthermore the Society ofCritical Care Medicine has endorsed the
Table 1 Selected demographic features of the study population
Admissions to the PICUWith Rx
Recommendations(n 77)
Admissions to the PICUWithout Rx
Recommendations(n 138)
Age yrs median (25th 75th quartiles) 50 (01 105) 35 (08 107)Male n () 44 (57) 68 (49)PRISM Score median (25th 75th quartiles) 4 (0 5) 25 (0 4)PICU days median (25th 75th quartiles)a 3 (1 6) 1 (1 3)Total hospital days median (25th 75th
quartiles)a7 (3 13) 5 (2 11)
Pharmacist time in rounds mins median(25th 75th quartiles)a
2 (0 5) 0 (0 3)
Pharmacist total time in patient care minsmedian (25th 75th quartiles)a
7 (5 13) 35 (2 6)
PICU pediatric intensive care unit PRISM Pediatric Risk of Mortality Indexap 05
920 Crit Care Med 2002 Vol 30 No 4
11202012 Page 315 of 417
need for subspecialty pharmacy expertisein the care of critically ill patients (16)
Our findings are similar to reports ofadult ICUs (11 12) and general medicalwards (17ndash19) that have documented theimportant educational role of the phar-macist in addition to realized cost sav-ings Montazeri and Cook (10) reportedthat 575 interventions occurred over a3-month period in a 15-bed medical-surgical ICU resulting in a net savings of$1001060 (Canadian) Furthermore thepharmacist played an important educa-tional function by providing drug infor-mation to physicians and nurses Miya-gawa and Rivera (11) studied the impactof a clinical pharmacist in a 14-bed sur-gical ICU Over a 13-wk period a total of322 interventions to improve drug ther-apy were made resulting in an annualcost savings of $72000 (11) Anotherstudy found that 724 medication errorswere averted over a 4-yr period in theirICUs because of pharmacist intervention(17) A more recent prospective epide-miologic study in two academic univer-sity hospitals found that although thepreventable adverse drug event rate inchildren was similar to that of a previousadult hospital study the potential adversedrug event rate was three-fold higher(15) Physician reviewers judged thatward-based clinical pharmacists couldhave prevented 94 of potential adversedrug events (15)
The activities of critical care pharma-cists are expanding and evolving (6 20)Critical care pharmacists in many insti-tutions no longer primarily function inroles of drug preparation and dispensingThe new focuses are on monitoring drugdosages and interactions making recom-mendations to the physician staff regard-ing changes in medication therapy anddeveloping pharmacotherapeutic plans tooptimize drug therapy for ICU patients
and avoid adverse medication interac-tions and errors (15)
There are a number of limitations tothis study First although it was prospec-tively designed it was not a controlledtrial so there is no control populationThus benefits need be assumed ratherthan proven as causal We have takencare to provide conservative estimateswhen required Second the patientsrsquo clin-ical course was not factored into the po-tential savings or expenditures as a resultof the pharmacistrsquos interventions Thirdwe have no direct evidence of positive orlasting impact on medical staff educationonly intuitive assumptions based onchanges made in care Fourth it is pos-sible that bias was introduced as a resultof the clinical pharmacist being one ofthe authors (MIK) although this seemsunlikely
Even taking into account these realand potential limitations we suggest thatthe results from this study are valid takenwithin the context of the study designOur results add to the growing body ofevidence that supports the use safetyand cost-effectiveness of a clinical ICUpharmacist It is clear that additional eco-nomically sophisticated studies are re-quired to more completely evaluate therole of the clinical pharmacist in the ICU
REFERENCES
1 ASHP supplemental standard and learningobjectives for residency training in pediatricpharmacy practice In Practice Standards ofASHP 1995ndash96 Hickes WE (Ed) BethesdaMD American Society of Hospital Pharma-cists 1995
2 Hepler CD Strand LM Opportunities andresponsibilities in pharmaceutical care Am JHosp Pharm 1990 47533ndash543
3 American Society of Hospital PharmacistsASHP statement on the pharmacistrsquos clinicalrole in the organized health care settingAm J Hosp Pharm 1989 462345ndash2346
4 Folli HI Poole RL Benitx WE et al Medica-tion error prevention by clinical pharmacistsin two childrenrsquos hospitals Am J HospPharm 1993 50305ndash314
5 American Society of Hospital PharmacistsASHP guidelines for providing pediatricpharmaceutical services in organized healthcare systems Am J Hosp Pharm 1994 511690ndash1692
6 Lal LS Anassi EO McCants E Documenta-tion of the first steps of pediatric pharmaceu-tical care in a country hospital Hosp Pharm1995 301107ndash1108
7 Hutchinson RA Schumock GT Need to de-velop a legal and ethical base for pharmaceu-tical care Ann Pharmacother 1994 28954ndash956
8 Flack KA Darsey EH Naughton MJ Phar-macy interventions in a multidisciplinary pe-diatric intensive care unit J Pediatr PharmPract 1997 3162ndash167
9 Pollack M Ruttimann UK Getson PR Pre-dictive risk of mortality (PRISM) score CritCare Med 1988 161110ndash1116
10 Montazeri M Cook DJ Impact of a clinicalpharmacist in a multidisciplinary intensivecare unit Crit Care Med 1994 221044ndash1048
11 Miyagawa CI Rivera JO Effect of pharmacistinterventions on drug therapy costs in a sur-gical intensive-care unit Am J Hosp Pharm1986 433008ndash3013
12 Pharmacy Salary Review Available at http20815543155candidatesarticleaspsessionIDYJKSHERDamparticle_id32 Accessed May7 2001
13 For Want of Soap and Water New YorkTimes March 27 2000
14 Institute of Medicine To Err is HumanBuilding a Safer Health System Kohn LTCorrigan JM Donaldson MS (Eds) Washing-ton DC National Academy Press 2000
15 Kaushal R Bates DW Landrigan C et alMedication errors and adverse drug events inpediatric inpatients JAMA 2001 2852114ndash2120
16 Rudis MI Brandl KM for the Society ofCritical Care Medicine and AmericanCollege of Clinical Pharmacy Task Forceon Critical Care Pharmacy ServicesPosition paper on critical care pharmacyservices Crit Care Med 2000 283746 ndash3750
17 Kilroy RA Iafrate RP Provision of pharma-ceutical care in the intensive care unit CritCare Nurs Clin N Am 1993 5221ndash225
18 Haig GM Kiser LA Effect of pharmacist par-ticipation on a medical team on costscharges and length of stay Am J HospPharm 1991 481457ndash1462
19 Bjornson DC Hiner WO Potyk RP et alEffect of pharmacists on health care out-comes in hospitalized patients Am J HospPharm 1993 501875ndash1884
20 Dasta JF Anagaran DM Evolving role of thepharmacist in critical care Crit Care Med1992 20563ndash565
Table 2 Recommendations from the pharmacist
Interventions n
Change in drug dosing 49 28Drug information 45 26Miscellaneous information 38 22Discontinue drug 18 10Start new drug 5 3Change drug 5 3Order testdrug level 4 2Identification of actual or potential adverse drug reactions 3 2Change in dose form or route of administration 2 1Report adverse drug event 2 1Cancel laboratory test 1 06
921Crit Care Med 2002 Vol 30 No 4
11202012 Page 316 of 417
1626 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Survey of pharmaceutical servicesin pediatric resuscitation
KIMBERLY HAHN KAREN MARLOWE AND MIKE CHICELLA
Am J Health-Syst Pharm 2001 581626-8
KIMBERLY HAHN PHARMD is Clinical Phar-macist Childrenrsquos Healthcare of Atlanta At-lanta GA KAREN MARLOWE PHARMDBCPS is Assistant Professor Department ofClinical Pharmacy Practice Auburn Universi-ty (AU) Auburn AL and Clinical AssistantProfessor Department of Medicine Universi-ty of South Alabama (USA) Mobile MIKECHICELLA PHARMD is Assistant ProfessorDepartment of Clinical Pharmacy PracticeAU and Adjunct Assistant Professor Depart-ment of Pediatrics USA
Address correspondence to Dr Hahn at1405 Clifton Road NE Atlanta GA 30322(kimberlyhahnchoaorg)
Presented at the Southeastern ResidencyConference Athens GA April 27 2000 andthe Pediatric Pharmacy Advocacy Group An-nual Meeting San Antonio TX October 202001
Copyright copy 2001 American Society ofHealth-System Pharmacists Inc All rights re-served 1079-2082010901-1626$0600
Acardiopulmonary resuscitation(CPR) event can be chaotic andconfusing if participants lack
understanding of the roles of individ-ual resuscitation team members andhave inadequate training or educa-tion The confusion may be aggravat-ed by inadequate hospital policies onthe content and location of the emer-gency drug cart1 These factors aremultiplied in an emergency situationinvolving a child Children who suffercardiopulmonary arrest have a verypoor prognosis with reported survivalrates of 0ndash172 Emergency carewhich has traditionally focused onadult needs may leave some institu-tions unprepared for pediatric car-diopulmonary arrests
Pediatric patients include a diverserange of ages and sizes thereforemedication dosages and fluid re-quirements also vary widely Guide-lines for pediatric advanced life sup-port (PALS) provide instruction onthe use of certain emergency medica-
tions but do not give information onwhich drugs should be available forresuscitation efforts3 A large varietyof drugs and concentrations wouldonly encourage indecision and possi-bly delay action Ideally only onedrug per critical category should beincluded in the emergency drug cartunless clinically significant differ-ences exist among drugs in the sameclass4 Pharmacy departments havethe opportunity to play an importantrole in pediatric resuscitation and toinfluence which medications are in-cluded in the cart
The purpose of this survey was toassess pharmaceutical services relat-ed to pediatric resuscitations includ-ing medications routinely stored inpediatric emergency drug carts andpharmacist participation in resusci-tation activities
xxxMethods A 14-question two-pagequestionnaire was developed andevaluated for content and clarity byseveral pharmacists involved on an
11202012 Page 317 of 417
1627Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
emergency resuscitation team Thesurvey was mailed in March 2000 tothe directors of pharmacy at 558 insti-tutions selected according to infor-mation found in the 1998ndash99 AHAGuide5 Only institutions listing pe-diatric intensive care services andhaving ge100 licensed beds were in-cluded A cover letter explained thepurpose of the study and a postage-paid return envelope was providedThe pharmacy directors were invitedto forward the survey to the most ap-propriate person in the department
The survey asked for demographicdata such as the type of hospitalnumber of licensed pediatric bedsand pediatric intensive care beds andestimated number of pediatric emer-gency resuscitation attempts per yeara list of the medications included onthe institutionrsquos emergency drug cartand how other drugs might be ob-tained during an emergency situa-tion and the extent and nature ofpharmacist participation in resus-citation efforts A list of possiblepharmacist functions was providedincluding preparing medicationsadministering medications provid-ing drug information documentingdrug administration calculating dos-es and performing CPR The surveyalso asked whether the hospital had aspecial emergency drug cart for pedi-atric patients All results are reportedas means medians and in some in-stances ranges
Results One hundred forty-foursurveys were returned for a responserate of 258 Surveys were receivedfrom 39 states and the District of Co-lumbia Of the questionnaires 123(85) were returned by adult hospi-tals with some pediatric services and21 (15) came from specialized pe-diatric institutions Eighty-one(57) were teaching hospitals in-cluding all the specialized pediatricinstitutions
The mean number of pediatric re-suscitation attempts reported per in-stitution per year was 22 (median 9range 0ndash300) for all responding hospi-
Table 2Pharmacist Participation in Emergency Resuscitation by Type of Facility
Facility Total NoNo ()
Participating
Pediatric teachingAdult teachingAdult nonteachingOther
All
215857
8144
13 (619)37 (638)35 (614)
6 (750)91 (632)
Pharmacists
Table 1Medications Most Commonly Included in Emergency Medication Carts(n = 118 Hospitals)
DrugNo () Responding Hospitals Including
Drug in Emergency Carts
Sodium bicarbonateEpinephrineAtropineNaloxoneLidocaineDextroseDopamineCalcium chlorideAdenosineIsoproterenolDobutamineFurosemidea
BretyliumDiphenhydraminea
Heparina
Phenytoina
118 (100) 117 (99) 115 (98) 115 (98) 114 (97) 112 (95) 109 (92) 106 (90) 87 (74) 86 (73) 72 (61) 71 (60) 70 (59) 65 (55) 63 (53) 61 (52)
aDrug not mentioned in pediatric advanced life-support guidelines
tals The mean number of licensed pe-diatric beds was 75 (median 37 range2ndash325) There were an average of 14licensed pediatric intensive-care-unitbeds (median 9 range 0ndash100)
Respondents from 118 hospitalsprovided information about medica-tions included in their emergencycarts A total of 109 medications werereported Table 1 lists the drugs includ-ed in gt50 of respondentsrsquo carts Al-though no specific neuromuscularblocking agents are mentioned in thePALS guidelines3 vecuronium was themost commonly included neuromus-cular agent (32 institutions [277])Of the 123 adult institutions 109(89) reported having a separate pe-diatric cart Respondents reportedseveral mechanisms for obtainingmedications not included in the cartThe most common mechanism wasobtaining the medications from thecentral or a satellite pharmacy Medi-
cations were also supplied by auto-mated dispensing machines througha pneumatic tube system from floorstock or by pharmacists participatingin the resuscitation attempt
Of the institutions surveyed 91(63) reported pharmacist participa-tion on resuscitation teams (Table 2)Pharmacist participation was eitherrequired or voluntary and either 24hours a day or on certain shifts onlyThe most common duties of pharma-cists during resuscitation efforts werecalculating drug dosages (93 of re-spondents with pharmacist participa-tion) providing drug information(93) preparing medications(92) and mixing intravenous flu-ids (91) Other reported duties in-clude timing and documenting drugadministration (40 and 33 re-spectively) setting up infusionpumps (13) administering drugs(10) and performing CPR (6)
11202012 Page 318 of 417
1628 Am J Health-Syst PharmmdashVol 58 Sep 1 2001
NOTES Pediatric resuscitation
Discussion The PALS guidelinesalthough not specifically addressingwhich drugs should be included inemergency resuscitation carts dis-cuss the use of adenosine alprostadilatropine bretylium calcium chlo-ride dextrose dobutamine dopam-ine epinephrine isoproterenollidocaine naloxone and sodium bi-carbonate3 The results of this surveyindicate that adenosine isoprotere-nol dobutamine and bretylium areincluded in fewer than 75 of pediat-ric emergency carts Alprostadil wasincluded at less than 5 of the re-sponding institutionsa This finding isattributed to the refrigeration re-quirement for alprostadil as well asthe limited indications for its use dur-ing resuscitation efforts such asmaintaining a patent ductus arterio-sus in an infant with cyanosis relatedto congenital heart disease
The medications included inemergency carts represent a large in-vestment for a pharmacy departmentIn areas with few pediatric resuscita-tion needs these medications mayexpire without being used Hospitalsmust determine the best combina-tion of medications and formulationsfor emergency needs while comply-ing with PALS guidelines
The survey results indicate varied
means for obtaining medications notincluded in the carts Each institutionshould define the mechanism for ob-taining such drugs or for obtainingadditional stock when cart medica-tions are depleted during resuscita-tion efforts Automated dispensingmachines and pharmacists bringingsupplies may be the most efficientmechanisms
In a previous survey of pharmacydirectors the rate of pharmacist par-ticipation in resuscitation attempts(nonspecified as adult or pediatric)was estimated at 30ndash336 In the cur-rent survey pharmacist participationwas gt60 This may represent re-sponse bias it is possible that institu-tions interested in this information orinvolved in a resuscitation programwere more likely to respond to the sur-vey It is also possible that a broaderdefinition of participation increasedthis percentage The degree of participa-tion was similar between childrenrsquoshospitals and adult institutions Phar-macists are completing tasks rangingfrom calculating dosages and provid-ing drug information to administeringmedications Many of these skills arenot specifically addressed in basic oradvanced life support training Inpa-tient pharmacists should be trained forthese particular skills
Ideally duplicate letters shouldhave been sent to all nonrespondentsand a telephone survey of nonre-sponders should have been per-formed These interventions were notperformed because of cost con-straints
Conclusion Institutions differedin their choice of drugs stocked in pe-diatric emergency carts and mecha-nisms for obtaining necessary drugsnot in the carts A substantial percent-age of pharmacists participated in re-suscitation efforts
aAlprostadil (prostaglandin E) is not includ-ed in any PALS algorithms but is discussed inthe PALS manual3 We therefore included it inour list of drugs in the questionnaire
References1 Telesca K A simplistic approach to re-
stocking crash carts Hosp Pharm 1992271068-70
2 Wright JL Patterson MD Resuscitating thepediatric patient Emerg Med Clin NorthAm 1996 14219-31
3 Chameides L Hazinski MF eds Pediatricadvanced life support Elk Grove VillageIL American Academy of Pediatrics1997
4 Nobel JJ Making a critical evaluation ofcrash carts Crit Care Nurse 1989 9126-8
5 American Hospital Association AHAguide to the health care field ChicagoHealthcare Infosource 1997
6 Shimp LA Mason NA Toedter NM et alPharmacist participation in cardiopulmo-nary resuscitation Am J Health-SystPharm 1995 52980-4
11202012 Page 319 of 417
13 13 13
Appendix13 G-shy‐313 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Knowledge13 Activity13 13
11202012 Page 320 of 417
Run Date 09062012 Page 1 of 32
UAN Hours (CEUs)
City Provider Information
0180-0000-12-119-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0239-0000-11-076-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0239-0000-11-090-L01-P 15 (015) httpprofessionaldiabetesorgcc 0239 - American Diabetes
Association0239-0000-11-079-L01-P 083 (0083) httpprofessionaldiabetesorgcc 0239 - American
Diabetes Association
0266-0000-12-548-L01-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0180-0000-10-021-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-021-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0136-0000-12-034-L01-P 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0136-0000-12-034-L01-T 2 (02) Somerville 0136 - New Jersey Pharmacists Association
0180-0000-11-003-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-132-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0053-0000-11-030-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
Knowledge
26th Clinical Conference- The Team Approach to Pediatric Diabetes It takes a Village
Knowledge
26th Clinical Conference- Transitioning from Pediatric to Adult Care
Knowledge
26th Clinical Conference- Treatment and Diagnosis of Type 2 Diabetes in Children and Adolescents
Knowledge
4th Annual VITALine SymposiumTheres No Place Like
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Cast Approach to Fluid Electrolyte Nutrition Management in a Preemie
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Crash Course in Pediatric Pharmacotherapy
Knowledge
A Review of Antiemetic Therapy used for Chemotherapy Induced Nausea and Vomiting
Knowledge
A SURVEY OF CHILDRENS HOSPITALS ON THE USE OF EXTEMPORANEOUS LIQUID
Knowledge
A Weighty Issue Use of Medications in Overweight Children
Knowledge
11202012 Page 321 of 417
Run Date 09062012 Page 2 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-030-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-11-504-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-11-069-L04-P 15 (015) San Antonio 0294 - VCU School
of Pharmacy Office of Continuing
Education
0047-9999-10-130-L01-P 5 (05) Orlando 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-10-014-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-014-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0204-0000-10-263-L01-P 2 (02) Anaheim 0204 - American Society of Health-
System Pharmacists
0106-9999-10-036-L01-P 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0106-9999-10-036-L01-T 1 (01) Ledyard CT 0106 - Connecticut Pharmacists Association
0062-9999-12-096-L01-P 1 (01) North Charleston (843-876-1925) 0062 - South Carolina College of
Pharmacy
A Weighty Issue Use of Medications in Overweight Children
Knowledge
a How Much is Too Much The Use of Rasburicase in the Treatment of Tumor Lysis Syndrome
Knowledge
AACP11 Geriatric Pharmacy Education SIG Pediatrics and Geriatrics Integration or Specialization in the Curriculum
Knowledge
AAE Conference Day 2 Asthma Educators Called to Encourage Empower and Educate
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Academia Workshop The Changing Face of the Pediatric Faculty Member
Knowledge
Acetaminophen Poisoning Whats the FDA Thinking How Would You Vote
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
Addressing Trends in Pediatric Psychological Treatment
Knowledge
ADHD Knowledge
11202012 Page 322 of 417
Run Date 09062012 Page 3 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0204-0000-11-216-L01-P 1 (01) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-09-115-L04-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-033-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-033-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-116-L05-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-203-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-203-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-029-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-029-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-029-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-013-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-013-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0069-9999-11-207-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
ADHD Treatment Myths and Controversies
Knowledge
Adolescent Issues Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Advances in Antimicrobial Therapy in Pediatric Patients with Cystic Fibrosis in the Last 20 years (The
Knowledge
Adverse Drug Events in Children Using Voluntary Reports to Measure the Impact of Medication Safety
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Effects of Antiepileptic Medications
Knowledge
Adverse Events Associated with Parenteral Nutrition
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Getting Involved in a Child Health Initiative at the Local and International Levels
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Advocacy Workshop Healthcare Reform
Knowledge
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
11202012 Page 323 of 417
Run Date 09062012 Page 4 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0004-0000-11-063-L01-P 15 (015) Little Rock amp Fayetteville 0004 - University of Arkansas for
Medical Sciences College of Pharmacy
0180-0000-10-205-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-205-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-9999-11-006-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-008-L01-P 15 (015) Orlando mad-id-15th-annual-
meeting0485 - MAD-ID
Inc0180-0000-10-202-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-202-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-004-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-004-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-020-L04-P 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-020-L04-T 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0204-0000-10-235-L05-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-11-005-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Ahhh-choo Cough and cold medications in young children
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Antidepressants and Antipsychotics in Youth do the Benefits Outweigh the Risks
Knowledge
Anti-fungal Prophylaxis and Treatment Considerations in Neutropenic Patients
Knowledge
Antimicrobial Stewardship in Pediatric Practices
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Application of Pharmacogenomics to the treatment of the Patient with Epilepsy
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Approach to a Complicated Patient in the Pediatric Clinical Care Unit
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Argatroban and Lepirudin Utilization in a Pediatric Population A Five Year Experience
Knowledge
Assuring Safe Technology Implementation in Specialty Areas Pediatrics Oncology and Investigational Drug Services
Knowledge
Basics of Bone Marrow Transplant Knowledge
11202012 Page 324 of 417
Run Date 09062012 Page 5 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-096-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-10-010-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-128-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-030-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0202-0000-10-138-L01-P 15 (015) Washington 0202 - American Pharmacists Association
0180-0000-10-007-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-007-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0239-0000-10-018-L01-P 15 (015) San Francisco 0239 - American Diabetes
Association0038-0000-11-023-L04-P 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0038-0000-11-023-L04-T 3 (03) Piscataway 0038 - Rutgers
University Ernest Mario School of
Pharmacy0263-0000-09-090-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-023-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-023-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Bedside Feeding Practices Best Practice and Avoiding Morbidities
Knowledge
Beyond the Basics Vitamins and Pancreatic Enzymes in Cystic Fibrosis
Knowledge
Blinded Volume Verification in a Pediatric Bar-code Medication Administration System (BCMA) to
Knowledge
Blood Thinners in Babies Anticoagulation in infants lt 1 year of age
Knowledge
Breaking News I Patient Safety Issues
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Building A Standardized Approach to Acute Pediatric Care
Knowledge
Cardiometabolic Risk in Children Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for Kids Pediatric Therapeutic Update for Pharmacists
Knowledge
Caring for our Tiniest Babies Evidence-Based Practices for Better Outcomes
Knowledge
Cerebral Palsy Knowledge
Cerebral Palsy Knowledge
11202012 Page 325 of 417
Run Date 09062012 Page 6 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-138-L01-P 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-114-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-014-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0491-0000-09-008-L01-P 6 (06) Albuquerque 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Cincinnati 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Columbus 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Denver 0491 - Cross Country Education
LLC0491-0000-09-008-L01-P 6 (06) Indianapolis 0491 - Cross
Country Education LLC
0491-0000-09-008-L01-P 6 (06) Phoenix 0491 - Cross Country Education
LLC0180-0000-10-209-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-209-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-135-L04-P 1 (01) Richmond 0294 - VCU School
of Pharmacy Office of Continuing
Education
0180-0000-09-107-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Challenges of Antimicrobial Dosing in Obese Pediatric Patients
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chemotherapy Safety-Processes and Technology
Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chlidrens Health and Nutrition Knowledge
Chronic Dermatology Knowledge
Chronic Dermatology Knowledge
CJW NICU Updates Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
11202012 Page 326 of 417
Run Date 09062012 Page 7 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-119-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-016-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-016-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0112-0000-12-106-L04-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0112-0000-11-146-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-11-035-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-130-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-255-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-038-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-011-L01-P 075 (0075) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-113-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0465-0000-12-022-L01-P 05 (005) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls - Changing Times Updates from the World of Poisonings
Knowledge
Clinical Pearls Pediatrics Pulmonary Arterial Hypertension Refeeding Syndrome
Knowledge
Community Acquired Methicillin-resistant Staphylococcus aureus (MRSA) in Pediatric Patients
Knowledge
Community Acquired Pneumonia in the Critical Care Setting
Knowledge
Comparison of Initial and Final Alprostadil Dose Needed to Maintain Patency of the Ductus Arteriosus
Knowledge
Complex Cases of Neonatal Resuscitation
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous Infusion Beta-Lactam Therapy for Management of Acute Exacerbations in Cystic Fibrosis
Knowledge
Continuous infusion versus scheduled antibiotics
Knowledge
Corticosteroids in Pediatric HematologyOncology Clinical Applications Toxicities and Controversies
Knowledge
11202012 Page 327 of 417
Run Date 09062012 Page 8 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-013-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-023-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-207-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-207-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-087-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0069-0000-11-149-L01-P 15 (015) Las Vegas 0069 - American
Association of Diabetes Educators
0180-0000-09-126-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-009-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0180-0000-10-034-L01-P 05 (005) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-032-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-032-L01-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-032-L01-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
CPOE and chemotherapy The Implementation Process
Knowledge
Cultural Considerations in Clinical Practice
Knowledge
Cultural Diversity Knowledge
Cultural Diversity Knowledge
Current Advances in Neonatal Nutrition
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Cystic Fibrosis Knowledge
Cystic Fibrosis Current Challenges and Implicationf for Drug Therapy
Knowledge
Development of Novel Therapies for the Treatment of RSV Infection
Knowledge
Devices Gadgets and Gizmos Knowledge
Devices Gadgets and Gizmos Knowledge
11202012 Page 328 of 417
Run Date 09062012 Page 9 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0062-9999-12-012-L01-P 1 (01) North Charleston (843-876-0968) 0062 - South Carolina College of
Pharmacy0180-0000-09-100-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-022-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-008-L04-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-115-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-009-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-137-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-131-L04-P 025 (0025) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-017-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-017-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0277-0000-10-146-L01-P 1675 (1675) Wailea Maui 0277 - University of California Davis Health System Department of
Pharmacy0263-0000-09-089-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-021-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group
Diabetes in Children and Adolescents
Knowledge
DKA amp HHS Knowledge
Dosing in ECMO and CRRT Knowledge
Drug Adherance in Adolescence Knowledge
Drugs in Pregnancy Treating the Mother- Protecting the Unborn
Knowledge
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria
Knowledge
Educational Tours of Texas Childrens Hospital
Knowledge
Efficacy of Bar-code Medication Administration (BCMA) on Errors in a Pediatric Medical Surgical Unit
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Eicosapentaenoic Acid Attenuates Bile Acid-Induced Apoptosis via the Fas and TRAIL-R2 Death Receptors
Knowledge
Emergency Medicine Update Hot Topics 2010
Knowledge
Evaluation and Management of Infants with Suspected Heart Disease
Knowledge
Evaluation of the Incidence of Parenteral Nutrition-Associated Liver Disease in Infants Requiring
Knowledge
11202012 Page 329 of 417
Run Date 09062012 Page 10 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-018-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-018-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-086-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-09-116-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-035-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-035-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-083-L04-P 7 (07) San Francisco 0263 - Contemporary
Forums0003-0000-10-123-L01-P 2 (02) Tucson 0003 - University of
Arizona College of Pharmacy The
0180-0000-10-200-L01-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-200-L01-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0284-0000-10-014-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-11-007-L01-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-109-L04-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evaluation of Vancomycin Dosing for Complicated Infections in Pediatric Patients
Knowledge
Evidence Based Neonatal Skin Care Update on Bathing Disinfectants Adhesives and
Knowledge
Extreme Dosing Knowledge
Fetal Care Knowledge
Fetal Care Knowledge
Fetus amp Newborn-Main Conference Knowledge
Fundamental Updates in Pediatrics Outpatient and Inpatient Pearls
Knowledge
General Overview of Epilepsy Knowledge
General Overview of Epilepsy Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Glucarpidase for Methotrexate Toxicity
Knowledge
Grant Writing Knowledge
11202012 Page 330 of 417
Run Date 09062012 Page 11 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-039-L01-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0168-0000-10-110-L04-P 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii
Pharmacists Association (HPhA)
0168-0000-10-110-L04-T 1 (01) KapoleiIhilani wwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-P 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0168-0000-12-006-L04-T 1 (01) Honoluluwwwhipharmorg 0168 - Hawaii Pharmacists
Association (HPhA)
0096-0000-10-090-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-09-118-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-022-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-108-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-212-L04-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-212-L04-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
H2 blocker use and late onset sepsis in the neonate
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2010 Childhood Obesity
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Hawaii Pharmacists Annual Mtg 2012 Session6 - Can You Help Me Vaccinate My Child Tight Away
Knowledge
Head Shoulders Knees and Toes (and Ears and Mouth and Nose and ) Antibiotic Essentials for Children
Knowledge
Helms Award Knowledge
Helms Lecture Series Knowledge
Help I have Tricky-itis (Treatment of Tracheitis)
Knowledge
Hemophilia Workshop Knowledge
Hemophilia Workshop Knowledge
11202012 Page 331 of 417
Run Date 09062012 Page 12 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0156-0000-10-096-L04-T 1 (01) San Antonio 0156 - Texas Society of Health-
System Pharmacists The
0180-0000-09-124-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-092-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0204-0000-12-112-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0204-0000-12-111-L01-P 2 (02) Baltimore 0204 - American Society of Health-
System Pharmacists
0278-0000-11-034-L01-P 2 (02) Virginia Beach 0278 - Virginia Pharmaceutical
Association0278-0000-11-034-L01-T 2 (02) Virginia Beach 0278 - Virginia
Pharmaceutical Association
0180-0000-11-016-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-038-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0047-0000-11-136-L01-P 7 (07) Fargo 0047 - North Dakota State
University College of Pharmacy
Nursing and Allied Sciences
0180-0000-09-127-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Hospital Pharmacy Technicians and the Pediatric Patient
Knowledge
Hot Topics Knowledge
Hot Topics from the Neonatal-Perinatal Literature
Knowledge
Hot Topics in Clinical Pediatric Practice Antimicrobial Stewardship and Drug Disposition in ECMO
Knowledge
Hot Topics in Clinical Pediatric Practice Ketogenic Diet and Update on Antiepileptic Agents
Knowledge
Hot Topics in Pediatrics Knowledge
Hot Topics in Pediatrics Knowledge
How a Tennessee pharmacist became CEO of the worlds 1 pediatric cancer hospital
Knowledge
Immunization updateManagement of Pandemics
Knowledge
Immunization Update Expanding the Pharmacist Role
Knowledge
Improvement or Reversal of Parenteral Nutrition Associated Liver Disease in Six Infants with Short
Knowledge
11202012 Page 332 of 417
Run Date 09062012 Page 13 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0284-0000-10-002-L01-P 1 (01) San Antonio 0284 - College of Psychiatric and
Neurologic Pharmacists
0022-9999-10-173-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0180-0000-10-213-L02-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-213-L02-T 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-028-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-120-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0347-0000-09-065-L01-P 1 (01) Tacoma Western State Hospital Grand Rounds 800
0347 - Foundation for Care
Management0180-0000-12-132-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0298-9999-09-015-L01-P 165 (165) Clearwater 0298 - Bayfront Medical Center
0263-0000-09-097-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-12-103-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0284-9999-11-014-L04-P 1 (01) Phoenizcpnporg2011402-476-1677
0284 - College of Psychiatric and
Neurologic Pharmacists
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
In Search of a Healthy America Meeting Families Where They Begin Through Integrated Prenatal Pediatric and Behavioral Health
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Incorporating Pharmaceutical Care into Pediatric HIV
Knowledge
Infant and Pediatric Formulas History Content and Indications
Knowledge
Infectious Disease - CAMRSA Knowledge
Influenza Strategies to Diagnose Treat and Reduce Risk in Community and Patient Health Care
Knowledge
Informatics 101 Knowledge
Initiative for Pediatric Palliative Care Educational Retreat
Knowledge
Intrauterine Infections Prematurity and Neonatal Sepsis Strategies for Diagnosis and Prevention
Knowledge
Intravenous Lock Therapy Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
11202012 Page 333 of 417
Run Date 09062012 Page 14 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0173-0000-11-009-L04-P 1 (01) Boise wwwishpshuttlepodorg 0173 - Idaho Society of Health-
System Pharmacists
0485-0000-11-005-L01-P 15 (015) Orlando mid-idorgregistrationhtm
0485 - MAD-ID Inc
0180-0000-09-105-L04-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0499-9999-12-004-L01-T 1 (01) Florence 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0217-0000-11-090-L01-P 15 (015) Pittsburgh -- wwwaccpcomam 0217 - American College of Clinical
Pharmacy0180-0000-12-127-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0124-0000-10-006-L01-T 1 (01) Novi 0124 - Southeastern
Michigan Society of Health-System Pharmacists
0180-0000-11-033-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-017-L04-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0043-0000-11-024-L01-P 1 (01) Jamaica 0043 - St Johns University College of Pharmacy and Health Sciences
0180-0000-11-037-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-102-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
Issues in Pediatric HematologyOncology
Knowledge
Issues in Pediatric Infectious Diseases
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
KIDs are PEOPLE Too Drug Therapy in Children
Knowledge
Late Breakers II Knowledge
Lean Management Stories from the Frontline
Knowledge
Little Hands New Life Complications and Pharmaceutical Care of Newborns
Knowledge
Live at LeBonheur Childrens Hospital
Knowledge
Live at St Jude Childrens Research Hospital
Knowledge
Long Term Complications of Pediatric Chemotherapy
Knowledge
Mama Said Knock You Out Innovative Sedation
Knowledge
Management of Diabetes Type I Knowledge
11202012 Page 334 of 417
Run Date 09062012 Page 15 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-104-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-095-L01-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-11-041-L01-P 1 (01) Columbus 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-006-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-006-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-259-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-12-125-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-030-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0042-0000-11-004-L01-P 5 (05) E Elmhurst NY wwwliuedupharmce
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-102-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-091-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-10-211-L04-P 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group
Management of Diabetes Type II Knowledge
Management of Fluid amp Electrolyte Disorders in the LBW Infant
Knowledge
Management of Pancreatic Insufficiency in Cystic Fibrosis
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of Pulmonary Hypertension - General Session
Knowledge
Management of the Neonate with Critical Congenital Heart Disease From Birth Through Hospital
Knowledge
Managing Drug Shortages A Panel Discussion
Knowledge
Managing GI Issues in Children Knowledge
Managing the Treatment of Pediatric Patients
Knowledge
Mechanisms of Antibiotic Resistance amp Strategies for Prevention
Knowledge
Medical-Legal Issues in Neonatal Care Litigation Hot Spots
Knowledge
Medication Adherence Workshop Knowledge
11202012 Page 335 of 417
Run Date 09062012 Page 16 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-211-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0096-0000-10-091-L04-P 1 (01) TTUHSC SOP SW Campus -
Dallas0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0180-0000-12-118-L04-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0485-0000-12-011-L01-P 2 (02) Orlando Caribe Roylle 0485 - MAD-ID
Inc0263-0000-09-093-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0180-0000-09-121-L04-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-033-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-033-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-09-123-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-253-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0180-0000-10-002-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-027-L04-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Medication Adherence Workshop Knowledge
Medication Safety Issues in the Breastfeeding Mother
Knowledge
Medication Therapy Management in a Pediatric Medical Home
Knowledge
Meet the Professors Knowledge
Mending Tender Skin Diaper Dermatitis Ostomoies Excoriations and IV Infiltrates
Knowledge
Meta-Analysis Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
Mommy and Me Medications in Pregnancy
Knowledge
NarcoticsSedationNAS etc Knowledge
NEC The Road to Zero Knowledge
Neonatal Abstinence Syndrome Knowledge
Neonatal and Pediatric Hot Topics Knowledge
11202012 Page 336 of 417
Run Date 09062012 Page 17 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-027-L04-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-219-L01-P 7 (07) San Diego 0263 -
Contemporary Forums
0180-0000-10-005-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-09-085-L04-P 15 (015) San Francisco 0263 -
Contemporary Forums
0263-0000-09-098-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-011-L02-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0217-0000-09-088-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American College of Clinical
Pharmacy0217-0000-09-112-L01-P 15 (015) Anaheim wwwaccpcom 0217 - American
College of Clinical Pharmacy
0263-0000-11-258-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-11-026-L04-P 1 (01) Memhis 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-10-028-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0154-0000-10-018-L04-P 1 (01) wwwrxcellenceorg 0154 - Texas Pharmacy
Association0154-0000-10-018-L04-T 1 (01) wwwrxcellenceorg 0154 - Texas
Pharmacy Association
Neonatal and Pediatric Hot Topics Knowledge
Neonatal and Pediatric Nutrition - Day One
Knowledge
Neonatal Circulatory Support Knowledge
Neonatal Emergencies and Other Surprises in the Delivery Room Case Studies of Complex Situations
Knowledge
Neonatal Resuscitation Evidence-Based Care
Knowledge
New Therapies in Neuroblastoma Knowledge
Novel Strategies for Therapeutic Dilemmas -- Mental Health Across the Ages
Knowledge
Novel Strategies for Therapeutic Dilemmas -- The Problem with Lipids
Knowledge
Obesity in Pregnancy Implications for Mother and Baby
Knowledge
Off-Label Drug Use in Pediatric Patients How Can We Change the System
Knowledge
OSHP 2010 Annual Meeting Residency Project Pearls - Session 2
Knowledge
OTCs in Pediatrics Knowledge
OTCs in Pediatrics Knowledge
11202012 Page 337 of 417
Run Date 09062012 Page 18 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0455-0000-09-006-L01-P 2 (02) M Resort - Henderson NV 0455 - Roseman University of Health
Sciences0180-0000-11-010-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0046-9999-10-004-L01-P 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-004-L01-T 3 (03) Fayetteville 0046 - University of North Carolina
Eshelman School of Pharmacy
0180-0000-10-206-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-206-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0096-0000-10-088-L01-P 1 (01) TTUHSC SW Campus - Dallas 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0062-9999-11-133-L04-T 1 (01) Columbia (PHR Resident Series) 0062 - South Carolina College of
Pharmacy0180-0000-11-001-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-001-L01-T 1 (01) St Louis 0180 - Pediatric Pharmacy
Advocacy Group0053-0000-11-034-L04-P 15 (015) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
Over-the-counter medications in young children uses misuses and myths
Knowledge
Palliative Care Advances in Pediatric Oncology
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Pathology Diagnosis and Management of Type 1 Diabetes in Children and Adolescents
Knowledge
Patient Assistant Programs 101 Knowledge
Patient Assistant Programs 101 Knowledge
Pay Attention to This Lessons Learned on Medications for ADHD
Knowledge
Pediatric amp Neonatal Emergency Medications
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Controversies in Inhaled Therapy
Knowledge
Pediatric Clinical Pearls Knowledge
11202012 Page 338 of 417
Run Date 09062012 Page 19 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0053-0000-11-034-L04-P 15 (015) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-030-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-030-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-124-L02-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0173-0000-12-002-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho
Society of Health-System
Pharmacists0202-0000-10-206-L01-P 1 (01) Chattanooga 0202 - American
Pharmacists Association
0202-0000-10-206-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
0179-9999-11-029-L04-P 1 (01) Buffalo 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-P 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0179-9999-12-006-L04-T 1 (01) New Orleans 0179 - Louisiana Society of Health-
System Pharmacists
0134-0000-12-028-L05-P 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
Pediatric Clinical Pearls Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric Electronic Medical Record Knowledge
Pediatric HIVAIDS Treatment Worlds Apart
Knowledge
Pediatric Immunizations Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Infectious Disease Update for the Outpatient Setting
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Adherence and Counseling
Knowledge
Pediatric Medication Safety Across the Continuum
Knowledge
11202012 Page 339 of 417
Run Date 09062012 Page 20 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0134-0000-12-028-L05-T 1 (01) Saratoga 0134 - New York State Council of Health-System Pharmacists
0060-9999-11-030-L01-P 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-030-L01-T 5 (05) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0046-9999-09-182-L04-P 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-09-182-L04-T 15 (015) Wilson 0046 - University of North Carolina
Eshelman School of Pharmacy
0022-9999-10-156-L01-P 075 (0075) Louisville 0022 - University of Kentucky College
of Pharmacy
0136-0000-12-020-L01-P 1 (01) Newark 0136 - New Jersey Pharmacists Association
0173-0000-12-011-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0120-9999-12-007-L04-P 05 (005) Fort Wayne 0120 - Indiana Pharmacists
Alliance0165-0000-10-074-L04-P 1 (01) Orlando 0165 - Florida
Pharmacy Association
0165-0000-10-074-L04-T 1 (01) Orlando 0165 - Florida Pharmacy
Association
Pediatric Medication Safety Across the Continuum
Knowledge
Pediatric Medicine Knowledge
Pediatric Medicine Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Knowledge
Pediatric Obesity Clinical and Research Innovation
Knowledge
Pediatric OTC Therapy Options Knowledge
Pediatric Pain Knowledge
Pediatric Pearls Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
Pediatric PETCT Challenges Pitfalls and Normal Variants
Knowledge
11202012 Page 340 of 417
Run Date 09062012 Page 21 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-037-L04-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-037-L04-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-025-L01-P 3 (03) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0180-0000-12-120-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0499-0000-11-010-L01-P 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-P 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0499-0000-11-010-L01-T 2 (02) Charleston 0499 - Southeastern
Continuing Medical Education
Consultants LLC0499-0000-11-010-L01-T 2 (02) Greenville 0499 -
Southeastern Continuing Medical
Education Consultants LLC
0180-0000-11-036-L01-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-034-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacology and Therapeutics
Knowledge
Pediatric Pharmacotherapy Update for Pharmacists and Nurse Practitioners
Knowledge
Pediatric Pharmacy Practice Past Present and Future (What is old is new)
Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Pharmacy Update Knowledge
Pediatric Procedural sedation Knowledge
Pediatric Septic Shock Knowledge
11202012 Page 341 of 417
Run Date 09062012 Page 22 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0202-0000-11-176-L01-P 1 (01) Dallas 0202 - American Pharmacists Association
0202-0000-11-176-L01-T 1 (01) Dallas 0202 - American Pharmacists Association
0282-0000-10-018-L01-P 1 (01) Gillette WY 307-688-6009 0282 - Campbell County Memorial
Hospital0282-0000-10-018-L01-T 1 (01) Gillette WY 307-688-6009 0282 - Campbell
County Memorial Hospital
0266-0000-11-531-L04-P 6 (06) Danvillewwwgeisinegredu800-272-6692
0266 - Geisinger Health System
0266-0000-12-549-L04-P 65 (065) Danvillewwwgeisingeredu8002726692
0266 - Geisinger Health System
0097-0000-10-027-L04-P 3 (03) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0465-0000-12-013-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0465-0000-12-024-L01-P 1 (01) Orlando 0465 -
HematologyOncology Pharmacy Association
(HOPA)0204-0000-10-256-L04-P 175 (0175) Anaheim 0204 - American
Society of Health-System
Pharmacists0163-9999-12-088-L01-P 1 (01) Gainesville 0163 - Florida
Society of Health-System
Pharmacists Inc
Pediatric Sickle Cell Disease Knowledge
Pediatric Sickle Cell Disease Knowledge
Pediatric Thrombosis Knowledge
Pediatric Thrombosis Knowledge
Pediatric Update Knowledge
Pediatric Update Knowledge
Pediatric Updates 1 2 3s of Pediatric Assessment amp Sports Related Injuries in School-Age Children
Knowledge
Pediatrics 1 Knowledge
Pediatrics 3 Knowledge
Pediatrics for the Non-Pediatric Practitioner Practicing Evidence-Based Medicine without the Evidence
Knowledge
Pediatrics Part I Knowledge
11202012 Page 342 of 417
Run Date 09062012 Page 23 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-12-093-L01-P 1 (01) Gainesville 0163 - Florida Society of Health-
System Pharmacists Inc
0178-0000-11-013-L04-P 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0178-0000-11-013-L04-T 15 (015) Destin 0178 - Alabama Pharmacy
Association Research amp Education Foundation
0204-0000-11-227-L01-P 25 (025) New Orleans 0204 - American Society of Health-
System Pharmacists
0180-0000-10-204-L04-P 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-204-L04-T 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-257-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-026-L04-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-026-L04-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-122-L01-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0282-9999-11-011-L05-P 1 (01) Casper WY 307-688-6009 0282 - Campbell County Memorial
Hospital
Pediatrics Part II Knowledge
Pediatrics Primer Knowledge
Pediatrics Primer Knowledge
Pediatrics How to Knock em Out and Lock em Out
Knowledge
Personal and Organizational Greatness
Knowledge
Personal and Organizational Greatness
Knowledge
Perturbations in Blood Glucose Causes and Concerns
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist Development General Workshop
Knowledge
Pharmacist in ED Knowledge
Pharmacist Role in SIDS Risk Reduction
Knowledge
11202012 Page 343 of 417
Run Date 09062012 Page 24 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-129-L04-P 025 (0025) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-024-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-002-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-015-L01-P 1 (01) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0144-9999-12-017-L01-P 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0144-9999-12-017-L01-T 1 (01) Ocean City 410-727-0746 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0173-0000-12-006-L04-P 1 (01) Boise 208-342-2581 0173 - Idaho Society of Health-
System Pharmacists
0180-0000-09-112-L01-P 15 (015) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-031-L01-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0485-0000-12-004-L01-P 15 (015) Orlando mad-id-1th-annual-meeting
0485 - MAD-ID Inc
0263-0000-09-099-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums
Pharmacist Validation of Doses Outside Smart Pump Limits
Knowledge
Pharmacists involvement in Multi-Centered Clinical Trials in a Pediatric Hospital
Knowledge
Pharmacogenomics-Applications in Pediatric Oncology
Knowledge
Pharmacology of New Agents in Pediatric Oncology
Knowledge
Pharmacy Practice Pearls Knowledge
Pharmacy Practice Pearls Knowledge
Physiological and Pharmacokinetic Differences between Adults and Children
Knowledge
PkPD Knowledge
PKPD differences in infants and children with Acyanotic and Cyanotic Congenital Heart Disease
Knowledge
Pneumonia Knowledge
PPHN Causes Care and Controversies
Knowledge
11202012 Page 344 of 417
Run Date 09062012 Page 25 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-11-025-L04-P 15 (015) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-117-L04-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-09-094-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0053-0000-11-029-L01-P 1 (01) Oklahoma City 0053 - University of
Oklahoma College of Pharmacy
0053-0000-11-029-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0741-0000-12-004-L01-P 5 (05) Las VegaswwwUniversityLearningco
m800-940-5860
0741 - University Learning Systems
Inc0180-0000-12-107-L01-P 025 (0025) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-103-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-009-L01-P 1 (01) DallasFort Worth TBD 0022 - University of
Kentucky College of Pharmacy
0022-9999-10-009-L01-P 1 (01) Los Angeles Wilshire Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) NYC TBD 0022 - University of Kentucky College
of Pharmacy
Preceptor Development Mentorship Knowledge
Predictors of Hepatotoxicity in Pediatric Patients Receiving Voriconzole
Knowledge
Prevailing Ethical Issues in Neonatal Care Viability and Other Challenges
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Preventing Infectious Diseases Update on Pediatric Vaccines
Knowledge
Principles of Pediatric Pharmacotherapy
Knowledge
Pro-Calci what (Procalcitonin Use In Infectious Disease)
Knowledge
Pumps Pens amp Other Devices Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
11202012 Page 345 of 417
Run Date 09062012 Page 26 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0022-9999-10-009-L01-P 1 (01) Orlando Peabody Hotel 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Philadelphia TBD 0022 - University of Kentucky College
of Pharmacy
0022-9999-10-009-L01-P 1 (01) Washington TBD 0022 - University of Kentucky College
of Pharmacy
0263-0000-09-088-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0180-0000-11-020-L01-P 025 (0025) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-028-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-028-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-012-L04-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-012-L04-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0053-9999-12-032-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-10-001-L01-P 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-001-L01-T 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing the Burden of RSV Infection through Recommended Prevention and Treatment
Knowledge
Reducing your Infection Rate and Risk A Total Body Approach
Knowledge
Relationship of caffeine dosing with serum alkaline phosphatase levels in extremely low birth-weight infants
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop How to Get Your Residency Project Done in One Year
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Research Workshop Pharmacogenomics Impact on Pediatric Pharmacy Practice
Knowledge
Residency Project Pearls (2) Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
Resuscitation and RSI Pharmacotherapy - Level 1 (PICU)
Knowledge
11202012 Page 346 of 417
Run Date 09062012 Page 27 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0088-9999-11-041-L01-P 1 (01) Myrtle Beach 0088 - Campbell University College of Pharmacy and Health Sciences
0294-9999-11-101-L04-P 05 (005) Roanoke 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-10-036-L01-P 05 (005) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-025-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0060-9999-11-031-L04-P 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0060-9999-11-031-L04-T 1 (01) Bar Harbor 0060 - University of Rhode Island
College of Pharmacy
0263-0000-11-251-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-210-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-210-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-111-L04-P 2 (02) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0263-0000-11-256-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-214-L04-P 15 (015) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
Safety First The Ins and Outs of Medications in Pediatrics
Knowledge
SCCM11 Year in Review Pediatrics Knowledge
Selection of Antibiotics Dosing and Length of Therapy
Knowledge
Sepsis and Septic Shock Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Shots for Tots A Pharmacists Refresher
Knowledge
Should Kernicterus Be a Never Event
Knowledge
Sickle Cell Workshop Knowledge
Sickle Cell Workshop Knowledge
Simplifying Leadership Complexities in Pediatric Pharmacy Patient Care
Knowledge
Skin Breakdown and Wound Care in the NICU Patient
Knowledge
Solid Organ Transplant Long Term Considerations
Knowledge
11202012 Page 347 of 417
Run Date 09062012 Page 28 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-214-L04-T 15 (015) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-126-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-031-L01-P 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-031-L01-T 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0414-0000-11-214-L01-P 1 (01) Wingate 0414 - Wingate University School
of Pharmacy0453-9999-12-116-L01-P 15 (015) Boston 0453 - Amedco
LLC0453-9999-12-117-L01-P 15 (015) Boston 0453 - Amedco
LLC0180-0000-11-004-L04-P 15 (015) Memphis 0180 - Pediatric
Pharmacy Advocacy Group
0453-9999-12-126-L01-P 15 (015) Boston 0453 - Amedco LLC
0263-0000-11-260-L01-P 425 (0425) Las Vegas 0263 - Contemporary
Forums0180-0000-10-009-L01-P 1 (01) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-009-L01-T 1 (01) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0451-0000-12-025-L01-P 15 (015) Honolulu 0451 - American
Pain Society0263-0000-11-250-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0018-9999-11-140-L04-P 1 (01) Lafayette 0018 - Purdue University College
of Pharmacy
Solid Organ Transplant Long Term Considerations
Knowledge
Successful Mentoring Students Residents New Practitioners
Knowledge
Super Session Clinical Microbiology Review
Knowledge
Super Session Clinical Microbiology Review
Knowledge
The 411 on New Drugs in 2011 Knowledge
The Art and Science of Transition - Transition Nuts amp Bolts
Knowledge
The Art and Science of Transition - Transition Collaboration
Knowledge
The Childhood Cancer Survivor Study Defining Risks Among Long-term Survivors
Knowledge
The Complexity of Transplant Care-Partnering with the Medical
Knowledge
The Fetus amp Newborn State-of-the-Art Care - Day 3
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Impact of a Pharmacist-Managed RSV Prevention Clinic on Palivizumab Compliance and RSV
Knowledge
The Interrelationship Among Sleep Disturbances and Chronic Pain in
Knowledge
The Late Preterm Knowledge
The Late Pre-Term Infant Knowledge
11202012 Page 348 of 417
Run Date 09062012 Page 29 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0263-0000-09-084-L04-P 15 (015) San Francisco 0263 - Contemporary
Forums0022-9999-10-155-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0165-0000-10-090-L01-P 15 (015) Orlando 0165 - Florida Pharmacy
Association0165-0000-10-090-L01-T 15 (015) Orlando 0165 - Florida
Pharmacy Association
0042-0000-09-015-L01-P 5 (05) LaGuardia Marriott Hotel E Elmhurst
0042 - Arnold and Marie Schwartz
College of Pharmacy and
Health Sciences of Long Island University
0180-0000-12-109-L01-P 025 (0025) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-003-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-003-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0263-0000-11-243-L01-P 15 (015) Las Vegas 0263 -
Contemporary Forums
0069-0000-11-140-L01-P 15 (015) Las Vegas 0069 - American Association of
Diabetes Educators
0180-0000-12-105-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
The Late Preterm Infant A National Epidemic
Knowledge
The Role of Pediatric School Psychology in Integrated Health Care
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Skinny of Childhood Obesity and the Cardiovascular Consequences
Knowledge
The Treatment of Diabetes From Pediatrics to Geriatrics A Focus on Outpatient and Inpatient Management
Knowledge
Time to Appropriate Antimicrobial Use for Pediatric Pneumonia
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Topics in Pediatric Anticoagulation - General Session
Knowledge
Transfusion-Based Practices in the NICU Whats the Evidence
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Mycobacterium Infections
Knowledge
11202012 Page 349 of 417
Run Date 09062012 Page 30 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0154-0000-10-222-L01-P 1 (01) Austin 0154 - Texas Pharmacy
Association0289-0000-11-044-L01-P 6 (06) Asheville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Charleston 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Frederick 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Knoxville 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Morgantown 0289 - PESI
HealthCare 0289-0000-11-044-L01-P 6 (06) Nashville 0289 - PESI
HealthCare 0180-0000-10-201-L01-P 1 (01) Salt Lake City 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-201-L01-T 1 (01) Salt Lake City 0180 - Pediatric Pharmacy
Advocacy Group0007-0000-12-006-L01-P 15 (015) Ojai California 0007 - University of
Southern California School of Pharmacy
0180-0000-11-027-L04-P 1 (01) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0062-9999-11-115-L01-P 15 (015) Greenville ((864-560-6265) 0062 - South
Carolina College of Pharmacy
0277-0000-09-140-L01-P 85 (085) Monterey 0277 - University of California Davis Health System Department of
Pharmacy0112-9999-11-313-L01-P 1 (01) Internet 0112 - Michigan
Pharmacists Association
Treatment of Pediatric Asthma Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Pediatric Neurological Disorders
Knowledge
Treatment of Status Epilepticus Knowledge
Treatment of Status Epilepticus Knowledge
Troubled Teenager 101 Knowledge
Turning Your Clinical Observations into Publications
Knowledge
Type 1 Diabetes in Children and Adolescents
Knowledge
Update in Endocrinology and Metabolism New Therapies for Obesity Diabetes and Cardiovascular Disease
Knowledge
Updates in Neonatology Infant Vaccination and Neonatal Abstinence Syndrome
Knowledge
11202012 Page 350 of 417
Run Date 09062012 Page 31 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0046-9999-09-087-L04-P 15 (015) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0046-9999-10-029-L04-P 2 (02) Wilmington 0046 - University of North Carolina
Eshelman School of Pharmacy
0033-0000-09-051-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0180-0000-11-019-L04-P 025 (0025) Memphis 0180 - Pediatric Pharmacy
Advocacy Group0294-9999-10-128-L04-P 1 (01) Charlottesville 0294 - VCU School
of Pharmacy Office of Continuing
Education
0294-9999-11-037-L04-T 1 (01) Charlottesville 0294 - VCU School of Pharmacy Office
of Continuing Education
0180-0000-12-110-L01-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-043-L01-P 1 (01) St Louis 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-019-L04-P 025 (0025) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-019-L04-T 025 (0025) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-110-L01-P 2 (02) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group
Updates in Pediatric Self-Care Knowledge
Updates in Pediatric Self-Care Knowledge
Use of Dexmedetomidine for Sedation in Critically Ill Pediatric Patients
Knowledge
Use of subcutaneous catheters for enoxaparin administration
Knowledge
UVA Being the Pharmacist at a Pediatric Code
Knowledge
UVA Dont You Know that Im Toxic A Review of Pediatric Toxic Exposures
Knowledge
Vaccine Update Knowledge
Vaccines in the Neonatal Intensive Care Unit
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Validation of a Set of Asthma Illustrations in Children with Chronic Asthma in the Emergency
Knowledge
Vancomycin Dosing amp Monitoring Applying the IDSA Guidelines to Pediatric Patients
Knowledge
11202012 Page 351 of 417
Run Date 09062012 Page 32 of 32
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0294-9999-10-153-L01-P 1 (01) Wintergreen 0294 - VCU School of Pharmacy Office
of Continuing Education
0263-0000-11-252-L01-P 15 (015) Las Vegas 0263 - Contemporary
Forums0180-0000-10-024-L01-P 15 (015) St Charles 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-10-024-L01-T 15 (015) St Charles 0180 - Pediatric Pharmacy
Advocacy Group0278-0000-10-012-L01-P 1 (01) Hampton 0278 - Virginia
Pharmaceutical Association
0062-0000-11-137-L01-P 2 (02) Columbia (SCCP Fall Seminar) Call 803-777-9979 for
0062 - South Carolina College of
Pharmacy0180-0000-09-125-L01-P 1 (01) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-106-L01-P 1 (01) Cleveland 0180 - Pediatric Pharmacy
Advocacy Group0022-9999-10-160-L01-P 075 (0075) Louisville 0022 - University of
Kentucky College of Pharmacy
0202-0000-10-232-L01-P 1 (01) Chattanooga 0202 - American Pharmacists Association
0202-0000-10-232-L01-T 1 (01) Chattanooga 0202 - American Pharmacists Association
VASPEN10 The microbiome and probiotics in the pediatric patient
Knowledge
Viability and Ethics Knowledge
Warning Pregnant or Nursing Mom Knowledge
Warning Pregnant or Nursing Mom Knowledge
What Do I Say Now OTC Cough amp Cold Products in the Pediatric Patient
Knowledge
What the Pharmacist Needs to Know About Pediatric Emergencies
Knowledge
Whats New with RSV and Palivizumab Usage
Knowledge
Yaffe Award Lecture Knowledge
YES Youth Education and Screening in Primary Care
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
You Are What You Eat Guidelines for Adult and Pediatric Nutrition Support in the Critically Ill
Knowledge
11202012 Page 352 of 417
13 13 13
Appendix13 G-shy‐413 13
13 ACPE13 PLAN13
Programming13 Live13 Forum13
Application13 Activity13 13
11202012 Page 353 of 417
Run Date 09062012 Page 1 of 6
UAN Hours (CEUs)
City Provider Information
0180-0000-12-121-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0217-9999-11-047-L01-P 23 (23) San Antonio wwwaccpcom 0217 - American
College of Clinical Pharmacy
0217-9999-12-065-L01-P 15 (015) Denverwwwaccpcom 0217 - American College of Clinical
Pharmacy0180-0000-12-111-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0033-0000-09-054-L01-P 1 (01) St Louis 0033 - St Louis College of Pharmacy
0204-0000-10-267-L01-P 25 (025) Anaheim 0204 - American Society of Health-
System Pharmacists
0097-0000-09-045-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0180-0000-12-131-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-101-L01-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-106-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-01-L04-P 15 (15) 0236 - Society of
Critical Care Medicine
0180-0000-12-128-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
PharmaTECHonomics Implementing Technology in the Pediatric Setting
Application
2011 Oncology Pharmacy Preparatory Review Course
Application
2012 Oncology Pharmacy Preparatory Review Course Pediatric Malignancies
Application
Antimicrobial Stewardship Programs What works and what doesnt
Application
Application of Adult Vancomycin Guidelines to the Pediatric Population
Application
Clinical Considerations for Drug Dosing in Obesity
Application
Common Infections in Pediatrics Application
Communication Strategies for Inside and Outside Your Department
Application
Community Acquired Pneumonia- Evidence for Changes in Practice
Application
Controversies in Difficult to Treat Gram-negative Infections
Application
Current Concepts in Pediatric Critical Care
Application
Decision Support in EMR How Much is Enough (or Too Much)
Application
11202012 Page 354 of 417
Run Date 09062012 Page 2 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-12-134-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0202-0000-10-141-L04-P 15 (015) Washington 0202 - American
Pharmacists Association
0112-0000-10-148-L01-P 13 (013) Detroit 0112 - Michigan Pharmacists Association
0180-0000-12-123-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-136-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-114-L01-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0165-0000-10-009-L01-P 2 (02) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-009-L01-T 2 (02) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-006-L01-P 15 (015) Tampa 0165 - Florida
Pharmacy Association
0165-0000-10-006-L01-T 15 (015) Tampa 0165 - Florida Pharmacy
Association0204-0000-10-274-L01-P 2 (02) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-09-113-L01-P 15 (015) Cleveland 0180 - Pediatric
Pharmacy Advocacy Group
0236-0000-11-56-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Discovering and Developing Your Strengths
Application
Fostering Wellness and Safe Nonprescription Medication Use in Pediatric Patients
Application
How Sweet It Is Sucrose Analgesia in Infants
Application
How to Be a Great Journal Reviewer Application
How to Have Successful (and Meaningful) Resident or Student Projects for Your Department
Application
Infections You Thought You Would Never See
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Kids and Drugs The Changing Landscape of Substance Abuse
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Lifelong Protection A Focus on Pediatric and Geriatric Vaccinations
Application
Managing the Use of Propofol for Procedural Sedation in the Emergency Department
Application
Neuro Workshop Application
New Developments in Pediatric Cardiac Care
Application
11202012 Page 355 of 417
Run Date 09062012 Page 3 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0484-0000-09-014-L04-P 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-P 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Kenilworth Inn Kenilworth 0484 - Comprehensive
Continuing Education LLC
0484-0000-09-014-L04-T 35 (035) Woodcliff Lake Hilton Woodcliff Lake
0484 - Comprehensive
Continuing Education LLC
0009-0000-12-030-L04-P 1 (01) Storrs 0009 - University of Connecticut School
of Pharmacy
0180-0000-12-112-L02-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-28-L01-P 2 (02) 0236 - Society of
Critical Care Medicine
0133-9999-10-016-L04-P 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0133-9999-10-016-L04-T 1 (01) New Orleans 0133 - Louisiana Pharmacists Association
0097-0000-09-044-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-037-L04-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Overview of Autism Definitions and Treatments
Application
Patient and Caregiver Communications for Pediatric and Geriatric Populations
Application
Pediatric HIV Refresher Application
Pediatric Interactive Cases Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Medication Adherence and Counseling
Application
Pediatric Pharmacology A Primer Application
Pediatric Pharmacotherapy Pearls Application
11202012 Page 356 of 417
Run Date 09062012 Page 4 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0163-9999-10-037-L04-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-0000-10-052-L04-T 1 (01) Ft Myers 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-P 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-11-174-L01-T 1 (01) Orlando 0163 - Florida Society of Health-
System Pharmacists Inc
0165-0000-10-010-L01-P 15 (015) Tampa 0165 - Florida Pharmacy
Association0165-0000-10-010-L01-T 15 (015) Tampa 0165 - Florida
Pharmacy Association
0217-0000-10-123-L01-P 2 (02) Austin wwwaccpcomam 0217 - American College of Clinical
Pharmacy0204-0000-11-256-L04-P 175 (0175) New Orleans 0204 - American
Society of Health-System
Pharmacists0217-0000-11-082-L01-P 2 (02) Pittsburgh -- wwwaccpcomam 0217 - American
College of Clinical Pharmacy
0180-0000-12-130-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-12-122-L04-P 1 (01) Houston 0180 - Pediatric
Pharmacy Advocacy Group
Pediatric Pharmacotherapy Pearls Application
PEDIATRIC PHARMACY CLINICAL PEARLS
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Pneumonia Pharmacotherapy
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric Poisonings Pearls and Perils
Application
Pediatric PRN Focus SessionShake Rattle and Role Exploring the Place in Therapy for
Application
Pediatrics for the Non-Pediatric Practitioner Timely Topics in Caring for Tots
Application
Pediatrics PRN Focus SessionStaying Ahead of the Curve Contemporary Dosing
Application
Pharmacy Practice Model Initiative Application
Practice-Based Research Networks Application
11202012 Page 357 of 417
Run Date 09062012 Page 5 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0097-0000-09-043-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0053-0000-11-028-L05-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-028-L05-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0180-0000-12-135-L04-P 1 (01) Houston 0180 - Pediatric Pharmacy
Advocacy Group0107-0000-11-015-L01-P 1 (01) Des Moines 0107 -
Collaborative Education Institute
0097-0000-09-046-L01-P 1 (01) Wilkes-Barre 0097 - Nesbitt School of
Pharmacy at Wilkes University
0163-9999-10-138-L01-P 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0163-9999-10-138-L01-T 1 (01) Jacksonville 0163 - Florida Society of Health-
System Pharmacists Inc
0053-0000-11-031-L01-P 1 (01) Oklahoma City 0053 - University of Oklahoma College
of Pharmacy
0053-0000-11-031-L01-P 1 (01) Tulsa 0053 - University of Oklahoma College
of Pharmacy
0165-0000-10-008-L01-P 1 (01) Tampa 0165 - Florida Pharmacy
Association
Pregnancy and Lactation Application
Preventing Medicaton Errors in Children
Application
Preventing Medicaton Errors in Children
Application
Promoting Resiliency Recognizing and Preventing Burnout
Application
Recurrent Infections in Children Application
Responding to Pediatric Poisonings Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Small People in Big Trouble Pharmacotherapy of Common Pediatric Emergencies
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Sniffling Sneezing and Coughing Best OTC Treatments for Pediatrics
Application
Special Considerations in Pediatric Patients
Application
11202012 Page 358 of 417
Run Date 09062012 Page 6 of 6
PLAN Search ResultsAccreditation Council for Pharmacy Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0165-0000-10-008-L01-T 1 (01) Tampa 0165 - Florida Pharmacy
Association0180-0000-12-133-L04-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0294-9999-11-044-L01-P 1 (01) Newport Beach 0294 - VCU School of Pharmacy Office
of Continuing Education
0465-9999-12-028-L01-P 1 (01) Orlando 0465 - HematologyOncolo
gy Pharmacy Association
(HOPA)0217-0000-11-013-L01-P 3 (03) Columbus wwwaccpcomut 0217 - American
College of Clinical Pharmacy
0217-0000-12-019-L01-P 3 (03) Renowwwaccpcom 0217 - American College of Clinical
Pharmacy0451-0000-12-010-L04-P 15 (015) Honolulu 0451 - American
Pain Society0204-0000-10-245-L04-P 25 (025) Anaheim 0204 - American
Society of Health-System
Pharmacists0180-0000-12-104-L01-P 15 (015) Houston 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-12-129-L04-P 15 (015) Houston 0180 - Pediatric Pharmacy
Advocacy Group0236-0000-11-16-L04-P 1 (01) 0236 - Society of
Critical Care Medicine
0236-0000-11-72-L01-P 1 (01) 0236 - Society of Critical Care
Medicine
Special Considerations in Pediatric Patients
Application
Statistical Process Control What It Is and Why You Should Be Using It
Application
Symposium on Coagulation and Cardiovascular Pediatric Hemostasis
Application
The Emergence of Adolescent and Young Adult Oncology
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Pharmacotherapy Preparatory Review and Recertification Course -- Pediatrics Geriatrics and
Application
The Ripple Effect Systems-Level Interventions to Ameliorate Pediatric
Application
Treatment Controversies in Pediatric Pharmacotherapy RSV Antiepileptic Agents and Dexmedetomidine
Application
Year in Review Pediatrics Application
Treatment of Gastrointestinal Infectious in the Pediatric Patient
Application
What Makes a Great Residency Program
Application
Whats New in Pediatric Sepsis Application
11202012 Page 359 of 417
13 13 13
Appendix13 G-shy‐513 13
13 ACPE13 PLAN13
Programming13 Home13 Study13
Knowledge13 Activity13 13
11202012 Page 360 of 417
Run Date 09062012 Page 1 of 13
UAN Hours (CEUs)
Provider Information
0052-9999-11-2293-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2301-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1306-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2295-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2328-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2297-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2300-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2315-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2318-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2291-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2337-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-100-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2871-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-464-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2719-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-115-H04-P 15 (015) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2336-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
Title Activity Type
AAP Big Jump in Knee Injuries in Kids (29069)
Knowledge
AAP CPR Yields Low in Hospitalized Kids With CVD (29053)
Knowledge
AAP Dont Use Sensory Disorder Diagnosis (33018)
Knowledge
AAP Guideline Calls for Pre-K ADHD Evaluation (29066)
Knowledge
AAP Gun Injuries in Kids Up Sharply (29103)
Knowledge
AAP Low Back Pain in Kids Rarely Serious (29064)
Knowledge
AAP More Kids Going to ED for Psych Care (29057)
Knowledge
AAP Need to Re-Do Circumcision Rises Reasons Unclear (29075)
Knowledge
AAP New SIDS Guideline Says No to Bumper Pads (29091)
Knowledge
AAP One Course of Spinosad Exterminates Lice Nits (29065)
Knowledge
AAP SIDS Messages Miss the Mark for Some Parents (29070)
Knowledge
AAP Urinary Stones in Kids on the Rise (29119)
Knowledge
Access Enteral and Parenteral Knowledge
ACNP Moms Baby Blues Linked to Childs Psych Issues (30110)
Knowledge
Active Video Games No Fix for Kids Fitness (31374)
Knowledge
Acupuncture Safe for Kids (29817) Knowledge
Adolescent Issues Knowledge
Adults No Drain on Pediatric Heart Centers (29121)
Knowledge
11202012 Page 361 of 417
Run Date 09062012 Page 2 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0069-9999-11-207-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0052-9999-12-682-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0530-0000-10-052-H01-P 1 (01) 0530 - Global Education Group
0052-9999-12-634-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2292-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-10-1631-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1096-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2783-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-12-037-H01-P 15 (015) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-1095-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3018-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1430-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-821-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1310-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-499-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-296-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Agents of Change Systems and Strategies to Address Family Social and Developmental Needs in the Type 1 Pediatric Populations
Knowledge
Air Pollution Tied to Behavior Issues in Kids (31791)
Knowledge
ASBMR Exercise Builds Kids Bones Insulin Sensitivity (28687)
Knowledge
Assessment and Diagnosis of Pediatric Pain
Knowledge
Autism Drags on Familys Earning Power (31708)
Knowledge
Autism May Have Link to Low Birth Weight (29068)
Knowledge
Autistic Children Slower to Integrate Multiple Stimuli (21789)
Knowledge
Autistic Youth Face Hardship in Post-School Years (32661)
Knowledge
Baby-Led Weaning Improves Food Choices Later (31059)
Knowledge
Babys Flat Head Rarely Requires Helmet Surgery (29948)
Knowledge
BCPP Examination Review and Recertification Course-Pediatric Psychiatric Issues or Disorders Usually First Diagnosed in
Knowledge
Binky Sippy Cup Can be Source of Trip to the ER (32662)
Knowledge
Birth Certificate Problematic With International Adoption (30373)
Knowledge
Birth Control and ADHD Meds Top Rx for Kids (33321)
Knowledge
Breast Diseases May Manifest in Young Drinkers (32080)
Knowledge
Breastfeed Only Goal Missed by Many New Moms (33029)
Knowledge
Breastfeeding Is Health Not Lifestyle Choice (31444)
Knowledge
Breastfeeding Linked to Better Lung Function (31011)
Knowledge
11202012 Page 362 of 417
Run Date 09062012 Page 3 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-152-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-114-H01-P 15 (015) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2573-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-300-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-236-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0372-0000-11-009-H01-P 1 (01) 0372 - Rx School0372-0000-11-009-H01-T 1 (01) 0372 - Rx School0052-9999-12-872-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0204-0000-10-414-H01-P 2 (02) 0204 - American
Society of Health-System
Pharmacists0180-0000-09-107-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-09-119-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-108-H04-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0826-9999-10-028-H01-P 3 (03) 0826 - MED2000 Inc
0826-9999-10-028-H01-T 3 (03) 0826 - MED2000 Inc
0052-9999-12-975-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-021-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-543-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Caffeine Benefits for Preemies Mostly Gone by Age 5 (30715)
Knowledge
Chemotherapy Safety for You and the Patient
Knowledge
Chewing Gum Cuts Ear Infection Risk in Kids (29564)
Knowledge
Child Abuse in One Year Costs Billions in Long Run (31002)
Knowledge
Child Safety Takes a Back Seat During Carpooling (30910)
Knowledge
Childhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChildhood Type 2 Diabetes Awareness Prevention amp Treatment
KnowledgeChoking for Fun Tied to Other Dicey Teen Acts (32188)
Knowledge
Clinical and Economic Considerations in the Use of Inhaled Anesthesia from the Perspective of Health-System Pharmacists and
Knowledge
Clinical Lecture 1 The Role of Biologics in Pediatric Rheumatology
Knowledge
Clinical Lecture I Medication Use during ECMO and Continuous Renal
Knowledge
Clinical Lecture II Management of Pediatric Chemical Casualties Are We Prepared
Knowledge
Combating Childhood Obesity Knowledge
Combating Childhood Obesity Knowledge
Combo Tx Checks Blood Sugar in Diabetic Kids (32412)
Knowledge
Community Care Keeps Autistic Kids Out of Hospital (30483)
Knowledge
Concussion Symptoms Linger in Kids (31501)
Knowledge
11202012 Page 363 of 417
Run Date 09062012 Page 4 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0761-0000-12-006-H05-P 1 (01) 0761 - Educational Review Systems
Inc
0761-0000-12-006-H05-T 1 (01) 0761 - Educational Review Systems
Inc
0530-0000-10-053-H01-P 1 (01) 0530 - Global Education Group
0284-0000-10-024-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0069-0000-11-149-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0180-0000-09-126-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-133-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2510-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2527-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-11-410-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0180-0000-09-100-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-456-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-023-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-10-103-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Confronting the Challenges of Neonatal and Pediatric Medication Safety
Knowledge
Consequences in Not Treating Pain In Children
Knowledge
CPNP 2010 BCPP Literature Analysis Childhood Anxiety and Generalized Anxiety
Knowledge
Current Best Evidence for Education in the Type 2 Pediatric Population
Knowledge
Current Issues in the Management of Pediatric patients with Cystic Fibrosis Update 2009
Knowledge
Deaf Kids Benefit from Implants in Both Ears (30709)
Knowledge
Depressed Dads May Foster Troubled Kids (29473)
Knowledge
Diagnosis of Autism Hit or Miss Along the Spectrum (29490)
Knowledge
Dispensing Pediatric Antibiotic Suspensions
Knowledge
DKA amp HHS Knowledge
Drug May Protect Kids After Stem Cell Transplant (31333)
Knowledge
Early Cochlear Implant Best for Deaf Kids (30498)
Knowledge
Extreme Dosing in CF Aminoglycosides
Knowledge
11202012 Page 364 of 417
Run Date 09062012 Page 5 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-10-105-H04-P 025 (0025) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-10-104-H04-P 025 (0025) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2203-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-341-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-112-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-1937-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-363-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-427-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-014-H01-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0052-9999-12-418-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-249-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2331-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2028-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-507-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-118-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-1042-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-230-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-1917-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Extreme Dosing in OverweightObese Children - Focus on DVT Prophylaxis
Knowledge
Extreme Dosing Case Studies in Pediatric Transplantation
Knowledge
Facebook Posts Can ID Problem Drinkers (28856)
Knowledge
Factors Predict Post-NICU Death in Tiniest Babies (31098)
Knowledge
Fewer Drownings Among Kids Teens (30673)
Knowledge
Fewer Newborns Being Circumcised (28374)
Knowledge
Frequent Moves as Kid Take Toll Later (31135)
Knowledge
Gender Uncertainty Risky for Kids (31268)
Knowledge
Genetic Epidemiology of Early-Onset Depression and Alcohol Use Disorders
Knowledge
Global Infant Mortality Ranking Called Compromised (31250)
Knowledge
Go Slow With Drug Tx for Addicted Newborns (30924)
Knowledge
H Pylori Not a Factor in Adenoid Hyperplasia in Kids (29096)
Knowledge
Hard Times Lead to Hard Knocks for Kids (28587)
Knowledge
Health Risks as Kids High for Old Preemies (31454)
Knowledge
Helms Award Knowledge
High School Kids Report Early Pain Pill Abuse (32557)
Knowledge
Hormone Effect May Be Why Boys Talk Later than Girls (30890)
Knowledge
Hospital Volume Linked to Care of Stomach Flu in Kids (28364)
Knowledge
11202012 Page 365 of 417
Run Date 09062012 Page 6 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-1921-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-124-H04-P 2 (02) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2222-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1283-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0530-0000-10-111-H01-P 1 (01) 0530 - Global
Education Group0284-0000-10-002-H01-P 1 (01) 0284 - College of
Psychiatric and Neurologic
Pharmacists0052-9999-12-226-H05-P 025 (0025) 0052 - Projects In
Knowledge Inc0180-0000-09-120-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-12-612-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2538-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-9999-11-014-H04-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0180-0000-09-105-H04-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1967-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-355-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-979-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2511-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1319-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc
Hospitalized Kids Often Receive Multiple Meds (28362)
Knowledge
Hot Topics Knowledge
HSV Drug Boosts Babies Mental Progress (28896)
Knowledge
Hypothermia Cut Deaths in Infant Encephalopathy (32990)
Knowledge
Idiopathic Chronic Pain Syndromes in Children
Knowledge
In a World of Their Own Diagnosis and Treatment of Autism
Knowledge
Infant Brain Yields Autism Clues (30875)
Knowledge
Infectious Disease - CAMRSA Knowledge
Injury Rates from Stairs Tumble but Kids Still at Risk (31606)
Knowledge
Iron in Formula No Help for Babies With High Hbg (29501)
Knowledge
Irritabilty and Elation The Consequences of Thinking about Pediatric Bipolar Disorder and Severe Mood Dysregulation
Knowledge
Keynote Address National Commission on Children amp Disasters
Knowledge
Kids Cognition May be Harmed by Fired Up Cartoons (28455)
Knowledge
Kids Language Skills Tied to Moms Vitamin D (31145)
Knowledge
Kids Overlooked for Inclusion in Drug Trials (32406)
Knowledge
Kids Still Getting Too Many Antibiotics (29470)
Knowledge
Kids Who Survive Cancer at Risk Later Too (33063)
Knowledge
11202012 Page 366 of 417
Run Date 09062012 Page 7 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-12-111-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-016-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1019-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0284-0000-10-008-H05-P 1 (01) 0284 - College of Psychiatric and
Neurologic Pharmacists
0530-0000-10-110-H01-P 1 (01) 0530 - Global Education Group
0180-0000-09-102-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-09-104-H01-P 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0052-9999-11-2958-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-636-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1044-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-101-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-123-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-12-162-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-782-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-12-1492-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-12-404-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
Lead Exposure High in Refugee Camps (30676)
Knowledge
Lipitor No Help in Kids With SLE (30470)
Knowledge
Long Pregnancy Tied to Kids Behavior Issues (32488)
Knowledge
Long Term Effect of In-Utero Exposure to Psychotropic Medications
Knowledge
Management of Chronic Daily Headache in Children
Knowledge
Management of Diabetes Type I Knowledge
Management of Diabetes Type II Knowledge
Medical Home Model Serves Children Well (30290)
Knowledge
Moms Meth Use May Affect Kids Behavior (31704)
Knowledge
Moms Often Blind to Toddlers Weight (32555)
Knowledge
Mortality High in Native Alaskan Infants (30646)
Knowledge
NarcoticsSedationNAS etc Knowledge
Neuro Impairment Among Kids More Common (30751)
Knowledge
No Outdoor Play for Many Kids (31977)
Knowledge
Older Dads Likely to Sire Couch Potato Kids (33445)
Knowledge
OTC Medications for Children with Allergies A Review for Pharmacy Technicians
Knowledge
11202012 Page 367 of 417
Run Date 09062012 Page 8 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-12-205-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0422-0000-10-403-H01-T 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0022-0000-12-017-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-12-874-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-11-500-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-500-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-502-H01-P 075 (0075) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-502-H01-T 075 (0075) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-501-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0180-0000-11-501-H01-T 1 (01) 0180 - Pediatric
Pharmacy Advocacy Group
0180-0000-11-040-H01-P 25 (025) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-407-H01-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center
OTC Options for Treating Pediatric Allergic Rhinitis
Knowledge
Pain Management in Babies and Children Practical Considerations for Pharmacy Technicians
Knowledge
Pandemic Response Strategies Knowledge
Parasite Duo to Blame in Infant Toxoplasmosis (32184)
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Anatomic and Physiologic Differences Between Children and
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-Based Competency Fluids Electrolytes and Dehydration in Children
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-based Competency Pharmacokinetic Differences between Children and Adults
Knowledge
Pediatric Aged-Based Competency Physiologic and Pharmacokinetic Differences in Children Fluids and
Knowledge
Pediatric Asthma A Disease and Treatment Review for Technicians
Knowledge
11202012 Page 368 of 417
Run Date 09062012 Page 9 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-11-209-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0761-9999-11-081-H05-P 15 (015) 0761 - Educational Review Systems
Inc
0180-0000-10-101-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0422-0000-11-205-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-11-404-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-625-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0422-0000-10-319-H04-P 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0422-0000-10-319-H04-T 1 (01) 0422 -
Pharmacists Letter Therapeutic
Research Center0052-9999-12-289-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-014-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0052-9999-12-463-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-026-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-3017-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
Pediatric Asthma Disease Review and Treatment
Knowledge
Pediatric Medication Safety The Physician and Pharmacist Perspective
Knowledge
Pediatric Parental Nutrition Knowledge
Pediatric Pharmacy Practice An Introduction for Pharmacists
Knowledge
Pediatric Pharmacy An Introduction for Pharmacy Technicians
Knowledge
Peer Counseling Helps Parents and Kids (31679)
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Pharmacys Role in the Fight Against Childhood Obesity
Knowledge
Physical Child Abuse Sends Thousands to Hospitals (31022)
Knowledge
Planning and Coordination for Child-Focused Pandemic Response
Knowledge
Play Ball but Be Safe Say Pediatricians (31376)
Knowledge
Playgrounds Too Safe to Keep Little Kids Active (30493)
Knowledge
Playtime is More than Fun and Games (30390)
Knowledge
11202012 Page 369 of 417
Run Date 09062012 Page 10 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0422-0000-10-225-H01-P 1 (01) 0422 - Pharmacists Letter
Therapeutic Research Center
0052-9999-11-2191-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2067-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-09-033-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0052-9999-12-303-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1003-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0180-0000-09-103-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-2184-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0052-9999-11-2256-H04-P 025 (0025) 0052 - Projects In
Knowledge Inc0022-0000-12-015-H04-P 1 (01) 0022 - University of
Kentucky College of Pharmacy
0294-9999-11-126-H04-P 1 (01) 0294 - VCU School of Pharmacy Office
of Continuing Education
0052-9999-12-991-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0216-0000-10-075-H01-P 2 (02) 0216 - American Society for
Parenteral and Enteral Nutrition
Inc
Practical Considerations for Pediatric Pain Management
Knowledge
Preemies Breathe Easier With Less Invasive Therapy (28827)
Knowledge
Preemies Have Higher Mortality Risk as Young Adults (28639)
Knowledge
Prevention and Management of RSV Bronchiolitis
Knowledge
Program Puts Smackdown on Bullying (31040)
Knowledge
Pulse-Ox Works as Heart Defect Screen (32460)
Knowledge
Pumps Pens amp Other Devices Knowledge
Repeat Anesthesia for Tots May Lead to Learning Disabilities
Knowledge
Repeat UTI in Kids May Not Up Risk of Kidney Disease (28962)
Knowledge
Risk Communication for Child-Focused Pandemic Response
Knowledge
Roaoke Carillion Pediatric Advanced Life Support What Pharmacists Need to Know
Knowledge
Second-Hand Smoke Worsens Asthma in Kids (32430)
Knowledge
Self Assessment Online Module V V2 Considerations in Nutrition Support of the Pediatric Patient
Knowledge
11202012 Page 370 of 417
Run Date 09062012 Page 11 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0052-9999-11-2798-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-356-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2027-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2290-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-027-H04-P 125 (0125) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-409-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-196-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-512-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1272-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-770-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1280-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-285-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-1382-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-511-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2227-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-11-2962-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0096-0000-10-056-H04-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
Sexting Not Very Widespread Among Kids Teens (30009)
Knowledge
Shhh The Kids Need More Sleep -- Or Do They (31143)
Knowledge
Short or Long Parents Like Well-Child Visits (28568)
Knowledge
Shy Teens May Be More than Wallflowers (29073)
Knowledge
Sids Risk Reduction A Continuing Education Program for Pharmacists
Knowledge
Signs of Autism Show Up on MRI at 6 Months of Age (31242)
Knowledge
Ski Helmets Not Best for Sledding (30826)
Knowledge
Snoring Tots More Likely to Turn into Troubled Kids (31477)
Knowledge
Social Ties Move Kids to Exercise (32951)
Knowledge
Some Autistic Kids Make Gains as Late Bloomers (31963)
Knowledge
Soy Formula Has No Effect on Babys Cognition (32960)
Knowledge
Spanking No Help in Child-Rearing (31030)
Knowledge
Study Shows Even Little Kids Can Be Cutters (33184)
Knowledge
Teen Binging Tied to Drinking on Silver Screen (31484)
Knowledge
Teens Drink Smoke Less in Caring Communities (28891)
Knowledge
Texting May Turn Teens Off Alcohol (30285)
Knowledge
The ABCs of OTCs in Children Knowledge
11202012 Page 371 of 417
Run Date 09062012 Page 12 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0430-0000-11-006-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0096-0000-10-069-H01-P 1 (01) 0096 - Texas Tech University Health Sciences Center
School of Pharmacy
0430-0000-11-021-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0069-0000-11-140-H01-P 15 (015) 0069 - American Association of
Diabetes Educators
0430-0000-10-042-H01-P 2 (02) 0430 - Postgraduate
Healthcare Education LLC
0052-9999-11-3006-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-977-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0144-9999-11-075-H01-P 1 (01) 0144 - Maryland Pharmacy Continuing Education
Coordinating Council
0052-9999-12-768-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0052-9999-12-852-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
0022-0000-12-016-H04-P 1 (01) 0022 - University of Kentucky College
of Pharmacy
0052-9999-11-2899-H04-P 025 (0025) 0052 - Projects In Knowledge Inc
The Prevention and Treatment of Whooping Cough
Knowledge
The Terrible Twos Type 2 Diabetes in Children
Knowledge
Title Over-the-counter Treatment of Pediatric Allergic Rhinitis Review of Traditional and Natural Approaches
Knowledge
Transitioning Points in Students Lives - Navigating the Journey with Diabetes
Knowledge
Treatment of Otitis Media Knowledge
Truancy Signals Depression in Kids (30364)
Knowledge
TV Ads Linked to Unhealthy Diets in Young Adults (32408)
Knowledge
UPdated Clinical Practice Guideline on the Management of Head Lice Infestation in Children
Knowledge
Urine Odor Signals UTI in Infants (31966)
Knowledge
Vitamin D Not Tied to School Performance (32142)
Knowledge
Workforce Development and Care in Pandemic Planning
Knowledge
Worlds Smallest Newborns Still Small but Fine (30185)
Knowledge
11202012 Page 372 of 417
Run Date 09062012 Page 13 of 13
PLAN Search ResultsAccreditation Council for Pharmacy
Education20 North Clark Street Suite 2500 Chicago Illinois 60602-5109
Phone (312) 664-3575 Fax (312) 664-7008 httpwwwacpe-accreditorg
0180-0000-09-106-H01-P 1 (01) 0180 - Pediatric Pharmacy
Advocacy Group0052-9999-11-1941-H04-P 025 (0025) 0052 - Projects In
Knowledge IncYanking Adenoids Wont Cut Colds in Kids (28379)
Knowledge
Yaffe Award Lecture Knowledge
11202012 Page 373 of 417
Martine13 Antell13 PharmD13 Amplatz13 Childrens13 Hospital13 Minneapolis13 Minnesota13 13 13 13 Chris13 Shaffer13 PharmD13 MS13 BCPS13 Coordinator13 Personalized13 Pediatric13 Medicine13 Program13 University13 of13 Nebraska13 Medical13 Center13 98604513 Nebraska13 Medical13 Center13 Omaha13 Nebraska13 13 689198-shy‐604513 13 Kathryn13 Timberlake13 PharmD13 Clinical13 Pharmacy13 Specialist13 Antimicrobial13 Stewardship13 The13 Hospital13 for13 Sick13 Children13 55513 University13 Ave13 Toronto13 Canada13 13 Ashley13 Reilly13 PharmD13 Clincial13 Pharmacy13 Specialist13 -shy‐13 NICU13 University13 of13 Colorado13 Hospital13 1260513 East13 16th13 Ave13 Aurora13 Colorado13 13 8004513 13 Michelle13 Condren13 PharmD13 AE-shy‐C13 CDE13 Department13 Chair13 and13 Associate13 Professor13 University13 of13 Oklahoma13 College13 of13 Pharmacy13 450213 E13 41st13 St13 Tulsa13 Oklahoma13 13 7413513 13 Malgorzata13 Michalowska-shy‐Suterska13 PharmD13 Pediatric13 Clinical13 Pharmacy13 Specialist13 Westchester13 Medical13 Center13 10013 Woods13 Rd13 Valhalla13 New13 York13 13 1059513 13 Bernard13 Lee13 PharmD13 BCPS13 PGY113 Residency13 Program13 Director13 Mayo13 Eugenio13 Litta13 Childrens13 Hospital13 20013 First13 Ave13 SW13 Rochester13 Minnesota13 13 5590513 13 Erika13 Bergeron13 PharmD13 Pediatric13 Clinical13 Pharmacist13 Harris13 County13 Hospital13 District13 565613 Kelley13 St13
Houston13 Texas13 13 7702613 Matthew13 Gentry13 PharmD13 Pediatric13 Infectious13 Diseases13 Pharmacist13 CHOC13 Childrens13 Hospital13 45513 Main13 Street13 Orange13 California13 13 9286813 13 Lizbeth13 Hansen13 PharmD13 BCPS13 Pediatric13 Clinical13 Pharmacist13 University13 of13 MN13 Amplatz13 Childrens13 Hospital13 245013 Riverside13 Avenue13 Minneapolis13 Minnesota13 13 5545413 13 Rachel13 Meyers13 PharmD13 BCPS13 Clinical13 Assistant13 Professor13 Ernest13 Mario13 School13 of13 Pharmacy13 Rutgers13 University13 16013 Frelinghuysen13 Rd13 Piscataway13 New13 Jersey13 13 0885413 13 Kay13 Green13 RPh13 BCPS13 Clinical13 Specialist13 NICU13 PGY113 Residency13 Coordinator13 CE13 Administrator13 University13 Hospital13 450213 Medical13 Drive13 San13 Antonio13 Texas13 13 7822013 13 Kelly13 Pulte13 PharmD13 ICU13 Clinical13 Pharmacist13 Childrens13 Medical13 Center13 193513 Medical13 District13 Drive13 Dallas13 Texas13 13 7521913 13 Elizabeth13 Beckman13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 University13 of13 Michigan13 CS13 Mott13 Childrens13 Hospital13 154013 E13 Hospital13 Dr13 Ann13 Arbor13 Michigan13 13 4810913 13 Kelli13 Crowley13 PharmD13 BCPS13 Clinical13 Pharmacy13 Specialist13 Pediatric13 Intensive13 Care13 Childrens13 Hospital13 of13 Pittsburgh13 of13 UPMC13 440113 Penn13 Ave13 Pittsburgh13 Pennsylvania13 13 1522413
13 13
11202012 Page 417 of 417
- Petition Introduction FINAL
- Pediatrics Executive Summary - FINAL 10 31 12 V6
- Criterion A - Need 10 31 12 FINAL
- Criterion B - Demand 10 31 12 FINAL
- Criterion C - Number and Time 10 31 12 FINAL
- Criterion D - Specialized Knowledge 10 31 12 FINAL
- Criterion E - Functions 10 31 12 FINAL
- Criterion F Education and Training 10 31 12 FINAL
- Criterion G Transmission of Knowledge 10 31 12 FINAL
- Appendix B-1 Cover
- Appendix B-1 - Letters of Support
-
- Letter of Support - Benjamin
- Letter of Support - Block
- Letter of Support - Greene
- Letter of Support - Jerry
- Letter of Support - Jew
- Letter of Support - Kearns
- Letter of Support - Levine
- Letter of Support - Luten
- Letter of Support - Miller
- Letter of Support - Von Kohorn
-
- Appendix C-1 Cover
- Appendix C-1 Pediatric Pharmacist Survey
- Appendix D-1 Cover
- Appendix D-1 Pediatric Role Delineation Study
- Appendix D-2 Cover
- Appendix D-2 NAPLEX Blueprint
- Appendix F-1 Cover
- Appendix F-1 ASHP PGY2 Pharmacy Residencies in Pediatrics
- Appendix F-2 Cover
- Appendix F-2 ACCP Guidelines for Clinical Research Fellowship Training Programs
- Appendix G-1 Cover
- Appendix G-1 Pediatrics Bibliography
- Appendix G-2 Cover
- Appendix G-2 Selected Pediatric Literature
-
- 11 J of Rural Health Benavides A clinical rx roles in screening for Metabolic syndrome on a rural ped am clinic
- 09 The Joint Commis J of Quality and Pt Safety Gardner Pharmacists Med Rec - Related Clin Interventions in a Childrens Hosp
- 09 Paediatric Drugs Gazarian Training Ped Clin Pharmcol Therapeu_Specialists_of_the Future The Needs The Reality Opportun for intl Ntwrkng
- 08 Pediatric Cardiology Moffett Medication dosing and renal insufficiency in a pediatric cardiac intensive care unit- impact of pharmacist consultation
-
- Medication Dosing and Renal Insufficiency in a Pediatric Cardiac Intensive Care Unit Impact of Pharmacist Consultation
-
- Abstract
- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- Acknowledgments
- References
-
- 08 Kaushel AJHP Unit-based clinical pharmacists prevention of serious medication errors in pediatric inpatients
- 07 AJHP Costello Effects of a pharmacist-led pediatrics medication safety team on med error reporting
- 06 The Annals Nahata Evolution of Ped Clin RX
- 04 Pediatrics Potts Computerized Physician Order Entry and Med Errors in a Pediatric Critical Care Unit
- 02 Crit Care Med Krupicka Impact of a pediatric clinical pharmacist in the pediatric intensive care unit
- 01 AJHP Hahn Survey of pharmaceutical services in pediatric resuscitation
-
- Appendix G-3 Cover
- Appendix G-3 ACPE PLAN Programming - LIVE Knowledge
- Appendix G-4 Cover
- Appendix G-4 ACPE PLAN Programming - LIVE Application
- Appendix G-5 Cover
- Appendix G-5 ACPE PLAN Programming - HOMESTUDY Knowledge
- Appendix G-6 Cover
- Appendix G-6 ACPE PLAN Programming - HOMESTUDY Application
- Appendix G-7 Cover
- Appendix G-7 Sample Educational Program Materials
-
- 2009 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Annual Conference Handouts-Materials
- 2010 PPAG Specialty Conference Handouts-Materials
- 2011 PPAG Annual Conference Handouts-Materials
-
- Final Signature List Cover
- FINAL Signature List
-